- Follow us on Facebook
- Follow us on Twitter
- Criminal Justice
- Environment
- Politics & Government
- Race & Gender
Expert Commentary

Performance-enhancing drugs in athletics: Research roundup
2015 roundup of research on the use of performance-enhancing drugs in athletics and academics as well as their potential health effects.

Republish this article

This work is licensed under a Creative Commons Attribution-NoDerivatives 4.0 International License .
by Leighton Walter Kille, The Journalist's Resource June 9, 2015
This <a target="_blank" href="https://journalistsresource.org/health/athletic-academic-performance-enhancing-drugs-research-roundup/">article</a> first appeared on <a target="_blank" href="https://journalistsresource.org">The Journalist's Resource</a> and is republished here under a Creative Commons license.<img src="https://journalistsresource.org/wp-content/uploads/2020/11/cropped-jr-favicon-150x150.png" style="width:1em;height:1em;margin-left:10px;">
Performance-enhancing drugs have a long history in sports, of course, but pharmacological research has led to a surge in the number of substances available, each with its own potential for misuse.
Given the potential financial rewards of athletic success, it’s no surprise that we’ve been witness to a seemingly endless procession of allegations and scandals. Sluggers Barry Bonds (steroids) and Alex Rodriguez (human growth hormone); cyclists Lance Armstrong (EPO), Floyd Landis (testosterone) and Alberto Contador (clenbuterol); runners Tyson Gay (steroids) and Justin Gatlin (testosterone); and golfer Vijay Singh (IGF-1) are only some of the more prominent professionals implicated in such behavior. The complicity of medical professionals and shadowy labs is often involved, and a 2015 report from the International Cycling Union (UCI) found the sport’s own governing body bore significant responsibility.
Not surprisingly, hard numbers on rates of usage are difficult to come by, but anecdotal evidence isn’t lacking and anonymous surveys have provided some insight. Questionable use of medications and supplements have also been reported in the U.S. armed forces , fire and police departments , amateur athletics , and even high schools .
Below is a selection of studies on a range of issues related to performance-enhancing drugs. It has sections on their potential economic impacts, prevalence , health effects and athletes’ attitudes . For additional studies on these topics, you can search PubMed , which is the federal clearinghouse for all medical research. At bottom, we have also included some studies relating to cognitive-enhancing drugs and the related academic dimensions of this issue.
—————————-
“The Economics of Corruption in Sports: The Special Case of Doping” Dimant, Eugen; Deutscher, Christian. Edmond J. Safra Working Papers, No. 55, January 2015.
Abstract: “Corruption in general and doping in particular are ubiquitous in both amateur and professional sports and have taken the character of a systemic threat. In creating unfair advantages, doping distorts the level playing field in sporting competition. With higher stakes involved, such distortions create negative externalities not only on the individual level (lasting health damages, for example) but also frictions on the aggregate level (such as loss of media interest) and erode the principle of sports. In this paper, we provide a comprehensive literature overview of the individual’s incentive to dope, the concomitant detrimental effects and respective countermeasures. In explaining the athlete’s motivation to use performance enhancing drugs, we enrich the discussion by adapting insights from behavioral economics. These insights help to understand such an athlete’s decision beyond a clear-cut rationale but rather as a product of the interaction with the underlying environment. We stress that in order to ensure clean sports and fair competition, more sophisticated measurement methods have to be formulated, and the respective data made publicly available in order to facilitate more extensive studies in the future. So far, the lack of data is alarming, especially in the area of elite sports where the stakes are high and doping has a substantial influence.”
“The Frequency of Doping in Elite Sport: Results of a Replication Study” Pitsch, Werner; Emrich, Eike. International Review for the Sociology of Sport , October 2012, Vol. 47, No. 5, 559-580. doi: 10.1177/1012690211413969.
Abstract: “The difficulty of measuring the prevalence of doping in elite sport is a recurring topic in the scientific literature on doping. The Randomized Response Technique is a method for asking such embarrassing or even threatening questions while allowing the respondents to answer honestly. It was used to measure the prevalence of doping among German squad athletes by Pitsch et al. (2005, 2007). In a replication study with better sampling control, it was possible to replicate the general trend of the data from the 2005 study…. The paper-based survey resulted in a rate of 10.2% ‘honest dopers,’ irrespective of the disciplines, obtained with the question: ‘Have you ever knowingly used illicit drugs or methods in order to enhance your performance?’ By adding the rate of cheaters (24.7%), whose behaviour the researchers know nothing about, one can calculate the interval (10.2%, 34.9%), which should include the true rate of dopers throughout their career among German elite athletes. In contrast, this means that the larger proportion of athletes, namely, 65.2%, represents ‘honest non-dopers.’ In the 2008 season, this figure was 65%.”
“Growth Hormone Doping in Sports: A Critical Review of Use and Detection Strategies” Baumann, Gerhard P. Endocrine Reviews , April 2012, Vol. 33, No. 2 155-186. doi: 10.1210/er.2011-1035.
Abstract: “[Growth hormone] is believed to be widely employed in sports as a performance-enhancing substance. Its use in athletic competition is banned by the World Anti-Doping Agency, and athletes are required to submit to testing for GH exposure…. The scientific evidence for the [performance-enhancing characteristics] of GH is weak, a fact that is not widely appreciated in athletic circles or by the general public. Also insufficiently appreciated is the risk of serious health consequences associated with high-dose, prolonged GH use. This review discusses the GH biology relevant to GH doping; the virtues and limitations of detection tests in blood, urine, and saliva; secretagogue efficacy; IGF-I doping; and information about the effectiveness of GH as a performance-enhancing agent.”
“Supplements in Top-Level Track and Field Athletes” Tscholl, Philippe; Alonso, Juan M.; Dollé, Gabriel; Junge, Astrid; Dvorak, Jiri. American Journal of Sports Medicine , January 2010, Vol. 38, No. 1, 133-140. doi: 10.1177/0363546509344071.
Abstract: “Analysis of 3,887 doping control forms undertaken during 12 International Association of Athletics Federations World Championships and one out-of-competitions season in track and field. Results: There were 6,523 nutritional supplements (1.7 per athlete) and 3,237 medications (0.8 per athlete) reported. Nonsteroidal anti-inflammatory drugs (NSAIDs; 0.27 per athlete, n = 884), respiratory drugs (0.21 per athlete, n = 682), and alternative analgesics (0.13, n = 423) were used most frequently. Medication use increased with age (0.33 to 0.87 per athlete) and decreased with increasing duration of the event (from sprints to endurance events; 1.0 to 0.63 per athlete). African and Asian track and field athletes reported using significantly fewer supplements (0.85 vs. 1.93 per athlete) and medications (0.41 vs. 0.96 per athlete) than athletes from other continents. The final ranking in the championships was unrelated to the quantity of reported medications or supplements taken. Compared with middle-distance and long-distance runners, athletes in power and sprint disciplines reported using more NSAIDs, creatine, and amino acids, and fewer antimicrobial agents. Conclusion: The use of NSAIDs in track and field is less than that reported for team-sport events. However, nutritional supplements are used more than twice as often as they are in soccer and other multisport events; this inadvertently increases the risk of positive results of doping tests.”
“Alcohol, Tobacco, Illicit Drugs and Performance Enhancers: A Comparison of Use by College Student Athletes and Nonathletes” Yusko, David A.; et al. American Journal of Sports Medicine, August 2010. doi: 10.3200/JACH.57.3.281-290.
Abstract: Compares the prevalence and pattern of substance use in undergraduate student athletes and nonathletes from 2005-2006. Data was collected using questionnaires from male (n = 418) and female (n = 475) student athletes and nonathletes from 2005-2006 to assess prevalence, quantity, and frequency of alcohol and drug use, and to determine patterns of student athletes’ alcohol and drug use during their athletic season versus out of season. Male student athletes were found to be at high risk for heavy drinking and performance-enhancing drug use. Considerable in-season versus out-of-season substance use fluctuations were identified in male and female student athletes. Additional, and possibly alternative, factors are involved in a student athlete’s decision-making process regarding drug and alcohol use, which suggests that the development of prevention programs that are specifically designed to meet the unique needs of the college student athlete may be beneficial.”
Health effects
“Performance Enhancing Drug Abuse and Cardiovascular Risk in Athletes” Angell, Peter J.; Chester, Neil; Sculthorpe, Nick; Whyte, Greg; George, Keith; Somauroo, John. British Journal of Sports Medicine , July 2012. doi:10.1136/bjsports-2012-091186.
Abstract: “Despite continuing methodological developments to detect drug use and associated punishments for positive dope tests, there are still many athletes who choose to use performance- and image-enhancing drugs. Of primary concern to this review are the health consequences of drug use by athletes…. We will address current knowledge, controversies and emerging evidence in relation to cardiovascular (CV) health of athletes taking drugs. Further, we delimit our discussion to the CV consequences of anabolic steroids and stimulant (including amphetamines and cocaine) use. These drugs are reported in the majority of adverse findings in athlete drug screenings and thus are more likely to be relevant to the healthcare professionals responsible for the well-being of athletes.”
“Illicit Anabolic-Androgenic Steroid Use” Kanayama, Gen; Hudson, James I.; Pope Jr., Harrison G. Hormones and Behavior , Volume 58, Issue 1, June 2010, Pages 111-121. doi: 10.1016/j.yhbeh.2009.09.006.
Abstract: “The anabolic-androgenic steroids (AAS) are a family of hormones that includes testosterone and its derivatives. These substances have been used by elite athletes since the 1950s, but they did not become widespread drugs of abuse in the general population until the 1980s. Thus, knowledge of the medical and behavioral effects of illicit AAS use is still evolving. Surveys suggest that many millions of boys and men, primarily in Western countries, have abused AAS to enhance athletic performance or personal appearance. AAS use among girls and women is much less common. Taken in supraphysiologic doses, AAS show various long-term adverse medical effects, especially cardiovascular toxicity. Behavioral effects of AAS include hypomanic or manic symptoms, sometimes accompanied by aggression or violence, which usually occur while taking AAS, and depressive symptoms occurring during AAS withdrawal. However, these symptoms are idiosyncratic and afflict only a minority of illicit users; the mechanism of these idiosyncratic responses remains unclear. AAS users may also ingest a range of other illicit drugs, including both “body image” drugs to enhance physical appearance or performance, and classical drugs of abuse. In particular, AAS users appear particularly prone to opioid use. There may well be a biological basis for this association, since both human and animal data suggest that AAS and opioids may share similar brain mechanisms. Finally, AAS may cause a dependence syndrome in a substantial minority of users. AAS dependence may pose a growing public health problem in future years but remains little studied.”
“Adverse Health Effects of Anabolic-Androgenic Steroids” Van Amsterdama, Jan; Opperhuizena, Antoon; Hartgensb, Fred. Regulatory Toxicology and Pharmacology , Volume 57, Issue 1, June 2010, Pages 117-123. doi: 10.1016/j.yrtph.2010.02.001.
Abstract: “Anabolic-androgenic steroids (AAS) are synthetic drugs derived from testosterone. Illegally, these drugs are regularly self-administered by body builders and power lifters to enhance their sportive performance. Adverse side effects of AAS include sexual dysfunction, alterations of the cardiovascular system, psyche and behavior, and liver toxicity. However, severe side effects appear only following prolonged use of AAS at high dose and their occurrence is limited…. The overwhelming stereotype about AAS is that these compounds cause aggressive behavior in males. However, the underlying personality traits of a specific subgroup of the AAS abusers, who show aggression and hostility, may be relevant, as well. Use of AAS in combination with alcohol largely increases the risk of violence and aggression. The dependence liability of AAS is very low, and withdrawal effects are relatively mild. Based on the scores for acute and chronic adverse health effects, the prevalence of use, social harm and criminality, AAS were ranked among 19 illicit drugs as a group of drugs with a relatively low harm.”
“Effects of Growth Hormone Therapy on Exercise Performance in Men” Triay, Jessica M.; Ahmad, Bushra N. Trends in Urology & Men’s Health , July/August 2012, Vol. 3, Issue 4, 23-26. doi: 10.1002/tre.274.
Conclusions: “In the athletic arena, [growth hormone] doping is considered to be widespread and used in combination with other agents, and regimens vary depending on individual preferences and cost implications…. It must be recognised that the effects of GH administration in adults with a normal GH/IGF-1 axis are not comparable to those in GH deficiency and that the complexity of processes influencing GH release and peripheral actions means that overall performance should be considered as opposed to isolated effects. Although studies to date have been small in both subject numbers and treatment times, they have demonstrated measurable changes in GH and IGF-1 levels, as well as possible deleterious effects on exercise performance that should be taken seriously.”
“Performance-Enhancing Drugs on the Web: A Growing Public-Health Issue” Brennan, Brian P.; Kanayama, Gen; Pope Jr., Harrison G. American Journal on Addictions , March-April 2013, Vol. 22, Issue 2, 158-161. doi: 10.1111/j.1521-0391.2013.00311.x.
Abstract: “Today’s Internet provides extensive “underground” guidelines for obtaining and using illicit substances, including especially anabolic-androgenic steroids (AAS) and other appearance- and performance-enhancing drugs (APEDs). We attempted to qualitatively characterize APED-related Internet sites. We used relevant Internet search terms [and] found thousands of sites involving AAS and other APEDs. Most sites presented an unabashedly pro-drug position, often openly questioning the qualifications and motivations of mainstream medical practitioners. Offers of AAS and other APEDs for sale, together with medical advice of varying legitimacy, was widespread across sites. Importantly, many sites provided detailed guidelines for exotic forms of APED use, some likely associated with serious health risks, which are probably unknown to most practicing clinicians.”
“Doping in Sport: A Review of Elite Athletes’ Attitudes, Beliefs and Knowledge” Morente-Sánchez, Jaime; Zabala, Mikel. Sports Medicine , March 2013. doi: 10.1007/s40279-013-0037-x.
Abstract: “Although most athletes acknowledge that doping is cheating, unhealthy and risky because of sanctions, its effectiveness is also widely recognized. There is a general belief about the inefficacy of anti-doping programmes, and athletes criticise the way tests are carried out. Most athletes consider the severity of punishment is appropriate or not severe enough. There are some differences between sports, as team-based sports and sports requiring motor skills could be less influenced by doping practices than individual self-paced sports. However, anti-doping controls are less exhaustive in team sports. The use of banned substance also differs according to the demand of the specific sport. Coaches appear to be the main influence and source of information for athletes, whereas doctors and other specialists do not seem to act as principal advisors. Athletes are becoming increasingly familiar with anti-doping rules, but there is still a lack of knowledge that should be remedied using appropriate educational programmes. There is also a lack of information on dietary supplements and the side effects of [performance-enhancing substances].”
“Age and Gender Specific Variations in Attitudes to Performance Enhancing Drugs and Methods” Singhammer, John. Sport Science Review , December 2012. doi: 10.2478/v10237-012-0017-3.
Abstract: “Using a population-based cross-sectional sample of 1,703 Danish men and women aged 15-60 years, the present study examined age and gender variation in attitudes to performance enhancing drugs and methods…. Overall, participants held negative attitudes to drugs and methods enhancing predominantly cognitive-abilities-enhancing performance drugs and to appearance-modifying methods, but were positive to drugs for restoring physical functioning conditions. However, attitudes varied nonlinearly across age. Lenient attitudes peaked at around age 25 and subsequently decreased. Lenient attitudes to use of drugs against common disorders decreased in a linear fashion. No gender differences were observed and attitude did not vary with level of education, self-reported health or weekly hours of physical activity.”
“Drugs, Sweat and Gears: An Organizational Analysis of Performance Enhancing Drug Use in the 2010 Tour De France” Palmer, Donald; Yenkey, Christopher. University of California, Davis; University of Chicago. March 2013.
Abstract: “This paper seeks a more comprehensive explanation of wrongdoing in organizations by theorizing two under-explored causes: the criticality of a person’s role in their organization’s strategy-based structure, and social ties to known deviants within their organization and industry. We investigate how these factors might have influenced wrongdoing in the context of professional cyclists’ use of banned performance enhancing drugs (PEDs) in advance of the 2010 Tour de France….. We find substantial support for our prediction that actors who are more critical to the organization’s strategy-based structure are more likely to engage in wrongdoing. Further, we find that while undifferentiated social ties to known wrongdoers did not increase the likelihood of wrongdoing, ties to unpunished offenders increased the probability of wrongdoing and ties to severely punished offenders decreased it. These effects were robust to consideration of other known causes of wrongdoing: weak governance regimes and permissive cultural contexts, performance strain, and individual propensities to engage in wrongdoing.”
“Elite Athletes’ Estimates of the Prevalence of Illicit Drug Use: Evidence for the False Consensus Effect” Dunn, Matthew; Thomas, Johanna O.; Swift, Wendy; Burns, Lucinda. Drug and Alcohol Review , January 2012, Vol. 31, Issue 1, 27-32. doi: 10.1111/j.1465-3362.2011.00307.x.
Abstract: “The false consensus effect (FCE) is the tendency for people to assume that others share their attitudes and behaviours to a greater extent than they actually do…. The FCE was investigated among 974 elite Australian athletes who were classified according to their drug use history. Participants tended to report that there was a higher prevalence of drug use among athletes in general compared with athletes in their sport, and these estimates appeared to be influenced by participants’ drug-use history. While overestimation of drug use by participants was not common, this overestimation also appeared to be influenced by athletes’ drug use history.”
“The Role of Sports Physicians in Doping: A Note on Incentives” Korn, Evelyn; Robeck, Volker. Philipps-Universitat, Marburg, March 2013.
Abstract: “How to ban the fraudulent use of performance-enhancing drugs is an issue in all professional — and increasingly in amateur — sports. The main effort in enforcing a ‘clean sport’ has concentrated on proving an abuse of performance-enhancing drugs and on imposing sanctions on teams and athletes. An investigation started by Freiburg university hospital against two of its employees who had been working as physicians for a professional cycling team has drawn attention to another group of actors: physicians. It reveals a multi-layered contractual relations between sports teams, physicians, hospitals, and sports associations that provided string incentives for the two doctors to support the use performance-enhancing drugs. This paper argues that these misled incentives are not singular but a structural part of modern sports caused by cross effects between the labor market for sports medicine specialists (especially if they are researchers) and for professional athletes.”
“Socio-economic Determinants of Adolescent Use of Performance Enhancing Drugs” Humphreys, Brad R.; Ruseski, Jane E. Journal of Socio-Economics , April 2011, Vol. 40, Issue 2, 208-216. doi: 10.1016/j.socec.2011.01.008.
Abstract: “Evidence indicates that adolescents (athletes and non-athletes use performance enhancing drugs. We posit that adolescent athletes have different socio-economic incentives to use steroids than non-athletes. We examine adolescent steroid use using data from the Youth Risk Behavior Surveillance System. Multi-sport upperclassmen and black males have a higher probability of steroid use. Steroid use is associated with motivations to change physical appearance and experimentation with illicit substances. These results suggest there are different socio-economic motivations for adolescent steroid use and that steroid use is an important component of overall adolescent drug use.”
Cognitive-enhancing drugs
“Randomized Response Estimates for the 12-Month Prevalence of Cognitive-Enhancing Drug Use in University Students” Dietz, Pavel; et al. Pharmacotherapy , January 2013, Vol. 33, Issue 1, 44-50. doi: 10.1002/phar.1166.
Results: “An anonymous, specialized questionnaire that used the randomized response technique was distributed to students at the beginning of classes and was collected afterward. From the responses, we calculated the prevalence of students taking drugs only to improve their cognitive performance and not to treat underlying mental disorders such as attention-deficit-hyperactivity disorder, depression, and sleep disorders. The estimated 12-month prevalence of using cognitive-enhancing drugs was 20%. Prevalence varied by sex (male 23.7%, female 17.0%), field of study (highest in students studying sports-related fields, 25.4%), and semester (first semester 24.3%, beyond first semester 16.7%).”
“The Diversion and Misuse of Pharmaceutical Stimulants: What Do We Know and Why Should We Care?” Kaye, Sharlene; Darke, Shane. Addiction , February 2012, Vol. 107, Issue 3, 467-477. doi: 10.1111/j.1360-0443.2011.03720.x.
Results: “The evidence to date suggests that the prevalence of diversion and misuse of pharmaceutical stimulants varies across adolescent and young adult student populations, but is higher than that among the general population, with the highest prevalence found among adults with attention deficit-hyperactive disorder (ADHD) and users of other illicit drugs. Concerns that these practices have become more prevalent as a result of increased prescribing are not supported by large-scale population surveys…. Despite recognition of the abuse liability of these medications, there is a paucity of data on the prevalence, patterns and harms of diversion and misuse among populations where problematic use and abuse may be most likely to occur (e.g. adolescents, young adults, illicit drug users). Comprehensive investigations of diversion and misuse among these populations should be a major research priority, as should the assessment of abuse and dependence criteria among those identified as regular users.”
“Adderall Abuse on College Campuses: A Comprehensive Literature Review” Varga, Matthew D. Journal of Evidence-Based Social Work , 2012, Vol. 9, Issue 3. doi: 10.1080/15433714.2010.525402.
Abstract: “Prescription stimulant abuse has dramatically increased over the past 10 years, but the amount of research regarding college students and illicit prescription stimulant use is still very limited. This has important implications for college mental health professionals and higher education administrators. In this comprehensive literature review the author explores factors contributing to illicit use, self-medication, and recreational use of controlled prescription stimulants; discusses the potential consequences for those students abusing stimulants; and provides recommendations for educating, combating, and assisting students who illicitly use prescription stimulants on college campuses.”
“A Comparison of Attitudes Toward Cognitive Enhancement and Legalized Doping in Sport in a Community Sample of Australian Adults” Partridge, Brad; Lucke, Jayne; Hall, Wayne. AJOB Primary Research , November 2012. doi: 10.1080/21507716.2012.720639.
Abstract: “This article compares public attitudes toward the use of prescription drugs for cognitive enhancement with the use of performance enhancing drugs in sport. We explore attitudes toward the acceptability of both practices; the extent to which familiarity with cognitive enhancement is related to its perceived acceptability; and relationships between the acceptability of cognitive enhancement and legalized doping in sport. Of 1,265 [survey] participants, 7% agreed that cognitive enhancement is acceptable; 2.4% of the total sample said they had taken prescription drugs to enhance their concentration or alertness in the absence of a diagnosed disorder, and a further 8% said they knew someone who had done so. These participants were twice as likely to think cognitive enhancement was acceptable. Only 3.6% of participants agreed that people who play professional sport should be allowed to use performance-enhancing drugs if they wanted to. Participants who found cognitive enhancement acceptable were 9.5 times more likely to agree with legalized doping.”
Keywords: drugs, youth, sports, cheating, higher education, corruption, ADHD, research roundup
About The Author

Leighton Walter Kille
Appointments at Mayo Clinic
Performance-enhancing drugs: know the risks.
Hoping to get an edge by taking performance-enhancing drugs? Learn how these drugs work and how they can have effects on your health.
Most serious athletes feel a strong drive to win. They often dream big too. Some athletes want to play for professional sports teams. Others want to win medals for their countries. The pressure to win leads some athletes to use drugs that might give them an edge. These are called performance-enhancing drugs. Use of these drugs is known as doping.
But doping comes with risks. Learn more about the effects that performance-enhancing drugs can have on health.
Anabolic steroids
What are they.
Anabolic steroids are drugs that athletes take to boost their strength and add muscle. These drugs also are called anabolic-androgenic steroids. They are made to work like a hormone that the body makes called testosterone.
Testosterone has two main effects on the body:
- Helps build muscle.
- Causes features such as facial hair and a deeper voice.
The anabolic steroids used by athletes are often forms of testosterone made in a lab.
Some people use anabolic steroids for medical reasons. But doping for sports isn't one of the uses the drugs are approved for.
What makes some athletes want to use anabolic steroids? These drugs might lower the damage that happens to muscles during a hard workout. That could help athletes bounce back faster from a workout. They might be able to exercise harder and more often. Some people also may like how their muscles look when they take these drugs.
More-dangerous types of anabolic steroids are called designer steroids. Some drug tests may not be able to spot them in a person's body. Anabolic steroids have no medical use that's approved by the government.
Many athletes take anabolic steroids at doses that are too high. These doses are much higher than those that health care providers use for medical reasons. Anabolic steroids have serious side effects too.
- See their breasts grow.
- Notice their testicles shrink.
- Not be able to get their partner pregnant.
- Learn from a health care provider that their prostate gland has gotten bigger.
- Get a deeper voice. Treatment may not be able to change it back.
- Notice that a part of their genitals called the clitoris has gotten bigger.
- Grow more body hair.
- Lose the hair on the head. Treatment might not be able to bring the hair back.
- Stop getting periods or get them much less often than they used to.
All people who use anabolic steroids might start to get:
- Severe acne.
- A higher risk of swollen or torn cords in the body called tendons, which attach muscle to bone.
- Liver tumors, or other changes to the liver.
- Higher levels of the "bad" cholesterol, called low-density lipoprotein (LDL) cholesterol.
- Lower levels of the "good" cholesterol, called high-density lipoprotein (HDL) cholesterol.
- High blood pressure.
- Problems with the heart and blood flow.
- Issues with anger or violence.
- Mental health conditions, such as depression.
- A need for anabolic steroids that can't be controlled.
- Diseases, such as HIV or hepatitis, if using needles to give shots of the drugs.
Teens who take anabolic steroids might grow less than usual too. They also might raise their risk of health problems later in life.
Doping with anabolic steroids is banned by most sports leagues and groups. And it is not legal. It's never safe to buy anabolic steroids from a drug dealer. The drugs could be tainted or labeled the wrong way.
Androstenedione
What is it.
Androstenedione, also called andro, is a hormone everyone's body makes. The body turns andro into the hormone testosterone and a form of the hormone estrogen.
Andro can be made in a lab. Some drugmakers and workout magazines claim that andro products help athletes train harder and recover faster. But some studies show that andro doesn't boost testosterone. They also show that muscles don't get stronger.
Andro is legal to use only if a health care provider prescribes it. It's not legal to use as a doping drug in the United States.
Side effects of andro in men include:
- Testicles that shrink or make less sperm.
- Breast growth.
Side effects in women include:
- Deeper voice.
- Loss of hair on the head.
Andro can damage the heart and blood vessels in anyone who takes it. This raises the risk of a serious problem that can happen when the heart doesn't get enough blood, called a heart attack. It also raises the risk of a condition that keeps the brain from getting enough oxygen, called a stroke. Heart attack and stroke can be deadly.
Human growth hormone
Athletes take human growth hormone, also called somatotropin, to build more muscle and do better at their sports. But studies don't clearly prove that human growth hormone boosts strength or helps people exercise longer.
A health care provider can prescribe human growth hormone for some health reasons. It is given as a shot.
Side effects linked to human growth hormone may include:
- Pain in joints, where two or more bones come together.
- Muscles that feel weak.
- A buildup of extra fluid in the body.
- A condition that affects how the body uses sugar for energy. This is called diabetes.
- Trouble seeing.
- A problem that can make the hand and the arm get weak, tingle or lose feeling. This is called carpal tunnel syndrome.
- Trouble controlling blood sugar.
- A heart that grows bigger than usual, called cardiomegaly.
Erythropoietin
Erythropoietin is a type of hormone. It treats anemia in people with severe kidney disease. It raises the level of red blood cells. It also raises the levels of the protein in red blood cells that carries oxygen to the body's organs, called hemoglobin.
Taking erythropoietin improves how oxygen moves to the muscles. It's common for athletes who exercise for long amounts of time to use a lab-made type of erythropoietin called epoetin.
In the 1990s, it was common for pro cyclists to use erythropoietin. But the drug may have played a role in at least 18 deaths. Doping with erythropoietin may raise the risk of serious health problems. These include stroke, heart attack and blocked arteries in the lung.
Diuretics are drugs that change the body's balance of fluids and salts. They can cause the body to lose water, which can lower an athlete's weight. Diuretics also may help athletes pass drug tests that check for signs of drugs in the urine. They dilute the urine and may hide traces of drugs.
Diuretics can cause side effects when you take them at any dose — even at doses that health care providers suggest. These drugs make athletes more likely to have side effects such as:
- Losing more fluids than you take in. This is a serious problem called dehydration.
- Squeezing pain in muscles called cramps.
- Feeling faint, woozy, weak or not steady.
- Being low on a mineral called potassium, which the body needs to work well.
- Having a drop in blood pressure.
- Feeling clumsy when you move and having trouble keeping your balance.
Diuretics can lead to death if an athlete uses them for doping.
Nutrients are vitamins and minerals in foods that are good for you. Some people try to get more nutrients from products called supplements. Supplements are sold in stores and online as powders or pills. One supplement that's popular with athletes is called creatine monohydrate.
The body makes its own creatine too. It helps muscles release energy. Creatine supplements may help athletes gain small, short-term bursts of power.
Creatine seems to help muscles make more of an energy source called adenosine triphosphate (ATP). ATP stores and moves energy in the body's cells. It's used for activity that involves quick bursts of movement, such as weightlifting or sprinting. But there's no proof that creatine helps you do better at sports that make you breathe at a higher rate and raise your heart rate, called aerobic sports.
Side effects of creatine can include gaining weight and cramps in the belly or muscles.
Some athletes try to gain weight so they can get bigger in size. Creatine may help you put on weight over time. But that might be due to the extra water that creatine causes the body to hold on to. Water is drawn into muscle tissue, away from other parts of the body. That puts you at risk of getting dehydrated.
Studies show that it's safe for healthy adults to use creatine for a short or long time. It's important to use the doses that creatine makers suggest on the package.
Stimulants boost the levels of some chemicals in the brain. They also make the heart beat faster and raise blood pressure.
Stimulants can help an athlete:
- Exercise longer.
- Feel less tired or hungry.
- Feel more alert and aggressive.
Common stimulants include caffeine and drugs called amphetamines. Cold medicines often have a stimulant in them.
Energy drinks are popular among many athletes. They often have high doses of caffeine and other stimulants. The street drugs cocaine and methamphetamine also are stimulants.
Stimulants have side effects that can make an athlete play worse, such as:
- Lowered focus due to feeling nervous or angry.
- Trouble sleeping.
- Dehydration.
- Heatstroke, which happens when the body gets too hot and can't cool down.
- Addiction to stimulants, or needing higher doses to feel the effects.
Other side effects include:
- A feeling that the heart is beating fast, fluttering or pounding.
- A heartbeat that is too fast, too slow or out of rhythm.
- Weight loss.
- A type of shaking called tremors.
- The sensation of seeing things that aren't there, called hallucination.
- Heart attack or other problems with blood flow.
The bottom line
Some athletes may seem to get an edge from performance-enhancing drugs. But doping can have bad effects on health.
In general, the long-term effects of performance-enhancing drugs haven't been studied enough. And any short-term perks come with risks. Doping is banned by most sports leagues and groups too.
That's why it's risky to use performance-enhancing drugs.
There is a problem with information submitted for this request. Review/update the information highlighted below and resubmit the form.
From Mayo Clinic to your inbox
Sign up for free and stay up to date on research advancements, health tips, current health topics, and expertise on managing health. Click here for an email preview.
Error Email field is required
Error Include a valid email address
To provide you with the most relevant and helpful information, and understand which information is beneficial, we may combine your email and website usage information with other information we have about you. If you are a Mayo Clinic patient, this could include protected health information. If we combine this information with your protected health information, we will treat all of that information as protected health information and will only use or disclose that information as set forth in our notice of privacy practices. You may opt-out of email communications at any time by clicking on the unsubscribe link in the e-mail.
Thank you for subscribing!
You'll soon start receiving the latest Mayo Clinic health information you requested in your inbox.
Sorry something went wrong with your subscription
Please, try again in a couple of minutes
- Madden CC, et al. Drugs and doping in athletes. In: Netter's Sports Medicine. 2nd ed. Philadelphia, Pa.: Elsevier; 2018. https://www.clinicalkey.com. Accessed Oct. 11, 2018.
- Snyder PJ. Use of androgens and other hormones by athletes. https://www.uptodate.com/contents/search. Accessed Oct. 11, 2018.
- Effects of performance-enhancing drugs. U.S. Anti-Doping Agency. https://www.usada.org/substances/effects-of-performance-enhancing-drugs/. Accessed Oct. 11, 2018.
- Santos GH, et al. The risk environment of anabolic-androgenic steroid users in the UK: Examining motivations, practices and accounts of use. International Journal of Drug Policy. 2017;40:35.
- Fleisher LA, et al., eds. Androstenedione. In: Essence of Anesthesia Practice. 4th ed. Philadelphia, Pa.: Elsevier; 2018. https://www.clinicalkey.com. Accessed Oct. 19, 2018.
- La Gerche A, et al. Drugs in sport — A change is needed, but what? Heart, Lung, and Circulation. 2018;27:1099.
- Boardley ID, et al. Nutritional, medicinal, and performance enhancing supplementation in dance. Performance Enhancement & Health. 2016;4:3.
- Baron D, et al. Prohibited non-hormonal performance-enhancing drugs in sport. https://www.uptodate.com/contents/search. Accessed Oct. 11, 2018.
- Robinson D. Permitted non-hormonal performance-enhancing substances. https://www.uptodate.com/contents/search. Accessed Oct. 11, 2018.
- Madden CC, et al. Sports supplements. In: Netter's Sports Medicine. 2nd ed. Philadelphia, Pa.: Elsevier; 2018. https://www.clinicalkey.com. Accessed Oct. 11, 2018.
- Hall M, et al. Creatine supplementation: An update. Current Sports Medicine Reports. 2021; doi:10.1249/JSR.0000000000000863.
Products and Services
- The Mayo Clinic Diet Online
- A Book: The Mayo Clinic Diet Bundle
- Eating and exercise
- Daily water requirement
Mayo Clinic does not endorse companies or products. Advertising revenue supports our not-for-profit mission.
- Opportunities
Mayo Clinic Press
Check out these best-sellers and special offers on books and newsletters from Mayo Clinic Press .
- Mayo Clinic on Incontinence - Mayo Clinic Press Mayo Clinic on Incontinence
- The Essential Diabetes Book - Mayo Clinic Press The Essential Diabetes Book
- Mayo Clinic on Hearing and Balance - Mayo Clinic Press Mayo Clinic on Hearing and Balance
- FREE Mayo Clinic Diet Assessment - Mayo Clinic Press FREE Mayo Clinic Diet Assessment
- Mayo Clinic Health Letter - FREE book - Mayo Clinic Press Mayo Clinic Health Letter - FREE book
- Healthy Lifestyle
- Performance enhancing drugs Know the risks
Your gift holds great power – donate today!
Make your tax-deductible gift and be a part of the cutting-edge research and care that's changing medicine.

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Pediatr Rev
Performance-Enhancing Drugs
Christopher dandoy.
* Pediatric Hematology/Oncology, Fellow, Cincinnati Children’s Hospital, Cincinnati, OH.
Rani S. Gereige
† Clinical Professor of Pediatrics–Florida International University, Miami Children’s Hospital, Miami, FL.
Educational Gap
Performance-enhancing drug (PED) use by children and teenagers rose sharply in the past decade. One study shows 3.3% of high school students admit anabolic steroid use; another finds 8% of girls and 12% of boys report using products to improve appearance, muscle mass, or strength. Pediatrics clinicians must monitor PED usage trends, screen perceptively, and offer anticipatory guidance.
After completing this article, readers should be able to:
- Recognize the signs and symptoms of the use of anabolic steroids and growth hormone.
- Know how to diagnose the use of anabolic steroids and growth hormone by data collection (history, physical examination, and laboratory evaluation).
- Know the side effects of anabolic steroids.
Introduction
The use of performance-enhancing drugs (PEDs) by preteenagers and teenagers has increased tremendously over the past decade. This trend is driven by multiple factors, including the decrease in the age of participation in competitive sports; the increase in popularity of team/competitive sports; the focus of the media on thinness in females and muscular bodies in males; pressure from parents and coaches; the age-related characteristics of taking risks and feeling invincible; and the availability of various PEDs in many forms and shapes.
The pediatric clinician must be aware of the use of performance-enhancing substances by pediatric patients; be prepared to identify risk factors, signs, and symptoms; ask screening questions; and offer anticipatory guidance related to their use. Table 1 lists the common classes of PEDs. This review will focus on a select group of commonly used PEDs. The reader should know that anabolic steroids are synthetic substances derived from testosterone and are also called anabolic-androgenic steroids (AASs) or just “steroids.” Steroid precursors also are used as performance-enhancing agents.
Classes of Commonly Used Performance-Enhancing Drugs
Epidemiology
Over the past 25 years, there has been an explosion in youth sports participation, resulting in a dramatic increase in the total number of athletes under age 18 years. It is estimated that more than 30 million children and adolescents are participating in organized sports today. Title IX, which was passed in 1972, promoted equal numbers of male and female college athletes and increased the number of female athletes. In 1972, there were ∼25,000 female high school athletes, in comparison to 3 million in 2000. ( 1 ) This number has been stable at 3 million in 2007, according to Title IX data.
With the increase in number of childhood athletes, the stress to perform at a high level has increased. Parents, coaches, and the players themselves are constantly pushing themselves to perform. This drive to be successful in athletic competition often is a positive one, resulting in increased self-confidence, a drive for hard work, and cooperation among peers. This drive, however, can turn negative when competition and winning is “at all costs.” When athletes lose sight of the meaning of fair competition by taking performance-enhancing substances, they put their future health at risk and compromise their ability to practice sportsmanship.
There are many historic examples of athletes over the last century who relied on PEDs to improve their performance. During the original Olympic Games, cash awards were given to the winners of the games. At that time, the use of performance-enhancers was widely accepted. Athletes would consume large amounts of meat and herbs with the belief that it would give them a competitive edge. They would also consume a type of opium juice called “doop”; this term was the origin of the word “doping.”( 2 )
Gladiators of Roman times used to ingest strychnine to avoid injury and to decrease fatigue. During the 1950s, the Soviet Union dominated power lifting by providing their wrestlers testosterone injections. In the 1960s, Sports Illustrated documented the use of amphetamines, tranquilizers, cocaine, and other drugs by professional athletes. ( 3 ) In 1988, Ben Johnson turned in a record-breaking performance in the 100-m dash but was stripped of his title after he tested positive for the anabolic steroid stanozol. ( 4 )
Recently, over concerns about the medical complications of performance-enhancing substances and the potential influence professional athletes have on children’s performance in sports and sports-related behavior, athletes are being monitored for use of substances that enhance performance. Despite this focus, athletes in baseball, cycling, football, and basketball continue to test positive for PEDs on a frequent basis.
Risk Factors
Specific factors place the adolescent at increased risk for use of performance-enhancing substances. Adolescents, by their nature, are particularly vulnerable to risk-taking behaviors and experimentation. Teenagers often feel invincible and lack insight into long-term complications. Among athletes who use PEDs, those who play football, baseball, and basketball, who wrestle, and who are involved in gymnastics and weight training are at increased risk. ( 5 )
Some adolescents not involved in sports use performance-enhancing substances. At risk are the teenagers who are preoccupied with appearance or are focused on weight building or performance in the gym. Project EAT-II, a longitudinal study in which the authors reviewed eating, activity, and weight in 2,500 adolescents over a 5-year period of time, revealed that 1.4% of girls and 1.7% of boys reported having used anabolic steroids in the past year. The two variables that were predictors of steroid use in males were (a) having an ideal body size that is larger than one’s current body size and (b) self-report of healthy weight control behaviors. In girls, the two predictors of steroid use were (a) low satisfaction with weight and (b) high BMI. ( 6 ) Other factors that have been predictors of steroid use in adolescents include peer pressure, media influence, and parental pressures with regard to weight and muscles. Adolescents with a history of depression, those who have a negative body image, and teenagers who have a tendency to compare their own bodies to those who are known users of steroids are at increased risk of using as well. ( 7 )( 8 )
The pediatrician who cares for adolescents also must consider the media and its effects on adolescents taking performance-enhancing substances. Field et al ( 9 ) found that 8% of girls and 12% of boys reported using some type of product to improve appearance, gain muscle mass, or improve strength. Adolescents who reported that they wanted an improved physical appearance were more likely to use performance-enhancing substances. Also, girls who wanted to lose weight were more likely to use some type of PED.
Studies have revealed that males who read men’s, teenager, fashion, or health and fitness magazines were twice as likely to use a performance-enhancing substance to improve strength. Females wanting to look more like women in the media were more likely to use products that enhance their physiques. Adolescents who lift weights or play football were more likely to use creatine, amino acids, dehydroepiandosterone (DHEA), growth hormone, or anabolic steroids.
Anabolic Agents
Anabolic-androgenic steroids, physiologic effects.
As mentioned, AASs are synthetic derivatives of testosterone that have been modified to maximize anabolic effects. These testosterone derivatives have several general effects: they promote an increased nitrogen concentration in muscle, which in turn promotes an anabolic state; the agents inhibit the binding of catabolic glucocorticoids to muscle, preserving muscle mass and prohibiting muscle breakdown; and AASs have an effect on aggression, promoting athletes to train and push themselves harder. When combined with strength training, AASs increase fat-free mass and muscle strength. Strength gains can be substantial, with increase of strength to 5% to 20%. Clinical trials testing aerobic activity have not demonstrated significant improvements. With use of anabolic steroids, muscle mass increases through muscle hypertrophy as well as an increased number of muscle fibers. ( 10 )( 11 )( 12 )( 13 )( 14 )
Prevalence of Use
The National Youth Risk Behavior Surveillance System, conducted every 2 years, surveys ∼16,500 9th- through 12th-graders in private and public schools regarding priority health-risk behaviors. In relation to steroid use, the survey asks if the teenager “ever took steroid pills or shots without a doctor’s prescription one or more time during their life.” The incidence from 1991 to 2003 grew from 2.7% to 6.1%. That number has revealed a decrease from its peak in 2003 to 3.3% in 2009. Boy respondents (4.4%) were more likely than girls (2.2%) to have used steroids at least once. Race was not a contributing factor to steroid use. ( 15 )
Monitoring the Future is a long-term study of adolescents and adults based at the University of Michigan Institute for Social Research. Each year, the survey investigates substance abuse and use in ∼50,000 8th-, 10th-, and 12th-grade students. In 2010, the survey revealed the annual male adolescent prevalence rates for steroid use of 0.7% for 8th-graders, 1.3% for 10th-graders, and 2.5% for 12th-graders. The annual female adolescent prevalence is 0.3% in 8th-graders, 0.5% in 10th-graders, and 0.3% for 12th-graders.
Since 1993, perceived risk and disapproval were asked of the adolescents. Between 1998 and 2000, there was a sharp decline in perceived risk of steroid use. This decline could be related to the use of performance-enhancing substances by professional athletes. There has been a small rise in perceived risk of steroid use; however, the perceived risk still remains at 59%. Fewer adolescents perceive steroids as “fairly easy or very easy” to get since 2003. Finally, more adolescents disapprove of steroid use since 2003 as well. ( 16 )
Administration
Steroids can be injected, taken orally, or absorbed transdermally. Injectable forms of steroids are more potent and last longer. Oral anabolic steroids are converted in the liver into active testosterone. Anabolic steroids often are “stacked,” which means taking multiple steroids at the same time, and taken in 4- to 12-week cycles. The doses often are in a “pyramid” sequence with the largest dose at the middle of the cycle. The doses often are 50 to 100 times what would be needed to maintain the normal physiologic level of testosterone. A large market has developed creating “designer steroids” that are modified to evade detection.
Testing for exogenous testosterone can be accomplished by determining the urinary ratio of testosterone glucuronide to epitestosterone glucuronide. The ratio is normally 1–3:1. When someone is taking anabolic steroids, endogenous testosterone glucuronide and epitestosterone glucuronide are suppressed, leaving just the exogenous testosterone. A testosterone to epitestosterone ration of more than 4:1 is considered positive. Another way to monitor for exogenous testosterone is to obtain urine testosterone and luteinizing hormone. Because exogenous testosterone suppresses luteinizing hormone, this ratio is high (more than 30) in those taking anabolic steroids. ( 17 )
Adverse Effects
There are many adverse effects of anabolic steroids, and some can be serious and lifelong. These symptoms are prominent with the use of AASs as well as steroid precursors. Table 2 highlights the major adverse effects.
Adverse Effects of Androgenic-Anabolic Steroids and Steroid Precursors
The Anabolic Steroid Control Act of 1990 made AAS a schedule III controlled substance. The Anti-Drug Abuse Act of 1988 made AAS illegal to use for anything other than disease treatment.
Steroid Precursors
Anabolic steroid precursors or prohormones have gained popularity as PEDs in the past 15 years. These substances were first marketed and sold over the counter, promoting increased endogenous testosterone and thus promoting lean body mass. In the late 1990s and early part of this past decade, there was an explosion of the use of steroid precursors. These steroid precursors include, but are not limited to, the following: androstenedione (also known as “andro”), androstenediol, norandrostenedione, norandrostenediol, and DHEA. ( 18 )
Most androgenic steroids in humans are derived from DHEA, which is secreted from the adrenal cortex. DHEA is converted to androstenedione and androstenediol, which is then converted to testosterone. Steroid precursors were produced and distributed in hopes that these substances would increase free testosterone. The effects that are hoped for are often not seen because these precursors bind poorly to androgen receptors. Multiple studies have been done with steroid precursors; most of them have revealed increases in androstenedione and estradiol but little to no increase in serum testosterone. There have been no studies revealing increased muscle mass or improved athletic performance. ( 19 )
Although these steroids have minimal desired effects, they still have many of the negative effects of anabolic steroids ( Table 2 ). In female athletes, these substances have an androgenizing influence, including general virilization and male pattern baldness. Males can experience gynecomastia, acne, and testicular atrophy. In both genders, decreased high-density lipoproteins, increased lipids, and stunted growth can result. Finally, these substances can downregulate endogenous testosterone over time. ( 20 )( 21 )
In 2005, androstenedione was classified as a schedule III controlled substance. DHEA continues to remain an over-the-counter nutritional supplement. Unfortunately, the Dietary Supplement Health and Education Act of 1994 allows many steroid precursors to be sold over the counter with minimal regulation.
Nutritional Supplements
Nutritional supplements have become increasingly popular among adolescents in the past 18 years. In 1993, the Proxmire Amendment limited jurisdiction of the Food and Drug Administration over nutritional supplements. This decision severely limited federal regulation. From that point forward, there was a market explosion. Dietary supplements can be found in health food stores, supermarkets, and even the corner gas station. The easy availability and advertising campaigns directed at young athletes have lead to a high rate of use among adolescents.
There are hundreds of nutritional supplements and more are being produced each year. These products undergo little human testing and no testing in children and adolescents, which can be potentially dangerous. ( 22 ) Currently, most nutritional supplements are not recommended for consumption by those under age 18 years.
Creatine is the most popular nutritional supplement, accounting for $400 million in sales annually. Despite recommendations against creatine use in adolescents under age 18 years, its use is still common. In 2001, Metzl et al ( 23 ) questioned 1,103 adolescents and found creatine use in 5.6% of them. Those that used creatine were in each grade level from 6th to 12th, and improved sports performance was cited as the goal in 75% of these cases.
Creatine is a nonessential amino acid that is made in the liver, pancreas, and kidneys and helps create adenosine triphosphate. Creatine can be found in meat, milk, and fish among other foods, and the total daily requirement is 2 g per day. Often, athletes use two to three times this amount when using creatine for improved sports performance.
Creatine has been shown to improve performance in short, high intensity exercises, including weight lifting. There are smaller benefits found in performances of longer duration. Creatine-related adverse effects include weight gain, water retention, gastrointestinal cramping, fatigue, and diarrhea. ( 12 )
Human Growth Hormone
Human growth hormone (hGH) is an endogenous hormone produced in the pituitary gland. In children and adults, the main reason hGH is given is to treat growth hormone deficiency and short stature in order to increase linear growth. However, hGH has been used by sports competitors for performance-enhancement since the 1970s. Recently, the use of hGH by professional athletes has received attention in the media from players in the National Football League to Major League Baseball. The reason this drug has been popular among athletes is because it is difficult to detect.
Studies evaluating growth hormone in healthy individuals reveal that endogenous growth hormone does increase lean body mass and decreases fat mass. However, growth hormone has little effect on strength and athletic performance and might worsen exercise capacity by increasing exercise-induced lactate levels. ( 24 ) Adverse effects such as diabetes, cardiomyopathy, hepatitis, and renal failure have occurred with the use of high-dose growth hormone. Also, participants in studies evaluating the effects of growth hormone often complained of soft tissue edema, joint pain, carpal tunnel syndrome, and increased fatigue. ( 25 )
Currently, hGH is on the World Anti-Doping Agency banned substance list. Blood tests currently exist for its detection; however, there is only a small window of opportunity for its detection. Currently, there are two methods of detection in the blood. The “markers” method looks for alterations in the ratios of serum proteins that exogenous hGH would alter. The “isoform” method looks for alterations in the growth hormone structure. ( 26 )
Erythropoietin
Erythropoietin (EPO) has gained notoriety recently as a PED used by cyclists and endurance athletes. EPO administration leads to increased production of red blood cells, which in turns leads to increased oxygen delivery to muscles. Unfortunately, this rise in hematocrit can create complications, including dehydration and increased viscosity and sluggishness of blood, which can lead to stroke and pulmonary emboli. Detection of EPO can be done through urine sample electrophoresis. ( 27 )( 28 )
Stimulants such as ephedrine and caffeine are used by adolescent athletes for their ergogenic effects. ( 29 ) Stimulants are an attractive ergogenic option because they are widely available, easily accessible, and difficult to detect. Stimulants reduce the perception of fatigue and increase time to exhaustion. They improve alertness, as well as neurocognitive and aerobic performance.
Ephedrine is available in cough and cold remedies over the counter. Ephedra was banned by the Food and Drug Administration in 2004 due to its numerous adverse effects, such as hypertension, weight loss, insomnia, anxiety, tremors, headaches, arrhythmias, strokes, and psychosis. The drug has been implicated in several deaths in athletes. Since its ban, ephedra was replaced by other sympathomimetics that have similar effects.
Caffeine is used in beverages, soft drinks, and pill forms. Guarana is a plant extract sold in drinks and energy shots. Guarana seeds contain 9,100 to 76,000 ppm of caffeine. Caffeine use for performance-enhancement has been reported in 27% of adolescent athletes in the United States. Caffeine produces ergogenic effects at a dose as low as 250 mg (3.0–3.5 mg/kg). Caffeine does not seem to be useful for sprints or short bursts of activity but may be effective for prolonged sports containing short bursts, such as tennis and team sports.
General Approach
The general approach to dealing with PED use in the young athlete is similar to the approach to any other type of substance abuse. In fact, PEDs have been considered gateway drugs because teenagers and preteenagers who engage in the use of PEDs, marketed legally or illegally, are more likely to exhibit risk-taking behavior in other ways and to engage in the use of other substances of abuse (opioids, narcotics, and cocaine, etc). The clinician should maintain a high degree of suspicion and look for “red flags” in the history and physical examination.
The psychosocial history should include, in addition to inquiring about the use of alcohol, smoking, and drugs, asking about the use of PEDs in all shapes and forms, including nutritional supplements. The clinician should inquire about sources of PEDs, motives behind their use, the patient’s understanding of the effects and adverse effects of the PEDs being used, and the use of PEDs by peers, which is a strong predictor of use. It is important to remember that not all PED users are involved in athletic activities and the motive might be to enhance looks.
Physical Examination
The clinician must look for red flags on physical examination that might point to the effects and adverse effects of PEDs. Sudden increases in muscle mass and lean weight over a short period of time, facial and body acne at a time that is asynchronous with when acne is expected to develop in a teenager, stretch marks, even mood changes and anger outbursts in boys and signs of virilization in girls, all raise suspicion for AAS use. Coarse features and rapid growth suggest hGH use.
Anticipatory Guidance and the Role of the Clinician
The clinician must include questions about the use of PEDs in the psychosocial history on all youth, regardless of their involvement in sports. Education and discussion should begin early (elementary school) before the youth becomes a user. The following are a few tips for the clinician to address PED use in teenagers and preteenagers:
- Maintain an opened dialogue
- Understand the motive behind the use of PEDs
- Educate the athlete against the use of banned/illegal ergogenics
- Tell the youth what is known and not known about these substances
- Discuss the adverse effects and dangers
- Be aware that drug testing has not proven to be a deterrent alone
- Promote balanced meals, good nutrition, and training
- Discuss safe alternatives
- Know that occasionally, tests that reveal a low sperm count in AAS users can motivate the user to stop using AASs
- Clinicians should screen for anabolic steroid use because there is evidence that, based on results of the National Youth Risk Behavior Surveillance System, 3.3% of 9th- to 12th-graders admit to using steroids in the past. ( 15 )
- It is an established fact that adolescents are vulnerable to risk-taking behaviors and experimentation, feel invincible, and lack insight into long-term complications. ( 2 )
- Based on epidemiologic data, among all athletes who use performance-enhancing drugs, athletes who play football, wrestle, are involved in gymnastics, play baseball and basketball, and participate in weight training are at increased risk of use. ( 15 )( 23 )
- Based on strong evidence, the predictors of steroid use in boys are desire for an ideal body size that is larger than one’s current body size and self-report of healthy weight control behaviors, whereas in girls, predictors of steroid use are low satisfaction of weight and high BMI. ( 3 )
- Strong evidence suggests that risk factors for steroid use include: peer pressure, media exposure, parental pressure, a history of depression, a negative body image, and a tendency to compare one’s own body with those who are known users of steroids. ( 3 )( 4 )( 5 )( 15 )
Author Disclosure
Drs Dandoy and Gereige have disclosed no financial relationships relevant to this article. This commentary does contain a discussion of an unapproved/investigative use of a commercial product/device.
Suggested Reading
- Gomez J; American Academy of Pediatrics Committee on Sports Medicine and Fitness. Use of performance-enhancing substances . Pediatrics . 2005; 115 ( 4 ):1103–1106 [ PubMed ] [ Google Scholar ]
- Calfee R, Fadale P. Popular ergogenic drugs and supplements in young athletes . Pediatrics . 2006; 117 ( 3 ):e577–e589 [ PubMed ] [ Google Scholar ]
- Metzl JD. Performance-enhancing drug use in the young athlete . Pediatr Ann . 2002; 31 ( 1 ):27–32 [ PubMed ] [ Google Scholar ]

TOBIE SMITH, MD, MPH, Georgetown University Medical Center, Washington, District of Columbia
MATTHEW FEDORUK, PhD, AND AMY EICHNER, PhD, U.S. Anti-Doping Agency, Colorado Springs, Colorado
Am Fam Physician. 2021;103(4):203-204
Author disclosure: No relevant financial affiliations.
Family physicians may be surprised to learn the number of their patients who use performance-enhancing drugs, either deliberately to improve athletic performance or unknowingly through contaminated dietary supplements. Elite athletes account for only a small fraction of the approximately 3 million users of ergogenic drugs in the United States. 1 Sports organizations have broadened their efforts to detect and deter doping (i.e., the use of performance-enhancing drugs in competitive sports) at all levels of competition, resulting in a surprising number of positive doping test results in masters and recreational level athletes. 2 Recreational athletes who have been caught intentionally doping have reported many reasons for doing so, including keeping up with others in their age group in training and competition and for faster recovery from training and competitions so that they can continue to compete at a maximal level. 2 – 4
The prevalence of performance-enhancing drug use among athletes and the general public has led the World Health Organization to recognize the use of these drugs as a public health issue. 3 Over the past decade, the emergence of novel doping agents (particularly drugs aimed at boosting endogenous hormone levels and anabolic agents), increased acceptance of complementary and lifestyle medications, and increased contamination of dietary supplements have contributed to this growing public health concern.
The physical and psychological adverse effects of anabolic androgenic steroids (e.g., kidney and liver damage, acne, gynecomastia, suppression of normal testosterone production, aggression, depression) are well established. What physicians may not recognize are the potential adverse effects of novel, investigational drugs that are being used as doping agents. These include selective androgen receptor modulators (e.g., the investigational drugs ostarine [Enobosarm] and LGD-4033 [Ligandrol]), which have substantial anabolic effects on muscle and bone and significant potential for misuse in sports. These modulators are not approved for human use, and the adverse effects have not been well documented because they are still in clinical trials. Despite their experimental status, selective androgen receptor modulators have been found in dozens of dietary supplements and have caused more than 250 positive doping test results since 2010. 5 – 7 Growth hormone (GH) fragments (e.g., AOD-9604) and GH-releasing peptides, GH secretagogues (e.g., ibutamoren), metabolic modulators (e.g., meldonium), off-market drugs (e.g., sibutramine [Meridia]), and a handful of illegal designer stimulants (e.g., higenamine, 8 methylhexanamine, 9 octodrine 10 ) and other small molecules have also emerged on the doping stage. Consumers can easily buy all of these on the internet.
Even for the astute family physician, it can be difficult to identify patients who are using performance-enhancing drugs. Patients taking dietary supplements may be unintentionally ingesting performance-enhancing drugs because of contamination, and patients commonly do not disclose use of dietary supplements to their physicians. 11 Patients are less likely to disclose supplement use if the physician does not ask about it or if they believe that their physician is not knowledgeable about supplements. 11 Despite anti-doping agencies' warnings to elite athletes about supplement contamination risks, nonelite athletes are rarely educated about these risks.
Patients who are deliberately using performance-enhancing drugs may not disclose use because of shame, legality concerns, or lack of trust. In fact, users of performance-enhancing drugs often are not candid with their physicians about their use of these drugs. In one study, 56% of anabolic steroid users reported that they had never disclosed their use to their physician. 7 The adverse effects of many of the novel performance-enhancing drugs are not well documented or understood and thus may not trigger red flag findings on clinical history and physical examination that would alert a family physician to potential users of these drugs.
Patronage of wellness and antiaging clinics may also put recreational athletes at risk of inadvertent positive doping test results because treatments prescribed at these centers often include hormone replacement. Athletes can apply for a therapeutic use exemption for certain prescribed medications that are prohibited in competition (i.e., beta 2 agonists for asthma, glucocorticoids for inflammatory diseases, hormones for endocrine deficiencies); no exemptions are typically given for medications prescribed solely for symptom relief, antiaging purposes, or other purported health and wellness benefits (i.e., testosterone to treat “low” testosterone levels or nonspecific symptoms).
The family physician is a critical player in addressing the use of performance-enhancing drugs in recreational athletes of all ages. Family physicians should continue to be alert to signs of use of traditional performance-enhancing drugs, such as anabolic-androgenic steroids and stimulants, and also be aware of the emergence and accessibility of novel doping agents. In addition to the potential health risks of the performance-enhancing drug itself, harms of a positive doping test result can include the negative health and social impacts of sanctions prohibiting participation and the potential emotional damage related to being labeled a cheater.
Physicians should be aware of the competition status of athletic patients and consult the appropriate banned substances list (e.g., the World Anti-Doping Agency prohibited list) before prescribing medication and also understand the therapeutic use exemption process ( Table 1 ) . Family physicians should also be aware of the emergence of novel performance-enhancing drugs and their use among the general population; screen patients for use; and be prepared to discuss the safety, effectiveness, legality, and ethics of performance-enhancing drug use. 12
Pope HG, Kanayama G, Athey A, et al. The lifetime prevalence of anabolic-androgenic steroid use and dependence in Americans: current best estimates. Am J Addict. 2014;23(4):371-377.
Henning AD, Dimeo P. The complexities of anti-doping violations: a case study of sanctioned cases in all performance levels of USA cycling. Perform Enhanc Health. 2014;3(3–4):159-166.
Dreier F. Wider testing reveals doping among amateur cyclists, too. July 27, 2012. Accessed November 2, 2020. https://www.nytimes.com/2012/07/28/sports/cycling/doping-in-cycling-reaches-into-amateur-ranks.html
Henning AD, Dimeo P. The new front in the war on doping: amateur athletes. Int J Drug Policy. 2018;51:128-136.
Van Wagoner RM, Eichner A, Bhasin S, et al. Chemical composition and labeling of substances marketed as selective androgen receptor modulators and sold via the internet [published correction appears in JAMA . 2018; 319(7):724]. JAMA. 2017;318(20):2004-2010.
U.S. Anti-Doping Agency. Supplement 411: realize, recognize, reduce. High-risk supplement list; 2019. Accessed April 24, 2020. https://www.supplement411.org
World Anti-Doping Agency. Anti-doping testing figures report. December 20, 2019. Accessed April 24, 2020. https://www.wada-ama.org/en/resources/laboratories/anti-doping-testing-figures-report
Cohen PA, Travis JC, Keizers PHJ, et al. The stimulant higenamine in weight loss and sports supplements. Clin Toxicol (Phila). 2019;57(2):125-130.
Eliason MJ, Eichner A, Cancio A, et al. Case reports: death of active duty soldiers following ingestion of dietary supplements containing 1,3-dimethylamylamine (DMAA). Mil Med. 2012;177(12):1455-1459.
Cohen PA, Travis JC, Keizers PHJ, et al. Four experimental stimulants found in sports and weight loss supplements: 2-amino-6-methylheptane (octodrine), 1,4-dimethylamylamine (1,4-DMAA), 1,3-dimethylamylamine (1,3-DMAA) and 1,3-dimethylbutylamine (1,3-DMBA). Clin Toxicol (Phila). 2018;56(6):421-426.
Guzman JR, Paterniti DA, Liu Y, et al. Factors related to disclosure and nondisclosure of dietary supplements in primary care, integrative medicine, and naturopathic medicine. J Fam Med Dis Prev. 2019;5(4) ):10.23937/2469-5793/1510109.
Jenkinson DM, Harbert AJ. Supplements and sports. Am Fam Physician. 2008;78(9):1039-1046. Accessed November 2, 2020. https://www.aafp.org/afp/2008/1101/p1039.html
Continue Reading

More in AFP
More in pubmed.
Copyright © 2021 by the American Academy of Family Physicians.
This content is owned by the AAFP. A person viewing it online may make one printout of the material and may use that printout only for his or her personal, non-commercial reference. This material may not otherwise be downloaded, copied, printed, stored, transmitted or reproduced in any medium, whether now known or later invented, except as authorized in writing by the AAFP. See permissions for copyright questions and/or permission requests.
Copyright © 2024 American Academy of Family Physicians. All Rights Reserved.
Drugs in sports Essay
Introduction, drugs should be used in sports, drugs should not be allowed in sports.
Drug use in sports has gained momentum in the recent past. The drug is used for performance enhancing (Coe, p. 224). Different sports have set up laws that are used to curb drug doping. Sports personalities use drugs to gain an advantage over the others. Performance enhancing drugs have been used in the Olympics by different people. For example, Thomas Hicks won the marathon after using strychnine.
However, the use of stimulating substances was banned in 1928 by the International Amateur Athletic Federation (Hartgens, p. 513). Although the ban was instituted a long time ago, athletes still use drugs to enhance performance. In 1976, East Germany nearly won all the swimming gold medals after the players were given steroids (Longman, p. 124). There is a debate about whether to allow drugs to be used in sports or impose a total ban.
The proponents of this debate argue that drug use alone does not guarantee success in the field. A magnificent performance is a combination of proper nutrition and practice. However, this is not true because some drugs enhance the performance of an individual. Drug usage in sports should be banned because of its effects. These effects include; it provides an avenue for some athletes to cheat, it compromises the credibility and integrity of the results and it is illegal (Coe, p. 224).
A drug is a natural substance that is taken to alter the general body functions (Wilson, p. 180). Drugs are used for several purposes. The nature in which a drug is used depends on the purpose of the drug. It can be used for; curative, stimulating, performance enhancing or as food. People consider any substance to be a drug based on the existing culture or legislature. Some traditions consider some drugs as food.
Laws have been established about drugs based on the effects of the drug in the body. It is illegal to use a drug that has been prohibited by a government or any organization.
However, some drugs have been prohibited but can be used in the treatment of patients. Additionally, some drugs can be taken without the knowledge of an individual. In such a case, the drug is found in a substance that is taken as food. Using drugs to boost performance should be banned because it makes the sport lose its original intended meaning and it also causes several environmental and health problems (Hartgens, p. 513).
Performance enhancing drugs should be allowed to be used in sports. Drugs that enhance performance satisfy the expectation of spectators watching games. People expect to watch a unique ability in the sports personality. This is made possible through the use of drugs because it gives an athlete the ability to demonstrate sports creativity.
Many fans watch athletes with the expectation to watch unique traits in the athletes (Wannamethee, p. 163). This makes the sport to become interesting. It is difficult to display a unique trait that is different from the human traits without the influence of performance enhancing drugs (Longman, p. 124).
The major expectation of the fans is players to demonstrate creativity during the game. Therefore, many people consider a competition to be fair if all the players are allowed to use the drug. Here, all the players will have the same effect of the drug and the best will come out based on his creativity. It is upon the players to manipulate the drug through excellent training to obtain the best results (Wannamethee, p. 163).
Technology has been introduced into sports. All people around the globe are comfortable with the use of technology in sports and disregard drugs. Technology is a result of creativity in the sports. Since the genetic make up of athletes is the same, drugs would not provide an advantage over other players (Warburton, p. 78).
Performance enhancing drugs have been used in other aspects of the human life. For example, many classical musicians use drugs to enhance their performance on stage. An excellent classical presentation requires a proper control of the pulse rate and blood pressure (Russell, p. 442).
The musicians use the beta blockers to enhance the stage performance. A low pulse rate and blood pressure contributed by the beta blockers reduces the effects of stress and this gives the musician confidence to exhibit a sterling performance (Brantigan, p. 90). An outstanding stage performance is the expectation of the classical music fans. Using drugs to enhance a stage performance does not give the musician an advantage over others. It depends on the human creativity and practice (Brantigan, p. 90).
Drugs should not be allowed in sports because it provides an avenue for some athletes to cheat (Haugen, p. 67). The doping process for athletes is not accurate. This gives some athletes who use the drugs an added advantage over those who do not use the drugs (Haugen, p. 67). The doping process is not used in all games. Therefore, there is no level playing field for the players.
Consequently, a total ban on the use of drugs to enhance performance should be instituted to ensure that all the players have been given a level playing field. Players who use drugs and win competitions are not the genuine winners. Although other people argue that a level usage of drugs will make the players level in the field, the actual performance in the field does not reflect the potential of the player. A total ban on drugs in all sports gives a level playing field that reflects the exact potential of the players (Longman, p. 124).
Additionally, different players from different countries have varying abilities to access the drugs. Therefore, if the drugs should be allowed, athletes from developing countries will not access the best drugs. The only way to have a level playing field for all players is through a total ban on the drugs in sports.
Integrity in sports is the driving force behind the sports events. Using drugs by a section of players compromises the credibility and integrity of the results (Wilson, p. 214). To maintain credibility and integrity, drugs should be banned. Other players win after using drugs that have been prohibited. Here, the integrity of the results is compromised.
The results obtained as a result of using prohibited drugs are illegitimate (Warburton, p. 78). Also, they lack authenticity. The spirit of any competition is to allow for a level playing where every player is given an opportunity to express his ability. A winner in such a competition is accepted by all the fans around the globe. When a winner is declared after using drugs, the value of the sport is reduced.
Therefore, the value of the sport remains a major issue in any sport or competition. Additionally, good personalities are expected to be role models (Browne, p. 497). Using drugs is prohibited and illegal. Allowing athletes to use drugs is itself an act of breaking the law. Good role models should obtain success through hard work and determination as opposed to using drugs (Browne, p. 497).
In conclusion, drug use in sports should be based on the purpose of the drug. When the drug is used to enhance creativity, then it makes the sport interesting. However, these give the athletes a competitive advantage over the others. As such, the natural ability of the athletes is not properly rewarded.
Although drugs make sports interesting, it makes the sport’s lack integrity. Additionally, drugs make the results of a competition to lack integrity and lose value. Additionally, different players from different countries have varying abilities to access the drugs. Therefore, if the drugs should be allowed, athletes from developing countries will not access the best drugs. The only way to have a level playing field for all players is through a total ban on the drugs in sports. The best way to ban using drugs is through a global organization.
This institution should be equipped with excellent doping mechanisms to ensure that all the players are screened properly before participating in a competition. In addition, drug use in sports should be banned because of it adds a competitive advantage, and causes severe effects to the users. These effects include; it provides an avenue for some athletes to cheat, it compromises the credibility and integrity of the results and it is illegal.
Brantigan, C 2005, ‘Effect of beta blockade and beta stimulation on stage fright’, American Journal of Medicine, vol. 5. no. 72, pp. 88–94.
Browne, A 2009, ‘The ethics of blood testing as an element of doping control in sport’, Journal of Medical Science Sports, vol. 3. no. 31, pp. 497–501.
Coe, s 2004, ‘We cannot move from strict liability rule’, The Daily Telegraph, 25 Feb, p.21.
Hartgens, F 2004, ‘Effects of androgenic-anabolic steroids in athletes’, Sports Medical Journal, vol. 9. no. 34, pp. 513–554.
Haugen, K 2004, ‘The performance-enhancing drug game’, Journal of Sports Economics , vol. 4. no. 5, pp. 67–87.
Longman, J 2004, East German steroids’ toll: ‘they killed Heid , Oxford University Press, New York.
Russell, G 2002, ‘Effects of prolonged low doses of recombinant human erythropoietin during sub maximal and maximal exercise’, European Journal Applied Physiology , vol. 30. no. 86, pp. 442–449.
Wannamethee, G 2004, ‘Haematocrit, hypertension and risk of stroke’, J Intern Med, vol. 23. no. 235, pp. 163–168.
Warburton, C 2007, The Economic results of prohibition, Columbia University Press, New York.
Wilson, B 2004, Hall overcomes cancer, then red tape to reach Olympics , Associated Press, London.
- Chicago (A-D)
- Chicago (N-B)
IvyPanda. (2019, November 29). Drugs in sports. https://ivypanda.com/essays/drugs-in-sports/
"Drugs in sports." IvyPanda , 29 Nov. 2019, ivypanda.com/essays/drugs-in-sports/.
IvyPanda . (2019) 'Drugs in sports'. 29 November.
IvyPanda . 2019. "Drugs in sports." November 29, 2019. https://ivypanda.com/essays/drugs-in-sports/.
1. IvyPanda . "Drugs in sports." November 29, 2019. https://ivypanda.com/essays/drugs-in-sports/.
Bibliography
IvyPanda . "Drugs in sports." November 29, 2019. https://ivypanda.com/essays/drugs-in-sports/.
- Geert Leinders's Lifetime Ban for Doping Violations
- Doping in Sports and Related Concerns
- Doping in Sport: Bad or Good?
- The World Anti-Doping Agency
- Study by Kirby, Moran and Guerin on athletes using doping
- Sports: Discrimination, Match-Fixing and Doping
- The Urgent Problem of Doping in Youth Sports: Solutions and Impact
- Performance-Enhancing Drugs and Substances Use in Sports
- Drugs and Dopping Issues in Sports
- The Doping Scandal Documentary Analysis
- Sports and Steroids: Society’s Acceptance or Rejection of Steroids in Sports
- Violence in Sports: When Life Is Dangerously Threatened
- Random Drug Testing for Collage Athletes
- Use of Performance Enhancing Drugs
- Should We Have Mandatory Drug Testing For Professional Athletes?

Pushbikewriter
Riding through the past, present and future of cycling
How to argue about doping in sport
Associate Professor, Centre for Cultural Diversity and Wellbeing, Victoria University
Disclosure statement
Craig Fry has received funding from the NHMRC, ARC, and Victoria University. He leads the Culture and Values in Health research program at the Centre for Cultural Diversity and Wellbeing, Victoria University. He is a Research Associate of the Institute of Sport, Exercise and Active Living, Victoria University. Craig also writes cycling history articles in an unpaid capacity for Cycling Tips.
Victoria University provides funding as a member of The Conversation AU.
View all partners

There has been a huge amount of academic, policy, and public debate over the years about doping in sport (i.e. the use of banned performance enhancing substances or drugs and other prohibited practices), and significant resources devoted to addressing it.
Doping is a complex issue – we are still striving to understand how and why it happens, and how to prevent it. But despite the attention doping in sport has received, there is still significant public disagreement about how best to respond to this problem.
Public discussions on doping usually break down - sometimes because of the way we argue about such issues, and often due to inconsistent reasoning. If you want evidence of this take a look at the online comments pages on sports doping articles, or start your own debate with friends and see how far it goes.
Greater clarity is needed on how people think and argue about doping in sport. In this piece I look at the common positions people take on doping, what these commit us to, and the consequences of mixed messages going unchallenged.
Why people dope
Assuming you care about doping in the first place (some people don’t), a key issue to clarify is your theory about why people dope. Your position here is important for discussing the doping issue because, whether you realise it or not, this informs your views on what should be done about it.
Some people believe the doping decision simply comes down to the individual’s desire to win or gain advantages of some type. To them, doping is mostly determined by individual psychological factors , and should therefore be addressed as an issue of personal responsibility and culpability.
Others believe doping choices are driven by a mix of psychological, social, cultural, and systemic factors , rather than individual traits alone. In this view, doping occurs due to the interaction of individual factors (e.g. the desire for winning, improvement, pain management, recovery, career longevity, economic gains, and belonging), and wider socio-cultural and systemic factors (e.g. social background and experiences, team/club/sport culture, sport governance systems, perceived efficacy of anti-doping system, and so on).

Against doping in sport
The question of whether you are for or against doping in sport is also clearly important. If you are against doping in sport, as most people are, there are a number of arguments you might run here.
For example, you may think doping is wrong because:
- It is against the defined rules and laws governing sport.
- It is unfair and goes against the level playing field ideal.
- It represents a health risk and is harmful to the individual.
- It harms the athletes who choose not to dope (e.g. they exit sport early, or their career is impacted from being cheated out of results and earnings).
- It contravenes other values defined as the ‘spirit of sport’ (e.g. fair play and honesty; health; character and education; fun and joy; teamwork; respect for self and others; courage; community and solidarity).
- It sends an unacceptable message about the place and impact of sport in society.
The important thing to note here is that anti-doping advocates vary in their relative emphasis on the above arguments. For some, it is all about the rules of sport, and related ethics and integrity requirements. While for others, the health risk and harm issue is paramount.
For doping in sport
Some people in academic circles argue that doping should be permitted in sport – either in an open free for all as it used to be, under medical supervision, or under the framework of regulated decriminalisation.
The proponents of these more liberal positions on doping commonly argue the following:
- The level playing field ideal is a myth - there are numerous legal performance enhancing strategies that are unequally available across sports and countries (e.g. expensive training facilities and programs, technologically superior equipment, nutritional, medicinal and other aids etc).
- Current banned drugs and substances are not inherently harmful, nor the biggest sources of risk and harm when you consider injury rates and long-term physical outcomes in some sport.
- The true spirit of elite sporting competition is closer to the Athenian ideal of superhuman effort at any cost (including risks and injuries), and doping is consistent with that.
- Supervised regulated use of performance enhancing drugs and substances, and other banned practices (e.g. blood transfusions) would reduce health risks and harms.
- Prohibition policies and punitive measures create hidden, uninformed, and riskier doping which exacerbates health and other harms.
Again, people who argue for doping in sport may place different weight on some of the above arguments over others. Further, belief in one or other of these arguments doesn’t commit you to all of them.
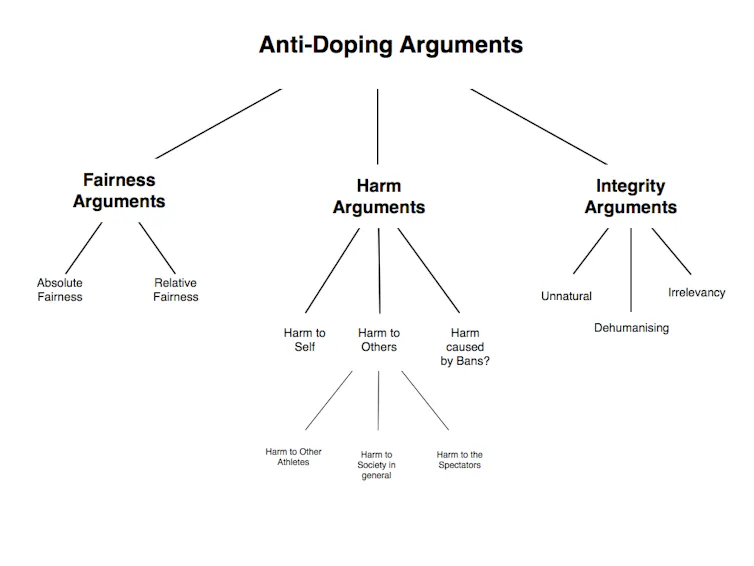
Doping prevention approaches
If you are opposed to doping, you should also have a position on how to prevent or reduce it – your discussions on the topic won’t get far if you’re against doping but have nothing to say on what to do about it.
On doping prevention you could take a zero tolerance stance , where you favour restrictive surveillance and testing protocols, and punitive responses for even minor doping transgressions. Implicit in this stance is the belief that because the individual chooses to break known rules by doping, they should take responsibility and be punished accordingly if caught or if they confess, or make later admissions.
Zero tolerance advocates might also believe that doping in sport can ultimately be eradicated. But this is not a necessary belief for this position - for example zero tolerance proponents might simply favour the strong public message in sports doping policy that includes punitive responses.
Alternatively, you could adopt a prevention stance based on harm minimisation principles. Implicit in this position is the belief that doping will always exist in sport, and so the pragmatic aim of prevention is to reduce doping harm (to dopers, other athletes, spectators, sport generally), rather than total eradication of the behaviour.
Harm reduction proponents emphasise an athlete health and welfare focus over harsh punitive measures (i.e. criminalisation specifically). People here are less concerned with upholding individual responsibility as far as punishment goes. They believe doping prevention is better achieved through a focus on broader social, cultural, and systemic factors (e.g. team/club/sport culture, sport governance systems, ethics and integrity culture and systems, etc) rather than individual factors alone.
Punishing dopers doesn’t work
People who argue for harm minimisation approaches believe punitive measures alone will be ineffective in reducing or preventing doping in sport. As above, one reason for this is they believe doping behaviour is driven by a range of factors, and so doping prevention too must take a broad focus (beyond individual behaviour and psychology) to achieve widespread and lasting change.
Another claim made here is that penalties for doping such as fines, suspensions, and even lifetime bans are unlikely to deter doping, and will not eradicate it. The analogy often cited here this is the case of death penalties for murder not halting murder rates, or harsh criminal penalties for illicit drug possession, supply and use failing to reduce or eliminate those proscribed behaviours.
People who are unconvinced about the effect of punitive measures might also point out that even the severest doping penalties are unlikely to work in most cases, because under the current system athletes would challenge such penalties legally to uphold their right to compete, or preserve their rights for future earnings.
Finally, many people against punitive responses to sports doping also place a high value on forgiveness and redemption – a chance to start again with a clean slate. What often comes with this position is the view that the punishment and public humiliations suffered by some dopers (and their families) can be wrongly disproportionate to their original doping offence.
Punitive measures have a place
Supporters of punitive measures do not accept the analogy made between doping and criminal behaviour. They would argue the social, cultural and individual factors (including psychological determinants) of doping in sport are very different to those for murder and illicit drug use. As such, they also claim the thinking behind doping prevention approaches, including the expected impact of severe sanctions (not necessarily criminal), should be different too.
Zero tolerance advocates believe that, if applied appropriately, punitive measures can achieve desired sports doping prevention outcomes (i.e. reduced doping behaviour, reduced harm, or complete eradication). The view here is if doping policy is to include punitive measures (as per the current anti-doping framework), then these should be implemented competently and consistently in accordance with the defined policy aims and processes; and with clear and consistent public messages from sports governing bodies giving unambiguous support.
Supporters of punitive measures might also argue that it is not the current anti-doping policy framework that has failed, but rather the inadequate implementation of this framework by sports governing bodies and systems weakened by inconsistent practices, ineffective leadership, and ambiguous public messages about high profile doping cases.

Middle ground or mixed messages?
Doping in sport debates are often framed around the two ‘sides’ of harm minimisation and zero tolerance. At first glance, such positions appear distinct. In reality, people commonly shift between positions or argue a mix of both.
For example, you might believe that doping requires social determinants focused education and prevention programs (including capacity building in ethics and integrity, athlete culture and health and welfare and so on), AND progressively severe punitive measures in certain circumstances (e.g. for repeat doping offences, systematic team-based doping, related fraud and criminal activity).
A significant challenge for the doping in sport debate is predicting how people will think about and respond to doping cases. Ideally, careful reasoning based on the types of beliefs and positions summarised in this article would lead us to consistent responses, but that is not what often happens.
We see this with the sport of cycling - for example, compare most people’s strident opinions and responses about the Lance Armstrong case, to the relatively muted reactions about other cyclists who have doped (e.g. David Millar, Jan Ullrich, Erik Zabel, George Hincapie, Tyler Hamilton, Stuart O'Grady, Matt White, Neil Stephens, Alberto Contador, Alejandro Valverde, Danilo Di Luca etc).
We also see this in the responses from governments, sports governing bodies, and the sport itself. Again, the official reactions to the above cases in cycling have been markedly different - take a moment to reflect on where each of these riders are currently.
Most sports governing bodies and officials would claim they occupy a middle position between ‘crime and punishment’ and ‘education and prevention’ thinking and approaches. At face value, this seems like a sensible space for doping policy - the best of both worlds. However, this middle space can also be a fertile ground for mixed public messages and inconsistencies on doping that can undermine prevention efforts - as I have argued before in this Column ( here and here ).
By trying to occupy the middle ground on doping between zero tolerance and harm minimisation - trying to have it both ways - sports governing bodies run the risk of subsequently failing to implement either aspect of their doping prevention policies competently and consistently. Again, take a look at the recent criticisms made about the International Cycling Union.
Doping prevention efforts in all sports are undermined when mixed messages emerge from inconsistent thinking and action around doping policy - and especially when they continue unchallenged in public discussion and debates (e.g. ‘say no to doping’ but ‘say yes to ex-dopers in coaching positions’; ‘our sport is anti-doping’ but ‘ex-dopers manage our pro teams’; ‘strong doping prevention messages are needed’ but ‘ex-dopers are sponsoring elite teams, sports blogs, and working in sports media’).
What does your position on doping in sport commit you to? What should be done to prevent doping? What should we say about the mixed messages that exist about doping in sport?
Further reading: There is of a large academic literature, and a growing research evidence base, underpinning many of the points made in this article. If you are interested in further reading, a reasonable coverage of the issues can be seen at the Wikipedia doping in sport site , and Routledge have published a number of excellent academic books on this topic by some of the leading thinkers in this area.
Senior Research Development Coordinator
Audience Development Coordinator (fixed-term maternity cover)
Lecturer (Hindi-Urdu)
Director, Defence and Security
Opportunities with the new CIEHF
Tapping to Agree I hereby consent to the use of cookies, confirm that I have read Cookie Policy and allow this website to collect and process my personal data in a safe and secure way
- Essay Writers for Hire
- Pay For Essays
- Plagiarism Free Essays
- Business Essay Writing Service
- Scholarship Essay Writing
- Masters Essay Writing Service
- Essay Editing
- Persuasive Essay Writing Service
- Personal Statement Writing Service
- College Paper Writing
- Coursework Writing
- Dissertation Editing
- Write My Dissertation
- Essays for Sale
- Buy Research Paper
- Research Paper Help
- Pay For Research Paper
- Write My Research Paper
- Research Paper Editing
- Write My Philosophy Research Paper
- Write My Assignment
- Conclusion Generator
- Paraphrasing Tool
- Essay Maker
- Testimonials
- How It Works
- Healthcare&Medicine
Performance Enhancing Drugs in Sports
The use of Performance Enhancing Drugs has been a significant subject in athletics over the years. Most athletes have used performance-enhancing drugs (PEDs) at some point in their careers. The use of performance-enhancing drugs dates back to the 1930s when scientists found that they could create a synthetic hormone that would help in the healing process of the weakest individuals, restore the sex lives of older men, and improve children with growth defect problems. These effects, however, were brought out of public athletes, and it was determined to help them improve their abilities to compete. This has been a big deal for the professional sporting activities and the banned athletic community.
Thesis: Performance enhancing drugs should not be allowed to be used by athletes since it is illegal and has harmful effects on the body.
P1: Performance Enhancing Drugs should not be allowed by athletes since they are illegal in sports.
P2: The use of PED causes harm in the body, for the athletes using it.
P3: Laws and penalties for the Performance Enhancing Drugs.
The first use of PED’s was in Olympics, which then started spreading to the other sporting world. The Olympic committee was the first to ban the use of PED’s and later followed suit to the other sports. The International Olympic Committee (IOC) established a medical commission in 1967 whose main mandate was to ban the use of drugs as well as the use of Performance enhancing substances. The PED’s are therefore illegal and have been banned by every sport.
The first point is justified through examples of sportsmen like A-Rod (Alex Rodriguez), Marion Jones, Lance Armstrong, Ben Johnson, Jose Canseco and Lyle Alzado. Lance Armstrong saw his win stripped and was banned for life from any sport after it was established that he was using PED’s. Ben Johnson and Marion Jones have stripped off their wins in field and track events while Lyle Alzado died from brain cancer which was believed to have been caused by PED’s. Other athletes have admitted to using PED’s, for instance, Jose Canseco. Alex Rodriguez was suspended for one hundred and sixty-two games after it was confirmed that he was using steroids (Greely et al 22). Most of the people who use performance enhancers have certain physical traits such as severe acne and loss of hair. Other deformities include male breast enlargement, paranoia, violent mood swings and infertility. Moreover, performance enhancers cause stroke, cancer as well as stunted growth due to bone deformities.
President George W. Bush once said in a state function that the performance enhancers like steroids, used in sports like baseball, football and other sports are dangerous as it sends a wrong message that they are shortcuts to accomplishment and that performance is more important than the character. Most athletes are role models and they do not think of their social impact when they use the illegal drugs. For quite some time, the use of drug enhancers gives athletes an edge over their competition and it is concerned with ethics for those who supply the drugs as well as those who take them to boost their careers.
Performance Enhancement Drugs are harmful, and athletes are always thinking of the short-term positive effects which are given by the PED’s. They fail to look ahead and see the long-term impacts which will later negatively affect their bodies. The men and women who use drugs end up developing medical conditions such as heart attack or stroke, high blood pressure, liver and kidney tumors, fluid retention, blood clots and high cholesterol, which alter growth permanently. There are many physiological conditions which affect the bodies of the PED users as well, besides the physical effect. The impacts of these drugs are very serious and dangerous and hence they should be aware of the effects and take the necessary measures from taking place.
The second premise is supported by the fact that those who praise the athletes and look to emulate their performances will copy what their idol sportsmen do. Performance enhancement drugs, mainly steroids have played a big role after it was first established that Mark McGwire used a substance androstenedione 103 during the 1998 season. It was estimated the sale of Performance Enhancement Drugs had increased more than five times. Most youths in the current times have looked up to the people outside their families who have a good example and an idol person who is not around them. This sends the wrong message to the young people that being alright to reach their limits even if they use illegal substances to reach there. This raises the question, how is it right when the athletes who are looked upon by so many people do illegal things and take substances which are harmful to their health?
When the government or governmental institutions like public schools or colleges desire to test an athlete for drugs, this calls for a state action. Usually, there are no state actions for the private sports leagues and thus there were amendments in the fourth, fifth and sixth issues on the private league sports. The Feral laws regulate the use of drugs and the Anabolic Steroid Control Act of 1990. It has been the wish of the US government to create integrity in the sports department in the country, without invading the privacy of the athletes. The athletes have constitutional safeguard which allows a challenge to test them on the basis of constitutionality. The courts have supported the of mandatory suspicionless testing to address the challenges of testing for the athletes who are tested on drugs. The fourth amendment gives the provision for testing athletes for drugs, where it states it’s the right of the people to secure their lives and property against unreasonable seizures and searches without warrants. Most competitions require a test as part of taking part in the competition, in the bid to control doping and use of drugs in spots. Some of the remedies for people found guilty of using drugs ins sports include fines, banning from specific sports for a particular period of time, jail terms and exclusion from the rest of the competitors, among others.
Objection to the arguments.
One of the projections would be PED should be allowed since they enhance the performance of the athletes. Studies have revealed that performance-enhancing drugs, such as anabolic steroid androgen increase the muscular performance of the employees by 5-20 %. Improving the strengths and the general durability of employees will help the athletes perform to their best when playing or taking part in an event. The fans and spectators push the athletes to perform their best and in the process, enhance a culture of doping in order to reach great heights. It is very difficult to reconcile the purity of the athletes and the expectations of the fans and their managers in whatever it takes to win so long as it does not go past the arbitrary conceptualization of natural. Performance Enhancing Drugs are a great level and is used to close the gap for the athletes to fill the gap between their performance and their potential (Savulescu, Bennett, and Megan, 668). When athletes use PED’s, it makes them perform at higher levels and meet the expectations of their fans and managers. It makes the athletes more interesting and exciting to watch since we are used to seeing athletes perform at the normal levels. when we see an individual playing well in any competition, we are poised to even watch them the more.
Though there are strong arguments made against the banning of PED’s I believe that the facts are evidenced by the effects and hence I support the banning of PED. Drugs are illegal and harmful to the physical and physiological effects in their bodies. Despite people thinking they should allow since it enhances the performance of athletes, which people argue that it leads to a more exciting game, it is very wrong. Arguments have been made that if one individual uses the PED’s then the others should use them too to make the game more exciting, but they fail to recognize the effects of the drugs. If everyone uses the PED drugs, it would be the same just like when no person was using, since the performance of all the players will be the same and they depend on the PED’s. My arguments are strongly based on the grounds that PED’s should remain illegal and banned from sports. With all the supporting evidence I believe that these arguments are valid and in case there are any objections, it would be difficult to put up a counter argument for these reasons.
Performance Enhancing Drugs in sports carries away the integrity of athletes just like the sports in general. PED’s are illegal and have adverse effects on the athletes. PED’s should be kept away from professional sports so as to create transparency and encourage individual efforts. The use of harmful substances like steroids, which are most common among athletes causes harm, which may cause even death. Performance Enhancement drugs not only affect the physical and physiological traits of athletes but has other effects like infertility and contracting other diseases like cancer. It is unfair for the athletes who work very hard and put all their efforts in becoming successful in sports to be compromised by the individuals who use performance enhancement drugs. Advocating for people who use PED’s will give them an upper hand in sports, which is not advisable for any sport. Young athletes should be aware of the effects which they will experience when they PED’s and which will prevent them have a prolonged life in their careers.
📌Boost GPA: Buy College Essays Online – Your Key to Academic Triumph!
Works Cited
Bahrke, Michael S. Performance-enhancing substances in sport and exercise. Human Kinetics 1, 2002.
Brotherton, Stephen L., Norman Fost, and Gary A. Green. "Performance-Enhancing Drugs in Sports." Virtual Mentor 6.7 (2004).
Catlin, Don H., and Thomas H. Murray. "Performance-enhancing drugs, fair competition, and Olympic sport." Jama276.3 (1996): 231-237.
Cross, Aaron, and Mr. Kulycky. "Performance-Enhancing Drugs in Sports." (2005).
Greely, Henry, et al. "Towards responsible use of cognitive-enhancing drugs by the healthy." Nature 456.7223 (2008): 702-705.
Kayser, Bengt, Alexandre Mauron, and Andy Miah. "Legalisation of performance-enhancing drugs." The Lancet366 (2005): S21.
Savulescu, Julian, Bennett Foddy, and Megan Clayton. "Why we should allow performance enhancing drugs in sport." British journal of sports medicine 38.6 (2004): 666-670.
Uvacsek, M., et al. "Self‐admitted behavior and perceived use of performance‐enhancing vs psychoactive drugs among competitive athletes." Scandinavian journal of medicine & science in sports 21.2 (2011): 224-234.
- The Birth of King Jamil
- Health's Social Determinants
- Matrix Health Insurance
- Capacity in the Management of Health Services
- In the health-care environment, coding has an i...
- Exchange of Health Data
Academic levels
Paper formats, urgency types, assignment types, prices that are easy on your wallet.
Our experts are ready to do an excellent job starting at $14.99 per page
We at GrabMyEssay.com
work according to the General Data Protection Regulation (GDPR), which means you have the control over your personal data. All payment transactions go through a secure online payment system, thus your Billing information is not stored, saved or available to the Company in any way. Additionally, we guarantee confidentiality and anonymity all throughout your cooperation with our Company.
Try our service with 15% Discount for your first order! Try our service with 15% Discount for your first order! Try our service with 15% Discount for your first order!
Home — Essay Samples — Nursing & Health — Performance Enhancing Drugs — Performance Enhancing Drugs no Place in Sport
Performance Enhancing Drugs No Place in Sport
- Categories: Doping Drugs Legalization Performance Enhancing Drugs
About this sample

Words: 653 |
Published: May 24, 2022
Words: 653 | Page: 1 | 4 min read
Table of contents
Drug taking in sport is morally/ethically wrong, the reasons why athletes turn to drugs, legalization of drugs in sports arguments both for and against.
- BBC, (2014) BBC - Ethics - Sporting Ethics: Body Modification, Bbc.co.uk. Available at: http://www.bbc.co.uk/ethics/sport/debate/drawingline_1.shtml (Accessed: 15 April 2017).
- Conlee, RK. (1991).Perspectives in exercise science and sports medicine, Vol. 4: ergogenics, enhancement of performance in exercise and sport.1991:285–329
- Ip, H. (2014) Drugs In Sport - Ethical Issues, Smapworld.tripod.com. Available at: http://smapworld.tripod.com/drugs/ethical.html (Accessed: 15 April 2017).
- McCalla, S. (2014) Moral/Ethical Analysis Of Performance Enhancement In Sports, University Publications. Available at: http://www.universitypublications.net/ijas/0704/pdf/T4N233.pdf (Accessed: 15 April 2017).
- McCormack, O. (2014) Drugs and Cheating in Sport: Ethical Issues, prezi.com. Available at: https://prezi.com/zn7cflrmn0mw/drugs-and-cheating-in-sport-ethical-issues/ (Accessed: 15 April 2017).
- Smith, J. (2012) Ethical Issues in Sports, Ethical Issues in Sports. Available at: http://john23jay.wixsite.com/sports-and-ethics/drug-use (Accessed: 15 April 2017).
- Tia, A. (2016) Should the use of performance-enhancing drugs in sports be legalized?Debate.org. Available at: http://www.debate.org/opinions/should-the-use-of-performance-enhancing-drugs-in-sports-be-legalized (Accessed: 15 April 2017).

Cite this Essay
Let us write you an essay from scratch
- 450+ experts on 30 subjects ready to help
- Custom essay delivered in as few as 3 hours
Get high-quality help

Prof Ernest (PhD)
Verified writer
- Expert in: Life Law, Crime & Punishment Nursing & Health

+ 120 experts online
By clicking “Check Writers’ Offers”, you agree to our terms of service and privacy policy . We’ll occasionally send you promo and account related email
No need to pay just yet!
Related Essays
2 pages / 994 words
2 pages / 891 words
1 pages / 435 words
1 pages / 673 words
Remember! This is just a sample.
You can get your custom paper by one of our expert writers.
121 writers online
Still can’t find what you need?
Browse our vast selection of original essay samples, each expertly formatted and styled
Related Essays on Performance Enhancing Drugs
The topic and discussion over most athletes’ use of performance-enhancing substances such as muscle builders, (steroids), is getting more challenging as biotechnologies like gene therapy become a reality. The accessibility of [...]
Performance enhancing drugs used in various sporting events in order to give competitors an advantage over their opponents have been involved in widespread use that can even be traced back to the first Olympic games. Ancient [...]
Bowers, M. B. (1998). Doping and performance-enhancing drugs. In B. R. Brown (Ed.), Ethical issues in sport (pp. 3-16). Sage Publications.Dixon, K. (2008). Steroid testing and legalising performance enhancing drugs: The [...]
Laws and rules govern sports in order to make it more entertaining as well as ensuring that the participants are using their skills to compete. There is a reason why there exists so many sports and the reason is that not [...]
The use of steroids in sports has been a controversial topic that has raised concerns about fairness, health risks, and the integrity of athletic competition. This essay examines the impact of steroids on sports, the ethical [...]
Adolescence is the most dramatic stage in development. Weed, alcohol, and marijuana are the most used. Adolescent substance users indicate abnormalities of brain functioning, connected to changes in neurocognition over time [...]
Related Topics
By clicking “Send”, you agree to our Terms of service and Privacy statement . We will occasionally send you account related emails.
Where do you want us to send this sample?
By clicking “Continue”, you agree to our terms of service and privacy policy.
Be careful. This essay is not unique
This essay was donated by a student and is likely to have been used and submitted before
Download this Sample
Free samples may contain mistakes and not unique parts
Sorry, we could not paraphrase this essay. Our professional writers can rewrite it and get you a unique paper.
Please check your inbox.
We can write you a custom essay that will follow your exact instructions and meet the deadlines. Let's fix your grades together!
Get Your Personalized Essay in 3 Hours or Less!
We use cookies to personalyze your web-site experience. By continuing we’ll assume you board with our cookie policy .
- Instructions Followed To The Letter
- Deadlines Met At Every Stage
- Unique And Plagiarism Free
IMAGES
VIDEO
COMMENTS
The main effort in enforcing a 'clean sport' has concentrated on proving an abuse of performance-enhancing drugs and on imposing sanctions on teams and athletes. An investigation started by Freiburg university hospital against two of its employees who had been working as physicians for a professional cycling team has drawn attention to ...
All performance enhancing drugs should be banned from sports. The history of performance enhancing drugs goes back to the 1800s. There were two reported cases before the 1900s. The first known use was by a 24 year old cyclist named Arthur Linton in 1886. He died in a race from Bordeaux to Paris. The cause of death was said to be Typhoid Fever ...
Doping from the beginning to the present day. Over time, there have been several definitions of doping. Beckmann's sports dictionary describes doping as the use of performance-increasing substances, which would place the athlete on a superior position than that he would normally have obtained. 7 The first official definition of doping dates from 1963 and it was issued by the European Committee ...
Performance-Enhancing Drugs in Sports Essay. Doping is defined as the infringement of the World Anti Doping Agency regulations. 1 It is said that most sportsmen and women have been using steroids and even stars like former American sprinter Marion Jones pleaded guilty of using these drugs. Some stars who do not use steroids claim that those who ...
performance enhancing drugs going as far back as ancient times. Despite this long and storied history of performance enhancing drugs in sports, doping is arguably the most controversial and most talked-about issue in modern sports. It is an issue that cuts across all sports, regardless of technology, popularity, or tradition.
Performance Enhancing Drugs in Sport Essay. The use of performance-enhancing drugs has always been a notorious issue in sports. Because of high competition rates and a relatively short amount of time that a sportsman has to break a record, the idea of using drugs that allow for impressive achievements has always been popular among sportsmen and ...
Some athletes may seem to get an edge from performance-enhancing drugs. But doping can have bad effects on health. In general, the long-term effects of performance-enhancing drugs haven't been studied enough. And any short-term perks come with risks. Doping is banned by most sports leagues and groups too.
Two major claims underpin the aversion to this use of drugs. The first is that it is cheating. The second is that performance-enhancing drugs threaten the health of athletes. But is either claim ...
Introduction. The use of performance-enhancing drugs (PEDs) by preteenagers and teenagers has increased tremendously over the past decade. This trend is driven by multiple factors, including the decrease in the age of participation in competitive sports; the increase in popularity of team/competitive sports; the focus of the media on thinness in females and muscular bodies in males; pressure ...
When used during sport, cocaine is considered to have performance enhancing effects and is prohibited under the World Anti-Doping Code and listed under the Substances of Abuse Category.
The family physician is a critical player in addressing the use of performance-enhancing drugs in recreational athletes of all ages. Family physicians should continue to be alert to signs of use ...
History of Performance-Enhancing Drugs and Technologies in Sports. Sports "ain't never been clean," says Charles Yesalis, former Pennsylvania State University professor and long-time performance-enhancing drug researcher. And by "never," Yesalis means never.Research suggests that the first Olympians were openly doping. "The ancient Olympic champions were professionals who competed ...
The drug is used for performance enhancing (Coe, p. 224). Different sports have set up laws that are used to curb drug doping. Sports personalities use drugs to gain an advantage over the others. Performance enhancing drugs have been used in the Olympics by different people. For example, Thomas Hicks won the marathon after using strychnine.
Supervised regulated use of performance enhancing drugs and substances, and other banned practices (e.g. blood transfusions) would reduce health risks and harms. Prohibition policies and punitive ...
Lewis, C. R. (2019). The Impact of Performance-Enhancing Drugs on Athletic Performance: A Review of the Literature. Journal of Sports Science, 37(5), 567-584. Davis, L. M. (2022). The Legal and Ethical Considerations of Performance-Enhancing Drug Use in Sports. International Journal of Sport Policy and Politics, 14(2), 245-263. Wilson, E. S ...
These drugs are life threatening to athlete's health. The use of performance enhancing drugs promotes that cheating is prohibited. It also provides a bad example for athletes to use. Research shows that these drugs have a negative effect to every sport. 863 Words.
Performance enhancing drugs should be eliminated from all sports because they create an unfair competitive advantage. I am against the use of Performance Enhancing Drugs in sports because it is a worldwide problem that takes the integrity out of the game. There are so many people involved from trainers, players and coaches.
Performance enhancing drugs has been used in sports for years. During modern Olympic Games, the drugs athletes choose to use included strychnine, heroin, cocaine, and morphine. In the early 1950s performance enhancing drugs was used in sports before that it was used by soldiers in the war.
Performance Enhancing Drugs In Sports Essay. Performance enhancing drugs in sports should not be tolerated and should be banned. The taking of these Performance Enhancing Drugs just isn't fair, we're encouraging youth (teens) to take these drugs and it can have dramatic health risks weather if it is short or long term damage. Performance ...
P1: Performance Enhancing Drugs should not be allowed by athletes since they are illegal in sports. P2: The use of PED causes harm in the body, for the athletes using it. P3: Laws and penalties for the Performance Enhancing Drugs. Conclusion. P1: Performance Enhancing Drugs should not be allowed by athletes since they are illegal in sports.
Drugs In Sports Research Paper Drugs in sport The nature of sports promotes a strong desire to win, and many athletes will do anything to rise to the top. Every elite athlete wants to get an edge over their competition, causing many athletes to turn to performance enhancing drugs to gain this edge. Drug use in sport can cost players their super
Stuck on your essay? Browse essays about Performance Enhancing Drugs and find inspiration. Learn by example and become a better writer with Kibin's suite of essay help services.
Legalization of drugs in sports arguments both for and against. It should not be allowed as it is not fair for the athletes who work really hard to be the best in their performance. Using drugs means you are ignoring the body's needs. An example would be if an individual has been working out and at the same time has been taking drugs, the ...
The use of performance enhancing drugs in sports can actually be described by one word 'Cheating. ' The laws need to become stricter in order to discourage the use of performance enhancing drugs. Every accusation, of a professional athlete using banned substances in professional sports has a negative affect on fans and spectators.
news hour | ait live | april 9th, 2024 | live now