Module 13: Disorders of Childhood and Adolescence
Case studies: disorders of childhood and adolescence, learning objectives.
- Identify disorders of childhood and adolescence in case studies

Case Study: Jake

Jake was born at full term and was described as a quiet baby. In the first three months of his life, his mother became worried as he was unresponsive to cuddles and hugs. He also never cried. He has no friends and, on occasions, he has been victimized by bullying at school and in the community. His father is 44 years old and describes having had a difficult childhood; he is characterized by the family as indifferent to the children’s problems and verbally violent towards his wife and son, but less so to his daughters. The mother is 41 years old, and describes herself as having a close relationship with her children and mentioned that she usually covers up for Jake’s difficulties and makes excuses for his violent outbursts. [1]
During his stay (for two and a half months) in the inpatient unit, Jake underwent psychiatric and pediatric assessments plus occupational therapy. He took part in the unit’s psycho-educational activities and was started on risperidone, two mg daily. Risperidone was preferred over an anti-ADHD agent because his behavioral problems prevailed and thus were the main target of treatment. In addition, his behavioral problems had undoubtedly influenced his functionality and mainly his relations with parents, siblings, peers, teachers, and others. Risperidone was also preferred over other atypical antipsychotics for its safe profile and fewer side effects. Family meetings were held regularly, and parental and family support along with psycho-education were the main goals. Jake was aided in recognizing his own emotions and conveying them to others as well as in learning how to recognize the emotions of others and to become aware of the consequences of his actions. Improvement was made in rule setting and boundary adherence. Since his discharge, he received regular psychiatric follow-up and continues with the medication and the occupational therapy. Supportive and advisory work is done with the parents. Marked improvement has been noticed regarding his social behavior and behavior during activity as described by all concerned. Occasional anger outbursts of smaller intensity and frequency have been reported, but seem more manageable by the child with the support of his mother and teachers.
In the case presented here, the history of abuse by the parents, the disrupted family relations, the bullying by his peers, the educational difficulties, and the poor SES could be identified as additional risk factors relating to a bad prognosis. Good prognostic factors would include the ending of the abuse after intervention, the child’s encouragement and support from parents and teachers, and the improvement of parental relations as a result of parent training and family support by mental health professionals. Taken together, it appears that also in the case of psychiatric patients presenting with complex genetic aberrations and additional psychosocial problems, traditional psychiatric and psychological approaches can lead to a decrease of symptoms and improved functioning.
Case Study: Kelli

Kelli may benefit from a course of comprehensive behavioral intervention for her tics in addition to psychotherapy to treat any comorbid depression she experiences from isolation and bullying at school. Psychoeducation and approaches to reduce stigma will also likely be very helpful for both her and her family, as well as bringing awareness to her school and those involved in her education.
- Kolaitis, G., Bouwkamp, C.G., Papakonstantinou, A. et al. A boy with conduct disorder (CD), attention deficit hyperactivity disorder (ADHD), borderline intellectual disability, and 47,XXY syndrome in combination with a 7q11.23 duplication, 11p15.5 deletion, and 20q13.33 deletion. Child Adolesc Psychiatry Ment Health 10, 33 (2016). https://doi.org/10.1186/s13034-016-0121-8 ↵
- Case Study: Childhood and Adolescence. Authored by : Chrissy Hicks for Lumen Learning. Provided by : Lumen Learning. License : CC BY: Attribution
- A boy with conduct disorder (CD), attention deficit hyperactivity disorder (ADHD), borderline intellectual disability.... Authored by : Gerasimos Kolaitis, Christian G. Bouwkamp, Alexia Papakonstantinou, Ioanna Otheiti, Maria Belivanaki, Styliani Haritaki, Terpsihori Korpa, Zinovia Albani, Elena Terzioglou, Polyxeni Apostola, Aggeliki Skamnaki, Athena Xaidara, Konstantina Kosma, Sophia Kitsiou-Tzeli, Maria Tzetis . Provided by : Child and Adolescent Psychiatry and Mental Health. Located at : https://capmh.biomedcentral.com/articles/10.1186/s13034-016-0121-8 . License : CC BY: Attribution
- Angry boy. Located at : https://www.pxfuel.com/en/free-photo-jojfk . License : Public Domain: No Known Copyright
- Frustrated girl. Located at : https://www.pickpik.com/book-bored-college-education-female-girl-1717 . License : Public Domain: No Known Copyright

Disclaimer » Advertising
- HealthyChildren.org

- Previous Article
- Next Article
Health Risks in Adolescence
Unique biological and psychosocial changes occurring during adolescence, brain development, sexual orientation and gender identification, legal status, mental health and emotional well-being, morbidity from high-risk sexual activity, the adolescent medical home, recommendations, appendix: online resources, lead authors, committee on adolescence, 2017–2018, unique needs of the adolescent.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
- Split-Screen
- Article contents
- Figures & tables
- Supplementary Data
- Peer Review
- CME Quiz Close Quiz
- Open the PDF for in another window
- Get Permissions
- Cite Icon Cite
- Search Site
Elizabeth M. Alderman , Cora C. Breuner , COMMITTEE ON ADOLESCENCE , Laura K. Grubb , Makia E. Powers , Krishna Upadhya , Stephenie B. Wallace; Unique Needs of the Adolescent. Pediatrics December 2019; 144 (6): e20193150. 10.1542/peds.2019-3150
Download citation file:
- Ris (Zotero)
- Reference Manager
Adolescence is the transitional bridge between childhood and adulthood; it encompasses developmental milestones that are unique to this age group. Healthy cognitive, physical, sexual, and psychosocial development is both a right and a responsibility that must be guaranteed for all adolescents to successfully enter adulthood. There is consensus among national and international organizations that the unique needs of adolescents must be addressed and promoted to ensure the health of all adolescents. This policy statement outlines the special health challenges that adolescents face on their journey and transition to adulthood and provides recommendations for those who care for adolescents, their families, and the communities in which they live.
Adolescence, defined as 11 through 21 years of age, 1 is a critical period of development in a young person’s life, one filled with distinctive and pivotal biological, cognitive, emotional, and social changes. 2 The World Health Organization 3 ; the Office of Adolescent Health of the US Department of Health and Human Services 4 ; the Health and Medicine Division of the National Academies of Sciences, Engineering, and Medicine (formerly the Institute of Medicine) 5 , 6 ; the Lancet , 7 with 4 international academic institutions 8 ; and the Society for Adolescent Health and Medicine 9 have called for a closer examination of the unique health needs of adolescents. In 2018, Nature devoted an issue to the advances in the science of adolescence and called for ongoing further study of this important population. 10 As a leader in adolescent health care, the American Academy of Pediatrics (AAP) is motivated to describe why adolescents are a unique and vulnerable population and why it is crucial that the AAP focus on adolescents’ health concerns to optimize healthy development during the transition to adulthood. Addressing the unique needs of adolescents with disabilities is outside the scope of this statement; several statements specific to this population are available at https://pediatrics.aappublications.org/collection/council-children-disabilities . In addition, specific guidance around the transition to adult health care is not covered in this statement; please refer to the list of transition resources at the end of this document.
The need for comprehensive health services for teenagers has been well documented since the 1990s. 11 – 13 The AAP advocates for the pediatrician to provide the medical home for adolescent primary care. 14 Other professional societies, such as the Society for Adolescent Health and Medicine, the American Academy of Family Physicians, and the American College of Obstetricians and Gynecologists and school-based health initiatives ( https://www.sbh4all.org/ ), recognize the unique needs of adolescents. These organizations recommend an increase in adolescent medicine training, along with the Accreditation Committee for Graduate Medical Education. The Accreditation Committee for Graduate Medical Education currently requires only 1 month of adolescent medicine training from a board-certified adolescent medicine specialist for all pediatric residency programs (adolescent medicine; [Core] IV.A.6.[b].[3].[a].[i]); there must be one educational unit). 15 The importance of addressing the physical and mental health of adolescents has become more evident, with investigators in recent studies pointing to the fact that unmet health needs during adolescence and in the transition to adulthood predict not only poor health outcomes as adults but also lower quality of life in adulthood. 16
A hallmark of adolescence is a gradual development toward autonomy and individual adult decision-making. However, adolescents are often faced with situations for which they may not be prepared, and many are likely to be involved in risk-taking behaviors, such as use of alcohol, tobacco, and other drugs and engaging in unprotected sex. Most recently, there is increased concern about the rise in electronic cigarette use among adolescence. 17 In fact, most health care visits by adolescents to their pediatricians or other health care providers are to seek treatment of conditions or injuries that could have been prevented if screened for and addressed at an earlier comprehensive visit. 18 Although some risk-taking behavior is considered normal in adolescence, engaging in certain types of risky behavior can have adverse and potentially long-term health consequences. The majority of mortality and morbidity during adolescence, which can be prevented, is attributable to unintentional injuries, suicide, and homicide. 19 Approximately 72% of deaths among adolescents are attributable to injuries from motor vehicle crashes, other unintentional and intentional injuries, injuries caused by firearms, injuries influenced by use of alcohol and illicit substances, homicide, or suicide. 20 , 21 These causes of death greatly surpass medical etiologies such as cancer, HIV infection, and heart disease in the United States and other industrialized nations. 21
The AAP Bright Futures: Guidelines for Health Supervision of Infants, Children, and Adolescents recommends a strength-based approach to screening and counseling around these behaviors that lead to mortality and morbidity in adolescents. 1 , 22 However, according to the National Ambulatory Medical Care Survey and the National Hospital Ambulatory Medical Care Survey, only 39% of adolescents received any type of preventive counseling during ambulatory visits. 23 Seventy-one percent of teenagers reported at least 1 potential health risk, yet only 37% of these teenagers reported discussing any of these risks with their pediatrician or primary care physician. Clearly, screening for and counseling around these high-risk behaviors needs to be improved. 24
New screening codes for depression, substance use, and alcohol and tobacco use as well as brief intervention services may provide opportunities to receive payment for the services pediatricians are providing to adolescents. These include 96127, brief emotional and behavioral assessment (eg, depression inventory, attention-deficit/hyperactivity disorder scale) with scoring and documentation, per standardized instrument, and 96150, health and behavior assessment (eg, health-focused clinical interview, behavioral observations, psychophysiological monitoring, health-oriented questionnaires). 25 However, it is important to recognize that coding for specific diagnoses may be challenging if the patient does not want his or her parent(s) to know the reasons for the clinical visit. Adolescent visits and documentation of visits are confidential to promote better access and to protect the rights of adolescents. 26
Another trend in the health status of adolescents (reflecting technological advances in pediatric medical care) is the increasing number of pediatric patients with chronic medical conditions and developmental challenges who enter adolescence. Adolescents with chronic conditions face developmental challenges similar to their healthy peers but may have special educational, vocational, and transitional concerns because of their medical issues. 27
The prevalence of chronic medical conditions and developmental and physical disabilities in adolescents is difficult to assess because of the variation of study methodologies and categorical versus noncategorical approaches to the epidemiology of chronic illness. 28 According to the National Survey of Children’s Health, funded by the US Department of Health and Human Services, almost 31% of adolescents have 1 moderate to severe chronic illness, such as asthma or a mental health condition. 29 Other common chronic illnesses include obesity, cancer, cardiac disease, HIV infection, spastic quadriplegia, and developmental disabilities. 30 – 32 One in 4 adolescents with chronic illness has at least 1 unmet health need that may affect physical growth and development, including puberty and overall health status as well as future adult health. 33
Within pediatric practice, integrating adolescent-centered, family-involved approaches into the care of adolescents as well as culturally competent and effective approaches (as outlined in Bright Futures: Guidelines for Health Supervision of Infants, Children, and Adolescents ) has the potential not only to identify threats to well-being but also to create a space to work with families to bolster opportunities for optimal development of all children. 1 When considering the health challenges adolescents face, it is imperative to take into account not only the ethnic and racial diversity of the adolescent population in the United States but also the social and ecologic factors (eg, socioeconomic status, family composition, parental education and engagement, neighborhood and school environment, religion, earlier childhood trauma and toxic stress, and access to health care).
The Search Foundation has conducted research that suggests that for minority youth, a positive ethnic identity is a critical spark for emergence of the required developmental assets to enable adolescents to develop into successful and contributing adults. 34 , 35 This theory is supported by a recent study in The Journal of Pediatrics that suggests minority youth are still prone to depression because of isolation and discrimination faced during adolescence while navigating neighborhood and school environments, even when they have educated and supportive parents. 36 African American male adolescents have the highest rates of mortality, followed by American Indian, white, Hispanic, and Asian American or Pacific Islander male adolescents, pointing to racial and ethnic disparities in adolescent health and the potential to achieve a healthy adulthood. 37
The AAP has previously published policy statements addressing the unique strengths and health disparities that exist for specific groups of adolescents, such as lesbian, gay, bisexual, and transgender youth and those in the juvenile justice system, foster care, and the military. 38 – 42 Pediatricians must pay attention to how care is delivered to the increasingly diverse adolescent populations to prevent a decline in health status and increase in health care disparities.
Biological and psychosocial changes that occur during adolescence make this age group unique. Research describing the timing and physiology of puberty has been invaluable in revealing not only differences between racial groups but also between adolescents with different chronic conditions. 43 – 46
Puberty is the hallmark of physiologic progression from child to adult body habitus. Chronic conditions, such as obesity and intracranial lesions, or trauma may cause early puberty, which may put the adolescent at risk for engagement in higher-risk behaviors at an earlier age. 44 Delayed puberty is often a variant of normal development but may also be seen in adolescents with inflammatory bowel disease, eating disorders, and chronic conditions that create malnutrition as well as adolescents who have undergone treatment of malignancies. Comorbid mental disease (eg, an eating disorder that causes delayed puberty) or medication for psychiatric illness that causes obesity, which may cause early puberty, can complicate optimal adolescent psychosocial development.
The work of Giedd 47 and others shows that brain development during adolescence is ongoing and affects behavior and health. Because of changes in signaling that relate to the reward system in which the brain motivates behavior and the continuing maturation of the parts of the brain that regulate impulse control, adolescents may have a propensity to be involved with high-risk behaviors and have heightened response to emotionally loaded situations. In addition, adverse childhood experiences can have an impact on brain development, affecting behaviors and health during adolescence. 48 During adolescence, there is a “pruning” of gray matter and synapses, which makes the brain more efficient. 47 White matter increases throughout adolescence, which allows the older adolescent and adult brain to conduct more-complex cognitive tasks and adaptive behavior. 49
Increasingly, studies show that the adolescent brain responds to alcohol and illicit substances differently than adults. 50 , 51 This difference may explain the increased risk of binge drinking as well as greater untoward cognitive effects of alcohol and marijuana.
Sexual (and gender) development is a process that starts early in childhood and involves negotiating and experimenting with identity, relationships, and roles. In early adolescence, people begin to recognize or become aware of their sexual orientation. 52 , 53
However, some adolescents are still unsure of their sexual attractions, and others struggle with their known sexual attraction. Adolescence is a time of identity formation and experimentation, so labels that one uses for their sexual orientation (eg, gay, straight, bisexual, etc) often do not correlate to actual sexual behaviors and partners. Sexual orientation and behaviors should be assessed by the pediatrician without making assumptions. Adolescents should be allowed to apply and explain the labels they choose to use for sexuality and gender using open-ended questions. 54 – 56
Sexual minority adolescents may engage in heterosexual practices, and heterosexual adolescents may engage in same-sex sexual activity. Depending on their specific behaviors and the gender of various partners, all sexually active adolescents may be at risk for sexually transmitted infections and unplanned pregnancy. Sexual minority youth are at higher risk of sexually transmitted infections and unplanned pregnancy, often because they do not receive education that applies to their sexual behaviors and are less likely to be screened appropriately ( http://www.cdc.gov/healthyyouth/disparities/smy.htm ). 57 , 58
Sexual minority and transgender youth, because of the stigma they face, are also at higher risk of mental health problems, including depression and suicidality, altered body image, and substance use. 38
There is strong evidence that when sexual minority and transgender youth feel they cannot express their true selves, they go underground by either hiding or denying their attractions and identity. 59 When this is combined with reinforcing parental rejection, bullying, etc, it is believed to lead to internalization, low self-esteem, and ultimately, depression and suicide. 59 Using an explanation like this places the problem on the societal context, not the adolescent or his or her identity. 38 , 39 , 60 , 61
A relatively higher proportion of homeless adolescents are lesbian, gay, bisexual, transgender, and queer or questioning youth. 61 They leave their family homes because of abuse or having been thrown out. These adolescents are at high risk for victimization and often need to engage in unsafe sexual practices to provide themselves food and shelter. 61
Mental health problems may become more pronounced when sexual minority teenagers come out during adolescence to unsupportive family members and friends or health care providers. 38 These youth are more likely to experience violence both in their homes and in their schools and communities. Studies have shown that sexual minority youth reveal higher rates of tobacco, alcohol, marijuana, and other illicit substance use. 62
Most adolescents identify by and express a gender that conforms to their anatomic sex. However, some adolescents experience gender dysphoria with their anatomic sex when entering puberty. As they consider transgender options, they are at an increased risk of mental or emotional health problems, including depression and suicidality, victimization and violence, eating disorders, substance use, and unaccepting or intolerant family members and peers. Crucial to the successful navigation of gender dysphoria issues are health care providers who can assist transgender youth and families to achieve safe, healthy transitioning both in the postponement of puberty, when indicated, and in transitioning to preferred gender with psychosocial and behavioral support. 59
Adolescence heralds a change of legal status, in which the age of 18 or 19 years transforms legal status from minors to adults with full legal privileges and obligations related to health care. However, certain states afford minors the right to confidentiality and consent to or for reproductive and mental health and substance use treatment confidential health services. 26 , 63 Generally, minors may receive confidential screening and care for sexually transmitted infections in all 50 states and the District of Columbia. However, accessing contraception to prevent unwanted pregnancy as well as the ability to self-consent to pregnancy options counseling, prenatal care, and termination of pregnancy vary between states. 64 These discrepancies also exist in accessing outpatient mental health and substance use services. Many adolescents in need of these services do not know they may have the right to access them on their own and may avoid interaction with the health care system to assist with reproductive and mental health concerns. 16 Delaying such care leads to adverse health outcomes. 16 A recent survey confirms that adolescents value private time with their health care providers, with confidentiality assurances by health care providers. 65 The need for office policies in negotiating private time was suggested. Moreover, health care providers reported needing more education in the provision of confidential services. 66 Adolescents in foster care may also be limited in their autonomous access to confidential services, which varies state to state. 41 In certain states, pregnant and parenting adolescents may have the right to consent for their care and the care of their child ( https://www.guttmacher.org/state-policy/explore/minors-rights-parents , https://www.schoolhouseconnection.org/state-laws-on-minor-consent-for-routine-medical-care/ ). Few adolescents are considered emancipated minors and, thereby, entitled to all legal privileges of adults. 67
Mental health and emotional well-being, in combination with issues pertaining to sexual and reproductive health, violence and unintentional injury, substance use, eating disorders, and obesity, create potential challenges to adolescents’ healthy emotional and physical development. 68 Approximately 20% of adolescents have a diagnosable mental health disorder. 69 Many mental health disorders present initially during adolescence. Twenty-five percent of adults with mood disorder had their first major depressive episode during adolescence. 70
Suicide is the second leading cause of death in adolescents, resulting in more than 5700 deaths in 2016. 71 Between 2007 and 2016, the overall suicide rate for children and adolescents ages 10 to 19 years increased by 56%. 71 Older adolescents (15–19 years of age) are at an increased risk of suicide, with a rate of 5 in 100 000 for girls and 20 in 100 000 for boys. 71 According to the 2017 Youth Risk Behavior Survey of high school students, 7.4% of high school students attempted suicide in the last 12 months, and 13.6% made a suicide plan. 72 Adolescents with parents in the military were at increased risk of suicidal ideation (odds ratio [OR]: 1.43; 95% confidence interval [CI]: 1.37–1.49), making a plan to harm themselves (OR: 1.19; 95% CI: 1.06–1.34), attempting suicide (OR: 1.67; 95% CI: 1.43–1.95), and an attempted suicide that required medical treatment. 73
Eating disorders typically present in the adolescent years. Although the incidence of eating disorders is low compared with depression, anxiety, and other mental health problems, these problems are often comorbid with eating disorders. 74 Moreover, the incidence of anorexia nervosa, bulimia nervosa, and other disordered eating is becoming more prevalent in formerly obese teenagers, male teenagers, and teenagers from lower socioeconomic groups. 75 – 77
Teenagers with mental health issues may have subsequent poor school performance, school dropout, difficult family relationships, involvement in the juvenile justice system, substance use, and high-risk sexual behaviors. 78 Almost 70% of youth in the juvenile justice system have a diagnosed mental health disorder. 79 , 80
Rates of serious mental health disorders among homeless youth range from 19% to 50%. 81 , 82 Homeless youth have a high need for treatment but rarely use formal treatment programs for medical, mental, and substance use services. 81 Confidentiality is also an issue for adolescents, as evidenced by the fact that in adolescents to whom confidentiality is not assured, there is a higher prevalence of depressive symptoms, suicidal thoughts, and suicide attempts. 83 There is a paucity of adequately trained mental health professionals to care for adolescents with these mental health challenges. 84 In addition, coverage for mental health services by insurance plans can be variable. 78
Multiple factors, including the increase in use of long-acting reversible contraception, have resulted in the teenage pregnancy rate decreasing in the United States over the past 20 years. 85 , 86 However, pregnancy still contributes to delays in educational and career success for adolescents. Moreover, pregnant teenagers are more likely to delay seeking medical care, putting them at risk for pregnancy-related health problems and putting their children at risk for prematurity and other negative birth outcomes. 87
Adolescents continue to have the highest rates of sexually transmitted infections (eg, gonorrhea and Chlamydia ). 88 Although screening most sexually active adolescents for Chlamydia infection is covered by the Patient Protection and Affordable Care Act (Pub L No. 111–148 [2010]) and recommended by the AAP Bright Futures: Guidelines for Health Supervision of Infants, Children, and Adolescents , adolescent concerns about billing and confidentiality are obstacles to medical screening. 1 , 89 Pediatricians can refer to AAP guidance to find appropriate codes for payment for providing adolescent health services ( https://www.aap.org/en-us/Documents/coding_factsheet_adolescenthealth.pdf ).
Consideration of the unique health risks as well as the biological and psychosocial elements of adolescence allows the AAP-endorsed patient-centered medical home (PCMH) to serve as an ideal conceptual framework by which a primary care practice can maximize the quality, efficiency, and patient experience of care. In 2007, the AAP joined the American Academy of Family Physicians, the American College of Physicians, and the American Osteopathic Association to endorse the “Joint Principals of the Patient-Centered Medical Home,” which describes 7 core characteristics: (1) personal physician for every patient; (2) physician-directed medical practice; (3) whole person orientation; (4) care is coordinated and/or integrated; (5) quality and safety are hallmarks of PCMH care; (6) enhanced access to care; and (7) appropriate payment for providing PCMH care. 90 The AAP, American Academy of Family Physicians, and American College of Physicians assert that optimal health care is achieved when each person, at every age, receives developmentally appropriate care. 91 Pediatricians provide quality adolescent care when they maintain relationships with families and with their patients and, thus, help patients develop autonomy, responsibility, and an adult identity. 92 Issues unique to adolescence to consider within the PCMH model include the following: adolescent-oriented developmentally appropriate care, which may require longer appointment times; confidentiality of health care visits, health records, billing, and the location where adolescents receive care; providers who offer such care; and the transition to adult care. 91 , 93 Moreover, using a strengths-based approach in the care of adolescents, as well as capitalizing on resiliency, is instrumental to maintaining the health of the individual adolescent. 94
Schools have an important role for adolescents who either do not have access to a PCMH or do not use their access to receive recommended preventive services. School-based health centers and school-based mental health services can meet the needs of adolescents who do not have a PCMH or can coordinate school-based health services with the PCMH if the student has one. School nurses can help identify and refer adolescents who need these services. 95
Financing health care of the adolescent can be challenging. Please see the detailed AAP policy statement on reforms in health care financing with the ultimate goal to improve the health care of all adolescents. 92
On the basis of the unique biological and psychosocial aspects of adolescence, the AAP supports the following:
continued recognition by international and national organizations, including the AAP, the Society for Adolescent Health and Medicine, the American College of Obstetricians and Gynecologists, the North American Society for Pediatric and Adolescent Gynecology, and the American Academy of Family Physicians, of the need for policies and advocacy related to adolescent health and well-being;
sustained funding for research to further elucidate the biological basis of the growth and development of adolescents and how they affect adolescent behavior;
educational programs and adequate financial compensation for pediatricians and other health care professionals to support them in providing evidence-based, quality primary care for adolescents;
pediatricians receiving training on how to maintain the clinical setting as a “safe space,” particularly in terms of confidentiality, especially when working with lesbian, gay, bisexual, transgender, and queer or questioning adolescents;
the role of schools, including school nurses and school-based health centers, and their role in promoting healthy adolescent development and providing access to health care;
further education, training, and advocacy for mental health care services that specifically address the needs of adolescents, preferably as part of a medical home model, stressing the importance of mental health for all youth;
federal confidentiality protection for mental health and reproductive services, as is currently provided in many states;
innovative postresidency training programs to increase the number of adolescent-trained pediatric providers in the workforce;
improved access to medical homes for all adolescents to ensure access to preventive medical care;
affiliation of middle and high schools with a physician trained to care for adolescents, unless the student already has access to comprehensive adolescent health services;
education for pediatricians so that they are aware of the laws regarding confidential care of adolescents in their states; and
familiarity with community resources for confidential reproductive and mental health care if they cannot provide confidential care themselves. Pediatricians who are unable to provide these services should learn about local community resources that provide confidential reproductive and mental health care.
The AAP recommends the following strategies targeted at improving financing for the health care of adolescents:
Federal and state agencies should increase their efforts to further reduce the number of adolescents who are not insured or who lack comprehensive and affordable health insurance.
The Centers for Medicare and Medicaid Services should implement its regulatory authority to update its standards for essential health benefits, as defined in the Patient Protection and Affordable Care Act, in the 2 categories of mental and behavioral health services and pediatric services. These essential health benefits should be consistent with the full scope of benefits outlined in Bright Futures: Guidelines for Health Supervision of Infants, Children, and Adolescents (including health supervision visits, recommended immunizations, screening for high-risk conditions, and adequate counseling and treatment of conditions related to sexual, reproductive, mental, and behavioral health and substance use disorder). In this way, all adolescents can access the full range of services needed during this developmentally critical period to secure optimal physical and mental health on entry into midadulthood.
All health plans should provide preventive services without member cost sharing. In addition, to reduce financial barriers to care for adolescents, payers should limit the burden on families by reducing or eliminating copayments and eliminating coinsurance for visits related to anticipatory guidance and/or treatment of sexual and reproductive health, behavioral health, and immunization visits.
To provide sufficient payment to physicians and other health care providers for medical services to adolescents, insurers’ claims systems should recognize and pay for all preventive medicine Current Procedural Terminology codes related to services for health and behavior assessment, counseling, risk screening, and/or appropriate interventions recommended in Bright Futures : Guidelines for Health Supervision of Infants, Children, and Adolescents. These services should not be bundled under a single health maintenance Current Procedural Terminology code.
Government and private insurance payers should increase the relative value unit allocation and level of payment for pediatricians delivering care and clinical preventive services to adolescents to a level that is commensurate with the time and effort expended, including health maintenance services, screening, and counseling.
The Centers for Medicare and Medicaid Services should mandate that payers provide enhanced access to cost-effective and clinically sound behavioral health services for adolescents, ensure that payment for all mental health services is more equitable with payment provided for medical and surgical services, and ensure that pediatricians are paid for mental health services provided during health maintenance and follow-up visits.
American Academy of Pediatrics
Confidentiality Protections for Adolescents and Young Adults in the Health Care Billing and Insurance Claims Process: http://pediatrics.aappublications.org/content/137/5/e20160593
Office-Based Care for Lesbian, Gay, Bisexual, Transgender, and Questioning Youth: http://pediatrics.aappublications.org/content/pediatrics/132/1/e297.full.pdf
Society for Adolescent Health and Medicine
Resources for adolescents and parents are online resources aimed specifically at adolescents and their parents. Health care providers and youth-serving professionals can offer these additional resources or print a 1-page reference sheet (PDF) for adolescents and parents looking for additional information, including support groups, peer networks, helplines, treatment locators, and advocacy opportunities.
Mental Health Resources for Adolescents: http://www.adolescenthealth.org/Topics-in-Adolescent-Health/Mental-Health/Mental-Health-Resources-For-Adolesc.aspx
Mental Health Resources for Parents of Adolescents: http://www.adolescenthealth.org/Topics-in-Adolescent-Health/Mental-Health/Mental-Health-Resources-For-Parents-of-Adolescents.aspx
Substance Use Resources for Adolescents: http://www.adolescenthealth.org/Topics-in-Adolescent-Health/Substance-Use/Substance-Use-Resources-For-Adolesc.aspx
Substance Use Resources for Parents of Adolescents: http://www.adolescenthealth.org/Topics-in-Adolescent-Health/Substance-Use/Substance-Use-Resources-For-Parents-of-Adolesc.aspx
Confidentiality in Health Care Resources for Adolescents and Parents of Adolescents: http://www.adolescenthealth.org/Topics-in-Adolescent-Health/Confidentiality/Confidentiality-Resources-For-Adolesc.aspx
Sexual and Reproductive Health Resources for Adolescents: http://www.adolescenthealth.org/Topics-in-Adolescent-Health/Sexual-Reproductive-Health/Sexual-Reproductive-Health-Resources-For-Adolesc.aspx
Sexual and Reproductive Health Resources for Parents of Adolescents: http://www.adolescenthealth.org/Topics-in-Adolescent-Health/Sexual-Reproductive-Health/SandRH-Resources-For-Parents-of-Adolesc.aspx
Physical and Psychosocial Development Resources for Adolescents: http://www.adolescenthealth.org/Topics-in-Adolescent-Health/Physical-and-Psychosocial-Development/Physical-Pschosocial-Develop-Resources-For-Adolesc.aspx
Physical and Psychosocial Development Resources for Parents of Adolescents: http://www.adolescenthealth.org/Topics-in-Adolescent-Health/Physical-and-Psychosocial-Development/Physical-Psych-Resources-For-Parents-of-Adolesc.aspx
Transition Resources
General resources.
National Health Care Transition Center ( www.gottransition.org )
Family Voices, Inc ( www.familyvoices.org )
National Alliance to Advance Adolescent Health ( www.thenationalalliance.org )
Transition Care Plans
AAP/National Center for Medical Home Implementation ( www.medicalhomeinfo.org/how/care_delivery/transitions.aspx )
British Columbia Ministry of Children and Family Development, “Transition Planning for Youth With Special Needs” ( www.mcf.gov.bc.ca/spec_needs/pdf/support_guide.pdf )
University of Washington, Adolescent Health Transition Project ( http://depts.washington.edu/healthtr )
Transition Assessment and Evaluation Tools
AAP/National Center for Medical Home Implementation ( www.medicalhomeinfo.org/health/trans.html )
JaxHATS, evaluation tools for youth and caregivers and training materials for medical providers ( www.jaxhats.ufl.edu/docs )
Texas Children's Hospital transition template ( http://leah.mchtraining.net/bcm/resources/tracs )
Carolina Health and Transition Project ( www.mahec.net/quality/chat.aspx?a=10 )
Wisconsin Community of Practice on Transition ( www.waisman.wisc.edu/wrc/pdf/pubs/THCL.pdf )
National Alliance to End Homelessness
• http://www.endhomelessness.org/
Policy statements from the American Academy of Pediatrics benefit from expertise and resources of liaisons and internal (AAP) and external reviewers. However, policy statements from the American Academy of Pediatrics may not reflect the views of the liaisons or the organizations or government agencies that they represent.
The guidance in this statement does not indicate an exclusive course of treatment or serve as a standard of medical care. Variations, taking into account individual circumstances, may be appropriate.
All policy statements from the American Academy of Pediatrics automatically expire 5 years after publication unless reaffirmed, revised, or retired at or before that time.
Drs Alderman and Breuner were equally responsible for writing and revising this policy statement with input from various internal and external reviewers as well as the Board of Directors, and both authors approved the final manuscript as submitted.
This document is copyrighted and is property of the American Academy of Pediatrics and its Board of Directors. All authors have filed conflict of interest statements with the American Academy of Pediatrics. Any conflicts have been resolved through a process approved by the Board of Directors. The American Academy of Pediatrics has neither solicited nor accepted any commercial involvement in the development of the content of this publication.
FUNDING: No external funding.
confidence interval
Patient-Centered Medical Home
Elizabeth M. Alderman, MD, FSAHM, FAAP
Cora C. Breuner, MD, MPH, FAAP
Cora Breuner, MD, MPH, FAAP, Chairperson
Laura K. Grubb, MD, MPH, FAAP
Makia E. Powers, MD, MPH, FAAP
Krishna Upadhya, MD, FAAP
Stephenie B. Wallace, MD, FAAP
Laurie Hornberger, MD, MPH, FAAP – Section on Adolescent Health
Liwei L. Hua, MD, PhD – American Academy of Child and Adolescent Psychiatry
Margo A. Lane, MD, FRCPC, FAAP – Canadian Paediatric Society
Meredith Loveless, MD, FACOG – American College of Obstetricians and Gynecologists
Seema Menon, MD – North American Society of Pediatric and Adolescent Gynecology
CDR Lauren B. Zapata, PhD, MSPH – Centers for Disease Control and Prevention
Karen S. Smith
James D. Baumberger, MPP
Competing Interests
Advertising Disclaimer »
Citing articles via
Email alerts.

Affiliations
- Editorial Board
- Editorial Policies
- Journal Blogs
- Pediatrics On Call
- Online ISSN 1098-4275
- Print ISSN 0031-4005
- Pediatrics Open Science
- Hospital Pediatrics
- Pediatrics in Review
- AAP Grand Rounds
- Latest News
- Pediatric Care Online
- Red Book Online
- Pediatric Patient Education
- AAP Toolkits
- AAP Pediatric Coding Newsletter
First 1,000 Days Knowledge Center
Institutions/librarians, group practices, licensing/permissions, integrations, advertising.
- Privacy Statement | Accessibility Statement | Terms of Use | Support Center | Contact Us
- © Copyright American Academy of Pediatrics
This Feature Is Available To Subscribers Only
Sign In or Create an Account
- Search Menu
- Advance articles
- Author Guidelines
- Submission Site
- About Children & Schools
- About the National Association of Social Workers
- Editorial Board
- Advertising and Corporate Services
- Journals Career Network
- Self-Archiving Policy
- Dispatch Dates
- Journals on Oxford Academic
- Books on Oxford Academic

Article Contents
Literature review, alive program, implications for school social work practice.
- < Previous
Trauma and Early Adolescent Development: Case Examples from a Trauma-Informed Public Health Middle School Program
- Article contents
- Figures & tables
- Supplementary Data
Jason Scott Frydman, Christine Mayor, Trauma and Early Adolescent Development: Case Examples from a Trauma-Informed Public Health Middle School Program, Children & Schools , Volume 39, Issue 4, October 2017, Pages 238–247, https://doi.org/10.1093/cs/cdx017
- Permissions Icon Permissions
Middle-school-age children are faced with a variety of developmental tasks, including the beginning phases of individuation from the family, building peer groups, social and emotional transitions, and cognitive shifts associated with the maturation process. This article summarizes how traumatic events impair and complicate these developmental tasks, which can lead to disruptive behaviors in the school setting. Following the call by Walkley and Cox for more attention to be given to trauma-informed schools, this article provides detailed information about the Animating Learning by Integrating and Validating Experience program: a school-based, trauma-informed intervention for middle school students. This public health model uses psychoeducation, cognitive differentiation, and brief stress reduction counseling sessions to facilitate socioemotional development and academic progress. Case examples from the authors’ clinical work in the New Haven, Connecticut, urban public school system are provided.
Within the U.S. school system there is growing awareness of how traumatic experience negatively affects early adolescent development and functioning ( Chanmugam & Teasley, 2014 ; Perfect, Turley, Carlson, Yohannan, & Gilles, 2016 ; Porche, Costello, & Rosen-Reynoso, 2016 ; Sibinga, Webb, Ghazarian, & Ellen, 2016 ; Turner, Shattuck, Finkelhor, & Hamby, 2017 ; Woodbridge et al., 2016 ). The manifested trauma symptoms of these students have been widely documented and include self-isolation, aggression, and attentional deficit and hyperactivity, producing individual and schoolwide difficulties ( Cook et al., 2005 ; Iachini, Petiwala, & DeHart, 2016 ; Oehlberg, 2008 ; Sajnani, Jewers-Dailley, Brillante, Puglisi, & Johnson, 2014 ). To address this vulnerability, school social workers should be aware of public health models promoting prevention, data-driven investigation, and broad-based trauma interventions ( Chafouleas, Johnson, Overstreet, & Santos, 2016 ; Johnson, 2012 ; Moon, Williford, & Mendenhall, 2017 ; Overstreet & Chafouleas, 2016 ; Overstreet & Matthews, 2011 ). Without comprehensive and effective interventions in the school setting, seminal adolescent developmental tasks are at risk.
This article follows the twofold call by Walkley and Cox (2013) for school social workers to develop a heightened awareness of trauma exposure's impact on childhood development and to highlight trauma-informed practices in the school setting. In reference to the former, this article will not focus on the general impact of toxic stress, or chronic trauma, on early adolescents in the school setting, as this work has been widely documented. Rather, it begins with a synthesis of how exposure to trauma impairs early adolescent developmental tasks. As to the latter, we will outline and discuss the Animating Learning by Integrating and Validating Experience (ALIVE) program, a school-based, trauma-informed intervention that is grounded in a public health framework. The model uses psychoeducation, cognitive differentiation, and brief stress reduction sessions to promote socioemotional development and academic progress. We present two clinical cases as examples of trauma-informed, school-based practice, and then apply their experience working in an urban, public middle school to explicate intervention theory and practice for school social workers.
Impact of Trauma Exposure on Early Adolescent Developmental Tasks
Social development.
Impact of Trauma on Early Adolescent Development
Traumatic experiences may create difficulty with developing and differentiating another person's point of view (that is, mentalization) due to the formation of rigid cognitive schemas that dictate notions of self, others, and the external world ( Frydman & McLellan, 2014 ). For early adolescents, the ability to diversify a single perspective with complexity is central to modulating affective experience. Without the capacity to diversify one's perspective, there is often difficulty differentiating between a nonthreatening current situation that may harbor reminders of the traumatic experience and actual traumatic events. Incumbent on the school social worker is the need to help students understand how these conflicts may trigger a memory of harm, abandonment, or loss and how to differentiate these past memories from the present conflict. This is of particular concern when these reactions are conflated with more common middle school behaviors such as withdrawing, blaming, criticizing, and gossiping ( Card, Stucky, Sawalani, & Little, 2008 ).
Encouraging cognitive discrimination is particularly meaningful given that the second social developmental task for early adolescents is the re-orientation of their primary relationships with family toward peers ( Henderson & Thompson, 2010 ). This shift may become complicated for students facing traumatic stress, resulting in a stunted movement away from familiar connections or a displacement of dysfunctional family relationships onto peers. For example, in the former, a student who has witnessed and intervened to protect his mother from severe domestic violence might believe he needs to sacrifice himself and be available to his mother, forgoing typical peer interactions. In the latter, a student who was beaten when a loud, intoxicated family member came home might become enraged, anxious, or anticipate violence when other students raise their voices.
Cognitive Development and Emotional Regulation
During normative early adolescent development, the prefrontal cortex undergoes maturational shifts in cognitive and emotional functioning, including increased impulse control and affect regulation ( Wigfield, Lutz, & Wagner, 2005 ). However, these developmental tasks can be negatively affected by chronic exposure to traumatic events. Stressful situations often evoke a fear response, which inhibits executive functioning and commonly results in a fight-flight-freeze reaction. If a student does not possess strong anxiety management skills to cope with reminders of the trauma, the student is prone to further emotional dysregulation, lowered frustration tolerance, and increased behavioral problems and depressive symptoms ( Iachini et al., 2016 ; Saltzman, Steinberg, Layne, Aisenberg, & Pynoos, 2001 ).
Typical cognitive development in early adolescence is defined by the ambiguity of a transitional stage between childhood remedial capacity and adult refinement ( Casey & Caudle, 2013 ; Van Duijvenvoorde & Crone, 2013 ). Casey and Caudle (2013) found that although adolescents performed equally as well as, if not better than, adults on a self-control task when no emotional information was present, the introduction of affectively laden social cues resulted in diminished performance. The developmental challenge for the early adolescent then is to facilitate the coordination of this ever-shifting dynamic between cognition and affect. Although early adolescents may display efficient and logically informed behaviors, they may struggle to sustain these behaviors, especially in the presence of emotional stimuli ( Casey & Caudle, 2013 ; Van Duijvenvoorde & Crone, 2013 ). Because trauma often evokes an emotional response ( Johnson & Lubin, 2015 ), these findings insinuate that those early adolescents who are chronically exposed will have ongoing regulation difficulties. Further empirical findings considering the cognitive effects of trauma exposure on the adolescent brain have highlighted detriments in working memory, inhibition, memory, and planning ability ( Moradi, Neshat Doost, Taghavi, Yule, & Dalgleish, 1999 ).
Using a Public Health Framework for School-Based, Trauma-Informed Services
The need for a more informed and comprehensive approach to addressing trauma within the schools has been widely articulated ( Chafouleas et al., 2016 ; Durlak, Weissberg, Dymnicki, Taylor, & Schellinger, 2011 ; Jaycox, Kataoka, Stein, Langley, & Wong, 2012 ; Overstreet & Chafouleas, 2016 ; Perry & Daniels, 2016 ). Overstreet and Matthews (2011) suggested that using a public health model to address trauma in schools will promote prevention, early identification, and data-driven investigation and yield broad-based intervention on a policy and communitywide level. A public health approach focuses on developing interventions that address the underlying causal processes that lead to social, emotional, and cognitive maladjustment. Opening the dialogue to the entire student body, as well as teachers and administrators, promotes inclusion and provides a comprehensive foundation for psychoeducation, assessment, and prevention.
ALIVE: A Comprehensive Public Health Intervention for Middle School Students
Note: ALIVE = Animating Learning by Integrating and Validating Experience.
Psychoeducation
The classroom is a place traditionally dedicated to academic pursuits; however, it also serves as an indicator of trauma's impact on cognitive functioning evidenced by poor grades, behavioral dysregulation, and social turbulence. ALIVE practitioners conduct weekly trauma-focused dialogues in the classroom to normalize conversations addressing trauma, to recruit and rehearse more adaptive cognitive skills, and to engage in an insight-oriented process ( Sajnani et al., 2014 ).
Using a parable as a projective tool for identification and connection, the model helps students tolerate direct discussions about adverse experiences. The ALIVE practitioner begins each academic year by telling the parable of a woman named Miss Kendra, who struggled to cope with the loss of her 10-year-old child. Miss Kendra is able to make meaning out of her loss by providing support for schoolchildren who have encountered adverse experiences, serving as a reminder of the strength it takes to press forward after a traumatic event. The intention of this parable is to establish a metaphor for survival and strength to fortify the coping skills already held by trauma-exposed middle school students. Furthermore, Miss Kendra offers early adolescents an opportunity to project their own needs onto the story, creating a personalized figure who embodies support for socioemotional growth.
Following this parable, the students’ attention is directed toward Miss Kendra's List, a poster that is permanently displayed in the classroom. The list includes a series of statements against adolescent maltreatment, comprehensively identifying various traumatic stressors such as witnessing domestic violence; being physically, verbally, or sexually abused; and losing a loved one to neighborhood violence. The second section of the list identifies what may happen to early adolescents when they experience trauma from emotional, social, and academic perspectives. The practitioner uses this list to provide information about the nature and impact of trauma, while modeling for students and staff the ability to discuss difficult experiences as a way of connecting with one another with a sense of hope and strength.
Furthermore, creating a dialogue about these issues with early adolescents facilitates a culture of acceptance, tolerance, and understanding, engendering empathy and identification among students. This fostering of interpersonal connection provides a reparative and differentiated experience to trauma ( Hartling & Sparks, 2008 ; Henderson & Thompson, 2010 ; Johnson & Lubin, 2015 ) and is particularly important given the peer-focused developmental tasks of early adolescence. The positive feelings evoked through classroom-based conversation are predicated on empathic identification among the students and an accompanying sense of relief in understanding the scope of trauma's impact. Furthermore, the consistent appearance of and engagement by the ALIVE practitioner, and the continual presence of Miss Kendra's list, effectively counters traumatically informed expectations of abandonment and loss while aligning with a public health model that attends to the impact of trauma on a regular, systemwide basis.
Participatory and Somatic Indicators for Informal Assessment during the Psychoeducation Component of the ALIVE Intervention
Notes: ALIVE = Animating Learning by Integrating and Validating Experience. Examples are derived from authors’ clinical experiences.
In addition to behavioral symptoms, the content of conversation is considered. All practitioners in the ALIVE program are mandated reporters, and any content presented that meets criteria for suspicion of child maltreatment is brought to the attention of the school leadership and ALIVE director. According to Johnson (2012) , reports of child maltreatment to the Connecticut Department of Child and Family Services have actually decreased in the schools where the program has been implemented “because [the ALIVE program is] catching problems well before they have risen to the severity that would require reporting” (p. 17).
Case Example 1
The following demonstrates a middle school classroom psychoeducation session and assessment facilitated by an ALIVE practitioner (the first author). All names and identifying characteristics have been changed to protect confidentiality.
Ms. Skylar's seventh grade class comprised many students living in low-income housing or in a neighborhood characterized by high poverty and frequent criminal activity. During the second week of school, I introduced myself as a practitioner who was here to speak directly about difficult experiences and how these instances might affect academic functioning and students’ thoughts about themselves, others, and their environment.
After sharing the Miss Kendra parable and list, I invited the students to share their thoughts about Miss Kendra and her journey. Tyreke began the conversation by wondering whether Miss Kendra lost her child to gun violence, exploring the connection between the list and the story and his own frequent exposure to neighborhood shootings. To transition a singular connection to a communal one, I asked the students if this was a shared experience. The majority of students nodded in agreement. I referred the students back to the list and asked them to identify how someone's school functioning or mood may be affected by ongoing neighborhood gun violence. While the students read the list, I actively monitored reactions and scanned for inattention and active avoidance. Performing both active facilitation of discussion and monitoring students’ reactions is critical in accomplishing the goals of providing quality psychoeducation and identifying at-risk students for intervention.
After inspection, Cleo remarked that, contrary to a listed outcome on Miss Kendra's list, neighborhood gun violence does not make him feel lonely; rather, he “doesn't care about it.” Slumped down in his chair, head resting on his crossed arms on the desk in front of him, Cleo's body language suggested a somatized disengagement. I invited other students to share their individual reactions. Tyreke agreed that loneliness is not the identified affective experience; rather, for him, it's feeling “mad or scared.” Immediately, Greg concurred, expressing that “it makes me more mad, and I think about my family.”
Encouraging a variety of viewpoints, I stated, “It sounds like it might make you mad, scared, and may even bring up thoughts about your family. I wonder why people have different reactions?” Doing so moved the conversation into a phase of deeper reflection, simultaneously honoring the students’ voiced experience while encouraging critical thinking. A number of students responded by offering connections to their lives, some indicating they had difficulty identifying feelings. I reflected back, “Sometimes people feel something, but can't really put their finger on it, and sometimes they know exactly how they feel or who it makes them think about.”
I followed with a question: “How do you think it affects your schoolwork or feelings when you're in school?” Greg and Natalia both offered that sometimes difficult or confusing thoughts can consume their whole day, even while in class. Sharon began to offer a related comment when Cleo interrupted by speaking at an elevated volume to his desk partner, Tyreke. The two began to snicker and pull focus. By the time they gained the class's full attention, Cleo was openly laughing and pushing his chair back, stating, “No way! She DID!? That's crazy”; he began to stand up, enlisting Tyreke in the process. While this disruption may be viewed as a challenge to the discussion, it is essential to understand all behavior in context of the session's trauma content. Therefore, Cleo's outburst was interpreted as a potential avenue for further exploration of the topic regarding gun violence and difficulties concentrating. In turn, I posed this question to the class: “Should we talk about this stuff? I wonder if sometimes people have a hard time tolerating it. Can anybody think of why it might be important? Sharon, I think you were saying something about this.” While Sharon continued to share, Cleo and Tyreke gradually shifted their attention back to the conversation. I noted the importance of an individual follow-up with Cleo.
Natalia jumped back in the conversation, stating, “I think we talk about stuff like this so we know about it and can help people with it.” I checked in with the rest of the class about this strategy for coping with the impact of trauma exposure on school functioning: “So it sounds like these thoughts have a pretty big impact on your day. If that's the case, how do you feel less worried or mad or scared?” Marta quickly responded, “You could talk to someone.” I responded, “Part of my job here is to be a person to talk to one-on-one about these things. Hopefully, it will help you feel better to get some of that stuff off your chest.” The students nodded, acknowledging that I would return to discuss other items on the list and that there would be opportunities to check in with me individually if needed.
On reflection, Cleo's disruption in the discussion may be attributed to his personal difficulty emotionally managing intrusive thoughts while in school. This clinical assumption was not explicitly named in the moment, but was noted as information for further individual follow-up. When I met individually with Cleo, Cleo reported that his cousin had been shot a month ago, causing him to feel confused and angry. I continued to work with him individually, which resulted in a reduction of behavioral disruptions in the classroom.
In the preceding case example, the practitioner performed a variety of public health tasks. Foremost was the introduction of how traumatic experience may affect individuals and their relationships with others and their role as a student. Second, the practitioner used Miss Kendra and her list as a foundational mechanism to ground the conversation and serve as a reference point for the students’ experience. Finally, the practitioner actively monitored individual responses to the material as a means of identifying students who may require more support. All three of these processes are supported within the public health framework as a means toward assessment and early intervention for early adolescents who may be exposed to trauma.
Individualized Stress Reduction Intervention
Students are seen for individualized support if they display significant externalizing or internalizing trauma-related behavior. Students are either self-referred; referred by a teacher, administrator, or staff member; or identified by an ALIVE practitioner. Following the principle of immediate engagement based on emergent traumatic material, individual sessions are brief, lasting only 15 to 20 minutes. Using trauma-centered psychotherapy ( Johnson & Lubin, 2015 ), a brief inquiry addressing the current problem is conducted to identify the trauma trigger connected to the original harm, fostering cognitive discrimination. Conversation about the adverse experience proceeds in a calm, direct way focusing on differentiating between intrusive memories and the current situation at school ( Sajnani et al., 2014 ). Once the student exhibits greater emotional regulation, the ALIVE practitioner returns the student to the classroom in a timely manner and may provide either brief follow-up sessions for preventive purposes or, when appropriate, refer the student to more regular, clinical support in or out of the school.
Case Example 2
The following case example is representative of the brief, immediate, and open engagement with traumatic material and encouragement of cognitive discrimination. This intervention was conducted with a sixth grade student, Jacob (name and identifying information changed to ensure confidentiality), by an ALIVE practitioner (the second author).
I found Jacob in the hallway violently shaking a trash can, kicking the classroom door, and slamming his hands into the wall and locker. His teacher was standing at the door, distressed, stating, “Jacob, you need to calm down and go to the office, or I'm calling home!” Jacob yelled, “It's not fair, it was him, not me! I'm gonna fight him!” As I approached, I asked what was making him so angry, but he said, “I don't want to talk about it.” Rather than asking him to calm down or stop slamming objects, I instead approached the potential memory agitating him, stating, “My guess is that you are angry for a very good reason.” Upon this simple connection, he sighed and stopped kicking the trash can and slamming the wall. Jacob continued to demonstrate physical and emotional activation, pacing the hallway and making a fist; however, he was able to recount putting trash in the trash can when a peer pushed him from behind, causing him to yell. Jacob explained that his teacher heard him yelling and scolded him, making him more mad. Jacob stated, “She didn't even know what happened and she blamed me. I was trying to help her by taking out all of our breakfast trash. It's not fair.”
The ALIVE practitioner listens to students’ complaints with two ears, one for the current complaint and one for affect-laden details that may be connected to the original trauma to inquire further into the source of the trigger. Affect-laden details in case example 2 include Jacob's anger about being blamed (rather than toward the student who pushed him), his original intention to help, and his repetition of the phrase “it's not fair.” Having met with Jacob previously, I was aware that his mother suffers from physical and mental health difficulties. When his mother is not doing well, he (as the parentified child) typically takes care of the household, performing tasks like cooking, cleaning, and helping with his two younger siblings and older autistic brother. In the past, Jacob has discussed both idealizing his mother and holding internalized anger that he rarely expresses at home because he worries his anger will “make her sick.”
I know sometimes when you are trying to help mom, there are times she gets upset with you for not doing it exactly right, or when your brothers start something, she will blame you. What just happened sounds familiar—you were trying to help your teacher by taking out the garbage when another student pushed you, and then you were the one who got in trouble.
Jacob nodded his head and explained that he was simply trying to help.
I moved into a more detailed inquiry, to see if there was a more recent stressor I was unaware of. When I asked how his mother was doing this week, Jacob revealed that his mother's health had deteriorated and his aunt had temporarily moved in. Jacob told me that he had been yelled at by both his mother and his aunt that morning, when his younger brother was not ready for school. I asked, “I wonder if when the student pushed you it reminded you of getting into trouble because of something your little brother did this morning?” Jacob nodded. The displacement was clear: He had been reminded of this incident at school and was reacting with anger based on his family dynamic, and worries connected to his mother.
My guess is that you were a mix of both worried and angry by the time you got to school, with what's happening at home. You were trying to help with the garbage like you try to help mom when she isn't doing well, so when you got pushed it was like your brother being late, and then when you got blamed by your teacher it was like your mom and aunt yelling, and it all came flooding back in. The problem is, you let out those feelings here. Even though there are some similar things, it's not totally the same, right? Can you tell me what is different?
Jacob nodded and was able to explain that the other student was probably just playing and did not mean to get him into trouble, and that his teacher did not usually yell at him or make him worried. Highlighting this important differentiation, I replied, “Right—and fighting the student or yelling at the teacher isn't going to solve this, but more importantly, it isn't going to make your mom better or have your family go any easier on you either.” Jacob stated that he knew this was true.
I reassured Jacob that I could help him let out those feelings of worry and anger connected to home so they did not explode out at school and planned to meet again. Jacob confirmed that he was willing to do that. He was able to return to the classroom without incident, with the entire intervention lasting less than 15 minutes.
In case example 2, the practitioner was available for an immediate engagement with disturbing behaviors as they were happening by listening for similarities between the current incident and traumatic stressors; asking for specific details to more effectively help Jacob understand how he was being triggered in school; providing psychoeducation about how these two events had become confused and aiding him in cognitively differentiating between the two; and, last, offering to provide further support to reduce future incidents.
Germane to the practice of school social work is the ability to work flexibly within a public health model to attend to trauma within the school setting. First, we suggest that a primary implication for school social workers is not to wait for explicit problems related to known traumatic experiences to emerge before addressing trauma in the school, but, rather, to follow a model of prevention-assessment-intervention. School social workers are in a unique position within the school system to disseminate trauma-informed material to both students and staff in a preventive capacity. Facilitating this implementation will help to establish a tone and sharpened focus within the school community, norming the process of articulating and engaging with traumatic material. In the aforementioned classroom case example, we have provided a sample of how school social workers might work with entire classrooms on a preventive basis regarding trauma, rather than waiting for individual referrals.
Second, in addition to functional behavior assessments and behavior intervention plans, school social workers maintain a keen eye for qualitative behavioral assessment ( National Association of Social Workers, 2012 ). Using this skill set within a trauma-informed model will help to identify those students in need who may be reluctant or resistant to explicitly ask for help. As called for by Walkley and Cox (2013) , we suggest that using the information presented in Table 1 will help school social workers understand, identify, and assess the impact of trauma on early adolescent developmental tasks. If school social workers engage on a classroom level in trauma psychoeducation and conversations, the information in Table 3 may assist with assessment of children and provide a basis for checking in individually with students as warranted.
Third, school social workers are well positioned to provide individual targeted, trauma-informed interventions based on previous knowledge of individual trauma and through widespread assessment ( Walkley & Cox, 2013 ). The individual case example provides one way of immediately engaging with students who are demonstrating trauma-based behaviors. In this model, school social workers engage in a brief inquiry addressing the current trauma to identify the trauma trigger, discuss the adverse experience in a calm but direct way, and help to differentiate between intrusive memories and the current situation at school. For this latter component, the focus is on cognitive discrimination and emotional regulation so that students can reengage in the classroom within a short time frame.
Fourth, given social work's roots in collaboration and community work, school social workers are encouraged to use a systems-based approach in partnering with allied practitioners and institutions ( D'Agostino, 2013 ), thus supporting the public health tenet of establishing and maintaining a link to the wider community. This may include referring students to regular clinical support in or out of the school. Although the implementation of a trauma-informed program will vary across schools, we suggest that school social workers have the capacity to use a public health school intervention model to ecologically address the psychosocial and behavioral issues stemming from trauma exposure.
As increasing attention is being given to adverse childhood experiences, a tiered approach that uses a public health framework in the schools is necessitated. Nevertheless, there are some limitations to this approach. First, although the interventions outlined here are rooted in prevention and early intervention, there are times when formal, intensive treatment outside of the school setting is warranted. Second, the ALIVE program has primarily been implemented by ALIVE practitioners; the results from piloting this public health framework in other school settings with existing school personnel, such as school social workers, will be necessary before widespread replication.
The public health framework of prevention-assessment-intervention promotes continual engagement with middle school students’ chronic exposure to traumatic stress. There is a need to provide both broad-based and individualized support that seeks to comprehensively ameliorate the social, emotional, and cognitive consequences on early adolescent developmental milestones associated with traumatic experiences. We contend that school social workers are well positioned to address this critical public health issue through proactive and widespread psychoeducation and assessment in the schools, and we have provided case examples to demonstrate one model of doing this work within the school day. We hope that this article inspires future writing about how school social workers individually and systemically address trauma in the school system. In alignment with Walkley and Cox (2013) , we encourage others to highlight their practice in incorporating trauma-informed, school-based programming in an effort to increase awareness of effective interventions.
Card , N. A. , Stucky , B. D. , Sawalani , G. M. , & Little , T. D. ( 2008 ). Direct and indirect aggression during childhood and adolescence: A meta-analytic review of gender difference, intercorrelations, and relations to maladjustment . Child Development, 79 , 1185 – 1229 .
Google Scholar
Casey , B. J. , & Caudle , K. ( 2013 ). The teenage brain: Self control . Current Directions in Psychological Science, 22 ( 2 ), 82 – 87 .
Chafouleas , S. M. , Johnson , A. H. , Overstreet , S. , & Santos , N. M. ( 2016 ). Toward a blueprint for trauma-informed service delivery in schools . School Mental Health, 8 ( 1 ), 144 – 162 .
Chanmugam , A. , & Teasley , M. L. ( 2014 ). What should school social workers know about children exposed to intimate partner violence? [Editorial]. Children & Schools, 36 , 195 – 198 .
Cook , A. , Spinazzola , J. , Ford , J. , Lanktree , C. , Blaustein , M. , Cloitre , M. , et al. . ( 2005 ). Complex trauma in children and adolescents . Psychiatric Annals, 35 , 390 – 398 .
D'Agostino , C. ( 2013 ). Collaboration as an essential social work skill [Resources for Practice] . Children & Schools, 35 , 248 – 251 .
Durlak , J. A. , Weissberg , R. P. , Dymnicki , A. B. , Taylor , R. D. , & Schellinger , K. B. ( 2011 ). The impact of enhancing students’ social and emotional learning: A meta-analysis of school-based universal interventions . Child Development, 82 , 405 – 432 .
Frydman , J. S. , & McLellan , L. ( 2014 ). Complex trauma and executive functioning: Envisioning a cognitive-based, trauma-informed approach to drama therapy. In N. Sajnani & D. R. Johnson (Eds.), Trauma-informed drama therapy: Transforming clinics, classrooms, and communities (pp. 179 – 205 ). Springfield, IL : Charles C Thomas .
Google Preview
Hartling , L. , & Sparks , J. ( 2008 ). Relational-cultural practice: Working in a nonrelational world . Women & Therapy, 31 , 165 – 188 .
Henderson , D. , & Thompson , C. ( 2010 ). Counseling children (8th ed.). Belmont, CA : Brooks-Cole .
Iachini , A. L. , Petiwala , A. F. , & DeHart , D. D. ( 2016 ). Examining adverse childhood experiences among students repeating the ninth grade: Implications for school dropout prevention . Children & Schools, 38 , 218 – 227 .
Jaycox , L. H. , Kataoka , S. H. , Stein , B. D. , Langley , A. K. , & Wong , M. ( 2012 ). Cognitive behavioral intervention for trauma in schools . Journal of Applied School Psychology, 28 , 239 – 255 .
Johnson , D. R. ( 2012 ). Ask every child: A public health initiative addressing child maltreatment [White paper]. Retrieved from http://www.traumainformedschools.org/publications.html
Johnson , D. R. , & Lubin , H. ( 2015 ). Principles and techniques of trauma-centered psychotherapy . Arlington, VA : American Psychiatric Publishing .
Moon , J. , Williford , A. , & Mendenhall , A. ( 2017 ). Educators’ perceptions of youth mental health: Implications for training and the promotion of mental health services in schools . Child and Youth Services Review, 73 , 384 – 391 .
Moradi , A. R. , Neshat Doost , H. T. , Taghavi , M. R. , Yule , W. , & Dalgleish , T. ( 1999 ). Everyday memory deficits in children and adolescents with PTSD: Performance on the Rivermead Behavioural Memory Test . Journal of Child Psychology and Psychiatry, 40 , 357 – 361 .
National Association of Social Workers . ( 2012 ). NASW standards for school social work services . Retrieved from http://www.naswdc.org/practice/standards/NASWSchoolSocialWorkStandards.pdf
Oehlberg , B. ( 2008 ). Why schools need to be trauma informed . Trauma and Loss: Research and Interventions, 8 ( 2 ), 1 – 4 .
Overstreet , S. , & Chafouleas , S. M. ( 2016 ). Trauma-informed schools: Introduction to the special issue . School Mental Health, 8 ( 1 ), 1 – 6 .
Overstreet , S. , & Matthews , T. ( 2011 ). Challenges associated with exposure to chronic trauma: Using a public health framework to foster resilient outcomes among youth . Psychology in the Schools, 48 , 738 – 754 .
Perfect , M. , Turley , M. , Carlson , J. S. , Yohannan , J. , & Gilles , M. S. ( 2016 ). School-related outcomes of traumatic event exposure and traumatic stress symptoms in students: A systematic review of research from 1990 to 2015 . School Mental Health, 8 ( 1 ), 7 – 43 .
Perry , D. L. , & Daniels , M. L. ( 2016 ). Implementing trauma-informed practices in the school setting: A pilot study . School Mental Health, 8 ( 1 ), 177 – 188 .
Porche , M. V. , Costello , D. M. , & Rosen-Reynoso , M. ( 2016 ). Adverse family experiences, child mental health, and educational outcomes for a national sample of students . School Mental Health, 8 ( 1 ), 44 – 60 .
Sajnani , N. , Jewers-Dailley , K. , Brillante , A. , Puglisi , J. , & Johnson , D. R. ( 2014 ). Animating Learning by Integrating and Validating Experience. In N. Sajnani & D. R. Johnson (Eds.), Trauma-informed drama therapy: Transforming clinics, classrooms, and communities (pp. 206 – 242 ). Springfield, IL : Charles C Thomas .
Saltzman , W. R. , Steinberg , A. M. , Layne , C. M. , Aisenberg , E. , & Pynoos , R. S. ( 2001 ). A developmental approach to school-based treatment of adolescents exposed to trauma and traumatic loss . Journal of Child and Adolescent Group Therapy, 11 ( 2–3 ), 43 – 56 .
Sibinga , E. M. , Webb , L. , Ghazarian , S. R. , & Ellen , J. M. ( 2016 ). School-based mindfulness instruction: An RCT . Pediatrics, 137 ( 1 ), e20152532 .
Tucker , C. , Smith-Adcock , S. , & Trepal , H. C. ( 2011 ). Relational-cultural theory for middle school counselors . Professional School Counseling, 14 , 310 – 316 .
Turner , H. A. , Shattuck , A. , Finkelhor , D. , & Hamby , S. ( 2017 ). Effects of poly-victimization on adolescent social support, self-concept, and psychological distress . Journal of Interpersonal Violence, 32 , 755 – 780 .
van der Kolk , B. A. ( 2005 ). Developmental trauma disorder: Toward a rational diagnosis for children with complex trauma histories . Psychiatric Annals, 35 , 401 – 408 .
Van Duijvenvoorde , A.C.K. , & Crone , E. A. ( 2013 ). The teenage brain: A neuroeconomic approach to adolescent decision making . Current Directions in Psychological Science, 22 ( 2 ), 114 – 120 .
Walkley , M. , & Cox , T. L. ( 2013 ). Building trauma-informed schools and communities [Trends & Resources] . Children & Schools, 35 , 123 – 126 .
Wigfield , A. W. , Lutz , S. L. , & Wagner , L. ( 2005 ). Early adolescents’ development across the middle school years: Implications for school counselors . Professional School Counseling, 9 ( 2 ), 112 – 119 .
Woodbridge , M. W. , Sumi , W. C. , Thornton , S. P. , Fabrikant , N. , Rouspil , K. M. , Langley , A. K. , & Kataoka , S. H. ( 2016 ). Screening for trauma in early adolescence: Findings from a diverse school district . School Mental Health, 8 ( 1 ), 89 – 105 .
Email alerts
Citing articles via.
- About Children & Schools
- Recommend to your Library
Affiliations

- Online ISSN 1545-682X
- Print ISSN 1532-8759
- Copyright © 2024 National Association of Social Workers
- About Oxford Academic
- Publish journals with us
- University press partners
- What we publish
- New features
- Open access
- Institutional account management
- Rights and permissions
- Get help with access
- Accessibility
- Advertising
- Media enquiries
- Oxford University Press
- Oxford Languages
- University of Oxford
Oxford University Press is a department of the University of Oxford. It furthers the University's objective of excellence in research, scholarship, and education by publishing worldwide
- Copyright © 2024 Oxford University Press
- Cookie settings
- Cookie policy
- Privacy policy
- Legal notice
This Feature Is Available To Subscribers Only
Sign In or Create an Account
This PDF is available to Subscribers Only
For full access to this pdf, sign in to an existing account, or purchase an annual subscription.
Academia.edu no longer supports Internet Explorer.
To browse Academia.edu and the wider internet faster and more securely, please take a few seconds to upgrade your browser .
Enter the email address you signed up with and we'll email you a reset link.
- We're Hiring!
- Help Center

Understanding Troubled Young Adolescents Who Have Problems at School: Case Studies

Related Papers
Travis McCoy
Journal of High Institute of Public Health
Dr Safaa Rabea Osman
Background & Objective(s): Emotional and behavioral problems among adolescents represent a considerable public health problem in developing countries. These problems are considered a source of stress for adolescents as well as their families, schools and community. Emotional health and well-being of young people have implications on their self-esteem, behavior, school attendance, educational achievement, social cohesion and future health and life chances. To estimate the prevalence of emotional and behavioral problems and to determine the association between these problems and socio-demographic variables among adolescent students in Assiut district. Methods: A cross sectional study was conducted in randomly selected secondary schools (2 urban and 2 rural) in Assiut district, and 400 students were included in the study. Self-administered questionnaires were used to collect study data which included: personal data, socioeconomic status scale and self-reported version of Strengths and Difficulties Questionnaire (SDQ) (Arabic version) which included 25 items divided into 5 subscales (conduct problems, hyperactivity, emotional symptoms, peer problems and prosocial behavior) Results: About 45 % of adolescents were identified with emotional and/or behavioral problems using the SDQ. These problems included conduct, emotional, peer problems, prosocial and hyperactivity difficulties (36.0%, 42.3%, 5.0%, 28.5% and 24.8% respectively). Emotional difficulties were significantly higher (p value= 0.02) among females (40.4%), while conduct difficulties were more prevalent among males (47.5%). The majority of students with emotional/ behavioral problems (90%) reported high negative impact of such problems that was significantly associated with female sex, rural residents, students of low socioeconomic level and whose mothers were housewives. Conclusion: Screening secondary school adolescents in Assiut district revealed high prevalence of emotional and behavioral problems that was associated with perceived enormous negative impact. Further studies and intervention programs are greatly needed to address adolescent mental health needs.
Journal of Child and Family Studies
Douglas Cullinan , Edward J Sabornie
Esther Mccartney
Students with emotional/behavioral disorders have identified disruptive behaviors that negatively impact their academic performance. The US Department of Education and the American School Counselor Association have supported the use of school-wide Multitiered Systems of Support (MTSS) to reinforce pro-social behaviors for all students, but to also ensure the development of targeted and intensive interventions for students who need more support. As stakeholders, school counselors are often involved in the development and implementation of MTSS’s tiered interventions to provide support to all students, especially those with disabilities. Using consensual qualitative research study, the research team aimed to examine elementary school counselor’s perspective in developing, implementing, and assessing behavioral plans within an MTSS framework and working with students with EBD. The results, implications, and suggestions for future research will also be presented
Evidence-Based Practice in Child and Adolescent Mental Health
Jennifer Keenan
Fariha Iram
Present study was conducted to find the profiles and patterns of emotional and behavioral problems in adolescents from general population who had never been reported or diagnosed. A sample of 300 adolescents from public and private schools of Lahore, (13 to 17 years old, Mean=14.8) participated in the study. Participants completed the self-report standardized questionnaires, Youth Self-Report (YSR: Achenbach, & Rescorla, 2001) in Urdu language. The study revealed that majority of the adolescents was found to have normal behavior but a noticeable number of adolescents show emotional and behavioral problems. About 2 to 15% adolescents were found in clinical range and 3 to 10% in border line range of problems. Findings also suggest that in broadband scales externalizing problems were most prevalent in adolescents i.e. 15% and among DSM oriented problems conduct problem and anxiety problem were found most common in adolescents.
Revija za elementarno izobraževanje
Katja Vrhunc Pfeifer
Employees in education, especially in residential treatment centres, face crisis situations as a result of emotional and behavioural problems/disorders of children and adolescents. They most often face various types of violence, self-aggression, use of illicit substances and abuse. Cases of children and adolescents with mental health problems are frequent. Crisis interventions differ with the complexity of the situation, and regardless of the approach, an appropriate relationship is crucial to any solution. The purpose of this article is to present and elaborate the most common crisis situations and some successful interventions in such cases.
International Research Journal Commerce arts science
Adolescents are highly vulnerable to psychiatric disorders. This study aimed to explore the prevalence and patterns of behavioural and emotional problems in adolescents. It was also aimed to explore associations between socio environmental stressors and maladaptive outcomes. A school based cross-sectional study was conducted between January and July 2008. A stratified random sampling was done. 1150 adolescents in 12 to 18 year age group in grades 7 to 12 in 10 co-educational schools (government run and private) were the subjects of the study. Behavioural and emotional problems were assessed using Youth Self-Report (2001) questionnaire. Family stressors were assessed using a pre-tested 23 item questionnaire. Univariate and multivariate analysis were performed. Multiple logistic regression analysis was also done.
Science Park Research Organization & Counselling
The aim of this study is to find out numerous situations and counseling approaches that school counselors are likely to encounter during their training and the first five years of practice. We believe that attention to the various theoretical approaches that can be applied to resolve different cases will better prepare school counselors to deal with each dilemma using an efficient approach to school counseling. Thus it is important to know the most common cases seen and counseling approaches used in school counseling to prepare school counseling students to the profession. In order to achieve data about school counseling cases and approaches, fourteen high school counselors from public and private schools are interviewed with semi structured questionnaire prepared by researchers. School counselors are asked about the cases that they see the most, the approaches that they use with these cases, support systems that they seek for and therapy trainings that they take after their graduation from college. Study group is settled with random sampling from schools in different districts of Istanbul that have school counselor with at least one year experience. The results are analyzed with thematic analysis.
Child Development Perspectives
Armando Pina
RELATED PAPERS
عشقي سر امتيازي بثوونه
Fritz Schwarz
Trish Stoddart
Analele Universităţii "Eftimie Murgu" Reşiţa: Fascicola I, Inginerie
Marius Tufoi
Journal of Medical Microbiology
Elisabeth Nagy
eko prasetyo
Erick Okello
Wydawnictwa Artystyczne i Filmowe
Aleksander Kwiatkowski
Solid State Sciences
Boris Rakvin
Éditions Lambert Lucas
Ozouf Sénamin AMEDEGNATO
Society : Jurnal Pengabdian Masyarakat
Sri Wahyuni
Neuropsychologia
Heidi Baseler
Comm-Edu (Community Education Journal)
novi widiastuti
High Performance Computing in Science and Engineering ‘14
Scientific Reports
Santanu Bera
kjgg fdfdgg
Robert Hermann
Claudia Trepmann
Native and Immigrant Entrepreneurship
Simone Guercini
jacques CALLEBERT
Agricultura Técnica en México
Trevor Suslow
原版制作澳洲悉尼科技大学毕业证 uts学位证书学位证书扫描件
Proceedings of The Royal Society A: Mathematical, Physical and Engineering Sciences
Claude Roger
Dennis Borghardt
RELATED TOPICS
- We're Hiring!
- Help Center
- Find new research papers in:
- Health Sciences
- Earth Sciences
- Cognitive Science
- Mathematics
- Computer Science
- Academia ©2024
- International edition
- Australia edition
- Europe edition

Teenagers' struggle for mental health care: 'I needed help quite badly'
As GPs warn young people could suffer harm because of treatment delays, one 16-year-old talks about her experience
- Lack of NHS mental health services puts under-18s at risk, say GPs
I ndia knows all about the importance of getting timely help for mental health problems. “I have had issues since late primary school although I only recognised it in myself about four years ago,” said the 16-year-old from south-west London. “I had body image issues and and general anxiety about odd things like talking to strangers. I had issues of not eating and binge eating, purging, stuff like that.”
She says that when she first confided in her mother about three years ago and sought help, her mother took her straight to the GP. India was referred to NHS child and adolescent mental health services (Camhs), and she estimates that it took her a couple of weeks to be seen. She believes that if she had been forced to wait longer, it could have had dire consequences for her.
“At that stage it was very important that I was seen quickly,” she says. “I was not great and I needed help quite badly.”
The 12 sessions she had helped her but her problems did not go away and a couple of months ago India, in her own words, relapsed.
She went back to the GP and was referred to Camhs again. After an assessment, the eating disorders team decided not to take her case but the psychotherapy team said they would see her. She was told she would have to wait more than a month to be seen by the psychotherapy team, which, she says politely, “did seem like a while”.
An interim measure was put in place, although she stresses that it was not a substitute for receiving proper professional help. “The psychologist who assessed me got in touch with my school and within 12 hours they arranged counselling within the school,” she says. “It’s more just a place to talk about feelings. It’s nice to have some space to talk about it but it’s not necessarily benefiting my recovery, it’s not helping with the eating disorder stuff. It’s just a good place to let things out, it’s probably helping it to not get worse.”
Asked if she thinks it would have been difficult to cope in that month had the school counselling not been there to plug the gap, she answers straight away: “100%.”
India’s experience illustrates the importance of being seen quickly, yet she has been relatively lucky. GPs say delays can be as long as 18 months because Camhs services are overwhelmed.
While India’s wait was relatively short, that does not mean she has been immune to the fallout from the pressure put on Camhs. She believes that the 12 sessions she was entitled to when she first went to her GP two years ago were not enough for her needs.
“At the end of the counselling sessions I felt like I have just broken through the barrier, I was just getting to the breakthrough,” she says. “I wish I had got more [sessions] at that point. It may well have helped things not being as bad as they were a couple of months ago. You have to build on your relationship with your counsellor.”
But she is well aware that demand for CBT and other Camhs services means resources are limited. “At the same time, I do get that they have got a number of people who need help and I’d had my dose.”
- Young people
- Mental health
Most viewed
Advertisement
Psychosocial Development Research in Adolescence: a Scoping Review
- Original Article
- Published: 01 February 2022
- Volume 30 , pages 640–669, ( 2022 )
Cite this article

- Nuno Archer de Carvalho ORCID: orcid.org/0000-0001-6620-0804 1 , 2 &
- Feliciano Henriques Veiga ORCID: orcid.org/0000-0002-2977-6238 1 , 2
3841 Accesses
Explore all metrics
Erikson’s psychosocial development is a well-known and sound framework for adolescent development. However, despite its importance in scientific literature, the scarcity of literature reviews on Erikson’s theory on adolescence calls for an up-to-date systematization. Therefore, this study’s objectives are to understand the extent and nature of published research on Erikson’s psychosocial development in adolescence (10–19 years) in the last decade (2011–2020) and identify directions for meaningful research and intervention. A scoping review was conducted following Arksey and O’Malley’s framework, PRISMA-ScR guidelines, and a previous protocol, including a comprehensive search in eight databases. From 932 initial studies, 58 studies were selected. These studies highlighted the burgeoning research on Erikson’s approach, with a more significant representation of North American and European studies. The focus of most studies was on identity formation, presenting cross-cultural evidence of its importance in psychosocial development. Most of the studies used quantitative designs presenting a high number of different measures. Regarding topics and variables, studies emphasized the critical role of identity in adolescents’ development and well-being and the relevance of supporting settings in psychosocial development. However, shortcomings were found regarding the study of online and school as privileged developmental settings for adolescents. Suggestions included the need to consider the process of identity formation in the context of lifespan development and invest in supporting adolescents’ identity formation. Overall, conclusions point out Erikson’s relevance in understanding adolescents’ current challenges while offering valuable research and intervention directions to enhance adolescent growth potential.
This is a preview of subscription content, log in via an institution to check access.
Access this article
Price includes VAT (Russian Federation)
Instant access to the full article PDF.
Rent this article via DeepDyve
Institutional subscriptions
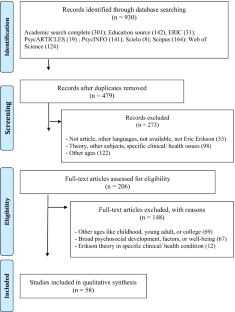
Similar content being viewed by others

Teenagers, screens and social media: a narrative review of reviews and key studies

Carl Rogers: A Person-Centered Approach
Social media and depressive symptoms in childhood and adolescence: a systematic review, materials availability.
All relevant data are included in this article or in its Supplementary Information.
Alberts, C., & Bennett, M. J. (2017). Identity formation among isiXhosa-speaking adolescents in a rural Eastern Cape community in South Africa: A brief report. Journal of Psychology in Africa, 27 (2), 198–202. https://doi.org/10.1080/14330237.2017.1303128
Article Google Scholar
Alfvén, T., Dahlstrand, J., Humphreys, D., Helldén, D., Hammarstrand, S., Hollander, A.-C., Målqvist, M., Nejat, S., Jørgensen, P. S., Friberg, P., & Tomson, G. (2019). Placing children and adolescents at the centre of the Sustainable Development Goals will deliver for current and future generations. Global Health Action, 12 (1), 1670015. https://doi.org/10.1080/16549716.2019.1670015
Article PubMed PubMed Central Google Scholar
APA. (2021). Thesaurus of psychological index terms—APA Publishing . Retrieved April 1, 2021, from https://www.apa.org/pubs/databases/training/thesaurus
APA. (2020). APA dictionary of psychology . Retrieved April 1, 2021, from https://dictionary.apa.org/
Arksey, H., & O’Malley, L. (2005). Scoping studies: Towards a methodological framework. International Journal of Social Research Methodology, 8 (1), 19–32. https://doi.org/10.1080/1364557032000119616
Arnett, J. J. (2008). The neglected 95%: Why American psychology needs to become less American. American Psychologist, 63 (7), 602–614. https://doi.org/10.1037/0003-066X.63.7.602
Article PubMed Google Scholar
Bazuin-Yoder, A. (2011). Positive and negative childhood and adolescent identity memories stemming from one’s country and culture-of-origin: A comparative narrative analysis. Child & Youth Care Forum, 40 (1), 77–92. https://doi.org/10.1007/s10566-010-9122-6
Becht, A. I., Nelemans, S. A., Branje, S. J. T., Vollebergh, W. A. M., Koot, H. M., Denissen, J. J. A., & Meeus, W. H. J. (2016). The quest for identity in adolescence: Heterogeneity in daily identity formation and psychosocial adjustment across five years. Developmental Psychology, 52 (12), 2010–2021. https://doi.org/10.1037/dev0000245
Becht, A. I., Nelemans, S. A., Branje, S. J. T., Vollebergh, W. A. M., Koot, H. M., & Meeus, W. H. J. (2017). Identity uncertainty and commitment making across adolescence: Five-year within-person associations using daily identity reports. Developmental Psychology, 53 (11), 2103–2112. https://doi.org/10.1037/dev0000374
Bogaerts, A., Claes, L., Schwartz, S. J., Becht, A. I., Verschueren, M., Gandhi, A., & Luyckx, K. (2019). Identity structure and processes in adolescence: Examining the directionality of between- and within-person associations. Journal of Youth and Adolescence, 48 (5), 891–907. https://doi.org/10.1007/s10964-018-0931-5
Brito, E. S., Schoen, T. H., Marteleto, M. R. F., & de Oliveira-Monteiro, N. R. (2017). Identity status of adolescents living in institutional shelters. Journal of Human Growth and Development, 27 (3), 315. https://doi.org/10.7322/jhgd.141279
Brittian, A. S., & Lerner, R. M. (2013). Early influences and later outcomes associated with developmental trajectories of Eriksonian fidelity. Developmental Psychology, 49 (4), 722–735. https://doi.org/10.1037/a0028323
Brown, G. H., Brunelle, L. M., & Malhotra, V. (2017). Tagging: Deviant behavior or adolescent rites of passage? Culture & Psychology, 23 (4), 487–501. https://doi.org/10.1177/1354067X16660852
Burkhard, B. M., Robinson, K. M., Murray, E. D., & Lerner, R. M. (2020). Positive youth development: Theory and perspective. Em S. Hupp & J. Jewell (Eds.), The Encyclopedia of Child and Adolescent Development (1st ed.). Wiley. https://doi.org/10.1002/9781119171492
Busey, C. L., & Russell, W. B., III. (2016). “We want to learn”: Middle school Latino/a students discuss social studies curriculum and pedagogy. RMLE Online, 39 (4), 1–20. https://doi.org/10.1080/19404476.2016.1155921
Caldeira, S. N., & Veiga, F. H. (2013). Desenvolvimento pessoal, psicossocial e moral [Personal, psychosocial, and moral development]. Em F. H. Veiga (Ed.), Psicologia da educação—Teoria, investigação e aplicação: Envolvimento dos alunos na escola (pp. 121–176). Climepsi.
Carvalho, N. A., & Veiga, F. H. (2020). Desenvolvimento psicossocial e envolvimento dos alunos na escola: Revisão teórica e empírica para estudo com alunos no 2o e 3o ciclo [Psychosocial development and student engagement in school: Theoretical and empirical revision for a study with adolescents]. Em F. H. Veiga (Ed.), Atas do III Congresso Internacional Envolvimento dos Alunos na Escola: Perspetivas da Psicologia e Educação—Inclusão e Diversidade. (pp. 799–815). Instituto de Educação da Universidade de Lisboa.
Carvalho, N. A. de. (2019). Formação Humana no Currículo: Um programa para fazer à medida [Human Development in the Curriculum: A Program to Customize]. Sisyphus — Journal of Education, 7 (2), 65–91. https://doi.org/10.25749/sis.17260
Chávez, R. (2016). Psychosocial development factors associated with occupational and vocational identity between infancy and adolescence. Adolescent Research Review, 1 (4), 307–327. https://doi.org/10.1007/s40894-016-0027-y
Claes, L., Luyckx, K., & Bijttebier, P. (2014). Nonsuicidal self-injury in adolescents: Prevalence and associations with identity formation above and beyond depression. Personality and Individual Differences, 61–62 , 101–104. https://doi.org/10.1016/j.paid.2013.12.019
Colquhoun, H. L., Levac, D., O’Brien, K. K., Straus, S., Tricco, A. C., Perrier, L., Kastner, M., & Moher, D. (2014). Scoping reviews: Time for clarity in definition, methods, and reporting. Journal of Clinical Epidemiology, 67 (12), 1291–1294. https://doi.org/10.1016/j.jclinepi.2014.03.013
Crocetti, E. (2017). Identity formation in adolescence: The dynamic of forming and consolidating identity commitments. Child Development Perspectives, 11 (2), 145–150. https://doi.org/10.1111/cdep.12226
Crocetti, E., Erentaitė, R., & Žukauskienė, R. (2014). Identity styles, positive youth development, and civic engagement in adolescence. Journal of Youth and Adolescence, 43 (11), 1818–1828. https://doi.org/10.1007/s10964-014-0100-4
Crocetti, E., Fermani, A., Pojaghi, B., & Meeus, W. (2011). Identity formation in adolescents from Italian, mixed, and migrant families. Child & Youth Care Forum, 40 (1), 7–23. https://doi.org/10.1007/s10566-010-9112-8
Cross, T. L. (2001). Social/emotional needs: Gifted children and Erikson’s theory of psychosocial. Gifted Child Today, 24 (1), 54–55. https://doi.org/10.4219/gct-2000-522
Cross, T. L., & Cross, J. R. (2017). Maximizing potential: A school-based conception of psychosocial development. High Ability Studies, 28 (1), 43–58. https://doi.org/10.1080/13598139.2017.1292896
Cuzzocrea, V. (2019). Moratorium or waithood? Forms of time-taking and the changing shape of youth. Time & Society, 28 (2), 567–586. https://doi.org/10.1177/0961463X18763680
Czyzowska, D., & Mikołajewska, K. (2014). Religiosity and young people’s construction of personal identity. Roczniki Psychologiczne/Annals of Psychology, 7 (1), 131–154.
Google Scholar
Dahl, R. E., Allen, N. B., Wilbrecht, L., & Suleiman, A. B. (2018). Importance of investing in adolescence from a developmental science perspective. Nature, 554 (7693), 441–450. https://doi.org/10.1038/nature25770
Dimitrova, R., Hatano, K., Sugimura, K., & Ferrer-Wreder, L. (2019). The Erikson psychosocial stage inventory in adolescent samples: Factorial validity and equivalence of identity as measured from the United States and Japan. European Journal of Psychological Assessment, 35 (5), 680–684. https://doi.org/10.1027/1015-5759/a000456
Driessens, C. M. E. F. (2015). Extracurricular activity participation moderates impact of family and school factors on adolescents’ disruptive behavioural problems. BMC Public Health, 15 (1), 1110. https://doi.org/10.1186/s12889-015-2464-0
Dunkel, C. S., & Harbke, C. (2017). A review of measures of Erikson’s stages of psychosocial development: Evidence for a general factor. Journal of Adult Development, 24 (1), 58–76. https://doi.org/10.1007/s10804-016-9247-4
Eichas, K., Kurtines, W. M., Rinaldi, R. L., & Farr, A. C. (2018). Promoting positive youth development: A psychosocial intervention evaluation. Psychosocial Intervention, 27 (1), 22–34. https://doi.org/10.5093/pi2018a5
Eichas, K., Montgomery, M. J., Meca, A., & Kurtines, W. M. (2017). Empowering marginalized youth: A self-transformative intervention for promoting positive youth development. Child Development, 88 (4), 1115–1124. https://doi.org/10.1111/cdev.12866
Erikson, E. H. (1993). Childhood and society . Norton. (Original work published 1950)
Erikson, E. H. (1994). Identity and the life cycle . Norton. (Original work published 1959)
Erikson, E. H. (1994). Identity, youth and crisis . Norton. (Original work published 1968)
Erikson, E. H., & Erikson, J. M. (1998). The life cycle completed (Extended version). Norton.
Furman, W., & Collibee, C. (2014). A matter of timing: Developmental theories of romantic involvement and psychosocial adjustment. Development and Psychopathology , 26 (4pt1), 1149–1160. https://doi.org/10.1017/S0954579414000182
Gandhi, A., Claes, L., Bosmans, G., Baetens, I., Wilderjans, T. F., Maitra, S., Kiekens, G., & Luyckx, K. (2016a). Nonsuicidal self-injury and adolescents attachment with peers and mother: The mediating role of identity synthesis and confusion. Journal of Child and Family Studies, 25 (6), 1735–1745. https://doi.org/10.1007/s10826-015-0350-0
Gandhi, A., Luyckx, K., Goossens, L., Maitra, S., & Claes, L. (2016b). Sociotropy, autonomy, and nonsuicidal self-injury: The mediating role of identity confusion. Personality and Individual Differences, 99 , 272–277. https://doi.org/10.1016/j.paid.2016.05.040
Gandhi, A., Luyckx, K., Maitra, S., Kiekens, G., & Claes, L. (2016c). Reactive and regulative temperament and nonsuicidal self-injury in Flemish adolescents: The intervening role of identity formation. Personality and Individual Differences, 99 , 254–259. https://doi.org/10.1016/j.paid.2016.05.007
Gandhi, A., Luyckx, K., Maitra, S., Kiekens, G., Verschueren, M., & Claes, L. (2017). Directionality of effects between nonsuicidal self-injury and identity formation: A prospective study in adolescents. Personality and Individual Differences, 109 , 124–129. https://doi.org/10.1016/j.paid.2017.01.003
Gandhi, A., Luyckx, K., Molenberghs, G., Baetens, I., Goossens, L., Maitra, S., & Claes, L. (2019). Maternal and peer attachment, identity formation, and nonsuicidal self-injury: A longitudinal mediation study. Child and Adolescent Psychiatry and Mental Health, 13 (1), 7. https://doi.org/10.1186/s13034-019-0267-2
García-Martínez, A. T., Guerrero-Bote, V., & Moya-Anegón, F. (2012). World scientific production in psychology. Universitas Psychologica, 11 (3), 699–717.
Gfellner, B. M., & Armstrong, H. D. (2012). Ego development, ego strengths, and ethnic identity among first nation adolescents. Journal of Research on Adolescence, 22 (2), 225–234. https://doi.org/10.1111/j.1532-7795.2011.00769.x
Ghavami, N., Fingerhut, A., Peplau, L. A., Grant, S. K., & Wittig, M. A. (2011). Testing a model of minority identity achievement, identity affirmation, and psychological well-being among ethnic minority and sexual minority individuals. Cultural Diversity and Ethnic Minority Psychology, 17 (1), 79–88. https://doi.org/10.1037/a0022532
Grigsby, T. J., Forster, M., Meca, A., Zamboanga, B. L., Schwartz, S. J., & Unger, J. B. (2018). Cultural stressors, identity development, and substance use attitudes among Hispanic immigrant adolescents. Journal of Community Psychology, 46 (1), 117–132. https://doi.org/10.1002/jcop.21920
Gu, H., Ma, P., & Xia, T. (2020). Childhood emotional abuse and adolescent nonsuicidal self-injury: The mediating role of identity confusion and moderating role of rumination. Child Abuse & Neglect, 106 , 104474. https://doi.org/10.1016/j.chiabu.2020.104474
Hatano, K., Sugimura, K., & Schwartz, S. J. (2018). Longitudinal links between identity consolidation and psychosocial problems in adolescence: Using bi-factor latent change and cross-lagged effect models. Journal of Youth and Adolescence, 47 (4), 717–730. https://doi.org/10.1007/s10964-017-0785-2
Hatano, K., Sugimura, K., Crocetti, E., & Meeus, W. H. J. (2020). Diverse-and-dynamic pathways in educational and interpersonal identity formation during adolescence: Longitudinal links with psychosocial functioning. Child Development, 91 (4), 1203–1218. https://doi.org/10.1111/cdev.13301
Hatton, C. (2012). Performing ‘girl’ in the Facebook era: Drama as a safe space for negotiating adolescent identities and agency. NJ , 36 (1), 36–49. https://doi.org/10.1080/14452294.2012.11649553
Hill, P. L., & Burrow, A. L. (2012). Viewing purpose through an Eriksonian lens. Identity, 12 (1), 74–91. https://doi.org/10.1080/15283488.2012.632394
Ja, N. M., & Jose, P. E. (2017). “I can’t take hold of some kind of a life”: The role of social connectedness and confidence in engaging “lost” adolescents with their lives. Journal of Youth and Adolescence, 46 (9), 2028–2046. https://doi.org/10.1007/s10964-017-0656-x
Jones, R. M., Dick, A. J., Coyl-Shepherd, D. D., & Ogletree, M. (2014). Antecedents of the male adolescent identity crisis: Age, grade, and physical development. Youth & Society, 46 (4), 443–459. https://doi.org/10.1177/0044118X12438904
Kay, A. (2018). Erikson online: Identity and pseudospeciation in the internet age. Identity, 18 (4), 264–273. https://doi.org/10.1080/15283488.2018.1523732
Keles, B., McCrae, N., & Grealish, A. (2020). A systematic review: The influence of social media on depression, anxiety and psychological distress in adolescents. International Journal of Adolescence and Youth, 25 (1), 79–93. https://doi.org/10.1080/02673843.2019.1590851
Knight, T., Skouteris, H., Townsend, M., & Hooley, M. (2014). The act of giving: A systematic review of nonfamilial intergenerational interaction. Journal of Intergenerational Relationships, 12 (3), 257–278. https://doi.org/10.1080/15350770.2014.929913
Koepke, S., & Denissen, J. J. A. (2012). Dynamics of identity development and separation–individuation in parent–child relationships during adolescence and emerging adulthood: A conceptual integration. Developmental Review, 32 (1), 67–88. https://doi.org/10.1016/j.dr.2012.01.001
Kroger, J. (2018). The epigenesis of identity - What does it mean? Identity, 18 (4), 334–342. https://doi.org/10.1080/15283488.2018.1523730
Lawford, H. L., Astrologo, L., Ramey, H. L., & Linden-Andersen, S. (2020). Identity, intimacy, and generativity in adolescence and young adulthood: A test of the psychosocial model. Identity, 20 (1), 9–21. https://doi.org/10.1080/15283488.2019.1697271
Lawford, H. L., Doyle, A.-B., & Markiewicz, D. (2018). Associations of attachment orientation with early generative concern across adolescence. Journal of Personality, 86 (4), 726–737. https://doi.org/10.1111/jopy.12353
Lee, C.-T., & Beckert, T. E. (2012). Taiwanese adolescent cognitive autonomy and identity development: The relationship of situational and agential factors. International Journal of Psychology, 47 (1), 39–50. https://doi.org/10.1080/00207594.2011.572972
Lerner, R. M. (2002). Concepts and theories of human development (3rd ed). L. Erlbaum Associates.
Lerner, R. M., Almerigi, J. B., Theokas, C., & Lerner, J. V. (2005). Positive youth development: A view of the issues. The Journal of Early Adolescence, 25 (1), 10–16. https://doi.org/10.1177/0272431604273211
Levac, D., Colquhoun, H., & O’Brien, K. K. (2010). Scoping studies: Advancing the methodology. Implementation Science, 5 (1), 69. https://doi.org/10.1186/1748-5908-5-69
Lisha, N. E., Grana, R., Sun, P., Rohrbach, L., Spruijt-Metz, D., Reifman, A., & Sussman, S. (2014). Evaluation of the psychometric properties of the revised inventory of the dimensions of emerging adulthood (IDEA-R) in a sample of continuation high school students. Evaluation & the Health Professions, 37 (2), 156–177. https://doi.org/10.1177/0163278712452664
Luyckx, K., Gandhi, A., Bijttebier, P., & Claes, L. (2015). Nonsuicidal self-injury in female adolescents and psychiatric patients: A replication and extension of the role of identity formation. Personality and Individual Differences, 77 , 91–96. https://doi.org/10.1016/j.paid.2014.12.057
MacPherson, E., Kerr, G., & Stirling, A. (2016). The influence of peer groups in organized sport on female adolescents’ identity development. Psychology of Sport and Exercise, 23 , 73–81. https://doi.org/10.1016/j.psychsport.2015.10.002
Makhubela, M. S. (2012). Exposure to domestic violence and identity development among adolescent university students in South Africa. Psychological Reports, 110 (3), 791–800. https://doi.org/10.2466/16.13.17.PR0.110.3.791-800
Marcia, J. E. (2015). Erikson, Erik Homburger (1902–94). In J. D. Wright (Ed.), International Encyclopedia of the Social & Behavioral Sciences (pp. 934–937). Elsevier. https://doi.org/10.1016/B978-0-08-097086-8.61031-0
Markstrom, C. A., Sabino, V. M., Turner, B. J., & Berman, R. C. (1997). The psychosocial inventory of ego strengths: Development and validation of a new Eriksonian measure. Journal of Youth and Adolescence, 26 (6), 705–732.
Matusov, E., & Smith, M. P. (2012). The middle-class nature of identity and its implications for education: A genealogical analysis and reevaluation of a culturally and historically bounded concept. Integrative Psychological and Behavioral Science, 46 (3), 274–295. https://doi.org/10.1007/s12124-012-9192-0
McLaughlin, C., & Clarke, B. (2010). Relational matters: A review of the impact of school experience on mental health in early adolescence. Educational and Child Psychology, 27 (1), 91–103.
McLean, K. C., & Pasupathi, M. (2012). Processes of identity development: Where I am and how I got there. Identity, 12 (1), 8–28. https://doi.org/10.1080/15283488.2011.632363
Meca, A., Rodil, J. C., Paulson, J. F., Kelley, M., Schwartz, S. J., Unger, J. B., Lorenzo-Blanco, E. I., Des Rosiers, S. E., Gonzales-Backen, M., Baezconde-Garbanati, L., & Zamboanga, B. L. (2019). Examining the directionality between identity development and depressive symptoms among recently immigrated Hispanic adolescents. Journal of Youth and Adolescence, 48 (11), 2114–2124. https://doi.org/10.1007/s10964-019-01086-z
Meca, A., Sabet, R. F., Farrelly, C. M., Benitez, C. G., Schwartz, S. J., Gonzales-Backen, M., Lorenzo-Blanco, E. I., Unger, J. B., Zamboanga, B. L., Baezconde-Garbanati, L., Picariello, S., Des Rosiers, S. E., Soto, D. W., Pattarroyo, M., Villamar, J. A., & Lizzi, K. M. (2017). Personal and cultural identity development in recently immigrated Hispanic adolescents: Links with psychosocial functioning. Cultural Diversity and Ethnic Minority Psychology, 23 (3), 348–361. https://doi.org/10.1037/cdp0000129
Meeus, W. (2011). The study of adolescent identity formation 2000–2010: A review of longitudinal research. Journal of Research on Adolescence, 21 (1), 75–94. https://doi.org/10.1111/j.1532-7795.2010.00716.x
Meeus, W. (2016). Adolescent psychosocial development: A review of longitudinal models and research. Developmental Psychology, 52 (12), 1969–1993. https://doi.org/10.1037/dev0000243
Mercer, N., Crocetti, E., Branje, S., van Lier, P., & Meeus, W. (2017). Linking delinquency and personal identity formation across adolescence: Examining between- and within-person associations. Developmental Psychology, 53 (11), 2182–2194. https://doi.org/10.1037/dev0000351
Nelson, S. C., Kling, J., Wängqvist, M., Frisén, A., & Syed, M. (2018). Identity and the body: Trajectories of body esteem from adolescence to emerging adulthood. Developmental Psychology, 54 (6), 1159–1171. https://doi.org/10.1037/dev0000435
Newman, B. M., & Newman, P. R. (2015). Development through life: A psychosocial approach (12th ed.). Cengage Learning.
O’Flaherty, J., & Phillips, C. (2015). The use of flipped classrooms in higher education: A scoping review. The Internet and Higher Education, 25 , 85–95. https://doi.org/10.1016/j.iheduc.2015.02.002
O’Gorman, J., Shum, D. H. K., Halford, W. K., & Ogilvie, J. (2012). World trends in psychological research output and impact. International Perspectives in Psychology, 1 (4), 268–283. https://doi.org/10.1037/a0030520
Okonkwo, E. (2013). Dual income family, gender and adolescents’ self-esteem. IFE PsychologIA, 21 (1), 127–138. https://doi.org/10.4314/ifep.v21i1
Oshri, A., Schwartz, S. J., Unger, J. B., Kwon, J. A., Des Rosiers, S. E., Baezconde-Garbanati, L., Lorenzo-Blanco, E. I., Córdova, D., Soto, D. W., Lizzi, K. M., Villamar, J. A., & Szapocznik, J. (2014). Bicultural stress, identity formation, and alcohol expectancies and misuse in Hispanic adolescents: A developmental approach. Journal of Youth and Adolescence, 43 (12), 2054–2068. https://doi.org/10.1007/s10964-014-0171-2
Patton, G. C., Sawyer, S. M., Santelli, J. S., Ross, D. A., Afifi, R., Allen, N. B., Arora, M., Azzopardi, P., Baldwin, W., Bonell, C., Kakuma, R., Kennedy, E., Mahon, J., McGovern, T., Mokdad, A. H., Patel, V., Petroni, S., Reavley, N., Taiwo, K., … Viner, R. M. (2016). Our future: A Lancet commission on adolescent health and well-being. The Lancet, 387 (10036), 2423–2478. https://doi.org/10.1016/S0140-6736(16)00579-1
Pham, M. T., Rajić, A., Greig, J. D., Sargeant, J. M., Papadopoulos, A., & McEwen, S. A. (2014). A scoping review of scoping reviews: Advancing the approach and enhancing the consistency. Research Synthesis Methods, 5 (4), 371–385. https://doi.org/10.1002/jrsm.1123
Pratt, M. W., Norris, J. E., Alisat, S., & Bisson, E. (2013). Earth mothers (and fathers): Examining generativity and environmental concerns in adolescents and their parents. Journal of Moral Education, 42 (1), 12–27. https://doi.org/10.1080/03057240.2012.714751
Ragelienė, T. (2016). Links of adolescents identity development and relationship with peers: A systematic literature review. Journal of the Canadian Academy of Child and Adolescent Psychiatry = Journal De l’Academie Canadienne De Psychiatrie De L’enfant Et De L’adolescent , 25 (2), 97–105.
Rivas-Drake, D., Markstrom, C., Syed, M., Lee, R. M., Umaña-Taylor, A. J., Yip, T., Seaton, E. K., Quintana, S., Schwartz, S. J., & French, S. (2014). Ethnic and racial identity in adolescence: Implications for psychosocial, academic, and health outcomes. Child Development, 85 (1), 40–57. https://doi.org/10.1111/cdev.12200
Rosenthal, D. A., Gurney, R. M., & Moore, S. M. (1981). From trust on intimacy: A new inventory for examining Erikson’s stages of psychosocial development. Journal of Youth and Adolescence, 10 (6), 525–537. https://doi.org/10.1007/BF02087944
Santrock, J. W. (2011). Educational psychology (5th ed). McGraw-Hill.
Sawyer, S. M., Azzopardi, P. S., Wickremarathne, D., & Patton, G. C. (2018). The age of adolescence. The Lancet Child & Adolescent Health, 2 (3), 223–228. https://doi.org/10.1016/S2352-4642(18)30022-1
Schwartz, S. J., Zamboanga, B. L., Meca, A., & Ritchie, R. A. (2012). Identity around the world: An overview. New Directions for Child and Adolescent Development, 138 , 1–18. https://doi.org/10.1002/cad.20019
Seligman, M. E. P., & Csikszentmihalyi, M. (2000). Positive psychology: An introduction. American Psychologist, 55 (1), 5–14. https://doi.org/10.1037/0003-066X.55.1.5 .
Shankleman, M., Hammond, L., & Jones, F. W. (2021). Adolescent social media use and well-being: A systematic review and thematic meta-synthesis. Adolescent Research Review, 6 , 471–492. https://doi.org/10.1007/s40894-021-00154-5
Shapiro, L. A. S., & Margolin, G. (2014). Growing up wired: Social networking sites and adolescent psychosocial development. Clinical Child and Family Psychology Review, 17 (1), 1–18. https://doi.org/10.1007/s10567-013-0135-1
Article PubMed Central Google Scholar
Silbereisen, R. K., & Lerner, R. M. (Eds.) (2007). Approaches to positive youth development . Sage Publications.
Solobutina, M. (2020). Ego identity of intellectually gifted and sport talented individuals in puberty and adolescence. Education & Self Development, 15 (1), 12–20. https://doi.org/10.26907/esd15.1.02
Sprinthall, N. A., & Collins, W. A. (2011). Psicologia do adolescente: Uma abordagem desenvolvimentista [Adolescent psychology: A developmental view] (5th ed.). Fundação Calouste Gulbenkian.
Steensma, T. D., Kreukels, B. P. C., de Vries, A. L. C., & Cohen-Kettenis, P. T. (2013). Gender identity development in adolescence. Hormones and Behavior, 64 (2), 288–297. https://doi.org/10.1016/j.yhbeh.2013.02.020
Symonds, J. E., & Galton, M. (2014). Moving to the next school at age 10–14 years: An international review of psychological development at school transition. Review of Education, 2 (1), 1–27. https://doi.org/10.1002/rev3.3021
Timler, A., McIntyre, F., Bulsara, C., Rose, E., & Hands, B. (2020). The influence of motor competence on adolescent identity health: A mixed method study. Research Quarterly for Exercise and Sport, 91 (1), 1–14. https://doi.org/10.1080/02701367.2019.1643821
Tricco, A. C., Lillie, E., Zarin, W., O’Brien, K. K., Colquhoun, H., Levac, D., Moher, D., Peters, M. D. J., Horsley, T., Weeks, L., Hempel, S., Akl, E. A., Chang, C., McGowan, J., Stewart, L., Hartling, L., Aldcroft, A., Wilson, M. G., Garritty, C., … Straus, S. E. (2018). PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Annals of Internal Medicine, 169 (7), 467. https://doi.org/10.7326/M18-0850
Tsang, S. K. M., Hui, E. K. P., & Law, B. C. M. (2012). Positive identity as a Positive youth development construct: A conceptual review. The Scientific World Journal, 2012 , 1–8. https://doi.org/10.1100/2012/529691
Twum-Antwi, A., Jefferies, P., & Ungar, M. (2020). Promoting child and youth resilience by strengthening home and school environments: A literature review. International Journal of School & Educational Psychology, 8 (2), 78–89. https://doi.org/10.1080/21683603.2019.1660284
Umaña-Taylor, A. J., Kornienko, O., Douglass Bayless, S., & Updegraff, K. A. (2018). A universal intervention program increases ethnic-racial identity exploration and resolution to predict adolescent psychosocial functioning one year later. Journal of Youth and Adolescence, 47 (1), 1–15. https://doi.org/10.1007/s10964-017-0766-5
UNESCO. (2019). Right to education handbook . Unesco Education Sector.
UNICEF. (2018). UNICEF programme guidance for the second decade: Programming with and for adolescents . UNICEF.
United Nations. (1989). Convention on the rights of the child (Adopted and opened for signature, ratification and accession by General Assembly resolution 44/25). General Assembly of the United Nations.
United Nations. (2001). General comment No. 1: The aims of education (article 29) . Committee on the Rights of the Child. https://www.ohchr.org/EN/Issues/Education/Training/Compilation/Pages/a)GeneralCommentNo1TheAimsofEducation(article29)(2001).aspx
Valkenburg, P. M., & Peter, J. (2011). Online communication among adolescents: An integrated model of its attraction, opportunities, and risks. Journal of Adolescent Health, 48 (2), 121–127. https://doi.org/10.1016/j.jadohealth.2010.08.020
van Halen, C., Bosma, H. A., & van der Meulen, M. (2020). Experiencing self-definition problems over the life span. Identity, 20 (3), 170–187. https://doi.org/10.1080/15283488.2020.1782913
Verschueren, M., Claes, L., Bogaerts, A., Palmeroni, N., Gandhi, A., Moons, P., & Luyckx, K. (2018). Eating disorder symptomatology and identity formation in adolescence: A cross-lagged longitudinal approach. Frontiers in Psychology, 9 , 816. https://doi.org/10.3389/fpsyg.2018.00816
Wang, M.-T., Degol, L., & J., Amemiya, J., Parr, A., & Guo, J. (2020). Classroom climate and children’s academic and psychological well-being: A systematic review and meta-analysis. Developmental Review, 57 , 100912. https://doi.org/10.1016/j.dr.2020.100912
Wängqvist, M., & Frisén, A. (2016). Who am I online? Understanding the meaning of online contexts for identity development. Adolescent Research Review, 1 (2), 139–151. https://doi.org/10.1007/s40894-016-0025-0
Waterman, A. S. (2015). What does it mean to engage in identity exploration and to hold identity commitments? A methodological critique of multidimensional measures for the study of identity processes. Identity, 15 (4), 309–349. https://doi.org/10.1080/15283488.2015.1089403
WHO. (1948). Constitution of the world health organization (General Assembly resolution 217 A). World Health Organization. https://www.un.org/en/universal-declaration-human-rights/index.html
WHO. (2019). Accelerated action for the health of adolescents (AA-HA!) . World Health Organization. https://apps.who.int/iris/bitstream/handle/10665/330483/9789241517058-eng.pdf?ua=1
Zacarés, J. J., & Iborra, A. (2015). Self and identity development during adolescence across cultures. In J. D. Wright (Ed.), International Encyclopedia of the Social & Behavioral Sciences (pp. 432–438). Elsevier. https://doi.org/10.1016/B978-0-08-097086-8.23028-6
Zhang, L. (2015). Erikson’s theory of psychosocial development. In J. D. Wright (Ed.), International Encyclopedia of the Social & Behavioral Sciences (pp. 938–946). Elsevier. https://doi.org/10.1016/B978-0-08-097086-8.23200-5
Zimmer-Gembeck, M. J., Hughes, N., Kelly, M., & Connolly, J. (2012). Intimacy, identity and status: Measuring dating goals in late adolescence and emerging adulthood. Motivation and Emotion, 36 (3), 311–322. https://doi.org/10.1007/s11031-011-9253-6
Download references
Acknowledgements
The authors thank Conceição Martins and Filomena Covas for their help in assessing methodological options and text revision and Rita Fonseca and Sandra Torres for their advice regarding English accuracy.
This work was supported by the FCT — Fundação para a Ciência e a Tecnologia, IP, within the scope of the UIDEF — Unidade de Investigação e Desenvolvimento em Educação e Formação, under the reference UID/CED/04107/2020.
Author information
Authors and affiliations.
Instituto de Educação da Universidade de Lisboa, Lisboa, Portugal
Nuno Archer de Carvalho & Feliciano Henriques Veiga
Alameda da Universidade, 1649-013, Lisboa, Portugal
You can also search for this author in PubMed Google Scholar
Contributions
NC and FV worked on the protocol and methodological design of the review. NC carried out the research, analyzed the studies, and presented the initial text for the results and their discussion. FV oversaw the conceptualization, research, and analysis of the studies. Both authors read and approved the final manuscript.
Corresponding author
Correspondence to Nuno Archer de Carvalho .
Ethics declarations
Conflict of interest.
The authors declare no competing interests.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary file1 (DOCX 107 kb)
Supplementary file2 (docx 94 kb), supplementary file3 (docx 109 kb), rights and permissions.
Reprints and permissions
About this article
de Carvalho, N.A., Veiga, F.H. Psychosocial Development Research in Adolescence: a Scoping Review. Trends in Psychol. 30 , 640–669 (2022). https://doi.org/10.1007/s43076-022-00143-0
Download citation
Accepted : 07 January 2022
Published : 01 February 2022
Issue Date : December 2022
DOI : https://doi.org/10.1007/s43076-022-00143-0
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Adolescent development
- Systematic literature review
- Identity formation
- Erik Erikson
- Find a journal
- Publish with us
- Track your research

Children and Families Policy Research Unit
NIHR Children and Families Policy Research Unit

Case Study: Adolescence
Helping young people say 'no': the prevalence of risk-taking behaviour and what works to reduce it.

How many adolescents smoke, drink and take drugs and what kind of interventions work best to stop them?
Adolescent years are a notoriously challenging time, as children go through the biggest changes since their first year of life. It's this life stage that presents the greatest risk to future health, with damaging habits most often picked up between the ages of 11 and 19.
Research under the adolescent theme has examined the trends in health risk behaviours and reviewed interventions designed to prevent them, in order to inform UK health policy for this susceptible group.
Key Points:
- Two studies looked at trends in risky behaviours in adolescents and interventions designed to prevent them
- Smoking, drinking and drug use have individually declined, but a core of young people remain who engage in all three
- School-based interventions designed to empower young people to say 'no' have proved most effective at reducing multiple harmful behaviours
This case study is for the Adolescence theme.
- Download pdf
- Download plain text version pdf
- Helping young people say no
- Cutting the risk
- Mental health in children
- Type 2 diabetes in children
- Family finances and disability
- Stories from data and young people
- Growing up happy in England
Our Case Studies
We have complied a series of publications and case studies to illustrate the type of projects we work on and how we support child health policy-making in England
- The Healthy Child
- Healthcare provision
- Mental health
- Adolescence
- Long-term conditions
- Sociology of health and illness:
- Health economics
- Social care
- Participation of children and families
- Children's mental health case studies
- Food, health and nutrition
- Mental wellbeing
- Mental health
Explore the experiences of children and families with these interdisciplinary case studies. Designed to help professionals and students explore the strengths and needs of children and their families, each case presents a detailed situation, related research, problem-solving questions and feedback for the user. Use these cases on your own or in classes and training events
Each case study:
- Explores the experiences of a child and family over time.
- Introduces theories, research and practice ideas about children's mental health.
- Shows the needs of a child at specific stages of development.
- Invites users to “try on the hat” of different specific professionals.
By completing a case study participants will:
- Examine the needs of children from an interdisciplinary perspective.
- Recognize the importance of prevention/early intervention in children’s mental health.
- Apply ecological and developmental perspectives to children’s mental health.
- Predict probable outcomes for children based on services they receive.
Case studies prompt users to practice making decisions that are:
- Research-based.
- Practice-based.
- Best to meet a child and family's needs in that moment.
Children’s mental health service delivery systems often face significant challenges.
- Services can be disconnected and hard to access.
- Stigma can prevent people from seeking help.
- Parents, teachers and other direct providers can become overwhelmed with piecing together a system of care that meets the needs of an individual child.
- Professionals can be unaware of the theories and perspectives under which others serving the same family work
- Professionals may face challenges doing interdisciplinary work.
- Limited funding promotes competition between organizations trying to serve families.
These case studies help explore life-like mental health situations and decision-making. Case studies introduce characters with history, relationships and real-life problems. They offer users the opportunity to:
- Examine all these details, as well as pertinent research.
- Make informed decisions about intervention based on the available information.
The case study also allows users to see how preventive decisions can change outcomes later on. At every step, the case content and learning format encourages users to review the research to inform their decisions.
Each case study emphasizes the need to consider a growing child within ecological, developmental, and interdisciplinary frameworks.
- Ecological approaches consider all the levels of influence on a child.
- Developmental approaches recognize that children are constantly growing and developing. They may learn some things before other things.
- Interdisciplinary perspectives recognize that the needs of children will not be met within the perspectives and theories of a single discipline.
There are currently two different case students available. Each case study reflects a set of themes that the child and family experience.
The About Steven case study addresses:
- Adolescent depression.
- School mental health.
- Rural mental health services.
- Social/emotional development.
The Brianna and Tanya case study reflects themes of:
- Infant and early childhood mental health.
- Educational disparities.
- Trauma and toxic stress.
- Financial insecurity.
- Intergenerational issues.
The case studies are designed with many audiences in mind:
Practitioners from a variety of fields. This includes social work, education, nursing, public health, mental health, and others.
Professionals in training, including those attending graduate or undergraduate classes.
The broader community.
Each case is based on the research, theories, practices and perspectives of people in all these areas. The case studies emphasize the importance of considering an interdisciplinary framework. Children’s needs cannot be met within the perspective of a single discipline.
The complex problems children face need solutions that integrate many and diverse ways of knowing. The case studies also help everyone better understand the mental health needs of children. We all have a role to play.
These case has been piloted within:
Graduate and undergraduate courses.
Discipline-specific and interdisciplinary settings.
Professional organizations.
Currently, the case studies are being offered to instructors and their staff and students in graduate and undergraduate level courses. They are designed to supplement existing course curricula.
Instructors have used the case study effectively by:
- Assigning the entire case at one time as homework. This is followed by in-class discussion or a reflective writing assignment relevant to a course.
- Assigning sections of the case throughout the course. Instructors then require students to prepare for in-class discussion pertinent to that section.
- Creating writing, research or presentation assignments based on specific sections of course content.
- Focusing on a specific theme present in the case that is pertinent to the course. Instructors use this as a launching point for deeper study.
- Constructing other in-class creative experiences with the case.
- Collaborating with other instructors to hold interdisciplinary discussions about the case.
To get started with a particular case, visit the related web page and follow the instructions to register. Once you register as an instructor, you will receive information for your co-instructors, teaching assistants and students. Get more information on the following web pages.
- Brianna and Tanya: A case study about infant and early childhood mental health
- About Steven: A children’s mental health case study about depression
Cari Michaels, Extension educator
Reviewed in 2023
© 2024 Regents of the University of Minnesota. All rights reserved. The University of Minnesota is an equal opportunity educator and employer.
- Report Web Disability-Related Issue |
- Privacy Statement |
- Staff intranet
- High contrast
- Press Centre
Search UNICEF
Adolescent development: case studies, investing in adolescents builds strong economies, inclusive communities and vibrant societies..
- Case studies
Adolescent development case studies
Advancing child-centred public policy in brazil through adolescent civic engagement in local governance, mainstreaming adolescent mental health & suicide prevention, adolescents take action to mitigate air pollution in vietnam, adolescent mental health knowledge summary: time for action.

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Int J Environ Res Public Health
Mental Health Problems among Young People—A Scoping Review of Help-Seeking
Katrin häggström westberg.
1 School of Health and Welfare, Halmstad University, SE-301 18 Halmstad, Sweden; [email protected] (M.N.); [email protected] (J.M.N.); [email protected] (P.S.)
2 Affecta Psychiatric Clinic, Sperlingsgatan 5, SE-302 48 Halmstad, Sweden
Maria Nyholm
Jens m. nygren, petra svedberg, associated data.
Documentation on the database searches, the stepped screening process and the thematic analysis are available from the corresponding author upon reasonable request.
Young people’s mental health is a public health priority, particularly as mental health problems in this group seem to be increasing. Even in countries with supposedly good access to healthcare, few young people seek support for mental health problems. The aim of this study was twofold, firstly to map the published literature on young people’s experiences of seeking help for mental health problems and secondly to validate whether the Lost in Space model was adaptable as a theoretical model of the help-seeking process described in the included articles in this scoping review. A scoping review was conducted in which we searched for literature on mental health help-seeking with a user perspective published between 2010 and 2020 in different databases. From the 2905 studies identified, we selected 12 articles for inclusion. The review showed how young people experience unfamiliarity and insecurity with regard to issues related to mental health and help-seeking. A strong wish for self-reliance and to safe-guard one’s own health were consistent among young people. Support structures were often regarded as inaccessible and unresponsive. There was a high level of conformity between the model on help-seeking and the analysed articles, reinforcing that help-seeking is a dynamic and psychosocial process.
1. Introduction
Young people’s mental health is a major public health issue. Mental health problems among young people contribute to impaired physical and mental health extending into adulthood [ 1 , 2 , 3 ]. Promoting young people’s mental health is an integral component in ensuring their development and improving health and social wellbeing across their lifespan [ 3 ]. In light of the high rate of mental health problems among this group, a corresponding high rate of help-seeking and use of support resources might be assumed; however, few young people actually seek and eventually access professional help. Delays in looking for help can be lengthy and are prevalent even in countries with good access to healthcare [ 4 , 5 , 6 , 7 , 8 , 9 ]. The process of searching for support involves barriers that relate to both individual and social context factors [ 8 , 10 ]. This contributes to the complexity involved in offering interventions to support them and highlights the need to understand the help-seeking process, whether online or in person, for young people with mental health problems.
Help-seeking is usually described as a rational, agency-based process where the individual plans, decides and acts on symptoms [ 11 ]. However, research also describes that help-seeking is not solely an individual act; rather, it is influenced by social factors throughout the process. Societal, organizational support structures set the limits and stipulate the opportunities to seek help [ 12 ]. Help-seeking thus depends both on factors at the individual level and structural resources for young people. Many studies that examine help-seeking for mental health among young people using cross-sectional designs on either the general community, or school populations [ 8 , 13 ] are based on descriptive data that is often generated through surveys, and focus on attitudes, rather than on experiences [ 14 ]. The main focus of previous literature has been on individual factors, such as mental health literacy, and less information can be found on the structural factors involved [ 8 , 13 ]. This calls for a deeper and more nuanced understanding of young people’s mental health help-seeking regarding contextual factors, with particular focus on their experiences and perspectives. An improved understanding of help-seeking for mental health problems can be used to improve practice and service delivery, and ultimately benefit young people’s mental health.
In this study, qualitative research exploring the help-seeking process in Sweden from the perspectives of young people with mental health problems was used as the theoretical point of departure [ 15 ]. Within this previous research, we produced a theoretical model of help-seeking, the Lost in Space model [ 15 ]. It showed how help-seeking was a long, non-sequential and dynamic process. In this research, young people described a process of moving in and out of the three help-seeking phases, Drifting, Navigating and Docking. Drifting was characterized by insecurity and unfamiliarity, with a lack of knowledge of mental health and the support system; Navigating was characterized by structural obstacles, a fragmented support system and wishes for help; while Docking was characterized by experiences of finding help. For the purpose of confirmability and usefulness, it is essential to validate and understand if the model can be applied to other settings and contexts—for example, whether the model is consistent with the experiences of help-seeking by young people in other countries. Therefore, the aim of this study was twofold, firstly to map the published literature on young people’s experiences of seeking help for mental health problems and secondly to validate whether the previously published Lost in Space model was adaptable as a theoretical model of the help-seeking process described in the included articles in this scoping review.
A scoping review was deemed the most preferable approach to responding to this broad area of interest [ 16 ]. Scoping reviews maintain a broad window for inclusion of studies of a range of types and levels of quality [ 17 ]. Our scoping review protocol was developed using the scoping review methodological framework proposed by Arksey and and O’Malley, entailing five framework stages. The framework was further developed by Levac, with a qualitative elaboration of the material [ 17 , 18 ]. These stages provide a clear sequential order in which to identify and collect studies, chart the data and report results, and the scoping review protocol was used for guiding the research.
2.1. Stage 1: Identifying the Research Question
A multidisciplinary research team with experience of health science research, including public health, nursing, and youth research was assembled to discuss and clarify the scope of inquiry and identify research questions. The target population of interest was defined as young people (ages 11–25) with experience of mental health problems, and experience of help-seeking in that regard. Mental health problems were defined as commonly experienced problems of depression or anxiety, as well as behavioural and emotional problems. Considering the concept of help-seeking, the term is used to understand the delay of care and to explore possible pathways for mental health promotion. For this study, help-seeking was defined as seeking and/or accessing professional help for mental health problems. Conceptually, help-seeking was regarded as a process influenced by social, psychological and contextual factors [ 12 ]. The research questions for this study were (1) to map general characteristics of published literature focusing on the young people’s experiences of seeking help for mental health problems, and (2) to explore how the previously published theoretical model Lost in Space could be further refined and complemented via an abductive approach, drawing the final set of categories and themes informed by the papers reviewed in this study.
2.2. Stage 2: Identifying Relevant Studies
A search strategy was developed in collaboration with a librarian to develop search terms using subject heading terms adapted to each of the three included databases: Medline/PubMed, PsycINFO and CINAHL. The search terms for the target population were adolescents, young and emerging adults; for the health outcome, they were mental health, depression, anxiety, and for the concept of interest, the term was help-seeking. Other criteria were limiting searches to studies written in English, and studies being published between 2010 and 2020 due to rapidly evolving research and policy changes in this area as well as the increased rates of mental health problems among young people. The searches were conducted during summer 2020. See Table S1 (Supplementary Materials) for the full search strategy.
Inclusion and Exclusion Criteria
Studies were eligible for inclusion if they investigated help-seeking among young people with mental health problems aged between 11 and 25. Only studies that specifically investigated young people’s own perspectives of experiencing or having experienced mental health problems and help-seeking were included. Since the intention was to understand help-seeking among young people with common mental health problems, studies on particular target groups or populations were excluded, such as studies on specific treatment interventions. Likewise, studies focusing on help-seeking attitudes or potential help-seeking intentions of general populations without personal experience of mental health help-seeking were excluded. Studies had to specifically focus on adolescents or young people; thus, studies with a more population-based perspective, or encompassing wider age groups, were excluded. Theses were not included as it was assumed that any material within a thesis on help-seeking, that otherwise fitted the inclusion criteria, would appear as published articles. Comments, editorials, consensus statements and other opinion-based papers were excluded, along with studies solely exploring the perspectives of others, other than the help-seekers themselves (e.g., families, helpers, professionals, etc.).
2.3. Stage 3: Study Selection
All identified studies from the searches were imported to the management reference tool EndNote, version 20.1, and duplicates were removed. Screening was carried out with a sequential, stepped approach and an iterative process between the authors of the study [ 18 ]. In the first step of study selection, titles and periodically abstracts were screened by KHW, who discarded obviously irrelevant studies based on the exclusion criteria. In the second step of study selection, abstracts of the remaining studies were screened independently by three of the authors (KHW, PS and MN) to determine eligibility based on the defined inclusion and exclusion criteria. Disagreements between the authors were discussed with a fourth author (JN) until consensus was reached. The third step required KHW to examine the full-text of the remaining articles to determine eligibility, subsequently discussing the articles with all authors. A PRISMA diagram ( Figure 1 ) details the screening process with number of papers retrieved and selection of the included studies.

Article search and selection process—PRISMA diagram.
2.4. Stage 4: Charting the Data
Data charting was conducted in accordance with scoping review standards using a template that was developed for the extraction of information from each study regarding the following: authorship, year of publication, journal, source of origin, design, population and age group, aims of the study, methodology and important results [ 17 ]. A descriptive, numerical summarization was made, presenting the extent, nature and scope of included studies [ 18 ], see Table S2 (Supplementary Materials) for the full bibliographic information of the included studies.
2.5. Stage 5: Collating, Summarizing and Reporting Results
A qualitative thematic analysis was conducted to examine and aggregate the findings from the help-seeking process, as depicted in the included studies [ 18 ]. For the thematic analysis, an abductive approach was taken [ 19 ], based on the previous Lost in Space model [ 15 ]. According to such an approach, hypotheses can be explicated through deduction and verified through induction. Abduction thus means that new explanations are based on background theories and, whilst taking empirical material and restrictions into account, may lead to elaborated knowledge [ 19 ].
The analysis began with reading the findings in the included articles several times, then identifying and inductively coding text and quotes [ 20 ] in relation to young people’s experiences of seeking help for mental health problems. In this phase, data were inductively scrutinized to discover experiences, expressions and perspectives, keeping codes close to the data; for example, the text ‘Some young people reported that discussing uncomfortable emotions was unfamiliar’ was coded as the theme Unfamiliarity. The deductive process followed, in which the theoretical model Lost in Space was employed. It describes help-seeking among young people with mental health problems in a Swedish context [ 15 ]. A categorization matrix was developed based on the model, emanating from the original subcategories and categories, the themes within the subcategories and the properties of themes. The deductive process in the analysis involved going back to the data and placing the inductively derived codes into themes and subcategories of the theoretical model. All themes from the original model were found through coding the analysed articles. Codes from the new material that did not match the original theoretical model subcategories contributed with new aspects to existing themes of the model and, in some cases, generated new themes, thereby broadening the understanding of help-seeking. In one instance, the name of one subcategory was altered to reflect new material. KWH performed the data analysis and, to enhance the quality and validity of the analysis, the data analysis was discussed continuously with all authors.
3.1. Mapping the Characteristics of Published Literature
In total, 1540 articles were identified as potentially relevant records, after duplicates were removed through the database searches. After the first screening of title and abstract, 1207 articles were excluded on the basis of age, format type, content (i.e., not dealing with help-seeking), focusing on specific populations or not being based on a user perspective. In the second round of screening, another 243 articles were excluded due to the eligibility criteria. In the third round of screening, the remaining 90 articles were reviewed in full-text and of these 12 articles met the full set of eligibility criteria.
The characteristics of the included studies are described in Table S2 (Supplementary Materials) . Seven articles were published between 2010 and 2015, and five after 2016. The designs were mostly qualitative, with individual interviews ( n = 9) and focus groups ( n = 7). Seven articles employed a combination of methods (for example, mixed methods), and two articles included information from surveys. The focus of articles covered: social and organizational factors impacting help-seeking, functional concerns, attitudes towards computerized mental health support, attitudes to consulting primary care, perceptions and help-seeking behaviours in schools, exploration and identification of barriers and facilitators in general populations with and without previous experience of mental health support, barriers and facilitators in male groups, links between masculinity and help-seeking, comparisons of groups’ help-seeking strategies and descriptions of experiences, self-management and help-seeking. The recruitment of participants varied, utilising educational settings ( n = 4), youth mental health services ( n = 2), community websites ( n = 1), primary care ( n = 1), youth services ( n = 2), previous participation in longitudinal studies ( n = 2) and community samples ( n = 3). Four articles focused specifically on young males, and four on barriers to help-seeking. Three articles were set in the USA, one in Canada, three in Australia and five in Europe. The age range, 11–25, was seen in a variation of age clusters, with the smallest age range being two years (ages 20–22) and the largest 13 years (ages 12–25); the mean age range covered was six years.
3.2. Examination of the Help-Seeking Process from the Perspectives of Young People
The findings from this examination showed a high level of agreement with the theoretical model Lost in Space. Overall, the results showed that help-seeking was a dynamic and psychosocial process without sequentially fixed stages, where young people expressed an unfamiliarity with, insecurity about and lack of knowledge of mental health issues, a longing for self-reliance and, in some contexts, a presence of stigma. Young people did not consider the support structures to be responsive or accessible. Below, Figure 2 outlines the examination of the help-seeking process from the perspectives of young people. It includes confirmed content of the old model, new content derived from the analysed articles, and elaborations according to the abductive method. The ‘number of meaning units’ refers to coded material in the analysed articles. ‘Original’ refers to subcategories and themes from the Lost in Space model, where findings were corroborated by codes from the analysed articles (‘confirmed content’), other elements that emerged showed further dimensions of experiences that contributed to new perspectives of established subcategories in the model (‘new content’), and some themes that emerged in the analysis were not readily encompassed within the subcategories in the original model (‘new’) (see Figure 2 ).

Examination of the help-seeking process from young people’s perspectives.
3.2.1. Drifting
Drifting, the initial category of the Lost in Space model, encompassed a general feeling of unfamiliarity, lack of knowledge, trivialising oneself and problems due to insecurity often by normalizing and minimizing one’s experiences. Young people’s voices in the analysed articles corroborated Drifting well, through similar expressions and experiences.
Fumbling in Life
In the original model, Fumbling in life encompassed themes of unfamiliarity, insecurity and trivialisation. Likewise, young people in the analysed articles expressed unfamiliarity with both mental health problems and not recognizing oneself. Lack of knowledge was frequently described both with regard to communicating, distinguishing and assessing emotions but also regarding where and when to seek help, leading to a sense of insecurity. Because of this insecurity, young people practised trivialisation, trying to make their problems smaller or unimportant. They also had the impression and fear that their problems would not be sufficient to receive support. In some of the analysed articles, trivialisation was presented as a rational strategy, enabling young people to downplay their problems and rationalizing not actively dealing with them or approaching others for help, whereas, in the original model, trivialisation was carried out due to a sense of insecurity. In this section, no conceptual changes to the original model are suggested.
In the original model, Struggling was characterized by simultaneous descriptions of mental health problems and incessant attempts and strategies to feel better, ambivalence and a longing for self-reliance. These themes re-appeared in the included articles. Mental health problems were described by the participants as emotional problems, panic attacks, sadness, self-harm, anxiety and lack of motivation. Within Struggling in the original model, young people usually referred to mental health problems as being something “within” (internal) rather than originating “outside” (global). However, in several of the analysed articles, the mental health problems were attributed to something “outside”. Hence, young people also related mental health problems to relationships, stress and risk-taking behaviour.
Themes on endeavouring strategies trying to deal with mental health problems were common in the included studies, as was also the case in the Lost in Space model, pointing to the more-or-less continual and relentless attempts and strategies young people performed in order to deal with their problems. Although it was proposed by young people in individual studies that seeking help requires effort, lack of effort was not a dominant issue for young people in either the original model or in most analysed articles. In some articles, an in-depth exploration of the strategies employed was undertaken, according to having an ‘approach’ or ‘avoidant’ character, or gendered differences, adding to the variation in strategies, whereas in the model, an abundance of strategies was ascertained; however, the type of strategy was not explored. Denial was a common strategy in both the original model and in the included articles. In the Lost in Space model, this was described as “shutting off”, with the intent of ignoring feelings and problems. This strategy was directed towards oneself: wanting to manage things, being strong and coping. In some of the analysed articles, denial was presented as relating to a sense of embarrassment, or as being done in order to protect others. Several reasons were attributed to this phenomenon: that young people did not want to trouble others, did not want to burden or alarm others, and did not trust others. In the model, reasons for denial were differentiated by a sense of responsibility, enacted by, for example, not sharing information with family and friends. Withholding information thus seemed to relate to aspects additional to a sense of responsibility and self-reliance.
A frequent theme in both the original model and in the findings from the included articles was self-reliance. Statements of wanting to be strong, trying to cope on one’s own, not sharing information and an elevated sense of responsibility to manage one’s life and mental health problems were evident. Ambivalence as a theme recurred throughout the material, in both the included studies and the original model. Young people expressed simultaneous and contradictory feelings and thoughts towards both themselves and their problems, others and help-seeking per se. They were often hesitant to seek help, whilst at the same time expressing a need and a longing for help.
The analysis of the included articles suggested no major conceptual changes to the original model, although the themes Endavouring strategies and Mental health problems are both elaborated.
Reaching a Point of No Return
Within Reaching a point of no return in the original model, young people expressed deterioration and a reaching out for support, often with the help of others. In Lost in Space, others were called ’catalysts’, showcasing their importance in actually initiating a help-seeking process. Within the analysed articles, important others were consistently brought up by the young people, with examples of others coaching, supporting, guiding and, in some instances, taking control of the help-seeking process. A new perspective in the included articles was a negative perception of control, and how others exerted control over them, compelling them to seek help. While this aspect of negative control did not emerge in the original model, an elaboration of the model may expand on the various functions of the important others, e.g., by dividing them into controllers vs. supporters. The other theme in this subcategory, deterioration, was brought up in several articles, as in the Lost in Space model. This indicated a worsening of symptoms and a decreased ability to function. Young people described not leaving the house, escalated behavioural problems, self-harm and suicide attempts, or ‘having a melt-down’ as triggers for seeking help. Young people also described how their problems were ‘revealed’ and others became aware of their problems, which in turn led to seeking help.
The included articles emphasise that seeking help is often a long process that takes place during a prolonged time-span. Therefore, in this section, a change of title of the subcategory Reaching a point of no return, to Transitioning towards decision, is suggested.
3.2.2. Navigating
The category Navigating depicted attempts of trying to find support, personal reflections, hopes and longings and wrestling with structural barriers. Expressions from young people in the analysed articles conformed well with the subcategories Trying to dock and Wrestling with structure.
Trying to Dock
This subcategory in the Lost in Space model entailed descriptions of personal reflections, hopes, longings and disappointment when trying to seek support. All themes from the original model were exemplified in the included articles. Hopes for help, as well as being safe, noticed and understood, were common in the included articles, as were accounts of the opposite, feeling unsupported. Miscommunication while not being understood or listened to also appeared in both materials as did accounts of being treated like a child and not taken seriously, thus containing references to issues of power. Several analysed articles contained descriptions by young people on how support was perceived as impersonal and instrumental rather than person-centred. This added aspects of negative references to professionalism and reliance on medication. Young people expressed the importance of reframing negative and medical terminology in positive and informal terms. Both materials contained descriptions of young people feeling unsupported, which led to continued and continual efforts of seeking support. A new theme, trust, was identified in the thematic analysis from descriptions of lack of confidence in treatment, and how familiarity facilitated help-seeking. A lack of trust was depicted as arising from limited prior contact, from anxiety about seeking help, from concerns about professional competence and from negative perceptions of professionals. Within the theme of trust in the articles, concerns about confidentiality and parental involvement surfaced, whereas, in the original model, these concerns were interpreted as structural obstacles.
Common themes in the articles were stigma and shame, whereas in the original model, this was not pervasive. The included articles relayed young people’s strong sense of shame about seeking help. They perceived it as a display of weakness. Fear of social consequences, ridicule and a longing to fit in led young people to describe a feeling of shame or embarrassment, and to having thoughts of what others would think and say. They also made efforts to conceal both mental health problems and help-seeking. Articles focusing exclusively on males stressed the gendered aspect of this, claiming that this group was affected by masculine ideals of strength and autonomy, which hindered displays of weakness and prevented help-seeking. In the original model, some findings relating to this theme were described; however, the term stigma was never used. Instead, this was described in the subcategory Wrestling with structure, in relation to seeking support in school, with references of embarrassment and an undesirable show of weakness in front of peers.
In this section, the analysed articles provide more aspects on the Feeling unsupported and Miscommunication themes. The large presence of codes in the new material relating to Stigma and Trust suggests the incorporation of Stigma and Trust as unique themes into the model.
Wrestling with Structure
In both the original model and the analysed articles, there were multiple references to structural obstacles, such as access, waiting times, resources, continuity, inadequate chains of support, and lack of coordination between supporters. Young people voiced feelings of not being met by professionals in an appropriate and timely manner, and concerns about how they were passed on, being referred to other support structures, and how there was a perceived lack of resources, making access difficult. Help-seeking was described as inconsistent, with repeated attempts at initiating and discontinuing help. Young people in several articles, and the original model, expressed that primary care was not an option when seeking support. Primary care was regarded as handling physical health complaints and that its practitioners were not being skilled in mental health issues. Particularly for the ‘younger’ of the young people, expressions that primary care was not directed at their age group were voiced. The inadequate support services theme was thus corroborated by young people in other contexts.
Confidentiality and age issues were concerns for the young people, both within the original model and the thematic analysis, primarily relating to parental control and insight. Both materials contained descriptions of how young people assumed and were concerned that confidential information shared with professional supporters would be communicated to parents. In some articles, this was said to relate to the theme of trust; however, confidentiality was mainly related to being a minor lacking power. Young people also voiced that being a minor was as an obstacle for independently accessing help. Likewise, age was an issue for the ‘older’ young people, who reported feeling out-of-place at youth-specific services. In the original model, a sense of resignation, often related to difficulties accessing support and feeling unsupported, was evident. The included articles provided additional material relating to this, as a sense of powerlessness appeared in several subcategories, and in the process as a whole.
The analysis supported a clearer conceptual division between subcategories Wrestling with structure and Trying to dock in the model. The latter entailed primarily personal accounts and experiences, expressions of hopes, disappointments and recounts of feelings, and the former referred primarily to structural conditions. Recurring references in relation to powerlessness suggest this is elevated to a permeating theme, capturing young people’s experience of seeking help.
3.2.3. Docking
Docking in the original model contained references from young people to the subcategories Finding support and Changing as a person.
Finding Support
All original themes of the subcategory Finding support were found in the thematic analysis. In both the original model and the analysed articles, young people described experiences of being validated, accepted, recognized and listened to. The importance of the comfort of support and initial positive contact was stressed. Descriptions of good and bad supporters and preferences regarding, for example, gender and profession, were evident. Both materials contained descriptions of negative outcomes and unwanted consequences from having sought help; for example, in the original model, this was described as problems being exaggerated and social services becoming involved. In the analysed articles were descriptions of referrals to support services appearing as punitive rather than helpful. This subcategory also contained accounts in both the analysed articles and the original model of young people being disregarded and not being taken seriously.
In this section, no changes to the model are suggested.
Changing as a Person
In the original model, this subcategory described the consequences of successful help-seeking in the form of gaining knowledge and positive personal change. Young people in the original model stressed the positive aspects and changes after having experienced mental health problems. Some references were found in the articles with regard to this subcategory, with personal change depicted as finding a more positive outlook on life through one’s own determination and decisiveness.
In this section, the analysed articles provide more aspects on the theme Changing as a person, but no changes to the model are suggested.
Overall, the findings from the analysis aided in developing an elaborated model of help-seeking, Figure 3 . The overall notion of help-seeking as a fluid and dynamic process with the three categories Drifting, Navigating and Docking was reinforced.

Elaborated and further developed theoretical model of help-seeking among young people for mental health problems.
4. Discussion
This scoping review aimed to map published literature on young people’s experiences of seeking help for mental health problems, and to validate whether the previously published model Lost in Space was adaptable as a theoretical model of the help-seeking process. A high level of conformity was found between help-seeking as depicted by the original Lost in Space model and the analysed articles of this study. The analysis reinforced that help-seeking is to be regarded as a fluid and psychosocial process, often experienced by users as unfamiliar and obstacle-laden, tainted by feelings of powerlessness [ 21 , 22 , 23 , 24 ].
4.1. Discussion and Implications in Relation to the Original Model Lost in Space
After reviewing up-to-date literature on user perspectives of help-seeking for mental health problems among young people, it is clear that the depiction of the initial stage of help-seeking, as being characterized by a sense of drifting, was, to a large extent, corroborated from young people’s experiences described in the reviewed articles. Regardless of context, young people expressed a general feeling of unfamiliarity and a lack of knowledge, often coupled with a sense of insecurity, and trivialisation of experiences [ 21 , 22 , 23 , 25 , 26 , 27 , 28 , 29 , 30 ]. This was also supported by a large number of codes and expressions relating to the endeavouring strategies theme in an effort to be self-reliant [ 22 , 23 , 25 , 26 , 27 , 28 , 29 , 30 , 31 ]. This points to the more-or-less continual and relentless nature of the efforts of young people to deal with their problems. A strong wish for self-reliance was consistently stressed in the reviewed articles, with a large variation and number of strategies used to implement self-reliance and deal with mental health problems. Incorporating an elaboration regarding the characteristics of strategies—whether positive/negative, destructive/constructive or approach/avoidant strategies—would provide an additional perspective on how mental health is dealt with by young people. The reviewed articles confirmed that reaching a decision to seek help often takes place with the aid of others [ 21 , 22 , 23 , 24 , 25 , 29 , 31 , 32 ] and distinction between ‘controllers’ and ‘supporters’ in this regard may further elaborate the model. Re-naming of the subcategory Reaching a point of no return into Transitioning towards decision would reflect the transitional nature of the mental health help-seeking process.
The category Navigating, capturing both personal experiences and structural barriers, was well confirmed by the review. Reflections of not being met by professionals in an appropriate and timely manner, and observations of a perceived lack of resources making access difficult, surfaced in both the original model and the included articles [ 23 , 26 , 29 ]. Accounts of not being taken seriously, being treated like a child, not listened to and disregarded, indicating power-issues relating to the experiences of young people, as well as descriptions of inconsistent use of support, repeatedly initiating and discontinuing help, appeared in the original model as well as the included articles [ 22 , 26 , 28 , 29 ]. Stigma and Trust surfaced as new themes, and Stigma in particular appeared with a large number of codes in the analysed articles. Young people described a feeling of shame, embarrassment, thoughts of what others would think and say and various efforts to conceal both mental health problems and their help-seeking [ 21 , 22 , 23 , 25 , 26 , 27 , 28 , 31 ]. Several articles dealt exclusively with young men and boys, proposing that the reasons for not seeking help were strongly conditioned by gender, with masculine ideals of strength and autonomy acting as obstacles for help-seeking [ 21 , 23 , 28 , 31 ]. Similar findings emerged in the Lost in Space model, where issues of self-reliance, wanting to be strong, and shunning displays of weakness, were shared between participants, and were not gender specific. Cultural variations may account for this difference between studies and findings. This said, most participants in studies on help-seeking are female and the findings may translate poorly to other populations and contexts. Help-seeking is exceptionally low among boys and young men, which in itself calls for a focus on specific populations with particularly low help-seeking [ 33 , 34 ].
The latter part of the original model, Docking, was not as well corroborated through the analysis. There were few descriptions of actually finding support and even fewer of personal reflections on the effects of finding help [ 21 , 22 , 31 ]. It may be that research on the help-seeking process does not focus on support and is discontinued as soon as support is established, and aspects of this may be found in other literature on service utilization or treatment satisfaction. However, by dividing the help-seeking journey into smaller isolated fractions, focus on the process as a whole could be missed, resulting in a stunted model and less understanding of the help-seeking process. Overall, the included articles reinforced the model of help-seeking as a dynamic and psychosocial process, consisting of different stages but without being sequentially fixed.
4.2. Discussion and Implications in Practice
This review on help-seeking for common mental health problems included young people from the age of 11 to 25, thus also including young adults. The studies described in the included articles were based on varied recruitment strategies from different contexts. No specific patterns according to age or context could be discerned. The concerns voiced in the studies included themes on structural barriers of the support system, an unfamiliarity and lack of knowledge of mental health and the support system, and simultaneously, a wish for self-reliance, suggesting possible strategies for meeting the help-seeking needs of young people. Although this study aimed to include articles focusing on groups that were wide enough to be defined as population-based, the focus of the included articles tended to be on particular populations, stressing the vulnerability and poor help-seeking of one particular group. Thus, the research had ethno-centric tendencies, whereas there were large overlaps and resemblances of experiences by young people in the help-seeking process regardless of contexts. The attribution of non-help-seeking to stigma and cultural norms amongst Black, Latino and Chinese American youth was observed by others, pointing to this being a more general, rather than group-specific phenomenon [ 32 ].
Structural factors, and how young people experience the support system, play an important role in the help-seeking process. Despite different contexts, young people expressed similar concerns relating to issues of availability and accessibility. There were views that waiting times were too long, resources were too few, and in some contexts, that costs and distances posed problems [ 21 , 23 , 25 , 26 , 28 , 29 ]. Other research has shown that there is a perceived inaccessibility of the support system across different groups of young people regarding resources, entry requirements and coordination between services [ 13 ]. Structural obstacles stretch over different geographical and socio-economic backgrounds at the macro level, with high-income countries still showing substantial delays and poor help-seeking rates for young people [ 14 , 35 ]. Thus, even in favourable circumstances, young people perceive structural barriers, pointing to how the support system does not accommodate the fluid and changeable nature of help-seeking. Young people regard mental health as a complex social and relational matter [ 36 ]. They often present with diagnostically confusing symptoms, and support systems that are traditionally organized according to medical specialities may not meet the needs of young people with common mental health problems [ 37 ]. Integrated youth centres, focusing on meeting young people’s needs in one place through multidisciplinary support with consideration of the context, show promising results [ 38 , 39 ]. In comparison to traditional support, which is by definition siloed and often entails entry requirements according to diagnostic thresholds, integrated youth-friendly services seem to increase help-seeking and access to support, even among groups that are usually hard to reach [ 33 , 39 ]. Studies in a Swedish context have pointed out that youth health clinics providing services to build upon with multi-professional teams and expertise on mental health are available throughout Sweden [ 40 ].
Young people reported a lack of knowledge on mental health and the support system, leading to a sense of insecurity and possibly a delay of help-seeking. Improved health literacy among young people may facilitate help-seeking through mechanisms of awareness of service availability and symptom recognition [ 13 ]. However, improved help-seeking and mental health among young people may require more than only improved knowledge. Previous reviews have, for example, shown past positive experiences and outcomes of help-seeking and positive contacts with support professionals to be facilitators for seeking help [ 4 , 8 ]. At the same time, a preference for self-reliance when facing mental health problems is consistently reported, with this being particularly prominent in studies with participants having previous experience of mental health problems and mental health support, contradicting the findings of past experiences facilitating help-seeking [ 8 , 23 ]. Young women in particular seem to have poor expectations regarding therapeutic outcomes, signalling a lack of trust in professional supporters, with treatment being perceived as impersonal and protocol-driven [ 23 ]. The results of this study identified the importance of supporters’ ability to meet young people responsively, using a person-centred approach. Young people felt more comfortable when the supporters did not use medical language and emphasized the importance of using positive and informal terms for improving communication between the young person and the supporter. Other studies have confirmed this finding, underlining the importance of having young staff who are skilled, respectful, welcoming, and allow for participation and shared decision-making [ 39 ].
With this review showing how young people experience mental health help-seeking as a psychosocial and fluid process, often with lack of knowledge and a sense of insecurity, prompt consideration of the organization of present support systems is needed. Young people need to be met in a person-centred and flexible manner. Perhaps, this is where the greatest effort is needed, addressing issues of power from the perspectives of young people, improving opportunities for personal self-reliance and personalized support.
5. Methodological Considerations
This review has some limitations. The choice of databases and keywords was developed in accordance with an experienced health literature librarian; however, making a choice always entails the risk that some information may have been missed. Other databases and different keywords may have produced different results. The criteria for including articles were that they should deal with the direct perspectives of young people who had experienced mental health problems and/or help-seeking. Whilst excluding those who had no experience of help-seeking (thus all articles dealing with intentions to seeking help only) might have been a clear-cut and easy choice, that would also have meant that we excluded those with experience of mental health problems who had not sought help for various reasons; thus, avoidance is also a perspective that is worth taking into consideration.
We aimed to include studies focusing on groups wide enough to be defined as population-based; nevertheless, these still often utilized an ethnocentric perspective, such as having a particular ethnic descent. This automatically raises the issue of generalizability and transferability. It was evident that studies consistently focused on particular populations, stressing the vulnerability and poor help-seeking of this particular group. However, similar claims kept reappearing, regardless of which particular group was being studied. A noteworthy phenomenon is that all included articles were published in Western countries. This also limits the transferability of the findings, as young people around the world may be situated in significantly different contexts.
In order to limit bias, the work was conducted by alternating methods of individual and joint reviews. However, subjectivity is a relevant issue that the authors of this review could not completely avoid.
6. Conclusions and Implication
The field of help-seeking among young people for mental health problems is receiving growing attention in research and academic literature. However, this review shows that there is substantial heterogeneity among studies with regard to methods, populations and how help-seeking is investigated. In qualitative literature exploring user perspectives, help-seeking is depicted as a fluid, dynamic and psychosocial process, validating the theoretical model of Lost in Space. Important findings include the presence of stigma, a lack of knowledge of mental health issues, a longing for self-reliance and a sense of powerlessness expressed by young people in various contexts and countries. Paying attention to these findings would imply acknowledging young people’s sense of feeling lost, making support services more flexible and person-centred.
Acknowledgments
Caroline Karlsson greatly contributed with the graphical model.
Supplementary Materials
The following are available online at https://www.mdpi.com/article/10.3390/ijerph19031430/s1 , Table S1, full search strategy, Table S2, characteristics of included studies.
Author Contributions
All authors (K.H.W., M.N., J.M.N. and P.S.) made significant contributions to the original paper. K.H.W., M.N., J.M.N. and P.S. together identified the research question and designed the study. The data search was conducted by K.H.W., and stepped screening was performed by K.H.W., M.N., J.M.N. and P.S. In addition, K.H.W. drafted the manuscript and M.N., J.M.N. and P.S. provided critical revision of the paper in terms of important intellectual content. All authors have read and agreed to the published version of the manuscript.
This research received no external funding.
Institutional Review Board Statement
This study did not require ethical clearance.
Informed Consent Statement
Not applicable.
Data Availability Statement
Conflicts of interest.
The authors declare no conflict of interest.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.
- News stories
- Blog articles
- NSPCC Learning podcast
- Why language matters
- Sign up to newsletters
- Safeguarding in Education Update
- CASPAR email alert
- Key topics home
- Safeguarding and child protection
- Child abuse and neglect
- Child health and development
- Safer recruitment
- Case reviews
- Online safety
- Research and resources home
- NSPCC research
- Safeguarding resources
- How Safe conference
- Self-assessment tool
- Schools and colleges
- Training home
- Basic safeguarding courses
- Advanced training
- Elearning courses
- Designated person training
- Schools and education courses
- Services home
- Direct work: children and families
- Talk Relationships
- Consultancy
- Library and Information Service
- Support for local communities
- NSPCC Helpline
- Speak out Stay safe schools service
- My learning
- Self-assessment
- /g,'').replace(/ /g,'')" v-html="suggestion">
Teenagers: learning from case reviews
Summary of risk factors and learning for improved practice around working with teenagers.
Published case reviews highlight that practitioners sometimes struggle to work with teenagers who are experiencing complex issues. Interventions can focus on tackling challenging behaviour, rather than exploring the underlying causes and risk factors. This sometimes causes practitioners to lose sight of the fact that teenagers are children in need of protection.
The learning from these reviews highlights that professionals need to listen to teenagers, but also be able to balance the young person’s wishes with their best interests. Intervention needs to be timely and appropriate.
Published: February 2021
Browse our full series of learning from case reviews briefings
Our series of thematic briefings highlight the learning from case reviews conducted when a child dies, or is seriously harmed, as a result of abuse or neglect. Each briefing focuses on a different topic or learning for specific sectors, pulling together key risk factors and practice recommendations.
> See the full series
More about case reviews
We work with local safeguarding partners to ensure that learning from case reviews can be accessed and shared at a local, regional and national level.

Find out how you can apply the lessons from case reviews and improve your practice to help protect children and young people.

Browse through our list of child safeguarding practice reviews, serious case reviews, significant case reviews and child practice reviews which were added to the National case review repository between 2019 and 2023.

Subscribe to our monthly email newsletter alerting you to the case reviews we have added to the National collection of case reviews repository at the NSPCC.
Find out more about case reviews
Related resources

Our online course will help you to understand your safeguarding responsibilities and learn how to act appropriately and confidently to protect the young people you work with.

Learn about new research from the Safer Young Lives Research Centre (SYLRC) covering how to best support adolescent mental health and wellbeing after sexual abuse .

Key messages about the criminal exploitation of children and young people in England based on rapid reviews received by the Child Safeguarding Practice Review Panel between July 2018 and March 2019.

Looking for more research and resources?
IMAGES
VIDEO
COMMENTS
The present case study was undertaken to document mental health vulnerability of school-going adolescent in rural Gujarat. The study reveals that 14% of the study population is vulnerable for mental health problems. More than 18% of adolescents have internalizing (emotional) and more than 16% have externalizing (conduct) manifestations.
Case Study: Kelli. A 15-year-old girl, Kelli, is referred to a neurologist due to unexplained symptoms of involuntary, uncontrollable behavior that includes eye-blinking, shoulder shrugging, frequent throat clearing, and randomly moving her arm around in circles. These symptoms have been present since she was in preschool and have increased in ...
An assessment identifies the needs of the child or adolescent and the family and establishes goals, intervention plans, discharge criteria, and a discharge plan. ... Tertiary level of Positive Behavior Support, 1 quasi-experimental study, 1 single-cohort study, 1 case study: Behavior problems: Intervention had some positive effects on reducing ...
For a diagnosis, an adolescent must have at least 5 symptoms, which must include at least one of either of the first 2 symptoms, for at least 2 weeks. 3. Symptoms of dysthymic disorder in adolescents. Depressed or irritable mood must be present for most of the day, more days than not, for at least 1 year.
Pediatrics (2019) 144 (6): e20193150. Adolescence is the transitional bridge between childhood and adulthood; it encompasses developmental milestones that are unique to this age group. Healthy cognitive, physical, sexual, and psychosocial development is both a right and a responsibility that must be guaranteed for all adolescents to ...
Research on mindfulness-based programs (MBPs) for adolescents suggests improvements in stress, emotion regulation, and ability to perform some cognitive tasks. However, there is little research examining the contextual factors impacting why specific students experience particular changes and the process by which these changes occur. Responding to the NIH call for "n-of-1 studies" that ...
This highlights the need to explore everyday challenges as experienced by adolescents and young adults in light of the increasingly prevalent rates of self-reported mental health problems. A Greek study found that pupils (13-16 years) described mental illness in a multi-dimensional way including, for example, being in a certain state of ...
p. 433). Furthermore, beyond an RCT, systematic case study can give in-depth information about "how a treatment works, and the processes set in motion when treatment is implemented" (p. 432). In this study, we applied a systematic case study approach to a subsample of adolescents who participated in a larger intervention study of the L2B ...
Traumatic experiences may create difficulty with developing and differentiating another person's point of view (that is, mentalization) due to the formation of rigid cognitive schemas that dictate notions of self, others, and the external world (Frydman & McLellan, 2014).For early adolescents, the ability to diversify a single perspective with complexity is central to modulating affective ...
THE ADOLESCENT CASE STUDY . Goals: • To look carefully at a developing adolescent to understand his or her social, psychological, ... You will have the opportunity to review case studies written by other students who have previously engaged in this kind of study. You will also the opportunity to have your case study reviewed by a peer and
Present study was conducted to find the profiles and patterns of emotional and behavioral problems in adolescents from general population who had never been reported or diagnosed. A sample of 300 adolescents from public and private schools of Lahore, (13 to 17 years old, Mean=14.8) participated in the study.
psychosocial problems ranging between 10-40%. AIM: To study the prevalence of psychosocial, emotional, behavioral problems and sexual orientation, drug abuse in adolescent (less than 18 years) and ...
I ndia knows all about the importance of getting timely help for mental health problems. "I have had issues since late primary school although I only recognised it in myself about four years ago ...
Erikson's psychosocial development is a well-known and sound framework for adolescent development. However, despite its importance in scientific literature, the scarcity of literature reviews on Erikson's theory on adolescence calls for an up-to-date systematization. Therefore, this study's objectives are to understand the extent and nature of published research on Erikson's ...
As such, anti-stigma interventions deserve heavy focus, particularly in high-risk populations. The students in this study represent a segment of general adolescents with demonstrated need for mental health promotion efforts. Although this study's sample size is small, it is enriched for youth with increased risk of developing mental health ...
Our Case Studies. We have complied a series of publications and case studies to illustrate the type of projects we work on and how we support child health policy-making in England. The Healthy Child; Healthcare provision; Mental health; Adolescence; Long-term conditions; Sociology of health and illness: Health economics; Social care
Mental health. Children's mental health case studies. Explore the experiences of children and families with these interdisciplinary case studies. Designed to help professionals and students explore the strengths and needs of children and their families, each case presents a detailed situation, related research, problem-solving questions and ...
A similar observation was found in a hospital-based retrospective study among adolescents (10-19 years), that white discharge was the most common reproductive health problem among adolescent girls . A significant reduction in counselling for SRH problems (<0.001), menstruation-related problems (<0.001), nutrition (<0.005), and other health ...
A study of the links between parenting and adolescent neglect 4 Child neglect has become topical in recent years with a burgeoning of research studies and the development of new policy and practice initiatives. This may be because neglect continues to be the main type of maltreatment recorded in official data on safeguarding and because it
Adolescent development: Case studies. Investing in adolescents builds strong economies, inclusive communities and vibrant societies.
The concerns voiced in the studies included themes on structural barriers of the support system, an unfamiliarity and lack of knowledge of mental health and the support system, and simultaneously, a wish for self-reliance, suggesting possible strategies for meeting the help-seeking needs of young people. Although this study aimed to include ...
Published case reviews highlight that practitioners sometimes struggle to work with teenagers who are experiencing complex issues. Interventions can focus on tackling challenging behaviour, rather than exploring the underlying causes and risk factors. This sometimes causes practitioners to lose sight of the fact that teenagers are children in ...
Kashmir (India) thfrom class 6 from a government school where the student with special need/learning difficulty is not able to understand concepts, despite teachers' effort, a research based on a case study may be conducted to understand the reasons behind that and find a reliable, applicable and effective solution of the problem of the child ...
May 7, 2024 - Teen mental health problems have hit a new peak in the U.S., and the gap between the number of teenagers who report conditions like anxiety, depression, and hopelessness and the ...