
An official website of the United States government
The .gov means it's official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you're on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
- Browse Titles
NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-.


StatPearls [Internet].
Breech presentation.
Caron J. Gray ; Meaghan M. Shanahan .
Affiliations
Last Update: November 6, 2022 .
- Continuing Education Activity
Breech presentation refers to the fetus in the longitudinal lie with the buttocks or lower extremity entering the pelvis first. The three types of breech presentation include frank breech, complete breech, and incomplete breech. In a frank breech, the fetus has flexion of both hips, and the legs are straight with the feet near the fetal face, in a pike position. This activity reviews the cause and pathophysiology of breech presentation and highlights the role of the interprofessional team in its management.
- Describe the pathophysiology of breech presentation.
- Review the physical exam of a patient with a breech presentation.
- Summarize the treatment options for breech presentation.
- Explain the importance of improving care coordination among interprofessional team members to improve outcomes for patients affected by breech presentation.
- Introduction
Breech presentation refers to the fetus in the longitudinal lie with the buttocks or lower extremity entering the pelvis first. The three types of breech presentation include frank breech, complete breech, and incomplete breech. In a frank breech, the fetus has flexion of both hips, and the legs are straight with the feet near the fetal face, in a pike position. The complete breech has the fetus sitting with flexion of both hips and both legs in a tuck position. Finally, the incomplete breech can have any combination of one or both hips extended, also known as footling (one leg extended) breech, or double footling breech (both legs extended). [1] [2] [3]
Clinical conditions associated with breech presentation include those that may increase or decrease fetal motility, or affect the vertical polarity of the uterine cavity. Prematurity, multiple gestations, aneuploidies, congenital anomalies, Mullerian anomalies, uterine leiomyoma, and placental polarity as in placenta previa are most commonly associated with a breech presentation. Also, a previous history of breech presentation at term increases the risk of repeat breech presentation at term in subsequent pregnancies. [4] [5] These are discussed in more detail in the pathophysiology section.
- Epidemiology
Breech presentation occurs in 3% to 4% of all term pregnancies. A higher percentage of breech presentations occurs with less advanced gestational age. At 32 weeks, 7% of fetuses are breech, and 28 weeks or less, 25% are breech.
Specifically, following one breech delivery, the recurrence rate for the second pregnancy was nearly 10%, and for a subsequent third pregnancy, it was 27%. Prior cesarean delivery has also been described by some to increase the incidence of breech presentation two-fold.
- Pathophysiology
As mentioned previously, the most common clinical conditions or disease processes that result in the breech presentation are those that affect fetal motility or the vertical polarity of the uterine cavity. [6] [7]
Conditions that change the vertical polarity or the uterine cavity, or affect the ease or ability of the fetus to turn into the vertex presentation in the third trimester include:
- Mullerian anomalies: Septate uterus, bicornuate uterus, and didelphys uterus
- Placentation: Placenta previa as the placenta is occupying the inferior portion of the uterine cavity. Therefore, the presenting part cannot engage
- Uterine leiomyoma: Mainly larger myomas located in the lower uterine segment, often intramural or submucosal, that prevent engagement of the presenting part.
- Prematurity
- Aneuploidies and fetal neuromuscular disorders commonly cause hypotonia of the fetus, inability to move effectively
- Congenital anomalies: Fetal sacrococcygeal teratoma, fetal thyroid goiter
- Polyhydramnios: Fetus is often in unstable lie, unable to engage
- Oligohydramnios: Fetus is unable to turn to vertex due to lack of fluid
- Laxity of the maternal abdominal wall: Uterus falls forward, the fetus is unable to engage in the pelvis.
The risk of cord prolapse varies depending on the type of breech. Incomplete or footling breech carries the highest risk of cord prolapse at 15% to 18%, while complete breech is lower at 4% to 6%, and frank breech is uncommon at 0.5%.
- History and Physical
During the physical exam, using the Leopold maneuvers, palpation of a hard, round, mobile structure at the fundus and the inability to palpate a presenting part in the lower abdomen superior to the pubic bone or the engaged breech in the same area, should raise suspicion of a breech presentation.
During a cervical exam, findings may include the lack of a palpable presenting part, palpation of a lower extremity, usually a foot, or for the engaged breech, palpation of the soft tissue of the fetal buttocks may be noted. If the patient has been laboring, caution is warranted as the soft tissue of the fetal buttocks may be interpreted as caput of the fetal vertex.
Any of these findings should raise suspicion and ultrasound should be performed.
Diagnosis of a breech presentation can be accomplished through abdominal exam using the Leopold maneuvers in combination with the cervical exam. Ultrasound should confirm the diagnosis.
On ultrasound, the fetal lie and presenting part should be visualized and documented. If breech presentation is diagnosed, specific information including the specific type of breech, the degree of flexion of the fetal head, estimated fetal weight, amniotic fluid volume, placental location, and fetal anatomy review (if not already done previously) should be documented.
- Treatment / Management
Expertise in the delivery of the vaginal breech baby is becoming less common due to fewer vaginal breech deliveries being offered throughout the United States and in most industrialized countries. The Term Breech Trial (TBT), a well-designed, multicenter, international, randomized controlled trial published in 2000 compared planned vaginal delivery to planned cesarean delivery for the term breech infant. The investigators reported that delivery by planned cesarean resulted in significantly lower perinatal mortality, neonatal mortality, and serious neonatal morbidity. Also, there was no significant difference in maternal morbidity or mortality between the two groups. Since that time, the rate of term breech infants delivered by planned cesarean has increased dramatically. Follow-up studies to the TBT have been published looking at maternal morbidity and outcomes of the children at two years. Although these reports did not show any significant difference in the risk of death and neurodevelopmental, these studies were felt to be underpowered. [8] [9] [10] [11]
Since the TBT, many authors since have argued that there are still some specific situations that vaginal breech delivery is a potential, safe alternative to planned cesarean. Many smaller retrospective studies have reported no difference in neonatal morbidity or mortality using these specific criteria.
The initial criteria used in these reports were similar: gestational age greater than 37 weeks, frank or complete breech presentation, no fetal anomalies on ultrasound examination, adequate maternal pelvis, and estimated fetal weight between 2500 g and 4000 g. In addition, the protocol presented by one report required documentation of fetal head flexion and adequate amniotic fluid volume, defined as a 3-cm vertical pocket. Oxytocin induction or augmentation was not offered, and strict criteria were established for normal labor progress. CT pelvimetry did determine an adequate maternal pelvis.
Despite debate on both sides, the current recommendation for the breech presentation at term includes offering external cephalic version (ECV) to those patients that meet criteria, and for those whom are not candidates or decline external cephalic version, a planned cesarean section for delivery sometime after 39 weeks.
Regarding the premature breech, gestational age will determine the mode of delivery. Before 26 weeks, there is a lack of quality clinical evidence to guide mode of delivery. One large retrospective cohort study recently concluded that from 28 to 31 6/7 weeks, there is a significant decrease in perinatal morbidity and mortality in a planned cesarean delivery versus intended vaginal delivery, while there is no difference in perinatal morbidity and mortality in gestational age 32 to 36 weeks. Of note, due to lack of recruitment, no prospective clinical trials are examining this issue.
- Differential Diagnosis
- Face and brow presentation
- Fetal anomalies
- Fetal death
- Grand multiparity
- Multiple pregnancies
- Oligohydramnios
- Pelvis Anatomy
- Preterm labor
- Primigravida
- Uterine anomalies
- Pearls and Other Issues
In light of the decrease in planned vaginal breech deliveries, thus the decrease in expertise in managing this clinical scenario, it is prudent that policies requiring simulation and instruction in the delivery technique for vaginal breech birth are established to care for the emergency breech vaginal delivery.
- Enhancing Healthcare Team Outcomes
A breech delivery is usually managed by an obstetrician, labor and delivery nurse, anesthesiologist and a neonatologist. The ultimate decison rests on the obstetrician. To prevent complications, today cesarean sections are performed and experienced with vaginal deliveries of breech presentation is limited. For healthcare workers including the midwife who has no experience with a breech delivery, it is vital to communicate with an obstetrician, otherwise one risks litigation if complications arise during delivery. [12] [13] [14]
- Review Questions
- Access free multiple choice questions on this topic.
- Comment on this article.
Disclosure: Caron Gray declares no relevant financial relationships with ineligible companies.
Disclosure: Meaghan Shanahan declares no relevant financial relationships with ineligible companies.
This book is distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0) ( http://creativecommons.org/licenses/by-nc-nd/4.0/ ), which permits others to distribute the work, provided that the article is not altered or used commercially. You are not required to obtain permission to distribute this article, provided that you credit the author and journal.
- Cite this Page Gray CJ, Shanahan MM. Breech Presentation. [Updated 2022 Nov 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-.
In this Page
Bulk download.
- Bulk download StatPearls data from FTP
Related information
- PMC PubMed Central citations
- PubMed Links to PubMed
Similar articles in PubMed
- [What effect does leg position in breech presentation have on mode of delivery and early neonatal morbidity?]. [Z Geburtshilfe Neonatol. 1997] [What effect does leg position in breech presentation have on mode of delivery and early neonatal morbidity?]. Krause M, Fischer T, Feige A. Z Geburtshilfe Neonatol. 1997 Jul-Aug; 201(4):128-35.
- The effect of intra-uterine breech position on postnatal motor functions of the lower limbs. [Early Hum Dev. 1993] The effect of intra-uterine breech position on postnatal motor functions of the lower limbs. Sival DA, Prechtl HF, Sonder GH, Touwen BC. Early Hum Dev. 1993 Mar; 32(2-3):161-76.
- The influence of the fetal leg position on the outcome in vaginally intended deliveries out of breech presentation at term - A FRABAT prospective cohort study. [PLoS One. 2019] The influence of the fetal leg position on the outcome in vaginally intended deliveries out of breech presentation at term - A FRABAT prospective cohort study. Jennewein L, Allert R, Möllmann CJ, Paul B, Kielland-Kaisen U, Raimann FJ, Brüggmann D, Louwen F. PLoS One. 2019; 14(12):e0225546. Epub 2019 Dec 2.
- Review Breech vaginal delivery at or near term. [Semin Perinatol. 2003] Review Breech vaginal delivery at or near term. Tunde-Byass MO, Hannah ME. Semin Perinatol. 2003 Feb; 27(1):34-45.
- Review [Breech Presentation: CNGOF Guidelines for Clinical Practice - Epidemiology, Risk Factors and Complications]. [Gynecol Obstet Fertil Senol. 2...] Review [Breech Presentation: CNGOF Guidelines for Clinical Practice - Epidemiology, Risk Factors and Complications]. Mattuizzi A. Gynecol Obstet Fertil Senol. 2020 Jan; 48(1):70-80. Epub 2019 Nov 1.
Recent Activity
- Breech Presentation - StatPearls Breech Presentation - StatPearls
Your browsing activity is empty.
Activity recording is turned off.
Turn recording back on
Connect with NLM
National Library of Medicine 8600 Rockville Pike Bethesda, MD 20894
Web Policies FOIA HHS Vulnerability Disclosure
Help Accessibility Careers

- Physician Physician Board Reviews Physician Associate Board Reviews CME Lifetime CME Free CME
- Student USMLE Step 1 USMLE Step 2 USMLE Step 3 COMLEX Level 1 COMLEX Level 2 COMLEX Level 3 96 Medical School Exams Student Resource Center NCLEX - RN NCLEX - LPN/LVN/PN 24 Nursing Exams
- Nurse Practitioner APRN/NP Board Reviews CNS Certification Reviews CE - Nurse Practitioner FREE CE
- Nurse RN Certification Reviews CE - Nurse FREE CE
- Pharmacist Pharmacy Board Exam Prep CE - Pharmacist
- Allied Allied Health Exam Prep Dentist Exams CE - Social Worker CE - Dentist
- Point of Care
- Free CME/CE
Breech Presentation
Introduction.
Breech presentation refers to the fetus in the longitudinal lie with the buttocks or lower extremity entering the pelvis first. The three types of breech presentation include frank breech, complete breech, and incomplete breech. In a frank breech, the fetus has flexion of both hips, and the legs are straight with the feet near the fetal face, in a pike position. The complete breech has the fetus sitting with flexion of both hips and both legs in a tuck position. Finally, the incomplete breech can have any combination of one or both hips extended, also known as footling (one leg extended) breech, or double footling breech (both legs extended). [1] [2] [3]
Register For Free And Read The Full Article
Learn more about a subscription to statpearls point-of-care.
Clinical conditions associated with breech presentation include those that may increase or decrease fetal motility, or affect the vertical polarity of the uterine cavity. Prematurity, multiple gestations, aneuploidies, congenital anomalies, Mullerian anomalies, uterine leiomyoma, and placental polarity as in placenta previa are most commonly associated with a breech presentation. Also, a previous history of breech presentation at term increases the risk of repeat breech presentation at term in subsequent pregnancies. [4] [5] These are discussed in more detail in the pathophysiology section.
Epidemiology
Breech presentation occurs in 3% to 4% of all term pregnancies. A higher percentage of breech presentations occurs with less advanced gestational age. At 32 weeks, 7% of fetuses are breech, and 28 weeks or less, 25% are breech.
Specifically, following one breech delivery, the recurrence rate for the second pregnancy was nearly 10%, and for a subsequent third pregnancy, it was 27%. Prior cesarean delivery has also been described by some to increase the incidence of breech presentation two-fold.
Pathophysiology
As mentioned previously, the most common clinical conditions or disease processes that result in the breech presentation are those that affect fetal motility or the vertical polarity of the uterine cavity. [6] [7]
Conditions that change the vertical polarity or the uterine cavity, or affect the ease or ability of the fetus to turn into the vertex presentation in the third trimester include:
- Mullerian anomalies: Septate uterus, bicornuate uterus, and didelphys uterus
- Placentation: Placenta previa as the placenta is occupying the inferior portion of the uterine cavity. Therefore, the presenting part cannot engage
- Uterine leiomyoma: Mainly larger myomas located in the lower uterine segment, often intramural or submucosal, that prevent engagement of the presenting part.
- Prematurity
- Aneuploidies and fetal neuromuscular disorders commonly cause hypotonia of the fetus, inability to move effectively
- Congenital anomalies: Fetal sacrococcygeal teratoma, fetal thyroid goiter
- Polyhydramnios: Fetus is often in unstable lie, unable to engage
- Oligohydramnios: Fetus is unable to turn to vertex due to lack of fluid
- Laxity of the maternal abdominal wall: Uterus falls forward, the fetus is unable to engage in the pelvis.
The risk of cord prolapse varies depending on the type of breech. Incomplete or footling breech carries the highest risk of cord prolapse at 15% to 18%, while complete breech is lower at 4% to 6%, and frank breech is uncommon at 0.5%.
History and Physical
During the physical exam, using the Leopold maneuvers, palpation of a hard, round, mobile structure at the fundus and the inability to palpate a presenting part in the lower abdomen superior to the pubic bone or the engaged breech in the same area, should raise suspicion of a breech presentation.
During a cervical exam, findings may include the lack of a palpable presenting part, palpation of a lower extremity, usually a foot, or for the engaged breech, palpation of the soft tissue of the fetal buttocks may be noted. If the patient has been laboring, caution is warranted as the soft tissue of the fetal buttocks may be interpreted as caput of the fetal vertex.
Any of these findings should raise suspicion and ultrasound should be performed.
Diagnosis of a breech presentation can be accomplished through abdominal exam using the Leopold maneuvers in combination with the cervical exam. Ultrasound should confirm the diagnosis.
On ultrasound, the fetal lie and presenting part should be visualized and documented. If breech presentation is diagnosed, specific information including the specific type of breech, the degree of flexion of the fetal head, estimated fetal weight, amniotic fluid volume, placental location, and fetal anatomy review (if not already done previously) should be documented.
Treatment / Management
Expertise in the delivery of the vaginal breech baby is becoming less common due to fewer vaginal breech deliveries being offered throughout the United States and in most industrialized countries. The Term Breech Trial (TBT), a well-designed, multicenter, international, randomized controlled trial published in 2000 compared planned vaginal delivery to planned cesarean delivery for the term breech infant. The investigators reported that delivery by planned cesarean resulted in significantly lower perinatal mortality, neonatal mortality, and serious neonatal morbidity. Also, there was no significant difference in maternal morbidity or mortality between the two groups. Since that time, the rate of term breech infants delivered by planned cesarean has increased dramatically. Follow-up studies to the TBT have been published looking at maternal morbidity and outcomes of the children at two years. Although these reports did not show any significant difference in the risk of death and neurodevelopmental, these studies were felt to be underpowered. [8] [9] [10] [11] (B2)
Since the TBT, many authors since have argued that there are still some specific situations that vaginal breech delivery is a potential, safe alternative to planned cesarean. Many smaller retrospective studies have reported no difference in neonatal morbidity or mortality using these specific criteria.
The initial criteria used in these reports were similar: gestational age greater than 37 weeks, frank or complete breech presentation, no fetal anomalies on ultrasound examination, adequate maternal pelvis, and estimated fetal weight between 2500 g and 4000 g. In addition, the protocol presented by one report required documentation of fetal head flexion and adequate amniotic fluid volume, defined as a 3-cm vertical pocket. Oxytocin induction or augmentation was not offered, and strict criteria were established for normal labor progress. CT pelvimetry did determine an adequate maternal pelvis.
Despite debate on both sides, the current recommendation for the breech presentation at term includes offering external cephalic version (ECV) to those patients that meet criteria, and for those whom are not candidates or decline external cephalic version, a planned cesarean section for delivery sometime after 39 weeks.
Regarding the premature breech, gestational age will determine the mode of delivery. Before 26 weeks, there is a lack of quality clinical evidence to guide mode of delivery. One large retrospective cohort study recently concluded that from 28 to 31 6/7 weeks, there is a significant decrease in perinatal morbidity and mortality in a planned cesarean delivery versus intended vaginal delivery, while there is no difference in perinatal morbidity and mortality in gestational age 32 to 36 weeks. Of note, due to lack of recruitment, no prospective clinical trials are examining this issue.
Differential Diagnosis
- Face and brow presentation
- Fetal anomalies
- Fetal death
- Grand multiparity
- Multiple pregnancies
- Oligohydramnios
- Pelvis Anatomy
- Preterm labor
- Primigravida
- Uterine anomalies
Pearls and Other Issues
In light of the decrease in planned vaginal breech deliveries, thus the decrease in expertise in managing this clinical scenario, it is prudent that policies requiring simulation and instruction in the delivery technique for vaginal breech birth are established to care for the emergency breech vaginal delivery.
Enhancing Healthcare Team Outcomes
A breech delivery is usually managed by an obstetrician, labor and delivery nurse, anesthesiologist and a neonatologist. The ultimate decison rests on the obstetrician. To prevent complications, today cesarean sections are performed and experienced with vaginal deliveries of breech presentation is limited. For healthcare workers including the midwife who has no experience with a breech delivery, it is vital to communicate with an obstetrician, otherwise one risks litigation if complications arise during delivery. [12] [13] [14]
Hinnenberg P, Toijonen A, Gissler M, Heinonen S, Macharey G. Outcome of small for gestational age-fetuses in breech presentation at term according to mode of delivery: a nationwide, population-based record linkage study. Archives of gynecology and obstetrics. 2019 Apr:299(4):969-974. doi: 10.1007/s00404-019-05091-2. Epub 2019 Feb 8 [PubMed PMID: 30734863]
Schlaeger JM, Stoffel CL, Bussell JL, Cai HY, Takayama M, Yajima H, Takakura N. Moxibustion for Cephalic Version of Breech Presentation. Journal of midwifery & women's health. 2018 May:63(3):309-322. doi: 10.1111/jmwh.12752. Epub 2018 May 18 [PubMed PMID: 29775226]
Niles KM, Barrett JFR, Ladhani NNN. Comparison of cesarean versus vaginal delivery of extremely preterm gestations in breech presentation: retrospective cohort study. The journal of maternal-fetal & neonatal medicine : the official journal of the European Association of Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, the International Society of Perinatal Obstetricians. 2019 Apr:32(7):1142-1147. doi: 10.1080/14767058.2017.1401997. Epub 2017 Nov 20 [PubMed PMID: 29157039]
Grabovac M, Karim JN, Isayama T, Liyanage SK, McDonald SD. What is the safest mode of birth for extremely preterm breech singleton infants who are actively resuscitated? A systematic review and meta-analyses. BJOG : an international journal of obstetrics and gynaecology. 2018 May:125(6):652-663. doi: 10.1111/1471-0528.14938. Epub 2017 Nov 2 [PubMed PMID: 28921813]
Andrews S, Leeman L, Yonke N. Finding the breech: Influence of breech presentation on mode of delivery based on timing of diagnosis, attempt at external cephalic version, and provider success with version. Birth (Berkeley, Calif.). 2017 Sep:44(3):222-229. doi: 10.1111/birt.12290. Epub 2017 May 8 [PubMed PMID: 28481464]
Walker S, Breslin E, Scamell M, Parker P. Effectiveness of vaginal breech birth training strategies: An integrative review of the literature. Birth (Berkeley, Calif.). 2017 Jun:44(2):101-109. doi: 10.1111/birt.12280. Epub 2017 Feb 17 [PubMed PMID: 28211102]
Hofmeyr GJ, Barrett JF, Crowther CA. Planned caesarean section for women with a twin pregnancy. The Cochrane database of systematic reviews. 2015 Dec 19:2015(12):CD006553. doi: 10.1002/14651858.CD006553.pub3. Epub 2015 Dec 19 [PubMed PMID: 26684389]
Ainsworth A, Sviggum HP, Tolcher MC, Weaver AL, Holman MA, Arendt KW. Lessons learned from a single institution's retrospective analysis of emergent cesarean delivery following external cephalic version with and without neuraxial anesthesia. International journal of obstetric anesthesia. 2017 May:31():57-62. doi: 10.1016/j.ijoa.2017.03.012. Epub 2017 Apr 2 [PubMed PMID: 28499551]
Hutton EK, Simioni JC, Thabane L. Predictors of success of external cephalic version and cephalic presentation at birth among 1253 women with non-cephalic presentation using logistic regression and classification tree analyses. Acta obstetricia et gynecologica Scandinavica. 2017 Aug:96(8):1012-1020. doi: 10.1111/aogs.13161. Epub 2017 May 27 [PubMed PMID: 28449212]
Adjaoud S, Demailly R, Michel-Semail S, Rakza T, Storme L, Deruelle P, Garabedian C, Subtil D. Is trial of labor harmful in breech delivery? A cohort comparison for breech and vertex presentations. Journal of gynecology obstetrics and human reproduction. 2017 May:46(5):445-448. doi: 10.1016/j.jogoh.2017.04.003. Epub 2017 Apr 13 [PubMed PMID: 28412313]
Poole KL, McDonald SD, Griffith LE, Hutton EK, Early ECV Pilot and ECV2 Trial Collaborative Group. Association of external cephalic version before term with late preterm birth. Acta obstetricia et gynecologica Scandinavica. 2017 Aug:96(8):998-1005. doi: 10.1111/aogs.13153. Epub 2017 May 16 [PubMed PMID: 28414857]
Domingues AP, Belo A, Moura P, Vieira DN. Medico-legal litigation in Obstetrics: a characterization analysis of a decade in Portugal. Revista brasileira de ginecologia e obstetricia : revista da Federacao Brasileira das Sociedades de Ginecologia e Obstetricia. 2015 May:37(5):241-6. doi: 10.1590/SO100-720320150005304. Epub [PubMed PMID: 26107576]
Delotte J, Oliver A, Boukaidi S, Mialon O, Breaud J, Benchimol D, Bongain A. [Who limit vaginal birth for breech presentation: medical practice or Law? Discussion between a medical doctor, a lawyer and the head chief of an university hospital]. Journal de gynecologie, obstetrique et biologie de la reproduction. 2011 Oct:40(6):587-9. doi: 10.1016/j.jgyn.2011.05.011. Epub 2011 Jul 16 [PubMed PMID: 21763083]
Burke G. The end of vaginal breech delivery. BJOG : an international journal of obstetrics and gynaecology. 2006 Aug:113(8):969-72 [PubMed PMID: 16827824]
Use the mouse wheel to zoom in and out, click and drag to pan the image
- Type 2 Diabetes
- Heart Disease
- Digestive Health
- Multiple Sclerosis
- Diet & Nutrition
- Supplements
- Health Insurance
- Public Health
- Patient Rights
- Caregivers & Loved Ones
- End of Life Concerns
- Health News
- Thyroid Test Analyzer
- Doctor Discussion Guides
- Hemoglobin A1c Test Analyzer
- Lipid Test Analyzer
- Complete Blood Count (CBC) Analyzer
- What to Buy
- Editorial Process
- Meet Our Medical Expert Board
What Is Breech?
When a fetus is delivered buttocks or feet first
- Types of Presentation
Risk Factors
Complications.
Breech concerns the position of the fetus before labor . Typically, the fetus comes out headfirst, but in a breech delivery, the buttocks or feet come out first. This type of delivery is risky for both the pregnant person and the fetus.
This article discusses the different types of breech presentations, risk factors that might make a breech presentation more likely, treatment options, and complications associated with a breech delivery.
Verywell / Jessica Olah
Types of Breech Presentation
During the last few weeks of pregnancy, a fetus usually rotates so that the head is positioned downward to come out of the vagina first. This is called the vertex position.
In a breech presentation, the fetus does not turn to lie in the correct position. Instead, the fetus’s buttocks or feet are positioned to come out of the vagina first.
At 28 weeks of gestation, approximately 20% of fetuses are in a breech position. However, the majority of these rotate to the proper vertex position. At full term, around 3%–4% of births are breech.
The different types of breech presentations include:
- Complete : The fetus’s knees are bent, and the buttocks are presenting first.
- Frank : The fetus’s legs are stretched upward toward the head, and the buttocks are presenting first.
- Footling : The fetus’s foot is showing first.
Signs of Breech
There are no specific symptoms associated with a breech presentation.
Diagnosing breech before the last few weeks of pregnancy is not helpful, since the fetus is likely to turn to the proper vertex position before 35 weeks gestation.
A healthcare provider may be able to tell which direction the fetus is facing by touching a pregnant person’s abdomen. However, an ultrasound examination is the best way to determine how the fetus is lying in the uterus.
Most breech presentations are not related to any specific risk factor. However, certain circumstances can increase the risk for breech presentation.
These can include:
- Previous pregnancies
- Multiple fetuses in the uterus
- An abnormally shaped uterus
- Uterine fibroids , which are noncancerous growths of the uterus that usually appear during the childbearing years
- Placenta previa, a condition in which the placenta covers the opening to the uterus
- Preterm labor or prematurity of the fetus
- Too much or too little amniotic fluid (the liquid that surrounds the fetus during pregnancy)
- Fetal congenital abnormalities
Most fetuses that are breech are born by cesarean delivery (cesarean section or C-section), a surgical procedure in which the baby is born through an incision in the pregnant person’s abdomen.
In rare instances, a healthcare provider may plan a vaginal birth of a breech fetus. However, there are more risks associated with this type of delivery than there are with cesarean delivery.
Before cesarean delivery, a healthcare provider might utilize the external cephalic version (ECV) procedure to turn the fetus so that the head is down and in the vertex position. This procedure involves pushing on the pregnant person’s belly to turn the fetus while viewing the maneuvers on an ultrasound. This can be an uncomfortable procedure, and it is usually done around 37 weeks gestation.
ECV reduces the risks associated with having a cesarean delivery. It is successful approximately 40%–60% of the time. The procedure cannot be done once a pregnant person is in active labor.
Complications related to ECV are low and include the placenta tearing away from the uterine lining, changes in the fetus’s heart rate, and preterm labor.
ECV is usually not recommended if the:
- Pregnant person is carrying more than one fetus
- Placenta is in the wrong place
- Healthcare provider has concerns about the health of the fetus
- Pregnant person has specific abnormalities of the reproductive system
Recommendations for Previous C-Sections
The American College of Obstetricians and Gynecologists (ACOG) says that ECV can be considered if a person has had a previous cesarean delivery.
During a breech delivery, the umbilical cord might come out first and be pinched by the exiting fetus. This is called cord prolapse and puts the fetus at risk for decreased oxygen and blood flow. There’s also a risk that the fetus’s head or shoulders will get stuck inside the mother’s pelvis, leading to suffocation.
Complications associated with cesarean delivery include infection, bleeding, injury to other internal organs, and problems with future pregnancies.
A healthcare provider needs to weigh the risks and benefits of ECV, delivering a breech fetus vaginally, and cesarean delivery.
In a breech delivery, the fetus comes out buttocks or feet first rather than headfirst (vertex), the preferred and usual method. This type of delivery can be more dangerous than a vertex delivery and lead to complications. If your baby is in breech, your healthcare provider will likely recommend a C-section.
A Word From Verywell
Knowing that your baby is in the wrong position and that you may be facing a breech delivery can be extremely stressful. However, most fetuses turn to have their head down before a person goes into labor. It is not a cause for concern if your fetus is breech before 36 weeks. It is common for the fetus to move around in many different positions before that time.
At the end of your pregnancy, if your fetus is in a breech position, your healthcare provider can perform maneuvers to turn the fetus around. If these maneuvers are unsuccessful or not appropriate for your situation, cesarean delivery is most often recommended. Discussing all of these options in advance can help you feel prepared should you be faced with a breech delivery.
American College of Obstetricians and Gynecologists. If your baby is breech .
TeachMeObGyn. Breech presentation .
MedlinePlus. Breech birth .
Hofmeyr GJ, Kulier R, West HM. External cephalic version for breech presentation at term . Cochrane Database Syst Rev . 2015 Apr 1;2015(4):CD000083. doi:10.1002/14651858.CD000083.pub3
By Christine Zink, MD Dr. Zink is a board-certified emergency medicine physician with expertise in the wilderness and global medicine.
Log in using your username and password
- Search More Search for this keyword Advanced search
- Latest content
- Current issue
- BMJ Journals More You are viewing from: Google Indexer
You are here
- Volume 99, Issue Suppl 1
- PLD.55 Introduction of Breech Clinic in a tertiary care setting to aid informed decision-making in mothers with breech presentation at term
- Article Text
- Article info
- Citation Tools
- Rapid Responses
- Article metrics
- Centre for Medical Education, Queens University Belfast, Belfast, UK
Background The incidence of breech presentation is 3–4% at tem. Since the publication of Term Breech Trial, elective Caesarian section (ELCS) has been the default mode of delivery with little or no opportunity for mothers to consider alternative approaches to manage breech presentation at term.
Methods Once a week Breech Clinic was introduced in June 2012 with a dedicated team of two midwives and two consultant obstetricians who are trained to counsel the mothers to aid informed decision making on their management and to undertake external cephalic version (ECV) if agreed. All mothers with breech presentation of a singleton fetus over 35 weeks of gestation with no known contraindications were booked to attend “Breech Clinic” at 37 weeks of gestation. They were provided with an information leaflet to read prior to the clinic appointment, and a detailed consultation on different approaches such as ECV, vaginal breech delivery (VBD) or ELCS was carried out with ample time for mothers to make their decision.
Results Since the implementation of Breech Clinic, more mothers are accepting ECV as their first choice, reaching a rate of 97% at the end of one-year period. 36% of attempted ECVs were successful with 80% of them achieving vaginal deliveries. 10% of mothers with unsuccessful ECVs opted for VBD over elective CS and eventually achieved vaginal deliveries.
Conclusion Introduction of Breech Clinic provides an opportunity for mothers to make an informed decision on the management of breech presentation resulting in higher acceptance of alternative approaches over ELCS.
Hannah ME, Hannah WJ, Hewson SA, Hodnett ED, Saigol S, Willan AR. Planned caesarean section versus planned vaginal birth for breech presentation at term: a randomised multi-centre trial. Lancet 2000;356:1375–85
Royal College of Obstetricians and Gynaecologists. Green top Guideline No 20b, Breech Presentation, Management, 2006
https://doi.org/10.1136/archdischild-2014-306576.354
Statistics from Altmetric.com
Request permissions.
If you wish to reuse any or all of this article please use the link below which will take you to the Copyright Clearance Center’s RightsLink service. You will be able to get a quick price and instant permission to reuse the content in many different ways.
Read the full text or download the PDF:
Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals
- Explore content
- About the journal
- Publish with us
- Sign up for alerts
- Review Article
- Published: 16 June 2023
Antigen presentation in cancer — mechanisms and clinical implications for immunotherapy
- Kailin Yang 1 ,
- Ahmed Halima 1 &
- Timothy A. Chan ORCID: orcid.org/0000-0002-9265-0283 1 , 2 , 3 , 4
Nature Reviews Clinical Oncology volume 20 , pages 604–623 ( 2023 ) Cite this article
14k Accesses
24 Citations
28 Altmetric
Metrics details
- Immunotherapy
- Predictive markers
- Tumour immunology
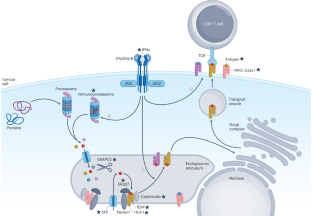
Over the past decade, the emergence of effective immunotherapies has revolutionized the clinical management of many types of cancers. However, long-term durable tumour control is only achieved in a fraction of patients who receive these therapies. Understanding the mechanisms underlying clinical response and resistance to treatment is therefore essential to expanding the level of clinical benefit obtained from immunotherapies. In this Review, we describe the molecular mechanisms of antigen processing and presentation in tumours and their clinical consequences. We examine how various aspects of the antigen-presentation machinery (APM) shape tumour immunity. In particular, we discuss genomic variants in HLA alleles and other APM components, highlighting their influence on the immunopeptidomes of both malignant cells and immune cells. Understanding the APM, how it is regulated and how it changes in tumour cells is crucial for determining which patients will respond to immunotherapy and why some patients develop resistance. We focus on recently discovered molecular and genomic alterations that drive the clinical outcomes of patients receiving immune-checkpoint inhibitors. An improved understanding of how these variables mediate tumour–immune interactions is expected to guide the more precise administration of immunotherapies and reveal potentially promising directions for the development of new immunotherapeutic approaches.
The clinical success of immune-checkpoint inhibitors has improved cancer care, although long-term durable remission is only achieved in a subset of patients.
Antigen processing and presentation by tumour cells are essential for long-lasting immune surveillance.
Alterations in the genes encoding MHC components and other parts of the antigen-presentation machinery are frequently found across several cancer types and are associated with both tumour development and the effectiveness of immunotherapies.
MHC-based antigen presentation exerts strong evolutionary pressure on the immunopeptidome, which in turn shapes the mutational landscape of the tumour genome.
Germline human leukocyte antigen diversity and somatic aberrations in the antigen-presentation machinery inform the therapeutic response to immune-checkpoint inhibitors.
Development of novel therapies based on an accurate understanding of antigen presentation in the setting of tumour–immune dynamics is crucial to the development of improved therapeutic approaches.
This is a preview of subscription content, access via your institution
Access options
Access Nature and 54 other Nature Portfolio journals
Get Nature+, our best-value online-access subscription
24,99 € / 30 days
cancel any time
Subscribe to this journal
Receive 12 print issues and online access
195,33 € per year
only 16,28 € per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others

Antigen presentation in cancer: insights into tumour immunogenicity and immune evasion

Towards new horizons: characterization, classification and implications of the tumour antigenic repertoire

Therapeutic cancer vaccines: advancements, challenges, and prospects
Waldman, A. D., Fritz, J. M. & Lenardo, M. J. A guide to cancer immunotherapy: from T cell basic science to clinical practice. Nat. Rev. Immunol. 20 , 651–668 (2020).
Article CAS PubMed PubMed Central Google Scholar
Hodi, F. S. et al. Improved survival with ipilimumab in patients with metastatic melanoma. N. Engl. J. Med. 363 , 711–723 (2010).
Larkin, J. et al. Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. N. Engl. J. Med. 373 , 23–34 (2015).
Article PubMed PubMed Central Google Scholar
Schadendorf, D. et al. Pooled analysis of long-term survival data from phase II and phase III trials of ipilimumab in unresectable or metastatic melanoma. J. Clin. Oncol. 33 , 1889–1894 (2015).
Robert, C. et al. Nivolumab in previously untreated melanoma without BRAF mutation. N. Engl. J. Med. 372 , 320–330 (2015).
Article CAS PubMed Google Scholar
Borghaei, H. et al. Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer. N. Engl. J. Med. 373 , 1627–1639 (2015).
Motzer, R. J. et al. Nivolumab versus everolimus in advanced renal-cell carcinoma. N. Engl. J. Med. 373 , 1803–1813 (2015).
Burtness, B. et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): a randomised, open-label, phase 3 study. Lancet 394 , 1915–1928 (2019).
Bellmunt, J. et al. Adjuvant atezolizumab versus observation in muscle-invasive urothelial carcinoma (IMvigor010): a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 22 , 525–537 (2021).
Kelly, R. J. et al. Adjuvant nivolumab in resected esophageal or gastroesophageal junction cancer. N. Engl. J. Med. 384 , 1191–1203 (2021).
Schmid, P. et al. Atezolizumab and Nab-paclitaxel in advanced triple-negative breast cancer. N. Engl. J. Med. 379 , 2108–2121 (2018).
Ribas, A. & Wolchok, J. D. Cancer immunotherapy using checkpoint blockade. Science 359 , 1350–1355 (2018).
Antonia, S. J. et al. Overall survival with durvalumab after chemoradiotherapy in stage III NSCLC. N. Engl. J. Med. 379 , 2342–2350 (2018).
Forde, P. M. et al. Neoadjuvant nivolumab plus chemotherapy in resectable lung cancer. N. Engl. J. Med. 386 , 1973–1985 (2022).
Snyder, A. et al. Genetic basis for clinical response to CTLA-4 blockade in melanoma. N. Engl. J. Med. 371 , 2189–2199 (2014).
Gao, J. et al. Loss of IFN-γ pathway genes in tumor cells as a mechanism of resistance to anti-CTLA-4 therapy. Cell 167 , 397–404.e9 (2016).
Zaretsky, J. M. et al. Mutations associated with acquired resistance to PD-1 blockade in melanoma. N. Engl. J. Med. 375 , 819–829 (2016).
Zhou, X. et al. Treatment-related adverse events of PD-1 and PD-L1 inhibitor-based combination therapies in clinical trials: a systematic review and meta-analysis. Lancet Oncol. 22 , 1265–1274 (2021).
Havel, J. J., Chowell, D. & Chan, T. A. The evolving landscape of biomarkers for checkpoint inhibitor immunotherapy. Nat. Rev. Cancer 19 , 133–150 (2019).
Halima, A., Vuong, W. & Chan, T. A. Next-generation sequencing: unraveling genetic mechanisms that shape cancer immunotherapy efficacy. J. Clin. Invest. 132 , e154945 (2022).
Pietanza, M. C. et al. Phase II trial of temozolomide in patients with relapsed sensitive or refractory small cell lung cancer, with assessment of methylguanine-DNA methyltransferase as a potential biomarker. Clin. Cancer Res. 18 , 1138–1145 (2012).
Rizvi, N. A. et al. Cancer immunology. Mutational landscape determines sensitivity to PD-1 blockade in non-small cell lung cancer. Science 348 , 124–128 (2015).
Dudley, J. C., Lin, M. T., Le, D. T. & Eshleman, J. R. Microsatellite instability as a biomarker for PD-1 blockade. Clin. Cancer Res. 22 , 813–820 (2016).
Le, D. T. et al. Mismatch repair deficiency predicts response of solid tumors to PD-1 blockade. Science 357 , 409–413 (2017).
Marcus, L., Lemery, S. J., Keegan, P. & Pazdur, R. FDA approval summary: pembrolizumab for the treatment of microsatellite instability-high solid tumors. Clin. Cancer Res. 25 , 3753–3758 (2019).
Cercek, A. et al. PD-1 blockade in mismatch repair-deficient, locally advanced rectal cancer. N. Engl. J. Med. 386 , 2363–2376 (2022).
Rosenberg, J. E. et al. Atezolizumab in patients with locally advanced and metastatic urothelial carcinoma who have progressed following treatment with platinum-based chemotherapy: a single-arm, multicentre, phase 2 trial. Lancet 387 , 1909–1920 (2016).
Gong, J., Chehrazi-Raffle, A., Reddi, S. & Salgia, R. Development of PD-1 and PD-L1 inhibitors as a form of cancer immunotherapy: a comprehensive review of registration trials and future considerations. J. Immunother. Cancer 6 , 8 (2018).
Chan, T. A. et al. Development of tumor mutation burden as an immunotherapy biomarker: utility for the oncology clinic. Ann. Oncol. 30 , 44–56 (2019).
Mahanty, S., Prigent, A. & Garraud, O. Immunogenicity of infectious pathogens and vaccine antigens. BMC Immunol. 16 , 31 (2015).
Pollard, A. J. & Bijker, E. M. A guide to vaccinology: from basic principles to new developments. Nat. Rev. Immunol. 21 , 83–100 (2021).
Li, F. et al. The association between CD8 + tumor-infiltrating lymphocytes and the clinical outcome of cancer immunotherapy: a systematic review and meta-analysis. EClinicalMedicine 41 , 101134 (2021).
Hellstrom, I., Hellstrom, K. E., Pierce, G. E. & Yang, J. P. Cellular and humoral immunity to different types of human neoplasms. Nature 220 , 1352–1354 (1968).
Horton, B. L. et al. Lack of CD8 + T cell effector differentiation during priming mediates checkpoint blockade resistance in non-small cell lung cancer. Sci. Immunol. 6 , eabi8800 (2021).
Lee, M. Y., Jeon, J. W., Sievers, C. & Allen, C. T. Antigen processing and presentation in cancer immunotherapy. J. Immunother. Cancer 8 , e001111 (2020).
Doherty, P. C. & Zinkernagel, R. M. A biological role for the major histocompatibility antigens. Lancet 1 , 1406–1409 (1975).
Doherty, P. C. & Zinkernagel, R. M. Enhanced immunological surveillance in mice heterozygous at the H-2 gene complex. Nature 256 , 50–52 (1975).
Parham, P. & Ohta, T. Population biology of antigen presentation by MHC class I molecules. Science 272 , 67–74 (1996).
Matsumura, M., Fremont, D. H., Peterson, P. A. & Wilson, I. A. Emerging principles for the recognition of peptide antigens by MHC class I molecules. Science 257 , 927–934 (1992).
Paul, S. et al. HLA class I alleles are associated with peptide-binding repertoires of different size, affinity, and immunogenicity. J. Immunol. 191 , 5831–5839 (2013).
Neefjes, J., Jongsma, M. L., Paul, P. & Bakke, O. Towards a systems understanding of MHC class I and MHC class II antigen presentation. Nat. Rev. Immunol. 11 , 823–836 (2011).
Colbert, J. D., Cruz, F. M. & Rock, K. L. Cross-presentation of exogenous antigens on MHC I molecules. Curr. Opin. Immunol. 64 , 1–8 (2020).
Chicz, R. M. et al. Predominant naturally processed peptides bound to HLA-DR1 are derived from MHC-related molecules and are heterogeneous in size. Nature 358 , 764–768 (1992).
Roche, P. A. & Furuta, K. The ins and outs of MHC class II-mediated antigen processing and presentation. Nat. Rev. Immunol. 15 , 203–216 (2015).
Dendrou, C. A., Petersen, J., Rossjohn, J. & Fugger, L. HLA variation and disease. Nat. Rev. Immunol. 18 , 325–339 (2018).
Arnaiz-Villena, A. et al. Evolution and molecular interactions of major histocompatibility complex (MHC)-G, -E and -F genes. Cell Mol. Life Sci. 79 , 464 (2022).
Baumeister, W., Walz, J., Zuhl, F. & Seemuller, E. The proteasome: paradigm of a self-compartmentalizing protease. Cell 92 , 367–380 (1998).
Groll, M. et al. Structure of 20S proteasome from yeast at 2.4 A resolution. Nature 386 , 463–471 (1997).
Dong, Y. et al. Cryo-EM structures and dynamics of substrate-engaged human 26S proteasome. Nature 565 , 49–55 (2019).
Cascio, P., Hilton, C., Kisselev, A. F., Rock, K. L. & Goldberg, A. L. 26S proteasomes and immunoproteasomes produce mainly N-extended versions of an antigenic peptide. EMBO J. 20 , 2357–2366 (2001).
Vigneron, N. et al. An antigenic peptide produced by peptide splicing in the proteasome. Science 304 , 587–590 (2004).
Warren, E. H. et al. An antigen produced by splicing of noncontiguous peptides in the reverse order. Science 313 , 1444–1447 (2006).
Rolfs, Z., Muller, M., Shortreed, M. R., Smith, L. M. & Bassani-Sternberg, M. Comment on “A subset of HLA-I peptides are not genomically templated: evidence for cis- and trans-spliced peptide ligands”. Sci. Immunol. 4 , eaaw1622 (2019).
Admon, A. Are there indeed spliced peptides in the immunopeptidome? Mol. Cell Proteom. 20 , 100099 (2021).
Article CAS Google Scholar
Rock, K. L. & Goldberg, A. L. Degradation of cell proteins and the generation of MHC class I-presented peptides. Annu. Rev. Immunol. 17 , 739–779 (1999).
Vigneron, N. & Van den Eynde, B. J. Proteasome subtypes and the processing of tumor antigens: increasing antigenic diversity. Curr. Opin. Immunol. 24 , 84–91 (2012).
Parcej, D. & Tampe, R. ABC proteins in antigen translocation and viral inhibition. Nat. Chem. Biol. 6 , 572–580 (2010).
Serwold, T., Gonzalez, F., Kim, J., Jacob, R. & Shastri, N. ERAAP customizes peptides for MHC class I molecules in the endoplasmic reticulum. Nature 419 , 480–483 (2002).
Pishesha, N., Harmand, T. J. & Ploegh, H. L. A guide to antigen processing and presentation. Nat. Rev. Immunol. https://doi.org/10.1038/s41577-022-00707-2 (2022).
Article PubMed Google Scholar
Garstka, M. A. et al. The first step of peptide selection in antigen presentation by MHC class I molecules. Proc. Natl Acad. Sci. USA 112 , 1505–1510 (2015).
Zarling, A. L. et al. Tapasin is a facilitator, not an editor, of class I MHC peptide binding. J. Immunol. 171 , 5287–5295 (2003).
Hermann, C. et al. TAPBPR alters MHC class I peptide presentation by functioning as a peptide exchange catalyst. eLife 4 , e09617 (2015).
Hildner, K. et al. Batf3 deficiency reveals a critical role for CD8α + dendritic cells in cytotoxic T cell immunity. Science 322 , 1097–1100 (2008).
Bonaccorsi, I. et al. Membrane transfer from tumor cells overcomes deficient phagocytic ability of plasmacytoid dendritic cells for the acquisition and presentation of tumor antigens. J. Immunol. 192 , 824–832 (2014).
Sanchez-Paulete, A. R. et al. Antigen cross-presentation and T-cell cross-priming in cancer immunology and immunotherapy. Ann. Oncol. 28 , xii44–xii55 (2017).
Blander, J. M. Regulation of the cell biology of antigen cross-presentation. Annu. Rev. Immunol. 36 , 717–753 (2018).
Canton, J. et al. The receptor DNGR-1 signals for phagosomal rupture to promote cross-presentation of dead-cell-associated antigens. Nat. Immunol. 22 , 140–153 (2021).
Shen, L., Sigal, L. J., Boes, M. & Rock, K. L. Important role of cathepsin S in generating peptides for TAP-independent MHC class I crosspresentation in vivo. Immunity 21 , 155–165 (2004).
Sanchez-Paulete, A. R. et al. Cancer immunotherapy with immunomodulatory anti-CD137 and anti-PD-1 monoclonal antibodies requires BATF3-dependent dendritic cells. Cancer Discov. 6 , 71–79 (2016).
Hanahan, D. Hallmarks of cancer: new dimensions. Cancer Discov. 12 , 31–46 (2022).
Lipsitch, M., Bergstrom, C. T. & Antia, R. Effect of human leukocyte antigen heterozygosity on infectious disease outcome: the need for allele-specific measures. BMC Med. Genet. 4 , 2 (2003).
Hraber, P., Kuiken, C. & Yusim, K. Evidence for human leukocyte antigen heterozygote advantage against hepatitis C virus infection. Hepatology 46 , 1713–1721 (2007).
Arora, J. et al. HLA heterozygote advantage against HIV-1 is driven by quantitative and qualitative differences in HLA allele-specific peptide presentation. Mol. Biol. Evol. 37 , 639–650 (2020).
Liu, Z. et al. HLA zygosity increases risk of hepatitis B virus-associated hepatocellular carcinoma. J. Infect. Dis. 224 , 1796–1805 (2021).
Gubin, M. M. et al. Checkpoint blockade cancer immunotherapy targets tumour-specific mutant antigens. Nature 515 , 577–581 (2014).
Tran, E. et al. Immunogenicity of somatic mutations in human gastrointestinal cancers. Science 350 , 1387–1390 (2015).
Chowell, D. et al. Patient HLA class I genotype influences cancer response to checkpoint blockade immunotherapy. Science 359 , 582–587 (2018).
Anagnostou, V. et al. Multimodal genomic features predict outcome of immune checkpoint blockade in non-small-cell lung cancer. Nat. Cancer 1 , 99–111 (2020).
Abed, A. et al. Prognostic value of HLA-I homozygosity in patients with non-small cell lung cancer treated with single agent immunotherapy. J. Immunother. Cancer 8 , e001620 (2020).
Kobayashi, M. et al. Effect of HLA genotype on intravesical recurrence after bacillus Calmette-Guerin therapy for non-muscle-invasive bladder cancer. Cancer Immunol. Immunother. 71 , 727–736 (2022).
Chowell, D. et al. Evolutionary divergence of HLA class I genotype impacts efficacy of cancer immunotherapy. Nat. Med. 25 , 1715–1720 (2019).
Chowell, D. et al. Improved prediction of immune checkpoint blockade efficacy across multiple cancer types. Nat. Biotechnol. 40 , 499–506 (2022).
Litchfield, K. et al. Meta-analysis of tumor- and T cell-intrinsic mechanisms of sensitization to checkpoint inhibition. Cell 184 , 596–614.e14 (2021).
Cuppens, K. et al. HLA-I diversity and tumor mutational burden by comprehensive next-generation sequencing as predictive biomarkers for the treatment of non-small cell lung cancer with PD-(L)1 inhibitors. Lung Cancer 170 , 1–10 (2022).
Lu, Z. et al. Germline HLA-B evolutionary divergence influences the efficacy of immune checkpoint blockade therapy in gastrointestinal cancer. Genome Med. 13 , 175 (2021).
Lee, C. H. et al. High response rate and durability driven by HLA genetic diversity in patients with kidney cancer treated with Lenvatinib and Pembrolizumab. Mol. Cancer Res. 19 , 1510–1521 (2021).
Takahashi, S. et al. Impact of germline HLA genotypes on clinical outcomes in patients with urothelial cancer treated with pembrolizumab. Cancer Sci. https://doi.org/10.1111/cas.15488 (2022).
Roerden, M. et al. HLA evolutionary divergence as a prognostic marker for AML patients undergoing allogeneic stem cell transplantation. Cancers 12 , 1835 (2020).
Feray, C. et al. Donor HLA class 1 evolutionary divergence is a major predictor of liver allograft rejection: a retrospective cohort study. Ann. Intern. Med. 174 , 1385–1394 (2021).
Cummings, A. L. et al. Mutational landscape influences immunotherapy outcomes among patients with non-small-cell lung cancer with human leukocyte antigen supertype B44. Nat. Cancer 1 , 1167–1175 (2020).
Naranbhai, V. et al. HLA-A*03 and response to immune checkpoint blockade in cancer: an epidemiological biomarker study. Lancet Oncol. 23 , 172–184 (2022).
Pyke, R. M. et al. A machine learning algorithm with subclonal sensitivity reveals widespread pan-cancer human leukocyte antigen loss of heterozygosity. Nat. Commun. 13 , 1925 (2022).
Hazini, A., Fisher, K. & Seymour, L. Deregulation of HLA-I in cancer and its central importance for immunotherapy. J. Immunother. Cancer 9 , e002899 (2021).
Shukla, S. A. et al. Comprehensive analysis of cancer-associated somatic mutations in class I HLA genes. Nat. Biotechnol. 33 , 1152–1158 (2015).
Salter, R. D. et al. A binding site for the T-cell co-receptor CD8 on the α 3 domain of HLA-A2. Nature 345 , 41–46 (1990).
Alspach, E. et al. MHC-II neoantigens shape tumour immunity and response to immunotherapy. Nature 574 , 696–701 (2019).
Shao, X. M. et al. HLA class II immunogenic mutation burden predicts response to immune checkpoint blockade. Ann. Oncol. 33 , 728–738 (2022).
Pagliuca, S. et al. The similarity of class II HLA genotypes defines patterns of autoreactivity in idiopathic bone marrow failure disorders. Blood 138 , 2781–2798 (2021).
Daull, A. M. et al. Class I/Class II HLA evolutionary divergence ratio is an independent marker associated with disease-free and overall survival after allogeneic hematopoietic stem cell transplantation for acute myeloid leukemia. Front. Immunol. 13 , 841470 (2022).
Steimle, V., Siegrist, C. A., Mottet, A., Lisowska-Grospierre, B. & Mach, B. Regulation of MHC class II expression by interferon-γ mediated by the transactivator gene CIITA. Science 265 , 106–109 (1994).
Rodig, S. J. et al. MHC proteins confer differential sensitivity to CTLA-4 and PD-1 blockade in untreated metastatic melanoma. Sci. Transl. Med. 10 , eaar3342 (2018).
Michelakos, T. et al. Differential role of HLA-A and HLA-B, C expression levels as prognostic markers in colon and rectal cancer. J. Immunother. Cancer 10 , e004115 (2022).
Meissner, T. B. et al. NLR family member NLRC5 is a transcriptional regulator of MHC class I genes. Proc. Natl Acad. Sci. USA 107 , 13794–13799 (2010).
Yoshihama, S. et al. NLRC5/MHC class I transactivator is a target for immune evasion in cancer. Proc. Natl Acad. Sci. USA 113 , 5999–6004 (2016).
Chew, G. L. et al. DUX4 suppresses MHC class I to promote cancer immune evasion and resistance to checkpoint blockade. Dev. Cell 50 , 658–671.e7 (2019).
Forloni, M. et al. NF-κB, and not MYCN, regulates MHC class I and endoplasmic reticulum aminopeptidases in human neuroblastoma cells. Cancer Res. 70 , 916–924 (2010).
Lorenzi, S. et al. IRF1 and NF-kB restore MHC class I-restricted tumor antigen processing and presentation to cytotoxic T cells in aggressive neuroblastoma. PLoS ONE 7 , e46928 (2012).
Yi, M. et al. The role of cancer-derived microRNAs in cancer immune escape. J. Hematol. Oncol. 13 , 25 (2020).
Mari, L. et al. microRNA 125a regulates MHC-I expression on esophageal adenocarcinoma cells, associated with suppression of antitumor immune response and poor outcomes of patients. Gastroenterology 155 , 784–798 (2018).
Colangelo, T. et al. Proteomic screening identifies calreticulin as a miR-27a direct target repressing MHC class I cell surface exposure in colorectal cancer. Cell Death Dis. 7 , e2120 (2016).
Huang, L. et al. The RNA-binding protein MEX3B mediates resistance to cancer immunotherapy by downregulating HLA-A expression. Clin. Cancer Res. 24 , 3366–3376 (2018).
Cano, F., Rapiteanu, R., Winkler, G. S. & Lehner, P. J. A non-proteolytic role for ubiquitin in deadenylation of MHC-I mRNA by the RNA-binding E3-ligase MEX-3C. Nat. Commun. 6 , 8670 (2015).
Yamamoto, K. et al. Autophagy promotes immune evasion of pancreatic cancer by degrading MHC-I. Nature 581 , 100–105 (2020).
Wang, Y. et al. Oncoprotein SND1 hijacks nascent MHC-I heavy chain to ER-associated degradation, leading to impaired CD8 + T cell response in tumor. Sci. Adv. 6 , eaba5412 (2020).
Fang, Y. et al. MAL2 drives immune evasion in breast cancer by suppressing tumor antigen presentation. J. Clin. Invest. 131 , e140837 (2021).
Jongsma, M. L. M. et al. The SPPL3-defined glycosphingolipid repertoire orchestrates HLA class I-mediated immune responses. Immunity 54 , 132–150.e9 (2021).
Rooney, M. S., Shukla, S. A., Wu, C. J., Getz, G. & Hacohen, N. Molecular and genetic properties of tumors associated with local immune cytolytic activity. Cell 160 , 48–61 (2015).
Bernal, M., Ruiz-Cabello, F., Concha, A., Paschen, A. & Garrido, F. Implication of the β2-microglobulin gene in the generation of tumor escape phenotypes. Cancer Immunol. Immunother. 61 , 1359–1371 (2012).
Gettinger, S. et al. Impaired HLA class I antigen processing and presentation as a mechanism of acquired resistance to immune checkpoint inhibitors in lung cancer. Cancer Discov. 7 , 1420–1435 (2017).
Sade-Feldman, M. et al. Resistance to checkpoint blockade therapy through inactivation of antigen presentation. Nat. Commun. 8 , 1136 (2017).
Challa-Malladi, M. et al. Combined genetic inactivation of β2-microglobulin and CD58 reveals frequent escape from immune recognition in diffuse large B cell lymphoma. Cancer Cell 20 , 728–740 (2011).
Fangazio, M. et al. Genetic mechanisms of HLA-I loss and immune escape in diffuse large B cell lymphoma. Proc. Natl Acad. Sci. USA 118 , e2104504118 (2021).
Chen, H. L. et al. A functionally defective allele of TAP1 results in loss of MHC class I antigen presentation in a human lung cancer. Nat. Genet. 13 , 210–213 (1996).
Klampfl, T. et al. Somatic mutations of calreticulin in myeloproliferative neoplasms. N. Engl. J. Med. 369 , 2379–2390 (2013).
Arshad, N. & Cresswell, P. Tumor-associated calreticulin variants functionally compromise the peptide loading complex and impair its recruitment of MHC-I. J. Biol. Chem. 293 , 9555–9569 (2018).
Tripathi, S. C. et al. Immunoproteasome deficiency is a feature of non-small cell lung cancer with a mesenchymal phenotype and is associated with a poor outcome. Proc. Natl Acad. Sci. USA 113 , E1555–E1564 (2016).
Kalaora, S. et al. Immunoproteasome expression is associated with better prognosis and response to checkpoint therapies in melanoma. Nat. Commun. 11 , 896 (2020).
Ramsuran, V. et al. Epigenetic regulation of differential HLA-A allelic expression levels. Hum. Mol. Genet. 24 , 4268–4275 (2015).
Ye, Q. et al. Hypermethylation of HLA class I gene is associated with HLA class I down-regulation in human gastric cancer. Tissue Antigens 75 , 30–39 (2010).
Burr, M. L. et al. An evolutionarily conserved function of polycomb silences the MHC class I antigen presentation pathway and enables immune evasion in cancer. Cancer Cell 36 , 385–401.e8 (2019).
Ennishi, D. et al. Molecular and genetic characterization of MHC deficiency identifies EZH2 as therapeutic target for enhancing immune recognition. Cancer Discov. 9 , 546–563 (2019).
Guo, B., Tan, X. & Cen, H. EZH2 is a negative prognostic biomarker associated with immunosuppression in hepatocellular carcinoma. PLoS ONE 15 , e0242191 (2020).
He, P. C. & He, C. m 6 A RNA methylation: from mechanisms to therapeutic potential. EMBO J. 40 , e105977 (2021).
McFadden, M. J. et al. Post-transcriptional regulation of antiviral gene expression by N6-methyladenosine. Cell Rep. 34 , 108798 (2021).
Jin, S. et al. m 6 A RNA modification controls autophagy through upregulating ULK1 protein abundance. Cell Res. 28 , 955–957 (2018).
Wang, X. et al. m 6 A mRNA methylation controls autophagy and adipogenesis by targeting Atg5 and Atg7. Autophagy 16 , 1221–1235 (2020).
Han, D. et al. Anti-tumour immunity controlled through mRNA m 6 A methylation and YTHDF1 in dendritic cells. Nature 566 , 270–274 (2019).
Vizcaino, J. A. et al. The human immunopeptidome project: a roadmap to predict and treat immune diseases. Mol. Cell Proteom. 19 , 31–49 (2020).
Marcu, A. et al. HLA ligand atlas: a benign reference of HLA-presented peptides to improve T-cell-based cancer immunotherapy. J. Immunother. Cancer 9 , e002071 (2021).
Kubiniok, P. et al. Understanding the constitutive presentation of MHC class I immunopeptidomes in primary tissues. iScience 25 , 103768 (2022).
Phillips, E. R. & Perdue, J. F. The expression and localization of surface neoantigens in transformed and untransformed cultured cells infected with avian tumor viruses. J. Supramol. Struct. 4 , 27–44 (1976).
Lennerz, V. et al. The response of autologous T cells to a human melanoma is dominated by mutated neoantigens. Proc. Natl Acad. Sci. USA 102 , 16013–16018 (2005).
Maletzki, C., Schmidt, F., Dirks, W. G., Schmitt, M. & Linnebacher, M. Frameshift-derived neoantigens constitute immunotherapeutic targets for patients with microsatellite-instable haematological malignancies: frameshift peptides for treating MSI + blood cancers. Eur. J. Cancer 49 , 2587–2595 (2013).
McGranahan, N. et al. Clonal neoantigens elicit T cell immunoreactivity and sensitivity to immune checkpoint blockade. Science 351 , 1463–1469 (2016).
Yang, W. et al. Immunogenic neoantigens derived from gene fusions stimulate T cell responses. Nat. Med. 25 , 767–775 (2019).
Khodadoust, M. S. et al. Antigen presentation profiling reveals recognition of lymphoma immunoglobulin neoantigens. Nature 543 , 723–727 (2017).
Haen, S. P., Loffler, M. W., Rammensee, H. G. & Brossart, P. Towards new horizons: characterization, classification and implications of the tumour antigenic repertoire. Nat. Rev. Clin. Oncol. 17 , 595–610 (2020).
Kreiter, S. et al. Mutant MHC class II epitopes drive therapeutic immune responses to cancer. Nature 520 , 692–696 (2015).
Kalaora, S. et al. Use of HLA peptidomics and whole exome sequencing to identify human immunogenic neo-antigens. Oncotarget 7 , 5110–5117 (2016).
Ott, P. A. et al. An immunogenic personal neoantigen vaccine for patients with melanoma. Nature 547 , 217–221 (2017).
Keskin, D. B. et al. Neoantigen vaccine generates intratumoral T cell responses in phase Ib glioblastoma trial. Nature 565 , 234–239 (2019).
Platten, M. et al. A vaccine targeting mutant IDH1 in newly diagnosed glioma. Nature 592 , 463–468 (2021).
Palmer, C. D. et al. Individualized, heterologous chimpanzee adenovirus and self-amplifying mRNA neoantigen vaccine for advanced metastatic solid tumors: phase 1 trial interim results. Nat. Med. 28 , 1619–1629 (2022).
Rotzschke, O. et al. Isolation and analysis of naturally processed viral peptides as recognized by cytotoxic T cells. Nature 348 , 252–254 (1990).
Hunt, D. F. et al. Characterization of peptides bound to the class I MHC molecule HLA-A2.1 by mass spectrometry. Science 255 , 1261–1263 (1992).
Bassani-Sternberg, M. et al. Direct identification of clinically relevant neoepitopes presented on native human melanoma tissue by mass spectrometry. Nat. Commun. 7 , 13404 (2016).
Schuster, H. et al. The immunopeptidomic landscape of ovarian carcinomas. Proc. Natl Acad. Sci. USA 114 , E9942–E9951 (2017).
Shao, W. et al. The SysteMHC Atlas project. Nucleic Acids Res. 46 , D1237–D1247 (2018).
Yi, X. et al. caAtlas: an immunopeptidome atlas of human cancer. iScience 24 , 103107 (2021).
Stopfer, L. E. et al. Absolute quantification of tumor antigens using embedded MHC-I isotopologue calibrants. Proc. Natl Acad. Sci. USA 118 , e2111173118 (2021).
Jaeger, A. M. et al. Deciphering the immunopeptidome in vivo reveals new tumour antigens. Nature 607 , 149–155 (2022).
Kalaora, S. et al. Identification of bacteria-derived HLA-bound peptides in melanoma. Nature 592 , 138–143 (2021).
Nielsen, M., Ternette, N. & Barra, C. The interdependence of machine learning and LC-MS approaches for an unbiased understanding of the cellular immunopeptidome. Expert. Rev. Proteom. 19 , 77–88 (2022).
Bassani-Sternberg, M. et al. Deciphering HLA-I motifs across HLA peptidomes improves neo-antigen predictions and identifies allostery regulating HLA specificity. PLoS Comput. Biol. 13 , e1005725 (2017).
Andreatta, M. et al. MS-Rescue: a computational pipeline to increase the quality and yield of immunopeptidomics experiments. Proteomics 19 , e1800357 (2019).
Alvarez, B. et al. NNAlign_MA; MHC peptidome deconvolution for accurate MHC binding motif characterization and improved T-cell epitope predictions. Mol. Cell Proteom. 18 , 2459–2477 (2019).
Jurtz, V. et al. NetMHCpan-4.0: improved peptide-MHC class I interaction predictions integrating eluted ligand and peptide binding affinity data. J. Immunol. 199 , 3360–3368 (2017).
O’Donnell, T. J., Rubinsteyn, A. & Laserson, U. MHCflurry 2.0: improved pan-allele prediction of MHC class I-presented peptides by incorporating antigen processing. Cell Syst. 11 , 418–419 (2020).
Sarkizova, S. et al. A large peptidome dataset improves HLA class I epitope prediction across most of the human population. Nat. Biotechnol. 38 , 199–209 (2020).
Chen, B. et al. Predicting HLA class II antigen presentation through integrated deep learning. Nat. Biotechnol. 37 , 1332–1343 (2019).
Erhard, F., Dolken, L., Schilling, B. & Schlosser, A. Identification of the cryptic HLA-I immunopeptidome. Cancer Immunol. Res. 8 , 1018–1026 (2020).
Ouspenskaia, T. et al. Unannotated proteins expand the MHC-I-restricted immunopeptidome in cancer. Nat. Biotechnol. 40 , 209–217 (2022).
Blass, E. & Ott, P. A. Advances in the development of personalized neoantigen-based therapeutic cancer vaccines. Nat. Rev. Clin. Oncol. 18 , 215–229 (2021).
Sahin, U. et al. Personalized RNA mutanome vaccines mobilize poly-specific therapeutic immunity against cancer. Nature 547 , 222–226 (2017).
Hilf, N. et al. Actively personalized vaccination trial for newly diagnosed glioblastoma. Nature 565 , 240–245 (2019).
Finn, O. J. A Believer’s overview of cancer immunosurveillance and immunotherapy. J. Immunol. 200 , 385–391 (2018).
Marty, R. et al. MHC-I genotype restricts the oncogenic mutational landscape. Cell 171 , 1272–1283.e15 (2017).
Marty Pyke, R. et al. Evolutionary pressure against MHC class II binding cancer mutations. Cell 175 , 1991 (2018).
Dersh, D., Holly, J. & Yewdell, J. W. A few good peptides: MHC class I-based cancer immunosurveillance and immunoevasion. Nat. Rev. Immunol. 21 , 116–128 (2021).
Van den Eynden, J., Jimenez-Sanchez, A., Miller, M. L. & Larsson, E. Lack of detectable neoantigen depletion signals in the untreated cancer genome. Nat. Genet. 51 , 1741–1748 (2019).
Claeys, A., Luijts, T., Marchal, K. & Van den Eynden, J. Low immunogenicity of common cancer hot spot mutations resulting in false immunogenic selection signals. PLoS Genet. 17 , e1009368 (2021).
Hoyos, D. et al. Fundamental immune-oncogenicity trade-offs define driver mutation fitness. Nature 606 , 172–179 (2022).
O’Donnell, J. S., Teng, M. W. L. & Smyth, M. J. Cancer immunoediting and resistance to T cell-based immunotherapy. Nat. Rev. Clin. Oncol. 16 , 151–167 (2019).
Balachandran, V. P. et al. Identification of unique neoantigen qualities in long-term survivors of pancreatic cancer. Nature 551 , 512–516 (2017).
Luksza, M. et al. A neoantigen fitness model predicts tumour response to checkpoint blockade immunotherapy. Nature 551 , 517–520 (2017).
Luksza, M. et al. Neoantigen quality predicts immunoediting in survivors of pancreatic cancer. Nature 606 , 389–395 (2022).
Fluckiger, A. et al. Cross-reactivity between tumor MHC class I-restricted antigens and an enterococcal bacteriophage. Science 369 , 936–942 (2020).
Zitvogel, L. & Kroemer, G. Cross-reactivity between cancer and microbial antigens. Oncoimmunology 10 , 1877416 (2021).
Au, L. et al. Determinants of anti-PD-1 response and resistance in clear cell renal cell carcinoma. Cancer Cell 39 , 1497–1518.e11 (2021).
Yarchoan, M., Hopkins, A. & Jaffee, E. M. Tumor mutational burden and response rate to PD-1 inhibition. N. Engl. J. Med. 377 , 2500–2501 (2017).
Devarakonda, S. et al. Tumor mutation burden as a biomarker in resected non-small-cell lung cancer. J. Clin. Oncol. 36 , 2995–3006 (2018).
Samstein, R. M. et al. Tumor mutational load predicts survival after immunotherapy across multiple cancer types. Nat. Genet. 51 , 202–206 (2019).
Attermann, A. S., Bjerregaard, A. M., Saini, S. K., Gronbaek, K. & Hadrup, S. R. Human endogenous retroviruses and their implication for immunotherapeutics of cancer. Ann. Oncol. 29 , 2183–2191 (2018).
Faulkner, G. J. et al. The regulated retrotransposon transcriptome of mammalian cells. Nat. Genet. 41 , 563–571 (2009).
Rycaj, K. et al. Cytotoxicity of human endogenous retrovirus K-specific T cells toward autologous ovarian cancer cells. Clin. Cancer Res. 21 , 471–483 (2015).
Jang, H. S. et al. Transposable elements drive widespread expression of oncogenes in human cancers. Nat. Genet. 51 , 611–617 (2019).
Smith, C. C. et al. Endogenous retroviral signatures predict immunotherapy response in clear cell renal cell carcinoma. J. Clin. Invest. 128 , 4804–4820 (2018).
Saini, S. K. et al. Human endogenous retroviruses form a reservoir of T cell targets in hematological cancers. Nat. Commun. 11 , 5660 (2020).
Bullman, S. et al. Analysis of Fusobacterium persistence and antibiotic response in colorectal cancer. Science 358 , 1443–1448 (2017).
Nejman, D. et al. The human tumor microbiome is composed of tumor type-specific intracellular bacteria. Science 368 , 973–980 (2020).
Jin, C. et al. Commensal microbiota promote lung cancer development via γδ T cells. Cell 176 , 998–1013.e16 (2019).
Riquelme, E. et al. Tumor microbiome diversity and composition influence pancreatic cancer outcomes. Cell 178 , 795–806.e12 (2019).
Fu, A. et al. Tumor-resident intracellular microbiota promotes metastatic colonization in breast cancer. Cell 185 , 1356–1372.e26 (2022).
Matson, V. et al. The commensal microbiome is associated with anti-PD-1 efficacy in metastatic melanoma patients. Science 359 , 104–108 (2018).
Routy, B. et al. Gut microbiome influences efficacy of PD-1-based immunotherapy against epithelial tumors. Science 359 , 91–97 (2018).
Sepich-Poore, G. D., Carter, H. & Knight, R. Intratumoral bacteria generate a new class of therapeutically relevant tumor antigens in melanoma. Cancer Cell 39 , 601–603 (2021).
Xavier, J. B. et al. The cancer microbiome: distinguishing direct and indirect effects requires a systemic view. Trends Cancer 6 , 192–204 (2020).
Yoo, S. K., Chowell, D., Valero, C., Morris, L. G. T. & Chan, T. A. Outcomes among patients with or without obesity and with cancer following treatment with immune checkpoint blockade. JAMA Netw. Open 5 , e220448 (2022).
Yoo, S. K., Chowell, D., Valero, C., Morris, L. G. T. & Chan, T. A. Pre-treatment serum albumin and mutational burden as biomarkers of response to immune checkpoint blockade. NPJ Precis. Oncol. 6 , 23 (2022).
Krishna, C., Chowell, D., Gonen, M., Elhanati, Y. & Chan, T. A. Genetic and environmental determinants of human TCR repertoire diversity. Immun. Ageing 17 , 26 (2020).
Middha, S. et al. Majority of B2M-mutant and -deficient colorectal carcinomas achieve clinical benefit from immune checkpoint inhibitor therapy and are microsatellite instability-high. JCO Precis. Oncol. 3 , PO.18.00321 (2019).
PubMed PubMed Central Google Scholar
Yeon Yeon, S. et al. Immune checkpoint blockade resistance-related B2M hotspot mutations in microsatellite-unstable colorectal carcinoma. Pathol. Res. Pract. 215 , 209–214 (2019).
Zhang, C. et al. B2M and JAK1/2-mutated MSI-H colorectal carcinomas can benefit from anti-PD-1 therapy. J. Immunother. 45 , 187–193 (2022).
Zhang, H. et al. B2M overexpression correlates with malignancy and immune signatures in human gliomas. Sci. Rep. 11 , 5045 (2021).
Li, D. et al. β2-Microglobulin maintains glioblastoma stem cells and induces M2-like polarization of tumor-associated macrophages. Cancer Res. 82 , 3321–3334 (2022).
Bern, M. D. et al. Inducible down-regulation of MHC class I results in natural killer cell tolerance. J. Exp. Med. 216 , 99–116 (2019).
McGranahan, N. et al. Allele-specific HLA loss and immune escape in lung cancer evolution. Cell 171 , 1259–1271.e11 (2017).
Gong, X. & Karchin, R. Pan-cancer HLA gene-mediated tumor immunogenicity and immune evasion. Mol. Cancer Res. 20 , 1272–1283 (2022).
Thorsson, V. et al. The immune landscape of cancer. Immunity 48 , 812–830.e14 (2018).
Shklovskaya, E. et al. Tumor MHC expression guides first-line immunotherapy selection in melanoma. Cancers 12 , 3374 (2020).
Liu, D. et al. Integrative molecular and clinical modeling of clinical outcomes to PD1 blockade in patients with metastatic melanoma. Nat. Med. 25 , 1916–1927 (2019).
Axelrod, M. L., Cook, R. S., Johnson, D. B. & Balko, J. M. Biological consequences of MHC-II expression by tumor cells in cancer. Clin. Cancer Res. 25 , 2392–2402 (2019).
Neuwelt, A. J. et al. Cancer cell-intrinsic expression of MHC II in lung cancer cell lines is actively restricted by MEK/ERK signaling and epigenetic mechanisms. J. Immunother. Cancer 8 , e000441 (2020).
Johnson, D. B. et al. Melanoma-specific MHC-II expression represents a tumour-autonomous phenotype and predicts response to anti-PD-1/PD-L1 therapy. Nat. Commun. 7 , 10582 (2016).
Roemer, M. G. M. et al. Major histocompatibility complex class II and programmed death ligand 1 expression predict outcome after programmed death 1 blockade in classic Hodgkin lymphoma. J. Clin. Oncol. 36 , 942–950 (2018).
Gonzalez-Ericsson, P. I. et al. Tumor-specific major histocompatibility-II expression predicts benefit to anti-PD-1/L1 therapy in patients with HER2-negative primary breast cancer. Clin. Cancer Res. 27 , 5299–5306 (2021).
Schirrmacher, V., Schild, H. J., Guckel, B. & von Hoegen, P. Tumour-specific CTL response requiring interactions of four different cell types and recognition of MHC class I and class II restricted tumour antigens. Immunol. Cell Biol. 71 , 311–326 (1993).
Tay, R. E., Richardson, E. K. & Toh, H. C. Revisiting the role of CD4 + T cells in cancer immunotherapy-new insights into old paradigms. Cancer Gene Ther. 28 , 5–17 (2021).
Zander, R. et al. CD4 + T cell help is required for the formation of a cytolytic CD8 + T cell subset that protects against chronic infection and cancer. Immunity 51 , 1028–1042.e4 (2019).
Rosenthal, R. et al. Neoantigen-directed immune escape in lung cancer evolution. Nature 567 , 479–485 (2019).
Thol, K., Pawlik, P. & McGranahan, N. Therapy sculpts the complex interplay between cancer and the immune system during tumour evolution. Genome Med. 14 , 137 (2022).
Homma, Y. et al. Changes in the immune cell population and cell proliferation in peripheral blood after gemcitabine-based chemotherapy for pancreatic cancer. Clin. Transl. Oncol. 16 , 330–335 (2014).
Jimenez-Sanchez, A. et al. Unraveling tumor-immune heterogeneity in advanced ovarian cancer uncovers immunogenic effect of chemotherapy. Nat. Genet. 52 , 582–593 (2020).
Szikriszt, B. et al. A comprehensive survey of the mutagenic impact of common cancer cytotoxics. Genome Biol. 17 , 99 (2016).
Wu, T. et al. Quantification of neoantigen-mediated immunoediting in cancer evolution. Cancer Res. 82 , 2226–2238 (2022).
Motzer, R. J. et al. Molecular subsets in renal cancer determine outcome to checkpoint and angiogenesis blockade. Cancer Cell 38 , 803–817.e4 (2020).
Dong, L. Q. et al. Heterogeneous immunogenomic features and distinct escape mechanisms in multifocal hepatocellular carcinoma. J. Hepatol. 72 , 896–908 (2020).
Tawbi, H. A. et al. Relatlimab and nivolumab versus nivolumab in untreated advanced melanoma. N. Engl. J. Med. 386 , 24–34 (2022).
Frampton, A. E. & Sivakumar, S. A new combination immunotherapy in advanced melanoma. N. Engl. J. Med. 386 , 91–92 (2022).
Marin-Acevedo, J. A., Kimbrough, E. O. & Lou, Y. Next generation of immune checkpoint inhibitors and beyond. J. Hematol. Oncol. 14 , 45 (2021).
Guo, E. et al. WEE1 inhibition induces anti-tumor immunity by activating ERV and the dsRNA pathway. J. Exp. Med. 219 , e20210789 (2022).
Andre, P. et al. Anti-NKG2A mAb is a checkpoint inhibitor that promotes anti-tumor immunity by unleashing both T and NK cells. Cell 175 , 1731–1743.e13 (2018).
Roschewski, M., Longo, D. L. & Wilson, W. H. CAR T-cell therapy for large B-cell lymphoma — who, when, and how? N. Engl. J. Med. 386 , 692–696 (2022).
Yarmarkovich, M. et al. Cross-HLA targeting of intracellular oncoproteins with peptide-centric CARs. Nature 599 , 477–484 (2021).
Bonaventura, P. et al. Identification of shared tumor epitopes from endogenous retroviruses inducing high-avidity cytotoxic T cells for cancer immunotherapy. Sci. Adv. 8 , eabj3671 (2022).
Rapoport, A. P. et al. NY-ESO-1-specific TCR-engineered T cells mediate sustained antigen-specific antitumor effects in myeloma. Nat. Med. 21 , 914–921 (2015).
Cameron, B. J. et al. Identification of a Titin-derived HLA-A1-presented peptide as a cross-reactive target for engineered MAGE A3-directed T cells. Sci. Transl. Med. 5 , 197ra103 (2013).
Zhao, X. et al. Tuning T cell receptor sensitivity through catch bond engineering. Science 376 , eabl5282 (2022).
Bekes, M., Langley, D. R. & Crews, C. M. PROTAC targeted protein degraders: the past is prologue. Nat. Rev. Drug Discov. 21 , 181–200 (2022).
Massafra, V. et al. Proteolysis-targeting chimeras enhance T cell bispecific antibody-driven T cell activation and effector function through increased MHC class I antigen presentation in cancer cells. J. Immunol. 207 , 493–504 (2021).
Duan, Z. & Ho, M. T-cell receptor mimic antibodies for cancer immunotherapy. Mol. Cancer Ther. 20 , 1533–1541 (2021).
Hansen, T. H., Connolly, J. M., Gould, K. G. & Fremont, D. H. Basic and translational applications of engineered MHC class I proteins. Trends Immunol. 31 , 363–369 (2010).
Chang, A. Y. et al. A therapeutic T cell receptor mimic antibody targets tumor-associated PRAME peptide/HLA-I antigens. J. Clin. Invest. 127 , 3557 (2017).
Dao, T. et al. Targeting the intracellular WT1 oncogene product with a therapeutic human antibody. Sci. Transl. Med. 5 , 176ra133 (2013).
Article Google Scholar
Carvajal, R. D. et al. Advances in the clinical management of uveal melanoma. Nat. Rev. Clin. Oncol. 20 , 99–115 (2023).
Nathan, P. et al. Overall survival benefit with tebentafusp in metastatic uveal melanoma. N. Engl. J. Med. 385 , 1196–1206 (2021).
Carvajal, R. D. et al. Phase I study of safety, tolerability, and efficacy of tebentafusp using a step-up dosing regimen and expansion in patients with metastatic uveal melanoma. J. Clin. Oncol. 40 , 1939–1948 (2022).
Liu, X. et al. Development of a TCR-like antibody and chimeric antigen receptor against NY-ESO-1/HLA-A2 for cancer immunotherapy. J. Immunother. Cancer 10 , e004035 (2022).
Hsiue, E. H. et al. Targeting a neoantigen derived from a common TP53 mutation. Science 371 , eabc8697 (2021).
Douglass, J. et al. Bispecific antibodies targeting mutant RAS neoantigens. Sci. Immunol. 6 , eabd5515 (2021).
Ma, J. et al. Bispecific antibodies: from research to clinical application. Front. Immunol. 12 , 626616 (2021).
Hegde, P. S. & Chen, D. S. Top 10 challenges in cancer immunotherapy. Immunity 52 , 17–35 (2020).
FDA. FDA Approves Pembrolizumab for Adults and children with TMB-H Solid Tumors https://www.fda.gov/drugs/drug-approvals-and-databases/fda-approves-pembrolizumab-adults-and-children-tmb-h-solid-tumors (2020).
FDA. FDA Grants Accelerated Approval to Dostarlimab-gxly for dMMR Advanced Solid Tumors https://www.fda.gov/drugs/resources-information-approved-drugs/fda-grants-accelerated-approval-dostarlimab-gxly-dmmr-advanced-solid-tumors (2021).
Valero, C. et al. The association between tumor mutational burden and prognosis is dependent on treatment context. Nat. Genet. 53 , 11–15 (2021).
Valero, C. et al. Response rates to anti-PD-1 immunotherapy in microsatellite-stable solid tumors with 10 or more mutations per megabase. JAMA Oncol. 7 , 739–743 (2021).
Hellmann, M. D. et al. Tumor mutational burden and efficacy of Nivolumab monotherapy and in combination with Ipilimumab in small-cell lung cancer. Cancer Cell 33 , 853–861.e4 (2018).
Wang, F. et al. Evaluation of POLE and POLD1 mutations as biomarkers for immunotherapy outcomes across multiple cancer types. JAMA Oncol. 5 , 1504–1506 (2019).
Andre, T. et al. Pembrolizumab in microsatellite-instability-high advanced colorectal cancer. N. Engl. J. Med. 383 , 2207–2218 (2020).
Le, D. T. et al. PD-1 blockade in tumors with mismatch-repair deficiency. N. Engl. J. Med. 372 , 2509–2520 (2015).
Ma, X. et al. Functional landscapes of POLE and POLD1 mutations in checkpoint blockade-dependent antitumor immunity. Nat. Genet. 54 , 996–1012 (2022).
Bauer, J. et al. The oncogenic fusion protein DNAJB1-PRKACA can be specifically targeted by peptide-based immunotherapy in fibrolamellar hepatocellular carcinoma. Nat. Commun. 13 , 6401 (2022).
Weber, D. et al. Accurate detection of tumor-specific gene fusions reveals strongly immunogenic personal neo-antigens. Nat. Biotechnol. 40 , 1276–1284 (2022).
Yoshihama, S. et al. NLRC5/CITA expression correlates with efficient response to checkpoint blockade immunotherapy. Sci. Rep. 11 , 3258 (2021).
Takahashi, A. et al. Tyrosine kinase inhibitors stimulate HLA class I expression by augmenting the IFNγ/STAT1 signaling in hepatocellular carcinoma cells. Front. Oncol. 11 , 707473 (2021).
Chang, C. H., Hammer, J., Loh, J. E., Fodor, W. L. & Flavell, R. A. The activation of major histocompatibility complex class I genes by interferon regulatory factor-1 (IRF-1). Immunogenetics 35 , 378–384 (1992).
Kriegsman, B. A. et al. Frequent loss of IRF2 in cancers leads to immune evasion through decreased MHC class I antigen presentation and increased PD-L1 expression. J. Immunol. 203 , 1999–2010 (2019).
Schaafsma, E., Fugle, C. M., Wang, X. & Cheng, C. Pan-cancer association of HLA gene expression with cancer prognosis and immunotherapy efficacy. Br. J. Cancer 125 , 422–432 (2021).
Jung, H. et al. DNA methylation loss promotes immune evasion of tumours with high mutation and copy number load. Nat. Commun. 10 , 4278 (2019).
Zhou, L., Mudianto, T., Ma, X., Riley, R. & Uppaluri, R. Targeting EZH2 enhances antigen presentation, antitumor immunity, and circumvents anti-PD-1 resistance in head and neck cancer. Clin. Cancer Res. 26 , 290–300 (2020).
Gambacorta, V. et al. Integrated multiomic profiling identifies the epigenetic regulator PRC2 as a therapeutic target to counteract leukemia immune escape and relapse. Cancer Discov. 12 , 1449–1461 (2022).
Zheng, J. et al. miR-148a-3p silences the CANX/MHC-I pathway and impairs CD8 + T cell-mediated immune attack in colorectal cancer. FASEB J. 35 , e21776 (2021).
Song, D. et al. Insights into the role of ERp57 in cancer. J. Cancer 12 , 2456–2464 (2021).
Nielsen, M. et al. Coexisting alterations of MHC class I antigen presentation and IFNγ signaling mediate acquired resistance of melanoma to post-PD-1 immunotherapy. Cancer Immunol. Res. 10 , 1254–1262 (2022).
Cromme, F. V. et al. Loss of transporter protein, encoded by the TAP-1 gene, is highly correlated with loss of HLA expression in cervical carcinomas. J. Exp. Med. 179 , 335–340 (1994).
Seliger, B. et al. Reduced membrane major histocompatibility complex class I density and stability in a subset of human renal cell carcinomas with low TAP and LMP expression. Clin. Cancer Res. 2 , 1427–1433 (1996).
CAS PubMed Google Scholar
Kaklamanis, L. et al. Loss of major histocompatibility complex-encoded transporter associated with antigen presentation (TAP) in colorectal cancer. Am. J. Pathol. 145 , 505–509 (1994).
CAS PubMed PubMed Central Google Scholar
Lopez de Castro, J. A. How ERAP1 and ERAP2 shape the peptidomes of disease-associated MHC-I proteins. Front. Immunol. 9 , 2463 (2018).
Download references
Acknowledgements
The authors are grateful for the support from NIH grants R35CA232097 (T.A.C.), R01CA205426 (T.A.C.), U54CA274513 (T.A.C.) and T32CA094186 (K.Y.), a Young Investigator Award from ASCO Conquer Cancer Foundation (K.Y.), a RSNA Research Resident Grant (K.Y.), and a Cleveland Clinic VeloSano Impact Award (K.Y.).
Author information
Authors and affiliations.
Department of Radiation Oncology, Taussig Cancer Center, Cleveland Clinic, Cleveland, OH, USA
Kailin Yang, Ahmed Halima & Timothy A. Chan
Center for Immunotherapy and Precision Immuno-Oncology, Cleveland Clinic, Cleveland, OH, USA
Timothy A. Chan
National Center for Regenerative Medicine, Cleveland, OH, USA
Case Comprehensive Cancer Center, Cleveland, OH, USA
You can also search for this author in PubMed Google Scholar
Contributions
All authors made a substantial contribution to all aspects of the preparation of this manuscript.
Corresponding author
Correspondence to Timothy A. Chan .
Ethics declarations
Competing interests.
T.A.C. is a co-founder of and holds equity in Gritstone Oncology; holds equity in An2H; acknowledges grant funding from An2H, AstraZeneca, Bristol Myers Squibb, Eisai, Illumina and Pfizer; has served as an advisor for An2H, AstraZeneca, Bristol Myers Squibb, Eisai, Illumina and MedImmune; and holds ownership of intellectual property on using tumour mutational burden to predict immunotherapy response, which has been licensed to PGDx. K.Y. and A.H. declare no competing interests.
Peer review
Peer review information.
Nature Reviews Clinical Oncology thanks J. Balko and the other, anonymous, peer reviewer(s) for their contribution to the peer review of this work.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Reprints and permissions
About this article
Cite this article.
Yang, K., Halima, A. & Chan, T.A. Antigen presentation in cancer — mechanisms and clinical implications for immunotherapy. Nat Rev Clin Oncol 20 , 604–623 (2023). https://doi.org/10.1038/s41571-023-00789-4
Download citation
Accepted : 25 May 2023
Published : 16 June 2023
Issue Date : September 2023
DOI : https://doi.org/10.1038/s41571-023-00789-4
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies
Sign up for the Nature Briefing: Cancer newsletter — what matters in cancer research, free to your inbox weekly.

Like what you're reading?
How to create a great thesis defense presentation: everything you need to know
Get your team on prezi – watch this on demand video.

Anete Ezera April 13, 2024
Ready to take on your thesis defense presentation? It’s not just about wrapping up years of study; it’s your moment to share your insights and the impact of your work. A standout presentation can make all the difference. It’s your chance to highlight the essentials and really connect with your audience.
This is where Prezi comes into play. Forget about flipping through slide after slide. With Prezi, you craft a narrative that pulls your audience in. It simplifies the complex, ensuring your key points hit home. Let’s explore how Prezi can help transform your thesis defense into a successful presentation.

What is a thesis defense presentation and why are they needed?
Whether you’re preparing for a master’s thesis defense or a Ph.D. thesis defense, this final step in your academic journey is the one with the most significance, as it dramatically influences your final grade. It’s also your chance to display the dedication and effort you’ve put into your research, a way to demonstrate how significant your work is.
So, why is this such a big deal? A good presentation helps convince your teachers that your research is solid and makes a difference in your field. It’s your time to answer questions, show that your research methods were sound, and point out what’s new and interesting about your work. In the end, a great thesis defense presentation helps you finish strong and makes sure you leave a lasting impression as you wrap up this chapter of your academic life.
Best practices for making a successful thesis defense presentation
In order to craft a standout thesis defense presentation, you need to do more than just deliver research findings. Here are some key strategies to ensure success, and how Prezi can play a crucial role in elevating your presentation.
Start with a strong introduction
Kick-off with an engaging introduction that lays out your research question, its significance, and your objectives. This initial segment grabs attention and sets the tone. Using Prezi’s zoom feature can make your introduction pop by visually underscoring key points, helping your audience grasp the importance of your work right from the start.
Organize your presentation clearly
A coherent structure is essential for guiding your audience through your thesis defense presentation. Prezi can help by offering a map view of your content’s layout upfront, providing a clear path through your introduction, methodology, results, and conclusion. This clarity keeps your audience engaged and makes your arguments easier to follow.
Incorporate multimedia elements
Adding multimedia elements like videos, audio clips, and animations can greatly improve the appeal of your thesis defense presentation. Prezi supports the seamless integration of these elements, allowing you to bring your research to life in a more vibrant and engaging way. Videos can serve as powerful testimonials or demonstrations, while animations can help illustrate complex processes or changes over time. This variety keeps your audience engaged and helps convey your message in a more exciting way.

Simplify complex data
Your findings need to be presented in a way that’s easy for your audience to understand. Prezi shines here, with tools that transform intricate data into clear, engaging visuals. By implementing charts and graphs into your presentation, you can make your data stand out and support your narrative effectively.
Engage your audience
Make your thesis defense a two-way conversation by interacting with your audience. Whether it’s through questions, feedback, or direct participation, engagement is key. Prezi allows for a flexible presentation style, letting you navigate sections in response to audience input, creating a dynamic and engaging experience.
Highlight key takeaways
Emphasize the key takeaways of your research throughout your presentation to ensure your audience grasps the most critical aspects of your work. With Prezi, you can use spotlighting and strategic zooming to draw attention to these takeaways, making them stand out. This method helps reinforce your main points, ensuring they stick with your audience long after your presentation concludes. By clearly defining what your audience should remember, you guide their understanding and appreciation of your research’s value and implications.
Practice makes perfect
Confidence in delivery comes from thorough practice. Familiarize yourself with every aspect of your thesis defense presentation, including timing, voice control, and gestures. Prezi Video is a great tool for rehearsing, as it allows you to blend your presentation materials with your on-camera performance, mirroring the live defense setting and helping you polish your delivery.

End with a lasting impression
Conclude your presentation powerfully by summarizing your main findings, their implications, and future research directions. Prezi’s ability to zoom out and show the big picture at your conclusion helps reinforce how each section of your presentation contributes to your overall thesis, ensuring your research leaves a memorable impact on your audience.
By using these tips and taking advantage of what Prezi offers, you can make your thesis defense presentation really stand out. It’ll not only hit the mark with your audience but also clearly show why your research matters.
Meeting tight deadlines with Prezi
Facing a looming deadline for your thesis defense presentation? Prezi offers smart solutions to help you create a polished and engaging presentation quickly, even if it feels like you’re down to the wire.
A closer look at Prezi AI features
Prezi AI is a standout feature for those pressed for time. It assists in structuring your presentation efficiently, suggesting design elements and layouts that elevate your content. This AI-driven approach means you can develop a presentation that looks meticulously planned and executed in a fraction of the time it would normally take. The result? A presentation that communicates the depth and value of your research clearly and effectively, without the last-minute rush being evident. Here’s what Prezi AI can do:
- Streamlined creation process: At the core of Prezi’s efficiency is the AI presentation creator . Perfect for those last-minute crunch times, it’s designed to tackle tight deadlines with ease.
- Easy start: Kick off your presentation creation with just a click on the “Create with AI” button. Prezi AI guides you through a smooth process, transforming your initial ideas or keywords into a structured and visually appealing narrative.
- Visual impact: There’s no need to dive deep into design details. Simply provide some basic input, and Prezi AI will craft it into a presentation that grabs and holds your audience’s attention, making your thesis defense visually compelling.
- AI text editing: Spending too much time fine-tuning your message? Prezi AI text editing features can help. Whether you need to expand on a concept, clarify complex terms, or condense your content without losing impact, Prezi AI streamlines these tasks.
- Content refinement: Adjust text length for deeper explanation, simplify language for better understanding, and ensure your presentation’s content is precise and to the point. Prezi AI editing tools help you refine your message quickly, so you can focus on the essence of your research.
Using Prezi Video for remote thesis defense presentations
For remote thesis defenses, Prezi Video steps up to ensure your presentation stands out. It integrates your on-screen presence alongside your presentation content, creating a more personal and engaging experience for your audience. This is crucial in maintaining attention and interest, particularly in a virtual format where keeping your audience engaged presents additional challenges. Prezi Video makes it seem as though you’re presenting live alongside your slides, helping to simulate the in-person defense experience and keep your audience focused on what you’re saying.

Using these advanced Prezi features, you can overcome tight deadlines with confidence, ensuring your thesis defense presentation is both impactful and memorable, no matter the time constraints.
The Prezi experience: what users have to say
Prezi users have shared compelling insights on how the platform’s unique features have revolutionized their presentations. Here’s how their experiences can inspire your thesis defense presentation:
Storytelling with Prezi
Javier Schwersensky highlights the narrative power of Prezi: “This is a tool that is going to put you ahead of other people and make you look professional and make your ideas stand out,” he remarks. For your thesis defense, this means Prezi can help you craft a narrative that not only presents your research but tells a story that captures and retains the committee’s interest.
Flexibility and creativity
Tamara Montag-Smit appreciates Prezi for its “functionality of the presentation that allows you to present in a nonlinear manner.” This flexibility is key in a thesis defense, allowing you to adapt your presentation flow in real time based on your audience’s engagement or questions, ensuring a more dynamic and interactive defense.
The open canvas
Vitek Dočekal values Prezi’s open canvas , which offers “creative freedom” and the ability to “create a mind map and determine how to best present my ideas.” For your thesis defense, this means Prezi lets you lay out and show off your work in a way that makes sense and grabs your audience’s attention, turning complicated details into something easy and interesting to follow.
Engagement and retention
Adam Rose points out the engagement benefits of Prezi: “Being able to integrate videos is extremely effective in capturing their attention.” When you need to defend a thesis, using Prezi to include videos or interactive content can help keep your committee engaged, making your presentation much more memorable.
These real insights show just how effective Prezi is for crafting truly influential presentations. By incorporating Prezi into your thesis defense presentation, you can create a defense that not only shows how strong your research is but also leaves a lasting impression on your audience.
Thesis defense presentations for inspiration
Prezi is much more than a platform for making presentations; it’s a place where you can find inspiration by browsing presentations that other Prezi users have made. Not only that, but Prezi offers numerous templates that would be useful for thesis defense presentations, making the design process much easier. Here are a few examples that you may find helpful:
Research project template by Prezi
This Prezi research project template stands out as an ideal choice for thesis defense presentations due to its well-structured format that facilitates storytelling from start to finish. It begins with a clear introduction and problem statement, setting a solid foundation for the narrative. The inclusion of sections for user research, interviews, demographics, and statistics allows for a detailed presentation of the research process and findings, which are crucial when defending a thesis.
Visual elements like user mapping and journey maps help make complex information understandable and engaging, which is crucial for maintaining the committee’s attention. Additionally, addressing pain points and presenting prototypes showcases problem-solving efforts and practical applications of the research. The template culminates in a conclusion that ties everything together, emphasizing the research’s impact and future possibilities. Its comprehensive yet concise structure makes it an excellent tool for communicating the depth and significance of your work in a thesis defense.
Civil rights movement Prezi
This Prezi on the Civil Rights Movement exemplifies an effective thesis defense presentation by seamlessly blending structured content, multimedia enhancements, and dynamic navigation. It organizes information into coherent sections like “About,” “Key Events,” and “Key People,” offering a comprehensive view ideal for a thesis presentation. The strategic use of videos adds depth, providing historical context in a dynamic way that text alone cannot, enhancing the audience’s engagement and understanding.
Furthermore, Prezi’s open canvas feature brings the narrative to life, allowing for a fluid journey through the Civil Rights Movement. This method of presentation, with its zooming and panning across a virtual canvas, not only captivates but also helps to clarify the connections between various elements of the research, showcasing how to effectively communicate complex ideas in a thesis defense.
AI-assisted history template
This AI-assisted presentation template stands out as a great choice for thesis defense presentations, especially for those rooted in historical research. By merging striking visuals with rich, informative content, you can use this template to craft a narrative that breathes life into past events, guiding the audience on an engaging journey through time. Its sequential storytelling approach, empowered by Prezi AI , ensures a smooth transition from one historical point to the next, demonstrating the depth and continuity of your research. This template showcases Prezi AI’s capability to enhance narrative flow. By integrating advanced visuals and text, it captivates audiences and makes it an invaluable tool for presenting complex historical theses in a clear, compelling way.
Master your final grade with a Prezi thesis defense presentation
Preparing for a thesis defense, whether for a master’s or Ph.D., is a pivotal moment that significantly influences your final grade. It’s your platform to demonstrate the dedication behind your research and its importance in your field. A well-executed presentation convinces your educators of your research’s validity and your ability to bring fresh perspectives to light.
To craft a successful thesis defense presentation, Prezi’s innovative features can be a game-changer. Prezi can empower you to transform presentations into captivating stories and provide you with the flexibility and creative freedom needed to make your presentation an outstanding success. Incorporating videos or utilizing Prezi’s non-linear presentation style can keep your committee engaged and emphasize your research’s significance.
Prezi also serves as a hub of inspiration, offering templates perfect for thesis defenses. From structured research project templates to dynamic historical narratives, Prezi provides tools that communicate your thesis’s depth and significance effectively, ensuring you leave a memorable impact on your audience. So, it’s time to revamp your thesis defense presentation and change it from dull to inspirational with Prezi.

Give your team the tools they need to engage
Like what you’re reading join the mailing list..
- Prezi for Teams
- Top Presentations
COMMENTS
Introduction. Breech presentation refers to the fetus in the longitudinal lie with the buttocks or lower extremity entering the pelvis first. The three types of breech presentation include frank breech, complete breech, and incomplete breech. In a frank breech, the fetus has flexion of both hips, and the legs are straight with the feet near the ...
INTRODUCTION. Breech presentation, which occurs in approximately 3 percent of fetuses at term, describes the fetus whose presenting part is the buttocks and/or feet. Although most breech fetuses have normal anatomy, this presentation is associated with an increased risk for congenital malformations and mild deformations, torticollis, and ...
Breech presentation is defined as a fetus in a longitudinal lie with the buttocks or feet closest to the cervix. This occurs in 3-4% of all deliveries. The percentage of breech deliveries decreases with advancing gestational age from 22-25% of births prior to 28 weeks' gestation to 7-15% of births at 32 weeks' gestation to 3-4% of births at term.
It does not include antenatal or postnatal care. External cephalic version (ECV) is the topic of the separate Royal College of Obstetricians and Gynaecologists (RCOG) Green-top Guideline No. 20a: External Cephalic Version and Reducing the Incidence of Term Breech Presentation. 1. 2 Introduction and background epidemiology
Introduction. Breech presentation is a type of malpresentation and occurs when the fetal head lies over the uterine fundus and fetal buttocks or feet present over the maternal pelvis (instead of cephalic/head presentation). The incidence in the United Kingdom of breech presentation is 3-4% of all fetuses. 1.
Breech birth is a divisive clinical issue, however vaginal breech births continue to occur despite a globally high caesarean section rate for breech presenting fetuses. Inconsistencies are known to exist between clinical practice guidelines relating to the management of breech presentation.
Introduction. Breech presentation refers to the fetus in the longitudinal lie with the buttocks or lower extremity entering the pelvis first. The three types of breech presentation include frank breech, complete breech, and incomplete breech. In a frank breech, the fetus has flexion of both hips, and the legs are straight with the feet near the ...
1. Background. The management of breech presentation continues to cause academic and clinical contention globally [[1], [2], [3]].In recent years, research has shown that if certain criteria are met, and appropriately experienced and skilled clinicians are available, Vaginal Breech Birth (VBB) is a safe option [[4], [5], [6]].However, with Caesarean Section (C/S) rates for breech presentation ...
Background and Introduction Breech presentation occurs frequently among preterm babies in utero, however, most babies will spontaneously revert to a cephalic presentation. As a result approximately 3% of babies are in the breech position at term (Hickok DE et al, 1992). In clinical practice this presents challenges regarding mode of delivery
1. Introduction The incidence of breech presentation decreases from approximately 20% at 28 weeks gestation to between 3-4% at term. Spontaneous changes from breech to cephalic presentation occur with decreasing frequency as gestational age advances in the third trimester. Breech presentations are
At full term, around 3%-4% of births are breech. The different types of breech presentations include: Complete: The fetus's knees are bent, and the buttocks are presenting first. Frank: The fetus's legs are stretched upward toward the head, and the buttocks are presenting first. Footling: The fetus's foot is showing first.
The most widely quoted study regarding the management of breech presentation at term is the 'Term Breech Trial'. Published in 2000, this large, international multicenter randomised clinical trial compared a policy of planned vaginal delivery with planned caesarean section for selected breech presentations.
Comparing the results, the introduction of ECV has led to a 39% decrease (from 4.1 to 2.5%) in breech deliveries, a 47.1% decrease (from 22.7 to 12%) in breech presentation as an indication for CS ...
1 INTRODUCTION. Approximately 3% of all infants are born in breech presentation with bottom first, sometimes a foot or knee is leading. 1-3 The risk of breech presentation is sometimes increased, for example, in malformations of the child or the uterus; however, most of the infants and mothers among breech deliveries are totally healthy. 4 Vaginal delivery in breech compared with cephalic ...
Introduction. The prevalence of pregnancies with breech presentation is surprisingly similar globally, involving 3-4% of fetuses by the time of labor 1-4.There is some uncertainty regarding the exact etiology of breech presentation, although several risk factors are well described in the literature, such as older maternal age, primiparity, lower fetal weight, lower gestational age at ...
Background The incidence of breech presentation is 3-4% at tem. Since the publication of Term Breech Trial, elective Caesarian section (ELCS) has been the default mode of delivery with little or no opportunity for mothers to consider alternative approaches to manage breech presentation at term. Methods Once a week Breech Clinic was introduced in June 2012 with a dedicated team of two ...
Priming of CD8 + T cells via cross-presentation. Productive priming of naive CD8 + T cells to tumour cell-associated antigens, which commonly occurs in the draining lymph nodes, is a prerequisite ...
This AI-assisted presentation template stands out as a great choice for thesis defense presentations, especially for those rooted in historical research. By merging striking visuals with rich, informative content, you can use this template to craft a narrative that breathes life into past events, guiding the audience on an engaging journey ...
INTRODUCTION. Breech presentation, which occurs in approximately 3 percent of fetuses at term, describes the fetus whose presenting part is the buttocks and/or feet. Although most breech fetuses have normal anatomy, this presentation is associated with an increased risk for congenital malformations and mild deformations, torticollis, and ...
MJF 032024 US Public Health Service standards 1946 and 1968 established standard for coliforms, inorganic and radiological contaminants as well as aesthetic standard in public water supplies.