11.3 The Gap Model of Service Quality
Learning outcomes.
By the end of this section, you will be able to:
- 1 Describe the Gap Model of Service Quality.
- 2 List and describe the dimensions of service quality.

Dimensions of Service Quality
While we’re still on the subject of customer satisfaction, let’s take a look at still another model that aids marketers in better understanding customer satisfaction: the Gap Model of Service Quality (sometimes also known as the Customer Service Gap Model or the Five-Gap Model), first proposed in 1985. The importance of this model is that it demonstrates that customer satisfaction is essentially a function of perception. In other words, if the service provided meets or exceeds customers’ expectations, they will be satisfied; if not, they will be dissatisfied, likely as a result of one of the customer service gaps presented below. 27
According to the model (see Figure 11.11 ), there are five major gaps or potential inconsistencies organizations encounter in seeking to meet customers’ expectations of the customer experience. 28
The gaps are:
- Gap 1—knowledge gap: the difference between customer expectations and what managers think they expect
- Gap 2—policy gap: the difference between management’s understanding of the customer’s needs and how they translate that understanding into service delivery policies and standards for employees
- Gap 3—delivery gap: the difference between the experience specification and the actual results of the service
- Gap 4—communication gap: the difference between the delivery of the customer experience and what is communicated to the customer
- Gap 5—customer gap: the difference between the customer’s expectations of the service or experience and their perception of the experience
Let’s look at each one of these gaps in a little more detail.
Gap 1: The Knowledge Gap
The knowledge gap is the difference between what customers expect and what the company thinks they expect. 29 The bottom line here is that the company doesn’t know exactly what customers want. This could be due to a variety of factors—lack of communication between frontline employees and management, inadequate market research, or simply a failure to listen to customer feedback, including complaints. For example, a hotel manager may think that guests want a hot breakfast instead of a continental breakfast, but the reality is that guests are more concerned with the cleanliness of their rooms or the speed of the Internet service at the hotel than they are with breakfast.
Gap 2: The Policy Gap
The policy gap reflects the difference between management’s perception of the customer’s needs and the translation of that understanding into its service delivery policies and standards. Typically, management has an accurate understanding of what the customer wants, but performance standards haven’t been established that ensure the appropriate employee behaviors are displayed. 30 Using the hotel example again, assume that a number of customers have complained that the phone rings innumerable times before it is answered. Management wants to address this issue, so it establishes a policy that phones must be answered “quickly.” What’s your interpretation of the word quickly —two rings, four rings, six rings? Specificity here is the key.
Gap 3: The Delivery Gap
The delivery gap is the difference between service standards and policies and the actual delivery of the service. In this situation, frontline service workers know what to do to delight the customer; they simply aren’t doing it. For instance, management may have established a policy that the front desk phones get answered on or before the second ring, but the front desk employees are allowing phones to ring much longer before answering. This gap may arise due to improper training, lack of capability on the part of employees, unwillingness to meet the established service standards, or staff shortages.
Southwest Airlines is a great example of this. According to its website, the mission of the company is “dedication to the highest quality of Customer Service delivered with a sense of warmth, friendliness, individual pride and Company Spirit.” 31 The company doesn’t “overhype” its service, so there is no delivery gap—the difference between the experience specification and the actual delivery of its service. This is demonstrated by the fact that, compared to other airlines, Southwest has the greatest customer service rating, earning a 33.9 percent excellence rating. 32
Gap 4: The Communication Gap
If marketers are doing an effective job in terms of their promotion efforts, the customer is likely to be highly influenced by that promotion. The problem now becomes, the company had better deliver. The communication gap is the difference between the delivery of the service and what is communicated to the customer. In other words, what did the company promise versus what did it deliver?
For example, if your coffee shop asserts in its advertising and on its menu that its food is gluten-free, and it isn’t, customer expectations won’t be met. Failure to deliver on a promise hurts the company’s credibility. Former US President Donald Trump wrote, “A brand is two words: the ‘promise’ you telegraph, and the ‘experience’ you deliver.” 33
Gap 5: The Customer Gap
The customer gap is the difference between the customer’s expectations of the service or experience and their perception of the experience itself. In an ideal world, the customer’s expectations would be nearly identical to their perception, but customer perception is totally subjective and has been shaped by word of mouth, their personal needs, and their own past experiences. The problem here is that each individual perceives their world through their own eyes, and everyone perceives reality differently. In other words, while reality is a fixed factor, perception of reality is a variable.
Link to Learning
Understanding the gap model.
Watch this video and learn more about quality of service and the gap model from Jochen Wirtz, a well-known marketing author.
Also check out this article from Indeed about the GAP Model of Service Quality , with examples.
The RATER Model
In their book Delivering Quality Service, researchers Valerie Zeithaml, A. Parasuraman, and Leonard Berry identified five dimensions of service that customers use when evaluating service quality. Their research pointed to the fact that these five dimensions result in service excellence and lead to higher customer loyalty. This model is sometimes known as the RATER framework of service quality . 34 Refer to Figure 11.12 for a visual representation of the RATER framework.
Let’s explore each of these dimensions (represented by the acronym RATER) in some detail:
Reliability
R, for reliability , depicts the organization’s capability to provide accurate, dependable, and on-time service. 35 Consistency is critical. Companies that provide on-time, error-free service to customers tend to have repeat customers. Research has shown that service reliability is three times more important to customers than the latest equipment or flashy uniforms. 36 The bottom line when it comes to service reliability and quality is: Do you deliver as promised?
A, for assurance , is the degree to which the organization inspires trust in its customers. For example, when you take your sick pet to a veterinarian or have your income tax return prepared (or any other service, for that matter), you expect the service provider to be an expert in the service they’re delivering. Research has shown that communicating this expertise to customers is important. If customers aren’t aware of that expertise, they often have less confidence in that provider, which can lead to a low assessment of that provider’s service. 37
Does your organization inspire confidence in its service providers? Whether you’re a hairstylist, a physical therapist, a tattoo artist, or any number of other service professions, it’s important to communicate your expertise before you do the work. For example, a plumber’s business card may contain the words “licensed, bonded, and insured.” Hairstylists generally display their state licenses in their work space. Doctors often have framed diplomas in the office from medical school, residencies, and fellowships. These are all ways in which these service providers communicate their competencies. Communicating these competencies to customers helps shape expectations and influence assessments in advance of the service. 38
When we talk about tangibles in the RATER model, we’re focusing on factors such as the physical appearance of both the physical facility and employees. Does your organization present itself professionally? This is one of the factors in the RATER metric that is hard to define because it takes into account customers’ perceptions, and different customers may respond in different, subjective ways to the environment created.
Let’s imagine that you’re taking that special someone out for a romantic or special-occasion dinner at a fine-dining restaurant. What tangibles contribute to that experience? You may expect a knowledgeable, uniformed staff; soft lighting and background music; an appealing menu; and clean restrooms. All of these tangibles will factor into your overall perception of the quality of service you receive.
Another good example of tangibles in terms of the RATER model is the Mayo Clinic in Rochester, Minnesota, where tangibles include Warhol prints on the wall, Chihuly sculptures hanging from the ceiling, and a professionally attired staff that projects a sense of caring and expertise. There are 500 original pieces of art from 70 US artists on display throughout the hospital. 39
Customer perception isn’t the only challenge marketers face in terms of tangibles. It’s also the fact that, done right, customers may not even notice and point out the tangibles unless their feedback is negative. That’s why listening and acting on customer complaints is critical in improving an organization’s tangibles and promoting a strong customer service image. 40
Empathy in terms of the RATER model means focusing on customers attentively to ensure that they receive caring and distinguished service. It isn’t enough to be efficient and thorough in delivering service to customers—it’s also about service providers “connecting” with customers during delivery of the service and making them feel valued.
You may have heard the old saying that it’s not what was said, it’s how it was said. The same is true of providing service. For example, let’s go back to the example of that special dinner in the fine-dining restaurant. Imagine that you accidently spill your beverage all over the table. A busser is called to clean the spill, change the tablecloth, and provide you with new silverware and napkins. That busser may have taken care of those tasks effectively and efficiently but didn’t make eye contact, smile, or ask you if you needed anything else. In this hypothetical situation, the busser’s tasks were performed fully, but you didn’t feel that they cared about your predicament. 41
- Responsiveness
A service staff’s desire to treat customers with respect and provide satisfactory and quick service speaks to their responsiveness . This dimension focuses on promptness and willingness. Accordingly, the organization has to ensure that customers are getting quick service, without delay, and with an effort that makes customers believe the company genuinely wants to help them. 42
Responsiveness is directly in line with the amount of time that customers wait for an answer or a solution. Have you ever called an organization with a service question and had to play “20 Questions” with the company’s automated phone system? You know the drill—press 1 for option A, press 2 for option B, press 3 for option C, etc. The chances are that your patience evaporated after about the fourth telephone prompt and you were left screaming “Representative” into your phone. That’s a classic example of a company that needs to focus on its responsiveness if it wants to generate customer loyalty.
Applying the RATER Model to Real-World Companies
Check out this video about Disney guest service and the RATER model.
Also look at this article that applies the RATER model to Amazon , Thermomix , Apple , and a bank.
Knowledge Check
It’s time to check your knowledge on the concepts presented in this section. Refer to the Answer Key at the end of the book for feedback.
- Communication gap
- Customer gap
- Knowledge gap
- Delivery gap
- Responsibility, accuracy, tangibles, empathy, and responsiveness
- Risk, acceptance, transparency, earnings, and revenue
- Reliability, assurance, tangibles, empathy, and responsiveness
- Revenue, appreciation, trust, efficiency, and responsibility
- Transparency
As an Amazon Associate we earn from qualifying purchases.
This book may not be used in the training of large language models or otherwise be ingested into large language models or generative AI offerings without OpenStax's permission.
Want to cite, share, or modify this book? This book uses the Creative Commons Attribution License and you must attribute OpenStax.
Access for free at https://openstax.org/books/principles-marketing/pages/1-unit-introduction
- Authors: Dr. Maria Gomez Albrecht, Dr. Mark Green, Linda Hoffman
- Publisher/website: OpenStax
- Book title: Principles of Marketing
- Publication date: Jan 25, 2023
- Location: Houston, Texas
- Book URL: https://openstax.org/books/principles-marketing/pages/1-unit-introduction
- Section URL: https://openstax.org/books/principles-marketing/pages/11-3-the-gap-model-of-service-quality
© Jan 9, 2024 OpenStax. Textbook content produced by OpenStax is licensed under a Creative Commons Attribution License . The OpenStax name, OpenStax logo, OpenStax book covers, OpenStax CNX name, and OpenStax CNX logo are not subject to the Creative Commons license and may not be reproduced without the prior and express written consent of Rice University.
- Open access
- Published: 28 July 2016
Applying revised gap analysis model in measuring hotel service quality
- Yu-Cheng Lee 1 ,
- Yu-Che Wang 2 ,
- Chih-Hung Chien 3 , 4 ,
- Chia-Huei Wu 5 ,
- Shu-Chiung Lu 3 , 4 , 11 ,
- Sang-Bing Tsai 6 , 7 , 8 , 9 &
- Weiwei Dong 10
SpringerPlus volume 5 , Article number: 1191 ( 2016 ) Cite this article
29k Accesses
34 Citations
Metrics details
Introduction
With the number of tourists coming to Taiwan growing by 10–20 % since 2010, the number has increased due to an increasing number of foreign tourists, particularly after deregulation allowed admitting tourist groups, followed later on by foreign individual tourists, from mainland China. The purpose of this study is to propose a revised gap model to evaluate and improve service quality in Taiwanese hotel industry. Thus, service quality could be clearly measured through gap analysis, which was more effective for offering direction in developing and improving service quality.
Case description
The HOLSERV instrument was used to identify and analyze service gaps from the perceptions of internal and external customers. The sample for this study included three main categories of respondents: tourists, employees, and managers.
Discussion and evaluation
The results show that five gaps influenced tourists’ evaluations of service quality. In particular, the study revealed that Gap 1 (management perceptions vs. customer expectations) and Gap 9 (service provider perceptions of management perceptions vs. service delivery) were more critical than the others in affecting perceived service quality, making service delivery the main area of improvement.
This study contributes toward an evaluation of the service quality of the Taiwanese hotel industry from the perspectives of customers, service providers, and managers, which is considerably valuable for hotel managers. It was the aim of this study to explore all of these together in order to better understand the possible gaps in the hotel industry in Taiwan.
With the number of tourists coming to Taiwan growing by 10–20 % since 2010, the number has increased due to an increasing number of foreign tourists, particularly after deregulation allowed admitting tourist groups, followed later on by foreign individual tourists, from mainland China. Therefore, the tourism industry has become of greater economic importance, according to the Tourism Bureau statistics of Taiwan. The international tourist industry has experienced significant growth in recent years, and more and more hotels provide exquisite, high-quality and customized service that contributes to a hotel’s image and competitiveness in Taiwan (Chen 2013 ). Thence, the hotel sector within the tourism industry faces more intense global competition than other supply industries. Meanwhile, the rapidly growing number of visitors has increased the workload for hotel employees. Thus, they need to staff sufficient professional employees. However, the hotel industry may face the problem of finding qualified employees to provide services that could meet the standards of foreign tourists. Mei et al. ( 1999 ), Tsaur and Lin ( 2004 ) and Hooper et al. ( 2013 ) stated that one of the most influential factors on customers’ perceptions of service quality is the employees. Dedeoğlu and Demirer ( 2015 ) stress the factors contributing to hotel service quality are often the services related to employee behavior and tangibles. Tsang ( 2011 ) studied the Taiwanese hotel industry and found that success and failure in the service delivery of a hotel largely depends on the attitudes and behaviors of contact employees. Thus, determining how employees perceive the services they deliver becomes critical.
Service quality has been identified as crucial to the hotel industry and is measured to assist managers in making decisions, thus improving overall efficiency and profits. Service quality has gradually been recognized as a key factor in gaining competitive advantage and retaining customers (Callan and Kyndt 2001 ; Nasution 2016 ). Currently, Wu and Ko ( 2013 ) hotel organizations have difficulties in adequately assessing and improving their service performance from a customers’ perspective. They also fail to recognize which factors that customers consider important and when they should best evaluate their hotel experience. Moreover, while most of the studies on the hotel sector in the literature focus mainly on the evaluation of customers for service quality, other stakeholders’ (employees’ and managers’) perceptions have been ignored (Dedeoğlu and Demirer 2015 ).
Numerous empirical studies have shown that there were considerable differences in expectations of service quality between customers and management in the service industry (Tsang and Qu 2000 ; Kang and Bradley 2002 ; Lee et al. 2007 ; Chen and Chang 2005 ; Torres et al. 2013 ; Dedeoğlu and Demirer 2015 ). Tsang and Qu ( 2000 ) evaluated perceptions of service quality in China’s hotel industry, from the perceptions of both tourists and managers. Their results indicated that tourists’ perceptions of service quality were consistently lower than their expectations and managers overestimated the service delivery. Some studies have shown that front-line employees frequently serve on their way, so it is difficult for management to inspect their behavior (Bowen and Lawler 1992 ; Schneider and Bowen 1995 ; Yagil 2002 ). Dedeoğlu and Demirer ( 2015 ) addressed the nature and characteristics of differences in service quality perceptions among customers, managers and employees in the hotel industry. Moreover, Torres et al. ( 2013 ) emphasized that studies are required in the field that include the examination of various kinds of feedback (i.e. guests, experts, and operators). The different levels of value provide the need for tourism and hospitality operators to adopt a more comprehensive strategy to collect, analyze, and take appropriate actions. Little empirical research has existed on the evaluation of service quality from the perspective of managers, employees and customers in hotel industry in Taiwan. We believed that management should better understand the customers’ expectations that would influence design, development and delivery the service offering. Employees contact with customers should offer consistent quality of services that would attract and maintain customers directly. The evaluation of the service quality should not only base on customers and managers but also employees, consequently that it is able to assess customer needs and wants accurately. Hence, it is essential to understand the perceptions of customers in relation to the perceptions of managers and employees.
Although several researchers (e.g. Carman 1990 ; Teas 1993 ) have criticized Parasuraman and et al.’ ( 1985 , 1988 ) gap analysis in measuring customer’s service quality perceptions and expectations, it is still the leading measure of service quality (Lam and Woo 1997 ). However, Gap 5 has functional relationships with Gaps 1–4 in the PZB model, these relationships are problematic due to the individual measurement of a gap cannot be determined by combining the gaps. Therefore, a number of researchers have revised the gap model to focus on Gap 5, Gap 1, and other additional gaps (Jannadi et al. 2000 ; Tsang and Qu 2000 ; Chen and Chang 2005 ; Kang and Bradley 2002 ; Dedeoğlu and Demirer 2015 ). Some researchers have confirmed that a revised gap model was relevant to the research scope and effectively evaluated service quality problems which could provide management with important insights. Particularly, Lee et al. ( 2007 ) revised the gap model by decomposing service activities and focused on Gap 5, Gap 1, and three identified additional gaps (Gap 8, Gap 9, and Gap 10). Through the revised gap model, Lee et al. ( 2007 ) stressed that service quality could be clearly measured through these gap scores, which were more effective for offering direction in developing and improving service quality. This study contributes toward an evaluation of the service quality of the Taiwanese hotel industry from the perspectives of customers, service providers, and managers, which is considerably valuable for hotel managers. Furthermore, the study of various sources of perspectives (i.e. tourists, managers, and employees) is often studied separately in the tourism literature. It was the aim of this study to explore all of these together in order to better understand the possible gaps in the hotel industry in Taiwan.
Literature review
Service quality literature.
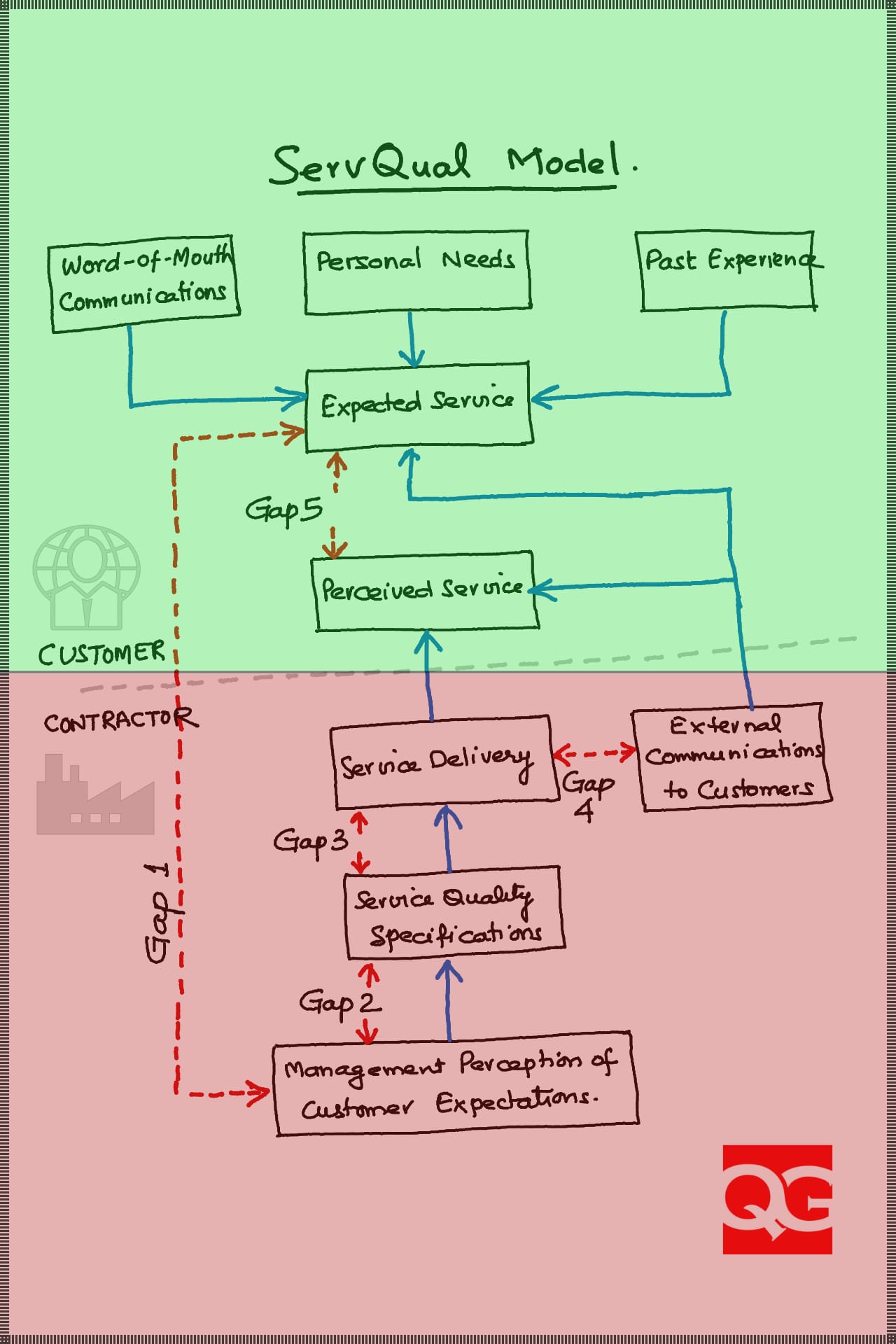
The SERVQUAL model is the most widely used instruments to measure the customer satisfaction in various industries and across different countries, developed by Parasuraman et al. 1985 , then refined in 1988 and 1991. The model is based on the customer’s assessment of service quality, which is a comparison of the expected and the obtain value as well as a consideration of gaps in the process of service provision. The foundation of SERVQUAL instrument was the gap model. The model shown in Fig. 1 identifies five gaps. Gap 1 is the difference between customer expectation and management perceptions of customer expectation, Gap 2 is the difference between management perceptions of customer expectations and service quality specifications, Gap 3 is the difference between service quality specifications and the service actually delivered, Gap 4 is the difference between service delivery and external communication, and Gap 5 is the difference between customer expectation on the service and their perceptions of service performance.
Service quality model
Previous studies (Brown et al. 1993 ; Babakus and Boller 1992 ; Martin 2003 ; Han and Baek 2004 ; Gonzalez et al. 2008 ; Wei et al. 2011 ; Stefano et al. 2015 ) have applied SERVQUAL to measure Gap 5 and Gap 5 has functional relationships with Gaps 1–4 in the PZB model. However, these relationships are problematic because the individual measurement of a gap cannot be determined by combining the gaps.
Application of the Gap model
Luo and Qu ( 2016 ) indicated quality of service is more difficult to define, measure, and manage than manufacturing products due to the unique characteristics of services.
Saleh and Ryan ( 1991 ) identified the existence of gaps between clients’ and management perceptions of attributes of the hotel, and between client expectation and perception of the services offered. Some researchers (Large and Konig 2009 ; Frederick and Mukesh 2001 ) designed INTSERVQUAL, an internal service quality measurement scale based on the “gap model” to successfully measure the difference between internal customers’ understanding and expectation from frontline service staff. Dedeoğlu and Demirer ( 2015 ) indicated while most of the studies on the hotel sector in the literature focus mainly on the evaluation of customers for service quality, other stakeholders’ (employees’ and managers’) perceptions have been ignored. It is argued that the existence of these gaps is a source of dissatisfaction with services provided (Saleh and Ryan 1991 ). Therefore, numerous of studies have been revised the gap model to focus on Gap 5, Gap 1, and other additional gaps (Jannadi et al. 2000 ; Tsang and Qu 2000 ; Chen and Chang 2005 ; Kang and Bradley 2002 ; Dedeoğlu and Demirer 2015 ). Jannadi et al. ( 2000 ) investigated four gaps of service quality in the Saudi Consolidated Electric Company in the Eastern Province and revealed that Gap 3 (service performance) was more critical than the others in affecting perceived service quality, making service delivery the main area of improvement. In addition, there was a revised gap model concentrated on Gap 5, Gap 1, and two additional identified gaps (Gap 6 and Gap 7) demonstrated by Tsang and Qu in 2000. Moreover, a conceptual “gaps model” of information technology (IT) service quality was developed by Kang and Bradly in 2002, which identified seven gaps between customers and IT service suppliers. Dedeoğlu and Demirer ( 2015 ) addressed the nature and characteristics of differences in service quality perceptions among customers, managers and employees. Torres et al. ( 2013 ) emphasized that studies are required in the field that include the examination of various kinds of feedback (i.e. guests, experts, and operators). The different levels of value provide the need for tourism and hospitality operators to adopt a more comprehensive strategy to collect, analyze, and take appropriate actions.
Some researchers have confirmed that a revised gap analysis was relevant to the research scope and effectively evaluated service quality problems which could provide management with important insights. Particularly, Lee et al. ( 2007 ) revised the conceptual model by decomposing service activities and focused on Gap 5, Gap 1, and three identified additional gaps (Gap 8, Gap 9, and Gap 10); Although Gap 5 has a functional relationship with Gaps 1–4 in the PZB model (Parasuraman et al. 1985 ), individual measurement of gap cannot be shown as the combination of gaps. Therefore, our studies applied the revised gap model designed by Lee et al. ( 2007 ). The structure is shown conveniently identified and service quality could be clearly measured through these gap scores in Fig. 2 .
Source: Adapted from Lee et al. ( 2007 )
Revised conceptual model.
The definitions of Gap 5 and Gap 1 are the same as in the PZB model; Gap 5 is the difference between customer perceptions and expectations, and Gap 1 is the difference between management perceptions and customer expectations. Gap 8 is the difference between management perceptions of customer expectations and service encounter perceptions of management perceptions. Gap 9 is the difference between service encounter perceptions of management perceptions and service delivery. This gap represents the gap of service perceptions through the service delivery process. Gap 10 is the difference between service delivery and the perceived service. The functional relationship can be indicated as follows:
The revised conceptual model is another better way to measure gaps of service quality, because it provides a functional relationship that indicates the combination of gaps and the decomposition of service activity. Especially, it offers direction for developing and improving service quality as well (Lee et al. 2007 ).
Service quality of an international hotel
Despite SERVQUAL’s wide use by academics and practicing managers in various industries, a number of studies have questioned the conceptual and operational base of the model (Babakus and Boller 1992 ; Carman 1990 ; Teas 1994 ; Saleh and Ryan 1991 ). Some researchers suggested that further customization of the scale for the hospitality industry was necessary (Saleh and Ryan 1991 ). Various measurement scales such as LODGSERV, HOLSERV, LODGQUAL and DINESERV have been developed for service quality evaluation purposes in the tourism industry. LODGSERV (Knutson et al. 1990 ) and HOLSERV (Mei et al. 1999 ) are used in the accommodation industry. LODGQUAL (Getty and Thompson 1994 ) is to assess service quality in the lodging industry while DINESERV (Stevens et al. 1995 ) is used in the restaurant services sector. Knutson et al. ( 1990 ) adapted SERVQUAL dimensions and developed an instrument called LODGSERV. Reliability is the most critical element in LODGSERV. By contrast, Kandampully and Suhartanto ( 2000 ) identified customer satisfaction with housekeeping as the only significant factor affecting customer loyalty. Mei et al. ( 1999 ) revised SERVQUAL (Parasuraman et al. 1991 ) to include three dimensions of service quality: employees, tangibles, and reliability. They found that the employee dimension was the best predictor of overall service quality. Dedeoğlu and Demirer ( 2015 ) stress the factors contributing to hotel service quality are often the services related to employee behavior and tangibles. In addition, HOLSERV scale more parsimonious and user-friendly than SERVQUAL (Wu and Ko 2013 ). Moreover, consideration of the type of hotel and the range of facilities available, the HOLSERV instrument is suitable for our study in the hospitality industry in Taiwan, to design service strategies that meet guest expectations.
Methodology
Questionnaire design and distribution.
After a review of the literature, the HOLSERV instrument by Mei et al. ( 1999 ) was used to identify and analyze service gaps among the perceptions of tourists, employees and hotel managers. The gap in service quality was measured using the 27 items of the HOLSERV, with a 9-point scale ranging from 1 (completely unfulfilled) to 9 (much fulfillment). The sample comprised three main categories of respondents: tourists; employees, and managers. The first category of the questionnaire was designed to examine the tourists’ expectations and perceptions of service quality. The second category of the questionnaire was designed to evaluated managers’ perceptions of customer expectations. The third category of the questionnaire was designed to assess employee perceptions of manager perceptions and employee perceptions of perceived service. The target population of the tourist survey was all international tourists who visited hotels in Taipei, Taiwan were chosen for this study.
A total of 382 tourists were invited to complete the questionnaire, and 341 effective samples were obtained (usable response rate of 89.2 %). The gender breakdown of the respondents was 56.3 % male and 43.7 % female. Of the 341 respondents, 255 were tourists, 40 were managers, and 46 were employees.
Demographic profile of the hotel tourists, employees, and managers
The questionnaire survey sites selected for this study were two international hotels in Taiwan. A convenience sampling method was applied. Ultimately, 300 tourists were invited to complete the questionnaire and 255 effective responses were obtained (for a usable response rate of 83.30 %). The sample of tourists contained more males (55.69 %) than females (44.31 %). More than half of the respondents had a university, college, or graduate education. Approximately 55 % of the respondents were professionals, executives, or sales people, and nearly 55 % earned an annual household income of US $32,000 or above. The majority of the respondents (60 %) were aged 21–40 years. Most of the respondents were from the cities of Taipei (55 %), Tainan (15 %), or Taichung (10 %), and the rest of the respondents (20 %) were from other countries.
The target population for the management survey was all supervisors and managers (ranging from the supervisor to the general manager level) who worked in two hotels located in the cities of Taipei and Taichung. The sample size was 40. The sample of managers contained more males (60 %) than females (40 %), and more than 80 % were aged 31–50 years. More than 60 % of the respondents had a university, college, or graduate education. The respondents ranged from supervisors to general managers, and 68 % were departmental managers or supervisors. More than a quarter of respondents worked in the housekeeping department, followed by the front desk (16 %), training (14 %), food and beverage (11 %) and other departments (30 %).
The target population for the employee surveys were from the housekeeping department, front desk, training, food and beverage, and other departments. The sample size was 46. The sample of employees contained more males (56.52 %) than females (43.48 %) and more than 70 % were aged 21–40 years. More than half of the respondents had a university, college, or graduate education.
As noted in Table 1 , the results of Gap 5 indicated that, all attributes were negative scores, and there was a significant difference between tourists’ actual perceptions and their expectations. And overall service quality provided below tourists’ expectation. The biggest gaps were on attributes, 6 “Gives prompt service (−1.048)”, 4 “Provides services at the time it promises to do so” (−0.932), 1 “Promises to provide a service and does so” (−0.915), 2 “Shows dependability in handling service problems” (−0.915), and 3 “Performs the service right the first time” (−0.881). Those attributes were the most serious deficiencies which would need pay close attention by managers and make improvement effectively. The overall Gap 5 score was −0.662 which would showed that the overall service quality provided by the hotel in Taiwan would not meet tourists’ expectation.
As shown in Table 1 , a comparison of managers’ perception for tourists’ expectation and the tourists’ themselves expectation. The result indicted that, the overall Gap 1 score was −0.583, which would indicated that managers do not have a good understanding of tourist expectation. This finding contrasts with previous studies (Nel and Pitt 1993 ; Tsang and Qu 2000 ) but consistent with past research (Choy et al. 1986 ; Wei et al. 1989 ).
All 27 attributes were negative and very big. The range from attribute 17 “Has guests’ best interests at heart” (−0.268) to attribute 1 “Promises to provide a service and does so” (−1.036) was big variation. The biggest gaps were on attributes, 1 “Promises to provide a service and does so” (−1.036), 3 “Performs the service right the first time” (−0.891), 8 “Never too busy to respond to guests’ requests” (−0.877) and 22 “Materials are visually appealing” (−0.873). Therefore, from the results of negative Gap 1 score and big difference, it can be concluded that Gap 1 tend to a major problems related to Gap 5 of service quality in the hotel case.
As noted in Table 1 , for the most part, employees’ perception for delivery are more than managers’ perception for tourists’ expectation except attribute 4 “Provides services at the time it promises to do so” (−0.077) and attribute 11 “Guests feel safe and secure in their stay” (−0.053). In addition, the overall Gap 8 score was +0.312, which would indicted that the managers tend to have good communication with employees for understanding tourists’ expectation. Hence, Gap 8 is probably not to be a major problem of service quality in the hotel case.
As shown in Table 1 , the mean score gaps along each of 27 attributes was calculated for employees’ perception of manager’s requirement and service delivery by themselves. The result of the overall Gap 9 score for this study was −0.547 and all difference of attributes were negative and very big. The range from attribute 24 (−0.391) to attribute 25 (−0.717), was quite big variation. The biggest gaps were on attributes, 25 “Equipment and facilities are generally clean” (−0.717), 1 “Promises to provide a service and does so” (−0.696), 17 “Has guests’ best interests at heart” (−0.674), 2 “Shows dependability in handling service problems” (−0.630) and 26 “Variety of food and beverages meet guests’ needs (−0.630)”. Accordingly, from the results of negative Gap 9 score and big difference, it also can be concluded that Gap 9 seems one of major problems related to Gap 5 of service quality in the hotel case.
The results of Table 1 show that, for most part, employees believed that their perception for delivery are more than tourists themselves perception except attributes 24 “Equipment and facilities are easy to use” (−0.050) and attribute 26 “Variety of food and beverages meet guests’ needs” (−0.050). In addition, the overall gap 10 score was 0.156, which would indicated that the employees tend to have a good understanding of customer expectations. Therefore, from the results of positive gap 10 score, consequently, Gap 10 did not seem to a major problem of service quality in the hotel case as well.
This study provided a new measurable instrument and expressed the evaluation results of the service quality gap between expectations and perceptions for tourists, managers, and employees in the hotel industry. Thus, this study identified the gaps (Gap 5, Gap 1, Gap 8, Gap 9, and Gap 10) that could appear from inconsistency in the expectations and perceptions of service quality among tourists, management, and employees and demonstrated how the gaps could be reduced.
An analysis of Gap 5 illustrated how the gaps between customers’ perceptions of service quality and their expectations could be reduced. The Gap 5 analysis indicated that tourists’ perceptions were consistently lower than their expectations. The overall Gap 5 score was −0.662, which showed that the overall service quality provided by the hotel industry in Taiwan was below tourists’ expectations. According to our Gap 5 analysis, the biggest gaps were associated with “gives prompt service,” “provides services at the time it promises to do so,” and “promises to provide a service and does so.” This indicates a problem of reliability and responsiveness in service quality. The negative Gap 5 scores clearly showed that managers in the Taiwanese hotel industry must still improve and enhance its service quality. The Gap 5 analysis was essential because it offered a measurable and useful tool for the management to identify the service problems in the hotel industry in Taiwan. In additional, managers should consistently implement such analysis so that they can further understand the tourists’ evaluation process and their consumer experiences and hence meet their expectations more consistently. However, to reduce Gap 5, managers should also concern themselves with the other four gaps (Gap 1, Gap 8, Gap 9, and Gap 10) that contribute to Gap 5. Therefore, this revised gap model offers a method for managers to identify the causes of Gap 5 that can be clearly measured through the gap scores of the hotel industry in Taiwan. According to our results, the functional relationship can be expressed as follows:
Examining Gap 1 was a necessary step that contributed toward the understanding of whether managers accurately perceive tourists’ service quality expectations from the Taiwanese hotel industry. The result showed that the overall Gap 1 score was −0.583, indicating that managers do not fully understand customer expectations. Accordingly, given the negative Gap 1 score results and the large difference in expectations and perceptions, we conclude that Gap 1 is one of the major problems of service quality and that it contributes to Gap 5. Moreover, when managers’ perception of tourists’ expectations is close to the tourists’ expectations (Gap 1), the difference in customers’ perceptions of service quality and their expectations can be narrowed (Gap 5) as well. Our findings are consistent with those of past studies (Coyle and Dale 1993 ; Zeithaml et al. 1990 ; Tsang and Qu 2000 ) that have argued that managers traditionally have the least contact with customers and are thus unable to understand customer wants accurately. Thus, they might initiate a chain of bad decisions, leading to poor perceived service quality. In improving the service quality (i.e., narrowing Gap 5), managers should re-examine the service delivery process that meets tourists’ requirements and wants in the Taiwanese hotel industry. The hotel management should attempt to address marketing research orientation, upward communication, and the quality of management. To gain first-hand knowledge of tourists’ expectations and perceptions, senior management should consistently contact tourists and inquire about the actual service delivery. Thus, managers can more accurately fulfill tourists’ expectations and provide the desired level of service performance.
Assessing Gap 8 was a critical task that contributed toward knowing whether employees accurately perceive tourists’ service quality expectations from the Taiwanese hotel industry. The overall Gap 8 score was 0.312, indicating that the managers did a good job at training or communicating with employees to understand customers’ expectations. Hence, Gap 8 was not a primary contributor to Gap 5.
Evaluating Gap 9 was crucial to identifying whether employees followed managers’ requirements and were able to perform services at the desired level in the Taiwanese hotel industry. The Gap 9 score in this study was −0.547, indicating a difference between service performance standards and the actual service delivered. Gap 9 often occurred because of some limits, such as poor service attitudes, poorly qualified employees, insufficient service capacity, and inadequate internal communication systems. Because of these constraints, employees could not offer services at the level required by the management. The existence of Gap 9 was related to Gap 1. Moreover, if managers do not fully understand tourists’ expectations, employees cannot deliver service adequately. Therefore, to reduce the gap between employees’ perceptions of managers’ requirements and service delivery, managers in the hotel industry in Taiwan should apply internal investigation systems to evaluate whether their employees can meet the stipulated service standards.
Measuring Gap 10 contributed toward assessing whether employees overestimate whether their service delivery meets tourists’ expectations. The overall score in Gap 10 for this study was 0.156, which indicated that employees tended to have a reasonably good understanding of customer expectations. Because of the positive score results, Gap 10 was deemed not to be a primary contributor to Gap 5.
This research makes the following three contributions. First, this research develops an evaluation of the service quality of the Taiwanese hotel industry from the perspectives of customers, service providers, and managers, which is considerably valuable for hotel managers. Second, this study explores all of perspectives (i.e. tourists, managers, and employees) together in order to better understand the possible gaps in the hotel industry in Taiwan. This revised gap analysis model can be the reference for related research. Third, the study revealed that Gap 1 (management perceptions vs. customer expectations) and Gap 9 (service provider perceptions of management perceptions vs. service delivery) were more critical than the others in affecting perceived service quality, making service delivery the main area of improvement.
The results of this study also provide a number of managerial contributions. Managers should understand the reason why these differences occur, suggesting that management in the hotel industry spend more time interacting with tourists and conduct internal investigations to assess if their employees are able to meet the service standards, so that the employees willingly provide a good quality of service that benefits hotel operations. Moreover, with the revised gap analysis, managers can effectively prioritize a task to effectively compensate for shortfalls in the provided service. Obviously, managers should eliminate the existence of Gap 1; subsequently, Gap 9 could be reduced. Likewise, if managers do not have a clear perception of customer expectations, employees cannot deliver adequate services. To improve service quality efficiently, managers must be able to identify the priorities of improvements of service attributes especially with limited resources. Finally, the revised gap analysis enable managers to understand the specific attributes that significantly affect service quality and thus enables them to recognize the explicit quality attributes that must be improved and would enhance customer satisfaction within the hotel industry. Overall, this study not only proposes reliable and effective methods but also obviously recognizes which factors that customers consider important as related to management when they should best evaluate their hotel experience. Applying reliable and effective methods for service quality improvement, will lead to a higher level of customer satisfaction and profitability of a firm. In summary, Travel and Tourism is an important economic activity in most countries around the world which not only affect the economic growth but also to increase employment opportunities.
Limitations and suggestions for future research
There are some limitations in this study that must be recognized. First, the international tourist hotels surveyed in this study were small- and medium-sized hotels operating in Taipei. Because Taipei is more modern and well developed than are some other Taiwanese cities, these results might not represent the quality of hotel services across Taiwan. Second, the sample size was quite small (N = 255), employees (N = 46), and managers (N = 40). Future research should collect a larger number of samples and include a more diverse range of tourists, employees, and hotel managers. Third, this study conducted preliminary research into hotel services. Thus, the findings cannot be generalized to other service sectors. Future studies should collect data from different industries, such as banks, airlines, insurance providers, and call centers, to extend the scope of our findings. Fourth, this research was only limited to three-star hotels in Taiwan. Future studies should attempt to examine service quality across different hotel ratings or countries. This may provide an opportunity to compare the quality of service based on different hotel ratings (e.g., four or five-star hotels) or countries. Likely, Luo and Qu ( 2016 ) indicated that Westerners were more satisfied with service quality than do Chinese guests. In addition, this research could be applied to different categories, for example three-star, aparthotels, motels, inns and boutique. Finally, the findings of this study were based on a survey. Hence, future studies should apply a qualitative design to obtain an in depth understanding of the perceptions of customers in relation to those of managers and employees.
Babakus E, Boller GW (1992) An empirical assessment of the SERVQUAL scale. J Bus Res 24(3):253–268
Article Google Scholar
Bowen D, Lawler EE III (1992) The empowerment of service workers: What, why, how, and when. Sloan Manag Rev 33:31–39
Google Scholar
Brown TJ, Churchill GA, Peter JP (1993) Improving the measurement of service quality. J Retail 69(1):127–139
Callan RJ, Kyndt G (2001) Business travelers’ perception of service quality: a prefatory study of two European city centre hotels. Int J Tourism Res 3(4):313–323
Carman JM (1990) Consumer perceptions of service quality: an assessment of the dimensions. J Retail 66(1):33–55
Chen FY, Chang YH (2005) Examining airline service quality from a process perspective. J Air Trans Manag 11:79–87
Chen WJ (2013) Factors influencing internal service quality at international tourist hotels. Int J Hosp Manag 35:152–160
Choy DJL, Guan LD, Zhang W (1986) Tourism in PR China. Marketing trends and changing policies. Tour Manag 7(3):197–201
Coyle MP, Dale BG (1993) Quality in the hospitality industry: a study. Int J Hosp Manag 12(2):141–153
Dedeoğlu BB, Demirer H (2015) Differences in service quality perceptions of stakeholders in the hotel industry. Int J Contemp Hosp Manag 27(1):130–146
Frederick AF, Mukesh K (2001) Service quality between internal customers and internal suppliers in an international airline. Int J Qual Reliab Manag 18(4):371–386
Getty JM, Thompson KN (1994) A procedure for scaling perceptions of lodging quality. Hosp Res J 18:75–96
Gonzalez ME, Mueller RF, Mack RW (2008) An alternative approach in service quality: an e-banking case study. Qual Manag J 15(1):41–59
Han SL, Baek S (2004) Antecedents and consequences of service quality in online banking: an application of the SERVQUAL instrument. Adv Consum Res 31:208–214
Hooper D, Coughlan J, Mullen MR (2013) The servicescape as an antecedent to service quality and behavioral intentions. J Serv Mark 27(4):271–280
Jannadi OA, Assaf S, Maghraby HM, Al-Saggaf HA (2000) Service quality gaps analysis at SCECO-East, Saudi Arabia. J Energy Eng 126(3):116–131
Kandampully J, Suhartanto D (2000) Customer loyalty in the hotel industry: the role of customer satisfaction and image. Int J Contemp Hosp Manag 12(6):346–351
Kang H, Bradley G (2002) Measuring the performance of IT services: an assessment of SERVQUAL. Int J Account Inf Syst 3:151–164
Knutson B, Stevens P, Wullaert C, Patton M, Yokoyama F (1990) LODGSERV: a service quality index for the lodging industry. Hosp Res J 14(2):227–284
Lam SK, Woo KS (1997) Measuring service quality: a test-retest reliability investigation of SERVQUAL. J Res Mark Res Soc 39:381–396
Large RO, Konig T (2009) A gap model of purchasing’s internal service quality: concept, case study and internal survey. J Purch Supply Manag 15:24–32
Lee YC, Chen JK, Lin SB (2007) Revised Gap analysis by decomposition of service activities: a case study of information system center. Int J Bus Strategy 8(2):74–98
Luo Z, Qu H (2016) Guest-defined hotel service quality and its impacts on guest loyalty. J Qual Assur Hosp Tour 17(3):311–332
Martin S (2003) Using SERVQUAL in health libraries across Somerset, Devon and Cornwall. Health Inf Libr J 20(1):15–21
Mei AWO, Dean AM, White CJ (1999) Analysing service quality in the hospitality industry. Manag Serv Qual Int J 9(2):136–143
Nasution H (2016) Coaligning service quality attributes and its implication to customer value. In: Colin C, Junzhao JM (eds) Looking forward, looking back: drawing on the past to shape the future of marketing. Springer, pp 751–759
Nel D, Pitt L (1993) Service quality in a retail environment: closing the gaps. J Gen Manag 18(3):37–56
Parasuraman A, Zeithaml VA, Berry LL (1985) A conceptual model of service quality and its implications for future research. J Mark 49(4):41–50
Parasuraman A, Zeithaml V, Berry LL (1988) SERVQUAL: a multiple-item scale for measuring consumer perceptions of service quality. J Retail 64(1):12–40
Parasuraman A, Zeithaml V, Berry LL (1991) Refinement and reassessment of the SERVQUAL scale. J Retail 67:420–450
Saleh F, Ryan C (1991) Analysing service quality in the hospitality industry using the SERVQUAL model. Serv Ind J 11(3):324–345
Schneider B, Bowen DE (1995) Winning the service game. Harvard Business School Press, Boston
Stefano NM, Casarotto Filho N, Barichello R, Sohn AP (2015) A fuzzy SERVQUAL based method for evaluated of service quality in the hotel industry. Proc CIRP 30:433–438
Stevens P, Knutson B, Patton M (1995) “DINESERV: a tool for measuring service quality in restaurants”. Cornell Hotel Restaur Adm Q 36(2):56–60
Teas RK (1993) Expectations, performance evaluation and customers’ perceptions of quality. J Mark 57:18–34
Teas RK (1994) Expectations as a comparison standard in measuring service quality: an assessment of a reassessment. J Mark 58(1):132–139
Tsang NK (2011) Dimensions of Chinese culture values in relation to service provision in hospitality and tourism industry. Int J Hosp Manag 30(3):670–679
Tsang N, Qu H (2000) Service quality in China’s hotel industry: a perspective from tourists and hotel managers. Int J Contemp Hosp Manag 12:316–326
Tsaur S-H, Lin Y-C (2004) Promoting service quality in tourist hotels: the role of HRM practices and service behavior. Tour Manag 25(4):471–481
Torres EN, Adler H, Lehto X, Behnke C, Miao L (2013) One experience and multiple reviews: the case of upscale US hotels. Tour Rev 68(3):3–20
Wei L, Crompton JL, Reid LM (1989) Cultural conflicts: experiences of US visitors to China. Tour Manag 10(4):322–332
Wei SP, Shih SC, Lin SC, Liu CJ, Lu YW, Chang WL (2011) Primary caregivers satisfaction and its related factors in home health care services. Int J Gerontol 5(2):107–111
Wu HC, Ko YJ (2013) Assessment of service quality in the hotel industry. J Qual Assur Hosp Tour 14(3):218–244
Yagil D (2002) The relationship of customer satisfaction and service workers’ perceived control examination of three models. Int J Serv Ind Manag 13(4):382–398
Zeithaml VA, Parasuraman A, Berry LL (1990) Delivering quality service balancing customer perceptions and expectations. The Free Press, New York
Download references
Authors’ contributions
Writing: C-HC; Providing case and idea: Y-CL, Y-CW, C-HW, S-CL; Providing revised advice: S-BT, WD. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Author information
Authors and affiliations.
Department of Technology Management, Chung-Hua University, Hsinchu, 300, Taiwan
Yu-Cheng Lee
Department of Business Administration, Chung-Hua University, Hsinchu, 300, Taiwan
Yu-Che Wang
PhD Program of Technology Management, Chung-Hua University, Hsinchu, 300, Taiwan
Chih-Hung Chien & Shu-Chiung Lu
Department of Business Administration, Lee-Ming Institute of Technology, Taipei City, 243, Taiwan
Department of Tourism and Leisure Management, Yuanpei University of Medical Technology, Hsinchu, 300, Taiwan
Chia-Huei Wu
Zhongshan Institute, University of Electronic Science and Technology of China, Guangdong, 528402, China
Sang-Bing Tsai
School of Economics & Management, Shanghai Maritime University, Shanghai, 201306, China
Law School, Nankai University, Tianjin, 300071, China
School of Business, Dalian University of Technology, Panjin, 124221, China
School of Economics and Management, Shanghai Institute of Technology, Shanghai, 201418, China
Weiwei Dong
Department of Food and Beverage Management, Lee-Ming Institute of Technology, Taipei City, 243, Taiwan
Shu-Chiung Lu
You can also search for this author in PubMed Google Scholar
Corresponding authors
Correspondence to Sang-Bing Tsai or Weiwei Dong .
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License ( http://creativecommons.org/licenses/by/4.0/ ), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Reprints and permissions
About this article
Cite this article.
Lee, YC., Wang, YC., Chien, CH. et al. Applying revised gap analysis model in measuring hotel service quality. SpringerPlus 5 , 1191 (2016). https://doi.org/10.1186/s40064-016-2823-z
Download citation
Received : 11 April 2016
Accepted : 12 July 2016
Published : 28 July 2016
DOI : https://doi.org/10.1186/s40064-016-2823-z
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Service quality
- Gap analysis
- Business management
Models of Service Quality
- First Online: 29 July 2023
Cite this chapter

- Manfred Bruhn 2
851 Accesses
Different models for the analysis of the emergence of service quality have been developed in the existing literature. Based on a comprehensive presentation and discussion of the best-known and most important models, it becomes clear in the context of this chapter that the so-called GAP model has gained international importance. As a result, the approach of the GAP model has been modified and adapted for different application areas and industries in the meantime. An explanation of these approaches is also given in the context of this chapter. In conclusion, central quality dimensions could be isolated in the scientific literature—based on the results of the GAP model—which come into effect for the customers of a service provider when assessing the experienced quality.
This is a preview of subscription content, log in via an institution to check access.
Access this chapter
- Available as PDF
- Read on any device
- Instant download
- Own it forever
- Available as EPUB and PDF
- Durable hardcover edition
- Dispatched in 3 to 5 business days
- Free shipping worldwide - see info
Tax calculation will be finalised at checkout
Purchases are for personal use only
Institutional subscriptions
Bitner, M. J., Ostrom, A. L., & Meuter, M. L. (2002). Implementing successful self-service technologies. Academy of Management Executive, 16 (4), 96–109.
Google Scholar
Boshoff, C., & Terblanche, N. S. (1997). Measuring retail service quality. A replication study. South African Journal of Business Management, 28 (4), 123–129.
Article Google Scholar
Boulding, W., & Staelin, R. (1993). A dynamic process model of service quality assessment. In E. E. Scheuing & W. F. Christopher (Eds.), The service quality handbook (pp. 177–194). New York.
Boulding, W., Kalra, A., Staelin, R., & Zeithaml, V. A. (1993). A dynamic process model of service quality. From expectations to behavioral intentions. Journal of Marketing Research, 30 (1), 7–27.
Bruggemann, A. (1974). Zur Unterscheidung verschiedener Formen von Arbeitszufriedenheit. Arbeit und Leistung, 28 (11), 281–284.
Bruhn, M. (2002). Electronic Services. Eine Einführung in die theoretischen und praktischen Probleme. In M. Bruhn, & B. Stauss (Eds.), Electronic Services. Jahrbuch Dienstleistungsmanagement 2002 (pp. 3–49). Wiesbaden: Gabler.
Bruhn, M., & Batt, V. (2015). Qualität von E-Health Services: Entwicklung und empirische Überprüfung eines Messinstruments. Marketing ZFP, 37 (1), 42–56.
Bruhn, M., & Georgi, D. (2006). Services marketing. Managing the service value chain. Harlow: Pearson Education Limited.
Collier, D. A. (1996). Tight and loose comprehensive customer contact (3c) plans and strategies. In T. A. Swartz, & S. W. Brown (Eds.), Advances in services marketing and management. Research and practice (5. Aufl., pp. 153–168). London.
Collier, J. E., & Bienstock, C. C. (2006). Measuring service quality in e-retailing. Journal of Service Research, 8 (3), 260–275.
Dabholkar, P. A., Thorpe, D. I., & Rentz, J. O. (1996). A measure of service quality for retail stores. Scale development and validation. Journal of the Academy of Marketing Science, 24 (1), 3–16.
Dimitriadis, S., & Stevens, E. (2008). Integrated customer relationship management for service activities: An internal/external gap model. Managing Service Quality: An International Journal, 18 (5), 496–511.
Eng, T. R. (2001). The e-health landscape: A terrain map of emerging information and communication technologies in health and health care. Princeton: Robert Wood Johnson Foundation.
Faßnacht, M., & Koese, I. (2006). Quality of electronic services. Journal of Service Research, 9 (1), 19–37.
Frost, F. A., & Kumar, M. (2000). INTSERVQUAL—An internal adaptation of the GAP model in a large service organisation. Journal of Services Marketing, 14 (4/5), 358–377.
Giovanis, A. N., & Athanasopoulou, P. (2014). Gaining customer loyalty in the e-tailing marketplace: The role of e-service quality, e-qatisfaction and e-trust. International Journal of Technology Marketing, 9 (3), 288–304.
Grönroos, C. (1984). A service quality model and its marketing implications. European Journal of Marketing, 18 (4), 36–44.
Grönroos, C. (2007). Service management and marketing. Customer management in service competition (3. Aufl.). Chichester: Wiley.
Grund, M. A. (1998). Interaktionsbeziehungen im Dienstleistungsmarketing. Zusammenhänge zwischen Zufriedenheit und Bindung von Kunden und Mitarbeitern. Wiesbaden: Gabler.
Hadwich, K., Georgi, D., Tuzovic, S., Büttner, J., & Bruhn, M. (2010). Perceived quality of e-health services. A conceptual scale development of e-health service quality based on the C-OAR-SE approach. International Journal of Pharmaceutical and Healthcare Marketing, 4 (2), 112–136.
Hentschel, B. (1999). Multiattributive Messung von Dienstleistungsqualität. In M. Bruhn, & B. Stauss (Eds.), Dienstleistungsqualität. Konzepte – Methoden – Erfahrungen (3rd Edn., pp. 289–320). Wiesbaden: Gabler.
Jayawardhena, C. (2004). Mesurement of service quality in internet banking. The development of an instrument. Journal of Marketing Management, 20 (1), 185–207.
Joseph, M., McClure, C., & Joseph, B. (1999). Service quality in the banking sector: The impact of technology on service delivery. International Journal of Bank Marketing, 20 (4/5), 182–192.
Kellogg, D. L., & Chase, R. B. (1995). Constructing an empirically derived measure for customer contact. Management Science, 41 (11), 1734–1749.
Kirchgeorg, M., & Lorbeer, A. (2002). Kundenbindungsstrategien von E-Health Service-Anbietern. In M. Bruhn, & B. Stauss (Eds.), Electronic Services. Jahrbuch Dienstleistungsmanagement 2002 (pp. 585–611). Wiesbaden: Gabler.
Kuo, T., Lu, I., Huang, C., & Wu, G. (2005). Measuring users’ perceived portal service quality: An empirical study. Total Quality Management, 16 (3), 309–320.
Lerer, L., & Rowell, N. (2000). The e-health consumer, INSEAD healthcare management initiative, the healthcare 2020 Platform. Fontainebleau.
Liljander, V., & Strandvik, T. (1995). The nature of customer relationships in services. In T. A. Swartz, D. E. Bowen, & S. W. Brown (Eds.), Advances in services marketing and management research and practice (4th Edn., pp. 141–167). Greenwich.
Liu, C. T., Guo, Y. M., & Lee, C. H. (2011). The effects of relationship quality and switching barriers on customer loyalty. International Journal of Information Management, 31 (1), 71–79.
Long, M., & McMellon, C. (2004). Exploring the determinants of retail service quality on the internet. Journal of Services Marketing, 18 (1), 78–90.
Luk, S. T., & Layton, R. (2002). Perception gaps in customer expectations: Managers versus service providers and customers. Service Industries Journal, 22 (2), 109–128.
Manschwetus, U., & Rumler, A. (2002). Strategisches Internetmarketing. Entwicklungen in der Net-Economy. Wiesbaden: Springer.
Meyer, A., & Mattmüller, R. (1987). Qualität von Dienstleistungen. Entwicklung eines praxisorientierten Qualitätsmodells. Marketing ZFP, 9 (3), 187–195.
Meyers, J., van Brunt, D., Patrick, K., & Greene, A. (2002). Personalizing medicine on the web: E-health offers hospitals several strategies for success. Health Forum Journal, 45 (1), 22–26.
Murmann, B. (1999). Qualität mehrstufiger Dienstleistungsinteraktionen. Besonderheiten bei Dienstleistungsunternehmen mit direktem und indirektem Kundenkontakt. Wiesbaden: Gabler.
Nielsen (2012). Gesundheitsinformationen aus dem Internet immer wichtiger. http://nielsen.com/de/de/insights/presseseite/2012/gesundheitsinformationen-aus-dem-internet-immer-wichtiger.html . Zugegriffen: 19. Febr. 2012.
Niranjan, T. T., & Metri, B. A. (2008). Client-vendor-end user triad: A service quality model for IS/ITES outsourcing. Journal of Services Research, 8 (1), 123–128.
Parasuraman, A., Zeithaml, V. A., & Berry, L. L. (1985). A conceptual model of service quality and its implications for future research. Journal of Marketing, 49 (1), 41–50.
Parasuraman, A., Zeithaml, V. A., & Berry, L. L. (1986). SERVQUAL. A multiple-item scale for measuring consumer perceptions of service quality. Report No. 86–108. Cambridge.
Parasuraman, A., Zeithaml, V. A., & Berry, L. L. (1988). SERVQUAL: A multiple-item scale for measuring consumer perceptions of service quality. Journal of Retailing, 64 (1), 12–40.
Parasuraman, A., Zeithaml, V. A., & Malhotra, A. (2005). ES-QUAL. A multiple-item scale for assessing electronic service quality. Journal of Service Research, 7 (3), 213–233.
Parikh, D. (2006). Measuring retail service quality: An empirical assessment of the instrument. Vikalpa, 31 (2), 45–55.
Reichwald, R. P., Möslein, K. M., Kölling, M., & Neyer, A. K. 2 Service-Innovation . Leipzig.
van Riehl, A., Semeijn, J., & Janssen, W. (2003). E-Service quality expectations. A case study. Total Quality Management, 14 (4), 437–450.
Santos, J. (2003). E-Service quality: A model of virtual service quality dimensions. Managing Service Quality, 13 (3), 233–246.
Schlötelburg, C., & Bröckerhoff, H.-P. (2010). E-Health-Compendium Telemonitoring 2010/11. Themen – Anwendungen – Service . Berlin.
Schneider, B., & Bowen, D. E. (1999). The service organization. Human resources management is critical. In J. E. G. Bateson (Eds.), Managing services marketing. Text and readings (3rd Edn., pp. 273–283). Texas.
Sousa, R., & Voss, C. (2012). The impacts of e-service quality on customer behaviour in multichannel e-services. Total Quality Management & Business Excellence, 23 (7–8), 789–806.
Stanforth, N. F., & Lennon, S. J. (1997). Salesperson service and customer satisfaction. The impact of store policies. In T. A. Swartz, D. E. Bowen, & D. Iacobucci (Eds.), Advances in services marketing and management research and practice (6th Edn., pp. 79–99). Greenwich.
Stauss, B., & Neuhaus, P. (1995). Das Qualitative Zufriedenheitsmodell, Diskussionsbeiträge Nr. 66 . Ingolstadt.
Wolfinbarger, M., & Gilly, M. (2003). eTailQ. Dimensionalizing, measuring and predicting eTail quality. Journal of Retailing, 79 (3), 183–198.
Yang, Z., & Jun, M. (2002). Consumer perception of e-service quality: From internet purchaser and non-purchaser perspectives. Journal of Business Strategies, 19 (1), 19–41.
Zeithaml, V. A. (2002). Service excellence in electronic channels. Managing Service Quality, 12 (3), 135–138.
Zeithaml, V. A., Berry, L. L., & Parasuraman, A. (1988). Communication and control processes in the delivery of service quality. Journal of Marketing, 52 (4), 35–48.
Zeithaml, V. A., Berry, L. L., & Parasuraman, A. (1996). The behavioral consequences of service quality. Journal of Marketing, 60 (2), 31–46.
Zeithaml, V. A., Parasuraman, A., & Berry, L. L. (1992). Qualitätsservice. Was Ihre Kunden erwarten – was Sie leisten müssen . Frankfurt a. M.: Campus.
Zollondz, H.-D. (2011). Grundlagen Qualitätsmanagement. Einführung in Geschichte, Begriffe, Systeme und Konzepte (3rd Edn.). München: Oldenbourg.
Download references
Author information
Authors and affiliations.
Faculty of Business and Economics, Marketing and Corporate Management, University Basel, Basel, Switzerland
Manfred Bruhn
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Manfred Bruhn .
Rights and permissions
Reprints and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer-Verlag GmbH, DE, part of Springer Nature
About this chapter
Bruhn, M. (2023). Models of Service Quality. In: Quality Management for Services. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-662-67032-3_4
Download citation
DOI : https://doi.org/10.1007/978-3-662-67032-3_4
Published : 29 July 2023
Publisher Name : Springer, Berlin, Heidelberg
Print ISBN : 978-3-662-67031-6
Online ISBN : 978-3-662-67032-3
eBook Packages : Business and Management Business and Management (R0)
Share this chapter
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Publish with us
Policies and ethics
- Find a journal
- Track your research
- ASQ® CQA Exam
- ASQ® CQE Exam
- ASQ® CSQP Exam
- ASQ® CSSYB Exam
- ASQ® CSSGB Exam
- ASQ® CSSBB Exam
- ASQ® CMQ/OE Exam
- ASQ® CQT Exam
- ASQ® CQPA Exam
- ASQ® CQIA Exam
- 7 Quality Tools
- Quality Gurus
- ISO 9001:2015
- Quality Cost
- Six Sigma Basics
- Risk Management
- Lean Manufacturing
- Design of Experiments
- Quality Acronyms
- Quality Awareness
- Quality Circles
- Acceptance Sampling
- Measurement System
- APQP + PPAP
- GD&T Symbols
- Project Quality (PMP)
- Full List of Quizzes >>
- Reliability Engineering
- Statistics with Excel
- Statistics with Minitab
- Multiple Regression
- Quality Function Deployment
- Benchmarking
- Statistical Process Control
- Quality Talks >> New
- Six Sigma White Belt
- Six Sigma Yellow Belt
- Six Sigma Green Belt
- Six Sigma Black Belt
- Minitab 17 for Six Sigma
- Casio fx-991MS Calculator
- CSSYB/LSSYB Mock Exam
- CSSGB/LSSGB Mock Exam
- CSSBB/LSSBB Mock Exam
- ASQ® CQA Preparation
- ASQ® CQE Preparation
- ASQ® CQPA Preparation
- ASQ® CQIA Preparation
- CQE Mock Exams
- CMQ/OE Mock Exams
- CQA Mock Exams
- CQIA Mock Exams
- CQPA Mock Exam
- CQT Mock Exam
- CQI Mock Exam
- CSQP Mock Exam
- Design of Experiments (DoE)
- Measurement System Analysis
- Statistics Using R
- Data Visualization with R
- Statistics Using Python
- Data Visualization with Python
- Regression with Minitab
- Logistic Regression
- Data Analysis Using Excel
- The Git Mindset
- Statistics Quiz
- Root Cause Analysis
Kano Analysis
- Lean Management
- QMS Lead Auditor
- Quality Management
- ISO 9001:2015 Transition
- Project Quality Manager
- गुणवत्ता.org
- Summary Sheets
- Practice Tests
- QG Hall of Fame
- Testimonials – ASQ Exams Preparation
Blogs , Customer , Management
- The Servqual Model – The Gap Model of Service Quality
** Unlock Your Full Potential **
For the product quality, Garvin provided eight dimensions of quality .
The Servqual model (also called the gap model) was developed by American authors A. Parasuraman, Valarie A. Zeithaml and Len Berry. In general, the SERVQUAL model identifies the principal dimensions of service quality.
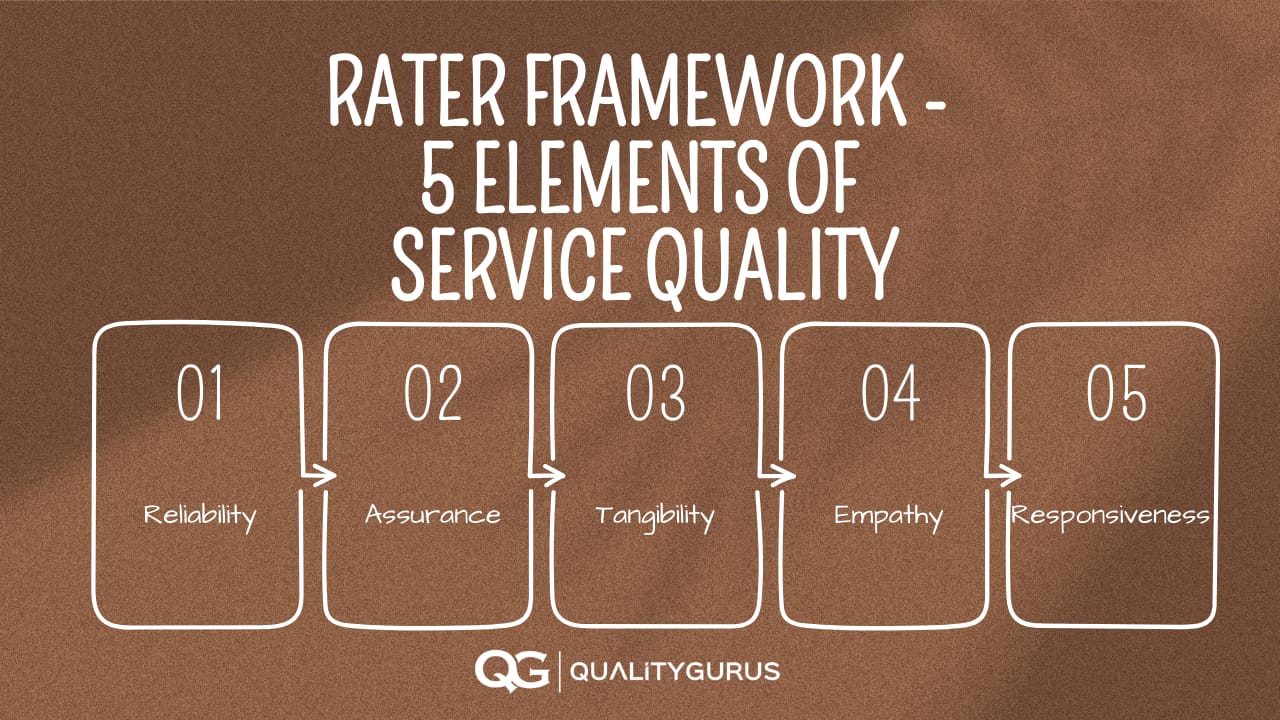
Initially, there were ten dimensions of service quality identified. However, later these were reduced to 5 as some of these dimensions were auto-correlated. These five dimensions of service quality are Reliability , Assurance, Tangibility, Empathy, and Responsiveness.
RATER Framework - Elements of Service Quality
According to the SERVQUAL model, a service provider must be able to provide five critical elements of service: reliability , responsiveness, tangibility, assurance, and empathy.
These five elements can be abbreviated as RATER.
1. Reliability
Reliability means the degree to which a service can be relied upon to produce the desired result or outcome at any given time. This measures the consistency of services provided by an organization. If an organization offers consistent services, then it will have high reliability .
2: Assurance
Assurance means the level of confidence that a customer has about the quality of service.
3: Tangibility
Tangibility means the physical appearance of the product or service provided by the organization. It includes things like cleanliness, neatness, and appearance.
Empathy means the ability of an organization to understand what its customers want and need.
5: Responsiveness
Responsiveness refers to how quickly a service responds to customers' needs.
In general, these five dimensions are considered representative of the dimensions of service quality for different types of services.
- Prioritize customer needs and expectations
- Get this $135 course for just $14.99 today!
- 2+ hours of videos, slides, template & quizzes

SERVQUAL Model: 5 Gaps
In order to provide services, companies must be aware of what their clients expect from them. Therefore, the SERVQUAL model identifies five gaps that can occur between the client's expectations and the services provided by the organization. These include:
Gap 1. Knowledge gap
A gap in the service arises if the organization is not aware of what customer wants. If the organization fails to understand customers' expectations, it will prevent them from serving customers better.
Gap 2. Standards gap
The organization has already formulated its ideas about what kind of services the customer wants. These ideas do not match up with what customers really want. There is, therefore, a high chance that the organization will translate them incorrectly into a quality policy and set of rules.
Gap 3. Delivery gap
Let's assume that the organization has clearly understood what the customer wants (no knowledge gap) and has appropriately formulated the customer's needs into their policies and work processes (no standard gap). Still, there is a possibility that the organization might fail to deliver the service in the planned way. This will be the delivery gap.
Gap 4. Communications gap
To avoid creating false expectations or misleading promises, organizations should ensure that their external communications accurately reflect what they can deliver. Over-promise and under-delivery could raise customer expectations high, and the organization fails to deliver at that standard. This will be the communication gap.
To reduce the risk of communication gaps, organizations should ensure that they communicate clearly about their products or services.
Gap 5. Satisfaction gap
Customers are unhappy because they expect a certain level of service but get something different. Eventually, customers will be dissatisfied with the product or service they receive.
Similar Posts:
December 5, 2021
Strategic Planning and Technology
March 20, 2022
The Basics Of Quality Management: What You Need To Know
March 4, 2023
Employee Failure to Follow Procedures: Going Beyond the Surface

49 Courses on SALE!
Lorem ipsum test link amet consectetur a
- Career Skills
- Change Management
- Communication Skills
- Decision Making
- Human Resources
- Interpersonal Skills
- Personal Development
- Program Management
- Project Management
- Team Management
- Learning Tracks
- Free Productivity Course

By Denis G.
Gap Model of Service Quality
In this article:
Service Gap Model Example
The gap model of service quality.

Gap 1: Knowledge Gap
- Lack of management and customer interaction.
- Lack of communication between service employees and management.
- Insufficient market research.
- Insufficient relationship focus.
- Failure to listen to customer complaints.
Gap 2: The Policy Gap
- Lack of customer service standards.
- Poorly defined service levels.
- Failure to regularly update service level standards.
Gap 3: The Delivery Gap
- Deficiencies in human resources policies.
- Failure to match supply to demand.
- Employee lack of knowledge of the product.
- Lack of cohesive teamwork to deliver the product or service.
Gap 4: The Communication Gap
- Overpromising.
- Viewing external communications as separate to what’s going on internally.
- Insufficient communications between the operations and advertising teams.
Gap 5: The Customer Gap
According to the Gap Model of Service Quality, the only way to close the customer gap is to close the other 4 gaps in the model. The extent to which one or more of these four gaps exist will determine the extent to which customer perceived quality falls short of their expectation.
Using the Model to Address Gaps
Gap 1: the knowledge gap.
- Using customer research.
- Increasing interactions between management and customers.
- Increasing interactions between management and service staff.
- Act on other customer insights you receive once validated.
- Ensure a good proportion of senior management remuneration is aligned to service quality.
- Set, communicate and reinforce quality standards.
- Set measurable service quality goals.
- Train managers to be service quality leaders.
- Update policies regularly.
- Reward staff for the achievement of quality goals.
- Train employees.
- Empower employees.
- Provide the right technology, tools, and equipment.
- Focus on internal marketing .
- Take steps to retain high-performing employees.
- Getting employee input to your advertising campaigns.
- Use reality advertising by using real customers, real reviews, and real employees etc.
- Ensure advertising campaigns are signed off by the operations team.
- Manage customer expectations realistically.
- The Knowledge Gap
- The Policy Gap
- The Delivery Gap
- The Communication Gap
- The Customer Gap
To use the model, companies should measure each gap and take steps to reduce them where necessary.
Cite this article
Minute Tools Content Team, Gap Model of Service Quality, Minute Tools, Mar, 2018 https://expertprogrammanagement.com/2018/03/gap-model-service-quality/

Originally hailing from Dublin, Denis has always been interested in all things business and started EPM in 2009. Before EPM, Denis held a leadership position at Nokia, owned a sports statistics business, and was a member of the PMI's (Project Management Institute’s) Global Executive Council for two years. Denis now spends his days helping others understand complex business topics.
How useful was this post?
Click on a star to rate it!
Average rating 3.3 / 5. Vote count: 3
No votes so far! Be the first to rate this post.
Related Tools
How to create a storybrand.
StoryBrand is a framework to help your business communicate clearly with potential customers, created by Donald Miller, an author, public […]
DRIP Model of Communication
The DRIP model an acronym standing for differentiate, reassure, inform, and persuade. It is also a marketing communications model. The […]
The AIDA Model
The AIDA model is a marketing communications model showing you the cognitive steps prospects take before purchasing your product. It […]
3Cs of Marketing
The 3Cs of Marketing model is a strategic framework to help you win in the marketplace by better satisfying your […]
The 4Ps of Marketing
The 4Ps of Marketing, also known as the marketing mix, is a tool that can help you offer the right […]
STP Marketing Model
STP Marketing Model (Segmenting, Targeting, Positioning) is a framework that simplifies the process of market segmentation. Your marketing will be […]
Three Product Levels (Kotler)
The Three Product Levels model by Philip Kotler provides a way to understand the different levels of need a customer […]
Services Marketing Triangle
The Services Marketing Triangle (or Services Triangle) shows the key actors involved in marketing a service business. It also shows […]
Services Marketing Mix: The 7 P’s of Marketing
The Services Marketing Mix consists of a set of tactics that a company can use to promote and encourage potential […]
Difference between Sales and Marketing
What’s the difference between sales and marketing? Isn’t it the case that if you’re marketing to someone your selling? If […]

In our course you will learn how to:
This 5-week course will teach you everything you need to know to set up and then scale a small, part-time business that will be profitable regardless of what’s happening in the economy.
So if you’ve always wanted to be your own boss and have the flexibility and freedom that entails, then…
Do your future self a favor and check out our course designed to help you achieve exactly that.

Academia.edu no longer supports Internet Explorer.
To browse Academia.edu and the wider internet faster and more securely, please take a few seconds to upgrade your browser .
Enter the email address you signed up with and we'll email you a reset link.
- We're Hiring!
- Help Center

analysis of Gap Model of Service quality

Service marketing Gap model Analysis
Related Papers
Service Science: Research and Innovations in the Service Economy
Mary Bitner , Valarie Zeithaml
Wiley International Encyclopedia of Marketing
Valarie Zeithaml
Exploring Manager’s Perspective of Service Quality Strategies in Malaysian Banking Industry
BC Chew , Lay Hong Tan
In service industry, the subject of service quality remains crucial as business strive to maintain a comparative advantage in the marketplace. In aftermath of globalization, the operating environment for banking industry has become more dynamic and competitive. Banks have evolved to become diversified financial providers instead of traditional banking-only service providers. With bank placing emphasis on a mutually beneficial bank–customer relationship, customer loyalty must be pursued through repeat purchases. Central to achieving this is often the quality of services offered by the bank should satisfy the customer’s needs. This article attempts to identify any service gaps in Malaysian banking industry and to recommend effective strategies to close these service gaps from bank mangers’ and executives perspectives based on GAPs Model of Service Quality (GAPs Model). Using qualitative data collected from interviews with 30 bank managers and executives, this article provides effectives strategies to close each of the gaps in GAPs Model. It is hoped that the empirical evidences and recommendations provided in this article shed some light to management of banks to improve upon their customer service quality in order to benefit from customer satisfaction, customer loyalty and other behavioural outcomes which will lead to greater competitive advantage and profitability to the banks concerned.
Service Quality Audit Based on Conceptual Gaps Model of Service Quality: A Case Study of Top Three Largest Local Bank in Malaysia
Syaiful Rizal Hamid , BC Chew , Lay Hong Tan
Parasuraman et al. (1985) developed a conceptual framework referred to as the gaps model. The primary objective of this model is that the service quality drawback is a result of a series of shortfall within the service organisations. Thus, improving the quality of service experienced by customers (gap 5) requires diagnosing the causes and correcting the internal deficiencies (gap 1–4). A service quality audit was conducted for top three largest banks in Malaysia namely: MayBank, CIMB Bank, and Public Bank based on the conceptual gaps model of service quality and to identify the effective strategies suggested by bank managers for implementation to reduce the provider gap (gaps 1-4). This paper made several suggestions for improving service quality in Malaysian banking industry. Nevertheless, these implications are going to be effective as long as all staff and management act along service quality improvement. Tan, L. H., Hamid, S. R. and Chew, B. C. 2016. Service Quality Audit Based on Conceptual Gaps Model of Service Quality: A Case Study of Top Three Largest Local Bank in Malaysia. International Journal Productivity and Quality Management vol. 18, no. 1, pp.99-115
Rodrigo Mello
Female participation in international assignments was the subject of this study. The literature regarding women in management has emphasized stereo-typing, discrimination and prejudice. Despite the advantageous female personalities and the world’s claim for diversity, the growth of female participation in international assignments has been undermined and the number of men as international assignees was nearly three times higher than women in 2013. This study verified the feasibility of applying a model from the service marketing literature, the SERVQUAL framework, into HR as a tool to implement an international assignment recruitment process in order to diminish the incidence of gender bias, and as a guideline to design and/or adjust expatriation policies. A qualitative survey was conducted by means of face-to-face interviews with ten expatriate women employed by two different German companies, both of the chemical sector in order to identify possible consequences of gender bias in the expatriation context. The application of the SERVQUAL framework to improve the service quality perception toward HR was demonstrated while the HR department was positioned as an internal service provider and the most relevant service quality dimensions were identified by the survey, revealing the service GAPs present in the expatriation process. Due to the fact there were no recruitment processes to be assessed by interviewees, gender bias was not perceived upon selection, but within expatriation. Yet, cultural and gender biases were recognized and identified as negative aspects present in multinational firms.
Cengiz Haksever
Delivering quality is as critical to survival of small service firms as it is to large corporations. Zeithaml, Parasuraman, and Berry (1990) developed a conceptual model of service quality (Gaps) that identified gaps in service quality and suggested measures to close them. The Gaps model has been used in large service corporations, but is yet to be applied to small service firms. Therefore, this paper examines the applicability of the Gaps model to the smaller service firm. Our analysis revealed that the resources and structure of smaller firms significantly affect the types of service quality gaps that occur and the closure measures.
Eric Johnson , Kenton Walker
Journal of Software Maintenance: Research and Practice
Hans van Vliet
Kimmy Nguyễn
RELATED PAPERS
Andrea Wolak
Pertanika Journal of Social Sciences & Humanities
Md Zabid Abdul Rashid
Indus Foundation International Journals UGC Approved
Business and Economic Research
obinna christian ojiaku
International Journal of Quality and Service Sciences
Moshe Davidow
Akaka Otemba
ebenezer antwi
Tgk Vasista
Paul Mugassa
Ahmad Imran
IOSR Journals publish within 3 days
Azimuddin Bahari
Thontteh Esther
David Arumainayagam
Dr. Kofi Agyekum , Sheila Akakpo
Yonatan Gebre
Disaster Mugondi
Emmanuel Baffour-Awuah
IAEME Publications
IAEME Publication
Promise Chika Oparah
SSRN Electronic Journal
nayanananda nilwala
ALEMAYEHU KEBEDE
International Journal of Advanced Research (IJAR)
IJAR Indexing
NELSON MANDELA UNIVERSITY
Dr Dr Motsamai John Modise MJ
Mhd.Rizky Zein
RELATED TOPICS
- We're Hiring!
- Help Center
- Find new research papers in:
- Health Sciences
- Earth Sciences
- Cognitive Science
- Mathematics
- Computer Science
- Academia ©2024
- Open access
- Published: 13 May 2024
Bridging the gap between research evidence and its implementation in public health practice: case studies of embedded research model
- Abisope Akintola 1 , 3 ,
- Dorothy Newbury-Birch 2 &
- Stephanie Kilinc 2
BMC Public Health volume 24 , Article number: 1299 ( 2024 ) Cite this article
27 Accesses
Metrics details
To investigate the potential of embedded research in bridging the gap between research evidence and its implementation in public health practice.
Using a case study methodology, semi-structured interviews were conducted with 4 embedded researchers, 9 public health practitioners, and 4 other stakeholders (2 teachers and 2 students) across four case study sites. Sites and individuals were purposively selected. Sites included two local authorities, one secondary school, and one sports organisation. Thematic data analysis was adopted to analyse the qualitative data.
Four themes were identified: (1) building and maintaining relationships, (2) working with stakeholders, (3) informing practice, and (4) critical reflection.
Conclusions
Embedded researchers build and maintain relationships with practitioners and other stakeholders to produce research. Evidence from the co-produced research informs future practice and research to improve service and delivery rendered to the public. Thus, embedded researchers use their role to bridge the research evidence - implementation gap in public health practice.
Peer Review reports
Implementation science is widely recognised as a study of methods to adopt and utilise evidence-based interventions in specific locations or settings to improve the health of the population [ 1 ]. However, the gap between research evidence and its implementation in public health practice is still globally recognised [ 2 ]. According to scholars, some of the factors associated with the problem of inadequate implementation of research evidence in practice could either originate from the researchers or the practitioners [ 3 , 4 , 5 ]. This implies that both researchers and practitioners could be responsible for the creation of the gap between research evidence and its implementation in public health practice.
Evidence suggests that lack of access to research evidence is one of the barriers to the implementation of research evidence in practice [ 6 , 7 , 8 ]. One report suggests that increased connectivity between researchers and practitioners would enhance the practitioners’ accessibility to research evidence [ 9 ]. The report explained further that creating some forums where practitioners and researchers could interact would not only bring about easy access to relevant research evidence, but also would serve as a means to share learning, and link researchers and practitioners who have a common interest. Similarly, other scholars report that increasing the interaction between researchers and practitioners among other factors could facilitate the use of research-based evidence in practice [ 10 , 11 ]. To that end, there is a need to increase the opportunities for practitioners and researchers to interact in order to facilitate the utilisation of research evidence in public health practice.
As there are many identified barriers to the use of research evidence in practice, the disparity between the context and the language by which researchers and practitioners operate has also been identified as one of the barriers. The incompatibility in the language spoken by the researchers with respect to the scientific methods and the evidence generated could be ambiguous for practitioners [ 12 ]. Therefore, to overcome this challenge, scholars advise that practitioners and researchers should work collaboratively from the onset of the research while putting into consideration each other’s differences [ 13 , 14 ]. Furthermore, it has been recommended that researchers need to present their research findings and explain the relevance to solving practical problems to the practitioners in a simple language without ambiguity [ 15 ]. This suggests a need for an approach that would involve practitioners and researchers undertaking the research agenda together, and also a need for effectively communicating research findings and their relevance in a simple language to the practitioners.
The context in which the researchers operate could also serve as a challenge to the utilisation of research evidence in practice [ 9 ]. As such, competing pressures such as teaching commitments and publishing academic papers [ 16 ] could pose a challenge to the researchers’ involvement in practical problems that could inform their research questions. Hence, there is a need for an approach for researchers to be more involved in practical problems to facilitate the conduction of research that is relevant and applicable to problem solving. It was noted that not all researchers have the relevant skills to conduct co-produced research [ 17 ]. There is a need to create opportunities for researchers who have relevant skills to co-produce research, to conduct research with suitable practitioners.
On the other hand, organisational factors such as time constraints are contributing factors to the gap between research evidence and practice as most practitioners do not have the skills nor the time needed to implement research outcomes in practice [ 18 ]. To tackle these challenges, some studies recommend continuous training and commitment to quality health delivery on the part of practitioners. They also recommended advancements in technological decision support systems as instruments to combat barriers between research evidence and practice [ 19 , 20 ]. There is an argument that achieving these may be difficult as a result of inadequate funds in health services [ 21 ]. Hence, there is a need for the adoption of a method that will bring about building the capacity of the practitioners towards conducting research that is achievable based on the available budget.
Furthermore, the disparity of influence and power between academics and practitioners could be responsible for the wide gap between research and practice [ 22 ]. This means the relationship between academic researchers and practitioners plays a vital role in the use of research evidence. Therefore, there is a need for a method that would enhance or build mutually beneficial relationships between academic researchers and practitioners to bridge the ‘research evidence-implementation’ gap.
The separation of the development of research evidence from the places it is to be used contributes to the challenges of using research evidence in practice [ 23 ]. This implies that the creation of research knowledge where it is to be utilised could bridge the ‘research evidence-implementation’ gap. As such, co-production has been recommended by scholars to bridge the ‘research evidence-implementation’ gap as co-production involves the collaborative working between the researchers and the practitioners [ 24 ]. Hence, the adoption of co-production to produce public health knowledge by researchers, practitioners, and other stakeholders in non-clinical settings [ 13 , 25 ]. This is essential in tackling the challenges of inadequate implementation of research evidence in public health settings.
Being involved in co-production could result in reputational risk for the researcher involved as the researcher could be used by politicians to enhance authenticity to their political stand [ 26 ]. Thus, being viewed to approve such a political stand can limit the researcher’s ability to work only with a certain political group – this can also impact the researcher’s personal safety [ 27 ]. Also, this can impact negatively on the credibility of the co-production findings as it might be viewed as biased and not a true representation but a narrative to back up a political viewpoint, thus generating “policy-based evidence” [ 28 ] rather than “research-based evidence”. On the other hand, policy-makers might be at risk of sharing sensitive information while participating in co-production work [ 29 ] such as disclosing political errors.
Also, co-production can be costly as it usually involves the stakeholders travelling to the co-production site. This could be viewed as challenging for those that are involved in the co-production project, as their presence at meetings for the co-production work is seen as crucial. Also, funding and sustainability of co-production can pose a great risk to the adoption of co-production [ 48 ]. However, the challenges associated with co-production can be overcome if stakeholders are involved and are carried along at every stage of co-production, from design to implementation [ 30 ]. The success of co-production depends on but is not limited to the following: the individuals involved; how clear the aims and objectives of the project are to all those involved, and how duties are allocated [ 31 ]. This also suggests a need to critically analyse the role of stakeholders involved in co-production to overcome the challenges associated with co-production, to achieve success.
Embedded research, also known as ‘researcher-in-residence’, is becoming popular as a type of co-production research [ 3 ]. Different authors used different terminologies for embedded researchers such as insider researcher [ 32 ], knowledge broker [ 33 , 34 ], or scholar-practitioner [ 35 ]. Within an embedded research model, one of the distinguishing features is that the researcher is located in the host organisation as a member of staff to carry out a research agenda with the host organisation’s staff, and at the same time maintaining affiliation with an academic institution [ 36 , 37 , 38 , 39 ]. In this paper we investigate how an embedded research model can help bridge the gap between research evidence and its implementation in public health practice.
We conducted qualitative case studies and drew data from semi-structured interviews with four embedded researchers, nine public health practitioners, and four other stakeholders (two teachers and two students) across four case study sites including two local authorities (Sites one and two), one secondary school (Site three), and one sports organisation (Site four) in the Northeast of England.
One of the advantages of qualitative research is the ability to generate rich in-depth data or knowledge that can serve as a basis for health and social practices being effective and relevant to the contexts they are applied to [ 40 ]. We adopted a qualitative multi-site case study to understand the context by providing in-depth description and analysis within sites and as well by comparing data between sites in order to identify the similarities and differences between the sites explored [ 41 ]. Thus, this will assist to maximise the applicability of the findings on how an embedded research model can help bridge the gap between research evidence and its implementation in other similar settings.
In site one, the embedded research project aimed to understand and make recommendations regarding population changes, and service needs, including health, education, housing, and social care, in the local communities. In site two, an embedded researcher works at the local authority to provide research support to the local authority’s public health team to secure their targets which include commissioning evidence-based services and interventions, and promotion of healthy lifestyles. Site three conducted an embedded research project to explore the academic and health impact of the recent changes to the General Certificate of Secondary Education (GCSE) system on both staff and students. Site four was established to encourage more people to engage in physical activities to improve their health and well-being. In order to improve the service rendered to the public, an embedded researcher was employed in site four to co-produce research with the sports organisation members of staff. All the embedded researchers across the four case study sites were PhD holders. The amount of time spent in their respective host organisations varied from one hour per fortnight to two and a half days a week to suit the embedded researchers and the host organisations. The embedded researchers’ positions were funded either by the University they are affiliated with, or their host organisation.
Purposive snowball sampling was used in this study. Requests for participants and sites who could volunteer to be part of the study were sent out via relevant professional contacts and networks. The participants and sites that volunteered to take part in this research were asked to assist in the search for participants and/or sites by circulating the study’s details to those who might meet the study’s criteria and would be willing to take part in the study. The inclusion criteria were: (1) being a public health embedded researcher, and (2) being a public health practitioner or stakeholder who is working or has worked with a public health embedded researcher. Potential participants were assessed for eligibility before being interviewed. A total of 17 participants were recruited for the interviews across the four case study sites. The sample size would have been larger than 17 but for the Covid-19 pandemic. Ethical approval was obtained from the Teesside University School of Health and Life Sciences Research Governance and Ethics Committee in November 2019. Data was collected between November 2019 and April 2020.
To facilitate participation, participants were offered alternative modes of interview for their convenience: face-to-face, telephone, and Skype-based interviews. The Covid-19 pandemic occurred during the interview period, but most interviews conducted before COVID-19 were face-to-face. All interviews conducted during the pandemic (March 2020 and onwards) were either Skype or telephone-based, as advised by the Ethics department at Teesside University and as per the requirements of the interviewees’ workplaces. Before each interview, oral and written informed consent was obtained from each participant. Each participant was asked to complete two copies of the consent form, one for their own records and one for the researcher.
Following each interview, a reflective note was taken to identify what went well and what could be done differently in the next interview. Since there were three categories of interview participants – embedded researchers (ERs), public health practitioners (PHPs), and other stakeholders (students (STs) and teachers (TRs)–three sets of interviews were prepared. Although the interview questions were nearly the same for each category of participants, some of the interview questions differed in the way they were structured. Here is an example of how a question was worded differently depending on the participant: (ERs) Can you cite an example where you have built practitioners and other stakeholders’ confidence to conduct their own research? (PHPs, TRs, and STs) Can you cite an example where an embedded researcher has built your confidence to conduct your own research? A full outline of the interview guide is in Appendix .
A summary of each interview was noted in a research diary for reference. Details noted included where each interview took place, the date of the interview, the length of the interview and how the interviewee responded to questions. Each interview lasted between 40 and 90 min. The interviews were recorded, and data was transcribed. We analysed data using inductive thematic analysis [ 42 ] to allow new themes besides the preconceived ones to emerge from the coding of the interviews. Trustworthiness of the analysis was assessed by triangulating between data sources.
Four themes emerged from the analysis of the interview data on the potential of embedded research in bridging the gap between research evidence and its implementation in public health practice: (1) building and maintaining relationships (2) working with stakeholders, (3) informing practice, and (4) critical reflection.
Building and maintaining relationships
All participants across the four case study sites, irrespective of their age, years of experience, or education, recounted the significance of this theme to the embedded research projects in their respective sites. They articulated the benefits of the role of the embedded researchers in building and maintaining relationships with the public health practitioners and other stakeholders to facilitate the co-production of research evidence. They all agreed that building and maintaining relationships played a vital role in the utilisation of the co-produced research evidence and in the closing of the gap between research evidence and its implementation. Overall, the strategies adopted by the embedded researchers to achieve this theme were identified as: (1) building internal/external relationships and sharing skills, and 2) maintaining regular contact with practitioners and other stakeholders.
Building internal/external relationships and sharing skills
Participants agreed that the embedded researchers’ role entails having diverse connections built on good relationships. These relationships assist the embedded researchers in connecting their partners to other relevant organisations such as academic institutions and third sector agencies.
“I think some of that is around having this kind of good grounding so sort of beginning the role with already having made, a lot of kind of contacts, a lot of sort of good relationships been built. [..] I have a line manager in the council, who was the project manager for the first phase so we’ve got that continuity there [..] I also have an academic supervisor who is also my kind of my line manager from the academic side” [ERsite1] .
“I can say that’s [having connections] actually key because they are straddling both worlds. [..] not somebody who sat in the academic institution who didn’t understand the wider context. I think these roles are really key in bridging the institutions” [PHP2site1] .
It was clear that building relationships and connecting the ‘two worlds’ is not only advantageous to both institutions but also assisted the embedded researchers to seek support from both their academic supervisor at the University they were employed and the local authority (LA) they are working with. Therefore, this enables the embedded researchers to be supported fully to carry out their role successfully. It was also recognised that while embedded researchers play their role in building relationships and connecting relevant organisations, the role assisted them to understand the context in which research evidence is to be utilised. Thus, the relevance of research evidence to the host organisation facilitates its use.
This relationship-building was seen as crucial to the success of the role, and it was felt that these relationships could determine the success of any work carried out.
“[..] I would go as far to say I think it’s the relationship that’s built with the individuals who developed that project was important. [..] are the most important elements of co-production” [ERsite2] .
This implies that lack of relationship-building between researchers and public health practitioners can serve as a barrier to embedded research project. Furthermore, it was evident that the relationship built with the stakeholders who were involved in the embedded research was crucial to the projects. For instance, an embedded researcher from site two used her skills to build relationships with the volunteers that participated in the project.
“She [embedded researcher] has been there longer, excellent relationships with the volunteers, that helped to build and shape this project, so she has a very useful experience in terms of relationship-building” [PHP6site2] .
Thus, this assisted in structuring the work which had a positive impact on the project. This two-way relationship with other organisations, including the local universities and research participants, was seen as a benefit of embedded research.
Findings showed that embedded researchers used their contacts and good relationships to facilitate the sharing of skills useful in carrying out embedded research projects and also enable working with other academics at the University.
“[..] even for me just working as an individual in that organisation, I don’t know everything about the research, but because you are linked with the University, that gives an avenue to ask questions and link up with people with expertise to then support an evaluation” [ERsite2] .
These connections and relationships, therefore, enable the sharing of skills useful to co-produce relevant high-quality research evidence useful to host organisations and policy makers.
Within this current study, it was clear that if the embedded researchers were not located or had spent time in the sites, they felt it would be difficult for them to build relationships, and understand the context in which the co-produced research is to be utilised.
“So, having the researcher embedded within in what we do, the researcher has the understanding of the project, and initially she has been with it from the start to finish, so she understands the journey that’s been on, and she understands why it’s been done, how it’s been done [..] So, I think, so the embedded researcher role in what we do is infallible resource really” [ PHP1site4 ] .
The ‘embeddedness’ gave the researchers an understanding of the projects they were involved in. As such, the embedded researchers were seen as ‘insiders’ and their ‘embeddedness’ was seen as key to the success of the work.
It is worth noting that the amount of time spent by the embedded researchers in their respective host organisation varied and was negotiated at the sites to suit the embedded researchers and the host organisations.
“[..] I was familiar with quite a lot of people but obviously kind of being there regularly I have got to know them much better basically. [..] I mean it really varies; I would say probably kind of at least a couple of days in a week” [ERsite1] .
“Being embedded within their team I spend half of the week working within the organisation. It’s been a real pleasure to work alongside them” [ERsite2] .
“ So, we tend to have meetings where I will go in for a few hours at a time. I would probably say, maybe an hour in a fortnight ” [ERsite3] .
“[..] I spend two and a half days working within the organisation. [..] you want to be seen as part of that team and not somebody who just pops up every now and again” [ERsite4] .
However, building relationships and sharing skills was not seen as without its challenges with some tension between roles and expectations.
“[..] it has become trickier splitting myself now between the organisations as they all have their roles and expectations on how they want things to be done” [ ERsite2] .
“The structure can be quite challenging as well, but probably [..] just having that balance in the relationships with the organisation you are working for and the organisation you are evaluating for. And I think yeah you have got to have that one, but that is a challenge of working in large organisation” [PHP6site2] .
The embedded researchers from sites one and two found there was some tension in working in both ‘worlds’ as a result of the responsibilities associated with it, such as building relationships, and balancing diverse responsibilities. This is due to their dual affiliation as such, they are expected to manage a large workload, managing both successfully. A practitioner from site two added that the structure of the organisations the embedded researcher works could also be a challenge, therefore, it is important for an embedded researcher to be able to discuss this with both sides in order that they balance the relationships between the host organisation and the academic institution.
Another notable challenge is having to manage diverse expectations including the ability to balance competing interests of the different organisations.
“There is sort of difference in expectations because I think from the academic point of view, [..] we want publications, we want things that give us an academic output, whereas someone who works in the school is not going to be bothered about that sort of things. They have to see where it positively affects their school, [..] so I think having that difference in agendas on what you want to achieve from this school research can be quite hard to manage. [..] you want different things from this piece of research is quite hard, and make sure that both sides are happy at the end of the day, and I think we did that quite well” [ERsite3] .
For instance, an embedded researcher from the school stated that the expectations from the embedded research project did differ. That is, while part of the aim of the academic input was to publish the outcome of the project to improve or boost their academic output, the school aimed for a practical positive impact of the project on the school, such as improvement in students’ engagement in academic activities. Hence, it was essential to balance the competing interests of the school and the academic side of the embedded research project.
Maintaining regular contact with practitioners and other stakeholders
Based on the participants’ experiences, the embedded researchers built relationships with the practitioners and other stakeholders by maintaining regular contact.
“I think what we did was to help build that relationship. It was not just a telephone conversation just to discuss. We actually worked side by side so there was time to actually do that embedded research. We spent time in the office, we spent like one or two days a week” [PHP1site2] .
“Yeah, but then we did send them emails and stuff, in between [..] yeah we did have time outside of the face to face sessions and sending stuff to the teachers to encourage them, ‘can you remind the students that we have got to do this week’, we have got to get this done by then, so I would say obviously we had the face to face sessions but then we had email correspondence as well” [ERsite3] .
The practitioners from site two reported that the embedded researcher maintained regular contact by face to face, or by telephone. They further explained that they worked side by side with the embedded researcher to build relationships. This implies that if the practitioners and the embedded researcher were not chanced to work together, which assisted in maintaining regular contact, it would have been difficult to build relationships. Thus, this widens the gap between academia and practice. The embedded researchers had similar experiences. For instance, an embedded researcher from site three (school) confirmed that she maintained regular contact to build relationships with the students and the teachers by email and face to face. This shows that it is important to develop project strategies in order to maintain regular contact with the practitioners and other stakeholders to build relationships.
According to the embedded researchers, building mutually beneficial relationships was achieved by maintaining regular contact not only with the stakeholders but also with their academic supervisors which enabled the embedded researchers to have the necessary support to achieve their role.
“I mean knowing that I do have kind of the support at the University to draw on and also have a kind of a good working relationship with my line manager in the council as well really. I don’t feel that I am lacking in any kind of support, which is a good kind of place to be in yeah. So I have monthly meetings in the University and that’s very much really useful in times of keeping track of some of the other parts of my roles so around kind of trying to ensure that we can get some like academic publications and things like that so yeah” [ERsite1] .
Another strategy that was mentioned regarding how the embedded researchers maintained regular contact to build relationships with the practitioners and other stakeholders was ‘attending formal meetings’.
“Interestingly, the researcher has always been on the co-production committee and she attends the meetings, so she is excellent, much better than me because she has been there longer, [..] that helped to build and shape this project [..]” [PHP6site2] .
“So, I have to go to all their team meetings that’s gonna help you form a lot of relationships. Meetings are where the real connection starts to happen. So, you have to invest that time ” [ERsite4] .
As well as making use of formal meeting, the embedded researchers adopted ‘informal conversations’ to maintain regular contact to build relationships with the public health practitioners and other stakeholders.
“For me, I am quite like a chatty person and I think that’s like the characteristics of an embedded researcher. You need somebody who is easy to get on with lots of different people. You need to have that ability to do that. Otherwise, you gonna struggle to form a relationship especially if you aren’t there as often as what you would be if it’s a full-time job” [ ERsite4] .
A practitioner from the sports organisation added that engaging in informal conversations also helped in building a trustworthy relationship with the embedded researcher.
“[..] We have that relationship and some other things you can visit, particularly when things get tough, it’s easy enough to fall back on different conversations on sport [..] These conversations increase our relationship and trust, we trust each other” [PHP1site4] .
The practitioner further explained that he has a good relationship with the embedded researcher and so they engage in informal conversations at difficult times thereby developing a relationship that is based on trust.
Working with stakeholders
Results showed that the embedded researchers build and maintain relationships with the practitioners, and with other stakeholders in order to effectively work together to produce research. This, therefore, facilitated the production and the use of the co-produced research evidence at the embedded sites and helped close the gap between research evidence and its implementation as results were shared quickly with all those that were involved. All participants across the four case study sites unanimously agreed that this theme is one of the primary roles of an embedded researcher, and the strategies identified include: (1) co-producing research, and (2) building research capacity.
Co-producing research
The participants confirmed that they worked together to identify, plan, and conduct research intended to help the host organisations improve their services and meet the needs of the communities with which they work.
“We liaise with the researcher to develop the initial kind of overview of that population [..] the researcher supports us in developing the initial questions, the questionnaire, and the initial research” [PHP1site4] .
“[..] embedding research into the public health team. [..] then helping us to explore the questionnaires. The embedded researcher helps us with the development of that work including the formulae and evaluation for the intervention. We design and develop and embed and undertake the research together. She is very much a part of the team and a core within the team” [PHP4site2] .
“[..] So, really it’s about giving us the exposure to that sort of research. Well, honestly, I have learnt how to conduct research” [ST1site3] .
The participants acknowledged that working together to co-produce research with the embedded researchers encouraged adjustments to and engagement with research-related activities. Furthermore, embedded research was considered a cost-effective research approach.
“ I have been out in a couple of beneficiary interviews with the researcher. Certainly, I would not normally get involved with going out to see clients, but I have gone out a couple of times with the researcher, so that was interesting” [PHP5site2] .
“[..] the embedded researcher worked alongside the public health practitioners [..] how to shape some of the evaluations, including how to be really clear about the methodology, the approach [..] And how to write protocol [..] So, I think that was the aim of it, it was to ensure that we have much more effective and cost-effective research ” [PHP2site1] .
One public health practitioner reported that she participated in several research activities with the embedded researcher at site two. She recognised that working with the researcher enabled her to do research work that she would not have ordinarily done. This suggests that not working together with practitioners to co-produce research may potentially prevent practitioners from being meaningfully involved in the research process. In such situations, the gap between the development and implementation of research evidence may actually become wider. One practitioner from site one explained that embedded research was adopted in the LA so that the authority could conduct cost-effective research. This only further indicates that having an embedded researcher on-site working collaboratively with practitioners and stakeholders to conduct cost-effective research can help bridge the research implementation gap.
However, it was noted that the process of co-producing research between the embedded researchers and the public health practitioners and other stakeholders also facilitated shared learning.
“Despite the fact that we went in obviously thinking of teaching them but the fact that we can learn from them about what was important to them, what was important to young pupils in schools, and how to speak to young pupils because that is schooling in itself. [..] and I think also you learn new skills [..] so I think you get sort of practical experience and learn new skills sort of more practical skills I suppose, not just research skills, so yeah that is why I think I say it’s the most important thing” [ERsite3] .
“[..] and when I have been out with staff members, they will ask questions that I would never have thought of asking, because of their knowledge at work. [..] I have been learning a lot as well from the staff, and that shows the importance of doing it together” [ ERsite2] .
One embedded researcher from site three (school) reported that although their aim was to teach the students how to conduct research, they were able to learn what was important to the young people among other things from the students. Another embedded researcher from site two shared a similar experience and confirmed that during the co-production work, the public health practitioners used their tacit knowledge of their field to ask relevant questions that had not occurred to her. Since the practitioners are more knowledgeable than the researcher regarding actual on-site practices, they added substantial value to the project. This indicates just how much learning is a two-way process, and demonstrates co-production of knowledge which involves the amalgamation of the practitioners’ tacit knowledge and the researchers’ explicit knowledge.
Researchers were explicitly recognised for their ability to co-produce research with the public health practitioners and other stakeholders. Thus, the co-produced research was jointly owned by those involved in the embedded research projects. As the research was co-produced with the intention to assist the organisations to improve the service they render to the public, thus, the embedded researchers’ role assisted in facilitating the utilisation of research evidence. In addition, given the embedded research projects focused on meeting the needs of the host organisations, there were no instances where there were conflicts related to the research emerged.
Building research capacity
The embedded researchers explained that they conducted training, and other developmental activities to help develop the practitioners’ and other stakeholders’ research skill-set.
“I have done a kind of number of training sessions with staff and actually with volunteers that will want to get involved in collecting data [..] so I have run workshops, training workshop, so that means that when I go out there for collection the staff can come and do it with me” [ERsite4] .
“[..] another element of my role is to deliver training to staff around the use of data around the benefits of collecting relevant information, how that information can be used to inform practice in decisions and planning and things like that, we just had a conference couple of weeks ago which was very much about kind of sharing the learning and then sort of getting people involved in the work that we do really, so they are my kind of key targets really” [ ERsite1] .
Research-based training were offered by the embedded researchers in a variety of forms, such as using workshop training, one to one training and through seminars and conferences. For instance, an embedded researcher from site four (sports organisation) reported that she taught the practitioners to collect data at a training workshop that she organised. She explained that this training assisted the embedded research project because it helped the practitioners to get involved in the data collection phase as they had the skills from the training. Similarly, another embedded researcher from site one reported that getting the practitioners involved in the embedded research work facilitated the sharing of learning, which was one of her main goals while working at the LA. This particular researcher trained the public health practitioners to collect data and taught them how research evidence can inform practical decision making.
The participants agreed that working together with the embedded researchers strengthened their ability to conduct high-quality research capable of benefiting their respective organisations.
“ It also allowed us to utilise and build the capacity of public health practitioners who would often not undertake any research for some time” [PHP2site1] .
“So, it’s more like continuous professional development [..] So, the research skills are learnt such that at the end of the day, next time the research could be conducted independently, even if we didn’t have somebody coming from the outside. That’s the whole approach [..] is for developing public health practitioners to the extent that research can be conducted in a rigorous manner” [PHP1site1] .
“I think probably when I attended two beneficiary interviews with her and just seeing how to speak to people when you are asking them questions so there is a way to ask the questions so that they understand, probably by listening to the researcher at that point I sort of learnt how” [ PHP5site2] .
As the above suggests, the embedded researchers encouraged some practitioners who would ordinarily not participate in research to engage in research activities. This implies that working together with researchers may be a significant facilitator to building practitioners’ research capacity and closing the research implementation gap. The absence of an embedded researcher may even serve to widen the gap. Indeed, the public health practitioners observed that working with embedded researchers could eventually build their research capacity to independently conduct high-quality research in the future.
Overall, it was clear that the participants were aware of the importance of working together with embedded researchers, and the researchers were acknowledged for their ability to assist greatly with research-related training and support to build their research capacity. It would have been difficult for these organisations to generate high-quality on-site research if the embedded researchers had not been present. Consequently, the embedded researchers helped work to close the research evidence implementation gap.
Informing practice
The embedded researchers built and maintained relationships with the practitioners and other stakeholders to work together with them to co-produce research. The participants from the four case study sites reflected upon how the embedded researchers informed the sites of relevant research-based evidence, which helped in the development of future practice and research. By doing so, the embedded researchers bridged the gap between the discovery and implementation of research-based evidence. The results showed that all participants across all the four case study sites, irrespective of age, years of experience, and education, agreed that the role of the embedded researchers includes this theme.
The strategies adopted by the embedded researchers include: (1) identifying challenges in the host organisations, (2) utilising research experience, (3) implementing research evidence, (4) disseminating findings, identifying future research areas, and applying for funding, (5) presenting and publishing findings.
Identifying challenges in the host organisations
Participants agreed that the research skills of the embedded researchers are essential to the process of identifying the practical challenges facing the research sites. For instance, an embedded researcher used their research skill to unravel the root cause of the challenges facing a school (site three) through a thorough investigation by developing and conducting relevant research with the students and the teachers.
“[…] the GSCE reforms of the time that was taking place, it was causing a significant amount of stress and pressure for the teachers. In the first instance, teachers were having to grasp new skills at work, they were having to understand the new curriculum and subject knowledge. Some of the teachers weren’t particularly strong, there was a level of undue pressure and stress being put on the students, so pupils nationally were having to learn lots of different contents, they were sort of taken away the security blankets of things like modular testing in course work and what that meant was that students will now have to recall so much more knowledge in exam conditions” [TR1site3] .
Following the identification of these challenges, research-based recommendations were offered through the co-production research. By using research evidence to help tackle the school’s challenges, the researcher bridged the gap between the discovery and implementation of research-based evidence.
Utilising research experience
It is worth noting that the embedded researchers used their research experience to inform their host organisations of relevant existing and newly co-produced research evidence. The embedded researchers’ research-related expertise and the time they spent searching for relevant evidence were both seen as useful to the public health practitioners and other stakeholders.
“The beauty is that because it is their bread and butter, doing reviews and searching for evidence […] one of the things the embedded researcher did to help me with it was to do that literature review [..] it would have taken me much longer [..], so that’s the benefit [..] it is their strength and their experience and skills which they have got and which we may not have and the time to do it which we may not also have because we are constantly under the treadmill” [ PHP1site1] .
It was evident that the practitioners’ busy work schedules often restrict their ability to develop and implement their own research skills. Thankfully, the embedded researchers were able to assist the practitioners by using their research skills to overcome research-related challenges, and in the process taught them how to look for research evidence effectively. This, therefore, facilitates the implementation of evidence-based practice. The implication of this is that practitioners’ lack of research skills and time would have served as a barrier for evidence-based practice in the research sites.
It was clear that the research-based evidence searched for, or co-produced by the embedded researchers and the public health practitioners including other stakeholders was used to inform practice and make positive changes. Evidence showed that the embedded researchers had informed the host organisations of relevant research evidence and had used their research experience and skills to make research-based recommendations. In other words, the embedded researchers made valuable research evidence, and knowledge accessible. As such, this brought about desirable changes that improved service and delivery in the research sites.
“ So the way this works here is that you do the final report which has the recommendations in form of what we feel there should be changes to in practice, and that goes to their public management team and then they will look at that” [ERsite2] .
Furthermore, the embedded researchers also discussed how they helped make positive on-site changes occur. For instance, an embedded researcher from site two reported that positive changes were made in practice after developing recommendations in the form of a report submitted for management’s approval. It was clear that the practitioners take evidence-based advice from the embedded researcher to improve the quality of the services being offered to the public. Thus, this closes the gap between research evidence and its implementation.
Implementing research evidence
The interviews inquired as to how research-based evidence was translated into practice at the four research sites. As the interview process continued, it became clear that desired changes and improvements were achieved through the on-site application of research-based evidence. The results showed that across the four research sites, this process did indeed happen.
“[..] as it is very much about kind of being a resource to implement the recommendations and embed kind of the key findings from the research, again my role is trying to get some of these things into practice really so its embedded research but the main one of the main things is around embedding the recommendations as well, so that’s sort of work my role is around doing” [ ERsite1] .
“ [..] at the same time, it also helps the researcher coming in to understand what goes on in practice so that you don’t just go and conduct a piece of research that goes on the shelves. [..] So we would then need to weigh the evidence and the circumstances under which we are going to implement an intervention but we still take advice from the researcher on the evidence of what works. They could advice on what works [..] It’s more about the outcome of research being used to influence practice for quality improvement” [ PHP1site1] “There are changes that are made with how they recruit their staff for the delivery staff […] that changes were made and that was in practice, and they also kind of put it in a set of recommendations as to the ones to be delivered in schools” [ERsite4] .
Participants reported that the embedded researchers recommended existing research evidence, co-produced research evidence with the intent of informing practice, and also used relevant evidence to help improve service and delivery. In other words, the role of embedded researchers provided accessibility to research-based evidence that was utilised to develop solutions to on-site challenges and create positive change.
Disseminating findings, identifying future research areas, and applying for funding
The embedded researchers reported that having to present reports to diverse audiences prompted them to produce easily understandable, user-friendly reports that did not rely heavily on academic language.
“[..] so I have quarterly reports that I have to produce which has to be user-friendly and appeal to a various range of agencies within the organisation [..] we had, basically we have had quite a few different presentations to different kind of groups or the senior management team and departmental teams and things which was about and sharing the results and recommendations, we have follow-ups sort of things from that” [ ERsite1] .
“[..] Yeah, just into writing report so she will do like verbal update or she provides like some blueprints in an email ” [PHP5site2] .
The reports created by the embedded researchers avoided scientific terms that might be difficult for public health practitioners and other stakeholders to understand. Furthermore, practitioners and other stakeholders were informed of relevant research evidence in an unambiguous way. It is important to add that it would have been difficult for the embedded researchers to appropriately simplify their language if they had not had the opportunity to spend time on-site becoming familiar with the language used by the practitioners and stakeholders.
The participants also reported that the embedded research projects effectively discovered potential areas for future research. By making suggestions regarding future research, the embedded researchers furthered each host organisation’s potential to engage in relevant, change-creating research.
“[..] then the research outcomes were used to inform the next phase, so obviously that was the first phase, which we felt was really successful and worked really well, so then we took those sort of the things we learnt to the next phase” [ERsite3] .
For example, an embedded researcher from site three (school) stated that the first phase of their embedded research project was such a success that the findings of the first phase informed the direction of the second phase, thereby ensuring continuous research activities in the school.
Furthermore, participants agreed that the outcomes of the embedded research projects assisted with the application for future funding.
“[..] the results of the work that we did has been kind of used in terms of future funding opportunities, for providing data, providing kind of context information that was used in sort of proposals and in bids pushing and for applying for future funding” [ERsite1] .
It was evident that the presence of the embedded researchers in their host organisations encouraged the push to apply for funding to develop projects. This, therefore, facilitates continuous engagement in research activities. The practitioners felt that the role of the embedded researchers is crucial to producing funding applications and program development.
Presenting and publishing findings
Once embedded researchers succeeded at co-producing relevant on-site research evidence with practitioners and other stakeholders, and offering practical solutions to on-site challenges, it became clear that it would be necessary to present and publish the outcomes of the projects. Consequently, embedded researchers used their academic skills to publish the findings with practitioners and other stakeholders as co-authors. One of the benefits of publication is that published research can inform the host organisation, and other organisations facing similar challenges. Another significance of the role of embedded research pertaining to this, is that as the embedded research project is co-produced by both the embedded researcher and the host organisation, the findings from the research are jointly owned by both parties. This also assisted in integrating research into the host organisations culture.
“We wrote a book chapter with their names on the published book chapter. We got all of them involved with the writing of the chapter [..] that makes a sort of massive difference ” [ERsite3] .
“We co-authored a chapter of a book. We used the findings to create a book chapter but all of us has input into it including the researchers” [ST2site3] .
For example, participants from site three (school) reported that a book chapter based on co-produced research that they had worked on with the embedded researcher had been published [ 43 ]. Co-produced and co-published research evidence informs the school and research community of the institutional value of embedded research projects. The embedded researcher from site three (school) added that the names of the students and staff involved in the research and writing processes were included in the book chapter. The book chapter was co-edited by both an academic and a public health consultant. This publication has made a tremendous positive difference to how a school labelled as ‘deprived’ views itself. Indeed, being involved in the co-production of valuable research has encouraged both students and teachers.
To further explore how embedded researchers can inform public health practice, the participants were asked whether any other evidence-sharing processes had been used by the embedded researchers. The embedded researchers in this study were connected to more than one organisation. Consequently, they have access to organisations with information that can benefit public health practitioners and other stakeholders. The participants felt that participating in other organisations helped the embedded researchers fulfil their role as the discoverers and sharers of information. The participants viewed this role of the embedded researcher in their sites important as it informs them of the latest research evidence and activities in the field. This could also be seen as a way to sustain evidence-based practice in the sites. As the practitioners are regularly informed of the latest relevant evidence by attending research-based programmes, it facilitates the integration of research into the host organisations’ culture.
“When I see opportunities for conferences or local events, I will send an email or circulating them, there might be public health conference, it might be a Fuse conference that’s linked in erm linked in heavily with the thing we have worked on and I circulate that to the staff member, to say here is an opportunity” [ERsite2] .
For instance, an embedded researcher from site two stated that she regularly informed the practitioners of programmes and events presenting research relevant to their practice. By attending such events, practitioners can stay informed and up to date and are more likely to make changes to their practice based on timely research evidence. Consequently, the findings of this study indicate that staying familiar with the latest relevant research is one of the ways to close the gap between the discovery and implementation of research-based evidence.
Overall, it was evident that the embedded researchers’ ability to inform the organisations with relevant co-produced research evidence, and the ability to identify relevant information and opportunities and then circulate these to public health practitioners and stakeholders helped to inform the sites in creating relevant, research-based changes to benefit their public health practices. The positive outcomes they generated indicate that the role of embedded researchers can seriously contribute to closing the gap between the discovery and implementation of research-based evidence in the research sites.
Critical reflection
Twelve out of seventeen participants across the four sites discussed this theme as part of the role of the embedded researcher in their respective organisations. Participants felt that critical reflection was an important process an embedded researcher must engage in throughout the ‘journey’ of becoming an agent of closing the gap between research evidence and its implementation in practice. The identified strategy adopted by the embedded researchers within this theme is continuous reflection.
“I constantly reflect on my role to know what I am doing right, and what can be done differently” [ERsite1] .
“I have to spend really more time reflecting” [ERsite2] .
“It might be while you drive home [..] might be in the shower [..] might be when I take the dog out for a walk and tea time to reflect because you do need time to reflect on your research, on your methodology [..] about what the findings need to show [..] at times my bag is full of paper everywhere, millions of notes in here and I have to open and jot down some questions so that I won’t forget them because they are so important” [ERsite4] .
“I think it’s always good to sort of like reflect on what we have done, how we do things I personally want to think about whether I could have done things better […] so I think it’s quite important to sort of reflect on how you have done things, and how you could do things in the future, like what lessons you have learnt, I think it’s important to sort of reflect, to sort of think more about how you have done things and whether it could be practiced in the future” [ERsite3] .
Overall, the participants agreed that reflection helps embedded researchers assess their roles and constantly improve their work. Therefore, reflection is crucial to successfully co-producing research and closing the research implementation gap.
All participants, irrespective of their age, working experience and education, acknowledged that the relationships between the people involved in an embedded research project are crucial to the project’s success. This is in keeping with those made in previous studies that have concluded that building and maintaining mutually beneficial relationships with practitioners and other stakeholders significantly helps embedded researchers co-produce public health knowledge in non-clinical settings [ 33 , 44 ]. The study participants were also unanimous in their view that the ‘embeddedness’ of the researchers, or the degree to which they become part of or spend time within the host organisation, is significant. A higher degree of embeddedness appears to lead to the development of beneficial relationships and also helps researchers develop a better understanding of organisational contexts, that in turn leads to the development of effective solutions and useful, co-produced research. Notably, becoming embedded to a significant degree helps others see the researchers as part of the team. Previous studies have also indicated it is the duty of the embedded researcher to become part of the host organisation by working collaboratively with practitioners and other stakeholders [ 17 , 45 ].
Although the amount of time each embedded researcher spent within their host organisation varied, the interview data gathered from all sites confirmed that embedded researchers felt they were able to develop meaningful relationships with the host organisation. The National Institute for Health Research (NIHR) embedded research team reported similar findings and observed that the amount of time spent within an organisation can depend on the intensity of a project [ 46 ].
Among other strategies, informal conversations with the practitioners and other stakeholders also assisted the embedded researchers to build relationships. This was confirmed only by the embedded researchers in case study sites two and four who had worked in the host organisations for more than three years. This might be because the embedded researchers from the local authority (site two) and the sports organisation (site four) had worked and familiarised themselves with the members of the host organisation staff. Consequently, this could have facilitated easier informal conversations, unlike the embedded researcher in site one who has just spent seven months in the site. This confirms that it takes time for embedded researchers to build trustworthy relationships in the host organisation and they recommend an ‘introductory period’ of a minimum of three months for familiarisation before an embedded research project starts [ 39 ]. This was beneficial to the three case studies explored in an earlier study as it allowed the embedded researchers to familiarise themselves with their host organisations and as well build relationships with the host organisations’ staff [ 39 ]. This also aligns with the view of other scholars that an ‘introductory period’ is important before the commencement of an embedded research project [ 44 ]. It is worth noting that the practicability of an ‘introductory period’ may depend on the agreement between the parties involved.
Furthermore, embedded researchers must build relationships not only with practitioners and other stakeholders, but also with their academic supervisors. Having a successful relationship with the academic supervisor can help the embedded researcher overcome the challenges that arise as a consequence of having a dual affiliation and needing to manage diverse expectations and competing interests. The embedded researchers interviewed in this study had the support of their academic supervisors. Thanks to the vast experience of their supervisors, they are often excellent at mitigating unforeseen challenges. Indeed, among other factors, the success of an embedded researcher depends on the relationship between the researcher and his or her academic supervisor [ 13 , 39 ].
The interview participants recounted that it is important to work together to co-produce relevant research which is useful to the organisations. Other scholars have similarly concluded that embedded researchers work with members of their host organisations to identify, plan, and conduct research that will meet the needs of the organisation [ 36 ]. By working collaboratively, embedded researchers were able to train the practitioners and other stakeholders and improve their ability to help co-produce meaningful and valuable research that can be used to implement evidence-based adjustments to on-site practices.
The findings of this study indicate that working together produces meaningful research and also teaches practitioners and other stakeholders who assist embedded researchers, how to conduct research. Similarly, an earlier study concluded that embedded researchers encourage practitioners and other stakeholders to participate in research activities and increase an organisation’s capacity to conduct research [ 17 ]. In other words, the collaborative work that accompanies embedded research helps close the research implementation gap. However, it was noted in this current qualitative inquiry that having the right researchers assisted in carrying out the projects successfully. This is similar to an earlier study that argue that having the right combination of researchers and practitioners in co-production is crucial to the success of such project [ 13 ]. Also, other scholars pointed out that not all researchers have the relevant skills to conduct co-produced research [ 17 ]. Therefore, it is essential to have the right combination of researchers, practitioners, and other stakeholders while working together to co-produce research to ensure its success.
Based on the current qualitative inquiry, the role of the embedded researchers includes informing practice by making recommendations and positive changes that utilise both existing and newly co-produced research evidence. Doing so makes research evidence more accessible to public health practitioners and other stakeholders and ultimately improves service and delivery. An earlier study similarly revealed that informing practice has been identified as a way by which embedded researchers communicate new and existing relevant research evidence and integrate research findings into practice [ 3 ].
As discussed earlier, two of the factors responsible for the gap between the discovery and implementation of research evidence are the disparity between the language spoken by the researchers and practitioners and the complexity of the language spoken by researchers, which is often include scientific jargon. Such complex language can be difficult for practitioners to understand or lead to ambiguities in interpretation [ 12 ]. To discover whether language differences was an issue in this study, the interviews included questions regarding how research evidence and recommendations were communicated to public health practitioners and other stakeholders. These questions were designed to create an understanding of how the embedded researchers had communicated. The interviews revealed that the embedded researchers communicated research outcomes and recommendations effectively to the practitioners by using simple, unambiguous language. Using such language helped make research evidence more accessible to the practitioners.
Providing evidence for reports and future funding applications was identified as an important part of the embedded researchers’ work within their host organisations [ 17 , 47 ]. The interview participants agreed that the researchers sometimes helped secure funds needed to conduct research at the host organisation. Doing so encouraged each host organisation’s staff to participate in research that could prove useful to the organisation in the future.
Critical reflection helps embedded researchers evaluate the role they play within their host organisation and keep track of their progress [ 33 , 48 ]. In other words, reflection helps researchers identify and improve upon the areas that are not meeting expectations and discover what approaches are working successfully. This corresponds with the findings from this current qualitative inquiry. The interview participants acknowledged that the embedded researchers continuously reflect on their role and their work in order to identify what is and is not working. This assists embedded researchers to think of ways to apply acquired learning to daily on-site practice to improve their role in the co-production of research to bridge the gap between research evidence and its implementation in public health practice.
Limitations of the study
One of the limitations of this study was the sample size. A total of 17 participants was recruited for this study, although the sample size would have been larger than 17 but for the COVID-19 pandemic. Another consideration of this piece of work, being qualitative research, was subjectivity. The information provided by the participants was based on their point of view. Hence, it might be difficult to objectively verify the qualitative information provided to ensure that accurate information was provided by the participant regarding the phenomenon of interest. Nevertheless, some practical measures were undertaken to ensure the credibility of this work. Data triangulation and site triangulation [ 49 ] were adopted in this study. These were done to increase the confidence in the outcome of the qualitative multi-site case study.
Overall, the success that the embedded researchers experienced, including building relationships, co-producing research, translating research into practical changes, evaluating projects, and informing future public health practices as well as future research, justifies increasing the amount of embedded research being conducted in public health practice. Embedded researchers also bring the tremendous benefit of strengthening the research capacities of public health practitioners and other stakeholders by providing research-based training and support. Such developments have the ability to prove the potential of embedded research projects. Finally, the relevant research-based recommendations made from the co-produced research guided by the embedded researchers are used to inform practice. The positive outcomes generated by the embedded research process indicate that embedded researchers can meaningfully contribute to closing the gap between the discovery and implementation of research evidence.
Availability of data and materials
The datasets generated and/or analysed during the current study are not publicly available. They are available from the corresponding author on reasonable request, subject to approval from the Teesside University School of Health and Life Sciences Research Governance and Ethics Committee.
Lobb R, Colditz GA. Implementation science and its application to population health. Annu Rev Public Health. 2013;34:235–51.
Article PubMed PubMed Central Google Scholar
Di Ruggiero E, Viehbeck S, Greyson D. Knowledge utilization and exchange. Oxford: Oxford University Press—Oxford Bibliographies in Public Health; 2017.
Google Scholar
Marshall M, Pagel C, French C, Utley M, Allwood D, Fulop N, Pope C, Banks V, Goldman A. Moving improvement research closer to practice: the researcher in residence model. BMJ Qual Saf. 2014;23:801–5.
Chew S, Armstrong N, Martin G. Institutionalising knowledge brokering as a sustainable knowledge translation solution in healthcare: how can it work in practice? Evid Policy. 2013;9:335–51.
Article Google Scholar
Proudfoot A, Mcauley D, Hind M, Griffith M. Translational research: what does it means, what has it delivered and what it might deliver? Curr Opin Crit Care. 2011;17:495–503.
Article PubMed Google Scholar
Albert MA, Fretheim A, Maiga D. Factors influencing the utilization of research findings by health policymakers in a developing country: the selection of mali’s essential medicines. Health Res Policy Syst. 2007;5:2.
Armstrong R, Doyle J, Lamb C, Waters E. Multi-sectoral health promotion and public health: the role of evidence. J Public Health. 2006;28(2):168–72.
Bunn F. Strategies to promote the impact of systematic reviews on healthcare policy: a systematic review of the literature. Evid Policy. 2011;7:428.
Allen T, Grace C, Martin S. From analysis to action: connecting research and local government in an age of austerity. Report of the local government knowledge navigator. London: Local Government Association; 2014.
Campbell D, Donald B, Moore G, Frew D. Evidence check: knowledge brokering to commission research reviews for policy. Evid Policy. 2011;7(1):97–107.
Dobbins M, Robeson P, Ciliska D, Hanna S, Cameron R, O’mara L, et al. A description of a Knowledge Broker Role implemented as part of a randomized controlled trial evaluating three knowledge translation strategies. Implement Sci. 2009;4:23.
Friese B, Bogenschneider K. The Voice of experience: how social scientists communicate family research to policymakers. Fam Relat. 2009;58(2):229–43.
Newbury-birch D, Allan K. Co-creating and co-producing Research evidence: a guide for practitioners and academics in Health, Social Care and Education Settings. London and New York: Routledge; 2019.
Book Google Scholar
Van der graaf P, Forrest L, Adams J, Shucksmith J, White M. How do public health professionals view and engage with research? A qualitative interview study and stakeholder workshop engaging public health professionals and researchers. BMC Public Health. 2017;17:892.
Hobin EP, Riley B, Hayward S, Ruggiero ED, Birdsell J. Maximising the use of evidence: exploring the Intersection between Population health intervention research and knowledge translation from a Canadian perspective. Evid Policy. 2012;8(1):97–115.
Oliver K, Kothari A, Mays N. The dark side of coproduction: do the costs outweigh the benefits for health research? Health Res Policy Syst. 2019;17:33.
Wong S. Tales from the frontline: the experiences of early childhood practitioners working with an ‘Embedded’ research team. Eval Program Plann. 2009;32:99–108.
Fathimath S, David E, Helen B. Nurses’ perceptions of barriers and facilitators to implement EBP in the Maldives. Adv Nurs. 2014;2014:7. Article ID 698604.
Aszkenasy OM, Dawson D, Gill M, Haines A, Patterson DLH. Audit of direct access cardiac investigations: experience in an inner london health district. J R Soc Med. 1994;87:588–90.
Article CAS PubMed PubMed Central Google Scholar
Davis DA, Thomson MA, Oxman AD, Haynes RB. Changing physician performance: a systematic review of the effect of educational strategies. J Am Med Assoc. 1995;274:700–5.
Article CAS Google Scholar
Sutton M. How to get the best health outcome for a given amount of money. BMJ. 1997;1997(315):47–9.
Rycroft-malone J. From knowing to doing: from the academy to practice, comment on the many meanings of evidence: implications for the translational science agenda in healthcare. Int J Health Policy Manag. 2014;2:1–2.
Walshe K, Davies H. Health research, development and innovation in England from 1988 to 2013: from Research production to knowledge mobilization. J Health Serv Res. 2013;18:1–12.
Ryan B. Coproduction: option or obligation? Aust J Public Adm. 2012;71:314–24.
Groundwater-smith S, Mockler N. The knowledge building school: from the outside in, from the inside out. Change Transform Educ. 2002;5:15–24.
Himmrich J. How should academics interact with policy makers? Lessons on building a long-term advocacy strategy. LSE Impact Blog. 2016. Available at: How should academics interact with policy makers? Lessons on building a long-term advocacy strategy. | Impact of Social Sciences (lse.ac.uk). Accessed 15/01/2022.
Zevallos Z. Protecting activist academics against public harassment. Other Sociologist. 2017. Available at: Protecting Activist Academics Against Public Harassment – The Other Sociologist. Accessed 15/01/2022.
Davey SG, Ebrahim S, Frankel S. How policy informs the evidence. BMJ. 2001;322(7280):184–5.
Maybin J. How proximity and trust are key factors in getting research to feed into policymaking. LSE Impact Blog. 2016. Available at: How proximity and trust are key factors in getting research to feed into policymaking | Impact of Social Sciences (lse.ac.uk). Accessed 15/01/2022.
Rycroft-malone J, Burton CR, Bucknall T, Graham ID, Hutchinson AM, Stacey D. Collaboration and co-production of knowledge in healthcare: opportunities and challenges. Int J Health Policy Manage. 2016;5(4):221–3.
Hegger D, Dieperink C. Toward successful joint knowledge production for Climate Change Adaptation: lessons from six Regional projects in the Netherlands. Ecol Soc. 2014;19(2):34.
Brannick T, Coghlan D. Defense of being native: the case for insider academic research. Organ Res Methods. 2007;10:59–74.
Langeveld K, Stronks K, Harting J. Use of a Knowledge Broker to establish healthy public policies in a city district: a developmental evaluation. BMC Public Health. 2016;16:271.
Yost J, Dobbins M, Traynor R, Decorby K, Workentine S, Greco L. Tools to support evidence-informed public health decision making. BMC Public Health. 2014;14:728.
Smith LS, Wilkins N. Mind the gap: approaches to addressing the research-to-practice, practice-to-research chasm. J Public Health Manage Pract. 2018;24:S6–11.
Mcginity R, Salokangas M. Introduction: “Embedded Research” as an Approach into academia for emerging researchers. Management in Education. 2014;28:3–5.
Dixon-woods M, Martin G. Does quality improvement improve quality? Future. Hosp J. 2016;3:191–4.
Dixon-woods M, Mcnicol S, Martin G. Ten challenges in improving quality in healthcare: lessons from the Health foundation’s programme evaluations and relevant literature. BMJ Qual Saf. 2012;21:876–84.
Vindrola-padros C, Eyre L, Baxter H, et al. Addressing the challenges of knowledge co-production in quality improvement: learning from the implementation of the researcher-in-residence model. BMJ Qual Saf. 2019;28:67–73.
Polit D, Beck C. Generalization in quantitative and qualitative research: myths and strategies. Int J Nurs Stud. 2010;47:1451–8.
Jenkins EK, Slemon A, Haines-saah RJ, Oliffe J. A Guide to multisite qualitative analysis. Qual Health Res. 2018;28(12):1969–77.
Braun V, Clarke V. Using thematic analysis in psychology. Qualitative Res Psychol. 2006;3(2):77–101.
Hayden MC, Waller G, Hodgson A, Brown S, Harris S, Miller K, Barber D, Hudson L, Newbury-Birch D. ‘Pupils, Teachers and Academics Working Together on a Research Project Examining How Students and Teachers Feel About the New GCSEs’, in Newbury-Birch and Allan. Co-creating and Co-producing Research Evidence: A Guide for Practitioners and Academics in Health, Social Care and Education Settings. London and New York: Routledge, Taylor & Francis Group; 2019.
Lewis S, Russell A. Being embedded: a way forward for ethnographic research. Ethnography. 2011;12:398–416.
Rowley H. Going beyond procedure: engaging with the ethical complexities of being an embedded researcher. Manage Educ. 2014;28:19–24.
Embedded research. https://www.embeddedresearch.org.uk . (No date). Accessed 22 Nov 2023.
Jenness V. Pluto, prisons, and plaintiffs: notes on systematic back-translation from an embedded researcher. Soc Probl. 2008;55:1–22.
Duggan J. Critical friendship and critical orphanship: embedded research of an english local authority initiative. Manage Educ. 2014;28(1):12–8.
Denzin N. The Research Act: A Theoretical Introduction to Sociological Methods (2nd edition). New York: McGraw Hill; 1978.
Download references
Acknowledgements
We thank the participants for sharing their expertise and time. We are grateful for the contribution of Ronnie Ramlogan who supported us in the preparation of this manuscript.
This research received no external funding.
Author information
Authors and affiliations.
School of Health and Life Science, Teesside University, Middlesbrough, UK
Abisope Akintola
School of School of Social Sciences, Humanities & Law, Teesside University, Middlesbrough, UK
Dorothy Newbury-Birch & Stephanie Kilinc
Manchester Institute of Innovation Research, Alliance Manchester Business School, University of Manchester, Manchester, UK
You can also search for this author in PubMed Google Scholar
Contributions
This study is part of AA’s PhD work, as such, AA conducted this piece of work with the supervision of DNB and SK.
Corresponding author
Correspondence to Abisope Akintola .
Ethics declarations
Ethics approval and consent to participate.
Ethical approval was obtained from the Teesside University School of Health and Life Sciences Research Governance and Ethics Committee. All methods were carried out in accordance with relevant research guidelines and regulations. The participants were informed about the purpose of the research, the voluntary nature of participation, and their right to withdraw at any time without any consequences. The anonymity and privacy of the participants were guaranteed throughout the study. Informed written and verbal consent was obtained from the participants before the interviews.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Interview schedule for embedded researchers
Role identification and background information about the embedded research initiative.
What is your role in your organisation? Prompt - Job title, Daily task, Responsibilities. B) How long have you been in this role? C) Can you tell me about your background and what you do? Prompt -The journey so far- How do you get to where you are now? D) As an embedded researcher where is your academic affiliation?
How long has your embedded research initiative been going on in your organisation? B) Do you know the rationale for employing an embedded researcher in your organisation? C) Who funds your project? D)What is the management arrangement?
Moving on to look at the embedded research initiative more specifically
What is the aim of the embedded research project you are involved in? B) How many hours/days do you spend in your host organisation in a week, and in the academic institution? C) Why? D) How often do you contact your academic supervisor?
How has embedded research gone so far in your organisation? B) How many people are involved in the co-production/embedded research you are involved in? or who do you work with? C) How many embedded researchers are involved in the project? Prompt - How many professionals/stakeholders?
What are your views and experience of embedded research? Prompt - what have you learnt? What, if anything, has helped? (Why do you say that?) What, if anything, has been more difficult or challenging? (Why do you say that)? What difference has embedded research made in your organisation? (so if embedded research has been useful, why and how?)
Looking more specifically at the role of the embedded researcher in the organisation
What is your role, as an embedded researcher in bridging the gap between research evidence and its implementation in practice? Prompts - How do you inform practice with research evidence? How do you communicate research evidence to practitioners and other stakeholders to facilitate its use in practice? B) Does your role involve the translation of research evidence into practice? If yes, what is the process? can you please cite an example? What evidence-sharing methods or processes do you use?
Can you think of any changes in practice/policy as a result of research evidence being used? Prompt – What role did you play? Who was involved? What changed? How? For who?
Tell me what you think are the benefits of working as an embedded researcher? Why do you say that? B) How do you manage the dual affiliation? Prompt -what are the benefits (What has helped?) and also what are the challenges?
Tell me what you think are the challenges of working as an embedded researcher? Prompt - Why do you say that? B) What are the barriers to data sharing, if any?
Do you think building mutually beneficial relationships with the host organisation staff is important to the success of an embedded research project? If yes, Why? B) How do you build relationships with the host organisation’s staff?
Can you cite an example of where you have built practitioners and other stakeholders’ confidence in conducting their own research?
Does your role requires managing research funds? If yes, how do you manage this?
How often do you reflect on your role? Prompt- To know what works and what needs to be improved? Why is this important?
Do you think the development of a toolkit on the role of embedded research in bridging the gap between research evidence and its implementation in public health practice would be useful? If yes, Why and how do you think it could be used in practice?”
Any top tips for other researchers considering embedded research?
Please don’t mention names, but can you think of any potential participants- people you are working with or have worked with that you can pass on the details of this research? B) Would you be happy to be contacted afterward to circulate details of this research to those you have identified, to see if they will be willing to participate in this research?
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Akintola, A., Newbury-Birch, D. & Kilinc, S. Bridging the gap between research evidence and its implementation in public health practice: case studies of embedded research model. BMC Public Health 24 , 1299 (2024). https://doi.org/10.1186/s12889-024-18727-z
Download citation
Received : 05 January 2024
Accepted : 28 April 2024
Published : 13 May 2024
DOI : https://doi.org/10.1186/s12889-024-18727-z
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Public health
- Embedded research
- Research-based evidence
- Co-production
- Research evidence- implementation gap
BMC Public Health
ISSN: 1471-2458
- Submission enquiries: [email protected]
- General enquiries: [email protected]
COMMENTS
Learning Outcomes. By the end of this section, you will be able to: 1 Describe the Gap Model of Service Quality.; 2 List and describe the dimensions of service quality.; Dimensions of Service Quality. While we're still on the subject of customer satisfaction, let's take a look at still another model that aids marketers in better understanding customer satisfaction: the Gap Model of Service ...
The gap model of service quality addresses five gaps that the framework addresses. Each gap is a difference between an expectation and a deliverable. The five gaps that the framework examines are: 1. Gap between management perception and customer expectation. This gap measures what customers expect and what management thinks they want.
customer's perspectives of service importance and service performance satisfaction through the analysis of Service Quality Gap Model. The theory suggests that 5 gaps of service quality; the knowledge gap, the standards gap, the delivery gap, the communication gap and the service gap, should be identified to investigate the service inefficiency.
Large RO, Konig T (2009) A gap model of purchasing's internal service quality: concept, case study and internal survey. J Purch Supply Manag 15:24-32. Article Google Scholar Lee YC, Chen JK, Lin SB (2007) Revised Gap analysis by decomposition of service activities: a case study of information system center.
In this context, and against the background of the GAP model and service quality, information about customer expectations is particularly in the focus. ... E-Service quality expectations. A case study. Total Quality Management, 14(4), 437-450. Article Google Scholar Santos, J. (2003). E-Service quality: A model of virtual service quality ...
The gap model of service quality serves as an outline for service firms to improve service quality, service delivery, and services marketing. 3.2 The Thr ee-Component Model: developed by Rust ...
The purpose of this research is aimed to identify the gaps or discrepancies between the hotel managers and the customer's perspectives of service importance and service performance satisfaction through the analysis of Service Quality Gap Model. The theory suggests that 5 gaps of service quality; the knowledge gap, the standards gap, the delivery gap, the communication gap and the service gap ...
Design of the case study3.1. MethodsThe method applied to verify the internal service gap model of purchasing is an in-depth case study including an internal survey of purchasers' and internal customers' perspectives of service quality.
A comprehensive Service Quality Gap (SQG) model is presented that explains the areas to look for and some of which can be disaggregated, according to the organization's strategic quality dimensions, namely, strategy formulation, development and delivery. This paper, drawing on several studies, presents a comprehensive Service Quality Gap (SQG) model that explains the areas to look for SQGs.
SERVQUAL Model Key Dimensions. The Service Gap Model involves the concepts of service quality and customer satisfaction. As a result, it is also known as the SERVQUAL model, abbreviating "service ...
The service quality gap model, which identifies the antecedents of SERVQAUL, reveals that service quality depends on the gap between customer perceived and expected service (Gap 5), which can be caused by other gaps in the service process (Gaps 1-4). The emergence of service robots has affected the quality of services provided; however, little is known about how these impacts happen.
The Servqual model (also called the gap model) was developed by American authors A. Parasuraman, Valarie A. Zeithaml and Len Berry. In general, the SERVQUAL model identifies the principal dimensions of service quality. Initially, there were ten dimensions of service quality identified. However, later these were reduced to 5 as some of these ...
The method applied to verify the internal service gap model of purchasing is an in-depth case study including an internal survey of purchasers' and internal customers' perspectives of service quality. At first glance, the research might appear to be of limited scope as the subject of analysis is the purchasing department of one individual ...
Abstract. The study aims to contribute to the research on service quality, analyzing almost 30 years of research on the. Gaps Model proposed by Parasuraman, Zeithaml and Berry in the 1980s. A ...
emphasises on add ressing different markets (6-market model) to increase the value. of customers and provide a better s ervice (Internal, referral, influence, recruitment. supplier/alliance ...
The model of service quality gaps has been critically reviewed and developed in order to make it more comprehensive and has been verified based using a survey on 16 experts. High service quality is imperative and important for competitiveness of service industry. In order to provide much quality service, a deeper research on service quality models is necessary.
quality and speed of the service handling, menu variety were perceived key value attributes. Selvakumar (2015) examined the impact of service quality on customer satisfaction in public sector and private sector banks in Coimbatore and the relative differences attached with the various determinants of service quality using the SERVQUAL model.
Gap 2: The Policy Gap. The policy gap is the difference between management's understanding of the customer needs and the translation of that understanding into service delivery policies and standards. There are a number of reasons why this gap can occur: Lack of customer service standards. Poorly defined service levels.
Service quality gap analysis in HDFC bank: A case study on housing finance customers perspective ... service quality model developed by Zeithamal, Parsuraman and Berry (1988) [5] has been used in the present study. The ... A case study method is adopted and supplemented with findings of a small survey to identify the determinants of
This paper aims to develop a multi-criteria evaluation model to evaluate the gap between passengers' perceptions (perceived service quality) and their expectations (expected service quality), and to diagnose managerial strategies of gap reduction within the airport passenger service context. ... This paper also provides an empirical case study ...
The g ap model of se rvice quality. The gap model is a marketing method to analyse per ception in relation t o expectations. This. model, developed by Parasuraman, Zeithaml, and Berry (1985 ...
Service marketing Gap model Analysis ... Tan, L. H., Hamid, S. R. and Chew, B. C. 2016. Service Quality Audit Based on Conceptual Gaps Model of Service Quality: A Case Study of Top Three Largest Local Bank in Malaysia. International Journal Productivity and Quality Management vol. 18, no. 1, pp.99-115.
Aim To investigate the potential of embedded research in bridging the gap between research evidence and its implementation in public health practice. Methods Using a case study methodology, semi-structured interviews were conducted with 4 embedded researchers, 9 public health practitioners, and 4 other stakeholders (2 teachers and 2 students) across four case study sites. Sites and individuals ...
DOI: 10.1016/J.PURSUP.2008.10.001 Corpus ID: 167522105; A gap model of purchasing's internal service quality: Concept, case study and internal survey @article{Large2009AGM, title={A gap model of purchasing's internal service quality: Concept, case study and internal survey}, author={Rudolf O. Large and Tatjana M. K{\"o}nig}, journal={Journal of Purchasing and Supply Management}, year={2009 ...