
- Department of Economic and Social Affairs Social Inclusion
- Meet our Director
- Milestones for Inclusive Social Development.
- Second World Summit For Social Development 2025
- World Summit For Social Development 1995
- 2030 Agenda for Sustainable Development
- Sustainable Development Goals (SDGs)
- UN Common Agenda
- International Days
- International Years
- Social Media
- Social Development Issues
- Cooperatives
- Digital Inclusion
- Employment & Decent Work
- Indigenous Peoples
- Poverty Eradication
- Social Inclusion
- Social Protection
- Sport for Development & Peace
- Commission for Social Development (CSocD)
- Conference of States Parties to the CRPD (COSP)
- General Assembly Second Committee
- General Assembly Third Committee
- Open-Ended Working Group (OEWG) on Ageing
- United Nations Permanent Forum on Indigenous Issues (UNPFII)
- Publications
- World Social Report
- World Youth Report
- UN Flagship Report On Disability And Development
- State Of The World’s Indigenous Peoples
- Policy Briefs
- General Assembly Reports and Resolutions
- ECOSOC Reports and Resolutions
- UNPFII Recommendations Database
- Capacity Development
- Civil Society
- Expert Group Meetings

Everyone Included: Social Impact of COVID-19

We are facing a global health crisis unlike any in the 75-year history of the United Nations — one that is killing people, spreading human suffering, and upending people’s lives. But this is much more than a health crisis. It is a human, economic and social crisis. The coronavirus disease (COVID-19), which has been characterized as a pandemic by the World Health Organization (WHO), is attacking societies at their core.
The UN Department of Economic and Social Affairs (UN DESA) is a pioneer of sustainable development and the home of the Sustainable Development Goals (SDGs), where each goal finds its space and where all stakeholders can do their part to leave no one behind. UN DESA through the Division for Inclusive Social Development (DISD), monitors national and global socio-economic trends, identifies emerging issues, and assesses their implications for social policy at the national and international levels. To this end, we are a leading analytical voice for promoting social inclusion, reducing inequalities and eradicating poverty.
The COVID-19 outbreak affects all segments of the population and is particularly detrimental to members of those social groups in the most vulnerable situations, continues to affect populations, including people living in poverty situations, older persons, persons with disabilities, youth, and indigenous peoples. Early evidence indicates that that the health and economic impacts of the virus are being borne disproportionately by poor people. For example, homeless people, because they may be unable to safely shelter in place, are highly exposed to the danger of the virus. People without access to running water, refugees, migrants, or displaced persons also stand to suffer disproportionately both from the pandemic and its aftermath – whether due to limited movement, fewer employment opportunities, increased xenophobia etc.
If not properly addressed through policy the social crisis created by the COVID-19 pandemic may also increase inequality, exclusion, discrimination and global unemployment in the medium and long term. Comprehensive, universal social protection systems, when in place, play a much durable role in protecting workers and in reducing the prevalence of poverty, since they act as automatic stabilizers. That is, they provide basic income security at all times, thereby enhancing people’s capacity to manage and overcome shocks.
As emphasized by the United Nations Secretary-General, during the launch of a COVID-19 Global Humanitarian Response Plan on 23 March 2020 “We must come to the aid of the ultra-vulnerable – millions upon millions of people who are least able to protect themselves. This is a matter of basic human solidarity. It is also crucial for combating the virus. This is the moment to step up for the vulnerable.”
Older Persons

Older persons are not just struggling with greater health risks but are also likely to be less capable of supporting themselves in isolation. Although social distancing is necessary to reduce the spread of the disease, if not implemented correctly, such measures can also lead to increased social isolation of older persons at a time when they may be at most need of support.
The discourse around COVID-19, in which it is perceived as a disease of older people, exacerbates negative stereotypes about older persons who may be viewed as weak, unimportant and a burden on society. Such age-based discrimination may manifest in the provision of services because the treatment of older persons may be perceived to have less value than the treatment of younger generations. International human rights law guarantees everyone the right to the highest attainable standard of health and obligates Governments to take steps to provide medical care to those who need it. Shortages of ventilators, for example, necessitate the adoption of triage policies and protocols based on medical, evidence-based and ethical factors, rather than arbitrary decisions based on age. In this context, solidarity between generations, combating discrimination against older people, and upholding the right to health, including access to information, care and medical services is key. Read more..
Persons with Disabilities

General individual self-care and other preventive measures against the COVID-19 outbreak can entail challenges for persons with disabilities. For instance, some persons with disabilities may have difficulties in implementing measures to keep the virus at bay, including personal hygiene and recommended frequent cleaning of surfaces and homes. Cleaning homes and washing hands frequently can be challenging, due to physical impairments, environmental barriers, or interrupted services. Others may not be able to practice social distancing or cannot isolate themselves as thoroughly as other people, because they require regular help and support from other people for every day self-care tasks.
To ensure that persons with disabilities are able to access to information on COVID-19, it must be made available in accessible formats. Healthcare buildings must also be physically accessible to persons with mobility, sensory and cognitive impairments. Moreover, persons with disabilities must not be prevented from accessing the health services they need in times of emergency due to any financial barriers. Read more..

In terms of employment, youth are disproportionately unemployed, and those who are employed often work in the informal economy or gig economy, on precarious contracts or in the service sectors of the economy, that are likely to be severely affected by COVID-19.
More than one billion youth are now no longer physically in school after the closure of schools and universities across many jurisdictions. The disruption in education and learning could have medium and long-term consequences on the quality of education, though the efforts made by teachers, school administrations, local and national governments to cope with the unprecedented circumstances to the best of their ability should be recognized. Many vulnerable youth such as migrants or homeless youth are in precarious situations. They are the ones who can easily be overlooked if governments do not pay specific attention, as they tend to be already in a situation without even their minimum requirements being met on health, education, employment and well-being. Read more..

The first point of prevention is the dissemination of information in indigenous languages, thus ensuring that services and facilities are appropriate to the specific situation of indigenous peoples, and all are reached.
The large number of indigenous peoples who are outside of the social protection system further contributes to vulnerability, particularly if they are dependent on income from the broader economy – produce, tourism, handicrafts and employment in urban areas. In this regard, Governments should ensure that interim financial support measures include indigenous peoples and other vulnerable groups.
Indigenous peoples are also seeking their own solutions to this pandemic. They are taking action and using traditional knowledge and practices as well as preventive measures – in their languages. Read more..
Sport for Development and Peace

Since its onset, the COVID-19 pandemic has spread to almost all countries of the world. Social and physical distancing measures, lockdowns of businesses, schools and overall social life, which have become commonplace to curtail the spread of the disease, have also disrupted many regular aspects of life, including sport and physical activity. This policy brief highlights the challenges COVID-19 has posed to both the sporting world and to physical activity and well-being, including for marginalized or vulnerable groups. It further provides recommendations for Governments and other stakeholders, as well as for the UN system, to support the safe reopening of sporting events, as well as to support physical activity during the pandemic and beyond.
To safeguard the health of athletes and others involved, most major sporting events at international, regional and national levels have been cancelled or postponed – from marathons to football tournaments, athletics championships to basketball games, handball to ice hockey, rugby, cricket, sailing, skiing, weightlifting to wrestling and more. The Olympics and Paralympics, for the first time in the history of the modern games, have been postponed, and will be held in 2021. Read more..

“This is the moment to step up for the vulnerable” “Older persons, persons with chronic illness and persons with disabilities face particular, disproportionate risks, and require an all-out effort to save their lives and protect their future.” UN Secretary-General António Guterres launches a COVID-19 Global Humanitarian Response Plan together with Mark Lowcock, USG for Humanitarian Affairs; Tedros Ghebreyesus, Director-General of WHO and Henrietta Fore, Executive Director of UNICEF, 23 March 2020

Statement on COVID-19 by Under-Secretary-General Liu Zhenmin

It presents detailed analysis and solid evidence needed for effective decision-making on a number of critical social and economic issues – including designing inclusive stimulus packages; preventing a global debt crisis; supporting countries in special situations; protecting the most vulnerable groups of people; strengthening the role of science, technology and institutions for an effective response; and working together to build back better and achieve the 2030 Agenda for Sustainable Development.

We need solidarity, political will and innovative policy action to protect vulnerable people and their well-being, and uphold the right to health, including access to information, care and medical services.
* When Everyone is Included, Everyone Benefits. *
For more information about United Nations Coronavirus global health emergency, please visit: https://www.un.org/coronavirus

Our Common Agenda is the Secretary-General's vision for the future of global cooperation. It calls for inclusive, networked, and effective multilateralism to better respond and deliver for the people and planet and to get the world back on track by turbocharging action on the Sustainable Development Goals . It outlines possible solutions to address the gaps and risks that have emerged since 2015, calling for a Summit of the Future that will be held in 2024. Read the report / Read the Summary / Learn More About Our Common Agenda Policy Brief: - Future Generations - Emergency Platform - Youth Engagement - Global Digital Impact - Information Integrity
The 75th Anniversary of the United Nations was marked in June 2020 with a declaration by Member States that included 12 overarching commitments along with a request to the Secretary-General for recommendations to address both current and future challenges. In September 2021, the Secretary-General responded with his report, Our Common Agenda , a wake-up call to speed up the implementation of the Sustainable Development Goals and propel the commitments contained in the UN75 Declaration. In some cases, the proposals addressed gaps that emerged since 2015, requiring new intergovernmental agreements. The report, therefore, called for a Summit of the Future to forge a new global consensus on readying ourselves for a future that is rife with risks but also opportunities. The General Assembly welcomed the submission of the “rich and substantive” report and agreed to hold the Summit on 22-23 September 2024, preceded by a ministerial meeting in 2023. An action-oriented Pact for the Future is expected to be agreed by Member States through intergovernmental negotiations on issues they decide to take forward.
For 2023 SDG Summit, please visit https://www.un.org/en/ conferences/SDGSummit2023
- COVID-19: How the data and statistical community stepped up to the new challenges
- Social policy and social protection measures to build Africa better post-COVID-19
- Strengthening Data Governance for Effective Use of Open Data and Big Data Analytics for Combating COVID-19
- The long-term impact of COVID-19 on poverty
- COVID-19 and a primer on shock-responsive social protection systems
- Achieving SDGs in the wake of COVID-19: Scenarios for policymakers
- The role of public service and public servants during the COVID-19 pandemic
- Forests: at the heart of a green recovery from COVID-19 pandemic
- Resilient institutions in times of crisis: transparency, accountability and participation at the national level key to effective response to COVID-19
- Responses to the COVID-19 catastrophe could turn the tide on inequality
- Protecting and mobilizing youth in COVID-19 responses
- The COVID-19 crisis through the disability and gender lens
- United Nations Comprehensive Response to COVID-19 Saving Lives, Protecting Societies, Recovering Better
- UN Secretary-General’s Policy Brief: Impact of COVID-19 in Africa
- UN Secretary-General’s Policy Brief: The Impact of COVID-19 on South-East Asia
- UN Secretary-General’s Policy Brief: The Impact of COVID-19 on the Arab Region An Opportunity to Build Back Better
- UN Secretary-General’s Policy Brief: The Impact of COVID-19 on Latin America and the Caribbean
- UN Secretary-General’s Policy Brief: The Impact of COVID-19 on Food Security and Nutrition
- UN Secretary-General’s Policy Brief: COVID-19 and Universal Health Coverage
- COVID-19, Inequalities and Building Back Better: Policy Brief by the HLCP Inequalities Task Team
- UN Secretary-General’s Policy Brief: COVID-19 and the Need for Action on Mental Health
- Tackling the inequality pandemic: a New Social Contract for a new era
- UN Secretary-General’s Policy Brief: Education during COVID-19 and beyond
- UN Report on “Shared Responsibility, Global Solidarity: Responding to the socio-economic impacts of COVID-19 | The Secretary-General’s UN Response and Recovery Fund
- UN Secretary-General’s Policy Brief: The Impact of COVID-19 on older persons
- UN Secretary-General’s Policy Brief: A Disability-Inclusive Response to COVID-19
- UN Secretary-General’s Policy Brief: COVID-19 and Human Rights: We are all in this together
- Special UN DESA Voice edition puts spotlight on COVID-19 impact on our lives and societies
- WHO is working closely with global experts, governments and partners to rapidly expand scientific knowledge on this new virus, to track the spread and virulence of the virus, and to provide advice to countries and individuals on measures to protect health and prevent the spread of this outbreak. Resources on Coronavirus disease (COVID-19) Pandemic by WHO.
- A new web portal that showcases UN DESA’s response to the global COVID-19 pandemic has been launched. The portal will shine a light on the cutting-edge analysis and policy advice in those areas where UN DESA’s voice is critical to addressing this global crisis. The portal will feature a series of policy briefs on COVID-19, which draw on unique expertise from around the Department.
- COVID-19 Outbreak and Gender: Key Advocacy Points from Asia and the Pacific by UN Women
- COVID-19 and the world of work by ILO
- Why Indigenous languages matter: The International Decade on Indigenous Languages 2022–2032
- Promoting youth participation in decision-making and public service delivery through harnessing digital technologies
- Old age inequality begins at birth: life course influences on late-life disability
- Old-age poverty has a woman’s face
- The monetary policy response to COVID-19: the role of asset purchase programmes
- COVID-19 pandemic disruption – Implications on the full deployment of the United Nations Legal Identity Agenda
- Policy implications of the disruption of the implementation of the 2020 World Population and Housing Census Programme due to the COVID-19 pandemic
- Horizontal and vertical integration are more necessary than ever for COVID-19 recovery and SDG implementation
- Digitally enabled new forms of work and policy implications for labour regulation frameworks and social protection systems
- Reducing poverty and inequality in rural areas: key to inclusive development
- COVID-19 and Beyond: Scaling up Private Investment for Sustainable Development
- Leveraging digital technologies for social inclusion
- The politics of economic insecurity in the COVID-19 era
- A new global deal must promote economic security
- Recovering from COVID-19: the importance of investing in global public goods for health
- Achieving the SDGs through the COVID-19 response and recovery
- COVID-19 poses grievous economic challenge to landlocked developing countries
- How can investors move from greenwashing to SDG-enabling?
- COVID-19: Reaffirming State-People Governance Relationships
- The impact of COVID-19 on sport, physical activity and well-being and its effects on social development
- COVID-19 and sovereign debt
- COVID-19 pandemic deals a huge blow to the manufacturing exports from LDCs
- The Impact of COVID-19 on Indigenous Peoples
- Leaving no one behind: the COVID-19 crisis through the disability and gender lens
- COVID-19 and Older Persons: A Defining Moment for an Informed, Inclusive and Targeted Response
- Responses to the COVID-19 catastrophe could turn the tide on inequality
- COVID-19 pandemic: a wake-up call for better cooperation at the science-policy-society interface
- COVID-19: Embracing digital government during the pandemic and beyond
- Commodity-dependent economies face mounting economic challenge as the pandemic ravages developed countries
- Corona crisis causes turmoil in financial markets
- COVID-19: Addressing the social crisis through fiscal stimulus plans
- COVID-19: Disrupting lives, economies and societies
In order to highlight the work that civil society organizations are doing on the ground, and the value added that they bring to the global response to the pandemic, the UN is inviting civil society to share their stories. Whatever the area of work of your organization, we believe that our common purpose will lift us during this difficult time, and that we can learn from and build on each other’s efforts. If your organization has been active in identifying or meeting the needs arising from COVID19 in your community, please follow this link and share your experiences, photos and videos with us so we can highlight your learnings. Submit your story.
For more information, please visit: www.un.org/en/civil-society/page/coronavirus-disease-covid-19

UN Chief Economist Mr. Elliott Harris and other experts from UN DESA have shared the main findings of three new briefing papers on the social, economic and financial impacts of COVID-19, as well as public policy recommendations. The online webinar took place on Thursday, 9 April 2020.
Watch a recording of this event on Facebook. Access the presentation here.

Join UN DESA’s Assistant Secretary-General for Policy Coordination and Inter-Agency Affairs Ms. Maria-Francesca Spatolisano, Mr. Fabrizio Hochschild-Drummond , Special Adviser to the Secretary-General on the Preparations for the Commemoration of the United Nations 75th Anniversary, and UN DESA experts for the second UN DESA Webinar on COVID-19: Strengthening Science and Technology and Addressing Inequalities on 6 May 2020, from 10 am to 12 noon EDT.
Watch a recording of this event on Facebook. Access the presentation here .
For more webinars, please visit https://social.desa.un.org/events/type/webinar

Throughout the COVID-19 pandemic, UN DESA has published a series of policy briefs in addition to its regular work in support of the Sustainable Development Goals (SDGs). To support this work and other initiatives of the Department and the wider UN system, UN DESA launched a Global Policy Dialogue Series in July 2020 aimed at highlighting solutions to the economic and social impacts of the pandemic. The series is made possible through the United Nations Peace and Development Trust Fund .
The sessions are dynamic, with UN DESA using its convening power to bring together global thought leaders and its own socioeconomic experts to consider today’s major issues. The conversations, typically 90 minutes long, are led by a journalist moderator to ensure that the discussions are sharp and to the point. UN DESA partners with other UN entities and top socioeconomic forums, and broadcasts everything live on the Department’s Facebook page to expand its reach to audiences that may not typically follow UN proceedings. The events are held in English with translation in American Sign Language and captions available in the six official UN languages.
The Dialogues aim to help countries recover better from the pandemic and closely align UN DESA’s work with the Decade of Action . The results of these discussions are shared with UN leadership and will inform future work on the economic and social effects of the pandemic.
- UN DESA Global Policy Dialogues to Turbocharge SDG Implementation
- Youth and Indigenous Solutions for Water
- Leaving No One Behind in an Ageing World: A UN DESA Global Policy Dialogue
- Building a Sustainable World for 8 Billion People: A UN DESA Fireside Chat
- Preparing for 8 Billion People: A UN DESA Global Policy Dialogue
- Protecting Biodiversity in Times of Crisis: Exploring SDGs 14 and 15
- Promoting Gender Equality Through Education: Exploring SDGs 4 and 5
- Big Questions for the Global Economic Recovery
- The Future of Sustainable Development Financing
- The Future of Population Growth
- The Future of Money
- The Future of Trust in Government
- The Future of Our Planet
- The Future of Community
- The Future of Work
- Financing Global Climate Action and Promoting Digital Solutions
- Strengthening Sustainable Forest and Ocean Management to Mitigate Climate Change
- Imagining the Carbon-neutral Future: Transformations in Energy and Transport
- Building Food and Water Security in an Era of Climate Shocks
- Shaping a New Social Contract: Session 2
- Shaping a New Social Contract: Session 1
- Advancing equitable livelihoods in food systems
- Gender Equality: A Data and Policy Dialogue
- Technological and Science-based Solutions to the COVID-19 Challenge
- Navigating Uncertainties: An Intergenerational dialogue on COVID-19 and youth employment
- Recover Better: Economic and Social Challenges and Opportunities
- COVID 19 and the disability movement by the International Disability Alliance (IDA)
- Families and family policies after COVID-19 by the International Federation for Family Development (IFFD)
- Search Search
Social and economic impact of COVID-19
Download the full working paper
Subscribe to Global Connection
Eduardo levy yeyati and eduardo levy yeyati former nonresident senior fellow - global economy and development @eduardoyeyati federico filippini federico filippini visiting professor - universidad torcuato di tella @efefilippini.
June 8, 2021
Introduction
The impact of the pandemic on world GDP growth is massive. The COVID-19 global recession is the deepest since the end of World War II (Figure 1). The global economy contracted by 3.5 percent in 2020 according to the April 2021 World Economic Outlook Report published by the IMF, a 7 percent loss relative to the 3.4 percent growth forecast back in October 2019. While virtually every country covered by the IMF posted negative growth in 2020 (IMF 2020b), the downturn was more pronounced in the poorest parts of the world (Noy et al. 2020) (Figure 2).

The impact of the shock is likely to be long-lasting. While the global economy is expected to recover this year, the level of GDP at the end of 2021 in both advanced and emerging market and developing economies (EMDE) is projected to remain below the pre-virus baseline (Figure 3). As with the immediate impact, the magnitude of the medium-term cost also varies significantly across countries, with EMDE suffering the greatest loss. The IMF (2021) projects that in 2024 the World GDP will be 3 percent (6 percent for low-income countries (LICs)) below the no-COVID scenario. Along the same lines, Djiofack et al. (2020) estimate that African GDP would be permanently 1 percent to 4 percent lower than in the pre-COVID outlook, depending on the duration of the crisis.

The pandemic triggered a health and fiscal response unprecedented in terms of speed and magnitude. At a global scale, the fiscal support reached nearly $16 trillion (around 15 percent of global GDP) in 2020. However, the capacity of countries to implement such measures varied significantly. In this note, we identify three important preexisting conditions that amplified the impact of the shock:
- Fiscal space: The capacity to support household and firms largely depends on access to international financial markets,
- State capacity: Fast and efficient implementation of policies to support household and firms requires a substantial state capacity and well-developed tax and transfer infrastructure; and
- Labor market structure: A large share of informal workers facing significant frictions to adopt remote working, and high levels of poverty and inequality, deepen the deleterious impact of the crisis.
Additionally, the speed and the strength of the recovery will be crucially dependent on the capacity of the governments to acquire and roll out the COVID-19 vaccines.
This paper presents a succinct summary of the existing economic literature on the economic and fiscal impact of the pandemic, and a preliminary estimate of the associated economic cost. It documents the incidence of initial conditions (with a particular focus on the role of the labor market channel) on the transmission of the shock and the speed and extent of the expected recovery, summarizes how countries attempted to attenuate the economic consequences and the international financial institutions assisted countries, reports preliminary accounts of medium-term COVID-related losses, and concludes with some forward-looking considerations based on the lessons learned in 2020.
Related Content
Homi Kharas, Meagan Dooley
June 2, 2021
Wolfgang Fengler, Homi Kharas
May 20, 2021
Global Economy and Development
Mark Schoeman
May 16, 2024
Ben S. Bernanke, Olivier Blanchard
Joseph Asunka, Landry Signé
May 15, 2024
- Frontiers in Genetics
- ELSI in Science and Genetics
- Research Topics
COVID-19 pandemics: ethical, legal and social issues
Total Downloads
Total Views and Downloads
About this Research Topic
Living through the Covid-19 pandemic, many have seen a number of ethical, legal, and social issues arise as a result of the virus rapidly spreading worldwide. This timely special issue is designed to be a mid-stream retrospective: look at presenting a broad array of topics at the intersection of science and ...
Keywords : covid-19, pandemic, ESLI, patient screening, data privacy, contact tracing, quarantine measures, lockdown, drug and vaccine development
Important Note : All contributions to this Research Topic must be within the scope of the section and journal to which they are submitted, as defined in their mission statements. Frontiers reserves the right to guide an out-of-scope manuscript to a more suitable section or journal at any stage of peer review.
Topic Editors
Topic coordinators, recent articles, submission deadlines.
Submission closed.
Participating Journals
Total views.
- Demographics
No records found
total views article views downloads topic views
Top countries
Top referring sites, about frontiers research topics.
With their unique mixes of varied contributions from Original Research to Review Articles, Research Topics unify the most influential researchers, the latest key findings and historical advances in a hot research area! Find out more on how to host your own Frontiers Research Topic or contribute to one as an author.
Special Issue: COVID-19
This essay was published as part of a Special Issue on Misinformation and COVID-19, guest-edited by Dr. Meghan McGinty (Director of Emergency Management, NYC Health + Hospitals) and Nat Gyenes (Director, Meedan Digital Health Lab).
Peer Reviewed
The causes and consequences of COVID-19 misperceptions: Understanding the role of news and social media
Article metrics.
CrossRef Citations
Altmetric Score
PDF Downloads
We investigate the relationship between media consumption, misinformation, and important attitudes and behaviours during the coronavirus disease 2019 (COVID-19) pandemic. We find that comparatively more misinformation circulates on Twitter, while news media tends to reinforce public health recommendations like social distancing. We find that exposure to social media is associated with misperceptions regarding basic facts about COVID-19 while the inverse is true for news media. These misperceptions are in turn associated with lower compliance with social distancing measures. We thus draw a clear link from misinformation circulating on social media, notably Twitter, to behaviours and attitudes that potentially magnify the scale and lethality of COVID-19.
Department of Political Science, McGill University, Canada
Munk School of Global Affairs and Public Policy, University of Toronto, Canada
Max Bell School of Public Policy, McGill University, Canada
School of Computer Science, McGill University, Canada
Department of Languages, Literatures, and Cultures, McGill University, Canada
Computer Science Program, McGill University, Canada
Research Questions
- How prevalent is misinformation surrounding COVID-19 on Twitter, and how does this compare to Canadian news media?
- Does the type of media one is exposed to influence social distancing behaviours and beliefs about COVID-19?
- Is there a link between COVID-19 misinformation and perceptions of the pandemic’s severity and compliance with social distancing recommendations?
Essay Summary
- We evaluate the presence of misinformation and public health recommendations regarding COVID-19 in a massive corpus of tweets as well as all articles published on nineteen Canadian news sites. Using these data, we show that preventative measures are more encouraged and covered on traditional news media, while misinformation appears more frequently on Twitter.
- To evaluate the impact of this greater level of misinformation, we conducted a nationally representative survey that included questions about common misperceptions regarding COVID-19, risk perceptions, social distancing compliance, and exposure to traditional news and social media. We find that being exposed to news media is associated with fewer misperceptions and more social distancing compliance while conversely, social media exposure is associated with more misperceptions and less social distancing compliance.
- Misperceptions regarding the virus are in turn associated with less compliance with social distancing measures, even when controlling for a broad range of other attitudes and characteristics.
- Association between social media exposure and social distancing non-compliance is eliminated when accounting for effect of misperceptions, providing evidence that social media is associated with non-compliance through increasing misperceptions about the virus.
Implications
The COVID-19 pandemic has been accompanied by a so-called “infodemic”—a global spread of misinformation that poses a serious problem for public health. Infodemics are concerning because the spread of false or misleading information has the capacity to change transmission patterns (Kim et al., 2019) and consequently the scale and lethality of a pandemic. This information can be shared by any media, but there is reason to be particularly concerned about the role that social media, such as Facebook and Twitter, play in incidentally boosting misperceptions. These platforms are increasingly relied upon as primary sources of news (Mitchell et al., 2016) and misinformation has been heavily documented on them (Garrett, 2019; Vicario et al., 2016). Scholars have found medical and health misinformation on the platforms, including that related to vaccines (Radzikowski et al., 2016) and other virus epidemics such as Ebola (Fung et al., 2016) and Zika (Sharma et al., 2017).
However, misinformation content typically makes up a low percentage of overall discussion of a topic (e.g. Fung et al., 2016) and mere exposure to misinformation does not guarantee belief in that misinformation. More research is thus needed to understand the extent and consequences of misinformation surrounding COVID-19 on social media. During the COVID-19 pandemic, Twitter, Facebook and other platforms have engaged in efforts to combat misinformation but they have continued to receive widespread criticism that misinformation is still appearing on prominent pages and groups (Kouzy et al., 2020; NewsGuard, 2020). The extent to which misinformation continues to circulate on these platforms and influence people’s attitudes and behaviours is still very much an open question.
Here, we draw on three data sets and a sequential mixed method approach to better understand the consequences of online misinformation for important behaviours and attitudes. First, we collected nearly 2.5 million tweets explicitly referring to COVID-19 in the Canadian context. Second, we collected just over 9 thousand articles from nineteen Canadian English-language news sites from the same time period. We coded both of these media sets for misinformation and public health recommendations. Third, we conducted a nationally representative survey that included questions related to media consumption habits, COVID-19 perceptions and misperceptions, and social distancing compliance. As our outcome variables are continuous, we use Ordinary Least Squares (OLS) regression to identify relationships between news and social media exposure, misperceptions, compliance with social distancing measures, and risk perceptions. We use these data to illustrate: 1) the relative prevalence of misinformation on Twitter; and 2) a powerful association between social media usage and misperceptions, on the one hand, and social distancing non-compliance on the other.
Misinformation and compliance with social distancing
We first compare the presence of misinformation on Twitter with that on news media and find, consistent with the other country cases (Chadwick & Vaccari, 2019; Vicario et al., 2016), comparatively higher levels of misinformation circulating on the social media platform. We also found that recommendations for safe practices during the pandemic (e.g. washing hands, social distancing) appeared much more frequently in the Canadian news media. These findings are in line with literature examining fake news which finds a large difference in information quality across media (Al-Rawi, 2019; Guess & Nyhan, 2018).
Spending time in a media environment that contains misinformation is likely to change attitudes and behaviours. Even if users are not nested in networks that propagate misinformation, they are likely to be incidentally exposed to information from a variety of perspectives (Feezell, 2018; Fletcher & Nielsen, 2018; Weeks et al., 2017). Even a highly curated social media feed is thus still likely to contain misinformation. As cumulative exposure to misinformation increases, users are likely to experience a reinforcement effect whereby familiarity leads to stronger belief (Dechêne et al., 2010).
To evaluate this empirically, we conducted a national survey that included questions on information consumption habits and a battery of COVID-19 misperceptions that could be the result of exposure to misinformation. We find that those who self-report exposure to the misinformation-rich social media environment do tend to have more misperceptions regarding COVID-19. These findings are consistent with others that link exposure to misinformation and misperceptions (Garrett et al., 2016; Jamieson & Albarracín, 2020). Social media users also self-report less compliance with social distancing.
Misperceptions are most meaningful when they impact behaviors in dangerous ways. During a pandemic, misperceptions can be fatal. In this case, we find that misperceptions are associated with reduced COVID-19 risk perceptions and with lower compliance with social distancing measures. We continue to find strong effects after controlling for socio-economic characteristics as well as scientific literacy. After accounting for the effect of misperceptions on social distancing non-compliance, social media usage no longer has a significant association with non-compliance, providing evidence that social media may lead to less social distancing compliance through its effect on COVID-19 misperceptions.
While some social media companies have made efforts to suppress misinformation on their platforms, there continues to be a high level of misinformation relative to news media. Highly polarized political environments and media ecosystems can lead to the spread of misinformation, such as in the United States during the COVID-19 pandemic (Allcott et al., 2020; Motta et al., 2020). But even in healthy media ecosystems with less partisan news (Owen et al., 2020), social media can continue to facilitate the spread of misinformation. There is a real danger that without concerted efforts to reduce the amount of misinformation shared on social media, the large-scale social efforts required to combat COVID-19 will be undermined.
We contribute to a growing base of evidence that misinformation circulating on social media poses public health risks and join others in calling for social media companies to put greater focus on flattening the curve of misinformation (Donovan, 2020). These findings also provide governments with stronger evidence that the misinformation circulating on social media can be directly linked to misperceptions and public health risks. Such evidence is essential for them to chart an effective policy course. Finally, the methods and approach developed in this paper can be fruitfully applied to study other waves of misinformation and the research community can build upon the link clearly drawn between misinformation exposure, misperceptions, and downstream attitudes and behaviours.
We found use of social media platforms broadly contributes to misperceptions but were unable to precise the overall level of misinformation circulating on non-Twitter social media. Data access for researchers to platforms such as Facebook, YouTube, and Instagram is limited and virtually non-existent for SnapChat, WhatsApp, and WeChat. Cross-platform content comparisons are an important ingredient for a rich understand of the social media environment and these social media companies must better open their platforms to research in the public interest.
Finding 1: Misinformation about COVID-19 is circulated more on Twitter as compared to traditional media.
We find large differences between the quality of information shared about COVID-19 on traditional news and Twitter. Figure 1 shows the percentage of COVID-19 related content that contains information linked to a particular theme. The plot reports the prevalence of information on both social and news media for: 1) three specific pieces of misinformation; 2) a general set of content that describes the pandemic itself as a conspiracy or a hoax; and 3) advice about hygiene and social distancing during the pandemic. We differentiate content that shared misinformation (red in the plot) from content that debunked misinformation (green in the plot).
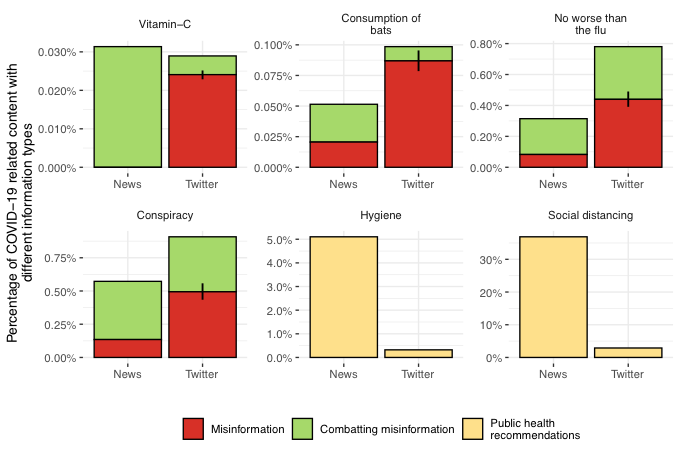
There are large differences between the levels of misinformation on Twitter and news media. Misinformation was comparatively more common on Twitter across all four categories, while debunking was relatively more common in traditional news. Meanwhile, advice on hygiene and social distancing appeared much more frequently in news media. Note that higher percentages are to be expected for longer format news articles since we rely on keyword searches for identification. This makes the misinformation findings even starker – despite much higher average word counts, far fewer news articles propagate misinformation.
Finding 2: There is a strong association between social media exposure and misperceptions about COVID-19. The inverse is true for exposure to traditional news.
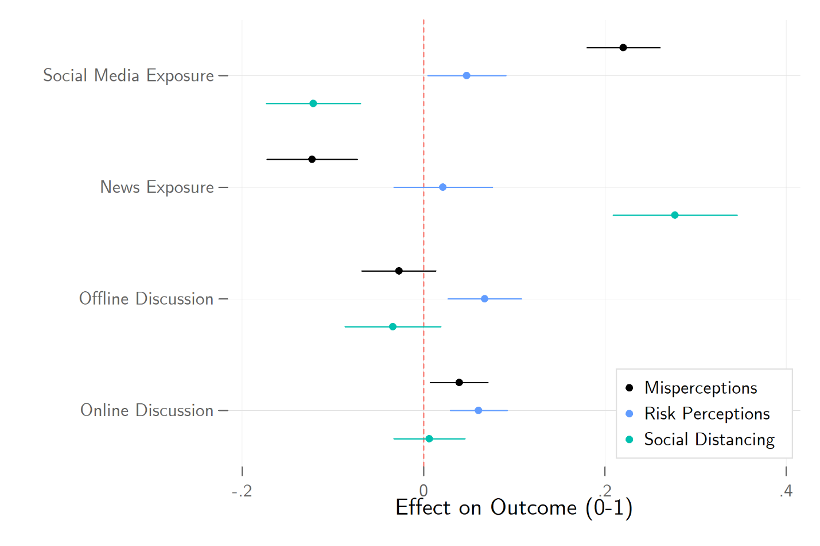
Among our survey respondents we find a corresponding strong association between social media exposure and misperceptions about COVID-19. These results are plotted in Figure 2, with controls included for both socioeconomic characteristics and demographics. Moving from no social media exposure to its maximum is expected to increase one’s misperceptions of COVID-19 by 0.22 on the 0-1 scale and decreased self-reported social distancing compliance by 0.12 on that same scale.
This result stands in stark contrast with the observed relationship between traditional news exposure and our outcome measures. Traditional news exposure is positively associated with correct perceptions regarding COVID-19. Moving from no news exposure to its highest level is expected to reduce misperceptions by 0.12 on the 0-1 scale and to increase social distancing compliance by 0.28 on that same scale. The effects are plotted in Figure 2. Social media usage appears to be correlated with COVID-19 misperceptions, suggesting these misperceptions are partially a result of misinformation on social media. The same cannot be said of traditional news exposure.
Finding 3: Misperceptions about the pandemic are associated with lower levels of risk perceptions and social distancing compliance.
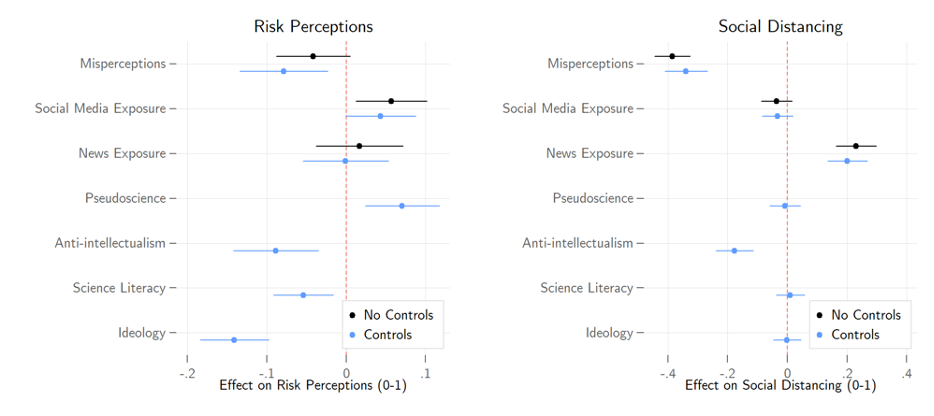
COVID-19 misperceptions are also powerfully associated with lower levels of social distancing compliance. Moving from the lowest level of COVID-19 misperceptions to its maximum is associated with a reduction of one’s social distancing by 0.39 on the 0-1 scale. The previously observed relationship between social media exposure and misperceptions disappears, suggestive of a mediated relationship. That is, social media exposure increases misperceptions, which in turn reduces social distancing compliance. Misperceptions is also weakly associated with lower COVID-19 risk perceptions. Estimates from our models using COVID-19 concern as the outcome can be found in the left panel of Figure 3, while social distancing can be found in the right panel.
Finally, we also see that the relationship between misinformation and both social distancing compliance and COVID-19 concern hold when including controls for science literacy and a number of fundamental predispositions that are likely associated with both misperceptions and following the advice of scientific experts, such as anti-intellectualism, pseudoscientific beliefs, and left-right ideology. These estimates can similarly be found in Figure 3.
Canadian Twitter and news data were collected from March 26 th to April 6 th , 2020. We collected all English-language tweets from a set of 620,000 users that have been determined to be likely Canadians. For inclusion, a given user must self-identify as Canadian-based, follow a large number of Canadian political elite accounts, or frequently use Canadian-specific hashtags. News media was collected from nineteen prominent Canadian news sites with active RSS feeds. These tweets and news articles were searched for “covid” or “coronavirus”, leaving a sample of 2.25 million tweets and 8,857 news articles.
Of the COVID-19 related content, we searched for terms associated with four instances of misinformation that circulated during the COVID-19 pandemic: that COVID-19 was no more serious than the flu, that vitamin C or other supplements will prevent contraction of the virus, that the initial animal-to-human transfer of the virus was the direct result of eating bats, or that COVID-19 was a hoax or conspiracy. Given that we used keyword searches to identify content, we manually reviewed a random sample of 500 tweets from each instance of misinformation. Each tweet was coded as one of four categories: propagating misinformation, combatting misinformation, content with the relevant keywords but unrelated to misinformation, or content that refers to the misinformation but does not offer comment.
We then calculated the overall level of misinformation for that instance on Twitter by multiplying the overall volume of tweets by the proportion of hand-coded content where misinformation was identified. Each news article that included relevant keywords was similarly coded. The volume of the news mentioning these terms was sufficiently low that all news articles were hand coded. To identify health recommendations, we used a similar keyword search for terms associated with particular recommendations: 1) social distancing including staying at home, staying at least 6 feet or 2 meters away and avoiding gatherings; and 2) washing hands and not touching any part of your face. 1 Further details on the media collection strategy and hand-coding schema are available in the supporting materials.
For survey data, we used a sample of nearly 2,500 Canadian citizens 18 years or older drawn from a probability-based online national panel fielded from April 2-6, 2020. Quotas we set on age, gender, region, and language to ensure sample representativeness, and data was further weighted within region by gender and age based on the 2016 Canadian census.
We measure levels of COVID-19 misperceptions by asking respondents to rate the truthfulness of a series of nine false claims, such as the coronavirus being no worse than the seasonal flu or that it can be warded off with Vitamin C. Each was asked on a scale from definitely false (0) to definitely true (5). We use Cronbach’s Alpha as an indicator of scale reliability. Cronbach’s Alpha ranges from 0-1, with scores above 0.8 indicating the reliability is “good.” These items score 0.88, so we can safely construct a 0-1 scale of misperceptions from them.
We evaluate COVID-19 risk perceptions with a pair of questions asking respondents how serious of a threat they believe the pandemic to be for themselves and for Canadians, respectively. Each question was asked on a scale from not at all (0) to very (4). We construct a continuous index with these items.
We quantify social distancing by asking respondents to indicate which of a series of behaviours they had undertaken in response to the pandemic, such as working from home or avoiding in-person contact with friends, family, and acquaintances. We use principal component analysis (PCA) to reduce the number of dimensions in these data while minimizing information loss. The analysis revealed 2 distinct dimensions in our questions. One dimension includes factors strongly determined by occupation, such as working from home and switching to online meetings. The other dimension contains more inclusive behaviours such as avoiding contact, travel, and crowded places. We generate predictions from the PCA for this latter dimension to use in our analyses. The factor loadings can be found in Table A1 of the supporting materials.
We gauge news and social media consumption by asking respondents to identify news outlets and social media platforms they have used over the past week for political news. The list of news outlets included 17 organizations such as mainstream sources like CBC and Global, and partisan outlets like Rebel Media and National Observer. The list of social media platforms included 10 options such as Facebook, Twitter, YouTube, and Instagram. We sum the total number of outlets/platforms respondents report using and take the log to adjust for extreme values. We measure offline political discussion with an index based on questions asking how often respondents have discussed politics with family, friends, and acquaintances over the past week. Descriptions of our primary variables can be found in Table A2 of the supporting materials.
We evaluate our hypotheses using a standard design that evaluates the association between our explanatory and outcome variables controlling for other observable factors we measured. In practice, randomly assigning social media exposure is impractical, while randomly assigning misinformation is unethical. This approach allows us to describe these relationships, though we cannot make definite claims to causality.
We hypothesize that social media exposure is associated with misinformation on COVID-19. Figure 2 presents the coefficients of models predicting the effects of news exposure, social media exposure, and political discussion on COVID-19 misinformation, risk perceptions, and social distancing. Socio-economic and demographic control estimates are not displayed. Full estimation results can be found in the Table A3 of the supporting materials.
We further hypothesize that COVID-19 misinformation is associated with lower COVID-19 risk perceptions and less social distancing compliance. Figure 3 presents the coefficients for models predicting the effects of misinformation, news exposure, and social media exposure on severity perceptions and social distancing. We show models with and without controls for science literacy and other predispositions. Full estimation results can be found in the Table A4 of the supporting materials.
Limitations and robustness
A study such as this comes with clear limitations. First, we have evaluated information coming from only a section of the overall media ecosystem and during a specific time-period. The level of misinformation differs across platforms and online news sites and a more granular investigation into these dynamics would be valuable. Our analysis suggests that similar dynamics exist across social media platforms, however. In the supplementary materials we show that associations between misperceptions and social media usage are even higher for other social media platforms, suggesting that our analysis of Twitter content may underrepresent the prevalence of misinformation on social media writ large. As noted above, existing limitations on data access make such cross-platform research difficult.
Second, our data is drawn from a single country and language case study and other countries may have different media environments and levels of misinformation circulating on social media. We anticipate the underlying dynamics found in this paper to hold across these contexts, however. Those who consume information from platforms where misinformation is more prevalent will have greater misperceptions and that these misperceptions will be linked to lower compliance with social distancing and lower risk perceptions. Third, an ecological problem is present wherein we do not link survey respondents directly to their social media consumption (and evaluation of the misinformation they are exposed to) and lack the ability to randomly assign social media exposure to make a strong causal argument. We cannot and do not make a causal argument here but argue instead that there is strong evidence for a misinformation to misperceptions to lower social distancing compliance link.
- / Fake News
- / Mainstream Media
- / Public Health
- / Social Media
Cite this Essay
Bridgman, A., Merkley, E., Loewen, P. J., Owen, T., Ruths, D., Teichmann, L., & Zhilin, O. (2020). The causes and consequences of COVID-19 misperceptions: Understanding the role of news and social media. Harvard Kennedy School (HKS) Misinformation Review . https://doi.org/10.37016/mr-2020-028
Bibliography
Allcott, H., Boxell, L., Conway, J. C., Gentzkow, M., Thaler, M., & Yang, D. Y. (2020). Polarization and Public Health: Partisan Differences in Social Distancing during the Coronavirus Pandemic (Working Paper No. 26946; Working Paper Series). National Bureau of Economic Research. https://doi.org/10.3386/w26946
Al-Rawi, A. (2019). Gatekeeping Fake News Discourses on Mainstream Media Versus Social Media. Social Science Computer Review , 37 (6), 687–704. https://doi.org/10.1177/0894439318795849
Chadwick, A., & Vaccari, C. (2019). News sharing on UK social media: Misinformation, disinformation, and correction [Report]. Loughborough University. https://repository.lboro.ac.uk/articles/News_sharing_on_UK_social_media_misinformation_disinformation_and_correction/9471269
Dechêne, A., Stahl, C., Hansen, J., & Wänke, M. (2010). The Truth About the Truth: A Meta-Analytic Review of the Truth Effect. Personality and Social Psychology Review , 14 (2), 238–257. https://doi.org/10.1177/1088868309352251
Donovan, J. (2020). Social-media companies must flatten the curve of misinformation. Nature . https://doi.org/10.1038/d41586-020-01107-z
Feezell, J. T. (2018). Agenda Setting through Social Media: The Importance of Incidental News Exposure and Social Filtering in the Digital Era. Political Research Quarterly , 71 (2), 482–494. https://doi.org/10.1177/1065912917744895
Fletcher, R., & Nielsen, R. K. (2018). Are people incidentally exposed to news on social media? A comparative analysis. New Media & Society , 20 (7), 2450–2468. https://doi.org/10.1177/1461444817724170
Fung, I. C.-H., Fu, K.-W., Chan, C.-H., Chan, B. S. B., Cheung, C.-N., Abraham, T., & Tse, Z. T. H. (2016). Social Media’s Initial Reaction to Information and Misinformation on Ebola, August 2014: Facts and Rumors. Public Health Reports , 131 (3), 461–473. https://doi.org/10.1177/003335491613100312
Garrett, R. K. (2019). Social media’s contribution to political misperceptions in U.S. Presidential elections. PLoS ONE , 14 (3). https://doi.org/10.1371/journal.pone.0213500
Garrett, R. K., Weeks, B. E., & Neo, R. L. (2016). Driving a Wedge Between Evidence and Beliefs: How Online Ideological News Exposure Promotes Political Misperceptions. Journal of Computer-Mediated Communication , 21 (5), 331–348. https://doi.org/10.1111/jcc4.12164
Guess, A., & Nyhan, B. (2018). Selective Exposure to Misinformation: Evidence from the consumption of fake news during the 2016 U.S. presidential campaign. European Research Council , 49.
Jamieson, K. H., & Albarracín, D. (2020). The Relation between Media Consumption and Misinformation at the Outset of the SARS-CoV-2 Pandemic in the US. Harvard Kennedy School Misinformation Review , 2 . https://doi.org/10.37016/mr-2020-012
Kim, L., Fast, S. M., & Markuzon, N. (2019). Incorporating media data into a model of infectious disease transmission. PLOS ONE , 14 (2), e0197646. https://doi.org/10.1371/journal.pone.0197646
Kouzy, R., Abi Jaoude, J., Kraitem, A., El Alam, M. B., Karam, B., Adib, E., Zarka, J., Traboulsi, C., Akl, E. W., & Baddour, K. (2020). Coronavirus Goes Viral: Quantifying the COVID-19 Misinformation Epidemic on Twitter. Cureus , 12 (3). https://doi.org/10.7759/cureus.7255
Mitchell, A., Gottfried, J., Barthel, M., & Shearer, E. (2016, July 7). The Modern News Consumer. Pew Research Center’s Journalism Project . https://www.journalism.org/2016/07/07/the-modern-news-consumer/
Motta, M., Stecula, D., & Farhart, C. E. (2020). How Right-Leaning Media Coverage of COVID-19 Facilitated the Spread of Misinformation in the Early Stages of the Pandemic [Preprint]. SocArXiv. https://doi.org/10.31235/osf.io/a8r3p
NewsGuard. (2020). Superspreaders . https://www.newsguardtech.com/superspreaders/
Owen, T., Loewen, P., Ruths, D., Bridgman, A., Gorwa, R., MacLellan, S., Merkley, E., & Zhilin, O. (2020). Lessons in Resilience: Canada’s Digital Media Ecosystem and the 2019 Election . Public Policy Forum. https://ppforum.ca/articles/lessons-in-resilience-canadas-digital-media-ecosystem-and-the-2019-election/
Radzikowski, J., Stefanidis, A., Jacobsen, K. H., Croitoru, A., Crooks, A., & Delamater, P. L. (2016). The Measles Vaccination Narrative in Twitter: A Quantitative Analysis. JMIR Public Health and Surveillance , 2 (1), e1. https://doi.org/10.2196/publichealth.5059
Sharma, M., Yadav, K., Yadav, N., & Ferdinand, K. C. (2017). Zika virus pandemic—Analysis of Facebook as a social media health information platform. American Journal of Infection Control , 45 (3), 301–302. https://doi.org/10.1016/j.ajic.2016.08.022
Shin, J., Jian, L., Driscoll, K., & Bar, F. (2018). The diffusion of misinformation on social media: Temporal pattern, message, and source. Computers in Human Behavior , 83 , 278–287. https://doi.org/10.1016/j.chb.2018.02.008
Vicario, M. D., Bessi, A., Zollo, F., Petroni, F., Scala, A., Caldarelli, G., Stanley, H. E., & Quattrociocchi, W. (2016). The spreading of misinformation online. Proceedings of the National Academy of Sciences , 113 (3), 554–559. https://doi.org/10.1073/pnas.1517441113
Weeks, B. E., Lane, D. S., Kim, D. H., Lee, S. S., & Kwak, N. (2017). Incidental Exposure, Selective Exposure, and Political Information Sharing: Integrating Online Exposure Patterns and Expression on Social Media. Journal of Computer-Mediated Communication , 22 (6), 363–379. https://doi.org/10.1111/jcc4.12199
The project was funded through the Department of Canadian Heritage’s Digital Citizens Initiative.
Competing Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The research protocol was approved by the institutional review board at University of Toronto. Human subjects gave informed consent before participating and were debriefed at the end of the study.
This is an open access article distributed under the terms of the Creative Commons Attribution License , which permits unrestricted use, distribution, and reproduction in any medium, provided that the original author and source are properly credited.
Data Availability
All materials needed to replicate this study are available via the Harvard Dataverse: https://doi.org/10.7910/DVN/5QS2XP .
Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals
- My Account Login
- Explore content
- About the journal
- Publish with us
- Sign up for alerts
- Open access
- Published: 16 February 2024
Changes in social norms during the early stages of the COVID-19 pandemic across 43 countries
- Giulia Andrighetto 1 , 2 , 3 na1 ,
- Aron Szekely ORCID: orcid.org/0000-0001-5651-4711 1 , 4 na1 ,
- Andrea Guido 1 , 2 , 5 ,
- Michele Gelfand 6 ,
- Jered Abernathy 7 ,
- Gizem Arikan ORCID: orcid.org/0000-0002-2083-7321 8 ,
- Zeynep Aycan 9 , 10 ,
- Shweta Bankar 11 ,
- Davide Barrera ORCID: orcid.org/0000-0002-0441-5073 4 , 12 ,
- Dana Basnight-Brown ORCID: orcid.org/0000-0002-7200-6976 13 ,
- Anabel Belaus ORCID: orcid.org/0000-0001-9657-8496 14 , 15 ,
- Elizaveta Berezina ORCID: orcid.org/0000-0003-1972-8133 16 ,
- Sheyla Blumen ORCID: orcid.org/0000-0002-9960-7413 17 ,
- Paweł Boski ORCID: orcid.org/0000-0003-0984-5686 18 ,
- Huyen Thi Thu Bui 19 ,
- Juan Camilo Cárdenas ORCID: orcid.org/0000-0003-0005-7595 20 , 21 ,
- Đorđe Čekrlija ORCID: orcid.org/0000-0001-8177-8663 22 , 23 ,
- Mícheál de Barra ORCID: orcid.org/0000-0003-4455-6214 24 ,
- Piyanjali de Zoysa ORCID: orcid.org/0000-0002-7382-6503 25 ,
- Angela Dorrough ORCID: orcid.org/0000-0002-5645-949X 26 ,
- Jan B. Engelmann ORCID: orcid.org/0000-0001-6493-8792 27 ,
- Hyun Euh ORCID: orcid.org/0000-0003-0972-1640 28 ,
- Susann Fiedler ORCID: orcid.org/0000-0001-9337-2142 29 ,
- Olivia Foster-Gimbel ORCID: orcid.org/0000-0002-4583-3060 30 ,
- Gonçalo Freitas ORCID: orcid.org/0000-0001-5888-3000 31 ,
- Marta Fülöp 32 , 33 ,
- Ragna B. Gardarsdottir ORCID: orcid.org/0000-0003-3368-4616 34 ,
- Colin Mathew Hugues D. Gill ORCID: orcid.org/0000-0002-3225-246X 16 , 35 ,
- Andreas Glöckner ORCID: orcid.org/0000-0002-7766-4791 26 ,
- Sylvie Graf ORCID: orcid.org/0000-0002-7810-5457 36 ,
- Ani Grigoryan ORCID: orcid.org/0000-0001-5453-2879 37 ,
- Katarzyna Growiec ORCID: orcid.org/0000-0002-4448-2561 18 ,
- Hirofumi Hashimoto ORCID: orcid.org/0000-0003-3648-9912 38 ,
- Tim Hopthrow ORCID: orcid.org/0000-0003-2331-7150 39 ,
- Martina Hřebíčková ORCID: orcid.org/0000-0002-8700-1326 36 ,
- Hirotaka Imada ORCID: orcid.org/0000-0003-3604-4155 40 ,
- Yoshio Kamijo ORCID: orcid.org/0000-0002-2184-9594 41 ,
- Hansika Kapoor ORCID: orcid.org/0000-0002-0805-7752 42 ,
- Yoshihisa Kashima 43 ,
- Narine Khachatryan ORCID: orcid.org/0000-0003-3590-7131 37 ,
- Natalia Kharchenko 44 ,
- Diana León ORCID: orcid.org/0000-0003-4596-3858 45 ,
- Lisa M. Leslie 30 ,
- Yang Li ORCID: orcid.org/0000-0002-8239-3279 46 ,
- Kadi Liik ORCID: orcid.org/0000-0002-5166-9893 47 ,
- Marco Tullio Liuzza ORCID: orcid.org/0000-0001-6708-1253 48 ,
- Angela T. Maitner ORCID: orcid.org/0000-0003-3896-5783 49 ,
- Pavan Mamidi 11 ,
- Michele McArdle 8 ,
- Imed Medhioub ORCID: orcid.org/0000-0003-4676-7330 50 ,
- Maria Luisa Mendes Teixeira ORCID: orcid.org/0000-0002-0606-1723 51 ,
- Sari Mentser ORCID: orcid.org/0000-0003-1520-8253 52 ,
- Francisco Morales ORCID: orcid.org/0000-0003-0785-8838 53 ,
- Jayanth Narayanan ORCID: orcid.org/0000-0003-2720-1593 54 ,
- Kohei Nitta 55 ,
- Ravit Nussinson ORCID: orcid.org/0000-0002-7331-548X 56 , 57 ,
- Nneoma G. Onyedire ORCID: orcid.org/0000-0002-4941-2300 58 ,
- Ike E. Onyishi 58 ,
- Evgeny Osin ORCID: orcid.org/0000-0003-3330-5647 59 ,
- Seniha Özden 9 ,
- Penny Panagiotopoulou 60 ,
- Oleksandr Pereverziev 61 ,
- Lorena R. Perez-Floriano ORCID: orcid.org/0000-0001-6898-7794 62 ,
- Anna-Maija Pirttilä-Backman ORCID: orcid.org/0000-0002-7437-9645 63 ,
- Marianna Pogosyan 64 ,
- Jana Raver 65 ,
- Cecilia Reyna ORCID: orcid.org/0000-0002-6097-4961 14 ,
- Ricardo Borges Rodrigues 66 ,
- Sara Romanò 12 ,
- Pedro P. Romero ORCID: orcid.org/0000-0002-2616-4498 67 , 68 ,
- Inari Sakki ORCID: orcid.org/0000-0001-8717-5804 63 ,
- Angel Sánchez ORCID: orcid.org/0000-0003-1874-2881 69 , 70 ,
- Sara Sherbaji ORCID: orcid.org/0000-0002-7815-8962 49 , 71 ,
- Brent Simpson ORCID: orcid.org/0000-0001-9468-157X 7 ,
- Lorenzo Spadoni ORCID: orcid.org/0000-0002-1208-2897 72 ,
- Eftychia Stamkou 73 ,
- Giovanni A. Travaglino ORCID: orcid.org/0000-0003-4091-0634 40 ,
- Paul A. M. Van Lange ORCID: orcid.org/0000-0001-7774-6984 74 ,
- Fiona Fira Winata 75 ,
- Rizqy Amelia Zein ORCID: orcid.org/0000-0001-7840-0299 75 ,
- Qing-peng Zhang 76 &
- Kimmo Eriksson ORCID: orcid.org/0000-0002-7164-0924 2 , 77 , 78
Nature Communications volume 15 , Article number: 1436 ( 2024 ) Cite this article
4273 Accesses
1 Citations
33 Altmetric
Metrics details
- Human behaviour
The emergence of COVID-19 dramatically changed social behavior across societies and contexts. Here we study whether social norms also changed. Specifically, we study this question for cultural tightness (the degree to which societies generally have strong norms), specific social norms (e.g. stealing, hand washing), and norms about enforcement, using survey data from 30,431 respondents in 43 countries recorded before and in the early stages following the emergence of COVID-19. Using variation in disease intensity, we shed light on the mechanisms predicting changes in social norm measures. We find evidence that, after the emergence of the COVID-19 pandemic, hand washing norms increased while tightness and punishing frequency slightly decreased but observe no evidence for a robust change in most other norms. Thus, at least in the short term, our findings suggest that cultures are largely stable to pandemic threats except in those norms, hand washing in this case, that are perceived to be directly relevant to dealing with the collective threat.
Similar content being viewed by others

Evidence from 43 countries that disease leaves cultures unchanged in the short-term

Social and moral psychology of COVID-19 across 69 countries

Predictors of adherence to public health behaviors for fighting COVID-19 derived from longitudinal data
Introduction.
Societies vary extensively in the kinds and number of social norms—the unwritten social rules that guide behavior 1 , 2 —that they adopt and the extent to which people within those societies follow them. From religious ceremonies and dress codes to environmental conservation and infection-containment, we embrace an astonishing diversity of social norms. An influential theory proposes that societies with many strong social norms, and in which individuals who deviate from the script face severe social punishment, can be classified as tight, while those that are permissive, have few and weak social norms, and norm-breakers are subject to little punishment are known as loose 3 , 4 . Such differences in cultural tightness are also reflected in prevailing socio-political institutions and practices. Tighter countries, or regions, are likelier to have restrictive socio-political institutions (e.g., government, media, education, legal, and religious), stricter constraints across everyday situations (e.g., public park, library, restaurant, workplace, classroom), more incremental innovation, lower debt, and stronger metanorms (norms about punishment) among others 3 , 5 , 6 , 7 , 8 , 9 , 10 , 11 . Loose cultures are instead more open to new ideas, more predisposed to change and substantial innovation, but may have difficulties in facing collective risks. Indeed, recent work finds that looser societies had less success in limiting COVID-19 cases and deaths in the first stages of the pandemic 12 .
Given the broad practical and scientific importance of tightness-looseness, it is essential to understand what factors are associated with these differences across countries and cultures. Tightness-Looseness theory 3 contends that societies that have experienced chronic ecological and social threats—frequent disease, warfare, and environmental catastrophes—throughout history develop tighter cultures to maintain order and survive chaos and crises. In contrast, societies with less exposure to such ecological threats can afford to develop looser cultures that allow innovation and creativity at the cost of order. This core hypothesis, that social norm strength is related to the threats that nations have (or have not) historically encountered, is well supported by correlational evidence from cross-sectional surveys 3 , 6 , 7 , ethnographic datasets 8 , a long-term online experiment 13 , and a long-term survey about social distancing norms 14 . Moreover, computational models have shown that dramatic increases in threat cause tightening 15 . On the other hand, cultural evolution has been argued to be a slow process 16 , 17 , suggesting the alternative that norm strength is stable after a collective threat. The COVID-19 pandemic provides an opportunity to examine whether tightening naturally occurs or if culture remains stable in the early stages of a collective threat. This knowledge can help us not only predict the future responses of countries to similar situations and potentially identify effective interventions to deal with these crises but also to better anticipate social changes that can impact our societies for generations to come.
Here we address this question by studying a dataset on cultural tightness, social norms, and metanorms—norms about the punishment of norm-breakers 18 —and exploit variation in disease severity due to the COVID-19 pandemic to test whether tightening evolves after a collective threat. Specifically, we combine data from a survey collected between April–December 2019 (Wave 1) 5 prior to the pandemic with a repeat of the same survey, in the same countries and sampled from the same populations, that we conducted in March–July 2020 (Wave 2) during the first months of the COVID-19 pandemic. The combined data come from 30,431 respondents (samples from both students and non-students) and cover 55 cities in 43 countries (see Table S1 for summary).
The follow-up data (Wave 2) were collected during the initial stages of the pandemic so they capture the early changes (or their stability) in norms that occurred. While this means that we cannot infer the long-run consequences of the pandemic on norms, it also presents important advantages. First, our data provide an insight into norm change under extreme circumstances—while social, political, and economic systems were in upheaval—which provides strong stimuli for change to occur potentially shaping norms. Put differently, if norm change occurs, then there is a good chance we should be able to observe this in the early stages. Second, early data give an insight into the non-equilibrium dynamics of how cultures move from one stable state to another. Third, we are able to test the boundaries of tightness-looseness theory in terms of timeline: our data indicate a lower bound on the time that may be needed for large-scale norm change to occur in response to pandemic threat. Fourth, endogeneity issues are reduced. Specifically, it reduces the possibility for other large-scale shocks to affect the data and the possibility of time varying factors (e.g. hospital infrastructure development) to confound our results.
To study whether a change in disease threat is associated with a change in norms, we study five outcomes. (i) Tightness-looseness: elicited using the standard six questions (e.g., “There are many social norms that people are supposed to abide by in this country”) with ratings standardized to control for response sets 3 , 5 . (ii) Situation-specific social norms’ strength: measured with disapproval of norm-breaking in four settings (e.g., listening to music on headphones at a funeral 19 ) and stealing shared resources 20 . (iii) Metanorm strength: for each of the prior scenarios respondents also rated the appropriateness of different responses to the norm-breaker by another individual (verbal confrontation, ostracism, gossip, physical punishment, and non-action) 5 , 18 . (iv) Frequency of punishing norm-breakers. (v) Hand washing norms: respondents indicated the situations (e.g., after shaking someone’s hand) in which people should wash their hands. Our core expectation is that these outcomes are higher after the emergence of COVID-19 than before.
These outcomes vary in their relevance to the COVID-19 pandemic. Hand hygiene is strongly related, stealing is partly related (i.e. stealing shared resources during a pandemic is particularly harmful), while others, such as listening to music on headphones at a funeral, are unrelated to the pandemic. Intuitively, norms most related to preventing disease spread should change the most. Yet tightness-looseness theory does not make such detailed predictions. Instead, it proposes the overarching hypothesis that norms and metanorms strengthen. Such a broad change may happen for two interlinked reasons: in the presence of threats, people rely more on social norms as heuristics to safely determine what to do and this increase in conformity leads to a general tightening 21 ; it is beneficial to have tight norms across the board since tightening even irrelevant norms can increase a general norm-following tendency that implies increased norm-following for the more relevant ones.
To gain a deeper insight into the mechanisms that may be associated with change, we exploit the heterogeneity across countries in their exposure to COVID-19 and we collected data on three pathways through which we conjecture that COVID-19 pandemics may shape norms. Two of these are the respondent’s beliefs about the prevalence of COVID-19 and their fear of COVID-19, as we conjecture that disease threat shapes the strength of norms through individuals’ perceptions. The final pathway concerns government policy. By implementing strict (or lenient) anti-disease policies, governments can signal to their citizens the severity of the threat. Moreover, they impose policies that change their citizens’ behavioral patterns (e.g., not shaking hands, socially isolating) and these may have consequences on social expectations and norms. While all countries in the sample have been exposed to the pandemic, the continuous variation in our collected measures helps shed light on the association between cultural change and intensity of COVID-19 pandemic. The study, including the hypotheses and analyses, was pre-registered with the Open Science Framework (see Methods).
Overall, we find that in the short term, the global threat posed by the COVID-19 pandemic was associated with a significant strengthening of social norms related to hand washing, a behavior highly relevant to limit disease spread. Contrary to our initial predictions, other established social norms governing our daily lives exhibit resilience and remain largely unchanged. In addition, cultural tightness slightly decreased accompanied by small decrease in punishment frequency. These findings suggest that the immediate impact of a global threat is selective in changing those norms that are directly relevant to cope with the threat and emphasizes the adaptive nature of societies in the face of a collective crisis.
Our analytic strategy proceeds in two stages. We first compare Wave 1 to Wave 2 averages using multilevel models with individual responses grouped on city and country. We then seek to identify the mechanisms associated with changes for only those outcomes that show significant associations which are robust across both models and sub-items. To do this we use the change across waves (Wave 2 - Wave 1) as the dependent variable as predicted by perceived prevalence, fear, and government stringency and use country-level observations and OLS regression models with heteroskedastic robust standard errors. Prevalence is measured using “What percent of people living in your province do you think have been infected with COVID-19?” and fear is the combination of three items (Cronbach’s α = 0.84, see Methods for country-level variation). To capture variation in governmental policies, we use the Stringency Index from the Oxford COVID-19 Government Response Tracker 22 .This second stage of our analysis is similar in spirit to a difference-in-differences design but differs to the classical setup in that we have no entirely untreated control group—all countries in our sample were to some extent affected by the emergence of the COVID-19 pandemic—and instead of a treated and untreated group, we have many groups with different COVID-19 pandemic exposure levels. All analyses account for age, gender, and student status to control for any sample composition differences between the waves (see Methods). We also check whether deaths and cases, which account for the different levels of COVID-19 across countries, affect our results and find that they do not (see Supplementary Materials ).
After our analyses were conducted, we added equivalence tests using the two one-sided tests procedure 23 , 24 , 25 to identify whether significant changes that we find are practically meaningful and if non-significant findings provide evidence for the absence of a meaningful change. In this procedure, we specify a series of smallest effect size of interest (SESOI) and then compare Wave 1 to Wave 2 changes and the mechanism associations to these SESOIs. Our SESOIs were set ex-post and not pre-registered and, given the lack of existing literature, or even data, concerning the changes in our outcome variables, there is large uncertainty about how the SESOI should be set (see Methods for discussion). Consequently, we use a benchmark-based approach and set the SESOI to Cohen’s d = 0.1 (a small effect size 26 ) for our main individual-level analyses and β = ± 0.10 (a small effect size 26 ) for the mechanisms analyses (see Methods for details).
Tightness-Looseness
Tightness decreases (x̅ 1 = 1.90, x̅ 2 = 1.81; Fig. 1A ; Table S1 ) although the effect size is small (Cohen’s d = 0.11; b = −0.028, 95% CI = [−0.047; −0.009], p = 0.003; Table S2 ), and the change is heterogeneous across countries (varying slope model: b = −0.037, 95% CI = [−0.073; −0.001], p = 0.042; random effect variance τ 11 = 0.01; Table S2 ; Figure S2 ). In most countries, the change is not significant (81.4%; 35/43), it is negative in 16.3% (7/43) and even positive in 2.3% (1/43) (Fig. S2 ). Countries that have higher fear levels towards COVID-19 reduced their tightness the most ( b = −0.081, 95% CI = [−0.157; −0.005], p = 0.037; Table S3 ) though this association is small. Perceived prevalence and government stringency are not significantly associated with change in tightness-looseness ( b = −0.003, 95% CI = [−0.010; 0.003], p = 0.306 and b = 0.0003, 95% CI = [−0.002; 0.001], p = 0.721, respectively; Table S3 ).

( A ) tightness-looseness, ( B ) situation-specific norms, ( C ) metanorms, ( D ) punishing frequency and ( E ) hand washing norms. Tightness and punishing frequency slightly decrease while hand washing norms increase after the emergence of the COVID−19 pandemic. Other social and metanorms display non-robust changes. Change in appropriateness items is computed by scaling the average change in each country to the maximum possible change. Hence, the index can take values from −1 to +1. Red and black dots depict sampled cities; red dots represent cities sampled in both waves while black dots refer to cities only sampled in Wave 2. Indonesia is not included in hand washing norm data because of a mistake in the survey translation (see Methods).
Situation-specific norms
Situation-specific norm strength decrease slightly from Wave 1 to Wave 2 (x̅ 1 = 1.15, x̅ 2 = 1.12; Fig. 1B ; Cohen’s d = 0.04; b = −0.017, 95% CI = [−0.028; −0.006], p = 0.003; Table S4 ) but this is not robust as it becomes non-significant when allowing for heterogeneous effects across countries (varying slope model: b = −0.011, 95% CI = [−0.054; 0.033], p = 0.628, τ 11 = 0.02; Table S4 ; Fig. S3 ). Analyses conducted on the five specific norm-breaking scenarios separately also show no consistent pattern (three are negative and two are positive) and the size of the changes is minimal (Table S5 ). These results demonstrate that COVID-19 has no consistent effect on situation-specific norms, and, even where it does, the effect is minor.
We report similar findings for metanorms (Fig. 1C ). There is no significant change across the waves (x̅ 1 = 2.15, x̅ 2 = 2.17; Cohen’s d = 0.03; b = 0.006, 95% CI = [−0.001; 0.013], p = 0.120; Table S6 ; Fig. S4 ) and there is little consistency across the different kinds of punishments: approval of ostracism slightly increases ( b = 0.028, 95% CI = [0.015; 0.040], p < 0.001; Table S7 ) while gossip approval slightly decreases ( b = −0.024, 95% CI = [−0.035; −0.013], p < 0.001; Table S7 ). Estimates from our models show no significant change in verbal confrontation, physical confrontation, and non-action (reverse coded) items.
Punishing frequency
In contrast, we find a statistically significant decrease in frequency of punishment (x̅ 1 = 3.00, x̅ 2 = 2.96; Fig. 1D ; Cohen’s d = −0.07; b = −0.034, 95% CI = [−0.047; −0.022], p < 0.001; Table S8 ). This effect remains negative and significant with a varying slopes model ( b = −0.031, 95% CI = [−0.059; −0.003], p = 0.028, τ 11 = 0.01; Table S8 ) and it is generally consistent across sub-items with the frequency of gossip ( b = −0.091, 95% CI = [−0.112; −0.070], p < 0.001; Table S9 ) and confronting ( b = −0.021, 95% CI = [−0.041; −0.002], p = 0.035; Table S9 ) both decreasing. Perhaps due to distancing and self-isolating measures, avoiding shows no significant change ( b = 0.011, 95% CI = [−0.012; 0.034], p = 0.335; Table S9 ). Frequency of gossiping tended to decrease more in countries with a higher level of fear of COVID-19 ( b = −0.139, 95% CI = [−0.261; −0.016], p = 0.028; Table S10 ). The other change in punishing frequency categories, including the overall index, are not associated with the mechanism variables (Table S10 ).
Hand washing norms
Hand washing norms increase on average (x̅ 1 = 4.07, x̅ 2 = 4.50; Fig. 1E ; Cohen’s d = 0.32; b = 0.420, 95% CI = [0.390; 0.450], p < 0.001; Table S11 ) and in almost every country (41 out of 42 countries, Fig. 1E ; all countries when considering only COVID relevant items, Fig. S1 ). Results remain unchanged when accounting for country-level heterogeneity (varying slope model: b = 0.433, 95% CI = [0.361; 0.506], p < 0.001; τ 11 = 0.04; Table S11 Fig. S3 ). The increase is most strongly associated in the categories perceived to be relevant to reducing COVID-19 spread (Table S12 ). Fear of COVID−19 accounts for most of the increase across all items ( b = 0.040, 95% CI = [0.004; 0.076], p = 0.032; Table S13 ) and this effect becomes stronger when predicting only the change of COVID-relevant items ( b = 0.092, 95% CI = [0.035; 0.148], p = 0.002; Table S13 ). Perceived prevalence does not predict hand washing norm change both when considering all items ( b = 0.002, 95% CI = [−0.0003; 0.0049], p = 0.085; Table S13 ) and relevant items ( b = 0.004, 95% CI = [−0.001; 0.008], p = 0.086; Table S13 ) but does so after shaking hands ( b = 0.004, 95% CI = [0.001; 0.008], p = 0.015; Table S13 ). Governmental stringency does not predict change in hand washing norms ( b = 0.0002, 95% CI = [−0.001; 0.001], p = 0.723; Table S13 ).
Equivalence tests
For tightness-looseness, situation-specific norms, metanorms, and punishing frequency, we find that the between wave variation observed are statistically equivalent (all p < 0.001) implying that the differences are statistically smaller than the SESOI we set. For hand washing norms, we find that the change is statistically greater than the SESOI, exceeding the upper equivalence bound (see Methods for details). For the mechanisms analyses, fear of COVID-19 is significantly associated with the outcomes of tightness-looseness and hand washing norms while all the other relevant mechanism coefficients are not significantly different to zero. Yet they all overlap with either the upper or lower equivalence bounds meaning that there is insufficient evidence to conclude a negligible effect (see Methods for details).
Our findings show that even a crisis as profound, global, and multifaceted as COVID-19 does not dramatically change the social norms of cultures in the short-term, except those believed to directly reduce disease spread, hand washing norms in this case. Nevertheless, and contrary to our expectations, we find a small decrease in tightness and punishing frequency and no significant robust changes in most social norms and metanorms in the early stages of the pandemic. Importantly, the non-significant findings are due to the absence of substantial changes and not because of a lack of power. What explains these results? One possibility is that the key prediction of tightness-looseness theory needs to be revised. Due to existing large-scale studies across multiple fields, which support the association between threat and tightness-looseness 3 , 6 , 7 , 8 , 9 , 10 , 11 , 12 and more broadly social norm strength 13 , 27 , 28 , we do not think this is the likeliest explanation. Instead, we think that there are more probable interpretations.
A distinct possibility is that cultural evolution is slow and extensive time is necessary between a collective threat and a subsequent change in cultures 16 , 17 . Indeed, if cultures do change slowly, we may expect specific cultural evolutionary mismatches—i.e., when traits that evolved in one environment become disadvantageous in a different environment 29 , 30 . Specifically, tight societies that have historically experienced threat may have traits that are better matched to dealing with a collective threat such as COVID-19, whereas looser societies would experience more of a cultural mismatch, as evidenced in 12 . Another interpretation is that different threats may tighten different norms, namely those most relevant to overcoming the specific immediate threats: pandemics may make hygiene norms stronger while earthquakes may, instead, increase norms of helping. This would be consistent with an experimental study which found that a risk of collective loss increased the strength of norms concerning cooperation 13 . Over time, this would create a mosaic of norms that together correspond to the emergent notion of tightness. If correct, cultures that face a variety of threats will be those that end up the tightest. Another possibility is that pathogen threats, which are abstract and invisible, have particular characteristics and produce different tightening dynamics than threats which are concrete and visible (e.g., earthquakes, terrorism, or warfare) 31 , 32 . The former are harder to assess, potentially causing uncertainty and panic that may have led to egoistic behavior during early stages of the pandemic. Indeed, as extensively reported by the mass media, there was hoarding of resources in the early stages of the pandemic 33 , 34 and recent work finds evidence for the erosion of social trust 35 .
These conclusions should also be considered in light of the limitations to our study. First, we use convenience samples (albeit both students and non-students). While this is unlikely to have substantial implications on our between-wave estimates, since the samples are broadly similar between the waves, it should be kept in mind when generalizing our findings to the broader populations. Specifically, it is possible that social norm change, or a lack thereof, occurred differently outside of cities, varied with socio-economic factors, or that younger people, who are overrepresented in our samples, experience fewer health-risks and our findings may not generalize to more senior people or those facing health issues. Second, our design allows us to avoid key endogeneity issues that are present in prior work, but cannot cleanly identify causal effects. More specifically, our first-stage analyses, comparing Wave 1 to Wave 2 averages, allows us to exclude reverse causality and country-constant confounders but it cannot exclude time-trends (e.g. changes in norm strength occurring over time irrespective of the pandemic). Our second-stage analyses, using perceived prevalence, fear, and government stringency to predict changes in the outcomes, reduces the possibility that such time-trends (or other confounding factors) are responsible for the observed changes as these would need to be correlated with our predictors and changes in social norms. In addition, we find little evidence for pre-existing time trends in tightness-looseness (see Methods and Fig. S7 ). Still, we do not have the power in the mechanisms analyses to detect small effects and cannot entirely identify causality.
Our sample includes data from a first study wave collected before the breakout of the pandemic (April–December 2019, Wave 1 5 ) and data from a second wave (March–July 2020, Wave 2) that we collected during the initial stages of the COVID−19 emergence. For comparability of samples across waves and among countries, we set out to collect data from approximately 200 college students at least in a major city in each country, which was achieved in all countries (Table S1 ). To assess the robustness of the country-level measures obtained from these samples, we complemented the main sampling strategy by collecting additional data from non-student samples.
When administering Wave 2, we aimed to collect data also from a subset of participants who took part in Wave 1 study. These participants were marked as “experienced” participants and were re-contacted (e.g. through laboratory recruitment systems). For six locations (Bosnia-Herzegovina, Canada, Colombia, Czech Republic, Italy, United States), we were able to recruit participants who had participated in Wave 1 but without matching their responses across waves. For two locations (Israel and Poland), we were able to uniquely identify participants and match their responses. Privacy and anonymity were nevertheless preserved in these samples. This allowed us to check whether experience of participation affects our findings. When specifically checking among participants matched across waves we find non-significant results that go in the same direction (see end of Methods).
In our analyses, we considered a response valid if a participant correctly passed an attention check placed at the end of the survey (i.e., participants had to click a specific item response). We discarded observations because of missing responses (4074 in Wave 1, 4660 in Wave 2) or failed attention checks (197 in Wave 1, 202 in Wave 2). We additionally excluded participants who declared an age under 18 (157 in Wave 1, 222 in Wave 2). The final dataset includes responses from 43 countries, 55 locations (six of which were sampled only in Wave 1, while only one sampled exclusively in Wave 2), and 30,431 valid respondents (see Table S1 ).
We used the survey administered in 5 to preserve comparability, with the sole addition of a small number of questions (at the end of the survey precluding any effects on the prior questions) regarding COVID-19 fear and prevalence, desired Tightness-Looseness measures, generalized trust, and risk aversion. The survey was translated into 30 different languages, following the standard practice of independent translation and back-translation. The study was conducted anonymously online using Qualtrics. The English version of the survey is publicly available as part of our pre-registration ( https://osf.io/9ve4t ). Our study is a survey therefore no randomization occurred and some of the investigators were not blinded to the study’s hypotheses.
All participants gave their informed consent and we complied with all relevant ethical regulations. Approval of the study protocol was obtained from ethics committees and institutional review boards where required including for the University of Melbourne (Australia), Queen’s University at Kingston (Canada), Universidad de los Andes (Colombia), Institute of Psychology, Czech Academy of Sciences (Czech Republic), Universidad San Francisco de Quito (Ecuador), United Research Ethics Committee of Psychology (Hungary), Monk Prayogshala (India), Trinity College Dublin (Ireland), Open University of Israel (Israel), LUISS University (Italy), United States International University - Africa (Kenya), Sunway University (Malaysia), University of Amsterdam (Netherlands), SWPS University (Poland), Universidade de Lisboa (Portugal), National University of Singapore (Singapore), University of Colombo (Sri Lanka), Koc University (Turkey), American University of Sharjah (United Arab Emirates), Brunel University London (United Kingdom), University of Kent (United Kingdom), University of South Carolina (United States of America), and New York University (United States of America). Ethical approval was not sought in countries where the approval received for the study conducted in Wave 1 5 was considered sufficient or where local legislation did not require ethical approval in the first place.
Study preregistration
We pre-registered our study in two phases. Our initial pre-registration was submitted before data gathering ( https://osf.io/zvdkt/ ) (March 23rd 2020) and contained a design and provisional data analysis plan. Due to the short timeframe before data collection began, the analysis plan was only provisional. Our second pre-registration, which was submitted after the data were collected but before the data were examined or analyzed (October 22nd 2020), contains a detailed analysis plan that we completely followed ( https://osf.io/9ve4t ).
The hypotheses that we pre-registered and test are the following:
H1: Tightness-Looseness levels in Wave 2 will be higher on average than in Wave 1.
H2a: Perceived threat will be positively associated with change in tightness.
H2b: Perceived prevalence will be positively associated with change in tightness.
H2c: A stricter governmental response will be positively associated with change in tightness.
H3a: Punishments, on average, are perceived as more appropriate.
H3b: People are likelier to engage in punishing norm violations.
In addition to the aforementioned hypotheses, we investigate the differences in situation specific norms and a set of items measuring hand hygiene norms between waves 1 and 2 to provide a fuller understanding in social norm changes. Furthermore, to study the mechanisms for hand hygiene norms and punishment change, we complement our analyses by exploring the moderating role of perceived threat, COVID-19 prevalence, and governmental stringency on the change in hand hygiene norms and frequency of punishment, both of which show consistent changes from Wave 1 to Wave 2.
Survey measures
We measured the following variables through survey questions. These were elicited in both Wave 1 and Wave 2 unless stated otherwise.
Tightness-looseness scores
We compute tightness-looseness scores (TL) following individual-level standardization as in past work 3 , 5 . Standardization is needed to adjust for cross-cultural variation in response sets given that some cultures are more likely to provide extreme responses or acquiesce to survey items than others 3 , 36 . Following guidelines from cross-cultural psychology 36 , 37 , and from data published in the first wave 5 , we calculate appropriateness scores by averaging each individual’s responses to a large set of heterogeneous items (i.e. 50 appropriateness items that all used the same response scale, from extremely inappropriate to extremely appropriate). This score is then subtracted from participants’ responses in the tightness-looseness questionnaire (6 items from ref. 3 ). The final individual TL scores are computed by averaging the adjusted 6 items. After transformation, TL scores display an overall average x̅ = 1.85, standard deviation s = 0.81, min = −2.26, max = 5.25. Differently from 5 , we did not impute missing TL data. This resulted in tiny differences in TL scores between studies (difference between mean TL scores = 0.01) that do not affect the validity of our results. The correlation between our TL scores and those appearing in 5 is essentially perfect (Spearman test, r = 0.997, p < 0.001). Standardizing tightness-looseness scores does not affect our results (checked for all tightness-looseness analyses reported in the manuscript). Furthermore, the correlation between standardized and non-standardized measures of TL is high and significant ( r = 0.84 for Wave 1 measures, r = 0.85 for Wave 2 measures, p < 0.001 in both cases).
Given our empirical interest in assessing the change in tightness-looseness associated with the emergence of the pandemic, we also checked whether TL scores changed or not between 2000–2003 (Wave 0), using data from 3 , and 2019 (Wave 1) 5 , and 2020 (Wave 2). We find that tightness-looseness scores have remained unchanged in almost all countries since 2000–2003 (Wave 0 to Wave 1: r = 0.89; Wave 0 to Wave 2: r = 0.88, all p < 0.001) and that there is strong stability in the ordering of countries (Kendall rank test, t = 0.752, p < 0.001, Fig. S7 panels A, B) implying that TL is a stable measure. More formally, to check whether trends in TL scores were similar across our countries pre-pandemic, with respect to their post-pandemic COVID-19 intensity, we use the following model:
Where TL indicates tightness-looseness from country c , at time t; Wave are dummy variables indicating the study wave (Wave 1 or Wave 2; Wave 0 is the baseline), and Covid Severity is fear of COVID-19, perceived cases, actual COVID-19 cases, or COVID-19 deaths (we check each sequentially). If there are no systematic differences in trend pre-pandemic then δ 1 = 0. This would indicate that countries that were later affected by the pandemic with heterogenous intensities had TL change that followed the same pattern between Wave 0 and Wave 1. We find no evidence for systematic differences in trends of TL scores between 2000–2003 and 2019 according to later COVID-19 severity (Table S14 ).
Participants’ appropriateness ratings are measured with their responses to five scenarios that cover potential norm-violating behavior in several domains concerning cooperation and out-of-place everyday behavior (see Analysis Plan of the pre-registration Analysis Plan). Ratings of the appropriateness of each item were elicited through a six-point scale, ranging from extremely inappropriate (coded 0) to extremely appropriate (coded 5). Average rating across countries is x̅ = 1.13, standard deviation s = 0.60, min = 0, max = 5.
Metanorm scenarios
Metanorms were collected for each situation (five in total) based on survey items reported in our pre-registered analyses plan. Items covered five different punishment behaviors for each situation (hence, a total of 25 items, see Analysis Plan of pre-registration Analysis Plan), which are: verbal and physical confrontation, gossip, non-action (reverse coded) and ostracism, and we collected participants’ ratings of the appropriateness of each. Appropriateness was elicited through a six-point scale, ranging from extremely inappropriate (coded 0) to extremely appropriate (coded 5). Each punishment behavior is used as a separate dependent variable. Average appropriateness across countries is x̅ = 2.22, standard deviation s = 1.25, min = 0, max = 5.
We consider three survey items eliciting the frequency at which respondents engaging in confronting, gossiping, and ostracizing someone who behaves inappropriately. Frequency of punishment was elicited using a five-point scale ranging from never (coded 1) to always (coded 5). We analyzed these all together (with mixed effects at the scenario level) and also conducted separate analyses for each item separately. Average frequency of punishment across countries is x̅ = 2.98, standard deviation s = 0.59, min = 1, max = 5.
Hand washing norms
Our survey asked participants in which of six situations they think people should wash hands. These situations are: before eating a meal, after eating a meal, after defecating, after urinating, when they come home, and after shaking someone’s hand. Hand washing norms are analyzed using as both the number of situations considered as appropriate (number of ticks) as well as whether a participant considered a given situation as appropriate (participant ticked or not a given situation). Because of a translation mistake in our survey, one country (Indonesia) has been excluded from all the analyses of these items. Average number of appropriate situations across countries was x̅ = 4.28, standard deviation s = 1.30, min = 0, max = 6.
Fear of COVID-19
Our measure of COVID-19 fear comes from the Wave 2 survey. In particular, respondents answered three items: “How concerned are you by the spread of the new Coronavirus (COVID-19)?” “How much fear do you have by the spread of the Coronavirus?” “How dangerous do you think the Coronavirus is?”. Participants responded on a six-point scale. We then compute the average over items. Average COVID-19 fear is x̅ = 4.42, standard deviation s = 0.41, min = 3.42, max = 5.20. Following our pre-registration, we checked internal consistency of the items listed above reporting (Cronbach’s α = 0.84). We additionally computed Cronbach’s alphas for each country separately. Estimated values range from 0.58 (Kenya) to 0.90 (Poland) (see below for full list). The cross-country average is 0.80 ( s = 0.07) which is close to the value obtained when merging all countries in our sample. Since estimated Cronbach alphas fall within the range of satisfactory internal consistency, throughout our main analyses, we averaged these items to create a single variable at the individual level. The only country with alpha <0.60 is Kenya; all our analyses reported in the manuscript are robust and do not substantially change when excluding Kenya from the dataset.
The full list of countries’ alphas is: ARE: 0.81, ARG: 0.76, ARM: 0.82, AUS: 0.78, BIH: 0.83, BRA: 0.79, CAN: 0.82, CHL: 0.80, CHN: 0.77, COL: 0.80, CZE: 0.85, DEU: 0.86, ECU: 0.75, ESP: 0.79, EST: 0.87, FIN: 0.84, GBR: 0.86, GRC: 0.85, HUN: 0.87, IDN: 0.83, IND: 0.71, IRL: 0.84, ISL: 0.77, ISR: 0.90, ITA: 0.86, JPN: 0.85, KEN: 0.58, KOR: 0.87, LKA: 0.63, MYS: 0.66, NGA: 0.65, NLD: 0.78, POL: 0.91, PRT: 0.88, RUS: 0.77, SAU: 0.84, SGP: 0.82, SWE: 0.80, TUR: 0.84, UKR: 0.89, USA: 0.82, VNM: 0.83. PER: items missing due to error in data collection.
Perceived COVID-19 prevalence
Our measure of disease prevalence was elicited with the Wave 2 survey question “What percent of people living in your province do you think have been infected with COVID-19? Please do not look up actual statistics to answer this question—just enter your best guess” (0–100). Average perceived COVID-19 prevalence across countries is x̅ = 21.87, standard deviation s = 7.05, min = 8.53, max = 42.65.
External measures
We measured the following variables through external data sources that we matched with our survey data.
Stringency Index
Our measure of the intensity of government response to COVID-19 is the Stringency Index from the Oxford COVID-19 Government Response Tracker 22 . The measure contains indicators reporting the severity of containment and closures (e.g. school and workplace closures and restrictions on gathering size; see items C1-C8 in ref. 23 ) and public information campaigns (item H1 in ref. 23 ). The Stringency Index can vary between 0 and 100. We match participants’ responses to our survey with Stringency Index data calculated on the same day. Average stringency across countries is x̅ = 78.12, standard deviation s = 13.54, min = 32.77, max = 99.48.
Deaths and cases
We use COVID-19 deaths and cases per million from Our World in Data 38 (downloaded November 2020). Data were matched with participants’ responses to our survey based on day of response (thus case and deaths data run from March–July 2020). Average of deaths across countries and periods is x̅ = 47.88 per million, standard deviation s = 103.70, min = 0.05, max = 481.99. Average of cases across countries and periods is x̅ = 834.95 per million, standard deviation s = 1067.72, min = 1.98, max = 4389.68.
Computed measures
The following measures were computed based on changes between Wave 1 and Wave 2. In addition to the pre-registered test ΔTightness-Looseness, we did this only for those variables that showed robust changes between the waves (see Analyses).
ΔTightness-looseness, Δpunishing, and Δhand washing
When computing change in TL, we averaged individual scores for each country and compute the difference between Wave 2 and Wave 1 values (Wave 2–Wave 1). A similar procedure is followed for computing change in other items. For hand washing and punishing items (frequency of punishment) we computed changes across waves both for each individual item and for the average of all items.
We started by analyzing the between-wave changes in Tightness-Looseness, situation-specific norms, metanorms, punishing, and hand washing norms. Then, for those changes that are shown to be robust (across sub-items and model specifications, including with random slopes and with controls for COVID-19 cases and deaths), we examine the mechanisms predicting a change in our variables of interest (ΔTightness-Looseness, Δpunishing, and Δhand washing). The models used for both stages are outlined below. In addition to these models, we replicated all of our analyses with the addition of random slopes to allow for country-level variation of the effect associated with COVID-19 pandemic. For these, we additionally report τ 11 , the variance of the main parameter of interest ( Wave 2) to shed light on the heterogeneity of the effect due to COVID-19 pandemic among countries. Moreover, we also conducted these analyses controlling for deaths and cases (adjusted to each country population size) to account for the different levels of COVID-19 pandemic across the countries and this does not affect our results. For all coefficient estimates we report the results from two-sided t -tests. All tests meet the relevant assumptions. We do not adjust for multiple comparisons.
Tightness-looseness, situation-specific norms, and punishing
We use multilevel models with random intercepts at the individual ( n ≈ 29,000), city ( n = 55), and country ( n = 43) level. Put formally, to test Hypothesis 1, we estimate the following multilevel model with varying intercepts at the country ( c ), city ( k ) and individual ( i ) level:
where Z is the vector of control variables to account for possible between-wave sample variation (age, gender, and student/non-student status), Wave 2 is a dummy variable taking value 1 when an observation was collected in Wave 2 and 0 otherwise. Our analyses for situation-specific norms, punishing, and hand washing norms follow the same model structure with the dependent variable changed to those variables.
We use multilevel models with random intercepts at the country ( c ), city ( k ), scenario ( s ), and individual ( i ) levels and implement the following model specification:
where A is the appropriateness score given by individual i to the punishment scenario s , in country c , city k . N is the average appropriateness at the location level that participants have given to the norm violation of scenario s (see also Methods in ref. 3 ) and Z is a vector of demographic controls (age, gender, and student/non-student status).
We used two approaches to test hand washing norms. First, to model the number of ticked categories we use the same model structure as Eq. 2 but with the dependent variable replaced with the number of ticks given by participant i , in county c , and city k . Second, to test the probability of ticking each single situation we use a multilevel logit regression with random intercepts at the country and city level:
Where H is the odds of participant i , in country c , and city k , ticking that it is appropriate to wash hands for a given setting. Z is a vector of demographic controls (age, gender, and student/non-student status).
ΔTightness-looseness, Δpunishing frequency, and Δhand washing
These analyses are conducted using heteroskedasticity-robust OLS regressions with observations at the country level. Observations are country-level as the dependent variable is Wave 1 to Wave 2 change in a given country. We do not use city-level because in a small number of countries different cities were sampled between Wave 1 and Wave 2. Put formally we estimate the following model for ΔTightness-Looseness:
where Fear is fear of COVID-19, PC is perceived cases of COVID-19, and SI is the Stringency Index from the Oxford COVID-19 Government Response Tracker.
We performed similar analyses for the change in hand washing and punishment. In particular, for the former, we conducted analyses for the change in the number of ticks for (i) all items, (ii) specifically for items that were not directly related to the COVID-19 pandemic (before meal, after meal, after defecating, and after urinating), (iii) specifically for items that are directly related to the pandemic (after shaking hands and after coming home), and (iv) each item separately that is directly related to the pandemic (Table S12 ).
For the items measuring punishing frequency, we estimate the change in responses for each single item individually (Table S9 ), and change in the mean of all of our 3 items (grand mean change) (Table S10 ).
Tightness-looseness change for tracked participants
We were able to perfectly match responses to our survey across waves for two locations in our sample: Israel and Poland. Below, we report the results from a robustness check aimed to test tightness score decrease.
For our Israel sub-sample of tracked participants ( N = 57), tightness scores decrease on average of 0.16 (Cohen’s d = 0.17, Wilcoxon paired samples r = 0.172), yet the change is not significant (Wilcoxon paired samples test, V = 30, p = 0.195). For our Poland sub-sample ( N = 10), tightness scores decrease by about 0.12 (Cohen’s d = 0.15), but the change is not significant (Wilcoxon paired samples test, V = 30, p = 0.85). We interpret results from our sub-samples as highly noisy but consistent with our general results from the full dataset showing a small decrease in tightness scores.
For 6 locations (Bosnia-Herzegovina, Canada, Colombia, Czech Republic, Italy, United States), we were able to distinguish responses coming from participants who previously participated in the first wave, but were not able to match the id of each responses. By running multilevel linear regression models, we report evidence of no significant change in tightness-looseness scores for these sub-populations ( b = 0.046, p = 0.222).
Power analysis
The main aim of this study was to examine whether the pandemic was associated with a systematic change in tightness-looseness (TL) scores compared to pre-pandemic scores. To make sure that our sample is large enough to detect small changes in TL, we compute the power achieved based on the mixed effects model in Eq. 2 . We adopt the common convention that a small effect be equivalent to a Cohen’s d of at least 0.10. From our sample, it means that the average TL score changes by at least 10% of its standard deviation, that is a change in TL of 0.08 (TL s = 0.80). By using the R package “simr”, we estimate the 95% CI of achieved power from the model in Eq. 2 to be 95% CI = [96.38; 100] (predictor “Wave2”, α = 0.05, 100 simulations).
We then perform sensitivity analysis to provide evidence of sufficient achieved power for models testing the change in TL scores. Given a sample of 28,374 individuals, a significance level of α = 0.05, and a desired power 0.80, we estimate the minimum detectable change in raw TL scores of 0.025 (equivalent to Cohen’s d = 0.03).
We also perform sensitivity analysis for the proposed mechanisms variables (Eq. 5 ). Given a sample of 41 countries, a significance level of α = 0.05, and a desired power 0.80, we estimate the minimum detectable effect size f². Results show that the minimum effects that could be detected are of medium to large size f² = 0.2 (two sided) for the proposed mediating variables.
We performed equivalence tests for all the Wave 1 to Wave 2 change analyses following the two one-sided test (TOST) procedure 23 , 24 , 25 . To set the smallest effect size of interest (SESOI) it is recommended to use substantive motivations (e.g. prior findings in the literature) 23 , 24 . Yet, for our analyses, we were unable to identify clear substantive bases for setting the SESOI. For instance, comparable meta-norm measures do not exist, to our knowledge, while for tightness-looseness, there is only one other source for comparable large-scale cross-country data 3 but this is solely available in a transformed form making a comparison in mean change to our waves meaningless (see Supplementary Note 1 ). Given this absence of comparable prior empirical evidence for setting the SESOIs, we consider a Cohen’s d = 0.10 as the SESOI for changes in our measures over time. While for all mechanism analyses, we considered standardized betas as effect size measure, and consider a threshold of β = ±0.10 (a small effect size 26 ) as the SESOI benchmark for all mechanisms tested.
We conducted the TOST procedure (set at the 5% significance level) using the coefficients and standard errors derived from the model estimates displayed in the main text and supplementary materials . For example, when analyzing the SESOI for TL, we estimate the equivalent change Δ in the raw scale corresponding to d = 0.10. The coefficient estimate and standard error are drawn from Model 1 (Table S2 ) and the TOST procedure is applied. The SESOIs of all other norm measures are calculated by applying the same reasoning and the TOSTs are conducted in the same way. For each equivalence test, we report the smallest magnitude t- value from among the two one-sided tests performed.
Tightness-looseness
We find a significant difference between our estimate of TL change and the SESOI (Δ = ±0.08, t (28369) = 5.53, p < 0.001) such that the relevant coefficient ( b = −0.028, 90% CI = [−0.047; −0.009]) is contained within the upper and lower equivalence bounds. This indicates that although there is a significant decrease in TL from Wave 1 to Wave 2 the change is statistically equivalent.
We find a significant difference between our estimate of situation-specific norms change and the within-country SESOI (Δ = ±0.06, t (142531) = 7.802, p < 0.001) such that the relevant coefficient ( b = −0.017, 90% CI = [−0.028; −0.006]) is contained within the upper and lower equivalence bounds. This indicates that while we find a significant decrease in situation-specific norms from Wave 1 to Wave 2, the change is statistically equivalent.
We find a significant difference between our estimate of metanorms change and the SESOI (Δ = ±0.05, t (484665) = −12.925, p < 0.001) such that the relevant coefficient ( b = 0.006, 90% CI = [−0.001; 0.012]) is contained within the upper and lower equivalence bounds. This implies that the change in metanorms is not significant from Wave 1 to Wave 2 and statistically equivalent.
We find a significant difference between our estimate of punishing frequency change and the SESOI ( Δ = ±0.1, t (85490) = 9.603, p < 0.001) such that the relevant coefficient ( b = −0.034, 90% CI = [−0.047; −0.022]) is contained within the upper and lower equivalence bounds. This means that, although we find a statistically significant decrease in punishing frequency, the change is statistically equivalent.
We find a significant difference between our estimate of hand washing norms change and the SESOI (Δ = ±0.13, t (28134) = −49.84, p < 0.001) such that the relevant coefficient ( b = 0.420, 90% CI = [0.390; 0.450]) is above the upper equivalence bound. This implies that the change in hand washing norms is significant from Wave 1 to Wave 2 and not statistically equivalent.
Mechanism analyses
When running the equivalence tests for the factors included in the mechanism analysis of the change in TL scores , we find that all standardized coefficients of our factors (Fear of COVID-19, β = −0.283, 90% CI [−0.503; −0.063]; Perceived Prevalence, β = −0.201, 90% CI [−0.526; 0.124]; Gov. Stringency, β = −0.036, 90% CI [−0.205; 0.133]) overlap with either the upper or lower equivalence bounds. This means that there is insufficient evidence to conclude a negligible effect.
The same analyses run for the change in hand washing norms give similar results in terms of equivalence. The coefficient associated with Fear of COVID-19 ( β = 0.352, 90% CI = [0.087; 0.618]), Perceived Prevalence ( β = 0.343, 90% CI [0.017; 0.669]) as well as Gov. Stringency ( β = −0.058, 90% CI [−0.333; 0.216]) overlap with either the upper or lower bound of the equivalence interval indicating that there is insufficient evidence to conclude a negligible effect.
Likewise, results from the equivalence tests for the change in punishing frequency show that the coefficient associated with Fear of COVID−19 ( β = −0.080, 90% CI = [−0.2314; 0.071]), Perceived Prevalence ( β = 0.008, 90% CI [−0.241; 0.257]) as well as Gov. Stringency ( β = −0.096, 90% CI [−0.255; 0.062]) overlap with either the upper or lower bound of the equivalence interval indicating that there is insufficient evidence to conclude a negligible effect.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The data generated in this study have been deposited in the Open Science Framework ( https://doi.org/10.17605/OSF.IO/STKFR ). Non-experimental data included in our datasets (i.e., intensity of government response to COVID-19 is the Stringency Index, COVID-19 deaths and cases per million) are taken from the Oxford COVID−19 Government Response Tracker 22 and Our World in Data 38 (downloaded November 2020). Wave 0 data are from 3 and Wave 1 data are from 5 .
Code availability
The survey and analysis code are available at the Open Science Framework ( https://doi.org/10.17605/OSF.IO/STKFR ).
Bicchieri, C. The Grammar of Society: The Nature and Dynamics of Social Norms (Cambridge University Press, 2006).
Elster, J. The Cement of Society: A Survey of Social Order (Cambridge University Press, 1989).
Gelfand, M. J. et al. Differences between tight and loose cultures: a 33-nation study. Science 332 , 1100–1104 (2011).
Article CAS PubMed ADS Google Scholar
Pelto, P. J. The differences between “tight” and “loose” societies. Trans.-action 5 , 37–40 (1968).
Google Scholar
Eriksson, K. et al. Perceptions of the appropriate response to norm violation in 57 societies. Nat. Commun. 12 , 1481 (2021).
Article CAS PubMed PubMed Central ADS Google Scholar
Chua, R. Y. J., Huang, K. G. & Jin, M. Mapping cultural tightness and its links to innovation, urbanization, and happiness across 31 provinces in China. Proc. Natl Acad. Sci. USA 116 , 6720–6725 (2019).
Harrington, J. R. & Gelfand, M. J. Tightness–looseness across the 50 united states. Proc. Natl Acad Sci. USA 111 , 7990–7995 (2014).
Jackson, J. C., Gelfand, M. & Ember, C. R. A global analysis of cultural tightness in non-industrial societies. Proc. R. Soc. B: Biol. Sci. 287 , 20201036 (2020).
Article Google Scholar
Chua, R. Y. J., Roth, Y. & Lemoine, J.-F. The impact of culture on creativity: how cultural tightness and cultural distance affect global innovation crowdsourcing work. Adm. Sci. Q. 60 , 189–227 (2015).
Jackson, J. C., Gelfand, M., De, S. & Fox, A. The loosening of American culture over 200 years is associated with a creativity–order trade-off. Nat. Hum. Behav. 3 , 244–250 (2019).
Article PubMed Google Scholar
Jackson, J. C. et al. Ecological and cultural factors underlying the global distribution of prejudice. PLoS ONE 14 , e0221953 (2019).
Article CAS PubMed PubMed Central Google Scholar
Gelfand, M. J. et al. The relationship between cultural tightness–looseness and COVID-19 cases and deaths: a global analysis. Lancet Planet. Health 5 , e135–e144 (2021).
Article PubMed PubMed Central Google Scholar
Szekely, A. et al. Evidence from a long-term experiment that collective risks change social norms and promote cooperation. Nat. Commun. 12 , 5452 (2021).
Vriens, E., Andrighetto, G. & Tummolini, L. Risk, sanctions and norm change: the formation and decay of social distancing norms. Philos Trans. R. Soc. Lond. B. Biol. Sci. 379 , 20230035 (2024).
Roos, P., Gelfand, M., Nau, D. & Lun, J. Societal threat and cultural variation in the strength of social norms: an evolutionary basis. Organ. Behav. Hum. Decis. Process. 129 , 14–23 (2015).
Nunn, N. On the Causes and consequences of cross-cultural differences: an economic perspective. in Handbook of Advances in Culture and Psychology : 9 (eds. Gelfand, M. J., Chiu, C.-Y. & Hong, Y.-Y.) 125–188 (Oxford University Press, 2022).
Algan, Y. & Cahuc, P. Inherited trust and growth. Am. Econ. Rev. 100 , 2060–2092 (2010).
Axelrod, R. An evolutionary approach to norms. Am. Political Sci. Rev. 80 , 1095–1111 (1986).
Price, R. H. & Bouffard, D. L. Behavioral appropriateness and situational constraint as dimensions of social behavior. J. Personal. Soc. Psychol. 30 , 579–586 (1974).
Eriksson, K., Andersson, P. A. & Strimling, P. Moderators of the disapproval of peer punishment. Group Process. Intergroup Relat. 19 , 152–168 (2016).
Griskevicius, V., Goldstein, N. J., Mortensen, C. R., Cialdini, R. B. & Kenrick, D. T. Going along versus going alone: when fundamental motives facilitate strategic (non)conformity. J. Personal. Soc. Psychol. 91 , 281–294 (2006).
Hale, T. et al. A global panel database of pandemic policies (Oxford COVID−19 Government Response Tracker). Nat. Human Behav. https://doi.org/10.1038/s41562-021-01079-8 (2021).
Lakens, D. Equivalence tests: a practical primer for t tests, correlations, and meta-analyses. Soc. Psychol. Personal. Sci. 8 , 355–362 (2017).
Lakens, D., Scheel, A. M. & Isager, P. M. Equivalence testing for psychological research: a tutorial. Adv. Methods Pract. Psychol. Sci. 1 , 259–269 (2018).
Schuirmann, D. J. A comparison of the two one-sided tests procedure and the power approach for assessing the equivalence of average bioavailability. J. Pharmacokinet. Biopharm. 15 , 657–680 (1987).
Article CAS PubMed Google Scholar
Cohen, J. Statistical Power Analysis for the Behavioral Sciences . (Routledge, 1988). https://doi.org/10.4324/9780203771587 .
Sosis, R., Kress, H. C. & Boster, J. S. Scars for war: evaluating alternative signaling explanations for cross-cultural variance in ritual costs. Evol. Hum. Behav. 28 , 234–247 (2007).
Roes, F. L. & Raymond, M. Belief in moralizing gods. Evol. Hum. Behav. 24 , 126–135 (2003).
Gelfand, M. J. Cultural evolutionary mismatches in response to collective threat. Curr. Dir. Psychol. Sci. 30 , 401–409 (2021).
Gelfand, M. J., Gavrilets, S. & Nunn, N. Norm dynamics: Interdisciplinary perspectives on social norm emergence, persistence, and change. Annu. Rev. Psychol. 75 , (2024).
Barclay, P. & Benard, S. The effects of social vs. asocial threats on group cooperation and manipulation of perceived threats. Evol. Hum. Sci. 2 , e54 (2020).
Gavrilets, S. Collective action and the collaborative brain. J. R. Soc. Interface 12 , 20141067 (2015).
Baddeley, M. Hoarding in the age of COVID-19. J. Behav. Econ. Policy 4 , 69–75 (2020).
Syahrivar, J., Genoveva, G., Chairy, C. & Manurung, S. P. COVID-19-induced hoarding intention among the educated segment in Indonesia. SAGE Open 11 , 21582440211016904 (2021).
Lo Iacono, S., Przepiorka, W., Buskens, V., Corten, R. & van de Rijt, A. COVID-19 vulnerability and perceived norm violations predict loss of social trust: a pre-post study. Soc. Sci. Med. 291 , 114513 (2021).
Gelfand, M. J., Raver, J. L. & Ehrhart, K. H. Methodological issues in cross-cultural organizational research. in Handbook of Research Methods in Industrial and Organizational Psychology 216–246 (Blackwell Publishing, 2002).
van de Vijver, F. J. R. & Leung, K. Methods and data analysis for cross-cultural research . (Sage Publications, Inc, 1997).
Ritchie, H. et al. Coronavirus Pandemic (COVID-19). Our World in Data . https://ourworldindata.org/coronavirus (2020).
Download references
Acknowledgements
Knut and Wallenberg Grant “How do human norms form and change?” 2016.0167. (G.An.). The Swedish Research Council grant “Norms & Risk: Do social norms help dealing with collective threats” 2021-06271 (G.An.). Ministero dell’Istruzione dell’Università e della Ricerca, PRIN 2017, prot. 20178TRM3F (D.B.). Universidad de Los Andes, Fondo Vicerrectoría de Investigaciones (J.-C.C.). Ministry of Innovation and Technology of Hungary, National Research, Development and Innovation Fund NKFIH-OTKA K135963 (M.F.). Grant 23-061770 S of the Czech Science Foundation (M.H. and S.G.). RVO: 68081740 of the Institute of Psychology, Czech Academy of Sciences (M.H. and S.G.). RA Science Committee, research project N.20TTSH-070 (A.Gr. and N.Khac.). Open University of Israel, 511687 (R.N.). HSE University Basic Research Program (E.O.). Project BASIC (PID2022-141802NB-I00) funded by MCIN/AEI/10.13039/501100011033 and by “ERDF A way of making Europe” (A.Sá.). US Army Research Office Grant W911NF-19-1-910281 (B.S.). Netherlands Organisation for Scientific Research, 019.183SG.001 (E.S.). Netherlands Organisation for Scientific Research, VI.Veni.201 G.013 (E.S.). European Commission, Horizon 2020-ID 870827 (E.S.). UKRI Grant “Secret Power” No. EP/X02170X/1 awarded under the European Commission’s “European Research Council - STG” Scheme (G.A.T.).
Author information
These authors contributed equally: Giulia Andrighetto, Aron Szekely.
Authors and Affiliations
Institute of Cognitive Sciences and Technologies, National Research Council of Italy, Rome, Italy
Giulia Andrighetto, Aron Szekely & Andrea Guido
Institute for Futures Studies, Stockholm, Sweden
Giulia Andrighetto, Andrea Guido & Kimmo Eriksson
Institute for Analytical Sociology, Linköping University, Linköping, Sweden
Giulia Andrighetto
Collegio Carlo Alberto, Turin, Italy
Aron Szekely & Davide Barrera
CEREN EA 7477, Burgundy School of Business, Université Bourgogne Franche-Comté, Dijon, France
Andrea Guido
Graduate School of Business and Department of Psychology, Stanford University, Stanford, USA
Michele Gelfand
Department of Sociology, University of South Carolina, Columbia, USA
Jered Abernathy & Brent Simpson
Department of Political Science, Trinity College Dublin, Dublin, Ireland
Gizem Arikan & Michele McArdle
Department of Psychology, Koç University, Istanbul, Turkey
Zeynep Aycan & Seniha Özden
Faculty of Management, Koç University, Istanbul, Turkey
Zeynep Aycan
Ashoka University, Sonipat, India
Shweta Bankar & Pavan Mamidi
Department of Culture, Politics, and Society, University of Turin, Turin, Italy
Davide Barrera & Sara Romanò
United States International University – Africa, Nairobi, Kenya
Dana Basnight-Brown
Instituto de Investigaciones Psicológicas (IIPsi), Consejo Nacional de Investigaciones Científicas y Técnicas (CONICET); CABA, Córdoba, Argentina
Anabel Belaus & Cecilia Reyna
Facultad de Psicología, Universidad Nacional de Córdoba (UNC), Córdoba, Argentina
Anabel Belaus
Sunway University, Bandar Sunway, Malaysia
Elizaveta Berezina & Colin Mathew Hugues D. Gill
Departamento de Psicología, Pontificia Universidad Católica del Perú, Lima, Perú
Sheyla Blumen
SWPS University, Warsaw, Poland
Paweł Boski & Katarzyna Growiec
Hanoi National University of Education, Hanoi, Vietnam
Huyen Thi Thu Bui
Universidad de los Andes, Bogota, Colombia
Juan Camilo Cárdenas
University of Massachusetts Amherst, Amherst, USA
Faculty of Philosophy, University of Banja Luka, Banja Luka, Bosnia and Herzegovina
Đorđe Čekrlija
Institute of Psychology, University of Greifswald, Greifswald, Germany
Centre for Culture and Evolution, Brunel University London, Uxbridge, UK
Mícheál de Barra
Faculty of Medicine, University of Colombo, Colombo, Sri Lanka
Piyanjali de Zoysa
Department of Psychology, University of Cologne, Cologne, Germany
Angela Dorrough & Andreas Glöckner
Center for Research in Experimental Economics and Political Decision Making (CREED), Amsterdam School of Economics, University of Amsterdam, Amsterdam, The Netherlands
Jan B. Engelmann
Gies College of Business, University of Illinois at Urbana-Champaign, Champaign, USA
Vienna University of Economics and Business, Vienna, Austria
Susann Fiedler
Stern School of Business, New York University, New York, USA
Olivia Foster-Gimbel & Lisa M. Leslie
Instituto de Ciências Sociais, Universidade de Lisboa, Lisboa, Portugal
Gonçalo Freitas
HUN-REN Institute of Cognitive Neuroscience and Psychology, Research Centre of Natural Sciences, Budapest, Hungary
Marta Fülöp
Institute of Psychology, Karoli Gáspár University of the Reformed Churches, Budapest, Hungary
Faculty of Psychology, University of Iceland, Reykjavik, Iceland
Ragna B. Gardarsdottir
Universal College Bangladesh, Dhaka, Bangladesh
Colin Mathew Hugues D. Gill
Institute of Psychology, Czech Academy of Sciences, Brno, Czech Republic
Sylvie Graf & Martina Hřebíčková
Department of Personality Psychology, Yerevan State University, Yerevan, Armenia
Ani Grigoryan & Narine Khachatryan
Osaka Metropolitan University, Osaka, Japan
Hirofumi Hashimoto
School of Psychology, University of Kent, Canterbury, UK
Tim Hopthrow
Royal Holloway, University of London, Egham, UK
Hirotaka Imada & Giovanni A. Travaglino
Waseda University, Tokyo, Japan
Yoshio Kamijo
Department of Psychology, Monk Prayogshala, Mumbai, India
Hansika Kapoor
Melbourne School of Psychological Sciences, The University of Melbourne, Melbourne, Australia
Yoshihisa Kashima
Kyiv International Institute of Sociology, Kyiv, Ukraine
Natalia Kharchenko
DeJusticia, Bogotá, Colombia
Nagoya University, Nagoya, Japan
School of Natural Sciences and Health, Tallinn University, Tallinn, Estonia
Department of Medical and Surgical Sciences, “Magna Græcia” University of Catanzaro, Catanzaro, Italy
Marco Tullio Liuzza
Department of Psychology, American University of Sharjah, Sharjah, United Arab Emirates
Angela T. Maitner & Sara Sherbaji
Department of Finance and Investment, Imam Mohammad Ibn Saud Islamic University, Riyadh, Saudi Arabia
Imed Medhioub
Presbyterian Mackenzie University, São Paulo, Brazil
Maria Luisa Mendes Teixeira
The Hebrew University of Jerusalem, Jerusalem, Israel
Sari Mentser
Universidad de los Andes, Santiago, Chile
Francisco Morales
Northeastern University, Boston, USA
Jayanth Narayanan
Ritsumeikan University, Shiga, Japan
Kohei Nitta
Department of Education and Psychology, The Open University of Israel, Ra’anana, Israel
Ravit Nussinson
Institute of Information Processing and Decision Making (IIPDM), University of Haifa, Haifa, Israel
Department of Psychology, University of Nigeria, Nsukka, Nigeria
Nneoma G. Onyedire & Ike E. Onyishi
HSE University, Moscow, Russia
Evgeny Osin
Department of Education and Social Work, University of Patras, Patras, Greece
Penny Panagiotopoulou
POLLSTER, Kiev, Ukraine
Oleksandr Pereverziev
Universidad Diego Portales, Santiago, Chile
Lorena R. Perez-Floriano
Faculty of Social Sciences, Social Psychology, University of Helsinki, Helsinki, Finland
Anna-Maija Pirttilä-Backman & Inari Sakki
Leadership and Management, Amsterdam Business School (ABS), University of Amsterdam, Amsterdam, The Netherlands
Marianna Pogosyan
Queen’s University at Kingston, Ontario, Canada
Centro de Investigação e Intervenção Social, Instituto Universitário de Lisboa (ISCTE-IUL), Lisbon, Portugal
Ricardo Borges Rodrigues
School of Economics, Universidad San Francisco de Quito, Quito, Ecuador
Pedro P. Romero
Experimental and Computational Economics Lab (ECEL), Universidad San Francisco de Quito, Quito, Ecuador
Grupo Interdisciplinar de Sistemas Complejos (GISC), Departamento de Matemáticas, Universidad Carlos III de Madrid, Leganés, Spain
Angel Sánchez
Instituto de Biocomputación y Física de Sistemas Complejos (BIFI), Universidad de Zaragoza, Zaragoza, Spain
Department of Anthropology, University College London, London, UK
Sara Sherbaji
Department of Economics and Law, University of Cassino and Southern Lazio, Cassino (FR), Italy
Lorenzo Spadoni
Department of Psychology, University of Amsterdam, Amsterdam, The Netherlands
Eftychia Stamkou
Department of Experimental and Applied Psychology, Vrije Universiteit, Amsterdam, The Netherlands
Paul A. M. Van Lange
Faculty of Psychology, Universitas Airlangga, Surabaya, Indonesia
Fiona Fira Winata & Rizqy Amelia Zein
Guangzhou University, Guangzhou, P. R. China
Qing-peng Zhang
Center for Cultural Evolution, Stockholm University, Stockholm, Sweden
Kimmo Eriksson
Malardalens University, Vasteras, Sweden
You can also search for this author in PubMed Google Scholar
Contributions
G.An., A.Sz. and A.Gu. designed the study and wrote the manuscript. A.Gu. analyzed the data. K.E., M.G., A.Gl. and M.T.L. provided critical input on the study and/or the manuscript. All other authors arranged translations where required, gave feedback on wording of items, collected data, and reviewed the manuscript.
Corresponding author
Correspondence to Giulia Andrighetto .
Ethics declarations
Competing interests.
The authors declare no competing interests.
Peer review
Peer review information.
Nature Communications thanks Pat Barclay, Andrew Delton, Peder Isager, Anne Scheel and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Supplementary information, reporting summary, peer review file, rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ .
Reprints and permissions
About this article
Cite this article.
Andrighetto, G., Szekely, A., Guido, A. et al. Changes in social norms during the early stages of the COVID-19 pandemic across 43 countries. Nat Commun 15 , 1436 (2024). https://doi.org/10.1038/s41467-024-44999-5
Download citation
Received : 14 September 2021
Accepted : 12 January 2024
Published : 16 February 2024
DOI : https://doi.org/10.1038/s41467-024-44999-5
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
By submitting a comment you agree to abide by our Terms and Community Guidelines . If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies
Sign up for the Nature Briefing newsletter — what matters in science, free to your inbox daily.

Discussion: The COVID-19 Crisis Essay
Introduction, weakness and strengths exposed by covid-19 in our society, roles leaders in government should play, ethical issues of the covid-19 pandemic, works cited.
The COVID-19 pandemic was more than a health crisis because it affected the world’s human, economic, and social stability. Although we are not yet over the coronavirus pandemic because new mutations like the Micron variant are emerging across many countries, the 2020 outbreak was the most destructive phase. The 2020 widespread COVID-19 infections led to a dramatic loss of lives and presented unprecedented challenges to public health, food systems, and work life. The economic and social destruction caused by the pandemic was devastating, where millions of the world’s workforces risked losing their livelihoods due to constant lockdowns and border closures. Many vulnerable people, such as the homeless, were exposed to precarious situations with curfews and lockdowns affecting their daily lives. The coronavirus crisis revealed weaknesses in the world’s preparedness for COVID-19 to provide the minimum health, education, employment, and well-being requirements.
The pandemic revealed the deep inequities in our society, where millions of people without paid work or sick leave had to stay home without financial support. It was already difficult for people with secure jobs, stable housing, and economic security to deal with the difficult times, meaning it must have been worse for those lacking all three. Secondly, the COVID-19 disruption showed that humans favor personal rights over our duties to each other. For instance, some people failed to self-isolate or recognize that humans are connected to one another, making the virus spread faster. Finally, income loss and insufficient access to health care exposed our frail social safety nets. Therefore, we must upgrade our public health infrastructure and address the underlying economic and social inequities.
Despite the crisis, our strength as a society was demonstrated by state capacity and consensually oriented collective culture to mobilize against the virus. Albeit early stumbles that sort to stem the flow of information instead of the virus, various governments acted decisively to enforce containment measures. Radical information transparency, including public disclosure of tracked cases, closure of schools and public gatherings, widespread testing, work-from-home, and face-mask policies, alongside other measures, facilitated the recovery from the pandemic. The heart of sharing, where people volunteered to donate foodstuffs to the less fortunate, showed our strength as a single race with intertwined destiny. Nations working together, organizations, and individuals cared for each other through the donation of face masks, financial assistance, and manufacturing and distributing vaccines that were useful in containing the virus. Overall, we learned that well-being, safety, and health depend on those of others. Therefore, protecting the most vulnerable members of society benefits everyone.
A strong political leadership, a technocratic approach, and a highly skilled public sector workforce could result in even greater success in managing crises like the COVID-19 pandemic. For example, the coronavirus outbreak in the U.S. was marked with misinformation and contractions, even from senior political figures. As a result, politics significantly impacted pandemic response effectiveness, even at the clinical level (Phillips et al. 1). At a time of crisis like COVID-19, leaders should provide reliable information and maintain utmost transparency, which is essential for pandemic response. Expert clinicians addressed decision-makers with authority, emphasizing safety, quality, and service obligation (Phillips et al. 8). The bold move helped enhance transparent communication, collaboration, mutual respect and trust, and unity between front-line clinicians and top-level administrators.
Government leadership requires building and sustaining trust in times of uncertainty like the coronavirus pandemic. When political, administrative, and clinical actors collaborate in a partnership characterized by trust, transparency, and evidence, governance becomes effective (Phillips et al. 12). Political and healthcare leaders must leverage the cultural assets of relationship-building and community cohesion to strengthen their responses. It is expected that leaders, including those in health organizations, will respond to a crisis’s direct and indirect effects with little time for preparation and in a constantly changing environment (Ahern and Loh 266). For instance, social media has disrupted the critical task of crisis leadership. Still, government leaders and scientific and public health experts need to remain trusted by the public during a pandemic. Therefore, they must inspire confidence from past behaviors through honest actions and motives.
The public health facilities became overwhelmed, including the medics on the front lines, due to rising cases and complications of COVID-19. However, the main ethical question was how medical practitioners presided over the destiny of patients when equipment cannot support patients in critical conditions. For instance, the decision on whom to allocate an intensive care bed caused a dilemma because one cannot justify their choices if the other person died. However, most people seemed to agree that a patient’s ability to benefit from treatment and to survive should be first-order considerations (McGuire et al. 16). Therefore, guidance on the ethical allocation of scarce resources hinged on who is more likely to benefit than life preservation.
Front-line healthcare workers took significant risks during the COVID-19 pandemic amidst an inadequate supply of personal protective equipment (PPE) and an overwhelming surge of covid patients (McGuire et al. 16). Society arguably owes them reciprocity, prioritizing them for medical treatment and vaccines. However, controversy arises about whether they should receive priority for the scarcest and most critical facilities like ventilator support and ICU beds. For instance, it is difficult to determine if physicians, nurses, social workers, and emergency medical technicians should receive priority over those working in hospital transport, pharmacy, and security. Other issues arose from uneasiness around the sudden albeit temporary loss of personal liberties. Citizens questioned the restrictions of their rights enforced through quarantine, curfews, closed borders, and limited ability to move freely. Some were denied access to family members even when seriously sick or dying. Contact tracing technologies also raised concerns about data privacy, such as intrusion of personal privacy via surveillance.
Being a good citizen in the face of a pandemic should start with those who are government-mandated to provide essential services. Government officials should take responsibility and improve public health infrastructure, as well as equip them with appropriate facilities to prevent dilemmas faced by medics during COVID-19. Everyone else should focus on what they can control, such as complying with COVID-19 guidelines and making intentional choices with the greater good of others in mind. Overall, we can define ourselves during this pandemic by using our skills and resources to better humanity.
COVID-19 revealed the inequities in our society and the underdeveloped public healthcare infrastructure. It showed that humans favor personal rights over duties to others, even during a pandemic. However, our collective culture demonstrated the strength to fight the virus, including the government’s bold move to implement containment measures. The success against the COVID-19 pandemic could be attributed to information transparency, willingness to share resources and collaboration in vaccine production. The government needs to upgrade the public health infrastructure and address inequities evident during the 2020 COVID-19 pandemic. A stronger leadership quality, including transparent communication, collaboration, mutual respect, and trust during times of uncertainty, would be fundamental in fighting the next pandemic. However, ethical concerns must be our primary concern in fighting the next pandemic, such as criteria for prioritizing patient care, restriction of civil liberties, and allocation of scarce but critical infrastructure.
Ahern, Susannah and Erwin Loh. “Leadership during the COVID-19 pandemic: building and sustaining trust in times of uncertainty.” British Journal of Management Leader, vol. 5, no. 4, 2020, pp. 266-269.
McGuire, Amy, et al. “Ethical Challenges Arising in the COVID-19 Pandemic: An Overview from the Association of Bioethics Program Directors (ABPD) Task Force.” The American Journal of Bioethics, vol. 20, no. 7, 2020, pp. 15-27.
Phillips, George, et al. “Lessons from the frontline: Leadership and governance experiences in the COVID-19 pandemic response across the Pacific region.” The Lancet Regional Health-Western Pacific , vol. 25, no. 1, 2022, pp. 1-14.
- Chicago (A-D)
- Chicago (N-B)
IvyPanda. (2024, May 18). Discussion: The COVID-19 Crisis. https://ivypanda.com/essays/discussion-the-covid-19-crisis/
"Discussion: The COVID-19 Crisis." IvyPanda , 18 May 2024, ivypanda.com/essays/discussion-the-covid-19-crisis/.
IvyPanda . (2024) 'Discussion: The COVID-19 Crisis'. 18 May.
IvyPanda . 2024. "Discussion: The COVID-19 Crisis." May 18, 2024. https://ivypanda.com/essays/discussion-the-covid-19-crisis/.
1. IvyPanda . "Discussion: The COVID-19 Crisis." May 18, 2024. https://ivypanda.com/essays/discussion-the-covid-19-crisis/.
Bibliography
IvyPanda . "Discussion: The COVID-19 Crisis." May 18, 2024. https://ivypanda.com/essays/discussion-the-covid-19-crisis/.
- Inequity Issue in the Workplace
- The COVID-19 RNA Vaccines: Pros and Cons
- Perception of Inequity in Assessment
- The Role of MSN in Ensuring the Safety of Public Health
- Government Intervention and Public Health
- Health and Safety Challenges in Ypsilanti
- Barriers to Healthcare Delivery in the U.S.: Case Studies Analysis
- High-Reliability Organizations(HRO) in Healthcare
Official websites use .gov
A .gov website belongs to an official government organization in the United States.
Secure .gov websites use HTTPS
A lock ( ) or https:// means you've safely connected to the .gov website. Share sensitive information only on official, secure websites.
COVID-19 Vaccine Equity for Racial and Ethnic Minority Groups

CDC is committed to COVID-19 vaccine equity, which is when everyone has fair and just access to COVID-19 vaccination. There are many social, geographic, political, economic, and environmental factors that create challenges to vaccination access and acceptance, and that often affect racial and ethnic minority groups. Some of these factors include:
- Education, income, and wealth gaps
- Job access and working conditions
- Racism and other forms of discrimination
- Gaps in healthcare access
- Transportation and neighborhood conditions
- Lack of trust as a result of past medical racism and experimentation
Because of these and other challenges, some Black or African American people and Hispanic or Latino people are less likely to be vaccinated against COVID-19 than people in other racial and ethnic minority groups and non-Hispanic White people. [1-3] You can view the most current race and ethnicity data on COVID-19 vaccination . In addition to being less likely to get a vaccine, Black or African American people and Hispanic or Latino people are more likely to get seriously ill and die from COVID-19 due to the factors listed above. [4-6] CDC uses the Social Vulnerability Index (SVI) to assess the potential negative effects on communities caused by external stresses on human health. You can view the most current health equity data on COVID-19.
Other racial and ethnic minority groups, including American Indian or Alaska Native people, have also been more severely affected by COVID-19 than non-Hispanic White people, due to the challenges listed above. However, vaccination rates among American Indian or Alaska Native people were among the highest earlier in the pandemic among racial and ethnic minority groups, [7] in part due to vaccination efforts from CDC and partners. Regardless, the gains early on can be lost if the follow up requirements are not sustained. Efforts to maintain sufficient up-to-date vaccination must be responsive to community needs. You can find more information about CDC COVID-19 activities in Tribal communities, including vaccination efforts, and communication resources.
CDC Is Committed to Vaccine Equity for Racial and Ethnic Minority Groups
CDC is paving the way in vaccine equity efforts with national, state, tribal, territorial, local, and community partners to ensure that Black or African American people and Hispanic or Latino people have fair and just access to COVID-19 vaccination. To support vaccine equity, CDC continues to communicate with and listen to all communities affected by COVID-19. CDC is working to build trust, increase collaboration, and create tools and resources to respond to the concerns and feedback from all communities affected by COVID-19, especially those disproportionately impacted. These activities, along with messages supported by science, can help to increase COVID-19 vaccine acceptance and make it easier to get vaccinated.
Communication and Educational Resources
You can use the resources below to engage with communities that have been affected by COVID-19. Many of the resources available can be tailored for racial and ethnic minority communities to:
- Help build vaccine confidence
- Share clear and accurate information to educate about COVID-19
- Raise awareness about the benefits of vaccination and address common questions and concerns
- Adapt key messages to the language, tone, and format that will resonate with communities
- Understand community needs regarding COVID-19 vaccines
COVID-19 Vaccines for Children and Teens : Resources for parents and caregivers to help find COVID-19 vaccines for children and information about COVID-19 vaccination for children 5 years and older.
COVID-19 Vaccination for Children 5-11 Years Old : Information for providers, jurisdictions, and partners planning vaccination of children, clinical research, and information for children with developmental disabilities.
A Guide for Community Partners—Increasing COVID-19 Vaccine Uptake Among Racial and Ethnic Minority Communities : A resource for community organizations to engage in or support COVID-19 vaccination confidence and access in racial and ethnic minority communities. Explore strategies, interventions, and ready-made messages and materials. This document is also available in Spanish .
COVID-19 Vaccination Toolkit for Health Departments and Other Public Health Partners and Community-Based Organizations Vaccine Toolkit: Include key messages and community engagement strategies that build trust and educate communities about COVID-19 vaccines.
Communication Toolkit for Migrants, Refugees, and Other Limited- English-Proficient Populations : Prevention and vaccination messaging for public health professionals, health care providers, and community organizations to reach communities that speak languages other than English.
Rapid Community Assessment Guide : Resources for state and local health departments to identify communities at risk for low COVID-19 vaccine uptake and understand community needs regarding COVID-19 vaccination.
COVID-19 Vaccination for Essential Workers: Racial and ethnic minority groups are disproportionately represented among essential work and industries . This page includes resources for employees and employers to help plan for and encourage COVID-19 vaccination to protect the workplace.
CDC has printable resources covering a wide range of topics related to COVID-19 vaccines that can be filtered by audience.
- Facts About COVID-19 Vaccines : General information about COVID-19 vaccines. Available in 27 languages.
- What to Expect after Getting a COVID-19 Vaccine : Information on what to expect after getting a COVID-19 vaccine. Available in 10 languages.
- A Safe and Effective COVID-19 Vaccine is Now Available : Comic-book style graphic fotonovela that tells the story of a daycare worker’s decision to get vaccinated against COVID-19. Available in English, Spanish, and Haitian Creole.
CDC Partnerships and Funding
Health and vaccine equity are essential parts of CDC’s mission. CDC works with national, state, tribal, territorial, local, and community partners to promote COVID-19 vaccination among Black or African American people and Hispanic or Latino people. To support these partnerships, CDC has provided funding for organizations that reach racial and ethnic minority groups. This funding includes:
- $3 billion awarded to 64 jurisdictions to support local health departments and community-based organizations in launching new programs and initiatives to increase vaccine access, acceptance, and uptake in communities disproportionately impacted by COVID-19
- $2.25 billion awarded to health departments across the United States and its territories to work in collaboration with community partners to support efforts to address COVID-19 health disparities
- $348 million to organizations for community health worker (CHW) services to support COVID-19 prevention and control, and $32 million to organizations for CHW services to support training, technical assistance, and evaluation, all funded through the CDC’s Community Health Workers for COVID Response and Resilient Communities initiative .
Additional CDC efforts toward vaccine equity for racial and ethnic minority groups include funding for:
- 8 national organizations through CDC’s Partnering with National Organizations to Increase Vaccination Coverage Across Different Racial and Ethnic Adult Populations Currently Experiencing Disparities , including: Asian and Pacific Islander American Health Forum, National Alliance for Hispanic Health, National Minority Quality Forum, National Urban League, Northwest Portland Area Indian Health Board, National Council of Negro Women, UnidosUS, Conference of National Black Churches
- 4 medical organizations serving racial and ethnic minority groups through CDC’s Partnering with Professional and Medical Associations to Increase Vaccination Coverage Across Different Racial and Ethnic Adult Populations Experiencing Disparities , including: National Medical Association, National Hispanic Medical Association, Association of American Indian Physicians, National Council of Urban Indian Health
- 3 national foundations through CDC’s Partnering with National Organizations to Support Community-Based Organizations to Increase Vaccination Coverage Across Different Racial and Ethnic Adult Populations Currently Experiencing Disparities , including: CDC Foundation, Community Catalyst, Urban Institute
- 34 national, state, tribal, and community organizations through CDC’s Racial and Ethnic Approaches to Community Health – REACH , including: Alaska Native Tribal Health Consortium, Allegheny County, PA, American Heart Association, California Department of Public Health, Cicatelli Associates, Inc., City of Hartford, CT, City of Miami Gardens, FL, City of San Antonio Metropolitan Health District, TX, City of Worcester, MA, County of San Diego, Health and Human Services Agency, CA, Cuyahoga County Board of Health, Dekalb County Board of Health, GA, Eastern Michigan University, Health and Hospital Corporation of Marion County, Health Partners Initiative DBA Partnership for a Healthy Lincoln, NE, Houston County Board of Health, TX, Leadership Council for Healthy Communities, Lowell Community Health Center, Mississippi Public Health Institute, Montgomery Area Community Wellness Coalition, AL, Multnomah County Health Department, National Kidney Foundation of Michigan, Partners in Health, Penn State Health Milton S. Hershey Medical Center, Pima County Health Department, AZ, Presbyterian Healthcare Services, Public Health Advocates, Rosedale Assistance & Opportunities, Seattle-King County Public Health Department, WA, Southern Nevada Health District, The Institute for Family Health, University of Arkansas for Medical Sciences, YMCA of Coastal Georgia
Through these and other partnerships, CDC is working to remove barriers to COVID-19 vaccination access and promote vaccine equity. In line with this effort, CDC works with the Federal Retail Pharmacy Program to conduct community-based activities and use data to ensure COVID-19 vaccines are accessible in all communities.
Because of the availability of COVID-19 vaccines, the nation is closer than ever to ending the COVID-19 pandemic in the United States. Yet challenges remain in ensuring all people have fair and just access to COVID-19 vaccination. CDC is committed to ongoing work to promote vaccine equity.
Resources on COVID-19 and Health Equity
Cdc health equity resources.
- COVID Data Tracker’s Health Equity Landing Page
- COVID-19 Racial and Ethnic Health Disparities
- Health Equity in Action
- Health Equity: Promoting Fair Access to Health
Other Resources
- Emory University’s COVID-19 Health Equity Interactive Dashboard
- Morehouse School of Medicine, Satcher Health Leadership Institute’s Health Equity Tracker
- National Academy of Medicine’s Resources on Health Equity in the Context of COVID-19 & Disproportionate Outcomes for Marginalized Groups
- Khubchandani, J., & Macias, Y. (2021). COVID-19 Vaccination Hesitancy in Hispanics and African-Americans: A Review and Recommendations for Practice. Brain, behavior, & immunity-health, 100277.
- Baack, B. N., Abad, N., Yankey, D., Kahn, K. E., Razzaghi, H., Brookmeyer, K, et al. (2021). MMWR—COVID-19 vaccination coverage and intent among adults aged 18–39 years—United States, March–May 2021.
- Kricorian, K., & Turner, K. (2021). Covid-19 vaccine reluctance in older Black and Hispanic adults: Cultural sensitivity and institutional trust. Journal of the American Geriatrics Society, S214-S214.
- Romano, S. D. (2021). Trends in racial and ethnic disparities in COVID-19 hospitalizations, by region—United States, March–December 2020. MMWR. Morbidity and mortality weekly report, 70.
- Mackey, K., Ayers, C. K., Kondo, K. K., Saha, S., Advani, S. M., Young, S. et al. (2021). Racial and ethnic disparities in COVID-19–related infections, hospitalizations, and deaths: a systematic review. Annals of internal medicine, 174(3), 362-373.
- Mude, W., Oguoma, V. M., Nyanhanda, T., Mwanri, L., & Njue, C. (2021). Racial disparities in COVID-19 pandemic cases, hospitalizations, and deaths: A systematic review and meta-analysis. Journal of Global Health, 11.
- CDC COVID Data Tracker Vaccination Demographics Trends
To receive email updates about COVID-19, enter your email address:
Exit Notification / Disclaimer Policy
- The Centers for Disease Control and Prevention (CDC) cannot attest to the accuracy of a non-federal website.
- Linking to a non-federal website does not constitute an endorsement by CDC or any of its employees of the sponsors or the information and products presented on the website.
- You will be subject to the destination website's privacy policy when you follow the link.
- CDC is not responsible for Section 508 compliance (accessibility) on other federal or private website.

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Elsevier - PMC COVID-19 Collection
Impact of COVID-19 on the social, economic, environmental and energy domains: Lessons learnt from a global pandemic
a School of Information Systems and Modelling, Faculty of Engineering and Information Technology, University of Technology Sydney, NSW 2007, Australia
I.M. Rizwanul Fattah
Md asraful alam.
b School of Chemical Engineering, Zhengzhou University, Zhengzhou 450001, China
A.B.M. Saiful Islam
c Department of Civil and Construction Engineering, College of Engineering, Imam Abdulrahman Bin Faisal University, Dammam 31451, Saudi Arabia
Hwai Chyuan Ong
S.m. ashrafur rahman.
d Biofuel Engine Research Facility, Queensland University of Technology (QUT), Brisbane, QLD 4000, Australia
e Tarbiat Modares University, P.O.Box: 14115-111, Tehran, Iran
f Science and Math Program, Asian University for Women, Chattogram 4000, Bangladesh
Md. Alhaz Uddin
g Department of Civil Engineering, College of Engineering, Jouf University, Sakaka, Saudi Arabia
T.M.I. Mahlia
COVID-19 has heightened human suffering, undermined the economy, turned the lives of billions of people around the globe upside down, and significantly affected the health, economic, environmental and social domains. This study aims to provide a comprehensive analysis of the impact of the COVID-19 outbreak on the ecological domain, the energy sector, society and the economy and investigate the global preventive measures taken to reduce the transmission of COVID-19. This analysis unpacks the key responses to COVID-19, the efficacy of current initiatives, and summarises the lessons learnt as an update on the information available to authorities, business and industry. This review found that a 72-hour delay in the collection and disposal of waste from infected households and quarantine facilities is crucial to controlling the spread of the virus. Broad sector by sector plans for socio-economic growth as well as a robust entrepreneurship-friendly economy is needed for the business to be sustainable at the peak of the pandemic. The socio-economic crisis has reshaped investment in energy and affected the energy sector significantly with most investment activity facing disruption due to mobility restrictions. Delays in energy projects are expected to create uncertainty in the years ahead. This report will benefit governments, leaders, energy firms and customers in addressing a pandemic-like situation in the future.
1. Introduction
The newly identified infectious coronavirus (SARS-CoV-2) was discovered in Wuhan and has spread rapidly since December 2019 within China and to other countries around the globe ( Zhou et al., 2020 ; Kabir et al., 2020 ). The source of SARS-CoV-2 is still unclear ( Gorbalenya et al., 2020 ). Fig. 1 demonstrates the initial timeline of the development of SARS-CoV-2 ( Yan et al., 2020 ). The COVID-19 pandemic has posed significant challenges to global safety in public health ( Wang et al., 2020 ). On 31 st January 2020, the World Health Organization (WHO), due to growing fears about the rapid spread of coronavirus, announced a global epidemic and on 11 th March, the disease was recognised as a pandemic ( Chowdhury et al., 2021 ). COVID-19 clinical trials indicate that almost all patients admitted to hospital have trouble breathing and pneumonia-like symptoms ( Holshue et al., 2020 ). Clinical diagnosis has identified that COVID-19 (disease caused by SARS-CoV-2) patients have similar indications to other coronavirus affected patients, e.g. Middle East Respiratory Syndrome (MERS) and Severe Acute Respiratory Syndrome (SARS) ( Wang and Su, 2020 ). The initial indication of a COVID-19 infection is coughing, fever, and short breath, and in the later stages, it can damage the kidney, cause pneumonia, and unexpected death ( Mofijur et al., 2020 ). The vulnerability of the elderly (>80 years of age) is high, with a fatality rate of ~22% of cases infected by COVID-19 ( Abdullah et al., 2020 ). The total number of confirmed COVID-19 cases has reached over 33 million as of 29 th September 2020, with more than 213 countries and regions affected by the pandemic ( Worldometer, 2020 ). Over 1,003,569 people have already passed away ( Worldometer, 2020 ) due to COVID-19. Most countries are currently trying to combat the virus spread by screening for COVID-19 in large numbers and maintaining social distancing policies with an emphasis on the health of human beings.

The initial stage development timeline for COVID-19 ( Yan et al., 2020 ).
Fig. 2 shows infections and replication cycle of the coronavirus. In extreme cases, the lungs are the most severely damaged organ of a SARS-CoV-2 infected person (host). The alveoli are porous cup-formed small cavities located in the structure of the lungs where the gas exchange of the breathing process take place. The most common cells on the alveoli are the type II cells.

Infections and replication cycle of the coronavirus ( Acter et al., 2020 ).
It has been reported that travel restrictions play a significant role in controlling the initial spread of COVID-19 ( Chinazzi et al., 2020 ; Aldila et al., 2020 ; Beck and Hensher, 2020 ; Bruinen de Bruin et al., 2020 ; de Haas et al., 2020 ). It has been reported that staying at home is most useful in controlling both the initial and last phase of infectious diseases ( de Haas et al., 2020 ; Cohen, 2020 , Pirouz et al., 2020 ). However, since the start of the COVID-19 pandemic, quarantines, entry bans, as well as other limitations have been implemented for citizens in or recent travellers to several countries in the most affected areas ( Sohrabi et al., 2020 ). Also, most of the industries were shutdown to lower mobility. A potential benefit of these measures is the reduction of pollution by the industrial and transportation sector, improving urban sustainability ( Jiang et al., 2021 ). Fig. 3 shows the global responses to lower the impact of the COVID-19 outbreak. There have been negative economic and social implications due to restrictions and decreased travel readiness worldwide ( Leal Filho et al., 2020 ). A fall in the volume of business activity and international events and an increase in online measures could have a long-term impact. The status of global transport and air activity as a result of the COVID-19 pandemic is shown in Fig. 4 ( International Energy Agency (IEA), 2020 ). By March 2020, the average global road haulage activity in regions with lockdowns had declined to almost 50% of the 2019 standard. Air travel has almost completely stopped in certain regions with aviation activity decreasing by over 90% in some European countries. Air activity in China recovered slightly from a low in late February, with lockdown measures somewhat eased. Nevertheless, as lockdowns spread, by the end of Q1 2020, global aviation activity decreased by a staggering 60%.

Initial preventive measures to lower the COVID-19 outbreak ( Bruinen de Bruin et al., 2020 ).

Global transport and aviation activity in the first quarter of the year 2020 ( International Energy Agency (IEA), 2020 ).
The spread of COVID-19 continues to threaten the public health situation severely ( Chinazzi et al., 2020 ) and greatly affect the global economy. Labour displacement, business closures and stock crashes are just some of the impacts of this global lockdown during the pandemic. According to the International Monetary Fund (IMF), the effect of COVID-19 will result in a worldwide economic decline in 2020 and a decline in the economic growth to 3% ( International Monetary Fund (IMF) ). COVID-19 has a detrimental impact on economic growth due to two primary factors. In the beginning, the exponential growth of the global epidemic directly contributed to considerable confusion about instability in the financial and capital markets. Secondly, countries have strictly regulated human movement and transport to monitor the growth of the epidemic and significantly reduced economic activity, putting pressure on both consumer and productive economic activity.
Since the 1970s, the link between economic growth and pollution has been an important global concern. The assessment of energy and financial efficiency is usually connected to environmental pollution research. Green practices at a national level, the inclusion of renewable energy, regulatory pressure and the sustainable use of natural resources are associated with environmental sustainability ( Khan et al., 2020 ). One study has shown that environmental pollution increases with economic growth and vice versa ( Cai et al., 2020 ). The strict control over movement and business activity due to COVID-19 has led to an economic downturn, which is in turn, expected to reduce environmental pollution. This paper systematically assesses how the novel coronavirus has had a global effect on society, the energy sector and the environment. This study presents data compiled from the literature, news sources and reports (from February 2020 to July 2020) on the management steps implemented across the globe to control and reduce the impact of COVID-19. The study will offer guidelines for nations to assess the overall impact of COVID-19 in their countries.
2. Impact of COVID-19 on the environmental domain
2.1. waste generation.
The generation of different types of waste indirectly creates a number of environmental concerns ( Schanes et al., 2018 ). The home isolation and pop-up confinement services in countries that have experienced major impacts of COVID-19 are standard practise, as hospitals are given priority to the most serious cases. In some countries, hotels are being used to isolate travellers for at least two weeks on entry. In several countries, such quarantine measures have resulted in consumers increasing their domestic online shopping activity that has increased domestic waste. In addition, food bought online is packaged, so inorganic waste has also increased. Medical waste has also increased. For instance, Wuhan hospitals produced an average of 240 metric tonnes of medical waste during the outbreak compared to their previous average of fewer than 50 tonnes ( Zambrano-Monserrate et al., 2020 ). This unusual situation poses new and major obstacles in the implementation of waste collection services, thus creating a new challenge for waste collection and recycling groups. With the global adaptation to exponential behavioural and social shifts in the face of COVID-19 challenges, municipal services such as waste collection and management need to alter their operations to play an important role in reducing the spread of infectious diseases.
2.1.1. Lifespan of COVID-19 on different waste media
SARS-CoV-2′s transmission activity has major repercussions for waste services. SARS-CoV-2 attacks host cells with ACE2 proteins directly. ACE2 is a cell membrane-associated enzyme in the lungs, heart and kidneys. When all the resources in the host cell are infected and depleted, the viruses leave the cell in the so-called shedding cycle ( Nghiem et al., 2020 ). Clinical and virological evidence suggests that the elimination of the SARS-CoV-2 virus is most relevant early on, right before and within a couple of days of the onset of the illness ( AEMO, 2020 ). Fomites are known as major vectors for the replication of other infectious viruses during the outbreak ( Park et al., 2015 ). Evidence from SARS-CoV-2 and other coronaviruses show that they remain effective for up to a few days in the atmosphere and on a variety of surfaces ( Fig. 5 ). The survival time of SARS-CoV-2 on hard and plastic surfaces is up to three days indicating that waste materials from COVID-19 patients may contain coronavirus and be a source of infection spread ( Chin et al., 2020 ). During the early stages of this epidemic, updated waste disposal methods to tackle COVID-19 were not implemented on the broader community. The concept of clinical waste essentially also applies to waste from contaminated homes and quarantine facilities. Throughout this pandemic, huge volumes of domestic and hospital waste, particularly plastic waste, has been generated. This has already impeded current efforts to reduce plastic waste and decrease its disposal in the environment. More effort should be made to find alternatives to heavily used plastics.

The lifespan of SARS-CoV-2 on different media ( Chin et al., 2020 ; van Doremalen et al.; 2020 ; Ye et al., 2016 )
2.1.2. Waste recycling service
COVID-19 has already had significant effects on waste recycling. Initially, as the outbreak spread and lockdowns were implemented in several countries, both public authorities and municipal waste management officials had to adjust to the situation quickly. Waste disposal has also been a major environmental problem for all technologically advanced nations, as no clear information was available about the retention time of SARS-CoV-2 ( Liu et al., 2020 ). Recycling is a growing and efficient means of pollution control, saving energy and conserving natural resources ( Ma et al., 2019 ). Recycling projects in various cities have been put on hold due to the pandemic, with officials worried about the possibility of COVID-19 spreading to recycling centres. Waste management has been limited in affected European countries. For example, Italy prohibited the sorting of waste by infected citizens. Extensive waste management during the pandemic is incredibly difficult because of the scattered nature of the cases and the individuals affected. The value of implementing best management practises for waste handling and hygiene to minimise employee exposure to potentially hazardous waste, should be highlighted at this time. Considering the possible role of the environment in the spread of SARS-CoV-2 ( Qu et al., 2020 ), the processing of both household and quarantine facility waste is a crucial point of control. Association of Cities and Regions for sustainable Resource management (ACR+) has reported on the provision of separate collection services to COVID-19 contaminated households and quarantine facilities to protect frontline waste workers in Europe, as shown in Fig. 6 . ACR+ also suggests a 72-hour delay in waste disposal (the possible lifespan of COVID-19 in the environment) ( Nghiem et al., 2020 ). Moreover, the collected waste should be immediately transported to waste incinerators or sites without segregation.

Recommended waste management during COVID-19 ( ACR+ 2020 ).
2.2. NO 2 emissions
Without the global pandemic, we had naively anticipated that in 2020 global emissions would rise by around 1% on a five-year basis. Instead, the sharp decline in economic activity in response to the current crisis will most probably lead to a modest drop in global greenhouse emissions. The European Space Agency (ESA), with its head office in Paris, France, is an intergovernmental body made up of 22 European countries committed to exploring the international space. To monitor air pollution in the atmosphere, the ESA uses the Copernicus Sentinel-5P Satellite. In addition to the compound contents measurement, the Copernicus Sentinel-5P troposphere monitor (TROPOMI) and other specified precision equipment measure ozone content, sulphur dioxide, carbon monoxide, and methane. Table 1 shows NO 2 emissions data acquisition by ESA using Sentinel-5P across different regions of Europe ( Financial Times, 2020 ).
NO 2 emissions data acquisition by ESA using Sentinel-5P across different regions of Europe ( Financial Times, 2020 ).
Burning fossil fuels, such as coal, oil, gas and other fuels, is the source of atmospheric nitrogen dioxide ( Munawer, 2018 ). The bulk of the NO 2 in cities, however, comes from emissions from motor vehicles (approximately 80%). Other NO 2 sources include petroleum and metal refining, coal-fired electricity, other manufacturing and food processing industries. Some NO 2 is naturally produced by lightning in the atmosphere and from the soil, water, and plants, which, taken together, constitutes not even 1% of the total NO 2 found in the air of our localities. Due to pollution variations as well as changes in weather conditions, the levels of the NO 2 in our atmosphere differ widely every day. Anthropogenic pollution is estimated to contain around 53 million tonnes of NO 2 annually. Nitrogen dioxide, together with nitrogen oxide (NO), are considered the major components of oxides of nitrogen (NOx) ( M Palash et al., 2013 ; Fattah et al., 2013 ). NO, and NO 2 are susceptible to other chemicals and form acid rain that is toxic to the environment ( Mofijur et al., 2013 ; Ashraful et al., 2014 ), WHO lists NO 2 as one of the six typical air contaminants in the atmosphere. For this reason, the amount of NO 2 in the atmosphere is used as a precise measure for determining whether the COVID-19 outbreak affects environmental pollution.
NO 2 is an irritating reddish-brown gas with an unpleasant smell, and when cooled or compressed, it becomes a yellowish-brown liquid ( Wang and Su, 2020 ). NO 2 inflames the lung linings and can decrease lung infection immunity. High levels of NO 2 in the air we breathe can corrode our body's lung tissues . Nitrogen dioxide is a problematic air pollutant because it leads to brown photochemical smog formation, which can have significant impacts on human health ( Huang et al., 2020 ). Brief exposure to high concentrations of NO 2 can lead to respiratory symptoms such as coughing, wheezing, bronchitis, flu, etc., and aggravate respiratory illnesses such as asthma. Increased NO 2 levels can have major effects on individuals with asthma, sometimes leading to frequent and intense attacks ( Munawer, 2018 ). Asthmatic children and older individuals with cardiac illness are most vulnerable in this regard. However, its main drawback is that it produces two of the most harmful air pollutants, ozone and airborne particles. Ozone gas affects our lungs and the crops we eat.
2.2.1. NO₂ emissions across different countries
According to the ESA ( European Space Agency (ESA), 2020 ), average levels of NO 2 declined by 40% between 13 th March 2020 to 13 th April 2020. The reduction was 55% compared to the same period in 2019. Fig. 7 compares the 2019-2020 NO 2 concentration ( European Space Agency (ESA), 2020 ). The displayed satellite image was captured with the TROPOMI by ESA satellite Sentinel-5P. The percentage reductions in average NO 2 emissions in European countries during the COVID-19 outbreak from 1 st April to 30 th April 2020 can be seen in Fig. 8 ( Myllyvirta, 2020 ). Portugal, Spain, Norway, Croatia, France, Italy, and Finland are the countries that experienced the largest decrease in NO 2 levels, with 58%, 48%, 47%, 43% and 41%, respectively.

Comparison of the NO 2 concentration between 2019 and 2020 in Europe ( European Space Agency (ESA), 2020 ).

Changes in average NO 2 emission in different countries ( Myllyvirta, 2020 ).
The average 10-day animation of NO 2 emissions throughout Europe (from 1 st January to 11 th March 2020), demonstrated the environmental impact of Italy's economic downturn, see Fig. 9 ( European Space Agency (ESA), 2020 ). In the recent four weeks (Last week of February 2020 to the third week of March 2020) the average concentration of NO 2 in Milan, Italy, has been at least 24% less than the previous four weeks. In the week of 16 – 22 March, the average concentration was 21% lower than in 2019 for the same week. Over the last four weeks of January 2020, NO 2 emissions in Bergamo city has been gradually declining. During the week of 16–22 March, the average concentration was 47% less than in 2019. In Rome, NO 2 rates were 26–35% lower than average in the last four weeks (third week of January 2020 to the third week of February 2020) than they were during the same week of 2019 ( Atmosphere Monitoring Service, 2020 ).

Changes of NO 2 emission (a) over entire Italy (b) capital city (c) other cities ( European Space Agency (ESA), 2020 ; Atmosphere Monitoring Service, 2020 ).
Fig. 10 shows a comparison of NO 2 volumes in Spain in March 2019 and 2020. As per ( European Space Agency (ESA), 2020 ), Spain's NO 2 pollutants decreased by up to 20–30% due to lockdown, particularly across big cities like Madrid, Barcelona, and Seville. ESA Sentinel-5P captured the satellite image using TROPOMI. Satellite images of the 10 days between 14 th and 25 th March 2020 show that NO 2 tropospheric concentration in the areas of Madrid, Barcelona, Valencia, and Murcia ranges from 0–90 mg/m 3 . The NO 2 tropospheric concentration for Seville is almost 0 mg/m 3 for the same time. For March 2019, the average NO 2 tropospheric concentration for the Madrid area was between 90 and 160 mg/m 3 . At the same time, the range of NO 2 tropospheric concentration for Barcelona, Valencia, and Seville area was between 90–140 mg/m 3 , 90-130 mg/m 3 , and 30–50 mg/m 3 , respectively.

Comparison between before and after lockdown NO 2 emissions in Spain ( European Space Agency (ESA), 2020 ).
Fig. 11 shows the reduction in the amount of NO 2 emissions in France in March 2019 and 2020 ( European Space Agency (ESA), 2020 ). In France, levels of NO 2 have been reduced by 20% to 30%. The ESA Sentinel-5P satellite image was captured with the TROPOMI. In Paris and other major cities, the emission levels of NO 2 considerably lowered due to lockdown. The three major areas of France where NO 2 tropospheric concentration was significant are Paris, Lyon, Marseille and their surroundings. Satellite images of the ten days between 14 th and 25 th March 2020 show that NO 2 tropospheric concentration of the Paris, Lyon, Marseille areas ranges 30–90 mg/m 3 , 20–40 mg/m 3 and 40–80 mg/m 3 , respectively. For March 2019, the average NO 2 tropospheric concentration for the same areas was reported as 100–160 mg/m 3 , 30–60 mg/m 3, and 90–140 mg/m 3 , respectively.

Comparison of NO 2 emissions in France before and after lockdown ( European Space Agency (ESA), 2020 ).
Various industries across the UK have been affected by COVID-19, which has influenced air contamination. As shown in Fig. 12 , there were notable drops in the country's NO 2 emissions on the first day of quarantine ( Khoo, 2020 ). Edinburgh showed the most significant reduction. The average NO 2 emissions on 26 th March 2020, were 28 μg/m 3 while on the same day of 2019, this was 74 μg/m 3 ( Khoo, 2020 ). The second biggest reduction was observed in London Westminster where emissions reduced from 58 µg/m 3 to 30 µg/m 3 . Not all cities have seen such a significant decrease, with daily air pollution reducing by 7 μg/m 3 compared to the previous year in Manchester Piccadilly, for example ( Statista, 2020 ).

(a) Changes in NO 2 emissions in the UK during lockdown ( European Space Agency (ESA), 2020 ); (b) comparison of NO 2 emissions in 2019 and 2020 ( Khoo, 2020 ).
2.3. PM emission
The term particulate matter, referred to as PM, is used to identify tiny airborne particles. PM forms in the atmosphere when pollutants chemically react with each other. Particles include pollution, dirt, soot, smoke, and droplets. Pollutants emitted from vehicles, factories, building sites, tilled areas, unpaved roads and the burning of fossil fuels also contribute to PM in the air ( Baensch-Baltruschat et al., 2020 ). Grilling food (by burning leaves or gas grills), smoking cigarettes, and burning wood on a fireplace or stove also contribute to PM. The aerodynamic diameter is considered a simple way to describe PM's particle size as these particles occur in various shapes and densities. Particulates are usually divided into two categories, namely, PM 10 that are inhalable particles with a diameter of 10 μm or less and PM 2.5 which are fine inhalable particle with a diameter of 2.5 μm or less. PM 2.5 exposure causes relatively severe health problems such as non-fatal heart attacks, heartbeat irregularity, increased asthma, reduced lung function, heightened respiratory symptoms, and premature death ( Weitekamp et al., 2020 ).
PM 2.5 also poses a threat to the environment, including lower visibility (haze) in many parts of the globe. Particulates can be transported long distances then settle on the ground or in water sources. In these contexts and as a function of the chemical composition, PM 2.5 may cause acidity in lakes and stream water, alter the nutrient balance in coastal waters and basins, deplete soil nutrients and damage crops on farms, affect the biodiversity in the ecosystem, and contribute to acid rain. This settling of PM, together with acid rain, can also stain and destroy stones and other materials such as statues and monuments, which include valuable cultural artefacts ( Awad et al., 2020 ).
2.3.1. PM emission in different countries
Due to the COVID-19 outbreak, PM emission in most countries has been reduced ( Chatterjee et al., 2020 ; Ghahremanloo et al., 2021 ; Gualtieri et al., 2020 ; Sharifi and Khavarian-Garmsir, 2020 ; Srivastava, 2020 ). Fig. 13 shows the impact of COVID19 on PM emission in a number of some countries around the world ( Myllyvirta, 2020 ). The largest reductions in PM pollution took place in Portugal, with 55%, followed by Norway, Sweden, and Poland with reductions of 32%, 30%, and 28%, respectively. Spain, Poland, and Finland recorded PM emission reductions of 19%, 17% and 16%, respectively. Both Romania and Croatia recorded no changes in PM level, with Switzerland and Hungary recording about a 3% increase in PM emission.

Reduction of PM emission in different countries ( Myllyvirta, 2020 ).
PM emissions have been significantly reduced during the epidemic in most regions of Italy. Fig. 14 illustrates the changes in COVID-19 containment emissions before and after a lockdown in major cities in Italy. According to a recent study by Sicard et al. ( Sicard et al., 2020 ), lockdown interventions have had a greater effect on PM emission. They found that confinement measures reduce PM 10 emissions in all major cities by “around 30% to 53%” and “around 35% to 56%”.

Comparison of PM emission in Italy (a) PM 2.5 emission (b) Changes of PM 2.5 emission (c) PM 10 emission (d) Changes of PM 10 emission ( Sicard et al., 2020 ).
2.4. Noise emission
Noise is characterised as an undesirable sound that may be produced from different activities, e.g. transit by engine vehicles and high volume music. Noise can cause health problems and alter the natural condition of ecosystems. It is among the most significant sources of disruption in people and the environment ( Zambrano-Monserrate and Ruano, 2019 ). The European Environment Agency (EEA) states that traffic noise is a serious environmental problem that negatively affects the health and security of millions of citizens in Europe. The consequences of long-term exposure to noise include sleep disorders, adverse effects on the heart and metabolic systems, and cognitive impairment in children. The EEA estimates that noise pollution contributes to 48,000 new cases of heart disease and 12,000 early deaths per year. They also reported chronic high irritation for 22 million people and a chronic high level of sleep disorder for 6.5 million people ( Lillywhite, 2020 ).
Most governments have imposed quarantine measures that require people to spend much more time at home. This has considerably reduced the use of private and public transport. Commercial activities have almost completely stopped. In most cities in the world, these changes have caused a significant decline in noise levels. This was followed by a significant decline in pollution from contaminants and greenhouse gas emissions. Noise pollution from sources like road, rail or air transport has been linked to economic activity. Consequently, we anticipate that the levels of transport noise will decrease significantly due to the decreased demand for mobility in the short term ( Ro, 2020 ).
For example, it was obvious that environmental noise in Italy was reduced after 8 th March 2020 (the lockdown start date) due to a halt in commercial and recreational activities. A seismograph facility in Lombardy city in Italy that was severely affected by the COVID-19 pandemic indicated how the quarantine measures reduce both traffic and noise emissions. The comparison of the 24-hour seismic noise data before and after the lockdown period indicates a considerable drop in environmental noise in Italy ( Bressan, 2020 ).
3. Impact of COVID-19 on the socio-economic domain
COVID-19 has created a global health crisis where countless people are dying, human suffering is spreading, and people's lives are being upended ( Nicola et al., 2020 ). It is not only just a health crisis but also a social and economic crisis, both of which are fundamental to sustainable development ( Pirouz et al., 2020 ). On 11 th March 2020, when WHO declared a global pandemic, 118,000 reported cases spanning 114 countries with over 4,000 fatalities had been reported. It took 67 days from the first reported case to reach 100,000 cases, 11 days for the second 100,000, and just four days for the third ( United Nations Development Programme (UNDP), 2020 ). This has overwhelmed the health systems of even the richest countries with doctors being forced to make the painful decision of who lives and who dies. The COVID-19 pandemic has pushed the world into uncertainty and countries do not have a clear exit strategy in the absence of a vaccine. This pandemic has affected all segments of society. However, it is particularly damaging to vulnerable social groups, including people living in poverty, older persons, persons with disabilities, youths, indigenous people and ethnic minorities. People with no home or shelter such as refugees, migrants, or displaced persons will suffer disproportionately, both during the pandemic and in its aftermath. This might occur in multiple ways, such as experiencing limited movement, fewer employment opportunities, increased xenophobia, etc. The social crisis created by the COVID-19 pandemic may also increase inequality, discrimination and medium and long-term unemployment if not properly addressed by appropriate policies.
The protection measures taken to save lives are severely affecting economies all over the world. As discussed previously, the key protection measure adopted universally is the lockdown, which has forced people to work from home wherever possible. Workplace closures have disrupted supply chains and lowered productivity. In many instances, governments have closed borders to contain the spread. Other measures such as travel bans and the prohibition of sporting events and other mass gatherings are also in place. In addition, measures such as discouraging the use of public transport and public spaces, for example, restaurants, shopping centres and public attractions are also in place in many parts of the world. The situation is particularly dire in hospitality-related sectors and the global travel industry, including airlines, cruise companies, casinos and hotels which are facing a reduction in business activity of more than 90% ( Fernandes, 2020 ). The businesses that rely on social interactions like entertainment and tourism are suffering severely, and millions of people have lost their jobs. Layoffs, declines in personal income, and heightened uncertainty have made people spend less, triggering further business closures and job losses ( Ghosh, 2020 ).
A key performance indicator of economic health is Gross Domestic Product (GDP), typically calculated on a quarterly or annual basis. IMF provides a GDP growth estimate per quarter based on global economic developments during the near and medium-term. According to its estimate, the global economy is projected to contract sharply by 3% in 2020, which is much worse than the 2008 global financial crisis ( International Monetary Fund (IMF), 2020 ). The growth forecast was marked down by 6% in the April 2020 World Economic Outlook (WEO) compared to that of the October 2019 WEO and January 2020 WEO. Most economies in the advanced economy group are expected to contract in 2020, including the US, Japan, the UK, Germany, France, Italy and Spain by 5.9%, 5.4%, 6.5%, 7.0%, 7.2%, 9.1%, and 8.0% respectively. Fig. 15 a shows the effect of COVID-19 on the GDP of different countries around the globe. On the other hand, economies of emerging market and developing economies, excluding China, are projected to contract by only 1.0% in 2020. The economic recovery in 2021 will depend on the gradual rolling back of containment efforts in the latter part of 2020 that will restore consumer and investor confidence. According to the April 2020 WEO, the level of GDP at the end of 2021 in both advanced and emerging market and developing economies is expected to remain below the pre-virus baseline (January 2020 WEO Update), as shown in Fig. 15 b.

(a) Quarterly World GDP. 2019:Q1 =100, dashed line indicates estimates from January 2020 WEO; (b) GDP fall due to lockdown in selected countries.
A particular example of a country hardest hit by COVID-19 is Italy. During the early days of March, the Italian government imposed quarantine orders in major cities that locked down more than seventeen million people ( Andrews, 2020 ). The mobility index data by Google for Italy shows there has been a significant reduction in mobility (and therefore economic activity) across various facets of life. The reported decline of mobility in retail and recreation, grocery and pharmacy, transit stations and workplaces were 35%, 11%, 45% and 34% respectively ( Rubino, 2020 ). The Italian economy suffered great financial damage from the pandemic. The tourism, and hospitality sectors were among those most severely affected by foreign countries prohibiting travel to and from Italy, and by the government's national lockdowns in early March ( Brunton, 2020 ). A March 2020 study in Italy showed that about 99% of the companies in the housing and utility sector said the epidemic had affected their industry. In addition, transport and storage was the second most affected sector. Around 83% of companies operating in this sector said that their activities had been affected by the coronavirus ( Statista, 2020 ) pandemic. In April 2020, Italian Minister Roberto Gualtieri estimated a 6% reduction in the GDP for the year 2020 ( Bertacche et al., 2020 ). The government of Italy stopped all unnecessary companies, industries and economic activities on 21 st March 2020. Therefore The Economist estimates a 7% fall in GDP in 2020 ( Horowitz, 2020 ). The Economist predicted that the Italian debt-to-GDP ratio would grow from 130% to 180% by the end of 2020 ( Brunton, 2020 ) and it is also assumed that Italy will have difficulty repaying its debt ( Bertacche et al., 2020 ).
4. Impact of COVID-19 on the energy domain
COVID-19 has not only impacted health, society and the economy but it has also had a strong impact on the energy sector ( Chakraborty and Maity, 2020 ; Abu-Rayash and Dincer, 2020 ). World energy demand fell by 3.8% in the first quarter (Q1) of 2020 compared with Q1 2019. In Q1 of 2020, the global coal market was heavily impacted by both weather conditions and the downturn in economic activity resulting in an almost 8% fall compared to Q1 2019. The fall was primarily in the electricity sector as a result of substantial declines in demand (-2.5%) and competitive advantages from predominantly low-cost natural gas. The market for global oil has plummeted by almost 5%. Travel bans, border closures, and changes in work routines significantly decreased the demand for the use of personal vehicles and air transport. Thus rising global economic activity slowed down the use of fuel for transportation ( Madurai Elavarasan et al., 2020 ). In Q1 2020, the output from nuclear energy plants decreased worldwide, especially in Europe and the US, as they adjusted for lower levels of demand. Demand for natural gas dropped significantly, by approximately 2% in Q1 2020, with the biggest declines in China, Europe, and the United States. In the Q1 2020, the need for renewable energy grew by around 1.5%, driven in recent years by the increasing output of new wind and solar plants. Renewable energy sources substantially increased in the electricity generation mix, with record hourly renewable energy shares in Belgium, Italy, Germany, Hungary, and East America. The share of renewable energy sources in the electricity generation mix has increased. Table 2 shows the effect of COVID-19 outbreak on the energy demand around the world.
Impact of COVID-19 on global energy sector ( AEMO, 2020 ; CIS Editorial, 2020 ; Eurelectric, 2020 ; Livemint, 2020 ; Renewable Energy World, 2020 ; S&P Global, 2020 ; Madurai Elavarasan et al., 2020 ).
Different areas have implemented lockdown of various duration. Therefore, regional energy demand depends on when lockdowns were introduced and how lockdowns influence demand in each country. In Korea and Japan, the average impact on demand is reduced to less than 10%, with lower restrictions. In China, where the first COVID-19 confinement measures were introduced, not all regions faced equally stringent constraints. Nevertheless, virus control initiatives have resulted in a decline of up to 15% in weekly energy demand across China. In Europe, moderate to complete lockdowns were more radical. On average, a 17% reduction in weekly demand was experienced during temporary confinement periods. India's complete lockdown has cut energy requirements by approximately 30%, which indicates yearly energy needs are lowered by 0.6% for each incremental lockdown week ( International Energy Agency (IEA) 2020 ).
The International Energy Agency (IEA) has predicted an annual average decline in oil production of 9% in 2020, reflecting a return to 2012 levels. Broadly, as electricity demand has decreased by about 5% throughout the year, coal production may fall by 8%, and the output of coal-fired electricity generation could fall by more than 10%. During the entire year, gas demand may fall far beyond Q1 2020 due to a downward trend in power and industrial applications. Nuclear energy demand will also decrease in response to reduced electricity demand. The demand for renewable energies should grow due to low production costs and the choice of access to many power systems. Khan et al. (2020) reported that international trade is significantly and positively dependent on renewable energy. In addition, sustainable growth can be facilitated through the consumption of renewable energy which improves the environment, enhances national image globally and opens up international trade opportunities with environmentally friendly countries ( Khan et al., 2021 ). As such, policies that promote renewables can result in economic prosperity, create a better environment as well as meet critical goals for sustainable development ( Khan et al., 2020 ).
5. Preventive measures to control COVID-19 outbreak
COVID-19 is a major crisis needing an international response. Governments will ensure reliable information is provided to assist the public in combating this pandemic. Community health and infection control measures are urgently needed to reduce the damage done by COVID-19 and minimise the overall spread of the virus. Self-defence techniques include robust overall personal hygiene, face washing, refraining from touching the eyes, nose or mouth, maintaining physical distance and avoiding travel. In addition, different countries have already taken preventive measures, including the implementation of social distancing, medicine, forestation and a worldwide ban on wildlife trade. A significant aim of the community health system is to avoid SARS-CoV-2 transmission by limiting large gatherings. COVID-19 is transmitted by direct communication from individual to individual. Therefore, the key preventive technique is to limit mass gatherings. Table 3 shows the impact of lockdown measures on the recovery rate of COVID-19 infections. The baseline data for this table is the median value, for the corresponding day of the week, during the 5-week period 3 rd January to 6 th February 2020.
Mobility index report of different countries ( Ghosh, 2020 ; Johns Hopkins University (JHU), 2020 ; Worldometer, 2020 ).
As of today, no COVID-19 vaccine is available. Worldwide scientists are racing against time to develop the COVID-19 vaccine, and WHO is now monitoring more than 140 vaccine candidates. As of 29 th September 2020, about 122 candidates have been pre-clinically checked, i.e. determining whether an immune response is caused when administering the vaccine to animals ( Biorender, 2020 ). About 45 candidates are in stage I where tests on a small number of people are conducted to decide whether it is effective ( Biorender, 2020 ). About 29 candidates are in Phase II where hundreds of people are tested to assess additional health issues and doses ( Biorender, 2020 ). Only 14 candidates are currently in Phase III, where thousands of participants are taking a vaccine to assess any final safety concerns, especially with regard to side effects ( Biorender, 2020 ). 3 candidates are in Phase IV, where long-term effects of the vaccines on a larger population is observed ( Biorender, 2020 ). The first generation of COVID-19 vaccines is expected to gain approval by the end of 2020 or in early 2021 ( Peiris and Leung, 2020 ). It is anticipated that these vaccines will provide immunity to the population. These vaccines can also reduce the transmission of SARS-CoV-2 and lead to a resumption of a pre-COVID-19 normal. Table 4 shows the list of vaccines that have been passed in the pre-clinical stage. In addition, according to the COVID-19 vaccine and therapeutics tracker, there are 398 therapeutic drugs in development. Of these, 83 are in the pre-clinical phase, 100 in Phase I, 224 in Phase II, 119 in Phase III and 46 in Phase IV ( Biorender, 2020 ).
List of vaccines that have passed the pre-clinical stage ( Biorender, 2020 ).
In addition to the above, forestation and a worldwide ban on wildlife trade can also play a significant role in reducing the spread of different viruses. More than 30% of the ground area is covered with forests. The imminent increase in population contributes to deforestation in agriculture or grazing for food, industries and property. The rise in ambient temperature, sea levels and extreme weather events affects not only the land and environment but also public health ( Ruscio et al., 2015 ; Arora and Mishra, 2020 ). Huge investment has been made into treatments, rehabilitation and medications to avoid the impact of this epidemic. However, it is important to focus on basic measures, e.g. forestation and wildlife protection. The COVID-19 infection was initially spread from the Seafood Market, Wuhan, China. Therefore, China temporarily banned wildlife markets in which animals are kept alive in small cages. It has been reported that 60% of transmittable diseases are animal-borne, 70% of which are estimated to have been borne by wild animals ( Chakraborty and Maity, 2020 ). Deforestation is also related to various kinds of diseases caused by birds, bats, etc. ( Afelt et al., 2018 ). For example, COVID-19 is a bat-borne disease that is transmitted to humans. Therefore, several scientists have advised various countries to ban wildlife trade indefinitely so that humans can be protected from new viruses and global pandemics like COVID-19.
6. Conclusion
In this article, comprehensive analyses of energy, environmental pollution, and socio-economic impacts in the context of health emergency events and the global responses to mitigate the effects of these events have been provided. COVID-19 is a worldwide pandemic that puts a stop to economic activity and poses a severe risk to overall wellbeing. The global socio-economic impact of COVID-19 includes higher unemployment and poverty rates, lower oil prices, altered education sectors, changes in the nature of work, lower GDPs and heightened risks to health care workers. Thus, social preparedness, as a collaboration between leaders, health care workers and researchers to foster meaningful partnerships and devise strategies to achieve socio-economic prosperity, is required to tackle future pandemic-like situations. The impact on the energy sector includes increased residential energy demand due to a reduction in mobility and a change in the nature of work. Lockdowns across the globe have restricted movement and have placed people primarily at home, which has, in turn, decreased industrial and commercial energy demand as well as waste generation. This reduction in demand has resulted in substantial decreases in NO 2, PM, and environmental noise emissions and as a consequence, a significant reduction in environmental pollution. Sustainable urban management that takes into account the positive benefits of ecological balance is vital to the decrease of viral infections and other diseases. Policies that promote sustainable development, ensuring cities can enforce recommended measures like social distancing and self-isolation will bring an overall benefit very quickly. The first generation of COVID-19 vaccines is expected to gain approval by the end of 2020 or in early 2021, which will provide immunity to the population. It is necessary to establish preventive epidemiological models to detect the occurrence of viruses like COVID-19 in advance. In addition, governments, policymakers, and stakeholders around the world need to take necessary steps, such as ensuring healthcare services for all citizens, supporting those who are working in frontline services and suffering significant financial impacts, ensuring social distancing, and focussing on building a sustainable future. It is also recommended that more investment is required in research and development to overcome this pandemic and prevent any similar crisis in the future.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Editor: Dr. Syed Abdul Rehman Khan
- Abdullah S., et al. Air quality status during 2020 Malaysia movement control order (MCO) due to 2019 novel coronavirus (2019-nCoV) pandemic. Sci. Total Environ. 2020; 729 [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Abu-Rayash A., Dincer I. Analysis of the electricity demand trends amidst the COVID-19 coronavirus pandemic. Energy Res. Soc. Sci. 2020; 68 [ PMC free article ] [ PubMed ] [ Google Scholar ]
- ACR+, Municipal waste management and COVID-19. URL: https://www.acrplus.org/en/municipal-waste-management-covid-19 . Date accessed: 22nd September, 2020. 2020.
- Acter T., et al. Evolution of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) as coronavirus disease 2019 (COVID-19) pandemic: a global health emergency. Sci. Total Environ. 2020; 730 [ PMC free article ] [ PubMed ] [ Google Scholar ]
- AEMO, COVID-19 demand impact in Australia. https://aemo.com.au/en/news/demand-impact-australia-covid19 . Date accessed: 21st September, 2020. 2020.
- Afelt A., Frutos R., Devaux C. Bats, coronaviruses, and deforestation: toward the emergence of novel infectious diseases? Front. Microbiol. 2018; 9 702-702. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Aldila D., et al. A mathematical study on the spread of COVID-19 considering social distancing and rapid assessment: the case of Jakarta, Indonesia. Chaos Solitons Fractals. 2020; 139 [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Andrews, F., Before and after: Italy's tourist attractions left deserted amid coronavirus lockdown. https://www.thenational.ae/lifestyle/travel/before-and-after-italy-s-tourist-attractions-left-deserted-amid-coronavirus-lockdown-1.991274 . Date accessed: 21st September, 2020, in The National. 2020: Abu Dhabi.
- Arora N.K., Mishra J. COVID-19 and importance of environmental sustainability. Environ. Sustain. 2020; 3 (2):117–119. [ Google Scholar ]
- Ashraful A.M., et al. Production and comparison of fuel properties, engine performance, and emission characteristics of biodiesel from various non-edible vegetable oils: a review. Energy Convers. Manage. 2014; 80 :202–228. [ Google Scholar ]
- Atmosphere Monitoring Service. Air quality information confirms reduced activity levels due to lockdown in Italy. https://atmosphere.copernicus.eu/air-quality-information-confirms-reduced-activity-levels-due-lockdown-italy . Date accessed: 21st September, 2020. 2020.
- Awad O.I., et al. Particulate emissions from gasoline direct injection engines: a review of how current emission regulations are being met by automobile manufacturers. Sci. Total Environ. 2020; 718 [ PubMed ] [ Google Scholar ]
- Baensch-Baltruschat B., et al. Tyre and road wear particles (TRWP) - a review of generation, properties, emissions, human health risk, ecotoxicity, and fate in the environment. Sci. Total Environ. 2020; 733 [ PubMed ] [ Google Scholar ]
- Beck M.J., Hensher D.A. Insights into the impact of COVID-19 on household travel and activities in Australia – the early days under restrictions. Transp. Policy. 2020; 96 :76–93. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Bertacche, M., Orihuela, R., and Colten, J., Italy struck by deadliest day as virus prompts industry shutdown. https://www.bloomberg.com/news/articles/2020-03-21/germany-plans-extra-spending-of-eu150-billion-scholz-says . Date accessed: 21st September, 2020, in Bloomberg. 2020.
- Biorender, COVID-19 vaccine & therapeutics tracker. URL: https://biorender.com/covid-vaccine-tracker . Date accessed: 28th September, 2020. 2020.
- Bressan, D., Coronavirus lockdowns cause worldwide decrease in man-made seismic noise. https://www.forbes.com/sites/davidbressan/2020/04/04/coronavirus-lockdowns-cause-worldwide-decrease-in-man-made-seismic-noise/#1643453464da . Date accessed: 21st September, 2020, in Forbes. 2020.
- Bruinen de Bruin Y., et al. Initial impacts of global risk mitigation measures taken during the combatting of the COVID-19 pandemic. Saf. Sci. 2020; 128 [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Brunton, J., Nothing less than a catastrophe': Venice left high and dry by coronavirus. https://www.theguardian.com/travel/2020/mar/17/nothing-less-than-a-catastrophe-venice-left-high-and-dry-by-coronavirus . date accessed: 21st September, 2020, in The Guardian. 2020.
- Cai C., et al. Temperature-responsive deep eutectic solvents as green and recyclable media for the efficient extraction of polysaccharides from Ganoderma lucidum. J. Cleaner Prod. 2020; 274 [ Google Scholar ]
- Chakraborty I., Maity P. COVID-19 outbreak: migration, effects on society, global environment and prevention. Sci. Total Environ. 2020; 728 [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Chatterjee A., et al. High rise in carbonaceous aerosols under very low anthropogenic emissions over eastern Himalaya, India: impact of lockdown for COVID-19 outbreak. Atmos. Environ. 2020 [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Chin A.W.H., et al. Stability of SARS-CoV-2 in different environmental conditions. Lancet Microbe. 2020; 1 (1):e10. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Chinazzi M., et al. The effect of travel restrictions on the spread of the 2019 novel coronavirus (COVID-19) outbreak. Science. 2020; 368 (6489):395–400. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- CIS Editorial, Coronavirus impact on energy markets. URL: https://www.icis.com/explore/resources/news/2020/04/08/10482507/topic-page-coronavirus-impact-on-energy-markets . Date accessed: 2nd September, 2020. 2020.
- Cohen M.J. Does the COVID-19 outbreak mark the onset of a sustainable consumption transition? Sustainability. 2020; 16 (1):1–3. [ Google Scholar ]
- Chowdhury, M. A., M. B. A. Shuvho, M. A. Shahid, A. K. M. M. Haque, M. A. Kashem, S. S. Lam, H. C. Ong, M. A. Uddin and M. Mofijur (2021). "Prospect of biobased antiviral face mask to limit the coronavirus outbreak." Environmental Research 192: 110294. [ PMC free article ] [ PubMed ]
- de Haas M., Faber R., Hamersma M. How COVID-19 and the Dutch ‘intelligent lockdown’ change activities, work and travel behaviour: evidence from longitudinal data in the Netherlands. Transp. Res. Interdiscip. Perspect. 2020; 6 [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Eurelectric, Impact of COVID 19 on customers and society. URL: https://cdn.eurelectric.org/media/4313/impact_of_covid_19_on_customers_and_society-2020-030-0216-01-e-h-584D2757.pdf . Date accessed: 28th Spetember, 2020. 2020.
- European Space Agency (ESA). Sentinel-5P. https://www.esa.int/Applications/Observing_the_Earth/Copernicus/Sentinel-5P . Date accessed: 21st September, 2020. 2020.
- Fattah I.M.R., et al. Impact of various biodiesel fuels obtained from edible and non-edible oils on engine exhaust gas and noise emissions. Renew. Sustain. Energy Rev. 2013; 18 :552–567. [ Google Scholar ]
- Fernandes, N., Economic effects of coronavirus outbreak (COVID-19) on the world economy. https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3557504 . Date accessed: 21st September, 2020. 2020.
- Financial Times, Coronavirus: is Europe losing Italy? https://www.ft.com/content/f21cf708-759e-11ea-ad98-044200cb277f . Date accessed: 21st September, 2020, in Financial Times. 2020.
- Ghahremanloo M., et al. Impact of the COVID-19 outbreak on air pollution levels in East Asia. Sci. Total Environ. 2021; 754 [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Ghosh, I. The road to recovery: which economies are reopening? URL: https://www.visualcapitalist.com/the-road-to-recovery-which-economies-are-reopening-covid-19/ . Date accessed: 22nd September, 2020. 2020 [cited 2020 25th July, 2020]; Available from: https://www.visualcapitalist.com/the-road-to-recovery-which-economies-are-reopening-covid-19/.
- Gorbalenya A.E., et al. The species severe acute respiratory syndrome-related coronavirus: classifying 2019-nCoV and naming it SARS-CoV-2. Nat. Microbiol. 2020; 5 (4):536–544. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Gualtieri G., et al. Quantifying road traffic impact on air quality in urban areas: a Covid19-induced lockdown analysis in Italy. Environ. Pollut. 2020 [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Holshue M.L., et al. First case of 2019 novel coronavirus in the United States. N. Engl. J. Med. 2020; 382 (10):929–936. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Horowitz, J., Italy locks down much of the country's north over the coronavirus. URL: https://www.nytimes.com/2020/03/07/world/europe/coronavirus-italy.html . Date accessed: 21st September, 2020, in The New York Times. 2020.
- Huang, Y., W.-c. Mok, Y.-s. Yam, J. L. Zhou, N. C. Surawski, B. Organ, E. F. C. Chan, M. Mofijur, T. M. I. Mahlia and H. C. Ong (2020). Evaluating in-use vehicle emissions using air quality monitoring stations and on-road remote sensing systems. Science of The Total Environment 740: 139868. [ PubMed ]
- International Energy Agency (IEA) IEA; Paris: 2020. Global Energy Review. https://www.iea.org/reports/global-energy-review-2020 Date accessed: 21st September, 2020. 2020. [ Google Scholar ]
- International Monetary Fund (IMF), World Economic Outlook, April 2020: The Great Lockdown. https://www.imf.org/en/Publications/WEO/Issues/2020/04/14/weo-april-2020 . Date accessed: 22nd September, 2020. 2020.
- International Monetary Fund (IMF), World economic outlook, April 2020: The Great Lockdown. URL: https://www.imf.org/en/Publications/WEO/Issues/2020/04/14/weo-april-2020 . Date accessed: 21st September, 2020. 2020.
- Jiang P., et al. Spatial-temporal potential exposure risk analytics and urban sustainability impacts related to COVID-19 mitigation: a perspective from car mobility behaviour. J. Cleaner Prod. 2021; 279 [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Johns Hopkins University (JHU). COVID-19 dashboard by the center for systems science and engineering (CSSE) at Johns Hopkins University (JHU). https://coronavirus.jhu.edu/map.html . Date accessed: 25th July, 2020. 2020.
- Kabir M.T., et al. nCOVID-19 pandemic: from molecular pathogenesis to potential investigational therapeutics. Front. Cell Dev. Biol. 2020; 8 616-616. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Khan S.A.R., et al. Measuring the impact of renewable energy, public health expenditure, logistics, and environmental performance on sustainable economic growth. Sustain. Dev. 2020; 28 (4):833–843. [ Google Scholar ]
- Khan S.A.R., et al. Investigating the effects of renewable energy on international trade and environmental quality. J. Environ. Manage. 2020; 272 [ PubMed ] [ Google Scholar ]
- Khan S.A.R., et al. Determinants of economic growth and environmental sustainability in South Asian association for regional cooperation: evidence from panel ARDL. Environ. Sci. Pollut. Res. 2020 [ PubMed ] [ Google Scholar ]
- Khan S.A.R., et al. A state-of-the-art review and meta-analysis on sustainable supply chain management: future research directions. J. Cleaner Prod. 2021; 278 [ Google Scholar ]
- Khoo, A., Coronavirus lockdown sees air pollution plummet across UK. https://www.bbc.com/news/uk-england-52202974 . Date accessed: 21st September, 2020, in BBC News. 2020.
- Leal Filho W., et al. COVID-19 and the UN sustainable development goals: threat to solidarity or an opportunity? Sustainability. 2020; 12 (13):5343. [ Google Scholar ]
- Lillywhite, R., Air quality and wellbeing during COVID-19 lockdown. https://www.newswise.com/coronavirus/air-quality-and-wellbeing-during-covid-19-lockdown/?article_id=730455 . Date accessed: 21st September, 2020, in Newswise. 2020: USA.
- Liu M., et al. Waste paper recycling decision system based on material flow analysis and life cycle assessment: a case study of waste paper recycling from China. J. Environ. Manage. 2020; 255 [ PubMed ] [ Google Scholar ]
- Livemint. India's energy demand falls by 30% due to COVID-19 lockdown. URL: https://www.livemint.com/news/world/lockdown-cuts-india-s-energy-demand-by-30-says-iea-11588235067694.html . Date accessed: 28th September, 2020. 2020.
- M Palash S., et al. Impacts of biodiesel combustion on NOx emissions and their reduction approaches. Renewable Sustainable Energy Rev. 2013; 23 (0):473–490. [ Google Scholar ]
- Ma B., et al. Recycle more, waste more? When recycling efforts increase resource consumption. J. Cleaner Prod. 2019; 206 :870–877. [ Google Scholar ]
- Madurai Elavarasan R., et al. COVID-19: impact analysis and recommendations for power sector operation. Appl. Energy. 2020; 279 115739-115739. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Madurai Elavarasan R., et al. COVID-19: impact analysis and recommendations for power sector operation. Appl. Energy. 2020 [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Mofijur M., et al. A study on the effects of promising edible and non-edible biodiesel feedstocks on engine performance and emissions production: a comparative evaluation. Renew. Sustain. Energy Rev. 2013; 23 (0):391–404. [ Google Scholar ]
- Munawer M.E. Human health and environmental impacts of coal combustion and post-combustion wastes. J. Sustain. Min. 2018; 17 (2):87–96. [ Google Scholar ]
- Myllyvirta, L., 11,000 air pollution-related deaths avoided in Europe as coal, oil consumption plummet. https://energyandcleanair.org/air-pollution-deaths-avoided-in-europe-as-coal-oil-plummet/ . Date accessed: 21st September, 2020. 2020.
- Mofijur, M., I. M. Rizwanul Fattah, A. B. M. Saiful Islam, M. N. Uddin, S. M. Ashrafur Rahman, M. A. Chowdhury, M. A. Alam and M. A. Uddin (2020). "Relationship between Weather Variables and New Daily COVID-19 Cases in Dhaka, Bangladesh." Sustainability 12(20): 8319.
- Nghiem L.D., et al. The COVID-19 pandemic: considerations for the waste and wastewater services sector. Case Stud. Chem. Environ. Eng. 2020; 1 [ Google Scholar ]
- Nicola M., et al. The socio-economic implications of the coronavirus pandemic (COVID-19): a review. Int. J. Surg. 2020; 78 :185–193. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Park G.W., et al. Evaluation of a new environmental sampling protocol for detection of human norovirus on inanimate surfaces. Appl. Environ. Microbiol. 2015; 81 (17):5987–5992. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Peiris M., Leung G.M. What can we expect from first-generation COVID-19 vaccines? Lancet North Am. Ed. 2020 [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Pirouz B., et al. Investigating a serious challenge in the sustainable development process: analysis of confirmed cases of COVID-19 (new type of coronavirus) through a binary classification using artificial intelligence and regression analysis. Sustainability. 2020; 12 (6):2427. [ Google Scholar ]
- Qu G., et al. An imperative need for research on the role of environmental factors in transmission of novel coronavirus (COVID-19) Environ. Sci. Technol. 2020; 54 (7):3730–3732. [ PubMed ] [ Google Scholar ]
- Renewable Energy World, Renewables achieve clean energy record as COVID-19 hits demand. URL: https://www.renewableenergyworld.com/2020/04/06/renewables-achieve-clean-energy-record-as-covid-19-hits-demand/ . Date accessed: 28th September, 2020. 2020.
- Ro, C., Is coronavirus reducing noise pollution? https://www.forbes.com/sites/christinero/2020/04/19/is-coronavirus-reducing-noise-pollution/#2fe787d5766f . Date accessed: 21st September, 2020, in Forbes. 2020.
- Rubino, d.M., Coronavirus, il decreto del governo: tutte le misure per la zona arancione e quelle per il resto d'Italia. URL: https://www.repubblica.it/cronaca/2020/03/08/news/coronavirus_i_decreti_del_governo-250617415/ . Date accessed: 21st September, 2020, in la Repubblica. 2020.
- Ruscio B.A., et al. One health - a strategy for resilience in a changing arctic. Int. J. Circumpolar Health. 2015; 74 :27913. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- S&P Global, Japan, Singapore lockdowns to stifle Asian gas, power demand further. https://www.spglobal.com/platts/en/market-insights/latest-news/natural-gas/040720-japan-singapore-lockdowns-to-stifle-asian-gas-power-demand-further . Date accessed: 21st September, 2020. 2020.
- Schanes K., Dobernig K., Gözet B. Food waste matters - a systematic review of household food waste practices and their policy implications. J. Cleaner Prod. 2018; 182 :978–991. [ Google Scholar ]
- Sharifi A., Khavarian-Garmsir A.R. The COVID-19 pandemic: impacts on cities and major lessons for urban planning, design, and management. Sci. Total Environ. 2020 [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Sicard P., et al. Amplified ozone pollution in cities during the COVID-19 lockdown. Sci. Total Environ. 2020; 735 [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Sohrabi C., et al. World Health Organization declares global emergency: a review of the 2019 novel coronavirus (COVID-19) Int. J. Surg. 2020; 76 :71–76. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Srivastava A. COVID-19 and air pollution and meteorology-an intricate relationship: a review. Chemosphere. 2020 [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Statista, Perceived impact of coronavirus (COVID-19) among Italian companies in March 2020, by macro sector. https://www.statista.com/statistics/1103017/perceived-impact-of-coronavirus-covid-19-among-italian-companies-by-sector/ . Date accessed: 21st September, 2020. 2020.
- Statista, COVID-19 lockdown affect on nitrogen dioxide (NO2) emissions in UK cities in March 2020 compared with March 2019. https://www.statista.com/statistics/1111519/no2-emissions-decrease-due-to-lockdown-united-kingdom/ . Date accessed: 21st September, 2020. 2020.
- United Nations Development Programme (UNDP), The social and economic impact of COVID-19 in the Asia-Pacific region. https://www.undp.org/content/undp/en/home/librarypage/crisis-prevention-and-recovery/the-social-and-economic-impact-of-covid-19-in-asia-pacific.html . Date accessed: 21st September, 2020. 2020.
- van Doremalen N., et al. Aerosol and Surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N. Engl. J. Med. 2020; 382 (16):1564–1567. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Wang D., et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA. 2020; 323 (11):1061–1069. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Wang Q., Su M. A preliminary assessment of the impact of COVID-19 on environment – a case study of China. Sci. Total Environ. 2020; 728 [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Weitekamp C.A., et al. Health effects from freshly emitted versus oxidatively or photochemically aged air pollutants. Sci. Total Environ. 2020; 704 [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Worldometer, Reported cases and deaths by country, territory, or conveyance. https://www.worldometers.info/coronavirus/ . Date accessed: 25th July, 2020. 2020.
- Worldometer, Reported cases and deaths by country, territory, or conveyance. https://www.worldometers.info/coronavirus/ . Date accessed: 22nd September, 2020. 2020.
- Yan Y., et al. The first 75 days of novel coronavirus (SARS-CoV-2) outbreak: recent advances, prevention, and treatment. Int. J. Environ. Res. Public Health. 2020; 17 (7):2323. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Ye Y., et al. Survivability, partitioning, and recovery of enveloped viruses in untreated municipal wastewater. Environ. Sci. Technol. 2016; 50 (10):5077–5085. [ PubMed ] [ Google Scholar ]
- Zambrano-Monserrate M.A., Ruano M.A. Does environmental noise affect housing rental prices in developing countries? Evidence from Ecuador. Land Use Policy. 2019; 87 [ Google Scholar ]
- Zambrano-Monserrate M.A., Ruano M.A., Sanchez-Alcalde L. Indirect effects of COVID-19 on the environment. Sci. Total Environ. 2020; 728 [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Zhou P., et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. 2020; 579 (7798):270–273. [ PMC free article ] [ PubMed ] [ Google Scholar ]
Help | Advanced Search
Quantitative Biology > Populations and Evolution
Important: e-prints posted on arXiv are not peer-reviewed by arXiv; they should not be relied upon without context to guide clinical practice or health-related behavior and should not be reported in news media as established information without consulting multiple experts in the field.
Title: Optimal epidemic control by social distancing and vaccination of an infection structured by time since infection: the covid-19 case study
Abstract: Motivated by the issue of COVID-19 mitigation, in this work we tackle the general problem of optimally controlling an epidemic outbreak of a communicable disease structured by time since exposure, by the aid of two types of control instruments namely, social distancing and vaccination by a vaccine at least partly effective in protecting from infection. Effective vaccines are assumed to be made available only in a subsequent period of the epidemic so that - in the first period - epidemic control only relies on social distancing, as it happened for the COVID-19 pandemic. By our analyses, we could prove the existence of (at least) one optimal control pair, we derived first-order necessary conditions for optimality, and proved some useful properties of such optimal solutions. A worked example provides a number of further insights on the relationships between key control and epidemic parameters.
Submission history
Access paper:.
- HTML (experimental)
- Other Formats
References & Citations
- Google Scholar
- Semantic Scholar
BibTeX formatted citation
Bibliographic and Citation Tools
Code, data and media associated with this article, recommenders and search tools.
- Institution
arXivLabs: experimental projects with community collaborators
arXivLabs is a framework that allows collaborators to develop and share new arXiv features directly on our website.
Both individuals and organizations that work with arXivLabs have embraced and accepted our values of openness, community, excellence, and user data privacy. arXiv is committed to these values and only works with partners that adhere to them.
Have an idea for a project that will add value for arXiv's community? Learn more about arXivLabs .

Login | Register
- Current Issues
- Previous Issues
- Editorial Team
- Managerial Board
- Become a Reviewer
- Submission Guidelines
- Harvard Citation Style
- Vancouver Citation Style
- APA Citation Style
- Download RIS
- Download BibTeX
Multistakeholder Participation, Collaboration, and Networking in Disaster Risk Reduction and Pandemic Management: Insights and Future Policy Framework
- Sigamani Panneer (Jawaharlal Nehru University)
- Subhabrata Dutta (Assam University)
- Lekha D Bhat (Central University of Tamil Nadu)
- Prakash Chand Kandpal (Jawaharlal Nehru University)
- Robert Ramesh Babu P (Department of Social Work)
- Rubavel M (Consultant UNDP)
- Vigneshwaran Subbiah Akkayasamy (Department of Sociology and Social Work)
The natural and manmade disasters impact a society with loss of assets and human lives. Disasters leavepeople in vulnerable conditions and an overall economic slowdown is observed. The impact of disasters is highly complex and multidimensional in nature. It becomes imperative to handle the complexity of issues with comprehensive approach. Managing disasters effectively is one of the important challenges any government faces when it tries to be prepared with appropriate mitigation, rescue, and relief strategies. The unexpected nature and urgency related to Disaster Risk Reduction makes it important and relevant to involvemultistakeholders. This will help to bring down the severity and impact of the disaster on human lives and losses. Disaster Risk Reductionrequires meticulous planning and sharing of the responsibility among multistakeholders through networking so as to bring down the severity and minimize the negative impact of a disaster. Many research studies have suggested the multistakeholder approach in addressing the disasters. There are several gaps such as inefficiency of vertical management to deal the issues, involvement of multiple stakeholders, and lack of local public supportfor disaster. This paper, considering the case of COVID-19 as a pandemic and disaster, discusses the importance of multistakeholder participation. The paper presents an extensive review of the papers on the relevance ofparticipation of multistakeholdersin Disaster Risk Reduction and explores the scope and challenges involved and suggests policies to address the disasters, which utilizes Multistakeholder Participation.
Keywords: global health diplomacy, governance, collaboration andnetworking, disaster risk reduction, multistakeholder participation, transdisciplinary approach
Panneer, S., Dutta, S., Bhat, L. D., Kandpal, P. C., Babu P, R. R., M, R. & Akkayasamy, V. S., (2024) “Multistakeholder Participation, Collaboration, and Networking in Disaster Risk Reduction and Pandemic Management: Insights and Future Policy Framework”, Social Development Issues 46(2): 11. doi: https://doi.org/10.3998/sdi.5989
Downloads: Download XML Download PDF
1 Downloads
Published on 17 may 2024, peer reviewed, creative commons attribution 4.0, introduction.
Disasters cause not only economic crisis but also humanitarian loss, mental and psychological trauma, and slow downof a society’s development process. Disasters are to be handled with priority and to be addressed comprehensively with innovative and pragmaticmultistakeholder participation approach. In multistakeholder participation, to address disasters most effectively, sharing of information, coordination, and quick decision are most important ( Hayne & Smith, 2005 ). The terms “Multistakeholder platform” and “multistakeholder’s participation”are used to represent the process where different actors witha common pool of resources and common interests come together, discuss the possibilities, and develop proactive and pragmatic solutions for the good of the public ( Warner, Waalewijn, & Hilhorst, 2002 ). The past experiences in disaster risk reduction show that even after efforts, the affected society takes a long timeto cope with the aftermath of disasters because multistakeholder participation is not channelized properly in mitigation and rehabilitation efforts ( Fletcher et al., 2013 ). The COVID-19 pandemic serves as a prime example of global health crisis and the importance of networking, collaboration, and multistakeholder participation in handling disasters. The complexity of handling pandemics and disasters has increased recently, necessitating a more coordinated, inclusive strategy that makes use of a variety of resources and areas of expertise.
After a disaster occurs, a number of key stakeholders are involved in providing relief and rehabilitation support. One of the major challenges in the field of Disaster Risk Reductionis to understand how to develop a response with appropriate coordination between various stakeholders and ensure flexibility and lucidity in the system at the same time ( Nowell, Steelman, Velez, & Yang, 2018 ). During the last two decades, disasters are all transboundary in nature and uncertain, and collective stress is very high which demands rapid responses from multiple agencies or stakeholders ( Ansell, Boin, & Keller, 2010 ). Disasters bring constraints such as hierarchical organizations tend to break down, personnels are hindered by lack of information, lack of flexibility in the administrative procedures, constraints for innovation, and inability to shift resources and actions to meet the new demands quickly, which lead to cumulative stress in the Disaster Risk Reduction ( McDonald & Sinha, 2008 ). Multistakeholders are required to respond, network, and share the information to have strategic, tactical, and operational plans to handle the disasters. Optimal use of available time is one of the crucial aspects in the disaster risk reduction; timely information is required, and it depicts the need for collaboration with involvement of multistakeholders at wider level. A better multistakeholder management can improve the effectiveness and efficiency of Disaster Risk Reduction in humanitarian operations.
The stakeholders involved in disaster management include military and paramilitary forces, contributors, and government and nongovernment organizations, who have to cooperate and collaborate with people from different cultures and ethnic groups ( Cozzolino, 2012 ). Availability of scientific knowledge and appropriate information is mandatory for decision-making, clear assessment, and formulation of appropriate measures ( Zhou et al., 2020 ). Making policy decisions by providing inputs and delegating responsibilities among themselves to develop proactive prevention strategies with the involvement of community are imperative ( Biekart & Fowler, 2018 ). During a disaster, no individual, agency, or government machinery have the legitimacy, authority, or professional competency to handle the situation exclusively; it demands collective action, interaction, and networking ( Nolte & Boenigk, 2013 ). Effective response to a disaster is about networking and enterprising ( Moynihan, 2008 ). Multistakeholder participation has always helped to improve societal ownership and response of the Disaster Risk Reductionor rehabilitation measures. Multistakeholder initiatives are helpful in bringing in collective actions for public benefits; and as theyrely on one common factor, they are more productive, efficient, and effective ( Beisheim & Simon, 2016 ).
Stakeholders are classified into three groups: primary, secondary, and key stakeholders. Key stakeholders are mainly responsible for policy decision and are involved directly. Primary and secondary stakeholders have interest in the program but are not directly involved ( Freeman, Harrison, Wicks, Parmar, & De Colle, 2010 ). The process aims to bring all the stakeholders together, based on recognition to the concept of equity and accountability. The participation process involving multistakeholdersis democratic in nature, following the principles of transparency and participation. This ideally develops partnership and strengthen the networks among them, and thus disaster relief and management becomeefficient and effective ( Hemmati, 2012 ). Multistakeholder participation improves capacity-building, ensures innovation, and promotes faster decision-making process, which ultimately benefits the community ( Achyar, Schmidt-Vogt, & Shivakoti, 2015 ).
There are studies that show the success and relevance of multistakeholder participation in Disaster Risk Reduction. In the case of Hudhud cyclone in Vishakapattanam, multistakeholder participation under the leadership of the State Government has shown a positive impact in terms of rehabilitation and bringing back the normalcy ( Meduri, 2016 ). The study from Indonesia showed that multistakeholder participation and collaboration, as a crucial and important factor, has helped reduce the disaster risk and helped implement balanced Disaster Risk Reduction policies ( Trimurti, Endang, Hardi, & Hartuti, 2020 ). Hui (Hu, Lei, Hu, Zhang, Kavan, 2018) analyzed the situation in China and pointed out that the failure of government networks and its inefficiency of disaster relief measures are due to the lack of multistakeholder collaboration and internal dynamics of the system.
Global health Governance during COVID-19 pandemic was crucial; however, what the world witnessed was that the nations adopted uncoordinated, ad hoc responses partially adhering to the WHO guidelines ( Jones & Hameiri, 2022 ). International organizationssuch as the WHO was tasked with developing and disseminating “best practice” policies, whereas different nations adopted it with a lot of flexibility and their own suitability and adaptability. An overall coordination between nations was largely not observed ( Taylor & Habibi 2020 ). In this paper, we have reviewedthe available literature and identified the role of multistakeholder participation, coordination, and networking in handling disasters (with special focus on COVID-19 pandemic) in an effective manner. As the world is expecting more zoonotic diseases, developing effective strategies for Disaster Risk Reduction of infectious pandemics is very crucial.
COVID-19 Pandemic and the Role of Multi-stakeholders
The pandemic has left a deep impact on the global economy wherein the Gross Domestic Production (GDP) of the countries sharply decreased, and this slowing down of the economies has led to various livelihood issues. The COVID-19 pandemic not only has disturbed the social lives and financial status but also has affected the health and wellbeing ( Jha & Pankaj, 2021 ). International community and various stakeholders have taken steps to provide immediate relief, rehabilitation, and reconstruction. The traditional models orapproaches of coordination are inadequate for volatile and dynamic situations like that of pandemics, floods, and disasters ( Faraj & Xiao, 2006 ). COVID-19 has showed the contingent, fragile nature of global governance institutions, as well as the limitations of power and authority in the face of large-scale crises ( Levy, 2021 ). Multistakeholder collaboration is an important key to handle issues developed by disasters as it reduces the pressure on the government machinery and enhances the effectiveness of relief and rehabilitation.
Multistakeholder partnership in health emergency response situations tends to be futile when concerns about the ownership of outcomes and differences in organizational working practices amalgamate ( Ryu & Johansen, 2017 ). If the collaborative efforts or partners have transparency about the roles and responsibilities, then the public health emergency can be handled more effectively within a short duration ( de Vries et al., 2019 ). When multistakeholder participation is attempted in addressing earlier pandemics in the Asian region, issues such as resource limitation, unethical priority setting, and less confidence in the adopted surveillance technology inhibited effective pandemic preparedness ( Bennett & Carney, 2011 ). Major issues identified in multistakeholder collaboration in health preparedness include the partners’ lack of commitment, non-supportive collaborative work environment, absence of clarity about mutual expectations, informal interactive style of communication, and limited resource commitment over a longer period of time ( Akenroye et al., 2022 ).
It is important to involve multistakeholders before the occurrence of disaster as a preparatory work. Better preparatory works reduce the impactof severity of the pandemics. The preparatory work requires multilevel coordination, collection of information, and appropriate coordination mechanism among stakeholders in the pandemic situation. Hence, there is a need to develop flexible multistakeholder coordination mechanisms that can be easily customized for a specific situation and provide better support for improvised responses ( Janssen, Lee, Bharosa, & Cresswell, 2010 ). Domestic support alone is not sufficient;a collective action isrequired to handle the situation which mainly involves international support, international law, and geopolitics. It reiterates the need to have global partnerships with multilateral and bilateral agencies, media, research institutions, civil society organization (CSOs), religious and cultural groups, and nongovernmental organizations (NGOs). It is important to work on for international cohesion, coordination in disaster response, leveraging the technologies for mitigation, and management of multihazard risks and vulnerability. The multistakeholder platform is helpful mainly to create a space for the empowerment and active participation of common stakeholders intending to search for solutions to a common problem.
It is important to facilitate multistakeholder participation, preparatory activities, clinical intervention, and public health ( Faysse, 2006 ). Multistakeholders should be involved in the policy formulation and implementation to address the complex Disaster Risk Reduction issues. The participatory approaches must be adopted in planning, preparing action plans, training personnels, identifying problems and correcting mistakes, and implementation.
Objectives and Methods
The recent case of COVID-19 provides an example at world level to explore the relevance of multistakeholder participation in the preparedness and response for addressing the pandemic. The paper focuses on the following objectives: (1) to highlight the relevance of multistakeholders in Disaster Risk Reduction, including COVID-19 preparedness and response; (2) to document the issues and challenges in collaboration, networking for timely intervention in health Disaster Risk Reduction including COVID-19; and (3) to provide suggestions to enhance multistakeholder participation in most infectious and reemerging diseases outbreak management. In order to better understand the dynamics of multistakeholder participation in disaster risk reduction, this paper specifically looks at the lessons that may be drawn from the COVID-19 pandemic.
Review Methods
This paper conducts an extensive review, employing a broad and inclusive approach to literature analysis. Key terms such as “Disaster Risk Reduction,” “multistakeholders,” “pandemic,” “transdisciplinary research,” “networking,” and “COVID-19” were used to guide the search across databases including Google Scholar, JSTOR, BMC, Springer, JAMA, Scopus, JPHP, Elsevier, Lancet, PLOS ONE, MDPI Journals, Nature, APA, WHO Documents, Government Policy Documents, and PubMed. The search, from January 2020 to October 2022, aimed to capture a diverse array of sources reflecting the multifaceted nature of multistakeholder participation in disaster risk reduction, with a particular focus on the COVID-19 pandemic. Selected materials included peer-reviewed publications, journal articles, reviews, meta-analyses, disaster mitigation reports, feedback reports, reference books, strategic preparedness, and response plans. Prioritizing English language literature, this review emphasizes empirical studies, reviews, meta-analyses, and policy documents, ensuring a comprehensive understanding of the subject matter.
Multi stakeholder Participation in Disaster Risk Reduction and its Challenges
The international communityshares the responsibilities to provide immediate relief, rehabilitation, and reconstruction, providing health services, including water, sanitation, food, shelter, appropriate medical care, and helping in the livelihood sustainability of the affected population. However, issues of the victims especially related tolivelihood and health continues to be a big challenge. The victims also require psycho-social help, economic reconstruction, and opportunities for livelihood rebuilding. In a post-disaster scenario, the preparatory work requires multilevel coordination, collection of information, and the appropriate coordination mechanism among the stakeholders ( Jillson et al., 2019 ). Therefore, there is a need to develop flexible and multistakeholder networking mechanisms that can easily be customized for the specific situation and provide better support for improvised responses. It highlights the need to have global partnerships with multilateral and bilateral agencies, media, research institutions, CSOs, religious groups, and NGOs. It is important to work for international cohesion, coordination for the disaster response, leveraging the technically viable and economically feasible technologies for mitigation and management of multihazard risk and vulnerability ( Satapathy & Walia, 2007 ). The multistakeholder platform is mainly helpful in creating a space for the empowerment and active participation of common stakeholders intending to search for solutions to a common problem ( Obeng, Marfo, Owusu-Ansah, & Nantwi, 2014 ). It is important to facilitate the multistakeholder participation in preparatory activities, clinical intervention, and public health. Multistakeholders should be involved in policy formulation and implementation to address the complex disaster risk reduction issues. In this review, we have identified some of the important barriers and challenges which are presented in Table 1 .
Challenges and barriers to successful collaboration among multistakeholders
Source : The above data is collected by the authors from different sources.
A Case of COVID-19 Pandemic Management
As per data from the World Health Organization (WHO) as on December 14, 2023, COVID-19 infected cases were 773 million and total reported deaths were 6.98 million. The pandemic which affected the whole world has left deep impact on societies andhas led to heavy economic standstill and losses. One of the strategies to combat the pandemic is to minimize social and economic hardship through multisectoral partnerships (WHO Coronavirus [COVID-19] Dashboard, 2023). The Novel Corona Virus Strategic Preparedness and Responsive Plan released on February 03, 2020 emphasized on the aspectwherein the WHO highlighted the need to encourage networking and multistakeholder participation at all levels, sharing the resources, expertise, and skills.
Based on the intensity of the pandemic, the number of players involved in the preparedness and operation vary. Thispredominantly involvehealthcare providers and administrators, experts, logistics organizations, government and NGOs, communities in the villages, and ethnic groups ( Cozzolino, 2012 ). Many countries carried outexercises to identify the gaps and problems involved in adopting an efficient swift response strategy to address the pandemic aftermath. For example, India, in its preparedness to combat COVID-19, conducted the civil servants feedback survey wherein ten majorgaps wereidentified, which were as follows: (1) hospital preparedness and infrastructure; (2) quarantine and isolation facility; (3) testing facilities; (4) personal protection equipment; (5) lack of public awareness; (6) law and order administration (State/District); (7) foreign travel history and contact tracing; (8) temporary and wage-worker exodus; (9) sanitizing public places; and (10) essential goods and services. (The National preparedness Survey on COVID-19 conducted by the Department of Administrative Reforms and Public Grievances, Government of India [GOI, 2020]). The survey also acknowledged that all the above-mentioned requirements cannot be arranged and coordinated solely by the government system and it called for multistakeholder collaboration, various actors’ role in the restoration, rehabilitation, and reconstruction of the pandemic-affected areas.
Pandemic: Response, Recovery, and Mitigation Experiences
A few countries including South Korea and New Zealand have taken timely efforts to address the pandemic management. In other countries such as Italy, Sweden, France, the UK, and the USA, a strict quarantine mechanism was not enforced during the initial period of COVID-19, whichresulted inthe quick spread of the virus. In India, the Government started intensifying preparedness for the unprecedented threat posed by COVID-19, where it constituted an interministerial committee represented by the ministers of the health and family welfare, civil aviation, external affairs, and home, as well as the National Disaster Management Authority ( Dikid et al., 2020 ). However, no private institutions ororganizationswere involved in preparedness of the pandemic at this early stage. The only decision in the direction where multistakeholderswere engagedwas the attempt made to include the village-level communities. The Panchayat-level governments through the GramSabhastried toconductawareness drives on the clinical presentation of the novel COVID-19 disease, its preventive measures, and the need for reporting the cases especially in the village areas. Much of the technical support was made available by the epidemic intelligence service by the NCDC in collaboration with the US Centers for Disease Control and Prevention (CDC). This was one the important aspects of leveraging technical resource for addressing the COVID-19, and it activelysupported the COVID-19 response. This helped India mobilize external support to update the disease surveillance systems; investigate outbreaks; respond to disasters, emergencies, and mass gatherings; and conduct epidemiological evaluations. This intervention hada great potential in strengthening the epidemiological capacity of health professionals in the country to respond efficiently to public health emergencies such as strengthening core capacity in the areas of disease surveillance, early detection, and rapid response, generating evidence that could be used for policymaking and implementation.
It is suggested to have strong national surveillance to detect COVID-19 cases and other similar future epidemics, respond to active case findings, prompt treatment and isolation of cases, contact tracing, and preventing an outbreak from happening or limiting its spread to the public by taking containment measures. The Corporate Social Responsibility components of profitable companies can play major role as they have already developed rapport and confidence in village communities ( Patuelli, Caldarelli, Lattanzi, & Saracco, 2021 ). The involvement of multistakeholders such as private organizations, technocrats, international agencies, and community members to address the COVID-19 pandemic will ensure more efficiency and effectiveness ( Jiang, 2020 ).
Cooperation and understanding between the Federal (Central) and State governments are also important ( Ghosh, Nundy, & Mallick, 2020 ). It is important that the National Pandemic Preparedness Plan (NPPP) and State Pandemic Preparedness Plan (SPPP) should be coordinated, collaborated, and integrated at an appropriate level to ensure efficiency A rich technical expertise available with a large number of research and academic institutions must be identified and utilized ( Babbar & Gupta, 2022 ). The pharmaceutical industry should beengaged for the promotion of Research and Development in the production of local technology-driven solutions including door-step diagnostics, drugs and vaccines, and as well as the innovative use of information and communication technologies for data collection and analyses (Ayati, Malik, Raees, & Anwar, 2020). COVID-19 has brought untold misery to a large section of low-income strata and to ensure the sustainability of the livelihood and restore normalcy in post-COVID-19 era, collaboration between local self-governments, civil societies, and NGOs is crucial to ensure maximum community participation ( Raychaudhuri, 2020 ).
The involvement of private research organizations, efficient utilization of medical infrastructure, and availability of technical support from both national and global experts are important to adopt and upgrade combat strategy over a period of time. Enhancing the capacities of health workers and mental health institutions to deal with the mental health of patients and quarantine population is also a priority area ( Wosik et al., 2020 ). The pandemic response requires integrated proactive measures and capacities that involve all sectors and professionals from various fields. It is important to secure, coordinate, and involve interested institutions and stakeholders to enhance the effectiveness of COVID-19 combat strategy ( Ballard et al., 2020 ).
The greatest challenge in managing a disaster like thisis arranging and deploying all the necessary resources, reaching the disaster site in minimum possible time, and helping the areas begin the recovery process ( Day, Melnyk, Larson, Davis, & Whybark, 2012 ). Early intervention, decision-making, and on-time deliveryof services are key for addressing pandemics like COVID-19. All these together demand for proactive leadership, proper planning, and involving multistakeholders to control and eliminate COVID-19-like pandemicsin the future ( Holmes et al., 2020 ). A plan of action developed with the involvement of all the stakeholders and executed meticulously would definitely help the communities to face the pandemic complexities. Engaging with the existing health and community-based networks, media, local NGOs, self-help groups, schools, colleges, universities, local governments and other sectors, such as healthcare service providers, education sector, business, travel and food or agriculture sectors, using a consistent mechanism of communication is very important to develop a long-term financially viable, effective strategy and a set of positive interventions (WHO, 2020). The possibilities of IT-based technology, telecommunications, mobile technology, and social media platforms also need to be explored and integrated to the strategy ( He, Zhang, & Li, 2021 ).
Best Practices for Managing the COVID-19 Pandemic
To effectively manage the pandemic and lessen its effects, multiple best practices have been identified. The significance of transparency, efficiency, and equity in pandemic response efforts has been demonstrated by the adoption of these best practices in both high-, low-, and middle-income countries. This underscores the importance of these principles in effectively managing the pandemic and minimizing its impact on healthcare systems and populations. Understanding the execution and implementation of these best practices is crucial to address such pandemics successfully in the future.
Pandemic management demands a multifaceted approach to effectively respond to the global threat. Clear communication is one of the best practices that must be employed for an effective pandemic response. This involves providing accurate, timely, and easily understandable information to the public to reduce fear and confusion, encourage adherence to public health guidelines, and foster trust in healthcare officials. This involves providing timely and transparent updates about the pandemic and involving stakeholders in decision-making processes ( El-Jardali, Bou-Karroum, & Fadlallah, 2020 ). For instance, in the United States, the Centers for Disease Control and Prevention (CDC) offered daily updates on the pandemic and held regular briefings to ensure that all stakeholders were well-informed and engaged in response efforts (CDC, 2020).
Another effective approach is to collaborate with various sectors and stakeholders, such as governments, healthcare providers, and businesses, to leverage their resources and expertise. By doing so, it can guarantee the equitable distribution of essential resources such as personal protective equipment (PPE) and medical equipment, and promote well-coordinated response efforts. Rwanda’s national COVID-19 Task Force devised a thorough plan that encompassed managing the pandemic, procuring and distributing PPE and medical equipment, and engaging and educating the community ( Dzinamarira, Mapingure, Rwibasira, Mukwenha, & Musuka, 2022 ).
In managing a pandemic, it is crucial to prioritize equity and inclusivity by acknowledging the distinct requirements and viewpoints of marginalized groups like low-income individuals, racial and ethnic minorities, and people with disabilities. This involves addressing the fundamental social factors that influence health outcomes. Brazil’s COVID-19 national Task Force has taken this approach by incorporating members from indigenous communities, who are at higher risk of contracting the virus due to inadequate healthcare and sanitation facilities. To safeguard and assist these communities, the Task Force has created a strategy that involves specialized measures ( Flores-Ramírez et al., 2021 ).
In managing a pandemic, adopting data-driven techniques is vital. This entails leveraging data and technology to track the transmission of the virus, detect high-risk areas, and implement appropriate interventions. South Korea employed a thorough data-driven strategy for contact tracing and testing, which was instrumental in containing the spread of virus during the early stages of the pandemic ( Ferretti et al., 2020 ).
Strengthening healthcare systems is a critical aspect of managing the COVID-19 pandemic. Healthcare systems must have the capacity to respond to the pandemic and maintain essential health services. In Kenya, a COVID-19 response plan was developed that included measures to ensure that healthcare workers had access to PPE and training and that health facilities had the necessary resources to manage COVID-19 cases while maintaining other essential health services. This approach allowed Kenya to effectively manage the pandemic and limit its impact on its healthcare system and population ( Wangari et al., 2021 ). Table 2 presents a summary of the best practices in managing the COVID-19 pandemic. Efficient management of COVID-19-like pandemic demands a well-coordinated approach among multiple sectors and stakeholders. The best practices described, which consist of clear communication, coordinated resource allocation, prioritizing equity and inclusivity, data-driven techniques, and reinforcing healthcare systems, have been derived from both high-, low-, and middle-income nations. These practices underscore the significance of openness, effectiveness, and fairness in responding to pandemics.
Best practices for COVID-19 pandemic management
Issues and Challenges in Management of COVID-19
Most profound and consequential impact of COVID-19 was on physical and mental health, well-being, and livelihood of common people ( Wang et al., 2021 ). COVID-19 has posed a new set of unforeseen challenges because all the sectors have been affected with severe job and profit loss, fall in production, and restricted or no migration or international movements ( Paul et al., 2021 ). During the course of the pandemic, it was observed that the cases increased exponentially, the healthcare system reached the optimal operating capacity, and the patientsdid not get adequate medical care. This pattern of pandemic spread was observed even in most of the developed countries ( Kringos et al., 2020 ).
Following COVID-19, it is necessary to adopt focused and sector-wide approaches to restore lives to normalcy and get the country’s economy back on a growth trajectory. ( Le et al., 2020 ). It is important to assess the severity or magnitude of effects with appropriate long-term research and interventions in which people’s participation is ensured. The challenge is to integrate the approaches of vertical management into horizontal management to involve multistakeholders to work on the needs such as new technologies, flexibility, and innovation in addressing the COVID-19 by deploying all the necessary resources ( Panneer et al., 2021 ). The maintenance of effective coordination between different stakeholders to fulfill the demand is very important ( Janssen et al., 2010 ). There is need to increase humanitarian logistics service, neutrality, and impartiality to COVID-19 healthcare and livelihood-related issues ( Tomasini & Van Wassenhove, 2009 ). The political leadership plays a major role in identification of issues, and proactive politicalleadership is required to ensure participatory, goal-oriented decision-making ( Grint, 2020 ). The major challenges faced by multistakeholder approach include implementing an efficient, dynamic, proactive leadership that shapes such processes or decisions, organize stakeholder groups; and the lack of financial or technical capacities to implement multistakeholder platforms ( Djalante, 2012 ). Table 3 presents a summary of the Post-COVID-19 crisis management and strategies.
Post-COVID-19 crisis management and strategies
Suggestions and policy framework
Having successfully combated and controlled COVID-19, the next task is to restore livelihood options because most of the people have been badly affected by the pandemic. This is essential tobring the country’s economy back to the growth trajectory. For this, long- and short-term planning and interventions are required. The multistakeholder involvement, cooperation, and collaboration are key to address these areas effectively and efficiently within the shortest possible period of time ( Memish et al., 2020 ). We propose the following broad guidelines for different stakeholders to effectively develop and deploy multistakeholder participation and networking in controlling the pandemic.
Government (Federal and State governments)
The Government must arrange for the necessary first-line health infrastructure and sufficient medical care facilities along with deployment of healthcare professionals, mental health professionals, development planners, and humanitarian relief workers ( Edwards & Ott, 2021 ). The understanding and mutual respect between different sectors or departments and sufficient dialog between different actors is required ( Sharma, Borah, & Moses, 2021 ). The Government must bring together and coordinate between clinical and social scientists, government and NGOs, affected persons, and experts from other relevant fields ( Twigg, 2001 ). The Government has to promote participation, coordination, and cooperation among the multistakeholders, so that alldimensions related to the pandemic are addressed appropriately. Evidence-based interventions and policies must be given priority; the advisories and guidelines charted out by expert groups such as the WHO must be given adequate importance in the strategy planning or implementation ( Ullah, Pinglu, Ullah, Abbas, & Khan, 2021 ). There must be adequate fund allocation for developing networks and partnerships. The government must facilitate the involvement of the community members to manage the risks and thus promote adoption of locally appropriate solutions ( Carrasco, Ochiai, & Okazaki, 2016 ). Promoting evidence-based approaches would bring effective outcome, and multistakeholder platform will help achieve clear linkages between institutions, agreements, clear targets, accountability, and mechanisms of evaluation ( Bäckstrand, 2006 ). Promoting the usage of e-governance and e-reporting system is also crucial to increase coverage and efficiency of the pandemic combat system ( Hua & Shaw, 2020 ). The promotion of public–private partnership for developing innovative solutions either to control COVID-19 or to promote livelihood in COVID-19 is also an important task for the Government ( Kudtarkar, 2020 ). Developing and maintaining repositories is also the responsibility of government for which partnership with IT sector companies can be of much use ( Budd et al., 2020 ).
Civil Society Organizations (CSO)
This comprises different organizations, including international aid agencies who work in the humanitarian service area. International aid agencies will be able to bring in the required technical expertise and international funds, whereas the local civil society organizations can take part in the ground-level preparedness, combat interventions related to COVID-19 ( Fry, Cai, Zhang, & Wagner, 2020 ). There is need to develop the knowledge and do capacity-building for taking up activities of emergency relief operations, and COVID-19 combat work, so that the sector can contribute to tackle COVID-19 situations ( Mohseni, Azami-Aghdash, Mousavi Isfahani, Moosavi, & Fardid, 2021 ). Apart from COVID-19 containment, these NGOs will also be having expertise and experience in dealing with mental health issues and provide appropriate care to the affected ( Anand, Verma, Aggarwal, Nanjundappa, & Rai, 2021 ).
Local community
Local communities play an important role in reducing risks related to pandemics such as COVID-19. Along with vulnerable communities, involvement and trust-building to combat against COVID-19 can be intensified ( Panigrahi, Majumdar, Galhotra, Kadle, & John, 2021 ). Local community knowledge and practices can be utilized; dissemination and local awareness methods like folk art can be used for propagating social distancing and personal hygiene etiquettes ( Marston, Renedo, & Miles, 2020 ). Community representatives may provide helpful insight on the local settings and act as main actors for dissemination information and as a primary communication or liaison link between the project officials, targeted communities, and their established networks ( Li, Tan, Wu, & Gao, 2020 ). Legitimacy of the community representatives can be verified by talking informally to a random group of community members and heeding their views on who can be representing their interests in the most effective way. When the legitimate leaders who have high acceptance in the community are involved, the community’s overall involvement and cooperation improves, which ultimately helps tackle the pandemic-related issues ( Canals Lambarri, 2020 ).
Other stakeholders
Governments, Civil Society Organizations, communities, self-help groups, and other stakeholders, including other professionals and personnel, can perform through the suggested model as mentioned in Figure 1 , where at the center there will be Local NGOs and Local Self Governments (Municipalities or Panchayats), to effectively contain COVID-19. Scientists, volunteers, philanthropists, social workers, doctors, psychologists, development and emergency planners, and humanitarian relief workers must be involved in good faith and trust ( Moradian et al., 2020 ). Their professional training, resources, skills, and expertise can be utilized to provide effective and efficient services related to COVID-19 control. Public health workforce development will be supported to ensure that a complete spectrum of expertise is covered including epidemiologists, data managers, laboratory technicians, emergency management and risk communications specialists, and public health managers ( Lavazza & Farina, 2020 ). The services and expertise of other partners such as Red Cross humanitarian workers, National Service Scheme volunteers, National Cadet Corps, and police officials, charitable organizations, private and public sector companies, traditional media (television, radio, and print media), participants of social media, politicians or elected representatives, other national and international health organizations and NGOs, local businesses with international links, and the public at large other ministries (Environment, Finance, External Affairs, Home, etc.) can also contribute effectively ( Anwar, Malik, Raees, & Anwar, 2020 ).

The review emphasizes how crucial the role of multistakeholder cooperation is in lessening the effects of pandemics and disasters. It illustrates how varied collaborations can result in more adaptable and successful solutions. In order to ensure that lessons from recent experiences like COVID-19 are incorporated into future disaster risk reduction efforts, the study looks ahead and calls for a persistent focus on novel and inclusive techniques for stakeholder participation. Disaster Risk Reduction including pandemics needs transformative approaches, systems, strategy, and new technologies, which are to be adopted with flexibility and innovation. The approaches have to be changed from single-direction approach to a comprehensive approach. There need to be a change from the traditional system of administration to a modern citizen-centric management system with networking and collaboration by engaging multistakeholders and contributors. It is important to facilitate the collaboration of multiple stakeholders to create synergy to manage risks for effective disaster risk reduction. This in turn also brings resources into a system such as new innovative ideas, experience, skills and competency, technology, and professionalism. It is important to partner with global-level multistakeholders of multilateral or bilateral agencies and look for opportunities to promote public–private partnership to develop appropriate Disaster Risk Reduction strategies and resilience plans. The disaster intervention should focus on evidence-based interventions and approaches to bring better outcome of mitigation, rescue, relief, and rehabilitation. The COVID-19pandemic has taught a lesson that networking and collaboration are significant for the effective governance of COVID-like pandemics in the near future, where the role of the multistakeholders, local, public, and community civil society groups, and public–private partnership is inevitable.
Conflicts of Interest
The authors declare that there are no conflicts of interest to disclose. All authors have read and agreed to this version of the manuscript.
Authors’ Contributions
SP contributed to the conceptualization of the article. SP, LB, and RRP contributed to the methodology. The data analysis synthesis wasdone by SP, SD, LB, and RRP. The writing and preparation of original draft was done by SP, SD, RM, LB, RRP, and VSA. SP, SD, LB, PCK, RRP, and VSA contributed to the review and editing of the manuscript. The visualization and supervision was performed by SP, SD, and LB.
This research received no external funding.
Achyar, E., Schmidt-Vogt, D., & Shivakoti, G. P. (2015). Dynamics of the multi-stakeholder forum and its effectiveness in promoting sustainable forest fire management practices in South Sumatra, Indonesia. Environmental Development , 13, 4–17. https://doi.org/10.1016/j.envdev.2014.11.002 https://doi.org/10.1016/j.envdev.2014.11.002
Akenroye, T. O., Abubakre, A., Elbaz, J., Vishnu, C. R., Beka Be Nguema, J.-N., Rana, G., … Falode, O. (2022). Modeling the barriers to multistakeholder collaboration for COVID-19 pandemic response: Evidence from Sub-Saharan Africa. International Public Management Journal , 25(2), 192–216. https://doi.org/10.1080/10967494.2021.1970061 https://doi.org/10.1080/10967494.2021.1970061
Anand, V., Verma, L., Aggarwal, A., Nanjundappa, P., & Rai, H. (2021). COVID-19 and psychological distress: Lessons for India. PLoS One , 16(8), e0255683. https://doi.org/10.1371/journal.pone.0255683 https://doi.org/10.1371/journal.pone.0255683
Ansell, C., Boin, A., & Keller, A. (2010). Managing transboundary crises: Identifying the building blocks of an effective response system. Journal of Contingencies and Crisis Management , 18(4), 195–207. https://doi.org/10.1111/j.1468-5973.2010.00620.x https://doi.org/10.1111/j.1468-5973.2010.00620.x
Anwar, A., Malik, M., Raees, V., & Anwar, A. (2020). Role of mass media and public health communications in the COVID-19 pandemic. Cureus , 12(9), e10453. https://doi.org/10.7759/cureus.10453 https://doi.org/10.7759/cureus.10453
Ayati, N., Saiyarsarai, P., & Nikfar, S. (2020). Short and long-term impacts of COVID-19 on the pharmaceutical sector. DARU Journal of Pharmaceutical Sciences , 28(2), 799–805. https://doi.org/10.1007/s40199-020-00358-5 https://doi.org/10.1007/s40199-020-00358-5
Babbar, M., & Gupta, T. (2022). Response of educational institutions to COVID-19 pandemic: An inter-country comparison. Policy Futures in Education , 20(4), 469–491. https://doi.org/10.1177/14782103211021937 https://doi.org/10.1177/14782103211021937
Bäckstrand, K. (2006). Multi-stakeholder partnerships for sustainable development: Rethinking legitimacy, accountability and effectiveness. European Environment , 16(5), 290–306. https://doi.org/10.1002/eet.425 https://doi.org/10.1002/eet.425
Ballard, M., Bancroft, E., Nesbit, J., Johnson, A., Holeman, I., Foth, J., … Palazuelos, D. (2020). Prioritising the role of community health workers in the COVID-19 response. BMJ Global Health , 5(6), e002550. https://doi.org/10.1136/bmjgh-2020-002550 https://doi.org/10.1136/bmjgh-2020-002550
Beisheim, M., & Simon, N. (2016). Multi-stakeholder partnerships for implementing the 2030 Agenda: Improving accountability and transparency . Analytical Paper for the 2016 ECOSOC Partnership Forum.
Bennett, B., & Carney, T. (2011). Review paper: Pandemic preparedness in Asia: A role for law and ethics? Asia Pacific Journal of Public Health , 23(3), 419–430. https://doi.org/10.1177/1010539511408411 https://doi.org/10.1177/1010539511408411
Biekart, K., & Fowler, A. (2018). Ownership dynamics in local multi-stakeholder initiatives. Third World Quarterly , 39(9), 1692–1710. https://doi.org/10.1080/01436597.2018.1450139 https://doi.org/10.1080/01436597.2018.1450139
Budd, J., Miller, B. S., Manning, E. M., Lampos, V., Zhuang, M., Edelstein, M., … McKendry, R. A. (2020). Digital technologies in the public-health response to COVID-19. Nature Medicine , 26(8), 1183–1192. https://doi.org/10.1038/s41591-020-1011-4 https://doi.org/10.1038/s41591-020-1011-4
Canals Lambarri, M. (2020). Learning from the COVID-19 pandemic: Concepts for good decision-making. RevistaMédica de Chile , 148(3), 418–420. https://doi.org/10.4067/s0034-98872020000300418 https://doi.org/10.4067/s0034-98872020000300418
Carrasco, S., Ochiai, C., & Okazaki, K. (2016). Disaster induced resettlement: Multi-stakeholder interactions and decision making following tropical storm Washi in Cagayan de Oro, Philippines. Procedia - Social and Behavioral Sciences , 218, 35–49. https://doi.org/10.1016/j.sbspro.2016.04.008 https://doi.org/10.1016/j.sbspro.2016.04.008
Centers for Disease Control and Prevention (CDC). (2020). Coronavirus Disease 2019 (COVID-19) . Centers for Disease Control and Prevention. Retrieved from https://www.cdc.gov/coronavirus/2019-ncov/index.html https://www.cdc.gov/coronavirus/2019-ncov/index.html
Cozzolino, A. (2012). Humanitarian logistics and supply chain management. In A. Cozzolino (Ed.), Humanitarian logistics: Cross-sector cooperation in disaster relief management (pp. 5–16). Berlin Heidelberg: Springer. https://doi.org/10.1007/978-3-642-30186-5_2 https://doi.org/10.1007/978-3-642-30186-5_2
Crispo, A., Bimonte, S., Porciello, G., Forte, C. A., Cuomo, G., Montagnese, C., … Cuomo, A. (2021). Strategies to evaluate outcomes in long-COVID-19 and post-COVID survivors. Infectious Agents and Cancer , 16(1), 62. https://doi.org/10.1186/s13027-021-00401-3 https://doi.org/10.1186/s13027-021-00401-3
Cruz, P. L. (2014). Cross-border governance on the U.S.–Mexico border: Institutional challenges and developments in health collaboration. Regions and Cohesion , 4(1), 53–71. https://doi.org/10.3167/reco.2014.040104 https://doi.org/10.3167/reco.2014.040104
Day, J. M., Melnyk, S. A., Larson, P. D., Davis, E. W., & Whybark, D. C. (2012). Humanitarian and disaster relief supply chains: A matter of life and death. Journal of Supply Chain Management , 48(2), 21–36. https://doi.org/10.1111/j.1745-493X.2012.03267.x https://doi.org/10.1111/j.1745-493X.2012.03267.x
Dayour, F., Adongo, C. A., Amuquandoh, F. E., & Adam, I. (2021). Managing the COVID-19 crisis: Coping and post-recovery strategies for hospitality and tourism businesses in Ghana. Journal of Hospitality and Tourism Insights , 4(4), 373–392. https://doi.org/10.1108/JHTI-08-2020-0150 https://doi.org/10.1108/JHTI-08-2020-0150
de Vries, M., Kenis, P., Kraaij-Dirkzwager, M., Ruitenberg, E. J., Raab, J., & Timen, A. (2019). Collaborative emergency preparedness and response to cross-institutional outbreaks of multidrug-resistant organisms: A scenario-based approach in two regions of the Netherlands. BMC Public Health , 19(1), 52. https://doi.org/10.1186/s12889-018-6376-7 https://doi.org/10.1186/s12889-018-6376-7
Dikid, T., Chaudhary, S., Goel, K., Padda, P., Sahu, R., Kumar, T., … Narain, J. P. (2020). Responding to COVID-19 pandemic: Why a strong health system is required. The Indian Journal of Medical Research , 151(2–3), 140. https://doi.org/10.4103/ijmr.IJMR_761_20 https://doi.org/10.4103/ijmr.IJMR_761_20
Djalante, R. (2012). Adaptive governance and resilience: The role of multi-stakeholder platforms in disaster risk reduction. Natural Hazards and Earth System Sciences , 12(9), 2923–2942. https://doi.org/10.5194/nhess-12-2923-2012 https://doi.org/10.5194/nhess-12-2923-2012
Dunlop, A. L., Logue, K. M., Vaidyanathan, L., & Isakov, A. P. (2016). Facilitators and barriers for effective academic-community collaboration for disaster preparedness and response. Journal of Public Health Management and Practice , 22(3), E20–E28. https://doi.org/10.1097/PHH.0b013e3182205087 https://doi.org/10.1097/PHH.0b013e3182205087
Dzinamarira, T., Mapingure, M. P., Rwibasira, G. N., Mukwenha, S., & Musuka, G. (2022). COVID-19: Comparison of the response in Rwanda, South Africa and Zimbabwe. MEDICC Review , 23, 15–20. https://doi.org/10.37757/mr2021.v23.n3.4 https://doi.org/10.37757/mr2021.v23.n3.4
Edwards, F. L., & Ott, J. S. (2021). Governments’ responses to the COVID-19 pandemic. International Journal of Public Administration , 44(11–12), 879–884. https://doi.org/10.1080/01900692.2021.1936964 https://doi.org/10.1080/01900692.2021.1936964
El-Jardali, F., Bou-Karroum, L., & Fadlallah, R. (2020). Amplifying the role of knowledge translation platforms in the COVID-19 pandemic response. Health Research Policy and Systems , 18(1), 58. https://doi.org/10.1186/s12961-020-00576-y https://doi.org/10.1186/s12961-020-00576-y
Faraj, S., & Xiao, Y. (2006). Coordination in fast-response organizations. Management Science , 52(8), 1155–1169. https://doi.org/10.1287/mnsc.1060.0526 https://doi.org/10.1287/mnsc.1060.0526
Faysse, N. (2006). Troubles on the way: An analysis of the challenges faced by multi-stakeholder platforms. Natural Resources Forum , 30(3), 219–229. https://doi.org/10.1111/j.1477-8947.2006.00112.x https://doi.org/10.1111/j.1477-8947.2006.00112.x
Ferretti, L., Wymant, C., Kendall, M., Zhao, L., Nurtay, A., Abeler-Dörner, L., … Fraser, C. (2020). Quantifying SARS-CoV-2 transmission suggests epidemic control with digital contact tracing. Science , 368(6491), eabb6936. https://doi.org/10.1126/science.abb6936 https://doi.org/10.1126/science.abb6936
Fletcher, S. M., Thiessen, J., Gero, A., Rumsey, M., Kuruppu, N., & Willetts, J. (2013). Traditional coping strategies and disaster response: Examples from the South Pacific Region. Journal of Environmental and Public Health , 2013, 264503. https://doi.org/10.1155/2013/264503 https://doi.org/10.1155/2013/264503
Flores-Ramírez, R., Berumen-Rodríguez, A. A., Martínez-Castillo, M. A., Alcántara-Quintana, L. E., Díaz-Barriga, F., & Díaz de León-Martínez, L. (2021). A review of environmental risks and vulnerability factors of indigenous populations from Latin America and the Caribbean in the face of the COVID-19. Global Public Health , 16(7), 975–999. https://doi.org/10.1080/17441692.2021.1923777 https://doi.org/10.1080/17441692.2021.1923777
Freeman, R. E., Harrison, J. S., Wicks, A. C., Parmar, B. L., & De Colle, S. (2010). Stakeholder theory: The state of the art . Cambridge: Cambridge University Press. https://doi.org/10.1017/CBO9780511815768 https://doi.org/10.1017/CBO9780511815768
Fry, C. V., Cai, X., Zhang, Y., & Wagner, C. S. (2020). Consolidation in a crisis: Patterns of international collaboration in early COVID-19 research. PLoS One , 15(7), e0236307. https://doi.org/10.1371/journal.pone.0236307 https://doi.org/10.1371/journal.pone.0236307
Ghosh, A., Nundy, S., & Mallick, T. K. (2020). How India is dealing with COVID-19 pandemic. Sensors International , 1, 100021. https://doi.org/10.1016/j.sintl.2020.100021 https://doi.org/10.1016/j.sintl.2020.100021
Government of India (GOI). (2020). National Preparedness Survey on COVID-19: Responsesofdistrict collectors and IAS officers (2014–2018 batches) . G Department of Administrative Reforms and Public Grievances. Retrieved from https://darpg.gov.in/sites/default/files/COVID-19%20Impact%20Feedback%20Report.pdf https://darpg.gov.in/sites/default/files/COVID-19%20Impact%20Feedback%20Report.pdf
Grint, K. (2020). Leadership, management and command in the time of the Coronavirus. Leadership , 16(3), 314–319. https://doi.org/10.1177/1742715020922445 https://doi.org/10.1177/1742715020922445
Hayne, S. C., & Smith, C. A. P. (2005). The relationship between e-collaboration and cognition. International Journal of e-Collaboration (IJeC) , 1(3), 17–34. https://doi.org/10.4018/jec.2005070102 https://doi.org/10.4018/jec.2005070102
He, W., Zhang, Z. J., & Li, W. (2021). Information technology solutions, challenges, and suggestions for tackling the COVID-19 pandemic. International Journal of Information Management , 57, 102287. https://doi.org/10.1016/j.ijinfomgt.2020.102287 https://doi.org/10.1016/j.ijinfomgt.2020.102287
Hemmati, M. (2012). Multi-stakeholder processes for governance and sustainability: Beyond deadlock and conflict . New Delhi, India: Routledge. https://doi.org/10.4324/9781849772037 https://doi.org/10.4324/9781849772037
Holmes, E. A., O’Connor, R. C., Perry, V. H., Tracey, I., Wessely, S., Arseneault, L., … Bullmore, E. (2020). Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. The Lancet Psychiatry , 7(6), 547–560. https://doi.org/10.1016/S2215-0366(20)30168-1 https://doi.org/10.1016/S2215-0366(20)30168-1
Hu, H., Lei, T., Hu, J., Zhang, S., & Kavan, P. (2018). Disaster-mitigating and general innovative responses to climate disasters: Evidence from modern and historical China. International Journal of Disaster Risk Reduction , 28, 664–673. https://doi.org/10.1016/j.ijdrr.2018.01.022 https://doi.org/10.1016/j.ijdrr.2018.01.022
Hua, J., & Shaw, R. (2020). Corona virus (COVID-19) “Infodemic” and emerging issues through a data lens: The case of China. International Journal of Environmental Research and Public Health , 17(7), 2309. https://doi.org/10.3390/ijerph17072309 https://doi.org/10.3390/ijerph17072309
Janssen, M., Lee, J., Bharosa, N., & Cresswell, A. (2010). Advances in multi-agency disaster management: Key elements in disaster research. Information Systems Frontiers , 12(1), 1–7. https://doi.org/10.1007/s10796-009-9176-x https://doi.org/10.1007/s10796-009-9176-x
Jha, M. K., & Pankaj, A. K. (2021). Insecurity and fear travel as labour travels in the time of pandemic. In India’s migrant workers and the pandemic (pp. 177–190). New Delhi, India:Routledge. https://doi.org/10.4324/9781003246121-11 https://doi.org/10.4324/9781003246121-11
Jiang, Q. (2020). What small NGOs can deliver: A case study of a Canadian community-based project making fabric scrub caps for healthcare workers during the COVID-19 pandemic. International Social Work , 63(6), 851–856. https://doi.org/10.1177/0020872820959374 https://doi.org/10.1177/0020872820959374
Jillson, I. A., Clarke, M., Allen, C., Waller, S., Koehlmoos, T., Mumford, W., … Trant, A. (2019). Improving the science and evidence base of disaster response: A policy research study. BMC Health Services Research , 19(1), 274. https://doi.org/10.1186/s12913-019-4102-5 https://doi.org/10.1186/s12913-019-4102-5
Jones, L., & Hameiri, S. (2022). Explaining the failure of global health governance during COVID-19, International Affairs , 98(6), 2057–2076. https://doi.org/10.1093/ia/iiac231 https://doi.org/10.1093/ia/iiac231
Kringos, D., Carinci, F., Barbazza, E., Bos, V., Gilmore, K., Groene, O., … (2020). Managing COVID-19 within and across health systems: Why we need performance intelligence to coordinate a global response. Health Research Policy and Systems , 18(1), 80. https://doi.org/10.1186/s12961-020-00593-x https://doi.org/10.1186/s12961-020-00593-x
Kudtarkar, S. G. (2020). Resetting PPP in infrastructure model in India post-COVID-19 pandemic. The Indian Economic Journal , 68(3), 365–382. https://doi.org/10.1177/0019466220976678 https://doi.org/10.1177/0019466220976678
Lai, A. Y. (2012). Organizational collaborative capacity in fighting pandemic crises: A literature review from the public management perspective. Asia Pacific Journal of Public Health , 24(1), 7–20. https://doi.org/10.1177/1010539511429592 https://doi.org/10.1177/1010539511429592
Lavazza, A., & Farina, M. (2020). The role of experts in the Covid-19 pandemic and the limits of their epistemic authority in democracy. Frontiers in Public Health , 8, 356. https://doi.org/10.3389/fpubh.2020.00356 https://doi.org/10.3389/fpubh.2020.00356
Le, H. T., Mai, H. T., Pham, H. Q., Nguyen, C. T., Vu, G. T., Phung, D. T., … Ho, C. S. (2020). Feasibility of Intersectoral collaboration in epidemic preparedness and response at Grassroots levels in the threat of COVID-19 pandemic in Vietnam. Frontiers in Public Health , 8, 589437. https://doi.org//10.3389/fpubh.2020.589437 https://doi.org//10.3389/fpubh.2020.589437
Lee, J., Cho, H. S., & Shin, S. R. (2021). Nursing strategies for the post-COVID-19 era. International Nursing Review , 68(2), 149–152. https://doi.org/10.1111/inr.12653 https://doi.org/10.1111/inr.12653
Lee, S. M., & Lee, D. (2021). Opportunities and challenges for contactless healthcare services in the post-COVID-19 Era. Technological Forecasting and Social Change , 167, 120712. https://doi.org/10.1016/j.techfore.2021.120712 https://doi.org/10.1016/j.techfore.2021.120712
Levy, D. L. (2021). COVID-19 and global governance. Journal of Management Studies , 58(2), 562–566. https://doi.org/10.1111/joms.12654 https://doi.org/10.1111/joms.12654
Li, C.-H., Tan, C.-X., Wu, A.-H., & Gao, C.-Q. (2020). COVID-19: The role of community in China’s response. Journal of the Royal Society of Medicine , 113(7), 280–281. https://doi.org/10.1177/0141076820935344 https://doi.org/10.1177/0141076820935344
Marinelli, M. (2020). Emergency healthcare facilities: Managing design in a post-Covid-19 world. IEEE Engineering Management Review , 48(4), 65–71. https://doi.org/10.1109/EMR.2020.3029850 https://doi.org/10.1109/EMR.2020.3029850
Marston, C., Renedo, A., & Miles, S. (2020). Community participation is crucial in a pandemic. The Lancet , 395(10238), 1676–1678. https://doi.org/10.1016/S0140-6736(20)31054-0 https://doi.org/10.1016/S0140-6736(20)31054-0
McCullough, J. M., Eisen-Cohen, E., & Lott, B. (2020). Barriers and facilitators to intraorganizational collaboration in public health: Relational coordination across public health services targeting individuals and populations. Health Care Management Review , 45(1). Retrieved from https://journals.lww.com/hcmrjournal/Fulltext/2020/01000/Barriers_and_facilitators_to_intraorganizational.8.aspx . https://doi.org/10.1097/HMR.0000000000000203 https://journals.lww.com/hcmrjournal/Fulltext/2020/01000/Barriers_and_facilitators_to_intraorganizational.8.aspx https://doi.org/10.1097/HMR.0000000000000203
McDonald, S. M., & Sinha, R. (2008). Information communication technology: Reform of organisational crisis management during natural disasters. International Journal of Management Practice , 3(2), 131–149. Retrieved from https://www.researchgate.net/profile/Sean-Mcdonald-4/publication/247834224_Information_communication_technology_Reform_of_organisational_crisis_management_during_natural_disasters/links/58c45cce45851538eb87568e/Information-communication-technology-Reform-of-organisational-crisis-management-during-natural-disasters.pdf . https://doi.org/10.1504/IJMP.2008.018367 https://www.researchgate.net/profile/Sean-Mcdonald-4/publication/247834224_Information_communication_technology_Reform_of_organisational_crisis_management_during_natural_disasters/links/58c45cce45851538eb87568e/Information-communication-technology-Reform-of-organisational-crisis-management-during-natural-disasters.pdf https://doi.org/10.1504/IJMP.2008.018367
Meduri, Y. (2016). Multi-stakeholder participation in disaster recovery: A case study. Procedia Engineering , 159, 179–185. https://doi.org/10.1016/j.proeng.2016.08.153 https://doi.org/10.1016/j.proeng.2016.08.153
Memish, Z. A., Ebrahim, S. H., Kattan, R. F., Alharthy, A., Alqahtani, S. A., & Karakitsos, D. (2020). Leadership to prevent COVID-19: Is it the most important mitigation factor? Travel Medicine and Infectious Disease , 38, 101925. https://doi.org/10.1016/j.tmaid.2020.101925 https://doi.org/10.1016/j.tmaid.2020.101925
Mohseni, M., Azami-Aghdash, S., Mousavi Isfahani, H., Moosavi, A., & Fardid, M. (2021). Role of nongovernmental organizations in controlling COVID-19. Disaster Medicine and Public Health Preparedness , 16(5), 1705. https://doi.org/10.1017/dmp.2021.60 https://doi.org/10.1017/dmp.2021.60
Moradian, N., Ochs, H. D., Sedikies, C., Hamblin, M. R., Camargo, C. A., Martinez, J. A., … Rezaei, N. (2020). The urgent need for integrated science to fight COVID-19 pandemic and beyond. Journal of Translational Medicine , 18(1), 205. https://doi.org/10.1186/s12967-020-02364-2 https://doi.org/10.1186/s12967-020-02364-2
Moynihan, D. P. (2008). Combining structural forms in the search for policy tools: Incident command systems in U.S. crisis management. Governance , 21(2), 205–229. https://doi.org/10.1111/j.1468-0491.2008.00395.x https://doi.org/10.1111/j.1468-0491.2008.00395.x
Nolte, I. M., & Boenigk, S. (2013). A study of ad hoc network performance in disaster response. Nonprofit and Voluntary Sector Quarterly , 42(1), 148–173. https://doi.org/10.1177/0899764011434557 https://doi.org/10.1177/0899764011434557
Nowell, B., Steelman, T., Velez, A.-L. K., & Yang, Z. (2018). The structure of effective governance of disaster response networks: Insights from the field. The American Review of Public Administration , 48(7), 699–715. https://doi.org/10.1177/0275074017724225 https://doi.org/10.1177/0275074017724225
Obeng, E. A., Marfo, E., Owusu-Ansah, N., & Nantwi, G. (2014). Assessment of the effectiveness of multi-stakeholder dialogue . Tropenbos International, Wageningen, The Netherlands, 82.
Panigrahi, S. K., Majumdar, S., Galhotra, A., Kadle, S. C., & John, A. S. (2021). Community based management of COVID-19 as a way forward for pandemic response. Frontiers in Public Health , 8, 589772. https://doi.org/10.3389/fpubh.2020.589772 https://doi.org/10.3389/fpubh.2020.589772
Panneer, S., Kantamaneni, K., Pushparaj, R. R. B., Shekhar, S., Bhat, L., & Rice, L. (2021). Multistakeholder participation in disaster management—The case of the COVID-19 pandemic. Healthcare , 9(2), 203. https://doi.org/10.3390/healthcare9020203 https://doi.org/10.3390/healthcare9020203
Patuelli, A., Caldarelli, G., Lattanzi, N., & Saracco, F. (2021). Firms’ challenges and social responsibilities during Covid-19: A Twitter analysis. PLoS One , 16(7), e0254748. https://doi.org/10.1371/journal.pone.0254748 https://doi.org/10.1371/journal.pone.0254748
Paul, A., Nath, T. K., Mahanta, J., Sultana, N. N., Kayes, A. S. M. I., … Paul, S. (2021). Psychological and livelihood impacts of COVID-19 on Bangladeshi lower income people. Asia Pacific Journal of Public Health , 33(1), 100–108. https://doi.org/10.1177/1010539520977304 https://doi.org/10.1177/1010539520977304
Raychaudhuri, A. (2020). COVID-19 pandemic crisis and the way forward for India. COVID-19 , 9. Retrieved from https://aic.ris.org.in/sites/aic.ris.org.in/files/Publication/COVID-19%20Report%202020%20Final%201-9_section-min_compressed.pdf#page=34 https://aic.ris.org.in/sites/aic.ris.org.in/files/Publication/COVID-19%20Report%202020%20Final%201-9_section-min_compressed.pdf#page=34
Ryu, S., & Johansen, M. S. (2017). Collaborative networking, environmental shocks, and organizational performance: Evidence from hurricane Rita. International Public Management Journal , 20(2), 206–225. https://doi.org/10.1080/10967494.2015.1059915 https://doi.org/10.1080/10967494.2015.1059915
Satapathy, S., & Walia, A. (2007). Affected parents’ and other stakeholders’perception of a fire disaster management in India: A situational analysis. Disaster Management & Response , 5(4), 111–118. https://doi.org/10.1016/j.dmr.2007.08.002 https://doi.org/10.1016/j.dmr.2007.08.002
Sharma, A., Borah, S. B., & Moses, A. C. (2021). Responses to COVID-19: The role of governance, healthcare infrastructure, and learning from past pandemics. Journal of Business Research , 122, 597–607. https://doi.org/10.1016/j.jbusres.2020.09.011 https://doi.org/10.1016/j.jbusres.2020.09.011
Shoaf, K. I., Kelley, M. M., O’Keefe, K., Arrington, K. D., & Prelip, M. L. (2014). Enhancing emergency preparedness and response systems: Correlates of collaboration between local health departments and school districts. Public Health Report , 129 Suppl 4(Suppl 4), 107–113. https://doi.org/10.1177/00333549141296s414 https://doi.org/10.1177/00333549141296s414
Taylor, A. L., & Habibi, R. (2020). The collapse of global cooperation under the WHO International Health Regulations at the outset of COVID-19: Sculpting the future of global health governance. American Society of International Law Insights , 24, 15. Retrieved from https://www.asil.org/insights/volume/24/issue/15/collapse-global-cooperation-under-who-international-health-regulations. https://www.asil.org/insights/volume/24/issue/15/collapse-global-cooperation-under-who-international-health-regulations.
Tomasini, R. M., & Van Wassenhove, L. N. (2009). From preparedness to partnerships: Case study research on humanitarian logistics. International Transactions in Operational Research , 16(5), 549–559. https://doi.org/10.1111/j.1475-3995.2009.00697.x https://doi.org/10.1111/j.1475-3995.2009.00697.x
Trimurti, N., Endang, L., Hardi, W., & Hartuti, P. (2020, 2020/12/21). Multi-stakeholder participation challenges in local disaster management policies: A case from Bojonegoro District, Indonesia . Proceedings of the 6th International Conference on Social and Political Sciences (ICOSAPS 2020), Indonesia.
Twigg, J. (2001). Physician heal thyself?: The politics of disaster mitigation . London: Benfield Greig Hazard Research Center, University College.
Ullah, A., Pinglu, C., Ullah, S., Abbas, H. S. M., & Khan, S. (2021). The role of e-Governance in combating COVID-19 and promoting sustainable development: A comparative study of China and Pakistan. Chinese Political Science Review , 6(1), 86–118. https://doi.org/10.1007/s41111-020-00167-w https://doi.org/10.1007/s41111-020-00167-w
Verguet, S., Hailu, A., Eregata, G. T., Memirie, S. T., Johansson, K. A., & Norheim, O. F. (2021). Toward universal health coverage in the post-COVID-19 era. Nature Medicine , 27(3), 380–387. https://doi.org/10.1038/s41591-021-01268-y https://doi.org/10.1038/s41591-021-01268-y
Wang, C., Tee, M., Roy, A. E., Fardin, M. A., Srichokchatchawan, W., Habib, H. A., … Kuruchittham, V. (2021). The impact of COVID-19 pandemic on physical and mental health of Asians: A study of seven middle-income countries in Asia. PLoS One , 16(2), e0246824. https://doi.org/10.1371/journal.pone.0246824 https://doi.org/10.1371/journal.pone.0246824
Wangari, E. N., Gichuki, P., Abuor, A. A., Wambui, J., Okeyo, S. O., Oyatsi, H. T. N., … Kulohoma, B. W. (2021). Kenya’s response to the COVID-19 pandemic: A balance between minimising morbidity and adverse economic impact. AAS Open Research , 4, 3. https://doi.org/10.12688/aasopenres.13156.2 https://doi.org/10.12688/aasopenres.13156.2
Warner, J., Waalewijn, P., & Hilhorst, D. (2002). Public participation in disaster-prone watersheds: Time for multi-stakeholder platforms . Retrieved from https://library.wur.nl/WebQuery/wurpubs/fulltext/233664 https://library.wur.nl/WebQuery/wurpubs/fulltext/233664
WHO Coronavirus (COVID-19) Dashboard. (2023). May 25, 2023. Retrieved from https://covid19.who.int https://covid19.who.int
World Health Organization (WHO). (2020). COVID-19 strategic preparedness and response plan: Operational planning guidelines to support country preparedness and response . Retrieved from https://www.who.int/docs/default-source/coronaviruse/covid-19-sprp-unct-guidelines.pdf https://www.who.int/docs/default-source/coronaviruse/covid-19-sprp-unct-guidelines.pdf
Wosik, J., Fudim, M., Cameron, B., Gellad, Z. F., Cho, A., Phinney, D., … Tcheng, J. (2020). Telehealth transformation: COVID-19 and the rise of virtual care. Journal of the American Medical Informatics Association , 27(6), 957–962. https://doi.org/10.1093/jamia/ocaa067 https://doi.org/10.1093/jamia/ocaa067
Zhou, C., Su, F., Pei, T., Zhang, A., Du, Y., Luo, B., … Xiao, H. (2020). COVID-19: Challenges to GIS with Big Data. Geography and Sustainability , 1(1), 77–87. https://doi.org/10.1016/j.geosus.2020.03.005 https://doi.org/10.1016/j.geosus.2020.03.005
Sigamani Panneer, is a Professor, Centre for the Study of Law and Governance, Jawaharlal Nehru University, New Delhi, India and D. Litt. Scholar, Department of Social Work, Assam University, Silchar. He can be contacted at [email protected].
Subhabrata Dutta is a Professor, Department of Social Work, Assam University, Silchar. He can be contacted at [email protected].
Lekha D. Bhat, is an Assistant Professor, Department of Epidemiology and Public Health, Central University of Tamil Nadu, Thiruvarur, India. She can be contacted at [email protected].
Prakash Chand Kandpal, is a Professor, Centre for the Study of Law and Governance, Jawaharlal Nehru University, New Delhi, India. He can be contacted at [email protected].
Robert Ramesh Babu P, is an Assistant Professor, PG Department of Social Work, Don Bosco College, Dharmapuri, India. He can be contacted at [email protected]; [email protected].
Rubavel M., PhD, Consultant UNDP, Bengaluru, Karnataka. He can be contacted at [email protected].
Vigneshwaran Subbiah Akkayasamy, is an Assistant Professor, Department of Sociology and Social Work, School of Social Sciences, CHRIST (Deemed to be University), Bangalore Central Campus, India. He can be contacted at [email protected].
Harvard-Style Citation
Panneer, S , Dutta, S , Bhat, L , Kandpal, P , Babu P, R , M, R & Akkayasamy, V. (2024) 'Multistakeholder Participation, Collaboration, and Networking in Disaster Risk Reduction and Pandemic Management: Insights and Future Policy Framework', Social Development Issues . 46(2) doi: 10.3998/sdi.5989
Show: Vancouver Citation Style | APA Citation Style
Vancouver-Style Citation
Panneer, S , Dutta, S , Bhat, L , Kandpal, P , Babu P, R , M, R & Akkayasamy, V. Multistakeholder Participation, Collaboration, and Networking in Disaster Risk Reduction and Pandemic Management: Insights and Future Policy Framework. Social Development Issues. 2024 5; 46(2) doi: 10.3998/sdi.5989
Show: Harvard Citation Style | APA Citation Style
APA-Style Citation
Panneer, S Dutta, S Bhat, L Kandpal, P Babu P, R M, R & Akkayasamy, V. (2024, 5 17). Multistakeholder Participation, Collaboration, and Networking in Disaster Risk Reduction and Pandemic Management: Insights and Future Policy Framework. Social Development Issues 46(2) doi: 10.3998/sdi.5989
Show: Harvard Citation Style | {% trans 'Vancouver Citation Style' %}
Non Specialist Summary
This article has no summary
IMAGES
COMMENTS
This essay examines key aspects of social relationships that were disrupted by the COVID-19 pandemic. It focuses explicitly on relational mechanisms of health and brings together theory and emerging evidence on the effects of the COVID-19 pandemic to make recommendations for future public health policy and recovery. We first provide an overview of the pandemic in the UK context, outlining the ...
Immigrants and refugees also have their own circumstances, and their fate in the context of the COVID-19 pandemic crisis cannot be ignored. Doing all of the above means that a small part of the social issues created by the COVID-19 pandemic crisis require capacities of trust, cross-sectoral cooperation, coordination, transparency and joint action.
The COVID-19 outbreak affects all segments of the population and is particularly detrimental to members of those social groups in the most vulnerable situations, continues to affect populations, including people living in poverty situations, older persons, persons with disabilities, youth, and indigenous peoples.
Go to: The coronavirus disease-2019 (COVID-19) pandemic, caused by the new coronavirus SARS-CoV-2, has spread around the globe with unprecedented consequences for the health of millions of people. While the pandemic is still in progress, with new incidents being reported every day, the resilience of the global society is constantly being ...
My commentary focuses on the relevance of social theory for understanding the social impacts of Covid-19 and sits alongside a number of other articles in the Journal of Sociology which focus on particular sociological themes. It is certainly not meant to be exhaustive or cover all areas of social theory - it's simply my thoughts on what I think are key areas worthy of sociological research.
Healthcare and COVID-19. One of the social impacts of COVID-19 is its influence on healthcare. Two main changes in healthcare include the providers' experience of patient care and delivery of care. ... These children may also experience a variety of social and psychological issues as the result of school closures, including food insecurity ...
September 03, 2021. " The Pandemic Reader " is a new collection of essays edited by faculty in Arizona State University's School of Social Transformation, in The College of Liberal Arts and Sciences. The collection explores the multitude of ways in which the COVID-19 pandemic has changed life in every aspect. As people around the world try ...
Qi Su. Joshua B. Plotkin. Nature Computational Science (2024) The COVID-19 pandemic represents a massive global health crisis. Because the crisis requires large-scale behaviour change and places ...
On a global scale and based on imputations and modeling from survey data of self-reported mental health problems, the Global Burden of Disease (GBD) study 29 estimated that the COVID-19 pandemic ...
The costs of COVID-19 in 3 stages The COVID-19 shock can be interpreted as a combination of supply and demand shocks (Baqaee and Farhi, 2020; Caballero and Simsek, 2020; Guerrieri et al., 2020).
1. Introduction. The coronavirus disease 2019 (COVID-19) pandemic has led to unprecedented changes in people's daily lives, with implications for mental health and well-being [1-4], both at the level of a given country's population, and when considering specific vulnerable groups [5-7].In order to mitigate the untoward impact of the pandemic (including lockdown) and support mental health ...
The COVID-19 global recession is the deepest since the end of World War II (Figure 1). The global economy contracted by 3.5 percent in 2020 according to the April 2021 World Economic Outlook ...
Furthermore, Spoorthy et al. (2020) conducted a review on the gendered impact of Covid-19 and found that 68.7-85.5% of medical staff is composed of women, and the mean age ranged between 26 and 40 years. Also, women are more likely to be affect by anxiety, depression, and distress ( Lai et al., 2020; Zanardo et al., 2020 ).
The COVID-19 pandemic has led to a dramatic loss of human life worldwide and presents an unprecedented challenge to public health, food systems and the world of work. The economic and social disruption caused by the pandemic is devastating: tens of millions of people are at risk of falling into extreme poverty, while the number of ...
The novel coronavirus disease 2019 (COVID-19), caused by the pathogen severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), originated in Wuhan, China, and has now spread internationally with over 4·3 million individuals infected and over 297 000 deaths as of May 14, 2020, according to the Johns Hopkins Coronavirus Resource Center. While COVID-19 has been termed a great equaliser ...
As the chapters in this volume reveal, the COVID-19 pandemic is related to a wide array of what are routinely described as social problems; they describe ways the disease makes many existing problems worse, even as it creates some new ones. These chapters focus narrowly on their various topics. This chapter adopts a broader perspective that ...
Abstract. This essay examines key aspects of social relationships that were disrupted by the COVID-19 pandemic. It focuses explicitly on relational mechanisms of health and brings together theory and emerging evidence on the effects of the COVID-19 pandemic to make recommendations for future public health policy and recovery.
To our knowledge, this is the first large-scale study to explore the issue of social inequalities relative to COVID-19 testing and the dynamics of the SARS-CoV-2 pandemic in France. The study benefited from the quality and exhaustiveness of national databases. The authors used data from the Système d'Information de Dépistage Populationnel ...
Living through the Covid-19 pandemic, many have seen a number of ethical, legal, and social issues arise as a result of the virus rapidly spreading worldwide. This timely special issue is designed to be a mid-stream retrospective: look at presenting a broad array of topics at the intersection of science and society, from a range of researchers, in many different fields, in light of what we ...
We investigate the relationship between media consumption, misinformation, and important attitudes and behaviours during the coronavirus disease 2019 (COVID-19) pandemic. We find that comparatively more misinformation circulates on Twitter, while news media tends to reinforce public health recommendations like social distancing. We find that exposure to social media is associated with ...
The emergence of COVID-19 dramatically changed social behavior across societies and contexts. Here we study whether social norms also changed. Specifically, we study this question for cultural ...
Ethical Issues of the COVID-19 Pandemic. The public health facilities became overwhelmed, including the medics on the front lines, due to rising cases and complications of COVID-19. However, the main ethical question was how medical practitioners presided over the destiny of patients when equipment cannot support patients in critical conditions.
CDC is committed to COVID-19 vaccine equity, which is when everyone has fair and just access to COVID-19 vaccination. There are many social, geographic, political, economic, and environmental factors that create challenges to vaccination access and acceptance, and that often affect racial and ethnic minority groups.
This essay serves as the introduction to TVNM's special issue on "Pandemic TV," an analysis of the ways in which the COVID-19 pandemic affected principally anglophone television and television-watching in 2020 to 2021 (including television's response to corresponding events such as the summer 2020 Black Lives Matter uprisings and the fall 2020 U.S. presidential election).
Then attention turns to considering social choice and economic trade-offs between the incidence of COVID-19 infections and the level of economic activity. This is followed up by a critical discussion of the desirability of isolating social groups in order to control the incidence of COVID-19 and possibly reduce economic losses from the pandemic.
Loneliness has long been a growing issue in Canada, but the COVID-19 pandemic has only amplified the problem with increased social isolation and decreased social support.. The link between ...
1. Introduction. The newly identified infectious coronavirus (SARS-CoV-2) was discovered in Wuhan and has spread rapidly since December 2019 within China and to other countries around the globe (Zhou et al., 2020; Kabir et al., 2020).The source of SARS-CoV-2 is still unclear (Gorbalenya et al., 2020).Fig. 1 demonstrates the initial timeline of the development of SARS-CoV-2 (Yan et al., 2020).
Motivated by the issue of COVID-19 mitigation, in this work we tackle the general problem of optimally controlling an epidemic outbreak of a communicable disease structured by time since exposure, by the aid of two types of control instruments namely, social distancing and vaccination by a vaccine at least partly effective in protecting from infection. Effective vaccines are assumed to be made ...
The pandemic has left a deep impact on the global economy wherein the Gross Domestic Production (GDP) of the countries sharply decreased, and this slowing down of the economies has led to various livelihood issues. The COVID-19 pandemic not only has disturbed the social lives and financial status but also has affected the health and wellbeing ...
ABSTRACT. This essay examines key aspects of social relationships that were disrupted by the COVID-19 pandemic. It focuses explicitly on relational mechanisms of health and brings together theory and emerging evidence on the effects of the COVID-19 pandemic to make recommendations for future public health policy and recovery.