Doping Prevalence in Competitive Sport: Evidence Synthesis with "Best Practice" Recommendations and Reporting Guidelines from the WADA Working Group on Doping Prevalence
Affiliations.
- 1 Department of Kinesiology, California State University Fullerton, 800 N State College Blvd, Fullerton, CA, 92834, USA. [email protected].
- 2 Kingston University London, Kingston upon Thames, UK.
- 3 University of Münster, Münster, Germany.
- 4 Doping Authority Netherlands, Capelle aan den IJssel, The Netherlands.
- 5 Penn State University, State College, USA.
- 6 University of Lausanne, Lausanne, Switzerland.
- 7 University of Utrecht, Utrecht, Netherlands.
- PMID: 33900578
- DOI: 10.1007/s40279-021-01477-y
Background: The prevalence of doping in competitive sport, and the methods for assessing prevalence, remain poorly understood. This reduces the ability of researchers, governments, and sporting organizations to determine the extent of doping behavior and the impacts of anti-doping strategies.
Objectives: The primary aim of this subject-wide systematic review was to collate and synthesize evidence on doping prevalence from published scientific papers. Secondary aims involved reviewing the reporting accuracy and data quality as evidence for doping behavior to (1) develop quality and bias assessment criteria to facilitate future systematic reviews; and (2) establish recommendations for reporting future research on doping behavior in competitive sports to facilitate better meta-analyses of doping behavior.
Methods: The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were used to identify relevant studies. Articles were included if they contained information on doping prevalence of any kind in competitive sport, regardless of the methodology and without time limit. Through an iterative process, we simultaneously developed a set of assessment criteria; and used these to assess the studies for data quality on doping prevalence, potential bias and reporting.
Results: One-hundred and five studies, published between 1975 and 2019,were included. Doping prevalence rates in competitive sport ranged from 0 to 73% for doping behavior with most falling under 5%. To determine prevalence, 89 studies used self-reported survey data (SRP) and 17 used sample analysis data (SAP) to produce evidence for doping prevalence (one study used both SRP and SAP). In total, studies reporting athletes totaled 102,515 participants, (72.8% men and 27.2% women). Studies surveyed athletes in 35 countries with 26 involving athletes in the United States, while 12 studies examined an international population. Studies also surveyed athletes from most international sport federations and major professional sports and examined international, national, and sub-elite level athletes, including youth, masters, amateur, club, and university level athletes. However, inconsistencies in data reporting prevented meta-analysis for sport, gender, region, or competition level. Qualitative syntheses were possible and provided for study type, gender, and geographical region. The quality assessment of prevalence evidence in the studies identified 20 as "High", 60 as "Moderate", and 25 as "Low." Of the 89 studies using SRP, 17 rated as "High", 52 rated as "Moderate", and 20 rated as "Low." Of the 17 studies using SAP, 3 rated as "High", 9 rated as "Moderate", and 5 rated as "Low." Examining ratings by year suggests that both the quality and quantity of the evidence for doping prevalence in published studies are increasing.
Conclusions: Current knowledge about doping prevalence in competitive sport relies upon weak and disparate evidence. To address this, we offer a comprehensive set of assessment criteria for studies examining doping behavior data as evidence for doping prevalence. To facilitate future evidence syntheses and meta-analyses, we also put forward "best practice" recommendations and reporting guidelines that will improve evidence quality.
© 2021. The Author(s), under exclusive licence to Springer Nature Switzerland AG.

Publication types
- Meta-Analysis
- Systematic Review
- Doping in Sports*
- Surveys and Questionnaires
- Search Menu
- Advance Articles
- Editor's Choice
- Supplements
- Image Library
- ESC Journals App
- ESC Content Collections
- Author Guidelines
- Submission Site
- Open Access Options
- Read & Publish
- Author Resources
- Self-Archiving Policy
- About European Journal of Preventive Cardiology
- Editorial Board
- ESC Publications
- About European Society of Cardiology
- Advertising & Corporate Services
- Developing Countries Initiative
- Journals on Oxford Academic
- Books on Oxford Academic

Article Contents
Introduction, doping substances, methods to increase skeletal muscle oxygen delivery, commonly prescribed medications, commonly used over-the-counter medications, legal ergogenic supplements, recreational drugs and energy drinks, new trends of doping, aspects for non-medics, ethical considerations.
- < Previous
Cardiovascular effects of doping substances, commonly prescribed medications and ergogenic aids in relation to sports: a position statement of the sport cardiology and exercise nucleus of the European Association of Preventive Cardiology
Paolo Emilio Adami and Nikolaos Koutlianos authors are Joint First Authors.
- Article contents
- Figures & tables
- Supplementary Data
Paolo Emilio Adami, Nikolaos Koutlianos, Aaron Baggish, Stéphane Bermon, Elena Cavarretta, Asterios Deligiannis, Francesco Furlanello, Evangelia Kouidi, Pedro Marques-Vidal, Josef Niebauer, Antonio Pelliccia, Sanjay Sharma, Erik Ekker Solberg, Mark Stuart, Michael Papadakis, Cardiovascular effects of doping substances, commonly prescribed medications and ergogenic aids in relation to sports: a position statement of the sport cardiology and exercise nucleus of the European Association of Preventive Cardiology, European Journal of Preventive Cardiology , Volume 29, Issue 3, February 2022, Pages 559–575, https://doi.org/10.1093/eurjpc/zwab198
- Permissions Icon Permissions
The use of substances and medications with potential cardiovascular effects among those practicing sports and physical activity has progressively increased in recent years. This is also connected to the promotion of physical activity and exercise as core aspects of a healthy lifestyle, which has led also to an increase in sport participation across all ages. In this context, three main users’ categories can be identified, (i) professional and amateur athletes using substances to enhance their performance, (ii) people with chronic conditions, which include physical activity and sport in their therapeutic plan, in association with prescribed medications, and (iii) athletes and young individuals using supplements or ergogenic aids to integrate their diet or obtaining a cognitive enhancement effect. All the substances used for these purposes have been reported to have side effects, among whom the cardiovascular consequences are the most dangerous and could lead to cardiac events. The cardiovascular effect depends on the type of substance, the amount, the duration of use, and the individual response to the substances, considering the great variability in responses. This Position Paper reviews the recent literature and represents an update to the previously published Position Paper published in 2006. The objective is to inform physicians, athletes, coaches, and those participating in sport for a health enhancement purpose, about the adverse cardiovascular effects of doping substances, commonly prescribed medications and ergogenic aids, when associated with sport and exercise.
Doping is defined as the use of a substance or method, which is potentially dangerous to athletes’ health or capable of enhancing their performance. 1 In order to lead a collaborative worldwide movement for doping-free sport, the World Anti-Doping Agency (WADA), an international independent agency, composed and funded equally by the sport movement and governments of the world, was established in 1999. In 2004, the WADA Code was introduced (latest revision in 2021), and up to date, it has been accepted by approximately 700 sport organizations, including the International Olympic Committee (IOC), the International Paralympic Committee (IPC), International Federations (IFs), National Olympic and Paralympic Committees, as well as National and Regional Anti-Doping Organizations (NADOs and RADOs). Moreover, the WADA updates yearly the List of Prohibited Substances and Methods. 2 Nevertheless, the use of novel and unclassified agents or off-label use of prescription medications continues to pose a problem in terms of safety, equity, and regulation. This is due to the lag between the time athletes start experimenting with novel substances, to the time when authorities become aware of these agents and are able to track them. 3 Based on a recent systematic review, 4 the prevalence of doping in competitive sport ranged from 0% to 73%, with most falling under 5% and it impacts all levels of sport, from elite to amateur levels, with an increasing use in recreational athletes, who have less health surveillance. 5 Furthermore, yearly WADA reports confirm that most accredited doping control laboratories have an adverse analytical findings of approximately 2%. 6 A retrospective re-analysis of anti-doping rule violations of all samples collected at Summer Olympics Games from 1968 to 2012 revealed that the majority of positive re-tested samples contained metabolites of exogenous anabolic androgenic steroids (AAS), 7 but the list of the WADA banned drugs is extensive. The prevalence of the reported adverse analytical findings by doping category is presented in Table 1 . Moreover, it is worthy to distinguish between the substances and methods prohibited at all times (in- and out-of-competition) and those prohibited in-competition only.
Prevalence of adverse analytical findings by substance category in WADA Anti-Doping Administration and Management System (ADAMS)—(WADA, 2019 Anti-Doping Testing Figures)
This article is an update of the 2006 adverse cardiovascular effects of doping in athletes position paper published by the European Society of Cardiology sports cardiology study group. 8 The objective of this position paper is to raise awareness and to inform cardiologists, physicians, and sport enthusiasts of the adverse cardiovascular effects of doping substances, performance-enhancing drugs, substances of abuse, and most frequently prescribed medication, with particular emphasis on their cardiovascular effects during sport participation and exercise. The authors undertook a comprehensive review of the published evidence. A critical evaluation of all substances implicated in doping, commonly prescribed medication and ergogenic aids athletes may use was performed, including assessment of pharmacological and pathophysiological mechanisms, impact on the cardiovascular system, impact on exercise performance, and the risk benefit ratio.
Anabolic agents
AAS are widely used not only by athletes competing in power or strength sports but also in endurance sports to aid in recovery and strength. The simultaneous use of AAS and erythropoietin is common both in strength and endurance athletes. 9 AAS act by activating androgen receptor (AR) signalling. Moreover, increased testosterone levels inhibit glucocorticoid action and protein catabolism. These mechanisms in combination with the stimulation of growth hormone and insulin-like growth factor-1 (IGF-1) axis cause muscle protein formation. 10 These effects are enhanced when combined with regular training, leading to increased muscle mass and strength and reduced fat body mass. 11–13 Significant increases in physical performance and strength have been observed in double-blinded randomized trials comparing AAS vs. placebo. 14 , 15
Mortality amongst athletes doping with AAS is estimated to be 6–20 times higher than in clean athletes, and around 30% of these deaths can be attributed to cardiovascular causes. 16 Four principal mechanisms responsible for sudden cardiac death (SCD) have been proposed in AAS abusers: (i) the atherogenic model, (ii) the thrombosis model, (iii) the nitric-oxide mediated vasospasm model, and (iv) the direct myocardial injury model. 17 Attempting to study the cardiovascular side effects of AAS comes with inherent limitations as ethical and legal considerations prohibit their administration in athletes even for research purposes. Accordingly, AAS preparations, dosage and duration of AAS use are based on athlete self-reporting in most studies. Additionally, the majority of studies included a small population size and most athletes use combination of different substances, prohibited or legal, such that results cannot be solely attributed to AAS use. 18 Despite these limitations, the results of 49 studies over the last 10 years in 1467 athletes taking AAS show that the most common disorders attributable to their use include early onset of coronary heart disease, hypertension, myocardial infarction and heart failure, arrhythmias, and SCD. 19
AAS and coronary atherosclerosis
Regarding atherosclerotic heart disease, Baggish et al . 20 found that there was an increase in coronary artery plaque volume in AAS users when compared with non-using weight-lifters, leading to rapidly progressive coronary artery disease. Numerous studies have shown that otherwise healthy young AAS-using athletes have elevated levels of low-density lipoprotein, markedly reduced levels of high-density lipoprotein, and increased arterial blood pressure. 16 , 21 Impaired coagulation leading to thrombotic complications and myocardial infarction have also been described. 19 Chang et al . 22 suggested that AAS use may reduce synthesis of coagulation factors, inhibitors, and fibrinolytic proteins, causing a procoagulant state that may lead to myocardial infarction and other thrombotic complications. On the contrary, Corona et al . 23 in a systematic review and meta-analysis, reported no increased cardiovascular risk in 1448 patients receiving testosterone over a mean duration of 34 weeks.
AAS and cardiomyopathies
Numerous studies have shown that AAS users are at increased risk for cardiomyopathy and left ventricular (LV) dysfunction. The existence of AAS-induced cardiomyopathy has been confirmed by data derived from post-mortem examination, echocardiography, and cardiac magnetic resonance imaging. 24–26 Indeed, AAS use has been shown to change the physiological cardiac remodelling typical of athletes to a pathophysiological cardiac hypertrophy with an increased risk of life-threatening arrhythmias. The condition shares similar characteristics with hypertrophic cardiomyopathy, showing greater cardiac mass, LV wall thickness/hypertrophy (LVH), prevalence of cardiac fibrosis, and impairment of systolic and diastolic LV function. 25 , 27–30 LVH was attributed to either arterial hypertension or to the direct binding of AAS to the ARs on the myocardium. 20 , 31 Even in cases with normal standard echocardiogram, tissue Doppler, strain, and strain rate echocardiography have been used to detect early regional myocardial dysfunction after AAS abuse. Mean dosage and duration of AAS use were found to be strongly associated with a subclinical reduction of both systolic and diastolic LV function. 29 Even past illicit AAS use was found to be associated with impaired LV global longitudinal strain, suggesting cardiac systolic dysfunction years after AAS cessation. 32 To explain early ventricular dysfunction in AAS users, it was suggested that high blood pressure may have a negative effect. 33 Montisci et al . supported that AAS can directly damage myocardial cells, causing a subsequent focal repair process and a disproportionate increase in the connective tissue content of the damaged area. 26 Cecchi et al . 34 described a direct apoptotic cardiac and endothelial change in the heart tissue in patients with heart failure who had a history of AAS abuse. Additionally, peak systolic right ventricular free wall strain and strain rate were found to be reduced in bodybuilders AAS users compared with non-users. 35 D'Andrea et al . 31 reported a more impaired left atrial (LA) deformation and LA systolic dysfunction with the use of speckle echocardiography in AAS users. LA enlargement has been proposed as a predictor of common cardiovascular outcomes such as atrial fibrillation, stroke, and death. 36 Many case reports described episodes of SCD in anabolic abuse, linked AAS to potentially life-threatening arrhythmias. 17 , 19 Hypertrophy, fibrosis, and necrosis represent a substrate for arrhythmias, especially when combined with exercise. BarbosaNeto et al . 37 found a marked cardiac autonomic alteration in AAS users, with a shift towards sympathetic modulation predominance and vagal attenuation. In a recent study, Kouidi et al . 38 found that long-term AAS in strength-trained athletes decreases baroreflex sensitivity (BRS) and short-term heart rate variability indices due to sympathetic overestimation. Moreover, a positive correlation between the reduced BRS and early LV diastolic dysfunction, which was mentioned in AAS users, was determined. An association between nandrolone use and life-threatening ventricular arrhythmias was also supported in an experimental study. 39 Moreover, Marocolo et al . 40 reported that anabolic administration in rats associated with cardiac autonomic dysfunction and ventricular repolarization and reflected an increase in QT interval ( Figure 1 ).

Cardiovascular effect of doping substances and drugs. The figure summarizes the main cardiovascular consequences of the different substance’s categories. BP, blood pressure; CAD, coronary artery disease; CMP, cardiomyopathy; LVH, left ventricular hypertrophy; SARM, selective androgen receptor modulators.
Human growth hormone
Human growth hormone (hGH) is an endogenous neurohormone considered to have anabolic effects when used in supra-physiologic doses. There is little evidence that recombinant hGH improves performance although it may aid more rapid recovery from soft tissue damage. 9 Little is known about the direct cardiovascular effects of excessive hGH administration in athletes; however, excess of endogenous hGH in patients with acromegaly may result in hypertension, congestive cardiac failure, and cardiomyopathy. 9 It has been suggested that hGH causes myocardial hypertrophy due to concentric remodelling, 41 and hGH may lead to increases in myocardial collagen deposition, fibrosis, cellular inflammation, and necrosis. 8 , 42 These alterations may be underlying mechanisms for malignant arrhythmias and the development of heart failure. 43 Finally, limited data suggest that hGH abuse can cause dose-dependent increase in cholesterol levels. 44
Selective androgen receptor modulators
Selective androgen receptor modulators (SARMs, e.g. thymosin beta-4) are a new class of substances designed to isolate the androgenic and anabolic effects of AAS. Limited information is available on the cardiovascular side effects of the several artificially designed SARMs that are used among athletes. Experimental data suggest that thymosin beta-4 can inhibit myocardial cell death, stimulate vessel growth, and activate endogenous cardiac progenitors. 45 At present, SARMs are considered experimental in humans with potential side effects including carcinogenicity and cardiovascular problems and their performance enhancing potential incompletely understood.
The WADA Prohibited List includes a number of narcotic analgesic drugs including buprenorphine, dextromoramide, diamorphine (heroin), fentanyl and its derivatives, hydromorphone, methadone, morphine, nicomorphine, oxycodone, oxymorphone, pentazocine, and pethidine. Narcotics may be used in athletes for treatment of pain due to sports-related injury, and post-traumatic pain syndrome in conjunction with an approved therapeutic use exemption (TUE). Oxycodone, a strong opioid analgesic, is increasingly used among young students and athletes for non-medical and recreational use. 46 Narcotics can cause dependency, a reduction in the perception of pain and a dangerous false sense of well-being. Several narcotics such as methadone and levomethadyl can also cause QT-lengthening and increase the risk of polymorphic ventricular tachycardia. 47 Other potential adverse effects include changes in QT dispersion, Takotsubo syndrome (stress cardiomyopathy), Brugada-like syndrome, and coronary artery diseases. 48
Stimulants include mainly amphetamines and methylphenidate, which are commonly prescribed for the treatment of attention-deficit hyperactivity disorder (ADHD), a common condition in athletes in some regions of the world. 49 ADHD treatment typically relies on methylphenidate or its derivatives. These substances are prohibited according to the WADA Prohibited List. 2 Amphetamine-based treatment is contraindicated in people with familial or personal history of arrhythmic diseases, in particular those with a genetic basis. The use of amphetamines and methylphenidate in athletes is only allowed upon acceptance of a TUE application. More recently, another psychoactive substance known as captagon (fenethylline), became widely popular for its addictive properties and its use as a powerful physiological and psychostimulant factor. Captagon can promote high physical performance and endurance, cognitive enhancement, and reduction of sleep and food requirements. 50
Stimulants have profound effects on the cerebrovascular and cardiovascular system, leading to congestive heart failure, acute myocardial infarction, cardiac chambers and valvular fibrosis, pulmonary hypertension, cerebral infarction, and haemorrhage. 51 , 52 Additionally, a drug-induced cardiomyopathy has also been described. 53 Pathologic mechanisms of amphetamine-related cardiomyopathy may include: direct toxic effects, neurohormonal activation, alteration of calcium homoeostasis, oxidative stress, modulation of cardiac gene expression, and apoptosis. 54 The histology of this cardiomyopathy is characterized by concentric LVH, atypical nuclei, interstitial and perivascular fibrosis, vacuolation of the cardiomyocytes, and hypertrophy of the middle layer of small intramyocardial vessels. 55 It is well known that amphetamines stimulate the release of norepinephrine affecting both alpha (α) and beta (β) adrenergic receptor sites. Alpha-adrenergic stimulation causes vasoconstriction and an increase in total peripheral resistance, while β-adrenergic receptor stimulation leads to an increase in heart rate, stroke volume, and skeletal muscle blood flow. These adverse reactions lead to tachycardia, increased body temperature, respiratory frequency and blood pressure. Furthermore, amphetamine and other nervous system stimulants lead to indirect stimulation of the autonomic nervous system through the release of catecholamines, dopamine, and serotonin in nerve terminals of the central and peripheral nervous systems, leading to cardiac arrhythmias. 56 The anatomical and functional changes derived from amphetamine abuse could act as substrates of SCD. 57 Besides the arrhythmogenic effect of amphetamine-derived substances, these drugs have also shown to increase the risk of heat-related illnesses . In particular, amphetamines could potentially mask or delay fatigue by slowing the exercise-induced internal temperature rise. This could also impact the thermoregulatory system potentially resulting in muscle overheating. 58 The use of dopamine reuptake inhibitors has shown to improve performance but also to cause hyperthermia without any change in the perception of effort or thermal stress, potentially increasing the risk of exertional heat injuries. 59 A similar effect is known for ephedrine-containing compounds, due to the sympathomimetic effect, impairing the body's ability to dissipate heat properly. 60 Ephedrine can be found in many over-the-counter preparations available from pharmacies.
Metabolic modulators
Meldonium (Mildronate) is licenced for clinical use in some Eastern European countries as an anti-anginal with a mechanism of action that is believed to be modulated, at least in part, by lowering of l -carnitine availability and a reduction in mitochondrial energy production. 61 Rare adverse effects were reported in athletes, including allergic reactions (redness and itchy skin, urticaria, rash, and/or angio-oedema), dyspepsia, tachycardia, and alterations (increase or decrease) in blood pressure. 62 After anecdotal reports of widespread use at the London 2012 Olympics, meldonium was detected in the urine of 9% of athletes at the 2015 European Games 63 and was subsequently included in the WADA Prohibited List in January 2016.
Beta-2 agonists
Beta-2 agonists such as salbutamol and clenbuterol are commonly prescribed as treatment for asthma, given their broncho-dilatory effects on the smooth muscles of the lung. In 2011, Pluim et al . 64 performed a meta-analysis of randomized controlled trials comparing inhaled or systemic beta-2 agonists to placebo and concluded that there are no data to support a positive effect on maximal oxygen uptake (VO 2max ), peak power output, strength, or endurance performance with inhaled beta-2 agonists (salbutamol, albuterol, or terbutaline). There was some weak evidence in support of high dose, oral salbutamol having a positive anaerobic capacity and strength 64 ; however, the doses used would be expected to produce adverse side effects such as tachycardia, ventricular ectopy, tremor, and hypokalaemia. 65 However, clenbuterol has recently emerged as a drug of misuse in both elite and recreational athletic circles, due to its effect on beta-3 receptors in adipocytes, resulting in lipolysis and weight loss, a desirable side effect in sports where being lean and/or light weight is desirable. 66 The doses required to achieve these effects are 120–160 µg daily, which is three to four times higher than the doses that are generally prescribed for the treatment of reactive airway disease. 66 Not surprisingly, side effects such as tachycardia, gastrointestinal disturbances, and tremor are common in individuals using clenbuterol in these doses. 67 Additionally, supraventricular and ventricular arrhythmias, myocardial ischaemia, sudden cardiac failure, and cardiac arrest have been reported. 68 , 69 The arrhythmogenic effect of the drugs is related both to their direct beta-2 stimulant action (particularly when inhaled). 70 Moreover, evidence of myocardial damage indicated by increased troponin concentrations was reported. 71 Clenbuterol is noted as an anabolic agent on the WADA Prohibited List.
Glucocorticoids
Glucocorticoids are classified as doping substances and they are prohibited in-competition when administered by oral, intravenous, intramuscular, or rectal route. 72 It has been suggested that they may increase the availability of metabolic substrates and improve the use of energy sources during exercise. 73 The major cardiovascular side effects include hypertension and dyslipidaemia. Arterial hypertension is attributed to fluid retention, increased systemic vascular resistance mainly due to reduced nitric oxide availability, and enhanced myocardial contractility. 73 Dyslipidaemia is mediated by impaired lipid metabolism and elevated levels of total plasma cholesterol, triglycerides, and low-density lipoprotein cholesterol have been reported. 18
Blood doping
Usually involving transfusion of autologous blood collected some time earlier to increase red blood cell mass, has been used for decades. There are small, blinded trials which support the notion that oxygen carrying capacity and hence performance are improved with blood doping. 74 , 75
Berglund et al . 74 performed a single blinded study on six cross-country skiers and observed a mean 6% reduction in 15 km race time both 3 and 14 days after reinfusion of 1350 mL of autologous blood.
Similar results were observed by Brien et al ., 75 who performed a double blinded cross-over study on six high level amateur 10 km runners, where haematocrit increased by 5% and 10 km race time was reduced by an average of 1 min after reinfusion of 400 mL of packed red blood cells, but not after infusion of saline.
Oxygen-carrying modulators
Agents that can increase oxygen availability to the working muscles, either by are theorized to improve endurance performance; however, the evidence for a positive effect on performance for many of these agents (e.g. perfluocarbons) is limited. 76
increasing oxygen content in the blood,
improving cardiac output, or
improving peripheral oxygen extraction.
Recombinant human erythropoietin
Recombinant human erythropoietin (rhEPO) triggers an increase in red blood cell mass and haemoglobin (Hb) concentration similar to that of blood doping, as well as an improvement in maximal oxygen consumption. However, systematic evidence that this translates into a positive effect on performance is limited. 77 , 78
Birkeland et al . 79 demonstrated an increase in both haematocrit and VO 2max following administration of rhEPO over 4 weeks in a double-blind placebo-controlled study with only a small cohort of trained cyclists ( n = 10). This period was needed to demonstrate a large treatment effect [42.7 vs. 50.8% ( P < 0.0001) and 63.6 vs. 68.1 mL/kg/min ( P < 0.0001) for haematocrit and VO 2max , respectively]. Although this study did not have a direct performance measure, time to exhaustion was increased significantly in the EPO group from 12.8 to 14 min ( P < 0.0001) as compared to 13.1 to 13.3 min ( P = 0.04) in the control group who were exposed to the same training effect. 79
Similar effects on VO 2max have been demonstrated in other placebo-controlled, double blind studies of rhEPO administration. 78 , 80–82 However, in the study of Heuberger et al ., 78 no improvement in a cycling race to Mont Ventoux with regards to time was observed despite a 5% improvement in VO 2max .
Nevertheless, it is not surprising that different EPO formulations, direct EPO receptor agonists and micro-dosing techniques are used by athletes with the aim of improving performance with minimal risk of being detected.
The potential negative cardiovascular consequences of such practices are underlined by a prospective cross-sectional study of 3000 healthy senior adults, which found that each doubling in serum EPO level was independently associated with a 25% increase in risk of incident heart failure over a mean follow-up of 10 years. 83 Cardiac side effects occurring in athletes with ‘haematologic doping’ (especially if they are dehydrated and exposed to strenuous exercise) are secondary to the circulatory overload, induced by the increased erythroid mass, increased blood viscosity, and altered endothelial and platelet function with possible thromboembolic events and hypertension during effort. 70 , 77 Additionally, it increases blood viscosity, coagulation, and platelet reactivity leading to an increased risk of thrombosis. 84 Some case reports of thromboembolic events as well as acute coronary syndrome with intraventricular thrombus in athletes following rhEpo doping have been reported. 85
Rather than increasing the blood oxygen content (like rhEPO), theoretically, the same effect may be achieved by increasing the amount of O 2 that Hb can deliver to the surrounding tissues. A number of agents with these properties have been reportedly used by athletes to aid performance:
Cobalt chloride is a water soluble compound that can stimulate erythropoiesis and angiogenesis, presumably due to activation of hypoxia-inducible factor-1 (HIF-1) signalling. 86 Although the direct cardiovascular effects in humans have not been prospectively studied, unintentional ingestion of cobalt has been associated with the development of a dilated cardiomyopathy. 87 , 88
Efaproxiral (right shifting reagent 13, RSR13 or Efaproxiral) is a synthetic modifier of Hb, with in vivo studies demonstrating a shift in the Hb/O 2 dissociation curve to the right, thereby increasing the dissociation of O 2 in the peripheral muscles. RSR13 has been shown to increase oxygen consumption in stimulated canine skeletal muscle, 89 when inspired O 2 was supplemented. However, in humans breathing sea level air, the right-shift of the O 2 curve induced by RSR13 causes significant hypoxaemia under resting conditions 90 that is likely to be further exacerbated by exercise. The side effects associated with exercising in a hypoxaemic state are not known and it is unlikely that the athletes in whom it is being used are aware of the physiology and potential risks.
There have also been attempts to improve muscle oxygen delivery by improving cardiac output. Specific pulmonary vasodilators such as Sildenafil are rumoured to be widely used amongst some endurance athletes. The rationale would seem that by reducing pulmonary vascular resistance it may be possible to reduce cardiac work, particularly of the right ventricle, thereby enabling the heart to maintain a high level of function for longer. 91 This is especially relevant given that exercise seems to place a disproportionate load on the pulmonary circulation and right ventricle. 92 In patients with pre-existing cardiovascular risk factors some cardiovascular, cerebrovascular, and vascular events, have been reported in the past, in temporal association with the use of sildenafil, 93 nevertheless more recent data on phosphodiesterase-5 (PDE5) inhibitors confirm the safety of the pharmacological class even in patients with cardiovascular risk factors and suggest a potential cardio-protective role of these molecules. 94 However, no complications have been reported in healthy athletes. Several studies have assessed whether pulmonary vasodilators can improve exercise performance in healthy volunteers and athletes.
Ghofrani et al . 95 documented improvements in exercise capacity in a randomized, double-blind placebo-controlled trial in 14 healthy subjects during normobaric hypoxia (10% O 2 ) and at altitude (Mount Everest base camp, 5245 m above sea level).
However, whilst studies using both PDE5 inhibitors and endothelin antagonists have consistently demonstrated improvements in haemodynamics and exercise performance in hypoxic conditions, they have failed to show any benefit in normoxia . 96–98 These agents are thus currently not banned by the WADA.
Beta-blockers and antiarrhythmics
According to the List of Prohibited Substances and Methods, 2 beta-blockers are banned drugs in certain skill-based sports such as shooting and archery, due to the performance benefit offered by lowering heart rate and reducing anxiety and tremor. Conversely, there is a general reluctance amongst athletes and prescribers to use beta-blockers in athletes with cardiovascular disease, due to the potentially detrimental effects of lowering the heart rate during exercise and reducing performance. 99 This is particularly true for endurance athletes and those requiring high cardiac output.
In a small group of healthy, untrained volunteers, nebivolol (a beta-1 selective beta blocker), at a dose of 5 mg daily, was found to result in no significant reduction in peak power output or VO 2max as compared to placebo, despite a 14% reduction in peak heart rate. 99
In the same study, 100 mg of atenolol (also a beta-1 selective blocker) was shown to result in a 25% reduction in maximum heart rate, and 5% reduction in both peak power output and VO 2max , leading the authors to conclude that the lack of impact on performance of nebivolol may have been due to the lesser impact on peak heart rate at the prescribed dose, or perhaps the vasodilatory effects of nebivolol.
At a dose of 240 mg/day, chronic administration of propranolol (a non-selective beta blocker) in untrained healthy subjects has been shown to reduce peak heart rate by 25%, VO 2max by 7.5% and maximum work load by 5%. 100
Sotalol (non-selective beta blocker) has been shown to have a dose-dependent reduction on maximum heart rate, with the reduction ranging from a 4% at a dose of 160 mg/24 h to 25% at 640 mg/24 h. 101
A similar dose-dependent relationship with heart rate reduction has also been demonstrated for propranolol (another non-selective agent), with marked individual variability. 102
Flecainide is a Class 1c antiarrhythmic used for the suppression of supraventricular and ventricular arrhythmias. It is commonly prescribed preferentially in athletic populations over beta-blockers due to the commonly held notion that it does not affect resting heart rate nor exercise performance, and also by the fact that it is an alternative treatment option not prohibited according to the WADA Prohibited List. Flecainide may be used regularly or as a ‘pill in the pocket’ for athletes with sympathetic- and vagal-mediated paroxysmal atrial fibrillation in the absence of structural heart disease. 103
Whilst flecainide does not lower resting heart rate, it’s effect on exercise heart rate was documented in a placebo double-blinded trial of 24 non-athletes, in whom exercise heart rate was reduced even at low-intensity exercise levels on a dose of 200 mg/day, with a difference of around 15 b.p.m. (9%) at peak exercise, despite no significant reduction in exercise time. 104
Although maximum heart rate is not a surrogate for exercise capacity, there does appear to be a threshold of around 15% heart rate reduction beyond which exercise performance would be expected to be reduced, and individual variability in the dose-heart rate response. Therefore, when prescribing beta-blockers and antiarrhythmics in athletes a TUE is needed in certain type of sports and, it is prudent to perform maximal exercise tests before prescription and during up-titration of therapy to guide exercise prescription and expectations. For more specific recommendations on anti-arrhythmic prescription and use in exercising individuals, the reader is suggested to refer to the ‘Recommendations for participation in leisure-time physical activity and competitive sports of patients with arrhythmias and potentially arrhythmogenic conditions. A position statement of the Section of Sports Cardiology and Exercise from the European Association of Preventive Cardiology (EAPC) and the European Heart Rhythm Association (EHRA), both associations of the European Society of Cardiology’. 105 , 106
Anti-coagulants and antiplatelets
One of the most important topics in the management of the athlete in treatment with anti-coagulants is the haemorrhagic risk during physical activity caused by traumas or collision with opponents, thus mostly in team sports and sports with a high intrinsic traumatic risk.
It is worth reminding that in subjects treated with vitamin K antagonists (VKAs), like acenocoumarin (Sintrom ® ) and warfarin (Coumadin ® ), an increase in the training intensity or volume can affect the international normalized ratio (INR) values.
VKA achieve their anticoagulant effect by interfering with several coagulative factors like II, V, VII, and IX. Their metabolism is significantly affected by substances acting on cytochrome (CYP) P450. VKA require periodic INR control and have a delayed and prolonged effect that lasts even after suspension.
Another class of anti-coagulants is made of new oral anti-coagulants (NOACs). NOACs are thrombin selective inhibitors (Dabigratan) or of the activated X Factor (Rivaroxaban, Apixaban, and Edoxaban).
It is still unknown if the NOAC’s effect is influenced by exercise intensity and volume.
NOACs have a short half-life and they are metabolized mostly through renal and hepatic excretion, therefore have a better and safer efficacy profile.
Given their pharmacokinetics, bioavailability, efficacy, and safety NOACs should be preferably prescribed in physically active and exercising subjects.
Furthermore, NOACs have very mild interactions with cardiovascular drugs, like atorvastatin, verapamil, diltiazem, quinidine, amiodarone, and dronedarone.
Having only recently been introduced, long-term therapy effects still require further investigation, in particular for the possible drug–drug interactions and the inhibiting or promoting effect on CYP3/A/4, which is directly involved in the hepatic clearance, for example, of rivaroxaban and apixaban. There is a paucity of long-term data about NOAC’s risk/benefit profile in the clinical management of athletes.
The most commonly used antiplatelet drugs include aspirin, clopidogrel (Plavix ® ), prasugrel (Efient ® ), and ticagrelor (Brilique ® ). Just like anti-coagulants, antiplatelet medications increase the haemorrhagic risk, particularly in physically active individuals that might be involved in contact sports or sports with a higher intrinsic risk of injury.
When establishing the individual risk, it is important to consider also other age-related cardiovascular diseases that might increase the likeliness of cardiovascular events such as coronary artery disease, hypertension, and atrial fibrillation. In this group of patients, anticoagulants and antiplatelet drugs reduce the risk of cardiovascular events but at the same time increase the risk of exercise-related and spontaneous haemorrhagic events. Thus, when prescribing this drug category to the exercising subject, several factors need to be addressed:
coexisting cardiovascular disease (in case of atrial fibrillation the CHA 2 DS 2 -VASc score), and
type and intensity of the physical activity practiced.
More detailed information on intensity and exercises prescription can be found in the recently published ‘2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease’. 107
Psychoactive drugs
Benzodiazepines.
Benzodiazepines differ among one another for kinetics, metabolic path, and active metabolites and should not be taken for a period exceeding 3–4 weeks because of the risk of tachyphylaxis and addiction. Chronic use can cause nocturnal hypoventilation, with a decrease in tissue oxygenation and clinical consequences. Particular attention should be paid to symptoms occurring after withdrawal of the agents (withdrawal syndrome):
In drugs with a short/medium half-life ( t 1/2) like triazolam, the withdrawal syndrome is more likely to occur once the treatment is interrupted while it rarely appears after cessation of drugs with a long t 1/2.
Withdrawal syndrome is virtually absent with molecules such as zolpidem and zopiclone.
Symptoms arise proportionally to t 1/2 (e.g. 24 h for lorazepam, 3–7 days for diazepam).
Withdrawal syndrome can cause
○ arrhythmic episodes such as
(1) sinus tachycardia,
(2) atrial fibrillation and atrial flutter,
(3) supra- and ventricular cardiac ectopy, and
○ atrial pressure abnormalities such as
(1) systolic hypertension,
(2) orthostatic hypotension,
(3) symptoms of sympathetic hyperactivity with diaphoresis, agitation, anxiety, tremors, and delirium.
A beta-blocker treatment is common in case of withdrawal syndrome. 108
Antidepressants and antipsychotics
Classic anti-depressant tricyclics (ADTs) are non-selective inhibitors of serotonin and noradrenaline reuptake. They can cause cardiotoxicity through different mechanisms, leading to impaired cardiac contractility and arrhythmias. 109
The most common effects, usually depending on the dose, are QRS enlargement, atrioventricular (AV) blocks to different extents, QT lengthening, and negative inotropic effect with a reduction in the ejection fraction.
They can also cause, especially in older athletes, Raynaud’s phenomenon, orthostatic hypotension, and sinus tachycardia and bradycardia.
Some antidepressants and antipsychotics might cause: QT lengthening with the torsadogenic risk of producing long QT syndrome, ventricular arrhythmias, and sudden death.
The risk is intended on the base of the single drug or attendant factors such as age, underlying pathology, hypokalaemia, and drugs coadministration.
These drugs are ADT: amitriptyline, amoxapine, clomipramine, desipramine, doxepin, imipramine, nortriptyline, trimipramine, and other antidepressants such as: citalopram, fluoxetine, sertraline (see the following section on selective serotonin reuptake inhibitor), amoxapine, venlafaxine, and doxepin.
Not all antidepressants cause QT lengthening, and the torsadogenic risk increases with higher doses or when drugs are co-administered (e.g. antiarrhythmics, antihistamines, stimulants, antibiotics and antimycotics). It might be also due to familial aggregation, as in 10% of cases. 110 Typical antipsychotics (chlorpromazine, pimozide, thioridazine, perphenazine, trifluoperazine, haloperidol, and droperidol) and atypical antipsychotics (clozapine, quetiapine, risperidone, sultopride, ziprasidone, and loxapine) are more likely to cause QT lengthening and torsade des pointes. However, the group of atypical antipsychotics is actually less hazardous.
Electrocardiograms (ECGs) show that some ADTs (amitriptyline, desipramine, and nortriptyline), other antidepressants (maprotiline and lithium) and some antipsychotic drugs (trifluoperazine and loxapine), might cause even highly arrhythmic Brugada like type 1 and coved type syndrome. This is more frequent in familial aggregation cases (associated with Na channel mutation, SCN5A). 110 , 111
The choice, initiation and continuation of an antidepressant and antipsychotic therapy require a careful ECG evaluation (PR, QRS, QTc, ventricular repolarization specific and non-specific alterations, bradycardia and supra- and ventricular arrhythmias).
Anti-epileptic drugs
Athletes might need prolonged anti-epileptics drug treatment and these drugs might have pharmacokinetic interactions with other drugs. The list of anti-epileptic drugs includes sodium valproate, phenytoin, gabapentin, lamotrigine, levetiracetam, oxcarbazepine, tiagabine, topiramate, vigabatrin, zonisamide, and carbamazepine. Treatment with anti-epileptic drugs in athletes should be always reported and plasma levels measured. Serial ECGs are necessary to verify tolerance to therapy and, as asymptomatic bradyarrhythmia and nocturnal AV block can occur, Holter monitor might be needed.
Anti-inflammatory drugs
The use of non-steroidal anti-inflammatories is more common in elite athletes than in non-athlete peers and this is mostly for pain and inflammation control reasons. 112 , 113 These drugs may cause:
delayed tissue regeneration,
gastrointestinal complications (gastralgia, heartburn, haemorrhage, alvus disorders),
disorders of the central nervous system (fatigue, headache, decreased perception of muscle strength),
decreased renal blood flow resulting in decreased kidney function (indomethacin, celecoxib), and
cardiovascular risks (cyclooxygenase inhibitor, Cox-2). There is evidence that the cyclooxygenase-2 inhibitors may increase cardiovascular risk, like hypertension and atherosclerotic lesions. However, the mechanisms for this potentially adverse cardiovascular effect are unknown. 114 , 115
The use of legal ergogenic aids is widespread in athletic populations and varies between 40% and 100% of athletes of both sexes, depending on the sport discipline and the level of competition. These supplements are intended to enhance performance and give a competitive edge. Many elite athletes consume a combination of supplements per day and various forms of sports supplements as well as vitamin/mineral supplements (VMS), which are generally the most used legal ergogenic aids. 116 Among VMS consumers, the most frequent types are multivitamins/multiminerals, vitamin C, vitamin D, and iron, with considerable variations in frequency according to countries. The reasons leading athletes to consume VMS also vary according to country, gender and the type of sports performed. The most common reasons are to optimize or enhance performance (most frequent in males) or to compensate for possible deficiencies (most frequent in females); other reasons include improvement of immune status, general health maintenance, or to reduce cold symptoms. 117
Numerous factors may be responsible for manifestation of adverse effects in athletes using nutritional aids, such as the safety and composition of the supplement per se and the used protocols of intake. Often, athletes take simultaneously various products without regard to optimal dose schemes and total dosage of some ingredients or synergic and antagonistic interactions between them. 116 Thus, some commonly used nutritional aids may lead to health disorders and in limited cases to adverse cardiovascular side effects ( Table 2 ).
Adverse cardiovascular effect of common legal nutritional supplements in sports 65–70 , 74 , 75 , 77
The legal nutritional supplements which are permitted by WADA and that are supported by reliable evidence of promoting athletes’ physical performance include caffeine, creatine, carbohydrate drinks/gels/bars, β-alanine, bicarbonate, nitrate (beetroot juice), and proteins. 117 , 118
Coffee with its ergogenic ingredient caffeine, a trimethylxanthine, is probably the most often consumed beverage worldwide. Caffeine is an adenosine antagonist, acts as a non-selective PDE inhibitor and prompts the secretion of catecholamines, 18 , 119 Caffeine acts as a sympathetic stimulus during exercise and has been shown to attenuate autonomic recovery post-exercise. It was suggested that this effect is dose-dependent. 120
Caffeine alone has been shown to be effective for the improvement of aerobic capacity in endurance athletes 119 but the ‘more is better’ philosophy, when applied to caffeine use in sports, may result in side effects that outweigh the performance benefits. Optimal performance benefits are usually achieved with intakes of 3–6 mg/kg (approximately 2–4 cups) and side effects become more common with caffeine doses over 9 mg/kg of body mass. Overdose may lead to cardiotoxicity with significant cardiovascular side effects such as tachycardia, coronary and peripheral vasoconstriction, and elevated blood pressure especially in caffeine-naive recreational athletes. 121 Hypertensive episodes, hypokalaemia, paroxysmal arrhythmias, and SCD have also been reported. 122 , 123 Additionally, vigorous exercise may exacerbate the known pharmacodynamic effects of caffeine. 18 , 121 , 124
Creatine has become the most popular non-stimulant legal ergogenic supplement in sports since early 1990s and it first gained popularity after the Barcelona Olympic Games in 1992, where medal winners in sprint and power disciplines publicly announced that they believed their performance had benefitted from its use. 125 Creatine is found predominantly (95%) in skeletal muscle tissue, and it is also synthesized in the liver, pancreas, and kidneys. It is reported that supplementation increases performance in anaerobic activities, delays muscle fatigue for short periods of time and contributes to the rapid resynthesis of adenosine triphosphate particularly in repeated short sprints of maximal intensity. 123 Creatine can be an effective legal ergogenic aid mostly when used for simple anaerobic exercise bouts of short duration and maximal effort. 119 , 123 Adverse effects are few and dose-dependent, including weight gain (1.6–2.4 kg), muscle cramps, gastrointestinal discomfort, and dehydration. There have been two case reports of transient renal function compromise referring to a significant loss of glomerular filtration rate and an interstitial nephritis, respectively. 125 To date, there are no well-established adverse cardiovascular effects or major cardiovascular toxicities. However, case reports have associated creatine supplementation with the presentation of deep-vein thromboses, atrial fibrillation, cardiac arrhythmia, chest pain, and even sudden death. 126 In the absence of definitive data, its use should be monitored carefully since relevant studies were mostly short-term and pertained to healthy individuals. The long-term effects of creatine supplementation, or any possible effects on other creatine-containing tissues such as the cardiac muscle have not yet been clarified. 125
Carbohydrates
The increased total thermal load determined by the environmental temperature and evaporative power as well as by the exercise intensity and duration justify the appropriate use of fluid carbohydrate supplements for energy intake, water and electrolyte replacement in continuous efforts predominantly lasting over 1 h. Carbohydrates as supplements usually refer to multiple transportable carbohydrates (such as glucose and fructose) and are often consumed in the form of isotonic sport drinks, gels, or energy bars. Health disorders include mainly gastrointestinal discomfort and no adverse cardiovascular effects have been reported. 127 Interestingly, the excessive consumption of grapefruit juice may lead to QT prolongation, which can cause arrhythmias, especially after the simultaneous administration of drugs that cause a prolongation of repolarization. 18
β-alanine as a supplement leads to enhanced intracellular muscle-buffering capacity increasing the level of carnosine by 40–80% in skeletal muscle. Carnosine is considered as a pH regulator in sarcoplasm delaying muscle fatigue, and β-alanine is reported to present an ergogenic effect in efforts lasting 1–4 min of maximal intensity. 128
Several studies and meta-analyses have shown that oral supplementation with β-alanine can improve human performance of high-intensity and intermittent exercise patterns. 129–131 Beta-alanine supplementation has been shown to increase carnosine levels in brain and cardiac tissue. 132 Moreover, β-alanine may increase heart rate training threshold.
Studies of adverse cardiovascular effects in humans taking oral β-alanine supplements are lacking. However, neurotoxicity, myotonia, transient paresthaesia (numbing in the skin), 133 and respiratory discomfort are clinical symptoms in humans with mitochondrial disorders associated with β-alanine plethora, and in vitro studies in which rat cardiomyocytes and fibroblasts were directly exposed to β-alanine, oxidative stress, and cell apoptosis were reported. 134 Therefore, it seems plausible that increased supplementation may have unfavourable cardiovascular effects.
Currently, β-alanine supplementation is legal under the WADA code and its use among athletes is widespread, with a self-reported usage of 60% in some sports. 135
Sodium bicarbonate
Sodium bicarbonate (NaHCO 3 ) has been suggested as a performance enhancing nutritional supplement by reducing acidosis during exercise of moderate duration and high intensity. Bicarbonate may cause gastrointestinal disorders when ingested. This can impair rather than improve sports performance and may counteract the benefits of other supplements taken at the same time. No cardiovascular side effects have been reported. 136
Oral supplementation with inorganic nitrate results in increased levels of nitric oxide thus promoting vasodilation and oxygen supply to the skeletal muscles and enhanced mitochondrial enzyme activity in endurance efforts. Thus, it is reported that intake of sodium nitrate or beetroot juice shows ergogenic effects on cardiorespiratory endurance that would benefit aerobic performance. 137 , 138 Moreover, it is noted that it may be also significantly effective in patients with cardiovascular diseases, and it should not only be addressed in healthy populations. 139 The lowering effect on blood pressure has led to the suggestion that beetroot juice could potentially be used in medical settings as an alternative to conventional anti-hypertensive drugs. 140 In sport populations, no cardiovascular side effects of nitrate supplementation have been reported although nitrates may be associated with a rapid and significant lowering of blood pressure, including syncope. Besides, further research should be conducted regarding the long-term effects since there are joint biochemical pathways in the metabolism of nitrates and the malignant nitrites.
High-quality whey protein supplementation (approximately 0.4–0.5 g/kg of lean body mass) increases muscle mass and strength during resistance-type exercise training when ingested both pre-and post-exercise within about 4–6 h of each other, depending on meal size. 141 , 142 No cardiovascular side effects have been reported in athletes. Nevertheless, the need for appropriate water intake during periods of protein consumption should be encouraged to counteract any risk of dehydration.
Alcohol is the oldest social beverage and is unlikely to have any ergogenic effect on human performance. Therefore, it is currently not listed on the WADA Prohibited List although is banned in some sports according to the rules of the sport for safety reasons, such as in motor racing. Initially, alcohol consumption may lead to an increase of heart rate, respiratory frequency, and blood pressure as well as to minimal vasodilation with a dose–response pattern. 8 In cases of heavy drinkers, hypertension, stroke, alcoholic cardiomyopathy, coronary events, cardiac arrhythmias such as atrial fibrillation have been reported. 143 Moreover, in chronic heavy-drinking, occurrence of hypertriglyceridaemia, tachycardia, and coronary spasm can increase the risk for ischaemic heart disease and SCD ( Figure 2 ). 8 , 143

Performance enhancing effects for doping substances and drugs. The figure summarizes the main performance enhancing effects of the most relevant different substance’s categories. SARM, selective androgen receptor modulators.
Nicotine and tobacco products
The use of numerous tobacco products and diverse smokeless alternatives in sports is increasing. Nicotine is a naturally occurring alkaloid and one of the most widely used psychostimulants. Athletes use nicotine either in a smokable form or during a sporting event in the form of gum (smokeless tobacco), chewable tobacco, or oral-dispersible nicotine strips or pouches, because of its psychokinetic effect. 144 Nicotine is not typically a truly ergogenic aid in terms of maximizing sports performance. However, it is reported that nicotine may improve time to exhaustion even in anaerobic bouts of exercise 144 while it seems to exert similar effects in endurance efforts as caffeine. 145 Nevertheless, it is well known that nicotine causes intense adrenergic stimulation and vasoconstriction of coronary artery segments and abuse may lead to atherosclerosis, dyslipidaemia, and cardiovascular events. 8 , 18 , 124 It also decreases cardiac contractility and output, possibly alter coronary blood flow, and may contribute to endothelial dysfunction that precipitates acute ischaemic events. 146 Moreover, nicotine has thrombogenic actions resulting in augmented coagulability. 145 Thus, tobacco use should be clearly discouraged and certainly avoided for 2 h before and after a sports event or training practice. 8
Energy drinks
The World Health Organization has named the use of energy drinks as a public health concern. 147 Energy drinks are non-alcoholic beverages containing predominantly caffeine in combination with other presumed energy enhancing ingredients that act mainly as stimulants and they are commonly consumed particularly by adolescents and young adults. 121 , 148 The most common ingredients are caffeine, guarana, taurine, glucuronolactone, ginseng, and bitter orange. Energy drinks and energy shots (concentrated form of energy drink) contain higher quantities of caffeine than conventional beverages and coffee products, and their caffeine concentration can range from 9 to 250 mg/oz. 121 Consumption of a caffeine, taurine, and glucuronolactone formulation may increase arterial blood pressure, act as a platelet aggregation enhancing factor and compromise endothelial function in healthy individuals. 148 Furthermore, it is reported that in vitro , taurine acts as a triggering factor for enhanced haemodynamic outcomes presenting both a positive inotropic effect and potentiated caffeine-induced cardiac muscle contraction. 149 Combination with alcohol is common, with many consumers self-mixing energy drinks or energy shots with alcohol. This usage does not counteract alcohol-induced motor coordination deficits and individuals who mix energy drinks with alcohol may underestimate their true level of impairment. 150 Depending on the product and the number of units imbibed, ingested caffeine dose can easily rise over 1000 mg. In healthy adults, a caffeine intake of less than 400 mg per day is typically safe. Acute toxicity-derived effects begin at 1000 mg, and 5000–10 000 mg can be lethal. 121
Numerous environmental, genetic, and medical settings may predispose individuals to the toxic caffeine effects of energy drinks or shots. 121 Moreover, energy shots may be more hazardous since significant increases in both systolic and diastolic blood pressure, lasting up to 6 h after intake have been noted. 151 According to the International Society of Sports Nutrition, the action and the side effects of energy drinks should be clarified since there is a variety of ingredients. The intake of more than a can may lead to side effects and patients should consume only under medical advice. 152 Energy drinks put individuals with genetic heart condition at risk and it is suggested that drinking two cans of an energy drink increases risk of cardiac arrest by 20% in people with an underlying heart condition such as in patients with long QT syndrome. 153 Cardiovascular side effects of energy drink use include increased blood pressure, coronary disease, heart failure, cardiac arrhythmias, abnormal exercise test, increased risk of atrial fibrillation, narrow complex tachycardia, prolonged QT interval, ventricular tachycardia, ventricular fibrillation, torsade des pointes, supraventricular arrhythmias, ST-segment elevation, hypokinesia with or without a reduced LV ejection fraction, and aortic dissection. 154 Furthermore, the mixture of alcohol with energy drinks may lead to severe cardiovascular disorders. 147 , 155 , 156 Children or adolescents should only consider using energy drinks with parental approval, and parents should be aware of potential adverse effects. The younger brain is more susceptible to excessive energy drink consumption and a high risk for disturbed neurodevelopment in children and adolescents has also been reported. 157 Additionally, individuals with underlying cardiovascular pathology should avoid energy drinks unless approved by their physician.
Synthetic peptides
Modern performance enhancing drugs can be designer synthetic peptides triggering stimulation of natural anabolic hormone secretion. However, of possibly far greater potential risk than using AAS or other prohibited drugs is athletes’ desire and consent to use experimental drugs that have not been proven safe in humans. 158 The ongoing use of SARMs like ostarine, ligandrol, andarine, and cardarine claiming anabolic to androgenic ratios high up to 90:1 or peptides like ipamorelin (growth hormone secretagogue) carry a substantial risk for long-term detrimental health consequences, which are usually understated by their promoters. Little is known about the cardiovascular side effects of the many peptides designed to modulate AR activity as it was previously reported in this paper. It is likely that side effects are less than AAS, but it is very difficult to know for certain. 3 Thus, in some respect, confirmation of biomedical side effects is always going to be one step behind use and not surprisingly, no cardiovascular side effects have been reported so far.
Furthermore, the HIF-proly hydroxylase inhibitors (i.e. cobalt, daprodustat, molidustat, roxadustat, enarodustat, vadadustat, xenon) are basically modern erythropoiesis-triggering agents and they are used in sports alternatively to injectable erythropoietin. The study of their cardiovascular effects is still ongoing mainly in vitro . 159 Besides, natural compounds like phytoekdysteroids or PDE5 inhibitors are also used in sports and PDE5 inhibitors are alleged to be frequently misused by healthy athletes to improve sporting performance. 160 Finally, the implementation of gene doping constitutes a great threat of major concern about the future of human performance manipulation.
Gene doping
Gene doping (WADA prohibited method) includes the use of normal or genetically modified cells as well as gene transfer, gene silencing and gene editing technologies. There are not yet any data about complications, as might be expected considering that officially there are no confirmed adverse analytical findings of gene doping in sports. Gene doping abuses the legitimate approach of gene therapy in analogue medical protocols. Over 200 genes are associated to human performance and play a role in muscle development, oxygen delivery to tissues, neuromuscular coordination, or even pain control, and are thus candidates for gene dopers. 161 The expected severe health side effects include lethal immunodeficiency and leukaemia. 162 Health risks may also result from gene overexpression, a common problem in gene therapy. IGF gene doping may be used for muscle repair and muscle performance. IGF-overexpression may cause cardiac hypertrophy, heart valve disease, and heart failure. 162–164 Additionally, increasing EPO levels may increase viscosity and the risk for heart attack. 165 Moreover, it is highly anticipated that genes for strength, analgesia, oxygen delivery, and tissue repair may be transferred simultaneously to the same athlete. Clearly, there will be hazardous side effects and probably severe gene interactions. Contrary to therapeutic gene protocols that are conducted under strict regulations and approval procedures, gene doping is expected to occur behind the scenes with limited protective actions and consequently increased health risks. Furthermore, since 2018, the WADA list also includes gene editing as agents designed to alter genome sequences and/or the transcriptional or epigenetic regulation of gene expression . Gene editing with genome editing tools such as CRISPR (clustered regularly interspaced short palindromic repeats) 166 involves tweaking existing genes, rather than adding completely new ones to the athlete’s body. Gene editing should make it possible to make tiny alterations to DNA in existing genes, or to just temporarily boost or switch off the activity of particular genes. Additionally, these effects could be oriented to specific tissues such as muscle, meaning the changes may not show up in blood anti-doping tests. However, it seems that there will always be the increased risk of mutation genesis and formation of malignant cells as well as unexpected side effects due to atypical regulation of cell growth and toxicity based on chronic hyper-expressions of growth factors and cytokines even affecting the cardiovascular function. 167
The indiscriminate use of nutritional supplements and legal ergogenic aids in sports is a cause for concern. Nutritional supplements are commonly viewed as risk-free substances that may improve performance. Nutritional supplements, however, that have the potential to enhance human performance may also have biomedical side effects. Some nutritional supplements, including various plant and ‘natural’ extracts, may pose a serious health risk and athletes may even risk contravening anti-doping rules. Moreover, contamination of supplements with unknown or prohibited substances remains a significant issue, with contamination rates reported between 12% and 58%. 116 , 168 Supplements widely available like fat-burners or products based on plant extracts may trigger cardiovascular disorders if contaminated with ephedra or ephedra-like compounds, which is also a common cause of unintended anti-doping rule violations.
Athletes who use supplements often have no knowledge regarding their effects on sports performance and overall health. It is reported that most athletes get nutritional advice from coaches, fellow athletes, family members and friends, 169 suggesting that more wide reaching educational interventions, at an early age, are necessary. Athletes, particularly at the higher echelons of sport, should consider consulting nutritional experts who will consider the need, potential benefits, as well as side-effects of supplements and provide an individually tailored prescription. 116 Examples when nutritional supplements may be indicated include (i) specific nutrient deficiencies; (ii) clinical manifestations due to chronic inadequate nutrient intake; (iii) low-calorie diets or diets excluding a group of nutrients either voluntarily, e.g. vegetarians/vegans or due to allergies or food intolerance; (iv) regular travelling with uncertain/insufficient food supply or quality; and (v) periods of extreme training loads and increased energy expenditure.
Key points for athletes using nutritional supplements
A natural supplement is not necessarily a safe supplement.
Use supplements if needed for known deficiencies and recommended by nutrition experts.
Use products by established manufacturers with known good quality standards.
Athletes are personally responsible for any substances they consume.
Ignorance is not accepted as an excuse in relation to a positive doping test.
Athletes with established heart disease should be even more vigilant and consult with their physician prior to using any supplements or ergogenic aids.
The basis of using doping substances is like that of nutritional supplements used as ergogenic aids in sports, since in both cases the objective is to improve physical performance. Athletes should be aware that supplement use exposes them to a risk of ingesting prohibited substances or prohormones and precursors of prohibited substances. Supplements are regulated as food ingredients and are not subject to the stringent regulations applied to pharmaceutical products. 116 The greatest risk to athletes’ health is the use of ‘cocktails’ and transference of effects of several substances, which might interact to the worse or the use of designer peptides produced in laboratories without rigorous safety standards. Unfortunately, it is common practice for athletes to ignore dosing recommendations and use multiple drugs simultaneously. Another aspect of consideration about ergogenic aids in sports is that when using nutritional ergogenic supplements to push physiological adaptations beyond normal under an extreme training load, supra-physiological structural and functional changes may be apparent. In this case, the induced stress reaction with high catecholamines release triggering cardiovascular response may lead to cardiovascular disorders such as atrial fibrillation or even more threatening arrhythmias. 3
Anti-doping authorities may claim that they increase the penalties for anti-doping rule violations or have developed new anti-doping strategies based on increased number of anti-doping tests and sophisticated reliable methods for detection of doping substances. Besides, regarding the claims that underestimate the health side effects and mention that doping will always exist in sports and it could be eventually allowed, we should foresee that (i) clinical trials establishing a safe level of intake would not exist for all probable dosage schemes, and (ii) the concept of sporting fairness would be challenged due to financial burden. Furthermore, the core of sports culture should always be the athlete and not the pharmacist or the geneticist.
Prescribing physicians should familiarize themselves with the status of a prescribed medication under the WADA anti-doping code, although the majority of the supporting information sources provides information about the prohibited drugs based on the current WADA Prohibited List, but does not provide the status of nutritional substances due to the fact many are unregulated and unlicensed. 158 Usually, these tools (electronic databases and official websites) provide specific information on products sold in just a limited number of countries. Undoubtedly, it needs to be recognized that physicians should be actively part of the fight against doping and should only prescribe or recommend supplements where a clinical need can be demonstrated, such as in vitamin deficiency syndromes. 170 Moreover, physicians should always discuss with the athletes to inform them about the potential risks of taking supplements. The important role of athletic coaches, equally or even more than dieticians and physicians, in providing nutritional information should be also noted. Therefore, there is a considerable need for well-educated coaches in collaboration with dieticians and doctors to provide an adequate nutritional support for athletes. Regarding young athletes, it should be noted that paediatricians are the primary contact for most young athletes and paediatric cardiologists are in a position to develop long-lasting relationships with their patients. Therefore, it is of great importance for paediatric physicians to be aware that drug use in sports is not only an adult problem.
An athlete guided by a strong ‘will to win’ may be vulnerable to cheating practices to satisfy his goals and society’s expectations. Doping within this pursuit of sports success is a multi-dimensional issue and the fight against arbitrary use of ergogenic aids in professional and recreational sports should involve all stakeholders of the modern sport system: athletes, clubs, scientists, spectators, sponsors, media, family, and official authorities. 170 Physicians need to become more educated about the drugs that are being used in sports and their side effects. It is essential to have a physician who will be perceptive to the potential for drugs abuse, well informed and able to discuss openly the ergogenic and the adverse effects of nutritional supplements and drugs. 125 Athletes with established heart disease should be even more vigilant and regularly consult with their physician prior to using any supplements or ergogenic aids. More research studies on biomedical side effects and educational campaigns particularly aiming at physicians, children, and athletes of developmental ages can have a significant influence on drug use in sports and may act as the most powerful tools for an effective fight against the indiscriminate use of ergogenic aids.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Kent M. The Oxford Dictionary of Sports Science & Medicine . 3rd ed. Oxford, UK: Oxford University Press ; 2007 .
Google Scholar
Google Preview
WADA World Anti-Doping Agency. World Anti-Doping Code International Standard Prohibited List 2021 . Montreal, Quebec, Canada : World Anti-Doping Agency ; 2020 . https://www.wada-ama.org/sites/default/files/resources/files/2021list_en.pdf (20 May 2021).
La Gerche A , Brosnan MJ. Cardiovascular effects of performance-enhancing drugs . Circulation 2017 ; 135 : 89 – 99 .
Gleaves J , Petróczi A , Folkerts D , De Hon O , Macedo E , Saugy M , Cruyff M. Doping prevalence in competitive sport: evidence synthesis with “best practice” recommendations and reporting guidelines from the WADA Working Group on Doping Prevalence . Sports Med 2021 ; 51 : 1909 – 1934 .
Bojsen-Møller J , Christiansen AV. Use of performance- and image-enhancing substances among recreational athletes: a quantitative analysis of inquiries submitted to the Danish anti-doping authorities . Scand J Med Sci Sports 2010 ; 20 : 861 – 867 .
WADA World Anti-Doping Agency. World Anti-Doping Agency Testing Figures Report . 2021 . https://www.wada-ama.org/en (1 July 2021).
Kolliari-Turner A , Lima G , Hamilton B , Pitsiladis Y , Guppy FM. Analysis of anti-doping rule violations that have impacted medal results at the summer olympic games 1968–2012 . Sports Med 2021 ; 51 : 2221 – 2229 .
Deligiannis A , Björnstad H , Carre F , Heidbüchel H , Kouidi E , Panhuyzen-Goedkoop NM , Pigozzi F , Schänzer W , Vanhees L ; on behalf of the ESC Study Group of Sports Cardiology. ESC study group of sports cardiology position paper on adverse cardiovascular effects of doping in athletes . Eur J Cardiovasc Prev Rehabil 2006 ; 13 : 687 – 694 .
Pope HG Jr , Wood RI , Rogol A , Nyberg F , Bowers L , Bhasin S. Adverse health consequences of performance-enhancing drugs: an Endocrine Society scientific statement . Endocr Rev 2014 ; 35 : 341 – 375 .
Albano GD , Amico F , Cocimano G , Liberto A , Maglietta F , Esposito M , Rosi GL , Di Nunno N , Salerno M , Montana A. Adverse effects of anabolic-androgenic steroids: a literature review. In: Healthcare , 2021 . Abstract 9, p.97. Basel, Switzerland: Multidisciplinary Digital Publishing Institute .
Bhasin S , Storer TW , Berman N , Callegari C , Clevenger B , Phillips J , Bunnell TJ , Tricker R , Shirazi A , Casaburi R. The effects of supraphysiologic doses of testosterone on muscle size and strength in normal men . N Engl J Med 1996 ; 335 : 1 – 7 .
Forbes GB , Porta CR , Herr BE , Griggs RC. Sequence of changes in body composition induced by testosterone and reversal of changes after drug is stopped . JAMA 1992 ; 267 : 397 – 399 .
Cardinale DA , Horwath O , Elings-Knutsson J , Helge T , Godhe M , Bermon S , Moberg M , Flockhart M , Larsen FJ , Hirschberg AL , Ekblom B. Enhanced skeletal muscle oxidative capacity and capillary-to-fiber ratio following moderately increased testosterone exposure in young healthy women . Front Physiol 2020 ; 11 : 585490 .
Giorgi A , Weatherby RP , Murphy PW. Muscular strength, body composition and health responses to the use of testosterone enanthate: a double blind study . J Sci Med Sport 1999 ; 2 : 341 – 355 .
Hirschberg AL , Elings Knutsson J , Helge T , Godhe M , Ekblom M , Bermon S , Ekblom B. Effects of moderately increased testosterone concentration on physical performance in young women: a double blind, randomised, placebo controlled study . Br J Sports Med 2020 ; 54 : 599 – 604 .
Achar S , Rostamian A , Narayan SM. Cardiac and metabolic effects of anabolic-androgenic steroid abuse on lipids, blood pressure, left ventricular dimensions, and rhythm . Am J Cardiol 2010 ; 106 : 893 – 901 .
Torrisi M , Pennisi G , Russo I , Amico F , Esposito M , Liberto A , Cocimano G , Salerno M , Li Rosi G , Di Nunno N , Montana A. Sudden cardiac death in anabolic-androgenic steroid users: a literature review . Medicina 2020 ; 56 : 587 .
Deligiannis AP , Kouidi EI. Cardiovascular adverse effects of doping in sports . Hellenic J Cardiol 2012 ; 53 : 447 – 457 .
Perry JC , Schuetz TM , Memon MD , Faiz S , Cancarevic I. Anabolic steroids and cardiovascular outcomes: the controversy . Cureus 2020 ; 12 : e9333 .
Baggish AL , Weiner RB , Kanayama G , Hudson JI , Lu MT , Hoffmann U , Pope HG Jr . Cardiovascular toxicity of illicit anabolic-androgenic steroid use . Circulation 2017 ; 135 : 1991 – 2002 .
Liu JD , Wu YQ. Anabolic-androgenic steroids and cardiovascular risk . Chin Med J (Engl) 2019 ; 132 : 2229 – 2236 .
Chang S , Münster AB , Gram J , Sidelmann JJ. Anabolic androgenic steroid abuse: the effects on thrombosis risk, coagulation, and fibrinolysis . Semin Thromb Hemost 2018 ; 44 : 734 – 746 .
Corona G , Maseroli E , Rastrelli G , Isidori AM , Sforza A , Mannucci E , Maggi M. Cardiovascular risk associated with testosterone-boosting medications: a systematic review and meta-analysis . Expert Opin Drug Saf 2014 ; 13 : 1327 – 1351 .
Deligiannis AP , Mandroukas K. Noninvasive cardiac evaluation of weight-lifters using anabolic steroids . Scand J Med Sci Sports 2007 ; 3 : 37 – 40 .
Far HR , Ågren G , Thiblin I. Cardiac hypertrophy in deceased users of anabolic androgenic steroids: an investigation of autopsy findings . Cardiovasc Pathol 2012 ; 21 : 312 – 316 .
Montisci M , El Mazloum R , Cecchetto G , Terranova C , Ferrara SD , Thiene G , Basso C. Anabolic androgenic steroids abuse and cardiac death in athletes: morphological and toxicological findings in four fatal cases . Forensic Sci Int 2012 ; 217 : e13 – e18 .
Baggish AL , Weiner RB , Kanayama G , Hudson JI , Picard MH , Hutter AM Jr , Pope HG Jr. Long-term anabolic-androgenic steroid use is associated with left ventricular dysfunction . Circ Heart Fail 2010 ; 3 : 472 – 476 .
Luijkx T , Velthuis BK , Backx FJ , Buckens CF , Prakken NH , Rienks R , Mali WP , Cramer MJ. Anabolic androgenic steroid use is associated with ventricular dysfunction on cardiac MRI in strength trained athletes . Int J Cardiol 2013 ; 167 : 664 – 668 .
D'Andrea A , Caso P , Salerno G , Scarafile R , De Corato G , Mita C , Di Salvo G , Severino S , Cuomo S , Liccardo B , Esposito N , Calabro R. Left ventricular early myocardial dysfunction after chronic misuse of anabolic androgenic steroids: a Doppler myocardial and strain imaging analysis . Br J Sports Med 2007 ; 41 : 149 – 155 .
Darke S , Torok M , Duflou J. Sudden or unnatural deaths involving anabolic-androgenic steroids . J Forensic Sci 2014 ; 59 : 1025 – 1028 .
D’Andrea A , Radmilovic J , Caselli S , Carbone A , Scarafile R , Sperlongano S , Tocci G , Formisano T , Martone F , Liccardo B , D’Alto M , Bossone E , Galderisi M , Golino P. Left atrial myocardial dysfunction after chronic abuse of anabolic androgenic steroids: a speckle tracking echocardiography analysis . Int J Cardiovasc Imaging 2018 ; 34 : 1549 – 1559 .
Rasmussen JJ , Schou M , Madsen PL , Selmer C , Johansen ML , Ulriksen PS , Dreyer T , Kümler T , Plesner LL , Faber J , Gustafsson F , Kistorp C. Cardiac systolic dysfunction in past illicit users of anabolic androgenic steroids . Am Heart J 2018 ; 203 : 49 – 56 .
Nottin S , Nguyen LD , Terbah M , Obert P. Cardiovascular effects of androgenic anabolic steroids in male bodybuilders determined by tissue Doppler imaging . Am J Cardiol 2006 ; 97 : 912 – 915 .
Cecchi R , Muciaccia B , Ciallella C , Di Luca NM , Kimura A , Sestili C , Nosaka M , Kondo T. Ventricular androgenic-anabolic steroid-related remodeling: an immunohistochemical study . Int J Legal Med 2017 ; 131 : 1589 – 1595 .
Alizade E , Avci A , Tabakcı MM , Toprak C , Zehir R , Acar G , Kargin R , Emiroğlu MY , Akçakoyun M , Pala S. Comparison of right ventricle systolic function between long-term anabolic-androgenic steroid user and nonuser bodybuilder athletes: a study of two-dimensional speckle tracking echocardiography . Echocardiography 2016 ; 33 : 1178 – 1185 .
Abhayaratna WP , Seward JB , Appleton CP , Douglas PS , Oh JK , Tajik AJ , Tsang TS. Left atrial size: physiologic determinants and clinical applications . J Am Coll Cardiol 2006 ; 47 : 2357 – 2363 .
Barbosa Neto O , da Mota GR , De Sordi CC , Resende E , Resende L , Vieira da Silva MA , Marocolo M , Côrtes RS , de Oliveira LF , Dias da Silva VJ. Long-term anabolic steroids in male bodybuilders induce cardiovascular structural and autonomic abnormalities . Clin Auton Res 2018 ; 28 : 231 – 244 .
Kouidi EJ , Kaltsatou A , Anifanti MA , Deligiannis AP. Early left ventricular diastolic dysfunction, reduced baroreflex sensitivity, and cardiac autonomic imbalance in anabolic–androgenic steroid users . Int J Environ Res Public Health 2021 ; 18 : 6974 .
Ghorbani Baravati H , Joukar S , Fathpour H , Kordestani Z. Nandrolone plus moderate exercise increases the susceptibility to lethal arrhythmias . Res Cardiovasc Med 2015 ; 4 : e26233 .
Marocolo M , Katayama PL , Meireles A , Barbosa Neto O. Combined effects of exercise training and high doses of anabolic steroids on cardiac autonomic modulation and ventricular repolarization properties in rats . Can J Physiol Pharmacol 2019 ; 97 : 1185 – 1192 .
Cittadini A , Berggren A , Longobardi S , Ehrnborg C , Napoli R , Rosén T , Fazio S , Caidahl K , Bengtsson BA , Saccà L. Supraphysiological doses of GH induce rapid changes in cardiac morphology and function . J Clin Endocrinol Metab 2002 ; 87 : 1654 – 1659 .
Colao A , Marzullo P , Di Somma C , Lombardi G. Growth hormone and the heart . Clin Endocrinol (Oxf) 2001 ; 54 : 137 – 154 .
Maffei P , Martini C , Milanesi A , Corfini A , Mioni R , de CE , Menegazzo C , Scanarini M , Vettor R , Federspil G , Sicolo N. Late potentials and ventricular arrhythmias in acromegaly . Int J Cardiol 2005 ; 104 : 197 – 203 .
Crist DM , Peake GT , Loftfield RB , Kraner JC , Egan PA. Supplemental growth hormone alters body composition, muscle protein metabolism and serum lipids in fit adults: characterization of dose-dependent and response-recovery effects . Mech Ageing Dev 1991 ; 58 : 191 – 205 .
Shrivastava S , Srivastava D , Olson EN , DiMaio JM , Bock-Marquette I. Thymosin beta4 and cardiac repair . Ann N Y Acad Sci 2010 ; 1194 : 87 – 96 .
Friedman RA. The changing face of teenage drug abuse—the trend toward prescription drugs . N Engl J Med 2006 ; 354 : 1448 – 1450 .
Fanoe S , Jensen G , Ege P. Proarrhythmic effect of methadone: an alternative explanation of sudden death in heroine addicts . PACE 2006 ; 29 : S30 .
Alinejad S , Kazemi T , Zamani N , Hoffman RS , Mehrpour O. A systematic review of the cardiotoxicity of methadone . EXCLI J 2015 ; 14 : 577 – 600 .
Polanczyk GV , Willcutt EG , Salum GA , Kieling C , Rohde LA. ADHD prevalence estimates across three decades: an updated systematic review and meta-regression analysis . Int J Epidemiol 2014 ; 43 : 434 – 442 .
Katselou M , Papoutsis I , Nikolaou P , Qammaz S , Spiliopoulou C , Athanaselis S. Fenethylline (captagon) abuse—local problems from an old drug become universal . Basic Clin Pharmacol Toxicol 2016 ; 119 : 133 – 140 .
Milroy CM , Parai JL. The histopathology of drugs of abuse . Histopathology 2011 ; 59 : 579 – 593 .
Hennissen L , Bakker MJ , Banaschewski T , Carucci S , Coghill D , Danckaerts M , Dittmann RW , Hollis C , Kovshoff H , McCarthy S , Nagy P , Sonuga-Barke E , Wong IC , Zuddas A , Rosenthal E , Buitelaar JK ; The ADDUCE consortium. Cardiovascular effects of stimulant and non-stimulant medication for children and adolescents with ADHD: a systematic review and meta-analysis of trials of methylphenidate, amphetamines and atomoxetine . CNS Drugs 2017 ; 31 : 199 – 215 .
Al-Imam A. Adverse effects of amphetamines on the cardiovascular system: Review and retrospective analyses of trends . Glob J Health Sci 2017 ; 9 : 102 .
Figueredo VM. Chemical cardiomyopathies: the negative effects of medications and nonprescribed drugs on the heart . Am J Med 2011 ; 124 : 480 – 488 .
Cohle SD. Fatal coronary artery intimal hyperplasia due to amphetamine use . Cardiovasc Pathol 2013 ; 22 : e1 – e4 .
Fischbach P. The role of illicit drug use in sudden death in the young . Cardiol Young 2017 ; 27 : S75 – S79 .
Morentin B , Callado LF , García-Hernández S , Bodegas A , Lucena J. The role of toxic substances in sudden cardiac death . Spanish J Legal Med 2018 ; 44 : 13 – 21 .
Roelands B , Hasegawa H , Watson P , Piacentini MF , Buyse L , De Schutter G , Meeusen RR. The effects of acute dopamine reuptake inhibition on performance . Med Sci Sports Exerc 2008 ; 40 : 879 – 885 .
Keisler BD , Hosey RG. Ergogenic aids: an update on ephedra . Curr Sports Med Rep 2005 ; 4 : 231 – 235 .
Morozova E , Yoo Y , Behrouzvaziri A , Zaretskaia M , Rusyniak D , Zaretsky D , Molkov Y. Amphetamine enhances endurance by increasing heat dissipation . Physiol Rep 2016 ; 4 : e12955 .
Dambrova M , Makrecka-Kuka M , Vilskersts R , Makarova E , Kuka J , Liepinsh E. Pharmacological effects of meldonium: Biochemical mechanisms and biomarkers of cardiometabolic activity . Pharmacol Res 2016 ; 113 : 771 – 780 .
Schobersberger W , Dünnwald T , Gmeiner G , Blank C. Story behind meldonium—from pharmacology to performance enhancement: a narrative review . Br J Sports Med 2017 ; 51 : 22 – 25 .
Stuart M , Schneider C , Steinbach K. Meldonium use by athletes at the Baku 2015 European Games . Br J Sports Med 2016 ; 50 : 694 – 698 .
Pluim BM , de Hon O , Staal JB , Limpens J , Kuipers H , Overbeek SE , Zwinderman AH , Scholten RJ. beta(2)-agonists and physical performance: a systematic review and meta-analysis of randomized controlled trials . Sports Med 2011 ; 41 : 39 – 57 .
Sears MR. Adverse effects of beta-agonists . J Allergy Clin Immunol 2002 ; 110 : S322 – S328 .
Milano G , Chiappini S , Mattioli F , Martelli A , Schifano F. beta-2 agonists as misusing drugs? Assessment of both clenbuterol- and salbutamol-related European Medicines Agency Pharmacovigilance Database Reports . Basic Clin Pharmacol Toxicol 2018 ; 123 : 182 – 187 .
Brett J , Dawson AH , Brown JA. Clenbuterol toxicity: a NSW poisons information centre experience . Med J Aust 2014 ; 200 : 219 – 221 .
Ferrua S , Varbella F , Conte M. Acute myocardial infarction due to coronary vasospasm and salbutamol abuse . Heart 2009 ; 95 : 673 – 673 .
Boucher A , Payen C , Garayt C , Ibanez H , Dieny A , Doche C , Chuniaud C , Descotes J. Salbutamol misuse or abuse with fatal outcome: a case-report . Hum Exp Toxicol 2011 ; 30 : 1869 – 1871 .
Furlanello F , Bentivegna S , Cappato R , De Ambroggi L. Arrhythmogenic effects of illicit drugs in athletes . Ital Heart J 2003 ; 4 : 829 – 837 .
Ghodse A , Galea S. O A , Narcotic Antagonists I. Side Effects of Drugs Annual . Amsterdam, The Netherlands: Elsevier ; 2010 , 183 – 224 .
Vernec A , Slack A , Harcourt PR , Budgett R , Duclos M , Kinahan A , Mjøsund K , Strasburger CJ. Glucocorticoids in elite sport: current status, controversies and innovative management strategies—a narrative review . Br J Sports Med 2020 ; 54 : 8 – 12 .
Duclos M. Glucocorticoids: a doping agent? Endocrinol Metab Clin North Am 2010 ; 39 : 107 – 126 , ix–x.
Berglund B , Hemmingson P. Effect of reinfusion of autologous blood on exercise performance in cross-country skiers . Int J Sports Med 1987 ; 8 : 231 – 233 .
Brien AJ , Simon TL. The effects of red blood cell infusion on 10-km race time . Jama 1987 ; 257 : 2761 – 2765 .
Borrione P , Mastrone A , Salvo RA , Spaccamiglio A , Grasso L , Angeli A. Oxygen delivery enhancers: past, present, and future . J Endocrinol Invest 2008 ; 31 : 185 – 192 .
Heuberger JA , Cohen Tervaert JM , Schepers FM , Vliegenthart AD , Rotmans JI , Daniels JM , Burggraaf J , Cohen AF. Erythropoietin doping in cycling: lack of evidence for efficacy and a negative risk-benefit . Br J Clin Pharmacol 2013 ; 75 : 1406 – 1421 .
Heuberger J , Rotmans JI , Gal P , Stuurman FE , van 't Westende J , Post TE , Daniels JMA , Moerland M , van Veldhoven PLJ , de Kam ML , Ram H , de Hon O , Posthuma JJ , Burggraaf J , Cohen AF. Effects of erythropoietin on cycling performance of well trained cyclists: a double-blind, randomised, placebo-controlled trial . Lancet Haematol 2017 ; 4 : e374 – e386 .
Birkeland KI , Stray-Gundersen J , Hemmersbach P , Hallen J , Haug E , Bahr R. Effect of rhEPO administration on serum levels of sTfR and cycling performance . Med Sci Sports Exerc 2000 ; 32 : 1238 – 1243 .
Wilkerson DP , Rittweger J , Berger NJ , Naish PF , Jones AM. Influence of recombinant human erythropoietin treatment on pulmonary O 2 uptake kinetics during exercise in humans . J Physiol 2005 ; 568 : 639 – 652 .
Connes P , Perrey S , Varray A , Prefaut C , Caillaud C. Faster oxygen uptake kinetics at the onset of submaximal cycling exercise following 4 weeks recombinant human erythropoietin (r-HuEPO) treatment . Pflugers Arch 2003 ; 447 : 231 – 238 .
Parisotto R , Gore CJ , Emslie KR , Ashenden MJ , Brugnara C , Howe C , Martin DT , Trout GJ , Hahn AG. A novel method utilising markers of altered erythropoiesis for the detection of recombinant human erythropoietin abuse in athletes . Haematologica 2000 ; 85 : 564 – 572 .
Garimella PS , Katz R , Patel KV , Kritchevsky SB , Parikh CR , Ix JH , Fried LF , Newman AB , Shlipak MG , Harris TB , Sarnak MJ ; Health ABC Study. Association of serum erythropoietin with cardiovascular events, kidney function decline, and mortality: the health aging and body composition study . Circ Heart Fail 2016 ; 9 : e002124 .
Rasmussen P , Kim Y-S , Krogh-Madsen R , Lundby C , Olsen NV , Secher NH , Lieshout JJ. Both acute and prolonged administration of EPO reduce cerebral and systemic vascular conductance in humans . FASEB J 2012 ; 26 : 1343 – 1348 .
Jelkmann W. Erythropoietin doping: cardiovascular effects in athletes . Ann Sports Med Res 2020 ; 7 : 1142 .
Lippi G , Franchini M , Guidi GC. Cobalt chloride administration in athletes: a new perspective in blood doping? Br J Sports Med 2005 ; 39 : 872 – 873 .
Alexander CS. Cobalt-beer cardiomyopathy. A clinical and pathologic study of twenty-eight cases . Am J Med 1972 ; 53 : 395 – 417 .
Ebert B , Jelkmann W. Intolerability of cobalt salt as erythropoietic agent . Drug Test Anal 2014 ; 6 : 185 – 189 .
Richardson RS , Tagore K , Haseler LJ , Jordan M , Wagner PD. Increased VO 2max with right-shifted Hb-O 2 dissociation curve at a constant O 2 delivery in dog muscle in situ . J Appl Physiol (1985) 1998 ; 84 : 995 – 1002 .
Suh JH , Stea B , Nabid A , Kresl JJ , Fortin A , Mercier JP , Senzer N , Chang EL , Boyd AP , Cagnoni PJ , Shaw E. Phase III study of efaproxiral as an adjunct to whole-brain radiation therapy for brain metastases . J Clin Oncol 2006 ; 24 : 106 – 114 .
La Gerche A , Claessen G. Is exercise good for the right ventricle? Concepts for health and disease . Can J Cardiol 2015 ; 31 : 502 – 508 .
La Gerche A , Heidbuchel H. Can intensive exercise harm the heart? You can get too much of a good thing . Circulation 2014 ; 130 : 992 – 1002 .
Kontaras K , Varnavas V , Kyriakides ZS. Does sildenafil cause myocardial infarction or sudden cardiac death? Am J Cardiovasc Drugs 2008 ; 8 : 1 – 7 .
Kloner RA , Goldstein I , Kirby MG , Parker JD , Sadovsky R. Cardiovascular safety of phosphodiesterase type 5 inhibitors after nearly 2 decades on the market . Sex Med Rev 2018 ; 6 : 583 – 594 .
Ghofrani HA , Reichenberger F , Kohstall MG , Mrosek EH , Seeger T , Olschewski H , Seeger W , Grimminger F. Sildenafil increased exercise capacity during hypoxia at low altitudes and at Mount Everest base camp: a randomized, double-blind, placebo-controlled crossover trial . Ann Intern Med 2004 ; 141 : 169 – 177 .
Faoro V , Boldingh S , Moreels M , Martinez S , Lamotte M , Unger P , Brimioulle S , Huez S , Naeije R. Bosentan decreases pulmonary vascular resistance and improves exercise capacity in acute hypoxia . Chest 2009 ; 135 : 1215 – 1222 .
Hsu AR , Barnholt KE , Grundmann NK , Lin JH , McCallum SW , Friedlander AL. Sildenafil improves cardiac output and exercise performance during acute hypoxia, but not normoxia . J Appl Physiol 2006 ; 100 : 2031 – 2040 .
Guidetti L , Emerenziani GP , Gallotta MC , Pigozzi F , Di Luigi L , Baldari C. Effect of tadalafil on anaerobic performance indices in healthy athletes . Br J Sports Med 2007 ; 42 : 130 – 133 .
Van Bortel LM , van Baak MA. Exercise tolerance with nebivolol and atenolol . Cardiovasc Drug Ther 1992 ; 6 : 239 – 247 .
Gullestad L , Hallen J , Medbo JI , Gronnerod O , Holme I , Sejersted OM. The effect of acute vs chronic treatment with beta-adrenoceptor blockade on exercise performance, haemodynamic and metabolic parameters in healthy men and women . Br J Clin Pharmacol 1996 ; 41 : 57 – 67 .
Funck-Brentano C , Kibleur Y , Le Coz F , Poirier JM , Mallet A , Jaillon P. Rate dependence of sotalol-induced prolongation of ventricular repolarization during exercise in humans . Circulation 1991 ; 83 : 536 – 545 .
Coltart DJ , Shand DG. Plasma propranolol levels in the quaniitative assessment of beta-adrenergic blockade in man . Br Med J 1970 ; 3 : 731 – 734 .
Turagam MK , Flaker GC , Velagapudi P , Vadali S , Alpert MA. Atrial fibrillation in athletes: Pathophysiology, clinical presentation, evaluation and management . J Atr Fibrillation 2015 ; 8 : 1309 .
Wang JA , Lau CP , Tai YT , Wu BZ. Effects of flecainide on exercise hemodynamics and electrocardiography in patients without structural heart disease . Clin Cardiol 1995 ; 18 : 140 – 144 .
Heidbuchel H , Adami PE , Antz M , Braunschweig F , Delise P , Scherr D , Solberg EE , Wilhelm M , Pelliccia A. Recommendations for participation in leisure-time physical activity and competitive sports in patients with arrhythmias and potentially arrhythmogenic conditions: Part 1: Supraventricular arrhythmias. A position statement of the Section of Sports Cardiology and Exercise from the European Association of Preventive Cardiology (EAPC) and the European Heart Rhythm Association (EHRA), both associations of the European Society of Cardiology . Eur J Prev Cardiol 2020 ;doi:10.1177/2047487320925635.
Heidbuchel H , Arbelo E , D’Ascenzi F , Borjesson M , Boveda S , Castelletti S , Miljoen H , Mont L , Niebauer J , Papadakis M , Pelliccia A , Saenen J , Sanz de la Garza M , Schwartz PJ , Sharma S , Zeppenfeld K , Corrado D. Recommendations for participation in leisure-time physical activity and competitive sports of patients with arrhythmias and potentially arrhythmogenic conditions. Part 2: ventricular arrhythmias, channelopathies, and implantable defibrillators: A position statement of the Section of Sports Cardiology and Exercise from the European Association of Preventive Cardiology (EAPC) and the European Heart Rhythm Association (EHRA), both associations of the European Society of Cardiology . Europace 2021 ; 23 : 147 – 148 .
Pelliccia A , Sharma S , Gati S , Bäck M , Börjesson M , Caselli S , Collet J-P , Corrado D , Drezner JA , Halle M , Hansen D , Heidbuchel H , Myers J , Niebauer J , Papadakis M , Piepoli MF , Prescott E , Roos-Hesselink JW , Graham Stuart A , Taylor RS , Thompson PD , Tiberi M , Vanhees L , Wilhelm M ; ESC Scientific Document Group. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease: the Task Force on sports cardiology and exercise in patients with cardiovascular disease of the European Society of Cardiology (ESC) . Eur Heart J 2021 ; 42 : 17 – 96 .
Shader RI , Greenblatt DJ. Use of benzodiazepines in anxiety disorders . N Engl J Med 1993 ; 328 : 1398 – 1405 .
Kassim T , Haddad TM , Rakhra A , Kabach A , Qurie A , Selim M , Nayfeh AS , Aly A , Holmberg MJ. A case of amitriptyline-induced myocarditis . Cureus 2018 ; 10 : e2840 .
Sicouri S , Antzelevitch C. Sudden cardiac death secondary to antidepressant and antipsychotic drugs . Expert Opin Drug Saf 2008 ; 7 : 181 – 194 .
Yap YG , Behr ER , Camm AJ. Drug-induced Brugada syndrome . Europace 2009 ; 11 : 989 – 994 .
Milberg P , Hilker E , Ramtin S , Cakir Y , Stypmann J , Engelen MA , Monnig G , Osada N , Breithardt G , Haverkamp W , Eckardt L. Proarrhythmia as a class effect of quinolones: increased dispersion of repolarization and triangulation of action potential predict torsades de pointes . J Cardiovasc Electrophysiol 2007 ; 18 : 647 – 654 .
Tscholl P , Feddermann N , Junge A , Dvorak J. The use and abuse of painkillers in international soccer: data from 6 FIFA tournaments for female and youth players . Am J Sports Med 2009 ; 37 : 260 – 265 .
Howard PA , Delafontaine P. Nonsteroidal anti-inflammatory drugs and cardiovascular risk . J Am Coll Cardiol 2004 ; 43 : 519 – 525 .
Cornu C , Grange C , Regalin A , Munier J , Ounissi S , Reynaud N , Kassai-Koupai B , Sallet P , Nony P. Effect of non-steroidal anti-inflammatory drugs on sport performance indices in healthy people: a meta-analysis of randomized controlled trials . Sports Med Open 2020 ; 6 : 20 – 11 .
Maughan RJ , Burke LM , Dvorak J , Larson-Meyer DE , Peeling P , Phillips SM , Rawson ES , Walsh NP , Garthe I , Geyer H , Meeusen R , van Loon LJC , Shirreffs SM , Spriet LL , Stuart M , Vernec A , Currell K , Ali VM , Budgett RG , Ljungqvist A , Mountjoy M , Pitsiladis YP , Soligard T , Erdener U , Engebretsen L. IOC consensus statement: dietary supplements and the high-performance athlete . Br J Sports Med 2018 ; 52 : 439 – 455 .
Garthe I , Maughan RJ. Athletes and supplements: prevalence and perspectives . Int J Sport Nutr Exerc Metab 2018 ; 28 : 126 – 138 .
Schubert MM , Astorino TA. A systematic review of the efficacy of ergogenic aids for improving running performance . J Strength Cond Res 2013 ; 27 : 1699 – 1707 .
Dhar R , Stout CW , Link MS , Homoud MK , Weinstock J , Estes NA 3rd . Cardiovascular toxicities of performance-enhancing substances in sports . Mayo Clin Proc 2005 ; 80 : 1307 – 1315 .
Sarshin A , Naderi A , da Cruz CJG , Feizolahi F , Forbes SC , Candow DG , Mohammadgholian E , Amiri M , Jafari N , Rahimi A , Alijani E , Earnest CP. The effects of varying doses of caffeine on cardiac parasympathetic reactivation following an acute bout of anaerobic exercise in recreational athletes . J Int Soc Sports Nutr 2020 ; 17 : 44 .
Gurley BJ , Steelman SC , Thomas SL. Multi-ingredient, caffeine-containing dietary supplements: history, safety, and efficacy . Clin Ther 2015 ; 37 : 275 – 301 .
Anderson O. Creatine propels British athletes to Olympic gold medals: is creatine the one true ergogenic aid . Running Res News 1993 ; 9 : 1 – 5 .
Tokish JM , Kocher MS , Hawkins RJ. Ergogenic aids: a review of basic science, performance, side effects, and status in sports . Am J Sports Med 2004 ; 32 : 1543 – 1553 .
Angell PJ , Chester N , Sculthorpe N , Whyte G , George K , Somauroo J. Performance enhancing drug abuse and cardiovascular risk in athletes: implications for the clinician . Br J Sports Med 2012 ; 46 (Suppl 1): i78 – i84 .
Calfee R , Fadale P. Popular ergogenic drugs and supplements in young athletes . Pediatrics 2006 ; 117 : e577 – e589 .
Francaux M , Poortmans JR. Side effects of creatine supplementation in athletes . Int J Sports Physiol Perform 2006 ; 1 : 311 – 323 .
Cermak NM , van Loon LJ. The use of carbohydrates during exercise as an ergogenic aid . Sports Med 2013 ; 43 : 1139 – 1155 .
Trexler ET , Smith-Ryan AE , Stout JR , Hoffman JR , Wilborn CD , Sale C , Kreider RB , Jäger R , Earnest CP , Bannock L , Campbell B , Kalman D , Ziegenfuss TN , Antonio J. International society of sports nutrition position stand: beta-alanine . J Int Soc Sports Nutr 2015 ; 12 : 30 .
Quesnele JJ , Laframboise MA , Wong JJ , Kim P , Wells GD. The effects of beta-alanine supplementation on performance: a systematic review of the literature . Int J Sport Nutr Exerc Metab 2014 ; 24 : 14 – 27 .
Bellinger PM , Minahan CL. The effect of β-alanine supplementation on cycling time trials of different length . Eur J Sport Sci 2016 ; 16 : 829 – 836 .
Bellinger PM , Minahan CL. Performance effects of acute beta-alanine induced paresthesia in competitive cyclists . Eur J Sport Sci 2016 ; 16 : 88 – 95 .
Smith-Ryan AE , Woessner MN , Melvin MN , Wingfield HL , Hackney AC. The effects of beta-alanine supplementation on physical working capacity at heart rate threshold . Clin Physiol Funct Imaging 2014 ; 34 : 397 – 404 .
Hoffman JR , Varanoske A , Stout JR. Effects of β-alanine supplementation on carnosine elevation and physiological performance . Adv Food Nutr Res 2018 ; 84 : 183 – 206 .
Shetewy A , Shimada-Takaura K , Warner D , Jong CJ , Mehdi AB , Alexeyev M , Takahashi K , Schaffer SW. Mitochondrial defects associated with beta-alanine toxicity: relevance to hyper-beta-alaninemia . Mol Cell Biochem 2016 ; 416 : 11 – 22 .
Kelly VG , Leveritt MD , Brennan CT , Slater GJ , Jenkins DG. Prevalence, knowledge and attitudes relating to beta-alanine use among professional footballers . J Sci Med Sport 2017 ; 20 : 12 – 16 .
Hadzic M , Eckstein ML , Schugardt M. The impact of sodium bicarbonate on performance in response to exercise duration in athletes: a systematic review . J Sports Sci Med 2019 ; 18 : 271 – 281 .
Breese BC , McNarry MA , Marwood S , Blackwell JR , Bailey SJ , Jones AM. Beetroot juice supplementation speeds O 2 uptake kinetics and improves exercise tolerance during severe-intensity exercise initiated from an elevated metabolic rate . Am J Physiol Regul Integr Comp Physiol 2013 ; 305 : R1441 – 50 .
Domínguez R , Cuenca E , Maté-Muñoz JL , García-Fernández P , Serra-Paya N , Estevan MC , Herreros PV , Garnacho-Castaño MV. Effects of beetroot juice supplementation on cardiorespiratory endurance in athletes. A systematic review . Nutrients 2017 ; 9 : 43 .
Woessner MN , McIlvenna LC , Ortiz de Zevallos J , Neil CJ , Allen JD. Dietary nitrate supplementation in cardiovascular health: an ergogenic aid or exercise therapeutic? Am J Physiol Heart Circ Physiol 2018 ; 314 : H195 – H212 .
Stanaway L , Rutherfurd-Markwick K , Page R , Wong M , Jirangrat W , Teh KH , Ali A. Acute supplementation with nitrate-rich beetroot juice causes a greater increase in plasma nitrite and reduction in blood pressure of older compared to younger adults . Nutrients 2019 ; 11 : 1683 .
Cermak NM , Res PT , de Groot LC , Saris WH , van Loon LJ. Protein supplementation augments the adaptive response of skeletal muscle to resistance-type exercise training: a meta-analysis . Am J Clin Nutr 2012 ; 96 : 1454 – 1464 .
Schoenfeld BJ , Aragon AA. Is there a postworkout anabolic window of opportunity for nutrient consumption? Clearing up controversies . J Orthop Sports Phys Ther 2018 ; 48 : 911 – 914 .
Rehm J. The risks associated with alcohol use and alcoholism . Alcohol Res Health 2011 ; 34 : 135 – 143 .
Johnston R , Crowe M , Doma K. Effect of nicotine on repeated bouts of anaerobic exercise in nicotine naïve individuals . Eur J Appl Physiol 2018 ; 118 : 681 – 689 .
Pesta DH , Angadi SS , Burtscher M , Roberts CK. The effects of caffeine, nicotine, ethanol, and tetrahydrocannabinol on exercise performance . Nutr Metab (Lond) 2013 ; 10 : 71 .
Mündel T. Nicotine: sporting friend or foe? A review of athlete use, performance consequences and other considerations . Sports Med 2017 ; 47 : 2497 – 2506 .
Breda JJ , Whiting SH , Encarnação R , Norberg S , Jones R , Reinap M , Jewell J. Energy drink consumption in Europe: a review of the risks, adverse health effects, and policy options to respond . Front Public Health 2014 ; 2 : 134 .
Gutiérrez-Hellín J , Varillas-Delgado D. Energy drinks and sports performance, cardiovascular risk, and genetic associations; future prospects . Nutrients 2021 ; 13 : 715 .
Chaban R , Kornberger A , Branski N , Buschmann K , Stumpf N , Beiras-Fernandez A , Vahl CF. In-vitro examination of the positive inotropic effect of caffeine and taurine, the two most frequent active ingredients of energy drinks . BMC Cardiovasc Disord 2017 ; 17 : 220 .
Ruiz LD , Scherr RE. Risk of energy drink consumption to adolescent health . Am J Lifestyle Med 2019 ; 13 : 22 – 25 .
Marczinski CA , Stamates AL , Ossege J , Maloney SF , Bardgett ME , Brown CJ. Subjective state, blood pressure, and behavioral control changes produced by an "energy shot" . J Caffeine Res 2014 ; 4 : 57 – 63 .
Campbell B , Wilborn C , La Bounty P , Taylor L , Nelson MT , Greenwood M , Ziegenfuss TN , Lopez HL , Hoffman JR , Stout JR , Schmitz S , Collins R , Kalman DS , Antonio J , Kreider RB. International Society of Sports Nutrition position stand: energy drinks . J Int Soc Sports Nutr 2013 ; 10 : 1 .
Gray B , Ingles J , Medi C , Driscoll T , Semsarian C. Cardiovascular effects of energy drinks in familial long QT syndrome: a randomized cross-over study . Int J Cardiol 2017 ; 231 : 150 – 154 .
Mangi MA , Rehman H , Rafique M , Illovsky M. Energy drinks and the risk of cardiovascular disease: a review of current literature . Cureus 2017 ; 9 : e1322 .
Chrysant SG , Chrysant GS. Cardiovascular complications from consumption of high energy drinks: recent evidence . J Hum Hypertens 2015 ; 29 : 71 – 76 .
Gunja N , Brown JA. Energy drinks: health risks and toxicity . Med J Aust 2012 ; 196 : 46 – 49 .
Serdar M , Mordelt A , Müser K , Kempe K , Felderhoff-Müser U , Herz J , Bendix I. Detrimental impact of energy drink compounds on developing oligodendrocytes and neurons . Cells 2019 ; 8 : 1381 .
La Gerche A , Brosnan MJ. Drugs in sport—a change is needed, but what? Heart Lung Circ 2018 ; 27 : 1099 – 1104 .
Uchida L , Tanaka T , Saito H , Sugahara M , Wakashima T , Fukui K , Nangaku M. Effects of a prolyl hydroxylase inhibitor on kidney and cardiovascular complications in a rat model of chronic kidney disease . Am J Physiol Renal Physiol 2020 ; 318 : F388 – F401 .
Di Luigi L , Sansone M , Sansone A , Ceci R , Duranti G , Borrione P , Crescioli C , Sgrò P , Sabatini S. Phosphodiesterase type 5 inhibitors, sport and doping . Curr Sports Med Rep 2017 ; 16 : 443 – 447 .
Roth SM , Rankinen T , Hagberg JM , Loos RJ , Pérusse L , Sarzynski MA , Wolfarth B , Bouchard C. Advances in exercise, fitness, and performance genomics in 2011 . Med Sci Sports Exerc 2012 ; 44 : 809 – 817 .
Harridge SD , Velloso CP. IGF-I and GH: potential use in gene doping . Growth Hormone & IGF Research 2009 ; 19 : 378 – 382 .
van der Gronde T , de Hon O , Haisma HJ , Pieters T. Gene doping: an overview and current implications for athletes . Br J Sports Med 2013 ; 47 : 670 – 678 .
Fischetto G , Bermon S. From gene engineering to gene modulation and manipulation: can we prevent or detect gene doping in sports? Sports Med 2013 ; 43 : 965 – 977 .
Unal M , Unal DO. Gene doping in sports . Sports Med 2004 ; 34 : 357 – 362 .
Vermersch E , Jouve C , Hulot J-S. CRISPR/Cas9 gene-editing strategies in cardiovascular cells . Cardiovasc Res 2020 ; 116 : 894 – 907 .
Brzeziańska E , Domańska D , Jegier A. Gene doping in sport - perspectives and risks . Biol Sport 2014 ; 31 : 251 – 259 .
Martínez-Sanz JM , Sospedra I , Ortiz CM , Baladía E , Gil-Izquierdo A , Ortiz-Moncada R. Intended or unintended doping? A review of the presence of doping substances in dietary supplements used in sports . Nutrients 2017 ; 9 : 1093 .
Denham BE. Athlete information sources about dietary supplements: a review of extant research . Int J Sport Nutr Exerc Metab 2017 ; 27 : 325 – 334 .
Negro M , Marzullo N , Caso F , Calanni L , D'Antona G. Opinion paper: scientific, philosophical and legal consideration of doping in sports . Eur J Appl Physiol 2018 ; 118 : 729 – 736 .
Author notes
- central nervous system stimulants
- cardiovascular system
- doping in sports
- energy drinks
Email alerts
Companion article.
- Medication for patient-athletes—the therapeutic use exemption procedure
Related articles in pubmed, citing articles via.
- Recommend to Your Librarian
- Advertising and Corporate Services
- Journals Career Network
Affiliations
- Online ISSN 2047-4881
- Print ISSN 2047-4873
- Copyright © 2024 European Society of Cardiology
- About Oxford Academic
- Publish journals with us
- University press partners
- What we publish
- New features
- Open access
- Institutional account management
- Rights and permissions
- Get help with access
- Accessibility
- Advertising
- Media enquiries
- Oxford University Press
- Oxford Languages
- University of Oxford
Oxford University Press is a department of the University of Oxford. It furthers the University's objective of excellence in research, scholarship, and education by publishing worldwide
- Copyright © 2024 Oxford University Press
- Cookie settings
- Cookie policy
- Privacy policy
- Legal notice
This Feature Is Available To Subscribers Only
Sign In or Create an Account
This PDF is available to Subscribers Only
For full access to this pdf, sign in to an existing account, or purchase an annual subscription.
- Follow us on Facebook
- Follow us on Twitter
- Criminal Justice
- Environment
- Politics & Government
- Race & Gender
Expert Commentary
Performance-enhancing drugs in athletics: Research roundup
2015 roundup of research on the use of performance-enhancing drugs in athletics and academics as well as their potential health effects.

Republish this article

This work is licensed under a Creative Commons Attribution-NoDerivatives 4.0 International License .
by Leighton Walter Kille, The Journalist's Resource June 9, 2015
This <a target="_blank" href="https://journalistsresource.org/health/athletic-academic-performance-enhancing-drugs-research-roundup/">article</a> first appeared on <a target="_blank" href="https://journalistsresource.org">The Journalist's Resource</a> and is republished here under a Creative Commons license.<img src="https://journalistsresource.org/wp-content/uploads/2020/11/cropped-jr-favicon-150x150.png" style="width:1em;height:1em;margin-left:10px;">
Performance-enhancing drugs have a long history in sports, of course, but pharmacological research has led to a surge in the number of substances available, each with its own potential for misuse.
Given the potential financial rewards of athletic success, it’s no surprise that we’ve been witness to a seemingly endless procession of allegations and scandals. Sluggers Barry Bonds (steroids) and Alex Rodriguez (human growth hormone); cyclists Lance Armstrong (EPO), Floyd Landis (testosterone) and Alberto Contador (clenbuterol); runners Tyson Gay (steroids) and Justin Gatlin (testosterone); and golfer Vijay Singh (IGF-1) are only some of the more prominent professionals implicated in such behavior. The complicity of medical professionals and shadowy labs is often involved, and a 2015 report from the International Cycling Union (UCI) found the sport’s own governing body bore significant responsibility.
Not surprisingly, hard numbers on rates of usage are difficult to come by, but anecdotal evidence isn’t lacking and anonymous surveys have provided some insight. Questionable use of medications and supplements have also been reported in the U.S. armed forces , fire and police departments , amateur athletics , and even high schools .
Below is a selection of studies on a range of issues related to performance-enhancing drugs. It has sections on their potential economic impacts, prevalence , health effects and athletes’ attitudes . For additional studies on these topics, you can search PubMed , which is the federal clearinghouse for all medical research. At bottom, we have also included some studies relating to cognitive-enhancing drugs and the related academic dimensions of this issue.
—————————-
“The Economics of Corruption in Sports: The Special Case of Doping” Dimant, Eugen; Deutscher, Christian. Edmond J. Safra Working Papers, No. 55, January 2015.
Abstract: “Corruption in general and doping in particular are ubiquitous in both amateur and professional sports and have taken the character of a systemic threat. In creating unfair advantages, doping distorts the level playing field in sporting competition. With higher stakes involved, such distortions create negative externalities not only on the individual level (lasting health damages, for example) but also frictions on the aggregate level (such as loss of media interest) and erode the principle of sports. In this paper, we provide a comprehensive literature overview of the individual’s incentive to dope, the concomitant detrimental effects and respective countermeasures. In explaining the athlete’s motivation to use performance enhancing drugs, we enrich the discussion by adapting insights from behavioral economics. These insights help to understand such an athlete’s decision beyond a clear-cut rationale but rather as a product of the interaction with the underlying environment. We stress that in order to ensure clean sports and fair competition, more sophisticated measurement methods have to be formulated, and the respective data made publicly available in order to facilitate more extensive studies in the future. So far, the lack of data is alarming, especially in the area of elite sports where the stakes are high and doping has a substantial influence.”
“The Frequency of Doping in Elite Sport: Results of a Replication Study” Pitsch, Werner; Emrich, Eike. International Review for the Sociology of Sport , October 2012, Vol. 47, No. 5, 559-580. doi: 10.1177/1012690211413969.
Abstract: “The difficulty of measuring the prevalence of doping in elite sport is a recurring topic in the scientific literature on doping. The Randomized Response Technique is a method for asking such embarrassing or even threatening questions while allowing the respondents to answer honestly. It was used to measure the prevalence of doping among German squad athletes by Pitsch et al. (2005, 2007). In a replication study with better sampling control, it was possible to replicate the general trend of the data from the 2005 study…. The paper-based survey resulted in a rate of 10.2% ‘honest dopers,’ irrespective of the disciplines, obtained with the question: ‘Have you ever knowingly used illicit drugs or methods in order to enhance your performance?’ By adding the rate of cheaters (24.7%), whose behaviour the researchers know nothing about, one can calculate the interval (10.2%, 34.9%), which should include the true rate of dopers throughout their career among German elite athletes. In contrast, this means that the larger proportion of athletes, namely, 65.2%, represents ‘honest non-dopers.’ In the 2008 season, this figure was 65%.”
“Growth Hormone Doping in Sports: A Critical Review of Use and Detection Strategies” Baumann, Gerhard P. Endocrine Reviews , April 2012, Vol. 33, No. 2 155-186. doi: 10.1210/er.2011-1035.
Abstract: “[Growth hormone] is believed to be widely employed in sports as a performance-enhancing substance. Its use in athletic competition is banned by the World Anti-Doping Agency, and athletes are required to submit to testing for GH exposure…. The scientific evidence for the [performance-enhancing characteristics] of GH is weak, a fact that is not widely appreciated in athletic circles or by the general public. Also insufficiently appreciated is the risk of serious health consequences associated with high-dose, prolonged GH use. This review discusses the GH biology relevant to GH doping; the virtues and limitations of detection tests in blood, urine, and saliva; secretagogue efficacy; IGF-I doping; and information about the effectiveness of GH as a performance-enhancing agent.”
“Supplements in Top-Level Track and Field Athletes” Tscholl, Philippe; Alonso, Juan M.; Dollé, Gabriel; Junge, Astrid; Dvorak, Jiri. American Journal of Sports Medicine , January 2010, Vol. 38, No. 1, 133-140. doi: 10.1177/0363546509344071.
Abstract: “Analysis of 3,887 doping control forms undertaken during 12 International Association of Athletics Federations World Championships and one out-of-competitions season in track and field. Results: There were 6,523 nutritional supplements (1.7 per athlete) and 3,237 medications (0.8 per athlete) reported. Nonsteroidal anti-inflammatory drugs (NSAIDs; 0.27 per athlete, n = 884), respiratory drugs (0.21 per athlete, n = 682), and alternative analgesics (0.13, n = 423) were used most frequently. Medication use increased with age (0.33 to 0.87 per athlete) and decreased with increasing duration of the event (from sprints to endurance events; 1.0 to 0.63 per athlete). African and Asian track and field athletes reported using significantly fewer supplements (0.85 vs. 1.93 per athlete) and medications (0.41 vs. 0.96 per athlete) than athletes from other continents. The final ranking in the championships was unrelated to the quantity of reported medications or supplements taken. Compared with middle-distance and long-distance runners, athletes in power and sprint disciplines reported using more NSAIDs, creatine, and amino acids, and fewer antimicrobial agents. Conclusion: The use of NSAIDs in track and field is less than that reported for team-sport events. However, nutritional supplements are used more than twice as often as they are in soccer and other multisport events; this inadvertently increases the risk of positive results of doping tests.”
“Alcohol, Tobacco, Illicit Drugs and Performance Enhancers: A Comparison of Use by College Student Athletes and Nonathletes” Yusko, David A.; et al. American Journal of Sports Medicine, August 2010. doi: 10.3200/JACH.57.3.281-290.
Abstract: Compares the prevalence and pattern of substance use in undergraduate student athletes and nonathletes from 2005-2006. Data was collected using questionnaires from male (n = 418) and female (n = 475) student athletes and nonathletes from 2005-2006 to assess prevalence, quantity, and frequency of alcohol and drug use, and to determine patterns of student athletes’ alcohol and drug use during their athletic season versus out of season. Male student athletes were found to be at high risk for heavy drinking and performance-enhancing drug use. Considerable in-season versus out-of-season substance use fluctuations were identified in male and female student athletes. Additional, and possibly alternative, factors are involved in a student athlete’s decision-making process regarding drug and alcohol use, which suggests that the development of prevention programs that are specifically designed to meet the unique needs of the college student athlete may be beneficial.”
Health effects
“Performance Enhancing Drug Abuse and Cardiovascular Risk in Athletes” Angell, Peter J.; Chester, Neil; Sculthorpe, Nick; Whyte, Greg; George, Keith; Somauroo, John. British Journal of Sports Medicine , July 2012. doi:10.1136/bjsports-2012-091186.
Abstract: “Despite continuing methodological developments to detect drug use and associated punishments for positive dope tests, there are still many athletes who choose to use performance- and image-enhancing drugs. Of primary concern to this review are the health consequences of drug use by athletes…. We will address current knowledge, controversies and emerging evidence in relation to cardiovascular (CV) health of athletes taking drugs. Further, we delimit our discussion to the CV consequences of anabolic steroids and stimulant (including amphetamines and cocaine) use. These drugs are reported in the majority of adverse findings in athlete drug screenings and thus are more likely to be relevant to the healthcare professionals responsible for the well-being of athletes.”
“Illicit Anabolic-Androgenic Steroid Use” Kanayama, Gen; Hudson, James I.; Pope Jr., Harrison G. Hormones and Behavior , Volume 58, Issue 1, June 2010, Pages 111-121. doi: 10.1016/j.yhbeh.2009.09.006.
Abstract: “The anabolic-androgenic steroids (AAS) are a family of hormones that includes testosterone and its derivatives. These substances have been used by elite athletes since the 1950s, but they did not become widespread drugs of abuse in the general population until the 1980s. Thus, knowledge of the medical and behavioral effects of illicit AAS use is still evolving. Surveys suggest that many millions of boys and men, primarily in Western countries, have abused AAS to enhance athletic performance or personal appearance. AAS use among girls and women is much less common. Taken in supraphysiologic doses, AAS show various long-term adverse medical effects, especially cardiovascular toxicity. Behavioral effects of AAS include hypomanic or manic symptoms, sometimes accompanied by aggression or violence, which usually occur while taking AAS, and depressive symptoms occurring during AAS withdrawal. However, these symptoms are idiosyncratic and afflict only a minority of illicit users; the mechanism of these idiosyncratic responses remains unclear. AAS users may also ingest a range of other illicit drugs, including both “body image” drugs to enhance physical appearance or performance, and classical drugs of abuse. In particular, AAS users appear particularly prone to opioid use. There may well be a biological basis for this association, since both human and animal data suggest that AAS and opioids may share similar brain mechanisms. Finally, AAS may cause a dependence syndrome in a substantial minority of users. AAS dependence may pose a growing public health problem in future years but remains little studied.”
“Adverse Health Effects of Anabolic-Androgenic Steroids” Van Amsterdama, Jan; Opperhuizena, Antoon; Hartgensb, Fred. Regulatory Toxicology and Pharmacology , Volume 57, Issue 1, June 2010, Pages 117-123. doi: 10.1016/j.yrtph.2010.02.001.
Abstract: “Anabolic-androgenic steroids (AAS) are synthetic drugs derived from testosterone. Illegally, these drugs are regularly self-administered by body builders and power lifters to enhance their sportive performance. Adverse side effects of AAS include sexual dysfunction, alterations of the cardiovascular system, psyche and behavior, and liver toxicity. However, severe side effects appear only following prolonged use of AAS at high dose and their occurrence is limited…. The overwhelming stereotype about AAS is that these compounds cause aggressive behavior in males. However, the underlying personality traits of a specific subgroup of the AAS abusers, who show aggression and hostility, may be relevant, as well. Use of AAS in combination with alcohol largely increases the risk of violence and aggression. The dependence liability of AAS is very low, and withdrawal effects are relatively mild. Based on the scores for acute and chronic adverse health effects, the prevalence of use, social harm and criminality, AAS were ranked among 19 illicit drugs as a group of drugs with a relatively low harm.”
“Effects of Growth Hormone Therapy on Exercise Performance in Men” Triay, Jessica M.; Ahmad, Bushra N. Trends in Urology & Men’s Health , July/August 2012, Vol. 3, Issue 4, 23-26. doi: 10.1002/tre.274.
Conclusions: “In the athletic arena, [growth hormone] doping is considered to be widespread and used in combination with other agents, and regimens vary depending on individual preferences and cost implications…. It must be recognised that the effects of GH administration in adults with a normal GH/IGF-1 axis are not comparable to those in GH deficiency and that the complexity of processes influencing GH release and peripheral actions means that overall performance should be considered as opposed to isolated effects. Although studies to date have been small in both subject numbers and treatment times, they have demonstrated measurable changes in GH and IGF-1 levels, as well as possible deleterious effects on exercise performance that should be taken seriously.”
“Performance-Enhancing Drugs on the Web: A Growing Public-Health Issue” Brennan, Brian P.; Kanayama, Gen; Pope Jr., Harrison G. American Journal on Addictions , March-April 2013, Vol. 22, Issue 2, 158-161. doi: 10.1111/j.1521-0391.2013.00311.x.
Abstract: “Today’s Internet provides extensive “underground” guidelines for obtaining and using illicit substances, including especially anabolic-androgenic steroids (AAS) and other appearance- and performance-enhancing drugs (APEDs). We attempted to qualitatively characterize APED-related Internet sites. We used relevant Internet search terms [and] found thousands of sites involving AAS and other APEDs. Most sites presented an unabashedly pro-drug position, often openly questioning the qualifications and motivations of mainstream medical practitioners. Offers of AAS and other APEDs for sale, together with medical advice of varying legitimacy, was widespread across sites. Importantly, many sites provided detailed guidelines for exotic forms of APED use, some likely associated with serious health risks, which are probably unknown to most practicing clinicians.”
“Doping in Sport: A Review of Elite Athletes’ Attitudes, Beliefs and Knowledge” Morente-Sánchez, Jaime; Zabala, Mikel. Sports Medicine , March 2013. doi: 10.1007/s40279-013-0037-x.
Abstract: “Although most athletes acknowledge that doping is cheating, unhealthy and risky because of sanctions, its effectiveness is also widely recognized. There is a general belief about the inefficacy of anti-doping programmes, and athletes criticise the way tests are carried out. Most athletes consider the severity of punishment is appropriate or not severe enough. There are some differences between sports, as team-based sports and sports requiring motor skills could be less influenced by doping practices than individual self-paced sports. However, anti-doping controls are less exhaustive in team sports. The use of banned substance also differs according to the demand of the specific sport. Coaches appear to be the main influence and source of information for athletes, whereas doctors and other specialists do not seem to act as principal advisors. Athletes are becoming increasingly familiar with anti-doping rules, but there is still a lack of knowledge that should be remedied using appropriate educational programmes. There is also a lack of information on dietary supplements and the side effects of [performance-enhancing substances].”
“Age and Gender Specific Variations in Attitudes to Performance Enhancing Drugs and Methods” Singhammer, John. Sport Science Review , December 2012. doi: 10.2478/v10237-012-0017-3.
Abstract: “Using a population-based cross-sectional sample of 1,703 Danish men and women aged 15-60 years, the present study examined age and gender variation in attitudes to performance enhancing drugs and methods…. Overall, participants held negative attitudes to drugs and methods enhancing predominantly cognitive-abilities-enhancing performance drugs and to appearance-modifying methods, but were positive to drugs for restoring physical functioning conditions. However, attitudes varied nonlinearly across age. Lenient attitudes peaked at around age 25 and subsequently decreased. Lenient attitudes to use of drugs against common disorders decreased in a linear fashion. No gender differences were observed and attitude did not vary with level of education, self-reported health or weekly hours of physical activity.”
“Drugs, Sweat and Gears: An Organizational Analysis of Performance Enhancing Drug Use in the 2010 Tour De France” Palmer, Donald; Yenkey, Christopher. University of California, Davis; University of Chicago. March 2013.
Abstract: “This paper seeks a more comprehensive explanation of wrongdoing in organizations by theorizing two under-explored causes: the criticality of a person’s role in their organization’s strategy-based structure, and social ties to known deviants within their organization and industry. We investigate how these factors might have influenced wrongdoing in the context of professional cyclists’ use of banned performance enhancing drugs (PEDs) in advance of the 2010 Tour de France….. We find substantial support for our prediction that actors who are more critical to the organization’s strategy-based structure are more likely to engage in wrongdoing. Further, we find that while undifferentiated social ties to known wrongdoers did not increase the likelihood of wrongdoing, ties to unpunished offenders increased the probability of wrongdoing and ties to severely punished offenders decreased it. These effects were robust to consideration of other known causes of wrongdoing: weak governance regimes and permissive cultural contexts, performance strain, and individual propensities to engage in wrongdoing.”
“Elite Athletes’ Estimates of the Prevalence of Illicit Drug Use: Evidence for the False Consensus Effect” Dunn, Matthew; Thomas, Johanna O.; Swift, Wendy; Burns, Lucinda. Drug and Alcohol Review , January 2012, Vol. 31, Issue 1, 27-32. doi: 10.1111/j.1465-3362.2011.00307.x.
Abstract: “The false consensus effect (FCE) is the tendency for people to assume that others share their attitudes and behaviours to a greater extent than they actually do…. The FCE was investigated among 974 elite Australian athletes who were classified according to their drug use history. Participants tended to report that there was a higher prevalence of drug use among athletes in general compared with athletes in their sport, and these estimates appeared to be influenced by participants’ drug-use history. While overestimation of drug use by participants was not common, this overestimation also appeared to be influenced by athletes’ drug use history.”
“The Role of Sports Physicians in Doping: A Note on Incentives” Korn, Evelyn; Robeck, Volker. Philipps-Universitat, Marburg, March 2013.
Abstract: “How to ban the fraudulent use of performance-enhancing drugs is an issue in all professional — and increasingly in amateur — sports. The main effort in enforcing a ‘clean sport’ has concentrated on proving an abuse of performance-enhancing drugs and on imposing sanctions on teams and athletes. An investigation started by Freiburg university hospital against two of its employees who had been working as physicians for a professional cycling team has drawn attention to another group of actors: physicians. It reveals a multi-layered contractual relations between sports teams, physicians, hospitals, and sports associations that provided string incentives for the two doctors to support the use performance-enhancing drugs. This paper argues that these misled incentives are not singular but a structural part of modern sports caused by cross effects between the labor market for sports medicine specialists (especially if they are researchers) and for professional athletes.”
“Socio-economic Determinants of Adolescent Use of Performance Enhancing Drugs” Humphreys, Brad R.; Ruseski, Jane E. Journal of Socio-Economics , April 2011, Vol. 40, Issue 2, 208-216. doi: 10.1016/j.socec.2011.01.008.
Abstract: “Evidence indicates that adolescents (athletes and non-athletes use performance enhancing drugs. We posit that adolescent athletes have different socio-economic incentives to use steroids than non-athletes. We examine adolescent steroid use using data from the Youth Risk Behavior Surveillance System. Multi-sport upperclassmen and black males have a higher probability of steroid use. Steroid use is associated with motivations to change physical appearance and experimentation with illicit substances. These results suggest there are different socio-economic motivations for adolescent steroid use and that steroid use is an important component of overall adolescent drug use.”
Cognitive-enhancing drugs
“Randomized Response Estimates for the 12-Month Prevalence of Cognitive-Enhancing Drug Use in University Students” Dietz, Pavel; et al. Pharmacotherapy , January 2013, Vol. 33, Issue 1, 44-50. doi: 10.1002/phar.1166.
Results: “An anonymous, specialized questionnaire that used the randomized response technique was distributed to students at the beginning of classes and was collected afterward. From the responses, we calculated the prevalence of students taking drugs only to improve their cognitive performance and not to treat underlying mental disorders such as attention-deficit-hyperactivity disorder, depression, and sleep disorders. The estimated 12-month prevalence of using cognitive-enhancing drugs was 20%. Prevalence varied by sex (male 23.7%, female 17.0%), field of study (highest in students studying sports-related fields, 25.4%), and semester (first semester 24.3%, beyond first semester 16.7%).”
“The Diversion and Misuse of Pharmaceutical Stimulants: What Do We Know and Why Should We Care?” Kaye, Sharlene; Darke, Shane. Addiction , February 2012, Vol. 107, Issue 3, 467-477. doi: 10.1111/j.1360-0443.2011.03720.x.
Results: “The evidence to date suggests that the prevalence of diversion and misuse of pharmaceutical stimulants varies across adolescent and young adult student populations, but is higher than that among the general population, with the highest prevalence found among adults with attention deficit-hyperactive disorder (ADHD) and users of other illicit drugs. Concerns that these practices have become more prevalent as a result of increased prescribing are not supported by large-scale population surveys…. Despite recognition of the abuse liability of these medications, there is a paucity of data on the prevalence, patterns and harms of diversion and misuse among populations where problematic use and abuse may be most likely to occur (e.g. adolescents, young adults, illicit drug users). Comprehensive investigations of diversion and misuse among these populations should be a major research priority, as should the assessment of abuse and dependence criteria among those identified as regular users.”
“Adderall Abuse on College Campuses: A Comprehensive Literature Review” Varga, Matthew D. Journal of Evidence-Based Social Work , 2012, Vol. 9, Issue 3. doi: 10.1080/15433714.2010.525402.
Abstract: “Prescription stimulant abuse has dramatically increased over the past 10 years, but the amount of research regarding college students and illicit prescription stimulant use is still very limited. This has important implications for college mental health professionals and higher education administrators. In this comprehensive literature review the author explores factors contributing to illicit use, self-medication, and recreational use of controlled prescription stimulants; discusses the potential consequences for those students abusing stimulants; and provides recommendations for educating, combating, and assisting students who illicitly use prescription stimulants on college campuses.”
“A Comparison of Attitudes Toward Cognitive Enhancement and Legalized Doping in Sport in a Community Sample of Australian Adults” Partridge, Brad; Lucke, Jayne; Hall, Wayne. AJOB Primary Research , November 2012. doi: 10.1080/21507716.2012.720639.
Abstract: “This article compares public attitudes toward the use of prescription drugs for cognitive enhancement with the use of performance enhancing drugs in sport. We explore attitudes toward the acceptability of both practices; the extent to which familiarity with cognitive enhancement is related to its perceived acceptability; and relationships between the acceptability of cognitive enhancement and legalized doping in sport. Of 1,265 [survey] participants, 7% agreed that cognitive enhancement is acceptable; 2.4% of the total sample said they had taken prescription drugs to enhance their concentration or alertness in the absence of a diagnosed disorder, and a further 8% said they knew someone who had done so. These participants were twice as likely to think cognitive enhancement was acceptable. Only 3.6% of participants agreed that people who play professional sport should be allowed to use performance-enhancing drugs if they wanted to. Participants who found cognitive enhancement acceptable were 9.5 times more likely to agree with legalized doping.”
Keywords: drugs, youth, sports, cheating, higher education, corruption, ADHD, research roundup
About The Author

Leighton Walter Kille
The Controversy Surrounding Barry Bonds and Steroids in Baseball
This essay about Barry Bonds and steroids in baseball delves into the controversy surrounding his career. Despite Bonds’ exceptional talent and record-breaking achievements, his legacy is overshadowed by allegations of performance-enhancing drug use, particularly during the Steroid Era. The essay explores Bonds’ connection to the BALCO scandal, the impact of steroid use on sports ethics, and the broader implications for athletic competition. It emphasizes the complexities of maintaining integrity in sports amidst advancements in performance enhancement methods, serving as a cautionary tale about the ethical dilemmas faced by athletes striving for greatness.
How it works
The intersection of performance-enhancing drugs (PEDs) and professional sports has long been a contentious issue, and few cases exemplify this more than that of Barry Bonds in baseball. Bonds, a legendary figure in the sport, is not only renowned for his extraordinary athletic abilities but also for the shadow cast over his career due to allegations of steroid use.
Barry Bonds’ career is a tale of two narratives: one of unparalleled success on the field and the other of suspicion and controversy off it.
Bonds, often hailed as one of the greatest baseball players of all time, holds numerous records, including the single-season and career home run records. However, these achievements are tarnished by the widespread belief that his accomplishments were artificially boosted by steroid use.
The use of performance-enhancing drugs in baseball came under intense scrutiny during the late 1990s and early 2000s, a period commonly referred to as the “Steroid Era.” This era saw a significant increase in player performance, characterized by inflated offensive statistics and an unprecedented number of home runs. While this era produced many remarkable moments and players, it also left a stain on the integrity of the game.
Barry Bonds’ involvement in the steroid controversy reached its peak during the BALCO scandal in the early 2000s. The Bay Area Laboratory Co-operative (BALCO) was at the center of a doping scandal that implicated numerous athletes across various sports, including Bonds. Bonds was accused of using performance-enhancing drugs supplied by BALCO, specifically the designer steroid tetrahydrogestrinone (THG), commonly known as “The Clear.”
Despite consistent denials and legal battles, Bonds’ association with PEDs has continued to overshadow his legacy. While he has never been convicted of steroid use, his connection to the BALCO scandal and the physical changes in his physique over the course of his career have fueled speculation and skepticism among fans and analysts alike.
The debate surrounding Barry Bonds and steroids extends beyond the confines of baseball. It raises broader questions about the ethics of using performance-enhancing drugs in sports, the responsibility of athletes as role models, and the integrity of athletic competition. Bonds’ case serves as a cautionary tale, highlighting the complexities and consequences of pursuing greatness at any cost.
In conclusion, the controversy surrounding Barry Bonds and steroids underscores the complex relationship between sports, ethics, and performance enhancement. While Bonds’ on-field achievements are undeniably remarkable, they are forever marred by allegations of steroid use. His legacy serves as a sobering reminder of the enduring impact of the Steroid Era on the game of baseball and the ongoing challenges faced in preserving the integrity of sports in the face of technological advancements and ethical dilemmas.
Cite this page
The Controversy Surrounding Barry Bonds and Steroids in Baseball. (2024, May 12). Retrieved from https://papersowl.com/examples/the-controversy-surrounding-barry-bonds-and-steroids-in-baseball/
"The Controversy Surrounding Barry Bonds and Steroids in Baseball." PapersOwl.com , 12 May 2024, https://papersowl.com/examples/the-controversy-surrounding-barry-bonds-and-steroids-in-baseball/
PapersOwl.com. (2024). The Controversy Surrounding Barry Bonds and Steroids in Baseball . [Online]. Available at: https://papersowl.com/examples/the-controversy-surrounding-barry-bonds-and-steroids-in-baseball/ [Accessed: 14 May. 2024]
"The Controversy Surrounding Barry Bonds and Steroids in Baseball." PapersOwl.com, May 12, 2024. Accessed May 14, 2024. https://papersowl.com/examples/the-controversy-surrounding-barry-bonds-and-steroids-in-baseball/
"The Controversy Surrounding Barry Bonds and Steroids in Baseball," PapersOwl.com , 12-May-2024. [Online]. Available: https://papersowl.com/examples/the-controversy-surrounding-barry-bonds-and-steroids-in-baseball/. [Accessed: 14-May-2024]
PapersOwl.com. (2024). The Controversy Surrounding Barry Bonds and Steroids in Baseball . [Online]. Available at: https://papersowl.com/examples/the-controversy-surrounding-barry-bonds-and-steroids-in-baseball/ [Accessed: 14-May-2024]
Don't let plagiarism ruin your grade
Hire a writer to get a unique paper crafted to your needs.

Our writers will help you fix any mistakes and get an A+!
Please check your inbox.
You can order an original essay written according to your instructions.
Trusted by over 1 million students worldwide
1. Tell Us Your Requirements
2. Pick your perfect writer
3. Get Your Paper and Pay
Hi! I'm Amy, your personal assistant!
Don't know where to start? Give me your paper requirements and I connect you to an academic expert.
short deadlines
100% Plagiarism-Free
Certified writers
Suggestions or feedback?
MIT News | Massachusetts Institute of Technology
- Machine learning
- Social justice
- Black holes
- Classes and programs
Departments
- Aeronautics and Astronautics
- Brain and Cognitive Sciences
- Architecture
- Political Science
- Mechanical Engineering
Centers, Labs, & Programs
- Abdul Latif Jameel Poverty Action Lab (J-PAL)
- Picower Institute for Learning and Memory
- Lincoln Laboratory
- School of Architecture + Planning
- School of Engineering
- School of Humanities, Arts, and Social Sciences
- Sloan School of Management
- School of Science
- MIT Schwarzman College of Computing
New treatment could reverse hair loss caused by an autoimmune skin disease
Press contact :, media download.

*Terms of Use:
Images for download on the MIT News office website are made available to non-commercial entities, press and the general public under a Creative Commons Attribution Non-Commercial No Derivatives license . You may not alter the images provided, other than to crop them to size. A credit line must be used when reproducing images; if one is not provided below, credit the images to "MIT."

Previous image Next image
Researchers at MIT, Brigham and Women’s Hospital, and Harvard Medical School have developed a potential new treatment for alopecia areata, an autoimmune disorder that causes hair loss and affects people of all ages, including children.
For most patients with this type of hair loss, there is no effective treatment. The team developed a microneedle patch that can be painlessly applied to the scalp and releases drugs that help to rebalance the immune response at the site, halting the autoimmune attack.
In a study of mice, the researchers found that this treatment allowed hair to regrow and dramatically reduced inflammation at the treatment site, while avoiding systemic immune effects elsewhere in the body. This strategy could also be adapted to treat other autoimmune skin diseases such as vitiligo, atopic dermatitis, and psoriasis, the researchers say.
“This innovative approach marks a paradigm shift. Rather than suppressing the immune system, we’re now focusing on regulating it precisely at the site of antigen encounter to generate immune tolerance,” says Natalie Artzi, a principal research scientist in MIT’s Institute for Medical Engineering and Science, an associate professor of medicine at Harvard Medical School and Brigham and Women’s Hospital, and an associate faculty member at the Wyss Institute of Harvard University.
Artzi and Jamil R. Azzi, an associate professor of medicine at Harvard Medical School and Brigham and Women’s Hospital, are the senior authors of the new study , which appears in the journal Advanced Materials . Nour Younis, a Brigham and Women’s postdoc, and Nuria Puigmal, a Brigham and Women’s postdoc and former MIT research affiliate, are the lead authors of the paper.
The researchers are now working on launching a company to further develop the technology, led by Puigmal, who was recently awarded a Harvard Business School Blavatnik Fellowship.
Direct delivery
Alopecia areata, which affects more than 6 million Americans, occurs when the body’s own T cells attack hair follicles, leading the hair to fall out. The only treatment available to most patients — injections of immunosuppressant steroids into the scalp — is painful and patients often can’t tolerate it.
Some patients with alopecia areata and other autoimmune skin diseases can also be treated with immunosuppressant drugs that are given orally, but these drugs lead to widespread suppression of the immune system, which can have adverse side effects.
“This approach silences the entire immune system, offering relief from inflammation symptoms but leading to frequent recurrences. Moreover, it increases susceptibility to infections, cardiovascular diseases, and cancer,” Artzi says.
A few years ago, at a working group meeting in Washington, Artzi happened to be seated next to Azzi (the seating was alphabetical), an immunologist and transplant physican who was seeking new ways to deliver drugs directly to the skin to treat skin-related diseases.
Their conversation led to a new collaboration, and the two labs joined forces to work on a microneedle patch to deliver drugs to the skin. In 2021, they reported that such a patch can be used to prevent rejection following skin transplant. In the new study, they began applying this approach to autoimmune skin disorders.
“The skin is the only organ in our body that we can see and touch, and yet when it comes to drug delivery to the skin, we revert to systemic administration. We saw great potential in utilizing the microneedle patch to reprogram the immune system locally,” Azzi says.
The microneedle patches used in this study are made from hyaluronic acid crosslinked with polyethylene glycol (PEG), both of which are biocompatible and commonly used in medical applications. With this delivery method, drugs can pass through the tough outer layer of the epidermis, which can’t be penetrated by creams applied to the skin.
“This polymer formulation allows us to create highly durable needles capable of effectively penetrating the skin. Additionally, it gives us the flexibility to incorporate any desired drug,” Artzi says. For this study, the researchers loaded the patches with a combination of the cytokines IL-2 and CCL-22. Together, these immune molecules help to recruit regulatory T cells, which proliferate and help to tamp down inflammation. These cells also help the immune system learn to recognize that hair follicles are not foreign antigens, so that it will stop attacking them.
Hair regrowth
The researchers found that mice treated with this patch every other day for three weeks had many more regulatory T cells present at the site, along with a reduction in inflammation. Hair was able to regrow at those sites, and this growth was maintained for several weeks after the treatment ended. In these mice, there were no changes in the levels of regulatory T cells in the spleen or lymph nodes, suggesting that the treatment affected only the site where the patch was applied.
In another set of experiments, the researchers grafted human skin onto mice with a humanized immune system. In these mice, the microneedle treatment also induced proliferation of regulatory T cells and a reduction in inflammation.
The researchers designed the microneedle patches so that after releasing their drug payload, they can also collect samples that could be used to monitor the progress of the treatment. Hyaluronic acid causes the needles to swell about tenfold after entering the skin, which allows them to absorb interstitial fluid containing biomolecules and immune cells from the skin.
Following patch removal, researchers can analyze samples to measure levels of regulatory T cells and inflammation markers. This could prove valuable for monitoring future patients who may undergo this treatment.
The researchers now plan to further develop this approach for treating alopecia, and to expand into other autoimmune skin diseases.
The research was funded by the Ignite Fund and Shark Tank Fund awards from the Department of Medicine at Brigham and Women’s Hospital.
Share this news article on:
Related links.
- Natalie Artzi
- Institute for Medical Engineering and Science
Related Topics
- Drug delivery
- Health sciences and technology
- Institute for Medical Engineering and Science (IMES)
Related Articles

A sprayable gel could make minimally invasive surgeries simpler and safer

Patch that delivers drug, gene, and light-based therapy to tumor sites shows promising results

MIT researchers design tailored tissue adhesives
Previous item Next item
More MIT News

Scientists develop an affordable sensor for lead contamination
Read full story →

MIT researchers discover the universe’s oldest stars in our own galactic backyard

Four from MIT named 2024 Knight-Hennessy Scholars

Taking RNAi from interesting science to impactful new treatments
The power of App Inventor: Democratizing possibilities for mobile applications

Using MRI, engineers have found a way to detect light deep in the brain
- More news on MIT News homepage →
Massachusetts Institute of Technology 77 Massachusetts Avenue, Cambridge, MA, USA
- Map (opens in new window)
- Events (opens in new window)
- People (opens in new window)
- Careers (opens in new window)
- Accessibility
- Social Media Hub
- MIT on Facebook
- MIT on YouTube
- MIT on Instagram
What the results of Wegovy’s longest clinical trial yet show about weight loss, side effects and heart protection
Four-year data from a clinical trial on Wegovy sheds light on how it helps people lose weight and additional ways it may protect the heart. Credit: Hannah Beier/Reuters via CNN Newsource
(CNN) — New analyses of the longest clinical trial yet of the weight-loss drug Wegovy are shedding light on how quickly it helps people lose weight, how long they sustain that weight loss and how safe the medicine is over four years of use.
The analyses – of a trial called Select, whose results showed last year that Wegovy significantly reduced heart risk in addition to helping with weight loss – also suggest that the drug may protect the heart in ways beyond weight loss alone, researchers said, raising new questions about how the wildly popular medicines in this drug class should be used – and covered by insurers.
“The implications are profound,” said Dr. Harlan Krumholz , a cardiologist and scientist at Yale University and Yale New Haven Hospital who was not involved in the research, noting that a second study this week showed a similar finding for heart failure. “We have not encountered a drug with such a breadth of heart benefits.”
More than 25,000 people in the US are starting Wegovy every week, drugmaker Novo Nordisk said this month. And in a KFF poll released Friday, 6% of respondents said they were currently using a drug in this class, known as GLP-1 receptor agonists. That translates to more than 15 million Americans.
One important question about these blockbuster medicines is how widely – and how long – they’ve been studied. The Select trial, which was funded by Novo Nordisk, showed last year that Wegovy reduced the risk of a heart attack, stroke or heart-related death by 20% in people with existing cardiovascular risk with obesity or who are overweight. It included more than 17,600 people from 41 countries between 2018 and 2021 and followed them for several years.
Researchers have continued to mine the data, and the new analyses, presented Monday at the European Congress on Obesity and published in the journal Nature Medicine , show results for people taking Wegovy as long as four years. Here are some major takeaways:
Weight loss continued for more than a year
The analysis showed an average weight loss of just over 10% for people who used semaglutide, the active ingredient in Wegovy, compared with 1.5% for study participants who got a placebo. The researchers, led by Dr. Donna Ryan of Pennington Biomedical Research Center in Baton Rouge, Louisiana, noted that the trend showed that participants on the medication typically lost weight for about 65 weeks, or a year and three months, before reaching a plateau.
A previous clinical trial showed even greater average weight loss for Wegovy: about 15% on average over 68 weeks, compared with 2.4% for people who got a placebo. The researchers on the new analysis noted that, in addition to some differences in the people who enrolled in each trial, the previous study was designed specifically for weight loss and included more structured lifestyle interventions about diet and exercise compared with the Select trial, which was designed to test whether the drug prevented cardiac events.
It was sustained for up to four years
The results showed that the 10% average weight loss for people using Wegovy was sustained for up to 208 weeks, or four years.
Patients stayed on the medicine while they sustained the weight loss. Other studies have shown that many people regain weight after stopping the drugs, including one published in December from Novo Nordisk competitor Eli Lilly: People using the GLP-1 drug Zepbound, which uses the active ingredient tirzepatide and targets a second hormone called GIP, lost an average of 21% of their body weight over 36 weeks. The participants were then split into two groups, and those who stayed on the medicine lost an additional 5.5% of their body weight, while those who unknowingly switched to a placebo regained 14% of their weight.
However, not everybody regained so much weight. The study also looked at how many people maintained at least 80% of the weight loss after the initial 36 weeks, and while many more who continued on the drug did – almost 90% – almost 17% of people who were switched to a placebo maintained that much weight loss without the drug.
Results vary for everyone
In the new analysis, the researchers reported that after two years, about 68% of people taking Wegovy had lost at least 5% of their body weight, while 21% of people on a placebo did. Almost 23% of people on Wegovy lost at least 15% of their body weight, compared with 1.7% on a placebo. And almost 5% of people on the drug lost more than 25% of their body weight, compared with 0.1% on placebo, showing that the top-line findings from studies are just averages; everyone has a different experience with medicines.
No safety surprises out to four years
Overall, more people on Wegovy decided to stop participating in the trial because of side effects than people who got a placebo: 17% of those on the drug versus 8% on placebo, a result that was previously reported. And the side effects were ones that are widely known with these medicines: mainly gastrointestinal disorders like nausea, diarrhea, vomiting and constipation, which usually affected people in the first few months of the study as the dose of the medicine increased.
The researchers noted that there were no new safety signals seen in the latest analyses. Acute pancreatitis, or inflammation of the pancreas, wasn’t seen at a higher rate among those on Wegovy than placebo, although gallbladder disorders like gallstones were: 2.8% for people on Wegovy, compared with 2.3% for people on placebo. Both are included in warnings in the drug’s prescribing information because they’d been seen previously in trials.
Benefits beyond weight loss
A key question when the full results of the Select trial were initially presented was whether the 20% reduction in heart risk was driven by weight-loss alone or some other protective effect of the drug. The new analysis suggests that there is something else at play.
That’s because the reduction in risk of heart attack or other events was seen even in people using Wegovy who didn’t lose weight.
“You probably don’t even need to lose weight to get the cardiovascular benefit” with semaglutide and similar medicines, said Dr. Daniel Drucker, a pioneer of research into GLP-1 at the University of Toronto who wasn’t involved in the new analyses. “That’s because that’s what GLP-1 does: It’s cardio-protective, at least in animals, independent of whether or not you have diabetes, independent of whether you have obesity, and you don’t require weight loss – it’s not the whole story.”
An analysis led by John Deanfield of University College London found that the reduction in major adverse cardiovascular events in the study for those on Wegovy, compared with placebo, was similar among people who lost 5% or more of their body weight and those who lost less than that or even those who gained weight.
“This suggests alternative mechanisms of improved cardiovascular outcome beyond reduction in adiposity,” or body fat, the researchers concluded.
A separate study published Monday about heart failure, for which Wegovy has shown a major benefit, suggested the same thing, Krumholz said.
“These two studies show that these anti-obesity medications are also heart-health drugs,” he wrote in an email. “The benefits to the heart for people with established cardiovascular disease or a certain type of heart failure occur regardless of the amount of weight loss.”
A benefit from reducing inflammation
Drucker suspects that GLP-1 drugs provide these kinds of benefits by reducing inflammation.
“We can’t ignore the reduction in blood pressure or triglycerides, and the reduction in body weight must help a little bit, and glucose must help a little as well,” he said.
But based on his lab’s research, he said, “one of my favorite theories is inflammation, because we know that people with cardiovascular disease do have increased inflammation in their blood vessels and in the heart.”
Drucker said studies have shown that GLP-1 drugs tamp down harmful inflammation, which his lab is studying. He even noted that he receives communications from people with conditions like Covid-related brain fog, ulcerative colitis and arthritis – driven by inflammation – who think their symptoms have improved while using GLP-1 medicines. Those links would need to be borne out in clinical studies to be considered definitive.
The results in the Select trial, he said, raise the question of whether people who don’t have obesity or aren’t overweight but who have had a heart attack or stroke could benefit from taking a drug like Wegovy to prevent another event – another thing that would need to be studied.
And, Drucker said, the results suggest that insurers should cover the medicines, which cost about $1,000 per month or more without it, more widely.
“We probably really need to rethink these criteria for reimbursing the medicines, because they are going to be helpful in terms of actually improving health and saving lives and saving health care dollars in people with obesity and heart disease even without much weight loss,” he said. “You don’t even need to lose weight to have a reduction in heart attack, strokes and death.”
(Copyright (c) 2024 CNN. All Rights Reserved. This material may not be published, broadcast, rewritten, or redistributed.)
- 7WEATHER: Terrific Tuesday
- LIVE STREAM: Watch live coverage of Karen Read trial
- LIVE UPDATES: Karen Read murder trial, day 11
- One seriously injured in bad multi-car crash in Andover
Google DeepMind and Isomorphic Labs reveal AI able to predict large swathes of molecular biology

Alphabet’s Google DeepMind and its sister company Isomorphic Labs have created a new AI model that they say can help predict both the structure and interaction of most molecules involved in biological processes, including proteins, DNA, RNA, and some of chemicals used to create new medicines. The new model is a potentially giant leap for biological research. The companies are allowing researchers working on non-commerical projects to query the model for free through an internet-based interface.
Isomorphic Labs, which was spun out of Google DeepMind, has also begun using the system internally to speed its efforts to discover new drugs. The company currently has partnerships with Eli Lilly and Novartis aimed at developing multiple drugs, although the specifics of which diseases the companies are targeting has not been revealed. Proteins are the building blocks of life and their interactions with one another and with other molecules are the mechanism through which life’s processes happen. Being able to predict those interactions more accurately will help researchers advance science. by helping them understand the mechanism behind diseases, and, potentially, how to better treat and cure them. Called AlphaFold 3, the new AI software represents a major update and expansion of capabilities beyond Google DeepMind’s previous AlphaFold 2 system . Researchers from the companies published a paper on AlphaFold 3 today in the prestigious scientific journal Nature . Demis Hassabis, who serves as CEO of both Google DeepMind and Isomorphic, described the new model’s interaction predictions as “incredibly important for drug discovery.” John Jumper, the senior researcher who heads the protein structure team at Google DeepMind, described AlphaFold 3 as “an evolution of AlphaFold 2, but a really big one that opens up new avenues.” He also said he was excited to see what researchers would do with the new model, noting that AlphaFold 2 had already opened up new areas of biological research that he could never have imagined. AlphaFold 2 has been cited more than 20,000 times in other published scientific papers and has been used to work on drugs for malaria, cancer, and many other diseases.
AlphaFold 2 and 3
Debuted in late 2020, AlphaFold 2 solved a grand scientific challenge because it was able to accurately predict the structure of most proteins simply from their DNA sequence. The company later published the system’s predicted structures for all 200 million proteins with known DNA sequences and made them freely available to scientists in a massive database. Prior to this, only about 100,000 proteins had known structural information. Knowing the shape and structure of a protein is often a key part of understanding how it will function. But proteins do not work in isolation. And AlphaFold 2 was not designed to predict how proteins would interact with one another—although scientists soon found ways to modify AlphaFold 2 to make some of these predictions. Nor could AlphaFold 2 predict protein interactions with other kinds of molecules, such as DNA, RNA, ligands, and ions, that are found inside living things. It also could not predict the interaction of these other molecules with one another. AlphaFold 3 can. The system is not always accurate, but represents a major leap forward in performance. According to tests conducted by Google DeepMind and Isomorphic, AlphaFold 3 can accurately predict 76% of protein interactions with small molecules, compared to 52% for the previous best predictive software. It can predict 65% of DNA interactions compared to the next leading system, which only achieves 28%. And in protein to protein interactions, it can predict 62% accurately, more than doubling what AlphaFold 2 could do. Like AlphaFold 2, AlphaFold 3 also includes a confidence score alongside its predictions that give scientists some indication of whether they should trust the system’s output. This reduces the chance that the AI model will experience the sort of “hallucinations”—plausible but inaccurate outputs—that have plagued recent generative AI models. Jumper said that so far researchers have found these confidence scores to be highly correlated with whether the structural and interaction predictions are accurate. In other words, the system is not likely to be confidently wrong. There are a few classes of proteins where AlphaFold 3 is still not accurate. These include proteins that scientists consider “intrinsically disordered,” meaning they only assume a particular structure in the presence of another protein or molecule, perhaps changing their shape radically depending on circumstance, according to Max Jaderberg, the chief AI scientist at Isomorphic Labs.
Bioweapons worries
While many, including former Google DeepMind cofounder Mustafa Suleyman , who is now heading up a new consumer AI division at Microsoft , and Dario Amodei, the confounder and CEO of Google DeepMind rival Anthropic, have warned that rapid advances in AI may lead to the proliferation of bioweapons by radically lowering the knowledge barrier to creating deadly pathogens, Jumper said Google DeepMind and Isomorphic had consulted more than 50 experts in biosecurity, bioethics, and AI safety and concluded that the marginal risk AlphaFold 3 might present in terms of bioweapons creation was far outweighed by the system’s potential benefits to science, including advancing human understanding of disease and finding possible treatments.
The two companies are also only allowing access to the model through an internet service that allows outside researchers to prompt the system and receive a prediction, but does not give them access to the model itself or its underlying computer code. Unlike some efforts to create large language models (LLMs) for biology that can be prompted in natural language to produce a formula for a compound with particular properties, AlphaFold 3 still requires someone to have a fairly good understanding of biology to use it effectively. In addition, any suggested molecular structure it predicts would still need to be produced or isolated in a lab, a process that also requires relatively specialized knowledge. AlphaFold 3 uses a significantly different AI design than its predecessor AlphaFold 2. While both AI models are based around transformers, a kind of artificial neural network architecture pioneered by Google researchers in 2017, Jumper said the team working on the new system replaced entire “blocks” of the large transformer that powered AlphaFold 2.
AlphaFold 2 relied heavily on evolutionary information about the proteins for which it was trying to predict structures, while AlphaFold 3 leans on this evolutionary signal far less, using it only at the first step of its structure prediction. Instead, the new system devotes the majority of its components to working through the physical shape of the molecules it is making predictions about.
AlphaFold 3 also uses a diffusion model, similar to ones used for popular text-to-image generation models such as OpenAI’s DALL-E 3 or Midjourney, to learn how to puzzle out the precise atomic structures of molecules. Overall, despite covering far more substances than AlphaFold 2, AlphaFold 3 is a simpler design, with fewer separate components, than its predecessor.
Latest in Tech

Tesla—which never buys ads—is buying ads to promote Elon Musk’s record $52 billion pay deal days before key shareholder vote

24/7 trading is already in full swing. Now Wall Street is considering ditching the opening and closing bells altogether

Biden administration makes increased China tariffs official, slapping 102.5% taxes on EVs and 50% duties on solar cells and chips

Exclusive: Jyoti Bansal-led Harness has raised $150 million in debt financing

After selling his startup for a life-changing $3.7 billion, Jyoti Bansal launched a VC firm and two high-value startups. Why?

Overcapacity is a ‘fake concept’, says the international head of a major Chinese carmaker: ‘They don’t know what is happening in my house’
Most popular.

The collapsed Baltimore bridge will be demolished soon, and the crew of the ship that’s trapped underneath will be onboard when the explosives go off

The housing crisis in the U.S. is flipped upside down in Japan, where each home that’s occupied could be next to an empty one by 2033

Meet the boomers who’d rather spend $100k to renovate their homes than risk the frozen housing market: ‘It would be too hard to purchase anything else’

Hedge fund billionaire Ken Griffin says college protests are the result of a ‘cultural revolution’ and Harvard should ’embrace our Western values’

TV chef Gordon Ramsay spends an extra $7.6 million on staff as U.K. restaurant empire losses triple

Meet the 81-year-old CEO who built a $10.4 billion luxury cruise line tailored just for baby boomers: ‘They’re the richest group we have around’
- Computer Vision
- Federated Learning
- Reinforcement Learning
- Natural Language Processing
- New Releases
- AI Dev Tools
- Advisory Board Members
- 🐝 Partnership and Promotion
Existing research in molecular representation learning has leveraged models like Denoising Diffusion Probabilistic Models (DDPMs) for generating accurate molecular structures by transforming random noise into structured data. Models such as GeoDiff and Torsional Diffusion have emphasized the importance of 3D molecular conformation, enhancing the prediction of molecular properties. Furthermore, methods integrating substructural details, like GeoMol, have improved by considering the connectivity and arrangement of atoms within molecules, advancing the field through more nuanced and precise modeling techniques.
International Digital Economy Academy (IDEA) researchers have introduced SubGDiff, a novel diffusion model aimed at enhancing molecular representation by strategically incorporating subgraph details into the diffusion process. This integration allows for a more nuanced understanding and representation of molecular structures, setting SubGDiff apart from traditional models. The key innovation of SubGDiff lies in its ability to leverage subgraph prediction within its methodology, thus allowing the model to maintain essential structural relationships and features critical for accurate molecular property prediction.
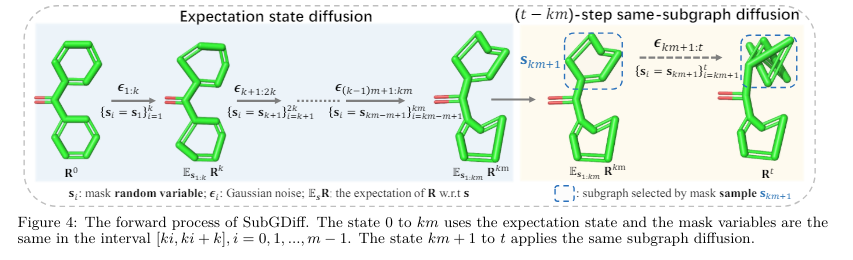
SubGDiff’s methodology centers around three principal techniques: subgraph prediction, expectation state diffusion, and k-step same-subgraph diffusion. For validation and training, the model utilizes the PCQM4Mv2 dataset, part of the larger PubChemQC project known for its extensive collection of molecular structures. SubGDiff’s approach integrates these techniques to improve the learning process by enhancing the model’s responsiveness to the intrinsic substructural features of molecules. This is achieved by employing a continuous diffusion process adjusted to focus on relevant subgraphs, thus preserving critical molecular information throughout the learning phase. This structured methodology enables SubGDiff to achieve superior performance in molecular property prediction tasks.
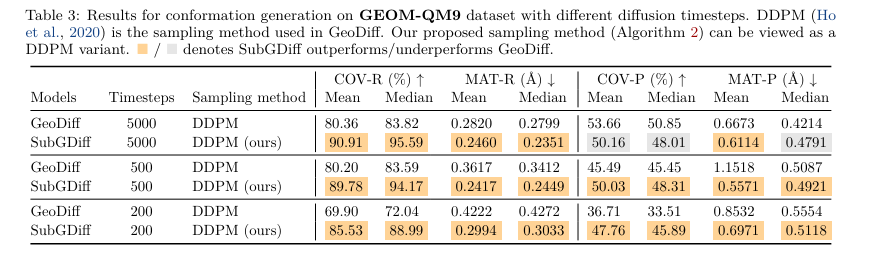
SubGDiff has shown impressive results in molecular property prediction, significantly outperforming standard models. In benchmark testing, SubGDiff reduced mean absolute error by up to 20% compared to traditional diffusion models like GeoDiff. Furthermore, it demonstrated a 15% increase in accuracy on the PCQM4Mv2 dataset for predicting quantum mechanical properties. These outcomes underscore SubGDiff’s effective use of molecular substructures, resulting in more accurate predictions and enhanced performance across various molecular representation tasks.
To conclude, SubGDiff significantly advances molecular representation learning by integrating subgraph information into the diffusion process. This novel approach allows for a more detailed and accurate depiction of molecular structures, leading to enhanced performance in property prediction tasks. The model’s ability to incorporate essential substructural details sets a new standard for predictive accuracy. It highlights its potential to significantly improve outcomes in drug discovery and material science, where precise molecular understanding is crucial.
Check out the Paper . All credit for this research goes to the researchers of this project. Also, don’t forget to follow us on Twitter . Join our Telegram Channel , Discord Channel , and LinkedIn Gr oup .
If you like our work, you will love our newsletter..
Don’t Forget to join our 42k+ ML SubReddit

Nikhil is an intern consultant at Marktechpost. He is pursuing an integrated dual degree in Materials at the Indian Institute of Technology, Kharagpur. Nikhil is an AI/ML enthusiast who is always researching applications in fields like biomaterials and biomedical science. With a strong background in Material Science, he is exploring new advancements and creating opportunities to contribute.
- Nikhil https://www.marktechpost.com/author/nikhil0980/ This AI Paper Presents SliCK: A Knowledge Categorization Framework for Mitigating Hallucinations in Language Models Through Structured Training
- Nikhil https://www.marktechpost.com/author/nikhil0980/ This AI Paper by the University of Michigan Introduces MIDGARD: Advancing AI Reasoning with Minimum Description Length
- Nikhil https://www.marktechpost.com/author/nikhil0980/ This AI Paper by Microsoft and Tsinghua University Introduces YOCO: A Decoder-Decoder Architectures for Language Models
- Nikhil https://www.marktechpost.com/author/nikhil0980/ This AI Paper by Alibaba Group Introduces AlphaMath: Automating Mathematical Reasoning with Monte Carlo Tree Search
RELATED ARTICLES MORE FROM AUTHOR
Large language model (llm) training data is running out. how close are we to the limit, openai launches chatgpt desktop app: enhancing productivity for mac users, top books on deep learning and neural networks, radonc-gpt: leveraging meta llama for a pioneering radiation oncology model, this ai paper presents slick: a knowledge categorization framework for mitigating hallucinations in language models through structured training, generative ai in marketing and sales: a comprehensive review, large language model (llm) training data is running out. how close are we to..., this ai paper presents slick: a knowledge categorization framework for mitigating hallucinations in language..., microsoft researchers propose dig: transforming molecular modeling with deep learning for equilibrium distribution prediction, advances and challenges in drone detection and classification techniques, microsoft researchers introduce syntheseus: a machine learning benchmarking python library for end-to-end retrosynthetic planning, breaking down barriers: scaling multimodal ai with cumo.
- AI Magazine
- Privacy & TC
- Cookie Policy
🐝 🐝 Join the Fastest Growing AI Research Newsletter Read by Researchers from Google + NVIDIA + Meta + Stanford + MIT + Microsoft and many others...
Thank You 🙌
Privacy Overview
IMAGES
VIDEO
COMMENTS
0.2%-5% for males depending on sport; 0.0%-1.6% for females depending on sport over past year 7, 8. Professional football players (self report) 9% used at some point in career 8. Competitive power lifters (self report) 67% used at some point in career 8. Cannabis. College athletes (self report) 28% over past year 7.
Conclusion. It is concluded that that the effects of doping on athletes are so significant, which gives many hormonal changes, damage to body tissues, mal social, to death. Substance abuse and methods of doping result in physical mall effects and are mentally or psychologically categorized as abnormal. Previous. Doping.
Destroying the trickle-down legacy. Although research suggests that the positive "trickle-down" impact of elite sports on public health may be more theoretical than real [14], the disillusionment caused through rumours of ubiquitous PED use cannot be helping in translating podium success to playground inspiration.Even worse, the increasing use of PEDs amongst recreational athletes suggests ...
Drug Testing and Analysis is a specialist journal covering sports doping, recreational drugs, pharmaceuticals, toxico-pathology, forensics, and the environment. Abstract The use of performance-enhancing substances not only undermines the core values of sports but also poses significant health risks to athletes.
Evidence for the ergogenic efficacy of many stimulants on sports performance is often equivocal and the use of such drugs can entail serious health risks including hyperthermia, stroke, respiratory and cardiac arrest. 99 A difficulty with clinical research on the ergogenicity of stimulants is that the laboratory/experimental setting can rarely ...
Current knowledge about doping prevalence in competitive sport relies upon weak and disparate evidence. To address this, we offer a comprehensive set of assessment criteria for studies examining doping behavior data as evidence for doping prevalence. To facilitate future evidence syntheses and meta- …
Interest in AAS persists as research identifies new information regarding the performance and health aspects of the drugs and through stories of purported use in the sports world. The World Anti-Doping Agency (WADA) has developed new antidoping measures, including blood sampling, guidelines for international information gathering and sharing ...
This article is an update of the 2006 adverse cardiovascular effects of doping in athletes position paper published by the European Society of Cardiology sports cardiology study group. 8 The objective of this position paper is to raise awareness and to inform cardiologists, physicians, and sport enthusiasts of the adverse cardiovascular effects ...
AJOB Primary Research, November 2012. doi: 10.1080/21507716.2012.720639. Abstract: "This article compares public attitudes toward the use of prescription drugs for cognitive enhancement with the use of performance enhancing drugs in sport. We explore attitudes toward the acceptability of both practices; the extent to which familiarity with ...
Pe rformance enhancing drugs and sports. Dheeraj Kumar Mishra and Dr. Vikram Singh. Abstract. This study aims to analyze the use of PEDs or doping in the world of spo rts. Drugs allow for harder ...
Drug use and doping in sports have a long and contentious history. The allure of improved ... This research paper aims to provide a comprehensive overview of drugs and doping practices in sports, including the historical context, types of drugs commonly used, their effects on athletes' performance and health, the detection and prevention ...
Journal of Y oung Pharmacists, Vol 11, Issue 4, Oct-Dec, 2019 344. Review Article. An Overview of Performance Enhancing Drugs (PED' s) in Sports. and W ADA. Karri Sowjanya, Chandrashekaran ...
Drug Abuse in Sports and Its Psychological Effects on Athletes Dr. J.B. Vipene ... The paper examined drugs and its abuses in competitive sports. The type of drugs that are banned in sports, that ... Research on Humanities and Social Sciences www.iiste.org ISSN (Paper)2224-5766 ISSN (Online)2225-0484 (Online) Vol.5, No.5, 2015 142 monetary ...
Drug abuse in athletes. Drug abuse occurs in all sports and at most levels of competition. Athletic life may lead to drug abuse for a number of reasons, including for performance enhancement, to self-treat otherwise untreated mental illness, and to deal with stressors, such as pressure to perform, injuries, physical pain, and retirement from ...
Research Paper Drug Abuse in Sports: Types, Potential Side-Effects and Rehabilitation Program for Sportspersons K. KALEEMULLA Physical Education Director, Anjuman Arts, Science, Commerce College and PG Center, Bhatkal - 581320 Uttar Kannada, Karwar District, Karnataka. Abstract: Drug abuse occurs in all sports and at most levels of competition.
Drugs In Sports Research Paper. The nature of sports promotes a strong desire to win, and many athletes will do anything to rise to the top. Every elite athlete wants to get an edge over their competition, causing many athletes to turn to performance enhancing drugs to gain this edge. Drug use in sport can cost players their super stardom dream ...
Drugs In Sports Research Paper. Satisfactory Essays. 378 Words. 2 Pages. Open Document. Professional athletes today are under such competitive pressure that they can resort to drugs. Competitive sports can be a cause for an exceeding amount of pressure that can cause good, talented people turn to drugs. This is a problem because drugs can ruin ...
Neuropathic pain is a debilitating condition characterized by abnormal signaling within the nervous system, resulting in persistent and often intense sensations of pain. It can arise from various causes, including traumatic nerve injury, neuropathy, and certain diseases. We present an overview of current and emerging pharmacotherapies for neuropathic pain, focusing on novel drug targets and ...
The Bay Area Laboratory Co-operative (BALCO) was at the center of a doping scandal that implicated numerous athletes across various sports, including Bonds. Bonds was accused of using performance-enhancing drugs supplied by BALCO, specifically the designer steroid tetrahydrogestrinone (THG), commonly known as "The Clear."
Caption: The microneedle patches used in this study are made from hyaluronic acid crosslinked with polyethylene glycol (PEG), both of which are biocompatible and commonly used in medical applications. The researchers designed the microneedle patches so that after releasing their drug payload, they can also collect samples that could be used to monitor the progress of the treatment.
(CNN) — New analyses of the longest clinical trial yet of the weight-loss drug Wegovy are shedding light on how quickly it helps people lose weight, how long they sustain that weight loss and ...
AlphaFold 2 has been cited more than 20,000 times in other published scientific papers and has been used to work on drugs for malaria, cancer, and many other diseases.
In the area of drug formulation design, this paper systematically discusses the development strategies for solid, liquid, and semi-solid dosage forms based on the unique physicochemical properties of Taxus extracts, their intended medical uses, and specific release characteristics, delving deeply into the selection of excipients and the ...
Molecular representation learning is an essential field focusing on understanding and predicting molecular properties through advanced computational models. It plays a significant role in drug discovery and material science, providing insights by analyzing molecular structures. The fundamental challenge in molecular representation learning involves efficiently capturing the intricate 3D ...