How to write a research plan: Step-by-step guide
Last updated
30 January 2024
Reviewed by
Today’s businesses and institutions rely on data and analytics to inform their product and service decisions. These metrics influence how organizations stay competitive and inspire innovation. However, gathering data and insights requires carefully constructed research, and every research project needs a roadmap. This is where a research plan comes into play.
There’s general research planning; then there’s an official, well-executed research plan. Whatever data-driven research project you’re gearing up for, the research plan will be your framework for execution. The plan should also be detailed and thorough, with a diligent set of criteria to formulate your research efforts. Not including these key elements in your plan can be just as harmful as having no plan at all.
Read this step-by-step guide for writing a detailed research plan that can apply to any project, whether it’s scientific, educational, or business-related.
- What is a research plan?
A research plan is a documented overview of a project in its entirety, from end to end. It details the research efforts, participants, and methods needed, along with any anticipated results. It also outlines the project’s goals and mission, creating layers of steps to achieve those goals within a specified timeline.
Without a research plan, you and your team are flying blind, potentially wasting time and resources to pursue research without structured guidance.
The principal investigator, or PI, is responsible for facilitating the research oversight. They will create the research plan and inform team members and stakeholders of every detail relating to the project. The PI will also use the research plan to inform decision-making throughout the project.
- Why do you need a research plan?
Create a research plan before starting any official research to maximize every effort in pursuing and collecting the research data. Crucially, the plan will model the activities needed at each phase of the research project.
Like any roadmap, a research plan serves as a valuable tool providing direction for those involved in the project—both internally and externally. It will keep you and your immediate team organized and task-focused while also providing necessary definitions and timelines so you can execute your project initiatives with full understanding and transparency.
External stakeholders appreciate a working research plan because it’s a great communication tool, documenting progress and changing dynamics as they arise. Any participants of your planned research sessions will be informed about the purpose of your study, while the exercises will be based on the key messaging outlined in the official plan.
Here are some of the benefits of creating a research plan document for every project:
Project organization and structure
Well-informed participants
All stakeholders and teams align in support of the project
Clearly defined project definitions and purposes
Distractions are eliminated, prioritizing task focus
Timely management of individual task schedules and roles
Costly reworks are avoided
- What should a research plan include?
The different aspects of your research plan will depend on the nature of the project. However, most official research plan documents will include the core elements below. Each aims to define the problem statement, devising an official plan for seeking a solution.
Specific project goals and individual objectives
Ideal strategies or methods for reaching those goals
Required resources
Descriptions of the target audience, sample sizes, demographics, and scopes
Key performance indicators (KPIs)
Project background
Research and testing support
Preliminary studies and progress reporting mechanisms
Cost estimates and change order processes
Depending on the research project’s size and scope, your research plan could be brief—perhaps only a few pages of documented plans. Alternatively, it could be a fully comprehensive report. Either way, it’s an essential first step in dictating your project’s facilitation in the most efficient and effective way.
- How to write a research plan for your project
When you start writing your research plan, aim to be detailed about each step, requirement, and idea. The more time you spend curating your research plan, the more precise your research execution efforts will be.
Account for every potential scenario, and be sure to address each and every aspect of the research.
Consider following this flow to develop a great research plan for your project:

Define your project’s purpose
Start by defining your project’s purpose. Identify what your project aims to accomplish and what you are researching. Remember to use clear language.
Thinking about the project’s purpose will help you set realistic goals and inform how you divide tasks and assign responsibilities. These individual tasks will be your stepping stones to reach your overarching goal.
Additionally, you’ll want to identify the specific problem, the usability metrics needed, and the intended solutions.
Know the following three things about your project’s purpose before you outline anything else:
What you’re doing
Why you’re doing it
What you expect from it
Identify individual objectives
With your overarching project objectives in place, you can identify any individual goals or steps needed to reach those objectives. Break them down into phases or steps. You can work backward from the project goal and identify every process required to facilitate it.
Be mindful to identify each unique task so that you can assign responsibilities to various team members. At this point in your research plan development, you’ll also want to assign priority to those smaller, more manageable steps and phases that require more immediate or dedicated attention.
Select research methods
Research methods might include any of the following:
User interviews: this is a qualitative research method where researchers engage with participants in one-on-one or group conversations. The aim is to gather insights into their experiences, preferences, and opinions to uncover patterns, trends, and data.
Field studies: this approach allows for a contextual understanding of behaviors, interactions, and processes in real-world settings. It involves the researcher immersing themselves in the field, conducting observations, interviews, or experiments to gather in-depth insights.
Card sorting: participants categorize information by sorting content cards into groups based on their perceived similarities. You might use this process to gain insights into participants’ mental models and preferences when navigating or organizing information on websites, apps, or other systems.
Focus groups: use organized discussions among select groups of participants to provide relevant views and experiences about a particular topic.
Diary studies: ask participants to record their experiences, thoughts, and activities in a diary over a specified period. This method provides a deeper understanding of user experiences, uncovers patterns, and identifies areas for improvement.
Five-second testing: participants are shown a design, such as a web page or interface, for just five seconds. They then answer questions about their initial impressions and recall, allowing you to evaluate the design’s effectiveness.
Surveys: get feedback from participant groups with structured surveys. You can use online forms, telephone interviews, or paper questionnaires to reveal trends, patterns, and correlations.
Tree testing: tree testing involves researching web assets through the lens of findability and navigability. Participants are given a textual representation of the site’s hierarchy (the “tree”) and asked to locate specific information or complete tasks by selecting paths.
Usability testing: ask participants to interact with a product, website, or application to evaluate its ease of use. This method enables you to uncover areas for improvement in digital key feature functionality by observing participants using the product.
Live website testing: research and collect analytics that outlines the design, usability, and performance efficiencies of a website in real time.
There are no limits to the number of research methods you could use within your project. Just make sure your research methods help you determine the following:
What do you plan to do with the research findings?
What decisions will this research inform? How can your stakeholders leverage the research data and results?
Recruit participants and allocate tasks
Next, identify the participants needed to complete the research and the resources required to complete the tasks. Different people will be proficient at different tasks, and having a task allocation plan will allow everything to run smoothly.
Prepare a thorough project summary
Every well-designed research plan will feature a project summary. This official summary will guide your research alongside its communications or messaging. You’ll use the summary while recruiting participants and during stakeholder meetings. It can also be useful when conducting field studies.
Ensure this summary includes all the elements of your research project. Separate the steps into an easily explainable piece of text that includes the following:
An introduction: the message you’ll deliver to participants about the interview, pre-planned questioning, and testing tasks.
Interview questions: prepare questions you intend to ask participants as part of your research study, guiding the sessions from start to finish.
An exit message: draft messaging your teams will use to conclude testing or survey sessions. These should include the next steps and express gratitude for the participant’s time.
Create a realistic timeline
While your project might already have a deadline or a results timeline in place, you’ll need to consider the time needed to execute it effectively.
Realistically outline the time needed to properly execute each supporting phase of research and implementation. And, as you evaluate the necessary schedules, be sure to include additional time for achieving each milestone in case any changes or unexpected delays arise.
For this part of your research plan, you might find it helpful to create visuals to ensure your research team and stakeholders fully understand the information.
Determine how to present your results
A research plan must also describe how you intend to present your results. Depending on the nature of your project and its goals, you might dedicate one team member (the PI) or assume responsibility for communicating the findings yourself.
In this part of the research plan, you’ll articulate how you’ll share the results. Detail any materials you’ll use, such as:
Presentations and slides
A project report booklet
A project findings pamphlet
Documents with key takeaways and statistics
Graphic visuals to support your findings
- Format your research plan
As you create your research plan, you can enjoy a little creative freedom. A plan can assume many forms, so format it how you see fit. Determine the best layout based on your specific project, intended communications, and the preferences of your teams and stakeholders.
Find format inspiration among the following layouts:
Written outlines
Narrative storytelling
Visual mapping
Graphic timelines
Remember, the research plan format you choose will be subject to change and adaptation as your research and findings unfold. However, your final format should ideally outline questions, problems, opportunities, and expectations.
- Research plan example
Imagine you’ve been tasked with finding out how to get more customers to order takeout from an online food delivery platform. The goal is to improve satisfaction and retain existing customers. You set out to discover why more people aren’t ordering and what it is they do want to order or experience.
You identify the need for a research project that helps you understand what drives customer loyalty. But before you jump in and start calling past customers, you need to develop a research plan—the roadmap that provides focus, clarity, and realistic details to the project.
Here’s an example outline of a research plan you might put together:
Project title
Project members involved in the research plan
Purpose of the project (provide a summary of the research plan’s intent)
Objective 1 (provide a short description for each objective)
Objective 2
Objective 3
Proposed timeline
Audience (detail the group you want to research, such as customers or non-customers)
Budget (how much you think it might cost to do the research)
Risk factors/contingencies (any potential risk factors that may impact the project’s success)
Remember, your research plan doesn’t have to reinvent the wheel—it just needs to fit your project’s unique needs and aims.
Customizing a research plan template
Some companies offer research plan templates to help get you started. However, it may make more sense to develop your own customized plan template. Be sure to include the core elements of a great research plan with your template layout, including the following:
Introductions to participants and stakeholders
Background problems and needs statement
Significance, ethics, and purpose
Research methods, questions, and designs
Preliminary beliefs and expectations
Implications and intended outcomes
Realistic timelines for each phase
Conclusion and presentations
How many pages should a research plan be?
Generally, a research plan can vary in length between 500 to 1,500 words. This is roughly three pages of content. More substantial projects will be 2,000 to 3,500 words, taking up four to seven pages of planning documents.
What is the difference between a research plan and a research proposal?
A research plan is a roadmap to success for research teams. A research proposal, on the other hand, is a dissertation aimed at convincing or earning the support of others. Both are relevant in creating a guide to follow to complete a project goal.
What are the seven steps to developing a research plan?
While each research project is different, it’s best to follow these seven general steps to create your research plan:
Defining the problem
Identifying goals
Choosing research methods
Recruiting participants
Preparing the brief or summary
Establishing task timelines
Defining how you will present the findings
Should you be using a customer insights hub?
Do you want to discover previous research faster?
Do you share your research findings with others?
Do you analyze research data?
Start for free today, add your research, and get to key insights faster
Editor’s picks
Last updated: 11 January 2024
Last updated: 15 January 2024
Last updated: 17 January 2024
Last updated: 12 May 2023
Last updated: 30 April 2024
Last updated: 18 May 2023
Last updated: 25 November 2023
Last updated: 13 May 2024
Latest articles
Related topics, .css-je19u9{-webkit-align-items:flex-end;-webkit-box-align:flex-end;-ms-flex-align:flex-end;align-items:flex-end;display:-webkit-box;display:-webkit-flex;display:-ms-flexbox;display:flex;-webkit-flex-direction:row;-ms-flex-direction:row;flex-direction:row;-webkit-box-flex-wrap:wrap;-webkit-flex-wrap:wrap;-ms-flex-wrap:wrap;flex-wrap:wrap;-webkit-box-pack:center;-ms-flex-pack:center;-webkit-justify-content:center;justify-content:center;row-gap:0;text-align:center;max-width:671px;}@media (max-width: 1079px){.css-je19u9{max-width:400px;}.css-je19u9>span{white-space:pre;}}@media (max-width: 799px){.css-je19u9{max-width:400px;}.css-je19u9>span{white-space:pre;}} decide what to .css-1kiodld{max-height:56px;display:-webkit-box;display:-webkit-flex;display:-ms-flexbox;display:flex;-webkit-align-items:center;-webkit-box-align:center;-ms-flex-align:center;align-items:center;}@media (max-width: 1079px){.css-1kiodld{display:none;}} build next, decide what to build next.

Users report unexpectedly high data usage, especially during streaming sessions.

Users find it hard to navigate from the home page to relevant playlists in the app.

It would be great to have a sleep timer feature, especially for bedtime listening.

I need better filters to find the songs or artists I’m looking for.
Log in or sign up
Get started for free
Academic & Employability Skills
Subscribe to academic & employability skills.
Enter your email address to subscribe to this blog and receive notifications of new posts by email.
Join 411 other subscribers.
Email Address

Writing your dissertation - making an action plan
Posted in: dissertations

Action stations!
Every successful route to completion of a dissertation begins with a practical and workable action plan. Your action plan is a vital tool to help you stay focused, on track and motivated throughout your journey. It is highly likely your supervisor will ask you to make a plan, so that she/he can advise on time frames, targets and goals, and so on.
Before you begin to plot your write-up plan, you need to know when, where, how, and with what or whom you will do your research, and how you will collect and analyse your data.
You need to think about how long it will take you to collect and collate your data and research, and then build that into overall time frames.
Planning your write-up

Then, once you have worked out how much time you will need for data collection, you can then devise your write-up plan.
Use the following rules to help you:
- Write about a page a day.
- Work backwards from at least two weeks before the submission date to calculate when you need to start your writing. (A page is about 500 words, so, for example, if your dissertation is 15,000 words long, you will need at least 30 days to do the writing.)
- Leave two or more weeks at the end for editing and proofreading.
- Include interim achievable targets to help you stay focused and on track.
- Work on different sections - and if you get bogged down switch from one to another.
- Ask a close friend to read it bit by bit and provide feedback on clarity, accuracy and appropriacy.
- Build in meetings slots with your supervisor. Make sure these are strategically placed to catch possible problems at different stages of the write up, or sections of your dissertation.
- Use time-management tools to help you stay on track, e.g. a Gantt chart, or a planning app on your phone.
- Once you have devised your plan, stick to it... It's there for a reason!
Remember it may take you up to three times longer than you expect to write up your dissertation, so build this contingency into your schedule.
Hopkins, D. and Reid, T., 2018. The Academic Skills Handbook: Your Guid e to Success in Writing, Thinking and Communicating at University . Sage.
Share this:
- Click to print (Opens in new window)
- Click to email a link to a friend (Opens in new window)
- Click to share on WhatsApp (Opens in new window)
- Click to share on LinkedIn (Opens in new window)
- Click to share on Twitter (Opens in new window)
- Click to share on Facebook (Opens in new window)
Click here to cancel reply.
- Email * (we won't publish this)
Write a response

Navigating the dissertation process: my tips for final years
Imagine for a moment... After months of hard work and research on a topic you're passionate about, the time has finally come to click the 'Submit' button on your dissertation. You've just completed your longest project to date as part...

8 ways to beat procrastination
Whether you’re writing an assignment or revising for exams, getting started can be hard. Fortunately, there’s lots you can do to turn procrastination into action.

My takeaways on how to write a scientific report
If you’re in your dissertation writing stage or your course includes writing a lot of scientific reports, but you don’t quite know where and how to start, the Skills Centre can help you get started. I recently attended their ‘How...

- Skip to main content
- Skip to primary sidebar
- Skip to footer
- QuestionPro

- Solutions Industries Gaming Automotive Sports and events Education Government Travel & Hospitality Financial Services Healthcare Cannabis Technology Use Case NPS+ Communities Audience Contactless surveys Mobile LivePolls Member Experience GDPR Positive People Science 360 Feedback Surveys
- Resources Blog eBooks Survey Templates Case Studies Training Help center
Home Market Research Research Tools and Apps
Action Research: What it is, Stages & Examples

The best way to get things accomplished is to do it yourself. This statement is utilized in corporations, community projects, and national governments. These organizations are relying on action research to cope with their continuously changing and unstable environments as they function in a more interdependent world.
In practical educational contexts, this involves using systematic inquiry and reflective practice to address real-world challenges, improve teaching and learning, enhance student engagement, and drive positive changes within the educational system.
This post outlines the definition of action research, its stages, and some examples.
Content Index
What is action research?
Stages of action research, the steps to conducting action research, examples of action research, advantages and disadvantages of action research.
Action research is a strategy that tries to find realistic solutions to organizations’ difficulties and issues. It is similar to applied research.
Action research refers basically learning by doing. First, a problem is identified, then some actions are taken to address it, then how well the efforts worked are measured, and if the results are not satisfactory, the steps are applied again.
It can be put into three different groups:
- Positivist: This type of research is also called “classical action research.” It considers research a social experiment. This research is used to test theories in the actual world.
- Interpretive: This kind of research is called “contemporary action research.” It thinks that business reality is socially made, and when doing this research, it focuses on the details of local and organizational factors.
- Critical: This action research cycle takes a critical reflection approach to corporate systems and tries to enhance them.
All research is about learning new things. Collaborative action research contributes knowledge based on investigations in particular and frequently useful circumstances. It starts with identifying a problem. After that, the research process is followed by the below stages:

Stage 1: Plan
For an action research project to go well, the researcher needs to plan it well. After coming up with an educational research topic or question after a research study, the first step is to develop an action plan to guide the research process. The research design aims to address the study’s question. The research strategy outlines what to undertake, when, and how.
Stage 2: Act
The next step is implementing the plan and gathering data. At this point, the researcher must select how to collect and organize research data . The researcher also needs to examine all tools and equipment before collecting data to ensure they are relevant, valid, and comprehensive.
Stage 3: Observe
Data observation is vital to any investigation. The action researcher needs to review the project’s goals and expectations before data observation. This is the final step before drawing conclusions and taking action.
Different kinds of graphs, charts, and networks can be used to represent the data. It assists in making judgments or progressing to the next stage of observing.
Stage 4: Reflect
This step involves applying a prospective solution and observing the results. It’s essential to see if the possible solution found through research can really solve the problem being studied.
The researcher must explore alternative ideas when the action research project’s solutions fail to solve the problem.
Action research is a systematic approach researchers, educators, and practitioners use to identify and address problems or challenges within a specific context. It involves a cyclical process of planning, implementing, reflecting, and adjusting actions based on the data collected. Here are the general steps involved in conducting an action research process:
Identify the action research question or problem
Clearly define the issue or problem you want to address through your research. It should be specific, actionable, and relevant to your working context.
Review existing knowledge
Conduct a literature review to understand what research has already been done on the topic. This will help you gain insights, identify gaps, and inform your research design.
Plan the research
Develop a research plan outlining your study’s objectives, methods, data collection tools, and timeline. Determine the scope of your research and the participants or stakeholders involved.
Collect data
Implement your research plan by collecting relevant data. This can involve various methods such as surveys, interviews, observations, document analysis, or focus groups. Ensure that your data collection methods align with your research objectives and allow you to gather the necessary information.
Analyze the data
Once you have collected the data, analyze it using appropriate qualitative or quantitative techniques. Look for patterns, themes, or trends in the data that can help you understand the problem better.
Reflect on the findings
Reflect on the analyzed data and interpret the results in the context of your research question. Consider the implications and possible solutions that emerge from the data analysis. This reflection phase is crucial for generating insights and understanding the underlying factors contributing to the problem.
Develop an action plan
Based on your analysis and reflection, develop an action plan that outlines the steps you will take to address the identified problem. The plan should be specific, measurable, achievable, relevant, and time-bound (SMART goals). Consider involving relevant stakeholders in planning to ensure their buy-in and support.
Implement the action plan
Put your action plan into practice by implementing the identified strategies or interventions. This may involve making changes to existing practices, introducing new approaches, or testing alternative solutions. Document the implementation process and any modifications made along the way.
Evaluate and monitor progress
Continuously monitor and evaluate the impact of your actions. Collect additional data, assess the effectiveness of the interventions, and measure progress towards your goals. This evaluation will help you determine if your actions have the desired effects and inform any necessary adjustments.
Reflect and iterate
Reflect on the outcomes of your actions and the evaluation results. Consider what worked well, what did not, and why. Use this information to refine your approach, make necessary adjustments, and plan for the next cycle of action research if needed.
Remember that participatory action research is an iterative process, and multiple cycles may be required to achieve significant improvements or solutions to the identified problem. Each cycle builds on the insights gained from the previous one, fostering continuous learning and improvement.
Explore Insightfully Contextual Inquiry in Qualitative Research
Here are two real-life examples of action research.
Action research initiatives are frequently situation-specific. Still, other researchers can adapt the techniques. The example is from a researcher’s (Franklin, 1994) report about a project encouraging nature tourism in the Caribbean.
In 1991, this was launched to study how nature tourism may be implemented on the four Windward Islands in the Caribbean: St. Lucia, Grenada, Dominica, and St. Vincent.
For environmental protection, a government-led action study determined that the consultation process needs to involve numerous stakeholders, including commercial enterprises.
First, two researchers undertook the study and held search conferences on each island. The search conferences resulted in suggestions and action plans for local community nature tourism sub-projects.
Several islands formed advisory groups and launched national awareness and community projects. Regional project meetings were held to discuss experiences, self-evaluations, and strategies. Creating a documentary about a local initiative helped build community. And the study was a success, leading to a number of changes in the area.
Lau and Hayward (1997) employed action research to analyze Internet-based collaborative work groups.
Over two years, the researchers facilitated three action research problem -solving cycles with 15 teachers, project personnel, and 25 health practitioners from diverse areas. The goal was to see how Internet-based communications might affect their virtual workgroup.
First, expectations were defined, technology was provided, and a bespoke workgroup system was developed. Participants suggested shorter, more dispersed training sessions with project-specific instructions.
The second phase saw the system’s complete deployment. The final cycle witnessed system stability and virtual group formation. The key lesson was that the learning curve was poorly misjudged, with frustrations only marginally met by phone-based technical help. According to the researchers, the absence of high-quality online material about community healthcare was harmful.
Role clarity, connection building, knowledge sharing, resource assistance, and experiential learning are vital for virtual group growth. More study is required on how group support systems might assist groups in engaging with their external environment and boost group members’ learning.
Action research has both good and bad points.
- It is very flexible, so researchers can change their analyses to fit their needs and make individual changes.
- It offers a quick and easy way to solve problems that have been going on for a long time instead of complicated, long-term solutions based on complex facts.
- If It is done right, it can be very powerful because it can lead to social change and give people the tools to make that change in ways that are important to their communities.
Disadvantages
- These studies have a hard time being generalized and are hard to repeat because they are so flexible. Because the researcher has the power to draw conclusions, they are often not thought to be theoretically sound.
- Setting up an action study in an ethical way can be hard. People may feel like they have to take part or take part in a certain way.
- It is prone to research errors like selection bias , social desirability bias, and other cognitive biases.
LEARN ABOUT: Self-Selection Bias
This post discusses how action research generates knowledge, its steps, and real-life examples. It is very applicable to the field of research and has a high level of relevance. We can only state that the purpose of this research is to comprehend an issue and find a solution to it.
At QuestionPro, we give researchers tools for collecting data, like our survey software, and a library of insights for any long-term study. Go to the Insight Hub if you want to see a demo or learn more about it.
LEARN MORE FREE TRIAL
Frequently Asked Questions(FAQ’s)
Action research is a systematic approach to inquiry that involves identifying a problem or challenge in a practical context, implementing interventions or changes, collecting and analyzing data, and using the findings to inform decision-making and drive positive change.
Action research can be conducted by various individuals or groups, including teachers, administrators, researchers, and educational practitioners. It is often carried out by those directly involved in the educational setting where the research takes place.
The steps of action research typically include identifying a problem, reviewing relevant literature, designing interventions or changes, collecting and analyzing data, reflecting on findings, and implementing improvements based on the results.
MORE LIKE THIS

Data Information vs Insight: Essential differences
May 14, 2024

Pricing Analytics Software: Optimize Your Pricing Strategy
May 13, 2024

Relationship Marketing: What It Is, Examples & Top 7 Benefits
May 8, 2024

The Best Email Survey Tool to Boost Your Feedback Game
May 7, 2024
Other categories
- Academic Research
- Artificial Intelligence
- Assessments
- Brand Awareness
- Case Studies
- Communities
- Consumer Insights
- Customer effort score
- Customer Engagement
- Customer Experience
- Customer Loyalty
- Customer Research
- Customer Satisfaction
- Employee Benefits
- Employee Engagement
- Employee Retention
- Friday Five
- General Data Protection Regulation
- Insights Hub
- Life@QuestionPro
- Market Research
- Mobile diaries
- Mobile Surveys
- New Features
- Online Communities
- Question Types
- Questionnaire
- QuestionPro Products
- Release Notes
- Research Tools and Apps
- Revenue at Risk
- Survey Templates
- Training Tips
- Uncategorized
- Video Learning Series
- What’s Coming Up
- Workforce Intelligence
Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
Putting Your Research Plan Together
Module 3, Part 1: Research Design
When putting your research plan together, answering the what , when and who questions will guide your thinking as you design your research study.
Let’s break these down further:
What and When?
While putting your research plan together it is important to consider:
- The activities included in the intervention
- The length of the intervention or time frame
Note: A timeline will help the researcher stay focused on their plan. Even if adjustments need to be made to the plan as you proceed it is important to have a timeline.
If your research does not involve an intervention (i.e. exploratory research) where the focus is on understanding or describing, the research plan typically includes simply the data collection strategies that will be used to answer the broad general question and a timeline for collecting data.
Your research plan should outline:
- Your research participants
- How you’ll choose them
Essentially, who will be part of your study?
Consider whether your action research will target:
- all students
- students in a particular course
- a specific section of a course

Source: Envato Elements
Ethical considerations, which we will address in Module 4, may come into play when dealing with course sections.
It’s important to keep in mind that in your project, you aren’t solely the researcher; you’re also a participant. While you might initially think of action research as a way to collect information from others, a significant aspect of it involves self-discovery (Hendricks, 2013).
When it comes to choosing your research participants, there are numerous methods available:
- Simple random sampling
- Systematic sampling
- Cluster sampling
- Convenience sampling
- Purposive sampling
Considering that most action research projects involve the researcher’s own students, it’s highly probable that purposive sampling, where participants are chosen for a particular reason will be the preferred approach .
Note: Your research question drives your research design.
The following are some guidelines that will help map out your research design:
- Research focus
- Research participant characteristics
- Sample size
- Length & frequency of intervention
- Data: what will be collected, how will it be accessed, what is the timing?
(Duesbery & Twyman, 2020)
Action Research Handbook Copyright © by Dr. Zabedia Nazim and Dr. Sowmya Venkat-Kishore is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License , except where otherwise noted.
Share This Book

Linking Research to Action: A Simple Guide to Writing an Action Research Report
What Is Action Research, and Why Do We Do It?
Action research is any research into practice undertaken by those involved in that practice, with the primary goal of encouraging continued reflection and making improvement. It can be done in any professional field, including medicine, nursing, social work, psychology, and education. Action research is particularly popular in the field of education. When it comes to teaching, practitioners may be interested in trying out different teaching methods in the classroom, but are unsure of their effectiveness. Action research provides an opportunity to explore the effectiveness of a particular teaching practice, the development of a curriculum, or your students’ learning, hence making continual improvement possible. In other words, the use of an interactive action-and-research process enables practitioners to get an idea of what they and their learners really do inside of the classroom, not merely what they think they can do. By doing this, it is hoped that both the teaching and the learning occurring in the classroom can be better tailored to fit the learners’ needs.
You may be wondering how action research differs from traditional research. The term itself already suggests that it is concerned with both “action” and “research,” as well as the association between the two. Kurt Lewin (1890-1947), a famous psychologist who coined this term, believed that there was “no action without research; no research without action” (Marrow, 1969, p.163). It is certainly possible, and perhaps commonplace, for people to try to have one without the other, but the unique combination of the two is what distinguishes action research from most other forms of enquiry. Traditional research emphasizes the review of prior research, rigorous control of the research design, and generalizable and preferably statistically significant results, all of which help examine the theoretical significance of the issue. Action research, with its emphasis on the insider’s perspective and the practical significance of a current issue, may instead allow less representative sampling, looser procedures, and the presentation of raw data and statistically insignificant results.
What Should We Include in an Action Research Report?
The components put into an action research report largely coincide with the steps used in the action research process. This process usually starts with a question or an observation about a current problem. After identifying the problem area and narrowing it down to make it more manageable for research, the development process continues as you devise an action plan to investigate your question. This will involve gathering data and evidence to support your solution. Common data collection methods include observation of individual or group behavior, taking audio or video recordings, distributing questionnaires or surveys, conducting interviews, asking for peer observations and comments, taking field notes, writing journals, and studying the work samples of your own and your target participants. You may choose to use more than one of these data collection methods. After you have selected your method and are analyzing the data you have collected, you will also reflect upon your entire process of action research. You may have a better solution to your question now, due to the increase of your available evidence. You may also think about the steps you will try next, or decide that the practice needs to be observed again with modifications. If so, the whole action research process starts all over again.
In brief, action research is more like a cyclical process, with the reflection upon your action and research findings affecting changes in your practice, which may lead to extended questions and further action. This brings us back to the essential steps of action research: identifying the problem, devising an action plan, implementing the plan, and finally, observing and reflecting upon the process. Your action research report should comprise all of these essential steps. Feldman and Weiss (n.d.) summarized them as five structural elements, which do not have to be written in a particular order. Your report should:
- Describe the context where the action research takes place. This could be, for example, the school in which you teach. Both features of the school and the population associated with it (e.g., students and parents) would be illustrated as well.
- Contain a statement of your research focus. This would explain where your research questions come from, the problem you intend to investigate, and the goals you want to achieve. You may also mention prior research studies you have read that are related to your action research study.
- Detail the method(s) used. This part includes the procedures you used to collect data, types of data in your report, and justification of your used strategies.
- Highlight the research findings. This is the part in which you observe and reflect upon your practice. By analyzing the evidence you have gathered, you will come to understand whether the initial problem has been solved or not, and what research you have yet to accomplish.
- Suggest implications. You may discuss how the findings of your research will affect your future practice, or explain any new research plans you have that have been inspired by this report’s action research.
The overall structure of your paper will actually look more or less the same as what we commonly see in traditional research papers.
What Else Do We Need to Pay Attention to?
We discussed the major differences between action research and traditional research in the beginning of this article. Due to the difference in the focus of an action research report, the language style used may not be the same as what we normally see or use in a standard research report. Although both kinds of research, both action and traditional, can be published in academic journals, action research may also be published and delivered in brief reports or on websites for a broader, non-academic audience. Instead of using the formal style of scientific research, you may find it more suitable to write in the first person and use a narrative style while documenting your details of the research process.
However, this does not forbid using an academic writing style, which undeniably enhances the credibility of a report. According to Johnson (2002), even though personal thoughts and observations are valued and recorded along the way, an action research report should not be written in a highly subjective manner. A personal, reflective writing style does not necessarily mean that descriptions are unfair or dishonest, but statements with value judgments, highly charged language, and emotional buzzwords are best avoided.
Furthermore, documenting every detail used in the process of research does not necessitate writing a lengthy report. The purpose of giving sufficient details is to let other practitioners trace your train of thought, learn from your examples, and possibly be able to duplicate your steps of research. This is why writing a clear report that does not bore or confuse your readers is essential.
Lastly, You May Ask, Why Do We Bother to Even Write an Action Research Report?
It sounds paradoxical that while practitioners tend to have a great deal of knowledge at their disposal, often they do not communicate their insights to others. Take education as an example: It is both regrettable and regressive if every teacher, no matter how professional he or she might be, only teaches in the way they were taught and fails to understand what their peer teachers know about their practice. Writing an action research report provides you with the chance to reflect upon your own practice, make substantiated claims linking research to action, and document action and ideas as they take place. The results can then be kept, both for the sake of your own future reference, and to also make the most of your insights through the act of sharing with your professional peers.
Feldman, A., & Weiss, T. (n.d.). Suggestions for writing the action research report . Retrieved from http://people.umass.edu/~afeldman/ARreadingmaterials/WritingARReport.html
Johnson, A. P. (2002). A short guide to action research . Boston, MA: Allyn & Bacon.
Marrow, A. J. (1969). The practical theorist: The life and work of Kurt Lewin . New York, NY: Basic Books.
Tiffany Ip is a lecturer at Hong Kong Baptist University. She gained a PhD in neurolinguistics after completing her Bachelor’s degree in psychology and linguistics. She strives to utilize her knowledge to translate brain research findings into practical classroom instruction.

- Section 2: Home
- Developing the Quantitative Research Design
- Qualitative Descriptive Design
- Design and Development Research (DDR) For Instructional Design
- Qualitative Narrative Inquiry Research
- Action Research Resource
What is Action Research?
Considerations, creating a plan of action.
- Case Study Design in an Applied Doctorate
- SAGE Research Methods
- Research Examples (SAGE) This link opens in a new window
- Dataset Examples (SAGE) This link opens in a new window
- IRB Resource Center This link opens in a new window
Action research is a qualitative method that focuses on solving problems in social systems, such as schools and other organizations. The emphasis is on solving the presenting problem by generating knowledge and taking action within the social system in which the problem is located. The goal is to generate shared knowledge of how to address the problem by bridging the theory-practice gap (Bourner & Brook, 2019). A general definition of action research is the following: “Action research brings together action and reflection, as well as theory and practice, in participation with others, in the pursuit of practical solutions to issues of pressing concern” (Bradbury, 2015, p. 1). Johnson (2019) defines action research in the field of education as “the process of studying a school, classroom, or teacher-learning situation with the purpose of understanding and improving the quality of actions or instruction” (p.255).
Origins of Action Research
Kurt Lewin is typically credited with being the primary developer of Action Research in the 1940s. Lewin stated that action research can “transform…unrelated individuals, frequently opposed in their outlook and their interests, into cooperative teams, not on the basis of sweetness but on the basis of readiness to face difficulties realistically, to apply honest fact-finding, and to work together to overcome them” (1946, p.211).
Sample Action Research Topics
Some sample action research topics might be the following:
- Examining how classroom teachers perceive and implement new strategies in the classroom--How is the strategy being used? How do students respond to the strategy? How does the strategy inform and change classroom practices? Does the new skill improve test scores? Do classroom teachers perceive the strategy as effective for student learning?
- Examining how students are learning a particular content or objectives--What seems to be effective in enhancing student learning? What skills need to be reinforced? How do students respond to the new content? What is the ability of students to understand the new content?
- Examining how education stakeholders (administrator, parents, teachers, students, etc.) make decisions as members of the school’s improvement team--How are different stakeholders encouraged to participate? How is power distributed? How is equity demonstrated? How is each voice valued? How are priorities and initiatives determined? How does the team evaluate its processes to determine effectiveness?
- Examining the actions that school staff take to create an inclusive and welcoming school climate--Who makes and implements the actions taken to create the school climate? Do members of the school community (teachers, staff, students) view the school climate as inclusive? Do members of the school community feel welcome in the school? How are members of the school community encouraged to become involved in school activities? What actions can school staff take to help others feel a part of the school community?
- Examining the perceptions of teachers with regard to the learning strategies that are more effective with special populations, such as special education students, English Language Learners, etc.—What strategies are perceived to be more effective? How do teachers plan instructionally for unique learners such as special education students or English Language Learners? How do teachers deal with the challenges presented by unique learners such as special education students or English Language Learners? What supports do teachers need (e.g., professional development, training, coaching) to more effectively deliver instruction to unique learners such as special education students or English Language Learners?
Remember—The goal of action research is to find out how individuals perceive and act in a situation so the researcher can develop a plan of action to improve the educational organization. While these topics listed here can be explored using other research designs, action research is the design to use if the outcome is to develop a plan of action for addressing and improving upon a situation in the educational organization.
Considerations for Determining Whether to Use Action Research in an Applied Dissertation
- When considering action research, first determine the problem and the change that needs to occur as a result of addressing the problem (i.e., research problem and research purpose). Remember, the goal of action research is to change how individuals address a particular problem or situation in a way that results in improved practices.
- If the study will be conducted at a school site or educational organization, you may need site permission. Determine whether site permission will be given to conduct the study.
- Consider the individuals who will be part of the data collection (e.g., teachers, administrators, parents, other school staff, etc.). Will there be a representative sample willing to participate in the research?
- If students will be part of the study, does parent consent and student assent need to be obtained?
- As you develop your data collection plan, also consider the timeline for data collection. Is it feasible? For example, if you will be collecting data in a school, consider winter and summer breaks, school events, testing schedules, etc.
- As you develop your data collection plan, consult with your dissertation chair, Subject Matter Expert, NU Academic Success Center, and the NU IRB for resources and guidance.
- Action research is not an experimental design, so you are not trying to accept or reject a hypothesis. There are no independent or dependent variables. It is not generalizable to a larger setting. The goal is to understand what is occurring in the educational setting so that a plan of action can be developed for improved practices.
Considerations for Action Research
Below are some things to consider when developing your applied dissertation proposal using Action Research (adapted from Johnson, 2019):
- Research Topic and Research Problem -- Decide the topic to be studied and then identify the problem by defining the issue in the learning environment. Use references from current peer-reviewed literature for support.
- Purpose of the Study —What need to be different or improved as a result of the study?
- Research Questions —The questions developed should focus on “how” or “what” and explore individuals’ experiences, beliefs, and perceptions.
- Theoretical Framework -- What are the existing theories (theoretical framework) or concepts (conceptual framework) that can be used to support the research. How does existing theory link to what is happening in the educational environment with regard to the topic? What theories have been used to support similar topics in previous research?
- Literature Review -- Examine the literature, focusing on peer-reviewed studies published in journal within the last five years, with the exception of seminal works. What about the topic has already been explored and examined? What were the findings, implications, and limitations of previous research? What is missing from the literature on the topic? How will your proposed research address the gap in the literature?
- Data Collection —Who will be part of the sample for data collection? What data will be collected from the individuals in the study (e.g., semi-structured interviews, surveys, etc.)? What are the educational artifacts and documents that need to be collected (e.g., teacher less plans, student portfolios, student grades, etc.)? How will they be collected and during what timeframe? (Note--A list of sample data collection methods appears under the heading of “Sample Instrumentation.”)
- Data Analysis —Determine how the data will be analyzed. Some types of analyses that are frequently used for action research include thematic analysis and content analysis.
- Implications —What conclusions can be drawn based upon the findings? How do the findings relate to the existing literature and inform theory in the field of education?
- Recommendations for Practice--Create a Plan of Action— This is a critical step in action research. A plan of action is created based upon the data analysis, findings, and implications. In the Applied Dissertation, this Plan of Action is included with the Recommendations for Practice. The includes specific steps that individuals should take to change practices; recommendations for how those changes will occur (e.g., professional development, training, school improvement planning, committees to develop guidelines and policies, curriculum review committee, etc.); and methods to evaluate the plan’s effectiveness.
- Recommendations for Research —What should future research focus on? What type of studies need to be conducted to build upon or further explore your findings.
- Professional Presentation or Defense —This is where the findings will be presented in a professional presentation or defense as the culmination of your research.
Adapted from Johnson (2019).
Considerations for Sampling and Data Collection
Below are some tips for sampling, sample size, data collection, and instrumentation for Action Research:
Sampling and Sample Size
Action research uses non-probability sampling. This is most commonly means a purposive sampling method that includes specific inclusion and exclusion criteria. However, convenience sampling can also be used (e.g., a teacher’s classroom).
Critical Concepts in Data Collection
Triangulation- - Dosemagen and Schwalbach (2019) discussed the importance of triangulation in Action Research which enhances the trustworthiness by providing multiple sources of data to analyze and confirm evidence for findings.
Trustworthiness —Trustworthiness assures that research findings are fulfill four critical elements—credibility, dependability, transferability, and confirmability. Reflect on the following: Are there multiple sources of data? How have you ensured credibility, dependability, transferability, and confirmability? Have the assumptions, limitations, and delimitations of the study been identified and explained? Was the sample a representative sample for the study? Did any individuals leave the study before it ended? How have you controlled researcher biases and beliefs? Are you drawing conclusions that are not supported by data? Have all possible themes been considered? Have you identified other studies with similar results?
Sample Instrumentation
Below are some of the possible methods for collecting action research data:
- Pre- and Post-Surveys for students and/or staff
- Staff Perception Surveys and Questionnaires
- Semi-Structured Interviews
- Focus Groups
- Observations
- Document analysis
- Student work samples
- Classroom artifacts, such as teacher lesson plans, rubrics, checklists, etc.
- Attendance records
- Discipline data
- Journals from students and/or staff
- Portfolios from students and/or staff
A benefit of Action Research is its potential to influence educational practice. Many educators are, by nature of the profession, reflective, inquisitive, and action-oriented. The ultimate outcome of Action Research is to create a plan of action using the research findings to inform future educational practice. A Plan of Action is not meant to be a one-size fits all plan. Instead, it is mean to include specific data-driven and research-based recommendations that result from a detailed analysis of the data, the study findings, and implications of the Action Research study. An effective Plan of Action includes an evaluation component and opportunities for professional educator reflection that allows for authentic discussion aimed at continuous improvement.
When developing a Plan of Action, the following should be considered:
- How can this situation be approached differently in the future?
- What should change in terms of practice?
- What are the specific steps that individuals should take to change practices?
- What is needed to implement the changes being recommended (professional development, training, materials, resources, planning committees, school improvement planning, etc.)?
- How will the effectiveness of the implemented changes be evaluated?
- How will opportunities for professional educator reflection be built into the Action Plan?
Sample Action Research Studies
Anderson, A. J. (2020). A qualitative systematic review of youth participatory action research implementation in U.S. high schools. A merican Journal of Community Psychology, 65 (1/2), 242–257. https://onlinelibrary-wiley-com.proxy1.ncu.edu/doi/epdf/10.1002/ajcp.12389
Ayvaz, Ü., & Durmuş, S.(2021). Fostering mathematical creativity with problem posing activities: An action research with gifted students. Thinking Skills and Creativity, 40. https://proxy1.ncu.edu/login?url=https://search.ebscohost.com/login.aspx?direct=true&db=edselp&AN=S1871187121000614&site=eds-live
Bellino, M. J. (2018). Closing information gaps in Kakuma Refugee Camp: A youth participatory action research study. American Journal of Community Psychology, 62 (3/4), 492–507. https://proxy1.ncu.edu/login?url=https://search.ebscohost.com/login.aspx?direct=true&db=ofs&AN=133626988&site=eds-live
Beneyto, M., Castillo, J., Collet-Sabé, J., & Tort, A. (2019). Can schools become an inclusive space shared by all families? Learnings and debates from an action research project in Catalonia. Educational Action Research, 27 (2), 210–226. https://proxy1.ncu.edu/login?url=https://search.ebscohost.com/login.aspx?direct=true&db=ehh&AN=135671904&site=eds-live
Bilican, K., Senler, B., & Karısan, D. (2021). Fostering teacher educators’ professional development through collaborative action research. International Journal of Progressive Education, 17 (2), 459–472. https://proxy1.ncu.edu/login?url=https://search.ebscohost.com/login.aspx?direct=true&db=ehh&AN=149828364&site=eds-live
Black, G. L. (2021). Implementing action research in a teacher preparation program: Opportunities and limitations. Canadian Journal of Action Research, 21 (2), 47–71. https://proxy1.ncu.edu/login?url=https://search.ebscohost.com/login.aspx?direct=true&db=ehh&AN=149682611&site=eds-live
Bozkuş, K., & Bayrak, C. (2019). The Application of the dynamic teacher professional development through experimental action research. International Electronic Journal of Elementary Education, 11 (4), 335–352. https://proxy1.ncu.edu/login?url=https://search.ebscohost.com/login.aspx?direct=true&db=ehh&AN=135580911&site=eds-live
Christ, T. W. (2018). Mixed methods action research in special education: An overview of a grant-funded model demonstration project. Research in the Schools, 25( 2), 77–88. https://proxy1.ncu.edu/login?url=https://search.ebscohost.com/login.aspx?direct=true&db=ehh&AN=135047248&site=eds-live
Jakhelln, R., & Pörn, M. (2019). Challenges in supporting and assessing bachelor’s theses based on action research in initial teacher education. Educational Action Research, 27 (5), 726–741. https://proxy1.ncu.edu/login?url=https://search.ebscohost.com/login.aspx?direct=true&db=ehh&AN=140234116&site=eds-live
Klima Ronen, I. (2020). Action research as a methodology for professional development in leading an educational process. Studies in Educational Evaluation, 64 . https://proxy1.ncu.edu/login?url=https://search.ebscohost.com/login.aspx?direct=true&db=edselp&AN=S0191491X19302159&site=eds-live
Messiou, K. (2019). Collaborative action research: facilitating inclusion in schools. Educational Action Research, 27 (2), 197–209. https://proxy1.ncu.edu/login?url=https://search.ebscohost.com/login.aspx?direct=true&db=ehh&AN=135671898&site=eds-live
Mitchell, D. E. (2018). Say it loud: An action research project examining the afrivisual and africology, Looking for alternative African American community college teaching strategies. Journal of Pan African Studies, 12 (4), 364–487. https://proxy1.ncu.edu/login?url=https://search.ebscohost.com/login.aspx?direct=true&db=ofs&AN=133155045&site=eds-live
Pentón Herrera, L. J. (2018). Action research as a tool for professional development in the K-12 ELT classroom. TESL Canada Journal, 35 (2), 128–139. https://proxy1.ncu.edu/login?url=https://search.ebscohost.com/login.aspx?direct=true&db=ofs&AN=135033158&site=eds-live
Rodriguez, R., Macias, R. L., Perez-Garcia, R., Landeros, G., & Martinez, A. (2018). Action research at the intersection of structural and family violence in an immigrant Latino community: a youth-led study. Journal of Family Violence, 33 (8), 587–596. https://proxy1.ncu.edu/login?url=https://search.ebscohost.com/login.aspx?direct=true&db=ccm&AN=132323375&site=eds-live
Vaughan, M., Boerum, C., & Whitehead, L. (2019). Action research in doctoral coursework: Perceptions of independent research experiences. International Journal for the Scholarship of Teaching and Learning, 13 . https://proxy1.ncu.edu/login?url=https://search.ebscohost.com/login.aspx?direct=true&db=edsdoj&AN=edsdoj.17aa0c2976c44a0991e69b2a7b4f321&site=eds-live
Sample Journals for Action Research
Educational Action Research
Canadian Journal of Action Research
Sample Resource Videos
Call-Cummings, M. (2017). Researching racism in schools using participatory action research [Video]. Sage Research Methods http://proxy1.ncu.edu/login?URL=https://methods.sagepub.com/video/researching-racism-in-schools-using-participatory-action-research
Fine, M. (2016). Michelle Fine discusses community based participatory action research [Video]. Sage Knowledge. http://proxy1.ncu.edu/login?URL=https://sk-sagepub-com.proxy1.ncu.edu/video/michelle-fine-discusses-community-based-participatory-action-research
Getz, C., Yamamura, E., & Tillapaugh. (2017). Action Research in Education. [Video]. You Tube. https://www.youtube.com/watch?v=X2tso4klYu8
Bradbury, H. (Ed.). (2015). The handbook of action research (3rd edition). Sage.
Bradbury, H., Lewis, R. & Embury, D.C. (2019). Education action research: With and for the next generation. In C.A. Mertler (Ed.), The Wiley handbook of action research in education (1st edition). John Wiley and Sons. https://ebookcentral.proquest.com/lib/nu/reader.action?docID=5683581&ppg=205
Bourner, T., & Brook, C. (2019). Comparing and contrasting action research and action learning. In C.A. Mertler (Ed.), The Wiley handbook of action research in education (1st edition). John Wiley and Sons. https://ebookcentral.proquest.com/lib/nu/reader.action?docID=5683581&ppg=205
Bradbury, H. (2015). The Sage handbook of action research . Sage. https://www-doi-org.proxy1.ncu.edu/10.4135/9781473921290
Dosemagen, D.M. & Schwalback, E.M. (2019). Legitimacy of and value in action research. In C.A. Mertler (Ed.), The Wiley handbook of action research in education (1st edition). John Wiley and Sons. https://ebookcentral.proquest.com/lib/nu/reader.action?docID=5683581&ppg=205
Johnson, A. (2019). Action research for teacher professional development. In C.A. Mertler (Ed.), The Wiley handbook of action research in education (1st edition). John Wiley and Sons. https://ebookcentral.proquest.com/lib/nu/reader.action?docID=5683581&ppg=205
Lewin, K. (1946). Action research and minority problems. In G.W. Lewin (Ed.), Resolving social conflicts: Selected papers on group dynamics (compiled in 1948). Harper and Row.
Mertler, C. A. (Ed.). (2019). The Wiley handbook of action research in education. John Wiley and Sons. https://ebookcentral.proquest.com/lib/nu/detail.action?docID=5683581
- << Previous: Qualitative Narrative Inquiry Research
- Next: Case Study Design in an Applied Doctorate >>
- Last Updated: Jul 28, 2023 8:05 AM
- URL: https://resources.nu.edu/c.php?g=1013605

Research Action Plan

It is a fact that a research action plan is needed not only to provide a solution for an existing problem but also to provide detailed information for a new study. Research action plans are conducted by numerous individuals and groups on different fields (i.e., business, science, academe, government, technology, etc.).
Research Action Plan Template

- Google Docs
Size: A4, US
To guide you in creating a research action plan, we have provided some examples (in PDF format) as well as tips on how to create a research action plan.
Action Plan Template

- Apple Pages
Size: 36 KB
Action Plan Template to Print

User Research Action Plan Example

Size: 71 KB
New Research Plan Outline Example

Size: 273 KB
Research Action Proposal Outline Example

Size: 40 KB
The Importance of Creating a Research Action Plan
The importance of research action plans cannot be understated. As previously mentioned, they are conducted by various individuals and groups on various fields. Although they are commonly used by business entities and scientific organizations, they are also used by academe (by both professors and students alike), government, technology, sports, and social welfare groups. You may also see quality plan examples & samples .
We will be discussing below the importance of research action plans to each sector that was mentioned.
1. Business
This is where research action plans are constantly created and used. Business entities, specifically companies, conduct research for various reasons. Some do research to develop a new product or improve an existing one, some do research to analyze a new market, some do it for investment analysis , while some companies do it to improve their competitive advantage.
The reasons are not limited to the ones mentioned above, as they are other numerous reasons why companies conduct research. But despite the reason, business research is always aimed toward two things: profitability and sustainability.
Similar to business entities, scientific organizations also do heavy research. Scientific research is always aimed to provide better living conditions for not only humans but all the organisms living on this planet. Additionally, scientific research also centers on discovering things that were not deemed possible before (for example: evolution, relativity, space travel, etc.). You may also like company plan examples & samples .
3. Technology
Science and technology are always intertwined. Technology uses scientific processes to discover new objects and possibilities, while science uses technology to do the same thing. Since the dawn of the digital age, technology has been moving at a breakneck speed. Research has resulted in the most groundbreaking technological discoveries in the 21st century, and more is yet it to come in the next few years. You may also check out advertising plan examples & samples .
The images you see in movies (for example, the Iron Man or Black Panther suit, hologram interaction, nanotechnology) will all be possible sooner than you think.
4. Government
The most advanced and progressive countries rely on their government to do research. Either research to develop new infrastructure, improve transportation and utility systems, eradicate poverty, or to increase foreign and domestic investors, research has been key to improve a country’s economic standing and decrease national debt. You might be interested in sales plan examples .
Similar to science and technology, government and academe are also intertwined in which both sectors benefit each other. In most countries, government asks the assistance of academic institutions to create a research action plan, especially in studies relating to education. You may have also noticed that various educators have taken government positions to extend their expertise to the government. You may also see event plan examples & samples .
Playing sports is both a great pastime and a great money earner. There is money in sports, which is why numerous organizations turn it into a business. Sports-centered research do not only focus on increasing physical abilities and skills but also on marketing. Sports apparel companies like Adidas and Nike, as well as sports personalities like Michael Jordan and Lionel Messi, have all benefited not only from sports health and wellness research but also from sports marketing research. You may also like daily plan examples & samples .
7. Social Welfare
Social welfare is a subcategory of government, but this focuses on human resource specifically the improving of living conditions of individuals and communities.
Social welfare is very important as human resource provides the backbone of every country. If individuals are struggling to meet their daily needs, they become unhealthy and unfocused, thus reducing their effectiveness as being part of the country’s workforce. An unproductive workforce cannot support the government in any way possible. You may also check out management plan examples .
That is why research based on social welfare helps government identify and solve issues in regards to their citizens, aiding them to improve their financial standing to become more effective and efficient in their respective industries.
Market Research Action Plan Example

Size: 253 KB
Research Plan Proposal Example

Size: 56 KB
Research Proposal Template Example

Size: 65 KB
Research Action Plan Outline Example

Size: 96 KB
Basic Research Action Plan Outline
There is no standard outline in creating a research action plan. But there are sections in which are found in most research action plans. Listed below is a basic research action plan outline which is highly recommended when you will be making your own research plan in the future. You may also see annual plan examples and samples .
Feel free to edit and add sections from the PDF research action plan examples we provided if you think some sections are relevant to your research.
1. Introduction
Sometimes, researchers tend to overlook the introduction as it does not contain the meat of the study. But the introduction is as important as the other sections of the research action plan.
The introduction contains information on why the research is being conducted, and also provides info on how the research will affect the industry or sector it was based on. Remember that the introduction is not a summary of the research . That section is called “abstract.” The abstract is written once the study has been accomplished, and is usually inserted after the introduction.
2. Statement of the Problem
The general statement of the problem identifies the problems or issues that need to be solved in the research. The statement of the problem is usually formulated using WH and H questions, but those questions need to be very specific. Providing general questions will be difficult for the researcher especially when he reaches the data-gathering stage.
Here is an example of a “how” question in a problem statement for a research focusing on hologram smartphone development in 2018:
Incorrect (general): How can smartphone companies develop hologram technology in their products in 2018?
Correct (specific): How can the leading smartphone manufacturers Apple, Samsung, and Vivo implement hologram technology in their high-end phones when they have functions and features lined up for their models in the next two years? You may also like audit plan examples & samples .
Based on the examples above, it will be easier for the researcher to conduct the research as he will be focused on three smartphone companies Apple, Samsung, and Vivo instead of all the smartphone manufacturers as stated in the first problem. Additionally, the second problem centers in on the hologram’s impact to the company’s current portfolio of products, while the first problem does not even recognize the current products of the companies. You may also check out work plan examples & samples .
3. Methodology
The methodology identifies the research’s respondents, locale, research design, and data-gathering procedure. This section basically lists down the methods and procedures the researcher will use in his study. The methodology tremendously aids the researcher as he focuses on the methods and procedures he previously chose, creating a more streamlined study that does not stray away from the problems the researcher wants to solve. You might be interested in weekly plan examples & samples .
4. Analysis of Data
Data analysis is basically the meat of the entire study or research. Data analysis is conducted after all the data have been compiled. There are numerous data analysis methods that researchers use, but the one that is actually used depends on the data that was gathered (number of respondents, type of study, research topic, etc.). You may also see implementation plan examples & samples .
Most of the time, a statistician assists the researcher on tabulating the data and also assists in identifying what analysis method to use. Data analysis will help the researcher determine what recommendations to use, so it is crucial that the data should be analyzed carefully. You may also like job plan examples & samples .
5. Recommendation
Recommendations are the result of data analysis. This section answers the statement of the problem through the data that was gathered and analyzed. Make sure each question in the statement of the problem has a corresponding recommendation. Recommendations are basically the solutions to the problems you presented, so again be specific in how you present your recommendations. You may also check out business plan examples .
Here is an example on a recommendation based on the problem listed above. How can the leading smartphone manufacturers Apple, Samsung, and Vivo implement hologram technology in their high-end phones when they have functions and features lined up for their models in the next two years? You might be interested in transition plan examples & samples .
Incorrect (general): The three smartphone companies should have a separate department to produce a new line of products that will implement hologram technology. (No further analysis is discussed).
Correct (specific): Based on 70% of the responses, the three smartphone companies should have a separate department to produce a new line of products that will implement hologram technology. This will create a more smooth production process as two departments will be working on different products, but still under the same company. (Detailed analysis to follow.) You may also see project plan examples .
6. Conclusion
The research conclusion is the last part of the research and serves a similar purpose to the introduction. The conclusion basically reiterates the information that was previously mentioned in the data analysis and recommendation, but it is not the summary of the entire research. The conclusion also agrees on what recommendations were made by the researcher. No further analysis is conducted in the conclusion. You may also like evaluation plan examples & samples .
Doctoral Thesis Research Plan Example

Size: 219 KB
Executive Summary for Research Plan Example

Size: 186 KB
Abstract Research Plan Example

Size: 92 KB
We hope you found this article to be informative as well as helpful when you will be making your own research action plan. We also included some examples in PDF to assist you (they are all free to download). Doing research requires long hours of hard work and patience, and sometimes the results do not even go the way you planned them to. The quality of data you compile and your eventual analysis of the said data are not the only determinants on creating a successful research study, as you also need to have a good research action plan .
Text prompt
- Instructive
- Professional
Create a study plan for final exams in high school
Develop a project timeline for a middle school science fair.
We use essential cookies to make Venngage work. By clicking “Accept All Cookies”, you agree to the storing of cookies on your device to enhance site navigation, analyze site usage, and assist in our marketing efforts.
Manage Cookies
Cookies and similar technologies collect certain information about how you’re using our website. Some of them are essential, and without them you wouldn’t be able to use Venngage. But others are optional, and you get to choose whether we use them or not.
Strictly Necessary Cookies
These cookies are always on, as they’re essential for making Venngage work, and making it safe. Without these cookies, services you’ve asked for can’t be provided.
Show cookie providers
- Google Login
Functionality Cookies
These cookies help us provide enhanced functionality and personalisation, and remember your settings. They may be set by us or by third party providers.
Performance Cookies
These cookies help us analyze how many people are using Venngage, where they come from and how they're using it. If you opt out of these cookies, we can’t get feedback to make Venngage better for you and all our users.
- Google Analytics
Targeting Cookies
These cookies are set by our advertising partners to track your activity and show you relevant Venngage ads on other sites as you browse the internet.
- Google Tag Manager
- Infographics
- Daily Infographics
- Popular Templates
- Accessibility
- Graphic Design
- Graphs and Charts
- Data Visualization
- Human Resources
- Beginner Guides
Blog What is an Action Plan & How to Write One [With Examples]
What is an Action Plan & How to Write One [With Examples]
Written by: Danesh Ramuthi Oct 26, 2023

An action plan is a meticulously structured strategy that pinpoints specific steps, tasks and resources vital to turning a goal into reality. It is extremely useful in any project management.
Crafting an action plan is like plotting a route for a cross-country journey. It’s the strategic map that outlines every step, decision and pitstop needed to reach your ultimate destination.
With a well-thought-out action plan, you’re not just shooting in the dark; you’re making informed, purposeful strides towards your goals. Dive deep with our guide and witness real-world examples that will inspire and guide you.
Need a tool to kickstart your planning? Try out the Venngage business plan maker and explore their extensive collection of action plan templates .
Click to jump ahead:
What is the purpose of an action plan?
When to develop an action plan, 7 components of a actions plan, 15 action plan examples.
- How to Write an action plan?
Final thoughts
An action plan serves as a strategic tool designed to outline specific steps, tasks and goals necessary to achieve a particular objective.
Its primary purpose is to provide a clear roadmap and direction for individuals, teams or organizations to follow in order to efficiently and effectively accomplish their goals.
Action plans break down complex projects into manageable, actionable components, making it easier to track progress and stay on course.
Moreover, action plans play a crucial role in fostering accountability and coordination among team members. By assigning responsibilities and deadlines for each task or milestone, they ensure that everyone involved is aware of their roles and the overall timeline, reducing confusion and enhancing teamwork.
Additionally, action plans help in resource allocation, budgeting and risk management by enabling stakeholders to identify potential challenges and plan for contingencies.
Overall, the purpose of an action plan is to transform abstract goals into concrete actions, making them more achievable and measurable while ensuring that the resources and efforts are aligned with the desired outcomes.
Developing an action plan is crucial when you’re looking to achieve a specific goal or outcome. Here are instances when you should consider developing an action plan:
- Start of an organization : Ideally, an action plan should be developed within the first six months to one year of the start of an organization. This initial plan lays the groundwork for the future direction and growth of the entity.
- Project initiation : At the start of any project, an action plan helps to clearly define the tasks, responsibilities, and timelines.
- Goal setting : Whenever you or your organization sets a new goal. Action plans transform these goals from abstract ideas into concrete steps.
- Strategic planning : For long-term visions and missions, action plans break down the journey into manageable pieces, each with its timeline and responsible parties.
- Performance improvement : If there are areas where performance is lacking, whether it’s personal or organizational, an action plan can outline the steps needed to elevate performance.
An action plan is a detailed outline that breaks down the steps necessary to achieve a specific goal. Here are the typical components of an action plan.
1. Objective or Goal
The cornerstone of your action plan is the objective or goal. This should be a clear and concise statement outlining the desired outcome or result. Having a well-defined objective provides a direction and purpose to the entire plan, ensuring all tasks and actions are aligned towards achieving this singular aim.
2. Tasks or Actions
Once the objective is set, the next step is to list down the specific tasks or actions required to achieve this goal. These tasks should be broken down into detailed steps, ensuring no essential activity is overlooked. The granularity of these tasks can vary based on the complexity of the goal.
3. Set deadline
For each task or action, set a realistic and achievable deadline. This timeline ensures that the plan stays on track and that momentum is maintained throughout the execution. It also allows for monitoring progress and identifying potential delays early.
4. Resources needed to complete the project
It’s crucial to recognize and list the resources you’ll need to complete the tasks. This can encompass financial resources, human resources, equipment, technological tools or any other assets. Identifying these early ensures that there are no bottlenecks during execution due to a lack of necessary resources.
5. Person responsible
Assign a person or a team for each task. This designation ensures accountability and clarity. When individuals are aware of their responsibilities, it reduces overlap, confusion and ensures that every task has someone overseeing its completion.
6. Potential barriers or challenges
Every plan will face challenges. By anticipating potential barriers or obstacles, you can be better prepared to address them. This proactive approach ensures smoother execution and less reactionary problem-solving.
7. Measurement of key performance indicators (KPIs)
Determine how you’ll measure the success of each task or the plan overall. KPIs are tangible metrics that allow you to gauge progress and determine whether you’re moving closer to your goals and objectives. They offer a quantifiable means to evaluate success.
Action plans serve as blueprints, guiding the steps and resources needed to achieve a specific goal.
They come in various formats, tailored to different scenarios and objectives. Here, we present a range of action plan examples that cater to diverse purposes and situations.
From business strategies to simple task lists, these examples illustrate the versatility and importance of well-structured planning.
Business action plan example
A business action plan is essentially a strategy roadmap, meticulously tailored for realizing broader business objectives. By crafting a solid action plan, businesses can channel their resources, manpower and strategies in a direction that harmonizes with their larger vision.

Key to this plan is the identification and alignment of steps that resonate with the company’s comprehensive strategy, ambitions of growth and aspirations for operational enhancements.
While this might entail a myriad of specific steps based on unique business goals, some common elements include setting clear key performance indicators (KPIs), undertaking a thorough SWOT (Strengths, Weaknesses, Opportunities, Threats) analysis to grasp the current business landscape and establishing a timeline to keep track of progress.

Furthermore, allocating responsibilities to team members or individuals ensures that every aspect of the strategy has a dedicated focus. Budgeting, essential to the success of the action plan, ensures that every initiative is financially viable and sustainable.

Regular reviews and iterations based on feedback and changing market dynamics keep the action plan agile and relevant.
Related: 5 Steps to Create an Actionable Employee Development Plan [with Templates & Examples]
Company action plan example
A comprehensive company action plan serves as the strategic linchpin, ensuring a coherent and coordinated approach to realizing organizational goals. Central to this plan is the incorporation of rigorous market research and analysis, which provides insights into consumer behaviors, market trends and potential opportunities.

Equally vital is the focus on product development and procurement, ensuring that the offerings align with market demands and stand out in terms of quality and relevance.
Alongside, adept legal and financial management safeguards the company’s interests, ensuring compliance with regulations and prudent fiscal oversight.

Moreover, the essence of any successful company action plan lies in its sales and marketing strategies. These define how the products or services are positioned and promoted in the market, ensuring visibility and engagement with the target audience.

However, while acquisition is crucial, retention plays an equally significant role. Hence, impeccable customer service and nurturing relationships become indispensable components, fostering loyalty and ensuring that clients remain ambassadors for the brand long after the initial transaction.
Related: 30+ Project Plan Examples to Visualize Your Strategy (2023)
Sales action plan example
A well-structured sales action plan serves as the backbone for systematic and efficient progress. Central to this plan is the identification and utilization of the most effective sales channels, whether they are direct, online or through third-party avenues.

Clarity on the products and services on offer, combined with their unique selling propositions, facilitates tailored and resonant sales pitches.
Budget considerations ensure that resources are judiciously allocated, balancing the act between expenditures and potential returns. This financial prudence is complemented by setting realistic sales projections, which act as both a motivational target and a yardstick for success.
Timelines, or proposed deadlines, infuse the process with a sense of urgency, ensuring that the momentum of the sales drive is maintained.

However, the true measure of the action plan’s efficacy lies in its key performance indicators (KPIs). These metrics, be it lead conversion rates or customer retention figures, serve as tangible markers, highlighting the plan’s strengths and signaling areas that might require recalibration to increase sales.

Corrective action plan example
The essence of a corrective action plan lies in its meticulous structure, tailored to address and rectify deviations or inefficiencies identified within an organization. At its core, each action item serves as a focal point, detailing specific areas or processes that require intervention.

Accompanying each action item is a clear description that provides a comprehensive understanding of the issue at hand.
However, merely identifying a problem isn’t enough; delving deep into its origins through root cause analysis ensures that solutions target the fundamental issues, rather than just addressing superficial symptoms.

This analysis then paves the way for defining the corrective action, a tangible step or series of steps designed to mitigate the identified problem and prevent its recurrence.
Besides, to ensure the plan’s effectiveness, assigning a responsible person to each action item is paramount. This individual or team is entrusted with the task’s execution, ensuring accountability and focus.

The status of each action keeps stakeholders informed about the progress, be it in the planning phase, ongoing, or completed.
Lastly, setting a due date for each corrective action introduces a sense of urgency and purpose, ensuring that issues are addressed in a timely manner, minimizing disruptions and maximizing operational efficiency.
Simple action plan example
A simple action plan strips away the layers of complexity, offering a concise and direct approach to achieving a goal or addressing an issue. This type of plan is characterized by its straightforward structure, devoid of extraneous details, yet powerfully effective in its clarity.
It is specifically designed for tasks or objectives that don’t necessitate elaborate strategies or multi-layered approaches.

The core components of a simple action plan usually include a clear statement of the task or objective at hand, followed by a sequence of actions or steps to be taken.
Each step is described succinctly, ensuring that anyone involved has a clear understanding of what is expected. Responsibilities are defined clearly, with each task allocated to an individual or a team, ensuring accountability. Timelines might be integrated, providing a clear framework for completion, even if they’re just broad milestones.

Regular check-ins or assessments, although minimal, might be incorporated to monitor progress.
The beauty of a simple action plan lies in its agility and adaptability, making it particularly suited for individual projects, short-term tasks or situations where a rapid response is required.

How to write an action plan?
Creating an effective action plan is a foundational step towards turning aspirations into tangible results. It provides a clear roadmap, ensuring that each step taken aligns with the overall objective.
Whether you’re aiming to enhance a business process or achieve a personal goal, a well-drafted action plan can be your guiding light. Here’s key steps on how you can craft one:
- Step 1: Establish SMART goals: Initiating with a goal that is specific, measurable, achievable, relevant and time-bound ensures you have a clear and focused endpoint in sight. Smart goals serves as the cornerstone for your entire strategic blueprint.
- Step 2: Determine necessary tasks: Decompose your overarching objective into smaller, actionable tasks. This modular approach not only makes the mission less daunting but also provides a sequential pathway to goal attainment.
- Step 3: Assign essential resources: Depending on the tasks at hand, designate necessary resources, be they human, financial or technological. This ensures that every activity has the backing it needs for successful execution.
- Step 4: Prioritize tasks by importance: Not all tasks hold equal weight. Determine the hierarchy of tasks based on their impact on the goal and their time sensitivity. This allows for a systematic progression.
- Step 5: Outline timelines and key markers: With tasks in hand, set clear deadlines for each. Introduce milestones, which act as periodic check-ins, ensuring you’re on track and allowing for celebrations of smaller victories.
- Step 6: Oversee and modify your strategy blueprint: As you progress, there will invariably be learnings and challenges. Regularly review your plan to make necessary adjustments, ensuring its relevance and effectiveness.
- Step 7: Consider ready-to-use templates: If starting from scratch feels overwhelming, lean on structured templates to guide your planning. There’s plenty of business plan softwares and platforms such as Venngage that offer a plethora of action plan templates , tailored to various needs, which can significantly streamline the process.
An action plan is more than just an action steps, it’s a strategic blueprint that bridges the gap between aspirations and realizations.
Through this comprehensive guide, I’ve walked you through the purpose, ideal timings, core components, and practical examples of action plans across various domains.
Leveraging tools of project management , you can track progress, assign tasks and ensure every team member stays on the same page.
It’s not just about setting goals, but about strategically planning every step, ensuring tasks completed align with the larger project goals.
Remember, success isn’t just about having goals but about charting the right course to achieve them
And if you’re looking to supercharge your planning efforts, don’t miss out on the Venngage business plan maker.
Dive into their extensive collection of action plan templates and make your strategic planning both efficient and effective.
Discover popular designs

Infographic maker
Brochure maker
White paper online

Newsletter creator

Flyer maker
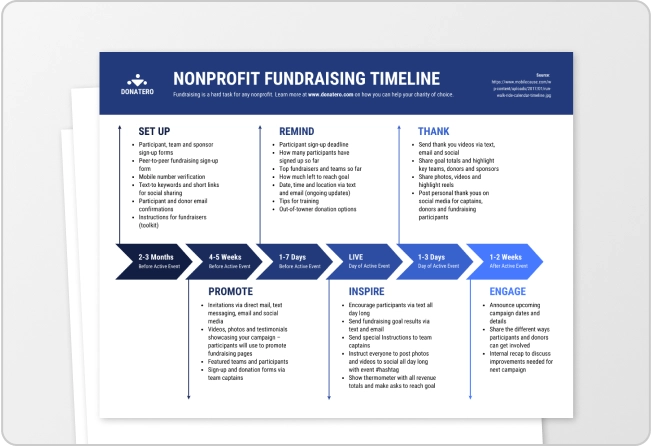
Timeline maker
Letterhead maker
Mind map maker

Ebook maker
- → What is Bibliography?
- → BSA Leadership
- → BSA Committees & Service
- → Strategic Pillars
- → Equity Action Plan
- → Land Acknowledgment
- → The 2023 BSA Annual Report
- → Contact
- → Membership: Info & Dues
- → Membership Benefits
- → Member Login
- → BSA Fellowships
- → New Scholars Program
- → Publication Prizes
- → Previous Recipients
- → Calendar
- → The BSA Annual Meeting
- → Bibliography Week
- → Funding for Bibliographical Events
- → Events Code of Conduct
- → PBSA
- → Books on Bibliography
- → Ways to Give: Stock, QCD, & More
- → Planned Giving
Examine the lives of texts.
We find out what books are made of and why.
As a field of inquiry, bibliography understands texts as artifacts – like books, manuscripts, fragments, tactile texts, image-based texts, digital texts, and more – that reflect the people and cultures that created, acquired, and exchanged them.
The BSA is a membership organization, open to all. Our members study, learn, and share knowledge derived from the close physical analysis of material artifacts in interdisciplinary and interprofessional settings: in libraries, universities, museums, the book trade, and as collectors. Bibliographers study the media and technologies that carry texts to readers, focusing on the relationship between form and content. Why does this text look the way that it does?
Isn’t bibliography about lists of books?
Yes, and so much more ! There are several different approaches to bibliography: enumerative (lists!), descriptive , historical, analytical , and critical . The BSA values all of them. Our programs, and especially our journal, The Papers of the Bibliographical Society of America ( PBSA ), focus mostly on historical, analytical, critical, and descriptive bibliography.

Trinity College, Cambridge MS R.7.15 fol. Ii.r. John Bale’s additions to John Leland’s De Viris Illustribus. Licensed under CC BY 4.0
The Bibliographical Society of America is an international, interdisciplinary scholarly organization that fosters the study of books and other textual artifacts in traditional and emerging formats. BSA pursues this mission by hosting public programs, funding scholarly research, conferring awards, issuing publications, and collaborating with related organizations. The Society is committed to adopting policies and procedures that support and promote equity and inclusion in all of our programs, and to providing equal access to our events and electronic resources to people with disabilities and other access needs.
What the BSA does
Fellowships foster cutting-edge research with grants of $3,000 and up.
Book Prizes recognize achievements in recent bibliographical scholarship.
Events all year, including our annual meeting, bring bibliographers together to learn and build community.
Peer-reviewed scholarship makes the latest research accessible to readers around the world.

Interior view of Printing Department, Eastern Tennessee Industrial School, 1903. Courtesy of the New York Public Library.
We are committed to the field of bibliography as a critical interpretive framework for understanding books and other textual artifacts and to bibliography’s enduring relevance to textual analysis.
We value the study of bibliography and the integration of bibliographical knowledge in a variety of academic, professional, and public settings.
We pursue collaborative, interdisciplinary relationships with cognate professional, scholarly, and bibliophilic organizations.
The Bibliographical Society of America seeks to build a community that embraces academic and non-academic constituencies, students, junior scholars, senior researchers, and all those interested in material texts. All are welcome as members of the Society, on its council, committees, and working groups, and as beneficiaries of or participants in its varied programs regardless of (in alphabetical order) ability, age, citizenship status, ethnicity, gender, gender expression and identity, income level, nationality, physical appearance, race, religion, sexual orientation, or technical experience.

Pactolus Prime: Bookplate. (Bookplate of Arthur A. Schomburg). Image courtesy of the Schomburg Center for Research in Black Culture, New York Public Library.

Students working in the old Memorial Hall Library. Courtesy Colby College Archives.
Governance, bylaws, & strategic pillars
The BSA is a 501(c)(30 non-profit organization (Tax ID: 13-1632509). The Society is governed by a board (the “Council”) and committees oversee many aspects of BSA’s programs. Members can shape the organization’s direction and activities by getting involved in one or both.
In 2023, the Council developed a set of strategic pillars designed to guide leaders. Drawing on the Society’s mission and values, the strategic pillars orient the BSA toward programmatic initiatives that highlight the organization’s role as a connector, cultivator, and catalyst in the field of bibliography.
Equity Action Plan
The BSA’s Equity Action Plan (EAP) is intended to address long-term issues of inequality within our Society. The council and officers of the BSA voted unanimously on 31 October 2020 to approve the EAP. Since then, the Society has issued quarterly reports on work toward achieving goals set in the EAP in the Society Information section of our journal, The Papers of the Bibliographical Society of America .
We use cookies to understand site usage. For more information, please read our Privacy Policy and Terms of Use .
Accept All Reject All
Cookies on GOV.UK
We use some essential cookies to make this website work.
We’d like to set additional cookies to understand how you use GOV.UK, remember your settings and improve government services.
We also use cookies set by other sites to help us deliver content from their services.
You have accepted additional cookies. You can change your cookie settings at any time.
You have rejected additional cookies. You can change your cookie settings at any time.
- Health and social care
- Public health
- Health protection
- Antimicrobial resistance (AMR)
- UK 5-year action plan for antimicrobial resistance 2024 to 2029
- Department for Environment Food & Rural Affairs
- Department of Agriculture, Environment and Rural Affairs (Northern Ireland)
- Department of Health (Northern Ireland)
- Department of Health & Social Care
- Scottish Government
- Welsh Government
Confronting antimicrobial resistance 2024 to 2029
Updated 8 May 2024

© Crown copyright 2024
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: [email protected] .
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/uk-5-year-action-plan-for-antimicrobial-resistance-2024-to-2029/confronting-antimicrobial-resistance-2024-to-2029
Executive summary
Antimicrobials are the cornerstone of modern medicine that treat millions of people worldwide. They are used in the treatment of minor and potentially life-threatening infections in humans and animals. They are used in support of surgery and modern cancer therapies. Organisms that become resistant to antimicrobials mean that treatments are less effective, causing harm to humans and animals. Resistant organisms spread through people, animals, food and the environment, creating a major public health threat.
In 2019 the UK published its 20-year vision for antimicrobial resistance ( AMR ). This set the ambitious goal of ensuring AMR will be controlled and contained by 2040. To deliver on this vision, the government committed to producing a series of 5-year national action plans. These will provide sustained and ongoing progress towards achieving the vision’s ambitions for change.
The first 5-year national action plan for antimicrobial resistance , ‘Tackling antimicrobial resistance 2019 to 2024’, was an important step towards achieving this vision. The work carried out across government led to progressive action towards reducing the negative impact of AMR in the UK and globally. Successes of that plan included:
- further reductions in the use of antibiotics in food-producing animals
- the development of improved surveillance systems
- the piloting of new payment schemes for antibiotics on the NHS
This national action plan ( NAP ), ‘Confronting antimicrobial resistance 2024 to 2029’, builds on the achievements and lessons of the first. It contains outcomes and commitments that will make progress towards the 20-year vision for AMR to be contained, controlled and mitigated. To confront AMR , the 2024 to 2029 national action plan has 9 strategic outcomes organised under 4 themes. Action will be taken across all sectors (human health, animal health, agriculture and the environment).
Theme 1 - Reducing the need for, and unintentional exposure to, antimicrobials
This theme has 3 outcomes:
1. Infection prevention and control and infection management - this outcome aims to reduce exposure to antimicrobials through a whole-systems approach to infection prevention and control ( IPC ), improved diagnostics and treatment in different settings (humans, animals, agriculture and the environment).
2. Public engagement and education - this aims to empower and engage the public on the risk of exposure to antimicrobials.
3. Strengthened surveillance - this aims to improve understanding of AMR through capability to measure, predict and understand how resistant microorganisms spread across and between humans, animals, agriculture and the environment.
Theme 2 - Optimising the use of antimicrobials
This theme has 2 outcomes:
4. Antimicrobial stewardship and disposal - this aims to improve the use of antimicrobials to preserve future effectiveness.
5. AMR workforce - this aims to raise awareness with the workforce in human health, animal health and agriculture to improve the optimal use of antimicrobials.
Theme 3 - Investing in innovation, supply and access
6. Innovation and influence - this calls on the life sciences sector to prioritise the development of new approaches to diagnose and treat infections, the development of vaccines to prevent infections as well as the development new antimicrobials.
7. Using information for action - this aims to enable decisions to be based on robust surveillance, scientific research and data sets to provide the best information for decision making. This section also sets out the top research priorities from policy makers.
8. Health disparities and health inequalities - this aims to improve the information available to identify where the burden of AMR is greatest. This will help to target future interventions where they will have the greatest impact.
Theme 4 - Being a good global partner
This theme has the last outcome:
9. AMR diplomacy - confronting AMR is a worldwide problem that requires global action. This outcome aims to fulfil the ambition to have sustained engagement via G7, G20 and other multilateral groups, technical networks, and bilateral relationships that will contribute to worldwide action on AMR .
The themes and outcomes of this plan will move the UK closer to achieving the vision to contain and control AMR by 2040. In taking a One Health approach across people, animals, food and the environment, this NAP aims to preserve the effectiveness of antimicrobials for future generations. The evidence gathered over the next 5 years, including through research, will help strengthen understanding of AMR as a fundamentally important issue and what works to address it.
Figure 1: summary of the 2024 to 2029 NAP
Introduction
The use of antimicrobials underpins modern medicine. Without effective antibiotics, even minor surgery and routine operations could become high-risk procedures if serious infections cannot be treated. Microorganisms which become resistant to antimicrobials, so-called ‘superbugs,’ do not respond or respond less well to available treatments. The emergence and spread of these superbugs affects:
- global public health
- animal health
- food security
- the economy
- sustainable development
The threat of AMR
Antimicrobial resistance is undermining modern medicine.
According to The King’s Fund essay What if antibiotics stopped working? , antimicrobials, particularly antibiotics, save lives and add on average 20 years to life expectancy across the globe. However, bacteria and other microbes can develop resistance to these medicines, which makes treatment much more difficult. This phenomenon, antimicrobial resistance ( AMR ), is a threat across all of medicine and undermines treatments that doctors, vets, their patients and the public have come to rely on.
Effective antimicrobials should be considered as essential infrastructure for a functioning society (see Chandler CIR, Current accounts of antimicrobial resistance: stabilisation, individualisation and antibiotics as infrastructure . Palgrave Communications 5, 53 (2019)). They are not obvious, in the way that other critical infrastructure like roads and railways are, and as such can be taken for granted. Antimicrobials underpin our treatment of infectious diseases. They protect patients with cancer, make childbirth safer, enable safe surgery and support the health and welfare of our animals, including those raised for food. As drug resistance spreads, common infections and injuries that were once easily treatable become harder, and in some cases impossible, to treat.
The rise of AMR
Drug-resistant infections arise when the microbes (including bacteria, fungi, viruses and parasites) that cause them change over time, developing the ability to resist the drugs designed to kill them. This genetic adaptation is driven by the exposure of microbes to antimicrobials in humans, animals and the environment over time. The result of this genetic adaptation is that many antimicrobial medicines - like antibiotics - are becoming less effective at treating certain infectious illnesses.
AMR is a natural phenomenon and a consequence of rapid evolution. It cannot be entirely prevented, therefore the focus is on containing, controlling and mitigating it, as set out in the UK 20-year vision for antimicrobial resistance (that by 2040 AMR is effectively contained, controlled and mitigated).
In Alexander Fleming’s 1945 Nobel Lecture , he delivered a prescient warning about the development of resistance:
It is not difficult to make microbes resistant to penicillin in the laboratory by exposing them to concentrations not sufficient to kill them, and the same thing has occasionally happened in the body.
While AMR occurs naturally, it is accelerated when microbes are exposed to antimicrobials and certain other ‘resistance-driving’ chemicals such as pesticides and heavy metals. When AMR emerges the resistance genes can spread between microbes. Resistant microbes can spread between humans, animals and through our shared environment, impacting the health of humans and animals. For that reason, AMR is a One Health issue, requiring action across sectors.
AMR affects us all
People are already dying from drug-resistant infections and unless we act now, these deaths will continue to rapidly increase. It is estimated that in 2019, 1.27 million deaths globally were caused by infections resistant to antibiotics (see the Antimicrobial Resistance Collaborators, Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis . The Lancet 399, 10325, pages 629 to 655 (2022)). Much like the coronavirus (COVID-19) pandemic, AMR affects people in all parts of the world; infectious diseases do not respect national borders. Due to the easy spread of resistance, no one is safe until we all are.
We are all at risk of infections from drug-resistant bacteria. According to the UK country briefing from the Institute for Health Metrics and Evaluation ( IHME ), there were an estimated 7,600 deaths directly from infections resistant to antibiotics in 2019, similar to the number of deaths in the UK due to stomach cancer, as well as 35,200 deaths as an indirect result of infections resistant to antibiotics.
Figure 2 below shows the impact of infection and AMR in the UK. The chart shows that in the UK in 2019 there were 87,500 deaths which involved bacterial infection and the number of deaths from other underlying causes of death in the UK in 2019 were:
- self-harm - 5,620
- breast cancer - 15,300
- Alzheimer’s disease and other dementias - 32,400
- lower respiratory infections - 41,900
- tracheal, bronchus and lung cancer - 42,800
- chronic obstructive pulmonary disease - 43,900
- stroke - 50,600
- ischemic heart disease - 93,400
This data is intended to illustrate the large burden of infection in the UK but a direct comparison cannot be made between the deaths which involved bacterial infection and the other underlying causes of death. This is because some of the deaths for non-communicable diseases (such as cancer) could have involved infection. For example, an individual whose underlying cause of death was breast cancer might have died with an infection.
Figure 2: impact of infection and AMR in the UK
Source: IHME Global Burden of Disease (GBD) Study 2019 .
People in the UK are directly affected by drug resistance every single day. AMR is already causing people to suffer longer infections which are difficult to treat. If AMR continues to spread, some infectious diseases, which in the UK would normally be simple to treat with an antibiotic, may become significant new causes of illness and death.
Case study: personal experience
The following is an excerpt taken from a digital story on YouTube told by Laila Hudson about her experience of getting an antibiotic resistant infection while undergoing treatment for bowel cancer.
A sharp pain in my abdomen tore me abruptly from my sleep. I knew immediately something was seriously wrong. This was not the first time we had rushed to the hospital in the dead of the night. Toxic chemotherapy drugs destroyed not just cancer cells but healthy cells too, giving rise to terrifying complications. My bowel had perforated, made weak from the powerful drugs that were supposed to be keeping me alive, allowing bacteria to flood into my abdomen through my blood and around my body. My immune system was fragile from the chemotherapy, meaning I’d had multiple courses of lifesaving antibiotics over the course of my cancer treatment. But this time was different, they didn’t work. My infection was resistant to treatment. Life threatening sepsis set in. My temperature soared, my blood pressure plummeted, and my heart pounded frantically in my chest as it pumped the infection through my veins. The surgeon’s face was grave. Terror gripped every atom of my being. The realisation that I might not wake up from this operation gripped me with an icy shock. I awoke in the intensive care unit. Bone chilling fevers continued to plague me. While the source of infection had been surgically removed, it would take time for the microbiologists to identify an antibiotic that would work to fully clear my infection. The doctors offered little reassurance, reminding me that my bacteria was highly resistant, that if the infection came back they might not be able to treat it. Until then, I thought it was the cancer that would kill me. Now I wondered whether a resistant infection might be a more imminent threat.
Laila’s story: the false peak
Building on the successes of the first national action plan, the core of this plan to tackle AMR is the need to protect patients, the public and the NHS. According to the Organisation for Economic Co-operation and Development ( OECD ) health policy study on Embracing a One Health framework to fight antimicrobial resistance , patients who develop resistant infections are more likely to develop complications and on average spend more time in hospital. AMR increases morbidity and mortality from infectious diseases, it places a demand on the finite resources of the health and care system, therefore impacts the whole of the NHS. Effective antimicrobials also underpin food security, animal welfare and the economy at large.
According to the above OECD health policy study, if we fail to take sufficient action, the costs associated with treating resistant infections could compare to having a COVID-19 pandemic every 5 years.
Our efforts to tackle AMR complement other efforts to improve health outcomes, as set out in the World Health Organization’s people centred approach to addressing AMR .
The UK response
Amr leadership.
AMR is a complex problem, but we can do something about it. This NAP sets out the actions that will be taken across the UK over the next 5 years to confront AMR . This NAP marks the next step towards achieving the UK’s 20-year vision of a world in which AMR is contained, controlled and mitigated.
The next 5 years represent a pivotal period in addressing the global threat of AMR . In a world recovering from the profound impact of the COVID-19 pandemic, international collaboration and preparedness for global health challenges have taken on an unprecedented importance. From 2024 to 2029, the UK is committed to playing a central role in the global effort to confront AMR by taking a comprehensive approach that leverages the UK expertise and domestic experience.
The COVID-19 pandemic underscored the critical importance of global co-operation in tackling biological threats. It showed that a co-ordinated, multilateral approach is essential to effectively respond to emerging global health crises. AMR poses a similar, or perhaps greater threat, and thus requires collaborative working with international partners to address this challenge. The interconnected nature of AMR demands collective action, as no nation or sector can address AMR in isolation.
UK progress to date
The UK was one of the first countries to establish a national action plan on AMR . Since then, extensive progress has been made in raising the profile of AMR and directing resources to tackle it. Since 2013, the UK has taken a One Health approach to tackling AMR , established with the publication of the 2013 to 2018 AMR strategy .
In January 2019, the UK published the vision for AMR to be contained and controlled by 2040. The vision recognises that a global problem as significant and complex as AMR requires long-term action, which must strengthen understanding of AMR itself and understanding of the measures that work best to control it.
To deliver the vision, the UK committed to develop a series of 5-year national action plans. The successes of the first national action plan include activity in all 9 ambitions. This NAP builds on these successes and marks the second in the series of 5-year national action plans.
The first national action plan
The first 5-year national action plan for antimicrobial resistance built a secure basis for the change required to fulfil the 20-year vision for AMR , with particular strengths in policy design, implementation, monitoring and evaluation (see Patel J and others, Measuring the global response to antimicrobial resistance, 2020 to 2021: a systematic governance analysis of 114 countries . The Lancet Infectious Diseases 23, 6, pages 706 to 718 (2023)). The first NAP took a broad approach that facilitated delivery of a wide programme of work to tackle AMR and strengthen health security in the UK and globally.
Notable achievements have included:
- reducing human exposure to antimicrobials by more than 8% since 2014 (despite the pandemic and an outbreak of group A streptococcus)
- piloting novel and innovative ways of evaluating and paying for antibiotics by the NHS
- publishing national IPC manuals in England and Wales (adapted from the Scottish IPC manual)
- publishing the Infection prevention workforce: strategic plan 2022 to 2024 in Scotland
- implementation of aseptic non-touch technique (ANTT) across healthcare services in Wales
- development of the antimicrobial data library portal to provide antimicrobial usage and resistance data for the NHS in Wales - primary and secondary care
- advocating for more action on AMR on the global stage, including through the UK’s G7 presidency where commitments to tackle AMR were secured in communiques from health ministers, finance ministers and environment ministers
- reducing the sales of highest priority critically important antibiotics ( HP-CIAs ) in food-producing animals by 81% between 2014 (3.9 tonnes) and 2022 (0.91 tonnes)
- further reducing the use of antibiotics in food-producing animals (59% reduction between 2014 and 2022)
- investing £19.2 million in One Health surveillance through the Food Standards Agency Pathogen Surveillance in Agriculture, Food and Environment Programme ( PATH-SAFE )
Lessons learnt
Evaluation of the first national action plan.
The national action plan published in 2019 was the first in a series of action plans intended to achieve the 20-year vision for AMR . To inform future policy the Department of Health and Social Care ( DHSC ) commissioned an evaluation of the first NAP , which was led by the National Institute for Health and Care Research ( NIHR ) Policy Innovation and Evaluation Research Unit ( PIRU ) at the London School of Hygiene and Tropical Medicine (LSHTM). See further detail about the evaluation and its findings on the PIRU website .
PIRU focused on aspects of the NAP where evaluation may assist with identifying opportunities for improvement of implementation of AMR policy.
In summary, PIRU ’s evaluation found that:
- there have been a variety of AMR -related policy initiatives in the UK, but without formal prioritisation
- environmental health and diagnostics are areas where there are opportunities for big policy wins to address AMR
- other countries, including Sweden, the Netherlands and Canada, have chosen different policy directions, especially in water industry regulation, antimicrobial use, stewardship and diagnostic implementation. With suitable understanding of each system’s context, the UK can learn some implementation lessons from these policy comparisons
- the UK water industry has the opportunity to play a meaningful role in addressing AMR
- the UK’s human health data systems are positively regarded internationally, but veterinary health and One Health data systems, and data linkage, lag behind
- improved data to inform AMR policy development is needed, including on appropriate prescribing, the contribution of the food chain to AMR rates, and environmental monitoring data
(The above data is also from Glover and others, ‘Evaluation of the 2019 to 2024 national action plan’, an unpublished draft report, not yet peer reviewed.)
Progress has been made in the past decade, since the publication of the UK’s 2013 to 2018 AMR strategy, and in the delivery of the 2019 to 2024 NAP . However, there are areas to tackle AMR where progress has been slow or where there is a need to apply more focus.
In some areas, slow progress has been due to a lack of evidence about ‘what works’. Some of the challenging issues affecting the delivery of healthcare can be difficult to solve (for example, a lack of evidence about the most effective interventions to reduce the incidence of Gram-negative bloodstream infections and by extension the AMR burden associated with these infections). In some areas, focus on and resources allocated to AMR have been insufficient to shift the dial, reflecting its status as an ‘ignored pandemic’. This was compounded when, from 2020 onwards, extensive effort and resource was (appropriately) diverted to the COVID-19 response. The COVID-19 pandemic has reinforced the cross-societal impacts of the spread of infectious diseases and highlighted that urgent action needs to be taken.
Due to the long-term nature of the issue, and the fact that AMR occurs across a variety of pathogens, it has proven difficult to ‘raise the alarm’ in the way seen during the COVID-19 pandemic, where a single pathogen was causing an acute threat to health security.
Lessons learnt from COVID-19
In December 2022, the UK Chief Medical Officers, government Chief Scientific Advisers, national medical directors and public health leaders authored a technical report on the COVID-19 pandemic in the UK , which includes 4 broad reflections throughout the report:
- There were multiple strands of scientific work from different disciplines needed, and these had to be integrated at considerable speed.
- The UK was relatively effective and rapid at responding in areas in which we already had strengths and substantial capacity, including in science and innovation, which could be adapted and built on.
- Science and medicine are international and pandemics by definition cross borders.
- The engagement of policy makers and the public in the scientific insights was profound and critical to the response.
In December 2021, the Academy of Medical Sciences’ FORUM, DHSC and NIHR held a workshop on lessons for AMR that could be learned from the response to the COVID-19 pandemic (see the report from the Academy of Medical Sciences, Antimicrobial resistance research: learning lessons from the COVID-19 pandemic ). Figure 3 shows some notable themes from the discussion. These themes are:
- repurposing of COVID-19 testing infrastructure
- engagement with industry
- regulatory pathways
- technical innovations and public adoptions
- end to end focus with multi-stakeholder engagement
- innovations in regulatory practice
- analysis of real-world and pragmatic trial data
- innovations in vaccine technology
Figure 3: notable themes from the learning lessons from the COVID-19 pandemic workshop
Like COVID-19, AMR is a public health challenge that requires urgent action and could, in time, have an impact far in excess of that of COVID-19. The unprecedented response to COVID-19 - including international focus, political commitment and public engagement - can and should be learnt from to tackle AMR .
About this national action plan
Underlying principles.
In developing this NAP , consideration has been given to the need to take a collaborative approach across the UK, maintain our One Health response, be a good global partner, reduce inequalities and maintain resilience. These principles are explained in the following pages.
Taking a collaborative approach across the UK
Co-ordinated action between England, Northern Ireland, Scotland and Wales, and across sectors is necessary to tackle AMR . Working together is prioritised because:
- there is a shared vision to contain and control AMR
- pathogens do not respect borders
- there are similar challenges in each part of the UK, and opportunities to learn from one another
Collaboration is facilitated through formal mechanisms such as the Common Framework on Health Protection and Health Security as well as through AMR -specific structures.
Taking a One Health approach
According to the World Health Organization ( WHO ), One Health is an integrated, unifying approach that aims to sustainably balance and optimise the health of humans, animals, plants and ecosystems. It recognises the close links between the health of humans, domestic and wild animals, plants and the wider environment (including ecosystems).
The approach mobilises multiple sectors, disciplines and communities at varying levels of society to work together to foster wellbeing and tackle threats to health and ecosystems, while addressing the collective need for clean water, energy and air, safe and nutritious food, taking action on climate change and contributing to sustainable development.
Drug-resistant microbes can be found in people, animals, food and in the environment. Through contact with other people, animals and the environment, these microbes and resistance mechanisms can be transferred between and among different species, affecting the health of people and animals, including companion animals, food-producing animals, and wildlife. It is vital to take an approach which recognises this interconnectivity. According to the UN Environment Programme ( UNEP ), a One Health approach means working collaboratively and inclusively across sectors to improve outcomes for humans, animals and the environment.
In this NAP , when referring to working across ‘all sectors’, this includes human health and social care, animal health, agriculture, food production and the environment. Unless otherwise specified, activity in this document should be assumed to cut across several or all of these sectors.
Figure 4 illustrates the interactions which allow for the spread of resistance, demonstrating the need for a One Health approach to AMR . These interactions are between:
- humans (including in hospitals and GPs , care homes and the community)
- animals (including food animals, companion animals and wildlife)
- the environment (including water, crops and land)
It shows that the spread of resistance is facilitated through direct contact between:
- humans and the environment
- humans and animals
- animals and the environment
It also shows that resistance can spread through food when:
- food animals are eaten by humans
- food animals are eaten by companion animals
- crops are eaten by humans
- crops are eaten by animals
It also shows that resistance can spread through waste when:
- human waste is released into the environment
- animal waste is released into the environment
Figure 4: the need for a One Health approach to AMR
Being a good global partner
The UK has an established history as an international leader in tackling AMR . The UK is dedicated to working with partners across the globe to ensure the efficacy of antimicrobials now and for generations to come by drawing on UK expertise, including in the life sciences sector, and the sharing of best practice to strengthen global capacity to tackle AMR . Actions to reduce AMR also tie in with other health and development goals, including the sustainable development goals ( SDGs ).
The UK will continue to work with international partners to galvanise global action on AMR , particularly through groups such as the G7 and G20 and with multilateral organisations including UN organisations. Further information on our global commitments over the next 5 years can be found in the ‘Outcome 9 - AMR diplomacy’ section.
The UK recognises the importance of working with, and building capacity in, low and middle income countries ( LMICs ) to tackle AMR . Through UK aid investments, the UK will continue to assist countries in implementing effective strategies to address AMR within their health and care, agricultural and environmental sectors. This aligns with the global commitment to equity and ensuring that all nations have the tools and resources necessary to tackle AMR . Our investments will include supporting early-stage priority research and innovation in underfunded areas via the Global AMR Innovation Fund ( GAMRIF ) and strengthening surveillance systems through the Fleming Fund.
Reducing inequalities
AMR impacts groups differently and the interventions required to meaningfully tackle AMR must therefore be tailored to different groups, settings and circumstances. Efforts to tackle health disparities and health inequalities are recognised for the first time in this NAP , with a specific outcome (outcome 8) focused on better understanding and addressing disparities in tackling AMR .
Just as AMR affects different groups within the UK differently, so too are its impacts unequally spread globally. There are patients in many parts of the world who cannot access the antibiotics and other antimicrobials they need. According to the Access to Medicine Foundation’s 2021 antimicrobial resistance benchmark , 5.7 million people die annually from treatable infections because of this lack of access to medicines. This is sometimes described as an access or excess trade-off. Lack of access to appropriate antimicrobials and fragile supply chains force the use of suboptimal treatments, giving pathogens further opportunities to develop resistance and thereby stoking the rise of resistant infections. Improving access to treatments, as well as strengthening IPC programmes, will save lives and prevent resistance arising and spreading.
The UK will continue to invest in tackling AMR where it is most impactful and ensure that our actions to address AMR to reduce the burden for the people who are more affected.
Resilience to a changing threat landscape
AMR is recognised as a key biological risk in the 2023 UK Biological Security Strategy ( BSS ). The BSS sets out the vision that by 2030, the UK is resilient to a spectrum of biological threats, including AMR . AMR is also captured as a chronic risk in the UK National Risk Register . The UK government’s wider Resilience Framework sets out an approach to strengthen the systems that provide resilience to risk, by focusing on a shared understanding of risks, preparation and prevention, and a whole of society approach.
AMR and pandemic preparedness are interconnected challenges that require a holistic approach at the local, national and international level. For example, the public health impacts of a pandemic might be worsened without access to effective antibiotics. Conversely, AMR might be accelerated if antibiotics are used indiscriminately to tackle a pathogen that is not well characterised. Efforts to tackle AMR , including the responsible use of antimicrobials and implementing effective IPC measures, as well as learning from COVID-19, will strengthen preparedness for the next pandemic. Tackling AMR should be integrated into efforts to prepare for future pandemics, including embedding a One Health approach in development of any WHO instrument on pandemic preparedness.
Climate change is widespread, rapid and intensifying. Many infectious diseases are climate sensitive, and climate change and AMR are linked emergencies. They are both One Health, global issues with the highest burden falling on LMICs .
Case study: AMR and climate change
There is evidence that climate change might worsen the impacts of AMR . The climate is an important driver of patterns of infections, year-to-year variations in incidence (including epidemics) and longer-term shifts in populations at risk.
Rising temperatures, water shortages, extreme weather and loss of biodiversity resulting from climate change might all change the dynamics of the spread of infections and our ability to prevent them.
The mitigation of both climate change and AMR requires:
- capacity building for local mitigation and adaption
- generation and dissemination of data
- public-private partnerships for new technologies and practices
- implementation research
- increased institutional commitment and co-ordination, and alignment of strategies
Development and delivery process
This 5-year NAP , outlined in the following chapters, builds on the UK response to date and the lessons learnt from evaluation of the first NAP , experiences during the COVID-19 pandemic and best practice from international leaders. Further information on the development process and the theory of change can be found in ‘Appendix A: NAP development’.
To confront AMR this NAP has 9 strategic outcomes, underpinned by 30 commitments that set out the activity that government organisations will undertake to achieve the outcomes. The outcomes and commitments were informed by extensive stakeholder engagement. Each of the commitments starts ‘we will’ - ‘we’ refers to government organisations (including departments and arm’s length bodies) and the NHS in England, Scotland, Wales and Northern Ireland.
AMR is a broad issue, encompassing resistance developed by a wide range of microorganisms, including bacteria, viruses, parasites and fungi. In line with the Interagency Coordination Group on Antimicrobial Resistance ( IACG ) framework for action, this NAP incorporates action to address resistance in all of these pathogenic domains. The focus will be on resistance to antibacterials (antibiotics), which poses the greatest, immediate risk to public health.
In addition to government activity, the active participation of public and private sector bodies across the human health, animal health and environment communities will be required to achieve the 9 outcomes. The support of the public as patients, consumers, animal owners and investors will also be important in achieving the outcomes.
The following chapters take each of the 9 strategic outcomes in turn, outlining the commitments underpinning each outcome and the rationale for each of them. Progress in delivering the national action plan will be determined based on the delivery of these commitments.
Outcome 1 - Infection prevention and control and infection management
By 2029, the UK takes a whole-systems approach to IPC and infection management in all sectors by reducing unnecessary exposure to antimicrobials and preventing infections, including identification, assessment, diagnosis and treatment of infections in an integrated way across different settings.
This outcome has:
- informed interventions
- the built environment
- waste minimisation and effective waste management
- target 1a: by 2029, we aim to prevent any increase in a specified set of drug-resistant infections in humans from the 2019 to 2020 financial year baseline
- target 1b: by 2029, we aim to prevent any increase in Gram-negative bloodstream infections in humans from the 2019 to 2020 financial year baseline
Tackling AMR requires a focus on preventing infection in humans and animals, therefore IPC is a core element of this NAP . Reducing the burden of infection in the human population by optimising IPC measures also improves patient safety. Prevention and control of infection in humans and animals means less use of antimicrobials and thus lower risk of resistance developing and reduced onward spread. When infection has not been prevented and needs treatment, ensuring the right antimicrobial is prescribed (and taken as prescribed) is crucial to minimising risk of resistance.
Bacteria and other organisms know no borders, as the COVID-19 pandemic demonstrated. Action to reduce infection burden to reduce risk of AMR must take place in both national and international contexts, aligning with organisations and plans such as the WHO EURO Roadmap 2023 to 2030 .
As also demonstrated during the COVID-19 pandemic, one of the main measures by which infections can be reduced both in number and severity is through vaccines. Vaccines can reduce the need for antimicrobial treatment and therefore minimise the selection pressures which cause antimicrobial-resistant strains to emerge. As vaccines not only protect the individual person or animal who has been immunised, but the whole community of which they are part, ensuring good and equitable immunisation rates within the UK, as well as working with international partners to improve coverage worldwide, is a fundamental part of our efforts to reduce AMR .
In the UK, there has been work over many years in animal agriculture to reduce endemic disease, with vaccination programmes playing a vital role in disease control. Initiatives such as the Department for the Environment and Rural Affairs’ ( Defra ) Animal Health and Welfare Pathway, support continual improvement by collaborating with farmers, vets, industry and the supply chain to deliver benefits for animal health and welfare, farm productivity, food security, trade and the environment.
Commitment 1.1 - Informed interventions
We will continue to improve IPC and biosecurity practices that are informed by the latest evidence base and social sciences to minimise the potential for infection transmission, including outbreaks, optimise the management of infections and reduce the need for antimicrobial exposure.
Applies to people and animals.
IPC is a practical, evidence-based approach to prevent harm from otherwise avoidable infections. It includes a variety of different measures, from handwashing to design and build of environments. IPC interventions must be informed by research and evidence, including surveillance, to inform tailored action against specific patterns of infection and resistance, ensuring efforts are maximised and have the highest impact. There is variation in the infections responsible for the biggest burden of disease in different parts of the UK, and IPC measures can and should be tailored to respond to the different contexts. In addition to ongoing monitoring, the UK Health Security Agency ( UKHSA ), National Services Scotland, Public Health Wales and the Public Health Agency (Northern Ireland) each publish surveillance reports which help identify trends and any areas of concern, which can then be addressed in the local context:
- English surveillance programme for antimicrobial utilisation and resistance ( ESPAUR ) report
- Scottish One Health antimicrobial use and antimicrobial resistance in 2021
- Welsh antimicrobial resistance and prescribing surveillance and reports
- surveillance of antimicrobial use and resistance in Northern Ireland, annual reports
For human populations, the health system can influence the emergence and spread of AMR through reliably applying measures to prevent and control infection and, when infection occurs, responding and managing these with evidence-based care pathways that support the appropriate (and timely) usage of antimicrobials in every day clinical care.
In veterinary and farm settings, ‘biosecurity’ is used to describe the application of IPC principles. Biosecurity focuses on measures which reduce the risk of disease entering and spreading in settings such as farms or veterinary practices. Good hygiene and husbandry practices are also required to mitigate the risk of disease spreading from animals to their keepers.
Research, evaluation and analysis of current practices, environmental factors, and human behavioural factors can inform which IPC interventions work best and where further work is needed, in human and animal healthcare, community, social care and farm settings. A good programme of informed interventions involves training of medical and veterinary healthcare professionals, as well as education of patients and animal keepers.
Commitment 1.2 - The built environment
We will prioritise IPC , the management of infections and biosecurity in the built environment, ensuring an understanding of AMR is integrated into health and social care estate design, veterinary practices and farm settings.
Applies to people, animals and the environment.
It is important that the design of health and care facilities, veterinary facilities, farm buildings and abattoirs facilitates good IPC practices and that the quality and design of finishes and fittings enable thorough access, cleaning and maintenance to take place.
For the human population, the healthcare environment can be a reservoir for organisms with the potential for infecting patients. For healthcare associated infections ( HCAIs ) to be reduced, it is imperative that IPC measures are ‘designed-in’ at the outset of the planning and design stages of a healthcare facility and that input continues up to, into and beyond the final building stage.
Designed-in IPC for healthcare facilities means that designers, architects, engineers, facilities managers and planners work with IPC teams, other healthcare staff, patients and visitors to deliver facilities in which IPC needs have been anticipated, planned for and met. Similarly, when older facilities are renovated or rebuilt, there is the opportunity to implement modern IPC measures and improve design.
These design considerations are also essential for veterinary facilities, where HCAIs , including MRSA , have been documented (see Weese JS and van Duijkeren E, Methicillin-resistant Staphylococcus aureus and Staphylococcus pseudintermedius in veterinary medicine . Veterinary Microbiology, 27, 140, pages 418 to 429 (2010)). Evidence-based IPC programmes should be implemented in every veterinary practice, hospital and small clinic to protect the health of animals, owners, and vet professionals.
In farm settings, careful consideration is needed to ensure the farm environment enables good husbandry, biosecurity and biocontainment measures to take place. Considerations such as the location of the farm relative to the community, structure and layout of the farm and procedural biosecurity should be included in farm development and/or design.
Commitment 1.3 - Waste minimisation and effective waste management
We will implement effective waste management, wastewater treatment methods and agrochemical stewardship to minimise dissemination of AMR and AMR -driving chemicals into the environment.
Applies to the environment and plants.
Addressing AMR in the environment is essential to reducing preventable, unintentional exposure to antimicrobials and to slowing the emergence and dissemination of resistance. The UNEP 2023 report, Bracing for superbugs: strengthening environmental action in the One Health response to antimicrobial resistance outlines 3 notable environmental dimensions of AMR :
- development of AMR in the environment: antimicrobials affect microbes in the environment just as they do in the body. These environmental microbes can develop resistance if they are exposed to antimicrobials, or other AMR -driving chemicals
- AMR and the triple planetary crisis: AMR shares drivers with the main environmental issues of this century - climate change, biodiversity loss and pollution and waste
- AMR transmission and spread in the environment: AMR can spread between humans, animals and the environment by a variety of pathways, including recreational use of bathing waters (such as swimming or surfing) and consumption of food or untreated water
Poor waste management and water treatment can lead to the transmission of drug resistant microbes from humans, animals and plants into the shared environment. In order to reduce AMR spread into the environment, stewardship initiatives to reduce pollution from hospital and community wastewater, agricultural activities and antimicrobial manufacturing need to be developed and implemented.
Attention is increasingly turning to water quality and the relationship between the environment and public health, and the environment and animal health. The PIRU evaluation of the first NAP found that co-ordination across the governments of the UK and with the academic community and the water industry could be improved.
Several initiatives across the UK are in place to ensure that citizens know that the water from their taps is safe to drink and that their sewage waste is properly managed and treated. This includes regulation of water companies and monitoring of waterways, and so regulators and water companies will play a vital role in this area. While these interventions are not all specific to AMR , they will help mitigate resistance.
Examples of recent interventions that have been developed or implemented include:
- setting new legally binding targets to significantly reduce pollution from farming, wastewater and abandoned metal mines (England)
- increasing monitoring of storm overflows from only 10% in 2015, to over 90% (England)
- establishing the Antibiotics and Pharmaceuticals Monitoring Programme to identify sources of AMR driving chemicals in the environment (Northern Ireland)
- testing for antibiotic resistance in bacteria at bathing water sites and producing a publicly accessible visualisation tool to present the data (Scotland)
- researching AMR genes and AMR driving chemicals in wastewater and sludge at different types of wastewater treatment plants through the UK Chemical Investigations Programme (England)
- development of pilot AMR surveillance in river catchments through PATH-SAFE
Initiatives to support responsible agrochemical stewardship will also mitigate AMR . Pesticides, including fungicides, play an important role in supporting crop production and food supply. However, antifungal resistance in humans, which is in part driven by the use of fungicides, is increasing globally (see Fisher and MC and Denning DW, The WHO fungal priority pathogens list as a game-changer . Nature Reviews Microbiology, 21, pages 211 to 212 (2023)) and in the UK. Fungicides must be used responsibly to reduce potential risk to public, environmental, or animal health. Antifungal resistance is being driven by antifungal use in crop protection products and fungal spores can be transmitted as airborne particles.
We are committed to minimising the risks and impacts of pesticides to human health and the environment, while ensuring pests and pesticide resistance are managed effectively, including through the uptake of integrated pest management and sustainable crop protection, in line with Defra ’s 25 year environment plan, the Welsh Minister’s natural resources policy, the environment strategy for Scotland, and the goals of the environment strategy for Northern Ireland to protect and enhance the environment for future generations.
Outcome 2 - Public engagement and education
By 2029, the public are empowered and equipped to engage on and help address AMR through an improved understanding of the scale and nature of the risk, and the individual behavioural actions that can be taken to address it.
- public awareness and campaigns
- use of educational settings
- engagement guide
- human health target 2a (see appendix B): by 2029, we aim to increase UK public and healthcare professionals’ knowledge on AMR by 10%, using 2018 and 2019 baselines, respectively
A collaborative approach is needed to solve AMR , with action taken by governments being only one part of the solution. Action is also required from professionals and professional bodies, patients or service users, the public, consumers and animal owners, the private sector and investors, and the research community and academia. Many people fall into more than one of these groups - a farmer or pharmacist could also be a pet owner and will almost certainly be a patient at some point. Collaborations across sectors will aid the development of targeted strategies, engage the public, and promote sustained behaviour change to effectively prevent AMR .
Stakeholders overwhelmingly called for action to increase public awareness in the call for evidence on AMR . Public engagement is only one component of tackling AMR , which can be influenced at personal and societal levels (see Smith E and Buchan S, Skewed perception of personal behaviour as a contributor to antibiotic resistance and underestimation of the risks . PLOS ONE, 18, 11 (2023)). Efforts on public engagement will be focused on that which is evidence-based and as effective as possible.
Case study: Fleming Centre
The UK government is investing £5 million of seed funding into the Imperial College London and Imperial Healthcare NHS Trust’s Fleming Initiative. This will make a major contribution to the UK’s vision to contain, control and mitigate AMR , by co-locating diverse expertise and centralising the role of civil society in addressing the crisis. It aims to deliver:
- world class laboratory, clinical and behavioural research to develop, incubate and test innovations against AMR
- a unique space to engage and involve the public in the past, present and future of AMR research, enabling the development of solutions with buy-in from all
- evidence-led advocacy, convening power and policy work to drive impact
- a global network to tackle AMR , by linking with other centres around the world
The centre, a physical space, is intended to open in 2028, the centenary of Alexander Fleming’s discovery of penicillin, on the St Mary’s Hospital site, in Paddington, where he made the discovery.
Commitment 2.1 - Public awareness and campaigns
We will launch and evaluate evidence-based campaigns to raise public awareness and understanding of IPC , infection management, antimicrobial stewardship and AMR , informed by surveys of public attitudes and adjusting content and approach to empower the public and effect sustainable behaviour change.
The threat of AMR can be mitigated, but only with participation from all aspects of society. The evidence base will be developed in order to tailor responses, harness the power of the public, and elicit sustained behaviour change on AMR .
To inform what action is required to engage the public, and effect sustainable behaviour change, understanding of the current public attitude and awareness of issues relating to AMR is required. This will enable targeted activity that can measure the impact of future awareness-raising activity. The call for evidence on AMR found that there is insufficient public awareness of AMR (95% of respondents), with campaigns commonly suggested as a route to increase awareness.
During the COVID-19 pandemic, the public made a meaningful contribution to reducing the spread of infection - see Antimicrobial resistance research: learning lessons from the COVID-19 pandemic from The Academy of Medical Sciences. Self-care can be a powerful tool to empower patients. It should, however, be noted that the PIRU evaluation of the first NAP cautioned against pushing self-care without protecting access to formal health services. The response to AMR needs to be sensitive not just to basic biology, but crucially to human behaviour. We are committed to testing and learning from interventions that help educate and inform the public.
There is a strong track record of public health communication in the UK, but it is critical to continue to adapt to the changing media landscape, including the spread of disinformation.
Case study: Keep Antibiotics Working
The Keep Antibiotics Working ( KAW ) media campaign was a multi-channel social marketing and communications campaign developed in 2017. It focused on increasing awareness within the general public and supporting general practitioners ( GPs ) in prudent antibiotic prescribing. The campaign was subsequently adopted in Scotland, Wales and Northern Ireland.
The campaign messaging aimed to reduce patient expectation for an antibiotic prescription and support confidence of GPs to prescribe appropriately. An evaluation of the KAW campaign showed that campaign recognition increased significantly and achieved a higher level of recognition compared to previous national antibiotic awareness campaigns (see Gilham EL and others, Assessing the impact of a national social marketing campaign for antimicrobial resistance on public awareness, attitudes, and behaviour, and as a supportive tool for healthcare professionals, England, 2017 to 2019 . Eurosurveillance, 28, 47, (2023)). In addition, aspects of participant knowledge, awareness and understanding of AMR increased significantly following the campaign. KAW also supported change among GPs with those who were aware of the campaign reporting greater confidence to say no to most patients asking for antibiotics. GPs who were aware of the campaign were also more likely to explain that prescription of antibiotics for viral infections was inappropriate when asked for antibiotics by a patient.
In 2023, the KAW branding was used in Scotland to promote an ‘antibiotic amnesty’ campaign encouraging people to return unused antibiotics to the pharmacy rather than sharing or keeping antibiotics. This shows the potential for the brand to be adaptable for future campaigns, depending on need.
Commitment 2.2 - Use of educational settings
We will work with schools and educators to consider guidance and information on IPC and AMR for use in all public authority educational settings.
Applies to people.
AMR can, and will, affect us all - we will all experience infections at some point in our lives, hopefully infrequently. Every day we all make choices about infection prevention (including hand washing and food hygiene) and how we manage our own infections - many of us will look after pets, travel abroad, swim in lakes and rivers, and choose how to invest our money.
Responses to the call for evidence on AMR indicated that targeting awareness-raising programmes at school children could build future understanding and support for AMR action. If IPC , infection management and AMR can be meaningfully presented in educational settings, then children may be able to drive change in behaviours. This is especially important as some of those children will grow up to be the next generation of doctors, nurses, other healthcare workers, scientists and professionals. By ensuring that they are aware of, and have an interest in AMR , we will encourage careers in the area, and can look forward to having a workforce where reducing AMR is forefront in everyone’s mind.
AMR should not be siloed and ‘left to the experts’. We plan to empower young people on this issue, which may disproportionately affect them. We need their buy-in to ensure that there are still working antibiotics for future generations.
Case study: e-Bug
There are existing resources used in schools to support IPC efforts and respond to AMR , including e-Bug , operated by UKHSA . This health education programme aims to promote positive behaviour change among children and young people, through provision of free resources for educators, community leaders, parents and caregivers, to ensure they can contribute to preventing infection outbreaks and using antimicrobials appropriately. The resources that e-Bug provides are evidence based and grounded in behaviour change methodology.
Commitment 2.3 - Engagement guide
We will publish an engagement guide covering communications approaches for AMR , which has been co-created by and for government, civil societies and local partners, to improve public understanding of the risk, and the individual actions they can take to reduce the spread of infections.
AMR affects every aspect of society. Framing of this complex issue is essential, and there is demand for clear, consistent messaging about AMR . Different communities seek their information and health advice from a wide range of sources, including local government, community organisations and local leaders.
An engagement guide focused on AMR would provide resources for use with a variety of stakeholders, to share the most pertinent information and give people the knowledge they need to change their AMR -driving behaviours and minimise their risk of infection to keep themselves and their communities healthy. By taking a collaborative, outward looking approach, we will ensure the guide is not limited to perspectives from government organisations but accurately reflects the needs of, and is accessible to, end users.
This engagement guide will provide materials which support the delivery of the previous 2 commitments on public engagement and education.
Outcome 3 - Strengthened surveillance
By 2029, the UK will have an improved capability to measure, predict, understand and mitigate the evolution and transmission of resistant microorganisms and genes, locally, nationally and internationally and across and between human, animals, agriculture and environmental sectors.
This outcome has 2 commitments:
- optimising surveillance of infections and outbreaks, and response
- optimising surveillance to inform interventions
Surveillance is a vital tool in understanding the extent of and risks associated with AMR . It provides essential data to allow the development of effective interventions and to detect and act on outbreaks. It helps target efforts where they can make the biggest difference and provides the data to inform modelling which can be used to predict the impact of interventions, future trends and the health and economic burden from AMR . Information on infection incidence, antimicrobial usage and AMR provided through surveillance programmes also helps to better understand mechanisms of resistance and, when successfully integrated, improves understanding of the transmission routes of AMR . A central aim of robust surveillance is longevity. Longstanding surveillance programmes allow us to track trends over time, and to evaluate the impact of interventions. Extensive surveillance is undertaken in the UK already, with regular reports published by the Veterinary Medicines Directorate ( VMD ) and the public health agencies in England, Scotland, Wales and Northern Ireland.
Global surveillance databases, such as Global Database for Tracking AMR Country Self- Assessment Survey (TrACSS) , Global Antimicrobial Resistance and Use Surveillance System (GLASS) and Animal Antimicrobial Use (ANIMUSE) facilitate access to a growing set of information and enable member states to benchmark progress. Reviewing data on AMR and antibiotic use can be a motivation for behaviour change from practitioners to policy makers. Access to this information can also help to identify gaps for capacity building and investment. The UK is supportive of the global, collaborative effort to standardise AMR surveillance, in line with the WHO global action plan on AMR .
Surveillance is also a significant enabler of high-quality research into AMR .
The PIRU evaluation of the first NAP found that there had been progress made in harmonisation and integration of surveillance between sectors over the past 5 years, though some gaps remain. Suggestions for ways to strengthen the surveillance systems in the UK included (but were not limited to) extending standardised data collection to the environment, monitoring AMR in the healthy population and facilitating data-sharing agreements.
Case study: PATH-SAFE
The rapid detection, identification and tracking of pathogens has always been fundamental to public health but recent advances in DNA-based methods have massively improved our ability to do this. Modern genome sequencing enables us to identify pathogen and resistance strains rapidly and cheaply and use this to reconstruct chains of transmission and trace outbreaks to their source.
The Pathogen Surveillance in Agriculture, Food and Environment ( PATH-SAFE ) programme, a £19.2 million Shared Outcomes Fund research programme, aimed to pilot the development of a national surveillance network, using the latest DNA-sequencing technology and environmental sampling to improve the detection and tracking of foodborne human pathogens and AMR through the whole agri-food system from farm to fork.
PATH-SAFE has explored the application of advanced genomic technologies to improve control and reduce disease via routes such as:
- source tracking: working back from outbreaks in humans or findings in food to the source of the infection or contamination and thus being able to remove this or mitigate its risk and prevent future outbreaks (‘reactive control’)
- earlier detection: enabling more efficient detection of pathogens at an earlier point in the chain and thus prevent the contamination of food or outbreaks (‘proactive control’)
This pilot project has taken a collaborative One Health approach (integrating human, animal and environmental health), establishing shared technology platforms, common data standards, methodology development and data generation in an innovative and dynamic way. Data interoperability and shared best practice allows for the tracking of pathogens across government departmental boundaries of responsibility and offers major efficiencies in terms of future procurement and resource needs. Involvement of industry and academic stakeholders in the PATH-SAFE programme, alongside government organisations, has strengthened the research undertaken.
The PATH-SAFE pilots have pushed forward the evidence base for AMR in UK livestock populations, generating new representative data on AMR in ruminants, while also trialling new surveillance techniques and approaches. PATH-SAFE has demonstrated what can be achieved in the One Health space with dedicated resource for co-ordination and cross-departmental funding.
Commitment 3.1 - Optimising surveillance of infections and outbreaks, and response
We will optimise surveillance processes through effective, standardised and integrated (where possible) systems to detect, track and model infections and outbreaks or incidents, to monitor antimicrobial usage (including quality of prescribing) and susceptibility, and to facilitate cross-organisational responses to mitigate risks to patients and the public.
It is crucial to review and, when needed, improve, surveillance processes to better detect and respond to outbreaks early and effectively. Improving data sharing across organisational boundaries and ensuring standardisation of information will improve our capability to understand and respond to infections, including resistant infections.
In the human population, the NHS will aim to measure the quality (in addition to quantity) of prescribing. This will enable clinicians to take a more nuanced approach, rather than solely focusing on the number of prescriptions issued. The nature of antimicrobial prescribing is changing with increasing numbers of non-medical prescribers, greater utilisation of patient group directions in hospitals and the community, and a shift from face-to-face prescribing to virtual and online prescribing. A better understanding of who (and how) antimicrobials are prescribed to is vital.
Poor quality coding currently hampers efforts to evaluate quality of prescribing and there is room for improvement. Therefore, the work to incentivise digital coding of diagnosis (set out in commitment 4.1), lays the vital foundation for quality improvement as well as providing intelligence on the ever-shifting burden of disease and disease severity that determines clinical need for antimicrobials.
In animal health, all antibiotics must be prescribed by a veterinarian. As use of antibiotics in animals continues to reduce, surveillance will improve understanding of other drivers of AMR through humans, animals and the environment. This can only be achieved through integrated One Health surveillance where data is shared between sectors, and a collaborative approach to mitigate the spread is taken. This work was advanced by the PATH-SAFE programme, with future progress expected through the BSS National Biosurveillance Network initiative.
Case study: Zambia One Health surveillance platform
DHSC ’s Global AMR Innovation Fund ( GAMRIF ) partnered with the global health non-profit Foundation for Innovation New Diagnostics to work with the Zambia National Public Health Institute and software engineers to launch a One Health surveillance platform for AMR . This new data management system tracks and maps the emergence of resistance, in humans and animals, forming the basis of national surveillance programmes, and enables the Zambian government to make data-driven decisions. The platform ensures burden-free implementation for health workers, no new data silos and long-term sustainability. It is also open source.
Zambia had several established data sources but previously lacked a systematic approach towards the collection and analysis of this data. Furthermore, this new system made it even easier to submit AMR data to the Global Antimicrobial Surveillance System, a WHO initiative. The system improves disease surveillance beyond AMR by identifying and monitoring outbreaks and enhancing clinical care. Following the launch, the platform is now being implemented in other countries in Africa and Asia as part of DHSC ’s Fleming Fund.
Commitment 3.2 - Optimising surveillance to inform interventions
We will enhance technical capacity for surveillance across sectors (and associated analytics and modelling) to inform intervention development, evaluation and application focused on areas of greatest risk, including highest burden of AMR and (where possible) sharing information and lessons to support personnel in all sectors to reduce AMR and its consequences.
One Health integrated surveillance will be used to inform effective interventions across sectors to reduce AMR and its consequences. In order to acquire the best possible data, the aim is to enhance surveillance by utilising techniques such as whole genome sequencing ( WGS ), modelling and analytics. WGS can help improve the depth of data generated from isolates, thereby enhancing routine surveillance, outbreak detection and outbreak response.
Modern sequencing technologies will be routinely used and provide the basis for more informative genomic surveillance of AMR . These modern technologies include metagenomics and those that provide longer sequence reads and therefore more complete information on the mobile genetic elements of AMR transmission. Implementation of the latest analytical techniques for identifying genes and mutations associated with AMR in WGS data will further improve the quality and quantity of data available for surveillance.
When applied in global, national and local AMR surveillance, these tools have the potential to improve understanding to support new policies and interventions, including novel diagnostic methods to support informed antimicrobial use and vaccination strategies for better controlling AMR .
To enable efficient and extensive use of genomic AMR data, the design and implementation of data handling solutions will be explored. The design should accommodate complexities such as AMR outbreaks caused by the same AMR -causing mobile genetic element transferred among different pathogen species, or longer-term trends in AMR epidemiology. These should provide new or use existing open standards, for the handling of AMR -related information, to facilitate working with international partners and allow convenient and effective querying for surveillance and response planning. Few countries offer large scale sequencing and analysis of AMR associated isolates so UK data would provide vital insight into the molecular epidemiology of these infections and position the UK to exploit the knowledge these new methods can provide.
Outcome 4 - Antimicrobial stewardship and disposal
By 2029, the UK has strengthened antimicrobial stewardship and diagnostic stewardship by improved targeting of antimicrobials and diagnostic tools for humans, animals and plants, and improved the disposal of antimicrobials, informed by the right data, risk stratification and guidance.
- clinical decision support
- appropriate prescribing and disposal
- behavioural interventions
- target 4a: by 2029, we aim to reduce total antibiotic use in human populations by 5% from the 2019 baseline
- target 4b: by 2029, we aim to achieve 70% of total use of antibiotics from the Access category (new UK category) across the human healthcare system
While all use of antimicrobials drives AMR , there is an opportunity to reduce inappropriate use of antimicrobials occurring, for example, when antimicrobials are taken when they are not needed, or when taken for longer than necessary.
According to the National Institute for Health and Care Excellence’s NICE guideline (NG15) :
The term ‘antimicrobial stewardship’ is defined as ‘an organisational or healthcare‑system‑wide approach to promoting and monitoring judicious use of antimicrobials to preserve their future effectiveness’.
Antimicrobial stewardship ( AMS ) approaches are employed to manage the use of antimicrobials, preserve their efficacy and minimise the emergence of AMR . Stewardship activities can be undertaken by anyone and should be encouraged by everyone, not just by human and veterinary healthcare professionals but also patients, animal owners, and the public. Similar principles apply for stewardship in people and animals.
In animal health, AMS activities centre around veterinary professionals and animal keepers and the commitments relating to stewardship in animals are therefore found in the ‘Outcome 5 - AMR workforce’ section.
In farming, antifungal use in crops is an emerging issue for AMS . Antifungals and pesticides are used for the benefit of plant health and help support food security. However, they differ to antimicrobials used in human and animal health as they are not prescribed medicines and are applied directly to the environment. According to the UNEP 2023 report, Bracing for superbugs: strengthening environmental action in the One Health response to antimicrobial resistance , fungicide and bactericides use in agriculture has been increasing globally.
There are close links between humans, animals and the environment but reducing the consumption of antibiotics in animals alone will not be sufficient to reduce the burden of AMR in humans. The significant reductions in antimicrobial use in animals provides some benefit to the risk of AMR in people, primarily by reducing foodborne disease but mostly mitigates the AMR threat to animal health. According to the third UK One Health report , most antibiotics in the UK are consumed by people (two-thirds) not animals, and human use drives AMR in bacteria in humans. Stewardship interventions within other settings have a proportionally smaller impact on AMR compared than those made within healthcare settings.
Case study: GAMSAS
Developed by the British Society for Antimicrobial Chemotherapy ( BSAC ) and led by experts in antimicrobial stewardship ( AMS ), the Global Antimicrobial Stewardship Accreditation Scheme ( GAMSAS ) initiative reviews, mentors and accredits hospital AMS programmes through a robust assessment process. GAMSAS aims to establish centres of excellence in the UK and around the world to tackle AMR by supporting the use of effective AMS .
GAMSAS is a quality-improvement focused, points-based accreditation scheme based on standards for AMS and the supporting IPC and microbiology laboratory services. AMS standards have been developed utilising published standards from around the world and reflect what is feasible across both high-income countries and LMICs . GAMSAS strives for a collaborative approach to stewardship globally, raising standards, sharing best practice, and facilitating mentorship between communities.
GAMSAS aims to:
- identify local areas of practice needing improvements and support
- develop regional networks to support the spread of good practice in AMS
- create awareness in healthcare payers and users of variation, and how this can be addressed
- support practice and policy research aimed at improving AMS
- develop and supply educational resources to support AMS practice (via the Global Antimicrobial Stewardship Partnership Hub)
Established in 2022, GAMSAS has now accredited the AMS programmes of 10 hospitals, 5 in the UK and 5 overseas. BSAC has worked with AMS experts and teams in these hospitals to assess their AMS systems, processes and practice via desktop reviews and hospital visits. BSAC is currently working with hospitals in a further 10 countries and plans to accredit a minimum of 20 hospitals in 2024 both in the UK and overseas. GAMSAS provides a sustainable approach to AMS via 3-yearly re-accreditation, utilisation of a pool of AMS experts across the world to support the assessment process and collaboration with partner organisations to support access to accreditation across all healthcare economies.
Commitment 4.1 - Clinical decision support
We will reduce avoidable human exposure to antimicrobials by supporting health and social care teams with decision support, risk stratification tools and judicious use of diagnostic tests, underpinned by improved diagnosis coding, to inform shared decision-making and target antimicrobials to patients most likely to benefit.
This commitment signals an evolution of antimicrobial stewardship and the adoption of new ways to safely reduce human exposure to antimicrobials. Enabling genuine shared decision-making is a fresh approach for this NAP . Existing clinical guidance does not contain sufficient useful information on the natural history of infection illness, the prognosis of untreated infection, the benefits and risks of antimicrobials or the alternatives to antimicrobials, to empower patients, enable shared decision-making and reduce demand for and expectation of antimicrobials.
Clinical decision support tools are aids which can guide clinicians in the complex area of treatment choices, especially when there is incomplete information, or in a busy environment. They can help ensure healthcare workers access accurate and real-time information which allows for informed decisions when prescribing antimicrobials. These tools can utilise large data sets, algorithms and local resistance patterns to provide the best possible picture for healthcare workers deciding which antimicrobial to prescribe (or not to prescribe).
Similarly, risk stratification tools (optimising the use of digital health information systems and artificial intelligence) enable a nuanced take on the difficult decisions around when to prescribe antimicrobials and, importantly, when not to. Being able to identify high-risk populations or settings for AMR means surveillance can be targeted and guidelines adapted, resulting in better stewardship. Helping clinicians in identifying the ‘threshold for treatment’ reduces unnecessary prescriptions, and encourages a shift from ‘what to prescribe?’ to ‘whether to prescribe?’
Diagnostics form part of decision support, aiding both the identification of infection and subsequent targeting of specific organisms. This can reduce unnecessary prescribing and overprescribing of broad-spectrum antimicrobials, and directly benefit patients who get the right treatment. Ensuring rapid, accurate diagnostic testing is available when and where needed is therefore necessary in reducing incidence of AMR .
Reducing unnecessary antimicrobial prescriptions is a core undertaking of this NAP . Supporting frontline clinicians in making the best choices regarding antimicrobial treatments, with decision support and risk stratification tools, alongside adequate availability of diagnostic tests in community and hospital settings, will create a clinical environment where the right antimicrobials are prescribed only to those that need them, at the right time.
Case study: artificial intelligence ( AI ) and digital tools
With the increasing digitalisation of the NHS, the next 5 years are crucial in terms of ensuring AMR is embedded as a consideration in digital transformation. AMR interventions can be hampered by poor implementation of digital systems and there is a need to adopt digital technologies that enhance AMS practices.
Innovative digital tools to support prescribers’ decision-making are emerging, such as the Scottish Antimicrobial Prescribing Group (SAPG)’s Antimicrobial Companion app and the MicroGuide app. These applications, and similar tools, may offer the opportunity to improve patient outcomes and rationalise antibiotic prescribing.
AI could further support risk-stratification of patients and targeting of antibiotic treatment based on available data. However, the implementation of AI tools would require the right data being available in the right format to enable ‘big data’ analysis by AI . The effectiveness and safety of AI for decision support depends on fully integrated digital systems with data governance permissions to access a large data lake and apply this learning to optimise decisions for individual patients.
Over the next 5 years, the focus in this space should be on research, evaluation and validation of AI technology (taking advantage of the data infrastructure of the NHS). Further evidence on acceptability to clinicians, clinical outcomes, and cost-effectiveness is needed, before routine implementation in the NHS would be possible.
Prescribing and supply of antimicrobials for humans is increasingly undertaken in the UK by health professionals other than doctors. Since 31 January 2024, antimicrobials have been available from community pharmacies through the Pharmacy First service in England (following similar services in Scotland and Wales). From 2026, all pharmacists will graduate with an independent prescribing qualification. Providing tools to support antimicrobial treatment targeted only to patients who need them is critically important for independent non-medical prescribers to optimise diagnostic and therapeutic decision-making, as is continuing to monitor and evaluate the impact of these services on antimicrobial use in the UK.
Commitment 4.2 - Appropriate prescribing and disposal
We will support health and social care teams to make decisions about the optimal selection of antimicrobials, dose, route and duration of treatment for individual patients, with guidance on spectrum of activity, route of administration, and alternatives in allergy or contra-indication and support patients and health and care professionals to safely dispose of antimicrobials.
Applies to people and the environment.
The UK has a good record in the field of AMS , and this is something to build upon further. There continues to be room for improvement in this area and it is important not to lose sight of antimicrobial use as a driver of AMR . AMS comprises a number of core components including:
- correct diagnosis
- optimal drug
- correct dose
- correct time
- correct route of administration
- optimal duration
- timely de-escalation
Prescribers and patients should also consider the safe disposal of antimicrobials.
Case study: monitoring of prescribing trends
Since 2020, Antimicrobial Resistance and Healthcare Associated Infection ( ARHAI ) Scotland has closely monitored and reported trends in antibiotic use in primary care to assess the impact of the COVID-19 pandemic on prescribing behaviour and antibiotic use in humans.
This assessment used near real-time monitoring of weekly trends in antibiotics used for respiratory infection with reporting for action within NHS boards. ARHAI Scotland has continued this regular monitoring and reporting to enable assessment of the impact of NHS remobilisation from COVID-19 and generate evidence for optimisation of antibiotic prescribing.
This enhanced monitoring information is shared with partners to allow for early detection and understanding of changes in antimicrobial prescribing practices to inform local and national interventions and initiatives.
The first decision for prescribers is whether an antimicrobial needs to be prescribed at all. Diseases may present with symptoms similar to antimicrobial sensitive infections, but may in fact be viral in nature, or of non-infective cause. Utilising the decision support and risk stratification tools, as described above, will help clinicians ensure a prescription is appropriate.
If antimicrobial treatment is suitable for the patient, the next question is which one. Current antimicrobial guidelines are available across the UK, and make recommendations for most infections, with specialist advice available from microbiologists and specialist antimicrobial pharmacists, as necessary. Commonly, broad-spectrum treatment is initiated until culture results with resistance data are available for the patient. Ensuring cultures are sent is therefore an important initial step in targeting treatment.
Penicillin allergy is a common contra-indication to the use of this critical class of antibiotics, forcing clinicians to use alternative treatments, putting patients at increased risk of AMR or adverse effects. Access to penicillin allergy de-labelling services is vital to ensure patients are not denied penicillin treatments unnecessarily.
As set out above, rapid and accurate diagnostics are a leading factor in antimicrobial choice, together with making real-time data available to healthcare workers.
Selecting the most appropriate route of administration is vital to ensure infection is treated effectively while not putting patients at risk from unnecessary use of the intravenous or parenteral routes of administration. Ensuring equitable access to outpatient parenteral antimicrobial therapy ( OPAT ) services is also important, to optimise the efficient use of NHS resources and reduce the risk of a prolonged hospital stay.
The next decision to be made is about de-escalation of treatment, whether that is from a broad-spectrum to a narrow spectrum drug, or from intravenous (IV) to oral treatment. This is a continuous process, depending on the clinical condition of the patient, which can also be aided by systems being put in place to prompt clinicians to consider de-escalation in their management plan for the patient, for instance during the ward round.
The duration of treatment is often delineated in guidelines, which aids in ensuring adequate length of treatment. However, growing evidence suggests shorter treatment durations than currently recommended may often be appropriate (see Palin V and others, Shorter and longer courses of antibiotics for common infections and the association with reductions of infection-related complications including hospital admissions . Clinical Infectious Diseases, 73, 10, pages 1805 to 1812 (2021)). Further studies in this field are necessary and we may soon see shorter treatment durations reflected in local antimicrobial guidance documents and prescribing support tools for certain infections.
These decision choices are reflected under ‘Recommendations to prescribers’ in NICE guideline (NG15) , which also encourages prescribers to consider AMR in their prescribing decision making:
When deciding whether or not to prescribe an antimicrobial, take into account the risk of antimicrobial resistance for individual patients and the population as a whole.
Digital and non-digital technologies play an important role in enabling timely clinical decision support, and incorporation of user experience is vital as part of the development, validation and evaluation process of these tools.
Commitment 4.3 - Use of behavioural interventions
We will use and apply evidence, including social and behavioural sciences, across all sectors to better understand, develop and implement behaviour change interventions and disseminate those strategies that are effective in bringing about improvement.
Applies to people, animals, plants and the environment.
This commitment relies on the active participation of public and private sector bodies, including investors, across the human health, animal health, the food chain and environment communities. There is a central role for members of the public too, as patients, consumers, animal owners and investors.
Case study: veterinary antimicrobial use behaviour change in the UK
In the veterinary sector, the UK has been supporting changes in behaviour for several years now and this has been central to the substantial reductions seen in antimicrobial use in animals in the past decade.
The UK’s 59% reduction in the use of antibiotics in food-producing animals makes it one of the lowest users of antibiotics across Europe, and the lowest of those countries with a significant livestock farming industry. Impressively, this has been achieved through a voluntary, sector-led approach, which has transformed attitudes and behaviours around antimicrobial use and has resulted in antimicrobial stewardship becoming a principle which is embedded in UK agriculture.
Industry’s ownership of the issue (led by the Responsible use of Medicines in Agriculture ( RUMA ) Alliance) has been critical, as well as the collaboration between industry and government, which varies from the more widely implemented regulatory and enforcement approaches seen in other countries.
Some of the fundamental principles of behaviour change which have enabled this success include:
- avoiding unproductive blame and guilt
- making the issue relevant and salient
- using ‘regulation by reputation’
- using the right messengers
- following the incentives
Further lessons learnt from this approach can be found in Tackling antimicrobial use and resistance in food-producing animals , a case study produced for the Food and Agriculture Organization ( FAO ) of the United Nations.
Facilitating behaviour change across sectors to protect the use of antibiotics is challenging. It needs to be easy for all involved to make the right decision about whether and how an antimicrobial should be used. Importantly, misconceptions and misperceptions about infections, AMR and AMS should be addressed across all sectors and all communities. Doing so depends on evidence base for behaviour change interventions which support improved antimicrobial use (informed by use of diagnostics and clinical scoring tools) and IPC practices. This will include significant learning from the COVID-19 pandemic. Evidence will inform implementation of practical, effective interventions to improve professional practice and public behaviours in the UK.
Outcome 5 - AMR workforce
By 2029, the UK’s human health, animal health and agriculture workforce and leadership have the appropriate objectives, support and capabilities to tackle AMR , empowered by clear, responsible governance and education.
This outcome has 5 commitments:
- health and social care training
- health and social care workforce
- health and social care governance
- veterinary workforce knowledge and skills
- systems to support animal health
Commitment 5.1 - Health and social care training
We will further embed, and will require, the completion of appropriate IPC and AMS training for all health and social care workers and students, to support implementation of best practice for IPC and AMS in their setting and, for specialist posts, to provide career pathways to promote skills retention and succession planning.
Success of this action plan depends on the practical application of its contents, which is in turn dependent on successful training. Embedding best practice within the curriculum, at undergraduate and post-graduate level, of those in frontline health and social care services is critically important. Ensuring that training programmes instil not just theoretical knowledge but hands-on experience in implementing IPC and AMS measures will improve IPC , infection management and antimicrobial stewardship and build on the already substantial common awareness of these issues in the health and care community.
In 1847, the Hungarian obstetrician Ignac Semmelweis introduced mandatory handwashing for those who wanted to enter the labour room, resulting in a remarkable decrease in maternal deaths from puerperal fever. The causative agent was still unknown, but the effectiveness of good IPC had been proven over 175 years ago.
IPC is paramount to reducing the burden of AMR , and it is everyone’s business. Everyone working in health and social care has a role to play in preventing the spread of infection within health and care settings, including students and visitors. Ensuring that staff have the requisite skills and training to implement and improve IPC practices is the responsibility of each employer.
Social care environments such as care homes have at times been overlooked in the arena of AMR programmes, but they are important places where gains can be made to reduce levels of resistant organisms. Poor antimicrobial stewardship in the social care setting not only affects residents but also carries risk to the wider community, given the mobile nature of staff, visitors and residents. According to the OECD health policy study on Embracing a One Health framework to fight antimicrobial resistance , challenges involve:
- the vulnerability of residents to infections
- difficulty in IPC implementation compared with the hospital setting
- limited access to rapid diagnostic testing
- preventative antimicrobial prescribing (which may be appropriate depending on context but can increase risk of AMR )
- limited surveillance capabilities
(See the ‘Long-term care is an emerging priority area for tackling AMR with a great potential for improvement’ section of the ‘Addressing antimicrobial resistance’ chapter of the above OECD policy study).
Similarly, institutional settings such as migration centres can be at risk of spread and outbreaks of infectious diseases, including infections from geographic regions with high resistance prevalence, and ensuring good IPC measures and AMS are in place in these settings is important in reducing AMR .
While some IPC measures are incredibly effective, further research is needed to gain an even better understanding of where the focus of efforts should be. Carrying out high-quality research into the effectiveness of current IPC programmes should also be encouraged, including the impact of specific measures, to ensure time and effort is spent on informed interventions.
Commitment 5.2 - Health and social care workforce
We will implement a system-wide approach to strong IPC and AMS in health and social care settings, aligning workforce planning with workforce needs and considering system-wide capacity and capability to mitigate and respond to incidents.
A system-wide infection management approach, which includes IPC and AMS , will deliver optimal outcomes for patients as well as improving the usage of antimicrobials. Investing in system strengthening and supporting the workforce for AMS and IPC is a must for the NHS, with AMR likely to increase the pressure on the system. While IPC measures may confer up-front costs, they are likely to be cost-effective in the long term through the avoidance of downstream costs of treating infections, especially resistant infections which typically lead to longer stays in hospital (see the OECD health policy study on Embracing a One Health framework to fight antimicrobial resistance ) and more complicated treatment (see Manoukian S and others, Bed-days and costs associated with the inpatient burden of healthcare-associated infection in the UK . Journal of Hospital Infection, 114, pages 43 to 50 (2021)).
An infection management approach includes national, regional and local integration of AMR teams with those working within IPC and those managing patients with mild and severe illness (including sepsis). It includes prevention of infection, use of diagnostics and appropriate treatment (including for resistant infections). Effective infection management is underpinned by data, education and communication. This is illustrated in figure 5, below.
Figure 5: an infection management approach
Delivery of high-quality healthcare requires consistent training across specialisms, including public health, microbiology, epidemiology and pathology. There is also a need to embed IPC and AMS as everyone’s job rather than leave it to specialists alone. The COVID-19 pandemic demonstrated that all healthcare professionals benefit from some expertise in managing infections. It is critical to embed infection management capability widely across the NHS and care settings as infections are a common reason for seeking help as an emergency, being admitted to hospital, being admitted to intensive care and dying in hospital. An informed workforce will ensure that resources are appropriately allocated according to risk, with the impact of infections not limited to individual patients but affecting public health at large. Role-specific training will be critical to empowering all staff groups, including physician assistants and pharmacy technicians, to implement IPC and AMS principles according to their specific roles and responsibilities.
A crucial element to improving appropriate and timely usage of antimicrobials in patients with both mild and severe infections is the development of useful clinical pathways that assist in the management of patients with suspected infection. Taking a system-wide approach is essential to ensure that evidence-based, practical interventions can be introduced across settings, including community care as most resistant infections are acquired in the community (see Manoukian S and others, Bed-days and costs associated with the inpatient burden of healthcare-associated infection in the UK . Journal of Hospital Infection, 114, pages 43 to 50 (2021)).
Commitment 5.3 - Health and social care governance
We will support appropriate systems for leadership and governance responsibility for infection management, AMS and IPC in health and social care providers and commissioning bodies.
The actions within this NAP focus specifically on AMR but reducing AMR must be embedded throughout the healthcare system. We need to put the right structures in place to centre infection management, AMS and IPC in our health and social care delivery. Efforts to tackle AMR in healthcare settings should not heavily rely on individual ‘champions’ - this is not a sustainable solution to this substantial threat.
All sectors can and must be involved in the work of reducing the number of infections, with social care, primary care and hospital care all potential places where transmission may occur. It is vital that all commissioners in these sectors ensure that effective and structured AMS and IPC programmes are in place. Appropriate systems for leadership and governance will enable implementation of clear policies and procedures, allocation of appropriate resource, effective monitoring and evaluation, and resilience to evolving threats.
We will work with the Care Quality Commission (CQC) and other regulators to support providers of health and social care services to meet their obligations, as set out in regulations (including the Health and Social Care Act 2008: code of practice on the prevention and control of infections in England ).
Commitment 5.4 - Veterinary workforce knowledge and skills
We will work alongside the veterinary profession to ensure that they have the necessary data, knowledge and skills so that veterinarians are empowered to advise on good husbandry and animal management strategies for disease prevention, prescribe antimicrobials responsibly, and, where appropriate, recommend evidence-based alternative treatments in place of antimicrobials.
Applies to animals.
Animal health targets
This NAP sets targets for antimicrobial use in humans but there are already targets in place for different animal sectors , as set out by the RUMA (Responsible use of Medicines in Agriculture) Alliance. The current sector targets cover the period from 2021 to 2024. These are tailored to the features of each sector:
- understanding and benchmarking use
- engagement between farmers and vets
- the development of health plans
- for those sectors where there is sufficient data and room to set targets (for example, pigs and gamebirds), the focus is on achieving specific antibiotic use reductions (30% in pigs and 40% in gamebirds)
- across the sectors, there will be efforts to improve farmer and vet training on antibiotic stewardship, increase vaccine uptake, and increase the uptake of health planning and governance to ensure that highest priority critically important antibiotics ( HP-CIAs ) are only used as a last resort
The collection and collation of antibiotic use data is crucial for monitoring antibiotic use in animal sectors nationally, identifying changes and trends, and exploring any changes. The ruminant sectors are aiming to increase the availability of antibiotic use data by encouraging the use of the Agriculture and Horticulture Development Board (AHDB) Medicine Hub and equivalent initiatives across the UK. Medicine Hub, launched in 2021, is a centralised antibiotic use data collection system. It has captured over 6,500 farm-level data sets so far.
The hub is a central collation point for antibiotic use data in ruminants, compatible with a wide range of antibiotic use data collection systems and with a range of existing industry software. The PIRU evaluation of the first NAP emphasised the need to continue improving the availability of antimicrobial use data in animal sectors.
When the current sector targets end in 2024 the industry has committed to create a new set of ambitious targets.
In the animal health sector, there has been a focus on reducing exposure to pathogens and improving prescribing practices by veterinary professionals, underpinned, where appropriate, by diagnostic tools. In the UK, many stewardship initiatives have been sector led, centred around collaboration between farmers, vets and government organisations. This has led to sustained behaviour change and significant decreases in animal antimicrobial use.
Antimicrobials are essential for veterinary professionals to treat infections and infectious diseases in animals under their care. Antimicrobial stewardship is therefore critical to preserve the availability of effective antimicrobials for animal health. Vets are the gatekeepers of antimicrobial use in animals. Responsible prescribing in the animal sector will help preserve the efficacy of critical medicines for humans and animals. Responsible prescribing is underpinned by evidence-based guidance, clinical decision tools, surveillance data and emerging research on AMR and behaviour change. Prescribing can be avoided through good animal husbandry and prevention tools such as vaccines.
Case study: Arwain DGC
Arwain DGC is a collaborative AMS initiative in Wales led by Menter a Busnes with project partners Iechyd Da, Welsh Lamb and Beef Producers, the University of Bristol and Aberystwyth University. The Arwain Veterinary Prescribing Champions ( VPC ) network has brought vets from 90% of farm or mixed practices in Wales together since 2020 to participate in a programme of training in responsible veterinary medicine use alongside discussion groups, peer learning, workshops, webinars and other in-person and online events.
The VPC network has designed and implemented antimicrobial stewardship interventions within vet practices. The VPC network has worked together with Aberystwyth University and other Arwain DGC project partners to develop 2 national antimicrobial stewardship interventions for the profession aimed at supporting practising vets to prescribe responsibly and develop strong working relationships with their farmers to ensure antimicrobials are used as prescribed.
The code of prescribing conduct is a voluntary code of conduct intended to drive positive change within Welsh farm vet practices, to ensure consistency and accountability in prescribing and to signpost farming clients towards practices that are actively engaged with responsible antimicrobial use, the VPC Network and the Arwain DGC program.
The network has also produced practical, useable clinical guidelines for 6 significant diseases in cattle and sheep:
- watery mouth (E. coli enterotoxaemia) - sheep
- joint ill (neonatal polyarthritis) - sheep
- lameness (scald, digital dermatitis, CODD ) - sheep
- bovine respiratory disease - cattle
- neonatal diarrhoea - cattle
- mastitis (selective dry cow therapy) - cattle
By combining the practical experience of clinical farm vets with literature reviews conducted by academics at Aberystwyth University, these clinical guidelines were launched in 2023 and are set out in a range of resources, including quick reference guides as a practical, on-farm resource for vets, in online documents, which include the underpinning literature reviews and in treatment planners, which farmers and vets can complete together for display to all farm staff.
This NAP will build upon the successful reduction of antibiotic use in animals over the past decade, including expanding stewardship work to the companion animal and equine sectors. In 2023, an online training initiative was launched, providing over 20 hours of continuous professional development relating to improving how antibiotics are used in dogs, cats and horses (funded by the VMD ) - including practical modules looking at different diseases and conditions where antibiotics are used and modules on diagnostics, behaviour change and infection control. This complements other recent companion animal initiatives.
The voluntary collaborative approach taken by the UK to reduce antibiotic consumption in animals was led by the RUMA Alliance, an independent non-profit group which aims to promote the highest standards of food safety and animal welfare. RUMA ’s Targets Task Force (TTF), composed of a specialist farmer and vet representing each livestock sector, developed sector-led targets for each sector by studying their systems closely and identifying opportunities for improved antibiotic use and antibiotic reduction. Targets set in 2017 led to a 52% reduction in antibiotic use and a 79% reduction in highest priority critically important antibiotic ( HP-CIA ) sales for UK food-producing animals.
Commitment 5.5 - Systems to support animal health
We will support the veterinary profession, the livestock and aquaculture industry, retailers and/or processors and animal keepers to ensure animal health and welfare is protected and that animal keepers have the necessary knowledge, skills and data to implement measures to prevent and control disease and infections, reducing the need to treat animals with antimicrobials and, where antimicrobials are necessary, adhere to responsible use and disposal practices.
Farming is an important industry in the UK, representing more than £14.7 billion and more than 72% of its total land area, according to Defra farming and environment evidence packs . In addition, it is the source of high-quality food for our population and a principal component of the UK trade market.
The UK has made huge strides in reducing the use of antibiotics in animal production, through tailored sector-specific approaches, improving husbandry and adopting disease prevention measures to reduce reliance on antibiotics. This collaborative voluntary approach with sector-led targets has resulted in a change of culture of antibiotic use in farming, with AMS now firmly embedded in UK agriculture.
Pivotal to this is supporting animal health and welfare, which reduces the need for antimicrobials. This can be done through improved husbandry, biosecurity and animal IPC . The Animal Health and Welfare Pathway is one example of an initiative to support farmers. The pathway will help to support this commitment by reducing endemic disease in cattle, pigs and sheep to reduce the need for antimicrobials. Programmes may involve diagnostic testing, veterinary advice, vaccination, improvements to on-farm management and active management planning. The PIRU evaluation of the first NAP reinforced the value of initiatives that facilitate engagement between farmers and veterinarians, and the international component of the evaluation found novel policy experiments aligning farmer and veterinarian goals in the Netherlands. More information will be available in the PIRU beef cattle report, due to be published on the PIRU website .
Current efforts to reduce AMR in animals have focused mainly on food-producing animals. However, in 2023, according to Pet ownership in the United Kingdom (UK) 2012 to 2023 published by Statista, 57% of UK households owned a companion animal. The principles of responsible use of antimicrobials applies to the companion animal and equine sectors as much as to food-producing animals. It is therefore essential that veterinary professionals and animal keepers of companion animals and equines have the appropriate guidance in place to make informed decisions about antimicrobial use.
There are lessons to be learnt in reducing antimicrobial use between different sectors. For example, when implementing services that allow community pharmacists (the private sector) to supply antibiotics to humans, there is an opportunity to learn from the collaborative, voluntary approach taken to improve antimicrobial use in the veterinary sector.
Outcome 6 - Innovation and influence
By 2029, the life sciences and technology sector (including government, public and private sector organisations) are actively engaging and responding to the demand for new tools, technologies and interventions for tackling AMR .
This outcome has 4 commitments:
- AMR solutions
- subscription models
- overcoming market barriers
- improvement and adoption
Commitment 6.1 - AMR solutions
We will work across the public sector, regulators, academia and industry to fund and deliver innovative scientific research to develop vaccines, diagnostics, antimicrobials and alternative therapies (including bacteriophage, polyclonal antibodies and host-directed therapies), which meet UK and global needs.
Antimicrobials are the only tools that reliably treat infections in humans and animals, but resistance is outpacing the development of new antimicrobials. There has been no new class of antibiotics since the 1980s. Alongside the development of new antimicrobials, a range of other tools to tackle resistance is needed. AMR is a complex problem and there is no single, technological solution for it.
The discovery and development of a range of new products for preventing, diagnosing and treating infection is essential to combat AMR and ensure we can continue to treat infections and protect public health and animal welfare. The products we need include:
- vaccines to prevent the emergence of infection
- diagnostic tools to identify infections and inform appropriate infection management
- new antimicrobials to treat resistant infections in people and better target treatment
- novel alternative, evidence-based therapies, such as bacteriophages
Science, Innovation and Technology Committee findings on the antimicrobial potential of bacteriophage
In February 2023, the Science, Innovation and Technology Committee ( SITC ) launched an inquiry into the antimicrobial potential of bacteriophages . Bacteriophages - or ‘phages’ - are viruses that can kill harmful bacteria but do not harm humans. The inquiry examined evidence on the safety and effectiveness of phages and the barriers to their development and use.
The inquiry found that:
- phage safety and effectiveness had been shown using observational clinical studies, but further research on phage biology and interactions is needed
- increased investment into phage research would enable more robust studies to be performed and higher quality clinical data gathered
- there is a ‘translation gap’ between phage research and the application of phages in clinical settings
- phage manufacturing within the UK must meet the high standards for pharmaceutical manufacturing set out in good manufacturing practice (GMP)
- phages could be useful tools across sectors, responding in a One Health way
The government response to the SITC report on bacteriophages was published on 1 March 2024.
The commitments in this section of the NAP lay the groundwork to develop a suite of tools (rather than focusing on a single technology) which will contribute to addressing AMR . As set out elsewhere in this NAP , we also need to apply genomic medicine tools to identify and protect vulnerable patients from harm from antimicrobials and digital technologies to promote optimal prevention, diagnosis and treatment of infections.
In addition to supporting the development of these tools, demonstrating their value through strengthening the evidence base for the economics of AMR is essential. Greater understanding of the societal value of new vaccines, therapies, diagnostics and other tools, beyond the benefit to the individual recipient, will support effective decision making over the next 5 years. This area is highlighted within our top 10 research priorities, set out in the ‘Outcome 7 - Using information for action’ section.
Case study: Open Innovation AMR
UKHSA supports open and collaborative work on AMR by offering its expertise and facilities to researchers. An infrastructure award from NIHR , Open Innovation AMR , supported the development of new facilities to enable evaluation of a range of interventions. UKHSA has capabilities in its Porton Down facility which can be accessed by AMR researchers, in academia and industry, including:
- a screening cascade for evaluation of novel antimicrobial therapies
- a unique facility to investigate the role of the built environment in transmission of AMR and the effectiveness of IPC procedures
UKHSA offers a screening cascade which can be accessed for the testing of traditional and non-traditional therapeutic approaches against multidrug resistant bacteria, fungi, and viruses. Expertise can also be applied to the evaluation of new diagnostics and antimicrobial susceptibility tests. Visits by students, post-doctoral researchers or staff to Porton Down are supported, and training is provided in the microbiological techniques used in screening therapies for antimicrobial activity against a large library of multidrug resistant clinical isolates. Work under this programme has resulted in 5 patent filings for novel therapeutics and diagnostics, with a company established to commercialise the lead technology for rapid antimicrobial susceptibility testing (iFAST Diagnostics).
The UKHSA Porton Down facility contains a full-scale, fully functional modular ward which was designed according to current UK guidelines and built to simulate a real-life clinical setting. The facility has a 4-bed ward and isolation rooms with dedicated heating, ventilation and air conditioning systems, realistic water and drainage systems and appropriate surfaces, fixtures, fittings and furnishings. This enables us to study how hospital facilities can be designed and operated to improve IPC and reduce transmission of antibiotic resistant infections, contributing to improved antibiotic stewardship. A range of studies are underway with collaborators looking at methods to control transmission of infections through fomites and aerosols, pathogen spread through hospital water systems and developing IPC guidance on hospital laundry and safe decontamination of linen.
Commitment 6.2 - Subscription models
We will implement purchasing arrangements for new antimicrobials that de-link the price paid for antimicrobials from the volumes sold, monitor and evaluate impact, and advocate for the wider use of these ‘subscription models’ in other countries.
There is a need to address the urgent issue of bringing new antimicrobials to market. Investment in novel antimicrobials is widely seen as commercially unattractive by industry. The high research and development costs and low returns (due to restrictions in use to slow down resistance) have led to market failure.
AMS (prescribing the right antimicrobial to treat the right pathogen at the right time), which is critical to preserve the effectiveness of new products, often means that new antimicrobials are used very little in the first few years after they have received marketing authorisation. Therefore, companies do not see the return on investment that they can with other innovative products where uptake is encouraged rather than restricted.
NHS England and NICE launched a pilot project in July 2019 to test a payment mechanism that de-linked the price paid for antimicrobials from the volumes sold, using a NICE -led healthcare technology assessment. In 2022, the evaluation process was completed and, in a global first, subscription style contracts were awarded in July 2022. The pilot provided the first health economic quantification of the full value of 2 antimicrobials, capturing the population health benefits that extend beyond the benefits for people receiving the drug. In light of lessons learnt from the subscription model pilot project in England ( NICE and NHS England), proposals have been developed to scale the model to more antimicrobials across the UK - see the Antimicrobial Products Subscription Model: consultation on proposals .
The UK represents a small proportion (approximately 3%) of the global antimicrobial market and therefore cannot solve the issues within the global antimicrobial pipeline alone. The adoption of pull incentives in other markets, in combination with the UK’s scheme, should create a meaningful incentive for global investment in antimicrobials. Sharing progress and learning from the project with international partners is an important part of the UK approach. This has been strengthened by advocacy from the UK Special Envoy on AMR , Professor Dame Sally Davies, working with finance ministers, including during the UK’s G7 presidency and subsequent Japanese and German presidencies.
There is also government support for the development of new antibiotics, including financing basic science and early-stage innovations. For example:
- UK Research and Innovation ( UKRI ) finances basic science
- the UKHSA Drug Discovery Group is developing procedures for the discovery of new drug combinations that may be effective against resistant pathogens
- DHSC ’s GAMRIF invests in early-stage innovations
- NIHR invests in a wide range of clinical and applied research
Commitment 6.3 - Overcoming market barriers
We will collaborate across the public sector, with academia and with industry to identify needs and to overcome market barriers, to enable new products to move from discovery to market in an equitable and sustainable way.
As highlighted by the Center for Global Development’s report, A new grand bargain to improve the antimicrobial market for human health , there are substantial barriers preventing the tools needed to tackle AMR from making it to market. Discovery needs to be matched with a supportive environment in which those new creations can be appropriately regulated, adopted and taken up in practice. There are specific challenges for different products. We want to help both small and large innovating companies bridge the ‘valley of death’ for novel therapeutics, vaccines and other tools targeting bacterial pathogens. This will primarily be implemented via Innovate UK’s pathways to antimicrobial clinical efficacy ( PACE ) initiative.
Case study: PACE
PACE is a UK-based £30 million programme of funding and support to be deployed over 5 years. PACE will bring together the right funding, resources and partnerships to help innovators progress their early-stage antimicrobial drug and diagnostics projects with greater speed, support and confidence - giving the best AMR innovations the greatest chance of success. PACE is a collaboration between 3 leaders in the UK health innovation and research community:
- Innovate UK
- Medicines Discovery Catapult
PACE harnesses their unique expertise, catalysing and working with the global AMR community to accelerate the speed of innovation to mitigate the risk of AMR .
There are 3 main strategic pillars to the PACE initiative:
- strengthen the pipeline - PACE will grow a pipeline of high-quality antimicrobial drugs and associated diagnostics aligned with unmet needs
- enable preclinical translation - PACE will provide innovative researchers in academia and SMEs the funding, advice and support they need to build de-risked and investment-ready assets
- accelerate progress and overcome barriers - PACE aims to convene collaborative networks to identify barriers to innovation, advance programmes, and drive new collaborative research and development
Through these mechanisms, PACE will further embrace innovation and maximise the diversity of approaches to meet the AMR threat. The PACE initiative will aim to provide wrap-around support for AMR products and their developers, going beyond a simple funding model. PACE aims to deepen and strengthen data packages for AMR assets and work alongside product developers, regulators and experts to identify the best partners to plug gaps in resource or capabilities. The intent is to improve the potential for future onward progression and investment.
Clinical trial infrastructure, including the use of platform trial methodology, successfully deployed by the NHS for the rapid evaluation of COVID-19 therapeutics, should be optimised for clinical development of antimicrobials, vaccines and diagnostic tests across pathogen types and AMR associated disease locations. This can help reduce the size (and cost) of trials targeting rare but increasingly resistant pathogens. Investing in building and retaining talent in non-viral infectious diseases is critical to ensuring we can develop new antimicrobials in the future (see The Wellcome Trust 2020 report, The global response to AMR : momentum, success and critical gaps ). Other infrastructure developed for COVID-19 can also be built on to tackle AMR . For example, monitoring of the effectiveness of deployment of novel antimicrobials can be adapted from the novel therapeutics surveillance programme at UKHSA .
The development of new antimicrobials, even if rapidly accelerated by investment into research and the advancement of digital tools, is not a magic bullet which will solve the problem of AMR . As new antimicrobials are developed, they will exert additional selection pressures on pathogens and therefore need to be used with great caution. For that reason, our efforts on antimicrobial stewardship (as described in the ‘Outcome 4 - Antimicrobial stewardship and disposal’ section) remain of the utmost importance.
Case study: vaccines and AMR
Vaccines are a central part of infection prevention by:
- reducing sensitive and resistant bacterial infections in vaccinated people and unvaccinated people (through herd immunity)
- reducing antibiotic use by reducing the number of infections which require treatment with antibiotics
In its 2021 action framework , the WHO describes how vaccines can contribute sustainably and equitably to the tackling of AMR by preventing infections and reducing antimicrobial use.
It included 3 goals:
- expand use of licensed vaccines to maximise impact on AMR
- develop new vaccines that contribute to prevention and control of infections
- expand and share knowledge of vaccine impact on AMR
The role of animal vaccines in reducing the development of AMR is part of a suite of measures required for successful infection control.
Commitment 6.4 - Improvement and adoption
We will drive improvement by assessing and regulating novel technologies and approaches at pace, using evidence to increase timely and appropriate adoption.
While development of new products is a crucial element of tackling AMR , it is only one piece of the puzzle of making sure they are used as needed. The pathway to market is underpinned by assessment of a product’s value to end users and by robust regulation. It is critical to ensure that safe and effective products work in real-world settings (particularly in human health and care and veterinary and farm settings).
Understanding of the social and behavioural factors involved in adoption of new products, tools and guidance will be strengthened through research commissioned in support of the top 10 AMR research priorities set out under the ‘Outcome 7 - Using information for action’ section.
We need to understand what works best to help staff on the frontlines. This will be supported by clarity on assessment, regulation and incentivisation for use of new products.
The Veterinary Medicines Directorate ( VMD ) is the regulator of veterinary medicines in the UK with the main objective of protecting animal health, public health and the environment. This includes fostering advances in pharmaceutical technology and novel therapies, offering scientific advice to strengthen marketing authorisation applications and providing robust safety and efficacy assessment of new veterinary medicines before approval in the UK.
The Medicines and Healthcare products Regulatory Agency ( MHRA ) is responsible for ensuring patients in the UK have access to safe and effective medicines and medical devices. The agency supports innovation from point of invention to point of care, and ensures that the quality, safety and efficacy of medicinal products and medical devices is demonstrated with robust scientific evidence along the entire product lifecycle. MHRA works with innovators to enable them to provide this evidence by developing reference reagents to benchmark the methodologies used to evaluate them, as well as providing guidance to understand what evidence is needed for regulatory approval.
Novel products, which are needed to tackle AMR , can present challenges to regulators as well as the scientific community. MHRA is therefore working closely with innovators from the early stages of product development to ensure that the regulatory science and frameworks needed to get safe and effective products to market are in place. Guidance is provided to help innovators understand what evidence MHRA requires in order to evaluate the quality, safety and efficacy of new products.
Outcome 7 - Using information for action
By 2029, public policy, clinical and funding decisions on AMR will continue to be informed by robust surveillance, modelling, strengthened scientific research, interconnected data sets and emerging international evidence.
- evidence generation and use
- research networks
Surveillance programmes generate information for action. Indeed, research and surveillance are closely related and will be coupled through the lifespan of the NAP . Surveillance continues to inform the development of research questions just as research outputs also inform priorities and direction setting for surveillance. This helps to set out what the unknowns are and what the most urgent areas are for monitoring levels of AMR and use of antimicrobials.
Commitment 7.1 - Evidence generation and use
We will fund, collect, generate and use research, innovation and evidence to improve understanding of AMR , its impact and how to mitigate it, with a focus on enabling the necessary research infrastructure, knowledge transfer and disciplines to meet identified research priorities (including those set out in the ‘top 10’).
Evidence will inform the actions taken in this NAP , across all sectors, practitioners and settings.
The UK already invests extensively in research to enable us to tackle AMR . UKRI directly supports and enables UK researchers to carry out unique research, in collaboration with colleagues around the world, to improve our understanding of AMR and to deliver innovative and effective AMR solutions. For the human population, DHSC invests over £1 billion a year in health and care research through NIHR , including funding of Health Protection Research Units ( HPRUs ), partnerships between UKHSA and academia. Through NIHR , DHSC will be investing up to £11 million of funding by inviting applications for HPRUs addressing healthcare associated infections and AMR .
NIHR funding for AMR research has seen a year-on-year increase in recent years. During delivery of the first NAP (from 2019 to 2024), NIHR programme funding for AMR research totalled £88 million.
Over the past 5 years, this has included:
- programme funding for researcher-identified topic areas across AMR
- 2 NIHR HPRUs with a specific focus on AMR and healthcare associated infections ( HCAIs ), based at Imperial College London and the University of Oxford
- numerous career development awards, PhDs, fellowships and professorships in AMR through the NIHR academy
This does not include NIHR infrastructure or Clinical Research Network support. NIHR also supports research into AMR in LMICs , with official development assistance ( ODA ) funding through the NIHR Global Health Research programme.
Through GAMRIF , DHSC funds and leverages wider investment in new innovative AMR research and development. A recent success was a new, first-in-class antibiotic (in over 30 years) zoliflodacin, which is in phase 3 clinical trials.
While there is a significant amount of research and evidence generation on different areas of AMR across the UK academic landscape, there are still unknowns in terms of our basic understanding of AMR , its associated risks and effects, and how best to mitigate it. In addition, there are areas where research has resulted in new interventions, but evaluation, social sciences, or implementation research is needed to drive use of the outcomes of research in practice.
Top 10 research priorities
To provide clarity about our priorities for AMR research which will best support policy, we have developed 10 AMR research priorities, set out as questions that UK policy makers most want answered. It was informed by stakeholder engagement and collaboration with funders, and by other research prioritisation exercises, including the WHO ’s 40 One Health AMR research priorities .
The top 10 is intended to identify priorities, not gaps, but there are some topics within AMR where there is a lack of evidence. For example, antifungal resistance has emerged as a rising threat within the environment which is not fully understood.
Government organisations will work with research funders in the UK, to support the top 10, remaining responsive to the most pressing research needs to inform policy. Some specific research questions for each of the top 10 research priorities can be found in Appendix C.
1. What is the cost of AMR ?
This priority is intended to build an understanding of the economics of AMR . There is currently a lack of evidence to provide a full economic case for interventions tackling AMR . Research to define and understand the costs and values of interventions and equipped with cost-effective tools to tackle AMR , will be important to confront the AMR challenge.
2. What is the relationship between AMR and health disparities?
This priority is intended to understand how socioeconomic determinants of health interplay with the susceptibility, risk, burden and impact of infections and rates of chronic infection. Building evidence of the risk and outcomes for vulnerable groups is important to inform appropriate action to address AMR . It is vital to understand how to facilitate timely patient access to relevant resources, services and treatment across vulnerable groups.
3. How to influence public awareness and behaviour on AMR ?
This priority is focused on how to improve understanding and awareness of AMR to empower and equip the public to act where appropriate.
4. How to address AMR in international settings?
This priority considers how to ensure that research on how to reduce and address AMR is applicable to international settings and population groups with different needs. This priority includes understanding what can realistically be achieved within low income settings and contexts where there may be limited resources and accessibility issues.
5. What are the basic drivers and effects of AMR , and how does it spread?
This priority focuses on strengthening understanding of the basic drivers of AMR , including how it spreads and evolves in the built and natural environments. There is still a lack of understanding in what drives AMR , how it can be characterised and how it spreads. There is a need to understand what drives resistance, for example how Gram-negative infections spread in the built environment and high-risk settings and understanding the impact of sewage overflows and the spread of resistance genes through soils, waterways, lakes and the seas.
6. How can we prevent AMR from spreading?
This priority focuses on how to mitigate the spread of AMR to minimise risk to humans and animals (including companion animals). Healthcare settings, and particularly hospitals, are a very high priority for understanding what works to reduce AMR and avoid its spread. However, there is also a need to understand and evaluate what works to mitigate AMR spread through the natural environment and if there are unintended consequences associated with interventions.
7. How can we optimise the use of antimicrobials?
This priority is intended to understand what works to optimise the use of antimicrobials and diagnostics across sectors. This might include consideration of shorter courses, targeted dosage, automatic stopping, rapid point of care tests and other novel approaches. There are fundamental gaps in our knowledge of antimicrobial use in human healthcare, animals and plants including knowing what is safe and appropriate as a form of treatment while minimising AMR .
8. What methods can be used to prevent, treat and manage infections without antimicrobial medicines?
This priority is focused on the most effective, and safe, non-antimicrobial medicine routes of care, including at home and community-based methods, for preventing infection, treating worsening infection and managing chronic infection in humans and animals. It may include building evidence for how individuals can safely treat their own infections, or receive treatment at home and in the community, through over-the-counter pharmaceutical and non-pharmaceutical methods like painkillers, nutrition and hydration.
9. How can we drive innovation of new products for tackling AMR ?
This priority is intended to ensure we can capitalise on the discovery of new products for tackling AMR (including prevention technologies, vaccines, diagnostics and new or alternative therapies), drive innovation, and overcome market barriers. Work is needed to strengthen the pipeline of new and alternative products that can both prevent infection (vaccines) and treat them (new antimicrobials and alternatives like phages) and ensure optimal treatment (diagnostic tests).
10. How can we ensure what is known to work is implemented?
This priority is intended to strengthen understanding of how to maximise adoption of existing, effective products, including for application in different sectors and global settings to prevent and manage infection. Improving implementation of effective interventions is essential to overcoming AMR . This includes enabling the uptake of products across settings where infections are controlled and ensuring adherence to interventions and tools on the front lines.
Figure 6: top 10 research priorities
Figure 6 shows that of the top 10 research priorities:
- numbers 1 to 3 are cross-cutting priorities
- number 4 is part of being a good global partner
- numbers 5 and 6 are part of reducing the need for, and unintentional exposure to, antimicrobials
- numbers 7 and 8 are part of optimising the use of antimicrobials
- numbers 9 and 10 are part of investing in innovation, supply and access
Application of the top 10
These research priorities should be considered through a One Health lens. This does not necessarily mean all research questions must cover more than one sector or discipline. Rather, that researchers should, for example, show they are aware of the wider context of AMR and consider where findings about what works to reduce AMR in one sector, setting or community could be applied in another.
Research to support the top 10 is underpinned by several enablers including, but not limited to:
- laboratories and equipment
- clinical trial infrastructure
- healthcare data platforms
- integrated One Health surveillance
- the research workforce
While this top 10 reflects the priorities of policy makers in the UK, research does not take place in a vacuum, but is part of a global system. Researchers may consider the international application of interventions designed for the UK context, and vice versa.
Case study: GAMRIF gap analysis
DHSC commissioned Ecorys to conduct a gap analysis of the current AMR research and development landscape to inform GAMRIF ’s funding decisions and identification of potential areas for future intervention. Findings were published in January 2023.
The analysis, which has informed the development of the top 10 research priorities in this NAP , found that there are some significant gaps in:
- operational research to reduce AMR in LMICs (noting that innovations and interventions exist in high income countries are not always feasible to adapt in LMIC settings)
- assessment of the feasibility and cost of regulatory measures in LMICs
- more openly available data and data sharing across countries (through harmonised surveillance) to further research and development on AMR solutions
- technical solutions which are relevant to LMIC settings (which may have different needs in terms of the pathogens and syndromes which have the highest burden)
- awareness about AMR , especially in plants and the environment, and animal health
Researchers in the UK are already doing a significant amount of work to understand the international picture and collaborate with their counterparts in other countries. For example, the Joint Programming Initiative on Antimicrobial Resistance ( JPIAMR ) is an international collaborative platform engaging 29 nations and the European Commission to curb AMR . JPIAMR co-ordinates national research funding and supports collaborative action for filling knowledge gaps on AMR with a One Health perspective.
A whole-systems approach to evidence generation and surveillance to resolve complex systems problems, like AMR , is necessary. The purpose of funding research on AMR is so that it can be used in practice, hence there is an ongoing commitment to strengthening the relationship between researchers and policy makers.
Case study: Health Protection Research Units - research to policy dialogue
Since 2014, NIHR has funded HPRUs dedicated to healthcare associated infections and AMR , based at the University of Oxford and Imperial College London, at a cost of £4.4 million each over 5 years. These are a partnership with UKHSA and support UKHSA ’s evidence base to enable it to deliver its strategic aims and statutory duties to protect the nation’s health.
The NIHR HPRUs fund high-quality health protection research to inform the delivery of UKHSA ’s objectives in distinct research priority areas. In addition, the HPRUs provide a flexible staff and research capacity, enabling them to respond to major or emerging health protection incidents and/or policy priorities, where appropriate, in a rapid and agile manner. They also offer advice to policy makers and analysts on the evidence base and options for policy development.
Commitment 7.2 - Research networks
We will fund and support transdisciplinary AMR networks and research and innovation grants that support the expansion of AMR communities, supporting cross-sector knowledge transfer and the delivery and implementation of timely, high impact, and independent research and innovation for AMR that meets identified needs of policy makers, practitioners, industry, civil, clinical and broader society.
The research landscape for AMR is fragmented. Communities, infrastructure and data across human, animal and plant health sectors are not well integrated and opportunities to share resources and learning are often undeveloped. There is an important need for innovative new tools and tactics to be developed based on a fully integrated systems-based approach. UKRI ’s transdisciplinary AMR programme works to address this via a 2-phase approach.
Phase 1 will support a broad suite of capacity building awards which will look to establish or expand existing networking opportunities in the UK AMR landscape, with phase 2 evolving into a more focused set of larger scale research grants and programmatic awards.
Outcome 8 - Health disparities and health inequalities
By 2029, the UK targets interventions and associated funding where there is the most burden from AMR , where it will have the greatest impact in controlling AMR , and where it will be cost-effective, including targeting specific regions, population groups and settings if appropriate.
This outcome has 3 commitments:
- data on health inequalities
- toolkit for addressing health inequalities
- interventions to reduce health inequalities
Good health is not spread equally in society. There are avoidable differences in health outcomes between groups or populations, and infections are no different. This plan is committed to developing understanding of the factors that affect variation in infection related health outcomes and how to address them.
It is the intention to embed the reduction of health disparities throughout delivery of this NAP , and activity focused on specific groups is not limited to this outcome. The activity and underpinning commitments are intended to demonstrate the priority of this cross-cutting area of work.
Case study: impact of infections and AMR on children and the elderly
The increased number of cases of group A streptococcus in the UK in the winter of 2022 to 2023 was a pertinent example of the way that infections affect different populations unequally, with children at particularly high risk during that surge.
Children are vulnerable to infections in general, and antibiotics are an essential tool to treating childhood illness and protecting the youngest in our society. Children are also at risk of unnecessary exposure to antibiotics, particularly for viral respiratory tract infection, and antibiotic exposure in children can adversely affect the normal development of innate and adaptive immunity, increasing susceptibility to infections in later life (see Shekhar S and Petersen FC, The dark side of antibiotics: adverse effects on the infant immune defence against infection . Frontiers in Pediatrics, 8 (2020)). Early diagnosis and prompt effective treatment of serious infection in children is critical but equally important is reducing unnecessary exposure of children to antibiotics through appropriate training and resources for prescribers, including clinical decision support tools and judicious use of diagnostic tests.
Similarly, older adults are more susceptible to AMR -related illness , likely due to incidence of infections (including healthcare-associated infections) and comorbidities. Frequent prescribing of antibiotics for older patients is widespread and there is evidence to suggest that there is frequent unnecessary prescribing in some settings, such as long-term care facilities.
Data is power when it comes to improving outcomes for the groups that need it most and our commitments below show how we will be using data to strengthen our understanding of infections and AMR in different groups, and to develop targeted interventions.
There remain large gaps in understanding and knowledge of how infection incidence, antibiotic use and clinical outcomes differ between populations. Therefore, this is an essential research priority (as set out in the top 10 under the ‘Outcome 7 - Using information for action’ section).
The PIRU evaluation of the first AMR NAP found that in addition to providing evidence-based guidelines for prescribing, consideration should also be given to local variation. This was to include geography, and population socioeconomic factors, which can affect the need for antimicrobial prescribing, especially in more deprived areas.
The ESPAUR report 2022 to 2023 showed that the AMR burden from bloodstream infections differed according to indices of multiple deprivation ( IMD ), with the rate of bloodstream infections highest in the most deprived groups (see table 2.2 in chapter 2).
Figure 7 below shows the AMR burden from bloodstream infections by IMD , where the first quintile represents the population in the most deprived 20% of areas in England and the fifth quintile represents the least deprived 20% of areas. The chart shows that the rate of bloodstream infections per 100,000 population was:
- 163.3 for IMD 1 (the most deprived group)
- 146.8 for IMD 2
- 142.8 for IMD 3
- 135.0 for IMD 4
- 125.9 for IMD 5 (the least deprived group)
Figure 7: AMR burden from bloodstream infections by deprivation
Commitment 8.1 - Data on health inequalities
We will establish pathways for collecting and reporting data annually on infection incidence, AMR and antimicrobial use, including (wherever possible) variation by age, sex, disability, ethnicity, nationality, deprivation, geography and high-risk settings, which will be used to inform intervention development.
There is excellent data available for the UK on a variety of health conditions (such as cancer and cardiovascular disease) and how they relate to protected characteristics and other categories, including ethnicity, sex and level of deprivation. While there is similar data on infections, enhancing this by committing to collecting and reporting AMR data in the context of health inequalities is essential to help inform interventions for marginalised, disadvantaged or vulnerable populations.
A targeted approach to tackling AMR is possible only by having granular enough data to know the scale of the problem at different levels and in different groups of people. Further to this, enhanced surveillance provides opportunities for more bespoke analysis of high-risk populations.
Commitment 8.2 - Toolkit for addressing health inequalities
We will collate cost-effective, evidence-based resources into a toolkit, adaptable to local needs, for identifying and addressing health inequalities in access, infection incidence, clinical outcomes, vaccine uptake and antimicrobial exposure to support organisations to develop interventions that address and do not exacerbate health inequalities.
Regional public health teams and other professionals involved in tackling AMR will benefit from a toolkit. This will ensure they are considering and addressing infection and AMR -related health disparities in their areas.
Several different groups are more vulnerable to infection and resistance, including socioeconomically disadvantaged populations, people with disabilities, migrants, refugees, children, the elderly and people living in high-risk settings. Providing support to those who need it is only possible if local government and organisations have the data and know how to address the issues identified in their areas. A toolkit for this purpose will support action at local community levels.
Research from the UK demonstrates that 10% of antibiotics in general practice are prescribed to 0.5% of registered patients, with some patients exposed to more than 10 courses of antibiotics per year (see Shallcross L and others, Antibiotic prescribing frequency amongst patients in primary care: a cohort study using electronic health records . Journal of Antimicrobial Chemotherapy, 72, 6, pages 1818 to 1824 (2017)). Work has begun to develop resources to support health professionals with the structured medication review of patients experiencing recurrent infection. This is essential to safeguard this vulnerable patient group from the threat of AMR .
Commitment 8.3 - Interventions to reduce health inequalities
We will develop, implement and evaluate interventions, underpinned by the use of health equity tools, to reduce infections and avoidable antimicrobial exposure, optimise clinical and population outcomes and patient safety, adapting approaches to consider the main groups and factors commonly associated with health inequalities.
The wider determinants of health have been well documented. The inequality observed in the outcomes from infection follow the same patterns as for non-communicable diseases, such as heart disease, mental ill health and cancer. As such, many of the interventions required, including broader, societal levers, are the same as for other health disparities.
However, there are still specific points in the patient infection pathway where there are opportunities to intervene to reduce health disparities. The commitments above will help to understand the nuance of these varied outcomes for infection and understand what specific interventions we can employ to mitigate them.
Interventions will be designed to recognise and address the different challenges that different groups, settings and localities might face. Action at a local level will be necessary to effectively mitigate the threat of AMR .
Outcome 9 - AMR diplomacy
By 2029, the UK is engaged with galvanising international action on AMR and works closely with global leaders, including through sustained engagement via the G7, G20 other multilateral groups, technical networks and bilateral relationships supporting on a clear strategy for reducing AMR risk through international research collaborations, agreed ways of measuring progress, including sharing of data and best practice.
- prevention and preparedness
- access and stewardship
- antimicrobial use in farming
- standards for manufacturing and waste management
- advocacy and engagement
AMR is a One Health global issue, respecting no borders and rendering siloed working futile. Mitigating the threat of growing AMR to global health and economic security demands international collaboration. Through work related to the first NAP as well as prior commitments, the UK is already established as an international partner in the global effort to tackle the spread of resistant infections.
International action will continue in 2 ways:
- By carrying out extensive AMR mitigation programmes in the UK through this NAP , setting a good example and sharing best practice on the international stage.
- By engagement and leadership in international multilateral and bilateral groups to:
- drive global awareness and advocacy: the UK has been instrumental in raising global awareness about AMR at the highest political level, particularly in the run up to the previous UN high-level meeting on AMR . Consistently advocating for AMR to be recognised as a major public health threat on the international stage, including prioritising it on 3 ministerial ‘tracks’ during the 2021 UK G7 presidency
- fund and foster research and innovation: the UK has invested in research and innovation to address AMR . Initiatives like GAMRIF and the UKRI cross council initiatives have provided funding for international partnerships that aim to develop new antibiotics, diagnostic tools and alternative treatments for both human and veterinary medicine. The UK’s strong pharmaceutical and research sectors also contribute to these efforts
- encourage responsible access and antimicrobial use: the UK has implemented robust policies and guidelines to promote responsible antimicrobial use in healthcare and agriculture and globally to ensure other countries do the same. Our ODA investments in research and development have been used to ensure access and stewardship requirements are built into early-stage research funding, so the next generation of products become both more accessible and better managed
- support international collaboration: the UK actively collaborates with other nations and organisations to combat AMR . Participation in international groups, such as the G7 and G20, as well as more technical forums such as the Transatlantic Task Force on AMR ( TATFAR ) and the Global Health Security Agenda to advocate for AMR mitigation and co-ordinate efforts with other leading nations
- strengthen prevention and preparedness capacity globally: the UK recognises the importance of assisting other countries to address AMR . Providing financial and technical support to build capacity for AMR surveillance, infection prevention, water and sanitation, and responsible antibiotic use programmes in these regions, including through the world’s largest single investment in AMR and antimicrobial use surveillance capability for LMICs through the Fleming Fund and Foreign, Commonwealth and Development Office (FCDO) official development assistance ( ODA )
- strengthen surveillance and reporting: the UK conducts rigorous surveillance of antibiotic resistance, contributing data to global monitoring efforts. This data helps track trends in AMR and informs international strategies for its containment
Case study: edible antibiotic alternative
A leading cause of death in LMICs , diarrhoeal disease remains a major global health problem killing around 525,000 children under 5. Globally, there are nearly 1.7 billion cases of childhood diarrhoeal disease per year, mostly resulting from contaminated food and water sources, which can lead to severe dehydration. Diarrhoeal disease is caused by a variety of bacteria, viruses and parasites which drives the use and misuse of antibiotics. While some bacterial causes of diarrhoea can be effectively treated with antibiotics, these drugs will not treat infections caused by viruses and parasites. Misuse of antibiotics can lead to the development of AMR . Sadly, many bacterial pathogens, such as Escherichia coli (E. coli) which is a leading cause of diarrhoea in LMICs , have developed resistance to commonly used antibiotics making it increasingly difficult to treat.
DHSC ’s GAMRIF tackles diarrhoeal disease in LMICs through innovative product development targeting E. coli. In partnership with the Combating Antibiotic Resistant Bacteria Biopharmaceutical Accelerator, GAMRIF has funded the development of a low-cost, edible antibiotic alternative product based on the algae spirulina. This product does not need to be stored in a fridge or freezer, making it easy to ship, store and use worldwide, including in resource-poor settings.
Considering the specific needs of LMICs throughout the development of a product is vital. This enables equitable access around the world to tools that prevent and treat diarrhoeal disease and helps to slow the spread of AMR .
Commitment 9.1 - Prevention and preparedness
We will support improved global prevention of, and preparedness for, rising levels of AMR , including through building sustainable partnerships, supporting global surveillance capabilities, capacity and capability building, and system strengthening.
AMR represents a significant threat to global health security and supporting improved global prevention of and preparedness for rising levels of AMR is of critical importance. By actively contributing to global prevention efforts, the UK plays a pivotal role in reducing the risk of pandemics and health crises that have the potential to disrupt economies and overwhelm healthcare systems, both domestically and internationally.
Investing in prevention is often more cost-effective than dealing with the consequences. Preventing the emergence and spread of AMR through vaccination, responsible antibiotic use, improved infection control, access to clean water and sanitation not only saves lives but also reduces the long-term financial burden on healthcare systems. The UK has supported the development of the WHO ’s global strategy on infection prevention and control , which highlights the central role that IPC plays in mitigating AMR , as well as in responding to outbreaks and enhancing patient safety.
Sustainable partnerships are also essential in the fight against AMR . Collaborating with other nations and international organisations - such as the WHO , World Organisation for Animal Health ( WOAH ), FAO and UNEP (the Quadripartite organisations ) - strengthens the global response to AMR , enabling improved resource mobilisation and co-ordination efforts.
This commitment aligns with international agreements and agendas, including the WHO SDGs and the global action plan on AMR . It reinforces the UK commitment to these global initiatives and the UK dedication to addressing pressing global health challenges.
Robust global surveillance capabilities are crucial for early detection of drug-resistant pathogens and tracking their spread. Through the Fleming Fund, the UK improves the ability of countries to identify instances of drug resistance and monitor antimicrobial use.
Case study: the Fleming Fund
The Fleming Fund is the single largest global aid programme for AMR surveillance, supporting up to 25 countries across Asia and Africa to generate, share and use data. It builds partnerships with local governments and organisations, adopting a One Health approach across sectors. The programme invests in strengthening surveillance systems through a portfolio of country and regional grants, global projects and fellowship schemes to highlight why AMR must be a priority and give countries the tools to develop policies and actions to tackle it.
The programme supports governments to produce NAPs, using data to inform the top priorities in their countries. It also supports countries in strengthening national surveillance systems and generating and sharing high quality AMR data. On a local level, the Fleming Fund helps clinicians to improve antimicrobial stewardship and encourages sharing good practice with colleagues in their community, and even in different countries.
In phase 1 alone, the Fleming Fund has:
- produced the most comprehensive analysis of the burden of AMR ever undertaken, with the University of Oxford and Institute for Health Metrics and Evaluation ( IHME )
- supported 22,713 training attendances through regional and country grants
- supported and mentored 7,144 AMR professionals through in-country grants
- launched the UK FAO Reference Centre for AMR which provides LMICs with policy, scientific, and technical expertise
- supported over 240 laboratories across 22 countries
- funded 184 AMR Fellows from LMICs
In August 2023, the Fleming Fund announced £210 million of funding for phase 2 which will bolster the surveillance capacity in up to 25 countries where the threat and burden of AMR is highest with more than 250 laboratories set to be upgraded. This investment includes new genome sequencing technology which will help track bacterial transmission between humans, animals and the environment.
Commitment 9.2 - Access and stewardship
We will support equitable access to, and stewardship of, new and existing quality antimicrobials, evidence-based alternative therapeutics, vaccines and diagnostics, underpinned by internationally recognised antimicrobial classification guidelines and through more resilient and transparent supply chains, improved market access and better alignment of regulatory pathways.
Ensuring that everyone, regardless of their geographical location or socioeconomic status, has access to antimicrobials, vaccines and diagnostics is crucial for tackling AMR and achieving health equity. In LMICs , infections due to lack of antibiotics still kill more people than drug-resistant infections. Action is therefore required to ensure access to the most important first-line antibiotics. This could include advocating for tiered pricing and voluntary licensing. Access complements the main preventive measures such as water, sanitation and hygiene (WASH), IPC , vaccines and wider strategic health initiatives.
As highlighted during the COVID-19 pandemic, secure and resilient supply chains are critical to guaranteeing the availability of essential medical products. Over the next 5 years, the UK will work with partners to improve, strengthen and diversify supply chains for antimicrobials, vaccines and diagnostics, ensuring that these critical tools are accessible.
Equally, stewardship of these essential medical resources is essential to preserve their effectiveness, as described under the ‘Outcome 4 - Antimicrobial stewardship and disposal’ section. The UK supports the adoption of internationally recognised antimicrobial classification guidelines, such as the WHO ’s AWaRe categorisation and the Codex Alimentarius code of practice and guidelines . International standardisation is crucial for harmonising evidence-informed practices and reducing the risk of misuse and overuse of antimicrobials.
It is important to not undervalue existing, older antibiotics, some of which remain effective against certain infections. Using older antibiotics, when appropriate, can help preserve the effectiveness of newer antibiotics and may also be more accessible in low-resource settings.
Case study: the Access to Medicine Foundation ( ATMF )
AMR surveillance programmes are typically co-ordinated by governments and public health authorities. However, surveillance programmes can be scarce in LMICs , especially in sub-Saharan Africa.
The ATMF ’s AMR benchmark identified opportunities for large pharmaceutical companies, which collect critical data, to contribute to the fight against AMR . This data can be used by third-party researchers who cannot access government or public health authority surveillance programmes.
In partnership with the Wellcome Trust, ATMF issued a call to action in 2020 for pharmaceutical companies to share their raw data on an open-access AMR register. Heeding this call to action, several pharmaceutical companies began publicly sharing their raw data for the first time on the AMR register in June 2022, with this action attributed by some companies to the 2020 AMR benchmark. The establishment of this open-access AMR register will facilitate research and surveillance in LMICs who do not have access to government surveillance programmes.
Commitment 9.3 - Antimicrobial use in farming
We will support efforts to optimise the use of antimicrobials in farming globally.
The responsible use of antimicrobials in agriculture is essential for mitigating the development and spread of drug-resistant infections. As the interface between animals, humans and the environment, farming practices play a critical role in shaping the evolution of AMR . It is vital that we advocate for stewardship initiatives and robust animal health systems to bring into balance the excess and access issues within the animal sectors.
In the UK, the use of antibiotics as growth promoters has been banned since 2006. However, this is not the case globally, and it is thought that most of the world’s antibiotics are used in animals, which contributes to the emergence of resistance.
Advocating for responsible farming practices such as improved animal husbandry, biosecurity measures and vaccination that reduce the need for antimicrobials is paramount in addressing AMR .
Supporting international alignment of regulation is crucial for harmonising standards and ensuring that farming practices are consistent across borders. A co-ordinated approach to regulation reduces the risk of AMR spreading through the global movement of food products and livestock.
The UK supports the adoption of internationally agreed best practices, such as the Codex Alimentarius guidelines, that reinforce the importance of global standards in AMR mitigation. These guidelines represent a consensus among nations on responsible antimicrobial use in food production. The adoption ensures that farmers worldwide are following the best practices to minimise the risk of AMR development.
In other parts of the world, inadequate animal health systems and limited access to antimicrobials impacts animal health and the livelihoods of animal keepers, with 1 in 5 people globally depending on production of animals for their income and livelihoods, according to the FAO ’s The State of World Fisheries and Aquaculture 2020 .
Efforts to improve access to essential antimicrobials are vital in the context of animal health. Ensuring that farmers have access to necessary treatments while also advocating for responsible farming practices is a delicate balance. This commitment reflects the UK recognition of the need to strike this balance and aligns with its commitment to equitable access to medical resources.
The current burden of disease in animals due to AMR at the global level remains largely unknown. However, several initiatives are ongoing to estimate it, notably the Global Burden of Animal Diseases led by WOAH and supported by the UK.
Commitment 9.4 - Standards for manufacturing and waste management
We will collaborate internationally and with industry partners to promote the development and use of global standards and certification systems for environmentally responsible antimicrobial manufacturing in human and veterinary medicines.
Applies to the environment.
The manufacturing process for antimicrobials and their raw ingredients, whether for human or veterinary use, and the management of waste generated during production, are drivers of AMR . There is therefore a critical need for responsible production practices to prevent the release of antimicrobial residues into the environment, which can contribute to the development of drug-resistant pathogens.
This could include support of standards such as the antibiotic manufacturing standard developed by the AMR Industry Alliance and the British Standards Institute ( BSI ). This standard, published in 2022, can be used to assess the impact of pharmaceuticals in the environment.
Alongside this, the AMR Industry Alliance and BSI developed an industry certification program , which launched on 6 June 2023. The BSI will act as an independent and impartial assessment body that will enable antibiotic manufacturers to demonstrate that the requirements of the antibiotic manufacturing standard have been satisfied.
The aim of the standard and certification is to serve as a mechanism for antibiotic manufacturers to show evolving good practice. It gives industry the opportunity to demonstrate its ability to self-regulate independent of government regulation.
Responsible manufacturing practices align closely with broader goals of environmental sustainability being adopted in the UK. By advocating for global standards and certification systems, the UK can contribute to the growing global effort to minimise the environmental impact of antimicrobial production, reduce the risk of AMR emergence, and protect both ecosystems and human health.
Commitment 9.5 - Advocacy and engagement
We will drive global advocacy and facilitate collaboration to address AMR by championing action at high-level international forums, strengthening global financing and accountability mechanisms, engaging in bilateral dialogues and negotiations, collaborating with civil society, and identifying and amplifying best practice internationally.
The UK is dedicated to addressing the global challenge of AMR through active diplomacy and engagement. Advocacy at high-level international groups is instrumental in raising the profile of AMR on the global political agenda and catalysing sustainable action. In the near future, this involves using the United Nations Global Assembly ( UNGA ) high-level meeting on AMR in September 2024 to secure the profile of AMR on the international agenda, foster high-level political commitment and secure ambitious, tangible commitments to combat it.
A science-led approach is critical to confronting AMR . At the UNGA high-level meeting, the UK delegation will work with other member states to establish an independent panel for evidence, as recommended by the UN Inter-Agency Coordination Group on AMR in 2019. Such an expert panel could provide member states with regular reports on the science and evidence related to AMR , its impacts and future risks, and recommend options for adaption and mitigation.
Strengthening global financing and accountability mechanisms is essential in the fight against AMR . The UK will work with partners and via multilateral groups to ensure AMR interventions have the funding they need, while promoting transparency and accountability in the use of resources. Where possible, this will happen by harnessing existing funding streams, private finance and capital investments that are already occurring in related fields such as pandemic preparedness, sustainable agriculture and health systems strengthening.
Collaborating with civil society is crucial for fostering a whole-of-society response to AMR . Civil society organisations play a vital role in raising awareness, advocating for policy changes and mobilising public support. The UK is committed to collaborating with civil society in addressing AMR , ensuring that a diverse spectrum of voices are heard.
Identifying and amplifying best practices internationally is essential for shared learning and continuous improvement. Via networks such as TATFAR , WHO networks and the Global Health Security Agenda, the UK can learn from and highlight successful approaches adopted by global partners.
Action can also be driven through engagement with the Quadripartite organisations - the WHO , WOAH , FAO and UNEP . These 4 organisations work to ensure AMR is prioritised in public health, animal health, agriculture and the environment. Through independent and joint initiatives, they drive global action on AMR . One such example is the Quadripartite Antimicrobial Resistance Multi-Stakeholder Partnership Platform . This aims to bring together all sectors and perspectives using a One Health approach, to create a shared vision responding to the need to improve co-ordination of efforts by stakeholders.
This NAP builds on progress made over the past 2 decades to strengthen our understanding of AMR , and of what works to mitigate it. It sets out an ambitious course of action, strengthening the existing UK commitment to:
- prevent infections
- optimise the use of antimicrobials
- invest in research and innovation to address AMR
The activity set out in this plan, combined with meaningful contributions from industry, academia and the public will help to achieve the 9 outcomes set out above. Action taken as part of this plan moves us one step closer to fulfilling the UK’s 20-year vision for AMR .
Progress will be monitored and evaluated to maintain momentum on confronting AMR in a One Health way. The evidence gathered over the next 5 years, including through research, will help strengthen understanding of AMR and lay the foundations for future work on AMR .
AMR is a pervasive threat. The emergence of infections is relentless, while the pipeline for new antibiotics has run dry. Through this national action plan, we set out the challenge to the UK and to other countries to continue our excellent work to confront AMR , to preserve and develop these essential medicines for generations to come and help us address one of the most pressing challenges we face this century.
Appendix A: national action plan development
The NAP has been co-developed by government organisations across the UK. It is informed by consultation with a wide range of stakeholders across sectors, including human healthcare, veterinary medicine, farming, environmental science and academia. Mitigating the threat posed by AMR requires action across all of society. In addition to the policies that governments and international organisations are developing, a willingness and engagement from many different stakeholders, including the research community, the private sector, professionals, civil societies and the general public is needed.
Taking a consultative approach was crucial to identifying and prioritising the most critical actions needed to tackle AMR over the next 5 years. In November 2022, a call for evidence on AMR was launched to inform the development of this NAP . The call for evidence gathered ideas and evidence from 200 respondents. The summary of the results of the call for evidence was published in August 2023.
Feedback gathered on the first NAP (2019 to 2024), including through the call for evidence, indicated that stakeholders outside of government found it difficult to discern government’s priorities (due to the large number of commitments) and to track progress over the 5 years. This NAP has therefore been designed to be more strategic, higher level and accessible, recognising the need to reach people outside of government.
The NAP has been developed in line with the UN IACG AMR framework for action working document (PDF, 1,710KB) . The framework identifies 3 main ways of tackling AMR (which have been adopted for this NAP , alongside the fourth theme: being a good global partner) and 15 different ‘content areas’ that describe what needs to be done. The IACG framework points to 5 ‘levers’ that describe how the content areas can be addressed and 3 ‘enablers’, describing the preconditions necessary to apply the levers successfully.
This plan aims to provide strategic direction to the work from across different government departments, public bodies and services across the UK to tackle AMR . It aligns with the roadmap on antimicrobial resistance for the WHO European region (ratified in 2023) and the WHO global action plan on AMR .
In light of learning from the first NAP , this NAP was developed in line with a ‘theory of change model’. This approach aims to balance ambition with realism about the scale of this challenge. The link between each of the outcomes and its underpinning commitments has been tested through extensive stakeholder engagement and expert review.
To reach the ambition of the outcomes over the next 5 years requires action across spheres. Spreading resources too thinly could limit our ability to achieve meaningful change. Therefore, this plan has been designed using a risk-based approach, targeting interventions where the evidence for impact is strongest. This approach includes supporting the necessary research to address the gaps where there is little evidence about which interventions work. This approach will have the highest impact and represents the best value for money. The specific activity undertaken to support each of the commitments in this NAP is subject to ongoing commitment to funding across government organisations.
Other action across sectors also has significant potential to reduce the spread of AMR . This includes actions on a systemic level such as increasing vaccination coverage, reducing overcrowding, increasing access to clean water and sanitation, and reducing pollution into waterways. There are existing government commitments (from UK government and the devolved governments) in several of these areas (for example, the Life Sciences Vision , FCDO’s International development strategy , and Defra ’s Plan for water ) and where that is the case, those commitments have not been duplicated in this document. Where appropriate, those documents have been referenced throughout this NAP .
While some activity in the NAP is specifically focused on reducing AMR (for example, IPC measures or use of antimicrobials across sectors) other measures pursue other objectives (for example, improving animal health or reducing the incidence of infectious diseases more broadly).
The 30 commitments in the NAP are underpinned by deliverables assigned and owned by delivery partners across government. A short report summarising progress made against the NAP will be published annually. Given the complexity of AMR , ensuring there are clear roles and responsibilities for all the partners involved in delivering the NAP is essential.
The NAP will be supported by a robust governance system, including monitoring and evaluation of progress. Oversight will be provided by a UK-wide, intersectoral AMR strategy board. In turn, this is informed by appropriate governance structures in England, Scotland, Wales and Northern Ireland that will ensure the delivery and monitoring of plans.
Advice will continue to be sought from expert advisers to government, including, but not limited to, the Advisory Committee on Antimicrobial Prescribing, Resistance and Healthcare Associated Infection (APRHAI) and the Advisory Committee on the Microbiological Safety of Food (ACMSF) and equivalent advisory structures in Scotland Wales and Northern Ireland. In addition, engagement with external stakeholders involved in tackling AMR can be gathered to inform government policy.
Appendix B: human health targets
The human health targets that have been included in this NAP were developed by short-term expert working groups, with representatives from across the UK. The targets have been informed by reviewing the evidence-base and learning from the measurable ambitions that were set out in the first NAP .
Each of the targets will be subject to an annual review, which will consider a range of factors to assess progress, with the potential to revise the targets if deemed appropriate and if agreed to by the UK-wide strategy board.
Target 1a: by 2029, we aim to prevent any increase in a specified set of drug-resistant infections in humans from the 2019 to 2020 financial year ( FY ) baseline.
Data will be collected from England, Scotland, Wales and Northern Ireland, with aggregate data used to generate the high-level UK metric. Data will be presented in the form of counts for the UK.
The specified set of drug-resistant infections can be found in annexe table 2.3 of the ESPAUR report 2022 to 2023: annexe .
E. coli is the causative pathogen of approximately 80% of all AMR bloodstream infections in the UK. Despite reductions in the numbers of E. coli bloodstream infection cases seen during the COVID-19 pandemic, case numbers have subsequently been rising annually. Driving down infections, the ambition of both targets 1a and 1b, should lead to reductions in prescribing and the associated risk of development of AMR .
The burden of AMR infections will be estimated using an adapted methodology developed by Cassini and others (see Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: a population-level modelling analysis . The Lancet Infectious Diseases, 19, 1, pages 56 to 66 (2018)) for a UK specific measure of AMR burden - see the ESPAUR report 2022 to 2023 .
Target 1b: by 2029, we aim to prevent any increase in Gram-negative bloodstream infections in humans from the 2019 to 2020 financial year baseline.
As for target 1a, data will be collected from England, Scotland, Wales and Northern Ireland, with aggregate data used to generate the high-level UK metric. Data will be presented in the form of counts and rates per 100,000 population for the UK.
While this target appears more conservative than the measurable ambition in the first (2019 to 2024) NAP , it has been assessed as challenging in the context of an ageing population with increasing comorbidities. The incidence of Gram-negative bloodstream infections ( GNBSIs ) is projected to increase and there is limited evidence in the literature for interventions which work to prevent GNBSIs .
Given this projected rise in incidence of GNBSIs by 2029, the target would seek to achieve a 17.2% (of 11,086) reduction in incidence, simply to remain at 2019 to 2020 levels.
Target 2a: by 2029, we aim to increase UK public and healthcare professionals’ knowledge on AMR by 10%, using 2018 and 2019 baselines, respectively.
A questionnaire-based assessment of knowledge regarding AMR will be used to assess improvements. Questionnaire data collected on healthcare professionals by a European Centre for Disease Prevention and Control ( ECDC ) project in 2019 and data collected on the public via the Eurobarometer in 2018 will be used as a baseline measure of knowledge. To measure improvements from baseline in levels of healthcare professionals’ knowledge the same knowledge questions will be repeated as part of questionnaires. For the public, questions from the Eurobarometer questionnaire can be incorporated in public surveys.
Knowledge questions from the ECDC questionnaire and Eurobarometer questionnaire will be used as a basis for surveys for healthcare professionals and public respectively.
The Eurobarometer data provides the most recent data on public knowledge attitudes and behaviours, which is representative across the UK. From Eurobarometer, UK data showed 29% of UK respondents answered all 4 questions correctly, with the overall average number of correct answers was 2.8 out of 4, compared to 43% (3.1 out of 4) for Finland and Sweden. Similarly for healthcare professionals the questionnaire conducted by ECDC in 2019 provides the most recent data for healthcare professionals across the UK. The UK data in 2019 showed that 59% of UK respondents were able to answer all 7 questions correctly. This was similar to the EU average of 58% with Croatia having the highest percentage at 73%. Data from these questionnaires will be used as a baseline with a 10% improvement in knowledge deemed achievable based on the current levels of knowledge seen and the levels of knowledge achieved within other EU countries. A 10% improvement would bring the UK in line with the highest scoring EU countries.
Although knowledge does not automatically lead to behaviour change, it’s an important first step. Including targets focused on behavioural outcomes will allow a deeper understanding of what knowledge and attitudes drive behaviour change, therefore allowing a more targeted public messaging approach for public engagement. Improving knowledge of healthcare professionals alongside increasing public knowledge is likely to be important when looking to facilitate behaviour change. Improving knowledge of both the public and healthcare workers may lead to improvements in antibiotic prescribing and consumption.
Target 4a: by 2029, we aim to reduce total antibiotic use in human populations by 5% from the 2019 baseline.
The metric for this target is defined daily doses ( DDDs ) per 1,000 inhabitants per day (DID or defined daily doses per inhabitant per day). Use of this high-level metric facilitates international benchmarking using a common definition of numerator and denominator.
A comprehensive literature review and expert consensus process, to identify optimal metrics for measuring antimicrobial consumption in hospital and outpatient settings, was conducted by the Innovative Medicines Initiative’s Driving Reinvestment in Research and Development and Responsible Antibiotic Use ( DRIVE-AB ) project. The proposed metrics align with DRIVE-AB recommendations .
The development of this target was informed by progress made and surveillance data collected during the first NAP .
Setting improvement ambitions at a UK level, such as percentage reduction targets, may not be directly applicable at regional and local settings. This is due to variation in past and current antibiotic usage levels and variation in infectious disease incidence associated with legitimate clinical demand for antimicrobials.
Target 4b: by 2029, we aim to achieve 70% of total use of antibiotics from the Access category (new UK category) across the human healthcare system.
Data will be provided by UKHSA , National Services Scotland, Public Health Wales and the Public Health Agency (Northern Ireland). Data is collected in respective prescribing and/or dispensing surveillance systems. A system is also in place to share this data to combine and form UK-level data.
The WHO ’s AWaRe categorisation for antimicrobials includes Access, Watch and Reserve categories which allows for evaluation and monitoring of use according to spectrum of activity and potential to drive resistance.
The UK has endorsed the Muscat ministerial manifesto which includes the global goal of ensuring ‘Access’ group antibiotics represent at least 60% of overall consumption in humans by 2030. The WHO has defined a target that at least 60% of human antibiotic use at the country level should be Access antibiotics. Total prescribing DDDs are being measured already.
Achieving 70% of total use of antibiotics from the new UK Access category is an ambitious task. The EU Commission recommends that, by 2030, at least 65% of the total consumption of antibiotics in humans belongs to the Access group of antibiotics ( WHO 2021 categories) in EU member states and the UK will be reporting against the UK-modified AWaRe classification which is more stringent than the WHO classification.
Budd and others (see Budd E and others, Adaptation of the WHO Essential Medicines List for national antibiotic stewardship policy in England: being AWaRe . Journal of Antimicrobial Chemotherapy, 74, 11, pages 3384 to 3389 (2019)) showed that Access antibiotics accounted for 60.9% of prescribing across all English healthcare sectors in 2016 (current UK AWaRe categories).
Appendix C: top 10 research priorities example questions
The description of the top 10 research priorities can be found in the ‘Outcome 7 - Using information for action’ section.
As the evidence base for AMR increases, there are more nuanced questions to be answered. It is critical to consider AMR in the context of other challenges, including climate change. Reducing AMR in sustainable ways that do not incur adverse unintended consequences is a priority.
The UK academic community has been a part of world-leading research on AMR . It has developed some of the most comprehensive data, surveillance and genomics capabilities in the world, which must be harnessed to underpin research and policy across sectors.
Priority setting in research is a necessary part of guiding collective policy-generation, investment in research and evaluation, implementation and delivery of actions to address AMR across sectors. The top 10 reflects a snapshot in time, showing what policy makers viewed as priorities at a particular point, inevitably influenced by the current context, wider priority agendas, and needs of the time. For this reason, the top 10 will be reviewed and updated as needed during the 5-year NAP period.
The following sub questions are intended to be an illustrative selection, rather than a comprehensive list, of the sorts of research questions which could be considered underneath each of the top 10 research priorities.
Example questions include:
- what is the economic cost of leaving AMR unchecked across the healthcare, agricultural and veterinary systems?
- how can we define the true value of a vaccine, alternative therapeutic or precision tool to reduce harm that would result from an untreatable, resistant infection?
- what are the co-benefits and trade-offs associated with the impact of different actions to tackle AMR within the agriculture sector, such as impacts on livestock productivity, crop protection, food yields and economic impacts in different animal husbandry systems?
- which socioeconomic factors (including age, sex, ethnicity, deprivation, living conditions, education, employment and so on) are associated with an increased risk of transmission, exposure, antimicrobial use, antimicrobial resistance and clinical outcomes?
- how does access to infection diagnostics differ by patient groups and what approaches should be prioritised to meet access needs?
- what works to reduce inequalities in infections, drug-resistant infections and sepsis burden across primary, secondary and community healthcare settings and how, for whom and in what situations?
- what are the current patterns of prescriber and patient knowledge, attitudes and practices relating to antibiotic prescription and use across population groups and geographic locations?
- what are the most important messages related to AMR to communicate to the public, including risks of exposure to resistant pathogens through antibiotic use and transmission risk between humans, companion animals, water and recreational activities?
- what are the most effective and cost-effective interventions to build public trust, reduce misinformation, communicate risks related to antibiotic exposure, communicate methods of self-care and reduce antibiotic seeking behaviours across population groups?
- what are the risks associated with use of antibiotics and antifungals use on crops, particularly in LMICs , and the ‘downstream’ impact on the environment, humans and animals?
- how can water and sanitation engineering solutions be developed to mitigate the environmental spread of antibiotic-resistant bacteria, considering local water treatment practices and infrastructure limitations in international settings?
- in resource-limited settings, what approaches can be employed to develop low-cost, point-of-care diagnostic tools that enable rapid and accurate identification of bacterial infections and their antibiotic resistance profiles?
- what are the other major drivers of resistance beyond the use of antimicrobials (for example, biocides, biofilms, metals, manures and slurries, sewage sludge and industrial organic wastes, chemicals, and wastewater processes in the environment)?
- how have reductions in the use of antibiotics in food-producing animals affected antibiotic resistance in people and animals?
- what is the reservoir of carriage of infectious agents and AMR in the healthy population and natural flow of resistance genes, considering a range of priority AMR pathogens, age and seasonality?
- what are the basic effects of exposure to antimicrobials, antimicrobial products and multi-purpose antimicrobials on hosts and the microbiome (human or animal), including impacts on future susceptibility to infection and sepsis?
- what is the impact of the way staff and patients move through buildings, services and the community on spread of resistant pathogens, and how can this knowledge be used to create design-led interventions to mitigate spread?
- how can effective domestic wastewater treatment, biosolid management, pharmaceutical stewardship and food waste disposal practices be used to reduce and prevent the spread of AMR in the environment in a harmonious and sustainable way?
- building and using understanding of how Gram-negative pathogens transmit in the built environment, how can we design buildings and vehicles to reduce transmission via water, air or contact surfaces (for example, environmental decontamination, ventilation, waterless systems, sinks and design of water waste systems, use of probiotic materials and antibiofilm)?
- what are the most optimal, cost-effective interventions for infection outbreak management across human healthcare settings where there is high staff turnover, competing priorities and limited resources (including long-term care facilities)?
- what is the optimal dose regimen, route of administration and duration of antibiotic therapy across antibiotics, syndromes, confirmed infections (including sepsis) and patient characteristics to maximise clinical outcomes and reduce selection of resistance?
- at what point along the healthcare pathway do diagnostic tools, including patient-led diagnostics, deliver the highest impact and return on investment, and when should they be prioritised in a resource-limited setting?
- what are the most safe and effective scenarios in which local teams (including doctors, pharmacists and dentists) can use electronic prescribing systems, ‘automatic stops,’ and clinical decision support tools to ensure risk stratification and targeted dosage of antimicrobials in different patient groups?
- when is it safe and effective to use non-pharmaceutical and/or non-antimicrobial methods at home (interventions, lifestyle factors and behaviours that is, hydration, nutrition, natural products, increased mobility, hygiene practices) to prevent common syndromes of infection, antimicrobial exposure and clinical outcomes?
- what are safe and effective alternatives to antibiotics in animals and how can farmers be supported to use non-antimicrobial medicines in agricultural practices?
- how to have culturally appropriate patient-to-healthcare professional interactions that influence patient expectations and awareness of antibiotics, risks of AMR and use of self-care? (These interactions would be in different settings including remote consultations, e-consults, urgent care settings, acute respiratory infection (ARI) hubs, community pharmacies and so on)
- how can we de-risk the early-stage development and evaluation of new therapeutic agents and vaccines to support their translation into clinical studies and encourage investment?
- how can we learn from and apply alternative payment models to incentivise development and implementation of new therapies, vaccines and diagnostics?
- how could we provide a framework to support the development and evaluation of a wider range of therapeutic and diagnostic modalities - including but not limited to new vaccines, antibody-based therapies, bacteriophage, host-directed therapy, microbiome modulators, biofilm disruptors and approaches that overcome resistance (for example, efflux resistance breakers, membrane permeabilities)?
- what are the enabling factors for ensuring confidence, acceptance and uptake of new products from the public and in different healthcare and veterinary settings (diagnostics, vaccines and alternative therapies for bacterial, fungal and viral infections) once they come to market?
- what are the blockers and enablers in mobilising the knowledge generated via research through to policies and practice which have an impact on reducing infections, drug-resistant infections and antimicrobial use?
- where should discovery and implementation of new products (that is, vaccines, therapies, diagnostics) take a One Health lens and where can existing products already used in one sector safely be used in another?
Appendix D: list of commitments
1.1 - informed interventions, 1.2 - the built environment, 1.3 - waste minimisation and effective waste management, 2.1 - public awareness and campaigns, 2.2 - use of educational settings, 2.3 - engagement guide, 3.1 - optimising surveillance of infections and outbreaks, and response, 3.2 - optimising surveillance to inform interventions, 4.1 - clinical decision support, 4.2 - appropriate prescribing and disposal, 4.3 - use of behavioural interventions, 5.1 - health and social care training, 5.2 - health and social care workforce, 5.3 - health and social care governance, 5.4 - veterinary workforce knowledge and skills, 5.5 - systems to support animal health, 6.1 - amr solutions, 6.2 - subscription models, 6.3 - overcoming market barriers, 6.4 - improvement and adoption, 7.1 - evidence generation and use, 7.2 - research networks, 8.1 - data on health inequalities, 8.2 - toolkit for addressing health inequalities, 8.3 - interventions to reduce health inequalities, 9.1 - prevention and preparedness, 9.2 - access and stewardship, 9.3 - antimicrobial use in farming, 9.4 - standards for manufacturing and waste management, 9.5 - advocacy and engagement, appendix e: glossary, antimicrobial.
A drug that selectively destroys or inhibits the growth of microorganisms. Examples include antibiotics (also known as antibacterials) antiviral and antifungal agents.
Antimicrobial stewardship ( AMS )
An organisational or healthcare-system-wide approach to promoting and monitoring judicious use of antimicrobials to preserve their future effectiveness.
AWaRe categorisation
A tool for monitoring antibiotic consumption, defining targets and monitoring the effects of stewardship policies that aim to optimise antibiotic use and curb antimicrobial resistance.
Bacteraemia
The presence of bacteria in the bloodstream.
Bacteriophage (phages)
A group of viruses that infect specific bacteria, usually causing their disintegration or dissolution.
Biosecurity
The prevention of disease-causing agents entering or leaving any place where they can pose a risk to farm animals, other animals, humans or the safety and quality of a food product.
Broad-spectrum antibiotics
These are drugs effective against a wide range of bacteria. For example, meropenem is a broad-spectrum antibacterial. Their use needs to be limited to resistant infections because they tend to increase the risk of resistance in other bacteria.
Codex Alimentarius guidelines
A collection of internationally recognised standards, codes of practice, guidelines, and other recommendations published by the Food and Agriculture Organization of the United Nations relating to food, food production, food labelling and food safety.
Critically important antibiotics ( CIAs )
Antibiotics identified by the World Health Organization as critically important for human health and their use needs to be restricted, especially in the veterinary sector. In the UK, we use the European Medical Agency definition of the CIAs . There are 3 classes of highest priority CIAs to which the animal industry applies restrictions.
Defined daily doses ( DDDs )
A statistical measure of drug consumption, defined by the World Health Organization Collaborating Centre for Drug Statistics Methodology, and is the average dose prescribed according to a representative sample of prescriptions.
Epidemiology
The study and analysis of the distribution, patterns and determinants of health and disease conditions in a defined population.
Eurobarometer
A collection of cross-country public opinion surveys conducted regularly on behalf of the EU Institutions since 1974.
The G20 (or Group of 20) is an international forum for the governments and central bank governors from 19 countries (Argentina, Australia, Brazil, Canada, China, France, Germany, India, Indonesia, Italy, Japan, Republic of Korea, Mexico, Russia, Saudi Arabia, South Africa, Türkiye, UK and USA) and 2 regional bodies: the EU and the African Union.
The Group of 7 (G7) is an international forum for the governments and heads of state of Canada, France, Germany, Italy, Japan, UK and USA. The EU is also represented at G7 meetings.
Gram-negative bacteria
Those bacteria that do not retain crystal violet dye in the Gram-staining procedure. They can cause many types of infection and include E. coli and Pseudomonas aeruginosa.
Gram-positive bacteria
Those bacteria that are stained dark blue or violet in the Gram-staining procedure. They include Staphylococcus aureus and Clostridium difficile.
Healthcare associated infections ( HCAIs )
Infections associated with the provision of healthcare in either a hospital or community setting.
Herd immunity
The indirect protection from an infectious disease that happens when a population is immune either through vaccination or immunity developed through previous infection.
Infection prevention and control ( IPC )
The use of safe practices and ways of working that help to prevent or reduce infections within healthcare settings.
Low and middle income countries ( LMICs )
As included at any time in the OECD Development Assistance Committee (DAC) list - a list of all countries and territories eligible to receive ODA . These consist of all low and middle income countries based on gross national income (GNI) per capita as published by the World Bank, except for G8 members, EU members and countries with a firm date for entry into the EU. The list also includes all the least developed countries (LDCs) as defined by the United Nations.
A type of bacteria that is resistant to several antibiotics.
One Health approach
Collaborative multi-disciplinary work at local, national and global levels to attain optimal health for people, animals and the environment.
Outpatient parenteral antimicrobial therapy ( OPAT )
An OPAT team manage the delivery of intravenous (into the vein or IV) antibiotics to patients who are medically stable, within their own homes.
Pandemic preparedness
The continuous process of planning, exercising, revising and translating into action national and sub-national pandemic preparedness and response plans.
An infectious agent (bug or germ), a microorganism such as a virus, bacterium or fungus that causes disease in its host.
Primary care
Services provided by GP practices, dental practices, community pharmacies and high street optometrists.
Secondary care
Covers acute healthcare, either elective care (planned specialist medical care or surgery, usually following referral) or emergency care.
Is a serious complication of an infection. Without quick treatment, sepsis can lead to multiple organ failure and death.
Sustainable development goals ( SDGs )
A set of 17 goals adopted by the United Nations in 2015 as a universal call to action to end poverty, protect the planet and ensure that by 2030 all people enjoy peace and prosperity.
Theory of change model
A model that explains how a given intervention, or set of interventions, are expected to lead to a specific development change drawing on a causal analysis based on available evidence.
A vaccine is a biological preparation that provides active acquired immunity to a particular infectious or malignant disease.
Whole genome sequencing
The process of determining the entirety, or nearly the entirety, of the DNA sequence of an organism’s genome at a single time.
Appendix F: abbreviations
This will only be in the PDF version
Is this page useful?
- Yes this page is useful
- No this page is not useful
Help us improve GOV.UK
Don’t include personal or financial information like your National Insurance number or credit card details.
To help us improve GOV.UK, we’d like to know more about your visit today. Please fill in this survey .
Exclusive: Corporate climate watchdog document deems carbon offsets largely ineffective
- Medium Text

- Company Amazon.com Inc Follow
- Company Microsoft Corp Follow
- Company Salesforce Inc Follow
POLICING THE QUALITY
Sign up here.
Reporting by Virginia Furness in London; Editing by Greg Roumeliotis and David Gregorio
Our Standards: The Thomson Reuters Trust Principles. New Tab , opens new tab
U.S regulators asked LNG exporter Venture Global LNG to update its emissions analysis for its proposed Calcasieu Pass 2 LNG export project in Louisiana, according to a letter sent on Wednesday.

Sustainability Chevron

Brazil flooding will take weeks to subside, experts warn
Brazil's southernmost state capital may suffer severe flooding for weeks to come, experts warn, compounding the struggles of half a million people forced to abandon their inundated homes.

The Federal Register
The daily journal of the united states government, request access.
Due to aggressive automated scraping of FederalRegister.gov and eCFR.gov, programmatic access to these sites is limited to access to our extensive developer APIs.
If you are human user receiving this message, we can add your IP address to a set of IPs that can access FederalRegister.gov & eCFR.gov; complete the CAPTCHA (bot test) below and click "Request Access". This process will be necessary for each IP address you wish to access the site from, requests are valid for approximately one quarter (three months) after which the process may need to be repeated.
An official website of the United States government.
If you want to request a wider IP range, first request access for your current IP, and then use the "Site Feedback" button found in the lower left-hand side to make the request.
IMAGES
VIDEO
COMMENTS
Introduction. The Action Plan is a guide to planning for change, and it describes: . A clear picture of where you are currently, where you are going, and where you want to be in 3-5 years. How you are going to get there. Who and what are involved. Elements of the Action Plan. Goal(s) Objectives.
Start by defining your project's purpose. Identify what your project aims to accomplish and what you are researching. Remember to use clear language. Thinking about the project's purpose will help you set realistic goals and inform how you divide tasks and assign responsibilities.
Write about a page a day. Work backwards from at least two weeks before the submission date to calculate when you need to start your writing. (A page is about 500 words, so, for example, if your dissertation is 15,000 words long, you will need at least 30 days to do the writing.) Leave two or more weeks at the end for editing and proofreading.
1. Define the project purpose. The first step to creating a research plan for your project is to define why and what you're researching. Regardless of whether you're working with a team or alone, understanding the project's purpose can help you better define project goals.
Stage 1: Plan. For an action research project to go well, the researcher needs to plan it well. After coming up with an educational research topic or question after a research study, the first step is to develop an action plan to guide the research process. The research design aims to address the study's question.
When putting your research plan together, answering the what, when and who questions will guide your thinking as you design your research ... you aren't solely the researcher; you're also a participant. While you might initially think of action research as a way to collect information from others, a significant aspect of it involves self ...
This brings us back to the essential steps of action research: identifying the problem, devising an action plan, implementing the plan, and finally, observing and reflecting upon the process. Your action research report should comprise all of these essential steps. Feldman and Weiss (n.d.) summarized them as five structural elements, which do ...
Research proposal examples. Writing a research proposal can be quite challenging, but a good starting point could be to look at some examples. We've included a few for you below. Example research proposal #1: "A Conceptual Framework for Scheduling Constraint Management".
Types of action research. There are 2 common types of action research: participatory action research and practical action research. Participatory action research emphasizes that participants should be members of the community being studied, empowering those directly affected by outcomes of said research. In this method, participants are effectively co-researchers, with their lived experiences ...
Plan and implement Action Research projects in their own schools and classrooms. Assess and share the results of their own Action Research with colleagues. Learn to improve instructional decision-making through a continuous reflection point of view. Real-life examples of Action Research projects
Thus, action research is often a cyclical process. The action research report that you write is based on this process. Typically, an action research report is written in the same way as you would write an original research article. However, you need to ensure that your report has the following components: The context or background.
Action research (AR) is a methodical process of self-inquiry accomplished by practitioners to unravel work-related problems. This paper analyzed the action research reports (ARRs) in terms of ...
The ultimate outcome of Action Research is to create a plan of action using the research findings to inform future educational practice. A Plan of Action is not meant to be a one-size fits all plan. ... (Ed.), Resolving social conflicts: Selected papers on group dynamics (compiled in 1948). Harper and Row. Mertler, C. A. (Ed.). (2019). The ...
By tracing action research literature across four subject areas—English language arts (ELA), mathematics, science, and the social studies—it reflects contemporary emphasis on these subjects in the public school "core" curriculum and professional development literature (Brady, 2010) and provides a basis for comparative analysis.The results contribute to the scholarship of teaching ...
You may also see quality plan examples & samples. We will be discussing below the importance of research action plans to each sector that was mentioned. 1. Business. This is where research action plans are constantly created and used. Business entities, specifically companies, conduct research for various reasons.
In this paper, the authors discuss some of the concerns and challenges underlying the conduct of action. research studies, and consider reasons for these concerns. They identify three elements ...
Step 7: Developing an Action Plan. Once the data have been analyzed and the results of the analysis interpreted, the next step in the action research process is the development of an action plan. This is really the ultimate goal of any action research study—it is the "action" part of action research.
Action Research Work Plan and Timelines . ... the aim of this paper is to provide a clear link between the theoretical principles of constructivism, the construction of technology-supported ...
EDCC 551: Action Research in Educational Settings (3 credits) Course Description: This course is designed to give an overview of action research, particularly action research that is conducted within educational settings. Emphasis is placed upon gaining an understanding of the difference
Action Research . Dissertation Outline . CHAPTER 1 INTRODUCTION (Statement of the problem and its significance; brief description of your specific study - i.e., research questions and design) What is your study about - i.e., what problem(s) is your study going to address, how,
An action plan is a detailed outline that breaks down the steps necessary to achieve a specific goal. Here are the typical components of an action plan. 1. Objective or Goal. The cornerstone of your action plan is the objective or goal. This should be a clear and concise statement outlining the desired outcome or result.
This paper intends to propose an action research plan and attempts to inquire into the educational situation, understand the students' skills and their situation better and act to improve both. ... Research Plan 5.1 Intervention First, I would like to require my students to listen to English attentively in and out of class and give them ...
Fellowships foster cutting-edge research with grants of $3,000 and up. Book Prizes recognize achievements in recent bibliographical scholarship. Events all year, including our annual meeting, bring bibliographers together to learn and build community. Peer-reviewed scholarship makes the latest research accessible to readers around the world.
Central to our strategy is the effort to build digital solidarity - working together to offer mutual assistance to the victims of malicious cyber activity and other digital harms; assist partners - especially emerging economies - in deploying safe, secure, resilient, and sustainable technologies to advance their development goals; and builds strong and inclusive innovation economies that ...
The biggest hit has come to Wiley, a 217-year-old publisher based in Hoboken, N.J., which Tuesday will announce that it is closing 19 journals, some of which were infected by large-scale research ...
The first national action plan. The first 5-year national action plan for antimicrobial resistance built a secure basis for the change required to fulfil the 20-year vision for AMR, with ...
Climate action planning continues to accelerate rapidly across the globe as communities seek to prepare to thrive in an uncertain future. Climate action planning is a particularly contentious and complex topic in the southern United States, however, because of significant economic reliance on industries that contribute substantially to greenhouse gas emissions, and due to a complicated ...
Staff at an influential corporate climate action group whose board announced a plan to allow companies to offset greenhouse gas emissions from their supply chain with carbon credits has now found ...
The aims and objectives of this action research are to: To improve students' active participation in classroom teaching and learning. To explore the reasons why students hardly take part in ...
Request for Comment on the NIH-Wide SGM Health Research Strategic Plan FY26—FY30: NIH is developing a strategic plan to advance SGM research in FY26-FY30. This RFI invites input from interested parties throughout the scientific research, advocacy, and clinical practice communities, federal partners, those employed by the Department of Health ...