

Archer Library
Qualitative research: literature review .
- Archer Library This link opens in a new window
- Schedule a Reference Appointment This link opens in a new window
- Qualitative Research Handout This link opens in a new window
- Locating Books
- ebook Collections This link opens in a new window
- A to Z Database List This link opens in a new window
- Research & Stats
- Literature Review Resources
- Citation & Reference
Exploring the literature review
Literature review model: 6 steps.

Adapted from The Literature Review , Machi & McEvoy (2009, p. 13).
Your Literature Review
Step 2: search, boolean search strategies, search limiters, ★ ebsco & google drive.

1. Select a Topic
"All research begins with curiosity" (Machi & McEvoy, 2009, p. 14)
Selection of a topic, and fully defined research interest and question, is supervised (and approved) by your professor. Tips for crafting your topic include:
- Be specific. Take time to define your interest.
- Topic Focus. Fully describe and sufficiently narrow the focus for research.
- Academic Discipline. Learn more about your area of research & refine the scope.
- Avoid Bias. Be aware of bias that you (as a researcher) may have.
- Document your research. Use Google Docs to track your research process.
- Research apps. Consider using Evernote or Zotero to track your research.
Consider Purpose
What will your topic and research address?
In The Literature Review: A Step-by-Step Guide for Students , Ridley presents that literature reviews serve several purposes (2008, p. 16-17). Included are the following points:
- Historical background for the research;
- Overview of current field provided by "contemporary debates, issues, and questions;"
- Theories and concepts related to your research;
- Introduce "relevant terminology" - or academic language - being used it the field;
- Connect to existing research - does your work "extend or challenge [this] or address a gap;"
- Provide "supporting evidence for a practical problem or issue" that your research addresses.
★ Schedule a research appointment
At this point in your literature review, take time to meet with a librarian. Why? Understanding the subject terminology used in databases can be challenging. Archer Librarians can help you structure a search, preparing you for step two. How? Contact a librarian directly or use the online form to schedule an appointment. Details are provided in the adjacent Schedule an Appointment box.
2. Search the Literature
Collect & Select Data: Preview, select, and organize
AU Library is your go-to resource for this step in your literature review process. The literature search will include books and ebooks, scholarly and practitioner journals, theses and dissertations, and indexes. You may also choose to include web sites, blogs, open access resources, and newspapers. This library guide provides access to resources needed to complete a literature review.
Books & eBooks: Archer Library & OhioLINK
Databases: scholarly & practitioner journals.
Review the Library Databases tab on this library guide, it provides links to recommended databases for Education & Psychology, Business, and General & Social Sciences.
Expand your journal search; a complete listing of available AU Library and OhioLINK databases is available on the Databases A to Z list . Search the database by subject, type, name, or do use the search box for a general title search. The A to Z list also includes open access resources and select internet sites.
Databases: Theses & Dissertations
Review the Library Databases tab on this guide, it includes Theses & Dissertation resources. AU library also has AU student authored theses and dissertations available in print, search the library catalog for these titles.
Did you know? If you are looking for particular chapters within a dissertation that is not fully available online, it is possible to submit an ILL article request . Do this instead of requesting the entire dissertation.
Newspapers: Databases & Internet
Consider current literature in your academic field. AU Library's database collection includes The Chronicle of Higher Education and The Wall Street Journal . The Internet Resources tab in this guide provides links to newspapers and online journals such as Inside Higher Ed , COABE Journal , and Education Week .
Search Strategies & Boolean Operators
There are three basic boolean operators: AND, OR, and NOT.
Used with your search terms, boolean operators will either expand or limit results. What purpose do they serve? They help to define the relationship between your search terms. For example, using the operator AND will combine the terms expanding the search. When searching some databases, and Google, the operator AND may be implied.
Overview of boolean terms
About the example: Boolean searches were conducted on November 4, 2019; result numbers may vary at a later date. No additional database limiters were set to further narrow search returns.
Database Search Limiters
Database strategies for targeted search results.
Most databases include limiters, or additional parameters, you may use to strategically focus search results. EBSCO databases, such as Education Research Complete & Academic Search Complete provide options to:
- Limit results to full text;
- Limit results to scholarly journals, and reference available;
- Select results source type to journals, magazines, conference papers, reviews, and newspapers
- Publication date
Keep in mind that these tools are defined as limiters for a reason; adding them to a search will limit the number of results returned. This can be a double-edged sword. How?
- If limiting results to full-text only, you may miss an important piece of research that could change the direction of your research. Interlibrary loan is available to students, free of charge. Request articles that are not available in full-text; they will be sent to you via email.
- If narrowing publication date, you may eliminate significant historical - or recent - research conducted on your topic.
- Limiting resource type to a specific type of material may cause bias in the research results.
Use limiters with care. When starting a search, consider opting out of limiters until the initial literature screening is complete. The second or third time through your research may be the ideal time to focus on specific time periods or material (scholarly vs newspaper).
★ Truncating Search Terms
Expanding your search term at the root.
Truncating is often referred to as 'wildcard' searching. Databases may have their own specific wildcard elements however, the most commonly used are the asterisk (*) or question mark (?). When used within your search. they will expand returned results.
Asterisk (*) Wildcard
Using the asterisk wildcard will return varied spellings of the truncated word. In the following example, the search term education was truncated after the letter "t."
Explore these database help pages for additional information on crafting search terms.
- EBSCO Connect: Searching with Wildcards and Truncation Symbols
- EBSCO Connect: Searching with Boolean Operators
- EBSCO Connect: EBSCOhost Search Tips
- EBSCO Connect: Basic Searching with EBSCO
- ProQuest Help: Search Tips
- ERIC: How does ERIC search work?
★ EBSCO Databases & Google Drive
Tips for saving research directly to Google drive.
Researching in an EBSCO database?
It is possible to save articles (PDF and HTML) and abstracts in EBSCOhost databases directly to Google drive. Select the Google Drive icon, authenticate using a Google account, and an EBSCO folder will be created in your account. This is a great option for managing your research. If documenting your research in a Google Doc, consider linking the information to actual articles saved in drive.
EBSCO Databases & Google Drive
EBSCOHost Databases & Google Drive: Managing your Research
This video features an overview of how to use Google Drive with EBSCO databases to help manage your research. It presents information for connecting an active Google account to EBSCO and steps needed to provide permission for EBSCO to manage a folder in Drive.
About the Video: Closed captioning is available, select CC from the video menu. If you need to review a specific area on the video, view on YouTube and expand the video description for access to topic time stamps. A video transcript is provided below.
- EBSCOhost Databases & Google Scholar
Defining Literature Review
What is a literature review.
A definition from the Online Dictionary for Library and Information Sciences .
A literature review is "a comprehensive survey of the works published in a particular field of study or line of research, usually over a specific period of time, in the form of an in-depth, critical bibliographic essay or annotated list in which attention is drawn to the most significant works" (Reitz, 2014).
A systemic review is "a literature review focused on a specific research question, which uses explicit methods to minimize bias in the identification, appraisal, selection, and synthesis of all the high-quality evidence pertinent to the question" (Reitz, 2014).
Recommended Reading

About this page
EBSCO Connect [Discovery and Search]. (2022). Searching with boolean operators. Retrieved May, 3, 2022 from https://connect.ebsco.com/s/?language=en_US
EBSCO Connect [Discover and Search]. (2022). Searching with wildcards and truncation symbols. Retrieved May 3, 2022; https://connect.ebsco.com/s/?language=en_US
Machi, L.A. & McEvoy, B.T. (2009). The literature review . Thousand Oaks, CA: Corwin Press:
Reitz, J.M. (2014). Online dictionary for library and information science. ABC-CLIO, Libraries Unlimited . Retrieved from https://www.abc-clio.com/ODLIS/odlis_A.aspx
Ridley, D. (2008). The literature review: A step-by-step guide for students . Thousand Oaks, CA: Sage Publications, Inc.
Archer Librarians
Schedule an appointment.
Contact a librarian directly (email), or submit a request form. If you have worked with someone before, you can request them on the form.
- ★ Archer Library Help • Online Reqest Form
- Carrie Halquist • Reference & Instruction
- Jessica Byers • Reference & Curation
- Don Reams • Corrections Education & Reference
- Diane Schrecker • Education & Head of the IRC
- Tanaya Silcox • Technical Services & Business
- Sarah Thomas • Acquisitions & ATS Librarian
- << Previous: Research & Stats
- Next: Literature Review Resources >>
- Last Updated: Apr 23, 2024 3:47 PM
- URL: https://libguides.ashland.edu/qualitative
Archer Library • Ashland University © Copyright 2023. An Equal Opportunity/Equal Access Institution.
Chapter 9. Reviewing the Literature
What is a “literature review”.
No researcher ever comes up with a research question that is wholly novel. Someone, somewhere, has asked the same thing. Academic research is part of a larger community of researchers, and it is your responsibility, as a member of this community, to acknowledge others who have asked similar questions and to put your particular research into this greater context. It is not simply a convention or custom to begin your study with a review of previous literature (the “ lit review ”) but an important responsibility you owe the scholarly community.

Too often, new researchers pursue a topic to study and then write something like, “No one has ever studied this before” or “This area is underresearched.” It may be that no one has studied this particular group or setting, but it is highly unlikely no one has studied the foundational phenomenon of interest. And that comment about an area being underresearched? Be careful. The statement may simply signal to others that you haven’t done your homework. Rubin ( 2021 ) refers to this as “free soloing,” and it is not appreciated in academic work:
The truth of the matter is, academics don’t really like when people free solo. It’s really bad form to omit talking about the other people who are doing or have done research in your area. Partly, I mean we need to cite their work, but I also mean we need to respond to it—agree or disagree, clarify for extend. It’s also really bad form to talk about your research in a way that does not make it understandable to other academics.…You have to explain to your readers what your story is really about in terms they care about . This means using certain terminology, referencing debates in the literature, and citing relevant works—that is, in connecting your work to something else. ( 51–52 )
A literature review is a comprehensive summary of previous research on a topic. It includes both articles and books—and in some cases reports—relevant to a particular area of research. Ideally, one’s research question follows from the reading of what has already been produced. For example, you are interested in studying sports injuries related to female gymnasts. You read everything you can find on sports injuries related to female gymnasts, and you begin to get a sense of what questions remain open. You find that there is a lot of research on how coaches manage sports injuries and much about cultures of silence around treating injuries, but you don’t know what the gymnasts themselves are thinking about these issues. You look specifically for studies about this and find several, which then pushes you to narrow the question further. Your literature review then provides the road map of how you came to your very specific question, and it puts your study in the context of studies of sports injuries. What you eventually find can “speak to” all the related questions as well as your particular one.
In practice, the process is often a bit messier. Many researchers, and not simply those starting out, begin with a particular question and have a clear idea of who they want to study and where they want to conduct their study but don’t really know much about other studies at all. Although backward, we need to recognize this is pretty common. Telling students to “find literature” after the fact can seem like a purposeless task or just another hurdle for completing a thesis or dissertation. It is not! Even if you were not motivated by the literature in the first place, acknowledging similar studies and connecting your own research to those studies are important parts of building knowledge. Acknowledgment of past research is a responsibility you owe the discipline to which you belong.
Literature reviews can also signal theoretical approaches and particular concepts that you will incorporate into your own study. For example, let us say you are doing a study of how people find their first jobs after college, and you want to use the concept of social capital . There are competing definitions of social capital out there (e.g., Bourdieu vs. Burt vs. Putnam). Bourdieu’s notion is of one form of capital, or durable asset, of a “network of more or less institutionalized relationships of mutual acquaintance or recognition” ( 1984:248 ). Burt emphasizes the “brokerage opportunities” in a social network as social capital ( 1997:355 ). Putnam’s social capital is all about “facilitating coordination and cooperation for mutual benefit” ( 2001:67 ). Your literature review can adjudicate among these three approaches, or it can simply refer to the one that is animating your own research. If you include Bourdieu in your literature review, readers will know “what kind” of social capital you are talking about as well as what kind of social scientist you yourself are. They will likely understand that you are interested more in how some people are advantaged by their social capital relative to others rather than being interested in the mechanics of how social networks operate.
The literature review thus does two important things for you: firstly, it allows you to acknowledge previous research in your area of interest, thereby situating you within a discipline or body of scholars, and, secondly, it demonstrates that you know what you are talking about. If you present the findings of your research study without including a literature review, it can be like singing into the wind. It sounds nice, but no one really hears it, or if they do catch snippets, they don’t know where it is coming from.
Examples of Literature Reviews
To help you get a grasp of what a good literature review looks like and how it can advance your study, let’s take a look at a few examples.
Reader-Friendly Example: The Power of Peers
The first is by Janice McCabe ( 2016 ) and is from an article on peer networks in the journal Contexts . Contexts presents articles in a relatively reader-friendly format, with the goal of reaching a large audience for interesting sociological research. Read this example carefully and note how easily McCabe is able to convey the relevance of her own work by situating it in the context of previous studies:
Scholars who study education have long acknowledged the importance of peers for students’ well-being and academic achievement. For example, in 1961, James Coleman argued that peer culture within high schools shapes students’ social and academic aspirations and successes. More recently, Judith Rich Harris has drawn on research in a range of areas—from sociological studies of preschool children to primatologists’ studies of chimpanzees and criminologists’ studies of neighborhoods—to argue that peers matter much more than parents in how children “turn out.” Researchers have explored students’ social lives in rich detail, as in Murray Milner’s book about high school students, Freaks, Geeks, and Cool Kids , and Elizabeth Armstrong and Laura Hamilton’s look at college students, Paying for the Party . These works consistently show that peers play a very important role in most students’ lives. They tend, however, to prioritize social over academic influence and to use a fuzzy conception of peers rather than focusing directly on friends—the relationships that should matter most for student success. Social scientists have also studied the power of peers through network analysis, which is based on uncovering the web of connections between people. Network analysis involves visually mapping networks and mathematically comparing their structures (such as the density of ties) and the positions of individuals within them (such as how central a given person is within the network). As Nicholas Christakis and James Fowler point out in their book Connected , network structure influences a range of outcomes, including health, happiness, wealth, weight, and emotions. Given that sociologists have long considered network explanations for social phenomena, it’s surprising that we know little about how college students’ friends impact their experiences. In line with this network tradition, I focus on the structure of friendship networks, constructing network maps so that the differences we see across participants are due to the underlying structure, including each participant’s centrality in their friendship group and the density of ties among their friends. ( 23 )
What did you notice? In her very second sentence, McCabe uses “for example” to introduce a study by Coleman, thereby indicating that she is not going to tell you every single study in this area but is going to tell you that (1) there is a lot of research in this area, (2) it has been going on since at least 1961, and (3) it is still relevant (i.e., recent studies are still being done now). She ends her first paragraph by summarizing the body of literature in this area (after giving you a few examples) and then telling you what may have been (so far) left out of this research. In the second paragraph, she shifts to a separate interesting focus that is related to the first but is also quite distinct. Lit reviews very often include two (or three) distinct strands of literature, the combination of which nicely backgrounds this particular study . In the case of our female gymnast study (above), those two strands might be (1) cultures of silence around sports injuries and (2) the importance of coaches. McCabe concludes her short and sweet literature review with one sentence explaining how she is drawing from both strands of the literature she has succinctly presented for her particular study. This example should show you that literature reviews can be readable, helpful, and powerful additions to your final presentation.
Authoritative Academic Journal Example: Working Class Students’ College Expectations
The second example is more typical of academic journal writing. It is an article published in the British Journal of Sociology of Education by Wolfgang Lehmann ( 2009 ):
Although this increase in post-secondary enrolment and the push for university is evident across gender, race, ethnicity, and social class categories, access to university in Canada continues to be significantly constrained for those from lower socio-economic backgrounds (Finnie, Lascelles, and Sweetman 2005). Rising tuition fees coupled with an overestimation of the cost and an underestimation of the benefits of higher education has put university out of reach for many young people from low-income families (Usher 2005). Financial constraints aside, empirical studies in Canada have shown that the most important predictor of university access is parental educational attainment. Having at least one parent with a university degree significantly increases the likelihood of a young person to attend academic-track courses in high school, have high educational and career aspirations, and ultimately attend university (Andres et al. 1999, 2000; Lehmann 2007a). Drawing on Bourdieu’s various writing on habitus and class-based dispositions (see, for example, Bourdieu 1977, 1990), Hodkinson and Sparkes (1997) explain career decisions as neither determined nor completely rational. Instead, they are based on personal experiences (e.g., through employment or other exposure to occupations) and advice from others. Furthermore, they argue that we have to understand these decisions as pragmatic, rather than rational. They are pragmatic in that they are based on incomplete and filtered information, because of the social context in which the information is obtained and processed. New experiences and information can, however, also be allowed into one’s world, where they gradually or radically transform habitus, which in turn creates the possibility for the formation of new and different dispositions. Encountering a supportive teacher in elementary or secondary school, having ambitious friends, or chance encounters can spark such transformations. Transformations can be confirming or contradictory, they can be evolutionary or dislocating. Working-class students who enter university most certainly encounter such potentially transformative situations. Granfield (1991) has shown how initially dislocating feelings of inadequacy and inferiority of working-class students at an elite US law school were eventually replaced by an evolutionary transformation, in which the students came to dress, speak and act more like their middle-class and upper-class peers. In contrast, Lehmann (2007b) showed how persistent habitus dislocation led working-class university students to drop out of university. Foskett and Hemsley-Brown (1999) argue that young people’s perceptions of careers are a complex mix of their own experiences, images conveyed through adults, and derived images conveyed by the media. Media images of careers, perhaps, are even more important for working-class youth with high ambitions as they offer (generally distorted) windows into a world of professional employment to which they have few other sources of access. It has also been argued that working-class youth who do continue to university still face unique, class-specific challenges, evident in higher levels of uncertainty (Baxter and Britton 2001; Lehmann 2004, 2007a; Quinn 2004), their higher education choices (Ball et al. 2002; Brooks 2003; Reay et al. 2001) and fears of inadequacy because of their cultural outsider status (Aries and Seider 2005; Granfield 1991). Although the number of working-class university students in Canada has slowly increased, that of middle-class students at university has risen far more steeply (Knighton and Mizra 2002). These different enrolment trajectories have actually widened the participation gap, which in tum explains our continued concerns with the potential outsider status Indeed, in a study comparing first-generation working-class and traditional students who left university without graduating, Lehmann (2007b) found that first-generation working-class students were more likely to leave university very early in some cases within the first two months of enrollment. They were also more likely to leave university despite solid academic performance. Not “fitting in,” not “feeling university,” and not being able to “relate to these people” were key reasons for eventually withdrawing from university. From the preceding review of the literature, a number of key research questions arise: How do working-class university students frame their decision to attend university? How do they defy the considerable odds documented in the literature to attend university? What are the sources of information and various images that create dispositions to study at university? What role does their social-class background- or habitus play in their transition dispositions and how does this translate into expectations for university? ( 139 )
What did you notice here? How is this different from (and similar to) the first example? Note that rather than provide you with one or two illustrative examples of similar types of research, Lehmann provides abundant source citations throughout. He includes theory and concepts too. Like McCabe, Lehmann is weaving through multiple literature strands: the class gap in higher education participation in Canada, class-based dispositions, and obstacles facing working-class college students. Note how he concludes the literature review by placing his research questions in context.
Find other articles of interest and read their literature reviews carefully. I’ve included two more for you at the end of this chapter . As you learned how to diagram a sentence in elementary school (hopefully!), try diagramming the literature reviews. What are the “different strands” of research being discussed? How does the author connect these strands to their own research questions? Where is theory in the lit review, and how is it incorporated (e.g., Is it a separate strand of its own or is it inextricably linked with previous research in this area)?
One model of how to structure your literature review can be found in table 9.1. More tips, hints, and practices will be discussed later in the chapter.
Table 9.1. Model of Literature Review, Adopted from Calarco (2020:166)
Embracing Theory
A good research study will, in some form or another, use theory. Depending on your particular study (and possibly the preferences of the members of your committee), theory may be built into your literature review. Or it may form its own section in your research proposal/design (e.g., “literature review” followed by “theoretical framework”). In my own experience, I see a lot of graduate students grappling with the requirement to “include theory” in their research proposals. Things get a little squiggly here because there are different ways of incorporating theory into a study (Are you testing a theory? Are you generating a theory?), and based on these differences, your literature review proper may include works that describe, explain, and otherwise set forth theories, concepts, or frameworks you are interested in, or it may not do this at all. Sometimes a literature review sets forth what we know about a particular group or culture totally independent of what kinds of theoretical framework or particular concepts you want to explore. Indeed, the big point of your study might be to bring together a body of work with a theory that has never been applied to it previously. All this is to say that there is no one correct way to approach the use of theory and the writing about theory in your research proposal.
Students are often scared of embracing theory because they do not exactly understand what it is. Sometimes, it seems like an arbitrary requirement. You’re interested in a topic; maybe you’ve even done some research in the area and you have findings you want to report. And then a committee member reads over what you have and asks, “So what?” This question is a good clue that you are missing theory, the part that connects what you have done to what other researchers have done and are doing. You might stumble upon this rather accidentally and not know you are embracing theory, as in a case where you seek to replicate a prior study under new circumstances and end up finding that a particular correlation between behaviors only happens when mediated by something else. There’s theory in there, if you can pull it out and articulate it. Or it might be that you are motivated to do more research on racial microaggressions because you want to document their frequency in a particular setting, taking for granted the kind of critical race theoretical framework that has done the hard work of defining and conceptualizing “microaggressions” in the first place. In that case, your literature review could be a review of Critical Race Theory, specifically related to this one important concept. That’s the way to bring your study into a broader conversation while also acknowledging (and honoring) the hard work that has preceded you.
Rubin ( 2021 ) classifies ways of incorporating theory into case study research into four categories, each of which might be discussed somewhat differently in a literature review or theoretical framework section. The first, the least theoretical, is where you set out to study a “configurative idiographic case” ( 70 ) This is where you set out to describe a particular case, leaving yourself pretty much open to whatever you find. You are not expecting anything based on previous literature. This is actually pretty weak as far as research design goes, but it is probably the default for novice researchers. Your committee members should probably help you situate this in previous literature in some way or another. If they cannot, and it really does appear you are looking at something fairly new that no one else has bothered to research before, and you really are completely open to discovery, you might try using a Grounded Theory approach, which is a methodological approach that foregrounds the generation of theory. In that case, your “theory” section can be a discussion of “Grounded Theory” methodology (confusing, yes, but if you take some time to ponder, you will see how this works). You will still need a literature review, though. Ideally one that describes other studies that have ever looked at anything remotely like what you are looking at—parallel cases that have been researched.
The second approach is the “disciplined configurative case,” in which theory is applied to explain a particular case or topic. You are not trying to test the theory but rather assuming the theory is correct, as in the case of exploring microaggressions in a particular setting. In this case, you really do need to have a separate theory section in addition to the literature review, one in which you clearly define the theoretical framework, including any of its important concepts. You can use this section to discuss how other researchers have used the concepts and note any discrepancies in definitions or operationalization of those concepts. This way you will be sure to design your study so that it speaks to and with other researchers. If everyone who is writing about microaggressions has a different definition of them, it is hard for others to compare findings or make any judgments about their prevalence (or any number of other important characteristics). Your literature review section may then stand alone and describe previous research in the particular area or setting, irrespective of the kinds of theory underlying those studies.
The third approach is “heuristic,” one in which you seek to identify new variables, hypotheses, mechanisms, or paths not yet explained by a theory or theoretical framework. In a way, you are generating new theory, but it is probably more accurate to say that you are extending or deepening preexisting theory. In this case, having a single literature review that is focused on the theory and the ways the theory has been applied and understood (with all its various mechanisms and pathways) is probably your best option. The focus of the literature reviewed is less on the case and more on the theory you are seeking to extend.
The final approach is “theory testing,” which is much rarer in qualitative studies than in quantitative, where this is the default approach. Theory-testing cases are those where a particular case is used to see if an existing theory is accurate or accurate under particular circumstances. As with the heuristic approach, your literature review will probably draw heavily on previous uses of the theory, but you may end up having a special section specifically about cases very close to your own . In other words, the more your study approaches theory testing, the more likely there is to be a set of similar studies to draw on or even one important key study that you are setting your own study up in parallel to in order to find out if the theory generated there operates here.
If we wanted to get very technical, it might be useful to distinguish theoretical frameworks properly from conceptual frameworks. The latter are a bit looser and, given the nature of qualitative research, often fit exploratory studies. Theoretical frameworks rely on specific theories and are essential for theory-testing studies. Conceptual frameworks can pull in specific concepts or ideas that may or may not be linked to particular theories. Think about it this way: A theory is a story of how the world works. Concepts don’t presume to explain the whole world but instead are ways to approach phenomena to help make sense of them. Microaggressions are concepts that are linked to Critical Race Theory. One could contextualize one’s study within Critical Race Theory and then draw various concepts, such as that of microaggressions from the overall theoretical framework. Or one could bracket out the master theory or framework and employ the concept of microaggression more opportunistically as a phenomenon of interest. If you are unsure of what theory you are using, you might want to frame a more practical conceptual framework in your review of the literature.
Helpful Tips
How to maintain good notes for what your read.
Over the years, I have developed various ways of organizing notes on what I read. At first, I used a single sheet of full-size paper with a preprinted list of questions and points clearly addressed on the front side, leaving the second side for more reflective comments and free-form musings about what I read, why it mattered, and how it might be useful for my research. Later, I developed a system in which I use a single 4″ × 6″ note card for each book I read. I try only to use the front side (and write very small), leaving the back for comments that are about not just this reading but things to do or examine or consider based on the reading. These notes often mean nothing to anyone else picking up the card, but they make sense to me. I encourage you to find an organizing system that works for you. Then when you set out to compose a literature review, instead of staring at five to ten books or a dozen articles, you will have ten neatly printed pages or notecards or files that have distilled what is important to know about your reading.
It is also a good idea to store this data digitally, perhaps through a reference manager. I use RefWorks, but I also recommend EndNote or any other system that allows you to search institutional databases. Your campus library will probably provide access to one of these or another system. Most systems will allow you to export references from another manager if and when you decide to move to another system. Reference managers allow you to sort through all your literature by descriptor, author, year, and so on. Even so, I personally like to have the ability to manually sort through my index cards, recategorizing things I have read as I go. I use RefWorks to keep a record of what I have read, with proper citations, so I can create bibliographies more easily, and I do add in a few “notes” there, but the bulk of my notes are kept in longhand.
What kinds of information should you include from your reading? Here are some bulleted suggestions from Calarco ( 2020:113–114 ), with my own emendations:
- Citation . If you are using a reference manager, you can import the citation and then, when you are ready to create a bibliography, you can use a provided menu of citation styles, which saves a lot of time. If you’ve originally formatted in Chicago Style but the journal you are writing for wants APA style, you can change your entire bibliography in less than a minute. When using a notecard for a book, I include author, title, date as well as the library call number (since most of what I read I pull from the library). This is something RefWorks is not able to do, and it helps when I categorize.
I begin each notecard with an “intro” section, where I record the aims, goals, and general point of the book/article as explained in the introductory sections (which might be the preface, the acknowledgments, or the first two chapters). I then draw a bold line underneath this part of the notecard. Everything after that should be chapter specific. Included in this intro section are things such as the following, recommended by Calarco ( 2020 ):
- Key background . “Two to three short bullet points identifying the theory/prior research on which the authors are building and defining key terms.”
- Data/methods . “One or two short bullet points with information about the source of the data and the method of analysis, with a note if this is a novel or particularly effective example of that method.” I use [M] to signal methodology on my notecard, which might read, “[M] Int[erview]s (n-35), B[lack]/W[hite] voters” (I need shorthand to fit on my notecard!).
- Research question . “Stated as briefly as possible.” I always provide page numbers so I can go back and see exactly how this was stated (sometimes, in qualitative research, there are multiple research questions, and they cannot be stated simply).
- Argument/contributions . “Two to three short bullet points briefly describing the authors’ answer to the central research question and its implication for research, theory, and practice.” I use [ARG] for argument to signify the argument, and I make sure this is prominently visible on my notecard. I also provide page numbers here.
For me, all of this fits in the “intro” section, which, if this is a theoretically rich, methodologically sound book, might take up a third or even half of the front page of my notecard. Beneath the bold underline, I report specific findings or particulars of the book as they emerge chapter by chapter. Calarco’s ( 2020 ) next step is the following:
- Key findings . “Three to four short bullet points identifying key patterns in the data that support the authors’ argument.”
All that remains is writing down thoughts that occur upon finishing the article/book. I use the back of the notecard for these kinds of notes. Often, they reach out to other things I have read (e.g., “Robinson reminds me of Crusoe here in that both are looking at the effects of social isolation, but I think Robinson makes a stronger argument”). Calarco ( 2020 ) concludes similarly with the following:
- Unanswered questions . “Two to three short bullet points that identify key limitations of the research and/or questions the research did not answer that could be answered in future research.”
As I mentioned, when I first began taking notes like this, I preprinted pages with prompts for “research question,” “argument,” and so on. This was a great way to remind myself to look for these things in particular. You can do the same, adding whatever preprinted sections make sense to you, given what you are studying and the important aspects of your discipline. The other nice thing about the preprinted forms is that it keeps your writing to a minimum—you cannot write more than the allotted space, even if you might want to, preventing your notes from spiraling out of control. This can be helpful when we are new to a subject and everything seems worth recording!
After years of discipline, I have finally settled on my notecard approach. I have thousands of notecards, organized in several index card filing boxes stacked in my office. On the top right of each card is a note of the month/day I finished reading the item. I can remind myself what I read in the summer of 2010 if the need or desire ever arose to do so…those invaluable notecards are like a memento of what my brain has been up to!
Where to Start Looking for Literature
Your university library should provide access to one of several searchable databases for academic books and articles. My own preference is JSTOR, a service of ITHAKA, a not-for-profit organization that works to advance and preserve knowledge and to improve teaching and learning through the use of digital technologies. JSTOR allows you to search by several keywords and to narrow your search by type of material (articles or books). For many disciplines, the “literature” of the literature review is expected to be peer-reviewed “articles,” but some disciplines will also value books and book chapters. JSTOR is particularly useful for article searching. You can submit several keywords and see what is returned, and you can also narrow your search by a particular journal or discipline. If your discipline has one or two key journals (e.g., the American Journal of Sociology and the American Sociological Review are key for sociology), you might want to go directly to those journals’ websites and search for your topic area. There is an art to when to cast your net widely and when to refine your search, and you may have to tack back and forth to ensure that you are getting all that is relevant but not getting bogged down in all studies that might have some marginal relevance.
Some articles will carry more weight than others, and you can use applications like Google Scholar to see which articles have made and are continuing to make larger impacts on your discipline. Find these articles and read them carefully; use their literature review and the sources cited in those articles to make sure you are capturing what is relevant. This is actually a really good way of finding relevant books—only the most impactful will make it into the citations of journals. Over time, you will notice that a handful of articles (or books) are cited so often that when you see, say, Armstrong and Hamilton ( 2015 ), you know exactly what book this is without looking at the full cite. This is when you know you are in the conversation.
You might also approach a professor whose work is broadly in the area of your interest and ask them to recommend one or two “important” foundational articles or books. You can then use the references cited in those recommendations to build up your literature. Just be careful: some older professors’ knowledge of the literature (and I reluctantly add myself here) may be a bit outdated! It is best that the article or book whose references and sources you use to build your body of literature be relatively current.
Keep a List of Your Keywords
When using searchable databases, it is a good idea to keep a list of all the keywords you use as you go along so that (1) you do not needlessly duplicate your efforts and (2) you can more easily adjust your search as you get a better sense of what you are looking for. I suggest you keep a separate file or even a small notebook for this and you date your search efforts.
Here’s an example:
Table 9.2. Keep a List of Your Keywords
Think Laterally
How to find the various strands of literature to combine? Don’t get stuck on finding the exact same research topic you think you are interested in. In the female gymnast example, I recommended that my student consider looking for studies of ballerinas, who also suffer sports injuries and around whom there is a similar culture of silence. It turned out that there was in fact research about my student’s particular questions, just not about the subjects she was interested in. You might do something similar. Don’t get stuck looking for too direct literature but think about the broader phenomenon of interest or analogous cases.
Read Outside the Canon
Some scholars’ work gets cited by everyone all the time. To some extent, this is a very good thing, as it helps establish the discipline. For example, there are a lot of “Bourdieu scholars” out there (myself included) who draw ideas, concepts, and quoted passages from Bourdieu. This makes us recognizable to one another and is a way of sharing a common language (e.g., where “cultural capital” has a particular meaning to those versed in Bourdieusian theory). There are empirical studies that get cited over and over again because they are excellent studies but also because there is an “echo chamber effect” going on, where knowing to cite this study marks you as part of the club, in the know, and so on. But here’s the problem with this: there are hundreds if not thousands of excellent studies out there that fail to get appreciated because they are crowded out by the canon. Sometimes this happens because they are published in “lower-ranked” journals and are never read by a lot of scholars who don’t have time to read anything other than the “big three” in their field. Other times this happens because the author falls outside of the dominant social networks in the field and thus is unmentored and fails to get noticed by those who publish a lot in those highly ranked and visible spaces. Scholars who fall outside the dominant social networks and who publish outside of the top-ranked journals are in no way less insightful than their peers, and their studies may be just as rigorous and relevant to your work, so it is important for you to take some time to read outside the canon. Due to how a person’s race, gender, and class operate in the academy, there is also a matter of social justice and ethical responsibility involved here: “When you focus on the most-cited research, you’re more likely to miss relevant research by women and especially women of color, whose research tends to be under-cited in most fields. You’re also more likely to miss new research, research by junior scholars, and research in other disciplines that could inform your work. Essentially, it is important to read and cite responsibly, which means checking that you’re not just reading and citing the same white men and the same old studies that everyone has cited before you” ( Calarco 2020:112 ).
Consider Multiple Uses for Literature
Throughout this chapter, I’ve referred to the literature of interest in a rather abstract way, as what is relevant to your study. But there are many different ways previous research can be relevant to your study. The most basic use of the literature is the “findings”—for example, “So-and-so found that Canadian working-class students were concerned about ‘fitting in’ to the culture of college, and I am going to look at a similar question here in the US.” But the literature may be of interest not for its findings but theoretically—for example, employing concepts that you want to employ in your own study. Bourdieu’s definition of social capital may have emerged in a study of French professors, but it can still be relevant in a study of, say, how parents make choices about what preschools to send their kids to (also a good example of lateral thinking!).
If you are engaged in some novel methodological form of data collection or analysis, you might look for previous literature that has attempted that. I would not recommend this for undergraduate research projects, but for graduate students who are considering “breaking the mold,” find out if anyone has been there before you. Even if their study has absolutely nothing else in common with yours, it is important to acknowledge that previous work.
Describing Gaps in the Literature
First, be careful! Although it is common to explain how your research adds to, builds upon, and fills in gaps in the previous research (see all four literature review examples in this chapter for this), there is a fine line between describing the gaps and misrepresenting previous literature by failing to conduct a thorough review of the literature. A little humility can make a big difference in your presentation. Instead of “This is the first study that has looked at how firefighters juggle childcare during forest fire season,” say, “I use the previous literature on how working parents juggling childcare and the previous ethnographic studies of firefighters to explore how firefighters juggle childcare during forest fire season.” You can even add, “To my knowledge, no one has conducted an ethnographic study in this specific area, although what we have learned from X about childcare and from Y about firefighters would lead us to expect Z here.” Read more literature review sections to see how others have described the “gaps” they are filling.
Use Concept Mapping
Concept mapping is a helpful tool for getting your thoughts in order and is particularly helpful when thinking about the “literature” foundational to your particular study. Concept maps are also known as mind maps, which is a delightful way to think about them. Your brain is probably abuzz with competing ideas in the early stages of your research design. Write/draw them on paper, and then try to categorize and move the pieces around into “clusters” that make sense to you. Going back to the gymnasts example, my student might have begun by jotting down random words of interest: gymnasts * sports * coaches * female gymnasts * stress * injury * don’t complain * women in sports * bad coaching * anxiety/stress * careers in sports * pain. She could then have begun clustering these into relational categories (bad coaching, don’t complain culture) and simple “event” categories (injury, stress). This might have led her to think about reviewing literature in these two separate aspects and then literature that put them together. There is no correct way to draw a concept map, as they are wonderfully specific to your mind. There are many examples you can find online.
Ask Yourself, “How Is This Sociology (or Political Science or Public Policy, Etc.)?”
Rubin ( 2021:82 ) offers this suggestion instead of asking yourself the “So what?” question to get you thinking about what bridges there are between your study and the body of research in your particular discipline. This is particularly helpful for thinking about theory. Rubin further suggests that if you are really stumped, ask yourself, “What is the really big question that all [fill in your discipline here] care about?” For sociology, it might be “inequality,” which would then help you think about theories of inequality that might be helpful in framing your study on whatever it is you are studying—OnlyFans? Childcare during COVID? Aging in America? I can think of some interesting ways to frame questions about inequality for any of those topics. You can further narrow it by focusing on particular aspects of inequality (Gender oppression? Racial exclusion? Heteronormativity?). If your discipline is public policy, the big questions there might be, How does policy get enacted, and what makes a policy effective? You can then take whatever your particular policy interest is—tax reform, student debt relief, cap-and-trade regulations—and apply those big questions. Doing so would give you a handle on what is otherwise an intolerably vague subject (e.g., What about student debt relief?).
Sometimes finding you are in new territory means you’ve hit the jackpot, and sometimes it means you’ve traveled out of bounds for your discipline. The jackpot scenario is wonderful. You are doing truly innovative research that is combining multiple literatures or is addressing a new or under-examined phenomenon of interest, and your research has the potential to be groundbreaking. Congrats! But that’s really hard to do, and it might be more likely that you’ve traveled out of bounds, by which I mean, you are no longer in your discipline . It might be that no one has written about this thing—at least within your field— because no one in your field actually cares about this topic . ( Rubin 2021:83 ; emphases added)
Don’t Treat This as a Chore
Don’t treat the literature review as a chore that has to be completed, but see it for what it really is—you are building connections to other researchers out there. You want to represent your discipline or area of study fairly and adequately. Demonstrate humility and your knowledge of previous research. Be part of the conversation.
Supplement: Two More Literature Review Examples
Elites by harvey ( 2011 ).
In the last two decades, there has been a small but growing literature on elites. In part, this has been a result of the resurgence of ethnographic research such as interviews, focus groups, case studies, and participant observation but also because scholars have become increasingly interested in understanding the perspectives and behaviors of leaders in business, politics, and society as a whole. Yet until recently, our understanding of some of the methodological challenges of researching elites has lagged behind our rush to interview them.
There is no clear-cut definition of the term elite, and given its broad understanding across the social sciences, scholars have tended to adopt different approaches. Zuckerman (1972) uses the term ultraelites to describe individuals who hold a significant amount of power within a group that is already considered elite. She argues, for example, that US senators constitute part of the country’s political elite but that among them are the ultraelites: a “subset of particularly powerful or prestigious influentials” (160). She suggests that there is a hierarchy of status within elite groups. McDowell (1998) analyses a broader group of “professional elites” who are employees working at different levels for merchant and investment banks in London. She classifies this group as elite because they are “highly skilled, professionally competent, and class-specific” (2135). Parry (1998:2148) uses the term hybrid elites in the context of the international trade of genetic material because she argues that critical knowledge exists not in traditional institutions “but rather as increasingly informal, hybridised, spatially fragmented, and hence largely ‘invisible,’ networks of elite actors.” Given the undertheorization of the term elite, Smith (2006) recognizes why scholars have shaped their definitions to match their respondents . However, she is rightly critical of the underlying assumption that those who hold professional positions necessarily exert as much influence as initially perceived. Indeed, job titles can entirely misrepresent the role of workers and therefore are by no means an indicator of elite status (Harvey 2010).
Many scholars have used the term elite in a relational sense, defining them either in terms of their social position compared to the researcher or compared to the average person in society (Stephens 2007). The problem with this definition is there is no guarantee that an elite subject will necessarily translate this power and authority in an interview setting. Indeed, Smith (2006) found that on the few occasions she experienced respondents wanting to exert their authority over her, it was not from elites but from relatively less senior workers. Furthermore, although business and political elites often receive extensive media training, they are often scrutinized by television and radio journalists and therefore can also feel threatened in an interview, particularly in contexts that are less straightforward to prepare for such as academic interviews. On several occasions, for instance, I have been asked by elite respondents or their personal assistants what they need to prepare for before the interview, which suggests that they consider the interview as some form of challenge or justification for what they do.
In many cases, it is not necessarily the figureheads or leaders of organizations and institutions who have the greatest claim to elite status but those who hold important social networks, social capital, and strategic positions within social structures because they are better able to exert influence (Burt 1992; Parry 1998; Smith 2005; Woods 1998). An elite status can also change, with people both gaining and losing theirs over time. In addition, it is geographically specific, with people holding elite status in some but not all locations. In short, it is clear that the term elite can mean many things in different contexts, which explains the range of definitions. The purpose here is not to critique these other definitions but rather to highlight the variety of perspectives.
When referring to my research, I define elites as those who occupy senior-management- and board-level positions within organizations. This is a similar scope of definition to Zuckerman’s (1972) but focuses on a level immediately below her ultraelite subjects. My definition is narrower than McDowell’s (1998) because it is clear in the context of my research that these people have significant decision-making influence within and outside of the firm and therefore present a unique challenge to interview. I deliberately use the term elite more broadly when drawing on examples from the theoretical literature in order to compare my experiences with those who have researched similar groups.
”Changing Dispositions among the Upwardly Mobile” by Curl, Lareau, and Wu ( 2018 )
There is growing interest in the role of cultural practices in undergirding the social stratification system. For example, Lamont et al. (2014) critically assess the preoccupation with economic dimensions of social stratification and call for more developed cultural models of the transmission of inequality. The importance of cultural factors in the maintenance of social inequality has also received empirical attention from some younger scholars, including Calarco (2011, 2014) and Streib (2015). Yet questions remain regarding the degree to which economic position is tied to cultural sensibilities and the ways in which these cultural sensibilities are imprinted on the self or are subject to change. Although habitus is a core concept in Bourdieu’s theory of social reproduction, there is limited empirical attention to the precise areas of the habitus that can be subject to change during upward mobility as well as the ramifications of these changes for family life.
In Bourdieu’s (1984) highly influential work on the importance of class-based cultural dispositions, habitus is defined as a “durable system of dispositions” created in childhood. The habitus provides a “matrix of perceptions” that seems natural while also structuring future actions and pathways. In many of his writings, Bourdieu emphasized the durability of cultural tastes and dispositions and did not consider empirically whether these dispositions might be changed or altered throughout one’s life (Swartz 1997). His theoretical work does permit the possibility of upward mobility and transformation, however, through the ability of the habitus to “improvise” or “change” due to “new experiences” (Friedman 2016:131). Researchers have differed in opinion on the durability of the habitus and its ability to change (King 2000). Based on marital conflict in cross-class marriages, for instance, Streib (2015) argues that cultural dispositions of individuals raised in working-class families are deeply embedded and largely unchanging. In a somewhat different vein, Horvat and Davis (2011:152) argue that young adults enrolled in an alternative educational program undergo important shifts in their self-perception, such as “self-esteem” and their “ability to accomplish something of value.” Others argue there is variability in the degree to which habitus changes dependent on life experience and personality (Christodoulou and Spyridakis 2016). Recently, additional studies have investigated the habitus as it intersects with lifestyle through the lens of meaning making (Ambrasat et al. 2016). There is, therefore, ample discussion of class-based cultural practices in self-perception (Horvat and Davis 2011), lifestyle (Ambrasat et al. 2016), and other forms of taste (Andrews 2012; Bourdieu 1984), yet researchers have not sufficiently delineated which aspects of the habitus might change through upward mobility or which specific dimensions of life prompt moments of class-based conflict.
Bourdieu (1999:511; 2004) acknowledged simmering tensions between the durable aspects of habitus and those aspects that have been transformed—that is, a “fractured” or “cleft” habitus. Others have explored these tensions as a “divided” or “fragmented” habitus (Baxter and Britton 2001; Lee and Kramer 2013). Each of these conceptions of the habitus implies that changes in cultural dispositions are possible but come with costs. Exploration of the specific aspects of one’s habitus that can change and generate conflict contributes to this literature.
Scholars have also studied the costs associated with academic success for working-class undergraduates (Hurst 2010; Lee and Kramer 2013; London 1989; Reay 2017; Rondini 2016; Stuber 2011), but we know little about the lasting effects on adults. For instance, Lee and Kramer (2013) point to cross-class tensions as family and friends criticize upwardly mobile individuals for their newly acquired cultural dispositions. Documenting the tension many working-class students experience with their friends and families of origin, they find that the source of their pain or struggle is “shaped not only by their interactions with non-mobile family and friends but also within their own minds, by their own assessments of their social positions, and by how those positions are interpreted by others” (Lee and Kramer 2013:29). Hurst (2010) also explores the experiences of undergraduates who have been academically successful and the costs associated with that success. She finds that decisions about “class allegiance and identity” are required aspects of what it means to “becom[e] educated” (4) and that working-class students deal with these cultural changes differently. Jack (2014, 2016) also argues that there is diversity among lower-income students, which yields varied college experiences. Naming two groups, the “doubly disadvantaged” and the “privileged poor,” he argues that previous experience with “elite environments” (2014:456) prior to college informs students’ ability to take on dominant cultural practices, particularly around engagement, such as help seeking or meeting with professors (2016). These studies shed light on the role college might play as a “lever for mobility” (2016:15) and discuss the pain and difficulty associated with upward mobility among undergraduates, but the studies do not illuminate how these tensions unfold in adulthood. Neither have they sufficiently addressed potential enduring tensions with extended family members as well as the specific nature of the difficulties.
Some scholars point to the positive outcomes upwardly mobile youth (Lehmann 2009) and adults (Stuber 2005) experience when they maintain a different habitus than their newly acquired class position, although, as Jack (2014, 2016) shows, those experiences may vary depending on one’s experience with elite environments in their youth. Researchers have not sufficiently explored the specific aspects of the habitus that upwardly mobile adults change or the conflicts that emerge with family and childhood friends as they reach adulthood and experience colliding social worlds. We contribute to this scholarship with clear examples of self-reported changes to one’s cultural dispositions in three specific areas: “horizons,” food and health, and communication. We link these changes to enduring tension with family members, friends, and colleagues and explore varied responses to this tension based on race.
Further Readings
Bloomberg, Linda Dale, and Marie F. Volpe. 2012. Completing Your Qualitative Dissertation: A Road Map from Beginning to End . 2nd ed. Thousand Oaks, CA: SAGE. In keeping with its general approach to qualitative research, includes a “road map” for conducting a literature review.
Hart, Chris. 1998. Doing a Literature Review: Releasing the Social Science Research Imagination . London: SAGE. A how-to book dedicated entirely to conducting a literature review from a British perspective. Useful for both undergraduate and graduate students.
Machi, Lawrence A., and Brenda T. McEvoy. 2022. The Literature Review: Six Steps to Success . 4th ed. Newbury Park, CA: Corwin. A well-organized guidebook complete with reflection sections to prompt successful thinking about your literature review.
Ridley, Diana. 2008. The Literature Review: A Step-by-Step Guide for Students . London: SAGE. A highly recommended companion to conducting a literature review for doctoral-level students.
The process of systematically searching through pre-existing studies (“literature”) on the subject of research; also, the section of a presentation in which the pre-existing literature is discussed.
Follow-up questions used in a semi-structured interview to elicit further elaboration. Suggested prompts can be included in the interview guide to be used/deployed depending on how the initial question was answered or if the topic of the prompt does not emerge spontaneously.
A tool for identifying relationships among ideas by visually representing them on paper. Most concept maps depict ideas as boxes or circles (also called nodes), which are structured hierarchically and connected with lines or arrows (also called arcs). These lines are labeled with linking words and phrases to help explain the connections between concepts. Also known as mind mapping.
The people who are the subjects of an interview-based qualitative study. In general, they are also known as the participants, and for purposes of IRBs they are often referred to as the human subjects of the research.
Introduction to Qualitative Research Methods Copyright © 2023 by Allison Hurst is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License , except where otherwise noted.
Dissertations and research projects
- Book a session
- Planning your research
Developing a theoretical framework
Reflecting on your position, extended literature reviews, presenting qualitative data.
- Quantitative research
- Writing up your research project
- e-learning and books
- SkillsCheck This link opens in a new window
- ⬅ Back to Skills Centre This link opens in a new window
- Review this resource
What is a theoretical framework?
Developing a theoretical framework for your dissertation is one of the key elements of a qualitative research project. Through writing your literature review, you are likely to have identified either a problem that need ‘fixing’ or a gap that your research may begin to fill.
The theoretical framework is your toolbox . In the toolbox are your handy tools: a set of theories, concepts, ideas and hypotheses that you will use to build a solution to the research problem or gap you have identified.
The methodology is the instruction manual: the procedure and steps you have taken, using your chosen tools, to tackle the research problem.
Why do I need a theoretical framework?
Developing a theoretical framework shows that you have thought critically about the different ways to approach your topic, and that you have made a well-reasoned and evidenced decision about which approach will work best. theoretical frameworks are also necessary for solving complex problems or issues from the literature, showing that you have the skills to think creatively and improvise to answer your research questions. they also allow researchers to establish new theories and approaches, that future research may go on to develop., how do i create a theoretical framework for my dissertation.
First, select your tools. You are likely to need a variety of tools in qualitative research – different theories, models or concepts – to help you tackle different parts of your research question.

When deciding what tools would be best for the job of answering your research questions or problem, explore what existing research in your area has used. You may find that there is a ‘standard toolbox’ for qualitative research in your field that you can borrow from or apply to your own research.
You will need to justify why your chosen tools are best for the job of answering your research questions, at what stage they are most relevant, and how they relate to each other. Some theories or models will neatly fit together and appear in the toolboxes of other researchers. However, you may wish to incorporate a model or idea that is not typical for your research area – the ‘odd one out’ in your toolbox. If this is the case, make sure you justify and account for why it is useful to you, and look for ways that it can be used in partnership with the other tools you are using.
You should also be honest about limitations, or where you need to improvise (for example, if the ‘right’ tool or approach doesn’t exist in your area).
This video from the Skills Centre includes an overview and example of how you might create a theoretical framework for your dissertation:
How do I choose the 'right' approach?
When designing your framework and choosing what to include, it can often be difficult to know if you’ve chosen the ‘right’ approach for your research questions. One way to check this is to look for consistency between your objectives, the literature in your framework, and your overall ethos for the research. This means ensuring that the literature you have used not only contributes to answering your research objectives, but that you also use theories and models that are true to your beliefs as a researcher.
Reflecting on your values and your overall ambition for the project can be a helpful step in making these decisions, as it can help you to fully connect your methodology and methods to your research aims.
Should I reflect on my position as a researcher?
If you feel your position as a researcher has influenced your choice of methods or procedure in any way, the methodology is a good place to reflect on this. Positionality acknowledges that no researcher is entirely objective: we are all, to some extent, influenced by prior learning, experiences, knowledge, and personal biases. This is particularly true in qualitative research or practice-based research, where the student is acting as a researcher in their own workplace, where they are otherwise considered a practitioner/professional. It's also important to reflect on your positionality if you belong to the same community as your participants where this is the grounds for their involvement in the research (ie. you are a mature student interviewing other mature learners about their experences in higher education).
The following questions can help you to reflect on your positionality and gauge whether this is an important section to include in your dissertation (for some people, this section isn’t necessary or relevant):
- How might my personal history influence how I approach the topic?
- How am I positioned in relation to this knowledge? Am I being influenced by prior learning or knowledge from outside of this course?
- How does my gender/social class/ ethnicity/ culture influence my positioning in relation to this topic?
- Do I share any attributes with my participants? Are we part of a s hared community? How might this have influenced our relationship and my role in interviews/observations?
- Am I invested in the outcomes on a personal level? Who is this research for and who will feel the benefits?
One option for qualitative projects is to write an extended literature review. This type of project does not require you to collect any new data. Instead, you should focus on synthesising a broad range of literature to offer a new perspective on a research problem or question.
The main difference between an extended literature review and a dissertation where primary data is collected, is in the presentation of the methodology, results and discussion sections. This is because extended literature reviews do not actively involve participants or primary data collection, so there is no need to outline a procedure for data collection (the methodology) or to present and interpret ‘data’ (in the form of interview transcripts, numerical data, observations etc.) You will have much more freedom to decide which sections of the dissertation should be combined, and whether new chapters or sections should be added.
Here is an overview of a common structure for an extended literature review:

Introduction
- Provide background information and context to set the ‘backdrop’ for your project.
- Explain the value and relevance of your research in this context. Outline what do you hope to contribute with your dissertation.
- Clarify a specific area of focus.
- Introduce your research aims (or problem) and objectives.
Literature review
You will need to write a short, overview literature review to introduce the main theories, concepts and key research areas that you will explore in your dissertation. This set of texts – which may be theoretical, research-based, practice-based or policies – form your theoretical framework. In other words, by bringing these texts together in the literature review, you are creating a lens that you can then apply to more focused examples or scenarios in your discussion chapters.
Methodology
As you will not be collecting primary data, your methodology will be quite different from a typical dissertation. You will need to set out the process and procedure you used to find and narrow down your literature. This is also known as a search strategy.
Including your search strategy
A search strategy explains how you have narrowed down your literature to identify key studies and areas of focus. This often takes the form of a search strategy table, included as an appendix at the end of the dissertation. If included, this section takes the place of the traditional 'methodology' section.
If you choose to include a search strategy table, you should also give an overview of your reading process in the main body of the dissertation. Think of this as a chronology of the practical steps you took and your justification for doing so at each stage, such as:
- Your key terms, alternatives and synonyms, and any terms that you chose to exclude.
- Your choice and combination of databases;
- Your inclusion/exclusion criteria, when they were applied and why. This includes filters such as language of publication, date, and country of origin;
- You should also explain which terms you combined to form search phrases and your use of Boolean searching (AND, OR, NOT);
- Your use of citation searching (selecting articles from the bibliography of a chosen journal article to further your search).
- Your use of any search models, such as PICO and SPIDER to help shape your approach.
- Search strategy template A simple template for recording your literature searching. This can be included as an appendix to show your search strategy.
The discussion section of an extended literature review is the most flexible in terms of structure. Think of this section as a series of short case studies or ‘windows’ on your research. In this section you will apply the theoretical framework you formed in the literature review – a combination of theories, models and ideas that explain your approach to the topic – to a series of different examples and scenarios. These are usually presented as separate discussion ‘chapters’ in the dissertation, in an order that you feel best fits your argument.
Think about an order for these discussion sections or chapters that helps to tell the story of your research. One common approach is to structure these sections by common themes or concepts that help to draw your sources together. You might also opt for a chronological structure if your dissertation aims to show change or development over time. Another option is to deliberately show where there is a lack of chronology or narrative across your case studies, by ordering them in a fragmentary order! You will be able to reflect upon the structure of these chapters elsewhere in the dissertation, explaining and defending your decision in the methodology and conclusion.
A summary of your key findings – what you have concluded from your research, and how far you have been able to successfully answer your research questions.
- Recommendations – for improvements to your own study, for future research in the area, and for your field more widely.
- Emphasise your contributions to knowledge and what you have achieved.
Alternative structure
Depending on your research aims, and whether you are working with a case-study type approach (where each section of the dissertation considers a different example or concept through the lens established in your literature review), you might opt for one of the following structures:
Splitting the literature review across different chapters:

This structure allows you to pull apart the traditional literature review, introducing it little by little with each of your themed chapters. This approach works well for dissertations that attempt to show change or difference over time, as the relevant literature for that section or period can be introduced gradually to the reader.
Whichever structure you opt for, remember to explain and justify your approach. A marker will be interested in why you decided on your chosen structure, what it allows you to achieve/brings to the project and what alternatives you considered and rejected in the planning process. Here are some example sentence starters:
In qualitative studies, your results are often presented alongside the discussion, as it is difficult to include this data in a meaningful way without explanation and interpretation. In the dsicussion section, aim to structure your work thematically, moving through the key concepts or ideas that have emerged from your qualitative data. Use extracts from your data collection - interviews, focus groups, observations - to illustrate where these themes are most prominent, and refer back to the sources from your literature review to help draw conclusions.
Here's an example of how your data could be presented in paragraph format in this section:
Example from 'Reporting and discussing your findings ', Monash University .
- << Previous: Planning your research
- Next: Quantitative research >>
- Last Updated: Apr 17, 2024 1:52 PM
- URL: https://libguides.shu.ac.uk/researchprojects

Purdue Online Writing Lab Purdue OWL® College of Liberal Arts
Writing a Literature Review

Welcome to the Purdue OWL
This page is brought to you by the OWL at Purdue University. When printing this page, you must include the entire legal notice.
Copyright ©1995-2018 by The Writing Lab & The OWL at Purdue and Purdue University. All rights reserved. This material may not be published, reproduced, broadcast, rewritten, or redistributed without permission. Use of this site constitutes acceptance of our terms and conditions of fair use.
A literature review is a document or section of a document that collects key sources on a topic and discusses those sources in conversation with each other (also called synthesis ). The lit review is an important genre in many disciplines, not just literature (i.e., the study of works of literature such as novels and plays). When we say “literature review” or refer to “the literature,” we are talking about the research ( scholarship ) in a given field. You will often see the terms “the research,” “the scholarship,” and “the literature” used mostly interchangeably.
Where, when, and why would I write a lit review?
There are a number of different situations where you might write a literature review, each with slightly different expectations; different disciplines, too, have field-specific expectations for what a literature review is and does. For instance, in the humanities, authors might include more overt argumentation and interpretation of source material in their literature reviews, whereas in the sciences, authors are more likely to report study designs and results in their literature reviews; these differences reflect these disciplines’ purposes and conventions in scholarship. You should always look at examples from your own discipline and talk to professors or mentors in your field to be sure you understand your discipline’s conventions, for literature reviews as well as for any other genre.
A literature review can be a part of a research paper or scholarly article, usually falling after the introduction and before the research methods sections. In these cases, the lit review just needs to cover scholarship that is important to the issue you are writing about; sometimes it will also cover key sources that informed your research methodology.
Lit reviews can also be standalone pieces, either as assignments in a class or as publications. In a class, a lit review may be assigned to help students familiarize themselves with a topic and with scholarship in their field, get an idea of the other researchers working on the topic they’re interested in, find gaps in existing research in order to propose new projects, and/or develop a theoretical framework and methodology for later research. As a publication, a lit review usually is meant to help make other scholars’ lives easier by collecting and summarizing, synthesizing, and analyzing existing research on a topic. This can be especially helpful for students or scholars getting into a new research area, or for directing an entire community of scholars toward questions that have not yet been answered.
What are the parts of a lit review?
Most lit reviews use a basic introduction-body-conclusion structure; if your lit review is part of a larger paper, the introduction and conclusion pieces may be just a few sentences while you focus most of your attention on the body. If your lit review is a standalone piece, the introduction and conclusion take up more space and give you a place to discuss your goals, research methods, and conclusions separately from where you discuss the literature itself.
Introduction:
- An introductory paragraph that explains what your working topic and thesis is
- A forecast of key topics or texts that will appear in the review
- Potentially, a description of how you found sources and how you analyzed them for inclusion and discussion in the review (more often found in published, standalone literature reviews than in lit review sections in an article or research paper)
- Summarize and synthesize: Give an overview of the main points of each source and combine them into a coherent whole
- Analyze and interpret: Don’t just paraphrase other researchers – add your own interpretations where possible, discussing the significance of findings in relation to the literature as a whole
- Critically Evaluate: Mention the strengths and weaknesses of your sources
- Write in well-structured paragraphs: Use transition words and topic sentence to draw connections, comparisons, and contrasts.
Conclusion:
- Summarize the key findings you have taken from the literature and emphasize their significance
- Connect it back to your primary research question
How should I organize my lit review?
Lit reviews can take many different organizational patterns depending on what you are trying to accomplish with the review. Here are some examples:
- Chronological : The simplest approach is to trace the development of the topic over time, which helps familiarize the audience with the topic (for instance if you are introducing something that is not commonly known in your field). If you choose this strategy, be careful to avoid simply listing and summarizing sources in order. Try to analyze the patterns, turning points, and key debates that have shaped the direction of the field. Give your interpretation of how and why certain developments occurred (as mentioned previously, this may not be appropriate in your discipline — check with a teacher or mentor if you’re unsure).
- Thematic : If you have found some recurring central themes that you will continue working with throughout your piece, you can organize your literature review into subsections that address different aspects of the topic. For example, if you are reviewing literature about women and religion, key themes can include the role of women in churches and the religious attitude towards women.
- Qualitative versus quantitative research
- Empirical versus theoretical scholarship
- Divide the research by sociological, historical, or cultural sources
- Theoretical : In many humanities articles, the literature review is the foundation for the theoretical framework. You can use it to discuss various theories, models, and definitions of key concepts. You can argue for the relevance of a specific theoretical approach or combine various theorical concepts to create a framework for your research.
What are some strategies or tips I can use while writing my lit review?
Any lit review is only as good as the research it discusses; make sure your sources are well-chosen and your research is thorough. Don’t be afraid to do more research if you discover a new thread as you’re writing. More info on the research process is available in our "Conducting Research" resources .
As you’re doing your research, create an annotated bibliography ( see our page on the this type of document ). Much of the information used in an annotated bibliography can be used also in a literature review, so you’ll be not only partially drafting your lit review as you research, but also developing your sense of the larger conversation going on among scholars, professionals, and any other stakeholders in your topic.
Usually you will need to synthesize research rather than just summarizing it. This means drawing connections between sources to create a picture of the scholarly conversation on a topic over time. Many student writers struggle to synthesize because they feel they don’t have anything to add to the scholars they are citing; here are some strategies to help you:
- It often helps to remember that the point of these kinds of syntheses is to show your readers how you understand your research, to help them read the rest of your paper.
- Writing teachers often say synthesis is like hosting a dinner party: imagine all your sources are together in a room, discussing your topic. What are they saying to each other?
- Look at the in-text citations in each paragraph. Are you citing just one source for each paragraph? This usually indicates summary only. When you have multiple sources cited in a paragraph, you are more likely to be synthesizing them (not always, but often
- Read more about synthesis here.
The most interesting literature reviews are often written as arguments (again, as mentioned at the beginning of the page, this is discipline-specific and doesn’t work for all situations). Often, the literature review is where you can establish your research as filling a particular gap or as relevant in a particular way. You have some chance to do this in your introduction in an article, but the literature review section gives a more extended opportunity to establish the conversation in the way you would like your readers to see it. You can choose the intellectual lineage you would like to be part of and whose definitions matter most to your thinking (mostly humanities-specific, but this goes for sciences as well). In addressing these points, you argue for your place in the conversation, which tends to make the lit review more compelling than a simple reporting of other sources.
A Guide to Writing a Qualitative Systematic Review Protocol to Enhance Evidence-Based Practice in Nursing and Health Care
Affiliations.
- 1 PhD candidate, School of Nursing and Midwifey, Monash University, and Clinical Nurse Specialist, Adult and Pediatric Intensive Care Unit, Monash Health, Melbourne, Victoria, Australia.
- 2 Lecturer, School of Nursing and Midwifery, Monash University, Melbourne, Victoria, Australia.
- 3 Senior Lecturer, School of Nursing and Midwifery, Monash University, Melbourne, Victoria, Australia.
- PMID: 26790142
- DOI: 10.1111/wvn.12134
Background: The qualitative systematic review is a rapidly developing area of nursing research. In order to present trustworthy, high-quality recommendations, such reviews should be based on a review protocol to minimize bias and enhance transparency and reproducibility. Although there are a number of resources available to guide researchers in developing a quantitative review protocol, very few resources exist for qualitative reviews.
Aims: To guide researchers through the process of developing a qualitative systematic review protocol, using an example review question.
Methodology: The key elements required in a systematic review protocol are discussed, with a focus on application to qualitative reviews: Development of a research question; formulation of key search terms and strategies; designing a multistage review process; critical appraisal of qualitative literature; development of data extraction techniques; and data synthesis. The paper highlights important considerations during the protocol development process, and uses a previously developed review question as a working example.
Implications for research: This paper will assist novice researchers in developing a qualitative systematic review protocol. By providing a worked example of a protocol, the paper encourages the development of review protocols, enhancing the trustworthiness and value of the completed qualitative systematic review findings.
Linking evidence to action: Qualitative systematic reviews should be based on well planned, peer reviewed protocols to enhance the trustworthiness of results and thus their usefulness in clinical practice. Protocols should outline, in detail, the processes which will be used to undertake the review, including key search terms, inclusion and exclusion criteria, and the methods used for critical appraisal, data extraction and data analysis to facilitate transparency of the review process. Additionally, journals should encourage and support the publication of review protocols, and should require reference to a protocol prior to publication of the review results.
Keywords: guidelines; meta synthesis; qualitative; systematic review protocol.
© 2016 Sigma Theta Tau International.
- Evidence-Based Practice / standards*
- Information Seeking Behavior
- Nursing / methods
- Qualitative Research*
- Research Design / standards*
- Systematic Reviews as Topic*
- Writing / standards*
Starting Literature Review in Qualitative Research: An Illustration Using the Mirror Effect
- First Online: 05 January 2019
Cite this chapter

- Wing Yee Ho 4
1146 Accesses
1 Citations
Mirroring is a group phenomenon. Through action, people can recognize themselves, or a characteristic of themselves (usually the repressed side), reflected in the verbal and nonverbal behaviors in others as if they were looking into a mirror. It is a fundamental process in the development of the ego. By distinguishing themselves from others, clients discover their own identity, which is what makes them individual. Positive, benign mirroring is implemented as a way to develop new self-image through the “constructive act of recognizing self in others, and others in self….
This is a preview of subscription content, log in via an institution to check access.
Access this chapter
- Available as EPUB and PDF
- Read on any device
- Instant download
- Own it forever
- Compact, lightweight edition
- Dispatched in 3 to 5 business days
- Free shipping worldwide - see info
Tax calculation will be finalised at checkout
Purchases are for personal use only
Institutional subscriptions
Amsterdam, B. (1972). Mirror self-image reactions before age two. Developmental Psychology, 5 (4), 297–305.
Article Google Scholar
Asendorpf, J. B., & Baudonnaiere, P. M. (1993). Self-awareness and other-awareness: Mirror self-recognition and synchronic imitation among unfamiliar peers. Developmental Psychology, 29 (1), 88–95.
Berger, M. (2012). The dynamics of mirror reactions and their impact on the analytic group. In J. L. Kleinberg (Ed.), The Wiley-Blackwell handbook of group psychotherapy (pp. 197–216). Madlen: Wiley.
Google Scholar
Bertenthal, B. I., & Longo, M. R. (2007). Is there evidence of a mirror system from birth? Developmental Science, 10 (5), 526–529.
Blatner, A. (2000). Foundations of psychodrama: History, theory, and practice (4th ed.). New York: Springer.
Bolton, G. (1984). Drama as Education . London: Longman.
Bulmer, M. (1979). Concepts in the analysis of qualitative data. Sociological Review, 27 (4), 651–677.
Chazan, R. (2001). The group as therapist . London: Jessica Kingsley.
Comer, J. S., & Kendall, P. C. (2013). Methodology, design, and evaluation in psychotherapy research. In M. J. Lambert (Ed.), Bergin and Garfield’s handbook of psychotherapy and behavior change (6th ed., pp. 21–48). New York, NY: Wiley.
Coon, D., & Mitterer, J. O. (2014). Psychology: Modules for active learning (13th ed.). Stamford: Cengage Learning.
Cottrell, R., & McKenzie, J. F. (2011). Health promotion and education research methods: Using the five-chapter thesis/dissertation model . Sudbury: Jones and Bartlett.
de Hamilton, A. F. C. (2008). Emulation and mimicry for social interaction: a theoretical approach to imitation in autism. The Quarterly Journal of Experimental Psychology, 61 (1), 101–115.
Di Pellegrino, G., Fadiga, L., Fogassi, L., Gallese, V., & Rizzolatti, G. (1992). Understanding motor events: A neurophysiological study. Experimental Brain Research, 91, 176–180.
Djurić, Z., Veljković, J., & Tomić, M. (2006). Psychodrama: A beginner’s guide . London: Jessica Kingsley Publishers.
Farmer, C., & Geller, M. (2003). Applying psychodrama in the family systems therapy of Bowen. In J. Gershoni (Ed.), Psychodrama in the 21st century: Clinical and educational applications (pp. 31–48). New York: Springer.
Glaser, B., & Strauss, A. (1967). The discovery of grounded theory: Strategies for qualitative research . Chicago, IL: Aldine.
Gallese, V., Rochat, M. J., & Berchio, C. (2013). The mirror mechanism and its potential role in autism spectrum disorder. Developmental Medicine and Child Neurology, 55 (1), 15–22.
Gallup, G. G., Jr. (1970). Chimpanzees: Self recognition. Science, 167 (3914), 86–87.
Karp, M. (2003). An introduction to psychodrama. In M. Karp, P. Holmes, & K. B. Tauvon (Eds.), The handbook of psychodrama (pp. 3–13). London, New York: Brunner-Routledge.
Katagiri, M., Inada, N., & Kamio, Y. (2010). Mirroring effect in 2- and 3-year-olds with autism spectrum disorder. Research in Autism Spectrum Disorders, 4 (3), 474–478.
Kellermann, P. F. (2000). The therapeutic aspects of psychodrama with traumatized people. In P. F. Kellermann & M. K. Hudgins (Eds.), Psychodrama with trauma survivors: Acting out your pain (pp. 23–40). London: Jessica Kingsley Publishers.
Kellermann, P. F. (2007). Let’s face it: Mirroring in psychodrama. In C. Baim, J. Burmeister, & M. Maciel (Eds.), Psychodrama: Advances in theory and practice (pp. 83–95). London: Routledge.
Kumar, R. (2014). Research methodology: A step by step guide for beginners (4th ed.). New Delhi, India: Sage.
Lacoboni, M. (2009). Mirroring people: The new science of how we connect with others . New York: Picador.
Leveton, E. (2001). A clinician’s guide to psychodrama (3rd ed.). New York: Springer.
Lewis, M., & Brooks-Gunn, J. (1979). Social cognition and the acquisition of self . New York: Plenum Press.
Book Google Scholar
Lewis, M., & Ramsay, D. (2004). Development of self-recognition, personal pronoun use, and pretend play during the 2nd year. Child Development, 75 (6), 1821–1831.
Lichtenberg, J. D. (1982). Reflections on the first year of life. Psychoanalytic Inquiry, 1 (4), 695–729.
Lichtenberg, J. D. (1985). Mirrors and mirroring: Developmental experiences. Psychoanalytic Inquiry, 5 (2), 199–210.
Lichtenberg, J. D. (1989). Psychoanalysis and motivation . Hillsdale: The Analytic Press.
Lo, T. W., & Ho, W. Y. (2012). Action therapy: Application of psychodrama in teaching counseling in Hong Kong tertiary education. DaTEAsia, 3, 93–110. [In Chinese].
Lousada, O. (2005). The three-layered cake, butter with everything. In M. Karp, P. Holmes, & K. B. Tauvon (Eds.), The handbook of psychodrama (pp. 213–236). London, New York: Brunner-Routledge.
McGarry, L. M., & Russo, F. A. (2011). Mirroring in dance/movement therapy: Potential mechanisms behind empathy enhancement. The Arts in Psychotherapy, 38 (3), 178–184.
Moreno, J. L. (1946). Psychodrama: First volume . Beacon: Beacon House.
Moreno, J. L., & Moreno, Z. T. (1969). Psychodrama: Third volume, action therapy and principles of practice . Beacon: Beacon House.
Nolte, J. (2012). Non-clinical psychodrama: Lawyers and the psychodramatic method. The Journal of Psychodrama, Sociometry and Group Psychotherapy, 60 (2), 7–14.
Oberman, L. M., & Ramachandran, V. S. (2009). Reflections on the mirror neuron system: Their evolutionary functions beyond motor representation. In J. A. Pineda (Ed.), Mirror neuron systems the role of mirroring processes in social cognition (pp. 39–62). New York, NY: Humana Press.
Pan, M. L. (2008). Literature reviews: Qualitative and quantitative approaches (3rd ed.). Glendale: Pryezak Publishing.
Paul, O. (2012). Succeeding with your literature review: A handbook for students . New York: Open University Press.
Peterson, J. (2003). The synergism of art therapy and psychodrama. In J. Gershoni (Ed.), Psychodrama in the 21st century: Clinical and educational applications (pp. 81–102). New York: Springer.
Povinelli, D. J., & Prince, C. G. (1998). In M. Ferrari & R. J. Sternberg (Eds.), Self-awareness: Its nature and development (pp. 39–108). New York: The Guilford Press.
Rizzolatti, G., & Craighero, L. (2004). The mirror-neuron system. Annual Review of Neuroscience, 27, 169–192.
Rizzolatti, G., Fogassi, L., & Gallese, V. (2006). Mirrors in the mind. Scientific American, 295 (5), 54–61.
Rosen, L. H., & Patterson, M. M. (2011). The self and identity. In M. K. Underwood & L. H. Rosen (Eds.), Social development: Relationships in infancy, childhood, and adolescence (pp. 73–100). New York: The Guilford Press.
Tauvon, K. B. (2003). Principles of psychodrama. In M. Karp, P. Holmes, & K. B. Tauvon (Eds.), The handbook of psychodrama (pp. 29–46). London, New York: Routledge.
Tolson, E. R., Reid, W. J., & Garvin, C. D. (2003). Generalist practice: A task-centred approach . New York: Columbia University Press.
Download references
Author information
Authors and affiliations.
Department of Social and Behavioural Sciences, City University of Hong Kong, Tat Chee Avenue, Kowloon Tong, Hong Kong, China
Wing Yee Ho
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Wing Yee Ho .
Editor information
Editors and affiliations.
Faculty of Education, Beijing Normal University, Beijing, China
Kwok Kuen Tsang
Faculty of Social Sciences, University of Stavanger, Stavanger, Norway
School of Humanities, Southeast University, Nanjing, Jiangsu, China
Rights and permissions
Reprints and permissions
Copyright information
© 2019 Springer Nature Singapore Pte Ltd.
About this chapter
Ho, W.Y. (2019). Starting Literature Review in Qualitative Research: An Illustration Using the Mirror Effect. In: Tsang, K., Liu, D., Hong, Y. (eds) Challenges and Opportunities in Qualitative Research. Springer, Singapore. https://doi.org/10.1007/978-981-13-5811-1_2
Download citation
DOI : https://doi.org/10.1007/978-981-13-5811-1_2
Published : 05 January 2019
Publisher Name : Springer, Singapore
Print ISBN : 978-981-13-5810-4
Online ISBN : 978-981-13-5811-1
eBook Packages : Social Sciences Social Sciences (R0)
Share this chapter
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Publish with us
Policies and ethics
- Find a journal
- Track your research
University Libraries
- Research Guides
- Blackboard Learn
- Interlibrary Loan
- Study Rooms
- University of Arkansas
Literature Reviews
- Qualitative or Quantitative?
- Getting Started
- Finding articles
- Primary sources? Peer-reviewed?
- Review Articles/ Annual Reviews...?
- Books, ebooks, dissertations, book reviews
Qualitative researchers TEND to:
Researchers using qualitative methods tend to:
- t hink that social sciences cannot be well-studied with the same methods as natural or physical sciences
- feel that human behavior is context-specific; therefore, behavior must be studied holistically, in situ, rather than being manipulated
- employ an 'insider's' perspective; research tends to be personal and thereby more subjective.
- do interviews, focus groups, field research, case studies, and conversational or content analysis.

Image from https://www.editage.com/insights/qualitative-quantitative-or-mixed-methods-a-quick-guide-to-choose-the-right-design-for-your-research?refer-type=infographics
Qualitative Research (an operational definition)
Qualitative Research: an operational description
Purpose : explain; gain insight and understanding of phenomena through intensive collection and study of narrative data
Approach: inductive; value-laden/subjective; holistic, process-oriented
Hypotheses: tentative, evolving; based on the particular study
Lit. Review: limited; may not be exhaustive
Setting: naturalistic, when and as much as possible
Sampling : for the purpose; not necessarily representative; for in-depth understanding
Measurement: narrative; ongoing
Design and Method: flexible, specified only generally; based on non-intervention, minimal disturbance, such as historical, ethnographic, or case studies
Data Collection: document collection, participant observation, informal interviews, field notes
Data Analysis: raw data is words/ ongoing; involves synthesis
Data Interpretation: tentative, reviewed on ongoing basis, speculative
- Qualitative research with more structure and less subjectivity
- Increased application of both strategies to the same study ("mixed methods")
- Evidence-based practice emphasized in more fields (nursing, social work, education, and others).
Some Other Guidelines
- Guide for formatting Graphs and Tables
- Critical Appraisal Checklist for an Article On Qualitative Research
Quantitative researchers TEND to:
Researchers using quantitative methods tend to:
- think that both natural and social sciences strive to explain phenomena with confirmable theories derived from testable assumptions
- attempt to reduce social reality to variables, in the same way as with physical reality
- try to tightly control the variable(s) in question to see how the others are influenced.
- Do experiments, have control groups, use blind or double-blind studies; use measures or instruments.

Quantitative Research (an operational definition)
Quantitative research: an operational description
Purpose: explain, predict or control phenomena through focused collection and analysis of numberical data
Approach: deductive; tries to be value-free/has objectives/ is outcome-oriented
Hypotheses : Specific, testable, and stated prior to study
Lit. Review: extensive; may significantly influence a particular study
Setting: controlled to the degree possible
Sampling: uses largest manageable random/randomized sample, to allow generalization of results to larger populations
Measurement: standardized, numberical; "at the end"
Design and Method: Strongly structured, specified in detail in advance; involves intervention, manipulation and control groups; descriptive, correlational, experimental
Data Collection: via instruments, surveys, experiments, semi-structured formal interviews, tests or questionnaires
Data Analysis: raw data is numbers; at end of study, usually statistical
Data Interpretation: formulated at end of study; stated as a degree of certainty
This page on qualitative and quantitative research has been adapted and expanded from a handout by Suzy Westenkirchner. Used with permission.
Images from https://www.editage.com/insights/qualitative-quantitative-or-mixed-methods-a-quick-guide-to-choose-the-right-design-for-your-research?refer-type=infographics.
- << Previous: Books, ebooks, dissertations, book reviews
- Last Updated: Jan 8, 2024 2:51 PM
- URL: https://uark.libguides.com/litreview
- See us on Instagram
- Follow us on Twitter
- Phone: 479-575-4104

Literature Review
Literature review is important because it:
- Provides ideas about what should be studied;
- Helps us conduct inquires that have not already been done
- Connects our research to existing studies
But…doing a literature review is not simply summarizing (or copying) what you think is related and useful to your work. BEING CRITICAL AND CAREFUL IS A MUST !
In reviewing existing literature, you may try to look for gaps in the field and rework your study in a different setting or with different people. Nonetheless, literature review is a continuous sense-making process -- you need to review the literature continuously in order to organize your thoughts and refine your analysis.
A good literature review should be able to:
- Connect to your research questions
- Connect to your choice of methods and research design
- Support your data analysis
- Help you draw conclusions and make claims about your research.
Selecting your literature with a purpose
It is impossible to read everything, so when selecting literature for reviewing, consider these:
- Is it relevant to your topic/field of study?
- Is it a primary source from the researcher(s) or secondary source (e.g. a summary you read in a book about someone’s research)?
- Is it updated?
Nature of literatures:
Your literature review can be of different dimensions. Each has its foci and purposes
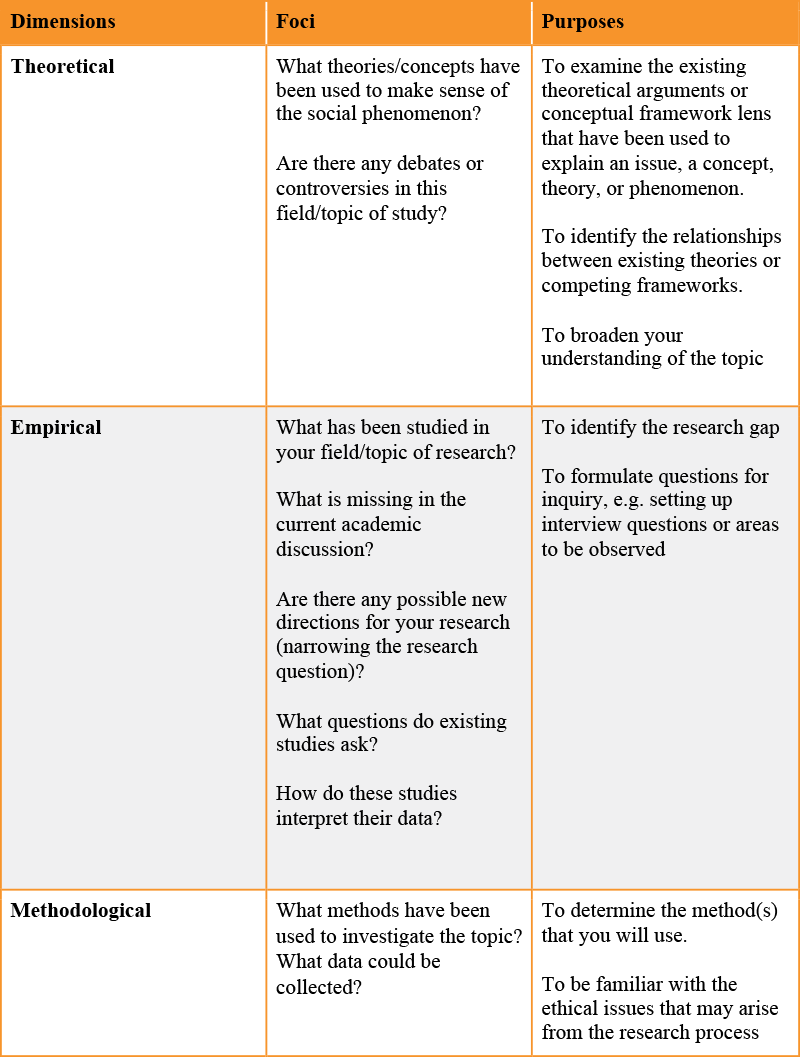
Log in using your username and password
- Search More Search for this keyword Advanced search
- Latest content
- Current issue
- BMJ Journals More You are viewing from: Google Indexer
You are here
- Volume 29, Issue 3
- Rapid reviews methods series: guidance on rapid qualitative evidence synthesis
- Article Text
- Article info
- Citation Tools
- Rapid Responses
- Article metrics
- http://orcid.org/0000-0003-4808-3880 Andrew Booth 1 , 2 ,
- Isolde Sommer 3 , 4 ,
- http://orcid.org/0000-0003-4238-5984 Jane Noyes 2 , 5 ,
- Catherine Houghton 2 , 6 ,
- Fiona Campbell 1 , 7
- The Cochrane Rapid Reviews Methods Group and Cochrane Qualitative and Implementation Methods Group (CQIMG)
- 1 EnSyGN Sheffield Evidence Synthesis Group , University of Sheffield , Sheffield , UK
- 2 Cochrane Qualitative and Implementation Methods Group (CQIMG) , London , UK
- 3 Department for Evidence-based Medicine and Evaluation , University for Continuing Education Krems , Krems , Austria
- 4 Cochrane Rapid Reviews Group & Cochrane Austria , Krems , Austria
- 5 Bangor University , Bangor , UK
- 6 University of Galway , Galway , Ireland
- 7 University of Newcastle upon Tyne , Newcastle upon Tyne , UK
- Correspondence to Professor Andrew Booth, Univ Sheffield, Sheffield, UK; a.booth{at}sheffield.ac.uk
This paper forms part of a series of methodological guidance from the Cochrane Rapid Reviews Methods Group and addresses rapid qualitative evidence syntheses (QESs), which use modified systematic, transparent and reproducible methodsu to accelerate the synthesis of qualitative evidence when faced with resource constraints. This guidance covers the review process as it relates to synthesis of qualitative research. ‘Rapid’ or ‘resource-constrained’ QES require use of templates and targeted knowledge user involvement. Clear definition of perspectives and decisions on indirect evidence, sampling and use of existing QES help in targeting eligibility criteria. Involvement of an information specialist, especially in prioritising databases, targeting grey literature and planning supplemental searches, can prove invaluable. Use of templates and frameworks in study selection and data extraction can be accompanied by quality assurance procedures targeting areas of likely weakness. Current Cochrane guidance informs selection of tools for quality assessment and of synthesis method. Thematic and framework synthesis facilitate efficient synthesis of large numbers of studies or plentiful data. Finally, judicious use of Grading of Recommendations Assessment, Development and Evaluation approach for assessing the Confidence of Evidence from Reviews of Qualitative research assessments and of software as appropriate help to achieve a timely and useful review product.
- Systematic Reviews as Topic
- Patient Care
Data availability statement
No data are available. Not applicable. All data is from published articles.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/ .
https://doi.org/10.1136/bmjebm-2023-112620
Statistics from Altmetric.com
Request permissions.
If you wish to reuse any or all of this article please use the link below which will take you to the Copyright Clearance Center’s RightsLink service. You will be able to get a quick price and instant permission to reuse the content in many different ways.
WHAT IS ALREADY KNOWN ON THIS TOPIC
Rapid Qualitative Evidence Synthesis (QES) is a relatively recent innovation in evidence synthesis and few published examples currently exists.
Guidance for authoring a rapid QES is scattered and requires compilation and summary.
WHAT THIS STUDY ADDS
This paper represents the first attempt to compile current guidance, illustrated by the experience of several international review teams.
We identify features of rapid QES methods that could be accelerated or abbreviated and where methods resemble those for conventional QESs.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This paper offers guidance for researchers when conducting a rapid QES and informs commissioners of research and policy-makers what to expect when commissioning such a review.
Introduction
This paper forms part of a series from the Cochrane Rapid Reviews Methods Group providing methodological guidance for rapid reviews. While other papers in the series 1–4 focus on generic considerations, we aim to provide in-depth recommendations specific to a resource-constrained (or rapid) qualitative evidence synthesis (rQES). 5 This paper is accompanied by recommended resources ( online supplemental appendix A ) and an elaboration with practical considerations ( online supplemental appendix B ).
Supplemental material
The role of qualitative evidence in decision-making is increasingly recognised. 6 This, in turn, has led to appreciation of the value of qualitative evidence syntheses (QESs) that summarise findings across multiple contexts. 7 Recognition of the need for such syntheses to be available at the time most useful to decision-making has, in turn, driven demand for rapid qualitative evidence syntheses. 8 The breadth of potential rQES mirrors the versatility of QES in general (from focused questions to broad overviews) and outputs range from descriptive thematic maps through to theory-informed syntheses (see table 1 ).
- View inline
Glossary of important terms (alphabetically)
As with other resource-constrained reviews, no one size fits all. A team should start by specifying the phenomenon of interest, the review question, 9 the perspectives to be included 9 and the sample to be determined and selected. 10 Subsequently, the team must finalise the appropriate choice of synthesis. 11 Above all, the review team should consider the intended knowledge users, 3 including requirements of the funder.
An rQES team, in particular, cannot afford any extra time or resource requirements that might arise from either a misunderstanding of the review question, an unclear picture of user requirements or an inappropriate choice of methods. The team seeks to align the review question and the requirements of the knowledge user with available time and resources. They also need to ensure that the choice of data and choice of synthesis are appropriate to the intended ‘knowledge claims’ (epistemology) made by the rQES. 11 This involves the team asking ‘what types of data are meaningful for this review question?’, ‘what types of data are trustworthy?’ and ‘is the favoured synthesis method appropriate for this type of data?’. 12 This paper aims to help rQES teams to choose methods that best fit their project while understanding the limitations of those choices. Our recommendations derive from current QES guidance, 5 evidence on modified QES methods, 8 13 and practical experience. 14 15
This paper presents an overview of considerations and recommendations as described in table 2 . Supplemental materials including additional resources details of our recommendations and practical examples are provided in online supplemental appendices A and B .
Recommendations for resource-constrained qualitative evidence synthesis (rQES)
Setting the review question and topic refinement
Rapid reviews summarise information from multiple research studies to produce evidence for ‘the public, researchers, policymakers and funders in a systematic, resource-efficient manner’. 16 Involvement of knowledge users is critical. 3 Given time constraints, individual knowledge users could be asked only to feedback on very specific decisions and tasks or on selective sections of the protocol. Specifically, whenever a QES is abbreviated or accelerated, a team should ensure that the review question is agreed by a minimum number of knowledge users with expertise or experience that reflects all the important review perspectives and with authority to approve the final version 2 5 11 ( table 2 , item R1).
Involvement of topic experts can ensure that the rQES is responsive to need. 14 17 One Cochrane rQES saved considerable time by agreeing the review topic within a single meeting and one-phase iteration. 9 Decisions on topics to be omitted are also informed by a knowledge of existing QESs. 17
An information specialist can help to manage the quantity and quality of available evidence by setting conceptual boundaries and logistic limits. A structured question format, such as Setting-Perspective-Interest, phenomenon of-Comparison-Evaluation or Population-Interest, phenomenon of-Context helps in communicating the scope and, subsequently, in operationalising study selection. 9 18
Scoping (of review parameters) and mapping (of key types of evidence and likely richness of data) helps when planning the review. 5 19 The option to choose purposive sampling over comprehensive sampling approaches, as offered by standard QES, may be particularly helpful in the context of a rapid QES. 8 Once a team knows the approximate number and distribution of studies, perhaps mapping them against country, age, ethnicity, etc), they can decide whether or not to use purposive sampling. 12 An rQES for the WHO combined purposive with variation sampling. Sampling in two stages started by reducing the initial number of studies to a more manageable sampling frame and then sampling approximately a third of the remaining studies from within the sampling frame. 20
Sampling may target richer studies and/or privilege diversity. 8 21 A rich qualitative study typically illustrates findings with verbatim extracts from transcripts from interviews or textual responses from questionnaires. Rich studies are often found in specialist qualitative research or social science journals. In contrast, less rich studies may itemise themes with an occasional indicative text extract and tend to summarise findings. In clinical or biomedical journals less rich findings may be placed within a single table or box.
No rule exists on an optimal number of studies; too many studies makes it challenging to ‘maintain insight’, 22 too few does not sustain rigorous analysis. 23 Guidance on sampling is available from the forthcoming Cochrane-Campbell QES Handbook.
A review team can use templates to fast-track writing of a protocol. The protocol should always be publicly available ( table 2 , item R2). 24 25 Formal registration may require that the team has not commenced data extraction but should be considered if it does not compromise the rQES timeframe. Time pressures may require that methods are left suitably flexible to allow well-justified changes to be made as a detailed picture of the studies and data emerge. 26 The first Cochrane rQES drew heavily on text from a joint protocol/review template previously produced within Cochrane. 24
Setting eligibility criteria
An rQES team may need to limit the number of perspectives, focusing on those most important for decision-making 5 9 27 ( table 2 , item R3). Beyond the patients/clients each additional perspective (eg, family members, health professionals, other professionals, etc) multiplies the additional effort involved.
A rapid QES may require strict date and setting restrictions 17 and language restrictions that accommodate the specific requirements of the review. Specifically, the team should consider whether changes in context over time or substantive differences between geographical regions could be used to justify a narrower date range or a limited coverage of countries and/or languages. The team should also decide if ‘indirect evidence’ is to substitute for the absence of direct evidence. An rQES typically focuses on direct evidence, except when only indirect evidence is available 28 ( table 2 , item R4). Decisions on relevance are challenging—precautions for swine influenza may inform precautions for bird influenza. 28 A smoking ban may operate similarly to seat belt legislation, etc. A review team should identify where such shared mechanisms might operate. 28 An rQES team must also decide whether to use frameworks or models to focus the review. Theories may be unearthed within the topic search or be already known to team members, fro example, Theory of Planned Behaviour. 29
Options for managing the quantity and quality of studies and data emerge during the scoping (see above). In summary, the review team should consider privileging rich qualitative studies 2 ; consider a stepwise approach to inclusion of qualitative data and explore the possibility of sampling ( table 2 , item R5). For example, where data is plentiful an rQES may be limited to qualitative research and/or to mixed methods studies. Where data is less plentiful then surveys or other qualitative data sources may need to be included. Where plentiful reviews already exist, a team may decide to conduct a review of reviews 5 by including multiple QES within a mega-synthesis 28 29 ( table 2 , item R6).
Searching for QES merits its own guidance, 21–23 30 this section reinforces important considerations from guidance specific to qualitative research. Generic guidance for rapid reviews in this series broadly applies to rapid QESs. 1
In addition to journal articles, by far the most plentiful source, qualitative research is found in book chapters, theses and in published and unpublished reports. 21 Searches to support an rQES can (a) limit the number of databases searched, deliberately selecting databases from diverse disciplines, (b) use abbreviated study filters to retrieve qualitative designs and (c) employ high yield complementary methods (eg, reference checking, citation searching and Related Articles features). An information specialist (eg, librarian) should be involved in prioritising sources and search methods ( table 2 , item R7). 11 14
According to empirical evidence optimal database combinations include Scopus plus CINAHL or Scopus plus ProQuest Dissertations and Theses Global (two-database combinations) and Scopus plus CINAHL plus ProQuest Dissertations and Theses Global (three-database combination) with both choices retrieving between 89% and 92% of relevant studies. 30
If resources allow, searches should include one or two specialised databases ( table 2 , item R8) from different disciplines or contexts 21 (eg, social science databases, specialist discipline databases or regional or institutional repositories). Even when resources are limited, the information specialist should factor in time for peer review of at least one search strategy ( table 2 , item R9). 31 Searches for ‘grey literature’ should selectively target appropriate types of grey literature (such as theses or process evaluations) and supplemental searches, including citation chaining or Related Articles features ( table 2 , item R10). 32 The first Cochrane rQES reported that searching reference lists of key papers yielded an extra 30 candidate papers for review. However, the team documented exclusion of grey literature as a limitation of their review. 15
Study selection
Consistency in study selection is achieved by using templates, by gaining a shared team understanding of the audience and purpose, and by ongoing communication within, and beyond, the team. 2 33 Individuals may work in parallel on the same task, as in the first Cochrane rQES, or follow a ‘segmented’ approach where each reviewer is allocated a different task. 14 The use of machine learning in the specific context of rQES remains experimental. However, the possibility of developing qualitative study classifiers comparable to those for randomised controlled trials offers an achievable aspiration. 34
Title and abstract screening
The entire screening team should use pre-prepared, pretested title and abstract templates to limit the scale of piloting, calibration and testing ( table 2 , item R11). 1 14 The first Cochrane rQES team double-screened titles and abstracts within Covidence review software. 14 Disagreements were resolved with reference to a third reviewer achieving a shared understanding of the eligibility criteria and enhancing familiarity with target studies and insight from data. 14 The team should target and prioritise identified risks of either over-zealous inclusion or over-exclusion specific to each rQES ( table 2 , item R12). 14 The team should maximise opportunities to capture divergent views and perspectives within study findings. 35
Full-text screening
Full-text screening similarly benefits from using a pre-prepared pretested standardised template where possible 1 14 ( table 2 , item R11). If a single reviewer undertakes full-text screening, 8 the team should identify likely risks to trustworthiness of findings and focus quality control procedures (eg, use of additional reviewers and percentages for double screening) on specific threats 14 ( table 2 , item R13). The Cochrane rQES team opted for double screening to assist their immersion within the topic. 14
Data extraction
Data extraction of descriptive/contextual data may be facilitated by review management software (eg, EPPI-Reviewer) or home-made approaches using Google Forms, or other survey software. 36 Where extraction of qualitative findings requires line-by-line coding with multiple iterations of the data then a qualitative data management analysis package, such as QSR NVivo, reaps dividends. 36 The team must decide if, collectively, they favour extracting data to a template or coding direct within an electronic version of an article.
Quality control must be fit for purpose but not excessive. Published examples typically use a single reviewer for data extraction 8 with use of two independent reviewers being the exception. The team could limit data extraction to minimal essential items. They may also consider re-using descriptive details and findings previously extracted within previous well-conducted QES ( table 2 , item R14). A pre-existing framework, where readily identified, may help to structure the data extraction template. 15 37 The same framework may be used to present the findings. Some organisations may specify a preferred framework, such as an evidence-to-decision-making framework. 38
Assessment of methodological limitations
The QES community assess ‘methodological limitations’ rather than use ‘risk of bias’ terminology. An rQES team should pick an approach appropriate to their specific review. For example, a thematic map may not require assessment of individual studies—a brief statement of the generic limitations of the set of studies may be sufficient. However, for any synthesis that underpins practice recommendations 39 assessment of included studies is integral to the credibility of findings. In any decision-making context that involves recommendations or guidelines, an assessment of methodological limitations is mandatory. 40 41
Each review team should work with knowledge users to determine a review-specific approach to quality assessment. 27 While ‘traffic lights’, similar to the outputs from the Cochrane Risk of Bias tool, may facilitate rapid interpretation, accompanying textual notes are invaluable in highlighting specific areas for concern. In particular, the rQES team should demonstrate that they are aware (a) that research designs for qualitative research seek to elicit divergent views, rather than control for variation; (b) that, for qualitative research, the selection of the sample is far more informative than the size of the sample; and (c) that researchers from primary research, and equally reviewers for the qualitative synthesis, need to be thoughtful and reflexive about their possible influences on interpretation of either the primary data or the synthesised findings.
Selection of checklist
Numerous scales and checklists exist for assessing the quality of qualitative studies. In the absence of validated risk of bias tools for qualitative studies, the team should choose a tool according to Cochrane Qualitative and Implementation Methods Group (CQIMG) guidance together with expediency (according to ease of use, prior familiarity, etc) ( table 2 , item R15). 41 In comparison to the Critical Appraisal Skills Programme checklist which was never designed for use in synthesis, 42 the Cochrane qualitative tool is similarly easy to use and was designed for QES use. Work is underway to identify an assessment process that is compatible with QESs that support decision-making. 41 For now the choice of a checklist remains determined by interim Cochrane guidance and, beyond this, by personal preference and experience. For an rQES a team could use a single reviewer to assess methodological limitations, with verification of judgements (and support statements) by a second reviewer ( table 2 , item R16).
The CQIMG endorses three types of synthesis; thematic synthesis, framework synthesis and meta-ethnography ( box 1 ). 43 44 Rapid QES favour descriptive thematic synthesis 45 or framework synthesis, 46 47 except when theory generation (meta-ethnography 48 49 or analytical thematic synthesis) is a priority ( table 2 , item R17).
Choosing a method for rapid qualitative synthesis
Thematic synthesis: first choice method for rQES. 45 For example, in their rapid QES Crooks and colleagues 44 used a thematic synthesis to understand the experiences of both academic and lived experience coresearchers within palliative and end of life research. 45
Framework synthesis: alternative where a suitable framework can be speedily identified. 46 For example, Bright and colleagues 46 considered ‘best-fit framework synthesis’ as appropriate for mapping study findings to an ‘a priori framework of dimensions measured by prenatal maternal anxiety tools’ within their ‘streamlined and time-limited evidence review’. 47
Less commonly, an adapted meta-ethnographical approach was used for an implementation model of social distancing where supportive data (29 studies) was plentiful. 48 However, this QES demonstrates several features that subsequently challenge its original identification as ‘rapid’. 49
Abbrevations: QES, qualitative evidence synthesis; rQES, resource-constrained qualitative evidence synthesis.
The team should consider whether a conceptual model, theory or framework offers a rapid way for organising, coding, interpreting and presenting findings ( table 2 , item R18). If the extracted data appears rich enough to sustain further interpretation, data from a thematic or framework synthesis can subsequently be explored within a subsequent meta-ethnography. 43 However, this requires a team with substantial interpretative expertise. 11
Assessments of confidence in the evidence 4 are central to any rQES that seeks to support decision-making and the QES-specific Grading of Recommendations Assessment, Development and Evaluation approach for assessing the Confidence of Evidence from Reviews of Qualitative research (GRADE-CERQual) approach is designed to assess confidence in qualitative evidence. 50 This can be performed by a single reviewer, confirmed by a second reviewer. 26 Additional reviewers could verify all, or a sample of, assessments. For a rapid assessment a team must prioritise findings, using objective criteria; a WHO rQES focused only on the three ‘highly synthesised findings’. 20 The team could consider reusing GRADE-CERQual assessments from published QESs if findings are relevant and of demonstrable high quality ( table 2 , item R19). 50 No rapid approach to full application of GRADE-CERQual currently exists.
Reporting and record management
Little is written on optimal use of technology. 8 A rapid review is not a good time to learn review management software or qualitative analysis management software. Using such software for all general QES processes ( table 2 , item R20), and then harnessing these skills and tools when specifically under resource pressures, is a sounder strategy. Good file labelling and folder management and a ‘develop once, re-use multi-times’ approach facilitates resource savings.
Reporting requirements include the meta-ethnography reporting guidance (eMERGe) 51 and the Enhancing transparency in reporting the synthesis of qualitative research (ENTREQ) statement. 52 An rQES should describe limitations and their implications for confidence in the evidence even more thoroughly than a regular QES; detailing the consequences of fast-tracking, streamlining or of omitting processes all together. 8 Time spent documenting reflexivity is similarly important. 27 If QES methodology is to remain credible rapid approaches must be applied with insight and documented with circumspection. 53 54 (56)
Ethics statements
Patient consent for publication.
Not applicable.
Ethics approval
- Klerings I ,
- Robalino S ,
- Booth A , et al
- Nussbaumer-Streit B ,
- Hamel C , et al
- Garritty C ,
- Tricco AC ,
- Smith M , et al
- Gartlehner G ,
- Devane D , et al
- NHS Scotland
- Campbell F ,
- Flemming K , et al
- Glenton C ,
- Lubarsky S ,
- Varpio L , et al
- Meskell P ,
- Glenton C , et al
- Houghton C ,
- Delaney H , et al
- Beecher C ,
- Maeso B , et al
- McKenzie JE , et al
- Harris JL ,
- Cargo M , et al
- Varley-Campbell J , et al
- Downe S , et al
- Shamseer L ,
- Clarke M , et al
- Nussbaumer-Streit B , et al
- Finlayson KW ,
- Lawrie TA , et al
- Lewin S , et al
- Frandsen TF ,
- Gildberg FA ,
- Tingleff EB
- Mshelia S ,
- Analo CV , et al
- Husk K , et al
- Carmona C ,
- Carroll C ,
- Ilott I , et al
- Meehan B , et al
- Munthe-Kaas H ,
- Bohren MA ,
- Munthe-Kaas HM ,
- French DP ,
- Flemming K ,
- Garside R , et al
- Shulman C , et al
- Dixon-Woods M
- Bright KS ,
- Norris JM ,
- Letourneau NL , et al
- Sadjadi M ,
- Mörschel KS ,
- Petticrew M
- France EF ,
- Cunningham M ,
- Ring N , et al
- McInnes E , et al
- Britten N ,
- Garside R ,
- Pope C , et al
Supplementary materials
Supplementary data.
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1
Correction notice Since this paper first published, updates have been made to the left hand column of table 2.
Contributors All authors (AB, IS, JN, CH, FC) have made substantial contributions to the conception and design of the guidance document. AB led on drafting the work and revising it critically for important intellectual content. All other authors (IS, JN, CH, FC) contributed to revisions of the document. All authors (AB, IS, JN, CH, FC) have given final approval of the version to be published. As members of the Cochrane Qualitative and Implementation Methods Group and/or the Cochrane Rapid Reviews Methods Group all authors (AB, IS, JN, CH, FC) agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests AB is co-convenor of the Cochrane Qualitative and Implementation Methods Group. In the last 36 months, he received royalties from Systematic Approaches To a Successful Literature Review (Sage 3rd edition), honoraria from the Agency for Healthcare Research and Quality, and travel support from the WHO. JN is lead convenor of the Cochrane Qualitative and Implementation Methods Group. In the last 36 months, she has received honoraria from the Agency for Healthcare Research and Quality and travel support from the WHO. CH is co-convenor of the Cochrane Qualitative and Implementation Methods Group.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Read the full text or download the PDF:
- Open access
- Published: 16 May 2024
Integrating qualitative research within a clinical trials unit: developing strategies and understanding their implementation in contexts
- Jeremy Segrott ORCID: orcid.org/0000-0001-6215-0870 1 ,
- Sue Channon 2 ,
- Amy Lloyd 4 ,
- Eleni Glarou 2 , 3 ,
- Josie Henley 5 ,
- Jacqueline Hughes 2 ,
- Nina Jacob 2 ,
- Sarah Milosevic 2 ,
- Yvonne Moriarty 2 ,
- Bethan Pell 6 ,
- Mike Robling 2 ,
- Heather Strange 2 ,
- Julia Townson 2 ,
- Qualitative Research Group &
- Lucy Brookes-Howell 2
Trials volume 25 , Article number: 323 ( 2024 ) Cite this article
6 Altmetric
Metrics details
Background/aims
The value of using qualitative methods within clinical trials is widely recognised. How qualitative research is integrated within trials units to achieve this is less clear. This paper describes the process through which qualitative research has been integrated within Cardiff University’s Centre for Trials Research (CTR) in Wales, UK. We highlight facilitators of, and challenges to, integration.
We held group discussions on the work of the Qualitative Research Group (QRG) within CTR. The content of these discussions, materials for a presentation in CTR, and documents relating to the development of the QRG were interpreted at a workshop attended by group members. Normalisation Process Theory (NPT) was used to structure analysis. A writing group prepared a document for input from members of CTR, forming the basis of this paper.
Actions to integrate qualitative research comprised: its inclusion in Centre strategies; formation of a QRG with dedicated funding/roles; embedding of qualitative research within operating systems; capacity building/training; monitoring opportunities to include qualitative methods in studies; maximising the quality of qualitative research and developing methodological innovation. Facilitators of these actions included: the influence of the broader methodological landscape within trial/study design and its promotion of the value of qualitative research; and close physical proximity of CTR qualitative staff/students allowing sharing of methodological approaches. Introduction of innovative qualitative methods generated interest among other staff groups. Challenges included: pressure to under-resource qualitative components of research, preference for a statistical stance historically in some research areas and funding structures, and difficulties faced by qualitative researchers carving out individual academic profiles when working across trials/studies.
Conclusions
Given that CTUs are pivotal to the design and conduct of RCTs and related study types across multiple disciplines, integrating qualitative research into trials units is crucial if its contribution is to be fully realised. We have made explicit one trials unit’s experience of embedding qualitative research and present this to open dialogue on ways to operationalise and optimise qualitative research in trials. NPT provides a valuable framework with which to theorise these processes, including the importance of sense-making and legitimisation when introducing new practices within organisations.
Peer Review reports
The value of using qualitative methods within randomised control trials (RCTs) is widely recognised [ 1 , 2 , 3 ]. Qualitative research generates important evidence on factors affecting trial recruitment/retention [ 4 ] and implementation, aiding interpretation of quantitative data [ 5 ]. Though RCTs have traditionally been viewed as sitting within a positivist paradigm, recent methodological innovations have developed new trial designs that draw explicitly on both quantitative and qualitative methods. For instance, in the field of complex public health interventions, realist RCTs seek to understand the mechanisms through which interventions generate hypothesised impacts, and how interactions across different implementation contexts form part of these mechanisms. Proponents of realist RCTs—which integrate experimental and realist paradigms—highlight the importance of using quantitative and qualitative methods to fully realise these aims and to generate an understanding of intervention mechanisms and how context shapes them [ 6 ].
A need for guidance on how to conduct good quality qualitative research is being addressed, particularly in relation to feasibility studies for RCTs [ 7 ] and process evaluations embedded within trials of complex interventions [ 5 ]. There is also guidance on the conduct of qualitative research within trials at different points in the research cycle, including development, conduct and reporting [ 8 , 9 ].
A high proportion of trials are based within or involve clinical trials units (CTUs). In the UK the UKCRC Registered CTU Network describes them as:
… specialist units which have been set up with a specific remit to design, conduct, analyse and publish clinical trials and other well-designed studies. They have the capability to provide specialist expert statistical, epidemiological, and other methodological advice and coordination to undertake successful clinical trials. In addition, most CTUs will have expertise in the coordination of trials involving investigational medicinal products which must be conducted in compliance with the UK Regulations governing the conduct of clinical trials resulting from the EU Directive for Clinical Trials.
Thus, CTUs provide the specialist methodological expertise needed for the conduct of trials, and in the case of trials of investigational medicinal products, their involvement may be mandated to ensure compliance with relevant regulations. As the definition above suggests, CTUs also conduct and support other types of study apart from RCTs, providing a range of methodological and subject-based expertise.
However, despite their central role in the conduct and design of trials, (and other evaluation designs) little has been written about how CTUs have integrated qualitative work within their organisation at a time when such methods are, as stated above, now recognised as an important aspect of RCTs and evaluation studies more generally. This is a significant gap, since integration at the organisational level arguably shapes how qualitative research is integrated within individual studies, and thus it is valuable to understand how CTUs have approached the task. There are different ways of involving qualitative work in trials units, such as partnering with other departments (e.g. social science) or employing qualitative researchers directly. Qualitative research can be imagined and configured in different ways—as a method that generates data to inform future trial and intervention design, as an embedded component within an RCT or other evaluation type, or as a parallel strand of research focusing on lived experiences of illness, for instance. Understanding how trials units have integrated qualitative research is valuable, as it can shed light on which strategies show promise, and in which contexts, and how qualitative research is positioned within the field of trials research, foregrounding the value of qualitative research. However, although much has been written about its use within trials, few accounts exist of how trials units have integrated qualitative research within their systems and structures.
This paper discusses the process of embedding qualitative research within the work of one CTU—Cardiff University’s Centre for Trials Research (CTR). It highlights facilitators of this process and identifies challenges to integration. We use the Normalisation Process Theory (NPT) as a framework to structure our experience and approach. The key gap addressed by this paper is the implementation of strategies to integrate qualitative research (a relatively newly adopted set of practices and processes) within CTU systems and structures. We acknowledge from the outset that there are multiple ways of approaching this task. What follows therefore is not a set of recommendations for a preferred or best way to integrate qualitative research, as this will comprise diverse actions according to specific contexts. Rather, we examine the processes through which integration occurred in our own setting and highlight the potential value of these insights for others engaged in the work of promoting qualitative research within trials units.
Background to the integration of qualitative research within CTR
The CTR was formed in 2015 [ 10 ]. It brought together three existing trials units at Cardiff University: the South East Wales Trials Unit, the Wales Cancer Trials Unit, and the Haematology Clinical Trials Unit. From its inception, the CTR had a stated aim of developing a programme of qualitative research and integrating it within trials and other studies. In the sections below, we map these approaches onto the framework offered by Normalisation Process Theory to understand the processes through which they helped achieve embedding and integration of qualitative research.
CTR’s aims (including those relating to the development of qualitative research) were included within its strategy documents and communicated to others through infrastructure funding applications, annual reports and its website. A Qualitative Research Group (QRG), which had previously existed within the South East Wales Trials Unit, with dedicated funding for methodological specialists and group lead academics, was a key mechanism through which the development of a qualitative portfolio was put into action. Integration of qualitative research within Centre systems and processes occurred through the inclusion of qualitative research in study adoption processes and representation on committees. The CTR’s study portfolio provided a basis to track qualitative methods in new and existing studies, identify opportunities to embed qualitative methods within recently adopted studies (at the funding application stage) and to manage staff resources. Capacity building and training were an important focus of the QRG’s work, including training courses, mentoring, creation of an academic network open to university staff and practitioners working in the field of healthcare, presentations at CTR staff meetings and securing of PhD studentships. Standard operating procedures and methodological guidance on the design and conduct of qualitative research (e.g. templates for developing analysis plans) aimed to create a shared understanding of how to undertake high-quality research, and a means to monitor the implementation of rigorous approaches. As the QRG expanded its expertise it sought to develop innovative approaches, including the use of visual [ 11 ] and ethnographic methods [ 12 ].
Understanding implementation—Normalisation Process Theory (NPT)
Normalisation Process Theory (NPT) provides a model with which to understand the implementation of new sets of practices and their normalisation within organisational settings. The term ‘normalisation’ refers to how new practices become routinised (part of the everyday work of an organisation) through embedding and integration [ 13 , 14 ]. NPT defines implementation as ‘the social organisation of work’ and is concerned with the social processes that take place as new practices are introduced. Embedding involves ‘making practices routine elements of everyday life’ within an organisation. Integration takes the form of ‘sustaining embedded practices in social contexts’, and how these processes lead to the practices becoming (or not becoming) ‘normal and routine’ [ 14 ]. NPT is concerned with the factors which promote or ‘inhibit’ attempts to embed and integrate the operationalisation of new practices [ 13 , 14 , 15 ].
Embedding new practices is therefore achieved through implementation—which takes the form of interactions in specific contexts. Implementation is operationalised through four ‘generative mechanisms’— coherence , cognitive participation , collective action and reflexive monitoring [ 14 ]. Each mechanism is characterised by components comprising immediate and organisational work, with actions of individuals and organisations (or groups of individuals) interdependent. The mechanisms operate partly through forms of investment (i.e. meaning, commitment, effort, and comprehension) [ 14 ].
Coherence refers to how individuals/groups make sense of, and give meaning to, new practices. Sense-making concerns the coherence of a practice—whether it ‘holds together’, and its differentiation from existing activities [ 15 ]. Communal and individual specification involve understanding new practices and their potential benefits for oneself or an organisation. Individuals consider what new practices mean for them in terms of tasks and responsibilities ( internalisation ) [ 14 ].
NPT frames the second mechanism, cognitive participation , as the building of a ‘community of practice’. For a new practice to be initiated, individuals and groups within an organisation must commit to it [ 14 , 15 ]. Cognitive participation occurs through enrolment —how people relate to the new practice; legitimation —the belief that it is right for them to be involved; and activation —defining which actions are necessary to sustain the practice and their involvement [ 14 ]. Making the new practices work may require changes to roles (new responsibilities, altered procedures) and reconfiguring how colleagues work together (changed relationships).
Third, Collective Action refers to ‘the operational work that people do to enact a set of practices’ [ 14 ]. Individuals engage with the new practices ( interactional workability ) reshaping how members of an organisation interact with each other, through creation of new roles and expectations ( relational interaction ) [ 15 ]. Skill set workability concerns how the work of implementing a new set of practices is distributed and the necessary roles and skillsets defined [ 14 ]. Contextual integration draws attention to the incorporation of a practice within social contexts, and the potential for aspects of these contexts, such as systems and procedures, to be modified as a result [ 15 ].
Reflexive monitoring is the final implementation mechanism. Collective and individual appraisal evaluate the value of a set of practices, which depends on the collection of information—formally and informally ( systematisation ). Appraisal may lead to reconfiguration in which procedures of the practice are redefined or reshaped [ 14 , 15 ].
We sought to map the following: (1) the strategies used to embed qualitative research within the Centre, (2) key facilitators, and (3) barriers to their implementation. Through focused group discussions during the monthly meetings of the CTR QRG and in discussion with the CTR senior management team throughout 2019–2020 we identified nine types of documents (22 individual documents in total) produced within the CTR which had relevant information about the integration of qualitative research within its work (Table 1 ). The QRG had an ‘open door’ policy to membership and welcomed all staff/students with an interest in qualitative research. It included researchers who were employed specifically to undertake qualitative research and other staff with a range of study roles, including trial managers, statisticians, and data managers. There was also diversity in terms of career stage, including PhD students, mid-career researchers and members of the Centre’s Executive team. Membership was therefore largely self-selected, and comprised of individuals with a role related to, or an interest in, embedding qualitative research within trials. However, the group brought together diverse methodological perspectives and was not solely comprised of methodological ‘champions’ whose job it was to promote the development of qualitative research within the centre. Thus whilst the group (and by extension, the authors of this paper) had a shared appreciation of the value of qualitative research within a trials centre, they also brought varied methodological perspectives and ways of engaging with it.
All members of the QRG ( n = 26) were invited to take part in a face-to-face, day-long workshop in February 2019 on ‘How to optimise and operationalise qualitative research in trials: reflections on CTR structure’. The workshop was attended by 12 members of staff and PhD students, including members of the QRG and the CTR’s senior management team. Recruitment to the workshop was therefore inclusive, and to some extent opportunistic, but all members of the QRG were able to contribute to discussions during regular monthly group meetings and the drafting of the current paper.
The aim of the workshop was to bring together information from the documents in Table 1 to generate discussion around the key strategies (and their component activities) that had been adopted to integrate qualitative research into CTR, as well as barriers to, and facilitators of, their implementation. The agenda for the workshop involved four key areas: development and history of the CTR model; mapping the current model within CTR; discussing the structure of other CTUs; and exploring the advantages and disadvantages of the CTR model.
During the workshop, we discussed the use of NPT to conceptualise how qualitative research had been embedded within CTR’s systems and practices. The group produced spider diagrams to map strategies and actions on to the four key domains (or ‘generative mechanisms’ of NPT) summarised above, to aid the understanding of how they had functioned, and the utility of NPT as a framework. This is summarised in Table 2 .
Detailed notes were made during the workshop. A core writing group then used these notes and the documents in Table 1 to develop a draft of the current paper. This was circulated to all members of the CTR QRG ( n = 26) and stored within a central repository accessible to them to allow involvement and incorporate the views of those who were not able to attend the workshop. This draft was again presented for comments in the monthly CTR QRG meeting in February 2021 attended by n = 10. The Standards for QUality Improvement Reporting Excellence 2.0 (SQUIRE) guidelines were used to inform the structure and content of the paper (see supplementary material) [ 16 ].
In the following sections, we describe the strategies CTR adopted to integrate qualitative research. These are mapped against NPT’s four generative mechanisms to explore the processes through which the strategies promoted integration, and facilitators of and barriers to their implementation. A summary of the strategies and their functioning in terms of the generative mechanisms is provided in Table 2 .
Coherence—making sense of qualitative research
In CTR, many of the actions taken to build a portfolio of qualitative research were aimed at enabling colleagues, and external actors, to make sense of this set of methodologies. Centre-level strategies and grant applications for infrastructure funding highlighted the value of qualitative research, the added benefits it would bring, and positioned it as a legitimate set of practices alongside existing methods. For example, a 2014 application for renewal of trials unit infrastructure funding stated:
We are currently in the process of undertaking […] restructuring for our qualitative research team and are planning similar for trial management next year. The aim of this restructuring is to establish greater hierarchical management and opportunities for staff development and also provide a structure that can accommodate continuing growth.
Within the CTR, various forms of communication on the development of qualitative research were designed to enable staff and students to make sense of it, and to think through its potential value for them, and ways in which they might engage with it. These included presentations at staff meetings, informal meetings between project teams and the qualitative group lead, and the visibility of qualitative research on the public-facing Centre website and Centre committees and systems. For instance, qualitative methods were included (and framed as a distinct set of practices) within study adoption forms and committee agendas. Information for colleagues described how qualitative methods could be incorporated within funding applications for RCTs and other evaluation studies to generate new insights into questions research teams were already keen to answer, such as influences on intervention implementation fidelity. Where externally based chief investigators approached the Centre to be involved in new grant applications, the existence of the qualitative team and group lead enabled the inclusion of qualitative research to be actively promoted at an early stage, and such opportunities were highlighted in the Centre’s brochure for new collaborators. Monthly qualitative research network meetings—advertised across CTR and to external research collaborators, were also designed to create a shared understanding of qualitative research methods and their utility within trials and other study types (e.g. intervention development, feasibility studies, and observational studies). Training events (discussed in more detail below) also aided sense-making.
Several factors facilitated the promotion of qualitative research as a distinctive and valuable entity. Among these was the influence of the broader methodological landscape within trial design which was promoting the value of qualitative research, such as guidance on the evaluation of complex interventions by the Medical Research Council [ 17 ], and the growing emphasis placed on process evaluations within trials (with qualitative methods important in understanding participant experience and influences on implementation) [ 5 ]. The attention given to lived experience (both through process evaluations and the move to embed public involvement in trials) helped to frame qualitative research within the Centre as something that was appropriate, legitimate, and of value. Recognition by research funders of the value of qualitative research within studies was also helpful in normalising and legitimising its adoption within grant applications.
The inclusion of qualitative methods within influential methodological guidance helped CTR researchers to develop a ‘shared language’ around these methods, and a way that a common understanding of the role of qualitative research could be generated. One barrier to such sense-making work was the varying extent to which staff and teams had existing knowledge or experience of qualitative research. This varied across methodological and subject groups within the Centre and reflected the history of the individual trials units which had merged to form the Centre.
Cognitive participation—legitimising qualitative research
Senior CTR leaders promoted the value and legitimacy of qualitative research. Its inclusion in centre strategies, infrastructure funding applications, and in public-facing materials (e.g. website, investigator brochures), signalled that it was appropriate for individuals to conduct qualitative research within their roles, or to support others in doing so. Legitimisation also took place through informal channels, such as senior leadership support for qualitative research methods in staff meetings and participation in QRG seminars. Continued development of the QRG (with dedicated infrastructure funding) provided a visible identity and equivalence with other methodological groups (e.g. trial managers, statisticians).
Staff were asked to engage with qualitative research in two main ways. First, there was an expansion in the number of staff for whom qualitative research formed part of their formal role and responsibilities. One of the three trials units that merged to form CTR brought with it a qualitative team comprising methodological specialists and a group lead. CTR continued the expansion of this group with the creation of new roles and an enlarged nucleus of researchers for whom qualitative research was the sole focus of their work. In part, this was linked to the successful award of projects that included a large qualitative component, and that were coordinated by CTR (see Table 3 which describes the PUMA study).
Members of the QRG were encouraged to develop their own research ideas and to gain experience as principal investigators, and group seminars were used to explore new ideas and provide peer support. This was communicated through line management, appraisal, and informal peer interaction. Boundaries were not strictly demarcated (i.e. staff located outside the qualitative team were already using qualitative methods), but the new team became a central focus for developing a growing programme of work.
Second, individuals and studies were called upon to engage in new ways with qualitative research, and with the qualitative team. A key goal for the Centre was that groups developing new research ideas should give more consideration in general to the potential value and inclusion of qualitative research within their funding applications. Specifically, they were asked to do this by thinking about qualitative research at an early point in their application’s development (rather than ‘bolting it on’ after other elements had been designed) and to draw upon the expertise and input of the qualitative team. An example was the inclusion of questions on qualitative methods within the Centre’s study adoption form and representation from the qualitative team at the committee which reviewed new adoption requests. Where adoption requests indicated the inclusion of qualitative methods, colleagues were encouraged to liaise with the qualitative team, facilitating the integration of its expertise from an early stage. Qualitative seminars offered an informal and supportive space in which researchers could share initial ideas and refine their methodological approach. The benefits of this included the provision of sufficient time for methodological specialists to be involved in the design of the proposed qualitative component and ensuring adequate costings had been drawn up. At study adoption group meetings, scrutiny of new proposals included consideration of whether new research proposals might be strengthened through the use of qualitative methods where these had not initially been included. Meetings of the QRG—which reviewed the Centre’s portfolio of new studies and gathered intelligence on new ideas—also helped to identify, early on, opportunities to integrate qualitative methods. Communication across teams was useful in identifying new research ideas and embedding qualitative researchers within emerging study development groups.
Actions to promote greater use of qualitative methods in funding applications fed through into a growing number of studies with a qualitative component. This helped to increase the visibility and legitimacy of qualitative methods within the Centre. For example, the PUMA study [ 12 ], which brought together a large multidisciplinary team to develop and evaluate a Paediatric early warning system, drew heavily on qualitative methods, with the qualitative research located within the QRG. The project introduced an extensive network of collaborators and clinical colleagues to qualitative methods and how they could be used during intervention development and the generation of case studies. Further information about the PUMA study is provided in Table 3 .
Increasing the legitimacy of qualitative work across an extensive network of staff, students and collaborators was a complex process. Set within the continuing dominance of quantitative methods with clinical trials, there were variations in the extent to which clinicians and other collaborators embraced the value of qualitative methods. Research funding schemes, which often continued to emphasise the quantitative element of randomised controlled trials, inevitably fed through into the focus of new research proposals. Staff and external collaborators were sometimes uncertain about the added value that qualitative methods would bring to their trials. Across the CTR there were variations in the speed at which qualitative research methods gained legitimacy, partly based on disciplinary traditions and their influences. For instance, population health trials, often located within non-health settings such as schools or community settings, frequently involved collaboration with social scientists who brought with them experience in qualitative methods. Methodological guidance in this field, such as MRC guidance on process evaluations, highlighted the value of qualitative methods and alternatives to the positivist paradigm, such as the value of realist RCTs. In other, more clinical areas, positivist paradigms had greater dominance. Established practices and methodological traditions across different funders also influenced the ease of obtaining funding to include qualitative research within studies. For drugs trials (CTIMPs), the influence of regulatory frameworks on study design, data collection and the allocation of staff resources may have played a role. Over time, teams gained repeated experience of embedding qualitative research (and researchers) within their work and took this learning with them to subsequent studies. For example, the senior clinician quoted within the PUMA case study (Table 3 below) described how they had gained an appreciation of the rigour of qualitative research and an understanding of its language. Through these repeated interactions, embedding of qualitative research within studies started to become the norm rather than the exception.
Collective action—operationalising qualitative research
Collective action concerns the operationalisation of new practices within organisations—the allocation and management of the work, how individuals interact with each other, and the work itself. In CTR the formation of a Qualitative Research Group helped to allocate and organise the work of building a portfolio of studies. Researchers across the Centre were called upon to interact with qualitative research in new ways. Presentations at staff meetings and the inclusion of qualitative research methods in portfolio study adoption forms were examples of this ( interactive workability ). It was operationalised by encouraging study teams to liaise with the qualitative research lead. Development of standard operating procedures, templates for costing qualitative research and methodological guidance (e.g. on analysis plans) also helped encourage researchers to interact with these methods in new ways. For some qualitative researchers who had been trained in the social sciences, working within a trials unit meant that they needed to interact in new and sometimes unfamiliar ways with standard operating procedures, risk assessments, and other trial-based systems. Thus, training needs and capacity-building efforts were multidirectional.
Whereas there had been a tendency for qualitative research to be ‘bolted on’ to proposals for RCTs, the systems described above were designed to embed thinking about the value and design of the qualitative component from the outset. They were also intended to integrate members of the qualitative team with trial teams from an early stage to promote effective integration of qualitative methods within larger trials and build relationships over time.
Standard Operating Procedures (SOPs), formal and informal training, and interaction between the qualitative team and other researchers increased the relational workability of qualitative methods within the Centre—the confidence individuals felt in including these methods within their studies, and their accountability for doing so. For instance, study adoption forms prompted researchers to interact routinely with the qualitative team at an early stage, whilst guidance on costing grants provided clear expectations about the resources needed to deliver a proposed set of qualitative data collection.
Formation of the Qualitative Research Group—comprised of methodological specialists, created new roles and skillsets ( skill set workability ). Research teams were encouraged to draw on these when writing funding applications for projects that included a qualitative component. Capacity-building initiatives were used to increase the number of researchers with the skills needed to undertake qualitative research, and for these individuals to develop their expertise over time. This was achieved through formal training courses, academic seminars, mentoring from experienced colleagues, and informal knowledge exchange. Links with external collaborators and centres engaged in building qualitative research supported these efforts. Within the Centre, the co-location of qualitative researchers with other methodological and trial teams facilitated knowledge exchange and building of collaborative relationships, whilst grouping of the qualitative team within a dedicated office space supported a collective identity and opportunities for informal peer support.
Some aspects of the context in which qualitative research was being developed created challenges to operationalisation. Dependence on project grants to fund qualitative methodologists meant that there was a continuing need to write further grant applications whilst limiting the amount of time available to do so. Similarly, researchers within the team whose role was funded largely by specific research projects could sometimes find it hard to create sufficient time to develop their personal methodological interests. However, the cultivation of a methodologically varied portfolio of work enabled members of the team to build significant expertise in different approaches (e.g. ethnography, discourse analysis) that connected individual studies.
Reflexive monitoring—evaluating the impact of qualitative research
Inclusion of questions/fields relating to qualitative research within the Centre’s study portfolio database was a key way in which information was collected ( systematisation ). It captured numbers of funding applications and funded studies, research design, and income generation. Alongside this database, a qualitative resource planner spreadsheet was used to link individual members of the qualitative team with projects and facilitate resource planning, further reinforcing the core responsibilities and roles of qualitative researchers within CTR. As with all staff in the Centre, members of the qualitative team were placed on ongoing rather than fixed-term contracts, reflecting their core role within CTR. Planning and strategy meetings used the database and resource planner to assess the integration of qualitative research within Centre research, identify opportunities for increasing involvement, and manage staff recruitment and sustainability of researcher posts. Academic meetings and day-to-day interaction fulfilled informal appraisal of the development of the group, and its position within the Centre. Individual appraisal was also important, with members of the qualitative team given opportunities to shape their role, reflect on progress, identify training needs, and further develop their skillset, particularly through line management systems.
These forms of systematisation and appraisal were used to reconfigure the development of qualitative research and its integration within the Centre. For example, group strategies considered how to achieve long-term integration of qualitative research from its initial embedding through further promoting the belief that it formed a core part of the Centre’s business. The visibility and legitimacy of qualitative research were promoted through initiatives such as greater prominence on the Centre’s website. Ongoing review of the qualitative portfolio and discussion at academic meetings enabled the identification of areas where increased capacity would be helpful, both for qualitative staff, and more broadly within the Centre. This prompted the qualitative group to develop an introductory course to qualitative methods open to all Centre staff and PhD students, aimed at increasing understanding and awareness. As the qualitative team built its expertise and experience it also sought to develop new and innovative approaches to conducting qualitative research. This included the use of visual and diary-based methods [ 11 ] and the adoption of ethnography to evaluate system-level clinical interventions [ 12 ]. Restrictions on conventional face-to-face qualitative data collection due to the COVID-19 pandemic prompted rapid adoption of virtual/online methods for interviews, observation, and use of new internet platforms such as Padlet—a form of digital note board.
In this paper, we have described the work undertaken by one CTU to integrate qualitative research within its studies and organisational culture. The parallel efforts of many trials units to achieve these goals arguably come at an opportune time. The traditional designs of RCTs have been challenged and re-imagined by the increasing influence of realist evaluation [ 6 , 18 ] and the widespread acceptance that trials need to understand implementation and intervention theory as well as assess outcomes [ 17 ]. Hence the widespread adoption of embedded mixed methods process evaluations within RCTs. These broad shifts in methodological orthodoxies, the production of high-profile methodological guidance, and the expectations of research funders all create fertile ground for the continued expansion of qualitative methods within trials units. However, whilst much has been written about the importance of developing qualitative research and the possible approaches to integrating qualitative and quantitative methods within studies, much less has been published on how to operationalise this within trials units. Filling this lacuna is important. Our paper highlights how the integration of a new set of practices within an organisation can become embedded as part of its ‘normal’ everyday work whilst also shaping the practices being integrated. In the case of CTR, it could be argued that the integration of qualitative research helped shape how this work was done (e.g. systems to assess progress and innovation).
In our trials unit, the presence of a dedicated research group of methodological specialists was a key action that helped realise the development of a portfolio of qualitative research and was perhaps the most visible evidence of a commitment to do so. However, our experience demonstrates that to fully realise the goal of developing qualitative research, much work focuses on the interaction between this ‘new’ set of methods and the organisation into which it is introduced. Whilst the team of methodological specialists was tasked with, and ‘able’ to do the work, the ‘work’ itself needed to be integrated and embedded within the existing system. Thus, alongside the creation of a team and methodological capacity, promoting the legitimacy of qualitative research was important to communicate to others that it was both a distinctive and different entity, yet similar and equivalent to more established groups and practices (e.g. trial management, statistics, data management). The framing of qualitative research within strategies, the messages given out by senior leaders (formally and informally) and the general visibility of qualitative research within the system all helped to achieve this.
Normalisation Process Theory draws our attention to the concepts of embedding (making a new practice routine, normal within an organisation) and integration —the long-term sustaining of these processes. An important process through which embedding took place in our centre concerned the creation of messages and systems that called upon individuals and research teams to interact with qualitative research. Research teams were encouraged to think about qualitative research and consider its potential value for their studies. Critically, they were asked to do so at specific points, and in particular ways. Early consideration of qualitative methods to maximise and optimise their inclusion within studies was emphasised, with timely input from the qualitative team. Study adoption systems, centre-level processes for managing financial and human resources, creation of a qualitative resource planner, and awareness raising among staff, helped to reinforce this. These processes of embedding and integration were complex and they varied in intensity and speed across different areas of the Centre’s work. In part this depended on existing research traditions, the extent of prior experience of working with qualitative researchers and methods, and the priorities of subject areas and funders. Centre-wide systems, sometimes linked to CTR’s operation as a CTU, also helped to legitimise and embed qualitative research, lending it equivalence with other research activity. For example, like all CTUs, CTR was required to conform with the principles of Good Clinical Practice, necessitating the creation of a quality management system, operationalised through standard operating procedures for all areas of its work. Qualitative research was included, and became embedded, within these systems, with SOPs produced to guide activities such as qualitative analysis.
NPT provides a helpful way of understanding how trials units might integrate qualitative research within their work. It highlights how new practices interact with existing organisational systems and the work needed to promote effective interaction. That is, alongside the creation of a team or programme of qualitative research, much of the work concerns how members of an organisation understand it, engage with it, and create systems to sustain it. Embedding a new set of practices may be just as important as the quality or characteristics of the practices themselves. High-quality qualitative research is of little value if it is not recognised and drawn upon within new studies for instance. NPT also offers a helpful lens with which to understand how integration and embedding occur, and the mechanisms through which they operate. For example, promoting the legitimacy of a new set of practices, or creating systems that embed it, can help sustain these practices by creating an organisational ambition and encouraging (or requiring) individuals to interact with them in certain ways, redefining their roles accordingly. NPT highlights the ways in which integration of new practices involves bi-directional exchanges with the organisation’s existing practices, with each having the potential to re-shape the other as interaction takes place. For instance, in CTR, qualitative researchers needed to integrate and apply their methods within the quality management and other systems of a CTU, such as the formalisation of key processes within standard operating procedures, something less likely to occur outside trials units. Equally, project teams (including those led by externally based chief investigators) increased the integration of qualitative methods within their overall study design, providing opportunities for new insights on intervention theory, implementation and the experiences of practitioners and participants.
We note two aspects of the normalisation processes within CTR that are slightly less well conceptualised by NPT. The first concerns the emphasis within coherence on identifying the distinctiveness of new practices, and how they differ from existing activities. Whilst differentiation was an important aspect of the integration of qualitative research in CTR, such integration could be seen as operating partly through processes of de-differentiation, or at least equivalence. That is, part of the integration of qualitative research was to see it as similar in terms of rigour, coherence, and importance to other forms of research within the Centre. To be viewed as similar, or at least comparable to existing practices, was to be legitimised.
Second, whilst NPT focuses mainly on the interaction between a new set of practices and the organisational context into which it is introduced, our own experience of introducing qualitative research into a trials unit was shaped by broader organisational and methodological contexts. For example, the increasing emphasis placed upon understanding implementation processes and the experiences of research participants in the field of clinical trials (e.g. by funders), created an environment conducive to the development of qualitative research methods within our Centre. Attempts to integrate qualitative research within studies were also cross-organisational, given that many of the studies managed within the CTR drew together multi-institutional teams. This provided important opportunities to integrate qualitative research within a portfolio of studies that extended beyond CTR and build a network of collaborators who increasingly included qualitative methods within their funding proposals. The work of growing and integrating qualitative research within a trials unit is an ongoing one in which ever-shifting macro-level influences can help or hinder, and where the organisations within which we work are never static in terms of barriers and facilitators.
The importance of utilising qualitative methods within RCTs is now widely recognised. Increased emphasis on the evaluation of complex interventions, the influence of realist methods directing greater attention to complexity and the widespread adoption of mixed methods process evaluations are key drivers of this shift. The inclusion of qualitative methods within individual trials is important and previous research has explored approaches to their incorporation and some of the challenges encountered. Our paper highlights that the integration of qualitative methods at the organisational level of the CTU can shape how they are taken up by individual trials. Within CTR, it can be argued that qualitative research achieved high levels of integration, as conceptualised by Normalisation Process Theory. Thus, qualitative research became recognised as a coherent and valuable set of practices, secured legitimisation as an appropriate focus of individual and organisational activity and benefitted from forms of collective action which operationalised these organisational processes. Crucially, the routinisation of qualitative research appeared to be sustained, something which NPT suggests helps define integration (as opposed to initial embedding). However, our analysis suggested that the degree of integration varied by trial area. This variation reflected a complex mix of factors including disciplinary traditions, methodological guidance, existing (un)familiarity with qualitative research, and the influence of regulatory frameworks for certain clinical trials.
NPT provides a valuable framework with which to understand how these processes of embedding and integration occur. Our use of NPT draws attention to the importance of sense-making and legitimisation as important steps in introducing a new set of practices within the work of an organisation. Integration also depends, across each mechanism of NPT, on the building of effective relationships, which allow individuals and teams to work together in new ways. By reflecting on our experiences and the decisions taken within CTR we have made explicit one such process for embedding qualitative research within a trials unit, whilst acknowledging that approaches may differ across trials units. Mindful of this fact, and the focus of the current paper on one trials unit’s experience, we do not propose a set of recommendations for others who are working to achieve similar goals. Rather, we offer three overarching reflections (framed by NPT) which may act as a useful starting point for trials units (and other infrastructures) seeking to promote the adoption of qualitative research.
First, whilst research organisations such as trials units are highly heterogenous, processes of embedding and integration, which we have foregrounded in this paper, are likely to be important across different contexts in sustaining the use of qualitative research. Second, developing a plan for the integration of qualitative research will benefit from mapping out the characteristics of the extant system. For example, it is valuable to know how familiar staff are with qualitative research and any variations across teams within an organisation. Thirdly, NPT frames integration as a process of implementation which operates through key generative mechanisms— coherence , cognitive participation , collective action and reflexive monitoring . These mechanisms can help guide understanding of which actions help achieve embedding and integration. Importantly, they span multiple aspects of how organisations, and the individuals within them, work. The ways in which people make sense of a new set of practices ( coherence ), their commitment towards it ( cognitive participation ), how it is operationalised ( collective action ) and the evaluation of its introduction ( reflexive monitoring ) are all important. Thus, for example, qualitative research, even when well organised and operationalised within an organisation, is unlikely to be sustained if appreciation of its value is limited, or people are not committed to it.
We present our experience of engaging with the processes described above to open dialogue with other trials units on ways to operationalise and optimise qualitative research in trials. Understanding how best to integrate qualitative research within these settings may help to fully realise the significant contribution which it makes the design and conduct of trials.
Availability of data and materials
Some documents cited in this paper are either freely available from the Centre for Trials Research website or can be requested from the author for correspondence.
O’Cathain A, Thomas KJ, Drabble SJ, Rudolph A, Hewison J. What can qualitative research do for randomised controlled trials? A systematic mapping review. BMJ Open. 2013;3(6):e002889.
Article PubMed PubMed Central Google Scholar
O’Cathain A, Thomas KJ, Drabble SJ, Rudolph A, Goode J, Hewison J. Maximising the value of combining qualitative research and randomised controlled trials in health research: the QUAlitative Research in Trials (QUART) study – a mixed methods study. Health Technol Assess. 2014;18(38):1–197.
Clement C, Edwards SL, Rapport F, Russell IT, Hutchings HA. Exploring qualitative methods reported in registered trials and their yields (EQUITY): systematic review. Trials. 2018;19(1):589.
Hennessy M, Hunter A, Healy P, Galvin S, Houghton C. Improving trial recruitment processes: how qualitative methodologies can be used to address the top 10 research priorities identified within the PRioRiTy study. Trials. 2018;19:584.
Moore GF, Audrey S, Barker M, Bond L, Bonell C, Hardeman W, et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ. 2015;350(mar19 6):h1258.
Bonell C, Fletcher A, Morton M, Lorenc T, Moore L. Realist randomised controlled trials: a new approach to evaluating complex public health interventions. Soc Sci Med. 2012;75(12):2299–306.
Article PubMed Google Scholar
O’Cathain A, Hoddinott P, Lewin S, Thomas KJ, Young B, Adamson J, et al. Maximising the impact of qualitative research in feasibility studies for randomised controlled trials: guidance for researchers. Pilot Feasibility Stud. 2015;1:32.
Cooper C, O’Cathain A, Hind D, Adamson J, Lawton J, Baird W. Conducting qualitative research within Clinical Trials Units: avoiding potential pitfalls. Contemp Clin Trials. 2014;38(2):338–43.
Rapport F, Storey M, Porter A, Snooks H, Jones K, Peconi J, et al. Qualitative research within trials: developing a standard operating procedure for a clinical trials unit. Trials. 2013;14:54.
Cardiff University. Centre for Trials Research. Available from: https://www.cardiff.ac.uk/centre-for-trials-research . Accessed 10 May 2024.
Pell B, Williams D, Phillips R, Sanders J, Edwards A, Choy E, et al. Using visual timelines in telephone interviews: reflections and lessons learned from the star family study. Int J Qual Methods. 2020;19:160940692091367.
Thomas-Jones E, Lloyd A, Roland D, Sefton G, Tume L, Hood K, et al. A prospective, mixed-methods, before and after study to identify the evidence base for the core components of an effective Paediatric Early Warning System and the development of an implementation package containing those core recommendations for use in th. BMC Pediatr. 2018;18:244.
May C, Finch T, Mair F, Ballini L, Dowrick C, Eccles M, et al. Understanding the implementation of complex interventions in health care: the normalization process model. BMC Health Serv Res. 2007;7:148.
May C, Finch T. Implementing, embedding, and integrating practices: an outline of normalization process theory. Sociology. 2009;43(3):535–54.
Article Google Scholar
May CR, Mair F, Finch T, Macfarlane A, Dowrick C, Treweek S, et al. Development of a theory of implementation and integration: normalization process theory. Implement Sci. 2009;4:29.
Ogrinc G, Davies L, Goodman D, Batalden PB, Davidoff F, Stevens D. SQUIRE 2.0 (Standards for QUality Improvement Reporting Excellence): Revised publication guidelines from a detailed consensus process. BMJ Quality and Safety. 2016;25:986-92.
Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ. 2008;337:a1655.
Jamal F, Fletcher A, Shackleton N, Elbourne D, Viner R, Bonell C. The three stages of building and testing mid-level theories in a realist RCT: a theoretical and methodological case-example. Trials. 2015;16(1):466.
Download references
Acknowledgements
Members of the Centre for Trials Research (CTR) Qualitative Research Group were collaborating authors: C Drew (Senior Research Fellow—Senior Trial Manager, Brain Health and Mental Wellbeing Division), D Gillespie (Director, Infection, Inflammation and Immunity Trials, Principal Research Fellow), R Hale (now Research Associate, School of Social Sciences, Cardiff University), J Latchem-Hastings (now Lecturer and Postdoctoral Fellow, School of Healthcare Sciences, Cardiff University), R Milton (Research Associate—Trial Manager), B Pell (now PhD student, DECIPHer Centre, Cardiff University), H Prout (Research Associate—Qualitative), V Shepherd (Senior Research Fellow), K Smallman (Research Associate), H Stanton (Research Associate—Senior Data Manager). Thanks are due to Kerry Hood and Aimee Grant for their involvement in developing processes and systems for qualitative research within CTR.
No specific grant was received to support the writing of this paper.
Author information
Authors and affiliations.
Centre for Trials Research, DECIPHer Centre, Cardiff University, Neuadd Meirionnydd, Heath Park, Cardiff, CF14 4YS, UK
Jeremy Segrott
Centre for Trials Research, Cardiff University, Neuadd Meirionnydd, Heath Park, Cardiff, CF14 4YS, UK
Sue Channon, Eleni Glarou, Jacqueline Hughes, Nina Jacob, Sarah Milosevic, Yvonne Moriarty, Mike Robling, Heather Strange, Julia Townson & Lucy Brookes-Howell
Division of Population Medicine, School of Medicine, Cardiff University, Neuadd Meirionnydd, Heath Park, Cardiff, CF14 4YS, UK
Eleni Glarou
Wales Centre for Public Policy, Cardiff University, Sbarc I Spark, Maindy Road, Cardiff, CF24 4HQ, UK
School of Social Sciences, Cardiff University, King Edward VII Avenue, Cardiff, CF10 3WA, UK
Josie Henley
DECIPHer Centre, School of Social Sciences, Cardiff University, Sbarc I Spark, Maindy Road, Cardiff, CF24 4HQ, UK
Bethan Pell
You can also search for this author in PubMed Google Scholar
Qualitative Research Group
- , D. Gillespie
- , J. Latchem-Hastings
- , R. Milton
- , V. Shepherd
- , K. Smallman
- & H. Stanton
Contributions
JS contributed to the design of the work and interpretation of data and was responsible for leading the drafting and revision of the paper. SC contributed to the design of the work, the acquisition of data and the drafting and revision of the paper. AL contributed to the design of the work, the acquisition of data and the drafting and revision of the paper. EG contributed to a critical review of the manuscript and provided additional relevant references. JH provided feedback on initial drafts of the paper and contributed to subsequent revisions. JHu provided feedback on initial drafts of the paper and contributed to subsequent revisions. NG provided feedback on initial drafts of the paper and contributed to subsequent revisions. SM was involved in the acquisition and analysis of data and provided a critical review of the manuscript. YM was involved in the acquisition and analysis of data and provided a critical review of the manuscript. MR was involved in the interpretation of data and critical review and revision of the paper. HS contributed to the conception and design of the work, the acquisition and analysis of data, and the revision of the manuscript. JT provided feedback on initial drafts of the paper and contributed to subsequent revisions. LB-H made a substantial contribution to the design and conception of the work, led the acquisition and analysis of data, and contributed to the drafting and revision of the paper.
Corresponding author
Correspondence to Jeremy Segrott .
Ethics declarations
Ethics approval and consent to participate.
Ethical approval was not sought as no personal or identifiable data was collected.
Consent for publication
Competing interests.
All authors are or were members of staff or students in the Centre for Trials Research. JS is an associate editor of Trials .
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Supplementary material 1., rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Segrott, J., Channon, S., Lloyd, A. et al. Integrating qualitative research within a clinical trials unit: developing strategies and understanding their implementation in contexts. Trials 25 , 323 (2024). https://doi.org/10.1186/s13063-024-08124-7
Download citation
Received : 20 October 2023
Accepted : 17 April 2024
Published : 16 May 2024
DOI : https://doi.org/10.1186/s13063-024-08124-7
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Qualitative research
- Qualitative methods
- Trials units
- Normalisation Process Theory
- Randomised controlled trials
ISSN: 1745-6215
- Submission enquiries: Access here and click Contact Us
- General enquiries: [email protected]

An official website of the United States government
The .gov means it's official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you're on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
- Browse Titles
NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
Lau F, Kuziemsky C, editors. Handbook of eHealth Evaluation: An Evidence-based Approach [Internet]. Victoria (BC): University of Victoria; 2017 Feb 27.

Handbook of eHealth Evaluation: An Evidence-based Approach [Internet].
Chapter 9 methods for literature reviews.
Guy Paré and Spyros Kitsiou .
9.1. Introduction
Literature reviews play a critical role in scholarship because science remains, first and foremost, a cumulative endeavour ( vom Brocke et al., 2009 ). As in any academic discipline, rigorous knowledge syntheses are becoming indispensable in keeping up with an exponentially growing eHealth literature, assisting practitioners, academics, and graduate students in finding, evaluating, and synthesizing the contents of many empirical and conceptual papers. Among other methods, literature reviews are essential for: (a) identifying what has been written on a subject or topic; (b) determining the extent to which a specific research area reveals any interpretable trends or patterns; (c) aggregating empirical findings related to a narrow research question to support evidence-based practice; (d) generating new frameworks and theories; and (e) identifying topics or questions requiring more investigation ( Paré, Trudel, Jaana, & Kitsiou, 2015 ).
Literature reviews can take two major forms. The most prevalent one is the “literature review” or “background” section within a journal paper or a chapter in a graduate thesis. This section synthesizes the extant literature and usually identifies the gaps in knowledge that the empirical study addresses ( Sylvester, Tate, & Johnstone, 2013 ). It may also provide a theoretical foundation for the proposed study, substantiate the presence of the research problem, justify the research as one that contributes something new to the cumulated knowledge, or validate the methods and approaches for the proposed study ( Hart, 1998 ; Levy & Ellis, 2006 ).
The second form of literature review, which is the focus of this chapter, constitutes an original and valuable work of research in and of itself ( Paré et al., 2015 ). Rather than providing a base for a researcher’s own work, it creates a solid starting point for all members of the community interested in a particular area or topic ( Mulrow, 1987 ). The so-called “review article” is a journal-length paper which has an overarching purpose to synthesize the literature in a field, without collecting or analyzing any primary data ( Green, Johnson, & Adams, 2006 ).
When appropriately conducted, review articles represent powerful information sources for practitioners looking for state-of-the art evidence to guide their decision-making and work practices ( Paré et al., 2015 ). Further, high-quality reviews become frequently cited pieces of work which researchers seek out as a first clear outline of the literature when undertaking empirical studies ( Cooper, 1988 ; Rowe, 2014 ). Scholars who track and gauge the impact of articles have found that review papers are cited and downloaded more often than any other type of published article ( Cronin, Ryan, & Coughlan, 2008 ; Montori, Wilczynski, Morgan, Haynes, & Hedges, 2003 ; Patsopoulos, Analatos, & Ioannidis, 2005 ). The reason for their popularity may be the fact that reading the review enables one to have an overview, if not a detailed knowledge of the area in question, as well as references to the most useful primary sources ( Cronin et al., 2008 ). Although they are not easy to conduct, the commitment to complete a review article provides a tremendous service to one’s academic community ( Paré et al., 2015 ; Petticrew & Roberts, 2006 ). Most, if not all, peer-reviewed journals in the fields of medical informatics publish review articles of some type.
The main objectives of this chapter are fourfold: (a) to provide an overview of the major steps and activities involved in conducting a stand-alone literature review; (b) to describe and contrast the different types of review articles that can contribute to the eHealth knowledge base; (c) to illustrate each review type with one or two examples from the eHealth literature; and (d) to provide a series of recommendations for prospective authors of review articles in this domain.
9.2. Overview of the Literature Review Process and Steps
As explained in Templier and Paré (2015) , there are six generic steps involved in conducting a review article:
- formulating the research question(s) and objective(s),
- searching the extant literature,
- screening for inclusion,
- assessing the quality of primary studies,
- extracting data, and
- analyzing data.
Although these steps are presented here in sequential order, one must keep in mind that the review process can be iterative and that many activities can be initiated during the planning stage and later refined during subsequent phases ( Finfgeld-Connett & Johnson, 2013 ; Kitchenham & Charters, 2007 ).
Formulating the research question(s) and objective(s): As a first step, members of the review team must appropriately justify the need for the review itself ( Petticrew & Roberts, 2006 ), identify the review’s main objective(s) ( Okoli & Schabram, 2010 ), and define the concepts or variables at the heart of their synthesis ( Cooper & Hedges, 2009 ; Webster & Watson, 2002 ). Importantly, they also need to articulate the research question(s) they propose to investigate ( Kitchenham & Charters, 2007 ). In this regard, we concur with Jesson, Matheson, and Lacey (2011) that clearly articulated research questions are key ingredients that guide the entire review methodology; they underscore the type of information that is needed, inform the search for and selection of relevant literature, and guide or orient the subsequent analysis. Searching the extant literature: The next step consists of searching the literature and making decisions about the suitability of material to be considered in the review ( Cooper, 1988 ). There exist three main coverage strategies. First, exhaustive coverage means an effort is made to be as comprehensive as possible in order to ensure that all relevant studies, published and unpublished, are included in the review and, thus, conclusions are based on this all-inclusive knowledge base. The second type of coverage consists of presenting materials that are representative of most other works in a given field or area. Often authors who adopt this strategy will search for relevant articles in a small number of top-tier journals in a field ( Paré et al., 2015 ). In the third strategy, the review team concentrates on prior works that have been central or pivotal to a particular topic. This may include empirical studies or conceptual papers that initiated a line of investigation, changed how problems or questions were framed, introduced new methods or concepts, or engendered important debate ( Cooper, 1988 ). Screening for inclusion: The following step consists of evaluating the applicability of the material identified in the preceding step ( Levy & Ellis, 2006 ; vom Brocke et al., 2009 ). Once a group of potential studies has been identified, members of the review team must screen them to determine their relevance ( Petticrew & Roberts, 2006 ). A set of predetermined rules provides a basis for including or excluding certain studies. This exercise requires a significant investment on the part of researchers, who must ensure enhanced objectivity and avoid biases or mistakes. As discussed later in this chapter, for certain types of reviews there must be at least two independent reviewers involved in the screening process and a procedure to resolve disagreements must also be in place ( Liberati et al., 2009 ; Shea et al., 2009 ). Assessing the quality of primary studies: In addition to screening material for inclusion, members of the review team may need to assess the scientific quality of the selected studies, that is, appraise the rigour of the research design and methods. Such formal assessment, which is usually conducted independently by at least two coders, helps members of the review team refine which studies to include in the final sample, determine whether or not the differences in quality may affect their conclusions, or guide how they analyze the data and interpret the findings ( Petticrew & Roberts, 2006 ). Ascribing quality scores to each primary study or considering through domain-based evaluations which study components have or have not been designed and executed appropriately makes it possible to reflect on the extent to which the selected study addresses possible biases and maximizes validity ( Shea et al., 2009 ). Extracting data: The following step involves gathering or extracting applicable information from each primary study included in the sample and deciding what is relevant to the problem of interest ( Cooper & Hedges, 2009 ). Indeed, the type of data that should be recorded mainly depends on the initial research questions ( Okoli & Schabram, 2010 ). However, important information may also be gathered about how, when, where and by whom the primary study was conducted, the research design and methods, or qualitative/quantitative results ( Cooper & Hedges, 2009 ). Analyzing and synthesizing data : As a final step, members of the review team must collate, summarize, aggregate, organize, and compare the evidence extracted from the included studies. The extracted data must be presented in a meaningful way that suggests a new contribution to the extant literature ( Jesson et al., 2011 ). Webster and Watson (2002) warn researchers that literature reviews should be much more than lists of papers and should provide a coherent lens to make sense of extant knowledge on a given topic. There exist several methods and techniques for synthesizing quantitative (e.g., frequency analysis, meta-analysis) and qualitative (e.g., grounded theory, narrative analysis, meta-ethnography) evidence ( Dixon-Woods, Agarwal, Jones, Young, & Sutton, 2005 ; Thomas & Harden, 2008 ).
9.3. Types of Review Articles and Brief Illustrations
EHealth researchers have at their disposal a number of approaches and methods for making sense out of existing literature, all with the purpose of casting current research findings into historical contexts or explaining contradictions that might exist among a set of primary research studies conducted on a particular topic. Our classification scheme is largely inspired from Paré and colleagues’ (2015) typology. Below we present and illustrate those review types that we feel are central to the growth and development of the eHealth domain.
9.3.1. Narrative Reviews
The narrative review is the “traditional” way of reviewing the extant literature and is skewed towards a qualitative interpretation of prior knowledge ( Sylvester et al., 2013 ). Put simply, a narrative review attempts to summarize or synthesize what has been written on a particular topic but does not seek generalization or cumulative knowledge from what is reviewed ( Davies, 2000 ; Green et al., 2006 ). Instead, the review team often undertakes the task of accumulating and synthesizing the literature to demonstrate the value of a particular point of view ( Baumeister & Leary, 1997 ). As such, reviewers may selectively ignore or limit the attention paid to certain studies in order to make a point. In this rather unsystematic approach, the selection of information from primary articles is subjective, lacks explicit criteria for inclusion and can lead to biased interpretations or inferences ( Green et al., 2006 ). There are several narrative reviews in the particular eHealth domain, as in all fields, which follow such an unstructured approach ( Silva et al., 2015 ; Paul et al., 2015 ).
Despite these criticisms, this type of review can be very useful in gathering together a volume of literature in a specific subject area and synthesizing it. As mentioned above, its primary purpose is to provide the reader with a comprehensive background for understanding current knowledge and highlighting the significance of new research ( Cronin et al., 2008 ). Faculty like to use narrative reviews in the classroom because they are often more up to date than textbooks, provide a single source for students to reference, and expose students to peer-reviewed literature ( Green et al., 2006 ). For researchers, narrative reviews can inspire research ideas by identifying gaps or inconsistencies in a body of knowledge, thus helping researchers to determine research questions or formulate hypotheses. Importantly, narrative reviews can also be used as educational articles to bring practitioners up to date with certain topics of issues ( Green et al., 2006 ).
Recently, there have been several efforts to introduce more rigour in narrative reviews that will elucidate common pitfalls and bring changes into their publication standards. Information systems researchers, among others, have contributed to advancing knowledge on how to structure a “traditional” review. For instance, Levy and Ellis (2006) proposed a generic framework for conducting such reviews. Their model follows the systematic data processing approach comprised of three steps, namely: (a) literature search and screening; (b) data extraction and analysis; and (c) writing the literature review. They provide detailed and very helpful instructions on how to conduct each step of the review process. As another methodological contribution, vom Brocke et al. (2009) offered a series of guidelines for conducting literature reviews, with a particular focus on how to search and extract the relevant body of knowledge. Last, Bandara, Miskon, and Fielt (2011) proposed a structured, predefined and tool-supported method to identify primary studies within a feasible scope, extract relevant content from identified articles, synthesize and analyze the findings, and effectively write and present the results of the literature review. We highly recommend that prospective authors of narrative reviews consult these useful sources before embarking on their work.
Darlow and Wen (2015) provide a good example of a highly structured narrative review in the eHealth field. These authors synthesized published articles that describe the development process of mobile health ( m-health ) interventions for patients’ cancer care self-management. As in most narrative reviews, the scope of the research questions being investigated is broad: (a) how development of these systems are carried out; (b) which methods are used to investigate these systems; and (c) what conclusions can be drawn as a result of the development of these systems. To provide clear answers to these questions, a literature search was conducted on six electronic databases and Google Scholar . The search was performed using several terms and free text words, combining them in an appropriate manner. Four inclusion and three exclusion criteria were utilized during the screening process. Both authors independently reviewed each of the identified articles to determine eligibility and extract study information. A flow diagram shows the number of studies identified, screened, and included or excluded at each stage of study selection. In terms of contributions, this review provides a series of practical recommendations for m-health intervention development.
9.3.2. Descriptive or Mapping Reviews
The primary goal of a descriptive review is to determine the extent to which a body of knowledge in a particular research topic reveals any interpretable pattern or trend with respect to pre-existing propositions, theories, methodologies or findings ( King & He, 2005 ; Paré et al., 2015 ). In contrast with narrative reviews, descriptive reviews follow a systematic and transparent procedure, including searching, screening and classifying studies ( Petersen, Vakkalanka, & Kuzniarz, 2015 ). Indeed, structured search methods are used to form a representative sample of a larger group of published works ( Paré et al., 2015 ). Further, authors of descriptive reviews extract from each study certain characteristics of interest, such as publication year, research methods, data collection techniques, and direction or strength of research outcomes (e.g., positive, negative, or non-significant) in the form of frequency analysis to produce quantitative results ( Sylvester et al., 2013 ). In essence, each study included in a descriptive review is treated as the unit of analysis and the published literature as a whole provides a database from which the authors attempt to identify any interpretable trends or draw overall conclusions about the merits of existing conceptualizations, propositions, methods or findings ( Paré et al., 2015 ). In doing so, a descriptive review may claim that its findings represent the state of the art in a particular domain ( King & He, 2005 ).
In the fields of health sciences and medical informatics, reviews that focus on examining the range, nature and evolution of a topic area are described by Anderson, Allen, Peckham, and Goodwin (2008) as mapping reviews . Like descriptive reviews, the research questions are generic and usually relate to publication patterns and trends. There is no preconceived plan to systematically review all of the literature although this can be done. Instead, researchers often present studies that are representative of most works published in a particular area and they consider a specific time frame to be mapped.
An example of this approach in the eHealth domain is offered by DeShazo, Lavallie, and Wolf (2009). The purpose of this descriptive or mapping review was to characterize publication trends in the medical informatics literature over a 20-year period (1987 to 2006). To achieve this ambitious objective, the authors performed a bibliometric analysis of medical informatics citations indexed in medline using publication trends, journal frequencies, impact factors, Medical Subject Headings (MeSH) term frequencies, and characteristics of citations. Findings revealed that there were over 77,000 medical informatics articles published during the covered period in numerous journals and that the average annual growth rate was 12%. The MeSH term analysis also suggested a strong interdisciplinary trend. Finally, average impact scores increased over time with two notable growth periods. Overall, patterns in research outputs that seem to characterize the historic trends and current components of the field of medical informatics suggest it may be a maturing discipline (DeShazo et al., 2009).
9.3.3. Scoping Reviews
Scoping reviews attempt to provide an initial indication of the potential size and nature of the extant literature on an emergent topic (Arksey & O’Malley, 2005; Daudt, van Mossel, & Scott, 2013 ; Levac, Colquhoun, & O’Brien, 2010). A scoping review may be conducted to examine the extent, range and nature of research activities in a particular area, determine the value of undertaking a full systematic review (discussed next), or identify research gaps in the extant literature ( Paré et al., 2015 ). In line with their main objective, scoping reviews usually conclude with the presentation of a detailed research agenda for future works along with potential implications for both practice and research.
Unlike narrative and descriptive reviews, the whole point of scoping the field is to be as comprehensive as possible, including grey literature (Arksey & O’Malley, 2005). Inclusion and exclusion criteria must be established to help researchers eliminate studies that are not aligned with the research questions. It is also recommended that at least two independent coders review abstracts yielded from the search strategy and then the full articles for study selection ( Daudt et al., 2013 ). The synthesized evidence from content or thematic analysis is relatively easy to present in tabular form (Arksey & O’Malley, 2005; Thomas & Harden, 2008 ).
One of the most highly cited scoping reviews in the eHealth domain was published by Archer, Fevrier-Thomas, Lokker, McKibbon, and Straus (2011) . These authors reviewed the existing literature on personal health record ( phr ) systems including design, functionality, implementation, applications, outcomes, and benefits. Seven databases were searched from 1985 to March 2010. Several search terms relating to phr s were used during this process. Two authors independently screened titles and abstracts to determine inclusion status. A second screen of full-text articles, again by two independent members of the research team, ensured that the studies described phr s. All in all, 130 articles met the criteria and their data were extracted manually into a database. The authors concluded that although there is a large amount of survey, observational, cohort/panel, and anecdotal evidence of phr benefits and satisfaction for patients, more research is needed to evaluate the results of phr implementations. Their in-depth analysis of the literature signalled that there is little solid evidence from randomized controlled trials or other studies through the use of phr s. Hence, they suggested that more research is needed that addresses the current lack of understanding of optimal functionality and usability of these systems, and how they can play a beneficial role in supporting patient self-management ( Archer et al., 2011 ).
9.3.4. Forms of Aggregative Reviews
Healthcare providers, practitioners, and policy-makers are nowadays overwhelmed with large volumes of information, including research-based evidence from numerous clinical trials and evaluation studies, assessing the effectiveness of health information technologies and interventions ( Ammenwerth & de Keizer, 2004 ; Deshazo et al., 2009 ). It is unrealistic to expect that all these disparate actors will have the time, skills, and necessary resources to identify the available evidence in the area of their expertise and consider it when making decisions. Systematic reviews that involve the rigorous application of scientific strategies aimed at limiting subjectivity and bias (i.e., systematic and random errors) can respond to this challenge.
Systematic reviews attempt to aggregate, appraise, and synthesize in a single source all empirical evidence that meet a set of previously specified eligibility criteria in order to answer a clearly formulated and often narrow research question on a particular topic of interest to support evidence-based practice ( Liberati et al., 2009 ). They adhere closely to explicit scientific principles ( Liberati et al., 2009 ) and rigorous methodological guidelines (Higgins & Green, 2008) aimed at reducing random and systematic errors that can lead to deviations from the truth in results or inferences. The use of explicit methods allows systematic reviews to aggregate a large body of research evidence, assess whether effects or relationships are in the same direction and of the same general magnitude, explain possible inconsistencies between study results, and determine the strength of the overall evidence for every outcome of interest based on the quality of included studies and the general consistency among them ( Cook, Mulrow, & Haynes, 1997 ). The main procedures of a systematic review involve:
- Formulating a review question and developing a search strategy based on explicit inclusion criteria for the identification of eligible studies (usually described in the context of a detailed review protocol).
- Searching for eligible studies using multiple databases and information sources, including grey literature sources, without any language restrictions.
- Selecting studies, extracting data, and assessing risk of bias in a duplicate manner using two independent reviewers to avoid random or systematic errors in the process.
- Analyzing data using quantitative or qualitative methods.
- Presenting results in summary of findings tables.
- Interpreting results and drawing conclusions.
Many systematic reviews, but not all, use statistical methods to combine the results of independent studies into a single quantitative estimate or summary effect size. Known as meta-analyses , these reviews use specific data extraction and statistical techniques (e.g., network, frequentist, or Bayesian meta-analyses) to calculate from each study by outcome of interest an effect size along with a confidence interval that reflects the degree of uncertainty behind the point estimate of effect ( Borenstein, Hedges, Higgins, & Rothstein, 2009 ; Deeks, Higgins, & Altman, 2008 ). Subsequently, they use fixed or random-effects analysis models to combine the results of the included studies, assess statistical heterogeneity, and calculate a weighted average of the effect estimates from the different studies, taking into account their sample sizes. The summary effect size is a value that reflects the average magnitude of the intervention effect for a particular outcome of interest or, more generally, the strength of a relationship between two variables across all studies included in the systematic review. By statistically combining data from multiple studies, meta-analyses can create more precise and reliable estimates of intervention effects than those derived from individual studies alone, when these are examined independently as discrete sources of information.
The review by Gurol-Urganci, de Jongh, Vodopivec-Jamsek, Atun, and Car (2013) on the effects of mobile phone messaging reminders for attendance at healthcare appointments is an illustrative example of a high-quality systematic review with meta-analysis. Missed appointments are a major cause of inefficiency in healthcare delivery with substantial monetary costs to health systems. These authors sought to assess whether mobile phone-based appointment reminders delivered through Short Message Service ( sms ) or Multimedia Messaging Service ( mms ) are effective in improving rates of patient attendance and reducing overall costs. To this end, they conducted a comprehensive search on multiple databases using highly sensitive search strategies without language or publication-type restrictions to identify all rct s that are eligible for inclusion. In order to minimize the risk of omitting eligible studies not captured by the original search, they supplemented all electronic searches with manual screening of trial registers and references contained in the included studies. Study selection, data extraction, and risk of bias assessments were performed independently by two coders using standardized methods to ensure consistency and to eliminate potential errors. Findings from eight rct s involving 6,615 participants were pooled into meta-analyses to calculate the magnitude of effects that mobile text message reminders have on the rate of attendance at healthcare appointments compared to no reminders and phone call reminders.
Meta-analyses are regarded as powerful tools for deriving meaningful conclusions. However, there are situations in which it is neither reasonable nor appropriate to pool studies together using meta-analytic methods simply because there is extensive clinical heterogeneity between the included studies or variation in measurement tools, comparisons, or outcomes of interest. In these cases, systematic reviews can use qualitative synthesis methods such as vote counting, content analysis, classification schemes and tabulations, as an alternative approach to narratively synthesize the results of the independent studies included in the review. This form of review is known as qualitative systematic review.
A rigorous example of one such review in the eHealth domain is presented by Mickan, Atherton, Roberts, Heneghan, and Tilson (2014) on the use of handheld computers by healthcare professionals and their impact on access to information and clinical decision-making. In line with the methodological guidelines for systematic reviews, these authors: (a) developed and registered with prospero ( www.crd.york.ac.uk/ prospero / ) an a priori review protocol; (b) conducted comprehensive searches for eligible studies using multiple databases and other supplementary strategies (e.g., forward searches); and (c) subsequently carried out study selection, data extraction, and risk of bias assessments in a duplicate manner to eliminate potential errors in the review process. Heterogeneity between the included studies in terms of reported outcomes and measures precluded the use of meta-analytic methods. To this end, the authors resorted to using narrative analysis and synthesis to describe the effectiveness of handheld computers on accessing information for clinical knowledge, adherence to safety and clinical quality guidelines, and diagnostic decision-making.
In recent years, the number of systematic reviews in the field of health informatics has increased considerably. Systematic reviews with discordant findings can cause great confusion and make it difficult for decision-makers to interpret the review-level evidence ( Moher, 2013 ). Therefore, there is a growing need for appraisal and synthesis of prior systematic reviews to ensure that decision-making is constantly informed by the best available accumulated evidence. Umbrella reviews , also known as overviews of systematic reviews, are tertiary types of evidence synthesis that aim to accomplish this; that is, they aim to compare and contrast findings from multiple systematic reviews and meta-analyses ( Becker & Oxman, 2008 ). Umbrella reviews generally adhere to the same principles and rigorous methodological guidelines used in systematic reviews. However, the unit of analysis in umbrella reviews is the systematic review rather than the primary study ( Becker & Oxman, 2008 ). Unlike systematic reviews that have a narrow focus of inquiry, umbrella reviews focus on broader research topics for which there are several potential interventions ( Smith, Devane, Begley, & Clarke, 2011 ). A recent umbrella review on the effects of home telemonitoring interventions for patients with heart failure critically appraised, compared, and synthesized evidence from 15 systematic reviews to investigate which types of home telemonitoring technologies and forms of interventions are more effective in reducing mortality and hospital admissions ( Kitsiou, Paré, & Jaana, 2015 ).
9.3.5. Realist Reviews
Realist reviews are theory-driven interpretative reviews developed to inform, enhance, or supplement conventional systematic reviews by making sense of heterogeneous evidence about complex interventions applied in diverse contexts in a way that informs policy decision-making ( Greenhalgh, Wong, Westhorp, & Pawson, 2011 ). They originated from criticisms of positivist systematic reviews which centre on their “simplistic” underlying assumptions ( Oates, 2011 ). As explained above, systematic reviews seek to identify causation. Such logic is appropriate for fields like medicine and education where findings of randomized controlled trials can be aggregated to see whether a new treatment or intervention does improve outcomes. However, many argue that it is not possible to establish such direct causal links between interventions and outcomes in fields such as social policy, management, and information systems where for any intervention there is unlikely to be a regular or consistent outcome ( Oates, 2011 ; Pawson, 2006 ; Rousseau, Manning, & Denyer, 2008 ).
To circumvent these limitations, Pawson, Greenhalgh, Harvey, and Walshe (2005) have proposed a new approach for synthesizing knowledge that seeks to unpack the mechanism of how “complex interventions” work in particular contexts. The basic research question — what works? — which is usually associated with systematic reviews changes to: what is it about this intervention that works, for whom, in what circumstances, in what respects and why? Realist reviews have no particular preference for either quantitative or qualitative evidence. As a theory-building approach, a realist review usually starts by articulating likely underlying mechanisms and then scrutinizes available evidence to find out whether and where these mechanisms are applicable ( Shepperd et al., 2009 ). Primary studies found in the extant literature are viewed as case studies which can test and modify the initial theories ( Rousseau et al., 2008 ).
The main objective pursued in the realist review conducted by Otte-Trojel, de Bont, Rundall, and van de Klundert (2014) was to examine how patient portals contribute to health service delivery and patient outcomes. The specific goals were to investigate how outcomes are produced and, most importantly, how variations in outcomes can be explained. The research team started with an exploratory review of background documents and research studies to identify ways in which patient portals may contribute to health service delivery and patient outcomes. The authors identified six main ways which represent “educated guesses” to be tested against the data in the evaluation studies. These studies were identified through a formal and systematic search in four databases between 2003 and 2013. Two members of the research team selected the articles using a pre-established list of inclusion and exclusion criteria and following a two-step procedure. The authors then extracted data from the selected articles and created several tables, one for each outcome category. They organized information to bring forward those mechanisms where patient portals contribute to outcomes and the variation in outcomes across different contexts.
9.3.6. Critical Reviews
Lastly, critical reviews aim to provide a critical evaluation and interpretive analysis of existing literature on a particular topic of interest to reveal strengths, weaknesses, contradictions, controversies, inconsistencies, and/or other important issues with respect to theories, hypotheses, research methods or results ( Baumeister & Leary, 1997 ; Kirkevold, 1997 ). Unlike other review types, critical reviews attempt to take a reflective account of the research that has been done in a particular area of interest, and assess its credibility by using appraisal instruments or critical interpretive methods. In this way, critical reviews attempt to constructively inform other scholars about the weaknesses of prior research and strengthen knowledge development by giving focus and direction to studies for further improvement ( Kirkevold, 1997 ).
Kitsiou, Paré, and Jaana (2013) provide an example of a critical review that assessed the methodological quality of prior systematic reviews of home telemonitoring studies for chronic patients. The authors conducted a comprehensive search on multiple databases to identify eligible reviews and subsequently used a validated instrument to conduct an in-depth quality appraisal. Results indicate that the majority of systematic reviews in this particular area suffer from important methodological flaws and biases that impair their internal validity and limit their usefulness for clinical and decision-making purposes. To this end, they provide a number of recommendations to strengthen knowledge development towards improving the design and execution of future reviews on home telemonitoring.
9.4. Summary
Table 9.1 outlines the main types of literature reviews that were described in the previous sub-sections and summarizes the main characteristics that distinguish one review type from another. It also includes key references to methodological guidelines and useful sources that can be used by eHealth scholars and researchers for planning and developing reviews.
Typology of Literature Reviews (adapted from Paré et al., 2015).
As shown in Table 9.1 , each review type addresses different kinds of research questions or objectives, which subsequently define and dictate the methods and approaches that need to be used to achieve the overarching goal(s) of the review. For example, in the case of narrative reviews, there is greater flexibility in searching and synthesizing articles ( Green et al., 2006 ). Researchers are often relatively free to use a diversity of approaches to search, identify, and select relevant scientific articles, describe their operational characteristics, present how the individual studies fit together, and formulate conclusions. On the other hand, systematic reviews are characterized by their high level of systematicity, rigour, and use of explicit methods, based on an “a priori” review plan that aims to minimize bias in the analysis and synthesis process (Higgins & Green, 2008). Some reviews are exploratory in nature (e.g., scoping/mapping reviews), whereas others may be conducted to discover patterns (e.g., descriptive reviews) or involve a synthesis approach that may include the critical analysis of prior research ( Paré et al., 2015 ). Hence, in order to select the most appropriate type of review, it is critical to know before embarking on a review project, why the research synthesis is conducted and what type of methods are best aligned with the pursued goals.
9.5. Concluding Remarks
In light of the increased use of evidence-based practice and research generating stronger evidence ( Grady et al., 2011 ; Lyden et al., 2013 ), review articles have become essential tools for summarizing, synthesizing, integrating or critically appraising prior knowledge in the eHealth field. As mentioned earlier, when rigorously conducted review articles represent powerful information sources for eHealth scholars and practitioners looking for state-of-the-art evidence. The typology of literature reviews we used herein will allow eHealth researchers, graduate students and practitioners to gain a better understanding of the similarities and differences between review types.
We must stress that this classification scheme does not privilege any specific type of review as being of higher quality than another ( Paré et al., 2015 ). As explained above, each type of review has its own strengths and limitations. Having said that, we realize that the methodological rigour of any review — be it qualitative, quantitative or mixed — is a critical aspect that should be considered seriously by prospective authors. In the present context, the notion of rigour refers to the reliability and validity of the review process described in section 9.2. For one thing, reliability is related to the reproducibility of the review process and steps, which is facilitated by a comprehensive documentation of the literature search process, extraction, coding and analysis performed in the review. Whether the search is comprehensive or not, whether it involves a methodical approach for data extraction and synthesis or not, it is important that the review documents in an explicit and transparent manner the steps and approach that were used in the process of its development. Next, validity characterizes the degree to which the review process was conducted appropriately. It goes beyond documentation and reflects decisions related to the selection of the sources, the search terms used, the period of time covered, the articles selected in the search, and the application of backward and forward searches ( vom Brocke et al., 2009 ). In short, the rigour of any review article is reflected by the explicitness of its methods (i.e., transparency) and the soundness of the approach used. We refer those interested in the concepts of rigour and quality to the work of Templier and Paré (2015) which offers a detailed set of methodological guidelines for conducting and evaluating various types of review articles.
To conclude, our main objective in this chapter was to demystify the various types of literature reviews that are central to the continuous development of the eHealth field. It is our hope that our descriptive account will serve as a valuable source for those conducting, evaluating or using reviews in this important and growing domain.
- Ammenwerth E., de Keizer N. An inventory of evaluation studies of information technology in health care. Trends in evaluation research, 1982-2002. International Journal of Medical Informatics. 2004; 44 (1):44–56. [ PubMed : 15778794 ]
- Anderson S., Allen P., Peckham S., Goodwin N. Asking the right questions: scoping studies in the commissioning of research on the organisation and delivery of health services. Health Research Policy and Systems. 2008; 6 (7):1–12. [ PMC free article : PMC2500008 ] [ PubMed : 18613961 ] [ CrossRef ]
- Archer N., Fevrier-Thomas U., Lokker C., McKibbon K. A., Straus S.E. Personal health records: a scoping review. Journal of American Medical Informatics Association. 2011; 18 (4):515–522. [ PMC free article : PMC3128401 ] [ PubMed : 21672914 ]
- Arksey H., O’Malley L. Scoping studies: towards a methodological framework. International Journal of Social Research Methodology. 2005; 8 (1):19–32.
- A systematic, tool-supported method for conducting literature reviews in information systems. Paper presented at the Proceedings of the 19th European Conference on Information Systems ( ecis 2011); June 9 to 11; Helsinki, Finland. 2011.
- Baumeister R. F., Leary M.R. Writing narrative literature reviews. Review of General Psychology. 1997; 1 (3):311–320.
- Becker L. A., Oxman A.D. In: Cochrane handbook for systematic reviews of interventions. Higgins J. P. T., Green S., editors. Hoboken, nj : John Wiley & Sons, Ltd; 2008. Overviews of reviews; pp. 607–631.
- Borenstein M., Hedges L., Higgins J., Rothstein H. Introduction to meta-analysis. Hoboken, nj : John Wiley & Sons Inc; 2009.
- Cook D. J., Mulrow C. D., Haynes B. Systematic reviews: Synthesis of best evidence for clinical decisions. Annals of Internal Medicine. 1997; 126 (5):376–380. [ PubMed : 9054282 ]
- Cooper H., Hedges L.V. In: The handbook of research synthesis and meta-analysis. 2nd ed. Cooper H., Hedges L. V., Valentine J. C., editors. New York: Russell Sage Foundation; 2009. Research synthesis as a scientific process; pp. 3–17.
- Cooper H. M. Organizing knowledge syntheses: A taxonomy of literature reviews. Knowledge in Society. 1988; 1 (1):104–126.
- Cronin P., Ryan F., Coughlan M. Undertaking a literature review: a step-by-step approach. British Journal of Nursing. 2008; 17 (1):38–43. [ PubMed : 18399395 ]
- Darlow S., Wen K.Y. Development testing of mobile health interventions for cancer patient self-management: A review. Health Informatics Journal. 2015 (online before print). [ PubMed : 25916831 ] [ CrossRef ]
- Daudt H. M., van Mossel C., Scott S.J. Enhancing the scoping study methodology: a large, inter-professional team’s experience with Arksey and O’Malley’s framework. bmc Medical Research Methodology. 2013; 13 :48. [ PMC free article : PMC3614526 ] [ PubMed : 23522333 ] [ CrossRef ]
- Davies P. The relevance of systematic reviews to educational policy and practice. Oxford Review of Education. 2000; 26 (3-4):365–378.
- Deeks J. J., Higgins J. P. T., Altman D.G. In: Cochrane handbook for systematic reviews of interventions. Higgins J. P. T., Green S., editors. Hoboken, nj : John Wiley & Sons, Ltd; 2008. Analysing data and undertaking meta-analyses; pp. 243–296.
- Deshazo J. P., Lavallie D. L., Wolf F.M. Publication trends in the medical informatics literature: 20 years of “Medical Informatics” in mesh . bmc Medical Informatics and Decision Making. 2009; 9 :7. [ PMC free article : PMC2652453 ] [ PubMed : 19159472 ] [ CrossRef ]
- Dixon-Woods M., Agarwal S., Jones D., Young B., Sutton A. Synthesising qualitative and quantitative evidence: a review of possible methods. Journal of Health Services Research and Policy. 2005; 10 (1):45–53. [ PubMed : 15667704 ]
- Finfgeld-Connett D., Johnson E.D. Literature search strategies for conducting knowledge-building and theory-generating qualitative systematic reviews. Journal of Advanced Nursing. 2013; 69 (1):194–204. [ PMC free article : PMC3424349 ] [ PubMed : 22591030 ]
- Grady B., Myers K. M., Nelson E. L., Belz N., Bennett L., Carnahan L. … Guidelines Working Group. Evidence-based practice for telemental health. Telemedicine Journal and E Health. 2011; 17 (2):131–148. [ PubMed : 21385026 ]
- Green B. N., Johnson C. D., Adams A. Writing narrative literature reviews for peer-reviewed journals: secrets of the trade. Journal of Chiropractic Medicine. 2006; 5 (3):101–117. [ PMC free article : PMC2647067 ] [ PubMed : 19674681 ]
- Greenhalgh T., Wong G., Westhorp G., Pawson R. Protocol–realist and meta-narrative evidence synthesis: evolving standards ( rameses ). bmc Medical Research Methodology. 2011; 11 :115. [ PMC free article : PMC3173389 ] [ PubMed : 21843376 ]
- Gurol-Urganci I., de Jongh T., Vodopivec-Jamsek V., Atun R., Car J. Mobile phone messaging reminders for attendance at healthcare appointments. Cochrane Database System Review. 2013; 12 cd 007458. [ PMC free article : PMC6485985 ] [ PubMed : 24310741 ] [ CrossRef ]
- Hart C. Doing a literature review: Releasing the social science research imagination. London: SAGE Publications; 1998.
- Higgins J. P. T., Green S., editors. Cochrane handbook for systematic reviews of interventions: Cochrane book series. Hoboken, nj : Wiley-Blackwell; 2008.
- Jesson J., Matheson L., Lacey F.M. Doing your literature review: traditional and systematic techniques. Los Angeles & London: SAGE Publications; 2011.
- King W. R., He J. Understanding the role and methods of meta-analysis in IS research. Communications of the Association for Information Systems. 2005; 16 :1.
- Kirkevold M. Integrative nursing research — an important strategy to further the development of nursing science and nursing practice. Journal of Advanced Nursing. 1997; 25 (5):977–984. [ PubMed : 9147203 ]
- Kitchenham B., Charters S. ebse Technical Report Version 2.3. Keele & Durham. uk : Keele University & University of Durham; 2007. Guidelines for performing systematic literature reviews in software engineering.
- Kitsiou S., Paré G., Jaana M. Systematic reviews and meta-analyses of home telemonitoring interventions for patients with chronic diseases: a critical assessment of their methodological quality. Journal of Medical Internet Research. 2013; 15 (7):e150. [ PMC free article : PMC3785977 ] [ PubMed : 23880072 ]
- Kitsiou S., Paré G., Jaana M. Effects of home telemonitoring interventions on patients with chronic heart failure: an overview of systematic reviews. Journal of Medical Internet Research. 2015; 17 (3):e63. [ PMC free article : PMC4376138 ] [ PubMed : 25768664 ]
- Levac D., Colquhoun H., O’Brien K. K. Scoping studies: advancing the methodology. Implementation Science. 2010; 5 (1):69. [ PMC free article : PMC2954944 ] [ PubMed : 20854677 ]
- Levy Y., Ellis T.J. A systems approach to conduct an effective literature review in support of information systems research. Informing Science. 2006; 9 :181–211.
- Liberati A., Altman D. G., Tetzlaff J., Mulrow C., Gøtzsche P. C., Ioannidis J. P. A. et al. Moher D. The prisma statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Annals of Internal Medicine. 2009; 151 (4):W-65. [ PubMed : 19622512 ]
- Lyden J. R., Zickmund S. L., Bhargava T. D., Bryce C. L., Conroy M. B., Fischer G. S. et al. McTigue K. M. Implementing health information technology in a patient-centered manner: Patient experiences with an online evidence-based lifestyle intervention. Journal for Healthcare Quality. 2013; 35 (5):47–57. [ PubMed : 24004039 ]
- Mickan S., Atherton H., Roberts N. W., Heneghan C., Tilson J.K. Use of handheld computers in clinical practice: a systematic review. bmc Medical Informatics and Decision Making. 2014; 14 :56. [ PMC free article : PMC4099138 ] [ PubMed : 24998515 ]
- Moher D. The problem of duplicate systematic reviews. British Medical Journal. 2013; 347 (5040) [ PubMed : 23945367 ] [ CrossRef ]
- Montori V. M., Wilczynski N. L., Morgan D., Haynes R. B., Hedges T. Systematic reviews: a cross-sectional study of location and citation counts. bmc Medicine. 2003; 1 :2. [ PMC free article : PMC281591 ] [ PubMed : 14633274 ]
- Mulrow C. D. The medical review article: state of the science. Annals of Internal Medicine. 1987; 106 (3):485–488. [ PubMed : 3813259 ] [ CrossRef ]
- Evidence-based information systems: A decade later. Proceedings of the European Conference on Information Systems ; 2011. Retrieved from http://aisel .aisnet.org/cgi/viewcontent .cgi?article =1221&context =ecis2011 .
- Okoli C., Schabram K. A guide to conducting a systematic literature review of information systems research. ssrn Electronic Journal. 2010
- Otte-Trojel T., de Bont A., Rundall T. G., van de Klundert J. How outcomes are achieved through patient portals: a realist review. Journal of American Medical Informatics Association. 2014; 21 (4):751–757. [ PMC free article : PMC4078283 ] [ PubMed : 24503882 ]
- Paré G., Trudel M.-C., Jaana M., Kitsiou S. Synthesizing information systems knowledge: A typology of literature reviews. Information & Management. 2015; 52 (2):183–199.
- Patsopoulos N. A., Analatos A. A., Ioannidis J.P. A. Relative citation impact of various study designs in the health sciences. Journal of the American Medical Association. 2005; 293 (19):2362–2366. [ PubMed : 15900006 ]
- Paul M. M., Greene C. M., Newton-Dame R., Thorpe L. E., Perlman S. E., McVeigh K. H., Gourevitch M.N. The state of population health surveillance using electronic health records: A narrative review. Population Health Management. 2015; 18 (3):209–216. [ PubMed : 25608033 ]
- Pawson R. Evidence-based policy: a realist perspective. London: SAGE Publications; 2006.
- Pawson R., Greenhalgh T., Harvey G., Walshe K. Realist review—a new method of systematic review designed for complex policy interventions. Journal of Health Services Research & Policy. 2005; 10 (Suppl 1):21–34. [ PubMed : 16053581 ]
- Petersen K., Vakkalanka S., Kuzniarz L. Guidelines for conducting systematic mapping studies in software engineering: An update. Information and Software Technology. 2015; 64 :1–18.
- Petticrew M., Roberts H. Systematic reviews in the social sciences: A practical guide. Malden, ma : Blackwell Publishing Co; 2006.
- Rousseau D. M., Manning J., Denyer D. Evidence in management and organizational science: Assembling the field’s full weight of scientific knowledge through syntheses. The Academy of Management Annals. 2008; 2 (1):475–515.
- Rowe F. What literature review is not: diversity, boundaries and recommendations. European Journal of Information Systems. 2014; 23 (3):241–255.
- Shea B. J., Hamel C., Wells G. A., Bouter L. M., Kristjansson E., Grimshaw J. et al. Boers M. amstar is a reliable and valid measurement tool to assess the methodological quality of systematic reviews. Journal of Clinical Epidemiology. 2009; 62 (10):1013–1020. [ PubMed : 19230606 ]
- Shepperd S., Lewin S., Straus S., Clarke M., Eccles M. P., Fitzpatrick R. et al. Sheikh A. Can we systematically review studies that evaluate complex interventions? PLoS Medicine. 2009; 6 (8):e1000086. [ PMC free article : PMC2717209 ] [ PubMed : 19668360 ]
- Silva B. M., Rodrigues J. J., de la Torre Díez I., López-Coronado M., Saleem K. Mobile-health: A review of current state in 2015. Journal of Biomedical Informatics. 2015; 56 :265–272. [ PubMed : 26071682 ]
- Smith V., Devane D., Begley C., Clarke M. Methodology in conducting a systematic review of systematic reviews of healthcare interventions. bmc Medical Research Methodology. 2011; 11 (1):15. [ PMC free article : PMC3039637 ] [ PubMed : 21291558 ]
- Sylvester A., Tate M., Johnstone D. Beyond synthesis: re-presenting heterogeneous research literature. Behaviour & Information Technology. 2013; 32 (12):1199–1215.
- Templier M., Paré G. A framework for guiding and evaluating literature reviews. Communications of the Association for Information Systems. 2015; 37 (6):112–137.
- Thomas J., Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. bmc Medical Research Methodology. 2008; 8 (1):45. [ PMC free article : PMC2478656 ] [ PubMed : 18616818 ]
- Reconstructing the giant: on the importance of rigour in documenting the literature search process. Paper presented at the Proceedings of the 17th European Conference on Information Systems ( ecis 2009); Verona, Italy. 2009.
- Webster J., Watson R.T. Analyzing the past to prepare for the future: Writing a literature review. Management Information Systems Quarterly. 2002; 26 (2):11.
- Whitlock E. P., Lin J. S., Chou R., Shekelle P., Robinson K.A. Using existing systematic reviews in complex systematic reviews. Annals of Internal Medicine. 2008; 148 (10):776–782. [ PubMed : 18490690 ]
This publication is licensed under a Creative Commons License, Attribution-Noncommercial 4.0 International License (CC BY-NC 4.0): see https://creativecommons.org/licenses/by-nc/4.0/
- Cite this Page Paré G, Kitsiou S. Chapter 9 Methods for Literature Reviews. In: Lau F, Kuziemsky C, editors. Handbook of eHealth Evaluation: An Evidence-based Approach [Internet]. Victoria (BC): University of Victoria; 2017 Feb 27.
- PDF version of this title (4.5M)
- Disable Glossary Links
In this Page
- Introduction
- Overview of the Literature Review Process and Steps
- Types of Review Articles and Brief Illustrations
- Concluding Remarks
Related information
- PMC PubMed Central citations
- PubMed Links to PubMed
Recent Activity
- Chapter 9 Methods for Literature Reviews - Handbook of eHealth Evaluation: An Ev... Chapter 9 Methods for Literature Reviews - Handbook of eHealth Evaluation: An Evidence-based Approach
Your browsing activity is empty.
Activity recording is turned off.
Turn recording back on
Connect with NLM
National Library of Medicine 8600 Rockville Pike Bethesda, MD 20894
Web Policies FOIA HHS Vulnerability Disclosure
Help Accessibility Careers
- Open access
- Published: 28 May 2024
Leadership in intellectual disability practice: design, development, and evaluation of a programme to support practice
- Owen Doody 1 ,
- Maeve O’Halloran 2 ,
- Eileen Carey 1 ,
- Marie Kilduff 3 ,
- Ann Gilmartin 4 &
- Ruth Ryan 1
BMC Health Services Research volume 24 , Article number: 674 ( 2024 ) Cite this article
Metrics details
Intellectual disability services have and continue to experience changes in service provision. This has an implication for leadership in practice as the quality of leadership has a direct influence on staff practice and care provided.
To design, deliver, and evaluate a leadership programme for nurse and social care managers in Ireland.
An accredited programme was designed based on evidence from literature, practice, and national expertise. A cross-sectional survey was used to collect information on the attitudes and behaviour of participants before commencing and after completing the programme. Data from the questionnaires were analysed using SPSS and open-ended questions were analysed using content analysis.
Intellectual disability services.
Participants
102 participants completed the programme and survey.
Pre-post survey and reported using the CROSS guidelines.
Participants’ expectations were rated highly, and all items scored higher in the post-survey. Qualitative data was overall positive regarding opportunities for more time to work through each aspect of the programme. The key learning was through the forum day where participants shared their group projects.
Conclusions
Overall, the programme was positively evaluated and through engaging with the programme participants’ perceptions moved from seeing leadership as mostly task-oriented to realising that qualities such as good communication, person-centredness, advocacy, supporting, role modelling, and empowering are key to leadership.
Peer Review reports
Introduction
Irish intellectual disability services have experienced a changing landscape of service provision over the past three decades [ 1 ]. This evolving landscape has seen a movement towards community settings, a changing culture, the provision of personalised supports, and a changing demographic profile [ 2 ]. Irish intellectual disability services are primarily funded through a combination of government allocations, health service budgets, and contributions from non-profit organisations. In Ireland, the context of practice leadership in intellectual disability services is shaped by various factors, including historical, societal, and political influences. The provision of support for people with intellectual disability has undergone significant changes over the years, often in response to various pressures and challenges within the healthcare system and broader society. One significant pressure for changing support provision has been the occurrence of hospital scandals, which have highlighted shortcomings in the care and treatment of individuals with intellectual disability. These scandals, exposed instances of neglect, abuse, and substandard living conditions within residential care settings and highlighted the urgent need for reform and improvement in the delivery of services for individuals with intellectual disability. Key policy documents and strategies guiding change in Ireland include; Time to Move on from Congregated Settings [ 3 ], Progressing Disability Services for Children and Young People [ 4 ], New Directions [ 5 ], A National Framework for Person-Centred Planning in Services for Persons with a Disability 6 , UNCRPD [ 7 ], Assisted Decision Making (Capacity) Act [ 8 ] and Sláintecare [ 9 ]. These policy documents and strategies have implications for intellectual disability services in terms of leadership, professional care, and support skills required to address the needs of people with intellectual disability (and their families). Key principles within these policies/strategies are person-centred care, rights, quality, safety, and risk management and in line with Irish policies, all designated centres for people with disabilities (children and adults) must be registered with the Health Information and Quality Authority (HIQA) since November 2013.
All registered designated centres are subject to inspections by HIQA inspectors who examine and evaluate services to safeguard that they comply with the National Standards for Residential Services for Children and Adults with Disabilities [ 10 ]. The legislation underpinning the standards also necessitates that a Person-in-Charge (PIC) for each designated centre be appointed and that the PIC should have relevant clinical and leadership skills and experience to safeguard the effective administration of their service and deliver safe, effective care to support clients/service users and their families. Under the most recent HIQA guidance [ 11 ], a PIC should have the appropriate qualifications to fulfil the post and have the relevant skills and experience to effectively manage the size of the centre, the number of residents, and the assessed needs of the residents. A PIC may be over more than one designated centre and variations exist in the number of designated centres and the number of residents. However, the specific requirement for leadership knowledge is vague with a requirement of 3 years in a management or supervisory role.
In the context of practice leadership for frontline managers, such as PICs in intellectual disability services in Ireland frontline managers often lead interdisciplinary teams comprising various professionals, including nurses, social care workers, psychologists, therapists, and support staff. Nurses in intellectual disability services may indeed work in both social care settings, such as community residences or day centres, and residential care settings, depending on the needs of the individuals they support. Ireland’s intellectual disability services encompass a mixed economy of care, involving voluntary, private, and state-managed organisations, and comprise a diverse range of supports tailored to meet the needs of individuals across the lifespan. Services vary in size, with some supporting a small number of residents in shared living arrangements, while others may accommodate larger groups. The exact number and size of services fluctuate across regions based on population demographics, local demand, and available resources.
The significance of leadership has been emphasised in the literature [ 12 , 13 ] and National reports [ 14 , 15 ]. Evidence within the international literature indicates that the quality of front-line management and leadership is a multi-faceted and complex role and has a direct influence on staff practice [ 16 , 17 ]. In recognition of the impact of leadership and the rapidly changing health and social care environments, there is a need to support managers/leaders working in intellectual disability services to provide support in the form of education and training to meet the PIC requirements/role. The National Clinical Leadership Centre for Nursing and Midwifery (NCLC) commissioned the authors to design, deliver, and evaluate a leadership programme for Clinical Nurse Manager (CNM) and Social Care Leader (SCL) grades with PIC responsibilities. The programme was developed based on preliminary work with CNMs and SCLs from intellectual disability services to identify core elements and priority areas of leadership competencies in intellectual disability health and social care leadership roles. This co-design element informed the development of the NCLC’s seven competencies (self-awareness, empowerment, advocacy, communication, decision-making, quality and safety, and teamwork) that underpinned the programme. To support the co-design of the programme an experienced intellectual disability nurse with experience in inspections, leadership, management, and consultancy work supported the design, delivery, and evaluation process (MO’H).
The need for leadership within all staff in the health and social care system has been expressed [ 18 ] and within intellectual disability, staff are from either a nursing or social care context who respond to situations that require intervention. Such responses require initiative, resourcefulness, motivation, an ability to solve problems, active awareness, persistence to achieve goals, and communication with team members i.e., leadership [ 19 ]. Effective leadership improves client/service user satisfaction and care outcomes [ 20 , 21 ] and while leadership is customarily considered in the context of upper management roles [ 22 ], leadership and teamwork within practice has gained interest [ 23 ]. The move away from a transactional model of leadership which emphasised a hierarchical top-down management structure 24 , has seen a shift to an approach that seeks to develop; the ethos, values, and motivation of team members, and effective relationships, communication, empowerment, and engagement of all staff [ 25 ]. Also, it is recognised that health and social care organisations, should support leadership that focuses on team building, work relationships, promoting participation, and the co-creation and facilitation of care processes [ 19 ].
Addressing leadership and supporting leaders is fundamental to intellectual disability organisations/service providers as they face numerous challenges that impact the effectiveness, efficiency, and sustainability of service design and delivery. Such impacts are seen in licensing requirements, accreditation standards, performance monitoring, and consumer expectations and this calls for a new kind of leadership away from heroic individual leaders to a model of distributed leadership across organisations and systems [ 26 ]. As we face the future, we must continually question if standard practices are working well, and how we will enhance personal outcomes and generate organisation outputs that reflect a good return on investment. Given that effective leadership is vital to prevent poor standards and ensure people with intellectual disability experience significant improvements in their lives there is a need for new leadership approaches and thinking within health and social services [ 27 ]. This paper describes the design, delivery, and evaluation of a leadership programme for CNMs and SCLs with PIC responsibilities in Ireland.
Methodology
Programme design and delivery.
Within the programme design stage, the academic leads, members of the NCLC, and the CNMs and SCLs involved in the preliminary work assisted in co-designed the programme based on the evidence from the literature and the NCLC seven leadership competencies. Within the co-design process, it was agreed academic and professional accreditation was important to value participant engagement and work. To acknowledge this firstly, the programme was submitted to the Nursing and Midwifery Board of Ireland (NMBI) to gain professional accreditation (5.5 days) and the maximum 35 Continuing Education Units (CEUs). The second accreditation process involved presenting the programme in a module format (9 Credit (ECTS) Level 9) for academic accreditation which would enable access to postgraduate level 9 courses for those who do not hold a degree level qualification (programme learning outline/outcomes Table 1 ).
The programme philosophy aimed to enhance participants’ confidence and skills to enable them to effectively apply these skills in developing plans for improvement or change. Moreover, to empower them to initiate initiatives in practice that prioritise the delivery of person-centred care and support. Participants were encouraged to draw on their experiences of practice and explore theories and models of leadership and management within the context of health and social care practice. Participants explored aspects of PIC leadership and management, focusing on learning, quality, and improvement e.g., communication, empowerment, decision-making, operational management, effective governance, and administration of the designated centres, health promotion, and protection activities, and supporting a safe quality service.
Participants were recruited through national intellectual disability services, where a poster advert for the programme was sent for distribution within the organisation. To avail of a place participants had to have service support and release to attend the 5.5-day programme and other than travel the programme was free to the service and participant. The programme delivery was coordinated by the lead author (OD) and facilitated in person by the academic leads, guests with leadership roles in health and social care services or leadership centres, and the intellectual disability nurse as part of the co-design team. Participants would reflect on their learning and document their professional knowledge through reflective inquiry. The accumulation of learning would be presented as group projects in a half-day event (forum day) open to service providers and staff. The forum day consisted of an opening presentation to mark the focus of the programme, a speaker from the NCLC, the group presentations, an invited inspirational guest speaker on leadership, and a closing event. Projects for the forum day (Table 2 ) were decided upon based on identifying areas of practice and leadership that participants wished to address and develop within their practice and translated across services so the group could benefit and participate. This process ensured initiatives spanned across services and was supported and mentored by the intellectual disability nurse on the co-design team.
Evaluation process
The forum day was the evaluation process for the project undertaken and this was assessed by academic colleagues, members of the NCLC, and service managers based on the value of the project to practice, its transferability across service, and its impact on client/service users lives. Permission to conduct the study was granted by the lead author’s University Research Ethics Committee (Education and Health Sciences, Research Ethics Committee), and participant’s rights to confidentiality and anonymity were upheld throughout the conduct of this study. Participants were Clinical Nurse Managers (1 or 2) or Social Care Managers with PIC responsibilities working in residential services for people with intellectual disability in Ireland. Four programmes were delivered over two years February to June and September to January with 25 to 30 participants per cohort. In total across the four programmes 110 participants registered of which 102 completed the programme. Attrition of the eight participants was due to personal reasons ( n = 1), issues regarding release from work due to staff shortages ( n = 6) and moving to a new job ( n = 1). A cross-sectional survey tool developed by the researchers for this study (Supplementary file S1 ) was used to collect information on the attitudes and behaviour of the participants before commencing and after completing the programme. The survey tool was developed for this study as this was a new programme and creating the survey tool allowed for the tailoring of questions to address the specific evaluation and unique elements of the programme. A hard copy format was distributed before the programme commenced and after the forum day and returned by participants on the day or by post. Data collection and analysis were managed by the intellectual disability nurse who was part of the co-design team. The questionnaire consisted of 53 questions divided into five sections. Section one covered demographic details (Q1-Q13), section two addressed aspects before commencing the programme (Q14-Q22), section three addressed expectations during the programme (Q23-Q33), section four addressed expectations upon completion of the programme (Q34-Q52) and section five (Q53) were an open text for additional comments to add depth and give meaning to participants experience. Data from the questionnaire pre/post were analysed using SPSS where descriptive statistics and a Cronbach value (α) were calculated to check the reliability of each subsection. Elo and Kyngäs [ 28 ] systematic approach to content analysis was used for categorising and analysing the textual data to identify patterns, themes, or relationships.
As part of the programme evaluation, a pre-post self-report survey was used to capture demographic details, perceptions regarding commencing the programme, expectations during the programme, and expectations upon completion of the programme. Of the participants on the programme, 15 (14.7%) were male and 87 (85.3%) were female with 93 (91.2%) working full-time and the remaining 9 (8.8%) working part-time. From a working pattern perspective, 52 (51%) worked day duty with no weekends, 31 (30.4%) worked day duty with weekends, and 19 (18.6%) worked shift work including nights. General demographic details of age, role, qualification, and years of experience are presented in Table 3 . Cronbach’s alpha was calculated to measure the internal consistency of scale reliability with the three scales performing well for the pre and post survey; scale 1 perceptions regarding commencing the programme, α (0.689 pre, 0.860 post), scale 2 expectation during the programme α (0.712 pre, 0.787 post) and scale 3 expectation upon completion of the programme α (0.960 pre, 0.943 post).
Scale one measured participants’ perception regarding the programme, and pre- and post-program delivery. Participants’ expectations were rated highly and regardless of the high expectation evident in the pre-survey all items did perform and scored higher in the post-survey. Of note was that participants rated the question on the programme assisting in the prospect of promotion lowest (58.8%) in the pre-survey and while it remained lowest in the post-survey it had increased to 91.2% indicating the potential and perceived value of the programme for the participant’s career advancement. The overall scoring of each item on the scale is presented in Table 4 .
The second scale measured participants expectations regarding the programme, pre- and post-programme delivery. Again, participants’ expectations were rated highly and regardless of the high expectation evident in the pre-survey all items did perform and scored higher in the post-survey. Of note was that participants rated the question on their perceived difficulty in adjusting to academic life lowest (39.2%) in the pre-survey and while it remained lowest in the post-survey it had increased to 78.4% indicating the difficulty participants have in balancing academic work, their daily work and family life. This is surprising given that 87.3% of the participants held a degree level or above. However, 87.3% were 11 years or more post qualification and participants’ difficulty may relate to their time out of education. The overall scoring of each item on the scale is presented in Table 4 .
The third scale measured participants’ expectations regarding the programme upon completion and pre- and post-programme delivery. Again, participants’ expectations were rated highly and regardless of the high expectation evident in the pre-survey all items did perform and scored higher in the post-survey. Of note was that participants rated the question on the possibility of the programme increasing their responsibility lowest (53.9%) in the pre-survey and while it remained lowest in the post-survey it had increased to 87.3% indicating that because of the programme participants perceived their level of responsibility had increased. The overall scoring of each item on the scale is presented in Table 4 .
Data from the qualitative open questions addressed; learning, anything participants would change, topics that participants would like included in the programme, the forum day, and general comments.
Qualitative comments regarding learning (n = 40) from the programme were positive and revolved around learning, the opportunity to meet other leaders, reflection, and linking theory and practice:
Thought provoking. good to have time to think about my role, very enjoyable, great to meet with people from different services. learning to self-evaluate and link it to everyday practice, it was very good and interesting with a good balance given between information and reflection.
Qualitative comments regarding anything they would change (n = 28) revolved around the assignment and group work and the one thing suggested for change was the aspect of including parents/family in decision-making and care provision:
‘More clarification on what overall assessment is, I thought I would do my own assignment, and group work was difficult at first, however, a practical example was very helpful’. ‘Would like more discussion on parent/family involvement, how to support it, how to lead it and how to role model it for staff’.
Qualitative comments regarding topics that participants would like to be included ( n = 15) revolved around the priority of topics rather than topics to be addressed. Participants were generally happy with the content and comment suggested participants knew the topics would be covered but emphasised the ongoing need for support around leadership issues and that having time as a group to interact and discuss topics as a peer support system would be beneficial:
We can’t get enough support on issues like ‘Supervision’ ‘Time management’ ‘Management conflict’ ‘Motivating the team’, ‘Team building’, ‘Engagement of frontline staff’, ‘Change Management’, ‘Promoting good leadership’, ‘Mentorship’ and ‘Reflective thinking’. ‘Allocate extra time to the groups as it’s difficult to get it all done and meet as a group as there are things you need to discuss as a group of peers that you need to bounce off others before you bring to the facilitators’.
Qualitative comments regarding the forum day (n = 34) acknowledged it as a key source of learning and sharing where participants presented their group project. A broad range of projects were addressed, and key areas addressed by participants across groups were regulation aspects (inspection, preparedness), supervision (process, engagement, recording) person-centredness (choice, goal setting, transition, quality of life, decision making, quality improvements (communication, paperwork, handover, team meetings) and staff support (debriefing, stress). Participants highly valued the forum day as it presented an opportunity to share their work gain peer validation and gain from other participants’ projects and take ideas back to practice and highlight:
‘This was a great day; I gained so much from it and all the presentations, I got so much from working with the group as we were all from different services and while it was difficult at the start to choose something, we could all do in our own service, in the end we did something of value to each of our services for the clients/service users and staff’. ‘I got some much from doing the group project but the real benefit was seeing and hearing the other groups as there was so much of their work that I can bring back to my area and want to introduce now also’.
Qualitative comments addressing general comments related to having clear information before the programme (n = 5), factors influencing their decision to undertake the programme (n = 8), and the programme meeting their expectations (n = 22). Regarding having clear information participants expressed their desire and motivation for programmes to meet their needs and that the programme was undersold in their organisation. In terms of the decision to undertake the programme participants expressed their desire to ‘ learn from others’, ‘update knowledge’, ‘improve their leadership’ , and ‘to be effective and confident’ . Regarding expectations participants expressed their appreciation for the programme and were happy to have undertaken it and that it had sparked their interest and passion:
‘Very beneficial to my current role, fantastic meeting others and networking a fantastic course and support I will miss it but have made valuable contacts which I will use in the future I have gained great insight and knowledge into areas as I have found the topics in the course thought-provoking’. ‘An excellent programme which has greatly increased my confidence and knowledge, great learning and shared opportunities, it has highlighted the importance of leadership and it has developed my way of thinking, the language I use and has brought me back to the beginning of being person-centred’. ‘I would be interested in doing another module like this as it has positively impacted on my career and learning as it increased my self-awareness and knowledge of how to communicate more effectively with colleagues’.
Overall, the programme was positively evaluated with all aspects increasing from pre to post programme. However, while this increase is small it is nonetheless important, and given that 70% of the sample had 11 + years in service the pre-scores may have been more positively reported and indicate leadership programmes may have greater value for those in the early career stage (0–8 years). The co-design aspect of the programme ensured a focus on person-centredness, participants’ experience/s, and viewing participants as shared decision-makers [ 29 ]. Fundamental to the co-design of the programme delivery was drawing on the experience of participants and recognising the importance of reflective practice [ 30 ]. This was embedded throughout the programme where facilitators utilised methods that sought to draw on the participants’ aesthetic experience of what and how it feels like to use or be part of the service. Within the programme participants initially perceived leadership as mostly task-oriented but came to realise that in the reality of current practice and service provision qualities such as communication, person-centredness, advocacy, supporting, role modelling and empowering are key to modern leadership and that leadership is regarded as a distinct field and separate from management [ 31 ]. It’s important to consider certain limitations when interpreting the results. Firstly, the absence of a validated survey tool may have impacted the reliability and validity of the data collected. Secondly, the use of a cross-sectional design, rather than a longitudinal one, limits our ability to assess changes over time and draw causal conclusions. Thirdly, to truly ensure the programme philosophy is achieved a follow-up study would be recommended. Fourthly, the self-selection process may have attracted participants interested, eager, and motivated to engage in the programme and leadership. Additionally, the involvement of authors in delivering the programme and participants being aware that their responses, while anonymous, would be known to the research team, may have influenced participants’ responses, and resulted in a positively biased response.
Nonetheless, this programme emphasises the crucial need for support in transitioning service provision to a community-based model, which necessitates a cultural shift and the identification of leaders at an organisation level capable of leading change. Change within intellectual disability services has long been anticipated, yet progress remains slow, and much remains to be done [ 32 ]. The evolution of leadership presents a challenge, particularly in congregated settings where a top-down model of organisational management exists. In addition, a challenge for community-based settings staff will be working in small teams where managerial support is more remote [ 33 ]. Without organisational support and adequate education, there may be an apprehension and reluctance to assume leadership roles, this is seen anecdotally in the difficulty to recruit to leadership/PIC positions. However, the findings of this study suggest that with adequate support, time for reflection, and networking opportunities, participants can develop confidence and interpersonal leadership skills necessary for navigating change. Supportive measures such as mentoring, role modelling, and empowerment contribute significantly to this process.
Changes in policy, legislation, and service delivery pose both challenges and opportunities necessitating a re-evaluation of leadership and the need to enhance leadership capacity, adapt to contextual demands, and fulfil responsibilities [ 34 ]. This programme has made strides in addressing these challenges by fostering capacity, framing leadership within current issues, recognising leadership at various levels, and nurturing leadership qualities among staff. Moreover, participants grew to realise their role within the system and how they could influence developments through their encounters, both formal and informal, with staff and within their organisation [ 35 ]. Consequently, leadership is viewed as relational [ 34 ] aligning with the holism, person-centredness, advocacy-focused, and empowering models of care and support within intellectual disability services. However, for many participants in the programme, this realisation only occurred after providing them with the time and space away from work to reflect and develop.
In the dynamic landscape of service provision landscape characterised by advances in technology, economic fluctuations, and shifting policy direction, swift change can be unsettling for both staff and clients/service users. Therefore, investment in education and training to augment employees’ personal and professional development is crucial in managing change effectively and fostering a sense of belonging and engagement. Personal development and growth are important and participants in this programme articulated evidence of personal growth regarding increased confidence and motivation through engagement with the programme. Recognising that change can be stressful leading to skill reduction or feelings of confusion, being overwhelmed, and being undervalued [ 36 , 37 , 38 ]. Leaders play a vital role in influencing individuals and groups through their behaviours, perceptions, thoughts, and beliefs [ 39 , 40 ]. Thereby, it is vital to cultivate leaders who can adapt their leadership style and principles to suit the goals, context, and characteristics of their team/s. Effective leaders are those who can learn, evolve, and navigate challenges with experience, thereby achieving results even in difficult situations [ 41 ].
Personal growth facilitated by self-awareness fosters a more accepting and compassionate self-view of oneself, enhances leadership capacities, and reshapes leaders’ values in navigating the change process [ 42 ]. Good leadership involves credibility through regular consistent feedback, role modelling, active presence in observing staff [ 43 ], and providing support [ 44 ]. Thus, leadership involves skilled professional guidance, instruction support, and an educational role that extends beyond mere direction [ 44 ]. Essential within this process is fostering dialogue between leaders, staff, and clients/service users, promoting mutual exploration of relationships [ 45 ]. This requires leaders, to articulate and communicate a clear vision, enhance knowledge and understanding through productive engagement, empowering others, providing feedback and reinforcement, and grounding new approaches [ 46 ]. Such an approach supports the distribution of responsibility, ensuring that rewards are collectively owned rather than individualistic. Effective change management hinges on strong communication strategies, early consultation with all stakeholders, and generating enthusiasm for change [ 47 ]. These strategies help mitigate against resistance and enhance implementation success [ 48 ] and encourage active participation and engagement of staff in the change process [ 49 ].
Within the programme, a key element in fostering effective communication was participants understanding of individual personality types and communication styles. The relationship between leaders and their teams’ hinges on trust, mutual respect, understanding, and the sharing of information. Strong leaders can empower individuals and teams to identify their learning needs, thus enhancing self-motivation and empowerment, crucial for sustaining a lifelong commitment to learning and instigating a cultural shift [ 50 ]. Strong organisational leadership plays a vital role in supporting educational opportunities for leaders tailored to the priorities of intellectual disability services. This enables leaders to motivate and maximise the benefit for individuals, staff, client/service users, and the overall service [ 51 , 52 ]. Evidence suggests that strong leadership and role modelling involve promoting continuous professional development for individual staff [ 53 ], facilitating mentorship programmes [ 50 ], and empowering team members to contribute to service improvement initiatives [ 53 , 54 ].
A three-pronged approach focusing on education, leadership, and practice cultivates an environment conducive to inquiry, facilitating and promoting evidence-based practice [ 52 ]. Investment in equipping leaders with the skills to provide high-quality, transformational, mentorship and leadership. Continuous professional development holds significant relevance as evidenced by the impact on participants. Such impact can influence one’s self-motivation, enhance practical relevance and application, affect workplace learning, foster enabling leadership, and contribute to a positive workplace culture [ 55 ]. However, while participants acknowledged the value of continuous professional development, their primary exposure to it, beyond this programme, often revolved around mandatary training provided through in-service programmes. The lack of outward continuous professional development initiatives may contribute to a sense of isolation, as articulated by participants who valued the opportunity to connect with peers from other services and the networking opportunities this fostered.
Effective leadership is fundamental to providing integrated health and social care [ 56 ], improving performance [ 57 , 58 ], ensuring quality care [ 59 ], and fostering organisational commitment [ 60 ]. Research across health and social care has established a connection between leadership and client/service user care outcomes, including patient mortality rates [ 61 , 62 ], medication errors [ 62 ], hospital-acquired infections [ 62 ], patient outcomes [ 19 ], and higher patient satisfaction [ 62 ]. Such correlations may be linked to supportive leadership fostering better work environments, improved resources, appropriate staffing levels, and effective care practices [ 19 , 60 , 63 ]. Given that change is unavoidable leaders must harness the knowledge, abilities, and skills of all team members, acknowledging that expertise can emerge from various sources within the team [ 64 ]. Such an approach necessitates a shift away from hierarchical managerial structures towards fostering and developing individuals as reflexive leaders [ 51 , 65 ]. Leadership education should strike a balance between individual development and wider service priorities to ensure the efficient delivery of person-centred, safe, and effective care [ 55 ]. Crucial to effective leadership is cultivating a positive workplace culture [ 66 ], knowing what needs to change, and implementing practical strategies for enacting change [ 67 , 68 ]. All members of staff hold some level of responsibility and it is advocated that leadership training be extended to all staff members [ 69 ]. This emphasis on leadership training is further reinforced by the focus on vulnerability and risk management embedded in policies and standards overseen by HIQA in Ireland.
Within the programme, participants were primarily focused on crisis-avoiding/managing and fulfilling the criteria set out by the funding and monitoring bodies. This position inhibits the potential for leadership to emerge and flourish, often resulting in ineffective adherence to policies and standards and a heightened risk of care erosion. Instances of such shortcomings have been observed in scandals in Ireland ( 70 , 71 ) and the UK [ 72 ] where the absence or failure of leadership has had profound consequences for all. Thereby, leadership is imperative at various levels within intellectual disability services and should be considered a role and responsibility of all staff. The diverse skills and strengths present within an organisation represent a vast reservoir of untapped leadership talent [ 34 ]. Recognising the contribution and value of all staff in a team necessitates a departure from the notion of concentrated leadership in the hands of a few, in favour of a more devolved leadership model and a collective decision-making approach. This entails expanding the pool of potential leaders and ensuring leadership emerges from collective efforts rather than relying solely on individual capabilities [ 73 ]. To accomplish this, there is a need to empower others to take initiative [ 74 , 75 ] and prioritise the support and empowerment of leaders, so they can in turn support and empower others. This reframes leadership as a collaborative endeavour focused on partnership, engagement, and shared responsibility, transcending hierarchical power dynamics and seniority-based perspectives within the health and social care hierarchy [ 76 ].
Practice leadership in intellectual disability services has been studied and documented in both Australia and the UK [ 12 , 13 , 43 , 77 , 78 , 79 ], with a focus on improving the quality of life for individuals with intellectual disability. A key concept that has emerged in this literature is the implementation of “active support,” which involves empowering individuals with disabilities to engage in meaningful activities and make choices in their daily lives, with appropriate support from staff members [ 77 , 78 , 79 ]. Practice leaders, including frontline managers and supervisors, play a pivotal role in creating a positive organisational culture that values person-centred care, fosters staff empowerment, and promotes continuous learning and improvement. Studies have shown that practice leaders who effectively implement active support report better staff experiences of working in challenging environments.
While service models have evolved towards a more person-centred approach, intellectual disability services, and their leaders still face challenges in the transition to modern leadership paradigms. These new approaches emphasise individualised support, self-determination, effective teamwork, and evidence-based practice, which are integral to developing inclusive and participatory human service models focused on supporting individuals in achieving their goals. Effective leadership serves as a catalyst for organisational change and is closely associated with delivering safe, effective quality care and promoting positive outcomes. ( 80 , 81 ) Despite widespread research into management and leadership in health and social care services, the field of intellectual disability remains relatively under-researched, often described as both an important and neglected area [ 82 ].
Effective leadership improves outcomes for clients/service users and what is evident within this evaluation is that intellectual disability leaders are eager for change and improvement but may lack clarity on how to enact such changes. Moreover, providing high-quality personalised care presents challenges, thereby there is a need to invest in leader development and illustrate how their skills can drive service improvement, engage clients/service users in care planning, and embed person-centred care across the health and social care system. There is a pressing need to create and nurture practice leaders within intellectual disability services and relay the message that leadership is a shared responsibility among all individuals striving to enhance people’s care experiences, particularly for those who are most vulnerable. This involves transforming services into human-centred care models focused on fulfilling person-centred outcomes. 83 . 84 Leaders play a pivotal role in promoting well-being, supporting independence, and ensuring people experience high-quality care and the best possible health outcomes. Overall, this evaluation reveals that participants’ knowledge and understanding of leadership improved through this programme and participants’ experiences were largely positive. However, consideration needs to be given to how leadership interventions related to support for individuals with intellectual disability, and future programme evaluation need to consider staff practice and service users’ experience has been measured.
Strengths and limitations of this study
This study captures the development and evaluation of a leadership programme for staff working in intellectual disability services with person in charge responsibilities in Ireland.
A large sample was achieved across four cohorts of the programme delivery and both survey and interview data were collected.
The survey instrument was developed for this study but was not a valid tool.
Social desirability bias from participants in their responses may have influenced their responses.
Data availability
Dataset is available on figshare open platform https://doi.org/10.6084/m9.figshare.22013186 and any additional information can be made to the corresponding author dependent upon privacy or ethical restrictions.
Doody O, Murphy F, Lyons R, Gallen A, Ryan J, Downey J, Sezgin D. Development of nursing quality care process metrics and indicators for intellectual disability services: a literature review and modified Delphi consensus study. BMC Health Serv Res. 2019;19(1):909. https://doi.org/10.1186/s12913-019-4749-y .
Article PubMed PubMed Central Google Scholar
McCarron M, Sheerin F, Roche L, Ryan AM, Griffiths C, Keenan P, Doody O, D’Eath M, Burke E, McCallion P. Shaping the future of intellectual disability nursing in Ireland. Dublin: Health Serv Exec. 2018. https://www.pna.ie/images/2109181.pdf .
Health Service Executive. Time to move on from congregated settings. A strategy for community inclusion. Report of the working group on congregated settings. Dublin: Health Service Exec. 2011. https://www.hse.ie/eng/services/list/4/disability/congregatedsettings/time-to-move-on-from-congregated-settings-%E2%80%93-a-strategy-for-community-inclusion.pdf .
Health Service Executive. Progressing disability services for children and young people. Dublin: Health Service Exec. 20204444. https://www.hse.ie/eng/services/list/4/disability/progressing-disability/pds-programme/progressing-disability-services-for-children-and-young-people-programme-2020.docx .
Health Service Executive. New Directions: Review of HSE Day Services and implementation plan 2012–2016. Working Group Report. Dublin: Health Service Executive. 2012. https://www.lenus.ie/bitstream/handle/10147/215139/newdirections2012.pdf?sequence=1&isAllowed=y
Health Service Executive. A National Framework for Person Centred Planning in Services for Persons with a Disability. Dublin: Health Service Executive. 2018. https://www.hse.ie/eng/services/list/4/disability/newdirections/framework-person-centred-planning-services-for-persons-with-a-disability.pdf .
United Nations. Convention on the Rights of Persons with Disabilities. Geneva: United Nations. 2006. https://www.ohchr.org/en/instruments-mechanisms/instruments/convention-rights-persons-disabilities .
Government of Ireland. Assisted Decision Making (Capacity) Act. Dublin: Government of Ireland. 2015. https://www.irishstatutebook.ie/eli/2015/act/64/enacted/en/html .
Government of Ireland, Houses of the Oireachtas. Committee on the Future of Healthcare: Sláintecare Report. Dublin: Government of Ireland. 2017. https://assets.gov.ie/22609/e68786c13e1b4d7daca89b495c506bb8.pdf .
Health Information and Quality Authority. National standards for residential services for children and adults with disabilities. Dublin: Health Inform Qual Auth. 2013. https://www.hiqa.ie/sites/default/files/2017-02/Standards-Disabilities-Children-Adults.pdf .
Health Information and Quality Authority. Regulation 14: Person in charge of a designated centre for disability. Dublin: Health Information and Quality Authority. 2021. https://www.hiqa.ie/sites/default/files/2017-05/Provider-guidance-on-Regulation-14-PIC.pdf .
Beadle-Brown J, Bigby C, Bould E. Observing practice leadership in intellectual and developmental disability services. J Intell Disabil Res. 2015;59(12):1081–93. https://doi.org/10.1111/jir.12208 .
Article CAS Google Scholar
Bould E, Beadle-Brown J, Bigby C, Iacono T. Measuring practice leadership in supported accommodation services for people with intellectual disability: comparing staff-rated and observational measures. J Intell Dev Dis. 2018;43(2):174–82. https://doi.org/10.3109/13668250.2016.1259466 .
Article Google Scholar
Health Service Executive. Health services people strategy (2015–2018): leaders in people services. Dublin: Health Service Exec. 2015. https://www.hse.ie/eng/staff/resources/hrstrategiesreports/peoplestrategy.pdf .
Health Service Executive. National Nursing and Midwifery Clinical Leadership Development Needs Analysis. Dublin: Office of the Nursing Services Director Quality and Clinical Care Directorate. 2010. https://www.choiceforum.org/docs/clinicaldes.pdf .
Larson SA, Tolbize MA, Kim O, York B, Center on Community Living. Direct support professional turnover costs in small group homes: A case study. Minneapolis: University of Minnesota, Research and Training. 2016. https://www.researchgate.net/profile/Sheryl-Larson/publication/311536964_Direct_Support_Professional_Turnover_Costs_in_Small_Group_Homes_A_Case_Study/links/584b20b808aecb6bd8c153ff/Direct-Support-Professional-Turnover-Costs-in-Small-Group-Homes-A-Case-Study.pdf .
Qian X, Larson SA, Tichá R, Stancliffe R, Pettingell SL. Active support training, staff assistance, and engagement of individuals with intellectual and developmental disabilities in the United States: Randomized controlled trial. AJIDD-Am J Intellect. 2019;124(2):157–73. https://doi.org/10.1352/1944-7558-124.2.157 .
de Vries JM, Curtis EA. Nursing leadership in Ireland: experiences and obstacles. Leadersh Heal Serv. 2019;32(3):348–63. https://doi.org/10.1108/LHS-11-2017-0068 .
Wong CA, Cummings GG, Ducharme L. The relationship between nursing leadership and patient outcomes: a systematic review update. J Nurs Manage. 2013;21(5):709–24. https://doi.org/10.1111/jonm.12116 .
Bahadori A, Peyrovi H, Ashghali-Farahani M, Hajibabaee F, Haghani H. The relationship between nursing leadership and patient satisfaction. Int J Med Res Health Sci. 2016;5(10):134–41. https://d1wqtxts1xzle7.cloudfront.net/64288954/565_iran_19th-libre.pdf?1598528920=&response-content-disposition=inline%3B+filename%3DThe_relationship_between_nursing_leaders.pdf&Expires=1704815766&Signature=GoG9LEwva1dz8hindyRwLecFJJ72GOFw6vrNvSPnO5~BL9iTMqzcTuoeJ8kTiIfbatBGZVaztmTdTJIbQo0CuUHAustcSezBWeLA-j02MGwZa3tJjyv7j9SAK7ZGHWw0cEG0GlCUG9HsoK1NgPK9bkayYEH7CVU6M8aJOll35ehxnpVo1q-I5e8IsXWADvbEj-6OlfHqyQjEOcAH8ggJfeENXct6kyS3K6r14B1yK~krVzJY0R4-4WdxoW~xiVsDO5ryix5xFWwBAUCIq~hR8H8dRjBJ3cfFbafqxIU0SKoNBN0lXRNGNcgpuHEB8H8M0qTBrHYegKTo5XDInu50-Q__&Key-Pair-Id=APKAJLOHF5GGSLRBV4ZA .
Google Scholar
Fischer SA. Transformational leadership in nursing: a concept analysis. J Adv Nurs. 2016;72(11):2644–53. https://doi.org/10.1111/jan.13049 .
Article PubMed Google Scholar
Gopee N, Galloway J. Leadership and management in healthcare. Third Edition. London: Sage; 2017.
Bender M. Conceptualizing clinical nurse leader practice: an interpretive synthesis. J Nurs Manage. 2016;24(1):E23–31. https://doi.org/10.1111/jonm.12285 .
West M, Armit K, Loewenthal L, Eckert R, West T, Lee A. Leadership and leadership development in health care: The evidence base. London: Kings Fund. 2015. https://www.kingsfund.org.uk/sites/default/files/field/field_publication_file/leadership-leadership-development-health-care-feb-2015.pdf .
West MA, Eckert R, Steward K, Pasmore WA. Developing collective leadership for health care. London: Kings Fund. 2014. https://www.kingsfund.org.uk/sites/default/files/field/field_publication_file/developing-collective-leadership-kingsfund-may14.pdf .
Ahmed NE, Ahmed F, Anis H, Carr P, Gauher S, Rahman F, An, NHS Leadership Team for the Future. London: Reform Research Trust. 2015. https://reform.uk/wp-content/uploads/2018/10/An-NHS-leadership-team-for-the-future.pdf .
Broderick B. Optimising leadership within the intellectual disability service delivery system. Frontline. 2017; 106.
Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–15. https://doi.org/10.1111/j.1365-2648.2007.04569.x .
Bate P, Robert G. Bringing user experience to health care improvement: the concepts, methods and practices of experience-based design. Oxford: Radcliffe Publishing; 2007.
McCloskey S, Taggart L. How much compassion have I left: an exploration of occupational stress among children’s palliative care nurses. Int J Palliat Nurs. 2010;16(5):233–40. https://doi.org/10.12968/ijpn.2010.16.5.48144 .
Cullen J, O’Connell R. Leadership in nursing and healthcare: an overview of theory, research and practice. In: Curtis EA, editor. Cullen J. Leadership and change for the health professional. London: Open University Press, McGraw-Hill Education; 2017.
Northway R. Knowledge, time and change. J Intellect Disabil. 2018;22(2):111–2. https://doi.org/10.1177/1744629518760052 .
Northway R. The need to move ‘upstream. J Intellect Disabil. 2018;22(3):211–2. https://doi.org/10.1177/1744629518787250 .
Clarke N. Relational leadership: theory, practice and development. Abingdon: Routledge; 2018.
Book Google Scholar
Weberg D. Complexity leadership: a healthcare imperative. Nurs Forum. 2012;47(4):268–77. https://doi.org/10.1111/j.1744-6198.2012.00276.x .
Higgs M, Dulewicz V. Antecedents of well-being: a study to examine the extent to which personality and emotional intelligence contribute to well-being. Int J Hum Resour Man. 2014;25(5):718–35. https://doi.org/10.1080/09585192.2013.815253 .
Gupta V, Singh S. Psychological capital as a mediator of the relationship between leadership and creative performance behaviours: empirical evidence from the Indian RandD sector. Int J Hum Resour Man. 2014;25(10):1373–94. https://doi.org/10.1080/09585192.2013.870311 .
McConachie DA, McKenzie K, Morris PG, Walley RM. Acceptance and mindfulness-based stress management for support staff caring for individuals with intellectual disabilities. Res Dev Disabil. 2014;35(6):1216–27. https://doi.org/10.1016/j.ridd.2014.03.00 .
Callahan C, Grunberg NE. Military medical leadership. In: Smith DC, Schoomaker EB, O’Connor F, editors. Fundamentals of military medical practice. Washington, DC: Borden Institute; 2018.
Northouse PG, Leadership. Theory and practice. Seventh edition. Los Angeles, CA: Sage; 2016.
Yarnell A, Grunberg NE. Developing allostatic leaders: a psychobiosocial perspective. In: Clark M, Gruber C, editors. Leader development deconstructed. Cham, Switzerland: Springer International Publishing; 2017.
Crook N, Alakavuklar ON, Bathurst R, Leader. Know yourself: bringing back self-awareness, trust and feedback with a theory O perspective. J Organ Change Manag. 2021;34(2):350–65. https://doi.org/10.1108/JOCM-05-2020-0131 .
Bould E, Beadle-Brown J, Bigby C, Iacono T. The role of practice leadership in active support: impact of practice leaders’ presence in supported accommodation services. Int J Dev Disabil. 2018;64(2):75–80. https://doi.org/10.1080/20473869.2016.1229524 .
Mansell J, Beadle-Brown J. Active support: enabling and empowering people who experience intellectual disabilities. London: Jessica Kingsley; 2012.
Kielhofner G. Rethinking disability and what to do about it: disability studies and its implications for occupational therapy. Am J Occup Ther. 2005;59(5):487–96. https://doi.org/10.5014/ajot.59.5.487 .
Schalock RL, Verdugo MA. A Leadership Guide for Today’s disabilities organizations: overcoming challenges and making Change Happen. Baltimore, MD: Brookes Publishing Company; 2012.
Bartunek JM, Greenberg DN, Humphries M, Davidson B. Participation, complexity, of understanding, and the assessment of organisational change. Acad Manage Proceed. 1996;19961:259–63. https://doi.org/10.5465/ambpp.1996.4980616 .
Zafar F, Naveed K. Organizational change and dealing with employees’ resistance. Int J Manage Excelle. 2014;2(3):237–46. https://techmindresearch.org/index.php/ijme/article/view/98 .
Lahana E, Tsaras K, Kalaitzidou A, Galanis P, Kaitelidou D, Sarafis P. Conflicts management in public sector nursing. Int J Healthc Manag. 2019;12(1):33–9. https://doi.org/10.1080/20479700.2017.1353787 .
Govranos M, Newton JM. Exploring ward nurses’ perceptions of continuing education in clinical settings. Nurs Educ Today. 2014;34(4):655–60. https://doi.org/10.1016/j.nedt.2013.07.003 .
Eddy K, Jordan Z, Stephenson M. Health professionals’ experience of teamwork education in acute hospital settings: a systematic review of qualitative literature. JBI Evid Synth. 2016;14(4):96–137. https://journals.lww.com/jbisrir/abstract/2016/04000/health_professionals__experience_of_teamwork.12.aspx .
Warren JI, McLaughlin M, Bardsley J, Eich J, Esche CA, Kropkowski L, Risch S. The strengths and challenges of implementing EBP in healthcare systems. Worldv Evid-Based Nu. 2016;13(1):15–24. https://doi.org/10.1111/wvn.12149 .
Beal JA, Riley JM. Best organizational practices that foster scholarly nursing practice in Magnet® hospitals. J Prof Nurs. 2019;35(3):187–94. https://doi.org/10.1016/j.profnurs.2019.01.001 .
McCauley K, Cross W, Moss C, Walsh K, Schofield C, Handley C, FitzGerald M, Hardy S. What does practice development (PD) offer mental health-care contexts? A comparative case study of PD methods and outcomes. J Psychiatr Ment Health Nurs. 2014;21(8):724–37. https://doi.org/10.1111/jpm.12134 .
Article CAS PubMed Google Scholar
Illing J, Corbett S, Kehoe A, Carter M, Hesselgreaves H, Crampton P, Sawdon M, Swamy M, Finn G, Medford W, Ikah D. How does the education and training of health and social care staff transfer to practice and benefit patients? A realist approach. Final Report for Department of Health. Newcastle: Newcastle University, Durham University, University of York. 2018. https://eprints.ncl.ac.uk/file_store/production/250597/0918BE55-648C-439F-8706-499322906059.pdf .
Sfantou DF, Laliotis A, Patelarou AE, Sifaki-Pistolla D, Matalliotakis M, Patelarou E. Importance of leadership style towards quality of care measures in healthcare settings. Healthc. 2017;5(4):73. https://doi.org/10.3390/healthcare5040073 .
Braun S, Peus C, Weisweiler S, Frey D. Transformational leadership, job satisfaction, and team performance: a multilevel mediation model of trust. Leadersh Quart. 2013;24(1):270–83. https://doi.org/10.1016/j.leaqua.2012.11.006 .
Kacmar KM, Bachrach DG, Harris KJ, Noble D. Exploring the role of supervisor trust in the associations between multiple sources of relationship conflict and organisational citizenship behaviour. Leadersh Quart. 2012;23(1):43–54. https://doi.org/10.1016/j.leaqua.2011.11.004 .
Gille F, Smith S, Mays N. Why public trust in health care systems matters and deserves greater research attention. J Health Ser Res Policy. 2015;20(1):62–4. https://doi.org/10.1177/135581961454316 .
Paliszkiewicz J, Koohang A, Nord JH. Management trust, organizational trust, and organizational performance: empirical validation of an instrument. Online J Appl Knowl Manag. 2014;2(1):28–39. https://www.iiakm.org/ojakm/articles/2014/volume2_1/OJAKM_Volume2_1pp28-39.pdf .
Cummings GG, Midodzi WK, Wong CA, Estabrooks CA. The contribution of hospital nursing leadership styles to 30-day patient mortality. Nurs Res. 2010;59(5):331–9. https://doi.org/10.1097/NNR.0b013e3181ed74d5 .
Wong CA. Connecting nursing leadership and patient outcomes: state of the Science. J Nurs Manage. 2015;23(3):275–8. https://doi.org/10.1111/jonm.12307 .
Brown S, Gray D, McHardy J, Taylor K. Employee trust and workplace performance. J Econ Behav Organ. 2015;116. https://doi.org/10.1016/j.jebo.2015.05.001 . :361 – 78.
Johnston MP. Distributed leadership theory for investigating teacher librarian leadership. Sch Libr Worldw. 2015;21(2):39–57. https://journals.library.ualberta.ca/slw/index.php/slw/article/view/6893/3891 .
Williams B, Perillo S, Brown T. What are the factors of organisational culture in health care settings that act as barriers to the implementation of evidence-based practice: a scoping review. Nurs Educ Today. 2015;35(2):e34–41. https://doi.org/10.1016/j.nedt.2014.11.012 .
Jackson C, Manley K, Martin A, Wright T. Continuing professional development (CPD) for quality care: context, mechanisms, outcome and impact: Canterbury, Kent: Canterbury Christ Church University, England Centre for Practice Development. 2015. https://repository.canterbury.ac.uk/download/deb3b4bc2d843783c5fcc2e525b867b6df48aba83a02f8f162903f9e4e73af79/1483243/EOF%2520-%2520FINAL%2520REPORT%252030th%2520January%25202015%2520FINAL%2520with%2520ISBN%2520-%2520978-1-909067-39-4.pdf .
Manley K, Jackson C. The Venus model for integrating practitioner-led workforce transformation and complex change across the health care system. J Eval Clin Pract. 2020;26(2):622–34. https://doi.org/10.1111/jep.13377 .
Manley K, Martin A, Jackson C, Wright T. A realist synthesis of effective continuing professional development (CPD): a case study of healthcare practitioners’ CPD. Nurse Educ Today. 2018;69:134–41. https://doi.org/10.1016/j.nedt.2018.07.010 .
Hughes RL, Ginnett RC, Curphy GJ. Leadership: enhancing the lessons of experience. Boston, MA: McGraw-Hill; 2006.
Áras Attracta Swinford Review Group. Time for Action: Priority actions arising from National Consultation. Dublin: Health Service Exec. 2016. https://www.hse.ie/eng/services/publications/disability/aasrgtimeforaction.pdf .
Áras Attracta Swinford Review Group. What matters most. Dublin: Health Service Exec. 2016. https://www.hse.ie/eng/services/publications/disability/aasrgwhatmattersmost.pdf .
Mencap. Out of sight: stopping the neglect and abuse of people with a learning disability. London: Mencap; 2014. https://www.mencap.org.uk/sites/default/files/2016-08/Out-of-Sight-Report.pdf .
Ospina SM. Collective leadership and context in public administration: bridging public leadership research and leadership studies. Public Admin Rev. 2017;77(2):275–87. https://doi.org/10.1111/puar.1270 .
Boak G, Dickens V, Newson A, Brown L. Distributed leadership, team working and service improvement in healthcare. Leadersh Health Ser. 2015;28(4):332–44. https://doi.org/10.1108/LHS-02-2015-0001 .
Rydenfält C, Johansson G, Odenrick P, Åkerman K, Larsson PA. Distributed leadership in the operating room: a naturalistic observation study. Cogn Tech Work. 2015;17:451–60. https://doi.org/10.1007/s10111-014-0316-9 .
Australian College of Nursing. Nurse Leadership. Canberra: Australian College of Nursing. 2015. https://www.scribd.com/document/306119638/ACN-Nurse-Leadership-White-Paper-FINAL .
Deveau R, McGill P. Impact of practice leadership management style on staff experience in services for people with intellectual disability and challenging behaviour: a further examination and partial replication. Res Dev Disabil. 2016:56:160–4. https://doi.org/10.1016/j.ridd.2016.05.02 .
Bigby C, Beadle-Brown J. Improving quality of life outcomes in supported accommodation for people with intellectual disability: what makes a difference. J Appl Res Intellect Disabil. 2018;31(2):e182–200. https://doi.org/10.1111/jar.12291 .
McGill P, Vanono L, Clover W, Smyth E, Cooper V, Hopkins L, Barratt N, Joyce C, Henderson K, Sekasi S, Davis S. Reducing challenging behaviour of adults with intellectual disabilities in supported accommodation: a cluster randomized controlled trial of setting-wide positive behaviour support. J Appl Res Intellect Disabil. 2018;81:143–54. https://doi.org/10.1016/j.ridd.2018.04.020 .
Deveau R, Rickard G. Contextual and individual barriers to providing practice leadership by frontline managers in community services for adults with intellectual disabilities: a qualitative study. Br J Learn Disabil. 2024;52(1):11–22. https://doi.org/10.1111/bld.12542 .
Rose J, Mills S, Silva D, Thompson L. Client characteristics, organizational variables and burnout in care staff: the mediating role of fear of assault. Res Dev Disabil. 2013;34(3):940–7. https://doi.org/10.1016/j.ridd.2012.11.014 .
Orellana K, Manthorpe J, Moriarty J. What do we know about care home managers? Findings of a scoping review. Health Soc Care Comm. 2017;25(2):366–77. https://doi.org/10.1111/hsc.12313 .
Department of Health. Transforming care: a National Response to Winterbourne View Hospital. London: Department of Health; 2012. https://assets.publishing.service.gov.uk/media/5a7b91f7ed915d13110601c3/final-report.pdf .
Jukes M, Aspinall SL. Leadership and learning disability nursing. Brit J Nurs. 2015;24(18):912–6. https://doi.org/10.12968/bjon.2015.24.18.912 .
Download references
Acknowledgements
The research team would like to thank all participants for their collaboration and the National Clinical Leadership Centre.
The programme design, delivery, and evaluation were funded by the National Clinical Leadership Centre for Nursing and Midwifery (Office of Nursing and Midwifery Service Directorate) of the Irish Health Service Executive.
Author information
Authors and affiliations.
Health Research Institute, Department of Nursing and Midwifery, University of Limerick, Limerick, Ireland
Owen Doody, Eileen Carey & Ruth Ryan
Intellectual Disability Services, Clare, Ireland
Maeve O’Halloran
National Clinical Leadership Centre for Nursing and Midwifery, Health Service Executive, Dublin, Ireland
Marie Kilduff
National Clinical Leadership Centre for Nursing and Midwifery, Health Service Executive, Sligo, Ireland
Ann Gilmartin
You can also search for this author in PubMed Google Scholar
Contributions
Funding acquisition OD, EC, RR; Conceptualization MK, OD, EC, RR; Methodology OD, EC, RR, MOH; Investigation OD, MOH; Formal analysis OD, MOH; Writing - Original Draft AG, MK, OD, EC, RR; Writing - Review & Editing AG, MK, OD, EC, RR; Project administration OD, MOH.
Corresponding author
Correspondence to Owen Doody .
Ethics declarations
Ethics approval and consent to participate.
All procedures were in accordance with the University of Limerick, Education, and Health Sciences, Research Ethics Committee ethical standards (approval 2018_10_07_EHS) and the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Voluntary participation and informed consent were utilised in the survey and written informed consent was obtained from all participants who engaged in the interview study. All participants were made aware that the data collected may be disseminated and used for publication, conferences, or posters.
Consent for publication
Not applicable.
Patient and public involvement
It was not appropriate or possible to involve patients or the public in the design, conduct, reporting, or dissemination plans of our research as this was a commissioned evaluation. However, stakeholders were involved throughout the design and development of the programme.
Competing interests
The programme design and delivery were co-production by the independent researchers and the National Clinical Leadership Centre for Nursing and Midwifery, and the evaluation was conducted by the independent researchers. The independent researchers have no competing interests to declare.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary material 2, rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Doody, O., O’Halloran, M., Carey, E. et al. Leadership in intellectual disability practice: design, development, and evaluation of a programme to support practice. BMC Health Serv Res 24 , 674 (2024). https://doi.org/10.1186/s12913-024-11124-7
Download citation
Received : 16 January 2024
Accepted : 20 May 2024
Published : 28 May 2024
DOI : https://doi.org/10.1186/s12913-024-11124-7
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Intellectual disability
- Practice leadership
- Social care
BMC Health Services Research
ISSN: 1472-6963
- General enquiries: [email protected]
COMMENTS
As mentioned previously, there are a number of existing guidelines for literature reviews. Depending on the methodology needed to achieve the purpose of the review, all types can be helpful and appropriate to reach a specific goal (for examples, please see Table 1).These approaches can be qualitative, quantitative, or have a mixed design depending on the phase of the review.
In The Literature Review: A Step-by-Step Guide for Students, Ridley presents that literature reviews serve several purposes (2008, p. 16-17). Included are the following points: Historical background for the research; Overview of current field provided by "contemporary debates, issues, and questions;" Theories and concepts related to your research;
Examples of literature reviews. Step 1 - Search for relevant literature. Step 2 - Evaluate and select sources. Step 3 - Identify themes, debates, and gaps. Step 4 - Outline your literature review's structure. Step 5 - Write your literature review.
For this review, a comprehensive literature search was performed from many databases using generic search terms such as Qualitative Research, Criteria, etc. The following databases were chosen for the literature search based on the high number of results: IEEE Explore, ScienceDirect, PubMed, Google Scholar, and Web of Science.
A literature review is a comprehensive summary of previous research on a topic. It includes both articles and books—and in some cases reports—relevant to a particular area of research. Ideally, one's research question follows from the reading of what has already been produced. For example, you are interested in studying sports injuries ...
Introduction. Literature review is an essential feature of academic research. Fundamentally, knowledge advancement must be built on prior existing work. To push the knowledge frontier, we must know where the frontier is. By reviewing relevant literature, we understand the breadth and depth of the existing body of work and identify gaps to explore.
A formal literature review is an evidence-based, in-depth analysis of a subject. There are many reasons for writing one and these will influence the length and style of your review, but in essence a literature review is a critical appraisal of the current collective knowledge on a subject. Rather than just being an exhaustive list of all that ...
Literature review. You will need to write a short, overview literature review to introduce the main theories, concepts and key research areas that you will explore in your dissertation. This set of texts - which may be theoretical, research-based, practice-based or policies - form your theoretical framework.
Qualitative research involves collecting and analyzing non-numerical data (e.g., text, video, or audio) to understand concepts, opinions, or experiences. It can be used to gather in-depth insights into a problem or generate new ideas for research. Qualitative research is the opposite of quantitative research, which involves collecting and ...
The literature review represents the most important step of the research process in qualitative, quantitative, and mixed research studies (Boote & Beile, 2005; Combs, Bustamante, & Onwuegbuzie, 2010; Onwuegbuzie, Collins, Leech, Dellinger, & Jiao, 2010). As noted by Boote and Beile (2005), A thorough, sophisticated literature review "
While many books and articles guide various qualitative research methods and analyses, there is currently no concise resource that explains and differentiates among the most common qualitative approaches. We believe novice qualitative researchers, students planning the design of a qualitative study or taking an introductory qualitative research course, and faculty teaching such courses can ...
In the field of research, the term method represents the specific approaches and procedures that the researcher systematically utilizes that are manifested in the research design, sampling design, data collec-tion, data analysis, data interpretation, and so forth. The literature review represents a method because the literature reviewer chooses ...
Qualitative versus quantitative research; Empirical versus theoretical scholarship; Divide the research by sociological, historical, or cultural sources; Theoretical: In many humanities articles, the literature review is the foundation for the theoretical framework. You can use it to discuss various theories, models, and definitions of key ...
The literature review provides the researcher with an opportunity to identify any gaps that may exist in the body of literature and to provide a rationale for how the proposed study may contribute to the existing body of knowledge. The literature review helps the researcher to refine the research questions and embed them in guiding hypotheses ...
Those doing qualitative research cannot "opt out" of knowing their relevant scholarly conversations. Undertaking a qualitative systematic review provides a vital means to know and tune into the past conversation in your topic area that allows the researcher to position themselves and their work substantively, ontologically, theoretically, and methodologically in this landscape.
Qualitative research has ample possibilities within the arena of healthcare research. This article aims to inform healthcare professionals regarding qualitative research, its significance, and applicability in the field of healthcare. ... The minimal literature review will help the researchers to avoid the conceptual pollution of the phenomenon ...
What is qualitative research? If we look for a precise definition of qualitative research, and specifically for one that addresses its distinctive feature of being "qualitative," the literature is meager. In this article we systematically search, identify and analyze a sample of 89 sources using or attempting to define the term ...
A qualitative systematic review brings together research on a topic, systematically searching for research evidence from primary qualitative studies and drawing the findings together. There is a debate over whether the search needs to be exhaustive. 1 , 2 Methods for systematic reviews of quantitative research are well established and explicit ...
Methodology: The key elements required in a systematic review protocol are discussed, with a focus on application to qualitative reviews: Development of a research question; formulation of key search terms and strategies; designing a multistage review process; critical appraisal of qualitative literature; development of data extraction ...
3.5 Step 5: Qualitative Analysis. The literature review is an essential part of the research process. There are several types of the literature review [44, 45]. However, in general, the literature review is a process of questioning. It is intended to answer some questions about a particular topic: What are the primary literature sources?
A literature review is "a synthesis of the literature on a topic" (Pan, 2008, p. 1), which can provide reasons for initiating research. After developing the research question, the author tries to explore existing research literature, to check if the question has been adequately and convincingly answered, and to search for other studies that ...
Quantitative research: an operational description. Purpose: explain, predict or control phenomena through focused collection and analysis of numberical data Approach: deductive; tries to be value-free/has objectives/ is outcome-oriented Hypotheses: Specific, testable, and stated prior to study. Lit. Review: extensive; may significantly influence a particular study
Nonetheless, literature review is a continuous sense-making process -- you need to review the literature continuously in order to organize your thoughts and refine your analysis. A good literature review should be able to: Connect to your research questions; Connect to your choice of methods and research design; Support your data analysis
Setting the review question and topic refinement. Rapid reviews summarise information from multiple research studies to produce evidence for 'the public, researchers, policymakers and funders in a systematic, resource-efficient manner'.16 Involvement of knowledge users is critical.3 Given time constraints, individual knowledge users could be asked only to feedback on very specific ...
This review of qualitative research followed the guidelines for systematic literature reviews proposed by Bettany-Saltikov and McSherry (Citation 2016) and was conducted in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses -PRISMA (Page et al., Citation 2021). This systematic review synthesises subjective ...
Critical narrative review of the literature and discussion groups: There is concern with ethics, with methodological rigor and reliability and with the reporting of data in the secondary analysis. ... In a study on the process of ethical review of qualitative research projects, conducted by means of interviews with 30 researchers, McMurphy et ...
The value of using qualitative methods within clinical trials is widely recognised. How qualitative research is integrated within trials units to achieve this is less clear. This paper describes the process through which qualitative research has been integrated within Cardiff University's Centre for Trials Research (CTR) in Wales, UK. We highlight facilitators of, and challenges to, integration.
9.3. Types of Review Articles and Brief Illustrations. EHealth researchers have at their disposal a number of approaches and methods for making sense out of existing literature, all with the purpose of casting current research findings into historical contexts or explaining contradictions that might exist among a set of primary research studies conducted on a particular topic.
A scoping literature review identifies five key QoL domains for older adults: autonomy, meaningful activities, positive social relationships, leisure opportunities, and health. ... the influence of context on QoL and the built environment, and the value of qualitative research in this field. By contributing to the understanding of QoL in ...
Research across health and social care has established a connection between leadership and client/service ... a literature review and modified Delphi consensus study. ... Z, Stephenson M. Health professionals' experience of teamwork education in acute hospital settings: a systematic review of qualitative literature. JBI Evid Synth. 2016;14(4 ...