An official website of the United States government
Official websites use .gov A .gov website belongs to an official government organization in the United States.
Secure .gov websites use HTTPS A lock ( Lock Locked padlock icon ) or https:// means you've safely connected to the .gov website. Share sensitive information only on official, secure websites.
- Publications
- Account settings
- Advanced Search
- Journal List

Educational Case: HER-2 Positive Breast Cancer
Julia jennings , md, jennifer l clark , md, phd.
- Author information
- Article notes
- Copyright and License information
Jennifer Clark, Department of Pathology, UMass Memorial Medical Center, Three Biotech, One Innovation Drive, Worcester, MA 01605, USA. Email: [email protected]
Received 2020 Sep 9; Revised 2021 Jun 6; Accepted 2021 Jun 27; Collection date 2021 Jan-Dec.
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 4.0 License ( https://creativecommons.org/licenses/by-nc-nd/4.0/ ) which permits non-commercial use, reproduction and distribution of the work as published without adaptation or alteration, without further permission provided the original work is attributed as specified on the SAGE and Open Access pages ( https://us.sagepub.com/en-us/nam/open-access-at-sage ).
The following fictional case is intended as a learning tool within the Pathology Competencies for Medical Education (PCME), a set of national standards for teaching pathology. These are divided into three basic competencies: Disease Mechanisms and Processes, Organ System Pathology, and Diagnostic Medicine and Therapeutic Pathology. For additional information, and a full list of learning objectives for all three competencies, see http://journals.sagepub.com/doi/10.1177/2374289517715040 . 1
Keywords: pathology competencies, organ system pathology, breast, molecular basis of breast neoplasms, factors affecting response and prognosis of breast cancer, HER-2
Primary Objective
Objective BR2.7: Factors Affecting Response and Prognosis of Breast Cancer . Explain the prognosis and likelihood of recurrence and response to therapy for breast cancer patients based on knowledge of molecular classification and/or gene expression profiling, morphologic classification, grade, prognostic marker studies, and other predictive factors.
Competency 2: Organ System Pathology, Topic: Breast (BR), Learning Goal 2: Molecular Basis of Breast Neoplasms
Patient Presentation
A 65-year-old woman with no relevant past medical history is found to have a spiculated right breast mass measuring approximately 1.6 cm on routine mammogram. She has had unremarkable annual screening mammograms since her first mammogram at age 50. Her family history is significant for breast cancer in her mother and maternal grandmother, both older than 75 years at diagnosis.
Diagnostic Findings, Part 1
The patient undergoes an ultrasound-guided core needle biopsy, shown in Figure 1 . The biopsy demonstrates small clusters and single cells with enlarged and pleomorphic, hyperchromatic nuclei and moderately increased mitoses infiltrating through stroma. A diagnosis of poorly differentiated invasive ductal carcinoma is rendered. There is no evidence of lymphovascular invasion or in situ carcinoma.

Results of breast core needle biopsy. A hematoxylin & eosin–stained tissue section from the breast core needle biopsy demonstrates poorly differentiated invasive ductal carcinoma (10× objective).
Questions/Discussion Points, Part 1
What biomarkers are routinely performed on new diagnoses of breast cancer.
Newly diagnosed cases of breast carcinoma undergo testing for estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor (HER-2) receptor.
How Are These Biomarkers Evaluated, and What Is Their Clinical Significance?
Both ER and PR status are evaluated by immunohistochemistry alone, while HER-2 status can be determined by immunohistochemistry and/or fluorescence in situ hybridization (FISH). The expression of these markers contributes to prognosis, as well as targeted therapy. 2
Estrogen receptor and PR are both nuclear hormone receptors that operate as ligand-dependent transcription factors. Approximately 50% to 60% of breast cancers are ER positive. Hormone receptor positivity predicts tumor progression and mortality benefit from endocrine therapies such as tamoxifen. 2
HER-2 is a transmembrane receptor with tyrosine kinase activity that mediates growth, differentiation, and survival of cells via multiple signal transduction pathways. Approximately 15% to 25% of breast cancers overexpress this gene which is typically associated with more aggressive tumor behavior. 3 In fact, the quantitative amount of HER-2 overamplification has been found to be in direct association with worse clinical outcomes. 4 HER-2 overexpression and amplification have also been found in cancers of other sites, such as the stomach, ovary, colon, bladder, and esophagus. 2
The first step in routine evaluation of HER-2 is immunohistochemistry, following a scoring system illustrated in Figure 2A to D . A tumor demonstrating circumferential membrane staining that is complete, intense, and in >10% of the tumor cells is scored immunohistochemistry (IHC) 3+ and is considered HER-2 positive. Conversely, a tumor with incomplete membrane staining that is faint and in >10% of tumor cells is classified as IHC 1+ and is considered HER-2 negative. Weak to moderate complete membrane staining observed in >10% of tumor cells is classified as IHC 2+ and is considered equivocal. In equivocal cases, the sample should be evaluated with FISH.

Human epidermal growth factor (HER-2) immunohistochemistry (IHC) and fluorescence in situ hybridization (FISH) guideline summary. (A) No perceptible staining or barely perceptible incomplete membrane staining in <10% of tumor cells (IHC 0; 40× objective), (B) faint, barely perceptible incomplete membrane staining in >10% of tumor cells (IHC 1+; 40× objective), (C) weak to moderate complete membrane staining in >10% of tumor cells (IHC 2+; 40× objective), (D) intense, complete circumferential membrane staining in >10% of tumor cells (IHC 3+; 40× objective), (E) negative HER-2 FISH demonstrating HER-2 copy number <4.0 and HER-2/CEP17 ratio <2.0 (HER-2: red signal, CEP17: green signal; 100× objective), (F) positive HER-2 FISH demonstrating HER-2 copy number >6.0 and HER-2/CEP17 ratio >2.0 (HER-2: red signal, CEP17: green signal; 100× objective).
Fluorescence in situ hybridization is used to identify and quantify amplification of the HER-2-neu gene and is viewed as the “gold standard” for determining which patients would benefit from HER-2-targeted therapy. Fluorescence in situ hybridization is a molecular technique that utilizes fluorescent probes complementary to the nucleic acid sequence of interest, in this case, the HER-2-neu gene. The HER-2-neu copy number can either be evaluated alone or in comparison to the copy number of internal centromeric control (typically the region termed CEP17), as summarized in Table 1 . Under normal circumstances, each cell will demonstrate 2 copies of both the HER-2-neu and CEP17 regions (1:1 ratio), but in the presence of an amplified HER-2-neu gene, there will be an excess of HER-2-neu signals in relation to CEP17 signals. Examples of both negative and positive FISH results are included in Figure 2E and F . A downside of FISH testing is that it is often more expensive than immunohistochemistry. 2 , 5
Summary of HER-2 FISH Reporting Guidelines.
Abbreviations: FISH, fluorescence in situ hybridization; HER-2, human epidermal growth factor; IHC, immunohistochemistry.
* Additional workup varies depending on the HER-2/CEP17 ratio and average HER-2 copy number in a particular case but may include review of HER-2 IHC, repeat FISH scoring by a second observer, and/or use of alternate probe sets.
What Other Factors Affect the Prognosis of Breast Cancer?
Tumor grade (well, moderately, or poorly differentiated), determined through scoring of tubule formation, nuclear atypia, and mitotic count, is a major factor affecting the prognosis of breast cancer. In addition, molecular subtypes, including luminal, normal breast-like, HER-2-enriched, and basal-like types, identified through extensive molecular profiling of a large number of breast cancer samples, play a major role in prognosis and treatment response. These topics are further discussed in a previously published educational case. 6
Diagnostic Findings, Part 2
This patient’s breast cancer is negative for ER and PR. Immunohistochemistry staining results for HER-2 are shown in Figure 3 . HER-2 IHC is scored as 2+ (equivocal) for HER-2, demonstrating weak to moderate complete membrane staining in >10% of tumor cells. Due to this result, the sample is tested reflexively by FISH.

Human epidermal growth factor (HER-2) immunohistochemistry (IHC) on breast core needle biopsy. The HER-2 IHC demonstrates moderate complete membrane staining in >10% of tumor cells (IHC 2+; 10× objective).
Fluorescence in situ hybridization results demonstrate amplification of the HER-2/neu gene. Using the CEP17 gene as an internal centromeric control, the HER-2/CEP17 ratio is 3.7, while the average nucleus contains 9.4 copies of HER-2. This result indicates that this patient’s breast cancer is HER-2 positive.
Questions/Discussion Points, Part 2
Discuss the biology of the her-2 protein and its role in breast cancer.
The HER-2/neu belongs to a family of 4 human epidermal growth factor receptors: HER-1, HER-2, HER-3, and HER-4. Each is characterized by a cysteine-rich extracellular ligand-binding site, a transmembrane lipophilic segment, and an intracellular domain with tyrosine kinase activity. More specifically, the HER-2 receptor is a 1255 amino acid, 185 kD transmembrane glycoprotein located on the long arm of human chromosome 17 (17q12). It has no direct activating ligand and thus requires heterodimerization with other epidermal growth factor receptor (EGFR) family receptors such as HER-1 and HER-3. Dimerization and autophosphorylation of the HER-2 receptor tyrosine residues initiates various signal transduction pathways including mitogen-activated protein kinase, phosphatidylinositol-4,5-bisphophate 3-kinase, and protein kinase C. 2 When amplified or overexpressed, uncontrolled overactivation of these pathways leads to tumorigenesis and increased tumor aggressiveness. The HER-2 overexpression in breast cancer is related to the amplification of the otherwise normal gene rather than mutation. For this reason, HER-2 targeted therapy does inherently carry the risk of damaging normal tissues which express the protein.
Discuss the Epidemiologic Features of HER-2 Positive Breast Cancer
It has been found that ER/PR+HER-2− breast cancers are associated with better survival rates, followed by ER/PR+HER-2+ breast cancers, while triple-negative cancers (ER/PR-HER-2−) are associated with the shortest survival rates of these categories. Although HER-2 positive breast cancers were historically among the most aggressive cancers with the worst prognosis, the advent of HER-2-targeted therapy has improved survival rates significantly, such that HER-2 positive breast cancers now demonstrate similar or better outcomes than triple-negative breast cancers when matched for stage. The distribution of breast cancer subtypes varies by age, race, ethnicity, and other factors. Compared with women who have ER/PR+/HER-2− breast cancer, those diagnosed with other subtypes (ER/PR+/HER-2+, ER/PR-/HER-2+, or ER/PR-/HER-2−) are more likely to be younger, belong to minority groups, and be diagnosed with cancer at a later stage. 7 BRCA1/BRCA2 mutations are associated with lower rates of HER-2 positive breast cancer. 8
What Is the Prognosis of HER-2 Positive Breast Cancer?
HER-2 positive breast cancers have been found to have a worse overall prognosis than HER-2 negative breast cancers. Population-based studies have shown that overexpression of HER-2 is associated with poorly differentiated, high-grade tumors, high proliferative rates, lymph node involvement, and relative resistance to certain types of chemotherapy. 9
Studies have shown that HER-2 positive breast cancers carry an increased risk of cerebral metastasis compared with ER/PR+ breast cancers and that HER-2-positivity is associated with earlier cerebral metastasis in the disease course. 10 It is believed that once HER-2 amplification occurs, the HER-2 phenotype is fixed throughout the tumor’s lifetime. As a result, testing for HER-2 may be performed on either a primary tumor or a metastatic deposit. 2
Discuss the Management of HER-2 Positive Breast Cancer
The advent of HER-2-targeted therapies has significantly improved the outlook for patients with HER-2 positive breast cancer. Trastuzumab (Herceptin), a monoclonal antibody targeting the HER-2 receptor, has been found to cause internalization and downregulation of the receptor. 11 It has also been found to reduce mortality and recurrence rates in HER-2 positive breast cancers. Studies have shown that the addition of trastuzumab to adjuvant chemotherapeutics such as paclitaxel, doxorubicin, and cyclophosphamide can reduce the rates of recurrence by half. 3 , 11 Due to the persistence of the HER-2 phenotype, trastuzumab has also been found to improve outcomes for both local and distant disease. 2 Additional therapy options include pertuzumab, a monoclonal antibody thought to interrupt HER-2/HER-3 dimerization, and neratinib, a tyrosine kinase inhibitor believed to interact with HER-2 and other EGFR kinases. 12
Approximately half of HER-2 positive breast cancers are also ER positive, PR positive, or both. However, the levels of these hormone receptors are typically lower than in HER-2 negative, hormone receptor positive tumors. For this reason, most HER-2 positive breast cancers are relatively resistant to tamoxifen and other endocrine therapies. 9
Current guidelines do not recommend the use of trastuzumab or other anti-HER-2 therapies in HER-2 negative breast cancers. Treatment for these tumors typically includes endocrine therapy (if ER/PR+) or single-agent chemotherapy.
Diagnostic Findings, Part 3
The patient’s stage is determined to be a clinical stage cT1cN0 based on physical examination and imaging findings.
Questions/Discussion Points, Part 3
How is breast cancer staged.
Breast cancer is staged using the TNM (tumor, node, metastasis) system which assesses the size and local extent of the primary tumor (T), presence or absence and number of axillary lymph node (N) metastases, and presence or absence of metastasis (M) at distant sites. Although clinical staging, designated by the prefix “c” is performed prior to surgery using data gathered from physical examination and imaging studies, including breast, axillary, and whole body imaging as indicated; pathologic staging, designated by the prefix “p,” is performed after surgery using data gathered from the resulting excision specimen. 13 In this patient case, stage cT1cN0 refers to a localized breast cancer measuring 1 to 2 cm on imaging without evidence of nodal metastasis.
How Does the Clinical Stage Affect Initial Management of Breast Cancer?
Treatment of breast cancer is interdisciplinary, utilizing expertise from medical oncology, radiation oncology, and surgery. Although low stage, localized cancer is often treated initially by surgical excision, higher stage cancers may require up-front neoadjuvant chemotherapy to reduce the tumor burden prior to surgery. Patients with known or suspected lymph node metastasis may undergo complete removal of the axillary lymph nodes at the time of surgery, as well. However, patients such as the one in this case without suspected lymph node metastasis may undergo sentinel lymph node biopsy only (the primary node draining from the breast lymphatics, as identified by a blue dye and/or radiotracer injected into the breast at the time of surgery). If the sentinel node is positive for metastatic tumor, further surgery or radiation may be pursued to treat the remaining axillary lymph nodes. The presence of distant metastasis may preclude surgery altogether, with a focus on palliative chemotherapy and radiation.
Teaching Points
Pathologic factors affecting the prognosis of breast cancer include tumor grade, molecular subtype, and expression of ER, PR, and HER-2.
HER-2 is part of a family of receptors that work together within various signal transduction pathways to promote growth, differentiation, and survival of cells. Amplification and overexpression of HER-2 may be seen in a subset of breast cancers.
Primary evaluation for HER-2 status should be performed by immunohistochemical staining, with equivocal results evaluated by FISH. A positive FISH result is the gold standard for determining whether a patient would benefit from HER-2-targeted therapy.
HER-2 positive breast cancers are often more aggressive, less responsive to treatment, and associated with decreased survival rates, though the advent of HER-2-targeted therapy has significantly improved prognosis.
Current management recommendations for HER-2 positive breast cancer include HER-2-targeted therapy (such as Trastuzumab) with adjuvant chemoradiation. Endocrine therapies (such as tamoxifen) have not been found to be effective for tumors with HER-2 amplification.
Acknowledgments
The authors would like to acknowledge Dr Dina Kandil for her assistance in reviewing the content of this manuscript.
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.

- 1. Knollmann-Ritschel BEC, Regula DP, Borowitz MJ, Conran R, Prystowsky MB. Pathology competencies for medical education and educational cases. Acad Pathol. 2017:4. doi:10.1177/2374289517715040 [ DOI ] [ PMC free article ] [ PubMed ] [ Google Scholar ]
- 2. Iqbal N, Iqbal N. human epidermal growth factor receptor 2 (HER2) in Cancers: overexpression and therapeutic implications. Mol Biol Int. 2014;2014:852748. doi:10.1155/2014/852748 [ DOI ] [ PMC free article ] [ PubMed ] [ Google Scholar ]
- 3. Piccart-Gebhart MJ, Procter M, Leyland-Jones B, et al. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N Engl J Med. 2005;353:1659–1672. doi:10.1056/NEJMoa052306 [ DOI ] [ PubMed ] [ Google Scholar ]
- 4. Hayes DF, Yamauchi H, Broadwater G, et al. Circulating HER-2/erbB-2/c-neu (HER-2) extracellular domain as a prognostic factor in patients with metastatic breast cancer: cancer and leukemia group B study 8662. Clin Cancer Res. 2001;7:2703–2711. [ PubMed ] [ Google Scholar ]
- 5. Wolff AC, Hammond MEH, Allison KH, et al. Human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline focused update. Arch Pathol Lab Med. 2018;142:1364–1382. doi:10.5858/arpa.2018-0902-SA [ DOI ] [ PubMed ] [ Google Scholar ]
- 6. Scholl AR, Flanagan MB. Invasive ductal carcinoma of the breast. Acad Pathol. 2020;7. doi:10.1177/2374289519897390 [ DOI ] [ PMC free article ] [ PubMed ] [ Google Scholar ]
- 7. Howlader N, Altekruse SF, Li CI, et al. US incidence of breast cancer subtypes defined by joint hormone receptor and HER2 status. J Natl Cancer Inst. 2014;106:dju055. doi:10.1093/jnci/dju055 [ DOI ] [ PMC free article ] [ PubMed ] [ Google Scholar ]
- 8. Evans DG, Lalloo F, Howell S, et al. Low prevalence of HER2 positivity amongst BRCA1 and BRCA2 mutation carriers and in primary BRCA screens. Breast Cancer Res Treat. 2016;155:597–601. doi:10.1007/s10549-016-3697-z [ DOI ] [ PubMed ] [ Google Scholar ]
- 9. Burstein HJ. The distinctive nature of HER2-positive breast cancers. N Engl J Med. 2005;353:1652–1654. doi:10.1056/NEJMp058197 [ DOI ] [ PubMed ] [ Google Scholar ]
- 10. Heitz F, Harter P, Lueck HJ, et al. Triple-negative and HER2-overexpressing breast cancers exhibit an elevated risk and an earlier occurrence of cerebral metastases. Eur J Cancer. 2009;45:2792–2798. doi:10.1016/j.ejca.2009.06.027 [ DOI ] [ PubMed ] [ Google Scholar ]
- 11. Romond EH, Perez EA, Bryant J, et al. Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer. N Engl J Med. 2005;353:1673–1684. doi:10.1056/NEJMoa052122 [ DOI ] [ PubMed ] [ Google Scholar ]
- 12. Arteaga CL, Sliwkowski MX, Osborne CK, et al. Treatment of HER2-positive breast cancer: current status and future perspectives. Nat Rev Clin Oncol. 2011;9:16–32. doi:10.1038/nrclinonc.2011.177 [ DOI ] [ PubMed ] [ Google Scholar ]
- 13. Hortobagyi GN, Connolly JL, D’Orsi CJ, et al. Breast. In: Amin MB, Edge S, Greene F, et al. , eds. AJCC Cancer Staging Manual. 8th ed. Springer; 2017:589–636. doi:10.1007/978-3-319-40618-3_48 [ Google Scholar ]
- View on publisher site
- PDF (490.9 KB)
- Collections
Similar articles
Cited by other articles, links to ncbi databases.
- Download .nbib .nbib
- Format: AMA APA MLA NLM
Add to Collections
- Open access
- Published: 26 October 2024
Associations of the Healthy Beverage Index (HBI) and the risk of Breast Cancer (BrCa): a case–control study
- Navideh Khodadadi 1 ,
- Mohammad Hassan Sohouli 3 ,
- Mojtaba Ghadiani 2 ,
- Hamid Rezvani 2 ,
- Mahdi Tabarraee 2 ,
- Hamid Reza Ahadi 2 ,
- Sina Salari 2 &
- Hamide Rahmani Seraji 2
BMC Women's Health volume 24 , Article number: 573 ( 2024 ) Cite this article
45 Accesses
7 Altmetric
Metrics details
Breast cancer (BrCa) is one of the leading causes of cancer-related deaths. There are several factors for getting BrCa, including some changeable factors related to lifestyle like unhealthy dietary patterns, so modifying them can prevent one third of the complications and deaths caused by BrCa. Therefore, we decided to investigate the relationship between Healthy Beverage Index (HBI) and the risk of BrCa.
In this hospital-based case–control study, 253 patients with BrCa and 267 non-BrCa controls were enrolled. Food consumption was recorded to calculate the HBI score using a semi-quantitative Food Frequency Questionnaire (FFQ). Additionally, by using binary logistic regression analysis with adjustment for confounders, the relationship between HBI and the risk of BrCa were assessed. HBI was established by Duffey et al. and is used to evaluate the overall quality of beverage intake and identify changes in consumption.
Mean ± SD of age and BMI of the study participants were 47.92 ± 10.33 years and 29.43 ± 5.51 kg/m 2 , respectively. Patients with BrCa considerably outperformed controls in terms of waist circumference (WC), age at first pregnancy, history of abortion, and number of children(Pvalue < 0.05). Compared with those in the lowest quartile of HBI, subjects in the highest quartile had higher intake of energy, carbohydrate, protein, fat, fiber, sodium, potassium, calcium, magnesium, zinc, vitamin C, E, B9, fruits, vegetables, fish and nut as well as lower BMI and WC (Pvalue < 0.05). After adjustment for potential confounders, individuals in highest compared to lowest quartile of HBI had significantly lower risk of BrCa for total population (odds ratio (OR): 0.40; 95% confidence interval (95%CI): 0.21–0.76, Pvalue < 0.05), premenopausal (OR: 0.38; 95% CI: 0.16–0.92, Pvalue = 0.013), and postmenopausal (OR: 0.27; 95% CI: 0.10–0.78, Pvalue = 0.023).
Findings of this study suggested that higher HBI score decreased the risk of BrCa. However, further investigation is needed.
Peer Review reports
Introduction
Breast cancer (BrCa), with nearly 2.3 million new cases in 2020, was the most often identified disease and the main cause of cancer-related deaths in women globally in 2018 [ 1 , 2 ]. There are several factors for getting BrCa, including some changeable factors related to lifestyle, the most important of which are physical inactivity [ 3 ] and dietary factors [ 4 ]. The most important modifiable risk factors for BrCa are unhealthy dietary patterns [ 5 , 6 ]. For instance, consuming enough and proper vegetables and soft drinks, industrially produced juices, fried meals, and sweets were found to be risk factors for BrCa [ 7 ]; as a result, altering dietary habits can avoid one third of the difficulties and fatalities brought on by BrCa [ 8 ]. In order to improve healthy beverage choices and effectively evaluate drinking patterns quality in adults, the Healthy Beverage Index (HBI) was developed [ 9 , 10 ].
The HBI can be utilized to identify the combined effects of numerous drinks as opposed to the marginal impact of a single drink on health outcomes [ 10 ]. It comprises fluid intake, eight beverage types, and beverage energy overall [ 10 ]. Drinks including milk, coffee, tea, and other unsweetened beverages might affect your overall health in a variety of ways [ 10 ]. In general, there are few evidences and studies about the potential effects of various types of drinks on the risk of developing chronic diseases, including breast cancer. In several studies, an increase in the risk of breast cancer and also the death rate was observed with sugar-sweetened beverages and even milk. However, in some evidences, no significant relationship was observed, and even in one study, replacing these types of drinks with tea, coffee, and drinking water did not show a significant effect on disease outcomes [ 11 , 12 , 13 ].
Due to the confusing nature of the literature and the fact that no study has specifically analyzed HBI in connection to BrCa risk, we set out to conduct the first ever study to look at the relationship between HBI and BrCa risk among Iranian women. Also, in this study, we examined food intake and other factors related to the disease between two groups of women under study, as well as the desired index quartiles.
Material & methods
Case-control research was used in this study. Two hundred and fifty-three persons with BrCa and two hundred and sixty-seven people without the illness were among the 520 participants in this study, who were chosen from Tehran’s Hazrat Rasool and Taleghani Hospitals during the years of 2018 and 2019. The minimal required sample size was calculated using the ability to detect an OR of 2 with a case to control ratio of 1 : 1, power of 90%, and a type I error ( \(\:\alpha\:\) ) rate of 5%.
A recent (within six months) diagnosis of BrCa was made by an oncologist in a patient with histologically proven BrCa. Our exclusion criteria included the presence of metastases, the history of previous malignancies, and hormone-related conditions such endometriosis or polycystic ovary syndrome (PCOS). The samples for control group did not have any history of cancer (benign and malignant), hormone-related and inflammatory diseases; they were chosen from other wards of hospitals like ophthalmology, otolaryngology, dermatology, and aesthetics. Also, they have had a regular diet for the past 6 months. The age and BMI matching was done between two groups. Furthermore, to ensure the absence of inflammation, an internal medicine specialist examined each member of this group, and also laboratory tests were done. We used a valid short form of the International Physical Activity Questionnaire (short IPAQ) to determine the level of physical activity of participants. The method of calculating the amount of physical activity in terms of MET-minutes/week was calculated as follows: Walking MET-minutes/week = 3.3 × Walking minutes × Walking days. Moderate MET-minutes/week = 4.0 × Moderate-intensity activity minutes × Moderate days. Vigorous MET-minutes/week = 8.0 × Vigorous-intensity activity minutes × Vigorous-intensity days. Total physical activity MET-minutes/week = Sum of Walking + Moderate + Vigorous METminutes/week scores.
Also, we obtained from all individuals an informed written consent.
Dietary assessment
A reliable semiquantitative food frequency questionnaire with 168 food items was utilized to measure food consumption in comparison to the previous year [ 14 ]. The main design element of this FFQ was to replicate normal Iranian cuisine with a standard serving size. For each dish, the participant filled out the FFQ to record how much of a regular quantity they typically ate and how many times they had consumed it. Each meal was consumed in the following ways: never, twice to three times per month, once per week, four to six times per week, and every day. Typical Iranian family measures were used to transform the portion sizes to gram [ 15 ]. The daily nutrient intakes for each patient were calculated using the national nutritional databank of the United States Department of Agriculture (USDA) [ 16 ]. To determine the consumption of daily nutrient and energy for each individual, Nutritionist IV software was applied.
Assessment of anthropometric variables
Standard techniques were used to acquire anthropometric data. The patients’ weights were determined while they were dressed comfortably and barefoot on a Seca digital scale (manufactured in Germany) with a precision of 100 g. Using a tape meter, standing height was measured with bare feet. The Body Mass Index (BMI) was determined by dividing the weight (kg) by the square of height (m2). The narrowest point of a non-elastic tape was used to measure waist circumference (WC) without applying pressure to the body’s surface.
Calculation of Healthy Beverage Index (HBI)
The Healthy Beverage Index (HBI) was established by Duffey et al. [ 10 ] and may be used, like the Healthy Eating Index, to evaluate the overall quality of beverage intake and identify changes in consumption. Health changes are connected to patterns. All beverages that were registered as beverages were split into eight kinds by the beverage guidance system. 100% fruit juice, water, unsweetened coffee and tea, low-fat milk, diet beverages (such as caffeine-free coffee and tea and other artificially sweetened beverages), alcohol (such as beer, wine, and spirits), and full-fat milk are all acceptable drinks. There were eight different types of drinks that people drank, including fruit drinks, sweet coffee and tea, and soft drinks. A higher number denotes better compliance with the drinking norm and a healthy drinking habit, and the final HBI score ranges from 0 to 100 [ 10 ]. Because our target group in this study did not use diet drinks (rated between 0 and 5) or alcohol (scoring between 0 and 5), the maximum final HBI score was 90. Because the goal of this study was to investigate adherence to healthy beverage intake recommendations rather than overall fluid intake, fluids ingested as part of a meal (such as soup) were eliminated.
Statistical analyses
We used SPSS software (version 19.0; SPSS Inc, Chicago IL) for all of our statistical analyses. The Shapiro-Wilk tests were used to assess the normality of the variables. For quantitative factors, the baseline characteristics and dietary intakes were presented as mean ± standard deviation (SD), and for qualitative variables, as a number and a percentage. Using independent sample T-Tests or, if necessary, its non-parametric counterpart (Mann-Whitney test) and chi-squared tests for continuous and categorical variables, respectively, we compared the data across two groups. Conditional logistic regression model was used to estimate odds ratios (ORs) and 95% confidence intervals (CIs) adjusted for multiple covariates in a different model and in all results, the significance level was determined as P < 0.05.
We adjusted the results in three models using a priori selected potential confounders, which included: model 1- age and BMI, model 2- additional adjustment for waist circumference, physical activity, and energy intake, model 3- the latter model plus first pregnancy age, number of children, history of abortion, hormone replacement therapy, use of NSAIDs drugs, and vitamin D supplementation. In adjusted models, confounders were used from statistical and conceptual approach respectively. In this way, the variables with Pvalue < 0.2 were considered as possible confounders and were entered into the logistic regression and the odds of getting cancer was investigated. Also, in the conceptual approach of adjusting confounders in the model 3, possible confounders were selected based on clinical concepts and based on past articles and added to other confounders.
Specifically, the case groups’ mean (SD) age and BMI were 48.91 (10.46) years and 29.61 (4.55) kg/m 2 , respectively, while the control groups’ mean age and BMI were 47.13 (10.08) years and 29.07 (5.39) kg/m 2 , respectively.
Table 1 displays the demographics, way of life, and medical background of research participants in the case and control groups. Patients with BrCa considerably outperformed controls in terms of waist circumference (WC), age at first pregnancy, history of abortion, and number of children(Pvalue < 0.05). Additionally, the case group’s average use of vitamin D supplements, HBI score, hormone replacement medication, and non-steroidal anti-inflammatory drugs (NSAIDs)drugs was much lower than that of the control group (Pvalue < 0.05). For other traits and factors, however, there were no appreciable distinctions between the case and control patients.
Table 2 shows the mean food consumption of the research participants based on the case and control groups. In comparison to controls, subjects with BrCa consumed more macronutrients (energy, carbohydrates, and fat) as well as saturated fatty acids (SFA), cholesterol, carbohydrates, sodium, folate, iron, sugar-sweetened beverages, grains, and starches, while consuming less protein, potassium, phosphorus, calcium, vitamin B12, and micronutrients antioxidants like zinc, magnesium, and vitamins E, C, and D (Pvalue < 0.05). The food intakes, anthropometric measurements, and lifestyle traits of study participants across HBI quartiles are displayed in Table 3 . Higher intakes of calories, carbohydrate, protein, fat, fiber, salt, potassium, calcium, magnesium, zinc, vitamin C, E, and B9, as well as reduced BMI and WC, were seen in patients in the highest quartile of HBI compared to those in the lowest quartile(Pvalue < 0.05). In addition, HBI score and physical activity level increased significantly during the index quartiles. Tukey’s test was used to compare food groups and nutrients two by two. The difference between quartiles 1 and 2, 1 and 3, 1 and 4, 2 and 3, 2 and 4, 3 and 4 for energy, potassium, calcium, zinc, magnesium, vitamin C, vitamin B12, and fruit was reported significant. The difference between quartiles 1 and 2, 1 and 3, 1 and 4, 2 and 4, 3 and 4 was significant for fiber, vitamin B9 and vegetables intake. The difference between quartiles 1 and 2, 1 and 3, 1 and 4, 2 and 4 for protein, the difference between quartiles 1 and 3, 1 and 4, 2 and 4 for vitamin D and the difference between quartiles 1 and 4, 2 and 4 for sodium intake were significant.
Table 4 presents the odds ratios (ORs) and 95% confidence intervals (CIs) for BrCa patients based on HBI. In the crude model, highest quartile of HBI scores compare to the lowest quartile, a decrease in the odds of BrCa was observed for the whole population of women (OR: 0.29; 95% CI: 0.17–0.50), premenopausal (OR: 0.30; 95% CI: 0.15–0.63), and postmenopausal women (OR: 0.20; 95% CI: 0.08–0.48). Furthermore, after additional adjusting for potential confounders in the final adjusted model, the reduction in the odds of BrCa remained significant (OR: 0.40; 95% CI: 0.21–0.76 for total population, OR: 0.38; 95% CI: 0.16–0.92 for premenopausal, and OR: 0.27; 95% CI: 0.10–0.78 for postmenopausal women).
Our findings showed a significant and potential relationship between HBI and reducing the odds of BrCa in Iranian women after adjusting for potential confounders. This potential relationship was also observed in women before and after menopause. Although it was slightly lower in pre-menopausal age than after menopause, this decrease in odds was observed.
Rare and contradictory studies on the relationship between several drinks and the risk of cancer, particularly BrCa, exist. For instance, one study found that drinking milk may raise the odds of developing BrCa [ 13 ], although no correlation was identified in another research [ 13 ]. Also, it was indicated that higher mortality of BrCa was associated with high intake of fruit juice as well as substituting coffee, tea, or water with sugar-sweetened beverages (SSB) was related with a reduced risk of mortality [ 12 ]. However, substituting SSB with other low or high calorie liquids, such as fruit juice, skim/low-fat, or whole milk, was not related with noticeably improved survival [ 12 ]. Additionally, higher coffee and tea consumption following BrCa diagnosis was associated with reduced all-cause mortality [ 11 ]. There are dietary factors related to the risk of BrCa, which are inconclusive. For instance, a diet high in fruits, vegetables, seafood, and olive oil may lessen the hazards associated with BrCa [ 17 ]. Juices, fried meals, and sweets made in factories may raise the risk of BrCa [ 7 ]. A significant prospective research by Fiolet et al. found that eating ultra-processed foods increased total cancer risk, particularly BrCa risk, among 104 980 individuals who were at least 18 years old [ 4 ]. According to population based prospective cohort study by, SSB was related with the risk of total cancer including BrCa [ 18 ]. Epidemiological findings regarding BrCa risk associated with beverage consumption are conflicting. According to Boyle et al.‘s meta-analysis, there is no link between drinking sweetened, carbonated beverages and the risk of cancer, especially BrCa [ 19 ]. According to Chen et al.‘s research, drinking milk or other dairy products does not significantly increase the odds of developing BrCa [ 13 ]. According to Dong et al.‘s meta-analysis of prospective cohort studies, increasing consumption of dairy products in general—not just milk—may be linked to a lower risk of BrCa [ 20 ]. In this investigation, we evaluate the relationship between HBI and the risk of BrCa. HBI may be used to identify the cumulative effects of numerous drinks rather than the marginal impact of a single drink on health outcomes since it can assess the quality of adult drinking behaviors [ 10 ]. It contains fluid intake, eight beverage types, and beverage energy overall [ 10 ]. In comparison to controls, BrCa patients exhibited considerably higher HBI scores, according to our research. Numerous research have been done on the connection between drinking a variety of drinks and the risk of brca, but to the best of our knowledge, this is the first study to assess the association between HBI and BrCa risk in Iranian women.
The findings of our study also showed that some micronutrients, including potassium, phosphorus, calcium, zinc, magnesium and vitamins E, C and D, received less in the case group compared to the control group. Studies suggest that lower intake of these micronutrients, which are usually associated with lower fiber intake, can increase and maintain weight and body fat mass. This accumulation and storage of fat in the body is usually associated with an increase and retention of estrogen in the tissues and can increase the risk of chronic diseases, especially hormone-related cancers such as BrCa [ 21 ]. Therefore, differences in these nutrients may be clinically impactful. Special attention should be paid to vitamin D, since it plays a key physiological role in the development and function of the mammary gland [ 22 ], although the literature remains conflicting regarding vitamin D status and the risk BrCa. For instance, a meta-analysis of 9 prospective studies suggests a 12% decrease in the risk of BrCa in postmenopausal women for each 5 ng/mL increase in 25(OH) D [ 23 ]. However, in a RCT including 36,282 postmenopausal women, a reduction in BrCa (in situ) was found for those patients who underwent 400 IU/d of vitamin D3 combined with 1000 mg/d of elemental calcium carbonate [ 22 ]. In our study, the control group reported higher use of vitamin D supplements compared to the case group (24.3% vs. 14.6%, p = 0.005). Nevertheless, due to the nature of our study design and the lack of control over the dosage across vitamin D supplements, we cannot infer that vitamin D supplements are protective for BrCa. Interestingly however, the Vitamin D and Omega-3 Trial (VITAL) represents ongoing research that may be able to elucidate the clinical magnitude of supplementing vitamin D in preventing cancer by addressing the effect of 2000 IU/d vitamin D3 with or without 1 g of omega-3 fatty acids in 25,871 healthy subjects.
The present study’s strong, comprehensive consideration models are one of its advantages. Additionally, since these individuals had just been diagnosed with the condition for a maximum of 6 months, it was far less likely that the sickness would have caused a change in their eating habits. The 168-item food frequency questionnaire that was employed in this study covers the majority of the foods that our study sample ate. Although this study is innovative, there are certain limitations that should be mentioned. Some confounders may not have been taken into account despite the possibility of confounders being taken into account in this study’s analysis. Although we discovered evidence of a link between HBI and BrCa, the retrospective methodology we used in this study prevented us from establishing causality of the observed correlations. Therefore, this finding has to be verified in further prospective investigations and RCTs. Additionally, data were gathered through self-reporting techniques, which are known to be linked to either excessive or inadequate reporting. However, by employing skilled interviewers and technologies with strong validation, we aimed to mitigate this. The statistical methodology was also suitable for reporting at the group level. Another research drawback might be the modest alterations in some dietary products between the time of the interview and before the diagnosis. The precise number of participants who altered their diet was excluded from the research, and we also looked at pre-diagnosis consumption for each food item. Finally, more studies based on solving these limitations and also with follow-up and a higher sample size are suggested.
We found that higher HBI was associated with reduced odds of BrCa in the overall female population as well as in pre- and postmenopausal age. In general, the dietary pattern reflected by this index can serve as a useful guide and recommendation for the prevention of chronic diseases, including breast cancer in women of different menopausal ages, and is of interest to specialists and other relevant experts and consultants.
Data availability
Data is available upon request from the corresponding author for the article due to privacy / ethical restrictions.
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Cancer J Clin. 2018;68(6):394–424.
Article Google Scholar
Shin S, Fu J, Shin W-K, Huang D, Min S, Kang D. Association of food groups and dietary pattern with breast cancer risk: a systematic review and meta-analysis. Clin Nutr. 2023;42(3):282–97.
Article PubMed Google Scholar
Loprinzi PD, Cardinal BJ, Smit E, Winters-Stone KM. Physical activity and breast cancer risk. J Exerc Sci Fit. 2012;10(1):1–7.
Fiolet T, Srour B, Sellem L, Kesse-Guyot E, Allès B, Méjean C, Deschasaux M, Fassier P, Latino-Martel P, Beslay M. Consumption of ultra-processed foods and cancer risk: results from NutriNet-Santé prospective cohort. bmj 2018, 360.
Romanos-Nanclares A, Toledo E, Gardeazabal I, Jiménez-Moleón J, Martínez-González M, Gea A. Sugar-sweetened beverage consumption and incidence of breast cancer: the Seguimiento Universidad De Navarra (SUN) Project. Eur J Nutr. 2019;58:2875–86.
Article PubMed CAS Google Scholar
Fernandez-Lazaro CI, Martínez-González MÁ, Aguilera-Buenosvinos I, Gea A, Ruiz-Canela M, Romanos-Nanclares A, Toledo E. Dietary antioxidant vitamins and minerals and breast cancer risk: prospective results from the SUN cohort. Antioxidants. 2021;10(3):340.
Article PubMed PubMed Central CAS Google Scholar
Marzbani B, Nazari J, Najafi F, Marzbani B, Shahabadi S, Amini M, Moradinazar M, Pasdar Y, Shakiba E, Amini S. Dietary patterns, nutrition, and risk of breast cancer: a case-control study in the west of Iran. Epidemiol Health 2019, 41.
Marzbani B, Nazari J, Najafi F, Marzbani B, Shahabadi S, Amini M, Moradinazar M, Pasdar Y, Shakiba E, Amini S. Dietary patterns, nutrition, and risk of breast cancer: a case-control study in the west of Iran. Epidemiol Health. 2019;41:e2019003.
Article PubMed PubMed Central Google Scholar
Parker MK, Davy BM, Hedrick VE. Preliminary Assessment of the healthy Beverage Index for US children and adolescents: a Tool to quantify the overall Beverage Intake Quality of 2- to 19-Year Olds. J Acad Nutr Dietetics. 2022;122(2):371–e383376.
Duffey KJ, Davy BM. The healthy beverage index is associated with reduced cardiometabolic risk in US adults: a preliminary analysis. J Acad Nutr Dietetics. 2015;115(10):1682–9. e1682.
Farvid MS, Spence ND, Rosner BA, Willett WC, Eliassen AH, Holmes MD. Post-diagnostic coffee and tea consumption and breast cancer survival. Br J Cancer. 2021;124(11):1873–81.
Farvid MS, Spence ND, Rosner BA, Chen WY, Eliassen AH, Willett WC, Holmes MD. Consumption of sugar-sweetened and artificially sweetened beverages and breast cancer survival. Cancer. 2021;127(15):2762–73.
Chen L, Li M, Li H. Milk and yogurt intake and breast cancer risk: a meta-analysis. Medicine 2019, 98(12).
Keshteli AH, Esmaillzadeh A, Rajaie S, Askari G, Feinle-Bisset C, Adibi P. A dish-based semi-quantitative food frequency questionnaire for assessment of dietary intakes in epidemiologic studies in Iran: design and development. Int J Prev Med. 2014;5(1):29.
PubMed PubMed Central Google Scholar
Ghafarpour M, Houshiar-Rad A, Kianfar H, Ghaffarpour M. The manual for household measures, cooking yields factors and edible portion of food. In.: Tehran: Keshavarzi Press; 1999.
Bowman SA, Friday JE, Moshfegh AJ. MyPyramid Equivalents Database, 2.0 for USDA survey foods, 2003–2004: documentation and user guide. US Department of Agriculture; 2008.
Toledo E, Salas-Salvadó J, Donat-Vargas C, Buil-Cosiales P, Estruch R, Ros E, Corella D, Fito M, Hu FB, Arós F. Mediterranean diet and invasive breast cancer risk among women at high cardiovascular risk in the PREDIMED trial: a randomized clinical trial. JAMA Intern Med. 2015;175(11):1752–60.
Chazelas E, Srour B, Desmetz E, Kesse-Guyot E, Julia C, Deschamps V, Druesne-Pecollo N, Galan P, Hercberg S, Latino-Martel P. Sugary drink consumption and risk of cancer: results from NutriNet-Santé prospective cohort. bmj 2019, 366.
Boyle P, Koechlin A, Autier P. Sweetened carbonated beverage consumption and cancer risk. Eur J Cancer Prev. 2014;23(5):481–90.
Dong J-Y, Zhang L, He K, Qin L-Q. Dairy consumption and risk of breast cancer: a meta-analysis of prospective cohort studies. Breast Cancer Res Treat. 2011;127:23–31.
Li Y, Li S, Meng X, Gan R-Y, Zhang J-J, Li H-B. Dietary natural products for prevention and treatment of breast cancer. Nutrients. 2017;9(7):728.
Cauley JA, Chlebowski RT, Wactawski-Wende J, Robbins JA, Rodabough RJ, Chen Z, Johnson KC, O’Sullivan MJ, Jackson RD, Manson JE. Calcium plus vitamin D supplementation and health outcomes five years after active intervention ended: the women’s Health Initiative. J Women’s Health. 2013;22(11):915–29.
Bauer SR, Hankinson SE, Bertone-Johnson ER, Ding EL. Plasma vitamin D levels, menopause, and risk of breast cancer: dose-response meta-analysis of prospective studies. Medicine. 2013;92(3):123.
Download references
Acknowledgements
We express our appreciation to the participants of this study.
No funding.
Author information
Authors and affiliations.
Department of Clinical Nutrition and Dietetics, Faculty of Nutrition Science and Food Technology, Shahid Beheshti University of Medical Sciences, Tehran, Iran
Navideh Khodadadi
Department of Hematology and Oncology, Taleghani Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran
Mojtaba Ghadiani, Hamid Rezvani, Mahdi Tabarraee, Hamid Reza Ahadi, Sina Salari & Hamide Rahmani Seraji
Pediatric Gastroenterology and Hepatology Research Center, Pediatrics Centre of Excellence, Children’s Medical Center, Tehran University of Medical Sciences, Tehran, Iran
Mohammad Hassan Sohouli
You can also search for this author in PubMed Google Scholar
Contributions
N.K., and Mh.S contributed in conception, design, and statistical analysis. Mh.S., N.K., M.G., H.R., M.T, HR.A., S.S, and H.RS contributed in data collection and manuscript drafting. Mh.S. and H.RS supervised the study. All authors approved the final version of the manuscript.
Corresponding authors
Correspondence to Mohammad Hassan Sohouli or Hamide Rahmani Seraji .
Ethics declarations
Ethics approval and consent to participate.
This study was approved by the research council and ethics committee Shahid Beheshti University of Medical Sciences, Tehran, Iran. The lead author affirms that this manuscript is an honest, accurate and transparent account of the study being reported. The reporting of this work is compliant with high-quality qualitative research methodology. All methods were carried out in accordance with STROBE guidelines and regulations. Also, we confirm that all experiments were performed in accordance with relevant guidelines and regulations (such as the Declaration of Helsinki).
Informed consent
A written informed consent was obtained from all participants.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/ .
Reprints and permissions
About this article
Cite this article.
Khodadadi, N., Sohouli, M.H., Ghadiani, M. et al. Associations of the Healthy Beverage Index (HBI) and the risk of Breast Cancer (BrCa): a case–control study. BMC Women's Health 24 , 573 (2024). https://doi.org/10.1186/s12905-024-03411-6
Download citation
Received : 04 July 2023
Accepted : 14 October 2024
Published : 26 October 2024
DOI : https://doi.org/10.1186/s12905-024-03411-6
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Breast cancer
- Healthy beverage index
- Case-control
BMC Women's Health
ISSN: 1472-6874
- General enquiries: [email protected]
An official website of the United States government
Official websites use .gov A .gov website belongs to an official government organization in the United States.
Secure .gov websites use HTTPS A lock ( Lock Locked padlock icon ) or https:// means you've safely connected to the .gov website. Share sensitive information only on official, secure websites.
- Publications
- Account settings
- Advanced Search
- Journal List
Inflammatory Breast Cancer: A Case Report
Zacharoula sidiropoulou, lurdes ramalho, rosa madureira.
- Author information
- Article notes
- Copyright and License information
*Zacharoula Sidiropoulou, MD Senology Department Hospital N. S. Rosário Av. Forças Armadas, P-2830-094 Barreiro, Portugal [email protected]
Issue date 2009 Dec.
Inflammatory breast cancer is a rare, yet controversial, syndrome of invasive breast cancer.
Case Report
A female, Caucasian, 57-year-old patient presented at the emergency department with complaints suggestive of inflammatory breast cancer.
Conclusions
Inflammatory breast cancer, besides the advances on its molecular profile, still remains a clinical entity difficult to diagnose, especially in the primary health care setting.
Key Words: Breast cancer; locally advanced, metastatic; Bone metastasis; Differential diagnosis; Inflammation
Zusammenfassung
Hintergrund.
Das inflammatorische Mammakarzinom ist ein seltenes und gleichzeitig kontroverses Syndrom der invasiven Brustkrebserkrankungen.
Fallbericht
Eine 57-jährige Patientin weiβer Hautfarbe wurde in der Notaufnahme mit Beschwerden vorstellig, die auf ein inflammatorisches Mammakarzinom hindeuteten.
Schlussfolgerungen
Abgesehen von Fortschritten bezüglich seines molekularen Profils ist das inflammatorische Mammakarzinom nach wie vor eine schwierig zu diagnostizierende klinische Entität, besonders in der primären medizinischen Versorgung.
Introduction
Inflammatory breast cancer is a rare syndrome of invasive breast cancer that is characterized by erythema and oedema of a third or more of the skin of the breast, with a palpable border to the erythema, and no palpable breast mass. The differential diagnosis includes cellulites of the breast or mastitis. Pathologically, tumour tissue is typically present in the dermal lymphatics of the involved skin, but dermal lymphatic involvement is neither required nor sufficient by itself for the diagnosis of inflammatory breast cancer [ 1 ].
A female, Caucasian, 57-year-old obese patient presented at the emergency department of our hospital and reported that 1 year ago she had felt a small lump in her breast; over the last 2 months the breast had become much bigger, heavy, itchy, and hot, and had taken on a cellulites-like appearance. She also complained of pain in her right leg, which she had been treating over the last months with acupuncture and homeopathic drugs, but with no results. Her anamnesis included G3P3, menarche at 11 years, and menopause at 46. All 3 children were breastfed for 12 months, and were all healthy. The patient's mother and 2 maternal aunts died of pre-menopausal breast cancer. No other important anamnestic data or former medical visits were reported.
Clinical examination revealed obesity, urinary and faecal incontinence, and paralysis of both lower limbs. The left breast showed widespread erythema and intense oedema with peau d'orange, and was augmented in size with an enormous and ill-defined mass with areolar erosion (fig. 1 .) and axillary pathological node involvement. A total body computed tomography scan revealed C1, L2, and L3 lytic lesions with medullar compression, and multiple disseminated lytic foci in cranial, chest, arm, and leg bones. No other secondary deposits were observed (figs. 2 and 3 ). A tru-cut biopsy of the breast, a fine needle aspiration biopsy of the axillary nodes, and a biopsy of the skin of the breast were performed immediately and all revealed ductal invasive carcinoma, GII, oestrogen and progesterone receptor-positive, and HER2/neu-positive, with dermal invasion and absence of lymphatic emboli (fig. 4 ). Tumour markers were as follows: CEA, 47.5 ng/ml; CA 15.3, 25.3 U/ml; CA 19.9, 58.4 U/ml; CA 125 normal. All other parameters including renal and liver function were normal. The patient was transferred to the oncology department, and after being presented to the breast committee, was started on analgesics, a biphosphonate protocol, and spinal column palliative radiotherapy. At present, the patient is receiving psychological care and physiotherapy. The treatment plan to be followed includes aromatase inhibitor (letrozole) and trastuzumab/chemotherapy protocols. At a later stage, a ‘cleaning mastectomy’ versus breast radiotherapy will be considered.

Left breast with oedema, erythema, peau d'orange and nipple areolar complex involvement.

Computed tomography scan of cervix.

Computed tomography scan of lumbar spine.

Dermal invasion without lymphatic involvement.
Inflammatory breast cancer is an aggressive and poorly understood disease with symptoms that differ from other types of breast cancer. At the time of diagnosis, most women have lymph node metastases, and roughly one third will have distant metastases. It accounts for an estimated 2% of breast cancer diagnoses in the U.S., but for 7% of breast cancer deaths [ 1 ].
The classic and clinical description was provided by Tannenbaum and Lee in 1924 when they cited: ‘The rate of growth is startling in its rapidity and often fills the entire breast in a few weeks … the overlying skin is reddened and brawny and its blush may extend far beyond the limits of the mammary gland … the inflamed area presents a distinct raised periphery after the fashion of erysipelas. The infiltration is so marked that the examiner, with his eyes closed, can distinguish readily the sharp contrast between normal and affected tissue’ [ 6 ]. In 1938, Taylor and Meltzer divided the inflammatory breast cancer in 2 distinct categories, primary and secondary, based on whether we deal with an ad hoc nosologic entity in the first case or with a locally advanced cancer that presents inflammatory signs in the second one [ 7 ].
According to the pathologic findings, the major determinant of this tumour entity is the dermal lymphatic invasion by carcinoma, but this invasion does not consist in a sine qua non condition. The diagnosis of this nosologic entity still relies on clinical features, and several centres have proposed various end points, like for example the one cited by the M.D. Anderson Cancer Center: ‘… our diagnostic criteria for primary breast cancer include clinical evolution shorter than 3 months’.
This specific case is a typical controversial case because there is still disagreement over whether it can be classified as primary or secondary inflammatory breast cancer [ 2 , 3 ]. Besides the clinical features present (oedema, peau d'orange, and erythema developed over a short period of 2 months) and the absence of a concrete palpable mass, no dermal lymphatic invasion was detected in the histological examination and there is a history of a long-standing uncharacterized breast lump and areolar-nipple invasion. Whether we are dealing with a primary inflammatory breast carcinoma with secondary local invasion, or with secondary inflammatory breast cancer due to local invasion of a primary lump, the finding of oestrogen receptor positivity was quite surprising [ 4 ]. Independent of its classification, in this specific case, we are dealing with TNM stage IV metastatic disease.
Inflammatory breast carcinoma still remains a challenging issue with regard to diagnosis and treatment. Its differentiation into primary and secondary disease needs to be more clarified since the two forms entail distinct management and prognosis. Recent inflammatory breast carcinoma research has examined two genes, RhoC GTPase and WISP3, which are concordantly altered in the majority of inflammatory breast tumours but not in non-inflammatory specimens [ 5 ]. A better definition of the clinical features of inflammatory breast cancer needs to be achieved. Currently ongoing clinical trials aim at a better understanding and differentiation of this rare but extremely aggressive type of breast cancer.
Conflict of Interest
The authors declare that they have no competing interests.
Acknowledgement
We thank Paula Vasconcelos and Ana Rios for their contribution to the immediate radiological staging of the patient.
- 1. Merajver SD, Sabel MS. Inflammatory breast cancer. In: Harris JR, Lippman ME, Morrow M, Osborne CK, editors. Diseases of the Breast. 3rd ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2004. pp. 971–982. [ Google Scholar ]
- 2. Lerebours F, Bieche I, Lidereau R. Update on inflammatory breast cancer. Breast Cancer Res. 2005;7:52–58. doi: 10.1186/bcr997. [ DOI ] [ PMC free article ] [ PubMed ] [ Google Scholar ]
- 3. Giordano SH, Hortobagyi GN. Inflammatory breast cancer: clinical progress and the main problems that must be addressed; review. Breast Cancer Res. 2003;5:284–288. doi: 10.1186/bcr608. [ DOI ] [ PMC free article ] [ PubMed ] [ Google Scholar ]
- 4. Silva O, Zurrida S. A Practical Guide. 3rd ed. Edinburgh: Elsevier Saunders; 2005. Breast Cancer; p. 236. [ Google Scholar ]
- 5. Houchens NW, Merajver SD. Molecular determinants of the inflammatory breast cancer phenotype. Oncology (Williston Park) 2008;22:1556–1561. [ PubMed ] [ Google Scholar ]
- 6. Lee BJ, Tannenbaum NE. Inflammatory carcinoma of the breast: a report of twenty-eight cases from the breast clinic of Memorial Hospital. Surg Gynecol Obstet. 1924;39:580–595. [ Google Scholar ]
- 7. Taylor GW, Meltzer A. Inflammatory carcinoma of the breast. Am J Cancer. 1938;33:33–49. [ Google Scholar ]
- View on publisher site
- PDF (214.7 KB)
- Collections
Similar articles
Cited by other articles, links to ncbi databases.
- Download .nbib .nbib
- Format: AMA APA MLA NLM
Add to Collections
- Around the Practice
- Between the Lines
- Contemporary Concepts
- Readout 360
- Insights from Experts at Mayo Clinic on Translating Evidence to Clinical Practice
- Optimizing Outcomes in Patients with HER2+ Metastatic Breast Cancer

- Conferences
- Publications
- Career Center
Clinical Case Presentation: A 36-Year-Old Woman with Breast Cancer and Brain Metastases
- Ruta Rao, MD
Ruta Rao, MD, presents the case of a 36-year-old woman with metastatic HER2+ breast cancer and brain metastases.

EP: 1 . Clinical Case Presentation: A 36-Year-Old Woman with Breast Cancer and Brain Metastases

EP: 2 . Treatment Options in the Frontline Setting for Metastatic HER2+ Breast Cancer
EP: 3 . Second-Line and Third-Line Treatment Options for Metastatic HER2+ Breast Cancer
Ep: 4 . tucatinib for metastatic her2+ breast cancer and brain metastases: patient selection, ep: 5 . treatment options for her2+ breast cancer after progression on tucatinib, ep: 6 . clinical case presentation: a 53-year-old woman with metastatic er/pr+ her2+ breast cancer and brain metastases, ep: 7 . neratinib for metastatic her2+ breast cancer and brain metastases, ep: 8 . leptomeningeal metastases in her2+ breast cancer, ep: 9 . novel agents under evaluation for her2+ breast cancer and brain metastases, ep: 10 . clinical case presentation: a 66-year-old woman with er+ her2+ invasive ductal carcinoma and brain metastases, ep: 11 . trastuzumab deruxtecan treatment for metastatic her2+ breast cancer with brain metastases, ep: 12 . role of neurooncologists in management of her2+ breast cancer and brain metastases.
EP: 13 . Recap: Updates in Treatment of HER2-Positive Breast Cancer and Brain Metastases

Bria-IMT Regimen Exceeds Survival Data of SOC in Metastatic Breast Cancer
Four of 13 patients with metastatic breast cancer recruited in 2022 for the phase 2 clinical study evaluating Bria-IMT remain in survival follow-up.

Applying Updated Breast Cancer Findings From ASCO to Clinical Practice
Neil M. Iyengar, MD, and Paolo Tarantino, MD, discuss updated data on agents such as T-DXd and abemaciclib in breast cancer presented at 2024 ASCO.

Ultra-Hypofractionated RT Shows Control, Tolerability in Elderly Breast Cancer
Bin Gui, MD, discussed how ultra-hypofractionated radiotherapy may be a convenient treatment option for elderly patients with early breast cancer.
Finding a Place for Exercise Oncology in the Treatment of Breast Cancer
Neil M. Iyengar, MD, spoke about the potential impact of exercise on patient-reported outcomes in cancer and achieving work-life balance.

Gene Expression Test May Predict Added Atezolizumab Benefit in TNBC
Phase 2 data indicate that the use of DetermaIO was predictive of a pathologic complete response with the addition of immunotherapy to chemotherapy in TNBC.

Elacestrant Combo Shows Activity, Tolerability in Metastatic Breast Cancer
Investigators report no grade 4 adverse effects among patients who received elacestrant/abemaciclib in the phase 1b/2 ELECTRA trial.
2 Commerce Drive Cranbury, NJ 08512
609-716-7777

CASE REPORT article
Case report: a case study documenting the activity of atezolizumab in a pd-l1-negative triple-negative breast cancer.

- 1 Translational Genomics and Targeted Therapies in Solid Tumors, August Pi i Sunyer Biomedical Research Institute (IDIBAPS), Barcelona, Spain
- 2 Department of Medical Oncology, Hospital Clínic of Barcelona, Barcelona, Spain
- 3 Cancer Genomics Group, Vall d’Hebron Institute of Oncology, Barcelona, Spain
- 4 Department of Oncology and Hematology, Health Research Institute of the Balearic Islands (IdISBa), Palma de Mallorca, Spain
- 5 Department of Pathology, Hospital Clínic de Barcelona, Barcelona, Spain
- 6 Department of Pharmacy, Hospital Clínic of Barcelona, Barcelona, Spain
- 7 Department of Radiology, Hospital Clínic of Barcelona, Barcelona, Spain
- 8 Molecular Biology Core, Hospital Clinic of Barcelona, Barcelona, Spain
- 9 Vall d’Hebron University Hospital and Vall d’Hebron Institute of Oncology (VHIO), Medical Oncology Service, Barcelona, Spain
- 10 SOLTI Cooperative Group, Barcelona, Spain
- 11 Department of Oncology, Institut Oncològic Baselga (IOB) Institute of Oncology, Quironsalud Group, Barcelona, Spain
- 12 Department of Medicine, University of Barcelona, Barcelona, Spain
The immune checkpoint inhibitor atezolizumab is approved for PD-L1-positive triple-negative breast cancer (TNBC). However, no activity of atezolizumab in PD-L1-negative TNBC has been reported to date. Here, we present the case study of a woman with TNBC with low tumor infiltrating lymphocytes and PD-L1-negative disease, which achieved a significant response to atezolizumab monotherapy and durable response after the combination of atezolizumab and nab-paclitaxel. The comprehensive genomic analysis that we performed in her tumor and plasma samples revealed high tumor mutational burden (TMB), presence of the APOBEC genetic signatures, high expression of the tumor inflammation signature, and a HER2-enriched subtype by the PAM50 assay. Some of these biomarkers have been shown to independently predict response to immunotherapy in other tumors and may explain the durable response in our patient. Our work warrants further translational studies to identify biomarkers of response to immune checkpoint inhibitors in TNBC beyond PD-L1 expression and to better select patients that will benefit from immunotherapy.
Introduction
Triple-negative breast cancer (TNBC) lacks expression of estrogen receptor (ER), progesterone receptor (PR), and the human epidermal growth factor receptor 2 (HER2); accounts for 15%–20% of all breast cancers; affects young women; and is highly aggressive. While targeted therapies are available for ER-positive (ER+) and HER2-positive (HER2+) breast cancer, chemotherapy remains the standard of care for TNBC. Among the different subtypes, TNBC is the most immunogenic and has the highest median number of tumor-infiltrating lymphocytes (TILs), PD-L1 expression, and tumor mutational burden (TMB), all of which are associated with immune activity ( 1 ). In this context, immunotherapy with atezolizumab, an anti-PD-L1 drug antibody, has been approved for PD-L1-positive (PD-L1+) (i.e., ≥1% PD-L1+ tumor-infiltrating immune cells) advanced TNBC in combination with nab-paclitaxel ( 2 ). On the other side, activity of pembrolizumab monotherapy in patients with pre-treated metastatic breast cancer with high TMB has recently been reported ( 3 ). However, no activity of immune checkpoint inhibitors in PD-L1-negative TNBC has been observed to date, and the predictive value of TMB beyond PD-L1 expression is still unknown.
Here, we describe a case of a woman with an initial diagnosis of HER2+ localized tumor treated with curative therapy that relapsed 9 years later being an ER+/HER2-negative metastatic breast cancer. She progressed to first-line endocrine therapy and palbociclib, a CDK4/6 inhibitor, and whose tumor became then triple-negative. Molecular characterization of her metastatic TNBC observed absence of PD-L1 expression, but high TMB, presence of the Apolipoprotein B mRNA Editing Catalytic Polypeptide-like (APOBEC) genetic signatures, high expression of the tumor inflammation signature (TIS), and a HER2-enriched subtype by the PAM50 assay. Based on this tumor profile, Hospital Clinic Molecular Tumor Board indicated one cycle of atezolizumab followed by atezolizumab in combination with nab-paclitaxel. Plasma circulating tumor DNA (ctDNA) and radiological imaging were used to assess treatment efficacy. The patient presented in this report has given her consent for publication.
Case Presentation
A 44-year-old white Spanish woman with no significant familiar or medical history was initially diagnosed with a left breast cancer in 2008 (pT2N3M0). The pathology report revealed an ER+, PR-positive, and HER2+ invasive carcinoma of the breast. She underwent surgery in October 2008 and received adjuvant anti-HER2-based chemotherapy, followed by locoregional radiotherapy and endocrine therapy.
In April 2018, the patient was diagnosed with right supraclavicular and axillary positive lymph nodes (17 mm and 3 mm) by ultrasound. Bone metastasis was detected by PET/CT scan. A core biopsy of the right supraclavicular lymph nodes was performed and revealed an ER+ and HER2-negative invasive lobular carcinoma. In this tumor biopsy, an amplicon-based DNA sequencing panel of pan-cancer genes showed the presence of a PIK3CA E545K (18% mutant allelic frequency [MAF]) and 726F (16% MAF) somatic mutations. As a first-line treatment, she received fulvestrant and palbociclib (125 mg daily, 3 weeks on, 1 week off) until May 2019 (13 months of treatment), when bone and lymph node progressions were observed.
Two new biopsies of the right breast and axillary node were performed and revealed a TNBC lobular carcinoma. In the breast lesion, the tumor had a Ki67 of 18% and less than 1% TILs and was PD-L1-negative by immunohistochemistry (Ventana PD-L1 antibody clone SP142). Intrinsic subtype by PAM50/Prosigna ® revealed a HER2-enriched subtype with low levels of ERBB2 mRNA. A DNA sequencing panel of 431 genes showed PIK3CA E545K and TP53 Q331* mutations, a high TMB of 38.5 mutations per megabase (mut/Mb) and an APOBEC-mutational profile, including signatures S2 and S13. Guardant360 74-gene panel confirmed the presence of multiple somatic mutations, including PIK3CA E545K mutation with a variant allele fraction of 12.2%.
Based on these results, the clinical case was presented at our weekly multidisciplinary Tumor Board at Hospital Clinic of Barcelona. Since activity of immunotherapy in patients with breast cancer with high TMB has been reported ( 3 ), a regimen of single-agent immunotherapy combined with chemotherapy was planned. More specifically, in July 2019, the patient received one dose of 1200 mg atezolizumab monotherapy and after 3 weeks continued with 1200 mg atezolizumab (day 1) plus weekly 100 mg/m 2 nab-paclitaxel. In August 2021 (24 months of treatment), the patient continues on treatment presenting a maintained partial response and an excellent performance status. The treatment history is summarized in Figure 1A .

Figure 1 Patient treatment timeline and DNA alterations. (A) Patient treatment timeline. (B) Mutant Allelic Frequency (MAF; %) in T1 (sample of 2008), T2 (sample of 2018), and T2-PD (sample of 2019) determined using the VHIO-300 panel. Variants classified as pathogenic or likely pathogenic are highlighted in bold; variants matching APOBEC DNA-sequence signature are underlined. (C) Overlap of somatic mutations between T1, T2, and T2-PD using the VHIO-300 panel and whole-exome sequencing (WES). (D) TMB expressed as mutations/megabase in T1, T2, and T2-PD using the VHIO-300 panel and WES. (E) COSMIC mutational signatures of age, APOBEC defect (APOBEC), defective mismatch repair/microsatellite instability (dMMR/MSI) reflected as small insertions and deletions (INDELs), ultraviolet light (UV), polymerase E defect (POLE), and aflotoxin effect in T1, T2, and T2-PD determined by WES. (F) MAF distribution for APOBEC-related and other mutations in T1, T2, and T2-PD determined by WES.
Genomic Analyses
Analysis of the DNA from the three tumor specimens and a buffy coat blood sample by next-generation sequencing using the VHIO-300 capture-based panel of 431 pan-cancer related genes and whole-exome sequencing (WES) revealed an independent genetic origin of samples from 2008 and 2018, while the tumor from 2019 clearly was a progression (PD) of the 2018 lesion. Thus, samples were relabeled as T1 (breast sample, 2008), T2 (lymph node sample, 2018), and T2-PD (breast sample, 2019). Genomic analyses revealed a completely different mutational profile of T1 versus T2 and T2-PD; the vast majority of mutations in T2 were also present in T2-PD, while none of them were present in T1, and 34 somatic variants were found exclusively in T2-PD (e.g., RB1 S567* and a nonsense NF1 mutation in residue Q315*) ( Figures 1B, C ). In addition, TMB was low in T1 compared to T2 and T2-PD ( Figure 1D ). Analysis of COSMIC mutational signatures from the WES results showed a dominant pattern related to age in T1, while the high TMB in T2 and T2-PD was linked to a sequence context preference of cytosine mutations caused by APOBEC enzymes ( 4 ) ( Figure 1E ). Finally, a study of MAF distribution showed a clonal peak for APOBEC-related mutations in T2, with increased average MAF % in T2-PD, plus a second peak of subclonal mutations also linked to APOBEC defect in the T2-PD ( Figure 1F ).
RNA from T2 and T2-PD were analyzed at the nCounter Breast Cancer 360 Panel. ESR1 expression was decreased in T2-PD compared to T2, consistent with the immunohistochemistry results. Both T2 and T2-PD were classified as HER2-enriched and showed high expression of immune signatures (i.e., MHC-II, IFN-gamma, TIS, antigen presenting machinery) ( Figure 2A ). PD-L1 and PD1 mRNA expression was low.

Figure 2 Gene expression and molecular and clinical response to atezolizumab and nab-paclitaxel. (A) The Wheel Plots depict the relative expression of each signature for T2 and T2-PD samples determined using the Breast Cancer 360 nCounter-based gene expression panel. Signatures are grouped based on the biological process in which they belong. The Luminal A, Luminal B, HER2-enriched, and Basal-like subtype correlation scores are shown as a radial arc. Signature scores (0–16, low to high) are represented as radial projections. (B) Guardant360 Tumor Response Map showing the highest variant allele fraction (%) and MAF (%) assessed in ctDNA using Guardant360 results before treatment, after 3 weeks of atezolizumab monotherapy, and after combining atezolizumab and nab-paclitaxel. (C) CT scan. Red arrows indicate lesions on the soft tissue of the chest wall (top) and a mammary node (middle) and bone (bottom) during treatment.
Since ctDNA can be a surrogate of response to therapy and long-term outcome ( 5 ), liquid biopsies were collected before atezolizumab, after 3 weeks of atezolizumab monotherapy and after 3 weeks of atezolizumab plus nab-paclitaxel. Plasma samples were sequenced using the standardized Guardant360 assay. Mutations in 37 genes were identified in the plasma sample before immunotherapy and highest variant allele frequency (VAF) was 12.2%. After atezolizumab monotherapy, the only detectable mutation was PDGFRA D691E (VAF = 0.1%). After 1 month of atezolizumab plus nab-paclitaxel, the only mutation detected was ALK R1061Q (VAF = 0.5%) ( Figure 2B ), and after 2 months, a chest CT scan confirmed a partial response as observed on the soft tissue of the chest wall and a mammary node, and in December 2020, the patient continued in clinical and radiological response ( Figure 2C ). Bone metastasis was followed up by CT scan every 3 months, with stable disease as the best response.
Acquisition of genomic alterations and changes in gene expression profiles may lead to treatment failure and disease progression. Here, we report a patient diagnosed of ER+/HER2-negative metastatic breast cancer who progressed to first-line endocrine therapy in combination with CDK4/6 inhibition, and the progressive disease lost ER expression and became TNBC; it was PD-L1-negative and benefited from atezolizumab in combination with nab-paclitaxel. Although our study cannot identify the main cause of the patient’s response to atezolizumab alone and in combination with nab-paclitaxel, the extensive molecular characterization performed could provide clues about the features associated with immunotherapy benefit in PD-L1-negative TNBC.
The genomic analysis performed revealed that the pre-treatment ER+/HER2-negative tumors and the progression tumor samples after endocrine therapy and palbociclib had the following features: (1) high TMB, (2) presence of the APOBEC genetic signatures, (3) HER2-enriched, and (4) high expression of immune gene signatures such as TIS or interferon-gamma but not PD-L1 or PD1 mRNA. However, some molecular features were different between the two time points. For example, NF1 and RB1 mutations and lower expression of ER were identified in the progression sample, which also had a higher TMB score. Consistently, loss of ER and acquisition of NF1 mutations have been associated with resistance to endocrine therapy ( 6 ), while acquisition of RB1 mutations, APOBEC signatures, and the HER2-enriched subtype has been associated with resistance to palbociclib ( 7 , 8 ). Moreover, the APOBEC genetic signatures have been previously associated with the HER2-enriched subtype and high TILs ( 9 , 10 ). Indeed, APOBEC genetic signatures contribute to the acquisition of subclonal mutations, leading to genomic instability and potential neoantigens expression, which could induce immune response ( 11 ). The genetic origin of the APOBEC signatures in this case remains unknown. Among the possible explanations, we excluded germline loss of APOBEC3B ( 12 ). Unfortunately, we were not able to study the expression levels of APOBEC3B ( 13 ).
Currently, three biomarkers have been clinically validated as predictors of response to immune checkpoint blockade in TNBC [i.e., PD-L1 ( 2 )] and across cancer types (i.e., TMB ( 3 , 14 ) and mismatch repair deficiency ( 15 ). Indeed, the immunotherapy drug pembrolizumab for the treatment of patients with TMB-high tumors is approved by the Food and Drug Administration (FDA) ( 14 ). In TNBC, a modest benefit of immune checkpoint blockade has been observed in patients who are PD-L1-positive ( 2 ), which has led to the approval of the combination of atezolizumab plus nab-paclitaxel in PD-L1+ TNBC by the FDA. Other suggested predictive factors of response to immune checkpoint blockade include the TIS score ( 16 ), the APC signature ( 17 ), PD1 mRNA expression ( 18 ), and a T cell–inflamed gene expression profile ( 19 ). Some of these biomarkers have been shown to independently predict response to immunotherapy and may capture distinct features of neoantigenicity. Therefore, composite biomarkers may help better identify those patients that benefit to immune checkpoint inhibition and warrant further translational studies to improve patient selection.
To conclude, we present the case study of a TNBC with low TILs and PD-L1-negative disease, which achieved a significant response to atezolizumab monotherapy and durable response after the combination of atezolizumab and nab-paclitaxel, possibly explained by the APOBEC signatures, the high TMB, the high TIS score, and the HER2-enriched subtype, or the combination of several of these features. Moreover, the addition of chemotherapy could have helped turn the cold tumor microenvironment into hot, recruiting more T cells and improving response to atezolizumab ( 20 ). After 24 months, the patient continues in clinical and radiological response.
Patient Perspective
After progression to first-line treatment (palbociclib + ET), the patient is really satisfied with a 24-month response to a well-tolerated scheme of atezolizumab plus weekly nab-paclitaxel with just alopecia G1 (she is using a cold cap to prevent it) and hepatotoxicity G2 that has been recovered just to delay treatment 1–2 weeks three times during these 2 years. She maintains an active life with ECOG 0.
Data Availability Statement
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding authors.
Ethics Statement
The studies involving human participants were reviewed and approved by Comité de Ética de la Investigación con medicamentos del Hospital Clínic de Barcelona. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author Contributions
Experimental study design: FB-M, MiS, AP, and AV. Provision of study materials or patients: FB-M, MiS, NC, DM, BG-F, ES, LG, EC, JG-C, MaS, DS, VP, CS, MM, AP, and AV. Data analysis and interpretation: FB-M, MiS, NC, MM, AP, and AV. Writing of the manuscript FB-M, MiS, AP, and AV. Revision of the manuscript: FB-M, MiS, NC, DM, BG-F, ES, LG, EC, JG-C, MaS, DS, VP, P-J, CS, MM, AP, and AV. Supervision: AP and AV. All authors contributed to the article and approved the submitted version.
This study has received funding from Instituto de Salud Carlos III—PI19/01846 (to AP), Breast Cancer Now—2018NOVPCC1294 (to AP), Breast Cancer Research Foundation-AACR Career Development Awards for Translational Breast Cancer Research 19-20-26-PRAT (to AP), Fundació La Marató TV3 201935-30 (to AP), the European Union’s Horizon 2020 research and innovation programme H2020-SC1-BHC-2018-2020 (to AP), Asociación de Cáncer de Mama Metastásico CMM_CHIARAG19_001 (to AP), Pas a Pas (to AP), Save the Mama (to AP), Fundación Científica Asociación Española Contra el Cáncer AECC_Postdoctoral17-1062 (to FB-M) and INVES19056SANS (to MiS), FERO-ghd 2020 breast cancer award (MS), and Generalitat de Catalunya Peris PhD4MD 2019 SLT008/18/00122 (to NC).
Conflict of Interest
Potential conflicts of interest are the following: AP reports consulting fees from Nanostring Technologies, Roche, Pfizer, Novartis, AstraZeneca, Foundation Medicine, Guardant Health, and Daiichi Sankyo outside the submitted work. AV reports consulting fees from Sysmex, Novartis, Merck, Bristol Meyers Squibb, Guardant Health, and Incyte; research funding from Bristol Meyers Squibb; and royalties from Ferrer outside the submitted work. VP has received fees as consultant, participated in advisory boards, or received travel grants from Sysmex, Roche, MSD, AstraZeneca, Bayer, and Exact Sciences outside the submitted work. CS has declared personal fees as consultant and advisory board or travel grants of AstraZeneca, Daiichi Sankyo, Eisai, Exact Sciences, Exeter Pharma, F. Hoffmann–La Roche Ltd, MediTech, Merck Sharp & Dohme, Novartis, Pfizer, Philips, Piere Fabre, Puma, Roche Farma, Sanofi-Aventis, SeaGen, and Zymeworks and institutional financial interests from AstraZeneca, Daiichi Sankyo, Eli Lilly and Company, Genentech, Immunomedics, Macrogenics, Merck, Sharp and Dhome España S.A., Novartis, Pfizer, Piqur Therapeutics, Puma, Roche, Synthon, and Zenith Pharma. CS and AP are Board Members of SOLTI Cooperative Group and are employed by Institut Oncològic Baselga (IOB), Quironsalud Group.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Keenan TE, Tolaney SM. Role of Immunotherapy in Triple-Negative Breast Cancer. JNCCN J Natl Compr Cancer Netw (2020) 18(4):479–89. doi: 10.6004/jnccn.2020.7554
CrossRef Full Text | Google Scholar
2. Schmid P, Adams S, Rugo HS, Schneeweiss A, Barrios CH, Iwata H, et al. Atezolizumab and Nab-Paclitaxel in Advanced Triple-Negative Breast Cancer. N Engl J Med (2018) 379:2108–21. doi: 10.1056/NEJMoa1809615
PubMed Abstract | CrossRef Full Text | Google Scholar
3. Alva AS, Mangat PK, Garrett-Mayer E, Halabi S, Hansra D, Calfa CJ, et al. Pembrolizumab in Patients With Metastatic Breast Cancer With High Tumor Mutational Burden: Results From the Targeted Agent and Profiling Utilization Registry (TAPUR) Study. J Clin Oncol (2021) 39(22):2443–51. doi: 10.1200/JCO.20.02923
4. Nik-Zainal S, Alexandrov LB, Wedge DC, Van Loo P, Greenman CD, Raine K, et al. Mutational Processes Molding the Genomes of 21 Breast Cancers. Cell (2012) 149:979–93. doi: 10.1016/j.cell.2012.04.024
5. Zhang Q, Luo J, Wu S, Si H, Gao C, Xu W, et al. Prognostic and Predictive Impact of Circulating Tumor DNA in Patients With Advanced Cancers Treated With Immune Checkpoint Blockade. Cancer Discov (2020) 10:CD–20-0047. doi: 10.1158/2159-8290.CD-20-0047
6. Hanker AB, Sudhan DR, Arteaga CL. Cancer Cell Review Overcoming Endocrine Resistance in Breast Cancer. Cancer Cell (2020) 37:496–513. doi: 10.1016/j.ccell.2020.03.009
7. O’Leary B, Hrebien S, Morden JP, Beaney M, Fribbens C, Huang X, et al. Early Circulating Tumor DNA Dynamics and Clonal Selection With Palbociclib and Fulvestrant for Breast Cancer. Nat Commun (2018) 9:896. doi: 10.1038/s41467-018-03215-x
8. Finn R, Liu Y, Martin M, Rugo H, Dieras V, Im S-A, et al. Abstract P2-09-10: Comprehensive Gene Expression Biomarker Analysis of CDK 4/6 and Endocrine Pathways From the PALOMA-2 Study. Cancer Res (2018) 78:P2‐09‐10‐P2‐09–10. doi: 10.1158/1538-7445.SABCS17-P2-09-10
9. Kanu N, Cerone MA, Goh G, Zalmas LP, Bartkova J, Dietzen M, et al. DNA Replication Stress Mediates APOBEC3 Family Mutagenesis in Breast Cancer. Genome Biol (2016) 17(1):185. doi: 10.1186/s13059-016-1042-9
10. Roberts SA, Lawrence MS, Klimczak LJ, Grimm SA, Fargo D, Stojanov P, et al. An APOBEC Cytidine Deaminase Mutagenesis Pattern Is Widespread in Human Cancers. Nat Genet (2013) 45:970–6. doi: 10.1038/ng.2702
11. Lefebvre C, Bachelot T, Filleron T, Pedrero M, Campone M, Soria J-C, et al. Mutational Profile of Metastatic Breast Cancers: A Retrospective Analysis. PloS Med (2016) 13:e1002201. doi: 10.1371/journal.pmed.1002201
12. Kidd JM, Newman TL, Tuzun E, Kaul R, Eichler EE. Population Stratification of a Common APOBEC Gene Deletion Polymorphism. McVean GAT. PloS Genet (2007) 3:e63. doi: 10.1371/journal.pgen.0030063
13. Burns MB, Lackey L, Carpenter MA, Rathore A, Land AM, Leonard B, et al. APOBEC3B Is an Enzymatic Source of Mutation in Breast Cancer. Nature (2013) 494:366–70. doi: 10.1038/nature11881
14. Domchek S, Postel-Vinay S, Im S-A, Park YH, Delord J-P, Italiano A, et al. Association of Tumour Mutational Burden With Outcomes in Patients With Select Advanced Solid Tumours Treated With Pembrolizumab in KEYNOTE-158. Ann Oncol (2019) 30(Suppl 5):v477–8. doi: 10.1093/annonc/mdz253.018
15. Le DT, Durham JN, Smith KN, Wang H, Bartlett BR, Aulakh LK, et al. Mismatch Repair Deficiency Predicts Response of Solid Tumors to PD-1 Blockade. Science (80- ) (2017) 357:409–13. doi: 10.1126/science.aan6733
16. Ayers M, Lunceford J, Nebozhyn M, Murphy E, Loboda A, Kaufman DR, et al. IFN-γ-Related mRNA Profile Predicts Clinical Response to PD-1 Blockade. J Clin Invest (2017) 127:2930–40. doi: 10.1172/JCI91190
17. Thompson JC, Davis C, Deshpande C, Hwang WT, Jeffries S, Huang A, et al. Gene Signature of Antigen Processing and Presentation Machinery Predicts Response to Checkpoint Blockade in Non-Small Cell Lung Cancer (NSCLC) and Melanoma. J Immunother Cancer (2020) 8:974. doi: 10.1136/jitc-2020-000974
18. Paré L, Pascual T, Seguí E, Teixidó C, Gonzalez-Cao M, Galván P, et al. Association Between PD1 mRNA and Response to Anti-PD1 Monotherapy Across Multiple Cancer Types. Ann Oncol (2018) 29:2121–8. doi: 10.1093/annonc/mdy335
19. Cristescu R, Mogg R, Ayers M, Albright A, Murphy E, Yearley J, et al. Pan-Tumor Genomic Biomarkers for PD-1 Checkpoint Blockade-Based Immunotherapy. Science (2018) 362(6411):eaar3593. doi: 10.1126/science.aar3593
20. Galon J, Bruni D. Approaches to Treat Immune Hot, Altered and Cold Tumours With Combination Immunotherapies. Nat Rev Drug Discov (2019) 18:197–218. doi: 10.1038/s41573-018-0007-y
Keywords: immunotherapy, breast cancer, biomarkers, ctDNA, case report
Citation: Brasó-Maristany F, Sansó M, Chic N, Martínez D, González-Farré B, Sanfeliu E, Ghiglione L, Carcelero E, Garcia-Corbacho J, Sánchez M, Soy D, Jares P, Peg V, Saura C, Muñoz M, Prat A and Vivancos A (2021) Case Report: A Case Study Documenting the Activity of Atezolizumab in a PD-L1-Negative Triple-Negative Breast Cancer. Front. Oncol. 11:710596. doi: 10.3389/fonc.2021.710596
Received: 16 May 2021; Accepted: 31 August 2021; Published: 20 September 2021.
Reviewed by:
Copyright © 2021 Brasó-Maristany, Sansó, Chic, Martínez, González-Farré, Sanfeliu, Ghiglione, Carcelero, Garcia-Corbacho, Sánchez, Soy, Jares, Peg, Saura, Muñoz, Prat and Vivancos. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY) . The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Aleix Prat, [email protected] ; Ana Vivancos, [email protected]
† These authors have contributed equally to this work
‡ These authors share senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Ohio State nav bar
The Ohio State University
- BuckeyeLink
- Find People
- Search Ohio State
Pathophysiology
Normal physiology of the human breast.
Prior to sexual maturity, male and female breasts are structurally and functionally similar; they are both comprised of small immature nipples, fatty and fibrous tissue and several duct-like arrangements beneath the areola.
When puberty is underway in males and females, this is where the major structural development occurs. Male breasts remain unchanged due to the lack of high levels of estrogen and progesterone. Females, on the other hand, have significant changes occur due to an assortment of hormones (estrogen, growth hormone, insulin-like growth factor-1, progesterone, and prolactin) (p.739) that cause the female breast to develop into a lactating system.
The mature female breast’s foundational unit is the lobe (each breast contains 15-20) a system of ducts which is comprised of and supported by Cooper ligaments. Each lobe is made up of 20-40 lobules (glands that produce milk). The lobules contain alveolar cells, which are complicated spaces lined with epithelial cells that secrete milk and sub-epithelial cells that contract, passing milk into the arrangement of ducts that leads to the nipple (p. 739).
The lobes and lobules are enclosed and separated by muscle strands and adipose connective tissue which varies in amount depending on weight, genetics, endocrine factors and contributes to the diversity of breast size and shape.
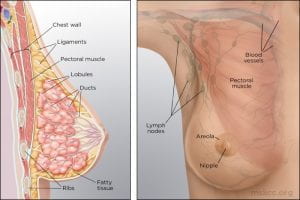
(Memorial Sloan Kettering Cancer Center)
During the reproductive years, breast tissue undergoes cyclic changes in response to hormonal changes of the menstrual cycle. After menopause, adipose deposits and connective tissue increases, glandular breast tissue becomes involuted, and breasts are reduced in size and form. Due to elevated aromatase (decreases circulating estrogen) there can be an increase in white adipose tissue inflammation (p.740).
The function of the female breast is primarily to provide a source of nourishment for the newborn; however, breasts are also a source of pleasurable sexual sensation and in Western cultures have become a sexual symbol (p.741).
(McCance, K. L., & Heuther, S. E. (2019). Pathophysiology: The biological basis for disease in adults and children (8th ed., pp.739-741). St. Louis, MO: Mosby.)
Pathophysiology of Breast Cancer
Except for skin cancer, breast cancer is the most common cancer in American women. Most breast cancer occurs in women older than 50 years. The major risk factors for breast cancer are classified as reproductive, such as nulliparity and pregnancy-associated breast cancer; familial, such as inherited gene syndromes; and environmental and lifestyle, such as hormonal factors and radiation exposure. Some examples of known carcinogenic agents with sufficient evidence in humans that contribute to the development of breast cancer are alcoholic beverages, diethylstilbestrol, estrogen-progestogen contraceptives, estrogen-progestogen menopausal therapy, X-radiation and γ-radiation (Rote, 2019). Other important factors are delayed involution of the mammary gland and increased breast density.
Overall, lifetime risk of breast cancer is reduced in parous women compared to nulliparous women, but pregnancy must occur at a young age. The influence of pregnancy on the risk of cancer also depends on family history, lactation postpartum, and overall parity. Breast gland involution after pregnancy and lactation uses some of the same tissue remodeling pathways activated during wound healing. The presence of macrophages in the involuting mammary gland contributes to carcinogenesis.
Most breast cancers are adenocarcinomas and first arise from the ductal/lobular epithelium as carcinoma in situ. Carcinoma in situ is an early-stage, noninvasive, proliferation of epithelial cells that is confined to the ducts and lobules, by the basement membrane. About 84% of all in situ disease is ductal carcinoma in situ (DCIS); the remainder is mostly lobular carcinoma in situ (LCIS) disease. Ductal carcinoma in situ (DCIS) refers to a heterogenous group of proliferative lesions limited to ducts and lobules without invasion to the basement membrane. DCIS occurs predominantly in women but can also occur in men. DCIS has a wide spectrum of risk for invasive cancers. Preinvasive lesions do not invariably progress to invasive malignancy. Lobular carcinoma in situ (LCIS) originates from the terminal duct-lobular unit. Unlike DCIS, LCIS has a uniform appearance; thus, the lobular structure is preserved. The cells grow in non-cohesive clusters, typically because of a loss of the tumor-suppressive adhesion protein E-cadherin . Also, unlike DCIS, LCIS is found as an incidental lesion from a biopsy and not mammography, is more likely to be present bilaterally.
(Winslow, 2012)
Breast cancer is a heterogeneous disease with diverse, molecular, genetic, phenotypic, and pathologic changes. Tumor heterogeneity results from the genetic, epigenetic, and microenvironmental influences (selective pressure) that tumor cells undergo during cancer progression. Cellular subpopulations from different sections of the same tumor vary in many ways including growth rate, immunogenicity, ability to metastasize, and drug response, demonstrating significant heterogeneity. The biological attributes of a tumor as a whole are strongly influenced by its subpopulation of cells with cellular populations communicating through paracrine or contact-dependent signaling (juxtacrine) from ligands and mediated from components of the microenvironment such as blood vessels, immune cells, and fibroblasts.
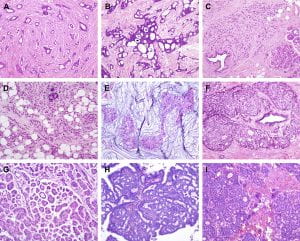
Figure 1. Histological special types of breast cancer preferentially oestrogen receptor positive. (A) Tubular carcinoma, (B) cribriform carcinoma, (C) classic invasive lobular carcinoma, (D) pleomorphic invasive lobular carcinoma, (E) mucinous carcinoma, (F) neuroendocrine carcinoma, (G) micropapillary carcinoma, (H) papillary carcinoma, (I) low grade invasive ductal carcinoma with osteoclast-like giant cells. (Weigelt, Geyer, & Reis-Filho, 2010)
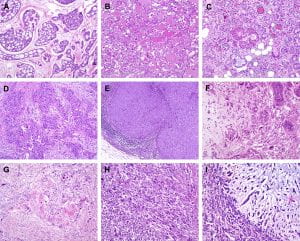
Figure 2. Histological special types of breast cancer preferentially oestrogen receptor negative. (A) Adenoid cystic carcinoma, (B) secretory carcinoma, (C) acinic-cell carcinoma, (D) apocrine carcinoma, (E) medullary carcinoma, (F) metaplastic carcinoma with heterologous elements, (G) metaplastic carcinoma with squamous metaplasia, (H) metaplastic spindle cell carcinoma, (I) metaplastic matrix-producing carcinoma. (Weigelt, Geyer, & Reis-Filho, 2010)
Gene expression profiling studies have identified major subtypes classified as luminal A, luminal B, HER2+, basal-like, Claudin-low, and normal breast. These subtypes have different prognoses and responses to therapy. Tumors can be stratified with gene expression profiles such as Oncotype Dx, Prosigna, and MammaPrint on the basis of genetic profiles. This information helps personalize breast cancer treatment and determine which women need aggressive systemic treatment for high-risk cancers versus close surveillance for indolent tumors.
Many models of breast carcinogenesis have been suggested and the expanding themes include (1) gene addiction, (2) phenotype plasticity, (3) cancer stem cells, (4) hormonal outcomes affecting cell turnover of mammary epithelium, stem cells, extracellular matrix, and immune function.
Cancer gene addiction includes oncogene addiction, whereby these driver genes play key roles in breast cancer development and progression. In non-oncogene addiction, these genes may not initiate cancer but play roles in cancer development and progression. Examples of key driver genes include HER2 and MYC, and examples of tumor-suppressor genes include TP53, BRCA1, and BRCA2. Once a founding tumor clone is established, genomic instability may assist through the establishment of other subclones and contribute to both tumor progression and therapy resistance.
Phenotypic plasticity is exemplified by a distinctive phenotype called epithelial-to-mesenchymal transition (EMT) . EMT is involved in the generation of tissues and organs during embryogenesis, is essential for driving tissue plasticity during development, and is hijacked during cancer progression. The EMT-associated programming is involved in many cancer cell characteristics, including suppression of cell death or apoptosis and senescence. It is reactivated during wound healing and is resistant to chemotherapy and radiation therapy. Remodeling or reprogramming of the breast during post-pregnancy involution is important because it involves inflammatory and “wound healing-like” tissue reactions known as reactive stroma or inflammatory stroma . The reactive stroma releases various signals and interleukins that affect nearby carcinoma cells, inducing these cells to activate their previously silent EMT programs. The activation is typically reversible (i.e., plasticity), and those EMT programs may revert through mesenchymal-epithelial (MET) to the previous phenotypic state before the induction of the EMT program. Reactive stroma increases the risk for tumor invasion and may facilitate the transition of carcinoma in situ to invasive carcinoma. Activation of an EMT program during cancer development often requires signaling between cancer cells and neighboring stromal cells. In advanced primary carcinomas, cancer cells recruit a variety of cell types into the surrounding stroma. Overall, increasing evidence suggests that interactions of cancer cells with adjacent tumor-associated stromal cells induce malignant phenotypes.
Figure 3. Putative EMT and MET in breast cancer progression. Normal epithelial cells undergo a series of transformational changes to become malignant tumor cells. Clonal proliferation of malignant cells gives rise to invasive carcinoma. Some of these cells undergo EMT and enter into the neighboring blood vessels or lymphatic vessels. These cells may remain in the circulation as circulating tumor cells or may extravasate at a distant site. The extravasated tumor cells form macrometastasis by a reverse mechanism known as MET. EMT, epithelial-mesenchymal transition; MET, mesenchymal-epithelial transition. (Liu, Gu, Shan, Geng, & Sang, 2016)
Using a mouse model of tumor heterogeneity, investigators demonstrated different clones within the heterogeneous population had distinct properties, such as the ability to dominate the primary tumor, or to contribute to metastatic populations, or to enter the lymphatic or vascular systems via vascular mimicry.
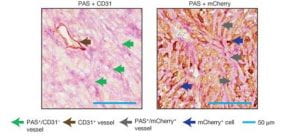
(Wagenblast et al., 2015)
Figure 4. Two adjacent sections of a mouse breast tumor. Tissue at left is stained so that normal blood vessels can be seen (brown arrow). Extending from these vessels are blood filled channels (green arrows). On the right, the tissue is stained for a fluorescent protein expressed by the tumor cells. Here it is seen that blood-filled channels are actually formed by tumor cells in a process known as vascular mimicry. The team demonstrate that the tumor cells lining these channels help drive metastasis, the process by which tumors spread. (Ravindran, 2019)
Invasion by primary tumor cells typically involves the collective migration of large cohesive groups into adjacent tissue rather than the scattering of individual carcinoma cells. However, still unknown are the precise events occurring at the invasive stage. Dormant carcinoma cells called minimal residual disease (MRD) appear to perpetuate carcinogenesis and form the precursors of eventual metastatic relapse and, sometimes, rapid cancer recurrence. Dormant cells have exited the cell cycle and are not proliferating. Thus current treatments that preferentially kill proliferating cells render dormant cells intrinsically more resistant and may remain after initial chemotherapy, radiotherapy, and surgery.
Emerging evidence supports three main prerequisites that must be met for metastatic colonization to succeed: the capacity to seed and maintain a population of tumor-initiating stem cells; the ability to create adaptive, organ-specific colonization programs; and the development of a supportive microenvironmental niche. Metastases may also occur early in the process of neoplastic transformation.
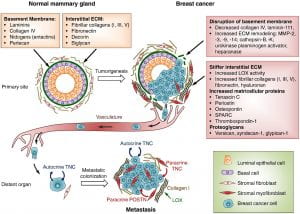
Figure 5 . Extracellular matrix (ECM) changes in breast cancer progression and metastasis. The primary components of the ECM in normal mammary gland are significantly changed in breast cancer. A desmoplastic reaction is associated with breast cancer development, due to the increased production of fibrous ECM by activated fibroblasts and cancer cells. The increased collagen deposition and crosslinking by lysyl oxidase (LOX) enzymes, together with the increased production of fibronectin and other ECM components, stiffens the ECM, which in turn promotes tumor aggressiveness. The basement membrane surrounding the mammary gland epithelium is broken down by ECM remodeling enzymes like MMPs, heparanase and others. Matricellular proteins that promote cancer cell fitness such as tenascin C, periostin, osteopontin, SPARC and thrombospondin-1 are also upregulated. Breast cancer cells from the primary tumor, that include cells with the ability to establish metastatic colonies, enter the blood circulation, disseminate and can reach distant sites. While the vast majority of disseminated cancer cells are eliminated or undergo dormancy due to the adverse environment, few cancer cells are able to resist the selective pressure and establish a metastatic colony. These cells may rely on signals from the ECM such as type I collagen (collagen I), crosslinked by LOX. Tenascin C (TNC) and periostin (POSTN), which are crucial ECM proteins of the metastatic niche, promote stem/progenitor pathways and metastatic fitness in disseminated breast cancer cells. (Insua-Rodríguez & Oskarsson, 2016)
The first clinical manifestation of breast cancer is usually a small, painless lump in the breast. Other manifestations include palpable lymph nodes in the axillae, dimpling of the skin, nipple and skin retraction, nipple discharge, ulcerations, reddened skin, and bone pain associated with bony metastases.
Treatment is based on the extent or stage of the cancer and includes surgery, radiation, chemotherapy, hormone therapy, and biologic therapy.
(Unless otherwise cited, all pathophysiology information was gathered from Danhausen, Phillippi, & McCance, 2019)
Click through the PLOS taxonomy to find articles in your field.
For more information about PLOS Subject Areas, click here .
Loading metrics
Open Access
Peer-reviewed
Research Article
Navigating the cancer care continuum: A comparative study of Black and White breast cancer patients
Roles Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Validation, Visualization, Writing – original draft, Writing – review & editing
Affiliation School of Industrial Engineering, Purdue University, West Lafayette, IN, United States of America
Roles Data curation, Formal analysis, Investigation, Validation, Writing – original draft, Writing – review & editing
Affiliation Independent Scholar, Bremerton, WA, United States of America
Roles Conceptualization, Funding acquisition, Project administration, Resources, Supervision, Writing – review & editing
Affiliation Pink-4-Ever Ending Disparities, Indianapolis, IN, United States of America
Roles Conceptualization, Investigation, Project administration, Resources, Supervision, Writing – review & editing
Affiliation Department of Human Development and Family Studies, Purdue University, West Lafayette, IN, United States of America
Roles Conceptualization, Methodology, Project administration, Resources, Software, Supervision, Writing – review & editing
* E-mail: [email protected]
Affiliations School of Industrial Engineering, Purdue University, West Lafayette, IN, United States of America, LASER PULSE (Long-Term Assistance and SErvices for Research, Partners for University-Led Solutions Engine) Consortium, Purdue University, West Lafayette, IN, United States of America
- Min K. Lee,
- Naomi T-T. Levine,
- Lisa R. Hayes,
- Cleveland G. Shields,
- Yuehwern Yih
- Published: October 24, 2024
- https://doi.org/10.1371/journal.pone.0312547
- Reader Comments
Despite improvements in early detection and therapeutic interventions, the mortality rate for Black breast cancer patients is still significantly higher than that of White breast cancer patients. This study seeks to understand differences in the patient experience that lead to this disparity. Semi-structured interviews were conducted to understand the breast cancer treatment process and patient experiences. This study collected health services and timeline data from medical records. Based on these two data sources, the patient’s journey in breast cancer treatment was mapped and a thematic analysis was conducted to identify challenges and barriers in the process. The cancer care continuum consists of four stages—diagnosis, surgery, chemotherapy/radiation, and follow-up care. The themes contributing to patient experiences and challenges were identified and compared in each stage for both Black and White patients. Both Black and White participants faced challenges related to financial constraints, treatment changes, lack of autonomy, and insufficient emotional support. However, Black participants additionally faced significant barriers in terms of cultural concordance, effective patient-provider communication, and delay in diagnosis. This study highlights the importance of incorporating effective provider-patient communication, navigation, and emotional support, especially for Black breast cancer patients throughout the cancer care continuum to address healthcare disparities.
Citation: Lee MK, Levine NT-T, Hayes LR, Shields CG, Yih Y (2024) Navigating the cancer care continuum: A comparative study of Black and White breast cancer patients. PLoS ONE 19(10): e0312547. https://doi.org/10.1371/journal.pone.0312547
Editor: Mary Diane Clark, Lamar University, UNITED STATES OF AMERICA
Received: May 16, 2024; Accepted: October 6, 2024; Published: October 24, 2024
Copyright: © 2024 Lee et al. This is an open access article distributed under the terms of the Creative Commons Attribution License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Data Availability: The datasets generated and analyzed in this study are not publicly available due to ethical and legal restrictions, as required by the approved Institutional Review Board (IRB) protocols (Purdue IRB: 1811021261). Given the small sample size and qualitative nature of the data, there is a potential for participant identification. However, de-identified data related to this publication may be made available upon reasonable request to the Purdue University Research Repository ( [email protected] ), provided that such a request falls within the ethical boundaries set by the IRB. The handling, storage, and protection of these datasets are conducted in strict accordance with the approved protocols.
Funding: This study was supported by the Indiana Clinical and Translational Sciences Institute, funded in part by grant # UL1TR002529 from the National Institutes of Health, National Center for Advancing Translational Sciences. This project was supported by the Indiana State Department of Health. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. There was no additional external funding received for this study.
Competing interests: The authors have declared that no competing interests exist.
Introduction
Breast cancer is the most commonly diagnosed form of cancer and the second leading cause of death among women in the United States [ 1 ]. Each year, over 280,000 new cases are reported, making up nearly 30% of all new cancer cases in the country, accompanied by more than 43,000 deaths [ 2 ]. Nonetheless, extensive research over the decades has illuminated the intricate nature of breast cancer and has contributed to enhanced clinical results [ 3 – 5 ]. Progress in early detection and therapeutic interventions has led to a decline in breast cancer mortality in the U.S. and various developed countries over the past few decades [ 6 ].
Unfortunately, this decrease in mortality is not uniform across populations. In the U.S., the age-adjusted breast cancer mortality rates are roughly 40% higher in Black women compared to non-Hispanic White women, even though Black women have a lower incidence rate [ 3 ]. Black women often face more advanced and aggressive forms of the disease, such as the triple-negative phenotype, and have a lower 5-year survival rate at every disease stage [ 4 ]. Additionally, they are more frequently diagnosed with comorbid conditions like hypertension, diabetes, and heart disease compared to their White counterparts [ 5 ].
The literature on racial disparities in breast cancer outcomes highlights significant differences in the patient experience, particularly regarding patient voice and patient-centered care. Black patients often encounter shorter and less detailed conversations with their clinicians compared to their White counterparts, which can hinder effective communication and shared decision-making [ 7 ]. Research indicates that Black patients often receive less information about their treatment options and prognosis, resulting in reduced participation in their own care and diminished empowerment to make informed healthcare decisions [ 8 – 10 ]. Furthermore, those who receive clear guidance are more likely to adhere to appropriate follow-up actions after an abnormal mammogram [ 11 ]; however, inadequate communication is disproportionately experienced by Black women compared to White women [ 12 ].
This disparity in communication is further compounded by racial discordance between patients and providers, where Black patients are more likely to report dissatisfaction with the care they receive from racially discordant clinicians [ 8 ]. The underrepresentation of Black nurses and clinicians in the healthcare system may contribute to structural racism, leading to challenges in establishing trust and rapport with Black patients [ 7 ].
The concept of ‘patient voice’ encapsulates the multi-dimensional challenges patients face–physical, emotional, and cognitive–underscoring the need for patient-centered care that fully considers the entire treatment journey [ 13 , 14 ]. While there is a growing body of literature addressing racial disparities in specific aspects of the breast cancer journey, a significant gap remains in understanding the experiences that span the entire treatment process [ 15 ]. Comprehensive studies that map out the entire experience are instrumental in ensuring personalized, empathetic, and effective care across all stages of the disease.
This study seeks to bridge existing knowledge gaps by comparing the experiences of Black and White breast cancer patients throughout their journey. By investigating the breast cancer patient’s journey and incorporating their personal experiences and expectations at each stage of the disease, our research not only offers insights that can reshape healthcare policies but also enhances patient care and outcomes. Furthermore, the findings can foster better relationships between the medical system, care teams, and patients, ensuring resources are tailored to patients’ needs, ultimately improving their quality of life. This study focuses on Indianapolis, a metropolitan area in the state of Indiana with a 29% Black population [ 16 ]. Consistent with the literature, despite improvements in the screening process, the gap in mortality rate between Black and White breast cancer patients has been persistent in Indiana [ 17 , 18 ].
Materials and methods
Study design and data collection.
In this qualitative research, we examined the conventional care pathway for women battling breast cancer to develop a comprehensive schematic that visually encapsulates their journey. An interview guide was created based on breast cancer literature and was adapted in collaboration with the Reaching to End Disparities (R.E.D.) Alliance (now known as Pink-4-Ever Ending Disparities). R.E.D. Alliance is a non-profit organization founded with the mission to empower, educate, and support breast cancer survivors, caregivers, and families, addressing breast health disparities and providing a range of services to aid individuals affected by breast cancer. A detailed outline of the interview questions is provided in S1 File . Demographic and health information was collected at the time of interview scheduling. We have also obtained protected health information (PHI) from the survivors’ health service providers to verify their progression timeline through the cancer care continuum. These medical records were accessed until November 2023 for research purposes.
Recruitment
Inclusion criteria included being female, over 18 years of age, a past diagnosis of breast cancer, and good mental status. Participants were recruited through the R.E.D. Alliance’s established collaborations with researchers, medical professionals, and cancer advocacy organizations and relationships with breast cancer survivors and women in the faith-based community. A study description was sent to potential participants through the R.E.D. Alliance mailing list and its social media platforms. Those expressing interest provided permission for their contact information to be shared with the principal investigator, who conducted all interviews. The investigator then reached out to those women, offering a more in-depth explanation of the study, and addressing any questions. Upon agreement to participate, an appointment was scheduled for either a videoconference or an in-person visit.
A total of 11 women voluntarily participated in this research. Interviews took place between February 2020 and January 2022, each lasting approximately 60 to 90 minutes. All interviews were audio-recorded and subsequently transcribed verbatim. Demographic and health information was gathered when scheduling the interviews, with variables including demographics and family history of cancer ( Table 1 ).
- PPT PowerPoint slide
- PNG larger image
- TIFF original image
https://doi.org/10.1371/journal.pone.0312547.t001
This study received approval from the Purdue Institutional Review Board (IRB #1811021261). Each participant signed an informed consent form, authorizing her participation and permitting the limited release of portions of her interview in a way that ensured confidentiality. The findings in this report have been presented while upholding the confidentiality of all study participants.
Data analysis
Interview data were analyzed using qualitative thematic analysis. Analyses were conducted following the framework of Ciria-Suarez et al. and Mitchell et al. [ 19 , 20 ]. Interview transcripts were thoroughly reviewed to discern recurring themes from the women’s experiences with cancer. Two researchers analyzed the transcripts independently, each identifying key themes, patterns, and concepts. They then collaborated to develop a unified codebook. Codes were grouped by similarities and differences, forming overarching themes. To ensure robustness, the team compared these insights with fixed data like sociodemographic and clinical characteristics. For each theme, representative quotes were determined separately for Black and White participants. The team reached a unanimous agreement on the theme categorization, and representative quotes were selected separately for Black and White participants to highlight these themes.
Researcher positionality
There are five authors for the current study. The primary author, who identifies as an ethnic minority, led the data collection and analysis, utilizing background in participatory action research and experience working with communities to address disparities in healthcare access. The second author, who identifies as White, has extensive experience in addressing disparities in healthcare access, contributed to the thematic analysis. The third author, an ethnic minority and breast cancer survivor, brought significant experience in breast cancer advocacy, particularly within marginalized communities, which was essential for contextualizing the findings. The fourth author, who identifies as White, offered valuable insights with his expertise in disparity of healthcare communication and patient-centered care. The fifth author, an ethnic minority scholar with expertise in systems engineering, leading this research project, contributed to the identification of the research question, overall study design and analysis, and offered perspectives on the broader structural issues affecting healthcare outcomes. All authors contributed to interpreting the findings and their implications. We acknowledge, however, that our backgrounds may have influenced our interpretations of the data. To mitigate this, we made deliberate efforts to bracket any existing biases or assumptions, documenting preconceptions during the data collection and analysis process to ensure our findings remained true to the participants’ voices.
Participants
In total, 11 women with a median age of 60 (Interquartile Range (IQR): 49.25–65.25) were interviewed. Most of the study population was married (73%), had a college education (64%), had a family history of cancer (91%) and were employed full-time (64%). Table 1 shows a comparison of sociodemographic and clinical characteristics between Black and White breast cancer study participants.
Breast cancer patient journey map
The journey for women diagnosed with breast cancer is intricately shaped by distinct medical stages, commonly framed within the cancer care continuum. This continuum represents the sequence of steps that people navigate from diagnosis through follow-up care. Each phase comes with its own set of unique experiences, eliciting specific physical, emotional, cognitive, and social responses. Many patients perceive this trajectory as a predefined path–a necessary course to potentially save their lives–that is largely dictated by the type and stage of their cancer. However, individuals may enter the cancer care continuum at any stage and aim to continue through it without delay. Table 2 outlines the differences in themes and subthemes experienced by Black and White participants throughout various stages of the breast cancer journey, as identified in this study.
https://doi.org/10.1371/journal.pone.0312547.t002
Fig 1 presents a plot illustrating the average time intervals between different stages of the cancer care continuum. The time delays are greater for Black participants at many of these stages and exhibit higher variability.
The gray shades indicate the confidence intervals for the time intervals between each stage of the cancer care continuum.
https://doi.org/10.1371/journal.pone.0312547.g001
Throughout the cancer care continuum.
The cancer care continuum represents the entire trajectory of cancer care, from the moment of diagnosis through the end of treatment and beyond into survivorship. There were two themes in the interview responses that reflected the overall care continuum: emotional response and support network.
Emotional response . Throughout the continuum, the emotional response becomes a critical aspect of the patient’s experience. Emotional support—or the lack thereof—is a theme that resonates across all patient experiences. Both Black and White participants reported feelings of isolation and a deficit of compassionate care within the healthcare system.
“ I received zero emotional support from the treatment team from screening to treatment. I didn’t know what to expect…I didn’t know the professional supports were available at that time.” (Participant 1; Black participant) “ In the beginning , you are overwhelmed . There is a different swirling of emotions , and that’s not really a comfortable thing to have to bring up . I feel like I needed more emotional support in the beginning . I didn’t get that towards halfway in .” (Participant 7; White participant) “ Within the hospital , there was no one I could turn to , to help with my fear . I don’t think any of the treatment team was addressing the emotional side ” (Participant 10; Black participant)
Support network . To cope with these challenges, family and friends emerged as one of the elements most intricately involved in the disease process. Both Black and White participants disclosed a broad range of support they received from family and friends, illustrating the crucial role loved ones play in providing emotional sustenance and practical assistance through the treatment journey.
“ When I was sick, my daughter was the caregiver. She made sure everything I needed was next to me .” (Participant 1; Black participant) “ The first time you go through , you’ll be so frightened and there will be lots of things that you will forget . You really need someone to help you go through this together .” (Participant 6; White participant)
Many participants also revealed a significant level of gratitude towards understanding and accommodating employers during their health crisis.
“ My boss, who was female and whose mother had a cancer issue, was informed. My boss was really helpful and asked me if I would like to be in FMLA or continue working. After 18 months of sick leave, I came back to work. All in all, my boss was supportive .” (Participant 1; Black participant) “ I had FMLA during my chemotherapy , which made my financial stable . It had no impact on my income and insurance . ” (Participant 5; White participant)
The diagnosis stage involves a battery of medical tests and screenings that enabled the identification of the disease. This stage is foundational in forming the treatment strategy based on the cancer type and stage. There were three themes in the interview responses that reflected this stage in the care continuum: delayed detection and diagnostic barriers, communication and information management, and shared experience and cultural connection.
Delayed detection and diagnostic barriers . During the diagnosis stage, patients encounter obstacles in accessing timely healthcare services and information. This barrier necessitates a degree of self-advocacy, which manifests distinctly across demographics. For Black participants, this self-advocacy was particularly pronounced, and it often arose from perceived neglect or oversight by their healthcare providers.
“ Despite routine screening , cancer was not detected . I discovered it myself when I felt some dimpling in my right breast .” (Participant 4; Black participant) “ Although previous mammo showed dense tissues , no one had talked to me about possible indications or possible treatment options . ” (Participant 8; Black participant) “ I felt a lump and scheduled appointment for regular mammogram , not diagnostic mammogram , which needs doctor’s approval . The doctor approved it on the same day , but I still had to wait a week . I don’t know why they sent me back when they could just call the doctor . The waiting time was like eternity . My mom and sister had it , so I was pretty sure that it was cancerous . ” (Participant 11; Black participant)
In contrast, White participants also demonstrated self-advocacy, but this was more focused on navigating systemic barriers related to insurance and finding alternative pathways to care, themes that both White and Black participants faced.
“ Insurance didn’t cover 3D mammogram, so I went with regular screening. It did cover genetic testing, so I did do this. ” (Participant 2; White participant) “ My physician sent the paperwork for additional mammogram but the nurse told me that it will not be covered by insurance as I have already had mammogram a few months ago .” (Participant 4; Black participant) “ In late 2020 , another lump was discovered , and I was recommended to get an MRI . My insurance wouldn’t cover MRI , so I had to price-shop to find an affordable MRI . I had my MRI done in early 2021 .” (Participant 9; White participant)
Communication and information management . As patients navigate these complexities, communication and information management become critical. The efficiency and clarity of the exchange between healthcare providers and patients are critical, yet both Black and White participants reported feeling overwhelmed by the deluge of information.
“ I was given a binder, but it was too much information at the beginning. I was not sure what estrogen/HER2 negative or positive meant. There was just so much in the air. ” (Participant 4; Black participant) “ I felt like they tried to combine some of my appointments if they could . And because of that I was overwhelmed with information . I was extremely overwhelmed .” (Participant 7; White participant) “ Throughout the process , there is a lot of information coming at you at one time . Sometimes I don’t know what questions to ask .” (Participant 8; Black participant)
Shared experience and cultural connection . This theme underscores the patients’ desire for healthcare professionals to resonate with their cultural background and personal experiences. The significance of this theme is particularly acute for Black participants, who consistently underscore the importance of representation and cultural competency in healthcare settings.
“ It would be nice to connect with other breast cancer patients on a more personal level, right from the time of diagnosis. It would have been helpful if someone on the treatment team, like doctors or nurses, had initiated the conversation about talking to different groups of people. ” (Participant 1; Black participant) “ I believe the African American woman (nurse practitioner) made the difference because of the comfort level and shared experience . I spent most of my time discussing with her throughout my care .” (Participant 4; Black participant) “ I wanted a Black doctor because I felt that they would understand my skin better . I wanted to be able to have that dialogue with ease and be comfortable .” (Participant 10; Black participant)
In this stage, patients undergo surgical procedures aimed at removing the tumor and potentially some surrounding tissue. Depending on the extent and type of cancer, different surgical methods may be employed. There were four themes in the interview responses that reflected this stage in the care continuum: insurance and financial barriers, unmet expectations and treatment changes, patient autonomy and involvement in care decisions, and communication and accessibility of providers.
Insurance and financial barriers . Both Black and White participants expressed concerns and challenges related to insurance and finances. Navigating these barriers is often intertwined with systemic inequalities, leading to discrepancies in treatment availability or affordability based on the type of insurance they had.
“ People were getting different answers on treatment plan depending on what insurance they have. It was based on my ability to pay. ” (Participant 4; Black participant) “ Whether or not to do the BRCA testing was based all on the cost of it . I heard from someone that it costed $10 , 000 so [he/she] didn’t do it . So that kind of number was floating around my head when they started talking about how much it was going to cost if I don’t meet the criteria .” (Participant 8; Black participant) “ The biggest barrier was from a financial perspective because of the hospital and their coding…There was a lot of back and forth to set it up with my insurance company .” (Participant 9; White participant)
Unmet expectations and treatment changes . The treatment process can deviate from initial plans. This divergence can introduce additional uncertainty into an already complex treatment landscape, necessitating adaptability, and resilience from patients and providers alike.
“ I feel like I was given false hopes. None of the plans happened as expected. ” (Participant 7; White participant) “ I went in (surgery) thinking I was at stage 1 or stage 2 , but it was actually stage 3 . They told me I had two small spots , but it was actually 10 . 4 cm . They discovered it only during the surgery . I had to have a second surgery . It was very painful .” (Participant 4; Black participant)
Patient autonomy and involvement in care decisions . Despite the often-unpredictable nature of the treatment process, a recurring concern among patients is the lack of involvement in the decision-making process. Both Black and White participants have expressed that they were not sufficiently informed or integrated into the decision-making process, and that they had little control over their appointments.
“ I wish I would have gotten more information and learned more about the treatment options. You know that would have played more into my discussion of when and where they would start.” (Participant 7; White participant) “ The nurse navigator was talking about the surgeon’s schedule , and it seemed like the surgeon wanted to get it done before his vacation . I got a feeling that he wants to rush before he goes on vacation and relax thereafter . ” (Participant 8; Black participant) “ We (the surgeon and I) were just talking about treatment options and then he did the MRI . I don’t know if he saw anything new , but he just said , you know , I’ve got to schedule you for this . So , it seemed like I was not getting enough information . ” (Participant 8; Black participant)
Communication and accessibility of providers . The theme highlights the struggle patients face in establishing and maintaining open lines of communication with their healthcare providers. Both Black and White participants showed frustration related to unanswered calls and unreturned voicemails, leading to emotional distress during a vulnerable time.
“ The doctor was not available when I had questions; [his/her] manner was very bad, was not supportive, and was not available most of the time.” (Participant 4; Black participant) “ The nurse navigator would be the obvious person to call but I couldn’t call her directly . I had to leave a voicemail and she didn’t return my calls half of the time .” (Participant 5; White participant) “ A week before my surgery , I called the nurse , and she was off for the week . Nobody called me and I was so scared…I spoke to probably two or three different nurses . But there was no follow-up even after I had the surgery . It was horrible . It would have been nice for her to think about the journey that I’m on . ” (Participant 10; Black participant)
Chemotherapy/radiation.
This stage involves intense treatments that can have strong side effects. Patients often encounter physical and emotional challenges that affect quality of life. There were two themes in the interview responses that reflected this stage in the care continuum: managing treatment side effects and balancing illness with daily life.
Managing treatment side effects . The patient’s experiences highlight the physical toll of the treatments and the importance of managing these side effects to maintain some quality of life. Many participants indicated that they have suffered physical discomfort such as fatigue, pain, and nausea.
“ After chemotherapy, I was really sick and couldn’t get up from bed. I was angry, but I understood that it was what I needed to do, and I didn’t want to be a complainer. ” (Participant 1; Black participant) “ I had a number of different side effects … I didn’t know where it was coming from , but it was coming very slowly . But eventually , I said , No I can’t , I can’t do that .” (Participant 4; Black participant) “ I had skin infection from chemo . Somehow my immune system was down . It was horrible .” (Participant 7; White participant)
However, they encountered a gap in understanding the potential adverse impacts of treatments or how to cope with the adverse impacts.
“ I do not feel that I was given as much information that I needed to help myself prepare for this. ” (Participant 4; Black participant)
Balancing illness with daily life . Both Black and White participants illustrated the diverse approaches to balancing the demands of treatment with personal and professional life, and how individual circumstances can significantly shape this experience.
“ During chemo, my daughter worked at night, so I took care of my granddaughter. I felt like having the responsibility to take care of my granddaughter was really helpful. She kept me more focused. The responsibility made a difference. ” (Participant 1; Black participant) “ While I was doing chemo , I was still a full-time mom , and I was still juggling being a full-time employee .” (Participant 7; White participant)
Post-treatment.
This stage is characterized by regular follow-ups and health assessments to ensure that cancer has not returned. Patients also receive medications or therapies to reduce the risk of recurrence, as well as breast reconstruction, if desired.
Treatment fatigue and decision to discontinue . The journey through cancer treatment is fraught with physical and emotional challenges that accumulate over time. For some Black participants, there comes a turning point where the prospect of additional treatment surpasses their threshold of what they can endure. In search of better options or second opinions, the patients may also seek out new doctors, which can lead to further delays in treatment and additional time lost in navigating the healthcare system.
“ I was unhappy with the oncologist because [he/she] didn’t have time to listen to me. I decided to find the second doctor .” (Participant 1; Black participant) “ The meeting was inappropriate and rude . I was exhausted thinking about it…So we thanked him for his time and we left there . I stayed awake all night thinking about it . The following week , I called the navigator to connect with another surgeon ” (Participant 8; Black participant) “ It was enough to be dealing with what I was already dealing with . I wanted to give myself some time and not jump in right away .” (Participant 10; Black participant)
Patient autonomy . Other participants find that they have an enhanced sense of control and empowerment over time in the later process. They emerge more informed and confident in making treatment-related decisions.
“ As we progress, I did my own research and took the initiative to share my findings with the professionals when deciding treatment choices…I felt more empowered.” (Participant 4; Black participant) “ I could have potentially had the reconstruction surgery , but I had my ovaries removed . I decided to just hold on , wait and do it next year . Because of my experience , I felt more empowered to make those kinds of decisions .” (Participant 7; White participant)
Follow-up care and continued support . This theme explores the experiences of patients with the continuum of care following active treatment. Many participants emphasized the need for ongoing support and communication to address the needs of patients as they transition out of active treatment and into survivorship.
“ A follow-up call from the office after surgery would be helpful. I hoped to get some questions answered, but there was no ‘open-door’ post-visit. ” (Participant 1; Black participant) “ After treatment , they teach you a little bit of stretches . But even this . They do this only when you demand it…That should be included in the treatment plan , like a follow up visit for physical therapy even if it’s just basic stretches .” (Participant 7; White participant) “ The nurse navigator was helpful , but once the chemotherapy is done , then you’re on your own . But I’m not done . I still need to start the oral chemotherapy drug .” (Participant 7; White participant)
In this study, we have illuminated the complex journey of breast cancer patients in Indianapolis, with a focus on the differing experiences of Black and White women. Our findings reveal persistent disparities in the treatment process, echoing the national trend of higher mortality rates among Black women, despite lower incidence rates.
As reported in the literature, the breast cancer care continuum is a process in which feelings of anxiety [ 21 ], financial strain [ 22 ], loss of health and self-identity [ 23 ], physical changes [ 24 ], and changes in employment status may arise [ 25 ]. To provide cancer care that addresses the full spectrum of a patient’s needs, a deep understanding of their priorities and perceptions regarding treatment is essential. Mapping the patient’s journey proves invaluable in this context, facilitating a thorough exploration of the emotional, cognitive, and communal aspects of patient interactions within the multifaceted healthcare system [ 26 ]. Additionally, process analysis plays a key role in identifying and addressing delays, challenges, and bottlenecks at each stage, leading to optimizing each stage of treatment, and fostering multidisciplinary collaboration, and ultimately enhancing the quality and effectiveness of the care continuum.
This study underscores the impact of emotional responses and emphasizes the critical need for a robust support network throughout the cancer care continuum. Both Black and White participants consistently reported a lack of emotional support from healthcare professionals, reflecting a common theme in their experiences. These findings are supported by the literature, which highlights the importance of emotional support in cancer care. Slevin et al. noted that patients dissatisfied with their emotional support were significantly more likely to experience anxiety and depression [ 27 ]. Similarly, Wortman found that patients who received strong and consistent emotional support tended to adjust more successfully over time [ 28 ]. This reinforces the need for integrated emotional care as a fundamental part of the overall treatment strategy. Cancer care, which poses both emotional and physical challenges to patients and their families, requires that strategies be developed to deliver such care starting from primary care settings. A multidisciplinary professional team spanning various health service sectors is needed to meet these needs effectively.
Another theme consistently echoed in the experiences of both Black and White participants was the lack of effective patient-provider communication, with participants emphasizing the need to establish open lines of communication with their healthcare providers. Effective patient-provider communication is an essential component of patient care, facilitating a complete, accurate, timely, and unambiguous communication between providers and patient [ 29 ]. Its absence has been identified as a significant factor contributing to adverse outcomes. For example, Barlett et al. found that patients facing communication problems were at the highest risk for preventable adverse events due to poor clinical management and drug errors [ 30 ]. Patients have the right to be informed about their care, make educated decisions, and be listened to by their providers, but patient communication needs are often unmet or are inadequately addressed [ 29 ]. Reflecting on this, in a 2007 public policy paper focusing on health literacy, the Joint Commission recommended that healthcare organizations should make effective communication an organizational priority to protect patient safety and incorporate strategies to address patients’ communication needs across the continuum of care [ 31 ]. Recognizing effective patient-provider communication is a vital component, and it must be prioritized to improve patient safety.
The analysis of our study revealed distinct themes where the differences in experiences between Black and White participants were particularly pronounced. Closely related to ineffective patient-provider communication was delay in diagnosis. Despite the possible negative impact of delayed diagnosis and treatment on breast cancer survival, literature has shown that Black women continue to experience significantly longer delays in diagnosis and treatment compared to their White counterparts in current practice, even after adjusting for sociodemographic, clinical, and situational factors [ 32 – 34 ]. In alignment with the literature, our findings indicate a higher delay in the time intervals between different stages of the breast cancer continuum for Black participants compared to White participants. Furthermore, in addition to the systemic and insurance-related barriers faced by both Black and White participants, Black participants encountered an additional layer of barriers, influenced by a combination of provider and health system-related factors. In particular, many Black participants shared that they self-detected their cancer despite routine mammogram screenings and that their providers did not adequately explain the implications of their abnormal mammogram results, consequently delaying the treatment. Properly and effectively communicating abnormal mammograms is crucial–yet a gap often exists between what patients actually understand and what is conveyed by healthcare professionals, highlighting a critical area for improvement in patient education and provider training.
A theme that was particularly pronounced for Black participants is racial concordance. Our findings are consistent with existing research, suggesting that patient-provider communication is generally more satisfying in racially concordant dyads of minority populations, especially for Black patients [ 35 , 36 ]. However, research spanning decades on concordance and physician-patient communication has produced conflicting results. Some studies, including a recent systematic review by Otte, have found minimal or no communication differences associated with concordance, and have deemed the relationship between patient outcomes and racial concordance inconclusive [ 37 ]. Conversely, other studies suggest that race and language concordance in patient navigators enhance the timeliness of care for minority populations [ 38 ]. These studies also note that patients who prefer racial concordance with their provider feel more at ease, find it easier to establish rapport, and appreciate the representation [ 39 ]. These findings underscore the need for a deeper understanding of provider support and social networks within the same race, advocating for the provision of individualized care where necessary.
We identified several barriers at systemic, social, and individual levels that influenced the experiences of Black women throughout the cancer care continuum. These factors were often interrelated and compounded in nature. Patient satisfaction decreased when they encountered barriers in any of these areas, and the challenges were exacerbated when multiple barriers were involved. Many Black participants sought a second opinion or decided to not receive further treatment as these challenges compounded. As such, although the reasons for seeking second opinions vary widely, studies suggest that patients’ primary motivations include a lack of trust, dissatisfaction with communication, a perceived need for certainty or confirmation, a need for more information, and a low understanding of the information provided [ 40 – 42 ]. It is also important to note that while obtaining second opinions provides patients with comprehensive treatment options, the process can delay treatment, as external imaging and records must be reviewed before presentation and assessment [ 43 ]. This underscores the importance of reducing adverse patient experiences through timely, effective communication and highlights the need for interventions to improve the referral process.
To our knowledge, this study is the first to compare the journey maps of Black and White breast cancer participants throughout the cancer care continuum. Our study illuminates the complex and varied experiences of breast cancer patients in Indianapolis, highlighting disparities between Black and White women. While both Black and White participants faced challenges related to financial barriers, treatment changes, lack of patient autonomy, and insufficient emotional support, Black participants additionally contended with barriers in cultural concordance and delays in diagnosis. These disparities mirror the national trend of higher mortality rates among Black breast cancer women. Central to these issues is the necessity for effective patient-provider communication and patient-centered care, which have proven to be crucial in influencing patient satisfaction, treatment timelines, and the overall quality of care. By addressing these challenges with equitable access to care and specific interventions, we can create a more equitable, responsive, and patient centered cancer care continuum, ultimately enhancing outcomes for all patients.
This study has certain limitations. The sample exclusively represents breast cancer survivors in the Indianapolis area, thus not fully capturing the breadth of socioeconomic disparities, as well as those faced in rural and other metropolitan areas. A larger national sample is required to comprehensively capture the disparities in care between Black and White breast cancer participants. Furthermore, qualitative research aims to understand specific phenomena and is not designed for generalization. Future research should focus on characterizing the barriers that lead to disparities in the care process throughout the patient journey, employing both quantitative and qualitative methods.
Supporting information
S1 file. semi-structured interview guide for breast cancer participants..
https://doi.org/10.1371/journal.pone.0312547.s001
Acknowledgments
The authors would like to thank all the study participants for their participation in the interview.
- View Article
- PubMed/NCBI
- Google Scholar
- 2. U.S. Cancer Statistics Working Group. U.S. cancer statistics data visualizations tool, based on 2021 submission data (1999–2019): U.S. Department of Health and Human Services, Centers for Disease Control and Prevention and National Cancer Institute; www.cdc.gov/cancer/dataviz , released in June 2022.
- 18. Halverson P, Crawford K. Indiana cancer facts and figures. Indiana Cancer Consortium: IN; 2018.Available from: https://www.in.gov/health/files/Indiana-Cancer-Facts-and-Figures-2018.pdf [Last accessed: November 10, 2022]
- 28. Wortman CB, Conway TL. The role of social support in adaptation and recovery from physical illness. In: Cohen S, Syme SL, editors. Social support and health. Academic Press; 1985. pp. 281–302.
- 31. The Joint Commission. What Did the Doctor Say?: Improving Health Literacy to Protect Patient Safety. Oakbrook Terrace, IL: The Joint Commission; 2007.
Reproductive History and Cancer Risk
Is there a relationship between pregnancy and breast cancer risk.
Studies have shown that a woman’s risk of developing breast cancer is related to her exposure to hormones that are produced by her ovaries ( endogenous estrogen and progesterone ). Reproductive factors that increase the duration and/or levels of exposure to ovarian hormones, which stimulate cell growth, have been associated with an increase in breast cancer risk. These factors include early onset of menstruation , late onset of menopause , and factors that may allow breast tissue to be exposed to high levels of hormones for longer periods of time, such as later age at first pregnancy and never having given birth.
Conversely, pregnancy and breastfeeding, which both reduce a woman’s lifetime number of menstrual cycles , and thus her cumulative exposure to endogenous hormones ( 1 ), are associated with a decrease in breast cancer risk. In addition, pregnancy and breastfeeding have direct effects on breast cells, causing them to differentiate, or mature, so they can produce milk. Some researchers hypothesize that these differentiated cells are more resistant to becoming transformed into cancer cells than cells that have not undergone differentiation ( 2 , 3 ).
Are any pregnancy-related factors associated with a lower risk of breast cancer?
Some pregnancy-related factors have been associated with a reduced risk of developing breast cancer later in life. These factors include:
- Early age at first full-term pregnancy. Women who have their first full-term pregnancy at an early age have a decreased risk of developing breast cancer later in life. For example, in women who have a first full-term pregnancy before age 20, the risk of developing breast cancer is about half that of women whose first full-term pregnancy occurs after the age of 30 ( 4 ). This risk reduction is limited to hormone receptor –positive breast cancer; age at first full-term pregnancy does not appear to affect the risk of hormone receptor-negative breast cancer ( 5 , 6 ).
- Increasing number of births. The risk of breast cancer declines with the number of children borne. Women who have given birth to five or more children have half the breast cancer risk of women who have not given birth ( 7 ). Some evidence indicates that the reduced risk associated with a higher number of births may be limited to hormone receptor–positive breast cancer.
- History of preeclampsia. Women who have had preeclampsia may have a decreased risk of developing breast cancer ( 8 – 11 ). Preeclampsia is a complication of pregnancy in which a woman develops high blood pressure and excess amounts of protein in her urine. Scientists are studying whether certain hormones and proteins associated with preeclampsia may affect breast cancer risk ( 8 , 12 , 13 ).
- Longer duration of breastfeeding. Breastfeeding for an extended period (at least a year) is associated with decreased risks of both hormone receptor–positive and hormone receptor–negative breast cancers ( 6 , 14 ).
Are any pregnancy-related factors associated with an increase in breast cancer risk?
Some factors related to pregnancy may increase the risk of breast cancer. These factors include:
- Older age at birth of first child. The older a woman is when she has her first full-term pregnancy, the higher her risk of breast cancer. Women who are older than 30 when they give birth to their first child have a higher risk of breast cancer than women who have never given birth ( 15 ).
- Recent childbirth. Women who have recently given birth have a short-term increase in breast cancer risk that declines after about 10 years. The reason for this temporary increase is not known, but some researchers believe that it may be due to the effect of high levels of hormones on the development of cancers or to the rapid growth of breast cells during pregnancy ( 16 ).
- Taking diethylstilbestrol ( DES ) during pregnancy. DES is a synthetic form of estrogen that was used between the early 1940s and 1971 to prevent miscarriages and other pregnancy problems. Women who took DES during pregnancy may have a slightly higher risk of developing breast cancer than women who did not take DES during pregnancy ( 17 ). Some studies have shown that daughters of women who took DES during pregnancy may also have a slightly higher risk of developing breast cancer after age 40 than women who were not exposed to DES while in the womb ( 18 ), but the evidence is inconsistent ( 19 ).
Is abortion linked to breast cancer risk?
A few retrospective (case-control) studies reported in the mid-1990s suggested that induced abortion (the deliberate ending of a pregnancy) was associated with an increased risk of breast cancer. However, these studies had important design limitations that could have affected the results. A key limitation was their reliance on self-reporting of medical history information by the study participants, which can introduce bias . Prospective studies , which are more rigorous in design and unaffected by such bias, have consistently shown no association between induced abortion and breast cancer risk ( 20 – 25 ). Moreover, in 2009, the Committee on Gynecologic Practice of the American College of Obstetricians and Gynecologists concluded that “more rigorous recent studies demonstrate no causal relationship between induced abortion and a subsequent increase in breast cancer risk” ( 26 ). Major findings from these studies include:
- Women who have had an induced abortion have the same risk of breast cancer as other women.
- Women who have had a spontaneous abortion (miscarriage) have the same risk of breast cancer as other women.
- Cancers other than breast cancer also appear to be unrelated to a history of induced or spontaneous abortion.
Does pregnancy affect the risk of other cancers?
Research has shown the following with regard to pregnancy and the risk of other cancers:
- Women who have had a full-term pregnancy have reduced risks of ovarian ( 27 , 28 ) and endometrial ( 29 ) cancers. Furthermore, the risks of these cancers decline with each additional full-term pregnancy.
- Pregnancy also plays a role in an extremely rare type of tumor called a gestational trophoblastic tumor . In this type of tumor, which starts in the uterus , cancer cells grow in the tissues that are formed following conception.
- There is some evidence that pregnancy-related factors may affect the risk of other cancer types, but these relationships have not been as well studied as those for breast and gynecologic cancers. The associations require further study to clarify the exact relationships.
As in the development of breast cancer, exposures to hormones are thought to explain the role of pregnancy in the development of ovarian, endometrial, and other cancers. Changes in the levels of hormones during pregnancy may contribute to the variation in risk of these tumors after pregnancy ( 30 ).
Does fertility treatment affect the risk of breast or other cancers?
Women who have difficulty becoming pregnant or carrying a pregnancy to term may receive fertility treatment. Such treatment can include surgery (to repair diseased, damaged, or blocked fallopian tubes or to remove uterine fibroids , patches of endometriosis , or adhesions); medications to stimulate ovulation ; and assisted reproductive technology. Ovarian stimulation and some assisted reproductive technologies involve treatments that temporarily change the levels of estrogen and progesterone in a woman’s body. For example, women undergoing in vitro fertilization (IVF) receive multiple rounds of hormone treatment to first suppress ovulation until the developing eggs are ready, then stimulate development of multiple eggs, and finally promote maturation of the eggs. The use of hormones in some fertility treatments has raised concerns about possible increased risks of cancer, particularly cancers that are linked to elevated levels of these hormones. Many studies have examined possible associations between use of fertility drugs or IVF and the risks of breast , ovarian , and endometrial cancers . The results of such studies can be hard to interpret because infertility itself is linked to increased risks of these cancers (that is, compared with fertile women, infertile women are at higher risk of these cancers even if they do not use fertility drugs). Also, these cancers are relatively rare and tend to develop years after treatment for infertility, which can make it difficult to link their occurrence to past use of fertility drugs.
- Breast cancer: The bulk of the evidence is consistent with no increased risk of breast cancer associated with the use of fertility drugs or IVF ( 31 – 34 ).
- Ovarian cancer: There is some uncertainty about whether treatment for infertility is a risk factor for ovarian cancer. A 2013 systematic review of 25 studies that included more than 180,000 women found, overall, no strong evidence of an increased risk of invasive ovarian cancer for women treated with fertility drugs ( 35 ). In one study, women who underwent IVF had an increase in risk of ovarian borderline malignant tumors ( 36 ).
- Endometrial cancer: Overall, the use of fertility drugs or IVF does not appear to increase the risk of endometrial cancer ( 34 ).
IMAGES
VIDEO
COMMENTS
For example, docetaxel and ... HER2-negative breast cancer: the TransNEOS study. ... Mehta V, Goel S, Kabarriti R, et al. Case fatality rate of cancer patients with COVID-19 in a New York hospital ...
Presentation of Case. Dr. Kevin S. Oh (Radiation Oncology): A 45-year-old woman was evaluated in the oncology clinic of this hospital because of metastatic triple-negative breast cancer. The ...
Adam M. Brufsky, MD, PhD: Let's talk about this case. This is a 48-year-old woman who presented to her primary care physician a number of years ago with a lump in her breast. She had a 4.4-cm left breast mass and 3 palpable axillary lymph nodes. Her ultrasound and mammogram confirmed these physical findings.
The Breast Cancer Surveillance Consortium (BCSC) model is a widely-used risk model that predicts five- and ten-year risk of developing invasive breast cancer for healthy women aged 35-74 years. ... it is important to note that the sample used in this study is not matched based on these two criteria. Results Patient Characteristics. Of the 339 ...
Objective BR2.7: Factors Affecting Response and Prognosis of Breast Cancer. Explain the prognosis and likelihood of recurrence and response to therapy for breast cancer patients based on knowledge of molecular classification and/or gene expression profiling, morphologic classification, grade, prognostic marker studies, and other predictive factors.
example, in a series of 8422 patients enrolled on International Breast Cancer Study Group trials between 1978 and 1999, the rate of node-negativity for medial compared to lateral/central tumors was 44 versus 33 percent, respectively. The most likely explanation for this difference is preferential drainage of some medial tumors to the IM nodes ...
1 Introduction. Breast cancer remains the most common cancer diagnosed among women in the United States and is the second leading cause of cancer-related deaths, with approximately 41,000 patients projected to die from this disease in 2018 alone. The prognosis for patients with metastatic breast cancer varies based on many factors including estrogen receptor (ER), progesterone receptor (PR ...
Hepin* had been diagnosed with triple negative breast cancer late in 2014, before going on to have surgery. Her treatment was initially successful, and for a number of years she led an active lifestyle. But in May 2018 she started to notice a change. 'I was feeling more tired than usual - yawning and flagging easily,' she explains.
Patient Case Presentation. Patient Mrs. B.C. is a 56 year old female who is presenting to her WHNP for her annual exam. She had to cancel her appointment two months ago and didn't reschedule until now. Her last pap smear and mammogram were normal. Today, while performing her breast exam, her nurse practitioner notices dimpling in the left ...
Background Breast cancer (BrCa) is one of the leading causes of cancer-related deaths. There are several factors for getting BrCa, including some changeable factors related to lifestyle like unhealthy dietary patterns, so modifying them can prevent one third of the complications and deaths caused by BrCa. Therefore, we decided to investigate the relationship between Healthy Beverage Index (HBI ...
Introduction. Breast cancer is one of the most common tumors, and its incidence rate ranks first in female malignant tumors ().Despite various treatments, the survival of patients with advanced breast cancer is still disappointing, and the overall survival (OS) is approximately 31% ().Because of the rapid progression of the tumor, it is of great importance to find an effective treatment in ...
The goal of this activity is for learners to be better able to select the most optimal anti-HER2 treatments for patients with HER2-positive breast cancer at every stage of care. Upon completion of this activity, participants will: Have increased knowledge regarding the. Clinical data associated with emerging anti-HER2 regimens for patients with ...
Abstract and Figures. In this case study, a women aged 40 was diagnosed with Metastatic breast cancer. Metastatic breast cancer is a complex multi-stage disease involving the expansion of ...
In 2015, Ms. M., a 60-year-old, unemployed, uninsured black woman, presented to the emergency department at a Chicago community hospital with a breast lump. The emergency medicine physician ...
This specific case is a typical controversial case because there is still disagreement over whether it can be classified as primary or secondary inflammatory breast cancer [2, 3]. Besides the clinical features present (oedema, peau d'orange, and erythema developed over a short period of 2 months) and the absence of a concrete palpable mass, no ...
EP: 1. Clinical Case Presentation: A 36-Year-Old Woman with Breast Cancer and Brain Metastases. EP: 2. Treatment Options in the Frontline Setting for Metastatic HER2+ Breast Cancer. EP: 3. Second-Line and Third-Line Treatment Options for Metastatic HER2+ Breast Cancer. EP: 4.
Breast cancer risk has been associated with age at menarche, menopause, and first pregnancy in multiple studies. Menarche before the age of 14 years raises the risk of breast cancer by a factor of 1.1 to 1.9 when compared to menarche after the age of 14 [14,15].
Thus, samples were relabeled as T1 (breast sample, 2008), T2 (lymph node sample, 2018), and T2-PD (breast sample, 2019). ... we present the case study of a TNBC with low TILs and PD-L1-negative disease, which achieved a significant response to atezolizumab monotherapy and durable response after the combination of atezolizumab and nab-paclitaxel ...
Pathophysiology of Breast Cancer. Except for skin cancer, breast cancer is the most common cancer in American women. Most breast cancer occurs in women older than 50 years. The major risk factors for breast cancer are classified as reproductive, such as nulliparity and pregnancy-associated breast cancer; familial, such as inherited gene ...
Introduction. Breast cancer is the most commonly diagnosed form of cancer and the second leading cause of death among women in the United States [].Each year, over 280,000 new cases are reported, making up nearly 30% of all new cancer cases in the country, accompanied by more than 43,000 deaths [].Nonetheless, extensive research over the decades has illuminated the intricate nature of breast ...
A few retrospective (case-control) studies reported in the mid-1990s suggested that induced abortion (the deliberate ending of a pregnancy) was associated with an increased risk of breast cancer. However, these studies had important design limitations that could have affected the results. A key limitation was their reliance on self-reporting of medical history information by the study ...