Log in using your username and password
- Search More Search for this keyword Advanced search
- Latest content
- Current issue
- Write for Us
- BMJ Journals More You are viewing from: Google Indexer

You are here
- Volume 24, Issue 4
- Understanding and interpreting regression analysis
- Article Text
- Article info
- Citation Tools
- Rapid Responses
- Article metrics
- http://orcid.org/0000-0002-7839-8130 Parveen Ali 1 , 2 ,
- http://orcid.org/0000-0003-0157-5319 Ahtisham Younas 3 , 4
- 1 School of Nursing and Midwifery , University of Sheffield , Sheffield , South Yorkshire , UK
- 2 Sheffiled University Interpersonal Violence Research Group , The University of Sheffiled SEAS , Sheffield , UK
- 3 Faculty of Nursing , Memorial University of Newfoundland , St. John's , Newfoundland and Labrador , Canada
- 4 Swat College of Nursing , Mingora, Swat , Pakistan
- Correspondence to Ahtisham Younas, Memorial University of Newfoundland, St. John's, NL A1C 5S7, Canada; ay6133{at}mun.ca
https://doi.org/10.1136/ebnurs-2021-103425
Statistics from Altmetric.com
Request permissions.
If you wish to reuse any or all of this article please use the link below which will take you to the Copyright Clearance Center’s RightsLink service. You will be able to get a quick price and instant permission to reuse the content in many different ways.
- statistics & research methods
Introduction
A nurse educator is interested in finding out the academic and non-academic predictors of success in nursing students. Given the complexity of educational and clinical learning environments, demographic, clinical and academic factors (age, gender, previous educational training, personal stressors, learning demands, motivation, assignment workload, etc) influencing nursing students’ success, she was able to list various potential factors contributing towards success relatively easily. Nevertheless, not all of the identified factors will be plausible predictors of increased success. Therefore, she could use a powerful statistical procedure called regression analysis to identify whether the likelihood of increased success is influenced by factors such as age, stressors, learning demands, motivation and education.
What is regression?
Purposes of regression analysis.
Regression analysis has four primary purposes: description, estimation, prediction and control. 1 , 2 By description, regression can explain the relationship between dependent and independent variables. Estimation means that by using the observed values of independent variables, the value of dependent variable can be estimated. 2 Regression analysis can be useful for predicting the outcomes and changes in dependent variables based on the relationships of dependent and independent variables. Finally, regression enables in controlling the effect of one or more independent variables while investigating the relationship of one independent variable with the dependent variable. 1
Types of regression analyses
There are commonly three types of regression analyses, namely, linear, logistic and multiple regression. The differences among these types are outlined in table 1 in terms of their purpose, nature of dependent and independent variables, underlying assumptions, and nature of curve. 1 , 3 However, more detailed discussion for linear regression is presented as follows.
- View inline
Comparison of linear, logistic and multiple regression
Linear regression and interpretation
Linear regression analysis involves examining the relationship between one independent and dependent variable. Statistically, the relationship between one independent variable (x) and a dependent variable (y) is expressed as: y= β 0 + β 1 x+ε. In this equation, β 0 is the y intercept and refers to the estimated value of y when x is equal to 0. The coefficient β 1 is the regression coefficient and denotes that the estimated increase in the dependent variable for every unit increase in the independent variable. The symbol ε is a random error component and signifies imprecision of regression indicating that, in actual practice, the independent variables are cannot perfectly predict the change in any dependent variable. 1 Multiple linear regression follows the same logic as univariate linear regression except (a) multiple regression, there are more than one independent variable and (b) there should be non-collinearity among the independent variables.
Factors affecting regression
Linear and multiple regression analyses are affected by factors, namely, sample size, missing data and the nature of sample. 2
Small sample size may only demonstrate connections among variables with strong relationship. Therefore, sample size must be chosen based on the number of independent variables and expect strength of relationship.
Many missing values in the data set may affect the sample size. Therefore, all the missing values should be adequately dealt with before conducting regression analyses.
The subsamples within the larger sample may mask the actual effect of independent and dependent variables. Therefore, if subsamples are predefined, a regression within the sample could be used to detect true relationships. Otherwise, the analysis should be undertaken on the whole sample.
Building on her research interest mentioned in the beginning, let us consider a study by Ali and Naylor. 4 They were interested in identifying the academic and non-academic factors which predict the academic success of nursing diploma students. This purpose is consistent with one of the above-mentioned purposes of regression analysis (ie, prediction). Ali and Naylor’s chosen academic independent variables were preadmission qualification, previous academic performance and school type and the non-academic variables were age, gender, marital status and time gap. To achieve their purpose, they collected data from 628 nursing students between the age range of 15–34 years. They used both linear and multiple regression analyses to identify the predictors of student success. For analysis, they examined the relationship of academic and non-academic variables across different years of study and noted that academic factors accounted for 36.6%, 44.3% and 50.4% variability in academic success of students in year 1, year 2 and year 3, respectively. 4
Ali and Naylor presented the relationship among these variables using scatter plots, which are commonly used graphs for data display in regression analysis—see examples of various scatter plots in figure 1 . 4 In a scatter plot, the clustering of the dots denoted the strength of relationship, whereas the direction indicates the nature of relationships among variables as positive (ie, increase in one variable results in an increase in the other) and negative (ie, increase in one variable results in decrease in the other).
- Download figure
- Open in new tab
- Download powerpoint
An Example of Scatter Plot for Regression.
Table 2 presents the results of regression analysis for academic and non-academic variables for year 4 students’ success. The significant predictors of student success are denoted with a significant p value. For every, significant predictor, the beta value indicates the percentage increase in students’ academic success with one unit increase in the variable.
Regression model for the final year students (N=343)
Conclusions
Regression analysis is a powerful and useful statistical procedure with many implications for nursing research. It enables researchers to describe, predict and estimate the relationships and draw plausible conclusions about the interrelated variables in relation to any studied phenomena. Regression also allows for controlling one or more variables when researchers are interested in examining the relationship among specific variables. Some of the key considerations are presented that may be useful for researchers undertaking regression analysis. While planning and conducting regression analysis, researchers should consider the type and number of dependent and independent variables as well as the nature and size of sample. Choosing a wrong type of regression analysis with small sample may result in erroneous conclusions about the studied phenomenon.
Ethics statements
Patient consent for publication.
Not required.
- Montgomery DC ,
- Schneider A ,
Twitter @parveenazamali, @@Ahtisham04
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.
Read the full text or download the PDF:

- Update librarian
Key Features
New features.
The combination from theory and applied exercises with detailed answers is very helpfull to support students transferring knwoledge in to practice
This is a well organised and provides undergraduate students with a clear understanding of statistics.
An excellent resource in statistics in health and social sciences which is also useful in physiotherapy studies; easy to read and follow and will highly recommend to students, educators and academics.
Good text for understanding statistics
Thank you. very essential
I think this book cover most of statistical subjects.
En la Facultad de Medicina Veracruz de la Universidad Veracruzana llevamos la EE Estadística por lo cual requiero revisar el libro para ver si reúne las características para se llevado al curso Agradezco el envío
Gives very good grounding in stats for year 4 and MSc students
Great for research students
Exactly what I need
Please verify your email.
We've sent you an email. Please follow the link to reset your password.
You can now close this window.
Edits have been made. Are you sure you want to exit without saving your changes?

Interpreting statistical significance in nursing research
Don’t let p values distract you from scientific reasoning..
- P values are useful to report the results of inferential statistics, but they aren’t a substitute for scientific reasoning.
- After a statistical analysis of data, the null hypothesis is either accepted or rejected based on the P value.
- Reading statistical results includes summary statistics (descriptive statistics), test statistics, and P value with other considerations such as one-tailed or two-tailed test, and sample size.
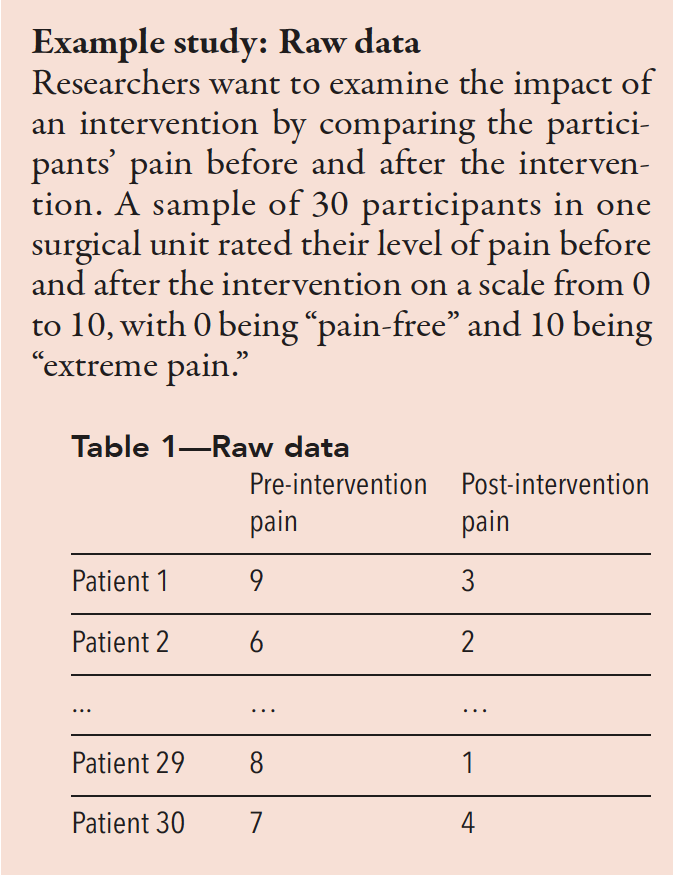
Improper interpretation of statistical analysis can lead to abuse or misuse of results. We draw valid interpretations when data meet fundamental assumptions and when we evaluate the probability of errors. Statistical analysis requires knowledge for proper interpretation, which relies on considering the null hypothesis, two-tailed or one-tailed tests, study power, type I and type II errors, and statistical vs. clinical significance. In many domains, including nursing, statistical significance ( P value) serves as an important threshold for interpretation, whether the result is statistically significant or not. However, statistical significance frequently is misunderstood and misused.
Statistical test components
In empirical research, all statistical tests begin with the null hypothesis and end with a test statistic and the associated statistical significance. A test of statistical significance determines the likelihood of a result assuming a null hypothesis to be true. Depending on the selected statistical analysis, researchers will use Z scores, t tests, or F tests. Although three methods exist for testing hypotheses (confidence intervals [CIs], P values, and critical values), essentially the P value serves as the significance level. Many researchers consider P values the most important summary of an inferential statistical analysis.
Null hypothesis
Before conducting a study, researchers propose a null hypothesis, which begins with an initial idea they want to demonstrate. It guides the statistical analysis and predicts the direction and nature of study results. Traditionally, a null hypothesis proposes no difference between two variables being studied or the characteristics of a population. An alternative hypothesis states a result that’s either not equal to, greater than, or less than the null hypothesis.
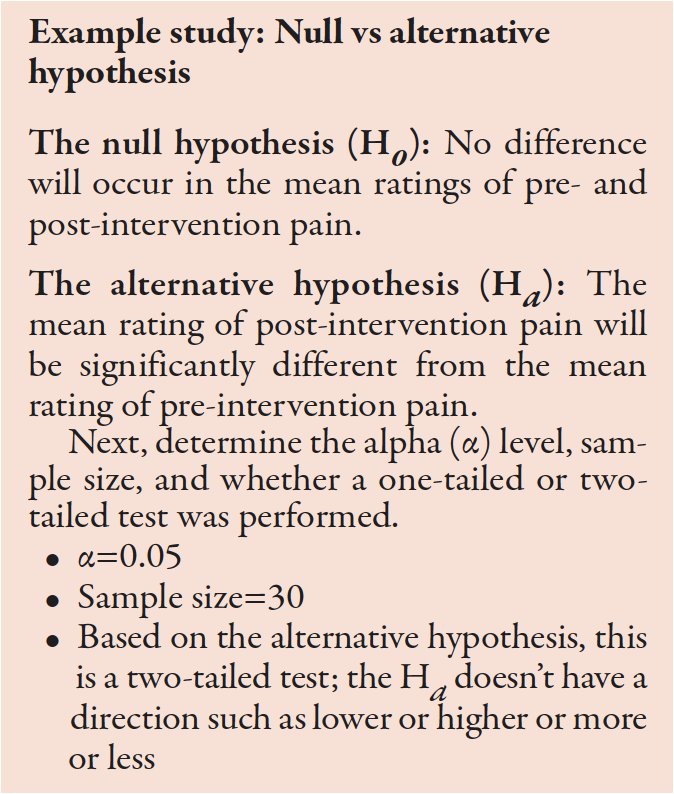
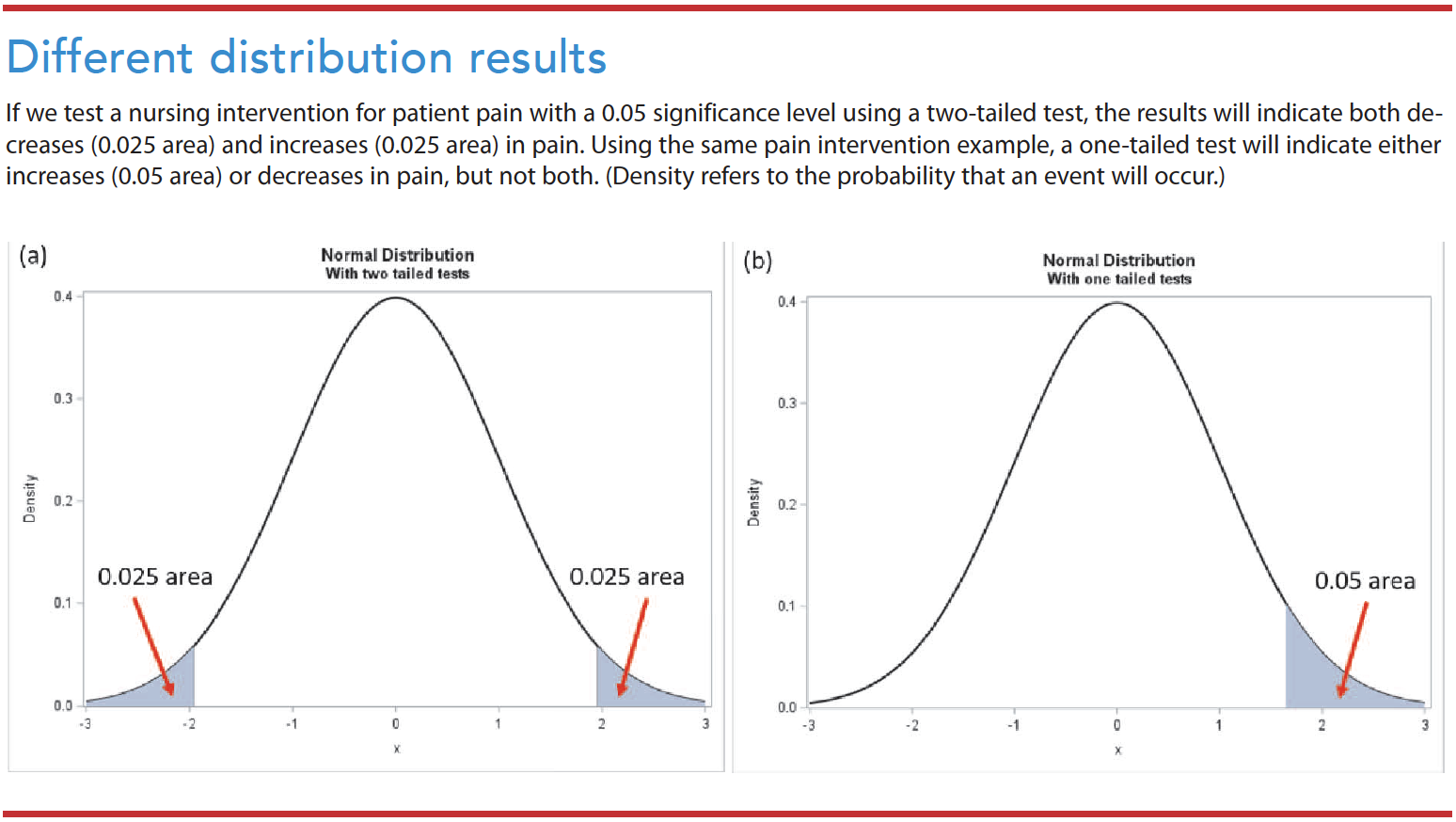
Two-tailed test vs. one-tailed test
Researchers commonly check a null hypothesis or statistical significance using a two-tailed test, which postulates that the sample mean is equal or unequal to the population. A one-tailed test postulates that the sample mean is higher or lower than the population mean. Nursing researchers rarely use a one-tailed test because of the consequences of missing an effect. (See Different distribution results .)
Study power and type I/type II errors
The possibility of error exists when testing a hypothesis. Type I errors (false alarms) occur when we reject a null hypothesis that’s true. Type II errors (misses) occur when we accept a null hypothesis that’s false. Sample size can influence the power of the study. For example, even small treatment effects can appear statistically significant in a large sample.
The alpha (α)—the probability of a type I error—refers to the likelihood that the truth lies outside the confidence interval (CI). The smaller the α, the smaller the area where we would reject the null hypothesis, which reduces the chance that will occur. The most widely acceptable α cutoff in nursing research is 0.05. Keep in mind that the confidence level and α are analogous. If the α=0.05, the confidence level is 95%. If α=0.01, the confidence level is 99%.
Confidence interval
A CI provides an idea of the range within which a value might occur by chance. It indicates the strength of the estimate by providing a range of uncertainty. Frequently, researchers use CIs without a dichotomous result of the P value. Consider the following example: On a scale between 0 and 10, patients with an advanced illness reported an average pain score of between 4.1 and 6.3 (95% CI: 4.1 to 6.3). With a 95% CI, researchers risk being wrong 5 out of 100 times.
Statistical vs. clinical significance
Statistical significance indicates the study results’ confidence in probability, while the clinical significance reflects its impact on clinical practice. Measures of statistical significance quantify the probability that a study result is due to chance rather than a real treatment effect. On the other hand, clinical significance indicates the magnitude of the actual treatment effect or impact in nursing practice.
Consider this example: Researchers compare two groups (exercise group and diet group). The mean body weight of subjects after treatment with exercise is 1 pound lower than after treatment with diet. The difference between these groups could be statistically significant, with a P value of <0.05. However, the clinical implications of a 1 pound weight loss wouldn’t be clinically significant. In this example, the mean weight—172 pounds (exercise group) vs. 173 pounds (diet group), P =0.04—is statistically significant . The 0.04 P value means only a 4% chance exists that this observed weight difference occurred randomly. However, the clinical significance of a 1 pound difference between the groups would be considered small and not clinically significant.
The results section of a quantitative research study report includes names of statistical tests, the value of the calculated statistics, and the statistical significance ( P value). After a statistical analysis of data, the null hypothesis is either accepted or rejected based on the P value. For example, if a report indicates a significant finding at the 0.05 probability level (α=0.05), the findings might have an error 5% of the time (only 5 out of 100) and a 95% confidence that the results aren’t erroneous after repeated testing. (See P value examples.)
Study example: Reading results and tables
Use the mean to understand the center of the data. Most statistical analyses use the mean and/or median for a central tendency. Also, use the standard deviation (SD) to understand how widely spread the data are from the mean. As shown in Table 2, the mean of pre-intervention pain is 7.2, while the mean of post-intervention pain is 4.6. The SD in pre-intervention pain is 1.4, and the SD in post-intervention pain is 1.8. A higher SD value indicates a greater spread in the data.
Table 2—The mean and SD of pre- and post-intervention pain for 30 patients
Table 3 shows a mean difference between pre- and post-intervention pain of 2.5667. Based on the t-test results, the t score is 7.92. The confidence interval (CI) is 95% for the mean difference, with pre- and post-intervention pain scores ranging from 1.41 to 2.39.
Table 3—Paired samples t-test of change score
95% CI of the difference
Next, find the associated P values
- If P <α (0.05), reject the H 0 and accept the H α .
- If P >α (0.05), accept the H 0 .
In this example, P <0.001, which means the Ho can be rejected. We accept the H α that the mean post-intervention pain score is significantly different from the mean pre-intervention pain score.
Interpreting statistical results
Reading and interpreting statistical results includes summary statistics (descriptive statistics), test statistics, and P value with other considerations such as one-tailed or two-tailed test, sample size, and multiple comparisons. We must not only understand the decision to accept or reject a hypothesis based on a test used, but also understand the descriptive statistics and other considerations such as normality and equal variance. For complex statistics, tables provide the most effective way to view the results.
Rely on scientific reasoning
Quantitative nursing research uses a testing hypothesis in decision making. P values are useful for reporting the results of inferential statistics, but we must be aware of their limitations. The P value isn’t the probability that the null hypothesis is true but the probability of the test statistics against a null hypothesis. It measures the compatibility of data with the null hypothesis but can’t reveal whether an alternative hypothesis is true. Also keep in mind that the 0.05 significance level is merely a convention. Researchers commonly use it as a threshold whether it’s statistically significant or not.
P values were never intended as a substitute for scientific reasoning. All results should be interpreted in the context of the research design (sample size, measurement validity or reliability, and study design rigor).
Joohyun Chung is a biostatistician and assistant professor at the University of Massachusetts Elaine Marieb College of Nursing in Amherst.
American Nurse Journal. 2023; 18(2). Doi: 10.51256/ANJ022345;
Key words: P value, statistical significance, significance level
Andrade C. The P value and statistical significance: Misunderstandings, explanations, challenges, and alternatives. Indian J Psychol Med. 2019;41(3):210-5. doi:10.4103/IJPSYM.IJPSYM_193_19
Cook C. Five per cent of the time it works 100 per cent of the time: The erroneousness of the P value. J Man Manip Ther. 2010;18(3):123-5. doi:10.1179/106698110X12640740712257
Heavey E. Statistics for Nursing: A Practical Approach. 3rd ed. Burlington, MA: Jones & Bartlett Learning; 2018.
Houser J. Nursing Research: Reading, Using, and Creating Evidence . 4th ed. Burlington, MA: Jones & Bartlett Learning; 2018.
Ioannidis JPA. The importance of predefined rules and prespecified statistical analyses: Do not abandon significance. JAMA . 2019;321(21):2067-8. doi:10.1001/JAMA.2019.4582
Polit DF, Beck CT. Essentials of Nursing Research: Appraising Evidence for Nursing Practice . 10th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2021.
Ranganathan P, Pramesh CS, Buyse M. Common pitfalls in statistical analysis: Clinical versus statistical significance. Perspect Clin Res . 2015;6(3):169-70. doi:10.4103/2229-3485.159943
Wasserstein RL, Lazar NA. The ASA statement on p -values: Context, process, and purpose. Am Stat . 2016;70(2):129-33. doi:10.1080/00031305.2016.1154108
Let Us Know What You Think
Leave a reply cancel reply.
Your email address will not be published. Required fields are marked *
Post Comment

NurseLine Newsletter
- First Name *
- Last Name *
- Hidden Referrer
*By submitting your e-mail, you are opting in to receiving information from Healthcom Media and Affiliates. The details, including your email address/mobile number, may be used to keep you informed about future products and services.
Test Your Knowledge
Recent posts.

Powerful peer-to-peer networks

Knowledge of intravascular determination

Why Mentorship?

Virtual reality: Treating pain and anxiety

What is a healthy nurse?
Nurses make the difference

From data to action

Connecting theory and practice

Turning the tide

Effective clinical learning for nursing students

Leadership style matters

Innovation in motion

Nurse referrals to pharmacy

Lived experience

Elevating the voice of nurses through advocacy
Chung J. Interpreting statistical significance in nursing research. American Nurse Journal. 2023;18(2):45-48. doi:10.51256/anj022345 https://www.myamericannurse.com/interpreting-statistical-significance-in-nursing-research/
Click through the PLOS taxonomy to find articles in your field.
For more information about PLOS Subject Areas, click here .
Loading metrics
Open Access
Peer-reviewed
Research Article
The development and structural validity testing of the Person-centred Practice Inventory–Care (PCPI-C)
Contributed equally to this work with: Brendan George McCormack, Paul F. Slater, Fiona Gilmour, Denise Edgar, Stefan Gschwenter, Sonyia McFadden, Ciara Hughes, Val Wilson, Tanya McCance
Roles Conceptualization, Data curation, Formal analysis, Methodology, Project administration, Validation, Writing – original draft, Writing – review & editing
* E-mail: [email protected]
Affiliation Faculty of Medicine and Health, Susan Wakil School of Nursing and Midwifery/Sydney Nursing School, The University of Sydney, Camperdown Campus, New South Wales, Australia
Roles Formal analysis, Methodology, Writing – original draft, Writing – review & editing
Affiliation Institute of Nursing and Health Research, Ulster University, Belfast, Northern Ireland
Roles Data curation, Investigation, Methodology, Writing – review & editing
Affiliation Division of Nursing, Queen Margaret University, Edinburgh, Scotland
Roles Data curation, Formal analysis, Writing – review & editing
Affiliation Nursing and Midwifery Directorate, Illawarra Shoalhaven Local Health District, New South Wales, Australia
Roles Data curation, Methodology, Validation, Writing – review & editing
Affiliation Division of Nursing Science with Focus on Person-Centred Care Research, Karl Landsteiner University of Health Sciences, Krems, Austria
Roles Data curation, Investigation, Validation, Writing – review & editing
Affiliation Prince of Wales Hospital, South East Sydney Local Health District, New South Wales, Australia
Roles Conceptualization, Formal analysis, Methodology, Validation, Writing – original draft, Writing – review & editing
- Brendan George McCormack,
- Paul F. Slater,
- Fiona Gilmour,
- Denise Edgar,
- Stefan Gschwenter,
- Sonyia McFadden,
- Ciara Hughes,
- Val Wilson,
- Tanya McCance
- Published: May 10, 2024
- https://doi.org/10.1371/journal.pone.0303158
- Reader Comments
Person-centred healthcare focuses on placing the beliefs and values of service users at the centre of decision-making and creating the context for practitioners to do this effectively. Measuring the outcomes arising from person-centred practices is complex and challenging and often adopts multiple perspectives and approaches. Few measurement frameworks are grounded in an explicit person-centred theoretical framework.
In the study reported in this paper, the aim was to develop a valid and reliable instrument to measure the experience of person-centred care by service users (patients)–The Person-centred Practice Inventory-Care (PCPI-C).
Based on the ‘person-centred processes’ construct of an established Person-centred Practice Framework (PCPF), a service user instrument was developed to complement existing instruments informed by the same theoretical framework–the PCPF. An exploratory sequential mixed methods design was used to construct and test the instrument, working with international partners and service users in Scotland, Northern Ireland, Australia and Austria. A three-phase approach was adopted to the development and testing of the PCPI-C: Phase 1 –Item Selection : following an iterative process a list of 20 items were agreed upon by the research team for use in phase 2 of the project; Phase 2 –Instrument Development and Refinement : Development of the PCPI-C was undertaken through two stages. Stage 1 involved three sequential rounds of data collection using focus groups in Scotland, Australia and Northern Ireland; Stage 2 involved distributing the instrument to members of a global community of practice for person-centred practice for review and feedback, as well as refinement and translation through one: one interviews in Austria. Phase 3 : Testing Structural Validity of the PCPI-C : A sample of 452 participants participated in this phase of the study. Service users participating in existing cancer research in the UK, Malta, Poland and Portugal, as well as care homes research in Austria completed the draft PCPI-C. Data were collected over a 14month period (January 2021-March 2022). Descriptive and measures of dispersion statistics were generated for all items to help inform subsequent analysis. Confirmatory factor analysis was conducted using maximum likelihood robust extraction testing of the 5-factor model of the PCPI-C.
The testing of the PCPI-C resulted in a final 18 item instrument. The results demonstrate that the PCPI-C is a psychometrically sound instrument, supporting a five-factor model that examines the service user’s perspective of what constitutes person-centred care.
Conclusion and implications
This new instrument is generic in nature and so can be used to evaluate how person-centredness is perceived by service users in different healthcare contexts and at different levels of an organisation. Thus, it brings a service user perspective to an organisation-wide evaluation framework.
Citation: McCormack BG, Slater PF, Gilmour F, Edgar D, Gschwenter S, McFadden S, et al. (2024) The development and structural validity testing of the Person-centred Practice Inventory–Care (PCPI-C). PLoS ONE 19(5): e0303158. https://doi.org/10.1371/journal.pone.0303158
Editor: Nabeel Al-Yateem, University of Sharjah, UNITED ARAB EMIRATES
Received: January 26, 2023; Accepted: April 20, 2024; Published: May 10, 2024
Copyright: © 2024 McCormack et al. This is an open access article distributed under the terms of the Creative Commons Attribution License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Data Availability: Data cannot be shared publicly because of ethical reason. Data are available from the Ulster University Institutional Data Access / Ethics Committee (contact via email on [email protected] ) for researchers who meet the criteria for access to confidential data
Funding: The author(s) received no specific funding for this work.
Competing interests: The authors have declared that no competing interests exist.
Introduction
Person-centred healthcare focuses on placing the beliefs and values of service users at the centre of decision-making and creating the context for practitioners to do this effectively. Person-centred healthcare goes beyond other models of shared decision-making as it requires practitioners to work with service users (patients) as actively engaged partners in care [ 1 ]. It is widely agreed that person-centred practice has a positive influence on the care experiences of all people associated with healthcare, service users and staff alike. International evidence shows that person-centred practice has the capacity to have a positive effect on the health and social care experiences of service users and staff [ 1 – 4 ]. Person-centred practice is a complex health care process and exists in the presence of respectful relationships, attitudes and behaviours [ 5 ]. Fundamentally, person-centred healthcare can be seen as a move away from neo-liberal models towards the humanising of healthcare delivery, with a focus on the development of individualised approaches to care and interventions, rather than seeing people as ‘products’ that need to be moved through the system in an efficient and cost-effective way [ 6 ].
Person-centred healthcare is underpinned by philosophical and theoretical constructs that frame all aspects of healthcare delivery, from the macro-perspective of policy and organisational practices to the micro-perspective of person-to-person interaction and experience of healthcare (whether as professional or service user) and so is promoted as a core attribute of the healthcare workforce [ 1 , 7 ]. However, Dewing and McCormack [ 8 ] highlighted the problems of the diverse application of concepts, theories and models all under the label of person-centredness, leading to a perception of person-centred healthcare being poorly defined, non-specific and overly generalised. Whilst person-centredness has become a well-used term globally, it is often used interchangeably with other terms such as ’woman-centredness’ [ 9 ], ’child-centredness’ [ 10 ], ’family-centredness’ [ 11 ], ’client-centredness’ [ 12 ] and ’patient-centredness’ [ 13 ]. In their review of person-centred care, Harding et al [ 14 ] identified three fundamental ‘stances’ that encompass person-centred care— Person-centred care as an overarching grouping of concepts : includes care based on shared-decision making, care planning, integrated care, patient information and self-management support; Person-centred care emphasising personhood : people being immersed in their own context and a person as a discrete human being; Person-centred care as partnership : care imbued with mutuality, trust, collaboration for care, and a therapeutic relationship.
Harding et al. adopt the narrow focus of ’care’ in their review, and others contend that for person-centred care to be operationalised there is a need to understand it from an inclusive whole-systems perspective [ 15 ] and as a philosophy to be applied to all persons. This inclusive approach has enabled the principles of person-centredness to be integrated at different levels of healthcare organisations and thus enable its embeddedness in health systems [ 16 – 19 ]. This inclusive approach is significant as person-centred care is impossible to sustain if person-centred cultures do not exist in healthcare organisations [ 20 , 21 ].
McCance and McCormack [ 5 ] developed the Person-centred Practice Framework (PCPF) to highlight the factors that affect the delivery of person-centred practices. McCormack and McCance published the original person-centred nursing framework in 2006. The Framework has evolved over two decades of research and development activity into a transdisciplinary framework and has made a significant contribution to the landscape of person-centredness globally. Not only does it enable the articulation of the dynamic nature of person-centredness, recognising complexity at different levels in healthcare systems, but it offers a common language and a shared understanding of person-centred practice. The Person-centred Practice Framework is underpinned by the following definition of person-centredness:
[A]n approach to practice established through the formation and fostering of healthful relationships between all care providers , service users and others significant to them in their lives . It is underpinned by values of respect for persons , individual right to self-determination , mutual respect and understanding . It is enabled by cultures of empowerment that foster continuous approaches to practice development [ 16 ].
The Person-centred Practice Framework ( Fig 1 ) comprises five domains: the macro context reflects the factors that are strategic and political in nature that influence the development of person-centred cultures; prerequisites focus on the attributes of staff; the practice environment focuses on the context in which healthcare is experienced; the person-centred processes focus on ways of engaging that are necessary to create connections between persons; and the outcome , which is the result of effective person-centred practice. The relationships between the five domains of the Person-centred Practice Framework are represented pictorially, that being, to reach the centre of the framework, strategic and policy frames of reference need to be attended to, then the attributes of staff must be considered as a prerequisite to managing the practice environment and to engaging effectively through the person-centred processes. This ordering ultimately leads to the achievement of the outcome–the central component of the framework. It is also important to recognise that there are relationships and there is overlap between the constructs within each domain.
- PPT PowerPoint slide
- PNG larger image
- TIFF original image
https://doi.org/10.1371/journal.pone.0303158.g001
In 2015, Slater et al. [ 22 ] developed an instrument for staff to use to measure person centred practice- the Person-centred Practice Inventory- Staff (PCPI-S). The PCPI-S is a 59-item, self-report measure of health professionals’ perceptions of their person-centred practice. The items in the PCPI-S relate to seventeen constructs across three domains of the PCPF (prerequisites, practice environment and person-centred processes). The PCPI-S has been widely used, translated into multiple languages and has undergone extensive psychometric testing [ 23 – 28 ].
No instrument exists to measure service users’ perspectives of person-centred care that is based on an established person-centred theoretical framework or that is designed to compare with service providers perceptions of it. In an attempt to address this gap in the evidence base, this study set out to develop such a valid and reliable instrument. The PCPI-C focuses on the person-centred processes domain, with the intention of measuring service users’ experiences of person-centred care. The person-centred processes are the components of care that directly affect service users’ experiences. The person-centred processes enable person-centred care outcomes to be achieved and include working with the person’s beliefs and values, sharing decision-making, engaging authentically, being sympathetically present and working holistically. Based on the ‘person-centred processes’ construct of the PCPF and relevant items from the PCPI-S, a version for service users was developed.
This paper describes the processes used to develop and test the instrument–The Person-centred Practice Inventory-Care (PCPI-C). The PCPI-C has the potential to enable healthcare services to understand service users’ experience of care and how they align with those of healthcare providers.
Materials and methods
The aim of this research was to develop and test the face validity of a service users’ version of the person-centred practice inventory–The Person-centred Practice Inventory-Care.
The development and testing of the instrument was guided by the instrument development principles of Boateng et al [ 29 ] ( Fig 2 ) and reported in line with the COSMIN guidelines for instrument testing [ 30 , 31 ]. An exploratory sequential mixed methods design was used to construct and test the instrument [ 29 , 30 ] working with international partners and service users. A three-phase approach was adopted to the development and testing of the PCPI-C. As phases 1 and 2 intentionally informed phase 3 (the testing phase), these two phases are included here in our description of methods.
https://doi.org/10.1371/journal.pone.0303158.g002
Ethical approval
Ethics approval was sought and gained for each phase of the study and across each of the participating sites. For phase 2 of the study, a generic research protocol was developed and adapted for use by the Scottish, Australian and Northern Irish teams to apply for local ethical approval. In Scotland, ethics approval was gained from Queen Margaret University Edinburgh Divisional Research Ethics Committee; in Australia, ethics approval was gained from The University of Wollongong and in Northern Ireland ethics approval was gained from the Research Governance Filter Committee, Nursing and Health Research, Ulster University. For phase 3 of the study, secondary analysis of an existing data set was undertaken. For the original study from which this data was derived (see phase 3 for details), ethical approval was granted by the UK Office of Research Ethics Committee Northern Ireland (ORECNI Ref: FCNUR-21-019) and Ulster University Research Ethics Committee. Additional local approvals were obtained for each partner site as required. In addition, a data sharing agreement was generated to facilitate sharing of study data between European Union (EU) sites and the United Kingdom (UK).
Phase 1 –Item selection
An initial item pool for the PCPI-C was identified by <author initials to be added after peer-review> by selecting items from the ‘person-centred processes’ sub-scale of the PCPI-S ( Table 1 ). Sixteen items were extracted, and the wording of the statements was adjusted to reflect a service-user perspective. Additional items were identified (n = 4) to fully represent the construct from a service-user perspective. A final list of 20 items was agreed upon and this 20-item questionnaire was used in Phase 2 of the instrument development.
https://doi.org/10.1371/journal.pone.0303158.t001
Phase 2 –Instrument development and refinement
Testing the validity of PCPI-C was undertaken through three sequential rounds of data collection using focus groups in Scotland, Australia and Northern Ireland. The purpose of these focus groups was to work with service users to share and compare understandings and views of their experiences of healthcare and to consider these experiences in the context of the initial set of PCPI-C items generated in phase 1 of the study. These countries were selected as the lead researchers had established relationships with healthcare partners who were willing to host the research. The inclusion of multiple countries provided different perspectives from service users who used different health services. In Scotland, a convenience sample of service users (n = 11) attending a palliative care day centre of a local hospice was selected. In Australia a cancer support group for people living with a cancer diagnosis (n = 9) was selected and in Northern Ireland, people with lived experience who were attending a community group hosted by a Cancer Charity (n = 9) were selected. All service users were current users of healthcare and so the challenge of memory recall was avoided. The type of conditions/health problems of participants was not the primary concern. Instead, we targeted persons who had recent experiences of the health system. The three centres selected were known to the researchers in those geographical areas and relationships were already established, which helped with gaining access to potential participants. Whilst the research team had potential access to other centres in each country, it was evident at focus group 3 that no significant new issues were being identified from the participants and thus we agreed to not do further rounds of refinement.
A Focus Group guide was developed ( Fig 3 ). Participants were invited to draw on their experiences as a user of the service; particularly remembering what they saw, the way they felt and what they imagined was happening [ 32 ]. The participants were invited to independently complete the PCPI-C and the purpose of the exercise was reiterated i.e. to think about how each question of the PCPI-C reflected their own experiences and their answers to the questions. Following completion of the questionnaire, participants were asked to comment on each question in the PCPI-C (20 questions), with a specific focus on their understanding of the question, what they thought about when they read the question, and any suggestions to improve readability. The focus group was concluded with a discussion on the overall usability of the PCPI-C. Each focus group was audiotaped and the audio recordings were transcribed in full. The facilitators of the focus group then listened to the audio recordings, alongside the transcripts, and identified the common issues that arose from the discussions and noted against each of the questions in the draft PCPI-C. Revisions were made to the questions in accordance with the comments and recommendations of the participants. At the end of the analysis phase of each focus group, a table of comments and recommendations mapped to the questions in the instrument was compiled and sent to the whole research team for review and consideration. The comments and recommendations were reviewed by the research team and amendments made to the draft PCPI-C. The amended draft was then used in the next focus group until a final version was agreed. Focus group 1 was held in Scotland, focus group 2 in Australia and focus group 3 in Northern Ireland. Table 2 presents a summary of the feedback from the final focus group.
https://doi.org/10.1371/journal.pone.0303158.g003
https://doi.org/10.1371/journal.pone.0303158.t002
A final stage of development involved distributing the agreed version of the PCPI-C to members of ‘The International Community of Practice for Person-centred Practice’ (PcP-ICoP) for review and feedback. The PcP-ICoP is an international community of higher education, health and care organisations and individuals who are committed to advancing knowledge in the field of person-centredness. No significant changes to the distributed version were suggested by the PcP-ICoP members, but several members requested permission to translate the instrument into their national language. PcP-ICoP members at the University of Vienna, who were leading on a large research project with nursing homes in the region of Lower Austria, agreed to undertake a parallel translation project as a priority, so they could use the PCPI-C in their research project. The instrument was culturally and linguistically adapted to the nursing home setting in an iterative process by the Austrian research team in collaboration with the international research team. Data were collected through face-to-face interviews by trained research staff. Residents of five nursing homes for older persons in Lower Austria were included. All residents who did not have a cognitive impairment or were physically unable to complete the questionnaire (because of ill-health) (n = 235) were included. 71% of these residents (N = 167) managed to complete the questionnaire. Whilst in Austria, formal ethical approval for non-intervention studies is not required, the team sought informed consent from participants. Particular attention was paid throughout the interviews to assure ongoing consent of residents by carefully guided conversations.
Phase 3: Testing structural validity of the PCPI-C
The aim of this phase was to test the structural validity of the PCPI-C using confirmatory factor analysis with an international sample of service users. The PCPI-C comprises 20 items measured on a 5-point scale ranging from ‘strongly disagree’ to ‘strongly agree. The 20 items represent the 5 constructs comprising the final model to be tested, which is outlined in Table 3 .
https://doi.org/10.1371/journal.pone.0303158.t003
A sample of 452 participants was selected for this phase of the study. The sample selected comprised two groups. Group 1 (n = 285) were service users with cancer (breast, urological and other) receiving radiotherapy in four Cancer Treatment Centres in four European Countries–UK, Malta, Poland and Portugal. These service users were participants in a wider SAFE EUROPE ( www.safeeurope.eu ) project exploring the education and professional migration of therapeutic radiographers in the European Union. In the UK a study information poster with a link to the PCPI-C via Qualtrics © survey was disseminated via UK cancer charity social media websites. Service user information and consent were embedded in the online survey and presented to the participant following the study link. At the non-UK sites, hard copy English versions of the surveys were available in clinical departments where a convenience sampling approach was used, inviting everyone in their final few days of radiotherapy to participate. The ‘DeepL Translator’ software (DeepL GmbH, Cologne, Germany) was used to make the necessary terminology adaptions for both the questionnaire and the participant information sheet across the various countries. Fluent speakers based in the participating sites and who were members of the SAFE EUROPE project team confirmed the accuracy of this process by checking the accuracy of the translated version against the original English version. Participants were provided with study information and had at least 24 hours to decide if they wished to participate. Willing participants were then invited to provide written informed consent by the local study researcher. The study researcher provided the hard copy survey to the service user but did not engage with or assist them during completion. Service users were informed they could take the survey home for completion if they wished. Completed surveys were returned to a drop box in the department or returned by post (data collected May 2021-March 2022). Group 2 were residents in nursing homes in Lower Austria (n = 125). No participating residents had a cognitive impairment and were physically able to complete the questionnaire. Data were collected through face-to-face interviews by trained research staff (data collected January 2021-March 2021).
Statistical analysis
Descriptive and measures of dispersion statistics were generated for all items to help inform subsequent analysis. Measures of appropriateness to conduct factor analysis were conducted using The Kaiser-Meyer-Olkin Measures of Sampling Adequacy and Bartletts Test of Sphericity. Inter-item correlations were generated to examine for collinearity prior to full analysis. Confirmatory factor analysis was conducted using maximum likelihood robust extraction testing of the 5-factor model.
Acceptable fit statistics were set at Root Mean Square Estimations of Approximation (RMSEA) of 0.05 or below; 90% RMSEA higher bracket below 0.08; and Confirmation Fit Indices (CFI) of 0.95 or higher and SRMR below 0.05 [ 33 – 35 ]. Internal consistency was measured using Cronbach alpha scores for factors in the accepted factor model.
The model was re-specified using the modification indices provided in the statistical output until acceptable and a statistically significant relationship was identified. All re-specifications of the model were guided by principles of (1) meaningfulness (a clear theoretical rationale); (2) transitivity (if A is correlated to B, and B correlated to C, then A should correlate with C); and (3) generality (if there is a reason for correlating the errors between one pair of errors, then all pairs for which that reason applies should also be correlated) [ 36 ].
Acceptance modification criteria of:
- The items to first order factors were initially fitted.
- Correlated error variance permitted as all items were measuring the same unidimensional construct.
- Only statistically significant relationship retained to help produce as parsimonious a model as possible.
- Factor loadings above 0.40 to provide a strong emergent factor structure.
Factor loading scores were based on Comrey and Lee’s [ 37 ] guidelines (>.71 = excellent, >.63 = very good, >.55 = good, >.45 = fair and >.32 = poor) and acceptable factor loading given the sample size (n = 452) were set at >0.3 [ 33 , 38 ].
Results and discussion
Demographic details.
The sample of 452 participants represented an international sample of respondents drawn from across five countries: UK (14.6% n = 66), Portugal (47.8%. n = 216), Austria (27.7%, n = 125), Malta (6.6, n = 30) and Poland (3.3%, n = 15). Table 4 outline the demographic characteristics of the sample. The final sample of 452 participants provides an acceptable ratio 33 of 22:1 respondent to items.
https://doi.org/10.1371/journal.pone.0303158.t004
The means scores indicate that respondents scored the items neutrally. The measures of skewness and kurtosis were acceptable and satisfied the conditions of normality of distribution for further psychometric testing. Examination of the Kaiser Meyer Olkin (0.947) and the Bartlett test for sphericity (4431.68, df = 190, p = 0.00) indicated acceptability of performing factor analysis on the items. Cronbach alpha scores for each of the constructs confirm the acceptability and unidimensionality of each construct.
Examination of the correlation matrix between items shows a range of between 0.144 and 0.740, indicating a broadness in the areas of care the questionnaire items address, as well as no issues of collinearity. The original measurement model was examined using maximum likelihood extraction and the original model had mixed fit statistics. All factor loadings (except for items 11 and 13) were above the threshold of 0.4 ( Table 3 ). Six further modifications were introduced into the original model based on highest scored modification indices until the fit statistics were deemed acceptable ( Table 5 for model fit statistics and Fig 4 for items correlated errors). Two item correlated error modifications were within factors and 4 between factors. The accepted model factor structure is displayed in Fig 4 .
https://doi.org/10.1371/journal.pone.0303158.g004
https://doi.org/10.1371/journal.pone.0303158.t005
Measuring person-centred care is a complex and challenging endeavour [ 39 ]. In a review of existing measures of person-centred care, DeSilva [ 39 ] identified that whilst there are many tools available to measure person-centred care, there was no agreement about which tools were most worthwhile. The complexity of measurement is further reinforced by the multiplicity of terms used that imply a person-centred approach being adopted without explicitly setting out the meaning of the term. Further, person-centred care is multifaceted and comprises a multitude of methods that are held together by a common philosophy of care and organisational goals that focus on service users having the best possible (personalised) experience of care. As DeSilva suggested, “it is a priority to understand what ‘person-centred’ means . Until we know what we want to achieve , it is difficult to know the most appropriate way to measure it . (p 3)” . However, it remains the case that many of the methods adopted are poorly specified and not embedded in clear conceptual or theoretical frameworks [ 40 , 41 ]. A clear advantage of the study reported here is that the PCPI-C is embedded in a theoretical framework of person-centredness (the PCPF) that clearly defines what we mean by person-centred practice. The PCPI-C is explicitly informed by the ‘person-centred processes’ domain of the PCPF, which has an explicit focus on the care processes used by healthcare workers in providing healthcare to service-users.
In the development of the PCPI-C, initial items were selected from the Person-centred Practice Inventory-Staff (PCPI-S) and these items are directly connected with the person-centred processes domain of the PCPF. The PCPI-S has been translated, validated and adopted internationally [ 23 – 28 ] and so provides a robust theoretically informed starting point for the development of the PCPI-C. This starting point contributed to the initial acceptability of the instrument to participants in the focus groups. Like DeSilva, [ 39 ] McCormack et al [ 42 ] and McCormack [ 41 ] have argued that measuring person-centred care as an isolated activity from the evaluation of the impact of contextual factors on the care experienced, is a limited exercise. As McCormack [ 41 ] suggests “ Evaluating person-centred care as a specific intervention or group of interventions , without understanding the impact of these cultural and contextual factors , does little to inform the quality of a service . ” (p1) Using the PCPI-C alongside other instruments such as the PCPI-S helps to generate contrasting perspectives from healthcare providers and healthcare service users, informed by clear definitions of terms that can be integrated in quality improvement and practice development programmes. The development of the PCPI-C was conducted in line with good practice guidelines in instrument development [ 29 ] and underpinned by an internationally recognised person-centred practice theoretical framework, the PCPF [ 5 ]. The PCPI-C provides a psychometrically robust tool to measure service users’ perspectives of person-centred care as an integrated and multi-faceted approach to evaluating person-centredness more generally in healthcare organisations.
With the advancement of Patient Reported Outcome Measures (PROMS) [ 43 , 44 ], Patient Reported Experience Measures (PREMS) [ 45 ] and the World Health Organization (WHO) [ 15 ] emphasis on the development of people-centred and integrated health systems, greater emphasis has been placed on developing measures to determine the person-centredness of care experienced by service users. Several instruments have been developed to measure the effectiveness of person-centred care in specific services, such as mental health [ 45 ], primary care [ 46 , 47 ], aged care [ 48 , 49 ] and community care [ 50 ]. However only one other instrument adopts a generic approach to evaluating services users’ experiences of person-centred care [ 51 ]. The work of Fridberg et al (The Generic Person-centred Care Questionnaire (GPCCQ)) is located in the Gothenburg Centre for Person-centred Care (GPCC) concept of person-centredness—patient narrative, partnership and documentation. Whilst there are clear connections between the GPCCQ and the PCPI-C, a strength of the PCPI-C is that it is set in a broader system of evaluation that views person-centredness as a whole system issue, with all parts of the system needing to be consistent in concepts used, definitions of terms and approaches to evaluation. Whilst the PCPI-S evaluates how person-centredness is perceived at different levels of the organisation, using the same theoretical framework and the same definition of terms, the PCPI-C brings a service user perspective to an organisation-wide evaluation framework.
A clear strength of this study lies in the methods engaged in phase 2. Capturing service user experiences of healthcare has become an important part of the evaluation of effectiveness. Service user experience evaluation methodologies adopt a variety of methods that aim to capture key transferrable themes across patient populations, supported by granular detail of individual specific experience [ 43 ]. This kind of service evaluation depends on systematically capturing a variety of experiences across different service-user groups. In the research reported here, service users from a variety of services including palliative care and cancer services from three countries, engaged in the focus group discussions and were freely able to discuss their experiences of care and consider them in the context of the questionnaire items. The use of focus groups in three different countries enabled different cultural perspectives to be considered in the way participants engaged with discussions and considered the relevance of items and their wording. The sequential approach enabled three rounds of refinement of the items and this enabled the most relevant wording to be achieved. The range of comments and depth of feedback prevented ‘knee-jerk’ changes being made based on one-off comments, but instead, it was possible to compare and contrast the comments and feedback and achieve a more considered outcome. The cultural relevance of the instrument was reinforced through the translation of the instrument to the German language in Austria, as few changes were made to the original wording in the translation process. This approach combined the capturing of individual lived experience with the systematic generation of key themes that can assist with the systematic evaluation of healthcare services. Further, adopting this approach provides a degree of confidence to users of the PCPI-C that it represents real service-user experiences.
The factorial validity of the instrument was supported by the findings of the study. The modified models fit indices suggest a good model fit for the sample [ 31 , 34 , 35 ]. The Confirmation Fit Indices (CFI) fall short of the threshold of >0.95. However, this is above 0.93 which is considered an acceptable level of fit [ 52 ]. Examination of the alpha scores confirm the reliability (internal consistency) of each construct [ 53 ]. All factor loadings were at a statistically significant level and above the acceptable criteria of 0.3 recommended for the sample size [ 38 ]. All but 2 of the loadings (v11 –‘ Staff don’t assume they know what is best for me’ and v13 – ‘My family are included in decisions about my care only when I want them to be’ ) were above the loadings considered as good to excellent [ 37 ]. At the level of construct, previous research by McCance et al [ 54 ] showed that all five constructs of the person-centred processes domain of the Person-centred Practice Framework carried equal significance in shaping how person-centred practice is delivered, and this is borne out by the approval of a 5-factor model in this study. However, it is also probable that there is a degree of overlap between items across the constructs, reflected in the 2 items with lower loadings. Other items in the PCPI-C address perspectives on shared decision-making and family engagement and thus it was concluded that based on the theoretical model and statistical analysis, these 2 items could be removed without compromising the comprehensiveness of the scale, resulting in a final 18-item version of the PCPI-C (available on request).
Whilst a systematic approach to the development of the PCPI-C was adopted, and we engaged with service users in several care settings in different countries, further research is required in the psychometric testing of the instrument across differing conditions, settings and with culturally diverse samples. Whilst the sample does provide an acceptable respondent to item ratio, and the sample contains international respondents, the model structure is not examined across international settings. Likewise, further research is required across service users with differing conditions and clinical settings. Whilst this is a limitation of this study reported here, the psychometric testing of an instrument is a continuous process and further testing of the PCPI-C is welcomed.
Conclusions
This paper has presented the systematic approach adopted to develop and test a theoretically informed instrument for measuring service users’ perspectives of person-centred care. The instrument is one of the first that is generic and theory-informed, enabling it to be applied as part of a comprehensive and integrated framework of evaluation at different levels of healthcare organisations. Whilst the instrument has good statistical properties, ongoing testing is recommended.
Acknowledgments
The authors of this paper acknowledge the significant contributions of all the service users who participated in this study.
- View Article
- Google Scholar
- 2. Institute of Medicine Committee on Quality of Health Care in America (2001) Crossing the Quality Chasm : A New Health System for the 21st Century . Washington: National Academies Press. https://nap.nationalacademies.org/catalog/10027/crossing-the-quality-chasm-a-new-health-system-for-the (Accessed 20/1/2023).
- PubMed/NCBI
- 5. McCance T. and McCormack B. (2021) The Person-centred Practice Framework, in McCormack B, McCance T, Martin S, McMillan A, Bulley C (2021) Fundamentals of Person-centred Healthcare Practice . Oxford. Wiley. PP: 23–32 https://www.perlego.com/book/2068078/fundamentals-of-personcentred-healthcare-practice-pdf?utm_source=google&utm_medium=cpc&gclid=Cj0KCQjwtrSLBhCLARIsACh6Rmj9sarf1IjwEHCseXMsPLGeUTTQlJWYL6mfQEQgwO3lnLkUU9Gb0A8aAgT1EALw_wcB .
- 7. Nursing and Midwifery Council (2018) Future Nurse : Standards of Proficiency for Registered Nurses . London. Nursing and Midwifery Council. https://www.nmc.org.uk/globalassets/sitedocuments/standards-of-proficiency/nurses/future-nurse-proficiencies.pdf (Accessed 20/1/2023).
- 14. Harding E., Wait S. and Scrutton J. (2015) The State of Play in Person-centred Care : A Pragmatic Review of how Person-centred Care is Defined , Applied and Measured . London: The Health Policy Partnership.
- 16. McCormack B. and McCance T. (2017) Person-centred Practice in Nursing and Health Care : Theory and Practice . Chichester, UK: Wiley-Blackwell.
- 17. Buetow S. (2016) Person-centred Healthcare : Balancing the Welfare of Clinicians and Patients . Oxford: Routledge.
- 32. Kruger R. A. and Casey M. A., (2000). Focus groups : A practical guide for applied research . 3rd ed. Thousand Oaks, CA: Sage Publications.
- 33. Kline P., (2014). An easy guide to factor analysis . Oxfordshire. Routledge.
- 34. Byrne B.M., (2013). Structural equation modeling with Mplus : Basic concepts , applications , and programming . Oxfordshire. Routledge.
- 35. Wang J. and Wang X., (2019). Structural equation modeling : Applications using Mplus . New Jersey. John Wiley & Sons.
- 37. Comrey A.L. and Lee H.B., (2013). A first course in factor analysis . New York. Psychology press.
- 38. Hair J.F., Black W.C., Babin B.J., Anderson R.E. R.L. and Tatham , (2018). Multivariate Data Analysis . 8th Edn., New Jersey. Pearson Prentice Hall.
- 39. DeSilva (2014) Helping measure person-centred care : A review of evidence about commonly used approaches and tools used to help measure person-centred care . London, The Health Foundation. https://www.health.org.uk/publications/helping-measure-person-centred-care .
- 42. McCormack B, McCance T and Maben J (2013) Outcome Evaluation in the Development of Person-Centred Practice In B McCormack, K Manley and A Titchen (2013) Practice Development in Nursing (Vol 2 ) . Oxford. Wiley-Blackwell Publishing. Pp: 190–211.
- 43. Irish Platform for Patients Organisations Science & Industry (IPPOSI) (2018). Patient-centred outcome measures in research & healthcare : IPPOSI outcome report . Dublin, Ireland: IPPOSI. https://www.ipposi.ie/wp-content/uploads/2018/12/PCOMs-outcome-report-final-v3.pdf (Accessed 20/1/2023).
Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals
- My Account Login
- Explore content
- About the journal
- Publish with us
- Sign up for alerts
- Data Descriptor
- Open access
- Published: 03 May 2024
A dataset for measuring the impact of research data and their curation
- Libby Hemphill ORCID: orcid.org/0000-0002-3793-7281 1 , 2 ,
- Andrea Thomer 3 ,
- Sara Lafia 1 ,
- Lizhou Fan 2 ,
- David Bleckley ORCID: orcid.org/0000-0001-7715-4348 1 &
- Elizabeth Moss 1
Scientific Data volume 11 , Article number: 442 ( 2024 ) Cite this article
686 Accesses
8 Altmetric
Metrics details
- Research data
- Social sciences
Science funders, publishers, and data archives make decisions about how to responsibly allocate resources to maximize the reuse potential of research data. This paper introduces a dataset developed to measure the impact of archival and data curation decisions on data reuse. The dataset describes 10,605 social science research datasets, their curation histories, and reuse contexts in 94,755 publications that cover 59 years from 1963 to 2022. The dataset was constructed from study-level metadata, citing publications, and curation records available through the Inter-university Consortium for Political and Social Research (ICPSR) at the University of Michigan. The dataset includes information about study-level attributes (e.g., PIs, funders, subject terms); usage statistics (e.g., downloads, citations); archiving decisions (e.g., curation activities, data transformations); and bibliometric attributes (e.g., journals, authors) for citing publications. This dataset provides information on factors that contribute to long-term data reuse, which can inform the design of effective evidence-based recommendations to support high-impact research data curation decisions.
Similar content being viewed by others

SciSciNet: A large-scale open data lake for the science of science research

Data, measurement and empirical methods in the science of science

Interdisciplinarity revisited: evidence for research impact and dynamism
Background & summary.
Recent policy changes in funding agencies and academic journals have increased data sharing among researchers and between researchers and the public. Data sharing advances science and provides the transparency necessary for evaluating, replicating, and verifying results. However, many data-sharing policies do not explain what constitutes an appropriate dataset for archiving or how to determine the value of datasets to secondary users 1 , 2 , 3 . Questions about how to allocate data-sharing resources efficiently and responsibly have gone unanswered 4 , 5 , 6 . For instance, data-sharing policies recognize that not all data should be curated and preserved, but they do not articulate metrics or guidelines for determining what data are most worthy of investment.
Despite the potential for innovation and advancement that data sharing holds, the best strategies to prioritize datasets for preparation and archiving are often unclear. Some datasets are likely to have more downstream potential than others, and data curation policies and workflows should prioritize high-value data instead of being one-size-fits-all. Though prior research in library and information science has shown that the “analytic potential” of a dataset is key to its reuse value 7 , work is needed to implement conceptual data reuse frameworks 8 , 9 , 10 , 11 , 12 , 13 , 14 . In addition, publishers and data archives need guidance to develop metrics and evaluation strategies to assess the impact of datasets.
Several existing resources have been compiled to study the relationship between the reuse of scholarly products, such as datasets (Table 1 ); however, none of these resources include explicit information on how curation processes are applied to data to increase their value, maximize their accessibility, and ensure their long-term preservation. The CCex (Curation Costs Exchange) provides models of curation services along with cost-related datasets shared by contributors but does not make explicit connections between them or include reuse information 15 . Analyses on platforms such as DataCite 16 have focused on metadata completeness and record usage, but have not included related curation-level information. Analyses of GenBank 17 and FigShare 18 , 19 citation networks do not include curation information. Related studies of Github repository reuse 20 and Softcite software citation 21 reveal significant factors that impact the reuse of secondary research products but do not focus on research data. RD-Switchboard 22 and DSKG 23 are scholarly knowledge graphs linking research data to articles, patents, and grants, but largely omit social science research data and do not include curation-level factors. To our knowledge, other studies of curation work in organizations similar to ICPSR – such as GESIS 24 , Dataverse 25 , and DANS 26 – have not made their underlying data available for analysis.
This paper describes a dataset 27 compiled for the MICA project (Measuring the Impact of Curation Actions) led by investigators at ICPSR, a large social science data archive at the University of Michigan. The dataset was originally developed to study the impacts of data curation and archiving on data reuse. The MICA dataset has supported several previous publications investigating the intensity of data curation actions 28 , the relationship between data curation actions and data reuse 29 , and the structures of research communities in a data citation network 30 . Collectively, these studies help explain the return on various types of curatorial investments. The dataset that we introduce in this paper, which we refer to as the MICA dataset, has the potential to address research questions in the areas of science (e.g., knowledge production), library and information science (e.g., scholarly communication), and data archiving (e.g., reproducible workflows).
We constructed the MICA dataset 27 using records available at ICPSR, a large social science data archive at the University of Michigan. Data set creation involved: collecting and enriching metadata for articles indexed in the ICPSR Bibliography of Data-related Literature against the Dimensions AI bibliometric database; gathering usage statistics for studies from ICPSR’s administrative database; processing data curation work logs from ICPSR’s project tracking platform, Jira; and linking data in social science studies and series to citing analysis papers (Fig. 1 ).

Steps to prepare MICA dataset for analysis - external sources are red, primary internal sources are blue, and internal linked sources are green.
Enrich paper metadata
The ICPSR Bibliography of Data-related Literature is a growing database of literature in which data from ICPSR studies have been used. Its creation was funded by the National Science Foundation (Award 9977984), and for the past 20 years it has been supported by ICPSR membership and multiple US federally-funded and foundation-funded topical archives at ICPSR. The Bibliography was originally launched in the year 2000 to aid in data discovery by providing a searchable database linking publications to the study data used in them. The Bibliography collects the universe of output based on the data shared in each study through, which is made available through each ICPSR study’s webpage. The Bibliography contains both peer-reviewed and grey literature, which provides evidence for measuring the impact of research data. For an item to be included in the ICPSR Bibliography, it must contain an analysis of data archived by ICPSR or contain a discussion or critique of the data collection process, study design, or methodology 31 . The Bibliography is manually curated by a team of librarians and information specialists at ICPSR who enter and validate entries. Some publications are supplied to the Bibliography by data depositors, and some citations are submitted to the Bibliography by authors who abide by ICPSR’s terms of use requiring them to submit citations to works in which they analyzed data retrieved from ICPSR. Most of the Bibliography is populated by Bibliography team members, who create custom queries for ICPSR studies performed across numerous sources, including Google Scholar, ProQuest, SSRN, and others. Each record in the Bibliography is one publication that has used one or more ICPSR studies. The version we used was captured on 2021-11-16 and included 94,755 publications.
To expand the coverage of the ICPSR Bibliography, we searched exhaustively for all ICPSR study names, unique numbers assigned to ICPSR studies, and DOIs 32 using a full-text index available through the Dimensions AI database 33 . We accessed Dimensions through a license agreement with the University of Michigan. ICPSR Bibliography librarians and information specialists manually reviewed and validated new entries that matched one or more search criteria. We then used Dimensions to gather enriched metadata and full-text links for items in the Bibliography with DOIs. We matched 43% of the items in the Bibliography to enriched Dimensions metadata including abstracts, field of research codes, concepts, and authors’ institutional information; we also obtained links to full text for 16% of Bibliography items. Based on licensing agreements, we included Dimensions identifiers and links to full text so that users with valid publisher and database access can construct an enriched publication dataset.
Gather study usage data
ICPSR maintains a relational administrative database, DBInfo, that organizes study-level metadata and information on data reuse across separate tables. Studies at ICPSR consist of one or more files collected at a single time or for a single purpose; studies in which the same variables are observed over time are grouped into series. Each study at ICPSR is assigned a DOI, and its metadata are stored in DBInfo. Study metadata follows the Data Documentation Initiative (DDI) Codebook 2.5 standard. DDI elements included in our dataset are title, ICPSR study identification number, DOI, authoring entities, description (abstract), funding agencies, subject terms assigned to the study during curation, and geographic coverage. We also created variables based on DDI elements: total variable count, the presence of survey question text in the metadata, the number of author entities, and whether an author entity was an institution. We gathered metadata for ICPSR’s 10,605 unrestricted public-use studies available as of 2021-11-16 ( https://www.icpsr.umich.edu/web/pages/membership/or/metadata/oai.html ).
To link study usage data with study-level metadata records, we joined study metadata from DBinfo on study usage information, which included total study downloads (data and documentation), individual data file downloads, and cumulative citations from the ICPSR Bibliography. We also gathered descriptive metadata for each study and its variables, which allowed us to summarize and append recoded fields onto the study-level metadata such as curation level, number and type of principle investigators, total variable count, and binary variables indicating whether the study data were made available for online analysis, whether survey question text was made searchable online, and whether the study variables were indexed for search. These characteristics describe aspects of the discoverability of the data to compare with other characteristics of the study. We used the study and series numbers included in the ICPSR Bibliography as unique identifiers to link papers to metadata and analyze the community structure of dataset co-citations in the ICPSR Bibliography 32 .
Process curation work logs
Researchers deposit data at ICPSR for curation and long-term preservation. Between 2016 and 2020, more than 3,000 research studies were deposited with ICPSR. Since 2017, ICPSR has organized curation work into a central unit that provides varied levels of curation that vary in the intensity and complexity of data enhancement that they provide. While the levels of curation are standardized as to effort (level one = less effort, level three = most effort), the specific curatorial actions undertaken for each dataset vary. The specific curation actions are captured in Jira, a work tracking program, which data curators at ICPSR use to collaborate and communicate their progress through tickets. We obtained access to a corpus of 669 completed Jira tickets corresponding to the curation of 566 unique studies between February 2017 and December 2019 28 .
To process the tickets, we focused only on their work log portions, which contained free text descriptions of work that data curators had performed on a deposited study, along with the curators’ identifiers, and timestamps. To protect the confidentiality of the data curators and the processing steps they performed, we collaborated with ICPSR’s curation unit to propose a classification scheme, which we used to train a Naive Bayes classifier and label curation actions in each work log sentence. The eight curation action labels we proposed 28 were: (1) initial review and planning, (2) data transformation, (3) metadata, (4) documentation, (5) quality checks, (6) communication, (7) other, and (8) non-curation work. We note that these categories of curation work are very specific to the curatorial processes and types of data stored at ICPSR, and may not match the curation activities at other repositories. After applying the classifier to the work log sentences, we obtained summary-level curation actions for a subset of all ICPSR studies (5%), along with the total number of hours spent on data curation for each study, and the proportion of time associated with each action during curation.
Data Records
The MICA dataset 27 connects records for each of ICPSR’s archived research studies to the research publications that use them and related curation activities available for a subset of studies (Fig. 2 ). Each of the three tables published in the dataset is available as a study archived at ICPSR. The data tables are distributed as statistical files available for use in SAS, SPSS, Stata, and R as well as delimited and ASCII text files. The dataset is organized around studies and papers as primary entities. The studies table lists ICPSR studies, their metadata attributes, and usage information; the papers table was constructed using the ICPSR Bibliography and Dimensions database; and the curation logs table summarizes the data curation steps performed on a subset of ICPSR studies.
Studies (“ICPSR_STUDIES”): 10,605 social science research datasets available through ICPSR up to 2021-11-16 with variables for ICPSR study number, digital object identifier, study name, series number, series title, authoring entities, full-text description, release date, funding agency, geographic coverage, subject terms, topical archive, curation level, single principal investigator (PI), institutional PI, the total number of PIs, total variables in data files, question text availability, study variable indexing, level of restriction, total unique users downloading study data files and codebooks, total unique users downloading data only, and total unique papers citing data through November 2021. Studies map to the papers and curation logs table through ICPSR study numbers as “STUDY”. However, not every study in this table will have records in the papers and curation logs tables.
Papers (“ICPSR_PAPERS”): 94,755 publications collected from 2000-08-11 to 2021-11-16 in the ICPSR Bibliography and enriched with metadata from the Dimensions database with variables for paper number, identifier, title, authors, publication venue, item type, publication date, input date, ICPSR series numbers used in the paper, ICPSR study numbers used in the paper, the Dimension identifier, and the Dimensions link to the publication’s full text. Papers map to the studies table through ICPSR study numbers in the “STUDY_NUMS” field. Each record represents a single publication, and because a researcher can use multiple datasets when creating a publication, each record may list multiple studies or series.
Curation logs (“ICPSR_CURATION_LOGS”): 649 curation logs for 563 ICPSR studies (although most studies in the subset had one curation log, some studies were associated with multiple logs, with a maximum of 10) curated between February 2017 and December 2019 with variables for study number, action labels assigned to work description sentences using a classifier trained on ICPSR curation logs, hours of work associated with a single log entry, and total hours of work logged for the curation ticket. Curation logs map to the study and paper tables through ICPSR study numbers as “STUDY”. Each record represents a single logged action, and future users may wish to aggregate actions to the study level before joining tables.

Entity-relation diagram.
Technical Validation
We report on the reliability of the dataset’s metadata in the following subsections. To support future reuse of the dataset, curation services provided through ICPSR improved data quality by checking for missing values, adding variable labels, and creating a codebook.
All 10,605 studies available through ICPSR have a DOI and a full-text description summarizing what the study is about, the purpose of the study, the main topics covered, and the questions the PIs attempted to answer when they conducted the study. Personal names (i.e., principal investigators) and organizational names (i.e., funding agencies) are standardized against an authority list maintained by ICPSR; geographic names and subject terms are also standardized and hierarchically indexed in the ICPSR Thesaurus 34 . Many of ICPSR’s studies (63%) are in a series and are distributed through the ICPSR General Archive (56%), a non-topical archive that accepts any social or behavioral science data. While study data have been available through ICPSR since 1962, the earliest digital release date recorded for a study was 1984-03-18, when ICPSR’s database was first employed, and the most recent date is 2021-10-28 when the dataset was collected.
Curation level information was recorded starting in 2017 and is available for 1,125 studies (11%); approximately 80% of studies with assigned curation levels received curation services, equally distributed between Levels 1 (least intensive), 2 (moderately intensive), and 3 (most intensive) (Fig. 3 ). Detailed descriptions of ICPSR’s curation levels are available online 35 . Additional metadata are available for a subset of 421 studies (4%), including information about whether the study has a single PI, an institutional PI, the total number of PIs involved, total variables recorded is available for online analysis, has searchable question text, has variables that are indexed for search, contains one or more restricted files, and whether the study is completely restricted. We provided additional metadata for this subset of ICPSR studies because they were released within the past five years and detailed curation and usage information were available for them. Usage statistics including total downloads and data file downloads are available for this subset of studies as well; citation statistics are available for 8,030 studies (76%). Most ICPSR studies have fewer than 500 users, as indicated by total downloads, or citations (Fig. 4 ).

ICPSR study curation levels.

ICPSR study usage.
A subset of 43,102 publications (45%) available in the ICPSR Bibliography had a DOI. Author metadata were entered as free text, meaning that variations may exist and require additional normalization and pre-processing prior to analysis. While author information is standardized for each publication, individual names may appear in different sort orders (e.g., “Earls, Felton J.” and “Stephen W. Raudenbush”). Most of the items in the ICPSR Bibliography as of 2021-11-16 were journal articles (59%), reports (14%), conference presentations (9%), or theses (8%) (Fig. 5 ). The number of publications collected in the Bibliography has increased each decade since the inception of ICPSR in 1962 (Fig. 6 ). Most ICPSR studies (76%) have one or more citations in a publication.

ICPSR Bibliography citation types.

ICPSR citations by decade.
Usage Notes
The dataset consists of three tables that can be joined using the “STUDY” key as shown in Fig. 2 . The “ICPSR_PAPERS” table contains one row per paper with one or more cited studies in the “STUDY_NUMS” column. We manipulated and analyzed the tables as CSV files with the Pandas library 36 in Python and the Tidyverse packages 37 in R.
The present MICA dataset can be used independently to study the relationship between curation decisions and data reuse. Evidence of reuse for specific studies is available in several forms: usage information, including downloads and citation counts; and citation contexts within papers that cite data. Analysis may also be performed on the citation network formed between datasets and papers that use them. Finally, curation actions can be associated with properties of studies and usage histories.
This dataset has several limitations of which users should be aware. First, Jira tickets can only be used to represent the intensiveness of curation for activities undertaken since 2017, when ICPSR started using both Curation Levels and Jira. Studies published before 2017 were all curated, but documentation of the extent of that curation was not standardized and therefore could not be included in these analyses. Second, the measure of publications relies upon the authors’ clarity of data citation and the ICPSR Bibliography staff’s ability to discover citations with varying formality and clarity. Thus, there is always a chance that some secondary-data-citing publications have been left out of the bibliography. Finally, there may be some cases in which a paper in the ICSPSR bibliography did not actually obtain data from ICPSR. For example, PIs have often written about or even distributed their data prior to their archival in ICSPR. Therefore, those publications would not have cited ICPSR but they are still collected in the Bibliography as being directly related to the data that were eventually deposited at ICPSR.
In summary, the MICA dataset contains relationships between two main types of entities – papers and studies – which can be mined. The tables in the MICA dataset have supported network analysis (community structure and clique detection) 30 ; natural language processing (NER for dataset reference detection) 32 ; visualizing citation networks (to search for datasets) 38 ; and regression analysis (on curation decisions and data downloads) 29 . The data are currently being used to develop research metrics and recommendation systems for research data. Given that DOIs are provided for ICPSR studies and articles in the ICPSR Bibliography, the MICA dataset can also be used with other bibliometric databases, including DataCite, Crossref, OpenAlex, and related indexes. Subscription-based services, such as Dimensions AI, are also compatible with the MICA dataset. In some cases, these services provide abstracts or full text for papers from which data citation contexts can be extracted for semantic content analysis.
Code availability
The code 27 used to produce the MICA project dataset is available on GitHub at https://github.com/ICPSR/mica-data-descriptor and through Zenodo with the identifier https://doi.org/10.5281/zenodo.8432666 . Data manipulation and pre-processing were performed in Python. Data curation for distribution was performed in SPSS.
He, L. & Han, Z. Do usage counts of scientific data make sense? An investigation of the Dryad repository. Library Hi Tech 35 , 332–342 (2017).
Article Google Scholar
Brickley, D., Burgess, M. & Noy, N. Google dataset search: Building a search engine for datasets in an open web ecosystem. In The World Wide Web Conference - WWW ‘19 , 1365–1375 (ACM Press, San Francisco, CA, USA, 2019).
Buneman, P., Dosso, D., Lissandrini, M. & Silvello, G. Data citation and the citation graph. Quantitative Science Studies 2 , 1399–1422 (2022).
Chao, T. C. Disciplinary reach: Investigating the impact of dataset reuse in the earth sciences. Proceedings of the American Society for Information Science and Technology 48 , 1–8 (2011).
Article ADS Google Scholar
Parr, C. et al . A discussion of value metrics for data repositories in earth and environmental sciences. Data Science Journal 18 , 58 (2019).
Eschenfelder, K. R., Shankar, K. & Downey, G. The financial maintenance of social science data archives: Four case studies of long–term infrastructure work. J. Assoc. Inf. Sci. Technol. 73 , 1723–1740 (2022).
Palmer, C. L., Weber, N. M. & Cragin, M. H. The analytic potential of scientific data: Understanding re-use value. Proceedings of the American Society for Information Science and Technology 48 , 1–10 (2011).
Zimmerman, A. S. New knowledge from old data: The role of standards in the sharing and reuse of ecological data. Sci. Technol. Human Values 33 , 631–652 (2008).
Cragin, M. H., Palmer, C. L., Carlson, J. R. & Witt, M. Data sharing, small science and institutional repositories. Philosophical Transactions of the Royal Society A: Mathematical, Physical and Engineering Sciences 368 , 4023–4038 (2010).
Article ADS CAS Google Scholar
Fear, K. M. Measuring and Anticipating the Impact of Data Reuse . Ph.D. thesis, University of Michigan (2013).
Borgman, C. L., Van de Sompel, H., Scharnhorst, A., van den Berg, H. & Treloar, A. Who uses the digital data archive? An exploratory study of DANS. Proceedings of the Association for Information Science and Technology 52 , 1–4 (2015).
Pasquetto, I. V., Borgman, C. L. & Wofford, M. F. Uses and reuses of scientific data: The data creators’ advantage. Harvard Data Science Review 1 (2019).
Gregory, K., Groth, P., Scharnhorst, A. & Wyatt, S. Lost or found? Discovering data needed for research. Harvard Data Science Review (2020).
York, J. Seeking equilibrium in data reuse: A study of knowledge satisficing . Ph.D. thesis, University of Michigan (2022).
Kilbride, W. & Norris, S. Collaborating to clarify the cost of curation. New Review of Information Networking 19 , 44–48 (2014).
Robinson-Garcia, N., Mongeon, P., Jeng, W. & Costas, R. DataCite as a novel bibliometric source: Coverage, strengths and limitations. Journal of Informetrics 11 , 841–854 (2017).
Qin, J., Hemsley, J. & Bratt, S. E. The structural shift and collaboration capacity in GenBank networks: A longitudinal study. Quantitative Science Studies 3 , 174–193 (2022).
Article PubMed PubMed Central Google Scholar
Acuna, D. E., Yi, Z., Liang, L. & Zhuang, H. Predicting the usage of scientific datasets based on article, author, institution, and journal bibliometrics. In Smits, M. (ed.) Information for a Better World: Shaping the Global Future. iConference 2022 ., 42–52 (Springer International Publishing, Cham, 2022).
Zeng, T., Wu, L., Bratt, S. & Acuna, D. E. Assigning credit to scientific datasets using article citation networks. Journal of Informetrics 14 , 101013 (2020).
Koesten, L., Vougiouklis, P., Simperl, E. & Groth, P. Dataset reuse: Toward translating principles to practice. Patterns 1 , 100136 (2020).
Du, C., Cohoon, J., Lopez, P. & Howison, J. Softcite dataset: A dataset of software mentions in biomedical and economic research publications. J. Assoc. Inf. Sci. Technol. 72 , 870–884 (2021).
Aryani, A. et al . A research graph dataset for connecting research data repositories using RD-Switchboard. Sci Data 5 , 180099 (2018).
Färber, M. & Lamprecht, D. The data set knowledge graph: Creating a linked open data source for data sets. Quantitative Science Studies 2 , 1324–1355 (2021).
Perry, A. & Netscher, S. Measuring the time spent on data curation. Journal of Documentation 78 , 282–304 (2022).
Trisovic, A. et al . Advancing computational reproducibility in the Dataverse data repository platform. In Proceedings of the 3rd International Workshop on Practical Reproducible Evaluation of Computer Systems , P-RECS ‘20, 15–20, https://doi.org/10.1145/3391800.3398173 (Association for Computing Machinery, New York, NY, USA, 2020).
Borgman, C. L., Scharnhorst, A. & Golshan, M. S. Digital data archives as knowledge infrastructures: Mediating data sharing and reuse. Journal of the Association for Information Science and Technology 70 , 888–904, https://doi.org/10.1002/asi.24172 (2019).
Lafia, S. et al . MICA Data Descriptor. Zenodo https://doi.org/10.5281/zenodo.8432666 (2023).
Lafia, S., Thomer, A., Bleckley, D., Akmon, D. & Hemphill, L. Leveraging machine learning to detect data curation activities. In 2021 IEEE 17th International Conference on eScience (eScience) , 149–158, https://doi.org/10.1109/eScience51609.2021.00025 (2021).
Hemphill, L., Pienta, A., Lafia, S., Akmon, D. & Bleckley, D. How do properties of data, their curation, and their funding relate to reuse? J. Assoc. Inf. Sci. Technol. 73 , 1432–44, https://doi.org/10.1002/asi.24646 (2021).
Lafia, S., Fan, L., Thomer, A. & Hemphill, L. Subdivisions and crossroads: Identifying hidden community structures in a data archive’s citation network. Quantitative Science Studies 3 , 694–714, https://doi.org/10.1162/qss_a_00209 (2022).
ICPSR. ICPSR Bibliography of Data-related Literature: Collection Criteria. https://www.icpsr.umich.edu/web/pages/ICPSR/citations/collection-criteria.html (2023).
Lafia, S., Fan, L. & Hemphill, L. A natural language processing pipeline for detecting informal data references in academic literature. Proc. Assoc. Inf. Sci. Technol. 59 , 169–178, https://doi.org/10.1002/pra2.614 (2022).
Hook, D. W., Porter, S. J. & Herzog, C. Dimensions: Building context for search and evaluation. Frontiers in Research Metrics and Analytics 3 , 23, https://doi.org/10.3389/frma.2018.00023 (2018).
https://www.icpsr.umich.edu/web/ICPSR/thesaurus (2002). ICPSR. ICPSR Thesaurus.
https://www.icpsr.umich.edu/files/datamanagement/icpsr-curation-levels.pdf (2020). ICPSR. ICPSR Curation Levels.
McKinney, W. Data Structures for Statistical Computing in Python. In van der Walt, S. & Millman, J. (eds.) Proceedings of the 9th Python in Science Conference , 56–61 (2010).
Wickham, H. et al . Welcome to the Tidyverse. Journal of Open Source Software 4 , 1686 (2019).
Fan, L., Lafia, S., Li, L., Yang, F. & Hemphill, L. DataChat: Prototyping a conversational agent for dataset search and visualization. Proc. Assoc. Inf. Sci. Technol. 60 , 586–591 (2023).
Download references
Acknowledgements
We thank the ICPSR Bibliography staff, the ICPSR Data Curation Unit, and the ICPSR Data Stewardship Committee for their support of this research. This material is based upon work supported by the National Science Foundation under grant 1930645. This project was made possible in part by the Institute of Museum and Library Services LG-37-19-0134-19.
Author information
Authors and affiliations.
Inter-university Consortium for Political and Social Research, University of Michigan, Ann Arbor, MI, 48104, USA
Libby Hemphill, Sara Lafia, David Bleckley & Elizabeth Moss
School of Information, University of Michigan, Ann Arbor, MI, 48104, USA
Libby Hemphill & Lizhou Fan
School of Information, University of Arizona, Tucson, AZ, 85721, USA
Andrea Thomer
You can also search for this author in PubMed Google Scholar
Contributions
L.H. and A.T. conceptualized the study design, D.B., E.M., and S.L. prepared the data, S.L., L.F., and L.H. analyzed the data, and D.B. validated the data. All authors reviewed and edited the manuscript.
Corresponding author
Correspondence to Libby Hemphill .
Ethics declarations
Competing interests.
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ .
Reprints and permissions
About this article
Cite this article.
Hemphill, L., Thomer, A., Lafia, S. et al. A dataset for measuring the impact of research data and their curation. Sci Data 11 , 442 (2024). https://doi.org/10.1038/s41597-024-03303-2
Download citation
Received : 16 November 2023
Accepted : 24 April 2024
Published : 03 May 2024
DOI : https://doi.org/10.1038/s41597-024-03303-2
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies
Sign up for the Nature Briefing newsletter — what matters in science, free to your inbox daily.

- Open access
- Published: 13 May 2024
Nursing students’ perspectives on patients' safety competencies: a cross-sectional survey
- Yasmin Ibrahim Abdelkader Khider 1 ,
- Shaimaa Mohamed Elghareeb Allam 1 ,
- Mohamed A. Zoromba 2 , 3 &
- Heba Mohammed Mahmoud Elhapashy 1
BMC Nursing volume 23 , Article number: 323 ( 2024 ) Cite this article
134 Accesses
Metrics details
Nurses constitute the largest body of healthcare professionals globally, positioning them at the forefront of enhancing patient safety. Despite their crucial role, there is a notable gap in the literature regarding the comprehension and competency of nursing students in patient safety within Egypt. This gap underscores the urgent need for research to explore how nursing students perceive patient safety and the extent to which these competencies are integrated into their clinical and educational experiences. Understanding these perspectives is essential for developing targeted interventions that can significantly improve patient safety outcomes. The objective of this study was to fill this gap by assessing the perspectives of nursing intern students on patient safety competencies, thereby contributing to the global efforts in enhancing patient safety education and practice.
In this research, a cross-sectional study design was employed to investigate the topic at hand. A purposive sample of 266 nursing intern students was enrolled from the Faculty of Nursing at Mansoura University. The data were collected using a patient safety survey. Subsequently, the collected data underwent analysis through the application of descriptive and inferential statistical techniques using SPSS-20 software.
Among the studied intern nursing students, we found that 55.3% and 59.4% of the involved students agreed that they could understand the concept of patient safety and the burden of medical errors. Regarding clinical safety issues, 51.1% and 54.9% of the participating students agreed that they felt confident in what they had learned about identifying patients correctly and avoiding surgical errors, respectively. Concerning error reporting issues, 40.2% and 37.2% of the involved students agreed that they were aware of error reports and enumerated the barriers to incident reporting, respectively. There was a statistically significant difference between the nursing student patient safety overview domain and their age ( p = 0.025).
Conclusions
Our study's compelling data demonstrated that intern students who took part in the patient safety survey scored higher overall in all patient safety-related categories. However, problems with error reporting showed the lowest percentage. The intern students would benefit from additional educational and training workshops to increase their perspectives on patients' safety competencies.
Peer Review reports
Introduction
Patient safety refers to the perspectives, beliefs, attitudes, and values shared among members of the health community that focus on the prevention of errors and adverse effects on patients associated with health care [ 1 ]. In addition to becoming more efficient, health care has also grown more complicated due to the increased use of novel tools, medications, and therapies [ 2 ]. Medical errors (MEs) are a major public health concern that endangers patient safety significantly. Research conducted in Australia found that 16.6% of all admissions resulted in preventable negative outcomes, with approximately 5% of cases involving an iatrogenic injury ending in death [ 3 ].
Adverse event incidence rates varied from 2.9% to 16.6%. About 5% to 13% of the patients in these situations passed away, but 25% to 50% of them were thought to have been avoidable [ 4 ]. MEs can occur in any care setting, including hospitals, health centers, clinics, and laboratories; thus, they can negatively affect patient safety [ 5 ].
Medical errors raise hospital and medical expense costs in both wealthy and underdeveloped nations, which lowers the standard of healthcare systems. The most common errors that practitioners should exercise great care to avoid are catheter-associated urinary tract infections, central line bloodstream infections, adverse drug events, falls, pressure ulcers, obstetrical adverse events, venous thrombosis, surgical site infections, and the development of ventilator-associated pneumonia. Errors can be prevented by changing the healthcare system to make it more difficult for practitioners to perform incorrect actions and easier for them to do correct ones [ 6 ].
More time is spent with patients by nurses than by any other healthcare practitioner, making them the largest profession in the health sector. Therefore, in addition to advocating for patient safety, nurses can significantly reduce errors [ 7 ]. Students’ perspectives are how students think to respond about what they have done or about what they learned [ 8 ]. The viewpoints of nursing students can shed light on how nursing education helps prepare students to give safe care both while they are enrolled in school and after they become practitioners. Their identification of the strengths and limitations of curriculum and teaching practices can help guide our efforts to enhance nurse education and improve healthcare systems [ 9 ].
Therefore, nursing college students must comprehend and develop patient safety competency, as this fosters patients' recuperation, averts unfavorable situations, and has been a global priority for academic and healthcare institutions. Additionally, ensuring patient safety not only improves healthcare outcomes but also enhances the reputation and credibility of healthcare institutions. By prioritizing patient safety, nursing colleges can produce competent and skilled nurses who contribute to the overall development and progress of the healthcare industry [ 10 ].
Consequently, we investigated how nursing college final-year students perceived their level of patient safety competency. These results will be useful in formulating plans to raise students' proficiency in patient safety among health professionals.
Significance of the study
Patient safety issues have become a priority in health policy and healthcare management. It was reported that MEs are the third principal cause of death in the USA, with an estimated 251,000 deaths annually. Patient safety is considered an endemic concern by the WHO. However, literature reports that nursing students might need more knowledge and skills to enhance patient safety. Moreover, the students need help managing errors that might occur [ 11 ].
Also, nursing curricula need more emphasis on patient safety. Graduate nurses should have sufficient knowledge to recognize potential safety risks [ 12 ]. Sufficient knowledge will increase nursing students' confidence to protect patients from potential harm, errors, and avoidable injuries [ 13 ]. Thus, it is imperative to evaluate nursing students’ perspectives on patients' safety competencies.
Aim of the study
The study aims to evaluate nursing students’ perspectives on patients' safety competencies.
Research objectives
Assess nursing students' knowledge regarding patient safety competencies.
Evaluate nursing students' perspectives on patient safety competencies.
Research questions
What are nursing students’ perspectives on patients' safety competencies?
Research design
A descriptive cross-sectional design was utilized in this study. Descriptive cross-sectional studies explain things or how things are related to each other at a specific time [ 14 ]. A descriptive cross-sectional design was suitable for assessing nursing students’ perspectives on patients' safety competencies in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STORBE) statement ( Appendix ).
This study was conducted at the Faculty of Nursing, Mansoura University, Egypt.
Study sample
A purposive sample of 266 internship nursing students from both genders was included in the study. Purposive sampling was chosen due to its effectiveness in identifying and selecting individuals that meet a predefined set of characteristics essential for the research question. This approach ensured that the participants had a foundational understanding of nursing practices and were in the process of applying these concepts in a clinical environment, making their perspectives on patient safety both unique and immediately relevant. Students were chosen because they have received sufficient training to practice nursing care, and it is also important to investigate nursing safety considerations among these students before offering complete care to patients.
The appropriate sample size for this investigation was determined using the Steven K. Thompson equation [ 15 ]. There are 516 students enrolled in nursing internships overall, according to the Student Affairs administration. A minimum of 221 students should be included in the sample size for this study, according to the previously provided data. As the confidence level is 95%, the error proportion is 0.05, and the probabilities are 50%, add 20% for better data and follow-up drop. So the final number should be 266 nursing students.
Inclusion criteria include intern nursing students of both genders who are enrolled in the orientation program in the faculty of nursing at Mansoura University, willing to participate, and signing informed consent. Exclusion criteria include students who have a nursing diploma before joining the faculty of nursing, as those students have more knowledge and clinical experience than other students.
One tool was used in this study to collect pertinent data.
Patient Safety Survey (PSS)
Our literature review revealed that while there are several established tools for assessing patient safety competencies, most are tailored to qualified healthcare professionals or general nursing students, without a specific focus on internship nursing students in the Egyptian context. Furthermore, our study aimed to explore nuanced aspects of patient safety competencies, including students' perspectives on error reporting and clinical safety issues specific to their internship experiences. These nuances were not adequately covered by existing tools. Therefore, to capture the specific competencies and perspectives of our target population accurately, we decided to develop PSS. Researchers developed this survey after reviewing national and international literature reviews [ 16 , 17 , 18 ]. This survey consists of 24 items, divided into two parts. Part one is used to assess internship nursing students’ socio-demographic data. This data includes four items: student name, age, gender, and residence.
Part two is designed to measure internship nursing students’ perspectives regarding patient safety issues. This part covers students’ perspectives in three domains: an overview of patient safety (five items), clinical safety issues (10 items), and error reporting (five items). A 5-point Likert scale, with one representing "strongly disagree" and five representing "strongly agree," was used to gauge the students' perspectives .
Validity and reliability
The researcher developed the study tool after reviewing national and international literature [ 16 , 17 , 18 ]. The content validity of the PSS was rigorously evaluated through a structured process involving a panel of seven experts in nursing education, patient safety, and research methodology. These experts were selected based on their extensive experience and contributions to the field, ensuring a comprehensive assessment of the tool's content. Initially, the development of the survey items was informed by an extensive review of both national and international literature on patient safety competencies. This ensured that the content of the tool was grounded in the latest research and best practices in the field. The draft version of the PSS was then presented to the expert panel for evaluation. Each expert independently assessed the relevance, clarity, and comprehensiveness of the survey items, using a standardized scale to rate each item.
Based on the expert ratings, the Content Validity Index (CVI) for the tool was calculated. The CVI provides a quantitative measure of the degree to which experts agree that the survey items are relevant and representative of the construct of patient safety competencies. For our tool, the CVI was calculated at 0.82, indicating a high level of agreement among experts and confirming the content validity of the PSS. A CVI of 0.82 suggests that the majority of the items were deemed relevant and essential for assessing patient safety competencies among nursing students.
In addition to assessing content relevance, the expert panel also provided feedback on the face validity of the tool, focusing on the clarity, simplicity, and readability of the items. This process ensured that the survey would be easily understood by the target population of nursing intern students. Following the expert panel review, several adjustments were made to enhance the clarity and respondent-friendliness of the survey. For instance, the original binary response format was modified to a five-point Likert scale to allow for a more nuanced expression of respondents' perspectives. Additionally, based on expert suggestions, specific items, such as “I know the institution of medicine report, To Error is Human, and its recommendations," were added to enrich the tool's comprehensiveness and relevance. The reliability of the tools was tested using Cronbach’s alpha coefficient (0.89 for the patient safety survey, part two).
Pilot study
A pilot study was conducted with 27 participants, representing 10% of the total sample, to test the tool's applicability in the research setting. Feedback from the pilot study identified potential issues and challenges. Modifications were made to the survey tool, ensuring relevance and comprehensibility and addressing practical issues.
Data collection
Ethical approval was obtained from the Research Ethics Committee of the Faculty of Nursing, Mansoura University . The study tool, a patient safety survey, was developed by the researcher based on a recent relevant literature review. A panel of seven experts in the associated fields evaluated the study instrument for face- and content-related validity, and any necessary adjustments were made in response. The reliability of the tools was tested using Cronbach’s alpha coefficient (0.89 for the patient safety survey, part two). A pilot study was carried out with 27 (10%) of the study sample to test the feasibility and applicability of the study tool, and it will be excluded from the study sample. The necessary modifications were made accordingly. The researchers introduced themselves to the selected internship nursing students. The researchers explained the nature and purpose of this study to the study sample. After accepting to participate in this study, the researchers started to collect students’ socio-demographic data and their perspectives regarding patient safety issues using the study tool. Each student was given the appropriate time to answer the patient safety survey (about 20–30 min). The data was collected from January to February 2024.
To avoid bias in the study, we employed a purposive sampling strategy to select a representative sample of internship nursing students from Mansoura University. This strategy was chosen based on specific inclusion and exclusion criteria designed to minimize selection bias and ensure that our sample accurately reflected the population of interest. Additionally, to address potential information bias, we rigorously developed and validated the Patient Safety Survey. The survey underwent a pilot study to identify and correct any ambiguities, further enhancing the reliability and validity of the data collected. The uniform application of a 5-point Likert scale across all survey items was a deliberate choice to provide a consistent measure of nursing students' perspectives, thereby reducing measurement bias. Additionally, we standardized the training for all researchers involved in data collection to ensure uniform survey administration. We took several measures to minimize response bias, including guaranteeing anonymity and confidentiality for all participants and making participation entirely voluntary. These steps were intended to foster an environment where students felt comfortable providing honest and accurate responses without fear of repercussions.
Statistical analysis of the data
The computer was fed data, and IBM SPSS software package version 20.0 was used for analysis. [IBM Corp. Armonk, NY] Numbers and percentages were used to describe the qualitative data. The distribution's normality was confirmed using the Kolmogorov–Smirnov test. The range (minimum and maximum), mean, standard deviation, and median were used to characterize quantitative data. The results were deemed significant at the 5% level. Student t-test: to compare two examined categories for quantitative variables that are regularly distributed. F-test (ANOVA): for normally distributed quantitative variables, to compare between more than two categories. Pearson coefficient: to correlate between two normally distributed quantitative variables.
Ethical considerations and human rights
The Research Ethical Committee of the Faculty of Nursing at Mansoura University in Egypt provided ethical permission (No.0526). After being fully informed about the purpose of the study, each intern nursing student who was enrolled gave their informed consent. The pupils were reminded by the researcher that participation is completely voluntary. Throughout the whole study, confidentiality, privacy, safety, and anonymity were guaranteed. Every participant was free to leave the research at any moment. The survey did not include participant names or any other type of identifying information. The Helsinki Declaration and other pertinent rules and regulations carry out every procedure.
Demographic characteristics
The study included a total of 266 students. About 57.9% of the involved students were aged 22, and 65% of them were female. Moreover, 64.7% of the enrolled students lived in rural areas. All the involved students (100%) were from Mansoura University (Table 1 ).
Students’ distribution according to the patient safety overview domain
Among the studied intern nursing students, we found that 55.3%, 59.4%, 40.6%, 41.7%, and 49.6% of the involved students agreed that they can understand the concept of patient safety, understand the burden of medical errors, differentiate between errors, adverse events, close call/near miss, and sentinel events, know the Institution of Medicine report “To Error is Human” and its recommendations, and are aware of the ethical aspect of patient safety. The total score of the patient safety overview domain (mean ± SD) was 19.76 ± 2.69 (Table 2 ).
Distribution of the studied students according to clinical safety issues
Regarding clinical safety issues, 50.4%, 51.1%, 54.9%, 52.3%, and 52.3% of the participating students agreed that they felt confident in what they had learned about curbing infection spread, identifying patients correctly, avoiding surgical errors, using medicines safely, and preventing venous thromboembolism, respectively. In addition, 51.1%, 52.3%, 47.7%, 48.1%, and 48.5% of the participating students agreed that they felt confident in what they had learned about customizing hospital discharges, using good hospital design principles, assembling better teams and rapid response systems, sharing data for quality improvement, and fostering an open-communication culture (Table 3 ).
Distribution of the studied students according to error reporting issues domain
Concerning their error reporting, 40.2%, 50%, 37.2%, 44.7%, and 41% of the involved students agreed that they were aware of error reports, understood the importance of incident reports, enumerated the barriers to incident reporting, listed the features of an incident report, and differentiated between manual and electronic incidence reports (Table 4 ).
Relation between nursing students’ perspectives toward patient safety, their gender, and their age
Regarding gender, there was no statistically significant difference between nursing students' perceptions of patient safety and their gender ( p > 0.05). At the same time, there was a statistically significant difference between the nursing student patient safety overview domain and their age ( p = 0.025) (Table 5 ).
Correlation among nursing students’ perspectives domains toward patient safety
There were very high positive correlations between the overall patient safety score and its three domains: the patient safety overview domain ( r = 0.806, p < 0.001), the clinical safety issues domain ( r = 0.932, p < 0.001), and the error reporting domain ( r = 0.842, p < 0.001). Moreover, there was a statistically significant difference between the patient safety overview domain and the clinical safety issues domain ( p < 0.001) with a high positive correlation ( r = 0.659). In addition, there was a moderately positive correlation between the patient safety overview domain and the error reporting domain with a statistically significant difference ( r = 0.543, p < 0.001). Also, there was a high positive correlation between the clinical safety issues domain and the error reporting domain ( r = 0.660, p < 0.001) (Table 6 ).
Nursing students are the foundation upon which nursing care for patients will be built, and patient safety must be considered the cornerstone of the student’s education before graduation to prepare them well to provide the best care with the highest quality and efficiency [ 19 ]. Working across professions in clinical fields requires an early understanding of the responsibilities of different healthcare providers and the extent of nursing students' engagement [ 20 ].
Using a self-reported approach, we evaluated nursing students' perspectives of patient safety competency concerning safety overview, clinical safety issues, and error reporting issues. Our study's compelling data demonstrated that intern students who took part in the patient safety survey scored higher overall in all patient safety-related categories. When it came to clinical safety considerations, the students received the highest percentage of points. On the other hand, problems with error reporting showed the lowest percentage.
The clinical safety dimension, with its focus primarily on infection control, patient identification, safe medication administration, and waste disposal, might be the most familiar to students, as our students start clinical training from the first academic level in the hospital with regular and varied evaluations that help them to have a comprehensive understanding of nursing students' proficiency in infection control and patient identification. Another possible explanation for this is that combining written assessments, practical evaluations, simulations, and real-world clinical experiences in our faculty allows educators to gauge students' competence and readiness for professional practice, which increases their knowledge base.
This is in line with the results of a study in Portugal, which reported a high perception of students in terms of infection control [ 21 ]. Another study conducted in Saudi Arabia indicated a modest perception among nursing students regarding infection prevention [ 22 ]. Regarding the error reporting issue, this is because students were worried about disciplinary actions, damage to their reputation, or a potential impact on their academic and professional future. Also, the majority of our students are from rural areas with a blame culture present that can discourage open communication about error reporting.
Another significant aspect of the safety overview domain is that students have a deeper perspective on the burden of medication errors and the concept of patient safety. This finding might relate to prior exposure to patient safety-related topics. This is in harmony with those of Chan 2019, who reported students had a good perception of general terms and the concept of safety [ 23 ]. Another study assessing medical students’ knowledge, skills, and attitudes also reported high perceptions of students regarding general aspects of patient safety [ 24 ].
Another interesting finding regarding clinical safety issues is that the high perspective and confidence percentage about avoiding surgical error and the lowered perspective percentage represented assembling better teams and rapid response systems. We attribute this superiority in preventing surgical errors to the fact that the majority of respondents work part-time in the surgical and plastic surgery hospitals spread across the governorate, which gave them practical experience in this part. In combination with education, experience, mentorship, and a supportive healthcare culture, this contributes to nursing interns developing a positive perception regarding avoiding surgical errors. Following the present results, a previous study in Turkey demonstrated that nurses who formerly received preparation on patient safety had a higher statistical percentage [ 25 ]. However, the findings of the current study do not support the previous research that reported that pre-licensure nursing students have little knowledge regarding perioperative care and should be well-trained again [ 26 ].
Regarding lack of perspective in assembling a better team and rapid response system, because interns feel hesitant to voice concerns or take charge due to hierarchical structures, insufficient resources, both in terms of staffing and equipment, may hinder the interns' ability to assemble an effective team and respond. This outcome is contrary to that of Kamran, who reported that the best score of safety was given for team functioning and response [ 27 ].
Regarding gender, there was no statistically significant difference between nursing students’ perspectives on patient safety and their gender ( p > 0.05). This is in line with those of Ramírez, who reported that the differences in means between genders were not significantly different in the overall perspective of patient safety [ 28 ]. Additionally, those who stated that there were no discernible variations in opinions about gender and past exposure to medical errors ( p = > 0.05) [ 27 ]. This outcome is contrary to that stated: male students apparent competence in “working in teams” is higher than that of females [ 29 ].
Another pilot study reported that the overall patient safety grade, the number of reported events, and the number of reported events by nursing students were significantly predicted by several patient safety competence dimensions ( p ≤ 0.05) [ 30 ].
Our results indicated that there is a significant relationship between age and patient safety. The rationale of this finding is that during the academic years, including clinical practicum, students’ ability to communicate with patients and other health professionals clearly and consistently seemed to increase with age. Similar positive student assessments about safety and age have been noted in a study by Usher, who reported highly significant scores of patient safety with age and level of students. The results are also inconsistent with those conducted in Australia and New Zealand that assess nursing students' patient safety knowledge. These results corroborate the findings of a great deal of the previous work reported a significant difference was found in the patient safety competence of nursing students with year of study [ 29 ].
Another finding that stands out from the results is that there were very high positive correlations between the overall patient safety score and the three domains. These results reflect those of another study that examined the relationship between all-cause harm and patient safety and demonstrated strong correlations between all-cause harm measures and patient safety culture [ 31 ]. These findings also lend support to previous literature, which reported that subscales of safety correlated positively with the perceived patient safety culture scale [ 32 ]. Our finding also supports evidence from previous observations that found a positive correlation between the six domains and safety-related behaviors [ 33 ].
Another finding is that there was a statistically significant difference between the patient safety overview domain and the clinical safety issues domain. The same results were reported in a cross-sectional study conducted in China that assessed the patient safety competency of Chinese nurses [ 34 ]. Also, there was a high positive correlation between the clinical safety issues domain and the error reporting domain; this finding is consistent with Mahsoon [ 35 ]. This finding is contrary to the findings of another Saudi cross-sectional study that showed a significant negative correlation [ 36 ]. Another vital aspect of patient safety that students recognized is likewise related to understanding the function of trust and error reporting in maintaining patient safety.
Nursing students ought to have a strong understanding of patient safety, grounded in the highest standards of nursing care. Students completing nursing internships knew about patient safety. This result supports the conclusion drawn from several recent studies that patient safety education improves nurses' patient safety competence. These elements could have an impact on nursing students' patient safety competence and performance. The intern students would benefit from additional educational and training workshops to increase their perspectives on patients' safety competencies. Therefore, we recommend that academic institutions and medical facilities reorganize the framework for patient safety education to begin at the earliest academic level while taking into account students' pedagogical demands and varying safety levels. This will be done to increase public awareness of patient safety education. Establishing a structured curriculum on patient safety and upholding this shift in hospital culture is also crucial if we are to optimize the impact of patient safety education. Future research in various cultural and contextual settings is necessary to enhance our understanding of the variables affecting patient safety in nursing practice and education.
Limitations
When evaluating the results, it is important to take into account the study's limitations, which include its cross-sectional design and the inclusion of only one site. An additional constraint pertains to the survey's timing, which was carried out during the internship's orientation program. The student was not entirely tasked with providing comprehensive and intense care to patients with minimal exposure to clinical safety and real-error reporting concerns. The results could have been altered if the data had been gathered closer to the internship's conclusion, when the students would have gained more clinical experience. The study was conducted at a single nursing faculty; the use of purposive sampling, while ensuring a detailed exploration of our specific research question, may also limit the generalizability of the results. Therefore, it is recommended that it be repeated across other faculties to enable generalization of results.
Availability of data and materials
The datasets generated and/or analyzed during the current study are not publicly available due to protecting the confidentiality of the participants, but are available from the corresponding author upon reasonable request.
Agbar F, Zhang S, Wu Y, Mustafa M. Effect of patient safety education interventions on patient safety culture of health care professionals: Systematic review and meta-analysis. Nurse Educ Pract. 2023;67: 103565. https://doi.org/10.1016/j.nepr.2023.103565 .
Article PubMed Google Scholar
World Health Organization. Global patient safety action plan 2021–2030: towards eliminating avoidable harm in health care. World Health Organization. 2021; Available at https://www.who.int/teams/integrated-health-services/patient-safety/policy/global-patient-safety-action-plan .
Doshmangir L, Najafi B, Akbari Sari A, Sergeevich GV. Incidence rate and financial burden of medical errors and policy interventions to address them: a multi-method study protocol. Health Serv Outcomes Res Method. 2022;22(2):244–52. https://doi.org/10.1007/s10742-021-00261-9 .
Article Google Scholar
Han Y, Kim JS, Seo Y. Cross-sectional study on patient safety culture, patient safety competency, and adverse events. West J Nurs Res. 2020;42(1):32–40. https://doi.org/10.1177/0193945919838990 .
Schwarz CM, Hoffmann M, Schwarz P, Kamolz LP, Brunner G, Sendlhofer G. A systematic literature review and narrative synthesis on the risks of medical discharge letters for patients’ safety. BMC Health Serv Res. 2019;19:1. https://doi.org/10.1186/s12913-019-3989-1 .
Article CAS Google Scholar
Khammarnia M, Setoodehzadeh F. Medical error as a challenge in Iran’s health system. Health Scope. 2017;6(1):61597. https://doi.org/10.17795/jhealthscope-39743 .
Dirik HF, Samur M, Seren Intepeler S, Hewison A. Nurses’ identification and reporting of medication errors. J Clin Nurs. 2019;28(5–6):931–8. https://doi.org/10.1111/jocn.14716 .
Nadhiroh NA. EFL Students’ Perception on The Use of Google Classroom in Language Assessment and Testing Development Course at IAIN Kediri (Doctoral dissertation, IAIN Kediri). 2022. https://etheses.iainkediri.ac.id:80/id/eprint/7700 .
Tuomikoski AM, Ruotsalainen H, Mikkonen K, Kääriäinen M. Nurses’ experiences of their competence at mentoring nursing students during clinical practice: a systematic review of qualitative studies. Nurse Educ Today. 2020;85: 104258. https://doi.org/10.1016/j.nedt.2019.104258 .
Julnes SG, Myrvang T, Reitan LS, Rønning G, Vatne S. Nurse leaders’ experiences of professional responsibility towards developing nursing competence in general wards: A qualitative study. J Nurs Manag. 2022;30(7):2743–50. https://doi.org/10.1111/jonm.13745 .
Article PubMed PubMed Central Google Scholar
Abdelrahman SM, Mohamed FR. Patient safety culture as perceived by internship nursing students as perceived by internship nursing students. Int J Adv Nurs Stud. 2017;6(2):67–70. https://doi.org/10.14419/ijans.v6i2.7681 .
Mousavi-Roknabadi RS, Momennasab M, Groot G, Askarian M, Marjadi B. Medical error and under-reporting causes from the viewpoints of nursing managers: A qualitative study. Int J Prev Med. 2022;13:103. https://doi.org/10.4103/ijpvm.IJPVM_500_20 .
Alshyyab MA, Albsoul R, Fitzgerald G. Factors influencing patient safety culture in the operating room in a teaching hospital in Jordan: a qualitative descriptive study. The TQM Journal. 2023;35(7):1722–42. https://doi.org/10.1108/TQM-04-2022-0133 .
Ihudiebube-Splendor CN, Chikeme PC. A descriptive cross-sectional study: Practical and feasible design in investigating health care–seeking behaviors of undergraduates. SAGE Publications Ltd; 2020. https://doi.org/10.4135/9781529742862 .
Thompson, Steven K. Sampling. Vol. 755. John Wiley & Sons. 2012. https://doi.org/10.1111/j.1083-6101.2007.00336.x .
Dimitriadou M, Merkouris A, Charalambous A, Lemonidou C, Papastavrou E. The knowledge about patient safety among undergraduate nurse students in Cyprus and Greece: a comparative study. BMC Nurs. 2021;20(1):110. https://doi.org/10.1186/s12912-021-00610-6 .
Torkaman M, Sabzi A, Farokhzadian J. The effect of patient safety education on undergraduate nursing students’ patient safety competencies. Community Health Equity Res Policy. 2022;42(2):219–24. https://doi.org/10.1177/0272684X20974214 .
Usher K, Woods C, Parmenter G, Hutchinson M, Mannix J, Power T, Chaboyer W, Latimer S, Mills J, Siegloff L, Jackson D. Self-reported confidence in patient safety knowledge among Australian undergraduate nursing students: A multi-site cross-sectional survey study. Int J Nurs Stud. 2017;71:89–96. https://doi.org/10.1016/j.ijnurstu.2017.03.006 .
Lee SE, Dahinten VS. Evaluating a patient safety course for undergraduate nursing students: A quasi-experimental study. Collegian. 2023;30(1):75–83. https://doi.org/10.1016/j.colegn.2022.06.00 .
Doody O, Hennessy T, Bright AM. The role and key activities of Clinical Nurse Specialists and Advanced Nurse Practitioners in supporting healthcare provision for people with intellectual disability: An integrative review. Int J Nurs Stud. 2022;129: 104207. https://doi.org/10.1016/j.ijnurstu.2022.104207 .
Parreira P, Santos-Costa P, Pardal J, Neves T, Bernardes RA, Serambeque B, Sousa LB, Graveto J, Silén-Lipponen M, Korhonen U, Koponen L. Nursing Students’ Perceptions on Healthcare-Associated Infection Control and Prevention Teaching and Learning Experience in Portugal. Journal of Personalized Medicine. 2022;12(2):180. https://doi.org/10.3390/jpm12020180 .
Tumala RB, Almazan J, Abdulaziz H, Felemban EM, Alsolami F, Alquwez N, Alshammari F, Tork HM, Cruz JP. Assessment of nursing students perceptions of their training hospital’s infection prevention climate: A multi-university study in Saudi Arabia. Nurse Educ Today. 2019;81:72–7. https://doi.org/10.1016/j.nedt.2019.07.003 .
Chan R, Booth R, Strudwick G, Sinclair B. Nursing students’ perceived self-efficacy and the generation of medication errors with the use of an electronic medication administration record (eMAR) in clinical simulation. Int J Nurs Educ Scholarsh. 2019;16(1):20190014. https://doi.org/10.1515/ijnes-2019-0014 .
Abdi Z, Delgoshaei B, Ravaghi H, Heyrani A. Changing medical students’ knowledge, skills, and attitudes about patient safety. HealthMED. 2012; 6(9):3129–5. Available at https://www.researchgate.net/publication/233843540_Changing_Medical_Students'_Knowledge_Skills_and_Attitudes_about_Patient_Safety .
Ünver S, Yeniğün SC. Patient safety attitude of nurses working in surgical units: A cross-sectional study in Turkey. J Perianesth Nurs. 2020;35(6):671–5. https://doi.org/10.1016/j.jopan.2020.03.012 .
Beitz JM. Addressing the perioperative nursing shortage through education: A perioperative imperative. AORN J. 2019;110(4):403–14. https://doi.org/10.1002/aorn.12805 .
Kamran R, Bari A, Khan RA, Al-Eraky M. Patient safety awareness among undergraduate medical students in Pakistani medical school. Pak J Med Sci. 2018;34(2):305. https://doi.org/10.12669/pjms.342.14563 .
Ramírez-Torres CA, Rivera-Sanz F, Cobos-Rincon A, Sufrate-Sorzano T, Juárez-Vela R, Gea-Caballero V, Tejada Garrido CI, ColadoTello ME, Durante A, Santolalla-Arnedo I. Perception of patient safety culture among nursing students: A cross-sectional study. Nurs Open. 2023;10(12):7596–602. https://doi.org/10.1002/nop2.1995 .
Alquwez N, Cruz JP, Alshammari F, Felemban EM, Almazan JU, Tumala RB, Alabdulaziz HM, Alsolami F, Silang JP, Tork HM. A multi-university assessment of patient safety competence during clinical training among baccalaureate nursing students: A cross-sectional study. J Clin Nurs. 2019;28(9–10):1771–81. https://doi.org/10.1111/jocn.14790 .
Dominika K, Daniela B, Dominika H, Katarina Z. Nursing students’ perception of patient safety culture during the Covid-19 pandemic–results of a pilot study. Acta Medica Martiniana. 2022;22(1):45–53. https://doi.org/10.2478/acm-2022-0006 .
Sammer C, Hauck LD, Jones C, Zaiback-Aldinger J, Li M, Classen D. Examining the relationship of an all-cause harm patient safety measure and critical performance measures at the frontline of care. J Patient Saf. 2020;16(1):110. https://doi.org/10.1097/PTS.0000000000000468 .
Mihdawi M, Al-Amer R, Darwish R, Randall S, Afaneh T. The influence of nursing work environment on patient safety. Workplace health & safety. 2020;68(8):384–90. https://doi.org/10.1177/2165079920901533 .
Kong LN, Zhu WF, He S, Chen SZ, Yang L, Qi L, Peng X. Attitudes towards patient safety culture among postgraduate nursing students in China: A cross-sectional study. Nurse Educ Pract. 2019;38:1–6. https://doi.org/10.1016/j.nepr.2019.05.014 .
Yan L, Yao L, Li Y, Chen H. Assessment and analysis of patient safety competency of Chinese nurses with associate degrees: A cross-sectional study. Nurs Open. 2021;8(1):395–403. https://doi.org/10.1002/nop2.640 .
Mahsoon AN, Dolansky M. Safety culture and systems thinking for predicting safety competence and safety performance among registered nurses in Saudi Arabia: a cross-sectional study. J Res Nurs. 2021;26(1–2):19–32. https://doi.org/10.1177/17449871209761 .
Alzahrani N, Jones R, Abdel-Latif ME. Attitudes of doctors and nurses toward patient safety within emergency departments of two Saudi Arabian hospitals. BMC Health Services Research. 2018; 18:1-7. https://orcid.org/0000-0001-9115-864 .
Download references
Acknowledgements
The authors would like to thank the nursing student who participated in this study.
Open access funding provided by The Science, Technology & Innovation Funding Authority (STDF) in cooperation with The Egyptian Knowledge Bank (EKB). This research did not receive explicit support from any public organizations, businesses, or the private sector.
Author information
Authors and affiliations.
Medical-Surgical Nursing Department, Faculty of Nursing, Mansoura University, Mansoura, Egypt
Yasmin Ibrahim Abdelkader Khider, Shaimaa Mohamed Elghareeb Allam & Heba Mohammed Mahmoud Elhapashy
College of Nursing, Prince Sattam Bin Abdulaziz University, Al-Kharj, Saudi Arabia
Mohamed A. Zoromba
Psychiatric and Mental Health Nursing Department, Faculty of Nursing, Mansoura University, Mansoura, Egypt
You can also search for this author in PubMed Google Scholar
Contributions
YIAK: conceptualization, data collection, validation, visualization, original draft preparation, and writing; SMEA: reviewing, editing, and resources; MAZ: software, and data analysis; HMME: reviewing, editing, and resources. All the authors have read and approved the final version of the manuscript to be published.
Corresponding author
Correspondence to Yasmin Ibrahim Abdelkader Khider .
Ethics declarations
Ethics approval and consent to participate.
The Mansoura University Faculty of Nursing's Research Ethical Committee approved the researchers after careful consideration of their proposal, as evidenced by the code Ref. No. 0526. The study's aims were effectively conveyed to all participants, and written consent, after proper explanation, was acquired from each individual. The experimental approach involving human subjects dutifully adhered to the guidelines set forth by national, international, and institutional bodies, or the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Supplementary material 1., rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Khider, Y.I.A., Allam, S.M.E., Zoromba, M.A. et al. Nursing students’ perspectives on patients' safety competencies: a cross-sectional survey. BMC Nurs 23 , 323 (2024). https://doi.org/10.1186/s12912-024-01966-1
Download citation
Received : 28 February 2024
Accepted : 22 April 2024
Published : 13 May 2024
DOI : https://doi.org/10.1186/s12912-024-01966-1
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Nursing students
- Patients’ safety
- Competencies
BMC Nursing
ISSN: 1472-6955
- General enquiries: [email protected]
ORIGINAL RESEARCH article
Relationships between job satisfaction, occupational burnout and rationing of care among intensive care unit nurses.

- 1 Department of Nursing, Institute of Health Protection, The Bronisław Markiewicz Academy of Applied Sciences, Jarosław, Poland
- 2 Department of Integrated Medical Care, Medical University of Bialystok, Bialystok, Poland
- 3 Department of Nursing, Institute of Health Protection, State Academy of Applied Sciences, Przemyśl, Poland
Introduction: Rationing of nursing care is referred to as overlooking aspects of required patient care. Its result is incomplete or delayed services provided to the patient. Anesthesia nurses employed in an intensive care unit are exposed to a significant workload. Particularly heavy is the psychological burden leading in many cases to the onset of burnout syndrome and a decrease in job satisfaction.
The aim of this paper: Was to determine the relationship between occupational burnout, job satisfaction and rationing of care among anesthesia nurses employed in intensive care units.
Materials and methods: The study group consisted of 477 anesthesia nurses employed in intensive care units in Poland. The study was conducted between December 2022 and January 2023. The research tools were BERNCA-R questionnaire, Job Satisfaction Scale questionnaire and Maslach Burnout Inventory questionnaire, which were distributed to selected hospitals with a request to be forwarded to intensive care units and completed. In the statistical analysis, correlations were calculated using Spearman’s rho coefficient, reporting the intensity of the relationship and its positive or negative direction. The analysis was performed using the IBM SPSS 26.0 package with the Exact Tests module.
Results: The mean score of the BERNCA questionnaire was 1.65 ± 0.82. The mean score of occupational burnout was 60.82 ± 10.46. The level of emotional exhaustion, which significantly affects occupational burnout, was 26.39 ± 6.07, depersonalization was 14.14 ± 3.21 and lack of personal achievement was 20.29 ± 4.70. All the scores obtained exceeded the threshold of 50% of total points, which indicates the presence of occupational burnout at a significant level. The job satisfaction of the nurses surveyed was above mean at 23.00 ± 5.2 out of 35 total points.
Conclusion: The results proved that there is a statistically significant, although with a weak strength of association, correlation between occupational burnout and rationing of care by anesthesia nurses. As the limitation of anesthesia nurses’ ability to perform certain activities increases, their job satisfaction decreases. In a work environment that is conducive to nurses, there are fewer job responsibilities that are unfulfilled. Therefore, it is essential to create a friendly work environment for nursing staff that will promote the provision of services at the highest possible level.
1 Introduction
Providing quality services is a priority activity for healthcare units, since good quality translates into health, trust and safety in terms of the patient’s life. The quality of care is considered mainly through the qualifications and competence of medical personnel, infrastructure and equipment base, as well as through the degree of patient satisfaction ( 1 ). Nurses, by virtue of their professional function, are in the closest contact with the patient. They are the ones who create the image of the facility and influence the climate of treatment ( 2 , 3 ).
The concept of care overlooking is a fairly new phenomenon. It first appeared in 2006 introduced by Beatrice J. Kalisch and can be considered in any field of nursing. It refers to errors associated with the omission of all or part of a particular aspect of care ( 4 , 5 ). The definition of care rationing in nursing refers to the deliberate failure to perform tasks resulting from patient care due to lack of time. Available publications prove that skipping care is directly related to the failure to ensure patient safety ( 6 – 9 ). The reasons for this phenomenon can be staff shortages, increased demand for care, new technologies and treatment methods, as well as greater patient awareness ( 10 , 11 ). The totality of the aforementioned aspects translates into increased expenditures of time and labor incurred by nursing staff ( 12 – 14 ). The concept of care rationing according to Schubert et al. assumes that all nursing activities are equivalent, so that it is possible to achieve not only the desired activities, but also those expected by patients and the nursing diagnosis made, has a very strong impact on care rationing ( 15 , 16 ).
Job satisfaction is understood as a higher level of job fulfillment. A satisfied employee has a higher sense of self-esteem and satisfaction of needs. In addition, work should be a place of self-fulfillment for employees; one in which they feel satisfied with their professional development and intellectual challenges. This, in turn, creates a sense of identification with the organization’s goals. Satisfaction, including job satisfaction, is also understood as an individual’s ability to realize their needs, goals, values, and beliefs ( 17 ).
Job satisfaction has been the subject of many studies on organizational behavior. Lu et al. ( 18 ) demonstrate that satisfaction on job satisfaction consists of several of various elements, including working conditions, communication, nature of work, organizational policies and procedures, pay and conditions, promotion opportunities, recognition, appreciation, safety, supervision and relationships. Although the description of job satisfaction varies, several common factors emerge in various studies, which include working conditions, organizational environment and perceived stress, role conflict and ambiguity, role perception and content, and organizational and professional commitment ( 19 ). Job satisfaction is considered a global problem; however, it is also necessary to improve the quality of care provided and the work environment in healthcare organizations, as lack of job satisfaction among nurses can affect their practice, which in turn can directly or indirectly affect patient satisfaction ( 20 ).
The nursing profession is associated with many stressful situations and a heavy workload. Contact with patients and their loved ones, lack of support from superiors often leads to psychotic symptoms, depression, sleep and wakefulness disorders in this professional group ( 21 , 22 ). The causes of burnout can be traced to three areas: individual interpersonal and organizational. The above conditions may or may not promote occupational burnout ( 23 ). Occupational burnout syndrome usually begins unnoticed and the person affected often does not recognize the first symptoms. A common definition of the process is that it is a prolonged reaction to interpersonal and emotional stressors operating at work. Initially there is fatigue, irritability, tension, hyperactivity associated with symptoms of psychophysical exhaustion. As a result of the stress associated with the state of tension in the next phase, there is a loss of energy, discouragement and there are signs of depression related solely to the work situation ( 24 ). While studying the phenomenon of burnout, Maslach and Jackson distinguished two groups of variables: factors that can promote burnout and behaviors that help effectively combat burnout. The result of the study was the clarification of a characteristic picture for occupational burnout among nurses. This phenomenon increases with an increase in assigned tasks or a decrease in decision-making opportunities at work. These factors result in feelings of emotional exhaustion and a tendency to depersonalize patients. Depersonalization increases when feedback from patients decreases. According to Jackson and Schuler’s study, the risk of occupational burnout increases with the inability to control the environment. This finding was based on the premise that a rewarding environment for an employee is one that he or she can influence, while an unfavorable environment is one in which the ability to control is limited ( 25 ).
The work of the anesthesia nurse is one of the most difficult and responsible specialties in the profession due to its nature. Nurses working in intensive care units are particularly vulnerable to occupational burnout syndrome and belong to high-risk groups. The work, the essence of which is the care and nursing of a person in a life-threatening condition, such as after an accident, after surgery, in an advanced stage of illness or in a terminal state, exhausts psychologically primarily by constantly moving around final, critical issues, exhausts by its intensity ( 26 ).
Rationing of nursing care has a significant impact on the quality of services provided ( 22 ). Therefore, the authors set the aim of this study to investigate the relationship between occupational burnout, job satisfaction and rationing of care by anesthesia nurses employed in intensive care units. Analysis of such correlations will answer the question of whether the number of skipped activities by anesthesia nurses is lower in a psychosocially friendly work environment.
2 Materials and methods
2.1 research design.
In the present study, a cross-sectional survey was conducted among nurses employed in intensive care units in Poland who were providing work during the survey. The research instruments were a survey questionnaire consisting of questions on sociodemographic data and standardized research tools: BERNCA-R questionnaire ( 27 ), Job Satisfaction Scale (JSS) questionnaire ( 28 ) and Maslach Burnout Inventory (MBI) questionnaire ( 29 ). The study was conducted from December 2022 to January 2023. The innovation of the study is the evaluation of the relationship of socio-professional factors such as occupational burnout and job satisfaction with the level of care by anesthesia nurses. This is one of the first studies of this scope in the indicated group in Poland. The survey was conducted between December 2022 and January 2023. The innovation of the study was assessment of the impact of socio-professional factors such as occupational burnout and job satisfaction related to the level of care of anesthesia nurses. This is one of the first studies of this scope in the indicated group in Poland.
2.2 Research tools
2.2.1 bernca-r care rationing questionnaire.
The study used the Polish version of the BERNCA-R questionnaire adapted by Uchmanowicz et al. to assess rationing of care ( 27 ). The reliability of the translated version of the questionnaire was assessed using internal consistency and trustworthiness of the respondents. Cronbach’s alpha and inter-item correlations were used to analyze the internal consistency of the Polish BERNCA-R questionnaire. The mean total BERNCA-R score was 1.9 points (SD = 0.74) on the 0–4 scale. Cronbach’s alpha for the unidimensional scale was 0.96. The mean inter-item correlation was 0.4 (range 0.1–0.84), indicating high internal consistency. The univariate solution showed stable loadings above 0.5 for almost all items of the Polish BERNCA-R questionnaire. A study using the Polish BERNCA-R questionnaire showed that the tool is relevant and reliable for studying care rationing in groups of Polish nurses.
The questionnaire contains 32 questions about nursing activities rated on a 5-point Likert scale against which skipping care may have occurred. It is divided into five sections and respondents are asked to indicate how often in the past 7 days they were unable to perform them. The questionnaire score is the mean value of above-mentioned 32 questions. It therefore ranges from 0 to 4 and can be interpreted analogously to the interpretation of a single question. In addition, the questionnaire included questions on sociodemographic data: age, gender and job seniority of respondents.
2.2.2 Job satisfaction scale (JSS)
The Job Satisfaction Scale (JSS) was used to measure overall cognitive job satisfaction. Zalewska constructed this tool based on the Satisfaction with Life Scale by Diener et al. ( 28 ). She reformulated the statements to address the sphere of work as a holistic, complex phenomenon and to require a conscious evaluation of work based on personal criteria. The scale is one-dimensional, consisting of five statements, rated on a seven-point scale. The JSS score is the total score of five questions.
There are no standard scores for low or high job satisfaction for this tool. The job satisfaction survey is based on 5 job-related statements, each rated on a 7-point scale: 1 – “strongly disagree,” 2 - “disagree,” 3 - “rather disagree,” 4 - “difficult to say,” 5 - “rather agree,” 6 - “agree,” 7 - “strongly agree.” A respondent can obtain between 5 and 35 points. The higher the score, the higher the perceived job satisfaction. The Job Satisfaction Scale measures the cognitive aspect of overall job satisfaction. The internal reliability of the scale is high in the heterogeneous group, Cronbach’s alpha is 0.864. JSS is a reliable tool for assessing overall job satisfaction, showing high consistency with similar scales.
2.2.3 Maslach burnout inventory (MBI)
The Maslach Burnout Inventory (MBI) developed by Maslach et al. ( 29 ) is recognized as a standard tool for research in this field. The tool consists of three parts that examine emotional exhaustion, depersonalization and lack of personal achievement. The inventory consists of 22 items in the form of statements that are related to the attitudes and feelings the respondent feels about her professional work. The purpose of the questionnaire is to measure the intensity and frequency with which she experiences certain symptoms related to job burnout. The higher the final score, the more likely the respondent is to experience occupational burnout. The exception is in the area of personal fulfillment.
2.3 Participants
The study involved 477 anesthesia nurses employed in intensive care units. Inclusion criteria were work as an anesthesia nurse in an intensive care unit and consent to participate in the study. All questionnaires are physically stored by the authors of this paper. Paper questionnaire forms were distributed to 120 public hospitals in Poland with a request to forward them to intensive care units. The hospitals were selected from a list available on the Polish National Health Fund portal, while the authors had no influence or knowledge of which nurses would complete the questionnaires. The average number of nurses employed in these units depends on the number of beds and ranges from about 30 to 60. It was assumed that up to 20% of the anesthesia nurses employed in the selected hospitals would be surveyed. 600 paper survey questionnaires were initially distributed, 512 were returned and, after final verification, 477 correctly filled ones were subjected to statistical analysis (79.5%). The exclusion criteria were lack of consent to participate in the study, working in the pediatric intensive care unit, working one shift, working outside the intensive care unit.
2.4 Statistical analysis
In the statistical analysis, correlations were calculated using Spearman’s rho coefficient, reporting the intensity of the relationship and its positive or negative direction. The analysis was performed using the IBM SPSS 26.0 package (IBM, New York City, NY, United States) with the Exact Tests module. All correlations and differences are statistically significant when p < 0.05.
2.5 Ethical procedures
The participation of nurses in the study was voluntary and anonymous. The study was conducted in accordance with the ethical standards set forth in the Declaration of Helsinki (64th WmA General Assembly, Fortaleza, Brazil, October 2013) and in accordance with Polish legal regulations. The application was favorably approved by the Bioethics Committee of the State Academy of Applied Sciences in Przemysl (KBPANS 2/2023).
The survey was conducted among 477 selected anesthesia nurses employed in intensive care units in Poland. 4.0% of the respondents were under 25 years old, 60.2% between 25 and 35 years old, 19.9% between 36 and 45 years old, and 14.9% were between 46 and 55 years old. Only 1.0% of respondents were over 56 years old. Respondents’ length of service as anesthesia nurses from 1 to 10 years was declared by 63.5% of respondents, from 11 to 20 years by 20.1% of respondents, 21 to 30 years by 12.6% and over 31 years by 3.8% of respondents. Detailed results are presented in Table 1 .

Table 1 . Characteristics of the study group.
Nurses participating in the study worked 12-h shifts. According to the Polish Labor Code, there is a two-and three-month reference period (decided by the employer). As a rule of thumb, during the indicated period, the number of night and holiday duties for each nurse should be comparable.
3.1 Results of the BERNCA-R questionnaire
Statistical analysis showed that the most frequently rationed activities in the work of anesthesia nurses (the highest mean questionnaire score) during on-call were talking to the patient and/or his family (1.91 ± 1.18), lack of time to review individual patients’ situations and care plans at the start of the on-call period (1.86 ± 1.05), showing emotional or psychosocial support to the patient (1.84 ± 1.16), or giving patients sufficient information about upcoming tests or treatment (1.83 ± 1.15). The results may indicate that respondents pay more attention to the implementation of instrumental activities and overlook those related to psychological support.
The mean total score of the degree of nursing care rationing assessed by the BERNCA-R questionnaire was 1.65 ± 0.82 on a scale of 0 to 4 (where 0 means “there was no need for it” and 4 means “often”) and ranged between “never” or “rarely.” The median of the results obtained was also at the mean level and was 1.66 ( Table 2 ).

Table 2 . Average score of the BERNCA-R questionnaire ( n = 477).
3.2 Results of the job satisfaction scale (JSS) questionnaire
Analysis of the data on the level of job satisfaction of the nurses surveyed (JSS) showed that it was above the mean level and was 23.00 ± 5.21, meaning that the majority of nurses were satisfied with their job at a level above average ( Table 3 ).

Table 3 . Average score of the MBI questionnaire ( n = 477).
3.3 Results of the Maslach burnout inventory (MBI) questionnaire
The mean overall score of occupational burnout among the anesthesia nurses surveyed was 60.82 ± 10.46 (median 62.00). The maximum number of points was 88. According to Maslach’s statement, his indicates that the higher the score, the higher the occupational burnout in the surveyed group. The mean score of emotional exhaustion, which significantly affects the level of occupational burnout, was 26.39 ± 6.07 out of 36 points, depersonalization was 14.14 ± 3.21 out of 20 points and lack of personal achievement was 20.29 ± 4.70 out of 30 points. All the scores obtained exceeded the threshold of 50.0% of possible points, which indicates the presence of occupational burnout at a significant level. The results are shown in Table 3 .
3.4 Correlations
Statistical analysis shows that respondents “never” or “rarely” ration instrumental activities, and the most frequently omitted ones are those relating to the patient’s mental sphere. There are statistically significant correlations between the level of occupational burnout and rationing of nursing care, which are characterized by insignificant strengths of association. Respondents with higher professional burnout in each area are characterized by greater inability to perform certain activities ( Table 4 ).

Table 4 . Correlations between MBI, rationing of nursing care and job satisfaction levels.
Greater inability to perform certain activities is associated with lower job satisfaction, which may confirm the fact that respondents are aware of skipping certain activities in patient care, which may cause them to have lower levels of satisfaction with their professional tasks and thus the overall level of fulfillment in the nursing profession. The correlation is statistically significant ( p < 0.001) but the strength of the association was found to be insignificant (Spearman’s rho equal to−0.202) ( Table 5 ).

Table 5 . Correlations between job satisfaction and rationing of nursing care.
4 Discussion
The aim of this paper was to determine the relationship between occupational burnout, job satisfaction and rationing of care among anesthesia nurses employed in intensive care units. This is an innovative study of a group of nurses providing services to patients in life-threatening conditions requiring intensive treatment, supervision, and enhanced care. The results of our study showed that the mean total score of the degree of nursing rationing assessed by the BERNCA-R questionnaire was 1.65 ± 0.82 (below average), which may mean that the surveyed group is aware of the fact of responsibility for the health of patients. In studies by other authors conducted in a professional group of nurses, the mean BERNCA-R score was 1.55 ± 0.15, indicating that the frequency of care rationing ranged from “never” to “rarely” ( 30 ) and was similar to the results in the own research. Other studies have shown a higher frequency of nursing rationing among nurses working on surgical wards, with a mean score of 2.72 ± 0.86, and nurses working on conservative wards (2.08 ± 0.86) ( 22 ) and were similar to the own research.
In the Schubert et al. study, the mean BERNCA score was 57 (1.69 ± 0.571) and, according to the authors, meant that nurses had to ration at least one of the 32 tasks indicated in the questionnaire during the last 7 days of work, which is confirmed by our own study and those of other authors ( 22 , 30 , 31 ). A slightly lower level of rationing (1.38 ± 0.62) was shown by Uchmanowicz et al. study ( 32 ).
The mean overall burnout score among the anesthesia nurses surveyed was 60.82 ± 10.46, which indicates the presence of burnout in the study group. The mean score of emotional exhaustion, which significantly affects the level of professional burnout was 26.39 ± 6.07, depersonalization was at 14.14 ± 3.21 and lack of personal achievement was at 20.29 ± 4.70. This was presumably due to too much mental stress, responsibility for human lives and working under constant stress. A study by other authors conducted in a group of professional nurses showed that the mean score of occupational burnout was at 49.27 ± 19.76, exhaustion 63.56, depersonalization 37.2, lack of achievement 47.07 ( 30 ). In another study, the total MBI score was 38.14 ± 22.93. The individual components of occupational burnout yielded values of emotional exhaustion equal to 44.8, lack of personal achievement equal to 40.66, depersonalization equal to 28.95 ( 33 ) and differed from the results of the own research.
In the own research, the level of job satisfaction of the nurses surveyed was above average at 23.00 ± 5.2, which means that most nurses were satisfied with their jobs at a level above average. In the Uchmanowicz et al. study, the average score obtained by respondents was 11.71 ± 5.97, suggesting that respondents’ answers indicate a state between “dissatisfied” and “rather dissatisfied” with their work. Scores ranged from 7 to 18, with a median score of 11 ( 34 ), which has been confirmed by other studies ( 30 , 35 ).
In the own research, there are statistically significant correlations between occupational burnout and rationing of nursing care, which are characterized by insignificant strengths of association. Greater inability to perform certain activities is associated with lower job satisfaction. The correlation is statistically significant ( p < 0.001) but the strength of the association was found to be insignificant (Spearman’s rho = −0.202).
A study by other authors observed a statistically significant positive correlation between the BERNCA-R scale and MBI ( p < 0.05), and a negative correlation between the BERNCA-R scale and JSS ( p < 0.05). Independent predictors of the BERNCA-R scale were the emotional exhaustion of the MBI scale and the assessment of the impact of independence on job satisfaction (p < 0.05) ( 34 ). Similarly, Radosz-Kanwa et al. proved that BERNCA-R scale scores correlated statistically significantly and positively ( r > 0) with two (of three) subscales of the MBI questionnaire: emotional exhaustion and depersonalization ( p < 0.001) ( 31 ), which was confirmed by our own research. Rascu et al. ( 36 ) showed that bedside rationing of care refers to the use of clinical judgment by nurses to prioritize how they allocate their time and skills in providing health care to patients due to major time and staffing constraints or other organizational issues. The study by Tamayo et al. ( 37 ) found that nurses most often rationed care, support and supervision tasks. It was less common to omit other aspects of care. Identifying factors influencing rationing can help identify starting points for hospital policy reforms, as evidenced by our own research. Studies by many authors have found an overall increase in rationing of care activities, with documentation and social support being the most rationed ( 22 , 38 , 39 ).
Jaworski et al. ( 8 ) demonstrate that higher job satisfaction can reduce the risk of rationing nursing care, which is supported by other studies ( 40 ). White et al. found that some respondents often reported not being able to provide necessary care to patients ( 41 ). Other research suggests that workplace atmosphere and relationships partially mediate the link between organizational climate and occupational burnout ( 42 ). A nurse’s job satisfaction is related to the level of nursing care provided; higher levels of rationed care mean higher levels of occupational burnout and lower job satisfaction, resulting in general dissatisfaction among this professional group ( 43 ). There were other studies conducted that identified lack of time, inadequacy of staff, lack of team dynamics as possible factors that affect rationing of nursing care ( 44 ).
5 Conclusion
The results proved that there is a statistically significant, although with a weak strength of association, correlation between occupational burnout and rationing of care by anesthesia nurses employed in intensive care units. As the limitation of anesthesia nurses’ ability to perform certain activities increases, their job satisfaction decreases. Therefore, it is important to ensure that intensive care units are adequately staffed with nurses, as there are fewer job responsibilities that are unfulfilled in the work environment that is conducive to nurses.
6 Limitations of the study
The results of the survey have a solid basis; however, the study may have some limitations. The study involved a professional group of anesthesia nurses employed in intensive care units of different ages and job seniority. The sample size was non-representative of the situation in Poland, also due to bias in the selection of respondents, which may limit the generalizability of the results. The sample size was not large enough, which may limit the generalizability of the results. Further multi-center surveys are needed to generalize the results and implement recommendations for management.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Bioethics Committee of the State Academy of Applied Sciences in Przemyśl. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
KT: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Writing – original draft, Writing – review & editing. KK: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Writing – original draft, Writing – review & editing. BM: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Karaca, A, and Durna, Z. Patient satisfaction with the quality of nursing care. Nurs Open . (2019) 6:535–45. doi: 10.1002/nop2.237
PubMed Abstract | Crossref Full Text | Google Scholar
2. Khademi, E, Abdi, M, Saeidi, M, Piri, S, and Mohammadian, R. Emotional intelligence and quality of nursing care: a need for continuous professional development. Iran J Nurs Midwifery Res . (2021) 26:361–7. doi: 10.4103/ijnmr.IJNMR_268_19
3. Gröndahl, W, Muurinen, H, Katajisto, J, Suhonen, R, and Leino-Kilpi, H. Perceived quality of nursing care and patient education: a cross-sectional study of hospitalised surgical patients in Finland. BMJ Open . (2019) 9:e023108. doi: 10.1136/bmjopen-2018-023108
Crossref Full Text | Google Scholar
4. Kalisch, BJ, and Xie, B. Errors of mission: missed nursing care. West J Nurs Res . (2014) 36:875–90. doi: 10.1177/0193945914531859
5. Kalisch, BJ. Missed nursing care: a qualitative study. J Nurs Care Qual . (2006) 21:306. doi: 10.1097/00001786-200610000-00006
6. Klimek, YJ. Rationing evidence-based nursing practice: considering a resource-based approach. OJIN . (2020) 26:1. doi: 10.3912/OJIN.Vol26No01PPT62
7. Mandal, L, Seethalakshmi, A, and Rajendrababu, A. Rationing of nursing care, a deviation from holistic nursing: a systematic review. Nurs Philos . (2020) 21:e12257. doi: 10.1111/nup.12257
8. Jaworski, M, Iwanow, L, Grochans, E, Młynarska, A, Gurowiec, PJ, Uchmanowicz, I, et al. Optimistic thinking, satisfaction with life and job and nursing care rationing: multicentre study in Poland. J Nurs Manag . (2020) 28:1948–59. doi: 10.1111/jonm.12974
9. Hernández-Cruz, R, Moreno-Monsiváis, MG, Cheverría-Rivera, S, and Díaz-Oviedo, A. Factors influencing the missed nursing Care in Patients from a private hospital. Rev Lat Am Enferm . (2017) 25:25. doi: 10.1590/1518-8345.1227.2877
10. Uchmanowicz, I, and Gotlib, J. What is rationing of nursing care? Współczesne Piel i Ochr, Zdr . (2018) 7:2.
Google Scholar
11. Uchmanowicz, I, Witczak, I, Rypicz, Ł, Szczepanowski, R, Panczyk, M, Wiśnicka, A, et al. A new approach to the prevention of nursing care rationing: cross-sectional study on positive orientation. J Nurs Manag . (2021) 29:317–25. doi: 10.1111/jonm.13156
12. Schubert, M, Glass, TR, Clarke, SP, Schaffert-Witvliet, B, and De Geest, S. Validation of the Basel extent of rationing of nursing care instrument. Nurs Res . (2007) 56:416–24. doi: 10.1097/01.NNR.0000299853.52429.62
13. Schubert, M, Clarke, SP, Aiken, LH, and de Geest, S. Associations between rationing of nursing care and inpatient mortality in Swiss hospitals. Int J Qual Health Care . (2012) 24:230–8. doi: 10.1093/intqhc/mzs009
14. Witczak, I, Rypicz, Ł, Karniej, P, Młynarska, A, Kubielas, G, and Uchmanowicz, I. Rationing of nursing care and patient safety. Front Psychol . (2021) 12:676970. doi: 10.3389/fpsyg.2021.676970
15. Schubert, M, Clarke, SP, Glass, TR, Schaffert-Witvliet, B, and De Geest, S. Identifying thresholds for relationships between impacts of rationing of nursing care and nurse-and patient-reported outcomes in Swiss hospitals: a correlational study. Int J Nurs Stud . (2009) 46:884–93. doi: 10.1016/j.ijnurstu.2008.10.008
16. Baszkiewicz, I. Rationing of nursing care at the Department of Hematology and Pediatric Oncology. Współ Piel i Ochr Zdr . (2019) 8:83–8.
17. Gawęda, A, Śnieżek, A, and Serzysko, B. Job satisfaction in the opinion of surveyed nurses. Piel Zdr Publ . (2018) 8:269–76. doi: 10.17219/pzp/91608
18. Lu, H, Barriball, KL, Zhang, X, and While, AE. Job satisfaction among hospital nurses revisited: a systematic review. Int J Nurs Stud . (2012) 49:1017–38. doi: 10.1016/j.ijnurstu.2011.11.009
19. Halcomb, E, Smyth, E, and McInnes, S. Job satisfaction and career intentions of registered nurses in primary health care: an integrative review. BMC Fam Pract . (2018) 19:136. doi: 10.1186/s12875-018-0819-1
20. Rodrigues, M, Gaspar, F, and Lucas, P. Nurses’ job satisfaction in hospital setting: a scoping review. NTQR . (2022) 13:e650.
21. Kowalczuk, K, Krajewska-Kułak, E, and Sobolewski, M. The effect of subjective perception of work in relation to occupational and demographic factors on the mental health of polish nurses. Front Psych . (2020) 11:591957. doi: 10.3389/fpsyt.2020.591957
22. Tomaszewska, K, Majchrowicz, B, and Ratusznik, D. Rationing of nursing care on example of selected health care facility. Int J Environ Res Public Health . (2021) 18:12824. doi: 10.3390/ijerph182312824
23. Świątek, A, Milecka, D, and Uchmanowicz, I. Occupational burnout and life satisfaction among anaesthetists and intensive care nurses. Współ. Piel. i Ochr. Zdr. (2017) 6:121–8.
24. Nowakowska, I, Rasińska, R, Roszak, K, and Bańkowska, A. Nursing – profession particularly vulnerable to stress and burnout. Selected theoretical assumptions and preliminary research report—part I. Piel pol . (2017) 63:120–4. doi: 10.20883/pielpol.2017.16
25. Cisek, M, Przewoźniak, L, Kózka, M, Brzostek, T, Brzyski, P, Ogarek, M, et al. Workload during the last duty in the opinions of nurses working in hospitals covered by the RN4CAST project. Zdr Publ i Zarz . (2013) 11:210–24. doi: 10.4467/20842627OZ.14.018.1628
26. Atashzadeh-Shoorideh, F, Shirinabadi Farahani, A, Pishgooie, AH, Babaie, M, Hadi, N, Beheshti, M, et al. A comparative study of patient safety in the intensive care units. Nurs Open . (2022) 9:2381–9. doi: 10.1002/nop2.1252
27. Uchmanowicz, I, Kirwan, M, Riklikiene, O, Wolfshaut-Wolak, R, Gotlib, J, and Schubert, M. Validation of polish version of the Basel extent of rationing of nursing care revised questionnaire. PLoS One . (2019) 14:e0212918. doi: 10.1371/journal.pone.0212918
28. Zalewska, A. Skala Satysfakcji z Pracy – pomiar poznawczego aspektu ogólnego zadowolenia z pracy. Zadowolenie z pracy i jego komponenty. Job satisfaction scale – measuring the cognitive aspect of overall job satisfaction. Job satisfaction and its components. Acta Universitatis Lodziensis Folia Psychologica . (2003) 7:49–61.
29. Maslach, C, Jackson, S, and Leiter, M. Maslach burnout inventory manual . 3rd ed. Washington, DC, USA: Consulting Psychologists Press (1996).
30. Piotrowska, A, Lisowska, A, Twardak, I, Włostowska, K, Uchmanowicz, I, and Mess, E. Determinants affecting the rationing of nursing care and professional burnout among oncology nurses. Int J Environ Res Public Health . (2022) 19:7180. doi: 10.3390/ijerph19127180
31. Radosz-Knawa, Z, Kamińska, A, Malinowska-Lipień, I, Brzostek, T, and Gniadek, A. Factors influencing the rationing of nursing Care in Selected Polish Hospitals. Healthcare (Basel) . (2022) 10:2190. doi: 10.3390/healthcare10112190
32. Schubert, M, Ausserhofer, D, Desmedt, M, Schwendimann, R, Lesaffre, E, Li, B, et al. Levels and correlates of implicit rationing of nursing care in Swiss acute care hospitals—a cross sectional study. Int J Nurs Stud . (2013) 50:230–9. doi: 10.1016/j.ijnurstu.2012.09.016
33. Uchmanowicz, I, Kubielas, G, Serzysko, B, Kołcz, A, Gurowiec, P, and Kolarczyk, E. Rationing of nursing care and professional burnout among nurses working in cardiovascular settings. Front Psychol . (2021) 12:726318. doi: 10.3389/fpsyg.2021.726318
34. Uchmanowicz, I, Karniej, P, Lisiak, M, Chudiak, A, Lomper, K, Wiśnicka, A, et al. The relationship between burnout, job satisfaction and the rationing of nursing care-a cross-sectional study. J Nurs Manag . (2020) 28:2185–95. doi: 10.1111/jonm.13135
35. Jędrzejczyk, M, Guzak, B, Czapla, M, Ross, C, Vellone, E, Juzwiszyn, J, et al. Rationing of nursing care in internal medicine departments-a cross-sectional study. BMC Nurs . (2023) 22:455. doi: 10.1186/s12912-023-01617-x
36. Rașcu, A, Postolache, P, Mazilu, D, and Oțelea, M. Factors influencing the rationing of nursing care in Romania. Rom J Occup Med . (2019) 70:28–32. doi: 10.2478/rjom-2019-0004
37. Tamayo, RLJ, Quintin-Gutierrez, MKF, Campo, MB, Lim, MJF, and Labuni, PT. Rationing of nursing care and its relationship to nurse practice environment in a tertiary public hospital. Acta Med Philipp . (2020) 56:64–71.
38. Dhaini, SR, Ausserhofer, D, El Bajjani, M, Dumit, N, Abu-Saad Huijer, H, and Simon, M. A longitudinal study on implicit rationing of nursing care among Lebanese patients - study protocol. J Adv Nurs . (2019) 75:1592–9. doi: 10.1111/jan.14012
39. Młynarska, A, Krawuczka, A, Kolarczyk, E, and Uchmanowicz, I. Rationing of nursing Care in Intensive Care Units. Int J Environ Res Public Health . (2020) 17:6944. doi: 10.3390/ijerph17196944
40. Maghsoud, F, Rezaei, M, Asgarian, FS, and Rassouli, M. Workload and quality of nursing care: the mediating role of implicit rationing of nursing care, job satisfaction and emotional exhaustion by using structural equations modeling approach. BMC Nurs . (2022) 21:273. doi: 10.1186/s12912-022-01055-1
41. White, EM, Aiken, LH, and McHugh, MD. Registered nurse burnout, job dissatisfaction, and missed Care in Nursing Homes. J Am Geriatr Soc . (2019) 67:2065–71. doi: 10.1111/jgs.16051
42. Giorgi, G, Mancuso, S, Fiz Perez, F, Castiello D’Antonio, A, Mucci, N, Cupelli, V, et al. Bullying among nurses and its relationship with burnout and organizational climate. Int J Nurs Pract . (2016) 22:160–8. doi: 10.1111/ijn.12376
43. Griffiths, P, Recio-Saucedo, A, Dallora, C, Briggs, J, Maruotti, A, Meredith, P, et al. The association between nurse staffing and omissions in nursing care: a systematic review. J Adv Nurs . (2018) 74:1474–87. doi: 10.1111/jan.13564
44. Zhu, X, Zheng, J, Liu, K, and You, L. Rationing of nursing care and its relationship with nurse staffing and patient outcomes: the mediation effect tested by structural equation modeling. Int J Environ Res Public Health . (2019) 16:1672. doi: 10.3390/ijerph16101672
Keywords: anesthesia nurses, care rationing, job satisfaction, occupational burnout, stress
Citation: Tomaszewska K, Kowalczuk K and Majchrowicz B (2024) Relationships between job satisfaction, occupational burnout and rationing of care among intensive care unit nurses. Front. Public Health . 12:1400169. doi: 10.3389/fpubh.2024.1400169
Received: 13 March 2024; Accepted: 22 April 2024; Published: 14 May 2024.
Reviewed by:
Copyright © 2024 Tomaszewska, Kowalczuk and Majchrowicz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY) . The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Katarzyna Tomaszewska, [email protected]
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research Technician I
Research tech.
- 1 Boston Medical Center Place, Boston, Massachusetts
Position: Research Technician I, Pathology
Location: Boston, MA
Schedule: 40 hours per week, on-site
POSITION SUMMARY:
Research Technician I will be required to analyze specimens; will be required to analyze data using statistical analysis software and create presentable graphs, figures, tables, etc. of the data. Research Technician I will interact with students, laboratory technicians, Principal Investigators, and research teams to plan, carry out, and maintain ongoing studies including coordinating and implementing subject recruitment, enrollment, sample collection, sample processing, follow-up, data collection, and study conduct. Additionally, Research Technician I will help to maintain equipment and reagent/materials and supplies used for research.
JOB RESPONSIBILITIES:
Communicate with research partners on and off campus to ensure proper data sharing, troubleshoot problems, and maintain organized data files.
Assists in the orientation and teaching of new trainees and technicians.
Prepares, submits, and presents written reports of scientific findings in scientific journals and at national meetings.
Uses SAS/R/GraphPad to analyze data and prepare figures and tables for publication.
The above statements in this job description are intended to depict the general nature and level of work assigned to the employee(s) in this job. The above is not intended to represent an exhaustive list of accountable duties and responsibilities required
JOB REQUIREMENTS
Bachelor's degree in Biology or related field required. Master's degree preferred.
EXPERIENCE:
Must have a minimum of two years of research experience.
Experience with laboratory protocols and human biology highly desirable but not required.
KNOWLEDGE AND SKILLS:
Requires the knowledge computer-based software and analytical ability to accurately analyze results.
Good computer skills, including data entry, use of spreadsheet (Microsoft Excel) and database, statistical analysis software (SAS, R)
Excellent interpersonal and English verbal and written language skills sufficient to exchange information with research staff, interact with other laboratory technicians and prepare written reports for publication.
Requires safe handling of potentially infectious materials or noxious chemicals, using appropriate hospital, laboratory, and bio-safety precautions.
Requires the manual/visual dexterity necessary to prepare specimens, prepare solutions, screen specimens, and operate a computer software system.
Experience with scientific writing is highly desirable.
JOB BENEFITS:
- Competitive pay
- Tuition reimbursement and tuition remission programs
- Highly subsidized medical, dental, and vision insurance options
- Career Advancement/Professional Development: Access a wealth of ongoing training and development opportunities that will not only enhance your skills but also expand your knowledge base especially for individuals pursuing careers in medicine or biomedical research.
- Pioneering Research: Engage in groundbreaking research projects that are driving the forefront of biomedical science.
ABOUT THE DEPARTMENT:
As the primary teaching hospital for Boston University Chobanian & Avedisian School of Medicine and BU schools of public health and dentistry, intellectual rigor shapes our inquiries. Our research is led by a belief that skin color, zip code, and financial circumstances shouldn’t dictate health.
Boston Medical Center is an Equal Opportunity/Affirmative Action Employer. If you need accommodation for any part of the application process because of a medical condition or disability, please send an e-mail to [email protected] or call 617-638-8582 to let us know the nature of your request.
Equal Opportunity Employer/Disabled/Veterans
Privacy policy
By clicking Submit, you acknowledge that you are willing to receive messages from Boston Medical Center relating to the status of your application or other recruitment related information to any mobile / cell phone number entered in the form above. You can easily opt-out of receiving messages by replying STOP to any messages you receive.
Not the right fit? Check out these other jobs
Research assistant, hematology/oncology, rn care manager, emergency department, 30 hours (day/evening), registered nurse, renal/family, medical surgical, 36 hours (day/night/every other weekend), senior audiologist, certified nursing assistant, medical surgical, per diem, refer a friend.
Your information:
Apply for this job now
EEO & Accommodation Statement Boston Medical Center is an equal employment/affirmative action employer. We ensure equal employment opportunities for all, without regard to race, color, religion, sex, national origin, age, disability, veteran status, sexual orientation, gender identity and/or expression or any other non-job-related characteristic. If you need accommodation for any part of the application process because of a medical condition or disability, please send an e-mail to [email protected] or call 617-638-8582 to let us know the nature of your request
E-Verify Program Boston Medical Center participates in the Electronic Employment Verification Program. As an E-Verify employer, prospective employees of BMC must complete a background check and receive medical clearance before beginning their employment at the hospital.
Federal Trade Commission Statement: According to the FTC, there has been a rise in employment offer scams. Our current job openings are listed on our website and applications are received only through our website. We do not ask or require downloads of any applications, or “apps” job offers are not extended over text messages or social media platforms. We do not ask individuals to purchase equipment for or prior to employment. To avoid becoming a victim of an employment offer scam, please follow these tips from the FTC: FTC Tips
Join the BMC Talent Community
Before you go, don't forget to join our talent community!
We use cookies to make your interactions with our website more meaningful. They help us better understand how our websites are used, so we can tailor content for you. For more information about the different cookies we are using, read the Privacy Statement . By continuing to navigate the site, you agree to the use of cookies on our behalf.

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- PMC10160712
Nurses’ and nursing students’ reasons for entering the profession: content analysis of open-ended questions
Lisa mckenna.
1 La Trobe University, Melbourne, Australia
Ian Ruddy Mambu
2 Universitas Pelita Harapan, Tangerang, Indonesia
Christine L. Sommers
Sonia reisenhofer.
3 Bairnsdale Regional Health Service, Bairnsdale, Australia
Julie McCaughan
4 Siloam Hospitals, Tangerang, Indonesia
Associated Data
The datasets generated and/or analysed during the current study are not publicly available due to ethical approval conditions but are available from the corresponding author on reasonable request.
Global nursing shortages require effective recruitment strategies and understanding of individuals’ motivations to enter the profession. These can be complex and bound by numerous factors such as gender and culture. While much research around this has been conducted, little has been undertaken in non-Western cultures where motivations could be different.
To explore Indonesian nurses’ and nursing students’ motivations for entering the nursing profession.
Online survey with closed and open-ended questions drawn from two different studies. This paper reports findings from one similar open-ended question.
As part of two larger surveys, nurses from 13 hospitals across one private health care group and nursing students with clinical experienced enrolled in a baccalaureate nursing program in Indonesia were asked the question, Why do you want to be a nurse? Responses were translated into English and back-translated into Indonesian prior to being subjected to summative content analysis.
In total, 1351 nurses and 400 students provided responses to the question, representing 98.72% and 99.70% respectively of those completing the survey. Both groups were primarily influenced by desire to serve others and God, personal calling and influence of family members and others. Nurses identified a desire to work in the health field and with the sick, in a noble and caring profession.
Conclusions
Nurses and nursing students were motivated by traditional perspectives on nursing. These should be considered in future recruitment activities. However, more research is needed to understand how these factors influence career choice.
Nurses have been identified as crucial to global achievement of Sustainable Development Goals (SDGs) and play a strong role in health policy, achievement of health targets [ 1 ]. However, global workforce shortages, along with an ageing nursing population [ 1 ] and COVID-19 related burnout further impacting retention [ 2 ], mean that strategies for recruitment into the nursing profession are paramount to meet community health care needs. While more than sufficient numbers of graduate nurses are being produced in Indonesia, 54.1% of nurses are located in urban areas, mostly in Java Island, while the other 45.9% are in rural areas with reported chronic shortages in some areas of the country, especially among communities in Eastern Indonesia [ 3 ]. The need for public education to improve the professional image of nursing has been advocated as one means for promoting recruitment of new nurses into the profession [ 4 ].
Understanding why individuals seek a career in nursing is important in facilitating the targeting of recruitment strategies. Some studies have reported on individual motivations to enter nursing courses, largely from western countries. In Italy, Messineo et al. [ 5 ] found that first year nursing students entered their courses with high levels of empathy and altruistic and prosocial motivations. However, there is also evidence that this declines over the duration of nursing studies [ 6 ]. Crick et al. [ 7 ] found that new nursing students in the United Kingdom were motivated to enter the course due to a desire to care for others. In a study of graduate entry nursing students in Australia, McKenna et al. [ 8 ] identified that previous exposure to nurses, either personally or family, played an important role in their decisions to enter the course, along with desire to care for others.
In a systematic review of 29 papers, Wu et al. [ 9 ] examined motivations of healthcare students influencing career choice, identifying a range of both intrinsic and extrinsic factors. They found that altruism through a desire to help others was strong among nursing students, particularly for those who were sick and in need of care. Job security and social status of nursing were considered important, while financial remuneration was not considered as important as for other health professions. Influence of family was mixed in nursing, with some families seeing nursing as having low pay and status, while having family members in the profession was positively influential.
The introduction of the Indonesian Nursing Act in 2014 saw rapid development in the nurse education system and nursing practice with introduction of curriculum standards and accreditation, national competency examination, and nurse registration across the country [ 10 ]. Four-year bachelor or three-year diploma courses can be undertaken to become professional or vocational nurses respectively. Furthermore, there has been recent growth in postgraduate and doctoral programs across the country [ 11 ]. Few previous studies could be sourced exploring why individuals are motivated (seek) to enter the nursing profession in Indonesia. In one study, 20 nursing diploma students participated in focus groups exploring their reasons for choosing to study nursing. Findings identified wanting to help family and others, being inspired by nurses, wanting to improve the image of nursing, influence of family and parents, and work opportunities all influenced choices [ 12 ]. In another study of 57 students in a bachelor degree nursing program, the majority entered the program because they were interested in the nursing profession or wanted to become nurses [ 13 ]. Around a third of students were motivated by their parents to enter the program. Previous studies regarding motivation among existing qualified nurses could not be sourced. Hence, this study sought to explore why Indonesian nurses and nursing students pursued nursing careers.
Data were drawn from two concurrent studies involving online questionnaires, the first focusing on Indonesian registered nurses’ training needs [ 14 ] and the second, on Indonesian nursing students’ experiences of their clinical learning environment [ 15 ]. In each study, participants were asked the same open-ended question: Why do you want to be a nurse? The responses to that question comprise the focus of this paper. Prior to commencement of data collection, approvals were obtained from ethics committees at La Trobe University (ID: S17-155) and Universitas Pelita Harapan (No.005/MRIN-EC/ECL/III/2018). In the original studies, inclusion criteria for the nurses were currently working at the private hospital with a 3-year nursing diploma level qualification or above. Inclusion criteria for nursing students were those who had completed a clinical placement in the private hospital, were enrolled as a nursing student in the university, and were 18 years of age or older. There were no specific exclusion criteria.
Links to the online Qualtrics surveys were provided in participant information materials. These were circulated via internal email and WhatsApp groups to a convenience sample of 2093 eligible registered nurses from 13 sites of an Indonesian private health care group across Jakarta, Sumatra, Sulawesi and Bali and Nusa Tenggara Timur and 796 students from one nursing degree program. Participants provided informed consent using a survey link in the study information provided and participation was voluntary and anonymous. In total, 406 s- and third-year students and 1355 nurses completed the open-ended question forming the basis of this paper.
Responses to the question from both datasets were translated from Indonesian into English and back-translated by two researchers to ensure original meanings were retained [ 16 ]. Data were then subjected to summative content analysis [ 17 ]. Key words were initially identified and coded within Microsoft Excel by two members of the research team. Codes were then manually collated into categories of like terms, quantified utilising frequency counts. Overarching themes were then identified from categories.
In total, 400 students and 1351 nurses provided responses to the question, representing response rates of 98.52% and 99.70% respectively. Among the student group, the average age was 20 years and 84% were female. In the registered nurse group, 80.8% were female and years of experience were relatively evenly distributed from less than one to more than 10 years. Of these, 39% had been in the profession for longer than five years, that is, before introduction of the Indonesian Nursing Act. From the analysis, seven categories and five themes emerged from the student data (Table 1 ) and eight categories and four themes from the nurse data (Table 2 ). Substantial overlap was evident across the two groups and rankings.
Student data (n = 400)
Nurse data (n = 1351)
Overwhelmingly, having an impact on others’ lives was key to both groups through helping or serving others or own family ranked highest for both groups, reported by 50.00% of students and 44.93% of nurses. Students also wanted to be a blessing to others , while nurses valued the interaction with people that is a fundamental part of nursing practice.
For both groups, factors around decision to enter nursing ranked second. Many described having a calling to nursing, while others described this in terms of a ‘childhood dream’, or for ‘personal reward or satisfaction’. Influence of family, others or circumstances played an important part for students and nurses, while a number of nurses described having no reason or choice around entering nursing. Service to God/religious response was also noted to have been the motivation for some students (9.50%); however, it is important to note that these students were enrolled in a faith-based university, so this could be expected. Attraction to the Profession of nursing was also identified as an important factor for both groups. Students expressed a desire to be a part of, or improve, the profession, while many nurses identified a desire to work in the health field or with the sick. For nurses, the status of the profession as noble and caring was a strong factor.
Finally, financial reasons were identified by a small number of participants in both groups who identified commencing their nursing education as they received an offer of a scholarship.
With a predicted continued global nursing shortage, targeted successful strategies need to be introduced to recruit into the profession. Understanding motivations for entering nursing courses can assist with the development of appropriate recruitment strategies and may also inform future retention strategies to keep nurses within the profession. Hence, this study sought to understand why nurses and nursing students in Indonesia chose to enter the profession. Prior to this study, little was known about such motivations in Indonesia, and outside of western countries.
A desire to impact others’ lives was the strongest reported influence for both nurses and nursing students in this study. This was seen as wanting to serve others, and desire to work with the sick. Altruism has long been identified as a reason why individuals choose nursing careers. However, Carter [ 18 ] cautions against simplifying such motivations just to this aspect, where “gender, culture and class and individual dispositions” (p.703) play an important role in the complex make-up of a nursing professional. These views may also change as students progress in their courses. A longitudinal study of nursing students in The Netherlands found that even though many students entered their courses with altruistic and empathic predispositions, their perceptions towards nursing changed to being more professional and focused on their role, knowledge and skills [ 6 ]. Conversely, this was not reflected in the current study where nurses still displayed strong altruistic characteristics beyond graduation from their nursing courses. This suggests that the caring aspect of nursing and ability to make a difference to people’s lives should be emphasised in recruitment to the profession. Additional research in the Indonesian context is needed to better understand the influences on nurses’ personal dispositions and whether these change over time.
Nurses and nursing students in this study both described a personal calling into nursing. Calling, itself, has been described as complex in nursing, and having changed from a traditional perspective based in religion and femininity, to a more contemporary conceptualisation focused on care provision, the profession and self-fulfilment [ 19 ]. In this study, a more traditional focus emerged with both focus on serving community and service to God. This may be, in part, related to the fact that the study was undertaken in a faith-based university and health care group. Being a strong faith-based country, this may be a particularly important consideration in Indonesia and would benefit from further research with other groups across the country. The importance of inclusion of this concept in recruitment into nursing in the country could be further explored. In a recent study in Indonesia, the concept of calling and reason for entering nursing played a role in student success in a nursing program [ 20 ]. The importance of understanding values is particularly pertinent in nursing recruitment strategies with a recent mandate in the United Kingdom for values-based recruitment of healthcare students aligning with those of the National Health Service [ 21 ].
The influence of families and others was a factor in this study for pursuing a nursing career. In Indonesia, families have been shown to play an important role in career pathways, particularly in family businesses [ 22 ]. However, the literature is mixed on whether this is an important factor for nursing. In their review, Wu et al. [ 9 ] identified that some studies identified parents as not being supportive of their children entering the nursing profession because of low pay and status, a view reflected elsewhere [ 23 ]. Despite this, families have been found to be a strong influencing factor influencing choice of nursing career in some studies [ 8 , 24 , 25 ]. Having family members or friends who are nurses or had experienced time in hospitals were identified as influencing factors in one study [ 8 ]. In a study conducted in the United States, Woods-Giscombe et al. [ 25 ] recommended including family members into recruitment processes into nursing, particularly for recruitment of students from underrepresented groups. This suggests that recruitment strategies should not only be directed towards potential students, but their families as well.
While career stability and vocational reasons have been identified by other researchers as guiding factors in pursuing nursing careers [ 8 , 18 ], these aspects were not identified by nurses and nursing students in this study. It is possible that cultural aspects may play a role. In a Norwegian study, nursing students from immigrant backgrounds were found to be more motivated by salary, status, and work flexibility than non-immigrants [ 26 ]. Findings from the current study suggest that such considerations might not be primary considerations for Indonesian nurses and students and that more research is needed to explore this aspect further.
Media representations have been identified in a number of studies as influencing decisions to pursue nursing careers. In one Australian study, hospital dramas on television as well as print and television news played a role in influencing graduate entry students to pursue nursing education [ 8 ]. In another Australian study focused on television representation of the nursing profession, nursing students perceived nurses to be negatively represented in comparison to doctors who were positively portrayed. They recognised that medical programs could provide some recruitment value [ 27 ]. However, a role of media influencing career choice was not identified in this study. Whether or not this plays some role in assisting career decisions for Indonesian students could also be examined further.
There are some acknowledged limitations to this study. The sample was drawn from one faith-based university and hospital group. While the study population was large and drawn from a number of locations, findings may be different in other Indonesian nurse populations across the diverse cultural groups in the country. Furthermore, data were only collected using one open-ended survey question. Further research that explores these concepts in greater depth would be highly valuable.
With global nursing shortages, there is an ongoing need for effective recruitment strategies into the profession. This makes it vital to understand motivations of those entering the profession to facilitate recruitment approaches. However, motivations may vary according to a wide range of intrinsic and extrinsic factors. This study identified that Indonesian nurses and nursing students were largely motivated by a need to serve others and God, personal calling, and the influence of family. As a strong faith-based country, this is likely to be an important consideration in future nursing recruitment. However, further research is needed across more communities to ensure that other motivating factors can be identified and incorporated into successful recruitment strategies. Further research is also needed to understand if these concepts play a role in nursing students successfully completing a program and entering the nursing profession.
Acknowledgements
The authors are grateful to all the nurses and nursing students for their contributions to the study.
Author Contribution
All authors have agreed on the final version and meet at least one of the following criteria (recommended by the ICMJE): (1) substantial contributions to conception and design (LM, CS, SR, IM, JC), acquisition of data, or analysis (LM, CS, IM) and interpretation (LM, CS, IM) of data; (2) drafting the article or revising it critically for important intellectual content (LM, CS).
This study was supported by a La Trobe Asia Research Grant Program grant and the Universitas Pelita Harapan Research and Community Service Grant Program.
Data Availability
Declarations.
The study was approved by Human Research Ethics Committees at La Trobe University (ID: S17-155) and Universitas Pelita Harapan (No.005/MRIN-EC/ECL/III/2018). All data collection was in accordance with relevant guidelines and regulations. Participants provided informed consent for this study using the survey link in study information provided.
Not applicable.
The authors have no competing interests to declare.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
IMAGES
VIDEO
COMMENTS
Correlation analysis has three general outcomes: (1) the two variables rise and fall together; (2) as values in one variable rise, the other falls; and (3) the two variables do not appear to be systematically related. To make those determinations, we use the correlation coefficient (r) and related p value or CI.
Nursing Research, Step by Step is coordinated by Bernadette Capili, PhD, NP-C: [email protected]. The authors have disclosed no potential conflicts of interest, financial or otherwise. ... and running a factor analysis (a statistical procedure that compares items or subscales within an instrument with each other and with the overall instrument ...
mentals of statistical analysis is required to incorporate the findings of empirical research into nursing practice. The primary focus of this article is to describe common statistical terms, present some common sta-tistical tests, and explain the interpretation of results from inferential statistics in nursing research. An overview of major ...
This table illustrates examples of statistical analysis using the information in Snapshot of aggregate data. Based on this analysis, the intervention appears to be successful in reducing the percentage of patients with uncontrolled diabetes (HbA1c > 7), average patient glycated hemoglobin (HbA1c) levels, and body mass index (BMI).
However, the basic research process, and the role that statistical analysis plays in that, has not changed. All research studies should be based on questions or hypotheses. Any statistical methods used for a study should be based on those hypotheses, taking into account specific characteristics of the variables and the design of the study.
Welcome to this focused issue on statistics in nursing research! Nursing Research put out a special call for papers on this topic in 2011. ... Finally, once data collection is complete, statistical analysis can be performed. The lifeline of scientific investigation is sequential and cumulative. For example, if the research question is poorly ...
Healthcare professionals and policy makers are increasingly aware of the need for their decisions to be informed by the best available research evidence. Although the articles selected for abstraction in Evidence-Based Nursing have already been appraised, and only the highest quality research selected, practitioners still need basic skills to identify and interpret methodologically sound ...
Statistical tests can be powerful tools for researchers. They provide valuable evidence from which we make decisions about the significance or robustness of research findings. Statistical tests are a critical part of the answers to our research questions and ultimately determine how confident we can be in the evidence to inform clinical practice. In addition to analysing data to answer ...
Regression analysis is a powerful and useful statistical procedure with many implications for nursing research. It enables researchers to describe, predict and estimate the relationships and draw plausible conclusions about the interrelated variables in relation to any studied phenomena. Regression also allows for controlling one or more ...
If we test a nursing intervention for patient pain with a 0.05 significance level using a two-tailed test, the results will indicate both de-creases (0.025 area) and increases (0.025 area) in pain. Using the same pain intervention example, a one-tailed test will indicate either increases (0.05 area) or decreases in pain, but not both.
Statistics for Nursing Research, 4th Edition helps you understand and interpret statistical methods, sampling and measurement techniques, and statistical analysis techniques. This unique and practical workbook is divided into two parts to differentiate between basic and advanced statistical methods, with dozens of hands-on exercises that will ...
A working understanding of the major fundamentals of statistical analysis is required to incorporate the findings of empirical research into nursing practice. The primary focus of this article is to describe common statistical terms, present some common statistical tests, and explain the interpretation of results from inferential statistics in nursing research. An overview of major concepts in ...
Examples of some of the most common statistical techniques used in nursing research, such as the Student independent t test, analysis of variance, and regression, are also discussed.
Nursing researchers may find it peculiar that a statistician is advocating for restraint when using statistical analysis. But it should always be that way. It is the nurse researcher's hypothesis that is of primary importance. The role of statistical analysis is to evaluate that hypothesis: does the evidence from the sampled data support the ...
Statistical analysis is the science of organizing, exploring, summarizing and presenting large amounts of data. to discover underlying patterns and trends (Daniel & Cross, 2013). Data is best ...
Written by nursing research and statistics experts Drs. Susan K. Grove and Daisha Cipher, this is the only statistics workbook for nurses to include research examples from both nursing and the broader health sciences literature. ... 36 sampling, measurement, and statistical analysis exercises provide a practical review of both basic and ...
In empirical research, all statistical tests begin with the null hypothesis and end with a test statistic and the associated statistical significance. A test of statistical significance determines the likelihood of a result assuming a null hypothesis to be true. Depending on the selected statistical analysis, researchers will use Z scores, t ...
The statistical analysis gives meaning to the meaningless numbers, thereby breathing life into a lifeless data. The results and inferences are precise only if proper statistical tests are used (Ali & Bhaskar, 2016). There are three purposes for statistical analysis: 1. To describe and summarize information, 2.
Service users participating in existing cancer research in the UK, Malta, Poland and Portugal, as well as care homes research in Austria completed the draft PCPI-C. Data were collected over a 14month period (January 2021-March 2022). Descriptive and measures of dispersion statistics were generated for all items to help inform subsequent analysis.
This paper introduces a dataset developed to measure the impact of archival and data curation decisions on data reuse. The dataset describes 10,605 social science research datasets, their curation ...
A purposive sample of 266 nursing intern students was enrolled from the Faculty of Nursing at Mansoura University. The data were collected using a patient safety survey. Subsequently, the collected data underwent analysis through the application of descriptive and inferential statistical techniques using SPSS-20 software.
Statistical analysis shows that respondents "never" or "rarely" ration instrumental activities, and the most frequently omitted ones are those relating to the patient's mental sphere. There are statistically significant correlations between the level of occupational burnout and rationing of nursing care, which are characterized by ...
Position: Research Technician I, PathologyLocation: Boston, MASchedule: 40 hours per week, on-sitePOSITION SUMMARY:Research Technician I will be required to analyze specimens; will be required to analyze data using statistical analysis software and create presentable graphs, figures, tables, etc. of the data. Research Technician I will interact with students, laboratory technicians, Principal ...
Nurses and nursing students in this study both described a personal calling into nursing. Calling, itself, has been described as complex in nursing, and having changed from a traditional perspective based in religion and femininity, to a more contemporary conceptualisation focused on care provision, the profession and self-fulfilment . In this ...