- Subject List
- Take a Tour
- For Authors
- Subscriber Services
- Publications
- African American Studies
- African Studies
- American Literature
- Anthropology
- Architecture Planning and Preservation
- Art History
- Atlantic History
- Biblical Studies
- British and Irish Literature
- Childhood Studies
- Chinese Studies
- Cinema and Media Studies
- Communication
- Criminology
- Environmental Science
- Evolutionary Biology
- International Law
- International Relations
- Islamic Studies
- Jewish Studies
- Latin American Studies
- Latino Studies
- Linguistics
- Literary and Critical Theory
- Medieval Studies
- Military History
- Political Science
- Public Health
- Renaissance and Reformation
- Social Work
- Urban Studies
- Victorian Literature
- Browse All Subjects

How to Subscribe
- Free Trials
In This Article Expand or collapse the "in this article" section Psychology of Stress and Coping
Introduction, definitions of stress.
- Main Theories of Stress
- Assessment of Stress
- Relationships
- Work-Related
- Environmental
- Cultural Perspectives on Stress
- Consequences of Stress
- Coping: Definitions and Main Theories
- Classifying Coping: Coping Styles and Strategies
- Assessment of Coping
- Coping Process
- Coping Functions and Goals
- Coping Resources
- Culture and Coping
- Theories and General Reviews
- Specific Interventions
Related Articles Expand or collapse the "related articles" section about
About related articles close popup.
Lorem Ipsum Sit Dolor Amet
Vestibulum ante ipsum primis in faucibus orci luctus et ultrices posuere cubilia Curae; Aliquam ligula odio, euismod ut aliquam et, vestibulum nec risus. Nulla viverra, arcu et iaculis consequat, justo diam ornare tellus, semper ultrices tellus nunc eu tellus.
- Health Psychology
- Measurement in Health Psychology Research and Practice
- Mindfulness
- Occupational Health Psychology
- Personality and Health
- Posttraumatic Stress Disorder (PTSD)
- Psychoneuroimmunology
- Rehabilitation Psychology
- Trauma Psychology
Other Subject Areas
Forthcoming articles expand or collapse the "forthcoming articles" section.
- Data Visualization
- Remote Work
- Workforce Training Evaluation
- Find more forthcoming articles...
- Export Citations
- Share This Facebook LinkedIn Twitter
Psychology of Stress and Coping by Angela R. Wendorf , Amanda M. Brouwer LAST REVIEWED: 11 January 2018 LAST MODIFIED: 11 January 2018 DOI: 10.1093/obo/9780199828340-0203
The psychology of stress and coping has been a prominent topic of scientific study and of popular interest over the last century. Applying the study of the mind and behavior to a concept such as stress and coping has led to an evolving definition of stress, more research on its physical, psychological and social effects, and the development of comprehensive ways in which individuals cope with stress. Our understanding of how individuals cope with stress has advanced to include perception of one’s ability to cope, approach to coping, assessment and utilization of coping resources available, and enacting of strategies. We review the psychology of stress and coping as it presents itself in the current evolving research and theoretical development, documenting historical, theoretical, and methodological perspectives on stress and coping. In so doing, we will provide sources and commentary on the definitions of stress, main theories of stress, categories of stressors, consequences of stress, definitions of coping, main theories of coping, coping styles and strategies, assessment of coping, descriptions of coping processes, coping functions and goals, coping resources, and coping and stress management interventions. We would like to acknowledge Samantha Lee for her assistance with this project.
Stress, although universally experienced, is defined differently depending on theoretical context. The definition of stress has evolved in accordance with research and theory development. Cannon 1929 was one of the first studies to describe stress within a physiological context noting that stress is the body’s nonspecific response to stimuli in an attempt to restore homeostasis. Other theorists challenged the notion that stress was only a stimulus-response system rooted in physiology and went on identify stress as a process that requires appraisal of the stressor and the resources available to meet the demands of the stressor ( Lazarus 1966 ). The introduction of this definition expanded the study of stress in a way that acknowledged the psychological and social contexts in addition to the physiological context of stress. McGrath 1970 , for example, summarizes the stress research in a way that defines stress from the context of imbalance. Stress is experienced as a result of an imbalance between the demands put forth by one’s environmental context and the degree to which one is able to meet those demands. Other works such as Kaplan 1983 have further elaborated on the psychological context of stress to define stress in terms of the psychological and behavioral consequences that result from the inability of one distance oneself from undesirable circumstances. Elliot and Eisdorfer 1982 approaches the task of defining stress by categorizing the types of stressors relative to the time they are experienced. Here a stimulus–response definition is endorsed but modified in the degree to which the stressor is acute or chronic and intermittent or in sequence. Mason 1975 proposes that a single term of stress is too vague and suggested that there be distinctions based on external challenges (i.e., stressors), psychophysiological responses (i.e., strain) and the interaction of the stimulus, responses, and appraisal processes (i.e., stress). To sum the diverse definitions of stress and the degree to which these definitions are rooted within the trajectory of research and theory development, Fink 2016 is a good overview of the different definitions of stress and how it is related to psychological experiences like fear and anxiety.
Cannon, W. B. 1929. Bodily changes in pain, hunger, fear, and rage . Oxford: Appleton.
Cannon’s book provides a comprehensive overview of his physiological work wherein he discovered changes in the sympathetic nervous system and endocrine system in response to stress. Consequently, he identifies stress as a change in the body’s homeostasis and the stress response is an attempt to restore that homeostatic state.
Elliot, G., and C. Eisdorfer. 1982. Conceptual issues in stress research. In Stress and human health: Analysis and implications of research a study by the Institute of Medicine National Academy of Sciences . Edited by G. Elliot and C. Eisdorfer, 11–24. New York: Springer.
In an analysis of research, supported by the Institute of Medicine and the National Academy of Sciences, Elliot and Eisdorfer attempt to unify the diverse perspectives of stress into a framework that represents three primary elements: the activator, the reaction and the consequence. They define stress using this framework and noting that many mediators that can alter the sequence.
Fink, G. 2016. Stress, definitions, mechanisms, and effects outlined: Lessons from anxiety. In Stress: Concepts, cognition, emotion, and behavior . Edited by G. Fink and G. Fink, 3–11. San Diego, CA: Elsevier Academic Press.
DOI: 10.1016/B978-0-12-800951-2.00001-7
An overview of several different definitions of stress. The author highlights the relevancy of Hans Selys’s definition that stress is a nonspecific response of the body and how this founding definition fits in with the evolving perspectives of stress given the advancement of research in this field. Fink also describes stress relative to fear and anxiety and discusses how they are linked.
Kaplan, H. B. 1983. Psychological distress in sociological context: Toward a general theory of psychosocial stress. In Psychosocial stress: Trends in theory and research . Edited by H. B. Kaplan, 195–264. New York: Academic Press.
DOI: 10.1016/B978-0-12-397560-7.50010-6
Kaplan presents a model specifically for psychosocial stress. He proposes that stress is experienced when an individual is unable to obtain a desired outcome. The unfulfilled need is then the source of distress. Kaplan supports the psychological role in the stress process noting that the cognitive interpretation of the separation of a desired outcome and one’s inability to obtain it is the source of one’s distress.
Lazarus, R. S. 1966. Psychological stress and the coping process . New York: McGraw-Hill.
Lazarus defines stress as a process wherein the demands of one’s environment exceed the resources available for one to deal with those demands. Although the entire book is valuable to understanding the theory proposed by Lazarus, in the first chapter (pp. 1–29), he specifies the definition of stress from a psychological perspective and defines core principles that differentiate his theory from others.
Mason, J. W. 1975. A historical view of the stress field. Journal of Human Stress 1:22–36.
DOI: 10.1080/0097840X.1975.9940405
Mason outlines the state of research in the stress field and argues against Selye’s conclusions that stress has nonspecific effects (i.e., all stress results in the same physiological outcome). He provides evidence that stress has discrete effects and argues that the terminology for stress be differentiated into external challenges (i.e., stressors), psychophysiological responses (i.e., strain), and a transactional process of appraisal (i.e., stress).
McGrath, J. E., ed. 1970. Social and psychological factors in stress . New York: Holt, Rinehart and Winston.
As a product of the proceedings from a conference, McGrath has put together several perspectives on defining stress and the methodological issues that are important to continuing stress research. In defining stress McGrath notes that stress is the imbalance between the responsibilities of one’s environment and the degree to which they are able to respond appropriately to them.
back to top
Users without a subscription are not able to see the full content on this page. Please subscribe or login .
Oxford Bibliographies Online is available by subscription and perpetual access to institutions. For more information or to contact an Oxford Sales Representative click here .
- About Psychology »
- Meet the Editorial Board »
- Abnormal Psychology
- Academic Assessment
- Acculturation and Health
- Action Regulation Theory
- Action Research
- Addictive Behavior
- Adolescence
- Adoption, Social, Psychological, and Evolutionary Perspect...
- Advanced Theory of Mind
- Affective Forecasting
- Affirmative Action
- Ageism at Work
- Allport, Gordon
- Alzheimer’s Disease
- Ambulatory Assessment in Behavioral Science
- Analysis of Covariance (ANCOVA)
- Animal Behavior
- Animal Learning
- Anxiety Disorders
- Art and Aesthetics, Psychology of
- Artificial Intelligence, Machine Learning, and Psychology
- Assessment and Clinical Applications of Individual Differe...
- Attachment in Social and Emotional Development across the ...
- Attention-Deficit/Hyperactivity Disorder (ADHD) in Adults
- Attention-Deficit/Hyperactivity Disorder (ADHD) in Childre...
- Attitudinal Ambivalence
- Attraction in Close Relationships
- Attribution Theory
- Authoritarian Personality
- Bayesian Statistical Methods in Psychology
- Behavior Therapy, Rational Emotive
- Behavioral Economics
- Behavioral Genetics
- Belief Perseverance
- Bereavement and Grief
- Biological Psychology
- Birth Order
- Body Image in Men and Women
- Bystander Effect
- Categorical Data Analysis in Psychology
- Childhood and Adolescence, Peer Victimization and Bullying...
- Clark, Mamie Phipps
- Clinical Neuropsychology
- Clinical Psychology
- Cognitive Consistency Theories
- Cognitive Dissonance Theory
- Cognitive Neuroscience
- Communication, Nonverbal Cues and
- Comparative Psychology
- Competence to Stand Trial: Restoration Services
- Competency to Stand Trial
- Computational Psychology
- Conflict Management in the Workplace
- Conformity, Compliance, and Obedience
- Consciousness
- Coping Processes
- Correspondence Analysis in Psychology
- Counseling Psychology
- Creativity at Work
- Critical Thinking
- Cross-Cultural Psychology
- Cultural Psychology
- Daily Life, Research Methods for Studying
- Data Science Methods for Psychology
- Data Sharing in Psychology
- Death and Dying
- Deceiving and Detecting Deceit
- Defensive Processes
- Depressive Disorders
- Development, Prenatal
- Developmental Psychology (Cognitive)
- Developmental Psychology (Social)
- Diagnostic and Statistical Manual of Mental Disorders (DSM...
- Discrimination
- Dissociative Disorders
- Drugs and Behavior
- Eating Disorders
- Ecological Psychology
- Educational Settings, Assessment of Thinking in
- Effect Size
- Embodiment and Embodied Cognition
- Emerging Adulthood
- Emotional Intelligence
- Empathy and Altruism
- Employee Stress and Well-Being
- Environmental Neuroscience and Environmental Psychology
- Ethics in Psychological Practice
- Event Perception
- Evolutionary Psychology
- Expansive Posture
- Experimental Existential Psychology
- Exploratory Data Analysis
- Eyewitness Testimony
- Eysenck, Hans
- Factor Analysis
- Festinger, Leon
- Five-Factor Model of Personality
- Flynn Effect, The
- Forensic Psychology
- Forgiveness
- Friendships, Children's
- Fundamental Attribution Error/Correspondence Bias
- Gambler's Fallacy
- Game Theory and Psychology
- Geropsychology, Clinical
- Global Mental Health
- Habit Formation and Behavior Change
- Health Psychology Research and Practice, Measurement in
- Heider, Fritz
- Heuristics and Biases
- History of Psychology
- Human Factors
- Humanistic Psychology
- Implicit Association Test (IAT)
- Industrial and Organizational Psychology
- Inferential Statistics in Psychology
- Insanity Defense, The
- Intelligence
- Intelligence, Crystallized and Fluid
- Intercultural Psychology
- Intergroup Conflict
- International Classification of Diseases and Related Healt...
- International Psychology
- Interviewing in Forensic Settings
- Intimate Partner Violence, Psychological Perspectives on
- Introversion–Extraversion
- Item Response Theory
- Law, Psychology and
- Lazarus, Richard
- Learned Helplessness
- Learning Theory
- Learning versus Performance
- LGBTQ+ Romantic Relationships
- Lie Detection in a Forensic Context
- Life-Span Development
- Locus of Control
- Loneliness and Health
- Mathematical Psychology
- Meaning in Life
- Mechanisms and Processes of Peer Contagion
- Media Violence, Psychological Perspectives on
- Mediation Analysis
- Memories, Autobiographical
- Memories, Flashbulb
- Memories, Repressed and Recovered
- Memory, False
- Memory, Human
- Memory, Implicit versus Explicit
- Memory in Educational Settings
- Memory, Semantic
- Meta-Analysis
- Metacognition
- Metaphor, Psychological Perspectives on
- Microaggressions
- Military Psychology
- Mindfulness and Education
- Minnesota Multiphasic Personality Inventory (MMPI)
- Money, Psychology of
- Moral Conviction
- Moral Development
- Moral Psychology
- Moral Reasoning
- Nature versus Nurture Debate in Psychology
- Neuroscience of Associative Learning
- Nonergodicity in Psychology and Neuroscience
- Nonparametric Statistical Analysis in Psychology
- Observational (Non-Randomized) Studies
- Obsessive-Complusive Disorder (OCD)
- Olfaction, Human
- Operant Conditioning
- Optimism and Pessimism
- Organizational Justice
- Parenting Stress
- Parenting Styles
- Parents' Beliefs about Children
- Path Models
- Peace Psychology
- Perception, Person
- Performance Appraisal
- Personality Disorders
- Personality Psychology
- Person-Centered and Experiential Psychotherapies: From Car...
- Phenomenological Psychology
- Placebo Effects in Psychology
- Play Behavior
- Positive Psychological Capital (PsyCap)
- Positive Psychology
- Prejudice and Stereotyping
- Pretrial Publicity
- Prisoner's Dilemma
- Problem Solving and Decision Making
- Procrastination
- Prosocial Behavior
- Prosocial Spending and Well-Being
- Protocol Analysis
- Psycholinguistics
- Psychological Literacy
- Psychological Perspectives on Food and Eating
- Psychology, Political
- Psychophysics, Visual
- Psychotherapy
- Psychotic Disorders
- Publication Bias in Psychology
- Reasoning, Counterfactual
- Reliability–Contemporary Psychometric Conceptions
- Religion, Psychology and
- Replication Initiatives in Psychology
- Research Methods
- Risk Taking
- Role of the Expert Witness in Forensic Psychology, The
- Sample Size Planning for Statistical Power and Accurate Es...
- Schizophrenic Disorders
- School Psychology
- School Psychology, Counseling Services in
- Self, Gender and
- Self, Psychology of the
- Self-Construal
- Self-Control
- Self-Deception
- Self-Determination Theory
- Self-Efficacy
- Self-Esteem
- Self-Monitoring
- Self-Regulation in Educational Settings
- Self-Report Tests, Measures, and Inventories in Clinical P...
- Sensation Seeking
- Sex and Gender
- Sexual Minority Parenting
- Sexual Orientation
- Signal Detection Theory and its Applications
- Simpson's Paradox in Psychology
- Single People
- Single-Case Experimental Designs
- Skinner, B.F.
- Sleep and Dreaming
- Small Groups
- Social Class and Social Status
- Social Cognition
- Social Neuroscience
- Social Support
- Social Touch and Massage Therapy Research
- Somatoform Disorders
- Spatial Attention
- Sports Psychology
- Stanford Prison Experiment (SPE): Icon and Controversy
- Stereotype Threat
- Stereotypes
- Stress and Coping, Psychology of
- Student Success in College
- Subjective Wellbeing Homeostasis
- Taste, Psychological Perspectives on
- Teaching of Psychology
- Terror Management Theory
- Testing and Assessment
- The Concept of Validity in Psychological Assessment
- The Neuroscience of Emotion Regulation
- The Reasoned Action Approach and the Theories of Reasoned ...
- The Weapon Focus Effect in Eyewitness Memory
- Theory of Mind
- Therapy, Cognitive-Behavioral
- Thinking Skills in Educational Settings
- Time Perception
- Trait Perspective
- Twin Studies
- Type A Behavior Pattern (Coronary Prone Personality)
- Unconscious Processes
- Video Games and Violent Content
- Virtues and Character Strengths
- Women and Science, Technology, Engineering, and Math (STEM...
- Women, Psychology of
- Work Well-Being
- Wundt, Wilhelm
- Privacy Policy
- Cookie Policy
- Legal Notice
- Accessibility
Powered by:
- [66.249.64.20|185.66.14.236]
- 185.66.14.236
- Tools and Resources
- Customer Services
- Affective Science
- Biological Foundations of Psychology
- Clinical Psychology: Disorders and Therapies
- Cognitive Psychology/Neuroscience
- Developmental Psychology
- Educational/School Psychology
- Forensic Psychology
- Health Psychology
- History and Systems of Psychology
- Individual Differences
- Methods and Approaches in Psychology
- Neuropsychology
- Organizational and Institutional Psychology
- Personality
- Psychology and Other Disciplines
- Social Psychology
- Sports Psychology
- Share This Facebook LinkedIn Twitter
Article contents
Work, stress, coping, and stress management.
- Sharon Glazer Sharon Glazer University of Baltimore
- and Cong Liu Cong Liu Hofstra University
- https://doi.org/10.1093/acrefore/9780190236557.013.30
- Published online: 26 April 2017
Work stress refers to the process of job stressors, or stimuli in the workplace, leading to strains, or negative responses or reactions. Organizational development refers to a process in which problems or opportunities in the work environment are identified, plans are made to remediate or capitalize on the stimuli, action is taken, and subsequently the results of the plans and actions are evaluated. When organizational development strategies are used to assess work stress in the workplace, the actions employed are various stress management interventions. Two key factors tying work stress and organizational development are the role of the person and the role of the environment. In order to cope with work-related stressors and manage strains, organizations must be able to identify and differentiate between factors in the environment that are potential sources of stressors and how individuals perceive those factors. Primary stress management interventions focus on preventing stressors from even presenting, such as by clearly articulating workers’ roles and providing necessary resources for employees to perform their job. Secondary stress management interventions focus on a person’s appraisal of job stressors as a threat or challenge, and the person’s ability to cope with the stressors (presuming sufficient internal resources, such as a sense of meaningfulness in life, or external resources, such as social support from a supervisor). When coping is not successful, strains may develop. Tertiary stress management interventions attempt to remediate strains, by addressing the consequence itself (e.g., diabetes management) and/or the source of the strain (e.g., reducing workload). The person and/or the organization may be the targets of the intervention. The ultimate goal of stress management interventions is to minimize problems in the work environment, intensify aspects of the work environment that create a sense of a quality work context, enable people to cope with stressors that might arise, and provide tools for employees and organizations to manage strains that might develop despite all best efforts to create a healthy workplace.
- stress management
- organization development
- organizational interventions
- stress theories and frameworks
Introduction
Work stress is a generic term that refers to work-related stimuli (aka job stressors) that may lead to physical, behavioral, or psychological consequences (i.e., strains) that affect both the health and well-being of the employee and the organization. Not all stressors lead to strains, but all strains are a result of stressors, actual or perceived. Common terms often used interchangeably with work stress are occupational stress, job stress, and work-related stress. Terms used interchangeably with job stressors include work stressors, and as the specificity of the type of stressor might include psychosocial stressor (referring to the psychological experience of work demands that have a social component, e.g., conflict between two people; Hauke, Flintrop, Brun, & Rugulies, 2011 ), hindrance stressor (i.e., a stressor that prevents goal attainment; Cavanaugh, Boswell, Roehling, & Boudreau, 2000 ), and challenge stressor (i.e., a stressor that is difficult, but attainable and possibly rewarding to attain; Cavanaugh et al., 2000 ).
Stress in the workplace continues to be a highly pervasive problem, having both direct negative effects on individuals experiencing it and companies paying for it, and indirect costs vis à vis lost productivity (Dopkeen & DuBois, 2014 ). For example, U.K. public civil servants’ work-related stress rose from 10.8% in 2006 to 22.4% in 2013 and about one-third of the workforce has taken more than 20 days of leave due to stress-related ill-health, while well over 50% are present at work when ill (French, 2015 ). These findings are consistent with a report by the International Labor Organization (ILO, 2012 ), whereby 50% to 60% of all workdays are lost due to absence attributed to factors associated with work stress.
The prevalence of work-related stress is not diminishing despite improvements in technology and employment rates. The sources of stress, such as workload, seem to exacerbate with improvements in technology (Coovert & Thompson, 2003 ). Moreover, accessibility through mobile technology and virtual computer terminals is linking people to their work more than ever before (ILO, 2012 ; Tarafdar, Tu, Ragu-Nathan, & Ragu-Nathan, 2007 ). Evidence of this kind of mobility and flexibility is further reinforced in a June 2007 survey of 4,025 email users (over 13 years of age); AOL reported that four in ten survey respondents reported planning their vacations around email accessibility and 83% checked their emails at least once a day while away (McMahon, 2007 ). Ironically, despite these mounting work-related stressors and clear financial and performance outcomes, some individuals are reporting they are less “stressed,” but only because “stress has become the new normal” (Jayson, 2012 , para. 4).
This new normal is likely the source of psychological and physiological illness. Siegrist ( 2010 ) contends that conditions in the workplace, particularly psychosocial stressors that are perceived as unfavorable relationships with others and self, and an increasingly sedentary lifestyle (reinforced with desk jobs) are increasingly contributing to cardiovascular disease. These factors together justify a need to continue on the path of helping individuals recognize and cope with deleterious stressors in the work environment and, equally important, to find ways to help organizations prevent harmful stressors over which they have control, as well as implement policies or mechanisms to help employees deal with these stressors and subsequent strains. Along with a greater focus on mitigating environmental constraints are interventions that can be used to prevent anxiety, poor attitudes toward the workplace conditions and arrangements, and subsequent cardiovascular illness, absenteeism, and poor job performance (Siegrist, 2010 ).
Even the ILO has presented guidance on how the workplace can help prevent harmful job stressors (aka hindrance stressors) or at least help workers cope with them. Consistent with the view that well-being is not the absence of stressors or strains and with the view that positive psychology offers a lens for proactively preventing stressors, the ILO promotes increasing preventative risk assessments, interventions to prevent and control stressors, transparent organizational communication, worker involvement in decision-making, networks and mechanisms for workplace social support, awareness of how working and living conditions interact, safety, health, and well-being in the organization (ILO, n.d. ). The field of industrial and organizational (IO) psychology supports the ILO’s recommendations.
IO psychology views work stress as the process of a person’s interaction with multiple aspects of the work environment, job design, and work conditions in the organization. Interventions to manage work stress, therefore, focus on the psychosocial factors of the person and his or her relationships with others and the socio-technical factors related to the work environment and work processes. Viewing work stress from the lens of the person and the environment stems from Kurt Lewin’s ( 1936 ) work that stipulates a person’s state of mental health and behaviors are a function of the person within a specific environment or situation. Aspects of the work environment that affect individuals’ mental states and behaviors include organizational hierarchy, organizational climate (including processes, policies, practices, and reward structures), resources to support a person’s ability to fulfill job duties, and management structure (including leadership). Job design refers to each contributor’s tasks and responsibilities for fulfilling goals associated with the work role. Finally, working conditions refers not only to the physical environment, but also the interpersonal relationships with other contributors.
Each of the conditions that are identified in the work environment may be perceived as potentially harmful or a threat to the person or as an opportunity. When a stressor is perceived as a threat to attaining desired goals or outcomes, the stressor may be labeled as a hindrance stressor (e.g., LePine, Podsakoff, & Lepine, 2005 ). When the stressor is perceived as an opportunity to attain a desired goal or end state, it may be labeled as a challenge stressor. According to LePine and colleagues’ ( 2005 ), both challenge (e.g., time urgency, workload) and hindrance (e.g., hassles, role ambiguity, role conflict) stressors could lead to strains (as measured by “anxiety, depersonalization, depression, emotional exhaustion, frustration, health complaints, hostility, illness, physical symptoms, and tension” [p. 767]). However, challenge stressors positively relate with motivation and performance, whereas hindrance stressors negatively relate with motivation and performance. Moreover, motivation and strains partially mediate the relationship between hindrance and challenge stressors with performance.
Figure 1. Organizational development frameworks to guide identification of work stress and interventions.
In order to (1) minimize any potential negative effects from stressors, (2) increase coping skills to deal with stressors, or (3) manage strains, organizational practitioners or consultants will devise organizational interventions geared toward prevention, coping, and/or stress management. Ultimately, toxic factors in the work environment can have deleterious effects on a person’s physical and psychological well-being, as well as on an organization’s total health. It behooves management to take stock of the organization’s health, which includes the health and well-being of its employees, if the organization wishes to thrive and be profitable. According to Page and Vella-Brodrick’s ( 2009 ) model of employee well-being, employee well-being results from subjective well-being (i.e., life satisfaction and general positive or negative affect), workplace well-being (composed of job satisfaction and work-specific positive or negative affect), and psychological well-being (e.g., self-acceptance, positive social relations, mastery, purpose in life). Job stressors that become unbearable are likely to negatively affect workplace well-being and thus overall employee well-being. Because work stress is a major organizational pain point and organizations often employ organizational consultants to help identify and remediate pain points, the focus here is on organizational development (OD) frameworks; several work stress frameworks are presented that together signal areas where organizations might focus efforts for change in employee behaviors, attitudes, and performance, as well as the organization’s performance and climate. Work stress, interventions, and several OD and stress frameworks are depicted in Figure 1 .
The goals are: (1) to conceptually define and clarify terms associated with stress and stress management, particularly focusing on organizational factors that contribute to stress and stress management, and (2) to present research that informs current knowledge and practices on workplace stress management strategies. Stressors and strains will be defined, leading OD and work stress frameworks that are used to organize and help organizations make sense of the work environment and the organization’s responsibility in stress management will be explored, and stress management will be explained as an overarching thematic label; an area of study and practice that focuses on prevention (primary) interventions, coping (secondary) interventions, and managing strains (tertiary) interventions; as well as the label typically used to denote tertiary interventions. Suggestions for future research and implications toward becoming a healthy organization are presented.
Defining Stressors and Strains
Work-related stressors or job stressors can lead to different kinds of strains individuals and organizations might experience. Various types of stress management interventions, guided by OD and work stress frameworks, may be employed to prevent or cope with job stressors and manage strains that develop(ed).
A job stressor is a stimulus external to an employee and a result of an employee’s work conditions. Example job stressors include organizational constraints, workplace mistreatments (such as abusive supervision, workplace ostracism, incivility, bullying), role stressors, workload, work-family conflicts, errors or mistakes, examinations and evaluations, and lack of structure (Jex & Beehr, 1991 ; Liu, Spector, & Shi, 2007 ; Narayanan, Menon, & Spector, 1999 ). Although stressors may be categorized as hindrances and challenges, there is not yet sufficient information to be able to propose which stress management interventions would better serve to reduce those hindrance stressors or to reduce strain-producing challenge stressors while reinforcing engagement-producing challenge stressors.
Organizational Constraints
Organizational constraints may be hindrance stressors as they prevent employees from translating their motivation and ability into high-level job performance (Peters & O’Connor, 1980 ). Peters and O’Connor ( 1988 ) defined 11 categories of organizational constraints: (1) job-related information, (2) budgetary support, (3) required support, (4) materials and supplies, (5) required services and help from others, (6) task preparation, (7) time availability, (8) the work environment, (9) scheduling of activities, (10) transportation, and (11) job-relevant authority. The inhibiting effect of organizational constraints may be due to the lack of, inadequacy of, or poor quality of these categories.
Workplace Mistreatment
Workplace mistreatment presents a cluster of interpersonal variables, such as interpersonal conflict, bullying, incivility, and workplace ostracism (Hershcovis, 2011 ; Tepper & Henle, 2011 ). Typical workplace mistreatment behaviors include gossiping, rude comments, showing favoritism, yelling, lying, and ignoring other people at work (Tepper & Henle, 2011 ). These variables relate to employees’ psychological well-being, physical well-being, work attitudes (e.g., job satisfaction and organizational commitment), and turnover intention (e.g., Hershcovis, 2011 ; Spector & Jex, 1998 ). Some researchers differentiated the source of mistreatment, such as mistreatment from one’s supervisor versus mistreatment from one’s coworker (e.g., Bruk-Lee & Spector, 2006 ; Frone, 2000 ; Liu, Liu, Spector, & Shi, 2011 ).
Role Stressors
Role stressors are demands, constraints, or opportunities a person perceives to be associated, and thus expected, with his or her work role(s) across various situations. Three commonly studied role stressors are role ambiguity, role conflict, and role overload (Glazer & Beehr, 2005 ; Kahn, Wolfe, Quinn, Snoek, & Rosenthal, 1964 ). Role ambiguity in the workplace occurs when an employee lacks clarity regarding what performance-related behaviors are expected of him or her. Role conflict refers to situations wherein an employee receives incompatible role requests from the same or different supervisors or the employee is asked to engage in work that impedes his or her performance in other work or nonwork roles or clashes with his or her values. Role overload refers to excessive demands and insufficient time (quantitative) or knowledge (qualitative) to complete the work. The construct is often used interchangeably with workload, though role overload focuses more on perceived expectations from others about one’s workload. These role stressors significantly relate to low job satisfaction, low organizational commitment, low job performance, high tension or anxiety, and high turnover intention (Abramis, 1994 ; Glazer & Beehr, 2005 ; Jackson & Schuler, 1985 ).
Excessive workload is one of the most salient stressors at work (e.g., Liu et al., 2007 ). There are two types of workload: quantitative and qualitative workload (LaRocco, Tetrick, & Meder, 1989 ; Parasuraman & Purohit, 2000 ). Quantitative workload refers to the excessive amount of work one has. In a summary of a Chartered Institute of Personnel & Development Report from 2006 , Dewe and Kompier ( 2008 ) noted that quantitative workload was one of the top three stressors workers experienced at work. Qualitative workload refers to the difficulty of work. Workload also differs by the type of the load. There are mental workload and physical workload (Dwyer & Ganster, 1991 ). Excessive physical workload may result in physical discomfort or illness. Excessive mental workload will cause psychological distress such as anxiety or frustration (Bowling & Kirkendall, 2012 ). Another factor affecting quantitative workload is interruptions (during the workday). Lin, Kain, and Fritz ( 2013 ) found that interruptions delay completion of job tasks, thus adding to the perception of workload.
Work-Family Conflict
Work-family conflict is a form of inter-role conflict in which demands from one’s work domain and one’s family domain are incompatible to some extent (Greenhaus & Beutell, 1985 ). Work can interfere with family (WIF) and/or family can interfere with work (FIW) due to time-related commitments to participating in one domain or another, incompatible behavioral expectations, or when strains in one domain carry over to the other (Greenhaus & Beutell, 1985 ). Work-family conflict significantly relates to work-related outcomes (e.g., job satisfaction, organizational commitment, turnover intention, burnout, absenteeism, job performance, job strains, career satisfaction, and organizational citizenship behaviors), family-related outcomes (e.g., marital satisfaction, family satisfaction, family-related performance, family-related strains), and domain-unspecific outcomes (e.g., life satisfaction, psychological strain, somatic or physical symptoms, depression, substance use or abuse, and anxiety; Amstad, Meier, Fasel, Elfering, & Semmer, 2011 ).
Individuals and organizations can experience work-related strains. Sometimes organizations will experience strains through the employee’s negative attitudes or strains, such as that a worker’s absence might yield lower production rates, which would roll up into an organizational metric of organizational performance. In the industrial and organizational (IO) psychology literature, organizational strains are mostly observed as macro-level indicators, such as health insurance costs, accident-free days, and pervasive problems with company morale. In contrast, individual strains, usually referred to as job strains, are internal to an employee. They are responses to work conditions and relate to health and well-being of employees. In other words, “job strains are adverse reactions employees have to job stressors” (Spector, Chen, & O’Connell, 2000 , p. 211). Job strains tend to fall into three categories: behavioral, physical, and psychological (Jex & Beehr, 1991 ).
Behavioral strains consist of actions that employees take in response to job stressors. Examples of behavioral strains include employees drinking alcohol in the workplace or intentionally calling in sick when they are not ill (Spector et al., 2000 ). Physical strains consist of health symptoms that are physiological in nature that employees contract in response to job stressors. Headaches and ulcers are examples of physical strains. Lastly, psychological strains are emotional reactions and attitudes that employees have in response to job stressors. Examples of psychological strains are job dissatisfaction, anxiety, and frustration (Spector et al., 2000 ). Interestingly, research studies that utilize self-report measures find that most job strains experienced by employees tend to be psychological strains (Spector et al., 2000 ).
Leading Frameworks
Organizations that are keen on identifying organizational pain points and remedying them through organizational campaigns or initiatives often discover the pain points are rooted in work-related stressors and strains and the initiatives have to focus on reducing workers’ stress and increasing a company’s profitability. Through organizational climate surveys, for example, companies discover that aspects of the organization’s environment, including its policies, practices, reward structures, procedures, and processes, as well as employees at all levels of the company, are contributing to the individual and organizational stress. Recent studies have even begun to examine team climates for eustress and distress assessed in terms of team members’ homogenous psychological experience of vigor, efficacy, dedication, and cynicism (e.g., Kożusznik, Rodriguez, & Peiro, 2015 ).
Each of the frameworks presented advances different aspects that need to be identified in order to understand the source and potential remedy for stressors and strains. In some models, the focus is on resources, in others on the interaction of the person and environment, and in still others on the role of the person in the workplace. Few frameworks directly examine the role of the organization, but the organization could use these frameworks to plan interventions that would minimize stressors, cope with existing stressors, and prevent and/or manage strains. One of the leading frameworks in work stress research that is used to guide organizational interventions is the person and environment (P-E) fit (French & Caplan, 1972 ). Its precursor is the University of Michigan Institute for Social Research’s (ISR) role stress model (Kahn, Wolfe, Quinn, Snoek, & Rosenthal, 1964 ) and Lewin’s Field Theory. Several other theories have since evolved from the P-E fit framework, including Karasek and Theorell’s ( 1990 ), Karasek ( 1979 ) Job Demands-Control Model (JD-C), the transactional framework (Lazarus & Folkman, 1984 ), Conservation of Resources (COR) theory (Hobfoll, 1989 ), and Siegrist’s ( 1996 ) Effort-Reward Imbalance (ERI) Model.
Field Theory
The premise of Kahn et al.’s ( 1964 ) role stress theory is Lewin’s ( 1997 ) Field Theory. Lewin purported that behavior and mental events are a dynamic function of the whole person, including a person’s beliefs, values, abilities, needs, thoughts, and feelings, within a given situation (field or environment), as well as the way a person represents his or her understanding of the field and behaves in that space. Lewin explains that work-related strains are a result of individuals’ subjective perceptions of objective factors, such as work roles, relationships with others in the workplace, as well as personality indicators, and can be used to predict people’s reactions, including illness. Thus, to make changes to an organizational system, it is necessary to understand a field and try to move that field from the current state to the desired state. Making this move necessitates identifying mechanisms influencing individuals.
Role Stress Theory
Role stress theory mostly isolates the perspective a person has about his or her work-related responsibilities and expectations to determine how those perceptions relate with a person’s work-related strains. However, those relationships have been met with somewhat varied results, which Glazer and Beehr ( 2005 ) concluded might be a function of differences in culture, an environmental factor often neglected in research. Kahn et al.’s ( 1964 ) role stress theory, coupled with Lewin’s ( 1936 ) Field Theory, serves as the foundation for the P-E fit theory. Lewin ( 1936 ) wrote, “Every psychological event depends upon the state of the person and at the same time on the environment” (p. 12). Researchers of IO psychology have narrowed the environment to the organization or work team. This narrowed view of the organizational environment is evident in French and Caplan’s ( 1972 ) P-E fit framework.
Person-Environment Fit Theory
The P-E fit framework focuses on the extent to which there is congruence between the person and a given environment, such as the organization (Caplan, 1987 ; Edwards, 2008 ). For example, does the person have the necessary skills and abilities to fulfill an organization’s demands, or does the environment support a person’s desire for autonomy (i.e., do the values align?) or fulfill a person’s needs (i.e., a person’s needs are rewarded). Theoretically and empirically, the greater the person-organization fit, the greater a person’s job satisfaction and organizational commitment, the less a person’s turnover intention and work-related stress (see meta-analyses by Assouline & Meir, 1987 ; Kristof-Brown, Zimmerman, & Johnson, 2005 ; Verquer, Beehr, & Wagner, 2003 ).
Job Demands-Control/Support (JD-C/S) and Job Demands-Resources (JD-R) Model
Focusing more closely on concrete aspects of work demands and the extent to which a person perceives he or she has control or decision latitude over those demands, Karasek ( 1979 ) developed the JD-C model. Karasek and Theorell ( 1990 ) posited that high job demands under conditions of little decision latitude or control yield high strains, which have varied implications on the health of an organization (e.g., in terms of high turnover, employee ill-health, poor organizational performance). This theory was modified slightly to address not only control, but also other resources that could protect a person from unruly job demands, including support (aka JD-C/S, Johnson & Hall, 1988 ; and JD-R, Bakker, van Veldhoven, & Xanthopoulou, 2010 ). Whether focusing on control or resources, both they and job demands are said to reflect workplace characteristics, while control and resources also represent coping strategies or tools (Siegrist, 2010 ).
Despite the glut of research testing the JD-C and JD-R, results are somewhat mixed. Testing the interaction between job demands and control, Beehr, Glaser, Canali, and Wallwey ( 2001 ) did not find empirical support for the JD-C theory. However, Dawson, O’Brien, and Beehr ( 2016 ) found that high control and high support buffered against the independent deleterious effects of interpersonal conflict, role conflict, and organizational politics (demands that were categorized as hindrance stressors) on anxiety, as well as the effects of interpersonal conflict and organizational politics on physiological symptoms, but control and support did not moderate the effects between challenge stressors and strains. Coupled with Bakker, Demerouti, and Sanz-Vergel’s ( 2014 ) note that excessive job demands are a source of strain, but increased job resources are a source of engagement, Dawson et al.’s results suggest that when an organization identifies that demands are hindrances, it can create strategies for primary (preventative) stress management interventions and attempt to remove or reduce such work demands. If the demands are challenging, though manageable, but latitude to control the challenging stressors and support are insufficient, the organization could modify practices and train employees on adopting better strategies for meeting or coping (secondary stress management intervention) with the demands. Finally, if the organization can neither afford to modify the demands or the level of control and support, it will be necessary for the organization to develop stress management (tertiary) interventions to deal with the inevitable strains.
Conservation of Resources Theory
The idea that job resources reinforce engagement in work has been propagated in Hobfoll’s ( 1989 ) Conservation of Resources (COR) theory. COR theory also draws on the foundational premise that people’s mental health is a function of the person and the environment, forwarding that how people interpret their environment (including the societal context) affects their stress levels. Hobfoll focuses on resources such as objects, personal characteristics, conditions, or energies as particularly instrumental to minimizing strains. He asserts that people do whatever they can to protect their valued resources. Thus, strains develop when resources are threatened to be taken away, actually taken away, or when additional resources are not attainable after investing in the possibility of gaining more resources (Hobfoll, 2001 ). By extension, organizations can invest in activities that would minimize resource loss and create opportunities for resource gains and thus have direct implications for devising primary and secondary stress management interventions.
Transactional Framework
Lazarus and Folkman ( 1984 ) developed the widely studied transactional framework of stress. This framework holds as a key component the cognitive appraisal process. When individuals perceive factors in the work environment as a threat (i.e., primary appraisal), they will scan the available resources (external or internal to himself or herself) to cope with the stressors (i.e., secondary appraisal). If the coping resources provide minimal relief, strains develop. Until recently, little attention has been given to the cognitive appraisal associated with different work stressors (Dewe & Kompier, 2008 ; Liu & Li, 2017 ). In a study of Polish and Spanish social care service providers, stressors appraised as a threat related positively to burnout and less engagement, but stressors perceived as challenges yielded greater engagement and less burnout (Kożusznik, Rodriguez, & Peiro, 2012 ). Similarly, Dawson et al. ( 2016 ) found that even with support and control resources, hindrance demands were more strain-producing than challenge demands, suggesting that appraisal of the stressor is important. In fact, “many people respond well to challenging work” (Beehr et al., 2001 , p. 126). Kożusznik et al. ( 2012 ) recommend training employees to change the way they view work demands in order to increase engagement, considering that part of the problem may be about how the person appraises his or her environment and, thus, copes with the stressors.
Effort-Reward Imbalance
Siegrist’s ( 1996 ) Model of Effort-Reward Imbalance (ERI) focuses on the notion of social reciprocity, such that a person fulfills required work tasks in exchange for desired rewards (Siegrist, 2010 ). ERI sheds light on how an imbalance in a person’s expectations of an organization’s rewards (e.g., pay, bonus, sense of advancement and development, job security) in exchange for a person’s efforts, that is a break in one’s work contract, leads to negative responses, including long-term ill-health (Siegrist, 2010 ; Siegrist et al., 2014 ). In fact, prolonged perception of a work contract imbalance leads to adverse health, including immunological problems and inflammation, which contribute to cardiovascular disease (Siegrist, 2010 ). The model resembles the relational and interactional psychological contract theory in that it describes an employee’s perception of the terms of the relationship between the person and the workplace, including expectations of performance, job security, training and development opportunities, career progression, salary, and bonuses (Thomas, Au, & Ravlin, 2003 ). The psychological contract, like the ERI model, focuses on social exchange. Furthermore, the psychological contract, like stress theories, are influenced by cultural factors that shape how people interpret their environments (Glazer, 2008 ; Thomas et al., 2003 ). Violations of the psychological contract will negatively affect a person’s attitudes toward the workplace and subsequent health and well-being (Siegrist, 2010 ). To remediate strain, Siegrist ( 2010 ) focuses on both the person and the environment, recognizing that the organization is particularly responsible for changing unfavorable work conditions and the person is responsible for modifying his or her reactions to such conditions.
Stress Management Interventions: Primary, Secondary, and Tertiary
Remediation of work stress and organizational development interventions are about realigning the employee’s experiences in the workplace with factors in the environment, as well as closing the gap between the current environment and the desired environment. Work stress develops when an employee perceives the work demands to exceed the person’s resources to cope and thus threatens employee well-being (Dewe & Kompier, 2008 ). Likewise, an organization’s need to change arises when forces in the environment are creating a need to change in order to survive (see Figure 1 ). Lewin’s ( 1951 ) Force Field Analysis, the foundations of which are in Field Theory, is one of the first organizational development intervention tools presented in the social science literature. The concept behind Force Field Analysis is that in order to survive, organizations must adapt to environmental forces driving a need for organizational change and remove restraining forces that create obstacles to organizational change. In order to do this, management needs to delineate the current field in which the organization is functioning, understand the driving forces for change, identify and dampen or eliminate the restraining forces against change. Several models for analyses may be applied, but most approaches are variations of organizational climate surveys.
Through organizational surveys, workers provide management with a snapshot view of how they perceive aspects of their work environment. Thus, the view of the health of an organization is a function of several factors, chief among them employees’ views (i.e., the climate) about the workplace (Lewin, 1951 ). Indeed, French and Kahn ( 1962 ) posited that well-being depends on the extent to which properties of the person and properties of the environment align in terms of what a person requires and the resources available in a given environment. Therefore, only when properties of the person and properties of the environment are sufficiently understood can plans for change be developed and implemented targeting the environment (e.g., change reporting structures to relieve, and thus prevent future, communication stressors) and/or the person (e.g., providing more autonomy, vacation days, training on new technology). In short, climate survey findings can guide consultants about the emphasis for organizational interventions: before a problem arises aka stress prevention, e.g., carefully crafting job roles), when a problem is present, but steps are taken to mitigate their consequences (aka coping, e.g., providing social support groups), and/or once strains develop (aka. stress management, e.g., healthcare management policies).
For each of the primary (prevention), secondary (coping), and tertiary (stress management) techniques the target for intervention can be the entire workforce, a subset of the workforce, or a specific person. Interventions that target the entire workforce may be considered organizational interventions, as they have direct implications on the health of all individuals and consequently the health of the organization. Several interventions categorized as primary and secondary interventions may also be implemented after strains have developed and after it has been discerned that a person or the organization did not do enough to mitigate stressors or strains (see Figure 1 ). The designation of many of the interventions as belonging to one category or another may be viewed as merely a suggestion.
Primary Interventions (Preventative Stress Management)
Before individuals begin to perceive work-related stressors, organizations engage in stress prevention strategies, such as providing people with resources (e.g., computers, printers, desk space, information about the job role, organizational reporting structures) to do their jobs. However, sometimes the institutional structures and resources are insufficient or ambiguous. Scholars and practitioners have identified several preventative stress management strategies that may be implemented.
Planning and Time Management
When employees feel quantitatively overloaded, sometimes the remedy is improving the employees’ abilities to plan and manage their time (Quick, Quick, Nelson, & Hurrell, 2003 ). Planning is a future-oriented activity that focuses on conceptual and comprehensive work goals. Time management is a behavior that focuses on organizing, prioritizing, and scheduling work activities to achieve short-term goals. Given the purpose of time management, it is considered a primary intervention, as engaging in time management helps to prevent work tasks from mounting and becoming unmanageable, which would subsequently lead to adverse outcomes. Time management comprises three fundamental components: (1) establishing goals, (2) identifying and prioritizing tasks to fulfill the goals, and (3) scheduling and monitoring progress toward goal achievement (Peeters & Rutte, 2005 ). Workers who employ time management have less role ambiguity (Macan, Shahani, Dipboye, & Philips, 1990 ), psychological stress or strain (Adams & Jex, 1999 ; Jex & Elaqua, 1999 ; Macan et al., 1990 ), and greater job satisfaction (Macan, 1994 ). However, Macan ( 1994 ) did not find a relationship between time management and performance. Still, Claessens, van Eerde, Rutte, and Roe ( 2004 ) found that perceived control of time partially mediated the relationships between planning behavior (an indicator of time management), job autonomy, and workload on one hand, and job strains, job satisfaction, and job performance on the other hand. Moreover, Peeters and Rutte ( 2005 ) observed that teachers with high work demands and low autonomy experienced more burnout when they had poor time management skills.
Person-Organization Fit
Just as it is important for organizations to find the right person for the job and organization, so is it the responsibility of a person to choose to work at the right organization—an organization that fulfills the person’s needs and upholds the values important to the individual, as much as the person fulfills the organization’s needs and adapts to its values. When people fit their employing organizations they are setting themselves up for experiencing less strain-producing stressors (Kristof-Brown et al., 2005 ). In a meta-analysis of 62 person-job fit studies and 110 person-organization fit studies, Kristof-Brown et al. ( 2005 ) found that person-job fit had a negative correlation with indicators of job strain. In fact, a primary intervention of career counseling can help to reduce stress levels (Firth-Cozens, 2003 ).
Job Redesign
The Job Demands-Control/Support (JD-C/S), Job Demands-Resources (JD-R), and transactional models all suggest that factors in the work context require modifications in order to reduce potential ill-health and poor organizational performance. Drawing on Hackman and Oldham’s ( 1980 ) Job Characteristics Model, it is possible to assess with the Job Diagnostics Survey (JDS) the current state of work characteristics related to skill variety, task identity, task significance, autonomy, and feedback. Modifying those aspects would help create a sense of meaningfulness, sense of responsibility, and feeling of knowing how one is performing, which subsequently affects a person’s well-being as identified in assessments of motivation, satisfaction, improved performance, and reduced withdrawal intentions and behaviors. Extending this argument to the stress models, it can be deduced that reducing uncertainty or perceived unfairness that may be associated with a person’s perception of these work characteristics, as well as making changes to physical characteristics of the environment (e.g., lighting, seating, desk, air quality), nature of work (e.g., job responsibilities, roles, decision-making latitude), and organizational arrangements (e.g., reporting structure and feedback mechanisms), can help mitigate against numerous ill-health consequences and reduced organizational performance. In fact, Fried et al. ( 2013 ) showed that healthy patients of a medical clinic whose jobs were excessively low (i.e., monotonous) or excessively high (i.e., overstimulating) on job enrichment (as measured by the JDS) had greater abdominal obesity than those whose jobs were optimally enriched. By taking stock of employees’ perceptions of the current work situation, managers might think about ways to enhance employees’ coping toolkit, such as training on how to deal with difficult clients or creating stimulating opportunities when jobs have low levels of enrichment.
Participatory Action Research Interventions
Participatory action research (PAR) is an intervention wherein, through group discussions, employees help to identify and define problems in organizational structure, processes, policies, practices, and reward structures, as well as help to design, implement, and evaluate success of solutions. PAR is in itself an intervention, but its goal is to design interventions to eliminate or reduce work-related factors that are impeding performance and causing people to be unwell. An example of a successful primary intervention, utilizing principles of PAR and driven by the JD-C and JD-C/S stress frameworks is Health Circles (HCs; Aust & Ducki, 2004 ).
HCs, developed in Germany in the 1980s, were popular practices in industries, such as metal, steel, and chemical, and service. Similar to other problem-solving practices, such as quality circles, HCs were based on the assumptions that employees are the experts of their jobs. For this reason, to promote employee well-being, management and administrators solicited suggestions and ideas from the employees to improve occupational health, thereby increasing employees’ job control. HCs also promoted communication between managers and employees, which had a potential to increase social support. With more control and support, employees would experience less strains and better occupational well-being.
Employing the three-steps of (1) problem analysis (i.e., diagnosis or discovery through data generated from organizational records of absenteeism length, frequency, rate, and reason and employee survey), (2) HC meetings (6 to 10 meetings held over several months to brainstorm ideas to improve occupational safety and health concerns identified in the discovery phase), and (3) HC evaluation (to determine if desired changes were accomplished and if employees’ reports of stressors and strains changed after the course of 15 months), improvements were to be expected (Aust & Ducki, 2004 ). Aust and Ducki ( 2004 ) reviewed 11 studies presenting 81 health circles in 30 different organizations. Overall study participants had high satisfaction with the HCs practices. Most companies acted upon employees’ suggestions (e.g., improving driver’s seat and cab, reducing ticket sale during drive, team restructuring and job rotation to facilitate communication, hiring more employees during summer time, and supervisor training program to improve leadership and communication skills) to improve work conditions. Thus, HCs represent a successful theory-grounded intervention to routinely improve employees’ occupational health.
Physical Setting
The physical environment or physical workspace has an enormous impact on individuals’ well-being, attitudes, and interactions with others, as well as on the implications on innovation and well-being (Oksanen & Ståhle, 2013 ; Vischer, 2007 ). In a study of 74 new product development teams (total of 437 study respondents) in Western Europe, Chong, van Eerde, Rutte, and Chai ( 2012 ) found that when teams were faced with challenge time pressures, meaning the teams had a strong interest and desire in tackling complex, but engaging tasks, when they were working proximally close with one another, team communication improved. Chong et al. assert that their finding aligns with prior studies that have shown that physical proximity promotes increased awareness of other team members, greater tendency to initiate conversations, and greater team identification. However, they also found that when faced with hindrance time pressures, physical proximity related to low levels of team communication, but when hindrance time pressure was low, team proximity had an increasingly greater positive relationship with team communication.
In addition to considering the type of work demand teams must address, other physical workspace considerations include whether people need to work collaboratively and synchronously or independently and remotely (or a combination thereof). Consideration needs to be given to how company contributors would satisfy client needs through various modes of communication, such as email vs. telephone, and whether individuals who work by a window might need shading to block bright sunlight from glaring on their computer screens. Finally, people who have to use the telephone for extensive periods of time would benefit from earphones to prevent neck strains. Most physical stressors are rather simple to rectify. However, companies are often not aware of a problem until after a problem arises, such as when a person’s back is strained from trying to move heavy equipment. Companies then implement strategies to remediate the environmental stressor. With the help of human factors, and organizational and office design consultants, many of the physical barriers to optimal performance can be prevented (Rousseau & Aubé, 2010 ). In a study of 215 French-speaking Canadian healthcare employees, Rousseau and Aubé ( 2010 ) found that although supervisor instrumental support positively related with affective commitment to the organization, the relationship was even stronger for those who reported satisfaction with the ambient environment (i.e., temperature, lighting, sound, ventilation, and cleanliness).
Secondary Interventions (Coping)
Secondary interventions, also referred to as coping, focus on resources people can use to mitigate the risk of work-related illness or workplace injury. Resources may include properties related to social resources, behaviors, and cognitive structures. Each of these resource domains may be employed to cope with stressors. Monat and Lazarus ( 1991 ) summarize the definition of coping as “an individual’s efforts to master demands (or conditions of harm, threat, or challenge) that are appraised (or perceived) as exceeding or taxing his or her resources” (p. 5). To master demands requires use of the aforementioned resources. Secondary interventions help employees become aware of the psychological, physical, and behavioral responses that may occur from the stressors presented in their working environment. Secondary interventions help a person detect and attend to stressors and identify resources for and ways of mitigating job strains. Often, coping strategies are learned skills that have a cognitive foundation and serve important functions in improving people’s management of stressors (Lazarus & Folkman, 1991 ). Coping is effortful, but with practice it becomes easier to employ. This idea is the foundation for understanding the role of resilience in coping with stressors. However, “not all adaptive processes are coping. Coping is a subset of adaptational activities that involves effort and does not include everything that we do in relating to the environment” (Lazarus & Folkman, 1991 , p. 198). Furthermore, sometimes to cope with a stressor, a person may call upon social support sources to help with tangible materials or emotional comfort. People call upon support resources because they help to restructure how a person approaches or thinks about the stressor.
Most secondary interventions are aimed at helping the individual, though companies, as a policy, might require all employees to partake in training aimed at increasing employees’ awareness of and skills aimed at handling difficult situations vis à vis company channels (e.g., reporting on sexual harassment or discrimination). Furthermore, organizations might institute mentoring programs or work groups to address various work-related matters. These programs employ awareness-raising activities, stress-education, or skills training (cf., Bhagat, Segovis, & Nelson, 2012 ), which include development of skills in problem-solving, understanding emotion-focused coping, identifying and using social support, and enhancing capacity for resilience. The aim of these programs, therefore, is to help employees proactively review their perceptions of psychological, physical, and behavioral job-related strains, thereby extending their resilience, enabling them to form a personal plan to control stressors and practice coping skills (Cooper, Dewe, & O’Driscoll, 2011 ).
Often these stress management programs are instituted after an organization has observed excessive absenteeism and work-related performance problems and, therefore, are sometimes categorized as a tertiary stress management intervention or even a primary (prevention) intervention. However, the skills developed for coping with stressors also place the programs in secondary stress management interventions. Example programs that are categorized as tertiary or primary stress management interventions may also be secondary stress management interventions (see Figure 1 ), and these include lifestyle advice and planning, stress inoculation training, simple relaxation techniques, meditation, basic trainings in time management, anger management, problem-solving skills, and cognitive-behavioral therapy. Corporate wellness programs also fall under this category. In other words, some programs could be categorized as primary, secondary, or tertiary interventions depending upon when the employee (or organization) identifies the need to implement the program. For example, time management practices could be implemented as a means of preventing some stressors, as a way to cope with mounting stressors, or as a strategy to mitigate symptoms of excessive of stressors. Furthermore, these programs can be administered at the individual level or group level. As related to secondary interventions, these programs provide participants with opportunities to develop and practice skills to cognitively reappraise the stressor(s); to modify their perspectives about stressors; to take time out to breathe, stretch, meditate, relax, and/or exercise in an attempt to support better decision-making; to articulate concerns and call upon support resources; and to know how to say “no” to onslaughts of requests to complete tasks. Participants also learn how to proactively identify coping resources and solve problems.
According to Cooper, Dewe, and O’Driscoll ( 2001 ), secondary interventions are successful in helping employees modify or strengthen their ability to cope with the experience of stressors with the goal of mitigating the potential harm the job stressors may create. Secondary interventions focus on individuals’ transactions with the work environment and emphasize the fit between a person and his or her environment. However, researchers have pointed out that the underlying assumption of secondary interventions is that the responsibility for coping with the stressors of the environment lies within individuals (Quillian-Wolever & Wolever, 2003 ). If companies cannot prevent the stressors in the first place, then they are, in part, responsible for helping individuals develop coping strategies and informing employees about programs that would help them better cope with job stressors so that they are able to fulfill work assignments.
Stress management interventions that help people learn to cope with stressors focus mainly on the goals of enabling problem-resolution or expressing one’s emotions in a healthy manner. These goals are referred to as problem-focused coping and emotion-focused coping (Folkman & Lazarus, 1980 ; Pearlin & Schooler, 1978 ), and the person experiencing the stressors as potential threat is the agent for change and the recipient of the benefits of successful coping (Hobfoll, 1998 ). In addition to problem-focused and emotion-focused coping approaches, social support and resilience may be coping resources. There are many other sources for coping than there is room to present here (see e.g., Cartwright & Cooper, 2005 ); however, the current literature has primarily focused on these resources.
Problem-Focused Coping
Problem-focused or direct coping helps employees remove or reduce stressors in order to reduce their strain experiences (Bhagat et al., 2012 ). In problem-focused coping employees are responsible for working out a strategic plan in order to remove job stressors, such as setting up a set of goals and engaging in behaviors to meet these goals. Problem-focused coping is viewed as an adaptive response, though it can also be maladaptive if it creates more problems down the road, such as procrastinating getting work done or feigning illness to take time off from work. Adaptive problem-focused coping negatively relates to long-term job strains (Higgins & Endler, 1995 ). Discussion on problem-solving coping is framed from an adaptive perspective.
Problem-focused coping is featured as an extension of control, because engaging in problem-focused coping strategies requires a series of acts to keep job stressors under control (Bhagat et al., 2012 ). In the stress literature, there are generally two ways to categorize control: internal versus external locus of control, and primary versus secondary control. Locus of control refers to the extent to which people believe they have control over their own life (Rotter, 1966 ). People high in internal locus of control believe that they can control their own fate whereas people high in external locus of control believe that outside factors determine their life experience (Rotter, 1966 ). Generally, those with an external locus of control are less inclined to engage in problem-focused coping (Strentz & Auerbach, 1988 ). Primary control is the belief that people can directly influence their environment (Alloy & Abramson, 1979 ), and thus they are more likely to engage in problem-focused coping. However, when it is not feasible to exercise primary control, people search for secondary control, with which people try to adapt themselves into the objective environment (Rothbaum, Weisz, & Snyder, 1982 ).
Emotion-Focused Coping
Emotion-focused coping, sometimes referred to as palliative coping, helps employees reduce strains without the removal of job stressors. It involves cognitive or emotional efforts, such as talking about the stressor or distracting oneself from the stressor, in order to lessen emotional distress resulting from job stressors (Bhagat et al., 2012 ). Emotion-focused coping aims to reappraise and modify the perceptions of a situation or seek emotional support from friends or family. These methods do not include efforts to change the work situation or to remove the job stressors (Lazarus & Folkman, 1991 ). People tend to adopt emotion-focused coping strategies when they believe that little or nothing can be done to remove the threatening, harmful, and challenging stressors (Bhagat et al., 2012 ), such as when they are the only individuals to have the skills to get a project done or they are given increased responsibilities because of the unexpected departure of a colleague. Emotion-focused coping strategies include (1) reappraisal of the stressful situation, (2) talking to friends and receiving reassurance from them, (3) focusing on one’s strength rather than weakness, (4) optimistic comparison—comparing one’s situation to others’ or one’s past situation, (5) selective ignoring—paying less attention to the unpleasant aspects of one’s job and being more focused on the positive aspects of the job, (6) restrictive expectations—restricting one’s expectations on job satisfaction but paying more attention to monetary rewards, (7) avoidance coping—not thinking about the problem, leaving the situation, distracting oneself, or using alcohol or drugs (e.g., Billings & Moos, 1981 ).
Some emotion-focused coping strategies are maladaptive. For example, avoidance coping may lead to increased level of job strains in the long run (e.g., Parasuraman & Cleek, 1984 ). Furthermore, a person’s ability to cope with the imbalance of performing work to meet organizational expectations can take a toll on the person’s health, leading to physiological consequences such as cardiovascular disease, sleep disorders, gastrointestinal disorders, and diabetes (Fried et al., 2013 ; Siegrist, 2010 ; Toker, Shirom, Melamed, & Armon, 2012 ; Willert, Thulstrup, Hertz, & Bonde, 2010 ).
Comparing Coping Strategies across Cultures
Most coping research is conducted in individualistic, Western cultures wherein emotional control is emphasized and both problem-solving focused coping and primary control are preferred (Bhagat et al., 2010 ). However, in collectivistic cultures, emotion-focused coping and use of secondary control may be preferred and may not necessarily carry a negative evaluation (Bhagat et al., 2010 ). For example, African Americans are more likely to use emotion-focused coping than non–African Americans (Knight, Silverstein, McCallum, & Fox, 2000 ), and among women who experienced sexual harassment, Anglo American women were less likely to employ emotion focused coping (i.e., avoidance coping) than Turkish women and Hispanic American women, while Hispanic women used more denial than the other two groups (Wasti & Cortina, 2002 ).
Thus, whereas problem-focused coping is venerated in Western societies, emotion-focused coping may be more effective in reducing strains in collectivistic cultures, such as China, Japan, and India (Bhagat et al., 2010 ; Narayanan, Menon, & Spector, 1999 ; Selmer, 2002 ). Indeed, Swedish participants reported more problem-focused coping than did Chinese participants (Xiao, Ottosson, & Carlsson, 2013 ), American college students engaged in more problem-focused coping behaviors than did their Japanese counterparts (Ogawa, 2009 ), and Indian (vs. Canadian) students reported more emotion-focused coping, such as seeking social support and positive reappraisal (Sinha, Willson, & Watson, 2000 ). Moreover, Glazer, Stetz, and Izso ( 2004 ) found that internal locus of control was more predominant in individualistic cultures (United Kingdom and United States), whereas external locus of control was more predominant in communal cultures (Italy and Hungary). Also, internal locus of control was associated with less job stress, but more so for nurses in the United Kingdom and United States than Italy and Hungary. Taken together, adoption of coping strategies and their effectiveness differ significantly across cultures. The extent to which a coping strategy is perceived favorably and thus selected or not selected is not only a function of culture, but also a person’s sociocultural beliefs toward the coping strategy (Morimoto, Shimada, & Ozaki, 2013 ).
Social Support
Social support refers to the aid an entity gives to a person. The source of the support can be a single person, such as a supervisor, coworker, subordinate, family member, friend, or stranger, or an organization as represented by upper-level management representing organizational practices. The type of support can be instrumental or emotional. Instrumental support, including informational support, refers to that which is tangible, such as data to help someone make a decision or colleagues’ sick days so one does not lose vital pay while recovering from illness. Emotional support, including esteem support, refers to the psychological boost given to a person who needs to express emotions and feel empathy from others or to have his or her perspective validated. Beehr and Glazer ( 2001 ) present an overview of the role of social support on the stressor-strain relationship and arguments regarding the role of culture in shaping the utility of different sources and types of support.
Meaningfulness and Resilience
Meaningfulness reflects the extent to which people believe their lives are significant, purposeful, goal-directed, and fulfilling (Glazer, Kożusznik, Meyers, & Ganai, 2014 ). When faced with stressors, people who have a strong sense of meaning in life will also try to make sense of the stressors. Maintaining a positive outlook on life stressors helps to manage emotions, which is helpful in reducing strains, particularly when some stressors cannot be problem-solved (Lazarus & Folkman, 1991 ). Lazarus and Folkman ( 1991 ) emphasize that being able to reframe threatening situations can be just as important in an adaptation as efforts to control the stressors. Having a sense of meaningfulness motivates people to behave in ways that help them overcome stressors. Thus, meaningfulness is often used in the same breath as resilience, because people who are resilient are often protecting that which is meaningful.
Resilience is a personality state that can be fortified and enhanced through varied experiences. People who perceive their lives are meaningful are more likely to find ways to face adversity and are therefore more prone to intensifying their resiliency. When people demonstrate resilience to cope with noxious stressors, their ability to be resilient against other stressors strengthens because through the experience, they develop more competencies (Glazer et al., 2014 ). Thus, fitting with Hobfoll’s ( 1989 , 2001 ) COR theory, meaningfulness and resilience are psychological resources people attempt to conserve and protect, and employ when necessary for making sense of or coping with stressors.
Tertiary Interventions (Stress Management)
Stress management refers to interventions employed to treat and repair harmful repercussions of stressors that were not coped with sufficiently. As Lazarus and Folkman ( 1991 ) noted, not all stressors “are amenable to mastery” (p. 205). Stressors that are unmanageable and lead to strains require interventions to reverse or slow down those effects. Workplace interventions might focus on the person, the organization, or both. Unfortunately, instead of looking at the whole system to include the person and the workplace, most companies focus on the person. Such a focus should not be a surprise given the results of van der Klink, Blonk, Schene, and van Dijk’s ( 2001 ) meta-analysis of 48 experimental studies conducted between 1977 and 1996 . They found that of four types of tertiary interventions, the effect size for cognitive-behavioral interventions and multimodal programs (e.g., the combination of assertive training and time management) was moderate and the effect size for relaxation techniques was small in reducing psychological complaints, but not turnover intention related to work stress. However, the effects of (the five studies that used) organization-focused interventions were not significant. Similarly, Richardson and Rothstein’s ( 2008 ) meta-analytic study, including 36 experimental studies with 55 interventions, showed a larger effect size for cognitive-behavioral interventions than relaxation, organizational, multimodal, or alternative. However, like with van der Klink et al. ( 2001 ), Richardson and Rothstein ( 2008 ) cautioned that there were few organizational intervention studies included and the impact of interventions were determined on the basis of psychological outcomes and not physiological or organizational outcomes. Van der Klink et al. ( 2001 ) further expressed concern that organizational interventions target the workplace and that changes in the individual may take longer to observe than individual interventions aimed directly at the individual.
The long-term benefits of individual focused interventions are not yet clear either. Per Giga, Cooper, and Faragher ( 2003 ), the benefits of person-directed stress management programs will be short-lived if organizational factors to reduce stressors are not addressed too. Indeed, LaMontagne, Keegel, Louie, Ostry, and Landsbergis ( 2007 ), in their meta-analysis of 90 studies on stress management interventions published between 1990 and 2005 , revealed that in relation to interventions targeting organizations only, and interventions targeting individuals only, interventions targeting both organizations and individuals (i.e. the systems approach) had the most favorable positive effects on both the organizations and the individuals. Furthermore, the organization-level interventions were effective at both the individual and organization levels, but the individual-level interventions were effective only at the individual level.
Individual-Focused Stress Management
Individual-focused interventions concentrate on improving conditions for the individual, though counseling programs emphasize that the worker is in charge of reducing “stress,” whereas role-focused interventions emphasize activities that organizations can guide to actually reduce unnecessary noxious environmental factors.
Individual-Focused Stress Management: Employee Assistance Programs
When stress become sufficiently problematic (which is individually gauged or attended to by supportive others) in a worker’s life, employees may utilize the short-term counseling services or referral services Employee Assistance Programs (EAPs) provide. People who utilize the counseling services may engage in cognitive behavioral therapy aimed at changing the way people think about the stressors (e.g., as challenge opportunity over threat) and manage strains. Example topics that may be covered in these therapy sessions include time management and goal setting (prioritization), career planning and development, cognitive restructuring and mindfulness, relaxation, and anger management. In a study of healthcare workers and teachers who participated in a 2-day to 2.5-day comprehensive stress management training program (including 26 topics on identifying, coping with, and managing stressors and strains), Siu, Cooper, and Phillips ( 2013 ) found psychological and physical improvements were self-reported among the healthcare workers (for which there was no control group). However, comparing an intervention group of teachers to a control group of teachers, the extent of change was not as visible, though teachers in the intervention group engaged in more mastery recovery experiences (i.e., they purposefully chose to engage in challenging activities after work).
Individual-Focused Stress Management: Mindfulness
A popular therapy today is to train people to be more mindful, which involves helping people live in the present, reduce negative judgement of current and past experiences, and practicing patience (Birnie, Speca, & Carlson, 2010 ). Mindfulness programs usually include training on relaxation exercises, gentle yoga, and awareness of the body’s senses. In one study offered through the continuing education program at a Canadian university, 104 study participants took part in an 8-week, 90 minute per group (15–20 participants per) session mindfulness program (Birnie et al., 2010 ). In addition to body scanning, they also listened to lectures on incorporating mindfulness into one’s daily life and received a take-home booklet and compact discs that guided participants through the exercises studied in person. Two weeks after completing the program, participants’ mindfulness attendance and general positive moods increased, while physical, psychological, and behavioral strains decreased. In another study on a sample of U.K. government employees, study participants receiving three sessions of 2.5 to 3 hours each training on mindfulness, with the first two sessions occurring in consecutive weeks and the third occurring about three months later, Flaxman and Bond ( 2010 ) found that compared to the control group, the intervention group showed a decrease in distress levels from Time 1 (baseline) to Time 2 (three months after first two training sessions) and Time 1 to Time 3 (after final training session). Moreover, of the mindfulness intervention study participants who were clinically distressed, 69% experienced clinical improvement in their psychological health.
Individual-Focused Stress Management: Biofeedback/Imagery/Meditation/Deep Breathing
Biofeedback uses electronic equipment to inform users about how their body is responding to tension. With guidance from a therapist, individuals then learn to change their physiological responses so that their pulse normalizes and muscles relax (Norris, Fahrion, & Oikawa, 2007 ). The therapist’s guidance might include reminders for imagery, meditation, body scan relaxation, and deep breathing. Saunders, Driskell, Johnston, and Salas’s ( 1996 ) meta-analysis of 37 studies found that imagery helped reduce state and performance anxiety. Once people have been trained to relax, reminder triggers may be sent through smartphone push notifications (Villani et al., 2013 ).
Smartphone technology can also be used to support weight loss programs, smoking cessation programs, and medication or disease (e.g., diabetes) management compliance (Heron & Smyth, 2010 ; Kannampallil, Waicekauskas, Morrow, Kopren, & Fu, 2013 ). For example, smartphones could remind a person to take medications or test blood sugar levels or send messages about healthy behaviors and positive affirmations.
Individual-Focused Stress Management: Sleep/Rest/Respite
Workers today sleep less per night than adults did nearly 30 years ago (Luckhaupt, Tak, & Calvert, 2010 ; National Sleep Foundation, 2005 , 2013 ). In order to combat problems, such as increased anxiety and cardiovascular artery disease, associated with sleep deprivation and insufficient rest, it is imperative that people disconnect from their work at least one day per week or preferably for several weeks so that they are able to restore psychological health (Etzion, Eden, & Lapidot, 1998 ; Ragsdale, Beehr, Grebner, & Han, 2011 ). When college students engaged in relaxation-type activities, such as reading or watching television, over the weekend, they experienced less emotional exhaustion and greater general well-being than students who engaged in resources-consuming activities, such as house cleaning (Ragsdale et al., 2011 ). Additional research and future directions for research are reviewed and identified in the work of Sonnentag ( 2012 ). For example, she asks whether lack of ability to detach from work is problematic for people who find their work meaningful. In other words, are negative health consequences only among those who do not take pleasure in their work? Sonnetag also asks how teleworkers detach from their work when engaging in work from the home. Ironically, one of the ways that companies are trying to help with the challenges of high workload or increased need to be available to colleagues, clients, or vendors around the globe is by offering flexible work arrangements, whereby employees who can work from home are given the opportunity to do so. Companies that require global interactions 24-hours per day often employ this strategy, but is the solution also a source of strain (Glazer, Kożusznik, & Shargo, 2012 )?
Individual-Focused Stress Management: Role Analysis
Role analysis or role clarification aims to redefine, expressly identify, and align employees’ roles and responsibilities with their work goals. Through role negotiation, involved parties begin to develop a new formal or informal contract about expectations and define resources needed to fulfill those expectations. Glazer has used this approach in organizational consulting and, with one memorable client engagement, found that not only were the individuals whose roles required deeper re-evaluation happier at work (six months later), but so were their subordinates. Subordinates who once characterized the two partners as hostile and akin to a couple going through a bad divorce, later referred to them as a blissful pair. Schaubroeck, Ganster, Sime, and Ditman ( 1993 ) also found in a three-wave study over a two-year period that university employees’ reports of role clarity and greater satisfaction with their supervisor increased after a role clarification exercise of top managers’ roles and subordinates’ roles. However, the intervention did not have any impact on reported physical symptoms, absenteeism, or psychological well-being. Role analysis is categorized under individual-focused stress management intervention because it is usually implemented after individuals or teams begin to demonstrate poor performance and because the intervention typically focuses on a few individuals rather than an entire organization or group. In other words, the intervention treats the person’s symptoms by redefining the role so as to eliminate the stimulant causing the problem.
Organization-Focused Stress Management
At the organizational level, companies that face major declines in productivity and profitability or increased costs related to healthcare and disability might be motivated to reassess organizational factors that might be impinging on employees’ health and well-being. After all, without healthy workers, it is not possible to have a healthy organization. Companies may choose to implement practices and policies that are expected to help not only the employees, but also the organization with reduced costs associated with employee ill-health, such as medical insurance, disability payments, and unused office space. Example practices and policies that may be implemented include flexible work arrangements to ensure that employees are not on the streets in the middle of the night for work that can be done from anywhere (such as the home), diversity programs to reduce stress-induced animosity and prejudice toward others, providing only healthy food choices in cafeterias, mandating that all employees have physicals in order to receive reduced prices for insurance, company-wide closures or mandatory paid time off, and changes in organizational visioning.
Organization-Focused Stress Management: Organizational-Level Occupational Health Interventions
As with job design interventions that are implemented to remediate work characteristics that were a source of unnecessary or excessive stressors, so are organizational-level occupational health (OLOH) interventions. As with many of the interventions, its placement as a primary or tertiary stress management intervention may seem arbitrary, but when considering the goal and target of change, it is clear that the intervention is implemented in response to some ailing organizational issues that need to be reversed or stopped, and because it brings in the entire organization’s workforce to address the problems, it has been placed in this category. There are several more case studies than empirical studies on the topic of whole system organizational change efforts (see example case studies presented by the United Kingdom’s Health and Safety Executive). It is possible that lack of published empirical work is not so much due to lack of attempting to gather and evaluate the data for publication, but rather because the OLOH interventions themselves never made it to the intervention stage, the interventions failed (Biron, Gatrell, & Cooper, 2010 ), or the level of evaluation was not rigorous enough to get into empirical peer-review journals. Fortunately, case studies provide some indication of the opportunities and problems associated with OLOH interventions.
One case study regarding Cardiff and Value University Health Board revealed that through focus group meetings with members of a steering group (including high-level managers and supported by top management) and facilitated by a neutral, non-judgemental organizational health consultant, ideas for change were posted on newsprint, discussed, and areas in the organization needing change were identified. The intervention for giving voice to people who initially had little already had a positive effect on the organization, as absence decreased by 2.09% and 6.9% merely 12 and 18 months, respectively, after the intervention. Translated in financial terms, the 6.9% change was equivalent to a quarterly savings of £80,000 (Health & Safety Executive, n.d. ). Thus, focusing on the context of change and how people will be involved in the change process probably helped the organization realize improvements (Biron et al., 2010 ). In a recent and rare empirical study, employing both qualitative and quantitative data collection methods, Sørensen and Holman ( 2014 ) utilized PAR in order to plan and implement an OLOH intervention over the course of 14 months. Their study aimed to examine the effectiveness of the PAR process in reducing workers’ work-related and social or interpersonal-related stressors that derive from the workplace and improving psychological, behavioral, and physiological well-being across six Danish organizations. Based on group dialogue, 30 proposals for change were proposed, all of which could be categorized as either interventions to focus on relational factors (e.g., management feedback improvement, engagement) or work processes (e.g., reduced interruptions, workload, reinforcing creativity). Of the interventions that were implemented, results showed improvements on manager relationship quality and reduced burnout, but no changes with respect to work processes (i.e., workload and work pace) perhaps because the employees already had sufficient task control and variety. These findings support Dewe and Kompier’s ( 2008 ) position that occupational health can be reinforced through organizational policies that reinforce quality jobs and work experiences.
Organization-Focused Stress Management: Flexible Work Arrangements
Dewe and Kompier ( 2008 ), citing the work of Isles ( 2005 ), noted that concern over losing one’s job is a reason for why 40% of survey respondents indicated they work more hours than formally required. In an attempt to create balance and perceived fairness in one’s compensation for putting in extra work hours, employees will sometimes be legitimately or illegitimately absent. As companies become increasingly global, many people with desk jobs are finding themselves communicating with colleagues who are halfway around the globe and at all hours of the day or night (Glazer et al., 2012 ). To help minimize the strains associated with these stressors, companies might devise flexible work arrangements (FWA), though the type of FWA needs to be tailored to the cultural environment (Masuda et al., 2012 ). FWAs give employees some leverage to decide what would be the optimal work arrangement for them (e.g., part-time, flexible work hours, compressed work week, telecommuting). In other words, FWA provides employees with the choice of when to work, where to work (on-site or off-site), and how many hours to work in a day, week, or pay period (Kossek, Thompson, & Lautsch, 2015 ). However, not all employees of an organization have equal access to or equitable use of FWAs; workers in low-wage, hourly jobs are often beholden to being physically present during specific hours (Swanberg McKechnie, Ojha, & James, 2011 ). In a study of over 1,300 full-time hourly retail employees in the United States, Swanberg et al. ( 2011 ) showed that employees who have control over their work schedules and over their work hours were satisfied with their work schedules, perceived support from the supervisor, and work engagement.
Unfortunately, not all FWAs yield successful results for the individual or the organization. Being able to work from home or part-time can have problems too, as a person finds himself or herself working more hours from home than required. Sometimes telecommuting creates work-family conflict too as a person struggles to balance work and family obligations while working from home. Other drawbacks include reduced face-to-face contact between work colleagues and stakeholders, challenges shaping one’s career growth due to limited contact, perceived inequity if some have more flexibility than others, and ambiguity about work role processes for interacting with employees utilizing the FWA (Kossek et al., 2015 ). Organizations that institute FWAs must carefully weigh the benefits and drawbacks the flexibility may have on the employees using it or the employees affected by others using it, as well as the implications on the organization, including the vendors who are serving and clients served by the organization.
Organization-Focused Stress Management: Diversity Programs
Employees in the workplace might experience strain due to feelings of discrimination or prejudice. Organizational climates that do not promote diversity (in terms of age, religion, physical abilities, ethnicity, nationality, sex, and other characteristics) are breeding grounds for undesirable attitudes toward the workplace, lower performance, and greater turnover intention (Bergman, Palmieri, Drasgow, & Ormerod, 2012 ; Velez, Moradi, & Brewster, 2013 ). Management is thus advised to implement programs that reinforce the value and importance of diversity, as well as manage diversity to reduce conflict and feelings of prejudice. In fact, managers who attended a leadership training program reported higher multicultural competence in dealing with stressful situations (Chrobot-Mason & Leslie, 2012 ), and managers who persevered through challenges were more dedicated to coping with difficult diversity issues (Cilliers, 2011 ). Thus, diversity programs can help to reduce strains by directly reducing stressors associated with conflict linked to diversity in the workplace and by building managers’ resilience.
Organization-Focused Stress Management: Healthcare Management Policies
Over the past few years, organizations have adopted insurance plans that implement wellness programs for the sake of managing the increasing cost of healthcare that is believed to be a result of individuals’ not managing their own health, with regular check-ups and treatment. The wellness programs require all insured employees to visit a primary care provider, complete a health risk assessment, and engage in disease management activities as specified by a physician (e.g., see frequently asked questions regarding the State of Maryland’s Wellness Program). Companies believe that requiring compliance will reduce health problems, although there is no proof that such programs save money or that people would comply. One study that does, however, boast success, was a 12-week workplace health promotion program aimed at reducing Houston airport workers’ weight (Ebunlomo, Hare-Everline, Weber, & Rich, 2015 ). The program, which included 235 volunteer participants, was deemed a success, as there was a total weight loss of 345 pounds (or 1.5 lbs per person). Given such results in Houston, it is clear why some people are also skeptical over the likely success of wellness programs, particularly as there is no clear method for evaluating their efficacy (Sinnott & Vatz, 2015 ).
Moreover, for some, such a program is too paternalistic and intrusive, as well as punishes anyone who chooses not to actively participate in disease management programs (Sinnott & Vatz, 2015 ). The programs put the onus of change on the person, though it is a response to the high costs of ill-health. The programs neglect to consider the role of the organization in reducing the barriers to healthy lifestyle, such as cloaking exempt employment as simply needing to get the work done, when it usually means working significantly more hours than a standard workweek. In fact, workplace health promotion programs did not reduce presenteeism (i.e., people going to work while unwell thereby reducing their job performance) among those who suffered from physical pain (Cancelliere, Cassidy, Ammendolia, & Côte, 2011 ). However, supervisor education, worksite exercise, lifestyle intervention through email, midday respite from repetitive work, a global stress management program, changes in lighting, and telephone interventions helped to reduce presenteeism. Thus, emphasis needs to be placed on psychosocial aspects of the organization’s structure, including managers and overall organizational climate for on-site presence, that reinforces such behavior (Cancelliere et al., 2011 ). Moreover, wellness programs are only as good as the interventions to reduce work-related stressors and improve organizational resources to enable workers to improve their overall psychological and physical health.
Concluding Remarks
Future research.
One of the areas requiring more theoretical and practical attention is that of the utility of stress frameworks to guide organizational development change interventions. Although it has been proposed that the foundation for work stress management interventions is in organizational development, and even though scholars and practitioners of organization development were also founders of research programs that focused on employee health and well-being or work stress, there are few studies or other theoretical works that link the two bodies of literature.
A second area that requires additional attention is the efficacy of stress management interventions across cultures. In examining secondary stress management interventions (i.e., coping), some cross-cultural differences in findings were described; however, there is still a dearth of literature from different countries on the utility of different prevention, coping, and stress management strategies.
A third area that has been blossoming since the start of the 21st century is the topic of hindrance and challenge stressors and the implications of both on workers’ well-being and performance. More research is needed on this topic in several areas. First, there is little consistency by which researchers label a stressor as a hindrance or a challenge. Researchers sometimes take liberties with labels, but it is not the researchers who should label a stressor but the study participants themselves who should indicate if a stressor is a source of strain. Rodríguez, Kozusznik, and Peiró ( 2013 ) developed a measure in which respondents indicate whether a stressor is a challenge or a hindrance. Just as some people may perceive demands to be challenges that they savor and that result in a psychological state of eustress (Nelson & Simmons, 2003 ), others find them to be constraints that impede goal fulfillment and thus might experience distress. Likewise, some people might perceive ambiguity as a challenge that can be overcome and others as a constraint over which he or she has little control and few or no resources with which to cope. More research on validating the measurement of challenge vs. hindrance stressors, as well as eustress vs. distress, and savoring vs. coping, is warranted. Second, at what point are challenge stressors harmful? Just because people experiencing challenge stressors continue to perform well, it does not necessarily mean that they are healthy people. A great deal of stressors are intellectually stimulating, but excessive stimulation can also take a toll on one’s physiological well-being, as evident by the droves of professionals experiencing different kinds of diseases not experienced as much a few decades ago, such as obesity (Fried et al., 2013 ). Third, which stress management interventions would better serve to reduce hindrance stressors or to reduce strain that may result from challenge stressors while reinforcing engagement-producing challenge stressors?
A fourth area that requires additional attention is that of the flexible work arrangements (FWAs). One of the reasons companies have been willing to permit employees to work from home is not so much out of concern for the employee, but out of the company’s need for the focal person to be able to communicate with a colleague working from a geographic region when it is night or early morning for the focal person. Glazer, Kożusznik, and Shargo ( 2012 ) presented several areas for future research on this topic, noting that by participating on global virtual teams, workers face additional stressors, even while given flexibility of workplace and work time. As noted earlier, more research needs to be done on the extent to which people who take advantage of FWAs are advantaged in terms of detachment from work. Can people working from home detach? Are those who find their work invigorating also likely to experience ill-health by not detaching from work?
A fifth area worthy of further research attention is workplace wellness programing. According to Page and Vella-Brodrick ( 2009 ), “subjective and psychological well-being [are] key criteria for employee mental health” (p. 442), whereby mental health focuses on wellness, rather than the absence of illness. They assert that by fostering employee mental health, organizations are supporting performance and retention. Employee well-being can be supported by ensuring that jobs are interesting and meaningful, goals are achievable, employees have control over their work, and skills are used to support organizational and individual goals (Dewe & Kompier, 2008 ). However, just as mental health is not the absence of illness, work stress is not indicative of an absence of psychological well-being. Given the perspective that employee well-being is a state of mind (Page & Vella-Brodrick, 2009 ), we suggest that employee well-being can be negatively affected by noxious job stressors that cannot be remediated, but when job stressors are preventable, employee well-being can serve to protect an employee who faces job stressors. Thus, wellness programs ought to focus on providing positive experiences by enhancing and promoting health, as well as building individual resources. These programs are termed “green cape” interventions (Pawelski, 2016 ). For example, with the growing interests in positive psychology, researchers and practitioners have suggested employing several positive psychology interventions, such as expressing gratitude, savoring experiences, and identifying one’s strengths (Tetrick & Winslow, 2015 ). Another stream of positive psychology is psychological capital, which includes four malleable functions of self-efficacy, optimism, hope, and resilience (Luthans, Youssef, & Avolio, 2007 ). Workplace interventions should include both “red cape” interventions (i.e., interventions to reduce negative experiences) and “green cape” interventions (i.e., workplace wellness programs; Polly, 2014 ).
A Healthy Organization’s Pledge
A healthy workplace requires healthy workers. Period. Among all organizations’ missions should be the focus on a healthy workforce. To maintain a healthy workforce, the company must routinely examine its own contributions in terms of how it structures itself; reinforces communications among employees, vendors, and clients; how it rewards and cares for its people (e.g., ensuring they get sufficient rest and can detach from work); and the extent to which people at the upper levels are truly connected with the people at the lower levels. As a matter of practice, management must recognize when employees are overworked, unwell, and poorly engaged. Management must also take stock of when it is doing well and right by its contributors’ and maintain and reinforce the good practices, norms, and procedures. People in the workplace make the rules; people in the workplace can change the rules. How management sees its employees and values their contribution will have a huge role in how a company takes stock of its own pain points. Providing employees with tools to manage their own reactions to work-related stressors and consequent strains is fine, but wouldn’t it be grand if organizations took better notice about what they could do to mitigate the strain-producing stressors in the first place and take ownership over how employees are treated?
- Abramis, D. J. (1994). Work role ambiguity, job satisfaction, and job performance: Meta-analyses and review. Psychological Report, 75 , 1411–1433.
- Adams, G. A. , & Jex, S. M. (1999). Relationships between time management, control, work–family conflict, and strain. Journal of Occupational Health Psychology, 1 , 72–77.
- Alloy, L. B. , & Abramson, L. Y. (1979). Judgment of contingency in depressed and nondepressed students: Sadder but wiser? Journal of Experimental Psychology: General, 108 , 441–483.
- Amstad, F. T. , Meier, L. L. , Fasel, U. , Elfering, A. , & Semmer, N. K. (2011). A meta-analysis of work-family conflict and various outcomes with a special emphasis on cross-domain versus matching-domain relations. Journal of Occupational Health Psychology, 16 , 151–169.
- Assouline, M. , & Meir, E. I. (1987). Meta-analysis of the relationship between congruence and well-being measures. Journal of Vocational Behavior, 31 , 319–332.
- Aust, B. , & Ducki, A. (2004). Comprehensive health promotion interventions at the workplace: Experiences with health circles in Germany. Journal of Occupational Health Psychology, 9 , 258–270.
- Bakker, A. B. Demerouti, E. , Sanz-Vergel, A. I. (2014). Burnout and work engagement: The JD-R approach. Annual Review of Organizational Behavior, 1 , 389–411.
- Bakker, A. B. , van Veldhoven, M. J. P. M. , & Xanthopoulou, D. (2010). Beyond the demand-control model: Thriving on high job demands and resources. Journal of Personnel Psychology, 9 , 3–16.
- Beehr, T. A. , Glaser, K. M. , Canali, K. G. , & Wallwey, D. A. (2001). Back to basics: Re-examination of demand control theory of occupational stress. Work & Stress, 15 , 115–130.
- Beehr, T. A. , & Glazer, S. (2001). A cultural perspective of social support in relation to occupational stress. In P. Perrewé , D. C. Ganster , & J. Moran (Eds.), Research in occupational stress and well-being (pp. 97–142). Amsterdam: JAI Press.
- Bergman, M. E. , Palmieri, P. A. , Drasgow, F. , & Ormerod, A. J. (2012). Racial/ethnic harassment and discrimination, its antecedents, and its effect on job-related outcomes. Journal of Occupational Health Psychology, 17 , 65–78.
- Bhagat, R. S. , Krishnan, B. , Nelson, T. A. , Leonard, K. M. , Ford, D. J. , & Billing, T. K. (2010). Organizational stress, psychological strain, and work outcomes in six national contexts: A closer look at the moderating influences of coping styles and decision latitude . Cross Cultural Management, 17 , 10–29.
- Bhagat, R. S. , O’Driscoll, M. P. , Babakus, E. , Frey, L. , Chokkar, J. , Ninokumar, B. H , et al. (1994). Organizational stress and coping in seven national contexts: A cross-cultural investigation . In G. P. Keita & J. J. Hurrell (Eds.), Job stress in a changing workforce: Investigating gender, diversity, and family issues (pp. 93–105). Washington, DC: American Psychological Association.
- Bhagat, R. S. , Segovis, J. C. , & Nelson, T. A. (2012). Work stress and coping in the era of globalization . New York: Routledge.
- Billings, A. G. , & Moos, R. H. (1981). The role of coping responses and social resources in attenuating the stress of life events. Journal of Behavioral Medicine, 4 , 139–157.
- Birnie, K. , Speca, M. , & Carlson, L. E. (2010). Exploring self-compassion and empathy in the context of mindfulness-based stress reduction (MBSR). Stress & Health, 26 , 359–371.
- Biron, C. , Gatrell, C. , & Cooper, C. L. (2010). Autopsy of a failure: Evaluating process and contextual issues in an organizational-level work stress intervention. International Journal of Stress Management, 17 , 135–158.
- Bowling, N. A. , & Kirkendall, C. (2012). Workload: A review of causes, consequences, and potential interventions. In J. Houdmont , S. Leka , & R. Sinclair (Eds.), Contemporary occupational health psychology (Vol. 2) (pp. 221–238). Chichester, U.K.: Wiley.
- Breaugh, J. A. , & Colihan, J. P. (1994). Measuring facets of job ambiguity: Construct validity evidence. Journal of Applied Psychology, 79 , 191–202.
- Bruk-Lee, V. , & Spector, P. E. (2006). The social stressors-counterproductive work behaviors link: Are conflicts with supervisors and coworkers the same? . Journal of Occupational Health Psychology, 11 , 145–156.
- Cancelliere, C. , Cassidy, J. D. , Ammendolia, C. , & Côte, P. (2011). Are workplace health promotion programs effective at improving presenteeism in workers? A systematic review and best evidence synthesis of the literature. BMC Public Health, 11 , 395–406.
- Caplan, R. D. (1987). Person–environment fit in organizations: Theories, facts, and values. In A. W. Riley & S. J. Zaccaro (Eds.), Occupational stress and organizational effectiveness (pp. 103–140). New York: Praeger.
- Cartwright, S. , & Cooper, C. L. (2005). Individually targeted interventions. In J. Barling , E. K. Kelloway , & M. R. Frone (Eds.), Handbook of work stress (pp. 607–622). Thousand Oaks, CA: SAGE.
- Cavanaugh, M. A. , Boswell, W. R. , Roehling, M. V. , & Boudreau, J. W. (2000). An empirical examination of self-reported work stress among U.S. managers . Journal of Applied Psychology, 85 , 65–74.
- Chong, D. S. F. , van Eerde, W. , Rutte, C. G. , & Chai, K. H. (2012). Bringing employees closer: The effect of proximity on communication when teams function under time pressure. Journal of Product Innovation Management, 29 , 205–215.
- Chrobot-Mason, D. , & Leslie, J. B. (2012). The role of multicultural competence and emotional intelligence in managing diversity. Psychologist-Manager Journal, 15 , 219–236.
- Cilliers, F. (2011). Individual diversity management and salutogenic functioning. International Review of Psychiatry, 23 , 501–507.
- Claessens, B. C. , Van Eerde, W. , Rutte, C. G. , & Roe, R. A. (2004). Planning behavior and perceived control of time at work . Journal of Organizational Behavior, 25 , 937–950.
- Cooper, C. L. , Dewe, P. D. , & O’Driscoll, M. P. (2011). Employee assistance programs: Strengths, challenges, and future roles. In J. C. Quick , L. E. Tetrick , J. C. Quick , L. E. Tetrick (Eds.), Handbook of occupational health psychology (2d ed.) (pp. 337–356). Washington, DC: American Psychological Association.
- Cooper, C. L. , Dewe, P. J. , & O’Driscoll, M. P. (2001). Organizational stress: A review and critique of theory, research, and applications . Thousand Oaks, CA: SAGE.
- Coovert, M. D. & Thompson, L. F. (2003). Technology and workplace health. In J. C. Quick & L. E. Tetrick (Eds.), Handbook of occupational health psychology (pp. 221–241). Washington, DC: American Psychological Association.
- Dawson, K. M. , O’Brien, K. E. , & Beehr, T. A. (2016). The role of hindrance stressors in the job demand-control-support model of occupational stress: A proposed theory revision . Journal of Organizational Behavior, 37 (3), 397–415.
- Dewe, P. , & Kompier, M. (2008). Foresight mental capital and wellbeing project: Wellbeing and work: Future challenges . London: The Government Office for Science.
- Dopkeen, J. C. , & DuBois, R. (2014). Stress in the workplace: A policy synthesis on its dimensions and prevalence . White paper. University of Illinois Chicago, Center for Employee Health Studies, School of Public Health.
- Dwyer, D. J. , & Ganster, D. C. (1991). The effects of job demands and control on employee attendance and satisfaction. Journal of Organizational Behavior, 12 , 595–608.
- Ebunlomo, E. O. , Hare-Everline, N. , Weber, A. , & Rich, J. (2015). Development of a comprehensive 12-week health promotion program for Houston Airport System. Texas Public Health Journal, 67 (1), 11–13.
- Edwards, J. R. (2008). Person-environment fit in organizations: An assessment of theoretical progress. The Academy of Management Annals, 2 , 167–230.
- Etzion, D. , Eden, D. , & Lapidot, Y. (1998). Relief from job stressors and burnout: Reserve service as a respite. Journal of Applied Psychology, 83 , 577–585.
- Firth-Cozens, J. (2003). Doctors, their wellbeing, and their stress: It’s time to be proactive about stress—and prevent it. British Medical Journal, 326 , 670–671.
- Flaxman, P. E. , & Bond, F. W. (2010). Worksite stress management training: Moderated effects and clinical significance. Journal of Occupational Health Psychology, 15 , 347–358.
- Folkman, S. , & Lazarus, R. S. (1980). An analysis of coping in a middle-aged community sample . Journal of Health and Social Behavior, 21 , 219–239.
- French, J. R. P., Jr. , & Caplan, R. D. (1972). Organizational stress and individual strain. In A. Marrow (Ed.), The failure of success . New York: AMACOM.
- French, J. R. P., Jr. , & Kahn, R. L. (1962). A programmatic approach to studying the industrial environment and mental health. Journal of Social Issues, 18 , 1–48.
- French, S. (2015, May 27). PCS workload and work-life balance survey 2013 . London: Public and Commercial Services Union.
- Fried, Y. , Laurence, G. A. , Shirom, A. , Melamed, S. , Toker, S. , Berliner, S. , & Shapira, I. (2013). The relationship between job enrichment and abdominal obesity: A longitudinal field study of apparently healthy individuals. Journal of Occupational Health Psychology, 18 , 458–468.
- Frone, M. R. (2000). Interpersonal conflict at work and psychological outcomes: Testing a model among young workers. Journal of Occupational Health Psychology, 5 , 246–255.
- Giga, S. I. , Cooper, C. L. , & Faragher, B. (2003). The development of a framework for a comprehensive approach to stress management interventions at work. International Journal of Stress Management, 10 , 280–296.
- Glazer, S. (2008). Cross-cultural issues in stress and burnout. In J. R. B. Halbesleben (Ed.), Handbook of Stress and Burnout in Health Care (pp. 79–93). Huntington, NY: Nova Science Publishers.
- Glazer, S. , & Beehr, T. A. (2005). Consistency of the implications of three role stressors across four countries. Journal of Organizational Behavior , 26 , 467–487.
- Glazer, S. , Kożusznik, M. W. , Meyers, J. H. , & Ganai, O. (2014). Cultural implications of meaningfulness as a resource to mitigate work stress. In S. Leka & R. Sinclair (Eds.), Contemporary occupational health psychology: Global perspectives on research and practice (Vol. 3) (pp. 114–130). Hoboken, NJ: Wiley.
- Glazer, S. , Kożusznik, M. W. , & Shargo, I. A. (2012). Global virtual teams: A cure for- or a cause of- stress. In P. L. Perrewé , J. Halbesleben , & C. Rosen (Eds.), Research in occupational stress and well being: The role of the economic context on occupational stress and well being (Vol. 10, pp. 213–266). Bingley, U.K.: Emerald.
- Glazer, S. , Stetz, T. A. , & Izso, L. (2004). Effects of personality on subjective job stress: A cultural analysis. Personality and Individual Differences, 37 , 645–658.
- Greenhaus, J. H. , & Beutell, N. J. (1985). Sources of conflict between work and family roles. Academy of Management Review, 10 , 76–88.
- Hackman, J. R. , & Oldham, G. R. (1980). Work Redesign . Reading, MA: Addison-Wesley.
- Hauke, A. , Flintrop, J. , Brun, E. , & Rugulies, R. (2011). The impact of work-related psychosocial stressors on the onset of musculoskeletal disorders in specific body regions: A review and meta-analysis of 54 longitudinal studies . Work & Stress, 25 , 243–256.
- Health & Safety Executive (n.d.). Cardiff and Value University Health Board—A stress case study .
- Heron, K. E. , & Smyth, J. M. (2010). Ecological momentary interventions: Incorporating mobile technology into psychosocial and health behaviour treatments. British Journal of Health Psychology, 15 , 1–39.
- Hershcovis, M. (2011). “Incivility, social undermining, bullying … oh my!”: A call to reconcile constructs within workplace aggression research . Journal of Organizational Behavior, 32 , 499–519.
- Higgins, J. E. , & Endler, N. S. (1995). Coping, life stress, and psychological and somatic distress . European Journal of Personality, 9 , 253–270.
- Hobfoll, S. E. (1989). Conservation of resources: A new attempt at conceptualizing stress. American Psychologist, 44 , 513–524.
- Hobfoll, S. E. (1998). Stress, culture, and community: The psychology and philosophy of stress . New York: Plenum Press.
- Hobfoll, S. E. (2001). The influence of culture, community, and the nested-self in the stress process: Advancing Conservation of Resources Theory. Applied Psychology: An International Review, 50 , 337–421.
- International Labor Organization (2012, July 5). Why stress at work matters . International Labor Organization.
- International Labor Organization (n.d.). Psychosocial risks and work-related stress . International Labor Organization.
- Jackson, S. E. , & Schuler, R. S. (1985). A meta-analysis and conceptual critique of research on role ambiguity and role conflict in work settings. Organizational Behavior and Human Decision Processes, 36 , 16–78.
- Jayson, S. (2012, January 11). Yeah, we’re stressed but dealing with it; Americans report a decrease in stress for the first time in five years, maybe because it’s just the new normal . USA Today .
- Jex, S. M. , & Beehr, T. A. (1991). Emerging theoretical and methodological issues in the study of work-related stress. Research in Personnel and Human Resources Management, 9 , 311–365.
- Jex, S. M. , & Elaqua, T. C. (1999). Time management as a moderator of relations between stressors and employee strain. Work & Stress, 13 , 182–191.
- Johnson, J. V. , & Hall, E. M. (1988). Job strain, workplace social support, and cardiovascular disease: A cross-sectional study of a random sample of the Swedish working population. American Journal of Public Health, 78 , 1336–1342.
- Kahn, R. L. , Wolfe, D. M. , Quinn, R. P. , Snoek, J. D. , & Rosenthal, R. A. (1964). Organizational stress: Studies in role conflict and ambiguity . New York: Wiley.
- Kannampallil, T. G. , Waicekauskas, K. , Morrow, D. G. , Kopren, K. M. , & Fu, W. (2013). External tools for collaborative medication scheduling. Cognition, Technology & Work, 15 , 121–131.
- Karasek, R. A. (1979). Job demands, job decision latitude, and mental strain: Implications for job redesign. Administrative Science Quarterly , 24 , 285–308.
- Karasek, R. A. , & Theorell, T. (1990). Healthy work: Stress, productivity, and the reconstruction of working life . New York: Basic Books.
- van der Klink, J. J. L. , Blonk, R. W. B. , Schene, A. H. , & van Dijk, F. J. H. (2001). The benefits of interventions for work-related stress. American Journal of Public Health, 91 , 270–276.
- Knight, B. G. , Silverstein, M. , McCallum, T. J. , & Fox, L. S. (2000). A sociocultural stress and coping model for mental health outcomes among African American caregivers in southern California . The Journals of Gerontology: Series B: Psychological Sciences and Social Sciences, 55B , 142–150.
- Kossek, E. E. , Thompson, R. J. , Lautsch, B. A. (2015). Balanced workplace flexibility: Avoiding the traps. California Management Review, 57 , 5–25.
- Kożusznik, M. , Rodriguez, I. , & Peiró, J. M. (2012). Cross-national outcomes of stress appraisal. Cross Cultural Management, 19 , 507–525.
- Kożusznik, M. , Rodriguez, I. , & Peiró, J. M. (2015). Eustress and distress climates in teams: Patterns and outcomes. International Journal of Stress Management, 22 , 1–23.
- Kristof-Brown, A. L. , Zimmerman, R. D. , & Johnson, E. C. (2005). Consequences of individuals’ fit at work: A meta-analysis of person-job, person-organization, person-group, and person-supervisor fit. Personnel Psychology, 58 , 281–342.
- LaMontagne, A. D. , Keegel, T. , Louie, A. M. , Ostry, A. , & Landsbergis, P. A. (2007). A systematic review of the job-stress intervention evaluation literature, 1990–2005. International Journal of Occupational and Environmental Health, 13 , 268–280.
- LaRocco, J. M. , Tetrick, L. E. , & Meder, D. (1989). Differences in perceptions of work environment conditions, job attitudes, and health beliefs among military physicians, dentists, and nurses. Military Psychology, 1 , 135–151.
- Lazarus, R. S. , & Folkman, S. (1984). Stress, appraisal, and coping . New York: Springer.
- Lazarus, R. S. , & Folkman, S. (1991). The concept of coping. In A. Monat & R. S. Lazarus (Eds.), Stress and coping: An anthology (3d ed.) (pp. 189–206). New York: Columbia University Press.
- LePine, J. A. , Podsakoff, N. P. , & LePine, M. A. (2005). A meta-analytic test of the challenge stressor-hindrance stressor framework: An explanation for inconsistent relationships among stressors and performance. Academy of Management Journal, 48 , 764–775.
- Lewin, K. (1936). Principles of topological psychology . New York: McGraw-Hill.
- Lewin K. (1951). Field theory in social science . New York: Harper and Row.
- Lewin, K. (1997). Resolving social conflicts & Field theory in social science . Washington, DC: American Psychological Association. Previously published in 1948 and 1951.
- Lin, B. C. , Kain, J. M. , & Fritz, C. (2013). Don’t interrupt me! An examination of the relationship between intrusions at work and employee strain. International Journal of Stress Management, 20 , 77–94.
- Liu, C. , & Li, H. (2017) Stressor and stressor appraisals: The moderating effect of task efficacy . Journal of Business and Psychology , 1–14.
- Liu, C. , Liu, Y. , Spector, P. E. , Shi, L. (2011). The interaction of job autonomy and conflict with supervisor in China and the United States: A qualitative and quantitative comparison. International Journal of Stress Management, 18 , 222–245.
- Liu, C. , Spector, P. E. , & Shi, L. (2007). Cross-national job stress: A quantitative and qualitative study. Journal of Organizational Behavior, 28 , 209–239.
- Luckhaupt, S. E. , Tak, S. , Calvert, G. M. (2010). The prevalence of short sleep duration by industry and occupational in the National Health Interview Survey. Sleep, 33 , 149–159.
- Luthans, F. , Youssef, C. M. , & Avolio, B. J. (2007). Psychological capital: Developing the human competitive edge . New York: Oxford University Press.
- Macan, T. H. (1994). Time management: Test of a process model. Journal of Applied Psychology, 79 , 381–391.
- Macan, T. H. , Shahani, C. , Dipboye, R. L. , & Philips, A. P. (1990). College students’ time management: Correlations with academic performance and stress. Journal of Educational Psychology, 82 , 760–768.
- Masuda, A. D. , Poelmans, S. A. Y. , Allen, T. D. , Spector, P. E. , Lapierre, L. M. , Cooper, C. L. , et al. (2012). Flexible work arrangements availability and their relationship with work-to-family conflict, job satisfaction, and turnover intentions: A comparison of three country clusters. Applied Psychology: An International Review, 61 , 1–29.
- McMahon, M. (2007). Think you might be addicted to email? You’re not alone . AOL.
- Monat, A. , & Lazarus, R. S. (Eds.). (1991). Stress and coping: An anthology (3d ed.). New York: Columbia University Press.
- Morimoto, H. , Shimada, H. , & Ozaki, K. (2013). Does stressor evaluation mediate sociocultural influence on coping selection? An investigation using Japanese employees. International Journal of Stress Management, 20 , 1–19.
- Narayanan, L. , Menon, S. , & Spector, P. E. (1999). A cross-cultural comparison of job stressors and reactions among employees holding comparable jobs in two countries. International Journal of Stress Management, 6 , 197–212.
- National Sleep Foundation (2005). Segment profiles . National Sleep Foundation.
- National Sleep Foundation (2013). How much sleep do adults need? . National Sleep Foundation.
- Nelson, D. L. , & Simmons, B. L. (2003). Health psychology and work stress: A more positive approach. In J. C. Quick & L. E. Tetrick (Eds.), Handbook of Occupational Health Psychology (pp. 97–119). Washington, DC: American Psychological Association.
- Norris, P. A. , Fahrion, S. L. , & Oikawa, L. O. (2007). Autogenic biofeedback training in psychophysiological therapy and stress management. In P. M. Lehrer , R. L. Woolfolk , & W. E. Sime (Eds.), Principles and practices of stress management (3d ed., pp. 175–205). New York: Guilford.
- Ogawa, N. (2009). Stress, coping behavior, and social support in Japan and the United States. Dissertation Abstracts International Section A , 69 , 3802.
- Oksanen, K. , & Ståhle, P. (2013). Physical environment as a source for innovation: Investigating the attributes of innovative space. Journal of Knowledge Management, 17 , 815–827.
- Page, K. M. , & Vella-Brodrick, D. A. (2009). The “what,” “why” and “how” of employee well-being: A new model. Social Indicators Research, 90 , 441–458.
- Parasuraman, S. , & Cleek, M. A. (1984). Coping behaviors and managers’ affective reactions to role stressors . Journal of Vocational Behavior, 24 , 179–193.
- Parasuraman, S. , & Purohit, Y. S. (2000). Distress and boredom among orchestra musicians: The two faces of stress. Journal of Occupational Health Psychology, 5 , 74–83.
- Pawelski, J. O. (2016). Defining the “positive” in positive psychology: Part II. A normative analysis . Journal of Positive Psychology, 11 , 357–365.
- Pearlin, L. I. , & Schooler, C. (1978). The structure of coping . Journal of Health and Social Behavior, 19 , 2–21.
- Peeters, M. A. G. , & Rutte, C. G. (2005). Time management behavior as a moderator for the job demand-control interaction. Journal of Occupational Health Psychology , 1 , 64–75.
- Peters, L. H. , & O’Connor, E. J. (1980). Situational constraints and work outcomes: The influence of a frequently overlooked construct. Academy of Management Review , 5, 391–397.
- Peters, L. H. , & O’Connor, E. J. (1988). Measuring work obstacles: Procedures, issues, and implications. In F. D. Schoorman & B. Schneider (Eds.), Facilitating work effectiveness (pp. 105–123). Lexington, MA: Lexington Books.
- Polly, S. (2014, July 2). Workplace well-being is not an oxymoron . Positive Psychology News Daily .
- Quick, C. J. , Quick, J. D. , Nelson, D. L. , & Hurrell, J. J. (2003). Preventive stress management in organizations . Washington, DC: APA.
- Quillian-Wolever, R. E. , & Wolever, M. E. (2003). Stress management at work . In J. C. Quick & L. E. Tetrick (Eds.), Handbook of occupational health psychology (pp. 355–375). Washington, DC: American Psychological Association.
- Ragsdale, J. M. , Beehr, T. A. , Grebner, S. , & Han, K. (2011). An integrated model of weekday stress and weekend recovery of students. International Journal of Stress Management, 18 , 153–180.
- Richardson, K. M. , & Rothstein, H. R. (2008). Effects of occupational stress management intervention programs: A meta-analysis. Journal of Occupational Health Psychology, 13 , 69–93.
- Rodríguez, I. , Kozusznik, M. W. , & Peiró, J. M. (2013). Development and validation of the Valencia Eustress-Distress Appraisal Scale. International Journal of Stress Management, 20 , 279–308.
- Rothbaum, F. , Weisz, J. R. , & Snyder, S. S. (1982). Changing the world and changing the self: A two-process model of perceived control. Journal of Personality and Social Psychology, 42 , 5–37.
- Rotter, J. B. (1966). Generalized expectancies for internal versus external control of reinforcement. Psychological Monographs, 80 , 609.
- Rousseau, V. , & Aubé, C. (2010). Social support at work and affective commitment to the organization: The moderating effect of job resource adequacy and ambient conditions. Journal of Social Psychology, 150 , 321–340.
- Saunders, T. , Driskell, J. E. , Johnston, J. , & Salas, E. (1996). The effect of stress inoculation training on anxiety and performance. Journal of Occupational Health Psychology, 1 , 170–186.
- Schaubroeck, J. , Ganster, D. C. , Sime, W. E. , & Ditman, D. (1993). A field experiment testing supervisory role clarification. Personnel Psychology, 46 , 1–25.
- Selmer, J. (2002). Coping strategies applied by Western vs overseas Chinese business expatriates in China. International Journal of Human Resource Management, 13 , 19–34.
- Siegrist, J. (1996). Adverse health effects of high effort/low reward conditions. Journal of Occupational Health Psychology, 1 , 27–41.
- Siegrist, J. (2010). Effort-reward imbalance at work and cardiovascular diseases. International Journal of Occupational Medicine and Environmental Health, 23 , 279–285.
- Siegrist, J. , Dragano, N. , Nyberg, S. T. , Lunau, T. , Alfredsson, L. , Erbel, R. , et al. (2014). Validating abbreviated measures of effort-reward imbalance at work in European cohort studies: The IPD-Work consortium. International Archives of Occupational and Environmental Health, 87 , 249–256.
- Sinha, B. K. , Willson, L. R. , & Watson, D. C. (2000). Stress and coping among students in India and Canada . Canadian Journal of Behavioural Science/Revue Canadienne Des Sciences Du Comportement , 32 (4), 218–225.
- Sinnott, J. , & Vatz, R. E. (2015, March 13). Maryland doesn’t trust state employees to manage their health . Baltimore Sun .
- Siu, O. L. , Cooper, C. L. , & Phillips, D. R. (2013, July 1). Intervention studies on enhancing work well-being, reducing burnout, and improving recovery experiences among Hong Kong health care workers and teachers . International Journal of Stress Management, 21 , 69–84.
- Sonnentag, S. (2012). Psychological detachment from work during leisure time: The benefits of mentally disengaging from work. Current Directions in Psychological Science, 21 , 114–118.
- Sørensen, O. H. , & Holman, D. (2014). A participative intervention to improve employee well-being in knowledge work jobs: A mixed-methods evaluation study. Work & Stress, 28 , 67–86.
- Spector, P. E. , Chen, P. Y. , & O’Connell, B. J. (2000). A longitudinal study of relations between job stressors and job strains while controlling for prior negative affectivity and strains. Journal of Applied Psychology, 85 , 211–218.
- Spector, P. E. , & Jex, S. M. (1998). Development of four self-report measures of job stressors and strains: Interpersonal Conflict at Work Scale, Organizational Constraints Scale, Quantitative Workload Inventory, and Physical Symptoms Inventory. Journal of Occupational Health Psychology, 3 , 356–367.
- State of Maryland . (n.d.). Wellness program frequently asked questions . Maryland.gov.
- Strentz, T. , & Auerbach, S. M. (1988). Adjustment to the stress of simulated captivity: Effects of emotion-focused versus problem-focused preparation on hostages differing in locus of control . Journal of Personality and Social Psychology, 55 , 652–660.
- Swanberg, J. E. , McKechnie, S. P. , Ojha, M. U. , & James, J. B. (2011). Schedule control, supervisor support and work engagement: A winning combination for workers in hourly jobs? Journal of Vocational Behavior, 79 , 613–624.
- Tarafdar, M. , Tu, Q. , Ragu-Nathan, B. S. , & Ragu-Nathan, T. , (2007). The impact of technostress on role stress and productivity. Journal of Management Information Systems, 24 , 301–328.
- Tepper, B. J. , & Henle, C. A. (2011). A case for recognizing distinctions among constructs that capture interpersonal mistreatment in work organizations . Journal of Organizational Behavior, 32 , 487–498.
- Tetrick, L. E. , & Winslow, C. J. (2015). Workplace stress management interventions and health promotion. Annual Review of Organizational Psychology and Organizational Behavior, 2 , 583–603.
- Thomas, D. C. , Au, K. , & Ravlin, E. C. (2003). Cultural variation and the psychological contract. Journal of Organizational Behavior, 24 , 451–471.
- Toker, S. , Shirom, A. , Melamed, S. , & Armon, G. (2012). Work characteristics as predictors of diabetes incidence among apparently healthy employees. Journal of Occupational Health Psychology, 17 , 259–267.
- Velez, B. L. , Moradi, B. , & Brewster, M. E. (2013). Testing the tenets of minority stres theory in workplace contexts. Journal of Counseling Psychology, 60 , 532–542.
- Verquer, M. L. , Beehr, T. A. , & Wagner, S. H. (2003). A meta-analysis of relations between person–organization fit and work attitudes. Journal of Vocational Behavior, 63 , 473–489.
- Villani, D. , Grassi, A. , Cognetta, C. , Toniolo, D. , Cipresso, P. , & Riva, G. (2013). Self-help stress management training through mobile phones: An experience with oncology nurses. Psychological Services , 10 , 315–322.
- Vischer, J. C. (2007). The effects of the physical environment on job performance: Towards a theoretical model of workspace stress. Stress & Health, 23 , 175–184.
- Wasti, S. A. , & Cortina, L. M. (2002). Coping in context: Sociocultural determinants of responses to sexual harassment . Journal of Personality and Social Psychology , 83, 394–405.
- Willert, M. V. , Thulstrup, A. M. , Hertz, J. , & Bonde, J. P. (2010). Sleep and cognitive failures improved by a three-month stress management intervention . International Journal of Stress Management, 17 , 193–213.
- Xiao Q. , Ottosson I. , & Carlsson I. (2013). Stressors and coping strategies in Chinese and Swedish students at a Swedish university. Chinese Journal of Clinical Psychology, 21 , 309–312.
Related Articles
- Work and Family
- Organizational Climate and Culture
- Physical Activity and Stress Reactivity
- The Roles of Psychological Stress, Physical Activity, and Dietary Modifications on Cardiovascular Health Implications
- Inflammation as a Biomarker Method in Lifespan Developmental Methodology
- Stress and Coping Theory Across the Adult Lifespan
- Occupational Health Psychology
Printed from Oxford Research Encyclopedias, Psychology. Under the terms of the licence agreement, an individual user may print out a single article for personal use (for details see Privacy Policy and Legal Notice).
date: 19 May 2024
- Cookie Policy
- Privacy Policy
- Legal Notice
- Accessibility
- [66.249.64.20|185.66.14.236]
- 185.66.14.236
Character limit 500 /500
Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals
- My Account Login
- Explore content
- About the journal
- Publish with us
- Sign up for alerts
- Review Article
- Open access
- Published: 09 February 2024
Major depressive disorder: hypothesis, mechanism, prevention and treatment
- Lulu Cui 1 , 2 , 3 ,
- Shu Li 1 , 2 , 3 ,
- Siman Wang 1 , 2 , 3 ,
- Xiafang Wu 1 , 2 , 3 ,
- Yingyu Liu 1 , 2 , 3 ,
- Weiyang Yu 1 , 2 , 3 ,
- Yijun Wang 1 , 2 , 3 ,
- Yong Tang ORCID: orcid.org/0000-0002-2543-066X 4 ,
- Maosheng Xia ORCID: orcid.org/0000-0003-4829-0812 5 &
- Baoman Li ORCID: orcid.org/0000-0002-3959-9570 1 , 2 , 3
Signal Transduction and Targeted Therapy volume 9 , Article number: 30 ( 2024 ) Cite this article
21k Accesses
323 Altmetric
Metrics details
- Cellular neuroscience
- Diseases of the nervous system
Worldwide, the incidence of major depressive disorder (MDD) is increasing annually, resulting in greater economic and social burdens. Moreover, the pathological mechanisms of MDD and the mechanisms underlying the effects of pharmacological treatments for MDD are complex and unclear, and additional diagnostic and therapeutic strategies for MDD still are needed. The currently widely accepted theories of MDD pathogenesis include the neurotransmitter and receptor hypothesis, hypothalamic-pituitary-adrenal (HPA) axis hypothesis, cytokine hypothesis, neuroplasticity hypothesis and systemic influence hypothesis, but these hypothesis cannot completely explain the pathological mechanism of MDD. Even it is still hard to adopt only one hypothesis to completely reveal the pathogenesis of MDD, thus in recent years, great progress has been made in elucidating the roles of multiple organ interactions in the pathogenesis MDD and identifying novel therapeutic approaches and multitarget modulatory strategies, further revealing the disease features of MDD. Furthermore, some newly discovered potential pharmacological targets and newly studied antidepressants have attracted widespread attention, some reagents have even been approved for clinical treatment and some novel therapeutic methods such as phototherapy and acupuncture have been discovered to have effective improvement for the depressive symptoms. In this work, we comprehensively summarize the latest research on the pathogenesis and diagnosis of MDD, preventive approaches and therapeutic medicines, as well as the related clinical trials.
Similar content being viewed by others

Prospective biomarkers of major depressive disorder: a systematic review and meta-analysis

Major depressive disorder

Brain connectivity in major depressive disorder: a precision component of treatment modalities?
Introduction.
Major depressive disorder (MDD), a main cause of disability worldwide, is characterized by physical changes such as tiredness, weight loss, and appetite loss. Anhedonia is a classic feature of MDD, and MDD is also accompanied by a lack of drive, sleep issues, cognitive challenges, and emotional symptoms such as guilt. 1 The prevalence of depression is increasing yearly. About 300 million people in the world are affected by MDD, which has become one of the main causes of disability. 2 In 2018, MDD ranked third in terms of disease burden according to the WHO, and it is predicted to rank first by 2030. 3 Pregnant women, elderly people, children, and others have a higher incidence rate of MDD, which may be related to genetic, psychological, and social factors. 4 Depression can be accompanied by recurrent seizures, which may occur even during remission or persist for longer than the disease itself. 5 Pharmacological therapies for MDD can effectively control symptoms; thus, patients may experience recurrence within a short time after discontinuing medication. 6 During recurrence, the patient experiences symptoms of low mood, loss of interest in life, fatigue, delayed thinking, and repeated fluctuations in mental state. 7
There is a certain correlation between the occurrence of MDD and social development. 8 A survey reported that with the development of the economy and increased life pressure, MDD has begun to emerge at a younger age, and the incidence of MDD in women is approximately twice that in men. 9 Specifically, women are more likely to develop depressive symptoms when they encounter social emergencies or are under significant stress. 8 Additionally, autumn and winter have been reported to be associated with a high incidence of MDD, namely, seasonal depression. 10
The clinical symptoms of MDD include a depressed mood, loss of interest, changes in weight or appetite, and increased likelihood of committing suicide. 11 These symptoms are also listed as the criteria for MDD in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). 12 In addition to the criteria listed in the DSM-5, the criteria reported in the International Classification of Diseases (ICD-10) are also used to guide clinical diagnosis. 13 However, due to the lack of characteristic symptoms and objective diagnostic evidence for MDD, identification and early prevention are difficult in the clinic. 14
Due to the complexity of the pathological mechanism of MDD, accurate diagnostic approaches and pharmacological therapeutic strategies are relatively limited. Several hypothesis were developed to explain MDD pathogenesis pathogenic including (i) the hypothalamic‒pituitary‒adrenal (HPA) axis dysfunction hypothesis, (ii) the monoamine hypothesis, (iii) the inflammatory hypothesis, (iv) the genetic and epigenetic anomaly hypothesis, (v) the structural and functional brain remodeling hypothesis, and (vi) the social psychological hypothesis 3 , 15 , 16 (Fig. 1 ). However, none of these hypotheses alone can fully explain the pathological basis of MDD, while many mechanisms proposed by these hypotheses interact with each other. In recent years, great progress has been made in identifying novel pharmacological therapies, diagnostic criteria, and nonpharmacological preventive measures for MDD, initiating related clinical trials. Specifically, increasing evidence suggests that astrocytic dysfunction plays a substantial role in MDD. 17 Pharmacological ablation of astrocytes in the medial prefrontal cortex (mPFC) causes depressive-like symptoms in experimental animals, 18 and postmortem studies of patients with MDD have shown reduced densities of glial cells in the prefrontal cortex (PFC), hippocampus and amygdala. 19 In addition, glial fibrillary acidic protein (GFAP), one of the markers of astrocytes, is expressed at various levels, 20 and the levels of connexins, 21 glutamine synthase (GS), glutamate transporter-1 (GLT-1), 21 , 22 and aquaporin-4 (AQP4) 23 are reduced in patients with MDD.

An outline map of the hypotheses to explain MDD pathogenesis. (I) HPA axis dysfunction hypothesis: high levels of glucocorticoids (GCs) play a core role in the pathogenesis of MDD, and thyroid hormone (TH) and estrogen are also involved in functions of the HPA axis; (II) the monoamine hypothesis: the functional deficiency of serotonin (5-HT), dopamine (DA) and norepinephrine (NE) are the main pathogenesis of MDD; (III) the inflammatory hypothesis: the neuro-inflammation induced by reactive oxygen species (ROS), inflammatory cytokines and inflammasomes activation is suggested to promote the occurrence of MDD; (IV) the genetic and epigenetic anomaly hypothesis: some genes are susceptible in the patients with MDD, including presynaptic vesicle trafficking (PCLO), D2 subtype of the dopamine receptor (DRD2), glutamate ionotropic receptor kainate type subunit 5 (GRIK5), metabotropic glutamate receptor 5 (GRM5), calcium voltage-gated channel subunit alpha1 E (CACNA1E), calcium voltage-gated channel auxiliary subunit alpha2 delta1(CACNA2D1), DNA methyltransferases (DNMTs), transcription levels of somatostatin (SST), fatty acid desaturase (FADS); (V) the structural and functional brain remodeling hypothesis: the postmortem results of patients with MDD are mostly associated with the reduced densities of glial cells in the prefrontal cortex (PFC), hippocampus, and amygdala; (VI) the social psychological hypothesis: the traumatic or stressful life events are the high risks of the occurrence of MDD. Adobe Illustrator was used to generate this figure
In this review, we summarize the latest research on the etiology, pathogenesis, diagnosis, prevention, mechanism, and pharmacological and nonpharmacological treatment of MDD as well as related clinical experiments.
Potential etiologies and pathogenic hypotheses
The common pathogenic factors.
Although the etiology of MDD is still unclear, it is widely accepted that MDD is associated with multiple pathogenic factor. In addition to well-known mental factors, MDD is also related to genetic factors, social stress, and even other common chronic diseases. Therefore, the etiology of MDD cannot be described from the perspective of a single factor.
Genetic factors
Although the etiology of MDD is still unclear, numerous studies have been performed and various models have been employed to explore the genetic factors, environmental factors and gene-environment interactions related to the disease. 24 Recent family, twin, and adoption studies suggests that genetic factors play a crucial role in the occurrence of MDD. 25 As a genetically diverse illness, MDD has a heritability of 30–50%. 26 Over 100 gene loci, including those associated with presynaptic vesicle trafficking (PCLO), dopaminergic neurotransmission (a primary target of antipsychotics), glutamate ionotropic receptor kainate type subunit 5 (GRIK5), and metabotropic glutamate receptor 5 (GRM5), and neuronal calcium signaling such as calcium voltage-gated channel subunit alpha1 E (CACNA1E) and calcium voltage-gated channel auxiliary subunit alpha2 delta1 (CACNA2D1), are found to be associated with an increased risk of MDD by genome-wide association studies. 19 , 27 , 28 In addition, rare copy number variants are also identified to be related to MDD risk, there may be three copy number variants (CNV) loci associated with Prader-Willis syndrome: 1q21.1 duplication, 15q11-13, and 16p11.2. However, no single genetic variation has been found to increase the risk of MDD thus far. 26 Genome Wide Association Studies (GWAS) identified 178 genetic risk loci and proposed over 200 candidate gene, using of biobank data, novel imputation methods, combined with clinical cases improved the ability to identify MDD specific pathways. 29 In the study of human MDD transcriptome, there are defects in the transcription levels of somatostatin (SST) in the subgenus anterior cingulate cortex and amygdala of MDD patients, 30 , 31 and SST levels are directly involved in the cellular processes that affect the synaptic output of intermediate neuronal circuits. 32 Recent studies revealed that gender specific genomic differences in MDD patients, the downregulation of the MDD-related gene Dusp6 in females leads to an increased susceptibility to stress, but this expression is not present in male mice. 33 In addition, studies of drug gene interactions, transcriptional genes associated with the risk of MDD are also reported, such as D2 subtype of the dopamine receptor (DRD2) and fatty acid desaturase (FADS), 34 which may serve as promising new targets for therapeutic intervention points. Thus, genetic variants are expected to have only minor effects on the overall risk of disease, and various hereditary factors combined with environmental factors such as stress are likely more essential for the development of MDD. 35
Stress factors
In addition to heritable factors, environmental influences such as stress also significantly contribute to the development of MDD, both independently and in conjunction with genetic factors. 26 Numerous studies have suggested that adverse life events can lead to the development of MDD. 18 A major depressive episode always follows a traumatic or stressful life event. In particular, severe events such as job loss, extramarital affairs and divorce are known to provoke the onset of the disease. 36 The exact pathological mechanism by which social stress results in the development of MDD is still not known, mainly due to the difficulty of separating social factors from genetic factors in patients and the impracticality of exposing disease model animals to relevant environmental factors. It has been proved that the changes in the structure and function of neurons may occur under the chronic stress and lead to the occurrence of MDD. 37 , 38 In some MDD patients, stress leads to long-term elevated glucocorticoids, resulting in synaptic structural changes and remodeling, and the stress-induced hyperactivity of the HPA axis leads to negative feedback imbalance of the HPA axis, which is also related to depression. 39 Studies on damage to microglia and astrocytes suggest the significance of glial cells in the development of environmental factor-induced depression-like behaviors in mice. 40 In addition, our previous studies proved that chronic environmental stress-induced depressive-like behaviors in mice can be dependent on purinergic ligand-gated ion channel 7 receptor (P2X 7 R) activation in astrocytes. 41
Comorbidity factors
The existence of various physiological and psychological comorbidities in patients with depression reveals a clear link between physical and mental health, which has given us a better understanding of MDD. The presence of MDD is a risk factor for a variety of complications, including neurodegenerative diseases (such as dementia, Alzheimer’s disease, and Parkinson’s disease), cardiovascular diseases (such as ischemic coronary artery disease and myocardial infarction), metabolic and endocrine diseases (such as obesity in females and diabetes in males), and some autoimmune diseases. 42 , 43 The relationship between the onset of MDD and several diseases is complex and potentially bidirectional in nature. 44 The impact of depression on society and the economy is increased by the existence of comorbidities. 45 Specifically, in 2018, comorbid disorders rather than MDD itself were responsible for 63% of all costs related to MDD in the United States. 46 , 47 Furthermore, compared to people without depression, patients with MDD have been demonstrated to have a shorter life expectancy. 48 Additionally, the worsening of comorbidities could be a factor in the premature mortality of MDD patients. 44
Neurotransmitter and receptor hypothesis
The traditional monoamine theory contends that in addition to common pathogenic factors, deficiencies in monoamine neurotransmitters, such as serotonin (5-HT), dopamine (DA) and norepinephrine (NE), are the root cause of clinical depression. 49 Selective serotonin reuptake inhibitors (SSRIs), a class of antidepressants that have been proven to successfully treat clinical depression, were developed in response to this hypothesis, which was derived primarily on the basis of the pharmacological mechanism of drug that were accidentally discovered to act as antidepressants. It is also crucial to note that astrocytes express NE transporter (NETT) and 5-HT transporter (SERT), which are the targets of some traditional antidepressants. 50 A previous study suggested that the function of astrocytes can be directly regulated by SSRIs. 51 Monoamine oxidase (MAO) activates the metabolism of adrenaline and triggers calcium signaling in astrocytes, 52 which suggests that antidepressants may directly affect astrocytes by preventing them from reabsorbing monoamines.
Serotonin (5-HT)
An essential neuromodulatory transmitter with specific neuroplastic properties is serotonin. Numerous investigations have demonstrated that 5-HT is intimately related to the pathophysiological process of major depression. The 5-HT hypothesis primarily asserts that a decrease in the 5-HT level is a risk factor for depression. 53 In addition, low levels of 5-HT and L-tryptophan, which is a precursor of 5-HT, 54 in blood platelets are also found in depressed people. Additionally, long-term treatment with fluoxetine, a typical SSRIs, reverses the stress-induced reduction in the quantity of astrocytic cells in the hippocampus in a tree shrew model of depression. 55
5-HT receptors, which are mostly found on the bodies and dendrites of neurons, play a role in the pathogenesis of MDD. 56 To date, 5-HT receptor subfamilies comprising 14 different receptor subunits expressed in various brain regions, namely, 5-HT 1A , 5-HT 1B , 5-HT 1D , 5-HT 1E , 5-HT 1F , 5-HT 2A , 5-HT 2B , 5-HT 2C , 5-HT 3 , 5-HT 4 , 5-HT 5A , 5-HT 5B , 5-HT 6 and 5-HT 7 , have been reported. Among these 5-HT receptor subtypes, the 5-HT 1 , 5-HT 2 , 5-HT 6 , and 5-HT 7 subtypes are expressed on brain and spinal astrocytes in humans and rodents. Numerous 5-HT receptors expressed on astrocytes are G-coupled proteins that are associated with changes in the concentration of free cytosolic calcium ([Ca 2+ ] i ). These changes may trigger the release of a variety of astrocyte-derived signaling modulators, which may control neuronal activity. 57 In astrocytes, 5-HT has a strong effect on the 5-HT 2B receptor. 58 5-HT receptors have been extensively studied to determine the pharmacological mechanism of antidepressants, and many novel pharmaceutical preparations are being investigated. For example, some novel antidepressants function as agonists of the 5-HT 1A , 5-HT 2B , or 5-HT 4 receptor or antagonists of the 5-HT 1B , 5-HT 2A , 5-HT 2C , 5-HT 3 , 5-HT 6 , or 5-HT 7 receptor. 59
Administration of fluoxetine in different concentrations to astrocytes expressing the 5-HT 2B receptor may activate distinct signaling pathways to control gene expression. Fluoxetine reduces the mRNA expression of c-Fos through the PI3K/AKT signaling pathway after acute application at concentrations below 1 μM, while the treatments with the higher doses (above 5 μM), it increases the gene expression of c-Fos via the MAPK/ERK signaling pathway in astrocytes. 60 Then, in the nucleus, the altered transcription factor c-Fos can further biphasic change the expression of caveoline under the chronic treatments, thus the alteration levels of caveoline on cellular membrane can finally affect the downstream activation of PTEN/PI3K/AKT/GSK3β 60 . The GSK3β polymorphisms are associated with the high risk of MDD in Chinese Han Population. 61 In our recent reports, the activation of GSK3β is also increased in the sorted astrocytes from the MDD-related stress-treated mice model and MDD clinic patients’ plasma. 62 In addition, after fluoxetine-mediated stimulation of the 5-HT 2B receptor in astrocytes, epidermal growth factor receptor (EGFR) is transactivated and subsequently activates the MAPK/ERK and PI3K/AKT signaling cascades, which control the expression of mRNA or proteins that may be linked to mood disorders, such as SERT. Ca 2+ -dependent phospholipase A2 (cPLA 2 ), adenosine deaminase acting on RNA 2 (ADAR2), and kainate receptor subtype 2 (GluK2) are all involved in kainate receptor signaling. 63 , 64 These discoveries promise astrocytic 5-HT 2B receptors can be the potential pharmacological target of SSRIs (Fig. 2 ).

Schematic illustration of the pharmacological mechanism of fluoxetine in astrocytes. Acute treatment with fluoxetine at low concentrations (green arrows) stimulates Src, which phosphorylates EGF receptors by activating 5-HT 2B receptors (5-HT 2B R) and activates the PI3K/AKT signaling pathway. AKT phosphorylation induced by fluoxetine at low concentrations inhibits the expression of cFos and subsequently decreases the expression of caveolin-1 expression (chronic effects), which in turn decreases the membrane content of PTEN, induces phosphorylation and stimulation of PI3K and increases the phosphorylation of GSK3β, thus suppressing its activity. At higher concentrations, fluoxetine (red arrows) stimulates metalloproteinases (MMP) by activating 5-HT 2B R and induces the release of growth factors, which stimulates EGF receptors and activates the mitogen-activated protein kinases (MAPK)/ERK 1/2 signaling pathway. ERK 1/2 phosphorylation induced by fluoxetine at high concentrations stimulates the expression of cFos and subsequently increases the expression of caveolin-1 (chronic effects), which inhibits PTEN/PI3K/AKT/GSK3β, 60 ultimately leading to MDD like behavior. At high concentration, fluoxetine can also stimulate the activation of cPLA 2a by the transactivation of EGFR/MAPK/ERK 1/2 pathway, and the activated ERK 1/2 can also increases the expression of cPLA 2a at chronic treatments. 61 In addition, the increased expression of cFos induced by fluoxetine can further increases the RNA editing of GluK2 by increasing the expression of ADAR2 at the chronic treatments, the function of the edited GluK2 by fluoxetine is down-regulated, which causes the acute glutamated induced Ca 2+ -dependent ERK phosphorylation is suppressed. 63 Adobe Illustrator was used to generate this figure
Norepinephrine (NE)
NE released by the locus coeruleus (LC) can participate in regulating various neural functions, such as smell, movement, and sensation. 65 It is significant to note that after being released, noradrenaline (NA) is not restricted to the area around the synaptic cleft and can reach nearby glial cells. 66 Atomoxetine is a norepinephrine reuptake inhibitor (NRI) clinically used for the treatment of MDD. After systemic inflammatory attack with bacterial lipopolysaccharide (LPS), atomoxetine can decrease neuroinflammation in the rat cerebral cortex. 67
The bioavailability of 5-HT and NE are increased by antidepressants called serotonin/norepinephrine reuptake inhibitors (SNRIs), which belong to antidepressants. Currently, new SNRIs, including duloxetine (DXT), 68 desvenlafaxine (DVS), 69 and venlafaxine, 70 are widely used in MDD patients resistant to other treatments. Chronic treatment with DXT increases the expression of connexin 43 (Cx43), a crucial component of astrocyte gap junctions, in the rat PFC, preventing chronic unpredictable stress-induced dysfunction of astrocyte gap junctions and reversing the depressive-like behaviors caused by gap junction inhibition. 71 A novel therapeutic target for MDD is transforming growth factor β1 (TGF-β1), the expression of which is controlled by antidepressants. Venlafaxine has also been found to exert neuroprotection by boosting the production of type 2 fibroblast growth factor (FGF-2) and transforming growth factor 1 TGF-β1 in astrocytes following stroke. 72 However, the expression of protein markers of astrocytes and neurons is unaffected by DVS, and the chronic unpredictable mild stress (CUMS)-induced reduction in the levels of myelin- and oligodendrocyte-related proteins can be prevented by DVS. 69 DVS may reduce oligodendrocyte dysfunction in the CUMS mouse model by altering cholesterol production and reducing depression-like phenotypes. 69
Dopamine (DA)
There is increasing evidence that people with depression have reduced dopamine neurotransmission. 73 Astrocytes in the lateral habeula are involved in regulating depressive-like behavior, 74 whereas the reward circuit is mediated by the striatum. 75 The dorsolateral part of the striatum is linked to the drug-seeking behavior and drug addiction associated with psychiatric disorders. As the major input to the basal ganglia, the striatum and related nuclei are linked to psychiatric morbidity, while the chronic stress reduces dopamine levels in areas such as the striatum and hippocampus. 76 Due to processes involving dopamine D2 receptor signaling, 77 the glutamine level increases in the presence of dopaminergic lesions and decreases in the presence of a high DA level. 78 DA signaling is considered to play a key role in astrocyte-neuron crosstalk in the striatum. 79 Sulpiride is an antidepressant that blocks the ability of the GLT-1 inhibitor TFB-TBOA to induce synaptic depression 80 and partly attenuates the impact of fluorocitrate (a metabolic uncoupler that blocks aconitase in the tricarboxylic acid (TCA) cycle) on synaptic output. According to these results, astrocyte dysfunction results in an increase in DA levels, which decreases neuronal activity resulting from the binding of DA to dopamine D2 receptors, 80 which generates neuronal depolarization, reducing DA selectivity at dopamine D1-like receptors and promoting DA inhibition through dopamine D2 receptors, which may contribute to increasing extracellular glutamate levels. 81 An increase in DA signaling brought on by compromised astrocyte activity may induce a long-lasting change in striatal neurotransmission 80 since DA signaling is crucial for both structural and synaptic plasticity. 82
Glutamate is the main excitatory neurotransmitter in the central nervous system (CNS) 83 and can be released by neurons through exocytosis, which in turn activates extracellular N-methyl-D-aspartate receptors (eNMDARs) in neurons, leading to synaptic loss. 84 Exosynaptic glutamate also contributes to metabolism in neurons and astrocytes. When exosynaptic glutamate is taken up by astrocytes, it can become a substrate for glutamine synthesis or be metabolized by astrocytes and neurons. 85 In addition, extracellular glutamate can also promote glucose uptake by astrocytes and inhibit glucose uptake by neurons. Therefore, glutamate is an important signal that mediates the interaction between central neurons and astrocytes, and its normal release and transport are the result of the functional cooperation between neurons and astrocytes. Glutamate homeostasis and neurotransmission play a major role in the onset of depression and anxiety. Studies have shown that glutamate levels in frontal cortex samples from autopsied patients with severe depression are increased, and antidepressants can restore normal glutamate levels. 86 It has been observed in animal models that sustained glucocorticoid stimulation can increase the excitability of glutamatergic neurons and simultaneously decrease the number and plasticity of astrocytes, in addition to decreasing neuronal dendrite connectivity in the hippocampus and frontal cortex, leading to depression. 87
It is well-documented that astrocytes have a wide range of modulatory functions that may either increase or decrease the release of many different neurotransmitters. Specifically, astrocytes are essential regulators of glutamatergic neurotransmission, and reuptake of glutamate by astrocytes regulates excitatory synaptic activity. 85 When a large amount of glutamate is released from neuronal vesicles, glutamate clearance is mainly achieved by glutamate transporters (EAATs) on the membrane of astrocytes, which transport excess glutamate into astrocytes, where it is converted to glutamylamine through the action of glutamine synthase, reducing damage to neurons. 88 , 89 In the classic glutamate-glutamine cycle, astrocytes and neurons convert glutamate to the nonexcitatory amino acid glutamine, which is then released back into the extracellular space and absorbed by neurons. Alterations in astrocytic glutamate clearance are known to occur in schizophrenia and other psychiatric illnesses, and mice with glutamate/aspartate transporter (GLAST) deletion show phenotypic abnormalities such as mental and behavioral deficits. 90 , 91
Adenosine triphosphate (ATP)
Ectonucleotidases that are found in synapses can catabolize extracellular ATP to produce adenosine, and synapses also contain bidirectional nucleoside transporters that can release adenosine. 92 Adenosine primarily stimulates inhibitory A1 and facilitatory adenosine receptors (A 2A R) to play function. 93 Notably, depressive behavior is linked to purinergic signaling. Depressive-like symptoms are exacerbated by activation of P2X 7 R in glial cells. 94 Polimorphisms at P2X 7 R increase vulnerability to mood disorders whereas P2X 2 R-mediated neuronal activity is decreased in mice exposed to chronic stress due to insufficient ATP release from astrocytes. 95 According to our earlier studies, chronic sleep deprivation (SD) can cause depressive-like behaviors by increasing extracellular ATP levels in vivo. 41 Acting through P2X 7 R and FoxO3a cascade ATP inhibits expression of the 5-HT 2B receptor, the decrease in extracellular ATP levels caused by chronic stress and an increase in ATP levels caused by SD are both linked to depressive-like behaviors. 41 In detail, the elevated extracellular ATP induced by SD stress stimulates P2× 7 R and down-regulates the expression of 5-HT 2B R by suppressing the activation of AKT, which inhibits the phosphorylation of FoxO3a and promotes its transportation into the nucleus, the reduced 5-HT 2B R alleviates the inhibition of STAT3 to cPLA 2 , the activated cPLA 2 further increases the release of AA and PGE2, these indicators have high relationship with the depressive-like behaviors, because in P2X 7 R knockout mice, the above changes of these indicators and behavioral performance are all eliminated. 41 This increased activation of cPLA 2 and the elevated levels of AA and PGE2 in astrocytes are supported by our discoveries in MDD patients’ plasma. 62
After building a stress injury model in rats through maternal separation (MS), it is found that MS obviously reduces the total length of apical dendrites, however, the use of A 2A R antagonists could prevent synaptic loss 96 and reverse behavioral, electrophysiological, and morphological damage caused by MS, 97 this is related to the activity reconstruction of the HPA axis. In another study, the abnormally increased A 2A R in the lateral septum(LS) is a key factor in recurrent stress for leading to depressive-like behaviors. This function is mainly achieved by the increased activity of A 2A R-positive neurons and the inhibited activity of ambient neurons, associating with the neural circuits of dorsomedial hypothalamus(DMH) and lateral habenular(LHb). 98
Caffeine is an adenosine receptor antagonist, and epidemiological studies have shown that the intake of caffeine is closely related to the occurrence of suicide 99 and depression. 100 Since A 2A R polymorphisms are associated with emotional problems, adenosine A 2A R overexpression leads to emotional dysfunction, and A 2A R blockade protects against the persistent emotional disturbance brought on by stress. 101 Moreover, animal experiments have demonstrated that A 2A R are upregulated in chronic stress animal models. 102 Additionally, neuronal A1 receptors exhibit hypofunction caused by a decrease in astrocyte-derived adenosine levels; 103 this decrease, as well as depressive-like behavior, can be reversed by certain antidepressants. 104 , 105
HPA axis hypothesis
Stress and MDD are closely related, and stressful life events can often lead to depressive episodes. The activation of the HPA axis by stress can cause cognitive and emotional changes. 106 An increase in HPA activity is one of the most common neurobiological alterations in depressed people. Studies have shown that the main factor contributing to the elevation of hypothalamic-pituitary activity is the increased production of corticotropin-releasing hormone (CRH). In addition, pituitary adrenal corticotropic hormone (ACTH) is released in response to CRH, which in turn triggers the adrenal cortex to release glucocorticoids (GCs).
Glucocorticoids
The HPA axis, a component of the neuroendocrine system, is commonly associated with the stress response. Hyperactivity of the HPA axis is thought to be an important pathophysiological mechanism underlying depression. High HPA activity is among the most typical neurobiological alterations in depressed individuals. The HPA axis is the primary stress response system that produces GCs, which are a class of steroid hormones. There is evidence that GCs, which are released in response to stress, are harmful to neurons in various brain regions. The hypothalamic paraventricular nucleus (PVN) rapidly secretes CRH and arginine vasopressin (AVP) 107 when the HPA axis is activated by stress. The anterior pituitary is stimulated by CRH and AVP to produce ACTH, which in turn increases the release of GCs into the bloodstream. 108
The GC and mineralocorticoid (MC) receptors GR and MR are members of the nuclear receptor (NR) superfamily. Both NRs can be triggered by binding to either MCs (such as aldosterone) or GCs (such as cortisol). However, the affinity of MR for its ligands is 10 times higher than that of GR for its ligands. 109 , 110 GRs are expressesd at higher levels and particularly concentrated in the pituitary and hypothalamus, as well as a variety of regions of the limbic system (including the amygdala, hippocampus, and PFC), which are important for cognitive and psychological functions.
To prevent loss of control over the HPA axis, GCs exert negative feedback on the axis in all regions involved (the limbic system, hypothalamus, and pituitary). Some data suggest that HPA axis imbalance and high levels of GCs play a core role in the pathogenesis of MDD and suggest that GR may serve as an important target for treating depression. 111
Thyroid hormone
Thyroxine (T4) and triiodothyronine (T3) are the two primary Thyroid hormones (THs) that regulate metabolism, protein synthesis, the growth of bones, and nervous system development. Thyrotropin-releasing hormone (TRH), which regulates the synthesis of thyroid-stimulating hormone (TSH) by the anterior pituitary gland, is mostly produced by neurons in the PVN. TSH stimulates the thyroid gland to produce T3 and T4. The levels of serum-free T4 and free T3 are regulated by negative feedback from pituitary TSH release. Tissue deiodinase mostly transforms T4 into the less physiologically active metabolite reverse T3 and the more biologically active metabolite T4. 112
Overactivity of the HPA axis may be caused by damaged astrocytes and aberrant GR function. The HPA and hypothalamic-pituitary-thyroid (HPT) axes are inextricably linked. The most important related finding is that cortisol directly affects TRH secretion (which regulates TSH release), potentially through the response of GCs to TRH mRNA expression in neurons. According to research, hypercortisolemia may result in a reduction in TRH mRNA levels in the mid-caudal PVN. 113 TRH expression in the PVN is lower in nonpsychiatric patients treated with corticosteroids, and the mRNA levels of TRH are lower in the PVN of depressed patients who have recurrent suicidal thoughts. This suggests that the effect of hypothalamic TRH is weaker in these individuals.
THs are required for neuronal growth and function not only in the periphery but also in the CNS, 114 where they promote the formation of microglia, astrocytes, including radial glial cells, and oligodendrocytes. The role of THs in glial cells is becoming clear because of new discoveries in the field of glial cell biology. THs affect the shape and proliferation of astrocytes, as well as the organization and expression of GFAP/vimentin, and boost GS activity. 115 T3 has an effect on glial morphology and hence on glial function in the adult brain; therefore, it also has an effect on neuron-glia interactions. 115 , 116 It has been shown that T3 induces astrocyte proliferation by autocrine production of growth factors such as epidermal growth factor (EGF) and FGF-2. Apart from their proliferation-promoting impact, these growth factors increase and modify the pattern of deposition of the extracellular matrix components laminin and fibronectin, therefore boosting cell adherence and attachment to the substratum. Together with the discovery that animals with hypothyroidism and mice with TH receptor mutations display significant defects in glial development, these findings indicate that astrocytes are TH targets and that TH can protect neurons and astrocytes from glutamate toxicity. 115
The hippocampus is closely related to memory and learning, and estrogen plays an important role in these processes. Estrogen increases the proliferation, migration, and differentiation of neurons in the dentate gyrus to maintain hippocampal function and is also important for controlling the HPA axis. 117
Estrone (E1), estradiol (E2), and estriol (E3) are the three physiological estrogens; among these estrogens, E2 is the most active, and its level quickly decreases throughout menopause. 118 E2 has been demonstrated in numerous studies to alter systems involved in the pathophysiology of depression, including the serotonin and norepinephrine systems, and to considerably alleviate depressive symptoms in animal models. Estrogen therapy can decrease the quantity of 5-HT 1 and β-adrenergic receptors while increasing the quantity of 5-HT 1 receptors. 119 In addition, estradiol may influence the pathogenesis of male MDD patients. 120 In animal models, E2 has been shown to alleviate depressive-like behavior. 121 , 122 Estrogen receptor 1 (ER1) and estrogen receptor 2 (ER2) are transcription factors that are members of the NR family. Activating ER2 with a range of ER2 agonists has been reported to reduce stress-induced HPA activity and anxiety-like behaviors. 123 , 124
Astrocytes are estrogen targets, 125 as both ER1 and ER2 receptors are present on the astrocyte membrane or intracellularly in astrocytes. The transmembrane receptors ER and GPR30 have been shown to facilitate nongenomic and fast estrogen signaling in astrocytes, contributing to the neuroprotective effects of E2. In mature astrocytes differentiated from human induced pluripotent stem cells (iPSC)-derived astrocyte progenitors, ketamine can exert rapid antidepressant effects through the activation of amino-3-hydroxy-5-methyl-4-isoxazole propionic acid (AMPA) glutamate receptors, and estrogen enhances this effect of ketamine by increasing the gene expression of AMPA receptor subunits. 126
The obese gene (OB) encodes the hormone leptin, which is derived from adipocytes and the stomach and exerts its function through a specific receptor (OB-R). Leptin controls the function of the HPA axis 127 via its receptor in the hypothalamus. The cerebral cortex, hippocampus, hypothalamus, dorsal raphe (DR) nucleus, arcuate nucleus, and solitary tract nucleus are some regions of the brain that can express leptin receptors. Increasing experimental data have recently shown that leptin is linked to the pathological and physiological processes of numerous mental illnesses and plays a vital regulatory role in the CNS. 128 , 129 According to our previous reports, leptin can enhance the pharmacological effects of fluoxetine in astrocytes sorting from GFAP-GFP transgenic mice. 130 Leptin selectively increases the expression of the astrocytic 5-HT 2B receptor by activating the JAK2/STAT3 pathway, and fluoxetine in turn stimulates the 5-HT 2B receptor and increases the secretion of brain-derived neurotrophic factor (BDNF) from astrocytes in vivo, thus ameliorating depressive-like behaviors. 130 All of these findings indicate leptin’s potential to boost protein expression and functionally stimulate SERT.
Cytokine hypothesis
MDD is accompanied by changes in the levels of proinflammatory cytokines and trophic factors, including BDNF, interleukins (IL-1β, IL-6), and tumor necrosis factor alpha (TNF-α). Increasing data suggest that the production of certain cytokines by brain astrocytes plays a significant role in the pathogenesis of MDD.
Oxidative stress
Oxidative stress (OS), which is caused by an imbalance between antioxidants and reactive oxygen species (ROS), can harm proteins, lipids, or DNA. The activity of monoamine oxidase, the enzymes that break down monoamines such as DA, 5-HT and NE, is influenced by ROS and in turn can increase ROS production in mitochondria. The brain is more vulnerable to OS than other organs. In depression, OS plays a crucial role. 131 , 132 The brain is particularly sensitive to OS due to numerous variables, including rapid oxidative energy metabolism (a process through which ROS, which are harmful molecules, are constantly produced), high levels of unsaturated fatty acids (which are vulnerable to lipid peroxidation), and relatively low intrinsic antioxidant capability. 133 Adults with MDD exhibit ROS-mediated reductions in nitric oxide (NO)-dependent dilation. 134
Thioredoxin reductase, heme-oxygenase 1, glutathione, and glutathione peroxidase are only a few of the ROS-detoxifying enzymes that are abundant in astrocytes. 135 Astrocytes are the major producers of glutathione in the brain because they express a system xc-cyttine/glutamate antiporter, which does not exist in neurons; hence, neurons cannot synthesize glutathione. Notably, astrocytes can protect nearby neurons against toxic dosages of NO, H 2 O 2 , and superoxide anion in combination with NO, iron, or 6-hydroxydopamine in coculture systems, 135 indicating that neurons rely on the strong antioxidant capacity of astrocytes for protection against OS. Nuclear factor erythroid 2 (Nrf2), a redox-sensitive transcription factor required for coordinating the cellular antioxidant response, can be activated by astrocytes. In our recent study, lithium salt (Li + ) was found to effectively alleviate ischemia-induced anhedonia in mice by suppressing the production of mitochondrial ROS in glial cells. 136
Recent investigations have indicated that MDD is caused by increased ROS production and promotes inflammation. 137 The brain has weak antioxidative defenses and a high oxygen consumption rate, making it particularly susceptible to OS. Inflammasomes in microglia can be activated by ROS, which causes inflammatory cytokines, including TNF-α, IL-1β, and IFN-γ, to be produced. 138 Neuroendocrine-immune activities can be compromised by inflammation, which can also result in numerous disorders, such as MDD. Proinflammatory cytokines have become pathological indicators of MDD, and using the right antioxidants to combat ROS may be a useful method for treating MDD.
Proinflammatory cytokines
Higher levels of inflammation increase the chance of developing new-onset depression. 138 , 139 Although depression can cause inflammation, its cause is still unclear and may be influenced and regulated by immune cells, inflammatory cytokines, and the nervous system. In addition to contributing to the etiology of depression, activation of proinflammatory signaling pathways occurs as a result of elevated OS. 140 Evidence suggests that MDD is associated with the immune response, as shown by increased levels of IL-1β, TNF-α, and IL-6. 141 LPS-induced astrocyte activation also contributes to the symptoms of MDD. Systemic treatment with LPS induces depressive-like behaviors and increases the production of inducible nitric oxide synthase (iNOS), IL-1β, TNF-α, and GFAP in the hippocampus and cortex. Inhibition of activated astrocytes reduces neuroinflammation. These alterations are followed by amelioration of LPS-induced depressive-like behaviors. 142
Neurotrophic factors
In the vast majority of patients with severe depression, antidepressants affect the levels of neurotrophic factors. For example, the primary regultaory factor of neuronal survival, growth, and differentiation during development is BDNF. For the treatment of depression, targeting signaling transduction by BDNF and its receptor, tropomycin receptor kinase B (TrkB), is essential. 143 , 144 Recent research has shown a link between decreased hippocampal neurogenesis and low levels of BDNF and glial-derived neurotrophic factor (GDNF) in the brains of depressed individuals. 145 Under normal conditions, astrocytes release various nutrients and cytokines. After cell reactivation, the secretion of these factors is further increased. 146 According to previous studies, fluoxetine stimulates c-Fos expression and ERK 1/2 phosphorylation, which in turn promotes BDNF production in astrocytes sorting from GFAP-GFP transgenic mice. 147 Imipramine acts as an antidepressant by increasing the mRNA expression of BDNF in astrocytes. Fluoxetine also induces BDNF expression by activating cAMP-response element binding protein(CREB) through the PKA and/or ERK pathways. 148
BDNF is an essential molecule for neural plasticity and development and is related to several CNS diseases. Currently, it is known that BDNF can regulate the activity of neurons and that it is produced not only by neurons but also by astrocytes. 149 SSRIs and tricyclic antidepressants increase BDNF expression in cultured primary astrocytes, and BDNF overexpression in mouse hippocampal astrocytes is sufficient to promote neurogenesis and causes anxiolytic behavior. 149 By promoting neurotransmitter release, facilitating vesicle docking, and upregulating the expression of synaptic vesicle proteins, BDNF, which is released by astrocytes in response to long-term antidepressant therapy, may assist in increasing synaptic plasticity at presynaptic terminals. 150 In addition, astrocyte-secreted BDNF can stimulate adult hippocampal neurogenesis and may contribute to synaptic and structural plasticity that underlies the long-lasting behavioral effects of antidepressants. 150 Astrocytes can secrete numerous nerve growth factors. Vascular endothelial growth factor (VEGF) is a member of the vasoactive growth factor family. It exerts its unique molecular effects by binding and activating endothelial cell tyrosine kinase receptors. VEGF is traditionally associated with angiogenesis and its stimulation. Recent evidence indicates, however, that it also influences nerve cells and plays a crucial role in hippocampal neurogenesis and neuroprotection. 151
Inflammasomes
Neuroinflammation is a central pathophysiological mechanism and defining characteristic of MDD. Numerous elements in the periphery and CNS interact to generate neuroinflammation, thereby stimulating astrocytes. The nucleotide-binding domain and leucine-rich repeat protein-3 (NLRP3) inflammasome is one of the largest typical inflammasomes discovered thus far. It is composed of pro-Casp-1 protein, NLRP3, and apoptosis-associated speck-like protein (ASC). 152 The sensitization of the NLRP3 inflammasome and the suppression of BDNF synthesis result in MDD. 153 In our research, SD is found to reduce BDNF levels and induce depressive-like behaviors in the sorted astrocytes from GFAP-GFP transgenic mice by activating the NLRP3 inflammasome. 130 NLRP3 inflammasome activation causes astrocytes to produce more IL-1β and IL-18. 154 , 155
The release of proinflammatory cytokines is the primary consequence of the activation of caspase-1, a component of the NLRP3 inflammasome. In addition, it has been observed that stimulating NLRP3 inflammasome assembly can induce depression-like behaviors in rodents exposed to LPS or CUMS. 156 , 157 Research on the effect of astrocyte-specific NLRP3 knockout suggests that the astrocytic NLRP3 inflammasome exerts a significant effect on astrocytic pyroptosis via the Casp-1/GSDMD pathway in depression. 156 , 157 Therefore, efficient NLRP3 inflammasome inhibitors are novel therapeutic agents for MDD. As we previously reported, chronic SD can specifically activate the NLRP3 inflammasome and decrease the level of BDNF in astrocytes to ameliorate depressive-like behaviors. Fluoxetine can suppress the effects of SD on astrocytes by stimulating astrocytic 5-HT 2B receptors directly. 147 Additionally, in the middle cerebral artery occlusion (MCAO) stroke model of mice, Li + can significantly attenuate GSDMD-mediated glial pyroptosis by regulating the AKT/GSK3β/TCF4/β-catenin signaling pathway, in which, the activation of AKT induced by Li + can also increase the phosphorylation of FoxO3a and promote the transportation of FoxO3a from nucleus into cytoplasm, the reduced FoxO3a in nucleus dissolves its competition with TCF4 in order to confirm more β-catenin/TCF4 complex. The increased latter complex further up-regulates the expression and activation of STAT3 in nucleus, the latter further inhibits the activation of the NLRP3 inflammasome by increase UCP2 which can decrease the production of ROS from mitochondrion. 136 This neuroprotective mechanism of Li + after ischemia-reperfusion injuries contributes to the improved depressive-like behaviors, besides of motor and cognitive capacities. 136
In conclusion, there have been so many hypothesis to explain the pathogenesis of MDD associating with many booming researches (Fig. 3 ). However, it is still hard to adopt only one above hypothesis to completely reveal pathophysiology of MDD. The main problem may contribute to the limitations of the theoretical perspective and the limitations of detection methods. Some key scientific problems in the neurobiology of neurological and psychiatric disorders are still unclear, such as how to identify the pathological characteristic changes for mood disorders, how to metabolize the cerebral metabolic waste under the pathological condition,how to observe the instant interactions of neural cells and the real-time changes of intracellular organelles in the patients of MDD? In the pathological conditions, conducting research from the perspective of comprehensive collaboration of the whole body and increasing the proportion of new technological applications in research will open up the new paths to reveal the pathogenesis of MDD in the future.

The molecular signaling schematic of cytokine hypothesis in the pathogenesis of MDD. The rodent performed the depressive like behaviors are impaired by some widely accepted risk factors, such as long-term sleep deprivation (SD), oxidative stress, lipopolysaccharide (LPS), ischemic damage and so on. Long-term SD can increase the extracellular ATP level, the latter inhibits the activation of AKT and the followed phosphorylation of FoxO3a by stimulating P2X7 receptors (P2X7R), the dephosphorylated FoxO3a translocates into the astrocytic nucleus, then the increased FoxO3a decreases the expression of 5-HT 2B R expression, which results the reduced phosphorylation of STAT3 which increases the activation of cPLA2 and the followed release of arachidonic acid (AA) and prostaglandin E2 (PGE2), finally causing the depressive-like behaviors. 41 Thus, antidepressant fluoxetine activates ERK 1/2 /cFos pathway by stimulating 5-HT 2B R and AC/cAMP/PKA pathway by activating GPCRs in order to increase the activation of CREB and the level of BDNF and TrkB, which can alleviate the depressive like behaviors induced by long-term SD. 147 , 148 As well as, imipramine, other SSIRs, and TCAs can also play antidepressive roles by increasing BDNF mRNA expression in astrocytes. 148 Ischemic stroke can trigger the increase of reactive oxygen species (ROS) which can induce the activation of NLRP3 inflammasome and the release of IL-1β/18, resulting in the neuroinflammation, however, Li + salt inhibits the activation of GSK3β and increases the phosphorylation of FoxO3a by activating AKT, which promotes the more FoxO3a transportation from nucleus into cytoplasm, and the reduced FoxO3a in nucleus lacks the competition with TCF4, the increased complex level of β-catenin and TCF4 further stimulates the expression and the phosphorylation of STAT3, which further induce the mRNA and protein expression of UCP2, then in mitochondrion, the increased UCP2 suppresses the production of ROS and results in the deactivation of NLRP3 inflammasomeincreases. 136 Superoxidation of Fe 2+ stimulates an increase in ROS, resulting in the production of inflammatory cytokines (including IFN-γ, TNF-α, IL-1β, IL-6) and inducible nitric oxide synthase (iNOS). 138 While, the treatments of oxidative stress (OS) can produce a large number of ROS, such as OH• and H 2 O 2 , resulting in neuronal impairments, while astrocytes can play their neuroprotective role by antioxidation. 135 Additionally, LPS can also increase TNF-α, IL-1β, and IL-6 by TLR-4/NFkB/AP-1 pathway and cause depressive-like behavior. 142 Adobe Illustrator was used to generate this figure
Interactions of multi-cells and multi-organs
Recently, increasing evidence has shown that pathological changes in a single cell type or brain region limited are insufficient explain the pathogenesis of MDD. This section mainly introduces the latest research on the pathogenesis of MDD, discussing the multiple interactions among neural cells and the multiple regulatory mechanisms between the brain and peripheral organs in detail.
The interaction between neuron and glial cell
Over the past few decades, studies on MDD have identified decreased PFC activity and excitatory/inhibitory (E/I) imbalance as probable mechanisms underlying depression. 158 Astrocytes are recognized to be essential for controlling neural network activity and to take part in higher brain activities. 159 To explore efficient treatments for MDD, it is important to focus on how to regulate the E/I balance and neuronal remodeling. 160
MDD-related marker proteins in neural cells
Astrocytes in the CNS form the neurovascular unit with neurons and blood vessels. The neurovascular unit mediates the exchange of nutrients and other functional substances between its components. 161 The blood-brain barrier (BBB) consists of endothelial cells tight junctions, a continuous basement membrane and astrocytic end-feet. Two proteins expressed on astrocytes, connexin 30 (Cx30) and Cx43, have been linked to the pathogenesis of depression. 162 Gap junctions that enable communication between astrocytes are formed by the membrane proteins Cx30 and Cx43. 163 Chronic unpredictable stress (CUS) and acute stress both specifically reduce the expression of the gap junction-forming proteins Cx30 and Cx43, 164 and the integrity of the BBB is weakened in mice lacking Cx30 and Cx43. 165
In addition to being an essential component of the developing astrocyte cytoskeleton, GFAP serves as the main intermediate filament protein in adult astrocytes. Although increased expression of GFAP is commonly observed in reactive astrogliosis, postmortem results suggest that the frequency and intensity of reactive astrogliosis are decreased in the brains of patients with MDD. 166 Accompanied by a decreased astrocyte density, the levels of GFAP and the GFAP intermediate filament domain are also reduced in brain samples from patients with MDD. 167 Researchers have even proposed that the GFAP content in serum can be used to determine the severity of MDD, 168 but this point is controversial.
AQP4, a kind of water channel, is mainly expressed on astrocytic end-feet in contact with blood vessels. The water channel AQP4 regulates the equilibrium of ions and water in the brain and is an essential part of the neurovascular unit. The vascular coverage of AQP4-immunopositive astrocytes in the orbitofrontal cortex (OFC) is lower in people with clinically significant depression than in psychiatrically healthy control patients. 169 In another postmortem study, it was found that the coverage of blood vessels by AQP4-positive astrocyte terminals was reduced in the OFC of MDD patients. 170 In addition, the K + -buffering capacity and presumably synaptic transmission are impaired in mice lacking AQP4, and impairment of these processes is associated with depressive-like behaviors. 171 In our previous study, we reported that the expression of AQP4 was decreased by exposure to CUMS, which contributed to dysfunction of glymphatic circulation and depressive-like behaviors in mice. 172 Additionally, the coverage of blood vessels by AQP4-positive astrocytic endfeet is decreased by 50% in MDD patients, indicating that decreased levels or mislocalization of AQP4 may contribute to the pathogenesis of MDD. 169 , 173
S100B is produced and secreted by astrocytes in the gray matter, 174 and changes in the levels of S100B in the blood and cerebrospinal fluid (CSF) of patients with MDD can cause glial cell dysfunction and damage. 175 , 176 In individuals with MDD, the number of S100B-immunopositive astrocytes in the pyramidal layer of the bilateral hippocampal CA1 region is decreased. 177 S100B secreted by damaged astrocytes can enter the extracellular space and CSF, 178 and the level of S100B is increased in the dorsolateral prefrontal cortex (dlPFC) of patients with MDD. 179 S100B levels are elevated in the CSF or serum of patients with MDD, 180 which suggests that S100B is a potential diagnostic biomarker for depressive episodes associated with MDD.
Communication between neurons and microglia plays an important role in the pathogenesis of depression. C-X3-C Motif Chemokine Ligand 1 (CX3CL1)- C-X3-C Motif Chemokine Ligand 1 receptor (CX3CR1) and OX-2 membrane glycoprotein (CD200)-OX-2 membrane glycoprotein receptor (CD200R) form ligand-receptor pairs, and these molecules are the most important chemokines and clusters of differentiation in maintaining CNS homeostasis. 181 CX3CL1 and CD200 are mainly expressed in neurons, and their receptors CX3CR1 and CD200R are expressed on microglia. 182 Activated microglia and decreased expression of CX3CL1 in the hippocampus were observed in an LPS-induced depression model. 183 CX3CR1-deficient mice show a temporary decrease in the number of microglia and a resulting deficiency of synaptic pruning, which may be related to neurodevelopmental and neuropsychiatric disorders. 184 However, CX3CR1-deficient mice show significant resistance to stress-induced depressive-like behaviors. 185 The level of CX3CL1 in the serum is increased in patients with moderate-severe depression compared with healthy subjects; thus, CX3CL1 could be used as a target for depression treatment. 186 Patients diagnosed with MDD with comorbid cocaine addiction show higher serum levels of CX3CL1. 187 Additionally, in a rat early-life social isolation (ESI) model, the expression of CD200 receptors in microglia is significantly reduced. 188 Exposure to unavoidable tail shock causes a decrease in CD200R expression in the hippocampus and amygdala, 189 and stress was also discovered to suppress CD200R expression in the hippocampus of rats. 190
Synaptic plasticity
Long-term potentiation (LTP) serves as the physiological basis for learning and conditioned responses. 191 Ketamine has a quick antidepressant effect, as it is a noncompetitive channel blocker of N-methyl-D-aspartate receptors (NMDARs). 192 Excessive glutamate in the synaptic cleft activates synaptic metabotropic glutamate receptors (mGluRs), which lead to neural excitotoxicity. 193 In a mouse model of chronic social defeat stress (CSDS), which causes depression, mGluR5 was shown to induce long-term depression (LTD). The major process responsible for synaptic plasticity is the mGluR-mediated LTD, which likely plays a significant role in the pathophysiological changes underlying depressive-like behaviors in the CSDS-induced depression paradigm. 194
ATP can mediate the activity of the astrocyte-neuron network, and ATP is a signaling molecule that also controls synaptic plasticity. 195 ATP can increase the expression of amino-3-hydroxy-5-methyl-4-isoxazole propionic acid receptors (AMPARs) by stimulating P2X 7 R and increasing the amplitude of miniature excitatory postsynaptic currents. 196 Stress exposure is a major pathogenic factor in disease models and can increase Ca 2+ -dependent release of ATP from neurons, which causes excitotoxicity. 197 , 198
Regulated in development and DNA damage response-1 (REDD1) is a stress response gene that can regulate development and the response to DNA damage. Virus-mediated overexpression of REDD1 in the rat PFC is sufficient to cause anxiety- and depressive-like behaviors and neuronal atrophy. 199 According to postmortem studies, the volume of the dlPFC is smaller and the density of neurons in the dlPFC is lower in MDD. 200 BDNF can modulate synaptic plasticity in the brain. TrkB is a functional receptor of BDNF. 201 BDNF produces antidepressant-like effects by increasing synaptic plasticity in a mouse model of CUMS. 202
Neuron-glia integrity
The term “tripartite synapse” was initially used to describe the intimate relationship between astrocytes and neurons at glutamatergic synapses, similar to the glutamate-glutamine cycle described above. 203 Moreover, glutamic acid decarboxylase, an enzyme that transforms glutamate into γ-aminobutyric acid (GABA), also exists in inhibitory GABAergic neurons. Increased inhibitory neurotransmission, glutamatergic/GABAergic E/I imbalance, and chronic stress-related emotional dysfunction reduce PFC activity. 204 , 205 In local circuits, various glutamatergic and GABAergic neurons interact in complicated ways to achieve E/I balance. 206 A meta-regression analysis indicated that glutamine and glutamate levels are decreased in the PFC, which is correlated with the therapies to MDD. 207 Global topological E/I imbalance in MDD is discovered through gene and protein expression of molecules related to inhibitory GABAergic and excitatory glutamatergic signaling in the postmortem MDD brains. 22 , 208 , 209 It shows the imbalance in cortical-subcortical limbic regions with decreased GABAergic signaling and increased glutamatergic signaling. 210 , 211 Meanwhile, GABAergic signaling is decreased in regions comprising the default mode network (DMN), while it is increased in the lateral prefrontal cortex (LPFC). 212 , 213 Stimulating P2X 7 R in neocortical nerve terminals can block the reuptake of GABA and glutamate by the presynaptic membrane and promote the release of these two neurotransmitters in the cerebral cortex of rats and humans, 214 , 215 and activation of P2X 7 R reduces the expression of GLAST. 216 This results in neuronal damage, a reduced number of synapses, decreased neurogenesis, and even impairment of key cerebral circuits that regulate mood.
Astrocytes are fundamental elements in synapses, participate in synaptogenesis and maturation, and maintain synaptic homeostasis. Ionic homeostasis in the extracellular space is critical for central nervous system function. 217 Astrocytes play an important role in maintaining extracellular K + homeostasis in the CNS, as well as H + , Cl - , and Ca 2+ homeostassis. 218 In addition, it also plays an important role in maintaining transmitter homeostasis, in which glutamate and GABA play particularly important roles. 219
In addition to the tripartite synapse, the more recent concepts of the four-part extracellular matrix and the microglial five-part synapse 220 also support the idea that glial dysfunction plays key roles in the early pathological features common to psychiatric disorders. 221 , 222 Under physiological conditions, microglia can play a neuroprotective role by producing cytokines. However, under pathological conditions, microglia can also affect the balance between excitatory and inhibitory synapses by phagocytosing synapses 223 and activating inflammatory factors in microglia. 224 In addition, the extracellular matrix (ECM) plays a significant role in maintaining normal communication in mature neural networks, which can limit the synaptic restriction of glutamate. 225 The components of the ECM are mainly produced by neurons and astrocytes, and microglia can also regulate the remodeling of the ECM. 226
Interaction mechanism in multi-organs
Abnormalities in cytokine levels in the brain and peripheral organs, disruption of the brain/immune system balance, and dysfunction of communication between the peripheral organs and the brain can cause neuroinflammation and depressive symptoms. For instance, cirrhosis and depression have been linked to intestinal dysbiosis, which results in intestinal barrier disruption, increasing bacterial translocation. Increased bacterial translocation then activates circulating immune cells, which produce cytokines and induce systemic inflammation. 227 In comparison with the healthy population, MDD patients have a much higher incidence and prevalence of chronic liver disease. 228 Inflammatory bowel disease (IBD) and irritable bowel syndrome (IBS) with increased intestinal permeability, which may have both inflammatory and autoimmune sources, are common comorbidities of MDD and anxiety. 229 , 230
Neuroendocrine-immune axis
Microglia secrete chemokines that disrupt the integrity of the BBB and increase the ability of immune cells to enter the brain parenchyma. 231 The stress response is a complex array of behavioral, neuroendocrine, autonomic, and immunological responses that enable adaptation to unpleasant psychological and physiological stimuli. 232 The HPA axis is a crucial endocrine system that orchestrates this response. 233 Stress can activate microglia, which are considered important immunocytes of the CNS. Mediators released by activated microglia can stimulate the HPA axis and induce GC production. 39 Similarly, high levels of GCs can also activate microglia, creating a vicious cycle. 234
Tryptophan (TRP) can be converted into a variety of biologically active molecules, and more than 95% of TRP is metabolized to kynurenine (KYN) and its breakdown products, with only a small portion of TRP being converted to 5-HT. 235 Indoleamine 2,3 dioxygenase (IDO) is an immune inducible enzyme that metabolizes TRP through the KYN pathway and plays an important role in the immune response. 236 In the brain, KYN is metabolized to the neurotoxic substance quinolinic acid (QUIN). 237
The primary GC in the HPA axis, corticosterone, plays a role in regulating the stress response in rodents. Stress, high GC levels, and serious depression are all linked. Analysis of transcriptomic changes associated with corticosterone-induced cytotoxicity revealed an association of neurite outgrowth-related genes with depression. Therapies for MDD may target the expression of genes involved in neurite formation, such as calpain 2 (Capn2), vesicle-associated membrane protein (Vamp7), and c-type natriuretic peptide (Cnp). 238
Consumption of a high-fat diet (HFD; for approximately 16 weeks) results in anxiety and anhedonic behaviors, and 4 months of HFD consumption results in increased levels of corticosterone and blood glucose, which also activate the innate immune system, increasing the release of inflammatory cytokines (i.e., IL-6, IL-1β, TNF-α). The behavioral abnormalities that arise from long-term consumption of a HFD are quickly reversed by ketamine. Additionally, giving HFD-fed rats a P2X 7 R antagonist greatly alleviates their anxiety. 239
Microbiota-gut–brain axis
In recent years, the microbiota-gut-brain axis has been reported to be disrupted in MDD. Stress stimulation can affect the gut microbiota, which in turn induces the production of inflammatory mediators (mainly IL-6 and IFN-γ) and a reduction in short-chain fatty acid levels. 240 The increased level of inflammatory cytokines may be caused by disturbance of the gut microbiota, which may also disrupt the gut barrier. 241 Alterations in the gut microbiota and inflammatory agents have an impact on the KYN pathway, metabolism, and toxin metabolism in the periphery. 242 Proinflammatory cytokines or toxic byproducts resulting from microbiota alterations may pass through the BBB and enter the brain. 243 This increases the levels of cytokines such as IL-1β and IL-6 and NLRP3 inflammasome activation in brain-resident cells. 244 In particular, microglia and astrocytes are activated and undergo atrophy, respectively. These glial cell changes, which affect the brain networks involved in learning and memory, mood regulation, and emotional regulation, may cause depressive symptoms or anxiety episodes. 245
According to clinical research, TRP and tryptophan catabolites (TRYCATs) may play a crucial role in psychiatric illnesses, including MDD. Peripheral and central inflammation can both stimulate the KYN pathway and trigger TRP metabolism and subsequent synthesis of various TRYCATs, including the toxic NMDAR activator QUIN, 246 which influences glutamate transmission, has a variety of immunomodulatory effects and has both neurotoxic and neuroprotective effects on the CNS. 141 Studies have proven that peripherally injected LPS increases the central and peripheral metabolism of TRP via the KYN pathway by exerting neurotoxic effects, inducing reactivation of microglia and astrocytes in the CNS. 247 Excessive production of QUIN, an NMDAR agonist, stimulates the release of glutamate and inhibits reuptake, leading to neuronal excitotoxicity. 248
Liver-brain axis
Patients with liver diseases often struggle with depression. According to one study on the frequency of liver disease and major depression in the United States, liver disease is linked to both major depression and suicidal thoughts. 249 A further population-based cohort study discovered that patients with MDD had much higher prevalence and incidence rates of chronic liver disease than the general population. 228 The incidence of depression is high in cirrhosis patients; moreover, depression is an independent predictor of mortality from cirrhosis. 250
An internal metabolic mechanism regulated by the liver can control depressive-like behavior. A crucial enzyme in epoxyeicosatrienoic acid (EET) signaling in the liver is epoxide hydrolase (sEH). Chronic stress selectively exacerbates sEH-induced depression-related changes in the liver while dramatically lowering the plasma levels of 14,15-EET. Deletion of hepatic epoxide hydrolase 2 (Ephx2) (which encodes sEH) rescues the chronic mild stress (CMS)-induced decrease in 14,15-EET plasma levels. 251 In a rat model of CUMS, electroacupuncture (EA) was found to downregulate P2X 7 R, NLRP3, and IL-1β expression in the prefrontal cortex and liver and relieved depression-like behavior. 252
In summary, as shown in Fig. 4 , although the etiology of MDD is still unclear, it is widely accepted that the common pathogenic factors of MDD are genetic, stress, and comorbidity. 3 The levels of monoamine neurotransmitters (5-HT, NE, and DA) are insufficient in the synaptic cleft of MDD patients, correspondingly, the explored antidepressants such as tricyclic antidepressants(TCAs), SSRIs and SNRIs almostly act on the channels responsible for inhibiting reuptake of these neurotransmitters. 51 Thus, according to these traditional pharmacological theories, these antidepressants always have the delayed clinical efficacy, this promises the potential new pharmacological mechanism still requires further study. As the well-known glutamate-glutamine cycle, astrocytes play key roles in resolving neuronal glutamate toxicity. However, under the MDD pathological condition, due to the decreased expression of EAATs in astrocytes, excessive glutamate in the synaptic cleft activates synaptic mGluRs, which leads to neuronal excitotoxicity. 194 In addition, the overdose glutamate can also be decarboxylated by glutamate decarboxylase (GAD) to GABA and activates the GABA receptors on the postsynaptic membranes. 206 In our previous studies, the expression of 5-HT 2B is selectively decreased in the sorting astrocytes from MDD model mice. 64 The antidepressants SSRIs and leptin can increase the expression of the astrocytic 5-HT 2B receptor. 147 Furthermore, OS plays a crucial role in the emergence of depression, including by elevating the levels of ROS and NO in the mitochondrion of astrocytes. 253 Proinflammatory signaling pathways are activated as a result of elevated OS, the mitochondrial dysfunction results in an increased generation of ROS and NO. 137 As well as, the pathogenesis of MDD are associated with the inflammatory-immune response, as shown by elevated levels of proinflammatory cytokines, mainly IL-1β, TNF-α, and IL-6. 141 The expression of neural cell marker proteins in neural cells, including Cx30/43, 162 GFAP, 167 AQP4, 172 and S100B, 177 are all decreased under MDD pathological conditions. In brain, KYN is metabolized by microglia to the neurotoxic metabolite QUIN and by astrocytes to the beneficial metabolite kynurenic acid (KynA), thus, QUIN is increased and KynA is decreased in MDD patients’ brain. 141 , 254 , 255 Recently, growing evidence support that the occurrence of MDD are the results of the correlational disorders from multiple systems or organs, not only limiting in brain. 227 , 228 The comorbidities of MDD have attracted widespread attention, the intestinal gut microbial dysbiosis, liver dysfunction, immune system disorders all play important roles in the pathogenesis of MDD. Stressful conditions can affect the gut microbiota, which in turn induces the production of inflammatory mediators (mainly IL-6 and IFN-γ). 256 Proinflammatory cytokines or toxic QUIN resulting from alterations in the microbiota may pass through the BBB and activate NMDARs. 243 Under the dysfunction of liver, the level of ammonia is increased in the brain. 257 The pathogenic factors of various organs at the body level and the pathological changes of glial cells at the cellular level should attract more attention to explain the pathogenesis of MDD.

The pathogenesis of MDD is closely related to synapses, astrocytes, microglia, and their interactions as well as interactions among organ. Genetic factors, stress and comorbidities are considered the most common pathogenic factors of MDD 3 . The traditional monoamine theory contends that MDD may cause by the deficits in monoamine neurotransmitters. 49 Moreover, the other abnormal increase of neurotransmitters in the synaptic cleft, such as glutamate, GABA and ATP, has the high relationship with the pathogenesis of MDD. 41 , 496 The interaction between neurons and glial cells can induce the oxidative stress, pro-inflammatory cytokines released, the reduction of neurotrophic factors. The microbiota-gut-brain axis is clearly disrupted in MDD. 243 , 248 When liver dysfunction occurs and causes OS and neuroinflammation in the brain, which also contribute to the pathophysiology of MDD. 497 Adobe Illustrator was used to generate this figure
New diagnostic approaches
MDD is a prevalent psychiatric disorder worldwide and is expected to become one of top disease in terms of burden by 2030. 258 However, the current clinical diagnostic criteria for MDD are subjective, and diagnoses are mainly based on clinical symptoms, leading to high rates of missed and incorrect diagnoses. This section summarizes the newest research on diagnostic approaches for MDD, including serum indicators, neuroimaging indicators and multimodality scales. Research on new diagnostic approaches for MDD has the potential to improve our understanding of MDD pathogenesis and the accuracy of clinical diagnosis.
Potential serum indicators
The pathological mechanism of MDD can be studied in two ways: by exploring the pathophysiology of the disease and by identifying MDD-related neurobiological indicators4. Hence, identifying potential biomarkers for MDD could allow accurate diagnosis, faster treatment and effective monitoring of the disease. Recently, an increasing number of studies have confirmed the involvement of OS and neuroinflammation in MDD pathology. 259 , 260 Two novel biomarkers, serum nicotinamide adenine dinucleotide phosphate oxidase 1 (NOX1) and Raftlin, are reported to have good diagnostic value in MDD patients. The effectiveness of elevated NOX1 and Raftlin levels in diagnosing MDD has been evaluated in clinical trials; the related mechanism is that NOX1 can regulate the ROS-antioxidant balance in patients with MDD through OS and the inflammatory repsonse. 261 The serum level of the chemokine-like protein TAFA-5 (FAM19A5) has also been reported to be increased in patients with MDD, and increased serum FAM19A5 levels are associated with reactive astrogliosis, neuroinflammation, and neurodegeneration. 262 In addition, the level of serum FAM19A5 was shown to have a negative correlation with cortical thickness in specific brain regions. These findings suggest that serum FAM19A5 could be a potential biomarker for neurodegenerative changes in MDD.
Functional magnetic resonance imaging indicators
In addition to serum indicators, neuroimaging metrics are potential objective tools for improving the accuracy of MDD diagnosis and must be studied in death. In recent years, many researchers have tried to diagnose MDD using MRI by identifying disease-specific functional and/or structural abnormalities in patients with MDD compared with healthy subjects. 263 Structural MRI techniques, such as voxel-based morphometry (VBM), can be used to detect volume changes in gray matter. 264 It has been reported that abnormal gray matter volume (GMV) in several brain regions is positively correlated with MDD. 265 , 266 Regarding functional MRI, recent studies have revealed that cerebral functional abnormalities are not limited to specific brain regions in patients with MDD. These differences are also associated with hypoconnectivity within the frontoparietal network (FN), the DMN, and midline cortical regions. 267 , 268 Furthermore, resting-state functional magnetic resonance imaging (R-fMRI) is an emerging neuroimaging technique used to study functional connectivity in the brain and holds great potential in aiding clinical diagnosis. 269 It has the benefits of being noninvasive and easy to perform and offering high temporal and spatial resolution. 270 As a result, it has played a significant role in MDD research and is a superior technique for researching MDD pathogenesis and identifying neuroimaging markers for MDD. 271 Thus, indicators such as amplitude of low-frequency fluctuation (ALFF), fractional amplitude of low-frequency fluctuation (fALFF), regional homogeneity and functional connectivity (FC) have shown promise as neuroimaging markers for MDD. Recently, a study reported that increased average values of ALFF and fALFF in the right caudate and corpus callosum may serve as potential markers for diagnosing MDD. 272 Another study based on the largest R-fMRI database of MDD patients confirmed that the DMN plays a crucial role in MDD diagnosis, as DMN FC is reduced in patients with recurrent MDD. 273 These findings also suggest that the DMN should continue to be a prominent focus of MDD research.
New multi-modal evaluation scales
Given that structural and functional abnormalities are associated with MDD, 274 using multimodal approaches is more appropriate than relying on a single feature for the diagnosis of MDD. However, research results related to the effectiveness of neuroimaging techniques in diagnosing MDD remain inconsistent. 275 This may be attributed to variations in the types of structural and functional features examined; however, more importantly, very few studies have used multimodal approaches to diagnose MDD. 276 Recently, in a study utilizing multimodal MRI data, patients with MDD were successfully distinguished from healthy controls by radiomics analysis. 276 Radiomics is a rapidly developing field involving the extraction of quantitative information from diagnostic images, and it can be mainly divided into three steps: image acquisition, analysis and model building. 277 Additionally, omics and neuroimaging techniques can be combined to construct models for diagnosing MDD; specifically, 5-hydroxytryptamine receptor 1 A/1B methylation data can be integrated with resting-state functional connectivity (rsFC) data. It was shown that this combination could be used to more accurately distinguish patients with MDD from healthy subjects than R-fMRI data or DNA methylation data alone. 278
By now, the widely accepted objective diagnostic indicators or methods for MDD are still deficient. In addition to the unclear pathogenesis of MDD, insufficient sensitivity and accuracy of detection instruments are also the main reasons, especially the correlation between imaging characterization and disease-specific changes that need to be discussed.
Preventing the occurrence and recurrence of MDD
MDD is a disease with a high prevalence worldwide, 279 and preventing its occurrence and recurrence is crucial. Lifestyle medicine is an evolving medical specialty that aims to prevent chronic, noncommunicable diseases through lifestyle interventions. The goal of lifestyle medicine is to prevent the occurrence and recurrence of disease by improving sleep hygiene and diet, increasing physical exercise, avoiding sedentary behavior, increasing social support, and improving mood. In recent years, an increasing number of studies have demonstrated that the occurrence and recurrence of MDD can be prevented by means of lifestyle medicine; 280 we summarize these reports in this section.
Sleep improvements
Improving sleep is an important strategy to prevent the occurrence of depression. Insomnia is included in the diagnostic criteria for MDD. 281 However, few studies have examined whether treating insomnia can prevent the exacerbation of depressive symptoms. Treating insomnia can prevent the worsening of depressive symptoms, and cognitive behavioral therapy for insomnia (CBT-I) is a recommended intervention for treating insomnia to improve sleep and mood. 282 , 283 , 284 As a first-line treatment for insomnia, CBT-I includes cognitive therapy, stimulus management, sleep restriction, improved sleep hygiene, and relaxation. 282 , 285 CBT-I can also lead to sustained remission of insomnia-related disorders, and continuous treatment of insomnia with CBT-I can also reduce the occurrence and recurrence of MDD. 286 Circadian rhythm support (CRS) can strengthen the circadian rhythm by means of scheduled bright light exposure, physical activity, and body warming. 287 Although CRS has been reported to have only an indirect effect in alleviating sleep disturbance and depressive symptoms, 288 treatment with CRS may help maintain the beneficial effects of CBT-I. 288 , 289 In one study, 44% of untreated patients but 38%, 28% and 9% of patients treated with CRS, CBT-I, and CBT-I + CRS, respectively, experienced clinically significant worsening of depressive symptoms during a 1-year follow-up period. Between-group comparisons showed that the percentage of patients who experienced worsening of depressive symptoms was significantly different between the CBT-I + CRS group and the nontreated and CRS groups. 289 In a randomized controlled trial, exacerbation of depressive symptoms over one year was decreased in insomia patients with an increased risk of depression and insomnia patients treated by therapist-guided CBT-I combined with CRS; however, untreated insomnia patients with a high risk of depression experienced clinically significant worsening of depressive symptoms. 288 , 289
Disrupted sleep is a common symptom of depressive episodes and increases the risk of MDD, 290 but the correlation between the onset of sleep disturbance and MDD is still unclear. Additionally, patients with symptoms of sleep disturbance have a greater risk of MDD occurrence and recurrence. 290 , 291 One study suggests that disrupted sleep may affect monoamine function and the HPA axis, 292 even causing hyperarousal and inflammation. 293 Additional studies on the pathological mechanism of depression have suggested that the HPA axis is hyperactive in MDD patients and that sensitivity to negative feedback is decreased. 15 Additionally, one prospective cohort study reported that a history of sleep disorders can increase the risk of depression later in life and that subjective sleep problems are associated with clinically significant depressive symptoms. 294
Dietary adjustment
Dietary adjustment is an effective, safe, and widely applicable method for preventing MDD, especially by inhibiting MDD-related pathological inflammation. 295 Various nutrients can possess different anti-inflammatory properties; in contrast, there are many proinflammatory foods, such as those high in refined starch, sugar, and saturated fat and low in fiber and omega-3 fatty acids, 296 which can promote the occurrence of inflammation to increase the risk of MDD. 297 One study reported that the chance of being diagnosed with depression is higher among individuals who consume a proinflammtory diet than among those who consume an anti-inflammatory diet. 295 Stimulation of the innate immune system by proinflammatory foods can result in mild inflammation and chronic illness, which may contribute to an increased risk of MDD. 298 Furthermore, an increasing number of studies suggest that at the molecular and cellular levels, dietary factors have effects on neuronal function and synaptic plasticity, which may be implicated in the etiology of MDD. 299 , 300 Therefore, adherence to a healthier diet can reduce the incidence of MDD, which is of great significance for the clinical treatment and prevention of depression. 295
In addition, an increasing number of studies have identified the importance of the interaction among the microbiota, gut permeability, and immune-inflammatory processes in the pathophysiology of MDD. 301 Because the interaction of bacteria of some taxa in the gut with peripheral inflammation with the brain may be related to depression pathophysiology, 302 , 303 regulating the gut-microbe-brain axis may be a therapeutic and preventive strategy for psychiatric disorders. 304 Restoration of the gut eubiosis can prevent the occurrence of MDD, and probiotics can normalize the gut ecosystem. Additionally, by altering the microbiota and regulating gut permeability, a gluten-free diet can alter the activity of the gut-microbe-brain axis, which has been discovered to be related to the pathogenesis of MDD. 305 , 306 , 307 Other studies report that consuming a gluten-free diet and probiotic supplements together may inhibit the immune-inflammatory cascade in MDD patients, and decreased inflammation can improve the integrity of the gut barrier and alleviate depressive symptoms. 307 Similarly, dietary fiber can also improve immune function by regulating the gut microbiota to prevent the occurrence of MDD, 308 which is attributed to the inhibition of OS and inflammation.
Increasing evidence suggests that physical exercise can prevent some mental disorders in addition to cardiovascular disease. 280 , 309 This finding suggests that physical exercise may be able to prevent MDD. As reported in some studies, physical exercise can effectively prevent depression by affecting many molecular and cellular pathways; for instance, physical exercise can stimulate VEGF expression, 310 , 311 leading to cellular level changes, such as stimulation of angiogenesis, increased delivery of neurotrophic factors and oxygen by the vascular system, 312 an increase in the neurogenesis rate and induction of synaptogenesis. 312 , 313 Ultimately, VEGF improves function in the hippocampus, which is one of the brain regions related to depression and stress regulation. 314 , 315 , 316 Exercise also reduces the levels of proinflammatory factors (e.g., IL-6) and increases the levels of anti-inflammatory factors (e.g., IL-10), which is beneficial for preventing the occurrence of MDD. 317 , 318 , 319 Furthermore, physical exercise for approximately 45 minutes per day can significantly reduce the risk of MDD. 320 , 321 High-intensity activity, such as aerobic exercise, dancing, and the usage of exercise machines, and low-intensity exercises, including yoga and stretching, can all reduce the occurrence of MDD. 322 Specifically, the combination of aerobic exercise and stretching as a multimodal therapeutic strategies has a significant antidepressant effect in depressed inpatients. 323
Patients with MDD have significantly more sedentary than ordinary people, and they engage in less physical activity than what is recommended, i.e., an average of 150 min of moderate- to high-intensity physical activity weekly. 324 This finding suggests that decreasing sedentary behavior or increasing physical activity levels should be a priority to prevent the occurrence of disease. In psychiatric centers, aerobic exercise has received increasing attention as a valuable method of prevention. 324 Studies report that reduced depressive symptoms in MDD patients can be observed after increasing aerobic exercise and stretching exercise, with more significant alleviation of depressive symptoms after 8 weeks of aerobic exercise. 325 Reward positivity (RewP) and error-related negativity (ERN) were identified as potential biomarkers of the exercise treatment response in depression. 325 In individuals with MDD, aerobic exercise was found to be beneficial in ameliorating depressive symptoms, particularly in those with more severe depressive symptoms and a higher baseline RewP. 325 , 326 RewP may be useful for identifying those who will benefit from exercise as a treatment for depression. 325
Social intervention
Social support refers to the help provided by social relations and transactions. 327 Social support may be obtained from a variety of individuals, including family members, friends, coworkers, and community members. 328 Furthermore, a variety of factors, including the quantity and quality of support as well as subjectively perceived social support by individuals, impact the level of social support. 329 It has been reported that MDD patients often lack social support, and receiving adequate social support can confer greater resistance to stress and prevent the occurrence and recurrence of MDD. 330 , 331 Low-functioning social support or self-perceived poor social support causes worse symptoms and treatment outcomes in depressed patients. 332 , 333 , 334 A previous study also reported that patients who lack adequate social support are more likely to experience MDD. 335 Social support may have an influence on depression through neuroendocrine pathways, 336 , 337 and social support can improve a person’s psychological wellbeing and make the individual more resistant to stress. 337
Studies on structural social support, social network size, and mental health disorders have shown that less social contact and loneliness can cause more severe depressive symptoms. 338 For individuals with MDD, it is necessary not only to increase the frequency of social contact but also to improve self-awareness and foster close functional supporttive relationships. 335 , 339 Studies have reported that when controlling for all other variables, each aspect of social support is clearly associated with MDD, and to some extent, the occurrence of panic disorder in patients with MDD is more strongly associated with poor functional support. This finding suggests that functional support may be an important protective factor against MDD. 331 , 335 Social support itself, especially emotional support, 340 may alleviate and prevent depressive symptoms, and support from family members or friends can replace formal health care. 341
In general, the pathological development of MDD is a gradual transition from subclinical state to clinical pathological changes. It is crucial to identify the core targets that lead to pathological changes from quantitative to qualitative changes during this process, and the above preventive interventions, sleep improvement, physical exercise, dietary regulation, and social intervention, may prolong or reverse the subclinical pathological stage (Fig. 5 ).

Schematic of prevention strategies for the occurrence and reoccurrence of MDD. An outline of various prevention strategies for MDD includes sleep improvement, dietary adjustment, exercise, and social intervention. Sleep disturbances have the high relationship with the occurrence of MDD, the anhedonia, anxiety and insomnia are the main symptoms of patients with MDD. The behavioral and educational strategies, cognitive reconstructing therapy and circadian rhythm support can be applied to improve sleep quality. 281 , 289 Dietary adjustments are also suggested to have the potential effects to prevent the occurrence or re-occurrence of MDD, the improvement mechanism of diet may involve in the regulated immune-inflammatory responses, the improved gut-microbe-brain axis and synaptic plasticity. 295 , 299 , 304 In addition, xxercise is an effective way to improve neuroplasticity, to maintain neuroendocrine homeostasis, and to regulate neuroinflammation, in order to effectively prevent the occurrence or re-occurrence of MDD. 280 , 309 Importantly, getting social support from family members, friends, coworkers and community members can be helpful for the MDD patients’ recovery, these social interventions can let patients get emotional support and improve their self-awareness. 328 , 340 Adobe Illustrator was used to generate this figure
Therapeutic drugs and strategies
This section summarizes new advances in research on the pharmacological mechanisms of common antidepressants and novel therapeutic strategies. Moreover, as laboratory animal models of MDD and other mental diseases are lacking, hindering the development of strategies for evaluating pharmacological effects and studying pathological mechanisms, we also discuss recent research on animal models.
The molecular mechanism of antidepressants
Tricyclic antidepressants.
In the late 1950s, the first TCAs were approved and used for the treatment of depression. 342 TCAs have a common three-ring chemical structure, and the main TCAs are imipramine, amitriptyline, clomipramine, desipramine and doxepin. The pharmacological mechanism of TCAs mainly involves its interaction with neurotransmitters in the brain, resulting in changes in neurotransmitter levels and an antidepressant effect. First, TCAs can inhibit the reuptake of neurotransmitters, leading to antidepressant effects. For example, they can influence the levels of 5-HT, NE, and to a lesser degree, DA, causing an increase in neurotransmitter concentrations in the synaptic gap and increasing neurotransmitter signaling to exert pharmacological effects. 343 However, different TCAs inhibit 5-HT and NE reuptake to varying degrees. For instance, amitriptyline, imipramine, and desipramine strongly inhibit 5-HT reuptake, 344 clomipramine specifically inhibits NE reuptake, and nortriptyline can inhibit both NE and 5-HT reuptake while also exerting central anticholinergic effects. 345 , 346 , 347 Additionally, TCAs can antagonize 5-HT 2A and 5-HT 2C , thereby increasing the release of NE and DA in cortical areas. 348 , 349 , 350 TCAs can bind to histamine receptors, especially H1 receptors, as well. 351 By blocking H1 receptors, they can induce sedation and drowsiness, which may benefit depressed patients with sleep disorders. 352 Furthermore, TCAs can also block muscarinic acetylcholine receptors, exerting anticholinergic effects and resulting in side effects such as dry mouth and constipation. 353
In addition to the above-known pharmacological mechanisms, some recent studies have reported that amitriptyline can induce the activation of fibroblast growth factor receptor (FGFR), leading to the production of GDNF. 354 In addition, amitriptyline can increase the expression of Cx43 to promote gap junction intercellular communication (GJIC) between astrocytes, thereby relieving depressive symptoms. 355 This suggests that TCAs may also ameliorate severe depression through additional mechanisms involving astrocytes that are independent of the monoamine system to some extent. Further exploration is needed to fully understand the specific mechanism. Another study demonstrated that FKBP51, a crucial modulator of the glucocorticoid receptor (GR) pathway, can bind to clomipramine and impede its interaction with PIAS4. Inhibition of this interaction subsequently hinders sumoylation; this alteration represents a newly discovered mechanism by which the antidepressant drug exerts its effect. 356
Selective serotonin reuptake inhibitor
According to a study, most severe depression patients are still advised to consider SSRIs as the initial choice for treatment. 350 The main representative SSRIs drugs include fluoxetine, sertraline, paroxetine, and escitalopram. The mechanisms of action of SSRIs are commonly known as follows: first, SSRIs can selectively inhibit SERT, inhibiting the reuptake of 5-HT in the synaptic cleft and thereby exerting pharmacological effects. 357 Second, SSRIs can impact the 5-HT signaling pathway, activating 5-HT 1A. 358 , 359 In addition, studies have shown that antagonism of 5-HT 2A/2C receptors can enhance the effects of SSRIs such as fluoxetine. 360 , 361 Third, long-term use of SSRIs can increase 5-HT transmission in the LC, 362 thereby increasing the release of GABA to exert inhibitory effects on NA neurons. 363 Fourth, long-term use of SSRIs is associated with neuroplasticity and neurogenesis in certain brain regions. 364 SSRIs have been found to increase the expression of BDNF, a protein crucial for neuronal growth and survival, by acting on TrkB, 365 which may contribute to the long-term therapeutic effects of SSRIs. Thus, our previous reports and others researches all suggested that astrocytic 5-HT 2B receptors may be the potential pharmacological target of SSIRs. 59 , 60 , 366 , 367 , 368
According to previous studies by our group, in the absence of SERT, SSRIs such as fluoxetine can act as direct agonists of astrocytic 5-HT 2B receptors to exert antidepressant-like effects. 60 , 64 , 179 , 366 , 369 In astroglia isolated from mice exposed to CUMS, fluoxetine activates the 5-HT 2B receptor, promoting ERK 1/2 phosphorylation. This increases downstream c-Fos expression, which in turn boosts BDNF synthesis. 147 Furthermore, administration of fluoxetine effectively inhibits SD-induced stimulation of the NLRP3 inflammasome by the AKT/STAT3 and ERK/STAT3 pathways in vivo, and SD dramatically triggers depressive-like behaviors by stimulating astrocytic P2X 7 Rs. 41 , 155 As previously mentioned, leptin may increase the expression of the 5-HT 2B receptor in astrocytes via the LepR/JAK2/STAT3 pathway, and fluoxetine may be more effective in increasing BDNF levels and alleviating depressive-like behaviors due to the leptin-mediated increase in 5-HT 2B receptor expression. 130 Both in vivo and in vitro, fluoxetine’s inhibitory actions on A1 reactive astrocytes depend on astrocytic 5-HT 2B R. 55 Recently, fluoxetine was shown to act as a 5-HT 2B agonist, and this finding is also supported by research by other groups. Fluoxetine has been reported to suppress the activation of A1 reactive astrocytes and decrease unusual behaviors in CMS-exposed mice. In vitro, Gq protein and b-arrestin1 are not necessary for fluoxetine’s effects on A1 astrocyte activation, and downstream signaling through astrocytic 5-HT 2B R is responsible for fluoxetine’s inhibitory effects on A1 astrocyte activation in primary culture. 55
Serotonin/norepinephrine reuptake inhibitors
SNRIs are often recommended as the initial choice for the treatment of MDD. Representative SNRIs include milnacipran, DXT, DVS, and venlafaxine. The molecular mechanisms of SNRIs can be summarized as follows: First, SNRIs inhibit the norepinephrine transporter (NET), which prevents the reuptake of NE into presynaptic neurons, leading to an increased concentration of NE in the synaptic cleft. 370 Second, similar to SSRIs, SNRIs also inhibit SERT, resulting in an increased concentration of 5-HT in the synaptic cleft. 371 For example, paroxetine and venlafaxine can inhibit SERT and, to a lesser extent, NET. 372 Third, SNRIs inhibit the reuptake of both NE and 5-HT; thus, they have a dual mechanism of action. This dual inhibitory effect is believed to contribute to the broader therapeutic effects of SNRIs compared to SSRIs. 373 Chronic treatment with fluoxetine has been shown to increase the expression of Cx43 in the rat PFC, which further prevents the dysfunction of astrocytic gap junctions induced by CUS and reverses the depressive-like behaviors caused by gap junction blockade. 71
In a randomized controlled trial, MRI scan were taken after treatment with duloxetine and desvenlafaxine, and the results showed that the thalamo-cortico-periaqueductal network, which is associated with the experience of pain, may be an important target of action of antidepressant drugs. 374
New potential pharmacological targets
The abovementioned antidepressants have been utilized as clinical therapies for MDD, but it is difficult to elucidate the exact pharmacological mechanisms of every medicine due to delayed clinical efficacy, poor treatment response to some patients, and difficulty in effectively controlling the incidence of suicide. Recently, several pharmacological agents have been discovered as potential antidepressants.
Ketamine, a noncompetitive antagonist of the NMDAR, has been shown to induce rapid and significant antidepressant effects within a few hours. 375 Due to the rapid antidepressant effects of ketamine, unlike the delayed effects of traditional antidepressant drugs, 376 research on this drug has continued and has revealed its mechanisms of action and potential drug targets. Ketamine can increase the level of BDNF in the prefrontal cortex, especially in the hippocampus, to exert antidepressant-like effects. 377 Studies have suggested that ketamine can increase the synthesis of synaptic proteins through BDNF signaling dependent on the activate protein kinase B (Akt) and mammalian target of rapamycin complex 1 (mTORC1) signaling cascades. 378 , 379 Ketamine may induce the activation of mTOR by the upstream kinase Akt, regulate the phosphorylation of GSK-3β, and exert antidepressant effects. 380 Ketamine can block NMDARs in postsynaptic principal neurons in the PFC and hippocampus, increase synaptic function through homeostatic mechanisms, and reverse synaptic defects caused by chronic stress. 381 , 382 Furthermore, by inhibiting NMDARs, ketamine can reduce the excitation of specific cortical GABAergic interneurons, resulting in a temporary increase in glutamate release that stimulates postsynaptic AMPA glutamate receptors. This, in turn, leads to the release of BDNF, activation of the TrkB receptor, and subsequent activation of the Akt/mTORC1 signaling pathway. These molecular events ultimately contribute to an increase in the number and functionality of synapses, leading to amelioration of depressive symptoms. 383
Similar as ketamine, some other psychedelics can also produce fast and persistent antidepressant effects. 384 Psilocybin, a classical psychedelic, can play its antidepressant roles by activating 5-HT 2A receptors (5-HT 2A R). 385 Thus, to block the 5-HT 2A R can not produce the antidepressant effects of psilocybin, only induce the hallucinogenic-like behaviors in mice. 386 This proposes 5-HT 2A R may not be the real pharmacological target for its antidepressant effects. Another study reports that the combination of lysergic acid diethylamide (LSD) and psilocybin may exert long-term antidepressant effects by promoting neural plasticity, which dose not involve in the hallucinogenic effects. 384 Additionally, to target 5-HT 2A R, the combination of LSD and psilocybin can lead to biased activation of the mediated signaling pathway and produce antidepressant effects without the side effects of hallucinations. 387 Thus, the administration of psilocybin can rapidly and persistently induce neuronal dendritic remodeling in the medial frontal cortex of mice, and the psilocybin-induced newly formed dendritic spines can successfully transform functional synapses, suggesting that synaptic rewiring may also be one pharmacological mechanism of the rapid antidepressant effects of psilocybin. 388 To further dissociate the hallucinogens effects from the psychedelics can be beneficial to develop more specific antidepressants with better therapeutic capacities.
Additionally, some novel potential therapeutic targets for MDD have also been reported, such as TGF-β1 389 and growth-associated protein 43 (GAP-43). 390 Multiple studies have shown that antidepressants may cause changes in TGF-β1 expression. Fluoxetine, paroxetine, venlafaxine, and sertraline have been shown to have the potential to increase the levels of TGF-β1, which may contribute to their antidepressant effects. 391 , 392 Venlafaxine has also been reported to exert neuroprotection by increasing the production of FGF-2 and TGF-β1 in astrocytes following stroke. 72 Then, chronic administration of desipramine has been shown to upregulate the expression of GAP-43 in the hippocampus of rats, potentially influencing neuronal plasticity in the CNS. 390 GAP-43 has been suggested as a relevant target for the pharmacological effects of antidepressants. 393 , 394
The most of above antidepressants have been widely used for the MDD patients according to the respective potential pharmacological actions (Fig. 6 ). Thus, the exactly neuromolecular mechanisms require deep studied and the new potential therapeutic targets and strategies still need further exploration.

The molecular mechanisms of tricyclic antidepressants (TCAs), selective serotonin reuptake inhibitors (SSRIs), serotonin/norepinephrine reuptake inhibitors (SNRIs) and ketamine. TCAs can inhibit the protein kinase C (PKC) pathway by blocking the H1 receptors (H1Rs), 351 , 352 TCAs decreases the reuptake of dopamine (DA) by inhibiting dopamine transporters (DATs) in the presynaptic membrane, and increases the DA concentration in the synaptic gap, increase the effect of DA on dopamine receptors (DARs) of postsynaptic membrane. 343 The activated DARs increase Ca 2+ dependent CaMKII and CaMK4, as well as, the secretion of CREB. 498 , 499 In another way, the stimulated DARs by DA can also activate the cAMP-PKA pathway, which in turn activates the levels of CREB and BDNF by stimulating MAPK/ERK 1/2 pathway. 500 TCAs, SSRIs, and SNRIs can all inhibit the reuptake of 5-HT by SERTs, specially SSRIs have the selective inhibition on SERTs, which increase the concentration of 5-HT in the synaptic gap and play antidepressive roles by effecting on 5-HTRs in postsynaptic membrane, 343 , 344 which also activate the cAMP-PKA pathway. 49 , 501 Moreover, TCAs and SNRIs can also inhibit the reuptake of NE by NETs, which also increase the concentration of NE in the synaptic gap, and in turn activate the effect of NE on adrenoceptors (ADRs) and activate the cAMP-PKA pathway in postsynaptic membrane. 502 Besides of the AC/cAMP/PKA pathway, the effect of NE on ADRs can also activate protein kinase B (Akt) phosphorylation and mammalian target of rapamycin complex 1 (mTORC1) by stimulating TrkB, in order to promote the secretion of postsynaptic density 95 (PSD95) and glutamate receptor 1 (GluR1). 502 Ketamine works as the antagonist of NMDAR on GABAergic interneurons, it suppresses the excitation of subsets of GABAergic interneurons, which reduces the gamma aminobutyric acid (GABA) effects on gamma aminobutyric acid type B receptor (GABABR), and relieves the inhibition of GABAergic interneurons on the release of glutamate, the latter further stimulates AMPAR on postsynaptic membrane and increases the level of BDNF, even the release of BDNF stimulates the above TrkB/AKT/mTORC1 pathway. 503 , 504 Adobe Illustrator was used to generate this figure
Novel therapeutic strategies
New animal models.
Establishing animal models with pathological features representative of those seen in humans is key for advancing MDD research. Currently, the widely utilized animal models of MDD include CUMS, behavioral despair (BD), learned helplessness (LH), and CSDS, drug withdrawal, and transgenic animal models. 395 The CUMS model, one of the most commonly used animal models for MDD, 64 , 172 exhibits depressive-like behaviors. 396 , 397 According to a meta-analysis of 408 papers involving stress protocols, the most commonly used stressors for CUMS models are food and water deprivation, light cycle modification, wet bedding, cage tilting, social stress, and forced swimming. 398 Recently, we constructed an improved depression model named the chronic unpredictable mild restraint (CUMR) model by using environmental interference. 62 The stressors used to construct this CUMR mouse model included activity restriction, damp bedding, cage shaking, tail suspension, forced swimming, and 45° cage tilting. These stressors all restrict the activity of the mice; moreover, stressors that disturb physiological rhythms, chronic unpredictable rhythm disturbance (CURD), can cause manic-like behaviors in mice (Fig. 7 ). The disease-related pathological changes and serum indicators in the CUMR and CURD models are highly similar to those in patients in the clinic, and therapeutic medicines can effectively improve brain function and behavior in these models. 62

The protocol and stressors used for CURD and CUMR. In order to establish the CUMR model, a combination of various stressors includes interference of constraint ( a ), damp bedding ( b ), cage shaking ( c ), tail suspension ( d ), forced swimming ( e ), and cage tilting ( f ). Among these six stressors, two were randomly selected and administered daily for a duration of 3 weeks. On the other hand, to establish the CUMR model, a set of behavioral constraints includes circadian rhythm ( g ), sleep deprivation ( h ), interference of cone light ( i ), interference of followed spotlight ( j ), high temperature stress ( k ), stroboscopic illumination ( l ), noise disturbance ( m ), and foot shock ( n ). Similarly, two out of these eight constraints were randomly chosen and applied daily for a period of 3 weeks 62
Phototherapy
Phototherapy plays a significant role in regulating emotional behavior 399 and can have strong and rapid effects on mood and alertness. 400 , 401 , 402 There is increasing evidence for the therapeutic efficacy of phototherapy for MDD. 403 , 404 The combination of phototherapy and antidepressants has better effects than antidepressants alone. 402 , 405 Phototherapy utilizes bright light with a specific wavelength to stimulate the retina and affect the production of 5-HT and hormones in the brain. 406 Furthermore, phototherapy can alleviate depressive-like behavior by targeting the retinal-thalamic ventral lateral geniculate nucleus/intergeniculate leaflet-lateral habenula (retinal-vlGN/IGL-LHb) circuit; this mechanism may explain how phototherapy alleviates MDD. 407
Repetitive transcranial magnetic stimulation
Repetitive transcranial magnetic stimulation (rTMS) is an effective method used in clinical practice for treating patients with MDD. 408 Multiple evaluations and analyses have shown that rTMS can effectively treat MDD in patients from different age groups, including children and adolescents, 409 , 410 adults, 411 , 412 and elderly patients. 413 , 414 It is suggested that early use of rTMS in the treatment of depression in elderly patients may yield better results. 415 Furthermore, research has indicated that rTMS can effectively treat perinatal depression. 416 Increasing evidence suggests that rTMS of the anterior stimulation site of the left dlPFC can yield optimal treatment outcomes. 417 , 418 , 419 A randomized controlled trial demonstrated that the efficacy of rTMS in treating depression is linked to precise targeting of the dlPFC, the activity of which exhibits a negative correlation with subgenual cingulate cortex activity. 420 Identifying the optimal site for stimulation may further enhance the ability of rTMS to treat depression. 421 Recently, a retrospective study was conducted, which included 29 systematic evaluations and reanalyzed 15 meta-analyses to assess the effectiveness and safety of transcranial magnetic stimulation (TMS) for treating MDD in adults. 422 The results of the study indicated significant variations in the efficacy of TMS for MDD across different settings and revealed poor tolerability in certain populations, the further research is necessary to identify specific beneficiary populations for TMS in treating MDD and to personalize treatment based on comprehensive and detailed information. 422
Psychological intervention
MDD is characterized by a gradual onset and a high risk of relapse. 421 The American Medical Association recommends psychological interventions for individuals who are at a high risk of MDD. Some of the interventions commonly used for depression treatment include acceptance and commitment therapy, cognitive therapy, cognitive behavioral therapy (CBT), interpersonal therapy, and psychodynamic therapies. 423 Specifically, the combination of psychological interventions and antidepressants effectively decreases the risk of relapse in cases of MDD. 424 , 425 , 426
Acupuncture
Acupuncture, which mainly includes traditional body needling, moxibustion, EA, and laser acupuncture, is a traditional Chinese treatment modality used to treat various diseases. 427 Compared with pharmacological therapies, acupuncture is more cost-effective and has fewer side effects. 428 EA stimulation can effectively treat MDD; 429 , 430 , 431 however, the specific mechanism by which acupuncture treats depression remains unclear. In previous research, EA at the ST36 acupoint was shown to prevent shrinkage of the prefrontal cortical astrocytes and alleviate depressive-like behavior in mice exposed to CUMS. 432 The results of an 8-week clinical study involving 46 female patients with severe depression suggested that acupuncture may achieve therapeutic effects by modulating the corticostriatal reward/motivation circuit in patients with severe depression. 433 Additionally, studies indicate that EA may have the potential to promote neuronal regeneration and exert antidepressant effects by elevating the phosphorylation of cyclic adenosine monophosphate response element binding protein and the levels of BDNF. 434 Acupuncture at the GV20 and GV24 acupoints may alleviate depression symptoms by regulating the calmodulin-dependent protein kinase (CaMK) signaling pathway. 435 The antidepressant effect of EA may also be associated with increased synaptic transmission in the ventromedial prefrontal cortex (vmPFC). 436 A recent meta-analysis of 43 randomized controlled trials involving adult subjects with acupuncture for MDD demonstrated that acupuncture, either alone or in combination with antidepressants, significantly reduced the hamilton depression scal scores and had fewer adverse effects compared to antidepressants, however, further rigorous experiments are still required to determine the optimal frequency of acupuncture for MDD in order to achieve better efficacy. 437
In conclusion, the common antidepressants can improve some depressive symptoms in some patients with depression, but are always associated with the risk of adverse effects or recurrence. Although some new developed treatment methods can improve depression symptoms in a certain program, the compatibility between potential treatment mechanisms and pathological mechanisms still needs further research. In particular, the therapeutic principle of acupuncture still needs to be explored in depth, and the accompanied therapeutic mechanism and application potential of traditional Chinese medicine in depression deserve to be explored in depth.
Clinical research progress
In summary, the pathological features of MDD and pharmacological mechanism of antidepressants have been widely studied. Furthermore, there have been many clinical studies on MDD, and studies of human postmortem tissues and clinical medical images, multomics studies, and preclinical/clinical trials of new therapeutic drugs have improved our understanding of the disease mechanism.
Transcriptional studies of human postmortem tissue
A recent meta-analysis of eight transcriptome datasets identified 566 disease-related genes that are consistently up- or downregulated in patients with MDD. The brain regions in which these genes are expressed include the amygdala, subgenual anterior cingulate, and dorsolateral prefrontal cortex, and the associated molecular pathways include reduced neurotrophic support, neural signaling, and GABA function. 438 Through the discovery of nonoverlapping proteins that bind to calcium parvalbumin, calretinin, and the neural peptide somatostatin, subgroups of GABA interneurons that govern main pyramidal neurons differently were identified. 439 Decreased cortical levels of GABA and specific populations of GABA neurons have been reported in investigations of postmortem MDD patient tissues, 440 and the SST mRNA level is specifically decreased in patients with MDD. 213
The DR nucleus is the largest and most significant conduit of forebrain serotonergic input. 441 In postmortem samples of the human brain, several transcriptional regulators are dysregulated within the DR, including transcription-related elements (such as EGR1, TOB1, and CSDA), which bind to genes to stimulate their expression directly or in response to environmental cues, and NRs (NR4A2, NR4A3, THRA, and THRB), which are activated by ligands and regulate translation by targeting genes. 442 In addition, transporters for GRs generally regulate the activity of the HPA axis by negative feedback. 443 According to studies of postmortem brain tissues, hyperactivity of the HPA axis in MDD patients could be caused by methylation-mediated changes in GR transcription. 444 The expression of nerve growth factor-inducible protein A (NGFI-A), an enzyme that bindss exon 1 F of GR, is reduced in the hippocampus of patients with MDD, which may contribute to low methylation levels in the brain. 444 Moreover, in postmortem MDD patients, total GR levels are unchanged, while level of GRα in the amygdala and cingulate gyrus is decreased.
Sex-related molecular markers of MDD
Women are more likely than males to experience recurring MDD 445 and are twice as likely to experience MDD throughout their lifetimes. 446 Compared with male patients, female patients with MDD have symptoms that manifest sooner in the disease course, last longer, and are more severe; in addition, they experience hunger changes, weight fluctuations, and sleep difficulties more frequently. 447 , 448
In postmortem samples of patients who committed suicide due to MDD, the expression of DNA methyltransferases (DNMTs) in the frontopolar cortex was found to be more significantly increased in women than in men; elevated methylation is associated with decreased levels of the GABA A receptor alpha-1 subunit in men, which supports sex-related epigenetic alterations in transcription. 449 A gene array meta-analysis also revealed sex differences in MDD, with depressed females being more likely than depressed men to have lower production of somatostatin, a GABA neuron biomarker in corticolimbic brain regions according to postmortem analysis. 450 X-linked chromosomal polymorphisms affect the expression of the GABA-synthesizing enzyme and somatostatin. 450 Analyses of postmortem brain tissues showed an increase in the transcription of numerous glutamate-related genes in the prefrontal cortex in depressed women but not in depressed men; depressed women exhibited more alterations in glutamate receptor expression, while depressed men showed only GRM5 downregulation. 451
In postmortem brain specimens, there were no transcription differences between MDD men and controls, and the levels of 5-HT 1D receptors and the transcription factors NUDR and REST, which regulate 5-HT activity, in 5-HT-containing neurons in the ventral raphe nuclei were found to be higher in MDD females. 452 5-HT receptors and regulators were shown to exhibit sex-specific alterations in expression at the protein level, and postmortem investigations have largely focused on female subjects. The protein levels of 5-HT 1A R and NUDR, which regulate 5-HT signaling, in the prefrontal cortex were found to be lower in MDD women than in control subjects; however, this difference was not observed in MDD males compared with controls. 453 The NA/NE system, especially in the LC, is another monoaminergic system that exhibits sex-related variations and influences MDD risk. In fact, some researchers have found that the levels of microRNAs (miRNAs), short RNA molecules that control the expression of genes and play roles in psychological disorders, 454 are higher in the LC of suicidal female subjects than in the LC of suicidal male subjects. MiR-1179 is associated with GRIA3 and MAOA, which are involved in neuropsychiatric diseases. 455
OS is commonly linked to the onset of MDD. A study found that whereas cysteine and 1-methylinosine levels were much higher in males with MDD, they were significantly lower in females with MDD. 456 These metabolites are related to OS. Furthermore, several studies found a significant link between MDD and lipid metabolism; 457 for example, as 1-Oalkyl-2-acyl-PEs levels are decreased in MDD, showing a negative correlation with the extent of depression, lysophospholipid (LPC) and phospholipid (PC) levels are increased in MDD, exhibiting a substantial positive correlation with depression severity. 458 Similarly, a study found that men and women had different lipid concentrations. 456 These clinical data suggest that sex differences in MDD may result from differences in OS and lipid metabolism, but further research is required to make this connection.
Multiomics studies
Transcriptome studies, which explore relationships among the expression of genes and diseases, are regarded as an essential for investigating disease-causing mutations in genes, the mechanisms of disease development and progression, and disease-related target genes. 459 Dorsolateral prefrontal cortex tissues have been employed to identify genes and miRNAs that show changes in expression and biological processes that are altered in patients with MDD. 460 Serpin Family H Member 1 (SERPINH1), IL-8, humanin like-8 (MTRNRL8), and chemokine ligand 4 (CCL4) are among the genes whose expression is altered in MDD. 460 , 461 According to Gene Ontology (GO) enrichment analysis, MDD is related to decreased expression of genes related to oligodendrocyte development, glutamatergic neurotransmission modulation, and oxytocin receptor expression. These findings confirm that impairment of the blood-brain barrier and microglial, endothelial cell, ATPase, and astrocyte function exacerbate MDD; the involvement of these cells, molecules, and structures in MDD should be further investigated. 460
The field of study known as genomics focuses on the transcription of genes, the precise interactions among genes, and the control of gene activity. MDD has been linked to numerous biological processes, including energy metabolism. When the transcription of genes involved in glycolysis and glycogen synthesis was examined in the hippocampus of depressed rats, it was found that the mRNA expression of Slc2a3, which codes for GLUT3, is considerably increased. 462 Glyceraldehyde-3-phosphate dehydrogenase (GAPDH) and lactate dehydrogenase B (LDHB) mRNA levels were found to be substantially decreased in MDD. 462 The transcription of genes in the brain tissues of IL18 - / - mice was examined with the use of genome-wide microarrays, and the results revealed that urocortin 3 (Ucn3) expression was increased. 463 Ucn3 controls how the body processes glucose; 464 therefore, a change in Ucn3 expression will result in energy imbalance. Gene comethylation analysis was performed in the brains of individuals with MDD. The findings revealed that the methylation of genes associated with mitochondria was dramatically decreased, indicating impaired mitochondrial function. 465
Metabolomics has recently emerged as a useful technique for identifying markers and pathways associated with a wide range of diseases. 466 It is often used to analyze the mechanisms underlying disease occurrence and progression and the effects of small-molecule compounds. In one study, targeted metabolomic analysis of the CSF of 14 MDD patients who were not taking medication, 14 MDD patients in remission, and 18 healthy controls was performed. 467 An analysis of the tryptophan, tyrosine, purine pathways, and associated pathways revealed that in patients in remission, methionine levels were higher, while tryptophan and tyrosine levels were lower. The same group of patients also showed changes in the methionine-to-glutathione ratio, indicating alterations in OS and methylation. The levels of these same metabolites were altered in MDD patients who were not taking medication, although not to a significant degree. 467
Clinical medical imaging studies
MRI has been widely employed in research in recent years to pinpoint patterns of brain alterations linked to MDD. Many studies have demonstrated that structural and fMRI has outstanding potential as trustworthy imaging modalities for monitoring MDD treatment responses. A study indicated that MDD patients had large volume decreases in various frontal areas, such as the anterior cingulate cortex and OFC, which were linked to problems with stress management and emotional processing. 468 People with MDD also exhibited structural changes in their parietal lobes. 469 Alterations in the total gray matter volume and an increase in cortical thickness are the two findings that are most consistent. 470
The functional changes in the frontal lobe in MDD are hotly contested. A study discovered lower precuneus, supragenual anterior cingulate cortex, dorsomedial PFC, and dorsomedial thalamus lower activity when processing pleasant stimuli in MDD patients. 471 Another study found that during the processing of favorable self-indulgent information, individuals with MDD displayed higher activity in the medial PFC and anterior cingulate cortex. 472 The right hippocampus, parahippocampal gyrus, left amygdala, and the whole caudate nucleus all had functional changes in activity in MDD patients compared to healthy controls, indicating that the temporal lobe might be involved in the pathogenesis of MDD. 473
Although it is not feasible to evaluate synapse density directly in people in vivo, positron emission tomography (PET) can be utilized to gather useful information. It is thought that impairments of functional connections and synaptic atrophy are two factors that contribute to the symptoms of MDD. An indirect method of estimating synaptic density is to count the number of nerve terminals using synaptic vesicle glycoprotein 2 A (SV2A). The researchers examined synaptic density in MDD patients who were not taking any medication using positron emission PET with the SV2A radioligand [ 11 C] UCB-J. 474 The results revealed that reductions in the synapse density in areas connected with various processes, such as emotion control and thought (the dorsolateral prefrontal cortex, anterior cingulate cortex, and hippocampus), are related to to the severity of depressive disorders. Additionally, it was shown that compared with healthy subjects, subjects with MDD had reduced dlPFC resting-state connectivity throughout the brain. It was found that the dlPFC-posterior cingulate cortex connection was inversely negatively linked to the severity of depression symptoms and connected with synapse activity in the dlPFC, indicating that synaptic loss may impair antagonistism within the centers of both networks, which are typically at odds. 474
Preclinical and clinical trials of new therapeutic drugs
Esmethadone is a new, noncompetitive NMDAR antagonist 475 that exhibits fast antidepressant-like action by improving performance of rats in the forced swim test. 476 Esmethadone can also alleviate neural dysfunction linked to symptoms of depression by boosting the synapse and spine density and restoring spinogenesis, in addition to correcting depressive-like behaviors in animal models of depression. 378 , 477 Esmethadone was found to reduce cognitive symptoms in individuals with MDD in a stage II clinical study 478 and to increase the levels of circulating BDNF in normal individuals in a stage I clinical investigation. 479 In a phase II study involving patients who had received insufficient benefit from conventional antidepressants, esmethadone demonstrated immediate, strong, and long-lasting antidepressant benefits. 478
Ketamine is the most well-known rapid-acting antidepressant and an NMDAR antagonist. 383 GluN1, GluN2, and GluN3 are NMDAR subunits. 480 Ketamine exerts a quick and effective antidepressant effect by binding to the asparagine 616 residue of GluN1 and the leucine 642 residue of GluN2A. 192 In a clinical experiment, the effect of supplementary injection of subanesthetic doses of ketamine on thoughts of suicide in MDD patients was evaluated, and the results showed that the reduction in thoughts of suicide among MDD patients receiving ketamine was mostly sustained. 481 In several studies, a single dose of ketamine reduced immobility in the forced swim test immediately after injection and had effects similar to those of an antidepressant. 482 , 483
The S-enantiomer of ketamine, esketamine, has been approved by the U.S. Food and Drug Administration (FDA) for depression treatment. 383 Moreover, formulations of ketamine are also being developed, and intranasal esketamine spray has shown high efficacy in treating MDD. 484 Additionally, hydroxynorketamine (HNK), a metabolite of ketamine, can exert its anti-depressive effects by an NMDAR-independent mechanism. 377 One of these mechanisms involves increasing BDNF levels; an increasing number of studies have shown that BDNF signaling is an important target of antidepressants. 377 Thus, ketamine can also exert anti-inflammatory effects, a large amount of evidence suggests a tight relationship between neuroinflammation and the pathogenesis of MDD. 485 , 486 , 487 A summary of clinical trials related to new therapeutic drugs for MDD is shown in Table 1 .
The development of the present therapeutic medicines in clinic mainly targets the discovered pharmacological targets, mainly focusing on the key receptors or enzymes. However, at the organelle level of neural cells, the disturbed energy metabolism of mitochondria and the related RNA drugs, as well as the dysfunctions of lipid and glucose metabolism in psychopathological condition, still need deep exploration. Totally, the research on the mechanism of therapeutic drugs always requires the development of pathological mechanisms as support.
Conclusions and future perspectives
MDD is a heterogeneous disease, its pathological and pharmacological mechanisms are still unclear, and diagnostic and therapeutic methods for MDD are limited. SSRIs and SNRIs are the first-line treatments for MDD in the clinic; however, a sizable portion of MDD patients do not respond well to the currently available antidepressants. According to research on real-world sequential therapies, even after numerous treatment attempts, almost 30% of MDD patients do not experience remission. This suggests that the existing theories and hypotheses cannot completely explain the pathogenesis of MDD and that more research on the pharmacological mechanisms of currently available antidepressants is still needed. We mainly discussed the potential etiology and pathogenesis of MDD from the perspective of widely accepted theories, including the neurotransmitter and receptor hypothesis, HPA axis hypothesis, cytokine hypothesis, neuroplasticity hypothesis and systemic influence hypothesis. A more comprehensive understanding of the pathophysiological mechanisms of MDD might significantly improve our capacity to develop preventive and more effective therapeutic methods that can help reduce the burden of and pain caused by major depression. Knowledge of the cellular processes that drive these alterations and the symptoms they cause may offer crucial will provide insight for new treatments.
MDD is connected with several cellular and structural modifications in the nervous system. Nonetheless, in the majority of these alterations cannot be consistently observed in vivo. Therefore, several issues need to be considered in future research: (i) Studies of animal models have made important contributions to our understanding of the pathophysiology of major depression, and more representative animal models of MDD should be developed. (ii) Because of our incomplete understanding of the disease and the disease’s intrinsic intricacy, there is an urgent need to develop updated imaging technologies and imaging software to allow advances in our understanding of the disease. (iii) The therapeutic shortcomings of traditional antidepressants have prompted the need for further drug discovery and development. (iv) MDD is strongly associated with many systems, and it will be important to further elucidate the mechanisms associated with MDD and other pathological conditions.
Disease, G. B. D., Injury, I. & Prevalence, C. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 392 , 1789–1858 (2018).
Article Google Scholar
Nagy, C. et al. Single-nucleus transcriptomics of the prefrontal cortex in major depressive disorder implicates oligodendrocyte precursor cells and excitatory neurons. Nat. Neurosci. 23 , 771–781 (2020).
Article CAS PubMed Google Scholar
Malhi, G. S. & Mann, J. J. Depression Lancet 392 , 2299–2312 (2018).
Article PubMed Google Scholar
Fellinger, M. et al. Seasonality in major depressive disorder: effect of sex and age. J. Affect Disord. 296 , 111–116 (2022).
Liu, C. H. et al. Role of inflammation in depression relapse. J. Neuroinflammation 16 , 90 (2019).
Article PubMed PubMed Central Google Scholar
Burcusa, S. L. & Iacono, W. G. Risk for recurrence in depression. Clin. Psychol. Rev. 27 , 959–985 (2007).
Monroe, S. M. & Harkness, K. L. Life stress, the “kindling” hypothesis, and the recurrence of depression: considerations from a life stress perspective. Psychol. Rev. 112 , 417–445 (2005).
Albert, K. M. & Newhouse, P. A. Estrogen, stress, and depression: cognitive and biological interactions. Annu. Rev. Clin. Psychol. 15 , 399–423 (2019).
Kessler, R. C., Chiu, W. T., Demler, O., Merikangas, K. R. & Walters, E. E. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 62 , 617–627 (2005).
Monteleone, P. & Maj, M. The circadian basis of mood disorders: recent developments and treatment implications. Eur. Neuropsychopharmacol. 18 , 701–711 (2008).
Rice, F. et al. Adolescent and adult differences in major depression symptom profiles. J. Affect Disord. 243 , 175–181 (2019).
Hasin, D. S. et al. Epidemiology of adult DSM-5 major depressive disorder and its specifiers in the United States. JAMA Psychiatry 75 , 336–346 (2018).
Howard, D. M. et al. Genome-wide association study of depression phenotypes in UK Biobank identifies variants in excitatory synaptic pathways. Nat. Commun. 9 , 1470 (2018).
Kovacs, M. & Lopez-Duran, N. Prodromal symptoms and atypical affectivity as predictors of major depression in juveniles: implications for prevention. J. Child Psychol. Psychiatry 51 , 472–496 (2010).
Stetler, C. & Miller, G. E. Depression and hypothalamic-pituitary-adrenal activation: a quantitative summary of four decades of research. Psychosom. Med. 73 , 114–126 (2011).
Milaneschi, Y., Lamers, F., Berk, M. & Penninx, B. Depression heterogeneity and its biological underpinnings: toward immunometabolic depression. Biol. Psychiatry 88 , 369–380 (2020).
Zhou, X. et al. Astrocyte, a promising target for mood disorder interventions. Front. Mol. Neurosci. 12 , 136 (2019).
Article CAS PubMed PubMed Central Google Scholar
Monroe, S. M. & Harkness, K. L. Major depression and its recurrences: life course matters. Annu. Rev. Clin. Psychol. 18 , 329–357 (2022).
Wray, N. R. et al. Genome-wide association analyses identify 44 risk variants and refine the genetic architecture of major depression. Nat. Genet. 50 , 668–681 (2018).
Gittins, R. A. & Harrison, P. J. A morphometric study of glia and neurons in the anterior cingulate cortex in mood disorder. J. Affect. Disord. 133 , 328–332 (2011).
Miguel-Hidalgo, J. J. et al. Glial and glutamatergic markers in depression, alcoholism, and their comorbidity. J. Affect. Disord. 127 , 230–240 (2010).
Sequeira, A. et al. Global brain gene expression analysis links glutamatergic and GABAergic alterations to suicide and major depression. PLoS ONE 4 , e6585 (2009).
Rajkowska, G. & Stockmeier, C. A. Astrocyte pathology in major depressive disorder: insights from human postmortem brain tissue. Curr. Drug Targets 14 , 1225–1236 (2013).
Tsuang, M. T., Taylor, L. & Faraone, S. V. An overview of the genetics of psychotic mood disorders. J. Psychiatr. Res 38 , 3–15 (2004).
Lohoff, F. W. Overview of the genetics of major depressive disorder. Curr. Psychiatry Rep. 12 , 539–546 (2010).
Kendall, K. M. et al. The genetic basis of major depression. Psychol. Med. 51 , 2217–2230 (2021).
Power, R. A. et al. Genome-wide association for major depression through age at onset stratification: Major Depressive Disorder Working Group of the psychiatric genomics consortium. Biol. Psychiatry 81 , 325–335 (2017).
Huang, C. et al. Proteomic analysis of olfactory bulb suggests CACNA1E as a promoter of CREB signaling in microbiota-induced depression. J. Proteom. 194 , 132–147 (2019).
Article CAS Google Scholar
Flint, J. The genetic basis of major depressive disorder. Mol. Psychiatry 28 , 2254–2265 (2023).
Tripp, A., Kota, R. S., Lewis, D. A. & Sibille, E. Reduced somatostatin in subgenual anterior cingulate cortex in major depression. Neurobiol. Dis. 42 , 116–124 (2011).
Seney, M. L., Tripp, A., McCune, S., Lewis, D. A. & Sibille, E. Laminar and cellular analyses of reduced somatostatin gene expression in the subgenual anterior cingulate cortex in major depression. Neurobiol. Dis. 73 , 213–219 (2015).
Hicks, E. M. et al. Integrating genetics and transcriptomics to study major depressive disorder: a conceptual framework, bioinformatic approaches, and recent findings. Transl. Psychiatry 13 , 129 (2023).
Labonte, B. et al. Sex-specific transcriptional signatures in human depression. Nat. Med. 23 , 1102–1111 (2017).
Levey, D. F. et al. Bi-ancestral depression GWAS in the Million Veteran Program and meta-analysis in >1.2 million individuals highlight new therapeutic directions. Nat. Neurosci. 24 , 954–963 (2021).
Cohen-Woods, S., Craig, I. W. & McGuffin, P. The current state of play on the molecular genetics of depression. Psychol. Med. 43 , 673–687 (2013).
Slavich, G. M. & Sacher, J. Stress, sex hormones, inflammation, and major depressive disorder: Extending Social Signal Transduction Theory of Depression to account for sex differences in mood disorders. Psychopharmacology 236 , 3063–3079 (2019).
McEwen, B. S., Nasca, C. & Gray, J. D. Stress effects on neuronal structure: hippocampus, amygdala, and prefrontal cortex. Neuropsychopharmacology 41 , 3–23 (2016).
Fries, G. R., Saldana, V. A., Finnstein, J. & Rein, T. Molecular pathways of major depressive disorder converge on the synapse. Mol. Psychiatry 28 , 284–297 (2023).
Keller, J. et al. HPA axis in major depression: cortisol, clinical symptomatology and genetic variation predict cognition. Mol. Psychiatry 22 , 527–536 (2017).
Dong, L., Li, B., Verkhratsky, A. & Peng, L. Cell type-specific in vivo expression of genes encoding signalling molecules in the brain in response to chronic mild stress and chronic treatment with fluoxetine. Psychopharmacology 232 , 2827–2835 (2015).
Xia, M. et al. Sleep deprivation selectively down-regulates astrocytic 5-HT(2B) receptors and triggers depressive-like behaviors via stimulating P2X(7) receptors in mice. Neurosci. Bull. 36 , 1259–1270 (2020).
Hare, D. L., Toukhsati, S. R., Johansson, P. & Jaarsma, T. Depression and cardiovascular disease: a clinical review. Eur. Heart J. 35 , 1365–1372 (2014).
Dunbar, J. A. et al. Depression: an important comorbidity with metabolic syndrome in a general population. Diabetes Care 31 , 2368–2373 (2008).
Arnaud, A. M. et al. Impact of major depressive disorder on comorbidities: a systematic literature review. J. Clin. Psychiatry 83 , 21r14328 (2022).
Sato, S. & Yeh, T. L. Challenges in treating patients with major depressive disorder: the impact of biological and social factors. CNS Drugs 27 , S5–10 (2013).
Greenberg, P. E., Fournier, A. A., Sisitsky, T., Pike, C. T. & Kessler, R. C. The economic burden of adults with major depressive disorder in the United States (2005 and 2010). J. Clin. Psychiatry 76 , 155–162 (2015).
Greenberg, P. E. et al. The economic burden of adults with major depressive disorder in the United States (2010 and 2018). Pharmacoeconomics 39 , 653–665 (2021).
Dean, J. & Keshavan, M. The neurobiology of depression: an integrated view. Asian J. Psychiatr. 27 , 101–111 (2017).
Bhatt, S., Devadoss, T., Manjula, S. N. & Rajangam, J. 5-HT(3) receptor antagonism a potential therapeutic approach for the treatment of depression and other disorders. Curr. Neuropharmacol. 19 , 1545–1559 (2021).
Inazu, M., Takeda, H. & Matsumiya, T. Functional expression of the norepinephrine transporter in cultured rat astrocytes. J. Neurochem. 84 , 136–144 (2003).
Schipke, C. G., Heuser, I. & Peters, O. Antidepressants act on glial cells: SSRIs and serotonin elicit astrocyte calcium signaling in the mouse prefrontal cortex. J. Psychiatr. Res. 45 , 242–248 (2011).
Novikova, I. N. et al. Adrenaline induces calcium signal in astrocytes and vasoconstriction via activation of monoamine oxidase. Free Radic. Biol. Med. 159 , 15–22 (2020).
Martin, H. et al. Insulin modulates emotional behavior through a serotonin-dependent mechanism. Mol. Psychiatry (2022). [Oline ahead of print].
Ogawa, S. et al. Plasma L-tryptophan concentration in major depressive disorder: new data and meta-analysis. J. Clin. Psychiatry 75 , e906–915 (2014).
Fang, Y. et al. Fluoxetine inhibited the activation of A1 reactive astrocyte in a mouse model of major depressive disorder through astrocytic 5-HT(2B)R/beta-arrestin2 pathway. J. Neuroinflammation 19 , 23 (2022).
Savitz, J., Lucki, I. & Drevets, W. C. 5-HT(1A) receptor function in major depressive disorder. Prog. Neurobiol. 88 , 17–31 (2009).
Verkhratsky, A., Rodriguez, J. J. & Parpura, V. Astroglia in neurological diseases. Future Neurol. 8 , 149–158 (2013).
Zhang, S. et al. 5-HT2B receptors are expressed on astrocytes from brain and in culture and are a chronic target for all five conventional ‘serotonin-specific reuptake inhibitors. Neuron Glia Biol. 6 , 113–125 (2010).
Verkhratsky, A., Parpura, V., Scuderi, C. & Li, B. Astroglial serotonin receptors as the central target of classic antidepressants. Adv. Neurobiol. 26 , 317–347 (2021).
Li, B. et al. Biphasic regulation of caveolin-1 gene expression by fluoxetine in astrocytes: opposite effects of PI3K/AKT and MAPK/ERK signaling pathways on c-fos. Front. Cell. Neurosci. 11 , 335 (2017).
Li, B., Zhang, S., Li, M., Hertz, L. & Peng, L. Chronic treatment of astrocytes with therapeutically relevant fluoxetine concentrations enhances cPLA2 expression secondary to 5-HT 2B -induced, transactivation-mediated ERK 1/2 phosphorylation. Psychopharmacology 207 , 1–12 (2009).
Li, X. et al. A novel murine model of mania. Mol. Psychiatry 28 , 3044–3054 (2023).
Li, B., Zhang, S., Zhang, H., Hertz, L. & Peng, L. Fluoxetine affects GluK2 editing, glutamate-evoked Ca(2+) influx and extracellular signal-regulated kinase phosphorylation in mouse astrocytes. J. Psychiatry Neurosci. 36 , 322–338 (2011).
Li, B. et al. Cell type-specific gene expression and editing responses to chronic fluoxetine treatment in the in vivo mouse brain and their relevance for stress-induced anhedonia. Neurochem. Res. 37 , 2480–2495 (2012).
Breton-Provencher, V., Drummond, G. T., Feng, J., Li, Y. & Sur, M. Spatiotemporal dynamics of noradrenaline during learned behaviour. Nature 606 , 732–738 (2022).
Mori, K. et al. Effects of norepinephrine on rat cultured microglial cells that express alpha1, alpha2, beta1 and beta2 adrenergic receptors. Neuropharmacology 43 , 1026–1034 (2002).
O’Sullivan, J. B., Ryan, K. M., Curtin, N. M., Harkin, A. & Connor, T. J. Noradrenaline reuptake inhibitors limit neuroinflammation in rat cortex following a systemic inflammatory challenge: implications for depression and neurodegeneration. Int. J. Neuropsychopharmacol. 12 , 687–699 (2009).
Choi, H. S. et al. The anti-inflammatory activity of duloxetine, a serotonin/norepinephrine reuptake inhibitor, prevents kainic acid-induced hippocampal neuronal death in mice. J. Neurol. Sci. 358 , 390–397 (2015).
Wang, J. et al. Desvenlafaxine prevents white matter injury and improves the decreased phosphorylation of the rate-limiting enzyme of cholesterol synthesis in a chronic mouse model of depression. J. Neurochem. 131 , 229–238 (2014).
Luo, Y., Kataoka, Y., Ostinelli, E. G., Cipriani, A. & Furukawa, T. A. National prescription patterns of antidepressants in the treatment of adults with major depression in the US Between 1996 and 2015: a population representative survey based analysis. Front. Psychiatry 11 , 35 (2020).
Sun, J. D., Liu, Y., Yuan, Y. H., Li, J. & Chen, N. H. Gap junction dysfunction in the prefrontal cortex induces depressive-like behaviors in rats. Neuropsychopharmacology 37 , 1305–1320 (2012).
Zepeda, R. et al. Venlafaxine treatment after endothelin-1-induced cortical stroke modulates growth factor expression and reduces tissue damage in rats. Neuropharmacology 107 , 131–145 (2016).
Bekhbat, M. et al. Correction to: functional connectivity in reward circuitry and symptoms of anhedonia as therapeutic targets in depression with high inflammation: evidence from a dopamine challenge study. Mol. Psychiatry 27 , 4122 (2022).
Cui, Y. et al. Astroglial Kir4.1 in the lateral habenula drives neuronal bursts in depression. Nature 554 , 323–327 (2018).
Skupio, U. et al. Astrocytes determine conditioned response to morphine via glucocorticoid receptor-dependent regulation of lactate release. Neuropsychopharmacology 45 , 404–415 (2020).
Rasheed, N. et al. Differential response of central dopaminergic system in acute and chronic unpredictable stress models in rats. Neurochem. Res. 35 , 22–32 (2010).
Morales, I., Fuentes, A., Ballaz, S., Obeso, J. A. & Rodriguez, M. Striatal interaction among dopamine, glutamate and ascorbate. Neuropharmacology 63 , 1308–1314 (2012).
Solis, O., Garcia-Sanz, P., Herranz, A. S., Asensio, M. J. & Moratalla, R. L-DOPA reverses the increased free amino acids tissue levels induced by dopamine depletion and rises GABA and tyrosine in the striatum. Neurotox. Res. 30 , 67–75 (2016).
Corkrum, M. et al. Dopamine-evoked synaptic regulation in the nucleus accumbens requires astrocyte activity. Neuron 105 , 1036–1047.e1035 (2020).
Adermark, L. et al. Astrocytes modulate extracellular neurotransmitter levels and excitatory neurotransmission in dorsolateral striatum via dopamine D2 receptor signaling. Neuropsychopharmacology 47 , 1493–1502 (2022).
Agren, R. & Sahlholm, K. Voltage-dependent dopamine potency at D(1)-like dopamine receptors. Front Pharmacol. 11 , 581151 (2020).
Fasano, C. et al. Dopamine facilitates dendritic spine formation by cultured striatal medium spiny neurons through both D1 and D2 dopamine receptors. Neuropharmacology 67 , 432–443 (2013).
Hao, Y. & Plested, A. J. R. Seeing glutamate at central synapses. J. Neurosci. Methods 375 , 109531 (2022).
Trudler, D. et al. alpha-synuclein oligomers induce glutamate release from astrocytes and excessive extrasynaptic NMDAR activity in neurons, thus contributing to synapse loss. J. Neurosci. 41 , 2264–2273 (2021).
Schmitz, F. et al. Methylphenidate decreases ATP levels and impairs glutamate uptake and Na(+),K(+)-ATPase activity in juvenile rat hippocampus. Mol. Neurobiol. 54 , 7796–7807 (2017).
Kucukibrahimoglu, E. et al. The change in plasma GABA, glutamine and glutamate levels in fluoxetine- or S-citalopram-treated female patients with major depression. Eur. J. Clin. Pharmacol. 65 , 571–577 (2009).
Chiba, S. et al. Chronic restraint stress causes anxiety- and depression-like behaviors, downregulates glucocorticoid receptor expression, and attenuates glutamate release induced by brain-derived neurotrophic factor in the prefrontal cortex. Prog. Neuropsychopharmacol. Biol. Psychiatry 39 , 112–119 (2012).
Sullivan, R. et al. Cloning, transport properties, and differential localization of two splice variants of GLT-1 in the rat CNS: implications for CNS glutamate homeostasis. Glia 45 , 155–169 (2004).
Zou, J. et al. Glutamine synthetase down-regulation reduces astrocyte protection against glutamate excitotoxicity to neurons. Neurochem. Int. 56 , 577–584 (2010).
Karlsson, R. M. et al. Assessment of glutamate transporter GLAST (EAAT1)-deficient mice for phenotypes relevant to the negative and executive/cognitive symptoms of schizophrenia. Neuropsychopharmacology 34 , 1578–1589 (2009).
Karlsson, R. M. et al. Reduced alcohol intake and reward associated with impaired endocannabinoid signaling in mice with a deletion of the glutamate transporter GLAST. Neuropharmacology 63 , 181–189 (2012).
Di Castro, M. A. et al. Local Ca2+ detection and modulation of synaptic release by astrocytes. Nat. Neurosci. 14 , 1276–1284 (2011).
Matos, M. et al. Deletion of adenosine A2A receptors from astrocytes disrupts glutamate homeostasis leading to psychomotor and cognitive impairment: relevance to schizophrenia. Biol. Psychiatry 78 , 763–774 (2015).
Yue, N. et al. Activation of P2X7 receptor and NLRP3 inflammasome assembly in hippocampal glial cells mediates chronic stress-induced depressive-like behaviors. J. Neuroinflammation 14 , 102 (2017).
Cao, X. et al. Astrocyte-derived ATP modulates depressive-like behaviors. Nat. Med. 19 , 773–777 (2013).
Cunha, G. M., Canas, P. M., Oliveira, C. R. & Cunha, R. A. Increased density and synapto-protective effect of adenosine A2A receptors upon sub-chronic restraint stress. Neuroscience 141 , 1775–1781 (2006).
Batalha, V. L. et al. Adenosine A(2A) receptor blockade reverts hippocampal stress-induced deficits and restores corticosterone circadian oscillation. Mol. Psychiatry 18 , 320–331 (2013).
Wang, M. et al. Lateral septum adenosine A(2A) receptors control stress-induced depressive-like behaviors via signaling to the hypothalamus and habenula. Nat. Commun. 14 , 1880 (2023).
Lucas, M. et al. Coffee, caffeine, and risk of completed suicide: results from three prospective cohorts of American adults. World J. Biol. Psychiatry 15 , 377–386 (2014).
Lucas, M. et al. Coffee, caffeine, and risk of depression among women. Arch. Intern. Med. 171 , 1571–1578 (2011).
Coelho, J. E. et al. Overexpression of adenosine A2A receptors in rats: effects on depression, locomotion, and anxiety. Front. Psychiatry 5 , 67 (2014).
Kaster, M. P. et al. Caffeine acts through neuronal adenosine A2A receptors to prevent mood and memory dysfunction triggered by chronic stress. Proc. Natl Acad. Sci. USA 112 , 7833–7838 (2015).
Hines, D. J., Schmitt, L. I., Hines, R. M., Moss, S. J. & Haydon, P. G. Antidepressant effects of sleep deprivation require astrocyte-dependent adenosine mediated signaling. Transl. Psychiatry 3 , e212 (2013).
Etievant, A. et al. Astroglial control of the antidepressant-like effects of prefrontal cortex deep brain stimulation. EBioMedicine 2 , 898–908 (2015).
Serchov, T. et al. Increased signaling via adenosine A1 receptors, sleep deprivation, imipramine, and ketamine inhibit depressive-like behavior via induction of Homer1a. Neuron 87 , 549–562 (2015).
Dostal, C. R., Carson Sulzer, M., Kelley, K. W., Freund, G. G. & McCusker, R. H. Glial and tissue-specific regulation of Kynurenine Pathway dioxygenases by acute stress of mice. Neurobiol. Stress 7 , 1–15 (2017).
Yang, W. et al. Dex modulates the balance of water-electrolyte metabolism by depressing the expression of AVP in PVN. Front. Pharmacol. 13 , 919032 (2022).
Jacobson, L. Forebrain glucocorticoid receptor gene deletion attenuates behavioral changes and antidepressant responsiveness during chronic stress. Brain Res. 1583 , 109–121 (2014).
Perez, P. Glucocorticoid receptors, epidermal homeostasis and hair follicle differentiation. Dermatoendocrinol 3 , 166–174 (2011).
Reichrath, J. Ancient friends, revisited: new aspects on the important role of nuclear receptor signalling for skin physiology and for the treatment of skin diseases. Dermatoendocrinol 3 , 121–124 (2011).
Herbert, J. & Lucassen, P. J. Depression as a risk factor for Alzheimer’s disease: genes, steroids, cytokines and neurogenesis - What do we need to know? Front. Neuroendocrinol. 41 , 153–171 (2016).
Rosenthal, L. J., Goldner, W. S. & O’Reardon, J. P. T3 augmentation in major depressive disorder: safety considerations. Am. J. Psychiatry 168 , 1035–1040 (2011).
Mokrani, M. C., Duval, F., Erb, A., Gonzalez Lopera, F. & Danila, V. Are the thyroid and adrenal system alterations linked in depression? Psychoneuroendocrinology 122 , 104831 (2020).
Stenzel, D. & Huttner, W. B. Role of maternal thyroid hormones in the developing neocortex and during human evolution. Front. Neuroanat. 7 , 19 (2013).
Mendes-de-Aguiar, C. B. et al. Thyroid hormone increases astrocytic glutamate uptake and protects astrocytes and neurons against glutamate toxicity. J. Neurosci. Res. 86 , 3117–3125 (2008).
Rastogi, L., Godbole, M. M., Sinha, R. A. & Pradhan, S. Reverse triiodothyronine (rT3) attenuates ischemia-reperfusion injury. Biochem. Biophys. Res. Commun. 506 , 597–603 (2018).
Isgor, C. & Watson, S. J. Estrogen receptor alpha and beta mRNA expressions by proliferating and differentiating cells in the adult rat dentate gyrus and subventricular zone. Neuroscience 134 , 847–856 (2005).
Russell, J. K., Jones, C. K. & Newhouse, P. A. The role of estrogen in brain and cognitive aging. Neurotherapeutics 16 , 649–665 (2019).
Biegon, A., Reches, A., Snyder, L. & McEwen, B. S. Serotonergic and noradrenergic receptors in the rat brain: modulation by chronic exposure to ovarian hormones. Life Sci. 32 , 2015–2021 (1983).
Arinami, H., Suzuki, Y., Tajiri, M., Tsuneyama, N. & Someya, T. Role of insulin-like growth factor 1, sex and corticosteroid hormones in male major depressive disorder. BMC Psychiatry 21 , 157 (2021).
Walf, A. A., Rhodes, M. E. & Frye, C. A. Antidepressant effects of ERbeta-selective estrogen receptor modulators in the forced swim test. Pharm. Biochem Behav. 78 , 523–529 (2004).
Frye, C. A. & Walf, A. A. Estrogen and/or progesterone administered systemically or to the amygdala can have anxiety-, fear-, and pain-reducing effects in ovariectomized rats. Behav. Neurosci. 118 , 306–313 (2004).
Hughes, Z. A. et al. WAY-200070, a selective agonist of estrogen receptor beta as a potential novel anxiolytic/antidepressant agent. Neuropharmacology 54 , 1136–1142 (2008).
Weiser, M. J., Wu, T. J. & Handa, R. J. Estrogen receptor-beta agonist diarylpropionitrile: biological activities of R- and S-enantiomers on behavior and hormonal response to stress. Endocrinology 150 , 1817–1825 (2009).
Irwin, R. W. et al. Selective oestrogen receptor modulators differentially potentiate brain mitochondrial function. J. Neuroendocrinol. 24 , 236–248 (2012).
Ho, M. F. et al. Ketamine and ketamine metabolites as novel estrogen receptor ligands: Induction of cytochrome P450 and AMPA glutamate receptor gene expression. Biochem. Pharmacol. 152 , 279–292 (2018).
Hochol, A. et al. Effects of neuropeptides B and W on the rat pituitary-adrenocortical axis: in vivo and in vitro studies. Int J. Mol. Med. 19 , 207–211 (2007).
CAS PubMed Google Scholar
Kurosawa, N., Shimizu, K. & Seki, K. The development of depression-like behavior is consolidated by IL-6-induced activation of locus coeruleus neurons and IL-1beta-induced elevated leptin levels in mice. Psychopharmacology 233 , 1725–1737 (2016).
Lee, J. Y. et al. The association between serum leptin levels and post-stroke depression: a retrospective clinical study. Ann. Rehabil. Med. 39 , 786–792 (2015).
Li, Z. et al. Fluoxetine improves behavioural deficits induced by chronic alcohol treatment by alleviating RNA editing of 5-HT(2C) receptors. Neurochem. Int. 134 , 104689 (2020).
de Morais, H. et al. Increased oxidative stress in prefrontal cortex and hippocampus is related to depressive-like behavior in streptozotocin-diabetic rats. Behav. Brain Res. 258 , 52–64 (2014).
Rawdin, B. J. et al. Dysregulated relationship of inflammation and oxidative stress in major depression. Brain Behav. Immun. 31 , 143–152 (2013).
Dringen, R. Metabolism and functions of glutathione in brain. Prog. Neurobiol. 62 , 649–671 (2000).
Greaney, J. L., Saunders, E. F. H. & Alexander, L. M. Short-term salicylate treatment improves microvascular endothelium-dependent dilation in young adults with major depressive disorder. Am. J. Physiol. Heart Circ. Physiol. 322 , H880–H889 (2022).
Belanger, M. & Magistretti, P. J. The role of astroglia in neuroprotection. Dialogues Clin. Neurosci. 11 , 281–295 (2009).
Chen, B. et al. The neuroprotective mechanism of lithium after ischaemic stroke. Commun. Biol. 5 , 105 (2022).
Maes, M. et al. Major differences in neurooxidative and neuronitrosative stress pathways between major depressive disorder and types I and II bipolar disorder. Mol. Neurobiol. 56 , 141–156 (2019).
Early, J. O. et al. Circadian clock protein BMAL1 regulates IL-1beta in macrophages via NRF2. Proc. Natl Acad. Sci. USA 115 , E8460–E8468 (2018).
Pasco, J. A. et al. Association of high-sensitivity C-reactive protein with de novo major depression. Br. J. Psychiatry 197 , 372–377 (2010).
Bakunina, N., Pariante, C. M. & Zunszain, P. A. Immune mechanisms linked to depression via oxidative stress and neuroprogression. Immunology 144 , 365–373 (2015).
Paul, E. R. et al. Peripheral and central kynurenine pathway abnormalities in major depression. Brain Behav. Immun. 101 , 136–145 (2022).
Wang, Y. et al. Inhibition of activated astrocyte ameliorates lipopolysaccharide- induced depressive-like behaviors. J. Affect Disord. 242 , 52–59 (2019).
Lenk, T., Rabet, S., Sprick, M., Raabe, G. & Schroder, U. Insight into the interaction of furfural with metallic surfaces in the electrochemical hydrogenation process. Chemphyschem 24 , e202200614 (2023).
Zhang, J. C., Yao, W. & Hashimoto, K. Brain-derived neurotrophic factor (BDNF)-TrkB signaling in inflammation-related depression and potential therapeutic targets. Curr. Neuropharmacol. 14 , 721–731 (2016).
Kennis, M. et al. Prospective biomarkers of major depressive disorder: a systematic review and meta-analysis. Mol. Psychiatry 25 , 321–338 (2020).
Norden, D. M., Trojanowski, P. J., Villanueva, E., Navarro, E. & Godbout, J. P. Sequential activation of microglia and astrocyte cytokine expression precedes increased Iba-1 or GFAP immunoreactivity following systemic immune challenge. Glia 64 , 300–316 (2016).
Li, X. et al. Leptin increases expression of 5-HT(2B) receptors in astrocytes thus enhancing action of fluoxetine on the depressive behavior induced by sleep deprivation. Front. Psychiatry 9 , 734 (2018).
Takano, K., Yamasaki, H., Kawabe, K., Moriyama, M. & Nakamura, Y. Imipramine induces brain-derived neurotrophic factor mRNA expression in cultured astrocytes. J. Pharmacol. Sci. 120 , 176–186 (2012).
Zhang, Y. et al. BDNF enhances electrophysiological activity and excitatory synaptic transmission of RA projection neurons in adult male zebra finches. Brain Res. 1801 , 148208 (2023).
Quesseveur, G. et al. BDNF overexpression in mouse hippocampal astrocytes promotes local neurogenesis and elicits anxiolytic-like activities. Transl. Psychiatry 3 , e253 (2013).
Zor, F. et al. Effect of VEGF gene therapy and hyaluronic acid film sheath on peripheral nerve regeneration. Microsurgery 34 , 209–216 (2014).
Sun, L. et al. Propofol directly induces caspase-1-dependent macrophage pyroptosis through the NLRP3-ASC inflammasome. Cell Death Dis. 10 , 542 (2019).
Alcocer-Gomez, E. & Cordero, M. D. NLRP3 inflammasome: a new target in major depressive disorder. CNS Neurosci. Ther. 20 , 294–295 (2014).
Beckwith, K. S. et al. Plasma membrane damage causes NLRP3 activation and pyroptosis during Mycobacterium tuberculosis infection. Nat. Commun. 11 , 2270 (2020).
Xia, M. et al. The ameliorative effect of fluoxetine on neuroinflammation induced by sleep deprivation. J. Neurochem. 146 , 63–75 (2018).
Jeon, S. A. et al. NLRP3 inflammasome contributes to lipopolysaccharide-induced depressive-like behaviors via indoleamine 2,3-dioxygenase induction. Int. J. Neuropsychopharmacol. 20 , 896–906 (2017).
Wong, M. L. et al. Inflammasome signaling affects anxiety- and depressive-like behavior and gut microbiome composition. Mol. Psychiatry 21 , 797–805 (2016).
Page, C. E. & Coutellier, L. Prefrontal excitatory/inhibitory balance in stress and emotional disorders: Evidence for over-inhibition. Neurosci. Biobehav. Rev. 105 , 39–51 (2019).
Santello, M., Toni, N. & Volterra, A. Astrocyte function from information processing to cognition and cognitive impairment. Nat. Neurosci. 22 , 154–166 (2019).
Castillo-Gomez, E., Perez-Rando, M., Vidueira, S. & Nacher, J. Polysialic acid acute depletion induces structural plasticity in interneurons and impairs the excitation/inhibition balance in medial prefrontal cortex organotypic cultures. Front. Cell. Neurosci. 10 , 170 (2016).
Haydon, P. G. & Carmignoto, G. Astrocyte control of synaptic transmission and neurovascular coupling. Physiol. Rev. 86 , 1009–1031 (2006).
Huang, D. et al. Dysfunction of astrocytic connexins 30 and 43 in the medial prefrontal cortex and hippocampus mediates depressive-like behaviours. Behav. Brain Res. 372 , 111950 (2019).
Nagy, C., Torres-Platas, S. G., Mechawar, N. & Turecki, G. Repression of astrocytic connexins in cortical and subcortical brain regions and prefrontal enrichment of H3K9me3 in depression and suicide. Int J. Neuropsychopharmacol. 20 , 50–57 (2017).
PubMed Google Scholar
Murphy-Royal, C. et al. Stress gates an astrocytic energy reservoir to impair synaptic plasticity. Nat. Commun. 11 , 2014 (2020).
Ezan, P. et al. Deletion of astroglial connexins weakens the blood-brain barrier. J. Cereb. Blood Flow Metab. 32 , 1457–1467 (2012).
Torres-Platas, S. G., Nagy, C., Wakid, M., Turecki, G. & Mechawar, N. Glial fibrillary acidic protein is differentially expressed across cortical and subcortical regions in healthy brains and downregulated in the thalamus and caudate nucleus of depressed suicides. Mol. Psychiatry 21 , 509–515 (2016).
Cobb, J. A. et al. Density of GFAP-immunoreactive astrocytes is decreased in left hippocampi in major depressive disorder. Neuroscience 316 , 209–220 (2016).
Steinacker, P. et al. Glial fibrillary acidic protein as blood biomarker for differential diagnosis and severity of major depressive disorder. J. Psychiatr. Res. 144 , 54–58 (2021).
Rajkowska, G., Hughes, J., Stockmeier, C. A., Javier Miguel-Hidalgo, J. & Maciag, D. Coverage of blood vessels by astrocytic endfeet is reduced in major depressive disorder. Biol. Psychiatry 73 , 613–621 (2013).
Rajkowska, G. & Miguel-Hidalgo, J. J. Glial pathology in major depressive disorder: an approach to investigate the coverage of blood vessels by astrocyte endfeet in human postmortem brain. Methods Mol. Biol. 1938 , 247–254 (2019).
Kong, H. et al. Aquaporin-4 knockout exacerbates corticosterone-induced depression by inhibiting astrocyte function and hippocampal neurogenesis. CNS Neurosci. Ther. 20 , 391–402 (2014).
Xia, M., Yang, L., Sun, G., Qi, S. & Li, B. Mechanism of depression as a risk factor in the development of Alzheimer’s disease: the function of AQP4 and the glymphatic system. Psychopharmacology 234 , 365–379 (2017).
Di Benedetto, B. et al. Fluoxetine requires the endfeet protein aquaporin-4 to enhance plasticity of astrocyte processes. Front. Cell. Neurosci. 10 , 8 (2016).
Du, J. et al. S100B is selectively expressed by gray matter protoplasmic astrocytes and myelinating oligodendrocytes in the developing CNS. Mol. Brain 14 , 154 (2021).
Schroeter, M. L., Abdul-Khaliq, H., Krebs, M., Diefenbacher, A. & Blasig, I. E. Serum markers support disease-specific glial pathology in major depression. J. Affect Disord. 111 , 271–280 (2008).
Michel, M. et al. Increased GFAP concentrations in the cerebrospinal fluid of patients with unipolar depression. Transl. Psychiatry 11 , 308 (2021).
Gos, T. et al. S100B-immunopositive astrocytes and oligodendrocytes in the hippocampus are differentially afflicted in unipolar and bipolar depression: a postmortem study. J. Psychiatr. Res. 47 , 1694–1699 (2013).
Michetti, F. et al. The S100B protein in biological fluids: more than a lifelong biomarker of brain distress. J. Neurochem. 120 , 644–659 (2012).
Zhang, L. et al. Changes in glial gene expression in the prefrontal cortex in relation to major depressive disorder, suicide and psychotic features. J. Affect Disord. 295 , 893–903 (2021).
Gules, E., Iosifescu, D. V. & Tural, U. Plasma neuronal and glial markers and anterior cingulate metabolite levels in major depressive disorder: a pilot study. Neuropsychobiology 79 , 214–221 (2020).
Chamera, K., Szuster-Gluszczak, M., Trojan, E. & Basta-Kaim, A. Maternal Immune Activation Sensitizes Male Offspring Rats to Lipopolysaccharide-Induced Microglial Deficits Involving the Dysfunction of CD200-CD200R and CX3CL1-CX3CR1 systems. Cells 9 , 1676 (2020).
Jiang, X. et al. Asperosaponin VI ameliorates the CMS-induced depressive-like behaviors by inducing a neuroprotective microglial phenotype in hippocampus via PPAR-gamma pathway. J. Neuroinflammation 19 , 115 (2022).
Tang, M. M., Lin, W. J., Pan, Y. Q. & Li, Y. C. Fibroblast growth factor 2 modulates hippocampal microglia activation in a neuroinflammation induced model of depression. Front. Cell. Neurosci. 12 , 255 (2018).
Zhan, Y. et al. Deficient neuron-microglia signaling results in impaired functional brain connectivity and social behavior. Nat. Neurosci. 17 , 400–406 (2014).
Hellwig, S. et al. Altered microglia morphology and higher resilience to stress-induced depression-like behavior in CX3CR1-deficient mice. Brain Behav. Immun. 55 , 126–137 (2016).
Merendino, R. A. et al. Involvement of fractalkine and macrophage inflammatory protein-1 alpha in moderate-severe depression. Mediat. Inflamm. 13 , 205–207 (2004).
Garcia-Marchena, N. et al. Inflammatory mediators and dual depression: Potential biomarkers in plasma of primary and substance-induced major depression in cocaine and alcohol use disorders. PLoS ONE 14 , e0213791 (2019).
Wang, H. T. et al. Early-Life Social Isolation-Induced Depressive-Like Behavior in Rats Results in Microglial Activation and Neuronal Histone Methylation that Are Mitigated by Minocycline. Neurotox. Res 31 , 505–520 (2017).
Frank, M. G., Fonken, L. K., Annis, J. L., Watkins, L. R. & Maier, S. F. Stress disinhibits microglia via down-regulation of CD200R: A mechanism of neuroinflammatory priming. Brain Behav. Immun. 69 , 62–73 (2018).
Fonken, L. K. et al. Neuroinflammatory priming to stress is differentially regulated in male and female rats. Brain Behav. Immun. 70 , 257–267 (2018).
Popov, A. et al. Astrocyte dystrophy in ageing brain parallels impaired synaptic plasticity. Aging Cell 20 , e13334 (2021).
Zhang, Y. et al. Structural basis of ketamine action on human NMDA receptors. Nature 596 , 301–305 (2021).
Wang, Q., Jie, W., Liu, J. H., Yang, J. M. & Gao, T. M. An astroglial basis of major depressive disorder? An overview. Glia 65 , 1227–1250 (2017).
Jiang, X., Lin, W., Cheng, Y. & Wang, D. mGluR5 facilitates long-term synaptic depression in a stress-induced depressive mouse model. Can. J. Psychiatry 65 , 347–355 (2020).
Guo, W. et al. Iptakalim alleviates synaptic damages via targeting mitochondrial ATP-sensitive potassium channel in depression. FASEB J. 35 , e21581 (2021).
Curro, D., Navarra, P., Samengo, I. & Martire, M. P2X7 receptors exert a permissive effect on the activation of presynaptic AMPA receptors in rat trigeminal caudal nucleus glutamatergic nerve terminals. J. Headache Pain 21 , 83 (2020).
Iwata, M. et al. Psychological stress activates the inflammasome via release of adenosine triphosphate and stimulation of the purinergic type 2X7 receptor. Biol. Psychiatry 80 , 12–22 (2016).
He, Y., Taylor, N., Fourgeaud, L. & Bhattacharya, A. The role of microglial P2X7: modulation of cell death and cytokine release. J. Neuroinflammation 14 , 135 (2017).
Ota, K. T. et al. REDD1 is essential for stress-induced synaptic loss and depressive behavior. Nat. Med 20 , 531–535 (2014).
Kang, H. J. et al. Decreased expression of synapse-related genes and loss of synapses in major depressive disorder. Nat. Med 18 , 1413–1417 (2012).
Tomassoni-Ardori, F. et al. Rbfox1 up-regulation impairs BDNF-dependent hippocampal LTP by dysregulating TrkB isoform expression levels. Elife 8 , e49673 (2019).
Wang, G. et al. Antidepressant-like effect of ginsenoside Rb1 on potentiating synaptic plasticity via the miR-134-mediated BDNF signaling pathway in a mouse model of chronic stress-induced depression. J. Ginseng Res. 46 , 376–386 (2022).
Lalo, U., Koh, W., Lee, C. J. & Pankratov, Y. The tripartite glutamatergic synapse. Neuropharmacology 199 , 108758 (2021).
Shepard, R., Page, C. E. & Coutellier, L. Sensitivity of the prefrontal GABAergic system to chronic stress in male and female mice: Relevance for sex differences in stress-related disorders. Neuroscience 332 , 1–12 (2016).
Shepard, R. & Coutellier, L. Changes in the prefrontal glutamatergic and parvalbumin systems of mice exposed to unpredictable chronic stress. Mol. Neurobiol. 55 , 2591–2602 (2018).
Bouamrane, L. et al. Reelin-haploinsufficiency disrupts the developmental trajectory of the E/I Balance in the Prefrontal Cortex. Front. Cell. Neurosci. 10 , 308 (2016).
Arnone, D., Mumuni, A. N., Jauhar, S., Condon, B. & Cavanagh, J. Indirect evidence of selective glial involvement in glutamate-based mechanisms of mood regulation in depression: meta-analysis of absolute prefrontal neuro-metabolic concentrations. Eur. Neuropsychopharmacol. 25 , 1109–1117 (2015).
Hu, Y. T., Tan, Z. L., Hirjak, D. & Northoff, G. Brain-wide changes in excitation-inhibition balance of major depressive disorder: a systematic review of topographic patterns of GABA- and glutamatergic alterations. Mol. Psychiatry 28 , 3257–3266 (2023).
Zhao, J. et al. Prefrontal alterations in GABAergic and glutamatergic gene expression in relation to depression and suicide. J. Psychiatr. Res. 102 , 261–274 (2018).
Douillard-Guilloux, G., Lewis, D., Seney, M. L. & Sibille, E. Decrease in somatostatin-positive cell density in the amygdala of females with major depression. Depress Anxiety 34 , 68–78 (2017).
Scifo, E. et al. Sustained molecular pathology across episodes and remission in major depressive disorder. Biol. Psychiatry 83 , 81–89 (2018).
Oh, D. H., Son, H., Hwang, S. & Kim, S. H. Neuropathological abnormalities of astrocytes, GABAergic neurons, and pyramidal neurons in the dorsolateral prefrontal cortices of patients with major depressive disorder. Eur. Neuropsychopharmacol. 22 , 330–338 (2012).
Sibille, E., Morris, H. M., Kota, R. S. & Lewis, D. A. GABA-related transcripts in the dorsolateral prefrontal cortex in mood disorders. Int J. Neuropsychopharmacol. 14 , 721–734 (2011).
Barros-Barbosa, A. R., Lobo, M. G., Ferreirinha, F., Correia-de-Sa, P. & Cordeiro, J. M. P2X7 receptor activation downmodulates Na(+)-dependent high-affinity GABA and glutamate transport into rat brain cortex synaptosomes. Neuroscience 306 , 74–90 (2015).
Barros-Barbosa, A. R. et al. Up-regulation of P2X7 receptor-mediated inhibition of GABA uptake by nerve terminals of the human epileptic neocortex. Epilepsia 57 , 99–110 (2016).
Liu, Y. P., Yang, C. S., Chen, M. C., Sun, S. H. & Tzeng, S. F. Ca(2+)-dependent reduction of glutamate aspartate transporter GLAST expression in astrocytes by P2X(7) receptor-mediated phosphoinositide 3-kinase signaling. J. Neurochem. 113 , 213–227 (2010).
Macaulay, N. & Zeuthen, T. Glial K(+) clearance and cell swelling: key roles for cotransporters and pumps. Neurochem. Res. 37 , 2299–2309 (2012).
Larsen, B. R. et al. Contributions of the Na(+)/K(+)-ATPase, NKCC1, and Kir4.1 to hippocampal K(+) clearance and volume responses. Glia 62 , 608–622 (2014).
Verkhratsky, A. & Nedergaard, M. Astroglial cradle in the life of the synapse. Philos. Trans. R. Soc. Lond. B Biol. Sci. 369 , 20130595 (2014).
Aramideh, J. A., Vidal-Itriago, A., Morsch, M. & Graeber, M. B. Cytokine signalling at the microglial penta-partite synapse. Int J. Mol. Sci. 22 , 13186 (2021).
Chung, W. S. et al. Astrocytes mediate synapse elimination through MEGF10 and MERTK pathways. Nature 504 , 394–400 (2013).
Yang, J. et al. Astrocytes contribute to synapse elimination via type 2 inositol 1,4,5-trisphosphate receptor-dependent release of ATP. Elife 5 , e15043 (2016).
Petrache, A. L. et al. Aberrant excitatory-inhibitory synaptic mechanisms in entorhinal cortex microcircuits during the pathogenesis of Alzheimer’s disease. Cereb. Cortex 29 , 1834–1850 (2019).
Arioz, B. I. et al. Melatonin attenuates LPS-Induced acute depressive-like behaviors and microglial NLRP3 inflammasome activation through the SIRT1/Nrf2 pathway. Front. Immunol. 10 , 1511 (2019).
Bikbaev, A., Frischknecht, R. & Heine, M. Brain extracellular matrix retains connectivity in neuronal networks. Sci. Rep. 5 , 14527 (2015).
Strackeljan, L. et al. Microglia depletion-induced remodeling of extracellular matrix and excitatory synapses in the hippocampus of adult mice. Cells 10 , 1862 (2021).
Leclercq, S., De Saeger, C., Delzenne, N., de Timary, P. & Starkel, P. Role of inflammatory pathways, blood mononuclear cells, and gut-derived bacterial products in alcohol dependence. Biol. Psychiatry 76 , 725–733 (2014).
Hsu, J. H., Chien, I. C. & Lin, C. H. Increased risk of chronic liver disease in patients with major depressive disorder: a population-based study. J. Affect Disord. 251 , 180–185 (2019).
Chen, D., Zhang, Y., Huang, T. & Jia, J. Depression and risk of gastrointestinal disorders: a comprehensive two-sample Mendelian randomization study of European ancestry. Psychol. Med . 53 , 7309–7321 (2023).
Facanali, C. B. G. et al. The relationship of major depressive disorder with Crohn’s disease activity. Clinics (Sao Paulo) 78 , 100188 (2023).
Ronaldson, P. T. & Davis, T. P. Regulation of blood-brain barrier integrity by microglia in health and disease: A therapeutic opportunity. J. Cereb. Blood Flow. Metab. 40 , S6–S24 (2020).
Qing, H. et al. Origin and Function of Stress-Induced IL-6 in Murine Models. Cell 182 , 1660 (2020).
Labad, J. et al. Hypothalamic-pituitary-adrenal axis function and exposure to stress factors and cannabis use in recent-onset psychosis. World J. Biol. Psychiatry 21 , 564–571 (2020).
Frank, M. G., Miguel, Z. D., Watkins, L. R. & Maier, S. F. Prior exposure to glucocorticoids sensitizes the neuroinflammatory and peripheral inflammatory responses to E. coli lipopolysaccharide. Brain Behav. Immun. 24 , 19–30 (2010).
Deng, Y. et al. Involvement of the microbiota-gut-brain axis in chronic restraint stress: disturbances of the kynurenine metabolic pathway in both the gut and brain. Gut Microbes 13 , 1–16 (2021).
Munn, D. H. & Mellor, A. L. Indoleamine 2,3 dioxygenase and metabolic control of immune responses. Trends Immunol. 34 , 137–143 (2013).
Gos, T. et al. Reduced microglial immunoreactivity for endogenous NMDA receptor agonist quinolinic acid in the hippocampus of schizophrenia patients. Brain Behav. Immun. 41 , 59–64 (2014).
Li, M. et al. Transcriptome profiles of corticosterone-induced cytotoxicity reveals the involvement of neurite growth-related genes in depression. Psychiatry Res. 276 , 79–86 (2019).
Dutheil, S., Ota, K. T., Wohleb, E. S., Rasmussen, K. & Duman, R. S. High-fat diet induced anxiety and anhedonia: impact on brain homeostasis and inflammation. Neuropsychopharmacology 41 , 1874–1887 (2016).
Skonieczna-Zydecka, K. et al. Faecal short chain fatty acids profile is changed in polish depressive women. Nutrients 10 , 1939 (2018).
Sampson, T. R. et al. Gut microbiota regulate motor deficits and neuroinflammation in a model of Parkinson’s disease. Cell 167 , 1469–1480.e1412 (2016).
Fan, L. et al. Total glycosides from stems of Cistanche tubulosa alleviate depression-like behaviors: bidirectional interaction of the phytochemicals and gut microbiota. Phytomedicine 83 , 153471 (2021).
Zhang, J. C. et al. Blockade of interleukin-6 receptor in the periphery promotes rapid and sustained antidepressant actions: a possible role of gut-microbiota-brain axis. Transl. Psychiatry 7 , e1138 (2017).
Pan, Y., Chen, X. Y., Zhang, Q. Y. & Kong, L. D. Microglial NLRP3 inflammasome activation mediates IL-1beta-related inflammation in prefrontal cortex of depressive rats. Brain Behav. Immun. 41 , 90–100 (2014).
Woodburn, S. C., Bollinger, J. L. & Wohleb, E. S. Synaptic and behavioral effects of chronic stress are linked to dynamic and sex-specific changes in microglia function and astrocyte dystrophy. Neurobiol. Stress 14 , 100312 (2021).
Zhang, K., Liu, R., Gao, Y., Ma, W. & Shen, W. Electroacupuncture relieves LPS-induced depression-like behaviour in rats through IDO-Mediated tryptophan-degrading pathway. Neuropsychiatr. Dis. Treat. 16 , 2257–2266 (2020).
Parrott, J. M., Redus, L. & O’Connor, J. C. Kynurenine metabolic balance is disrupted in the hippocampus following peripheral lipopolysaccharide challenge. J. Neuroinflammation 13 , 124 (2016).
Alzarea, S., Abbas, M., Ronan, P. J., Lutfy, K. & Rahman, S. The Effect of an alpha-7 nicotinic allosteric modulator PNU120596 and NMDA receptor antagonist memantine on depressive-like behavior induced by lps in mice: the involvement of brain microglia. Brain Sci. 12 , 1493 (2022).
Le Strat, Y., Le Foll, B. & Dubertret, C. Major depression and suicide attempts in patients with liver disease in the United States. Liver Int. 35 , 1910–1916 (2015).
Buganza-Torio, E. et al. Depression in cirrhosis - a prospective evaluation of the prevalence, predictors and development of a screening nomogram. Aliment. Pharmacol. Ther. 49 , 194–201 (2019).
Qin, X. H. et al. Liver soluble epoxide hydrolase regulates behavioral and cellular effects of chronic stress. Cell Rep. 29 , 3223–3234.e3226 (2019).
Pang, F. et al. Electroacupuncture alleviates depressive-like behavior by modulating the expression of P2X7/NLRP3/IL-1beta of prefrontal cortex and liver in rats exposed to chronic unpredictable mild stress. Brain Sci. 13 , 436 (2023).
Zhang, Y. et al. Effects of hydrogen-rich water on depressive-like behavior in mice. Sci. Rep. 6 , 23742 (2016).
Brown, S. J. et al. Sex- and suicide-specific alterations in the kynurenine pathway in the anterior cingulate cortex in major depression. Neuropsychopharmacology (2023). Online ahead of print.
Guillemin, G. J. et al. Characterisation of kynurenine pathway metabolism in human astrocytes and implications in neuropathogenesis. Redox Rep. 5 , 108–111 (2000).
Park, H. J., Kim, S. A., Kang, W. S. & Kim, J. W. Early-life stress modulates gut microbiota and peripheral and central inflammation in a sex-dependent manner. Int J. Mol. Sci. 22 , 1899 (2021).
Ninan, J. & Feldman, L. Ammonia levels and hepatic encephalopathy in patients with known chronic liver disease. J. Hosp. Med. 12 , 659–661 (2017).
Kautzky, A. et al. The influence of the rs6295 gene polymorphism on serotonin-1A receptor distribution investigated with PET in patients with major depression applying machine learning. Transl. Psychiatry 7 , e1150 (2017).
Das, R. et al. Higher levels of serum IL-1beta and TNF-alpha are associated with an increased probability of major depressive disorder. Psychiatry Res. 295 , 113568 (2021).
Lu, Z. et al. Oxidative stress and psychiatric disorders: evidence from the bidirectional mendelian randomization study. Antioxidants (Basel) 11 , 1386 (2022).
Hursitoglu, O. et al. Serum NOX1 and Raftlin as new potential biomarkers of Major Depressive Disorder: a study in treatment-naive first episode patients. Prog. Neuropsychopharmacol. Biol. Psychiatry 121 , 110670 (2023).
Han, K. M. et al. Serum FAM19A5 levels: A novel biomarker for neuroinflammation and neurodegeneration in major depressive disorder. Brain Behav. Immun. 87 , 852–859 (2020).
Winter, N. R. et al. Quantifying deviations of brain structure and function in major depressive disorder across neuroimaging modalities. JAMA Psychiatry 79 , 879–888 (2022).
Zhao, Y. et al. Gray matter abnormalities in non-comorbid medication-naive patients with major depressive disorder or social anxiety disorder. EBioMedicine 21 , 228–235 (2017).
Wise, T. et al. Common and distinct patterns of grey-matter volume alteration in major depression and bipolar disorder: evidence from voxel-based meta-analysis. Mol. Psychiatry 22 , 1455–1463 (2017).
Liu, Y. et al. Abnormal brain gray matter volume in patients with major depressive disorder: Associated with childhood trauma? J. Affect Disord. 308 , 562–568 (2022).
Kaiser, R. H., Andrews-Hanna, J. R., Wager, T. D. & Pizzagalli, D. A. Large-scale network dysfunction in major depressive disorder: a meta-analysis of resting-state functional connectivity. JAMA Psychiatry 72 , 603–611 (2015).
Wang, Y. et al. Topologically convergent and divergent functional connectivity patterns in unmedicated unipolar depression and bipolar disorder. Transl. Psychiatry 7 , e1165 (2017).
Kremneva, E. I., Sinitsyn, D. O., Dobrynina, L. A., Suslina, A. D. & Krotenkova, M. V. [Resting state functional MRI in neurology and psychiatry]. Zh. Nevrol. Psikhiatr Im. S S Korsakova 122 , 5–14 (2022).
Luo, Z. et al. Shared and specific dynamics of brain segregation and integration in bipolar disorder and major depressive disorder: A resting-state functional magnetic resonance imaging study. J. Affect. Disord. 280 , 279–286 (2021).
Drysdale, A. T. et al. Resting-state connectivity biomarkers define neurophysiological subtypes of depression. Nat. Med. 23 , 28–38 (2017).
Chen, Q. et al. Regional amplitude abnormities in the major depressive disorder: A resting-state fMRI study and support vector machine analysis. J. Affect. Disord. 308 , 1–9 (2022).
Yan, C. G. et al. Reduced default mode network functional connectivity in patients with recurrent major depressive disorder. Proc. Natl Acad. Sci. USA 116 , 9078–9083 (2019).
Pizzagalli, D. A. & Roberts, A. C. Prefrontal cortex and depression. Neuropsychopharmacology 47 , 225–246 (2022).
Muller, V. I. et al. Altered brain activity in unipolar depression revisited: meta-analyses of neuroimaging studies. JAMA Psychiatry 74 , 47–55 (2017).
Sun, K. et al. A two-center radiomic analysis for differentiating major depressive disorder using multi-modality MRI data under different parcellation methods. J. Affect. Disord. 300 , 1–9 (2022).
Mayerhoefer, M. E. et al. Introduction to radiomics. J. Nucl. Med. 61 , 488–495 (2020).
Xu, Z. et al. Combined HTR1A/1B methylation and human functional connectome to recognize patients with MDD. Psychiatry Res. 317 , 114842 (2022).
Verduijn, J. et al. Reconsidering the prognosis of major depressive disorder across diagnostic boundaries: full recovery is the exception rather than the rule. BMC Med. 15 , 215 (2017).
Blumenthal, J. A. & Rozanski, A. Exercise as a therapeutic modality for the prevention and treatment of depression. Prog. Cardiovasc. Dis. 77 , 50–58 (2023).
Baglioni, C., Spiegelhalder, K., Nissen, C. & Riemann, D. Clinical implications of the causal relationship between insomnia and depression: how individually tailored treatment of sleeping difficulties could prevent the onset of depression. EPMA J. 2 , 287–293 (2011).
Riemann, D. et al. European guideline for the diagnosis and treatment of insomnia. J. Sleep. Res. 26 , 675–700 (2017).
Soh, H. L., Ho, R. C., Ho, C. S. & Tam, W. W. Efficacy of digital cognitive behavioural therapy for insomnia: a meta-analysis of randomised controlled trials. Sleep. Med. 75 , 315–325 (2020).
Ho, F. Y., Chan, C. S., Lo, W. Y. & Leung, J. C. The effect of self-help cognitive behavioral therapy for insomnia on depressive symptoms: an updated meta-analysis of randomized controlled trials. J. Affect. Disord. 265 , 287–304 (2020).
Qaseem, A. et al. Management of chronic insomnia disorder in adults: a clinical practice guideline from the american college of physicians. Ann. Intern. Med. 165 , 125–133 (2016).
Irwin, M. R. et al. Prevention of incident and recurrent major depression in older adults with insomnia: a randomized clinical trial. JAMA Psychiatry 79 , 33–41 (2022).
Scheer, F. A., Pirovano, C., Van Someren, E. J. & Buijs, R. M. Environmental light and suprachiasmatic nucleus interact in the regulation of body temperature. Neuroscience 132 , 465–477 (2005).
Dekker, K. et al. Combined internet-based cognitive-behavioral and chronobiological intervention for insomnia: a randomized controlled trial. Psychother. Psychosom. 89 , 117–118 (2020).
Leerssen, J. et al. Treating insomnia with high risk of depression using therapist-guided digital cognitive, behavioral, and circadian rhythm support interventions to prevent worsening of depressive symptoms: a randomized controlled trial. Psychother. Psychosom. 91 , 168–179 (2022).
Zhai, L., Zhang, H. & Zhang, D. Sleep duration and depression among adults: a meta-analysis of prospective studies. Depress. Anxiety 32 , 664–670 (2015).
Baglioni, C. et al. Insomnia as a predictor of depression: a meta-analytic evaluation of longitudinal epidemiological studies. J. Affect. Disord. 135 , 10–19 (2011).
Utge, S. J. et al. Systematic analysis of circadian genes in a population-based sample reveals association of TIMELESS with depression and sleep disturbance. PLoS ONE 5 , e9259 (2010).
Irwin, M. R. Sleep and inflammation: partners in sickness and in health. Nat. Rev. Immunol. 19 , 702–715 (2019).
Hill Almeida, L. M. et al. Disrupted sleep and risk of depression in later life: A prospective cohort study with extended follow up and a systematic review and meta-analysis. J. Affect. Disord. 309 , 314–323 (2022).
Tolkien, K., Bradburn, S. & Murgatroyd, C. An anti-inflammatory diet as a potential intervention for depressive disorders: A systematic review and meta-analysis. Clin. Nutr. 38 , 2045–2052 (2019).
Galland, L. Diet and inflammation. Nutr. Clin. Pr. 25 , 634–640 (2010).
Oddy, W. H. et al. Dietary patterns, body mass index and inflammation: Pathways to depression and mental health problems in adolescents. Brain Behav. Immun. 69 , 428–439 (2018).
Bosma-den Boer, M. M., van Wetten, M. L. & Pruimboom, L. Chronic inflammatory diseases are stimulated by current lifestyle: how diet, stress levels and medication prevent our body from recovering. Nutr. Metab. (Lond.) 9 , 32 (2012).
Sanchez-Villegas, A. et al. The effect of the Mediterranean diet on plasma brain-derived neurotrophic factor (BDNF) levels: the PREDIMED-NAVARRA randomized trial. Nutr. Neurosci. 14 , 195–201 (2011).
Jiang, C. & Salton, S. R. The role of neurotrophins in major depressive disorder. Transl. Neurosci. 4 , 46–58 (2013).
Ogbonnaya, E. S. et al. Adult hippocampal neurogenesis is regulated by the microbiome. Biol. Psychiatry 78 , e7–9 (2015).
Zheng, P. et al. Gut microbiome remodeling induces depressive-like behaviors through a pathway mediated by the host’s metabolism. Mol. Psychiatry 21 , 786–796 (2016).
Jiang, H. et al. Altered fecal microbiota composition in patients with major depressive disorder. Brain Behav. Immun. 48 , 186–194 (2015).
Burokas, A. et al. Targeting the microbiota-gut-brain axis: prebiotics have anxiolytic and antidepressant-like effects and reverse the impact of chronic stress in mice. Biol. Psychiatry 82 , 472–487 (2017).
Bonder, M. J. et al. The influence of a short-term gluten-free diet on the human gut microbiome. Genome Med. 8 , 45 (2016).
Mohan, M. et al. Dietary gluten-induced gut dysbiosis is accompanied by selective upregulation of microRNAs with intestinal tight junction and bacteria-binding motifs in rhesus macaque model of celiac disease. Nutrients 8 , 684 (2016).
Karakula-Juchnowicz, H. et al. The study evaluating the effect of probiotic supplementation on the mental status, inflammation, and intestinal barrier in major depressive disorder patients using gluten-free or gluten-containing diet (SANGUT study): a 12-week, randomized, double-blind, and placebo-controlled clinical study protocol. Nutr. J. 18 , 50 (2019).
Khosravi, M. et al. The relationship between dietary patterns and depression mediated by serum levels of Folate and vitamin B12. BMC Psychiatry 20 , 63 (2020).
Schuch, F. B. et al. Exercise as a treatment for depression: a meta-analysis adjusting for publication bias. J. Psychiatr. Res. 77 , 42–51 (2016).
Morland, C. et al. Exercise induces cerebral VEGF and angiogenesis via the lactate receptor HCAR1. Nat. Commun. 8 , 15557 (2017).
Coelho, F. G. et al. Physical exercise modulates peripheral levels of brain-derived neurotrophic factor (BDNF): a systematic review of experimental studies in the elderly. Arch. Gerontol. Geriatr. 56 , 10–15 (2013).
Stimpson, N. J., Davison, G. & Javadi, A. H. Joggin’ the noggin: towards a physiological understanding of exercise-induced cognitive benefits. Neurosci. Biobehav Rev. 88 , 177–186 (2018).
De Rossi, P. et al. A critical role for VEGF and VEGFR2 in NMDA receptor synaptic function and fear-related behavior. Mol. Psychiatry 21 , 1768–1780 (2016).
Bugg, J. M. & Head, D. Exercise moderates age-related atrophy of the medial temporal lobe. Neurobiol. Aging 32 , 506–514 (2011).
Cole, R. C. et al. Cardiorespiratory fitness and hippocampal volume predict faster episodic associative learning in older adults. Hippocampus 30 , 143–155 (2020).
Zotcheva, E. et al. Associations of changes in cardiorespiratory fitness and symptoms of anxiety and depression with brain volumes: The HUNT Study. Front Behav. Neurosci. 13 , 53 (2019).
Dowlati, Y. et al. A meta-analysis of cytokines in major depression. Biol. Psychiatry 67 , 446–457 (2010).
Valkanova, V., Ebmeier, K. P. & Allan, C. L. CRP, IL-6 and depression: a systematic review and meta-analysis of longitudinal studies. J. Affect Disord. 150 , 736–744 (2013).
Kohler, C. A. et al. Peripheral cytokine and chemokine alterations in depression: a meta-analysis of 82 studies. Acta Psychiatr. Scand. 135 , 373–387 (2017).
Choi, K. W. et al. Assessment of bidirectional relationships between physical activity and depression among adults: a 2-sample mendelian randomization study. JAMA Psychiatry 76 , 399–408 (2019).
Schuch, F. B. et al. Physical activity and incident depression: a meta-analysis of prospective cohort studies. Am. J. Psychiatry 175 , 631–648 (2018).
Choi, K. W. et al. Physical activity offsets genetic risk for incident depression assessed via electronic health records in a biobank cohort study. Depress Anxiety 37 , 106–114 (2020).
Imboden, C. et al. Aerobic exercise or stretching as add-on to inpatient treatment of depression: Similar antidepressant effects on depressive symptoms and larger effects on working memory for aerobic exercise alone. J. Affect Disord. 276 , 866–876 (2020).
Vancampfort, D. et al. Sedentary behavior and physical activity levels in people with schizophrenia, bipolar disorder and major depressive disorder: a global systematic review and meta-analysis. World Psychiatry 16 , 308–315 (2017).
Brush, C. J. et al. A randomized trial of aerobic exercise for major depression: examining neural indicators of reward and cognitive control as predictors and treatment targets. Psychol. Med. 52 , 893–903 (2022).
Kujawa, A. et al. Reduced reward responsiveness predicts change in depressive symptoms in anxious children and adolescents following treatment. J. Child Adolesc. Psychopharmacol. 29 , 378–385 (2019).
Kandola, A., Ashdown-Franks, G., Hendrikse, J., Sabiston, C. M. & Stubbs, B. Physical activity and depression: towards understanding the antidepressant mechanisms of physical activity. Neurosci. Biobehav Rev. 107 , 525–539 (2019).
Yildirim, Y. & Kocabiyik, S. The relationship between social support and loneliness in Turkish patients with cancer. J. Clin. Nurs. 19 , 832–839 (2010).
Lin, J. et al. Perceived stressfulness mediates the effects of subjective social support and negative coping style on suicide risk in Chinese patients with major depressive disorder. J. Affect. Disord. 265 , 32–38 (2020).
Smith, L., Hill, N. & Kokanovic, R. Experiences of depression, the role of social support and its impact on health outcomes. J. Ment. Health 24 , 342–346 (2015).
Wang, X., Cai, L., Qian, J. & Peng, J. Social support moderates stress effects on depression. Int. J. Ment. Health Syst. 8 , 41 (2014).
Hybels, C. F., Pieper, C. F., Blazer, D. G. & Steffens, D. C. Heterogeneity in the three-year course of major depression among older adults. Int. J. Geriatr. Psychiatry 31 , 775–782 (2016).
Backs-Dermott, B. J., Dobson, K. S. & Jones, S. L. An evaluation of an integrated model of relapse in depression. J. Affect. Disord. 124 , 60–67 (2010).
Holma, I. A., Holma, K. M., Melartin, T. K., Rytsala, H. J. & Isometsa, E. T. A 5-year prospective study of predictors for disability pension among patients with major depressive disorder. Acta Psychiatr. Scand. 125 , 325–334 (2012).
Stewart, R. A., Patel, T. A., McDermott, K. A. & Cougle, J. R. Functional and structural social support in DSM-5 mood and anxiety disorders: a population-based study. J. Affect Disord. 308 , 528–534 (2022).
Ouakinin, S. R. S., Barreira, D. P. & Gois, C. J. Depression and obesity: integrating the role of stress, neuroendocrine dysfunction and inflammatory pathways. Front. Endocrinol. (Lausanne) 9 , 431 (2018).
Hallgren, M., Lundin, A., Tee, F. Y., Burstrom, B. & Forsell, Y. Somebody to lean on: Social relationships predict post-treatment depression severity in adults. Psychiatry Res. 249 , 261–267 (2017).
van Beljouw, I. M., Verhaak, P. F., Cuijpers, P., van Marwijk, H. W. & Penninx, B. W. The course of untreated anxiety and depression, and determinants of poor one-year outcome: a one-year cohort study. BMC Psychiatry 10 , 86 (2010).
Dour, H. J. et al. Perceived social support mediates anxiety and depressive symptom changes following primary care intervention. Depress Anxiety 31 , 436–442 (2014).
Teo, A. R., Choi, H. & Valenstein, M. Social relationships and depression: ten-year follow-up from a nationally representative study. PLoS ONE 8 , e62396 (2013).
Griffiths, K. M., Crisp, D. A., Barney, L. & Reid, R. Seeking help for depression from family and friends: a qualitative analysis of perceived advantages and disadvantages. BMC Psychiatry 11 , 196 (2011).
Hillhouse, T. M. & Porter, J. H. A brief history of the development of antidepressant drugs: from monoamines to glutamate. Exp. Clin. Psychopharmacol. 23 , 1–21 (2015).
Sulser, F., Vetulani, J. & Mobley, P. L. Mode of action of antidepressant drugs. Biochem. Pharmacol. 27 , 257–261 (1978).
Gillman, P. K. Tricyclic antidepressant pharmacology and therapeutic drug interactions updated. Br. J. Pharmacol. 151 , 737–748 (2007).
Taylor, C., Fricker, A. D., Devi, L. A. & Gomes, I. Mechanisms of action of antidepressants: from neurotransmitter systems to signaling pathways. Cell Signal. 17 , 549–557 (2005).
Jann, M. W. & Slade, J. H. Antidepressant agents for the treatment of chronic pain and depression. Pharmacotherapy 27 , 1571–1587 (2007).
Shultz, E. & Malone, D. A. Jr A practical approach to prescribing antidepressants. Cleve Clin. J. Med. 80 , 625–631 (2013).
Croom, K. F., Perry, C. M. & Plosker, G. L. Mirtazapine: a review of its use in major depression and other psychiatric disorders. CNS Drugs 23 , 427–452 (2009).
Benjamin, S. & Doraiswamy, P. M. Review of the use of mirtazapine in the treatment of depression. Expert Opin. Pharmacother. 12 , 1623–1632 (2011).
Cleare, A. et al. Evidence-based guidelines for treating depressive disorders with antidepressants: a revision of the 2008 British Association for Psychopharmacology guidelines. J. Psychopharmacol. 29 , 459–525 (2015).
Guloglu, C., Orak, M., Ustundag, M. & Altunci, Y. A. Analysis of amitriptyline overdose in emergency medicine. Emerg. Med. J. 28 , 296–299 (2011).
David, D. J. & Gourion, D. [Antidepressant and tolerance: determinants and management of major side effects]. Encephale 42 , 553–561 (2016).
Richelson, E. Antimuscarinic and other receptor-blocking properties of antidepressants. Mayo Clin. Proc. 58 , 40–46 (1983).
Hisaoka, K. et al. Tricyclic antidepressant amitriptyline activates fibroblast growth factor receptor signaling in glial cells: involvement in glial cell line-derived neurotrophic factor production. J. Biol. Chem. 286 , 21118–21128 (2011).
Morioka, N. et al. Amitriptyline up-regulates connexin43-gap junction in rat cultured cortical astrocytes via activation of the p38 and c-Fos/AP-1 signalling pathway. Br. J. Pharmacol. 171 , 2854–2867 (2014).
Budzinski, M. L. et al. Tricyclic antidepressants target FKBP51 SUMOylation to restore glucocorticoid receptor activity. Mol. Psychiatry 27 , 2533–2545 (2022).
Malison, R. T. et al. Reduced brain serotonin transporter availability in major depression as measured by [123I]-2 beta-carbomethoxy-3 beta-(4-iodophenyl)tropane and single photon emission computed tomography. Biol. Psychiatry 44 , 1090–1098 (1998).
Samuels, B. A. et al. 5-HT1A receptors on mature dentate gyrus granule cells are critical for the antidepressant response. Nat. Neurosci. 18 , 1606–1616 (2015).
Scorza, M. C. et al. Preclinical and clinical characterization of the selective 5-HT(1A) receptor antagonist DU-125530 for antidepressant treatment. Br. J. Pharmacol. 167 , 1021–1034 (2012).
Cremers, T. I. et al. Inactivation of 5-HT(2C) receptors potentiates consequences of serotonin reuptake blockade. Neuropsychopharmacology 29 , 1782–1789 (2004).
Boothman, L. J., Mitchell, S. N. & Sharp, T. Investigation of the SSRI augmentation properties of 5-HT(2) receptor antagonists using in vivo microdialysis. Neuropharmacology 50 , 726–732 (2006).
Haddjeri, N., de Montigny, C. & Blier, P. Modulation of the firing activity of noradrenergic neurones in the rat locus coeruleus by the 5-hydroxtryptamine system. Br. J. Pharmacol. 120 , 865–875 (1997).
Szabo, S. T., de Montigny, C. & Blier, P. Modulation of noradrenergic neuronal firing by selective serotonin reuptake blockers. Br. J. Pharmacol. 126 , 568–571 (1999).
Jang, S. W. et al. Amitriptyline is a TrkA and TrkB receptor agonist that promotes TrkA/TrkB heterodimerization and has potent neurotrophic activity. Chem. Biol. 16 , 644–656 (2009).
Casarotto, P. C. et al. Antidepressant drugs act by directly binding to TRKB neurotrophin receptors. Cell 184 , 1299–1313.e1219 (2021).
Li, B. et al. Down-regulation of GluK2 kainate receptor expression by chronic treatment with mood-stabilizing anti-convulsants or lithium in cultured astrocytes and brain, but not in neurons. Neuropharmacology 57 , 375–385 (2009).
Diaz, S. L., Narboux-Neme, N., Boutourlinsky, K., Doly, S. & Maroteaux, L. Mice lacking the serotonin 5-HT2B receptor as an animal model of resistance to selective serotonin reuptake inhibitors antidepressants. Eur. Neuropsychopharmacol. 26 , 265–279 (2016).
Sviridova, A. et al. The role of 5-HT(2B)-receptors in fluoxetine-mediated modulation of Th17- and Th1-cells in multiple sclerosis. J. Neuroimmunol. 356 , 577608 (2021).
Hertz, L. Isotope-based quantitation of uptake, release, and metabolism of glutamate and glucose in cultured astrocytes. Methods Mol. Biol. 814 , 305–323 (2012).
Arakawa, R. et al. Venlafaxine ER blocks the norepinephrine transporter in the brain of patients with major depressive disorder: a PET study using [18F]FMeNER-D2. Int J. Neuropsychopharmacol. 22 , 278–285 (2019).
Gould, G. G., Javors, M. A. & Frazer, A. Effect of chronic administration of duloxetine on serotonin and norepinephrine transporter binding sites in rat brain. Biol. Psychiatry 61 , 210–215 (2007).
Owens, M. J. et al. Estimates of serotonin and norepinephrine transporter inhibition in depressed patients treated with paroxetine or venlafaxine. Neuropsychopharmacology 33 , 3201–3212 (2008).
Sramek, J. J. et al. Exploratory biomarker study of the triple reuptake inhibitor sep-432 compared to the dual reuptake inhibitor duloxetine in healthy normal subjects. CNS Neurosci. Ther. 22 , 404–412 (2016).
Wang, Y. et al. The association between antidepressant treatment and brain connectivity in two double-blind, placebo-controlled clinical trials: a treatment mechanism study. Lancet Psychiatry 6 , 667–674 (2019).
Berman, R. M. et al. Antidepressant effects of ketamine in depressed patients. Biol. Psychiatry 47 , 351–354 (2000).
Murrough, J. W. et al. Antidepressant efficacy of ketamine in treatment-resistant major depression: a two-site randomized controlled trial. Am. J. Psychiatry 170 , 1134–1142 (2013).
Zanos, P. et al. NMDAR inhibition-independent antidepressant actions of ketamine metabolites. Nature 533 , 481–486 (2016).
Li, N. et al. mTOR-dependent synapse formation underlies the rapid antidepressant effects of NMDA antagonists. Science 329 , 959–964 (2010).
Li, N. et al. Glutamate N-methyl-D-aspartate receptor antagonists rapidly reverse behavioral and synaptic deficits caused by chronic stress exposure. Biol. Psychiatry 69 , 754–761 (2011).
Beurel, E., Grieco, S. F., Amadei, C., Downey, K. & Jope, R. S. Ketamine-induced inhibition of glycogen synthase kinase-3 contributes to the augmentation of alpha-amino-3-hydroxy-5-methylisoxazole-4-propionic acid (AMPA) receptor signaling. Bipolar Disord. 18 , 473–480 (2016).
Miller, O. H., Moran, J. T. & Hall, B. J. Two cellular hypotheses explaining the initiation of ketamine’s antidepressant actions: direct inhibition and disinhibition. Neuropharmacology 100 , 17–26 (2016).
Mingardi, J. et al. miR-9-5p is involved in the rescue of stress-dependent dendritic shortening of hippocampal pyramidal neurons induced by acute antidepressant treatment with ketamine. Neurobiol. Stress 15 , 100381 (2021).
Krystal, J. H., Charney, D. S. & Duman, R. S. A new rapid-acting antidepressant. Cell 181 , 7 (2020).
Moliner, R. et al. Psychedelics promote plasticity by directly binding to BDNF receptor TrkB. Nat. Neurosci. 26 , 1032–1041 (2023).
Halberstadt, A. L., Koedood, L., Powell, S. B. & Geyer, M. A. Differential contributions of serotonin receptors to the behavioral effects of indoleamine hallucinogens in mice. J. Psychopharmacol. 25 , 1548–1561 (2011).
Hesselgrave, N., Troppoli, T. A., Wulff, A. B., Cole, A. B. & Thompson, S. M. Harnessing psilocybin: antidepressant-like behavioral and synaptic actions of psilocybin are independent of 5-HT2R activation in mice. Proc. Natl Acad. Sci. USA 118 , e2022489118 (2021).
Cao, D. et al. Structure-based discovery of nonhallucinogenic psychedelic analogs. Science 375 , 403–411 (2022).
Shao, L. X. et al. Psilocybin induces rapid and persistent growth of dendritic spines in frontal cortex in vivo. Neuron 109 , 2535–2544 e2534 (2021).
Caraci, F. et al. Neurobiological links between depression and AD: The role of TGF-beta1 signaling as a new pharmacological target. Pharmacol. Res 130 , 374–384 (2018).
Chen, B., Wang, J. F., Sun, X. & Young, L. T. Regulation of GAP-43 expression by chronic desipramine treatment in rat cultured hippocampal cells. Biol. Psychiatry 53 , 530–537 (2003).
Lee, K. M. & Kim, Y. K. The role of IL-12 and TGF-beta1 in the pathophysiology of major depressive disorder. Int. Immunopharmacol. 6 , 1298–1304 (2006).
Sutcigil, L. et al. Pro- and anti-inflammatory cytokine balance in major depression: effect of sertraline therapy. Clin. Dev. Immunol. 2007 , 76396 (2007).
Zhao, Y. N. et al. Nelumbo nucifera gaertn stems (Hegeng) improved depression Behavior in CUMS mice by regulating NCAM and GAP-43 expression. Evid. Based Complement Altern. Med 2020 , 3056954 (2020).
Zavvari, F., Nahavandi, A. & Goudarzi, M. Fluoxetine attenuates stress-induced depressive-like behavior through modulation of hippocampal GAP43 and neurogenesis in male rats. J. Chem. Neuroanat. 103 , 101711 (2020).
Wang, Q., Timberlake, M. A. 2nd, Prall, K. & Dwivedi, Y. The recent progress in animal models of depression. Prog. Neuropsychopharmacol. Biol. Psychiatry 77 , 99–109 (2017).
Aten, S. et al. Chronic stress impairs the structure and function of astrocyte networks in an animal model of depression. Neurochem. Res. 48 , 1191–1210 (2023).
Liang, S. et al. Iron aggravates the depressive phenotype of stressed mice by compromising the glymphatic system. Neurosci. Bull. 36 , 1542–1546 (2020).
Antoniuk, S., Bijata, M., Ponimaskin, E. & Wlodarczyk, J. Chronic unpredictable mild stress for modeling depression in rodents: meta-analysis of model reliability. Neurosci. Biobehav Rev. 99 , 101–116 (2019).
Fernandez, D. C. et al. Light affects mood and learning through distinct retina-brain pathways. Cell 175 , 71–84.e18 (2018).
Smolders, K. C., de Kort, Y. A. & Cluitmans, P. J. A higher illuminance induces alertness even during office hours: findings on subjective measures, task performance and heart rate measures. Physiol. Behav. 107 , 7–16 (2012).
Liu, A. et al. Encoding of environmental illumination by primate melanopsin neurons. Science 379 , 376–381 (2023).
Lam, R. W. et al. Efficacy of bright light treatment, fluoxetine, and the combination in patients with nonseasonal major depressive disorder: a randomized clinical trial. JAMA Psychiatry 73 , 56–63 (2016).
Rutten, S. et al. Bright light therapy for depression in Parkinson disease: a randomized controlled trial. Neurology 92 , e1145–e1156 (2019).
Li, V. W. et al. Functional outcomes with bright light in monotherapy and combined with fluoxetine in patients with major depressive disorder: results from the LIFE-D trial. J. Affect. Disord. 297 , 396–400 (2022).
Guzel Ozdemir, P. et al. Comparison of venlafaxine alone versus venlafaxine plus bright light therapy combination for severe major depressive disorder. J. Clin. Psychiatry 76 , e645–654 (2015).
Lambert, G. W., Reid, C., Kaye, D. M., Jennings, G. L. & Esler, M. D. Effect of sunlight and season on serotonin turnover in the brain. Lancet 360 , 1840–1842 (2002).
Huang, L. et al. A visual circuit related to habenula underlies the antidepressive effects of light therapy. Neuron 102 , 128–142.e128 (2019).
McClintock, S. M. et al. Consensus recommendations for the clinical application of repetitive transcranial magnetic stimulation (rTMS) in the treatment of depression. J. Clin. Psychiatry 79 , 16cs10905 (2018).
Wall, C. A. et al. Adjunctive use of repetitive transcranial magnetic stimulation in depressed adolescents: a prospective, open pilot study. J. Clin. Psychiatry 72 , 1263–1269 (2011).
Qiu, H. et al. Efficacy and safety of repetitive transcranial magnetic stimulation in children and adolescents with depression: a systematic review and preliminary meta-analysis. J. Affect. Disord. 320 , 305–312 (2023).
Mutz, J. et al. Comparative efficacy and acceptability of non-surgical brain stimulation for the acute treatment of major depressive episodes in adults: systematic review and network meta-analysis. BMJ 364 , l1079 (2019).
Faller, J. et al. Daily prefrontal closed-loop repetitive transcranial magnetic stimulation (rTMS) produces progressive EEG quasi-alpha phase entrainment in depressed adults. Brain Stimul. 15 , 458–471 (2022).
Kaster, T. S. et al. Efficacy, tolerability, and cognitive effects of deep transcranial magnetic stimulation for late-life depression: a prospective randomized controlled trial. Neuropsychopharmacology 43 , 2231–2238 (2018).
Desbeaumes Jodoin, V., Miron, J. P. & Lesperance, P. Safety and efficacy of accelerated repetitive transcranial magnetic stimulation protocol in elderly depressed unipolar and bipolar patients. Am. J. Geriatr. Psychiatry 27 , 548–558 (2019).
Wathra, R. A. et al. Effect of prior pharmacotherapy on remission with sequential bilateral theta-burst versus standard bilateral repetitive transcranial magnetic stimulation in treatment-resistant late-life depression. Br. J. Psychiatry 223 , 504–506 (2023).
Cox, E. Q. et al. Repetitive transcranial magnetic stimulation for the treatment of postpartum depression. J. Affect. Disord. 264 , 193–200 (2020).
Pascual-Leone, A., Rubio, B., Pallardo, F. & Catala, M. D. Rapid-rate transcranial magnetic stimulation of left dorsolateral prefrontal cortex in drug-resistant depression. Lancet 348 , 233–237 (1996).
Zrenner, B. et al. Brain oscillation-synchronized stimulation of the left dorsolateral prefrontal cortex in depression using real-time EEG-triggered TMS. Brain Stimul. 13 , 197–205 (2020).
Fitzgerald, P. B. Targeting repetitive transcranial magnetic stimulation in depression: do we really know what we are stimulating and how best to do it? Brain Stimul. 14 , 730–736 (2021).
Rosen, A. C. et al. Targeting location relates to treatment response in active but not sham rTMS stimulation. Brain Stimul. 14 , 703–709 (2021).
Moffitt, T. E. et al. How common are common mental disorders? Evidence that lifetime prevalence rates are doubled by prospective versus retrospective ascertainment. Psychol. Med. 40 , 899–909 (2010).
Brini, S. et al. Efficacy and safety of transcranial magnetic stimulation for treating major depressive disorder: An umbrella review and re-analysis of published meta-analyses of randomised controlled trials. Clin. Psychol. Rev. 100 , 102236 (2023).
Qaseem, A., Barry, M. J. & Kansagara, D. Clinical Guidelines Committee of the American College of PhysiciansNonpharmacologic versus pharmacologic treatment of adult patients with major depressive disorder: a clinical practice guideline from the american college of physicians. Ann. Intern. Med. 164 , 350–359 (2016).
Biesheuvel-Leliefeld, K. E. et al. Effectiveness of psychological interventions in preventing recurrence of depressive disorder: meta-analysis and meta-regression. J. Affect. Disord. 174 , 400–410 (2015).
Breedvelt, J. J. F. et al. Psychological interventions as an alternative and add-on to antidepressant medication to prevent depressive relapse: systematic review and meta-analysis. Br. J. Psychiatry 219 , 538–545 (2021).
Guidi, J. & Fava, G. A. Sequential combination of pharmacotherapy and psychotherapy in major depressive disorder: a systematic review and meta-analysis. JAMA Psychiatry 78 , 261–269 (2021).
Tang, Y., Yin, H. Y., Rubini, P., Illes, P. & Acupuncture-Induced Analgesia: a neurobiological basis in purinergic signaling. Neuroscientist 22 , 563–578 (2016).
Chan, Y. Y., Lo, W. Y., Yang, S. N., Chen, Y. H. & Lin, J. G. The benefit of combined acupuncture and antidepressant medication for depression: a systematic review and meta-analysis. J. Affect Disord. 176 , 106–117 (2015).
Mischoulon, D., Brill, C. D., Ameral, V. E., Fava, M. & Yeung, A. S. A pilot study of acupuncture monotherapy in patients with major depressive disorder. J. Affect Disord. 141 , 469–473 (2012).
Yue, N. et al. Electro-acupuncture alleviates chronic unpredictable stress-induced depressive- and anxiety-like behavior and hippocampal neuroinflammation in rat model of depression. Front. Mol. Neurosci. 11 , 149 (2018).
Jung, J. et al. Lipidomics reveals that acupuncture modulates the lipid metabolism and inflammatory interaction in a mouse model of depression. Brain Behav. Immun. 94 , 424–436 (2021).
Lin, S. S. et al. Electroacupuncture prevents astrocyte atrophy to alleviate depression. Cell Death Dis. 14 , 343 (2023).
Wang, Z. et al. Acupuncture treatment modulates the corticostriatal reward circuitry in major depressive disorder. J. Psychiatr. Res. 84 , 18–26 (2017).
Duan, D. M., Tu, Y., Liu, P. & Jiao, S. Antidepressant effect of electroacupuncture regulates signal targeting in the brain and increases brain-derived neurotrophic factor levels. Neural Regen. Res. 11 , 1595–1602 (2016).
Bai, L. et al. Mechanisms underlying the antidepressant effect of acupuncture via the CaMK signaling pathway. Front Behav. Neurosci. 14 , 563698 (2020).
Cai, X. et al. Electroacupuncture alleviated depression-like behaviors in ventromedial prefrontal cortex of chronic unpredictable mild stress-induced rats: Increasing synaptic transmission and phosphorylating dopamine transporter. CNS Neurosci. Ther. 29 , 2608–2620 (2023).
Xu, G. et al. Clinical evidence for association of acupuncture with improved major depressive disorder: a systematic review and meta-analysis of randomized control trials. Neuropsychobiology 82 , 1–13 (2023).
Ding, Y. et al. Molecular and genetic characterization of depression: overlap with other psychiatric disorders and aging. Mol. Neuropsychiatry 1 , 1–12 (2015).
PubMed PubMed Central Google Scholar
Kay, R. B. & Brunjes, P. C. Diversity among principal and GABAergic neurons of the anterior olfactory nucleus. Front. Cell. Neurosci. 8 , 111 (2014).
Karolewicz, B. et al. Reduced level of glutamic acid decarboxylase-67 kDa in the prefrontal cortex in major depression. Int. J. Neuropsychopharmacol. 13 , 411–420 (2010).
Azmitia, E. C. Serotonin neurons, neuroplasticity, and homeostasis of neural tissue. Neuropsychopharmacology 21 , 33S–45S (1999).
Kerman, I. A. et al. Evidence for transcriptional factor dysregulation in the dorsal raphe nucleus of patients with major depressive disorder. Front. Neurosci. 6 , 135 (2012).
Keller-Wood, M. Hypothalamic-pituitary–adrenal axis-feedback control. Compr. Physiol. 5 , 1161–1182 (2015).
Alt, S. R. et al. Differential expression of glucocorticoid receptor transcripts in major depressive disorder is not epigenetically programmed. Psychoneuroendocrinology 35 , 544–556 (2010).
van Loo, H. M., Aggen, S. H., Gardner, C. O. & Kendler, K. S. Sex similarities and differences in risk factors for recurrence of major depression. Psychol. Med. 48 , 1685–1693 (2018).
Salk, R. H., Hyde, J. S. & Abramson, L. Y. Gender differences in depression in representative national samples: meta-analyses of diagnoses and symptoms. Psychol. Bull. 143 , 783–822 (2017).
Cavanagh, A., Wilson, C. J., Kavanagh, D. J. & Caputi, P. Differences in the expression of symptoms in men versus women with depression: a systematic review and meta-analysis. Harv. Rev. Psychiatry 25 , 29–38 (2017).
Marcus, S. M. et al. Gender differences in depression: findings from the STAR*D study. J. Affect Disord. 87 , 141–150 (2005).
Poulter, M. O. et al. GABAA receptor promoter hypermethylation in suicide brain: implications for the involvement of epigenetic processes. Biol. Psychiatry 64 , 645–652 (2008).
Seney, M. L. et al. The role of genetic sex in affect regulation and expression of GABA-related genes across species. Front. Psychiatry 4 , 104 (2013).
Gray, A. L., Hyde, T. M., Deep-Soboslay, A., Kleinman, J. E. & Sodhi, M. S. Sex differences in glutamate receptor gene expression in major depression and suicide. Mol. Psychiatry 20 , 1057–1068 (2015).
Goswami, D. B., May, W. L., Stockmeier, C. A. & Austin, M. C. Transcriptional expression of serotonergic regulators in laser-captured microdissected dorsal raphe neurons of subjects with major depressive disorder: sex-specific differences. J. Neurochem. 112 , 397–409 (2010).
Szewczyk, B. et al. Gender-specific decrease in NUDR and 5-HT1A receptor proteins in the prefrontal cortex of subjects with major depressive disorder. Int. J. Neuropsychopharmacol. 12 , 155–168 (2009).
Fiori, L. M. et al. miR-323a regulates ERBB4 and is involved in depression. Mol. Psychiatry 26 , 4191–4204 (2021).
Roy, B., Wang, Q., Palkovits, M., Faludi, G. & Dwivedi, Y. Altered miRNA expression network in locus coeruleus of depressed suicide subjects. Sci. Rep. 7 , 4387 (2017).
Zheng, P. et al. Identification of sex-specific urinary biomarkers for major depressive disorder by combined application of NMR- and GC-MS-based metabonomics. Transl. Psychiatry 6 , e955 (2016).
Liu, X. et al. Discovery and validation of plasma biomarkers for major depressive disorder classification based on liquid chromatography-mass spectrometry. J. Proteome Res. 14 , 2322–2330 (2015).
Liu, X. et al. Plasma lipidomics reveals potential lipid markers of major depressive disorder. Anal. Bioanal. Chem. 408 , 6497–6507 (2016).
Wang, Z., Gerstein, M. & Snyder, M. RNA-Seq: a revolutionary tool for transcriptomics. Nat. Rev. Genet 10 , 57–63 (2009).
Xu, Y. et al. Serum cytokines-based biomarkers in the diagnosis and monitoring of therapeutic response in patients with major depressive disorder. Int. Immunopharmacol. 118 , 110108 (2023).
Pantazatos, S. P. et al. Whole-transcriptome brain expression and exon-usage profiling in major depression and suicide: evidence for altered glial, endothelial and ATPase activity. Mol. Psychiatry 22 , 760–773 (2017).
Herbet, M. et al. Altered expression of genes involved in brain energy metabolism as adaptive responses in rats exposed to chronic variable stress; changes in cortical level of glucogenic and neuroactive amino acids. Mol. Med. Rep. 19 , 2386–2396 (2019).
Yamanishi, K. et al. Analysis of genes linked to depressive-like behaviors in interleukin-18-deficient mice: gene expression profiles in the brain. Biomed. Rep. 12 , 3–10 (2020).
Kuperman, Y. et al. Perifornical Urocortin-3 mediates the link between stress-induced anxiety and energy homeostasis. Proc. Natl Acad. Sci. USA 107 , 8393–8398 (2010).
Bustamante, A. C., Armstrong, D. L. & Uddin, M. Epigenetic profiles associated with major depression in the human brain. Psychiatry Res. 260 , 439–442 (2018).
Beger, R. D. et al. Metabolomics enables precision medicine: “A White Paper, Community Perspective”. Metabolomics 12 , 149 (2016).
Kaddurah-Daouk, R. et al. Cerebrospinal fluid metabolome in mood disorders-remission state has a unique metabolic profile. Sci. Rep. 2 , 667 (2012).
Schmaal, L. et al. Cortical abnormalities in adults and adolescents with major depression based on brain scans from 20 cohorts worldwide in the ENIGMA Major Depressive Disorder Working Group. Mol. Psychiatry 22 , 900–909 (2017).
Schmitgen, M. M. et al. Aberrant cortical neurodevelopment in major depressive disorder. J. Affect. Disord. 243 , 340–347 (2019).
Chen, Z. et al. High-field magnetic resonance imaging of structural alterations in first-episode, drug-naive patients with major depressive disorder. Transl. Psychiatry 6 , e942 (2016).
Grimm, S. et al. Increased self-focus in major depressive disorder is related to neural abnormalities in subcortical-cortical midline structures. Hum. Brain Mapp. 30 , 2617–2627 (2009).
Yoshimura, S. et al. Cognitive behavioral therapy for depression changes medial prefrontal and ventral anterior cingulate cortex activity associated with self-referential processing. Soc. Cogn. Affect. Neurosci. 9 , 487–493 (2014).
Yu, H. et al. Functional brain abnormalities in major depressive disorder using the Hilbert-Huang transform. Brain Imaging Behav. 12 , 1556–1568 (2018).
Holmes, S. E. et al. Lower synaptic density is associated with depression severity and network alterations. Nat. Commun. 10 , 1529 (2019).
Bettini, E. et al. Pharmacological comparative characterization of REL-1017 (Esmethadone-HCl) and Other NMDAR channel blockers in human heterodimeric N-methyl-D-aspartate receptors. Pharmaceuticals (Basel) 15 , 997 (2022).
Hanania, T., Manfredi, P., Inturrisi, C. & Vitolo, O. V. The N-methyl-D-aspartate receptor antagonist d-methadone acutely improves depressive-like behavior in the forced swim test performance of rats. Exp. Clin. Psychopharmacol. 28 , 196–201 (2020).
Fogaca, M. V. et al. N-Methyl-D-aspartate receptor antagonist d-methadone produces rapid, mTORC1-dependent antidepressant effects. Neuropsychopharmacology 44 , 2230–2238 (2019).
Fava, M. et al. REL-1017 (esmethadone) as adjunctive treatment in patients with major depressive disorder: a phase 2a randomized double-blind trial. Am. J. Psychiatry 179 , 122–131 (2022).
De Martin, S. et al. REL-1017 (Esmethadone) increases circulating BDNF levels in healthy subjects of a phase 1 clinical study. Front. Pharmacol. 12 , 671859 (2021).
Chou, T. H., Kang, H., Simorowski, N., Traynelis, S. F. & Furukawa, H. Structural insights into assembly and function of GluN1-2C, GluN1-2A-2C, and GluN1-2D NMDARs. Mol. Cell 82 , 4548–4563.e4544 (2022).
Hochschild, A. et al. Ketamine vs midazolam: Mood improvement reduces suicidal ideation in depression. J. Affect Disord. 300 , 10–16 (2022).
Burgdorf, J. et al. GLYX-13, a NMDA receptor glycine-site functional partial agonist, induces antidepressant-like effects without ketamine-like side effects. Neuropsychopharmacology 38 , 729–742 (2013).
Gigliucci, V. et al. Ketamine elicits sustained antidepressant-like activity via a serotonin-dependent mechanism. Psychopharmacology (Berl.) 228 , 157–166 (2013).
Daly, E. J. et al. Efficacy and safety of intranasal esketamine adjunctive to oral antidepressant therapy in treatment-resistant depression: a randomized clinical trial. JAMA Psychiatry 75 , 139–148 (2018).
Zhao, J. et al. Low-dose ketamine inhibits neuronal apoptosis and neuroinflammation in PC12 cells via alpha7nAChR mediated TLR4/MAPK/NF-kappaB signaling pathway. Int. Immunopharmacol. 117 , 109880 (2023).
Yang, Y. et al. Ketamine relieves depression-like behaviors induced by chronic postsurgical pain in rats through anti-inflammatory, anti-oxidant effects and regulating BDNF expression. Psychopharmacology (Berl.) 237 , 1657–1669 (2020).
Shibakawa, Y. S. et al. Effects of ketamine and propofol on inflammatory responses of primary glial cell cultures stimulated with lipopolysaccharide. Br. J. Anaesth. 95 , 803–810 (2005).
Abbasi, S., Hosseini, F., Modabbernia, A., Ashrafi, M. & Akhondzadeh, S. Effect of celecoxib add-on treatment on symptoms and serum IL-6 concentrations in patients with major depressive disorder: randomized double-blind placebo-controlled study. J. Affect. Disord. 141 , 308–314 (2012).
Akhondzadeh, S. et al. Clinical trial of adjunctive celecoxib treatment in patients with major depression: a double blind and placebo controlled trial. Depress Anxiety 26 , 607–611 (2009).
Nettis, M. A. et al. Augmentation therapy with minocycline in treatment-resistant depression patients with low-grade peripheral inflammation: results from a double-blind randomised clinical trial. Neuropsychopharmacology 46 , 939–948 (2021).
Hasebe, K. et al. Exploring interleukin-6, lipopolysaccharide-binding protein and brain-derived neurotrophic factor following 12 weeks of adjunctive minocycline treatment for depression. Acta Neuropsychiatr. 34 , 220–227 (2022).
Su, K. et al. Omega-3 fatty acids in the prevention of interferon-alpha-induced depression: results from arandomized, controlled trial. Biol. Psychiatry 76 , 559–566 (2014).
Berk, M. et al. Youth Depression Alleviation with Anti-inflammatory Agents (YoDA-A): a randomised clinical trial of rosuvastatin and aspirin. BMC Med . 18 , 16 (2020).
Meltzer-Brody, S. et al. Brexanolone injection in post-partum depression: two multicentre, double-blind, randomised, placebo-controlled, phase 3 trials. Lancet 392 , 1058–1070 (2018).
Leal, G. C. et al. Arketamine as adjunctive therapy for treatment-resistant depression: A placebo-controlled pilot study. J Affect. Disord. 330 , 7–15 (2023).
Kuga, N., Sasaki, T., Takahara, Y., Matsuki, N. & Ikegaya, Y. Large-scale calcium waves traveling through astrocytic networks in vivo. J. Neurosci. 31 , 2607–2614 (2011).
Shawcross, D. L. et al. Infection and systemic inflammation, not ammonia, are associated with Grade 3/4 hepatic encephalopathy, but not mortality in cirrhosis. J. Hepatol. 54 , 640–649 (2011).
Page, G. et al. The up-regulation of the striatal dopamine transporter’s activity by cAMP is PKA-, CaMK II- and phosphatase-dependent. Neurochem. Int. 45 , 627–632 (2004).
França, A. S. et al. D2 dopamine receptor regulation of learning, sleep and plasticity. Eur. Neuropsychopharmacol. 25 , 493–504 (2015).
Beaulieu, J. M. & Gainetdinov, R. R. The physiology, signaling, and pharmacology of dopamine receptors. Pharmacol. Rev. 63 , 182–217 (2011).
Opal, M. D. et al. Serotonin 2C receptor antagonists induce fast-onset antidepressant effects. Mol. Psychiatry 19 , 1106–1114 (2014).
Seki, K., Yoshida, S. & Jaiswal, M. K. Molecular mechanism of noradrenaline during the stress-induced major depressive disorder. Neural Regen. Res. 13 , 1159–1169 (2018).
Duman, R. S., Aghajanian, G. K., Sanacora, G. & Krystal, J. H. Synaptic plasticity and depression: new insights from stress and rapid-acting antidepressants. Nat. Med. 22 , 238–249 (2016).
Yang, B. et al. Comparison of R-ketamine and rapastinel antidepressant effects in the social defeat stress model of depression. Psychopharmacology 233 , 3647–3657 (2016).
Download references
Acknowledgements
This work was supported by the National Natural Science Foundation of China, MX [grant number 32271038] and BL [grant number 81871852]; Shenyang Science and Technology Innovation Talents Project, BL [grant number RC210251]; ‘ChunHui’ Program of Education Ministry, BL [grant number 2020703]; National Natural Science Foundation of China-Russian Science Foundation (NSFC-RSF), YT [grant number 82261138557]; Sichuan Provincial Administration of Traditional Chinese Medicine, YT [grant number 2023zd024].
Author information
Authors and affiliations.
Department of Forensic Analytical Toxicology, School of Forensic Medicine, China Medical University, Shenyang, China
Lulu Cui, Shu Li, Siman Wang, Xiafang Wu, Yingyu Liu, Weiyang Yu, Yijun Wang & Baoman Li
Liaoning Province Key Laboratory of Forensic Bio-evidence Sciences, Shenyang, China
China Medical University Centre of Forensic Investigation, Shenyang, China
International Joint Research Centre on Purinergic Signalling/Key Laboratory of Acupuncture for Senile Disease (Chengdu University of TCM), Ministry of Education/School of Health and Rehabilitation, Chengdu University of Traditional Chinese Medicine/Acupuncture and Chronobiology Key Laboratory of Sichuan Province, Chengdu, China
Department of Orthopaedics, The First Hospital, China Medical University, Shenyang, China
Maosheng Xia
You can also search for this author in PubMed Google Scholar
Contributions
L.C., X.W., and B.L. provided direction and guidance throughout the preparation of this manuscript. L.C., X.W., and B.L. wrote and edited the manuscript. L.C., S.L., S.W., M.X., and B.L. reviewed and made significant revisions to the manuscript. L.C., S.L., S.W., X.W., Y.L., W.Y., Y.W., Y.T., M.X., and B.L. collected and prepared the related papers. All authors have read and approved the article.
Corresponding authors
Correspondence to Maosheng Xia or Baoman Li .
Ethics declarations
Competing interests.
The authors declare no competing interests.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/ .
Reprints and permissions
About this article
Cite this article.
Cui, L., Li, S., Wang, S. et al. Major depressive disorder: hypothesis, mechanism, prevention and treatment. Sig Transduct Target Ther 9 , 30 (2024). https://doi.org/10.1038/s41392-024-01738-y
Download citation
Received : 20 September 2023
Revised : 24 December 2023
Accepted : 28 December 2023
Published : 09 February 2024
DOI : https://doi.org/10.1038/s41392-024-01738-y
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies

Premium Content
Can scientists ‘solve’ stress? They’re trying.
From cardiovascular disease and obesity to a weakened immune system, the side effects of stress can be life-altering. But there may be a way to prevent those outcomes.

As modern-day stress ratchets up to what feels like unbearable levels, researchers are striving to learn more about the precise mechanisms through which it affects our body and mind. The hope is that by unlocking more about how stress works physiologically, we can find ways to prevent it from permanently harming people.
Over the last five decades, scientists have established beyond doubt that persistent stress really can poison our overall health. In addition to increasing the risk of cardiovascular disease , stress plays a role in obesity and diabetes and can weaken the immune system , leaving us more vulnerable to infectious diseases. You can recover swiftly from an episode of acute stress—for example, the alarm one might feel when caught unprepared for a presentation. Chronic stress, on the other hand, is more toxic as it is an unrelenting circumstance that offers little chance for a return to normalcy. Financial strain, having a bully for a boss, and social isolation are all examples.

Today chronic stress seems to be increasing worldwide, as people grapple with rapid socioeconomic and environmental change. A 2023 national survey by the American Psychological Association found that stress has taken a serious toll since the start of the pandemic , with the incidence of chronic illnesses and mental health problems going up significantly, especially among those ages 35 to 44.
( Do you have chronic stress? Look for these signs. )
So far, one of the major realizations among scientists is that stress harms all of us in different and powerful ways. But is there any way to avoid it—or at least recover more quickly? Some promising avenues of research offer hope for the future.

Preventing chronic stress from harming you in the first place
Groundbreaking studies in orphans showed how stress in early life can leave an indelible mark on the brain.
For Hungry Minds
“Chronic stress in early life has more serious and lasting effects, because that’s when a lot of connections are being laid down in the brain,” says Aniko Korosi, a researcher at the University of Amsterdam who has been conducting experiments on mice to elucidate that link between early-life stress and brain development.
Korosi may have found a surprising link between stress and the resulting nutrient composition in the brain . She and her colleagues noticed that mouse pups that had been exposed to stress in the first week of their lives—having been moved from their mother’s care to a cage—had lower levels of certain fatty acids and amino acids in their brains compared with pups being raised in a stress-free environment.
She wondered if it was possible to normalize a stressed pup’s development by feeding it a diet rich in the specific nutrients its brain would be lacking. To find out, the researchers first fed a supplemented diet to the mothers so it would pass through their milk, then continued to provide it in the pups’ feed for two weeks after they were weaned. A few months later, the researchers tested the now adult mice in learning and memory. Unlike stressed mice that had never received an enriched diet, these mice did not display cognitive impairments.
( How wild animals cope with stress—from overeating to sleepless nights. )

“I was surprised that changing the nutrition could have such a powerful effect, because it’s such an easy intervention,” Korosi says.
If further studies provide more evidence of the nutritional pathway, she says, there would be a strong basis for supplementing the diets of infants born to mothers living in stressful conditions.
Developing an early warning system for stress
Katie McLaughlin, a psychologist at the University of Oregon, is investigating how mental health problems arise in adolescents as they’re going through a particularly vulnerable time in their lives, transitioning to adulthood.
She and her colleagues are still collecting data , but a smaller, precursor study tracking 30 teenagers offers clues about what the researchers might learn—and how it might help them identify stress before it goes too far.

In that study, McLaughlin found that the extent of stress experienced by a subject in the month before their lab visit changed how their brain responded to emotionally impactful information such as when they were shown a picture of a threatening face. The brain’s prefrontal cortex, which helps regulate emotions, showed less activation when the subject had experienced higher levels of stress.
McLaughlin is optimistic that data from the ongoing study will help pinpoint changes in behavior as well as brain activity that predict the emergence of mental health problems like anxiety and depression. This could enable the development of targeted interventions delivered to teenagers at just the right time, she says. If the identified marker of stress were a sudden decrease in sleep duration or a sharp decline in social interactions, for example, it would be possible to push the intervention out to the individual on their smartphone.
“Like, here’s a reminder about good sleep hygiene, or this might be a good time to check in with your counselor at school about what’s been going on in your life,” McLaughlin explains.
( ‘Hysterical strength’? Fight or flight? This is how your body reacts to extreme stress. )
Learn more about stress and how to manage it
Preventing inflammation caused by chronic stress.
Gaining a deeper understanding of how stress affects the immune system may also help find a way to reverse those effects.
You May Also Like

Does meditation actually work? Here’s what the science says.

How to cope with stress at work—and avoid burning out

20 stress-relief gifts for the frazzled friend in your life
In the 1980s, psychologist Janice Kiecolt-Glaser and her virologist husband, Ronald Glaser, began exploring the physiological impact of stress on two notably stressed segments of society: medical students and older caregivers. The researchers found the students’ immune systems were less robust when they were taking exams than during non-exam times—and that stress altered the body’s response to vaccines.

Researchers then administered the flu and pneumonia vaccines to individuals responsible for a spouse with dementia. Unlike medical students taking exams, who were likely stressed only in the short term, these people were experiencing unrelenting stress. When tested at set periods after inoculation, they had fewer antibodies compared with a control group —they couldn’t maintain their protective response. “That gave us good evidence that the changes brought on by stress were biologically meaningful,” says Kiecolt-Glaser, now an emeritus professor at the Ohio State University.
Around the same time, researchers led by Sheldon Cohen, now emeritus professor of psychology at Carnegie Mellon University, delivered cold-causing viruses into the nostrils of about 400 adult volunteers in the U.K. “The more stress they reported prior to our exposing them to a virus, the higher the risk was for them to develop a cold,” says Cohen. The duration and type of stress mattered: Chronic economic or interpersonal stress were what really put people at high risk—and the longer it went on, the greater the susceptibility to falling sick.

Cohen and his colleagues also learned that when exposed to viruses, chronically stressed people tended to produce an excess of cytokines—proteins that serve as messengers of the immune system, traveling to sites of infection and injury and activating inflammation and other cellular processes to protect the body. Too many cytokines cause an excess of inflammation.
Researchers still don’t know enough about how stress alters the immune system’s ability to regulate cytokines to devise an intervention to reduce the inflammation, but in one way, these findings signal some hope: There are clear targets for more work to be done.
Understanding stress on a cellular level
The future of understanding and combating stress may lie in our DNA.
In 2023, Ursula Beattie, then a doctoral student at Tufts University, and her colleagues found possible evidence that stress can overwhelm DNA’s repair mechanisms . In their study, researchers repeatedly tapped on sparrow cages with pens, played the radio loudly, and other actions designed to cause distress but no physical harm. Blood and tissue samples from the sparrows after three weeks of this unpleasant treatment revealed damage to the DNA. “It’s like if you had two pieces of string coiled up, just like DNA, and you took a pair of scissors and cut them,” Beattie says.

While these kinds of double-strand breaks in DNA occur all the time in sparrows and other species, including humans, the damage is typically reversed through self-repair mechanisms. In a chronic-stress setting, “those repair mechanisms get overwhelmed, which is how we see a buildup of DNA damage,” Beattie explains. The damage in the birds appears to be the most severe in cells of the liver, she adds, suggesting that for humans, too, the extent and type of damage inflicted by stress might be different for different tissues of the body.
Separately, Kiecolt-Glaser and psychologist Lisa Christian at OSU are conducting a longitudinal study to determine whether chronic stress ages you more quickly. If results support a smaller, earlier study, it appears that chronically stressed caregivers not only are more likely to get sick and heal more slowly but they also show signs of accelerated aging.
We’re still learning how deep stress goes into our bodies. But these exploratory findings mean we’re getting closer to solving the puzzle that is stress, which promises a future where we can better meet the ongoing demand for change.
( 20 stress-relief gifts for the frazzled friend in your life. )

Related Topics
- MENTAL HEALTH
- PUBLIC HEALTH

‘Hysterical strength’? Fight or flight? This is how your body reacts to extreme stress

Extreme heat can be deadly – here’s how to know if you’re at risk

What your biological age can reveal about your health

Do you really need 10,000 steps a day? Here’s what the science says.

Many people wean off antidepressants too quickly. That can be dangerous.
- Environment
- Perpetual Planet
History & Culture
- History & Culture
- History Magazine
- Mind, Body, Wonder
- Terms of Use
- Privacy Policy
- Your US State Privacy Rights
- Children's Online Privacy Policy
- Interest-Based Ads
- About Nielsen Measurement
- Do Not Sell or Share My Personal Information
- Nat Geo Home
- Attend a Live Event
- Book a Trip
- Inspire Your Kids
- Shop Nat Geo
- Visit the D.C. Museum
- Learn About Our Impact
- Support Our Mission
- Advertise With Us
- Customer Service
- Renew Subscription
- Manage Your Subscription
- Work at Nat Geo
- Sign Up for Our Newsletters
- Contribute to Protect the Planet
Copyright © 1996-2015 National Geographic Society Copyright © 2015-2024 National Geographic Partners, LLC. All rights reserved
Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
Chapter 16. Stress, Health, and Coping
16.2 Stress and Coping
Jennifer Walinga
Learning Objectives
- Define coping and adaptation.
- Understand the various conceptualizations of stress as stimulus, response, and transactional process.
- Understand the role of cognition and physiology in coping with stress.
- Recognize emotion-focused and problem-focused coping strategies.
- Understand the relationships and interactions between health, stress, and coping.
In order to understand how people learn to cope with stress, it is important to first reflect on the different conceptualizations of stress and how the coping research has emerged alongside distinct approaches to stress. Stress has been viewed as a response , a stimulus, and a transaction . How an individual conceptualizes stress determines his or her response, adaptation, or coping strategies.
Stress As a Response
Stress as a response model, initially introduced by Hans Selye (1956), describes stress as a physiological response pattern and was captured within his general adaptation syndrome (GAS) model (Figure 16.3). This model describes stress as a dependent variable and includes three concepts :
- Stress is a defensive mechanism.
- Stress follows the three stages of alarm, resistance, and exhaustion.
- If the stress is prolonged or severe, it could result in diseases of adaptation or even death.
Later, in The Stress Concept: Past, Present and Future (1983), Selye introduced the idea that the stress response could result in positive or negative outcomes based on cognitive interpretations of the physical symptoms or physiological experience (Figure 16.3, “The General Adaptation to Stress Model “) . In this way, stress could be experienced as eustress (positive) or dystress (negative). However, Selye always considered stress to be a physiologically based construct or response. Gradually, other researchers expanded the thinking on stress to include and involve psychological concepts earlier in the stress model.
The response model of stress incorporates coping within the model itself. The idea of adaptation or coping is inherent to the GAS model at both the alarm and resistance stages. When confronted with a negative stimulus, the alarm response initiates the sympathetic nervous system to combat or avoid the stressor (i.e., increased heart rate, temperature, adrenaline, and glucose levels). The resistance response then initiates physiological systems with a fight or flight reaction to the stressor, returning the system to homeostasis, reducing harm, or more generally accommodating the stressor, which can lead to adaptive diseases such as sleep deprivation, mental illness, hypertension, or heart disease. Thus, along with the early conceptualization of stress as a physiological response, early research on coping was also born. As early as 1932, Walter Cannon described the notion of self-regulation in his work The Wisdom of the Body.
Stress As a Stimulus
The theory of stress as a stimulus was introduced in the 1960s, and viewed stress as a significant life event or change that demands response, adjustment, or adaptation. Holmes and Rahe (1967) created the Social Readjustment Rating Scale (SRRS) consisting of 42 life events scored according to the estimated degree of adjustment they would each demand of the person experiencing them (e.g., marriage, divorce, relocation, change or loss of job, loss of loved one). Holmes and Rahe theorized that stress was an independent variable in the health-stress-coping equation — the cause of an experience rather than the experience itself. While some correlations emerged between SRRS scores and illness (Rahe, Mahan, & Arthur, 1970; Johnson & Sarason, 1979), there were problems with the stress as stimulus theory. The stress as stimulus theory assumes:
- Change is inherently stressful.
- Life events demand the same levels of adjustment across the population.
- There is a common threshold of adjustment beyond which illness will result.
Rahe and Holmes initially viewed the human subject as a passive recipient of stress, one who played no role in determining the degree, intensity, or valence of the stressor. Later, Rahe introduced the concept of interpretation into his research (Rahe & Arthur, 1978), suggesting that a change or life event could be interpreted as a positive or negative experience based on cognitive and emotional factors. However, the stress as stimulus model still ignored important variables such as prior learning, environment, support networks, personality, and life experience.
Stress As a Transaction
In attempting to explain stress as more of a dynamic process, Richard Lazarus developed the transactional theory of stress and coping (TTSC) (Lazarus, 1966; Lazarus & Folkman, 1984), which presents stress as a product of a transaction between a person (including multiple systems: cognitive, physiological, affective, psychological, neurological) and his or her complex environment . Stress as a transaction was introduced with the most impact when Dr. Susan Kobasa first used the concept of hardiness (Kobasa, 1979). Hardiness refers to a pattern of personality characteristics that distinguishes people who remain healthy under life stress compared with those who develop health problems. In the late 1970s, the concept of hardiness was further developed by Salvatore Maddi, Kobasa, and their graduate students at the University of Chicago (Kobasa, 1982; Kobasa & Maddi, 1981; Kobasa, Maddi, & Kahn, 1982; Kobasa, Maddi, Puccetti, & Zola, 1985; Maddi & Kobasa, 1984). Hardiness has some notable similarities with other personality constructs in psychology, including locus of control (Rotter, 1966), sense of coherence (Antonovsky, 1987), self-efficacy (Bandura, 1997), and dispositional optimism (Scheier & Carver, 1985), all of which will be discussed in the next section. Researchers introduced multiple variables to the stress-as-transaction model, expanding and categorizing various factors to account for the complex systems involved in experiencing a stressor (Werner, 1993). The nature of stress was described in multiple ways: acute, episodic or intermittent, and chronic. Different types of stressors emerged, such as event, situation, cue, and condition, which then fell into categories based on locus of control, predictability, tone, impact, and duration. Figure 16.4 illustrates theories of stress as a response, stimulus, and transaction.
In his book Psychological Stress and the Coping Process (1966), Lazarus presented an elegant integration of previous research on stress, health, and coping that placed a person’s appraisal of a stressor at the centre of the stress experience. How an individual appraises a stressor determines how he or she copes with or responds to the stressor. Whether or not a stressor is experienced as discomforting is influenced by a variety of personal and contextual factors including capacities, skills and abilities, constraints, resources, and norms (Mechanic, 1978). Lazarus and Folkman (1984) unpacked the concept of interpretation further in their model of stress appraisal, which includes primary, secondary, and reappraisal components (see Figure 16.5, “ The Transactional Theory of Stress and Coping”). Primary appraisal involves determining whether the stressor poses a threat . Secondary appraisal involves the individual’s evaluation of the resources or coping strategies at his or her disposal for addressing any perceived threats . The process of reappraisal is ongoing and involves continually reappraising both the nature of the stressor and the resources available for responding to the stressor .
Coping with Stress
There are many ways that people strive to cope with stressors and feelings of stress in their lives. A host of literature, both popular and academic, extols the practice of stress management and whole industries are devoted to it. Many techniques are available to help individuals cope with the stresses that life brings. Some of the techniques listed in Figure 16.6, “Stress Management Techniques,” induce a lower than usual stress level temporarily to compensate the biological tissues involved; others face the stressor at a higher level of abstraction. Stress management techniques are more general and range from cognitive (mindfulness, cognitive therapy, meditation) to physical (yoga, art, natural medicine, deep breathing) to environmental (spa visits, music, pets, nature).
Stress coping , as described by researchers such as Lazarus and Folkman, implies a more specific process of cognitive appraisal to determine whether an individual believes he or she has the resources to respond effectively to the challenges of a stressor or change (Folkman & Lazarus, 1988; Lazarus & Folkman, 1987). The appraisal literature explains the response or coping process in terms of problem-focused coping or emotion-focused coping (Folkman & Lazarus, 1980; Lazarus & Folkman, 1984), also referred to as active and passive coping styles (Jex, Bliese, Buzzell, & Primeau, 2001). As well, approach and avoidance-style measures of coping exist involving assertiveness or withdrawal (Anshel, 1996; Anshel & Weinberg, 1999; Roth & Cohen, 1986). When faced with a challenge, an individual primarily appraises the challenge as either threatening or non-threatening, and secondarily in terms of whether he or she has the resources to respond to or cope with the challenge effectively. If the individual does not believe he or she has the capacity to respond to the challenge or feels a lack of control, he or she is most likely to turn to an emotion-focused coping response such as wishful thinking (e.g., I wish that I could change what is happening or how I feel), distancing (e.g., I’ll try to forget the whole thing), or emphasizing the positive (e.g., I’ll just look for the silver lining) (Lazarus & Folkman, 1987). If the person has the resources to manage the challenge, he or she will usually develop a problem-focused coping response such as analysis (e.g., I try to analyze the problem in order to understand it better; I’m making a plan of action and following it). It is theorized and empirically demonstrated that a person’s secondary appraisal then determines coping strategies (Lazarus & Folkman, 1987). Coping strategies vary from positive thinking to denial (see Figure 16.7, “COPE Inventory”) and are measured and tested using a variety of instruments and scales such as the COPE inventory (Carver, Scheier, & Weintraub, 1989).
Research Focus: Stress and Playing Soccer
Walinga (2008), in her work with a university soccer team that was undergoing several stressful changes in addition to the usual performance stressors, recently elaborated upon the appraisal model by suggesting that reappraisal more specifically involves a reiteration of the primary-secondary appraisal process. Once a person determines that a stressor is indeed a threat, and secondarily appraises resources as lacking, he or she then primarily appraises the secondary appraisal. In other words, the person determines whether having a lack of resources indeed poses some sort of threat. If lack of resources is deemed not to be a threat, the person is much more likely to generate creative solutions to the initial stressor and therefore cope effectively. But if a lack of resources is deemed to be a threat, then the person tends to focus on finding resources rather than addressing the initial stressor, and arrives at ineffective control-focused coping strategies.
In the case of the university soccer players, some initial stressors were identified as “a particularly challenging or sizable opponent,” “rainy conditions,” “the cold,” “not connecting with the coach,” or “negative attitudes on the field.” Typical emotion- or control-focused coping strategies included “working harder” and “sucking it up,” as well as avoidance or passivity. One player who struggled with her opponent’s size felt that she had little control over the fact that her opponent was taller and thus “beat her to the header balls.” She explained how she would “just kinda fade away when we play that team…get passive and just fade into the background.” Her coping response signified a withdrawal subscale on the emotion-focused coping scale, and when asked about her degree of satisfaction with her chosen path of response, she replied that she was “unhappy but could see no other alternative.” However, generally the team and several of the key leaders expressed alternative coping strategies not accounted for in the transactional theory of stress and coping. While several members of the team had a negative secondary appraisal, believing themselves to be lacking in the resources required to deal with the changes that occurred to the team, during the interviews it became apparent that such powerlessness did not, as was expected, lead only to emotion-focused coping, such as defensiveness, blame, or withdrawal; an acknowledged lack of control often resulted in an ability to move on and solve the challenges of change effectively.
Many of the team members believed “hitting rock bottom” accounted for their successful transformation, acting as a sort of “trigger” or “restart” and enabling them to gain greater clarity about their goals, as well as strategies for achieving these goals. Rather than focusing on increasing control or controlling the barrier or threat itself, the tolerant individual accepts the barrier as reality and accepts the lack of control as a reality. This person can now attend to and identify the challenges that the barrier poses to attaining her goals. For instance, the goalkeeper focused not on regretting or blaming herself for a missed save, or even trying harder next time, but instead focused on the challenges that a difficult shot posed for her and how she might resolve an unexpected spin on the ball. When faced with rainy conditions, the tolerant player focused not on denying or pushing through the rain, but on the problems the rain creates for her and how to resolve the resulting lack of ball control or slippery field conditions:
- “I guess the spin on the ball was out of my control, but I had total control in terms of adjusting to it.”
- “I was not in control of what my opponent did with the ball or could have done to ensure that I did not win the ball, but I was in control of making sure I did not dive into the tackle, I held my check up so we could get numbers back and avoid a counterattack.”
- “I went forward when I probably shouldn’t have and I left our defenders outnumbered in the back, so I made sure I won the ball so that we would not be faced with a 3-on-2.”
- “Despite my fatigue, I decided to make better decisions on when to commit myself and made sure I communicated when I needed help so that my opponent wouldn’t get a breakaway.”
- “The lights in my eyes were beyond my control, but I could control my focus on the ball and my positioning.”
- “I was not in control of the fact that they were fast; I was in control of my positioning and my decision making.”
By extending the theory of stress and coping, it is hypothesized here that when an individual perceives that he or she is lacking in resources to manage a threat, the perceived lack of control, and not necessarily anxiety, becomes the new challenge and focal point. If the person deems the perceived lack of control to be threatening or problematic for any reason, this would hypothetically cause him or her to fixate on increasing resources for managing the threat (control-focused coping), and impede any kind of response to the particular threats the challenge itself generates. If, on the other hand, the person accepts the lack of control, deeming the lack of resources to be a benign reality, he or she would be able to move the focus to the problems this threat creates and consider options for resolution and goal achievement (problem-focused coping). Control-focused coping seems to be a more generalizable construct for explaining an individual’s inability to focus on the problem at hand. The readiness model proposes that the appraisal process continues to cycle through the primary and secondary phases to determine an individual’s coping response (i.e., primary appraisal = Is it a threat?; secondary appraisal = Do I have the resources to change or control the threat?; if not, we find ourselves back at primary appraisal = Is my lack of control a threat?), and it is this cyclical process of appraisal that offers leverage for facilitating effective coping.
Related concepts to stress coping include locus of control (Rotter, 1966), sense of coherence (Antonovsky, 1987), self-efficacy (Bandura, 1997), and stress-related growth (Scheier & Carver, 1985). Rotter posited that a person with an internal locus of control believes that their achievements and outcomes are determined by their own decisions and efforts. If they do not succeed, they believe it is due to their own lack of effort. Whereas, a person with an external locus of control believes that achievements and outcomes are determined by fate, luck, or other . If the person does not succeed, he or she believes it is due to external forces outside of the person’s control. Aaron Antonovsky (1987) defined sense of coherence as:
a global orientation that expresses the extent to which one has a pervasive, enduring though dynamic feeling of confidence that (1) the stimuli deriving from one’s internal and external environments in the course of living are structured, predictable and explicable; (2) the resources are available to one to meet the demands posed by these stimuli; and (3) these demands are challenges, worthy of investment and engagement (pg. 19).
Self-efficacy is often confused with self-confidence, but in fact confidence is merely one of the many factors that make up a strong sense of self-efficacy. Albert Bandura (1997) defined self-efficacy as the extent or strength of one’s belief in one’s own ability to complete tasks and reach goals . Self-confidence is a trait measure (a quality that is built over time) whereas self-efficacy is a state measure (a capacity experienced at a specific point in time and concerning a specific task). Stress-related growth or thriving is a dispositional response to stress that enables the individual to see opportunities for growth as opposed to threat or debilitation . Spreitzer and colleagues (2005) offered a preliminary definition of thriving as a “psychological state in which individuals experience both a sense of vitality and a sense of learning at work” (p. 538). Carver (1998) described thriving as being “better off after adversity” (p. 247). There are many examples of individuals surpassing previous performances when faced with particularly stressful scenarios, showing increased growth and strength in the face of adversity.
Coping and Health
The capacity for thriving, resilience, or stress-related growth has been associated with improved health outcomes. For example, building on Carver’s work on dispositional optimism and thriving, Shepperd, Maroto, and Pbert (1996) found, in their longitudinal study of cardiac patients, that optimism predicts success in making health changes associated with lower risk of cardiac disease. Optimism was significantly and directly correlated with improved health outcomes, including lower levels of saturated fat, body fat, and global coronary risk, and positively associated with success in increasing aerobic capacity. Billings and colleagues (2000) showed that coping affected positive and negative affect among men who were caregiving for AIDS patients. Social support coping predicted increases in positive affect, which in turn were related to fewer physical symptoms. Avoidant coping, however, was related to increases in negative affect, which were related to more physical symptoms.
Research Focus: Coping with Melanoma
Perhaps the most dramatic of stress coping interventions studies was conducted by Fawzy and his colleagues (Fawzy, Cousins, Fawzy, Kemeny, & Morton, 1990; Fawzy, Kemeny, et al., 1990; Fawzy, et al., 1993; Fawzy & Fawzy, 1994), who did specific coping skills interventions with melanoma patients. During a six-week structured program, participants experienced multiple program components including health education, psychological support, problem-solving, and stress management training. In the short term, the experimental subjects were more likely to use active behaviour coping than the controls, and also had more positive affect. Differences in immune functioning were evident between the two groups at the six-month assessment. Specifically, experimental subjects had a greater percentage of large granular lymphocytes, more NK cells, and better NK cytotoxicity. While coping strategies were not directly associated with immune cell changes, they were correlated with affect, which in turn was associated with immune functioning. The studies supported the hypothesis that effects of coping on biomedical outcomes may be mediated through affect. At a five-year follow-up, a third of the control group had died, compared with less than 10% of the experimental group. Longer survival was associated with more active coping at baseline.
Key Takeaways
- Stress has been conceived of in different ways: as a response, as a stimulus, and as a transaction.
- Stress as response treats stress as the physiological dependent variable.
- Stress as stimulus treats stress as a life event or change that acts as an independent variable.
- Stress as transaction considers the myriad personal, social, and environmental factors that come into play in determining the nature, degree, and impact of the stress experience.
- There are a variety of stress management techniques deriving from a multitude of theoretical derivations and philosophies.
- Coping with stress can be a trait or state-based process — an inherent quality or ability or a learned skill or capacity.
- How people appraise a stressor determines how they will attempt to cope with the stressor.
- Appraisal hinges on multiple human, social, and environmental factors.
- Concepts related to coping include optimism, thriving, hardiness, locus of control, and self-efficacy, all qualities and capacities that can influence the coping strategies an individual chooses to apply to a stressor.
Exercises and Critical Thinking
- Reflect on a recent emotionally or physiologically impactful stressor that you perceived to be threatening or negative. What social, environmental, and personal factors contributed to your appraisal of the stressor? Referencing the list of coping items on the COPE inventory, what types of coping strategies did you apply?
- Imagine a stressful situation that you believe you coped with positively. Can you identify some coping strategies you used? Can you determine whether you were able to grow through the experience? What factors facilitated a positive outcome for you?
- What are some major life events you have experienced? Can you identify differences in how you appraised these events? How you coped with these events?
Anshel, M.H. (1996). Coping styles among adolescent competitive athletes. The Journal of Social Psychology, 136, 311-323.
Anshel, M.H. & Weinberg, R.T. (1999). Re-examining coping among basketball referees following stressful events: Implications for coping interventions. Journal of Sport Behavior, 22, 144-161.
Antonovsky, A. (1987). Unraveling the mystery of health: How people manage stress and stay well . San Francisco: Jossey Bass.
Bandura, A. (1997 ). Self-efficacy: The exercise of control. New York: Freeman.
Billings, D. W., Folkman, S., Acree, M., & Moskowitz, J. T. (2000). Coping and physical health during caregiving: The roles of positive and negative affect. Journal of Personality and Social Psychology, 79 , 131–142.
Carver, C. S. (1998). Resilience and thriving: Issues, models, and linkages. Journal of Social Issues, 54 , 245–266.
Carver, C. S., Scheier, M. F., & Weintraub, J. K. (1989). Assessing coping strategies: A theoretically based approach . Journal of Personality and Social Psychology, 56 , 267–283.
Cannon, W. B. (1932). The Wisdom of the Body. New York: W.W. Norton.
Fawzy, F., & Fawzy, N. (1994). Psychoeducational interventions and health outcomes. In R. Glaser and J. K. Kiecolt-Glaser (Eds.). Handbook of human stress and immunity (pp. 365–402). San Diego: Academic Press.
Fawzy, F. I., Fawzy, N. W., Hyun, C., Elashoff, R., Guthrie, D., Fahey, J. L., & Moron, D. L. (1993). Malignant melanoma: Effects on early structured psychiatric intervention, coping, and affective state on recurrence and survival six years later. Archives of General Psychiatry, 50 , 681–689.
Fawzy, F. I., Cousins, N., Fawzy, N. W., Kemeny, M., & Morton, D. I. (1990). A structured psychiatric intervention for cancer patients: I. Changes over time in methods of coping and affective disturbance. Archives of General Psychiatry, 47 , 720–725.
Fawzy, F. I., Kemeny, M., Fawzy, N. W., Elashoff, R., Morton, D., Cousins, N., & Fahey, J. L. (1990). A structured psychiatric intervention for cancer patients: II. Changes over time in immunological measures. Archives of General Psychiatry, 47 , 729–235.
Folkman, S. & Lazarus, R.S. (1980). An analysis of coping in a middle-aged community sample. Journal of Health & Social Behavior, 21 (3), 219-239.
Folkman, S., Lazarus, R. S. (1988). Coping as a mediator of emotion. Journal of Personal and Social Psycholog,. 54, 466-75.
Holmes, T., & Rahe, R. (1967). The Social Reajustment Rating Scale. Journal of Psychosomatic Research, 12, (4), p. 213–233.
Jex, S.M., Bliese, P.D., Buzzell, S., & Primeau. J. (2001). The impact of self-efficacy on stressor–strain relations: Coping style as an explanatory mechanism. Journal of Applied Psychology 86 (3), 401.
Johnson , J. H., & Sarason , I. G. (1979). Moderator variables in life stress research. In I. Sarason & C. Spielberger (Eds.), Stress an d anxiety, 6, 151–167.
Kobasa, S. C. (1979). Stressful life events, personality, and health – Inquiry into hardiness. Journal of Personality and Social Psychology, 37 (1), 1–11.
Kobasa, S. C. (1982). The hardy personality: Toward a social psychology of stress and health. In G. Sanders & J. Suls (Eds), social Psychology of Health and Illness (p. 3-32). Hillsdale, NJ: Erlbaum.
Kobasa, S. C., Maddi, S. R., & Courington, S. (1981). Personality and constitution as mediators in the stress-illness relationship. Journal of Health and Social Behavior 22 (4), 368–378.
Kobasa, S. C., Maddi, S. R., & Kahn, S. (1982). Hardiness and health: A prospective study. Journal of Personality and Social Psychology 42 (1), 168–177.
Kobasa, S. C., Maddi, S. R., Puccetti, M. C., & Zola, M. A. (1985). Effectiveness of hardiness, exercise and social support as resources against illness. Journal of Psychosomatic Research 29 (5), 525–533.
Lazarus, R. S. (1966). Psychological stress and the coping process. New York, NY: McGraw-Hill.
Lazarus, R. S. (1999). Stress and emotion: A new synthesis. New York: Springer.
Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal, and coping . New York: Springer.
Lazarus, R. S., & Folkman, S. (1987). Transactional theory and research on emotions and coping. European Journal of Personality, 1, 141–169 .
Maddi, S. R., & Kobasa, S. C. (1984). The hardy executive: Health under stress . Homewood, IL: Dow Jones-Irwin.
Mechanic, D. (1978). Students under stress: A study in the social psychology of adaptation . Madison: University of Wisconsin Press.
Rahe, R. H., & Arthur, R. J. (1978). Life change and illness studies: Past history and future directions. Journal of Human Stress, 4, 3–15.
Rahe R. H., Mahan J. L., & Arthur R. J. (1970). Prediction of near-future health change from subjects’ preceding life changes. Journal of Psychosomatic Research, 14 (4), 401–6.
Roth, S., & Cohen, L.J. (1986). Approach, avoidance, and coping with stress. American Psychologist, 41 , 813-819.
Rotter, J. B. (1966) Generalized expectancies for internal versus external control of reinforcement. Psychological Monographs, 80 Sanders, G.S. & Suls, J. (Eds.), Social psychology of health and illness (pp. 1–25).
Scheier, M. F., & Carver, C. S. (1985). Optimism, coping, and health – Assessment and implications of generalized outcome expectancies. Health Psychology, 4 (3), 219–247.
Selye, H. (1956). The stress of life . New York: McGraw Hill.
Selye, H. (1983). The concept of stress: Past, present and future. In C.L. Cooper (Ed.). Stress research: Issues for the eighties. New York: John Wiley.
Shepperd, J. A., Maroto, J. J., & Pbert , L. A. (1996). Dispositional optimism as a predictor of health changes among cardiac patients. Journal of Research in Personality 30 , 517–534.
Spreitzer, G., Sutcliffe, K., Dutton, J., Sonenshein, S. & Grant, A. (2005). A socially embedded model of thriving at work. Organization Science 16 (5): 537-549.
Walinga, J. (2008). Change Readiness: The Roles of Appraisal, Focus, and Perceived Control. Journal of Applied Behavioral Science, 44 (3), 315–347.
Werner, E.E. (1993). Risk, resilience, and recovery: Perspectives from the Kauai longitudinal study. Development and Psychopathology, 5 , 503-515.
Image Attributions
Figure 16.3: A diagram of the General Adaptation syndrome model by David G. Myers (http://commons.wikimedia.org/wiki/File:General_Adaptation_Syndrome.jpg) used under the CC-BY 3.0 (http://creativecommons.org/licenses/by/3.0/deed.en).
Figure 16.4: by J. Walinga.
Figure 16.5: by J. Walinga.
Figure 16.6: by J. Walinga.
Figure 16.7: Adapted by J. Walinga from Carver, Scheier, & Weintraub, 1989.
Long Descriptions
[Return to Figure 16.6] Figure 16.7 long description: COPE Inventory scale of coping techniques
- positive reinterpretation and growth
- mental disengagement
- focus on and venting of emotions
- use of instrumental social support
- active coping
- religious coping
- behavioural disengagement
- use of emotional social support
- substance use
- suppression of competing activities
[Return to Figure 16.7]
Introduction to Psychology - 1st Canadian Edition Copyright © 2014 by Jennifer Walinga is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License , except where otherwise noted.
Share This Book
Stress, coping, and depression: testing a new hypothesis in a prospectively studied general population sample of U.S.-born Whites and Blacks
Affiliation.
- 1 Columbia University, Department of Epidemiology, 722 West 168th Street, Suite #720E, NY 10032, USA. [email protected]
- PMID: 21227557
- PMCID: PMC3072813
- DOI: 10.1016/j.socscimed.2010.12.005
The scarcity of empirically supported explanations for the Black/White prevalence difference in depression in the U.S. is a conspicuous gap in the literature. Recent evidence suggests that the paradoxical observation of decreased risk of depression but elevated rates of physical illness among Blacks in the U.S. compared with Whites may be accounted for by the use of coping behaviors (e.g., alcohol and nicotine consumption, overeating) among Blacks exposed to high stress levels. Such coping behaviors may mitigate deleterious effects of stressful exposures on mental health while increasing the risk of physical ailments. The racial patterning in mental and physical health outcomes could therefore be explained by this mechanism if a) these behaviors were more prevalent among Blacks than Whites and/or b) the effect of these behavioral responses to stress was differential by race. The present study challenges this hypothesis using longitudinal, nationally-representative data with comprehensive DSM-IV diagnoses. Data are drawn from 34,653 individuals sampled in Waves 1 (2001-2002) and 2 (2004-2005) as part of the US National Epidemiologic Survey on Alcohol and Related Conditions. Results showed that a) Blacks were less likely to engage in alcohol or nicotine consumption at low, moderate, and high levels of stress compared to Whites, and b) there was a significant three-way interaction between race, stress, and coping behavior for BMI only (F = 2.11, df = 12, p = 0.03), but, contrary to the hypothesis, elevated BMI was protective against depression in Blacks at low, not high, levels of stress. Further, engagement in unhealthy behaviors, especially at pathological levels, did not protect against depression in Blacks or in Whites. In sum, the impact of stress and coping processes on depression does not appear to operate differently in Blacks versus Whites. Further research testing innovative hypotheses that would explain the difference in Black/White depression prevalence is warranted.
Copyright © 2010 Elsevier Ltd. All rights reserved.
Publication types
- Research Support, N.I.H., Extramural
- Adaptation, Psychological*
- Alcohol Drinking / ethnology
- Black or African American / psychology*
- Black or African American / statistics & numerical data
- Body Mass Index
- Depression / ethnology*
- Empirical Research
- Obesity / ethnology
- Prospective Studies
- Risk Factors
- Smoking / ethnology
- Stress, Psychological / ethnology*
- United States / epidemiology
- White People / psychology*
- White People / statistics & numerical data
Grants and funding
- F31 DA026689/DA/NIDA NIH HHS/United States
- F31 DA026689-01/DA/NIDA NIH HHS/United States
- T32MH013043-36/MH/NIMH NIH HHS/United States
- F31-DA026689/DA/NIDA NIH HHS/United States
- T32 MH013043/MH/NIMH NIH HHS/United States
- Bipolar Disorder
- Therapy Center
- When To See a Therapist
- Types of Therapy
- Best Online Therapy
- Best Couples Therapy
- Best Family Therapy
- Managing Stress
- Sleep and Dreaming
- Understanding Emotions
- Self-Improvement
- Healthy Relationships
- Student Resources
- Personality Types
- Guided Meditations
- Verywell Mind Insights
- 2024 Verywell Mind 25
- Mental Health in the Classroom
- Editorial Process
- Meet Our Review Board
- Crisis Support
How to Write a Great Hypothesis
Hypothesis Definition, Format, Examples, and Tips
Kendra Cherry, MS, is a psychosocial rehabilitation specialist, psychology educator, and author of the "Everything Psychology Book."
:max_bytes(150000):strip_icc():format(webp)/IMG_9791-89504ab694d54b66bbd72cb84ffb860e.jpg "hypothesis on stress")
Amy Morin, LCSW, is a psychotherapist and international bestselling author. Her books, including "13 Things Mentally Strong People Don't Do," have been translated into more than 40 languages. Her TEDx talk, "The Secret of Becoming Mentally Strong," is one of the most viewed talks of all time.
:max_bytes(150000):strip_icc():format(webp)/VW-MIND-Amy-2b338105f1ee493f94d7e333e410fa76.jpg "hypothesis on stress")
Verywell / Alex Dos Diaz
- The Scientific Method
Hypothesis Format
Falsifiability of a hypothesis.
- Operationalization
Hypothesis Types
Hypotheses examples.
- Collecting Data
A hypothesis is a tentative statement about the relationship between two or more variables. It is a specific, testable prediction about what you expect to happen in a study. It is a preliminary answer to your question that helps guide the research process.
Consider a study designed to examine the relationship between sleep deprivation and test performance. The hypothesis might be: "This study is designed to assess the hypothesis that sleep-deprived people will perform worse on a test than individuals who are not sleep-deprived."
At a Glance
A hypothesis is crucial to scientific research because it offers a clear direction for what the researchers are looking to find. This allows them to design experiments to test their predictions and add to our scientific knowledge about the world. This article explores how a hypothesis is used in psychology research, how to write a good hypothesis, and the different types of hypotheses you might use.
The Hypothesis in the Scientific Method
In the scientific method , whether it involves research in psychology, biology, or some other area, a hypothesis represents what the researchers think will happen in an experiment. The scientific method involves the following steps:
- Forming a question
- Performing background research
- Creating a hypothesis
- Designing an experiment
- Collecting data
- Analyzing the results
- Drawing conclusions
- Communicating the results
The hypothesis is a prediction, but it involves more than a guess. Most of the time, the hypothesis begins with a question which is then explored through background research. At this point, researchers then begin to develop a testable hypothesis.
Unless you are creating an exploratory study, your hypothesis should always explain what you expect to happen.
In a study exploring the effects of a particular drug, the hypothesis might be that researchers expect the drug to have some type of effect on the symptoms of a specific illness. In psychology, the hypothesis might focus on how a certain aspect of the environment might influence a particular behavior.
Remember, a hypothesis does not have to be correct. While the hypothesis predicts what the researchers expect to see, the goal of the research is to determine whether this guess is right or wrong. When conducting an experiment, researchers might explore numerous factors to determine which ones might contribute to the ultimate outcome.
In many cases, researchers may find that the results of an experiment do not support the original hypothesis. When writing up these results, the researchers might suggest other options that should be explored in future studies.
In many cases, researchers might draw a hypothesis from a specific theory or build on previous research. For example, prior research has shown that stress can impact the immune system. So a researcher might hypothesize: "People with high-stress levels will be more likely to contract a common cold after being exposed to the virus than people who have low-stress levels."
In other instances, researchers might look at commonly held beliefs or folk wisdom. "Birds of a feather flock together" is one example of folk adage that a psychologist might try to investigate. The researcher might pose a specific hypothesis that "People tend to select romantic partners who are similar to them in interests and educational level."
Elements of a Good Hypothesis
So how do you write a good hypothesis? When trying to come up with a hypothesis for your research or experiments, ask yourself the following questions:
- Is your hypothesis based on your research on a topic?
- Can your hypothesis be tested?
- Does your hypothesis include independent and dependent variables?
Before you come up with a specific hypothesis, spend some time doing background research. Once you have completed a literature review, start thinking about potential questions you still have. Pay attention to the discussion section in the journal articles you read . Many authors will suggest questions that still need to be explored.
How to Formulate a Good Hypothesis
To form a hypothesis, you should take these steps:
- Collect as many observations about a topic or problem as you can.
- Evaluate these observations and look for possible causes of the problem.
- Create a list of possible explanations that you might want to explore.
- After you have developed some possible hypotheses, think of ways that you could confirm or disprove each hypothesis through experimentation. This is known as falsifiability.
In the scientific method , falsifiability is an important part of any valid hypothesis. In order to test a claim scientifically, it must be possible that the claim could be proven false.
Students sometimes confuse the idea of falsifiability with the idea that it means that something is false, which is not the case. What falsifiability means is that if something was false, then it is possible to demonstrate that it is false.
One of the hallmarks of pseudoscience is that it makes claims that cannot be refuted or proven false.
The Importance of Operational Definitions
A variable is a factor or element that can be changed and manipulated in ways that are observable and measurable. However, the researcher must also define how the variable will be manipulated and measured in the study.
Operational definitions are specific definitions for all relevant factors in a study. This process helps make vague or ambiguous concepts detailed and measurable.
For example, a researcher might operationally define the variable " test anxiety " as the results of a self-report measure of anxiety experienced during an exam. A "study habits" variable might be defined by the amount of studying that actually occurs as measured by time.
These precise descriptions are important because many things can be measured in various ways. Clearly defining these variables and how they are measured helps ensure that other researchers can replicate your results.
Replicability
One of the basic principles of any type of scientific research is that the results must be replicable.
Replication means repeating an experiment in the same way to produce the same results. By clearly detailing the specifics of how the variables were measured and manipulated, other researchers can better understand the results and repeat the study if needed.
Some variables are more difficult than others to define. For example, how would you operationally define a variable such as aggression ? For obvious ethical reasons, researchers cannot create a situation in which a person behaves aggressively toward others.
To measure this variable, the researcher must devise a measurement that assesses aggressive behavior without harming others. The researcher might utilize a simulated task to measure aggressiveness in this situation.
Hypothesis Checklist
- Does your hypothesis focus on something that you can actually test?
- Does your hypothesis include both an independent and dependent variable?
- Can you manipulate the variables?
- Can your hypothesis be tested without violating ethical standards?
The hypothesis you use will depend on what you are investigating and hoping to find. Some of the main types of hypotheses that you might use include:
- Simple hypothesis : This type of hypothesis suggests there is a relationship between one independent variable and one dependent variable.
- Complex hypothesis : This type suggests a relationship between three or more variables, such as two independent and dependent variables.
- Null hypothesis : This hypothesis suggests no relationship exists between two or more variables.
- Alternative hypothesis : This hypothesis states the opposite of the null hypothesis.
- Statistical hypothesis : This hypothesis uses statistical analysis to evaluate a representative population sample and then generalizes the findings to the larger group.
- Logical hypothesis : This hypothesis assumes a relationship between variables without collecting data or evidence.
A hypothesis often follows a basic format of "If {this happens} then {this will happen}." One way to structure your hypothesis is to describe what will happen to the dependent variable if you change the independent variable .
The basic format might be: "If {these changes are made to a certain independent variable}, then we will observe {a change in a specific dependent variable}."
A few examples of simple hypotheses:
- "Students who eat breakfast will perform better on a math exam than students who do not eat breakfast."
- "Students who experience test anxiety before an English exam will get lower scores than students who do not experience test anxiety."
- "Motorists who talk on the phone while driving will be more likely to make errors on a driving course than those who do not talk on the phone."
- "Children who receive a new reading intervention will have higher reading scores than students who do not receive the intervention."
Examples of a complex hypothesis include:
- "People with high-sugar diets and sedentary activity levels are more likely to develop depression."
- "Younger people who are regularly exposed to green, outdoor areas have better subjective well-being than older adults who have limited exposure to green spaces."
Examples of a null hypothesis include:
- "There is no difference in anxiety levels between people who take St. John's wort supplements and those who do not."
- "There is no difference in scores on a memory recall task between children and adults."
- "There is no difference in aggression levels between children who play first-person shooter games and those who do not."
Examples of an alternative hypothesis:
- "People who take St. John's wort supplements will have less anxiety than those who do not."
- "Adults will perform better on a memory task than children."
- "Children who play first-person shooter games will show higher levels of aggression than children who do not."
Collecting Data on Your Hypothesis
Once a researcher has formed a testable hypothesis, the next step is to select a research design and start collecting data. The research method depends largely on exactly what they are studying. There are two basic types of research methods: descriptive research and experimental research.
Descriptive Research Methods
Descriptive research such as case studies , naturalistic observations , and surveys are often used when conducting an experiment is difficult or impossible. These methods are best used to describe different aspects of a behavior or psychological phenomenon.
Once a researcher has collected data using descriptive methods, a correlational study can examine how the variables are related. This research method might be used to investigate a hypothesis that is difficult to test experimentally.
Experimental Research Methods
Experimental methods are used to demonstrate causal relationships between variables. In an experiment, the researcher systematically manipulates a variable of interest (known as the independent variable) and measures the effect on another variable (known as the dependent variable).
Unlike correlational studies, which can only be used to determine if there is a relationship between two variables, experimental methods can be used to determine the actual nature of the relationship—whether changes in one variable actually cause another to change.
The hypothesis is a critical part of any scientific exploration. It represents what researchers expect to find in a study or experiment. In situations where the hypothesis is unsupported by the research, the research still has value. Such research helps us better understand how different aspects of the natural world relate to one another. It also helps us develop new hypotheses that can then be tested in the future.
Thompson WH, Skau S. On the scope of scientific hypotheses . R Soc Open Sci . 2023;10(8):230607. doi:10.1098/rsos.230607
Taran S, Adhikari NKJ, Fan E. Falsifiability in medicine: what clinicians can learn from Karl Popper [published correction appears in Intensive Care Med. 2021 Jun 17;:]. Intensive Care Med . 2021;47(9):1054-1056. doi:10.1007/s00134-021-06432-z
Eyler AA. Research Methods for Public Health . 1st ed. Springer Publishing Company; 2020. doi:10.1891/9780826182067.0004
Nosek BA, Errington TM. What is replication ? PLoS Biol . 2020;18(3):e3000691. doi:10.1371/journal.pbio.3000691
Aggarwal R, Ranganathan P. Study designs: Part 2 - Descriptive studies . Perspect Clin Res . 2019;10(1):34-36. doi:10.4103/picr.PICR_154_18
Nevid J. Psychology: Concepts and Applications. Wadworth, 2013.
By Kendra Cherry, MSEd Kendra Cherry, MS, is a psychosocial rehabilitation specialist, psychology educator, and author of the "Everything Psychology Book."
Learned Helplessness
Charlotte Nickerson
Research Assistant at Harvard University
Undergraduate at Harvard University
Charlotte Nickerson is a student at Harvard University obsessed with the intersection of mental health, productivity, and design.
Learn about our Editorial Process
Saul Mcleod, PhD
Editor-in-Chief for Simply Psychology
BSc (Hons) Psychology, MRes, PhD, University of Manchester
Saul Mcleod, PhD., is a qualified psychology teacher with over 18 years of experience in further and higher education. He has been published in peer-reviewed journals, including the Journal of Clinical Psychology.
Olivia Guy-Evans, MSc
Associate Editor for Simply Psychology
BSc (Hons) Psychology, MSc Psychology of Education
Olivia Guy-Evans is a writer and associate editor for Simply Psychology. She has previously worked in healthcare and educational sectors.
Learned helplessness is a psychological state in which an individual, after repeated exposure to uncontrollable negative events, believes they are powerless to change their situation, even when opportunities to do so arise. This leads to passivity, decreased motivation, and a sense of hopelessness, which can persist even when circumstances change and control is possible. Learned helplessness is often associated with depression.

Key Takeaways
- Learned Helplessness is a phenomenon that occurs when a series of negative outcomes or stressors cause someone to believe that the outcomes of life are out of one’s control.
- If a person learns that their behavior makes no difference to their aversive environment, they may stop trying to escape from aversive stimuli even when escape is possible.
- Martin Seligman and Steven F. Maier first identified learned helplessness as a phenomenon in the 1960s. These psychologists conducted experiments on dogs, finding that, when exposed to repeated shocks that they could not control, the animals refrained from taking action when they could prevent the shocks.
- Learned helplessness has notably been linked to and used as an explanation for depression and post-traumatic stress disorder in humans, but not without criticism.
- There are a number of ways to overcome learned helplessness. One mentioned by Seligman himself is learned hopefulness.
What Is Learned Helplessness?
Learned Helplessness is a phenomenon where repeated exposure to uncontrollable stressors results in people failing to use any methods to control their response to those stressors that are at their disposal in the future.
Essentially, those experiencing learned helplessness are said to learn that they lack behavioral control over the events in their environment, which, in turn, undermines their motivation to make changes or attempt to alter situations.
The first people to describe learned helplessness were the American psychologists Steven F. Maier and Martin E. P. Seligman.
Martin Seligman conducted a series of classic experiments in the 1960s (Seligman & Maier, 1967). Some dogs were placed in a chamber where they received electric shocks from which they could not escape (the non-escape condition).
The dogs in the escape group could escape the shocks by pressing a panel with their nose.
In the second phase, the animals were placed in a shuttle box divided by a barrier in the middle so that the dogs could jump in order to escape the shocks. Only the dogs that had learned to escape in the previous phase tried to jump. The other dogs did not.
When the dogs in the “non-escape” condition were given the opportunity to escape the shocks by jumping across a partition, most failed even to try; they seemed just to give up and passively accept any shocks the experimenters chose to administer.
In comparison, dogs who were previously allowed to escape the shocks tended to jump the partition and escape the pain.
3 symptoms of learned helplessness
Martin Seligman, the psychologist who first described learned helplessness, identified three main features that characterize this behavior:
- Lack of motivation: When faced with new challenges or difficult situations, people with learned helplessness often fail to respond or even try. They feel like giving up before they start and have a low tolerance for even the smallest bumps in the road.
- Difficulty learning from success : Even when people with learned helplessness manage to cope with a situation successfully, they have trouble learning from that experience. They don’t see their success as a sign that they can handle similar challenges in the future.
- Emotional numbness : People with learned helplessness may seem less affected by painful or stressful events. They might appear to be emotionally flat or unresponsive.
However, later research found that even though people with learned helplessness might seem emotionally numb on the outside, they are actually experiencing high levels of stress on the inside.
Scientists discovered this by measuring cortisol levels, a stress hormone, in their blood (Ackerman, 2022).
Is learned helplessness a mental health condition?
Learned helplessness is not a diagnosable mental health condition but a thought disorder characterized by problematic thinking patterns that lead to maladaptive behavior.
Although not a standalone disorder, learned helplessness can feature in or exacerbate other mental health conditions such as anxiety, depression, phobias, and loneliness.
Symptoms of learned helplessness, including low motivation, perceived lack of control, and low self-esteem, overlap with those of depression and anxiety.
In the 1970s, Seligman extended the concept of learned helplessness from nonhuman animal research to clinical depression in humans and proposed a learned helplessness theory to explain how people become vulnerable to depression.
According to this theory, people who are repeatedly exposed to stressful situations beyond their control develop an inability to make decisions or engage effectively in purposeful behavior.
Subsequently, researchers have noticed that this learned helplessness theory is similar to posttraumatic stress disorder (Ackerman, 2022).
The Role of Explanatory Styles in Learned Helplessness
Although the initial learned helplessness theory was considered an important breakthrough in its time, it soon became accepted that the theory needed further development to apply to humans, who are more complex than other animals in terms of their cognitive processes.
Seligman and colleagues later reformulated the original learned helplessness model of depression (Abramson, Seligman, & Teasdale, 1978).
In their reformulation, they emphasized attributions (i.e., a mental explanation for why something occurred) that lead to the perception that one lacks control over negative outcomes and are important in fostering a sense of learned helplessness.
The explanatory style model of learned helplessness seeks to identify patterns in individual reactions to positive and negative events and occurrences in their lives.
The model’s logic is that when individuals find themselves in a situation where something has gone either right or wrong, they will ask why.
The answers that that person tends to give when asking themselves that kind of question will dictate whether that person defaults to an optimistic or pessimistic explanatory style (Healy, 2017).
Unhelpful : When a negative event occurs, if someone believes that the cause of the event is stable or long-lasting, this perspective can lead to chronic feelings of helplessness.
Helpful : When a negative event occurs, if someone believes that the cause is temporary, this perspective can reduce feelings of helplessness.
Unhelpful : If a person believes that the cause of a negative event will impact multiple areas of their life, they may be more susceptible to experiencing widespread helplessness.
Helpful : If a person believes that the cause of a negative event is specific to the issue at hand and will not affect other areas of their life, they will be less likely to experience helplessness.
Unhelpfu l: If someone attributes the cause of a negative event to their own actions or characteristics (an internal cause) rather than external factors, it can have negative consequences for their self-esteem.
In their writing on explanatory styles, Martin Seligman and Christopher Peterson (1967) stressed that one’s explanatory style will tend to follow a pattern. That means that someone will tend to respond to positive and negative events in consistent, habitual ways.
This can be very advantageous to someone’s well-being if they happen to default to an optimistic explanatory style, but very problematic for those who tend toward pessimism.
In fact, learned helplessness and a pessimistic explanatory style are each linked with the development of depression in individuals (Healy, 2017).
Optimistic vs. Pessimistic Explanatory Styles
The markers of an optimistic explanatory style stand in direct contrast to those signaling their pessimistic counterpart.
- For example, while the pessimistic style can view negative circumstances as something that will inevitably persist and positive occurrences as temporary, the optimistic style tends to view negative circumstances as temporary and expects positive occurrences to persist.
- Additionally, while the negative explanatory style tends toward self-blame for outcomes that go awry and credit external factors when things go right, the positive style leads to individuals crediting themselves when things go right and identifying external factors as key when things go wrong (Healy, 2017).
Nonetheless, moderation is required in considering the extent to which an optimistic explanatory style is the most beneficial for overcoming learned helplessness.
For example, always defaulting to blaming others or circumstances when things go wrong and always attributing successes as exclusively one’s doing can, while meeting the criteria for the optimistic explanatory style, constitute a problem in itself (Healy, 2017).
Overcoming Learned Helplessness
Ultimately, Learned helplessness provides an explanation for human behaviors that may otherwise seem odd or counterproductive, and understanding learned helplessness provides pathways to removing or reducing its negative impacts (Ackerman, 2022).
Focus on what you can control
Focusing on what you can control is a powerful way to combat learned helplessness. When you feel like everything is out of your control, it’s easy to give up and feel helpless.
But by shifting your focus to the things you can influence, you can start to regain a sense of power over your life.
For example, you might not be able to control whether or not you get a promotion at work, but you can control how much effort you put into your job.
You can’t control the weather, but you can control how you prepare for and respond to it.
Here are some things you can control:
- Your attitude : Choose to approach challenges with a positive, can-do mindset.
- Your effort : Decide how much time and energy you put into your goals.
- Your response : You can’t always control what happens to you, but you can control how you react to it.
- Your self-care : Prioritize taking care of your physical and mental health.
- Your relationships : Nurture the relationships that bring positivity into your life.
By focusing on these areas, you remind yourself that you have the power to influence your life, even in small ways.
This can help combat the feeling of helplessness and give you the confidence to tackle bigger challenges over time.
Learned optimism
Learned optimism, a concept introduced by Martin Seligman, is the antithesis of learned helplessness.
While learned helplessness involves internalizing a sense of hopelessness about one’s circumstances, learned optimism encourages individuals to challenge their negative thought processes and adopt a more positive outlook.
By doing so, people can change their behaviors and ultimately, their outcomes.
The process of developing learned optimism involves recognizing and questioning the automatic negative thoughts that contribute to feelings of helplessness.
When faced with a challenge or setback, individuals with learned optimism actively reframe their thoughts, looking for alternative explanations and solutions rather than defaulting to self-blame or despair.
For example, instead of thinking, “I failed because I’m not good enough,” a person practicing learned optimism might think, “This was a tough situation, but I can learn from it and do better next time.”
By consistently challenging negative self-talk and focusing on the aspects of a situation they can control, individuals can gradually shift their mindset from one of helplessness to one of resilience and empowerment.
Cultivating learned optimism takes time and practice, but it can have a profound impact on an individual’s well-being, motivation, and ability to overcome challenges.
By adopting a more optimistic outlook, people can break free from the cycle of learned helplessness and take active steps toward creating positive change in their lives.
Learn from failures
Carol Dweck, a psychologist, has found another powerful way to reduce learned helplessness, and it involves experiencing failure. In her research, Dweck divided people into two groups:
- The first group was given tasks that were designed for them to fail. After failing, they were told to take responsibility for their failure and to believe that it happened because they didn’t put in enough effort.
- The second group was given tasks that were easy enough for them to succeed every time. They never experienced failure during the study.
The results of Dweck’s (1975) study were interesting. The group that only experienced success showed no changes in how they reacted to failure later on. They still had extreme, negative reactions when they failed at something.
However, the group that experienced failure and was taught to take responsibility for it showed big improvements. They didn’t react as badly when they failed at something later on.
In simple terms, this study suggests that experiencing failure and learning to see it as a result of not trying hard enough, rather than a lack of ability, can help people overcome learned helplessness.
It teaches them that failure isn’t permanent and that they have the power to change the outcome next time by putting in more effort.
Learned hopefulness
Learned hopefulness is a concept that emphasizes the importance of empowering experiences in helping individuals overcome learned helplessness.
It suggests that by providing opportunities for people to learn new skills and develop a sense of control over their lives, they can become more resilient in the face of everyday challenges and barriers.
Unlike learned optimism, which focuses on changing thought patterns, learned hopefulness emphasizes the role of actual experiences in shaping one’s outlook and ability to cope with difficulties.
When individuals are exposed to situations that allow them to successfully navigate challenges, they develop a sense of mastery and control. This, in turn, helps them approach future obstacles with greater confidence and determination.
By fostering learned hopefulness through supportive environments and skill-building opportunities, individuals can break free from the cycle of learned helplessness and develop a more empowered, proactive approach to life.
This resilience can serve as a buffer against the negative effects of stress and adversity.
Overparenting and learned helplessness
Overparenting, often associated with “helicopter parents,” can inadvertently contribute to developing learned helplessness in adulthood.
When parents consistently intervene and solve their children’s problems, children may become overly dependent on their parents’ support.
This dependency can lead to a fear of failure and a belief that they are incapable of succeeding without their parent’s help.
While it can be difficult for parents to watch their children struggle, experiencing routine failures and challenges is essential to growing up.
These experiences teach children valuable skills such as problem-solving, coping with disappointment, and building resilience.
By facing and overcoming obstacles on their own, children develop a sense of self-efficacy and learn that they can navigate difficult situations.
While well-intentioned, overparenting can deprive children of these crucial learning opportunities, potentially leading to learned helplessness and a lack of confidence in their own abilities as adults.
Learned helplessness in education
Learned helplessness is a common subject of interest in the field of education. In particular, educators are interested in how early academic failure or low academic self-esteem can impact later success and how the relationship can be influenced to enhance chances of success (Firmin, Hwang, Copella, & Clark, 2004).
Learned helplessness in students creates a cycle where those who feel they are unable to succeed are unlikely to put effort into schoolwork. This, in turn, decreases their chances of success, leading to even less motivation and effort.
This cycle can culminate in a student having almost no motivation to learn a subject and no competence.
It can even lead to a more generalized sense of helplessness in which the student has no belief in their ability and no motivation to learn any subject at school (Firmin, Hwang, Copella, & Clark, 2004).
Educators have developed a few strategies that can help prevent students from learning to be habitually helpless, such as:
Providing praise and encouragement based on the student’s abilities to help them believe they are good at these subjects.
Providing praise and encouragement based on a student’s efforts.
Working on individual goal-setting with students to help them learn that goals can be achieved and that outcomes can be in their control (Firmin, Hwang, Copella, & Clark, 2004).
Learned helplessness in relationships
Learned helplessness is also of interest to researchers focused on domestic violence, as it’s often observed in relationships involving abuse.
The phenomenon of learned helplessness has helped researchers answer questions such as why those who are abused do not tell others, try to get help or leave the relationships (Ackerman, 2022).
Often, in abusive relationships, abusers subject their victims to repeated abuse to acclimatize the victims to the abuse and teach them that they do not have control over the situation.
The abusers, as a result, maintain complete control, and the victims learn that they are helpless about their circumstances (Ackerman, 2022). Often, these perceptions are very difficult to get rid of, often requiring intensive therapy and support (Ackerman, 2022).
Studies of learned helplessness in humans
Although experiments that are as extreme as Seligman’s have not been performed on humans — and would not pass ethically — experiments performed on humans have produced similar outcomes.
In one study of learned helplessness in humans, participants were split into three groups. One group was subjected to a loud and unpleasant noise but was able to end the noise by pressing a button four times, while the second group was subjected to the same noise, but the button was not functional.
Everyone was then given a box with a lever which, when manipulated, would turn off the sound. As in the animal experiments, those who had no control over the noise in the first part tended not even to try to turn the noise off, while the other participants did (Seligman, 1967; Ackerman, 2022).
Learned hopefulness at volunteer organizations
One example of an environment where individuals can learn hopefulness is voluntary organizations. Someone working at an after-school center, tutoring young children in mathematics and Seligman’s may be encouraged to see how their presence leads to students directly developing a better grasp of school material.
This may have run-off effects in other areas of the participant’s life. Zimmerman (1990) conducted a study of how empowered individuals felt after volunteering consistently in such environments, as measured by cognitive, personality, and motivational measures of perceived control.
He found that those who volunteered felt more in control of their own lives and were more likely to attribute their successes to their own actions (Zimmerman, 1990).
Criticisms of Learned Helplessness
Seligman’s original (1967) learned helplessness theory, as well as the reformulations of others, have received a number of criticisms.
Psychologists believe that there is more to depression than learned helplessness. While the symptoms of learned helplessness may mirror those of depression, there is an array of complex neurological and psychological factors underlying the condition.
Indeed, depression may not necessarily arise from a repeat failure.
For example, students may become depressed after repeatedly blaming themselves for chronic school stress and poor exam results.
Additionally, those in learned helplessness experiments have often described their task as skill tasks despite acting as if they were chance tasks.
That is to say, people participating in these learned helplessness experiments, while seemingly behaving as if they have no control over the outcome, have been known to say verbally that they still believe that their effort can influence its outcomes (Ackerman, 2022).
Abramson, L. Y., Seligman, M. E., & Teasdale, J. D. (1978). Learned helplessness in humans: critique and reformulation . Journal of abnormal psychology , 87 (1), 49.
Ackerman, C. (2022). Learned helplessness: Seligman’s Theory of Depression .
Dweck, C. S. (1975). The role of expectations and attributions in the alleviation of learned helplessness. Journal of personality and social psychology, 31 (4), 674.
Firmin, M. W., Hwang, C. E., Copella, M., & Clark, S. (2004). Learned helplessness: The effect of failure on test-taking. Education, 124 (4), 688.
Healy, C. (2017). Learned Helplessness & Explanatory Style .
Maier, S. F., & Seligman, M. E. (2016). Learned helplessness at fifty: Insights from neuroscience . Psychological Review, 123 (4), 349.
Seligman, M. E., & Maier, S. F. (1967). Failure to escape traumatic shock. Journal of experimental psychology, 74 (1), 1.
Seligman, M. E. (1972). Learned helplessness . Annual review of medicine , 23 (1), 407-412.
Thompson, J. A. (2010). Learned helplessness: You’re not trapped .
Zimmerman, M. A. (1990). Toward a theory of learned hopefulness: A structural model analysis of participation and empowerment. Journal of research in personality, 24 (1), 71-86.
Related Articles

Neurodiversity , Mental Health
How Cognitive Behavioral Therapy Can Help ADHD

How To Stop Being Passive-Aggressive

Dating Tips , Self-Care
How To Stop Being Insecure In A Relationship

Emotions , Self-Care
IQ vs EQ: Why Emotional Intelligence Matters More Than You Think

Signs of Low Emotional Intelligence

Mental Health
What Does Anorexia Feel Like? Living With An Eating Disorder

Common Causes of Stress and How They Impact Your Health
Many everyday occurrences can cause stress, and some may be more of a trigger for you than others.
What specifically causes or triggers stress can, of course, be different for everyone, says Alka Gupta, MD , the chief medical officer and the cofounder of Bluerock Care, a primary care facility for seniors in Washington, DC. “It’s really less about the so-called stressful event itself and more about your response, which arises from how you’re wired, what you’ve experienced in the past, and the strategies you’ve cultivated to cope with stressful situations,” she explains.
Still, certain causes of stress tend to be common for many people.
What Causes Stress?
On the broadest level, stress arises when events leave us feeling overwhelmed and out of control.
“Stress can come from any number of sources, whether it's trauma, difficult family relationships, health issues, or the dialogue in your own head,” says Michelle Dossett, MD, PhD, MPH , an assistant professor of medicine at Harvard Medical School and a staff physician at the Benson-Henry Institute for Mind Body Medicine at Massachusetts General Hospital in Boston. “Even what we think of as a happy event, like throwing a party, can be stressful.”
Here are the most common causes of stress.
“Money is tied to basic survival needs like food, shelter, and healthcare. Loss of income can mean big changes to your lifestyle and quality of life, such as needing to move or losing your health insurance,” says Seth J. Gillihan, PhD , a licensed psychologist in Pennsylvania and medical reviewer for Everyday Health.
Dr. Gillihan notes that finances can also stress us out because society equates wealth with self-worth and even morality, such as “assuming those who are less well-off must be ‘lazy’ or ‘undisciplined.’” We become stressed trying to make and hold onto money because we worry what others might think of us if our finances fall apart.
“With everyone connected to their digital devices, people are spending longer hours at work, even when they’re home — it’s harder to disconnect,” says Dr. Gupta. “That means we’re spending less time with family and friends, which makes things more stressful.”
The responsibilities that accompany raising kids can bring a roller coaster of emotions, including stress.
“The daily demands of parenting add to the list of what you’re expected to do, regardless of what’s going on with your job, your health, how much sleep you got last night, or other commitments,” Gillihan says.
In addition, parents face the difficult combination of high responsibility and low control. “You want the best for your kids in every way, and society largely blames parents for how kids turn out, and yet you have limited power to direct your children’s choices and the course of their life,” Gillihan explains. Many parents aim for perfection, only to inevitably fall short.
“Our politics have gotten so tense and heated, and that conflict makes politics a really difficult space for a lot of us,” Gillihan says. People worry about losing legal rights and protections, the fairness of elections, and what the other side will do if they win.
“Add the major conflicts around the world like in Ukraine and Gaza, and the role of politics in how our leaders respond to those conflicts, and it’s easy to see how political issues tap into deep fears around safety and security,” Gillihan says.
Health Issues
Getting — and, later, managing — a medical diagnosis such as type 2 diabetes , heart disease , and cancer can have a significant impact on your daily stress levels.
“Your health is foundational for so many of the most important parts of your life — your ability to work, do activities you enjoy, spend time with other people, and take care of your loved ones,” Gillihan says.
When you don’t feel well, it can create a cascade of other stressors, including loss of income, expensive medical bills, missing out on opportunities, relationship conflict, and worry over whether you’ll recover, he adds.
Mental health conditions such as depression , anxiety , post-traumatic stress disorder (PTSD) , and bipolar disorder are also often a major source of stress. Not only can they make stress harder to cope with, but they can add stress to your daily life.
“[Mental health conditions] often lead to a lot of impairment, meaning it’s hard to take care of important things in your life such as being present at work or cooking meals for your family,” Gillihan explains.
He notes that mental health conditions can also strain relationships. There may be conflict over not feeling supported or understood, disagreements about the best way to treat the condition, or if treatment is even necessary. This often adds an extra layer of stress.
Major Life Changes
Significant life events — whether positive or negative — can cause stress. Divorce, marriage, the birth of a child, moving to a new home, the death of a loved one, and losing or gaining a job can impact your well-being.
For example, while marriage and the birth of a child are often happy moments, both come with added responsibilities and disruptions to your typical routine. You may feel stressed trying to adapt to your “new normal.”
Learn How to Identify Your Stress Triggers
Stress is so commonplace, it’s common to feel stressed and not know exactly why. “I see that all the time,” says Gupta.
“I think many of us don't make the connections between situations and our stress response,” Gillihan adds. You may sense that work, money, or health issues are causing stress, but can’t pinpoint why.
For example, perhaps you tend to commit to too many work projects with deadlines far off in the future, only to wonder how you ended up with too much on your plate once the deadlines start piling up.
Learning how to recognize personal patterns that trigger your stress is a crucial first step toward minimizing or managing stress . In the above example, you might recognize that you tend to overestimate how much free time you’ll have weeks from now, and that this triggers your stress response, Gillihan says. This way, you can be more careful about which projects you say “yes” to.
To determine your stress triggers, begin by noticing how your body reacts to different situations and watch for patterns (or write them down).
It’s also helpful to look for thinking patterns that turn up your stress levels. “Sometimes, it’s not the situation or the person, but your beliefs that are driving the stress,” Gillihan notes.
For example, let’s say you’re running late and you tell yourself, “It will be terrible if I’m late.” In this instance, it’s not necessarily the tardiness that’s turning on your stress response — it’s your mind’s story about being late. “Once you know what stressful stories your mind is telling, you can start to question whether they’re really true,” Gillihan says.
What to Do if You’re Struggling With Stress
No one can avoid stress in their life full stop. Simple techniques, like deep breathing , time outdoors, and meditation , are all tools that can help you face the stressors that show up .
But if the stress you’re facing is challenging and feels overwhelming, there are a lot of steps you can take to better cope with it, too.
Gupta recommends talking things out with your doctor, a therapist or counselor, or someone who knows you well. “Often, it’s possible for me to get to the heart of a patient’s stress just by listening and continuing to dig deeper.” Other times, some type of therapy can do the trick. Whatever route you choose, “the key is to adopt an openness and willingness to explore,” says Gupta.
Moreover, a therapist can help you figure out healthy ways to cope with stress, as it’s probably easier and more effective to learn techniques for managing stress than it is to try to control the causes. “It’s tempting to try to avoid whatever stresses you out,” says Gupta. “But it’s more beneficial to learn coping skills and tools for managing stress, like problem-solving, time management, and mindfulness .”
Additional reporting by Lauren Bedosky.
Editorial Sources and Fact-Checking
Everyday Health follows strict sourcing guidelines to ensure the accuracy of its content, outlined in our editorial policy . We use only trustworthy sources, including peer-reviewed studies, board-certified medical experts, patients with lived experience, and information from top institutions.
- Stress Effects on the Body. American Psychological Association. March 8, 2023.
- Understanding the Stress Response. Harvard Health Publishing. April 3, 2024.
- Stress in America 2023. American Psychological Association. November 2023.
- Managing Your Stress in Tough Economic Times. American Psychological Association. November 3, 2023.
- State of the Global Workplace: 2023 Report. Gallup. 2023.
- Ford BQ. The Political Is Personal: The Costs of Daily Politics. Journal of Personality and Social Psychology: Attitudes and Social Cognition . July 2023.

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- HHS Author Manuscripts
Stress, coping, and depression: testing new hypotheses in a prospectively studied general population sample of U.S. born Whites and Blacks
1 Department of Epidemiology, Columbia University, New York, NY
The scarcity of empirically supported explanations for the Black/White prevalence difference in depression in the U.S. is a conspicuous gap in the literature. Recent evidence suggests that the paradoxical observation of decreased risk of depression but elevated rates of physical illness among Blacks in the U.S. compared with Whites may be accounted for by the use of coping behaviors (e.g., alcohol and nicotine consumption, overeating) among Blacks exposed to high stress levels. Such coping behaviors may mitigate deleterious effects of stressful exposures on mental health while increasing the risk of physical ailments. The racial patterning in mental and physical health outcomes could therefore be explained by this mechanism if a) these behaviors were more prevalent among Blacks than Whites and/or b) the effect of these behavioral responses to stress was differential by race. The present study challenges this hypothesis using longitudinal, nationally-representative data with comprehensive DSM-IV diagnoses. Data are drawn from 34,653 individuals sampled in Waves 1 (2001-2002) and 2 (2004-2005) as part of the US National Epidemiologic Survey on Alcohol and Related Conditions. Results showed that a) Blacks were less likely to engage in alcohol or nicotine consumption at low, moderate, and high levels of stress compared to Whites, and b) there was a significant three-way interaction between race, stress, and coping behavior for BMI only (F=2.11, df=12, p=0.03), but, contrary to the hypothesis, elevated BMI was protective against depression in Blacks at low, not high, levels of stress. Further, engagement in unhealthy behaviors, especially at pathological levels, did not protect against depression in Blacks or in Whites. In sum, the impact of stress and coping processes on depression do not appear to operate differently in Blacks versus Whites. Further research testing innovative hypotheses that would explain the difference in Black/White depression prevalence is warranted.
Introduction
Epidemiologic studies have consistently documented that Blacks living in the United States have higher rates of physical illness such as hypertension and diabetes, and higher rates of mortality, compared with non-Hispanic Whites controlling for indicators of socio-economic position (SEP) ( Heckler 1985 ; McCord and Freeman 1990 ; Williams and Jackson 2005 ). Conversely, major psychiatric epidemiologic household surveys have reported that Blacks have equal or lower rates of most psychiatric disorders, including major depression ( Kessler, McGonagle et al. 1994 ; Hasin, Goodwin et al. 2005 ; Breslau, Aguilar-Gaxiola et al. 2006 ; Williams, Gonzalez et al. 2007 ). These divergent patterns for mental and physical health outcomes have been termed a ‘paradox’ ( Williams 2001 ). Blacks in the U.S. face historic and contemporary institutionalized discrimination which exposes them to disadvantaged SEP, worse living conditions, and greater stress and adversity due to marginalized social status ( Kessler, Mickelson et al. 1999 ; Kreiger 2000 ; Williams and Williams-Morris 2000 ), all of which seemingly place Blacks at greater risk for depression compared with Whites ( Dohrenwend 2000 ). Indeed, among Blacks in the U.S., perception of discrimination and adversity due to race is associated with greater psychological distress and depressive symptoms ( Kessler, Mickelson et al. 1999 ; Williams and Williams-Morris 2000 ). However, absolute rates of depression remain lower among Blacks compared with Whites.
Many pathways have been posited to explain the elevated rates of physical health problems among Blacks in the U.S. compared with Whites. One well-studied mechanism is stress associated with disadvantaged social status. The physiologic responses to stress via allostatic load have been hypothesized to influence health by a process of ‘wear and tear’ whereby the body can no longer effectively regulate itself ( McEwen 2000 ; McEwen 2004 ). “Weathering” ( Geronimus 1994 ; Geronimus 1996 ), which describes a process of accelerated aging as an effect of the cumulative experience of stress and adversity, has been hypothesized to explain why Blacks have lower birthweights as well as higher mortality at younger ages than Whites after controlling for SEP. Further, interpersonal discrimination appraised by the individual as negative can result in fear, anger, and denial, thereby inducing injurious physiologic responses in cardiovascular, endocrine, neurologic and immune systems ( Krieger 1990 ; Krieger and Sidney 1996 ; Kreiger 2000 ). Adverse neighborhood conditions, to which Blacks have greater exposure than Whites, can influence health through inadequate access to social and health services, exposures to health hazards, and reduction in social cohesion and connectedness ( Massey 1985 ; Massey 2004 ). Greater stress, worse bodily wear and tear, reduced access to medical services, and greater exposure to deleterious neighborhood conditions are all risk factors for depression ( Leonard 2000 ; McEwen 2003 ; Stansfeld 2005 ), and yet Blacks consistently generate estimates of depression below those of Whites; this poses a perplexing, unresolved issue for social and psychiatric epidemiology.
Two methodological hypotheses advanced to explain this mental/physical health paradox posit that rates of depression among Blacks are underestimated in major psychiatric epidemiologic studies due to selection bias and measurement error. The selection bias hypothesis reflects the fact that all major psychiatric epidemiologic surveys conducted in the U.S. exclude institutionalized populations. Young Black men in the U.S. are overrepresented in prison and jail populations ( Petit and Western 2004 ), where depression is more prevalent compared with household populations ( Teplin 1990 ; Teplin, Abram et al. 1996 ). Thus, the underestimation of depression prevalence in household samples could affect Blacks to a greater extent compared with Whites, though the effect of this bias would primarily be age- and gender-specific. The measurement error hypothesis suggests potential diagnostic bias in the major survey instruments used to capture depression. Given the same symptom presentation, Blacks interviewed by clinicians in unstructured or semi-structured formats are more likely to be diagnosed as having a disorder in the psychotic spectrum and Whites as having a disorder in the mood spectrum ( Neighbors, Trierweiler et al. 1999 ; Neighbors, Trierweiler et al. 2003 ; Strakowski, Keck et al. 2003 ). Additionally, some argue that depression may manifest differently in Blacks compared with Whites, and current diagnostic nosology more appropriately captures depression in Whites compared with Blacks ( Rogler 1999 ; Baker 2001 ; Brown 2003 ; Kleinman 2004 ). Available data suggest that while these hypotheses may explain some of the Black/White difference in depression, methodological issues cannot account for the all of the difference ( Williams, Gonzalez et al. 2007 ; Breslau, Javaras et al. 2008 ). Thus, hypotheses exploring alternative mechanisms through which Blacks may have a lower prevalence of depression compared with Whites remain necessary.
In contrast to methodological hypotheses explaining the mental/physical health ‘paradox’, a recently advanced alternative hypothesis is that the patterning in physical and mental health outcomes in Blacks versus Whites arises from mechanisms for coping with stressors that on average operate differently for Black and White Americans ( Jackson and Knight 2006 ; Jackson, Knight et al. 2009 ). Jackson and colleagues have argued that Blacks in the U.S. face greater, and unique, stressors compared with Whites, and that strategies deployed to cope emotionally with this increased stress may protect mental health while having deleterious consequences for physical health. Recently, Jackson and colleagues reported that at high levels of stress, Blacks with elevated body mass index (BMI) and/or who smoke cigarettes and/or drink alcohol (collectively termed ‘unhealthy behaviors’ or ‘UHBs’ ( Jackson, Knight et al. 2009 )) were less likely than Blacks not engaging in these behaviors to develop depression, whereas the pattern trended in the opposite direction for Whites ( Jackson, Knight et al. 2009 ). Further empirical support for this hypothesis was recently reported using data from the Baltimore Epidemiologic Catchment Area Study ( Mezuk, Rafferty et al. 2010 ). Evidence indicates that UHBs can ameliorate immediate anxiety and depressive symptoms in response to stressful experiences by regulating corticotropin-releasing factor in the hypothalamic-pituitary-adrenalcortical (HPA) axis ( Benowitz 1988 ; Koob, Roberts et al. 1998 ; Dallman, Pecoraro et al. 2003 ). However, long-term heavy alcohol consumption, smoking, and high BMI can lead to a cascade of physical health consequences. This hypothesis suggests that, in the context of chronic stress, Blacks’ engagement in UHBs may serve to buffer the deleterious consequences of stress on depression through the HPA pathway, leading to a lower prevalence of depression but a greater prevalence of physical health problems than would have otherwise occurred. This hypothesis also suggests that the same processes operate differently or with different consequences in Whites. In the interest of brevity, we refer to these potentially differential patterns in the relationships between stress, coping, and depression between Blacks and Whites as “group-specific,” meaning that they arise from the unequal distribution of exposures and coping resources engendered by a racialized environment, rather than differences embedded in the individual.
Differences in stress and coping processes between Blacks and Whites could account for the mental/physical health ‘paradox’ under two scenarios. (1) UHBs are indeed protective against depression, among both Blacks and Whites, but Blacks are much more likely to engage in them compared with Whites at a given level of stress. This is unlikely in light of previous epidemiologic evidence suggesting that a) substance disorders and obesity are comorbid with depression ( Reiger, Farmer et al. 1990 ; Kessler, Crum et al. 1997 ; Hasin, Goodwin et al. 2005 ) and b) Blacks are less likely than Whites to engage in alcohol and nicotine consumption ( Grant, Hasin et al. 2004 ; Hasin, Stinson et al. 2007 ). However, patterns of comorbidity and Black/White differences in depression at all levels of stress have not been investigated systematically. (2) UHBs operate differentially by race, whereby they protect against depression to a greater extent among Blacks compared with Whites (either overall or variably by level of stress). This hypothesis is supported by data from the Americans’ Changing Lives Survey ( Jackson, Knight et al. 2009 ) and the Baltimore Epidemiologic Catchment Area Study ( Mezuk, Rafferty et al. 2010 ), as described above.
We propose to comprehensively investigate each of the above scenarios in a large nationally representative prospective study of U.S. adults. The present study is intended to both replicate and extend the analyses presented in Jackson et al. (2009) to provide a comprehensive test of the underlying theory. Using the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC) we accomplish five main aims. First, we construct as exact a replication as possible of Jackson et al. (2009) in order to provide a baseline for comparison and from which to broaden the analyses. The remaining four aims systematically test the theory underlying the two scenarios outlined above. We examine whether alcohol consumption, nicotine consumption, and body mass index (as a proxy for overeating, consistent with Jackson et al., (2009) ) are prospectively protective against depression; we examine whether Blacks engage in more of these behaviors than Whites at low, moderate, and/or high levels of stress; and we test the hypothesis that Blacks exposed to high levels of stress are protected against depression if engaged in UHBs at the time of the stressors and, simultaneously, that Whites are not similarly conferred such protection from these behaviors. Finally, the hypothesis outlined by Jackson et al. (2009) suggests that the stress exposure of Blacks is qualitatively different compared to that of Whites. The NESARC data allows us to examine a measure of perceived racial discrimination in order to test whether Blacks who report high levels of discrimination and engage in UHBs have less depression than Blacks who report high levels of discrimination and do not engage in UHBs.
The data used in the present study have distinct advantages over those in ( Jackson, Knight et al. 2009 ): namely a larger sample size, DSM-IV diagnoses of major depression at two time points, DSM-IV diagnoses of nicotine dependence and alcohol use disorders, and comprehensive measures of nicotine, alcohol consumption, and stressful life events. Extending the analyses of Jackson et al, (2009) to include pathological alcohol and nicotine consumption is important in testing the hypothesis, as high and chronic levels of nicotine and alcohol use are behaviors most associated with poor physical health outcomes; if the Black/White “paradox” can be attributed to discrepant mental and physical health consequences of unhealthy behaviors, the nature and degree of engagement in those behaviors most implicated in poor somatic health should be considered.
Data are drawn from the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC), a two-wave longitudinal survey of adults in the United States residing in households and group quarters. Wave 1 was conducted in 2001-2002 (N=43,093); young adults, Hispanics and Blacks were oversampled, with an overall response rate of 81%. Respondents were re-interviewed for Wave 2 approximately three years after Wave 1, with 34,653 (80.4%) successfully re-interviewed. More information on the study methods is found elsewhere ( Grant, Goldstein et al. 2009 ). The research protocol, including written informed consent procedures, received full ethical review and approval from the U.S. Census Bureau and the U.S. Office of Management and Budget.
All measures were assessed using the Alcohol Use Disorder and Associated Disabilities Interview Schedule-DSM-IV Version (AUDADIS-IV). We used measures of race/ethnicity, UHBs, and stressful life events ascertained at Wave 1 and measures of the outcomes, major depression and physical illness, from Wave 2. This design established the temporality of the exposures as occurring prior to the outcome; we controlled for major depression at Wave 1 in all analyses for which depression at Wave 2 was an outcome to further establish temporal sequence.
Race/ethnicity
We included self-identified non-Hispanic Whites (N=19,216) and non-Hispanic Blacks (N=6,065) who reported being born in the U.S. Foreign-born Blacks (N=664) and Whites (N=1,264) were excluded from the present analysis because patterns of substance use, depression and stressful life events differ between foreign- and non-foreign born individuals.
‘Unhealthy behaviors’ (UHBs)
We considered three types of ‘UHBs’: alcohol consumption, nicotine consumption, and body mass index (BMI). While a compelling argument can be made regarding the validity of terming alcohol consumption, nicotine consumption, and BMI collectively as ‘UHBs’ (e.g., moderate consumption of alcohol may be cardioprotective ( Klatsky 2009 )), we have used this terminology to remain consistent with the prior empirical support for the hypothesis we are testing ( Jackson, Knight et al. 2009 ). For our replication analysis, we use definitions exactly consistent with Jackson, Knight et al. (2009) , namely a UHB count measure (0-3) indicating if the individual ever consumed at least one alcoholic beverage in their lifetime, ever smoked at least 100+ cigarettes in their lifetime, and whether they currently have a BMI≥30. For our extended test of the overall theory, we used the following definitions:
- Alcohol consumption in the past 12 -months at Wave 1 was operationalized as a three-level variable: no consumption (N=2,293); non-pathological consumption (i.e., any level of consumption but no alcohol abuse/dependence diagnosis) at levels less than weekly binge (>4 drinks for men or >3 drinks per women on at least one occasion in the past year) (N=13,765); and DSM-IV alcohol abuse/dependence or at least weekly binge drinking (N=8,593). Measurement of alcohol consumption and diagnoses is a particular strength of the AUDADIS-IV instrument; diagnoses are made based on assessment of over 40 symptom items, and the excellent reliability and validity of alcohol diagnosis in the AUDADIS-IV have been extensively documented both the United States and internationally (see Hasin et al., 2007 ). Limited differential item functioning by race/ethnicity has been noted for alcohol disorder criteria in Item Response Theory analysis ( Saha, Chou et al. 2006 ).
- Nicotine consumption in the past 12 -months at Wave 1 was operationalized as a three-level variable: no nicotine use (N=18,601); non-pathological use (any level of use but no DSM-IV-defined nicotine dependence diagnosis) (N=3,358); and DSM-IV nicotine dependence (N=3,313). The good reliability and validity of nicotine dependence in the AUDADIS-IV have been well-documented ( Grant, Hasin et al. 2004 ). Limited differential item functioning by race/ethnicity has been noted for nicotine dependence criteria in Item Response Theory analysis ( Saha, Compton et al. 2010 ).
- Unhealthy eating in the past 12 -months at Wave 1 was operationalized using current BMI based on respondent’s self-reported height and weight. BMI an imperfect proxy for unhealthy eating; BMI is known to be determined by more than simply caloric intake, including exercise patterns and genetic vulnerability ( Hetherington and Cecil 2010 ). However, empirical studies have documented a robust correlation between unhealthy eating and BMI (e.g., ( Haimoto, Iwata et al. 2008 ; Kent and Worsley 2009 )). Three categories were created: BMI<25 (N=10,252), BMI greater than or equal to 25 but less than 35 (N=12,615), and BMI≥35 (N=2,414). While conventional cut-points define overweight as BMI between 25 and <30 and obese as ≥30 ( Centers for Disease Control and Prevention 2010 ), we chose more conservative cut points due to known error in the measurement BMI ( Rothman 2008 ), often overestimating an individual’s true body size.
- UHB count . The three measures described above were combined to create an overall measure of UHBs, comparable to that in Jackson et al. (2009) . Respondents were given a score of 0 for the least severe level of each behavior (i.e., no alcohol consumption, no nicotine consumption, or BMI<25), one point for the moderate level, and two points for the most severe level (i.e., DSM-IV alcohol abuse/dependence or at-least weekly binge drinking, DSM-IV nicotine dependence, or BMI≥35) within each unhealthy behavior category. Based on this summary score, we created a three level variable indicating no unhealthy behaviors (count was equal to zero) (N=2,539), low levels of unhealthy behavior (count was 1, 2, or 3) (N=20,077), and high levels of unhealthy behaviors (count of 4 or more) (N=2,656).
Stressful life events in the past 12-months
Twelve stressful life events were assessed at Wave 1 using a checklist with dichotomous response options: family member or close friend had a serious illness (38.4%), family member or close friend died (32.1%), respondent changed jobs/job responsibilities/work hours (23.8%), moved or someone new came to live with respondent (15.8%), major financial crisis/unable to pay bills/bankruptcy (10.6%), trouble with a boss or co-worker (8.7%), unemployed and looking for work >1 month (7.7%), respondent or family member was the victim of a crime (6.7%), fired or laid off (5.9%), problems with neighbor/friend/relative (5.8%), separated/divorced/broke up (5.4%), and respondent or a family member had trouble with police/got arrested/sent to jail (5.1%).
Figure 1 shows the relationship between number of past year stressful life events, race, and depression. As shown, the number of stressful life events at Wave 1 was not linearly related to depression at Wave 2 among Blacks, though the difference in prevalence between Blacks and Whites was not statistically significantly different at any level of stressful life events save for among those with one stressful life event (p=0.04). Also shown in Figure 1 , the confidence intervals for the proportions substantially overlap, indicative of the small sample sizes among those with high levels of stress. Therefore, we created a categorical measure of the number of stressful life events reported by the respondent. We extensively evaluated the appropriate threshold for ‘high stress’, and found that the direction and magnitude of the results were not dependent on the upper cutpoint used. We also evaluated whether the data would fit a quadratic term for past year stressful life events; the results did not change when a quadratic term was used. Therefore, to maximize statistical power and to provide the best fit to these data, we used the following cut points: no stressful life events in the past-year (N=7,274), one or two stressful life events (N=11,832), and three or more (N=6,175). Finer categorizations could not be utilized due to the minimum cell sizes required to conduct large-sample statistics.

Prevalence of depression at Wave 2 by number of past year stressor among non-Hispanic U.S.-born Whites (N=19,216) and non-Hispanic U.S.-born Blacks (N=6,065) in the general population
Perceived discrimination
Respondents self-reporting Black race were asked at the Wave 2 interview, “How often have you experienced discrimination, been prevented from doing something, or been hassled or made to feel inferior in any of the following situations because of your race?” The frequencies of seven discrimination experiences in the past 12 months were assessed (e.g., obtaining health care or health insurance coverage, obtaining a job or while on the job, or being called a racist name) ( Krieger, Smith et al. 2005 ). The scale showed good internal consistency reliability (α=0.76) ( Ruan, Goldstein et al. 2008 ). Responses were summed and a three-level variable was created indicating: no discriminatory experiences reported (N=3,708), a low level of discriminatory experiences (more than zero but less than the 75 th percentile on the scale, N=1,753), and a high level of discriminatory experiences (75 th percentile or greater, N=604).
Major Depressive Episode (MDE)
The good reliability and validity of DSM-IV major depression diagnosis in the AUDADIS-IV have been well-documented ( Hasin, Goodwin et al. 2005 ). At Wave 1, major depression in the past 12-months or prior to the past 12-months was assessed; we combined these timeframes to create a W1 lifetime depression diagnosis, and used this variable as a control in all analyses predicting major depression at Wave 2. At Wave 2, major depression was assessed in the past 12-months, and since the last interview but prior to the past 12-months. We combined these times frames to create a W2 depression diagnosis.
Physical illness
We examined Black/White differences in fourteen physical illnesses (e.g., arteriosclerosis, hypertension, diabetes, heart attack, high cholesterol, ulcer) assessed at Wave 2. Physical illness status was based on respondent self-report of a physician diagnosis.
Control variables
In all analyses we also controlled for age, sex, past-year personal income, education, and region of residence as assessed at Wave 1. We also controlled for major depression at prior to the past-year or the past-year Wave 1; Blacks had a lower prevalence of past year (OR=0.80, 95% C.I. 0.66-0.96) and lifetime depression (OR=0.56, 95% C.I. 0.49-0.64) at Wave 1.
Statistical analysis
Prevalence estimates by race, stressful life events, and UHBs were generated using cross-tabulations. Odds ratios and 95% confidence intervals were generated using logistic regression. All interaction tests are on the multiplicative scale. All analyses were conducted using SUDAAN software to adjust standard errors for the non-random probability of selection into the sample. All prevalence estimates and odds ratios are sample weighted to be representative of the U.S. population based on the year 2000 census.
Overall Black/White differences in the NESARC data
Consistent with prior literature, Blacks were less likely to have Wave 2 major depression (OR=0.80, 95% C.I. 0.70-0.91) and more likely to have a Wave 2 physical illness (OR=1.20, 95% C.I. 1.08-1.35) compared with Whites (data not shown).
Results of the Jackson et al. (2009) replication attempt
Our findings did not replicate those of Jackson et al. (2009) . Figures 2a and 2b show the predicted probability of depression based on the results of a logistic regression model categorizing UHB consumption (any lifetime smoking, any lifetime drinking, and/or current obesity) and past-year stressful life events, and controlling for age, sex, past-year personal income, education, region of residence, and major depression at Wave 1. Among Whites, the figures indicate a higher predicted probability of depression with each increasing level of UHB consumption and each increasing level of stressful life events. Among Blacks, the pattern is less consistent, but no evidence emerges suggesting that those who engage in more UHB consumption have less depression. There were no significant interactions between stressful life events and UHBs predicting depression among Blacks (F=1.20, df=6, p=0.32) or Whites (F=0.43, df=6, p=0.86), and no significant three-way interaction between stressful life events, UHBs, and race (F=1.05, df=17, p=0.42).

Predicted probability of depression at Wave 2 based on unhealthy behaviors as defined by Jackson et al. (2009) * and past-year stressful life events at Wave 1, by race, among non-Hispanic U.S.-born Whites (Figure 2a, N=19,216) and non-Hispanic U.S.-born Blacks Figure 2b, N=6,065) in the general population
* UHBs defined to be consistent with Jackson et al. (2009) : any consumption of at least one alcoholic beverage in lifetime, any consumption of 100+ cigarettes in lifetime, and/or current BMI≥30.
As part of our replication attempt, we also conducted an analysis with a mean centered, continuous stress variable in order to more closely approximate Jackson et al. (2009) and Mezuk et al. (2010) , despite the evident violation of the linearity assumption among Blacks (shown in Figure 1 ). Among Blacks at high levels of mean-centered stress, those with 0 UHBs have a higher predicted probability of depression compared to those with 1 UHB, and those with 1 UHB have a higher predicted probability of depression compared to those with 2 or 3 UHBs (consistent with Jackson et al. (2009) and Mezuk et al. (2010) ). The same pattern is not evident among Whites (results not shown). However, this result arises entirely from the misspecification of the regression model by entering stress as a continuous variable among Blacks. Further, none of the interactions were significant when using the mean centered, continuous stress variable (interaction of stress and UHBs among Blacks: F=0.89, df=3, p=0.45; interaction of stress and UHBs among Whites: F=1.46, df=3, p=0.23; three way interaction of stress, UHBs, and race: F=1.37, df=7, p=0.23).
Results of the extended test of the Jackson et al hypothesis
Are uhbs protective against depression and is stress associated with more depression.
We found that Wave 1 UHBs, at any level, are not protective against Wave 2 depression. Stress, however, is prospectively predictive of Wave 2 depression. Table 1 shows the odds of Wave 2 depression given Wave 1 UHBs among the whole sample, and for Blacks and Whites separately. Among Whites, greater Wave 1 alcohol, nicotine, BMI severity, and overall UHB score predicted higher odds of depression at Wave 2. Among Blacks, no significant odds ratios were observed for the relation between Wave 1 UHBs and Wave 2 depression. However, all four odds ratios for the highest UHB category were in the direction consistent with high levels of UHB predicting greater odds of depression. Among both Whites and Blacks, more stressful life events at Wave 1 predicted greater odds of depression at Wave 2 (see Table 1 ).
Alcohol consumption, nicotine consumption, BMI, and stressful life events prospectively predicting major depression three years later among non-Hispanic U.S.-Born Whites (N=19,216) and non-Hispanic U.S-born Blacks (N=6,065)
Bold text indicates statistical significance at p<0.05
AOR = odds ratio adjusted for age, sex, past-year personal income, education, region of residence, and major depression at Wave 1
Do Blacks report higher levels of UHBs?
Blacks had lower odds of Wave 1 alcohol consumption, nicotine consumption, and any UHBs compared with Whites, but a higher proportion of Blacks were in high Wave 1 BMI categories compared with Whites. This finding held in every level of Wave 1 stressful life events (see Table 2 ) save the lowest level. Among those with no stressful life events, there was no significant relationship between UHBs and race. The magnitude and strength of the relationship between UHB and race increased with each level of stressful life event category.
Odds of alcohol consumption, nicotine consumption, high BMI, and ‘unhealthy behaviors’ in non-Hispanic U.S.-born Blacks (N=6, 065) compared to non-Hispanic U.S.-born Whites (N=19,216) at low, moderate, and high levels of stress
AOR = odds ratio adjusted for age, sex, past-year personal income, education, and region of residence
Do UHBs have a differential effect on depression among Blacks and Whites at certain stress levels?
Little support was found for the hypothesis that UHBs have a differential effect on Blacks and Whites at high levels of stress. We examined whether the effect of Wave 1 UHBs on Wave 2 depression differed by race and Wave 1 stressful life event status ( Table 3 ). Results indicated that a low level of unhealthy behaviors is protective against depression in Blacks (OR=0.06, 95% C.I. 0.01-0.24) but not Whites (OR=2.14, 95% C.I. 0.71-6.48) among those at low levels of stress. However, the three-way interaction test was not significant, limiting the conclusions that can be drawn from this association. We did find a significant three-way interaction between race, Wave 1 stress, and Wave 1 BMI (F=2.11, df=12, p=0.03). Based on the patterns of odds ratios shown in Table 3 , we conclude that there is evidence to suggest a protective effect of Wave 1 BMI 25-34 on Wave 2 depression in Blacks but not Whites, but only at very low levels of stress.
Odds of depression at Wave 2 based on unhealthy behaviors and past-year stressful life events at Wave 1, by race and sex, among non-Hispanic U.S.-born Blacks (N=6,065) and non-Hispanic U.S.-born Whites (N=19,216) in the general population
We also examined these patterns by sex (results not shown). UHBs significantly interacted with race among men only (F=6.07, df=2, p=0.004), whereby Black men reporting a low level of unhealthy behaviors had significantly lower odds of depression compared to White men (OR=0.06, 95% C.I. 0.01-0.24). Similar to the aggregated analysis, a three way interaction between Wave 1 BMI, race, and Wave 1 stress was statistically significant in men (F=2.28, df=12, p=0.02). This interaction was significant at the trend level among women (F=1.7, df=12, p=0.09).
Are UHBs protective against depression among Blacks reporting more race-specific stress?
Wave 1 UHBs did not moderate the effect of perceived discrimination reported at Wave 2 among Blacks. The observed prevalence of Wave 2 depression by UHB consumption and discrimination experiences are shown in Figure 3 . In unadjusted analyses, Wave 1 non-pathological nicotine use was associated with a lower odds of depression at Wave 2 compared to no nicotine use (OR=0.48, 95% C.I. 0.24-0.96) (data not shown). However, the effect was no longer significant when lifetime depression at Wave 1 was controlled (OR=0.52, 95% C.I. 0.26, 1.05) (data not shown). No other odds ratios were significant in unadjusted or adjusted analyses. We also replicated these analyses using UHBs defined at Wave 2 (concurrent to measurement of discrimination): results were unchanged.

Prevalence of depression at Wave 2 based on unhealthy behaviors and lifetime perceived discrimination exposure among non-Hispanic U.S.-born Blacks (N=6,065) in the general population
The present study did not find support for the hypothesis that engaging in unhealthy behaviors ameliorates major depression among Blacks in the U.S. exposed to high levels of stress, or that a differential effect of UHBs on depression among Blacks compared with Whites accounts for the mental/physical health paradox. First, we showed that the results presented in Jackson et al. (2009) and Mezuk et al (2010) do not replicate in a nationally-representative sample using model specification to account for the non-linear association between stress and depression among Blacks that we observed in these data. Next, as part of a more in-depth investigation of the hypothesis, we demonstrated that the relationship between depression and alcohol consumption, nicotine consumption, and BMI among Blacks is not statistically significant and, in fact, the direction of association between UHBs and depression is positive, not negative. Third, we documented that Blacks are less likely to engage in alcohol and nicotine consumption but have higher BMI than Whites at all levels of stress. We note, however, that an overall count of UHBs was not associated with race among those with no stressful life events. This suggests a complex patterning of unhealthy behaviors and race across stress levels that should be more comprehensively examined in these and other data in future analyses.
Finally, we showed that while race, stress, and BMI did interact significantly to predict depression in this sample, being overweight was protective against depression among Blacks only at very low levels of stress . Similarly, among those with no stressful life events, we found that low levels of UHBs were associated with less depression in Blacks but not Whites, though this result was significant among men only and a three-way interaction test was not significant. Furthermore, examination of perceived discrimination as a measure of stress in Blacks revealed no significant effects of unhealthy behaviors on depression at any exposure level. Taken together, these results indicate that engagement in unhealthy behaviors, especially at pathological levels, does not protect against depression, and that stress pathways do not operate differently in Blacks compared with Whites in the U.S. Thus, our confidence in the group-specific stress and coping hypothesis proposed by Jackson and colleagues ( Jackson and Knight 2006 ; Jackson, Knight et al. 2009 ; Mezuk et al. 2010 ) is diminished. Although UHBs may have immediate positive psychological effects via the HPA axis, the evidence presented here suggests these effects are not robust enough to prevent the clinical manifestation of major depression.
We did find evidence that some measures of unhealthy behaviors were significant predictors of depression in Whites but not Blacks. For example, at high levels of stress, Whites with high BMI, nicotine dependence, and a high unhealthy behavior count were more likely to evidence depression compared with Whites without these unhealthy behaviors, but the same predictors were not significant among Blacks. However, we caution against over-interpretation of these findings; as noted by Gelman and Stern: “The Difference Between ‘Significant’ and ‘Not Significant’ is not Itself Statistically Significant” ( Gelman and Stern 2006 ). There were no significant interactions between race and unhealthy behaviors at high levels of stress, indicating that the odds ratios across race categories were not statistically distinguishable. Further, ignoring significance levels, thirty-two of forty-eight odds ratios calculated (67%) in the total sample were in the same direction for Whites and Blacks. Thus, the most appropriate conclusion from these data is the pathway through which unhealthy behaviors and stress impact depression does not differ in Blacks compared with Whites in the U.S., and that in general, UHBs increase the risk for depression at all levels of stress.
In the present analysis we predicted major depression during a three-year follow-up based on stressful events and UHBs assessed at baseline. While this strategy is most appropriate to establish temporality, it may overlook a key component of the hypothesis, namely, that UHBs in response to stress are active coping strategies for the suppression of immediate depressive symptoms ( Benowitz 1988 ; Koob, Roberts et al. 1998 ; Dallman, Pecoraro et al. 2003 ; Jackson and Knight 2006 ; Jackson, Knight et al. 2009 ). Thus, we may have failed to capture protective effects because we did not examine major depressive episodes concurrent with stressors and unhealthy behaviors. To explore this possibility, we re-analyzed our data using stress, UHBs and depression diagnoses all measured concurrently, at both baseline and follow-up. Neither analysis suggested different conclusions; results were generally consistent with those presented in our main analyses. Thus, we conclude that these data, analyzed multiple ways at multiple time points, do not provide sufficient evidence for either a protective effect of UHBs on depression, or a differential pathway through which unhealthy behaviors affect depression in Blacks compared with Whites, regardless of the exposure to stress.
These results decrease confidence in the validity of the hypothesis that group-specific stress processes explain the depression difference in Blacks and Whites, leaving open other theories to be tested. Measurement and selection bias hypotheses are unlikely to fully explain the “paradox” ( Breslau, Javaras et al. 2008 ), suggesting the need for both new theories and more direct tests of existing theories based on the premise that the lower prevalence of depression in Blacks is not artefactual. Studies suggest that Blacks develop different coping strategies when faced with life stress compared with Whites ( Smith 1985 ; Wilson 1989 ; Maton, Teti et al. 1996 ), which, given the extraordinary nature and degree of stress to which Blacks are exposed starting at a young age, are hypothesized to develop over the life course. Compared with Whites, Blacks are more likely to find emotional strength and support in religious communities ( Taylor, Chatters et al. 1996 ; Gibson and Hendricks 2006 ; Giger, Appel et al. 2008 ), and develop racial self-esteem and strong ethnic identity ( Nagel 1994 ). Further, extensive research has documented the ‘John Henryism’ effect among Blacks in the U.S., the personality trait characterized by active coping with stressful and negative experiences and associated with worse health outcomes for Blacks at high levels of socio-economic position ( James, Strogatz et al. 1987 ; James 1994 ). Alternatively, the present DSM nosology may not accurately tap Black psychological responses to their unique stress exposures, and therefore DSM-IV depression as currently defined may not be the appropriate outcome to fully understand racial differences in depressive mood states ( Brown 2003 ; Kendrick, Anderson et al. 2007 ). Support for this theory can be drawn from the multiple studies showing that Blacks report lower levels of well-being, higher levels of distress, and higher depressive scores when measured on non-DSM instruments ( Brown 2003 ; Mabry and Kiecolt 2005 ). Taken together, the results from the present study should serve as a catalyst to promote the advancement of innovative and alternative theories to explain the Black/White paradox in mental and physical health. Few studies are conducted with the primary aim of untangling this paradox, a situation that should be redressed. Such research should include rich measurement of the social and political context, and conduct in-depth examination of the role of ethnic identity, religion, and responses to group-specific stressor, such as racial discrimination.
Several limitations should be noted. First, our measure of stressful life events is a checklist of experiences susceptible to respondent subjectivity and appraisal processes, and without regard to salience, severity, or context of experience. Substantial evidence indicates that objective measures of stressful experiences as well as information on the context of the experience is necessary to fully analyze and interpret stress in mental health research ( Dohrenwend 1998 ; Dohrenwend 2006 ). Additionally, the stressful events experienced by Blacks in the U.S. may be more chronic and race-specific than what is captured in the scale of past-year stressors ( Jones 2000 ; Kreiger 2000 ). We attempted to mitigate this limitation by also using a measure of perceived racial/ethnic discrimination. Further, we evaluated whether results changed if higher cut-offs of past-year stressful experiences were used to define the ‘high stress’ exposure group; higher cut-offs did not change the results. Thus, the conclusions from these data are limited by the available stress measure.
In conclusion, the persistent differences in health outcomes between White and Black adults remain one of the most challenging public health issues in the U.S. As theories regarding the etiology of these differences continue to develop, the mental health ‘paradox’ will be increasingly important to explain as part of a robust etiologic pathway. Substantive etiologic hypotheses that simultaneously explain why Blacks in the U.S. have higher rates of physical illness and lower rates of mood disorders need to be tested directly in order to resolve the ‘paradox’ and progress toward intervention and prevention efforts.
Hypothesis that Black-White depression paradox is due to protective effects of unhealthy behaviors at high stress unsupported.
Blacks less likely to engage in alcohol consumption or cigarette smoking compared with Whites, but have higher average BMI.
Engaging in unhealthy behaviors is not protective against depression at any stress level in either Blacks or Whites.
Acknowledgments
This research was supported in part by a fellowship from the National Institute of Mental Health (T32MH013043-36, Barnes) and a fellowship from the National Institute of Drug Abuse (F31-DA026689, K. Keyes).
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
- Baker FM. Diagnosing depression in African Americans. Community Mental Health Journal. 2001; 37 (1):31–38. [ PubMed ] [ Google Scholar ]
- Benowitz NL. Drug therapy. Pharmacologic aspects of cigarette smoking and nicotine addition. N Engl J Med. 1988; 319 (20):1318–30. [ PubMed ] [ Google Scholar ]
- Breslau J, Aguilar-Gaxiola S, et al. Specifying race-ethnic differences in risk for psychiatric disorder in a USA national sample. Psychol Med. 2006; 36 (1):57–68. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Breslau J, Javaras KN, et al. Differential item functioning between ethnic groups in the epidemiological assessment of depression. J Nerv Ment Dis. 2008; 196 (4):297–306. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Brown T. Critical race theory speaks to the sociology of mental health: mental health problems produced by racial stratification. Journal of Health and Social Behavior. 2003; 44 (3):292–301. [ PubMed ] [ Google Scholar ]
- Centers for Disease Control and Prevention. 2010. http://www.cdc.gov/healthyweight/assessing/bmi/adult_bmi/index.html .
- Dallman MF, Pecoraro N, et al. Chronic stress and obesity: a new view of “comfort food” Proc Natl Acad Sci U S A. 2003; 100 (20):11696–701. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Dohrenwend BP. Adversity, stress, and Psychopathology. New York: Oxford University Press, USA; 1998. [ Google Scholar ]
- Dohrenwend BP. The role of adversity and stress in psychopathology: some evidence and its implications for theory and research. J Health Soc Behav. 2000; 41 (1):1–19. [ PubMed ] [ Google Scholar ]
- Dohrenwend BP. Inventorying stressful life events as risk factors for psychopathology: Toward resolution of the problem of intracategory variability. Psychol Bull. 2006; 132 (3):477–95. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Gelman A, Stern H. The Difference Between “Significant” and “Not Significant” is not Itself Statistically Significant. American Statistician. 2006; 60 (4):328–331. [ Google Scholar ]
- Geronimus AT. Power and Decision: The Social Control of Reproduction. Cambridge, MA: Harvard University Press; 1994. The weathering hypothesis and the health of African American women and infants: Implicatins for reproductive strategies and policy analysis. [ Google Scholar ]
- Geronimus AT. Black/White differences in the relationship of maternal age to brithweight: A population basd test of the weathering hypothesis. Soc Sci Med. 1996; 42 (4):589–597. [ PubMed ] [ Google Scholar ]
- Gibson LM, Hendricks CS. Integrative review of spirituality in African American breast cancer survivors. ABNF J. 2006; 17 (2):67–72. [ PubMed ] [ Google Scholar ]
- Giger JN, Appel SJ, et al. Church and spirituality in the lives of the African American community. J Transcult Nurs. 2008; 19 (4):375–83. [ PubMed ] [ Google Scholar ]
- Grant BF, Goldstein RB, et al. Sociodemographic and psychopathologic predictors of first incidence of DSM-IV substance use, mood and anxiety disorders: results from the Wave 2 National Epidemiologic Survey on Alcohol and Related Conditions. Mol Psychiatry. 2009; 14 (11):1051–66. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Grant BF, Hasin DS, et al. Nicotine dependence and psychiatric disorders in the United States: results from the national epidemiologic survey on alcohol and related conditions. Arch Gen Psychiatry. 2004; 61 (11):1107–15. [ PubMed ] [ Google Scholar ]
- Haimoto H, Iwata M, et al. Long-term effects of a diet loosely restricting carbohydrates on HbA1c levels, BMI and tapering of sulfonylureas in type 2 diabetes: a 2-year follow-up study. Diabetes Res Clin Pract. 2008; 79 (2):350–6. [ PubMed ] [ Google Scholar ]
- Hasin DS, Goodwin RD, et al. Epidemiology of major depressive disorder: results from the National Epidemiologic Survey on Alcoholism and Related Conditions. Arch Gen Psychiatry. 2005; 62 (10):1097–106. [ PubMed ] [ Google Scholar ]
- Hasin DS, Stinson FS, et al. Prevalence, correlates, disability, and comorbidity of DSM-IV alcohol abuse and dependence in the United States: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Arch Gen Psychiatry. 2007; 64 (7):830–42. [ PubMed ] [ Google Scholar ]
- Heckler MM. Report of the Secretary’s Task Force on Black and Minority Health. Wasington, DC: Natl. Academy Press; 1985. Task Force on Black and Minority Health. [ Google Scholar ]
- Hetherington MM, Cecil JE. Gene-environment interactions in obesity. Forum Nutr. 2010; 63 :195–203. [ PubMed ] [ Google Scholar ]
- Jackson JS, Knight KM. Race and self-regulatory behaviors: the role of the stress response and HPA axis in physical and mental health disparities. In: Carstensen LL, Schaie KW, editors. Social structure, Aging, and Self-Regulation in the Elderly. New York, NY: Springer; 2006. [ Google Scholar ]
- Jackson JS, Knight KM, et al. Race and Unhealthy Behaviors: Chronic Stress, the HPA Axis, and Physical and Mental Health Disparities Over the Life Course. Am J Public Health 2009 [ PMC free article ] [ PubMed ] [ Google Scholar ]
- James SA. John Henryism and the health of African Americans. Culture of Medicine and Psychiatry. 1994; 18 :163–182. [ PubMed ] [ Google Scholar ]
- James SA, Strogatz DS, et al. Socioeconomic status, John Henryism, and hypertension in blacks and whites. Am J Epidemiol. 1987; 126 (4):664–73. [ PubMed ] [ Google Scholar ]
- Jones CP. Levels of racism: a theoretic framework and a gardener’s tale. Am J Public Health. 2000; 90 (8):1212–5. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Kendrick L, Anderson NLR, et al. Perceptions of depression among young African American men. Family and Community Health. 2007; 30 (1):63–73. [ PubMed ] [ Google Scholar ]
- Kent LM, Worsley A. Trends in BMI, diet and lifestyle between 1976 and 2005 in North Sydney. Asia Pac J Clin Nutr. 2009; 18 (3):453–61. [ PubMed ] [ Google Scholar ]
- Kessler RC, Crum RM, et al. Lifetime co-occurrence of DSM-III-R Alcohol Abuse and Dependence WIth Other Psychiatric Disorders in the National COmorbidity Survey. Arch Gen Psychiatry. 1997; 54 :313–321. [ PubMed ] [ Google Scholar ]
- Kessler RC, McGonagle KA, et al. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States. Results from the National Comorbidity Survey. Arch Gen Psychiatry. 1994; 51 (1):8–19. [ PubMed ] [ Google Scholar ]
- Kessler RC, Mickelson KD, et al. The prevalence, distribution, and mental health correlates of perceived discrimination in the United States. J Health Soc Behav. 1999; 40 (3):208–30. [ PubMed ] [ Google Scholar ]
- Klatsky AL. Alcohol and cardiovascular diseases. Expert Rev Cardiovasc Ther. 2009; 7 (5):499–506. [ PubMed ] [ Google Scholar ]
- Kleinman A. Culture and depression. N Engl J Med. 2004; 351 (10):951–3. [ PubMed ] [ Google Scholar ]
- Koob GF, Roberts AJ, et al. Neurocircuitry targets in ethanol reward and dependence. Alcohol Clin Exp Res. 1998; 22 (1):3–9. [ PubMed ] [ Google Scholar ]
- Kreiger N. Social Epidemiology. New York: Oxford University Press; 2000. Discrimination and health; pp. 36–75. [ Google Scholar ]
- Krieger N. Racial and gender discrimination: risk factors for high blood pressure? Soc Sci Med. 1990; 30 (12):1273–81. [ PubMed ] [ Google Scholar ]
- Krieger N, Sidney S. Racial discrimination and blood pressure: the CARDIA Study of young black and white adults. Am J Public Health. 1996; 86 (10):1370–8. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Krieger N, Smith K, et al. Experiences of discrimination: validity and reliability of a self-report measure for population health research on racism and health. Soc Sci Med. 2005; 61 (7):1576–96. [ PubMed ] [ Google Scholar ]
- Leonard B. Stress, Depression, and the Activation of the Immune System. World Journal of Biological Psychiatry. 2000; 1 (1):17–25. [ PubMed ] [ Google Scholar ]
- Mabry JB, Kiecolt KJ. Anger in black and white: race, alienation, and anger. J Health Soc Behav. 2005; 46 (1):85–101. [ PubMed ] [ Google Scholar ]
- Massey DS. Residential segregation and neighborhood conditions in U.S. metropolitan areas. In: Smesler N, Wilson WJ, Mitchell F, editors. America Becoming Racial: Trends and Their Consequences. Wasington, D.C.: Natl Acad Press; 1985. pp. 391–434. [ Google Scholar ]
- Massey DS. Segregation and stratification: a biosocial perspective. DuBois Reviews of Social Science. 2004; 1 :7–25. [ Google Scholar ]
- Maton KI, Teti DM, et al. Cultural specificity of support sources, correlates and contexts: three studies of African-American and caucasian youth. Am J Community Psychol. 1996; 24 (4):551–87. [ PubMed ] [ Google Scholar ]
- McCord C, Freeman HP. Excess mortality in Harlem. N Engl J Med. 1990; 322 (3):173–7. [ PubMed ] [ Google Scholar ]
- McEwen BS. Allostasis and allostatic load: implications for neuropsychopharmacology. Neuropsychopharmacology. 2000; 22 (2):108–24. [ PubMed ] [ Google Scholar ]
- McEwen BS. Mood disordesr and allostatic load. Biological Psychiatry. 2003; 54 (3):200–207. [ PubMed ] [ Google Scholar ]
- McEwen BS. Protection and damage from acute and chronic stress: allostasis and allostatic overload and relevance to the pathophysiology of psychiatric disorders. Ann N Y Acad Sci. 2004; 1032 :1–7. [ PubMed ] [ Google Scholar ]
- Mezuk B, Rafferty JA, et al. Reconsidering the Role of Social Disadvantage in Physical and Mental Health: Stressful Life Events, Health Behaviors, Race, and Depression. Am J Epidemiology. 2010; 172 (11):1238–1249. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Nagel J. Constructing Ethnicity: Creating and Recreating Ethnic Identity and Culture. Social Problems. 1994; 41 (1) [ Google Scholar ]
- Neighbors HW, Trierweiler SJ, et al. Racial differences in DSM diagnosis using a semi-structured instrument: the importance of clinical judgment in the diagnosis of African Americans. J Health Soc Behav. 2003; 44 (3):237–56. [ PubMed ] [ Google Scholar ]
- Neighbors HW, Trierweiler SJ, et al. Psychiatric diagnosis of African Americans: diagnostic divergence in clinician-structured and semistructured interviewing conditions. J Natl Med Assoc. 1999; 91 (11):601–12. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Petit B, Western B. Mass imprisonment and the life course: race and class inequality in U.S. incarceration. American Sociological Review. 2004; 69 :601–612. [ Google Scholar ]
- Reiger DA, Farmer ME, et al. Comorbidity of mental disorders with alcohol and other drug abuse: results from the Epidemiologic Catchment Area (ECA) study. JAMA. 1990; 264 (19):2511–2518. [ PubMed ] [ Google Scholar ]
- Rogler LH. Methodological sources of cultural insensitivity in mental health research. Am Psychol. 1999; 54 (6):424–33. [ PubMed ] [ Google Scholar ]
- Rothman KJ. BMI-related errors in the measurement of obesity. Int J Obes (Lond) 2008; 32 (Suppl 3):S56–9. [ PubMed ] [ Google Scholar ]
- Ruan WJ, Goldstein RB, et al. The alcohol use disorder and associated disabilities interview schedule-IV (AUDADIS-IV): reliability of new psychiatric diagnostic modules and risk factors in a general population sample. Drug Alcohol Depend. 2008; 92 (1-3):27–36. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Saha TD, Chou SP, et al. Toward an alcohol use disorder continuum using item response theory: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Psychol Med. 2006; 36 (7):931–41. [ PubMed ] [ Google Scholar ]
- Saha TD, Compton WM, et al. Dimensionality of DSM-IV nicotine dependence in a national sample: an item response theory application. Drug Alcohol Depend. 2010; 108 (1-2):21–8. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Smith E. Ethnic minorities: life stress, social support, and mental health issues. The Counseling Psychologist. 1985; 13 :537–579. [ Google Scholar ]
- Stansfeld SA. Social support and social cohesion. In: Marmot MG, Wilkinson RG, editors. Social determinants of health. New York: Oxford University Press; 2005. [ Google Scholar ]
- Strakowski SM, Keck PE, Jr, et al. Ethnicity and diagnosis in patients with affective disorders. J Clin Psychiatry. 2003; 64 (7):747–54. [ PubMed ] [ Google Scholar ]
- Taylor RJ, Chatters LM, et al. Black and white differences in religious participation: A multi-sample comparison. Journal for the Scientific Study of Religion. 1996; 35 :403–410. [ Google Scholar ]
- Teplin LA. The prevalence of severe mental disorder among male urban jail detainees: comparison with the Epidemiologic Catchment Area Program. Am J Public Health. 1990; 80 (6):663–9. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Teplin LA, Abram KM, et al. Prevalence of psychiatric disorders among incarcerated women. I. Pretrial jail detainees. Arch Gen Psychiatry. 1996; 53 (6):505–12. [ PubMed ] [ Google Scholar ]
- Williams DR. Racial variations in adult health status: patterns, paradoxes, and prospects. In: Smelser NJ, Wilson WJ, Mitchell F, editors. America Becoming: Racial Trends and Their Consequences. Washington, D.C.: National Academy Press; 2001. [ Google Scholar ]
- Williams DR, Gonzalez HM, et al. Prevalence and distribution of major depressive disorder in African Americans, Caribbean blacks, and non-Hispanic whites: results from the National Survey of American Life. Arch Gen Psychiatry. 2007; 64 (3):305–15. [ PubMed ] [ Google Scholar ]
- Williams DR, Jackson PB. Social sources of racial disparities in health. Health Aff (Millwood) 2005; 24 (2):325–34. [ PubMed ] [ Google Scholar ]
- Williams DR, Williams-Morris R. Racism and mental health: the African American experience. Ethn Health. 2000; 5 (3-4):243–68. [ PubMed ] [ Google Scholar ]
- Wilson MN. Child development in the context of the Black extended family. American Psychologist. 1989; 44 :380–383. [ Google Scholar ]
An overlooked aspect concerning the effect of the spatial pattern of zonal wind stress anomalies on El Niño evolution and diversity
- Original Article
- Published: 18 May 2024
Cite this article

- Xianghui Fang ORCID: orcid.org/0000-0002-1210-0055 1 , 2 , 3 ,
- Henk Dijkstra 4 , 5 ,
- Claudia Wieners 4 , 5 &
- Francesco Guardamagna 4 , 5
Anomalous zonal wind stress in the central-to-western Pacific plays a crucial role in ENSO evolution by exciting oceanic waves that propagate eastward or westward. However, compared to its intensity, the importance of its spatial pattern is an overlooked aspect in ENSO theory. Using a linear regression model and numerical simulations with the Zebiak-Cane model, we here show that the zonal wind stress anomaly pattern significantly affects the development of El Niño and its type. Specifically, if the westerly wind stress is closer to the western Pacific (WP), the excited upwelling Rossby waves will take less time to reach the WP coast before they are reflected as Kelvin waves. This significantly weakens sea surface temperature anomalies in the eastern Pacific region since less time is provided for their amplification due to positive feedbacks. This causes the anomalous warming center to be closer to the central Pacific (CP) region, leading to a CP-type El Niño.
This is a preview of subscription content, log in via an institution to check access.
Access this article
Price includes VAT (Russian Federation)
Instant access to the full article PDF.
Rent this article via DeepDyve
Institutional subscriptions
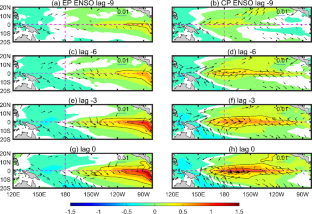
Data availability
The GODAS reanalysis is obtained at https://www.psl.noaa.gov//data/gridded/data.godas.html , the GPCP data is at https://psl.noaa.gov/data/gridded/data.gpcp.html .
An S-I, Kug J-S, Ham Y-G et al (2008) Successive modulation of ENSO to the future greenhouse warming. J Clim 21(1):3–21. https://doi.org/10.1175/2007JCLI1500.1
Article Google Scholar
Battisti DS (1988) Dynamics and thermodynamics of a warming event in a coupled tropical atmosphere–ocean model. J Atmos Sci 45(20):2889–2919. https://doi.org/10.1175/1520-0469(1988)045%3C2889:DATOAW%3E2.0.CO;2
Behringer D, Xue Y (2004) Evaluation of the global ocean data assimilation system at NCEP: The Pacific Ocean. Proceedings eighth symposium on integrated observing and assimilation systems for atmosphere, oceans, and land surface [Dataset]. Retrieved from https://www.researchgate.net/publication/2288
Bjerknes J (1969) Atmospheric teleconnections from the equatorial Pacific. Mon Weather Rev 97(3):163–172. https://doi.org/10.1175/1520-0493(1969)097%3C0163:ATFTEP%3E2.3.CO;2
Cai W-J et al (2019) Pantropical climate interactions. Science 363:944. https://doi.org/10.1126/science.aav4236
Article CAS Google Scholar
Capotondi A et al (2015) Understanding ENSO diversity. Bull Am Meteorological Soc 96:921–938. https://doi.org/10.1175/BAMS-D-13-00117.1
Chen N, Fang X (2023) A simple Multiscale Intermediate coupled Stochastic Model for El Niño Diversity and Complexity. J Adv Model Earth Syst 15(4). https://doi.org/10.1029/2022MS003469
Chen N, Fang X, Yu J-Y (2022) A multiscale model for El Niño complexity. Npj Clim Atmospheric Sci 5:16. https://doi.org/10.1038/s41612-022-00241-x
Clarke AJ, van Gorder S (2001) ENSO prediction using an ENSO trigger and a proxy for western equatorial pacific warm Pool Movement. Geophys Res Lett 28(4):579–582. https://doi.org/10.1029/2000GL012201
Fang X, Chen N (2023) Quantifying the predictability of ENSO complexity using a statistically accurate multiscale stochastic model and information theory. J Clim 36(8):2681–2702. https://doi.org/10.1175/JCLI-D-22-0151.1
Fang X, Mu M (2018a) Both air-sea components are crucial for El Niño forecast from boreal spring. Sci Rep 8(1):1–8. https://doi.org/10.1038/s41598-018-28964-z
Fang X, Mu M (2018b) A three-region conceptual model for central Pacific El Niño including zonal advective feedback. J Clim 31:4965–4979. https://doi.org/10.1175/JCLI-D-17-0633.1
Fang X, Zheng F (2021) Effect of the air-sea coupled system change on the ENSO evolution from boreal spring. Clim Dyn 57:109–120. https://doi.org/10.1007/s00382-021-05697-w
Fang X, Zheng F, Zhu J (2015) The cloud-radiative effect when simulating strength asymmetry in two types of El Niño events using CMIP5 models. J Geophys Research: Oceans 120(6):4357–4369. https://doi.org/10.1002/2014JC010683
Fang X, Dijkstra H, Wieners C, Guardamagna F (2024) A nonlinear full-field conceptual model for ENSO diversity. J Clim. https://doi.org/10.1175/JCLI-D-23-0382.1
Geng L, Jin F-F (2022) ENSO diversity simulated in a revised Cane-Zebiak model. Front Earth Sci 10:899323. https://doi.org/10.3389/feart.2022.899323
Geng L, Jin F-F (2023) Insights into ENSO Diversity from an intermediate coupled model. Part II: role of Nonlinear Dynamics and Stochastic forcing. J Clim 36:7527–7547. https://doi.org/10.1175/JCLI-D-23-0044.1
Geng T, Cai W, Wu L (2020) Two types of ENSO varying in tandem facilitated by nonlinear atmospheric convection. Geophys Res Lett 47(15). https://doi.org/10.1029/2020GL088784
Ham Y-G, Kim J-H, Luo J-J (2019) Deep learning for multi-year ENSO forecasts. Nature 573:568–572. https://doi.org/10.1038/s41586-019-1559-7
Harrison DE, Giese BS (1988) Remote westerly wind forcing of the eastern equatorial Pacific; some model results. Geophys Res Lett 15(8):804–807. https://doi.org/10.1029/GL015i008p00804
Jin F-F (1997) An equatorial ocean recharge paradigm for ENSO. Part I: conceptual model. J Atmos Sci 54(7):811–829. https://doi.org/10.1175/1520-0469(1997)054%3C0811:AEORPF%3E2.0.CO;2
Kao H-Y, Yu J-Y (2009) Contrasting eastern-pacific and central-pacific types of ENSO. J Clim 22(3):615–632. https://doi.org/10.1175/2008JCLI2309.1
Klein SA, Soden BJ, Lau N-C (1999) Remote sea surface temperature variations during ENSO: evidence for a tropical atmospheric bridge. J Clim 12:917–932. https://doi.org/10.1175/1520-0442(1999)012%3C0917:RSSTVD%3E2.0.CO;2
Kug J-S, Kang I-S, An S-I (2003) Symmetric and antisymmetric mass exchanges between the equatorial and off-equatorial Pacific associated with ENSO. J Geophys Research: Oceans 108(C8). https://doi.org/10.1029/2002JC001671
Kug JS, Jin F-F, An SI (2009) Two types of El Niño events: Cold tongue El Niño and warm pool El Niño. J Clim 22(6):1499–1515. https://doi.org/10.1175/2008JCLI2624.1
Lian T, Tang Y, Zhou L et al (2018) Westerly wind bursts simulated in CAM4 and CCSM4. Clim Dyn 50:1353–1371. https://doi.org/10.1007/s00382-017-3689-7
McPhaden MJ (2003) Tropical Pacific Ocean heat content variations and ENSO persistence barriers. Geophys Res Lett 30(9). https://doi.org/10.1029/2003GL016872
McPhaden MJ, Zebiak SE, Glantz MH (2006) ENSO as an integrating concept in Earth science. Science 314:1740–1745. https://doi.org/10.1126/science.1132588
Meinen CS, McPhaden MJ (2000) Observations of warm water volume changes in the equatorial Pacific and their relationship to El Niño and La Niña. J Clim 13(20):3551–3559. https://doi.org/10.1175/1520-0442(2000)013%3C3551:OOWWVC%3E2.0.CO;2
Pang D, Fang X, Wang L (2023) Importance of realistic zonal currents in depicting the evolution of tropical central Pacific sea surface temperature. Environ Res Lett 18(12):124031. https://doi.org/10.1088/1748-9326/ad0b21
Philander S (1983) El Niño Southern Oscillation phenomena. Nature 302(5906):295–301. https://doi.org/10.1038/302295a0
Ren HL, Zuo J, Deng Y (2019) Statistical predictability of Niño indices for two types of ENSO. Clim Dyn 52:5361–5382. https://doi.org/10.1007/s00382-018-4453-3
Ropelewski CF, Halpert MS (1987) Global and regional scale precipitation patterns associated with the El Niño/Southern Oscillation. Mon Weather Rev 115:1606–1626. https://doi.org/10.1175/1520-0493(1987)115%3C1606:GARSPP%3E2.0.CO;2
Ruiz JE, Cordery I, Sharma A (2005) Integrating ocean subsurface temperatures in statistical ENSO forecasts. J Clim 18(17):3571–3586. https://doi.org/10.1175/JCLI3477.1
Schopf PS, Suarez MJ (1988) Vacillations in a coupled ocean–atmosphere model. J Atmos Sci 45:549–566. https://doi.org/10.1175/1520-0469(1988)045%3C0549:VIACOM%3E2.0.CO;2
Tang Y et al (2018) Progress in ENSO prediction and predictability study. Natl Sci Rev 5:826–839. https://doi.org/10.1093/nsr/nwy105
Timmermann A et al (2018) El Niño–Southern Oscillation complexity. Nature 559:535–545. https://doi.org/10.1038/s41586-018-0252-6
Wang C (2018) A review of ENSO theories. Natl Sci Rev 5(6):813–825. https://doi.org/10.1093/nsr/nwy104
Wang J, Zhang S, Jiang H, Yuan D (2022) Effects of 2019 subsurface Indian Ocean initialization on the forecast of the 2020/2021 La Niña event. Clim Dyn 1–17. https://doi.org/10.1007/s00382-022-06442-7
Zebiak SE, Cane MA (1987) A model El Niño–Southern Oscillation. Mon Weather Rev 115(10):2262–2278. https://doi.org/10.1175/1520-0493(1987)115%3C2262:ameno%3E2.0.co;2
Zhang R, Min Q, Su J (2017) Impact of El Niño on atmospheric circulations over East Asia and rainfall in China: role of the anomalous western North Pacific anticyclone. Sci China Earth Sci 60:1124–1132. https://doi.org/10.1007/s11430-016-9026-x
Zheng F, Fang X, Yu J-Y, Zhu J (2014) Asymmetry of the bjerknes positive feedback between the two types of El Niño. Geophys Res Lett 41(21):7651–7657. https://doi.org/10.1002/2014GL062125
Download references
This work of Xianghui Fang was carried out at Utrecht University, the Netherlands and supported by the National Natural Science Foundation of China (Grant Nos. 42288101 and 42192564), Ministry of Science and Technology of the People’s Republic of China (Grant No. 2020YFA0608802), Guangdong Major Project of Basic and Applied Basic Research (Grant No. 2020B0301030004), and the scholarship provided by the China Scholarship Council (CSC, Grant No. 202106105010). The work of Francesco Guardamagna, Claudia Wieners and Henk Dijkstra was supported by the Netherlands Organization for Scientific Research (NWO) under grant OCENW.M20.277.
Author information
Authors and affiliations.
Department of Atmospheric and Oceanic Sciences, Institute of Atmospheric Sciences, Fudan University, Shanghai, China
Xianghui Fang
Shanghai Key Laboratory of Ocean-Land-Atmosphere Boundary Dynamics and Climate Change, Fudan University, Shanghai, China
Shanghai Frontiers Science Center of Atmosphere-Ocean Interaction, Shanghai, China
Institute for Marine and Atmospheric research Utrecht, Utrecht University, Utrecht, The Netherlands
Henk Dijkstra, Claudia Wieners & Francesco Guardamagna
Centre for Complex Systems Studies, Utrecht University, Utrecht, The Netherlands
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Xianghui Fang .
Ethics declarations
Competing interests.
The authors declare no competing interests
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Reprints and permissions
About this article
Fang, X., Dijkstra, H., Wieners, C. et al. An overlooked aspect concerning the effect of the spatial pattern of zonal wind stress anomalies on El Niño evolution and diversity. Clim Dyn (2024). https://doi.org/10.1007/s00382-024-07264-5
Download citation
Received : 04 January 2024
Accepted : 02 May 2024
Published : 18 May 2024
DOI : https://doi.org/10.1007/s00382-024-07264-5
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Find a journal
- Publish with us
- Track your research
IMAGES
VIDEO
COMMENTS
Table 1 contains an alphabetized and more in-depth description of each hypothesis, including definition; predictions; stage or transition; taxon specificity; proposed mediators - categorized as HPA/I axis (glucocorticoids; GCs), autonomic nervous system, or other; and if relevant, baseline or post-stress GCs; and any additional notes. Out of the 131 hypotheses, 111 include specific mention ...
According to this framework, we may easily differentiate each element of the stress system. Taking oxidative stress as an example, reactive oxygen species (ROS) are stressors, the factors that stimulate the generation of ROS are stressful stimuli, a disruption of redox signaling and control caused by ROS is oxidative stress, the response that the body attempts to restore redox homeostasis is ...
Summary. Stress is a broad and complex phenomenon characterized by environmental demands, internal psychological processes, and physical outcomes. The study of stress is multifaceted and commonly divided into three theoretical perspectives: social, psychological, and biological. The social stress perspective emphasizes how stressful life ...
Stress is ubiquitous and thus, not surprisingly, many hypotheses and models have been created to better study the role stress plays in life. Stress spans fields and is found in the literature of biology, psychology, psychophysiology, sociology, economics, and medicine, just to name a few. Stress, an …
Stress-Response Theory. Selye (1976a) initially proposed a triadic model as . the basis for the stress-response pattern. The ele-ments included adrenal cortex hypertrophy, thy-micolymphatic (e.g., the thymus, the lymph nodes, and the spleen) atrophy, and gastrointesti-nal ulcers. These three, he reasoned, were closely
The hypothesis that stress predicts susceptibility to the common cold received support from observational studies (Graham et al. 1986, Meyer & Haggerty 1962). One problem with such studies is that they do not control for exposure. Stressed people, for instance, might seek more outside contact and thus be exposed to more viruses.
The cumulative science linking stress to negative health outcomes is vast. Stress can affect health directly, through autonomic and neuroendocrine responses, but also indirectly, through changes in health behaviors. In this review, we present a brief overview of (a) why we should be interested in stress in the context of health; (b) the stress response and allostatic load; (c) some of the key ...
The word 'stress' is used in physics to refer to the interaction between a force and the resistance to counter that force, and it was Hans Selye who first incorporated this term into the medical lexicon to describe the " nonspecific response of the body to any demand ". Selye, who is known as the 'father of stress research ...
The psychology of stress and coping has been a prominent topic of scientific study and of popular interest over the last century. Applying the study of the mind and behavior to a concept such as stress and coping has led to an evolving definition of stress, more research on its physical, psychological and social effects, and the development of ...
The STRESS-NL database contains data that allow metaanalytical as well as proof-of-principle analyses, enabling human stress research to take new avenues in both explorative and hypothesis-driven ...
Psychological stress is a complex phenomenon and numerous theoretical models have attempted to explain its etiology. These theoretical explanations can be categorized according to their primary conceptualization of the stress experience: stress as an external stimulus; stress as a response; stress as an individual/environmental transaction. The transactional theory of stress and coping ...
Tend-and-Befriend. In spite of the fact that the human stress response has often been characterized as one of fight-or-flight, Taylor et al. have proposed a theory that constitutes a biobehavioral alternative to the fight-or-flight response.Taylor et al. maintain that as a result of gender differences in the stress response, human female responses are better characterized by a pattern termed ...
Kahn et al.'s role stress theory, coupled with Lewin's Field Theory, serves as the foundation for the P-E fit theory. Lewin wrote, "Every psychological event depends upon the state of the person and at the same time on the environment" (p. 12). Researchers of IO psychology have narrowed the environment to the organization or work team.
Epidemiological studies confirm that both experiencing a greater number of stressful events and reporting high perceived stress over long periods of time are associated with worse mental and physical health, and mortality (Epel et al., 2018).The association between greater stressor exposure and increased disease risk has been replicated with many different types of stressor exposures (e.g ...
HPA axis hypothesis. Stress and MDD are closely related, and stressful life events can often lead to depressive episodes.
Chronic stress, on the other hand, is more toxic as it is an unrelenting circumstance that offers little chance for a return to normalcy. Financial strain, having a bully for a boss, and social ...
Figure 16.5 The Transactional Theory of Stress and Coping, by J. Walinga. Coping with Stress. There are many ways that people strive to cope with stressors and feelings of stress in their lives. A host of literature, both popular and academic, extols the practice of stress management and whole industries are devoted to it.
stress theory (Burr, 1989) by sociologist Earl Koos (1946). Koos made the first effort at creating a stress theory with "the profile of trouble" (p. 107). Koos's research and profile, which appear in Part II of this book, led to the second era of family stress theory development. The Second Era (Late 1940s to Late 1970s)
The modern theory of stress, initially proposed by Hans Selye in 1956, signifies an important development in our understanding of this phenomenon. Selye's The Stress of Life serves as a foundational book for subsequent scientific questions. In this article, we focus on a comprehensive look at stress and use a literature review to explain its theoretical foundations as well as its clinical ...
The ongoing stress relating to education has demonstrated negative impact on students' learning capacity, academic performance, education and employment attainment, sleep quality and quantity, physical health, mental health and substance use outcomes. Increasing students' stress-management skills and abilities is an important target for change.
This stress moderation hypothesis has provided a fruitful situation for the advent of more complex models that investigate the relationships between stress, support, and illness. Hence, psychological models considering factors that are related to the buffering effect have attracted considerable attention in the last years [25, 26].
Results showed that a) Blacks were less likely to engage in alcohol or nicotine consumption at low, moderate, and high levels of stress compared to Whites, and b) there was a significant three-way interaction between race, stress, and coping behavior for BMI only (F = 2.11, df = 12, p = 0.03), but, contrary to the hypothesis, elevated BMI was ...
A hypothesis is a tentative statement about the relationship between two or more variables. It is a specific, testable prediction about what you expect to happen in a study. It is a preliminary answer to your question that helps guide the research process. Consider a study designed to examine the relationship between sleep deprivation and test ...
According to this theory, people who are repeatedly exposed to stressful situations beyond their control develop an inability to make decisions or engage effectively in purposeful behavior. Subsequently, researchers have noticed that this learned helplessness theory is similar to posttraumatic stress disorder (Ackerman, 2022).
Significant life events — whether positive or negative — can cause stress. Divorce, marriage, the birth of a child, moving to a new home, the death of a loved one, and losing or gaining a job ...
This hypothesis suggests that, in the context of chronic stress, Blacks' engagement in UHBs may serve to buffer the deleterious consequences of stress on depression through the HPA pathway, leading to a lower prevalence of depression but a greater prevalence of physical health problems than would have otherwise occurred.
Stress-induced increases in cortisol can stimulate or inhibit brain cell proliferation, but the mechanisms behind these opposing effects are unknown. We tested the hypothesis that 11β-hydroxysteroid dehydrogenase type 2 (Hsd11b2), a glucocorticoid-inactivating enzyme expressed in neurogenic regions of the adult zebrafish brain, mitigates cortisol-induced changes to brain cell proliferation ...
This tip sheet introduces what causes unmanageable stress in children, the role the brain plays, and the impact a child's unmanageable stress may have on caregiving adults. It also describes what children need to remain emotionally regulated. All humans use behavior to tell others how they are feeling physically and emotionally.
Anomalous zonal wind stress in the central-to-western Pacific plays a crucial role in ENSO evolution by exciting oceanic waves that propagate eastward or westward. However, compared to its intensity, the importance of its spatial pattern is an overlooked aspect in ENSO theory. Using a linear regression model and numerical simulations with the Zebiak-Cane model, we here show that the zonal wind ...