
21 Research Objectives Examples (Copy and Paste)

Research objectives refer to the definitive statements made by researchers at the beginning of a research project detailing exactly what a research project aims to achieve.
These objectives are explicit goals clearly and concisely projected by the researcher to present a clear intention or course of action for his or her qualitative or quantitative study.
Research objectives are typically nested under one overarching research aim. The objectives are the steps you’ll need to take in order to achieve the aim (see the examples below, for example, which demonstrate an aim followed by 3 objectives, which is what I recommend to my research students).
Research Objectives vs Research Aims
Research aim and research objectives are fundamental constituents of any study, fitting together like two pieces of the same puzzle.
The ‘research aim’ describes the overarching goal or purpose of the study (Kumar, 2019). This is usually a broad, high-level purpose statement, summing up the central question that the research intends to answer.
Example of an Overarching Research Aim:
“The aim of this study is to explore the impact of climate change on crop productivity.”
Comparatively, ‘research objectives’ are concrete goals that underpin the research aim, providing stepwise actions to achieve the aim.
Objectives break the primary aim into manageable, focused pieces, and are usually characterized as being more specific, measurable, achievable, relevant, and time-bound (SMART).
Examples of Specific Research Objectives:
1. “To examine the effects of rising temperatures on the yield of rice crops during the upcoming growth season.” 2. “To assess changes in rainfall patterns in major agricultural regions over the first decade of the twenty-first century (2000-2010).” 3. “To analyze the impact of changing weather patterns on crop diseases within the same timeframe.”
The distinction between these two terms, though subtle, is significant for successfully conducting a study. The research aim provides the study with direction, while the research objectives set the path to achieving this aim, thereby ensuring the study’s efficiency and effectiveness.
How to Write Research Objectives
I usually recommend to my students that they use the SMART framework to create their research objectives.
SMART is an acronym standing for Specific, Measurable, Achievable, Relevant, and Time-bound. It provides a clear method of defining solid research objectives and helps students know where to start in writing their objectives (Locke & Latham, 2013).
Each element of this acronym adds a distinct dimension to the framework, aiding in the creation of comprehensive, well-delineated objectives.
Here is each step:
- Specific : We need to avoid ambiguity in our objectives. They need to be clear and precise (Doran, 1981). For instance, rather than stating the objective as “to study the effects of social media,” a more focused detail would be “to examine the effects of social media use (Facebook, Instagram, and Twitter) on the academic performance of college students.”
- Measurable: The measurable attribute provides a clear criterion to determine if the objective has been met (Locke & Latham, 2013). A quantifiable element, such as a percentage or a number, adds a measurable quality. For example, “to increase response rate to the annual customer survey by 10%,” makes it easier to ascertain achievement.
- Achievable: The achievable aspect encourages researchers to craft realistic objectives, resembling a self-check mechanism to ensure the objectives align with the scope and resources at disposal (Doran, 1981). For example, “to interview 25 participants selected randomly from a population of 100” is an attainable objective as long as the researcher has access to these participants.
- Relevance : Relevance, the fourth element, compels the researcher to tailor the objectives in alignment with overarching goals of the study (Locke & Latham, 2013). This is extremely important – each objective must help you meet your overall one-sentence ‘aim’ in your study.
- Time-Bound: Lastly, the time-bound element fosters a sense of urgency and prioritization, preventing procrastination and enhancing productivity (Doran, 1981). “To analyze the effect of laptop use in lectures on student engagement over the course of two semesters this year” expresses a clear deadline, thus serving as a motivator for timely completion.
You’re not expected to fit every single element of the SMART framework in one objective, but across your objectives, try to touch on each of the five components.
Research Objectives Examples
1. Field: Psychology
Aim: To explore the impact of sleep deprivation on cognitive performance in college students.
- Objective 1: To compare cognitive test scores of students with less than six hours of sleep and those with 8 or more hours of sleep.
- Objective 2: To investigate the relationship between class grades and reported sleep duration.
- Objective 3: To survey student perceptions and experiences on how sleep deprivation affects their cognitive capabilities.
2. Field: Environmental Science
Aim: To understand the effects of urban green spaces on human well-being in a metropolitan city.
- Objective 1: To assess the physical and mental health benefits of regular exposure to urban green spaces.
- Objective 2: To evaluate the social impacts of urban green spaces on community interactions.
- Objective 3: To examine patterns of use for different types of urban green spaces.
3. Field: Technology
Aim: To investigate the influence of using social media on productivity in the workplace.
- Objective 1: To measure the amount of time spent on social media during work hours.
- Objective 2: To evaluate the perceived impact of social media use on task completion and work efficiency.
- Objective 3: To explore whether company policies on social media usage correlate with different patterns of productivity.
4. Field: Education
Aim: To examine the effectiveness of online vs traditional face-to-face learning on student engagement and achievement.
- Objective 1: To compare student grades between the groups exposed to online and traditional face-to-face learning.
- Objective 2: To assess student engagement levels in both learning environments.
- Objective 3: To collate student perceptions and preferences regarding both learning methods.
5. Field: Health
Aim: To determine the impact of a Mediterranean diet on cardiac health among adults over 50.
- Objective 1: To assess changes in cardiovascular health metrics after following a Mediterranean diet for six months.
- Objective 2: To compare these health metrics with a similar group who follow their regular diet.
- Objective 3: To document participants’ experiences and adherence to the Mediterranean diet.
6. Field: Environmental Science
Aim: To analyze the impact of urban farming on community sustainability.
- Objective 1: To document the types and quantity of food produced through urban farming initiatives.
- Objective 2: To assess the effect of urban farming on local communities’ access to fresh produce.
- Objective 3: To examine the social dynamics and cooperative relationships in the creating and maintaining of urban farms.
7. Field: Sociology
Aim: To investigate the influence of home offices on work-life balance during remote work.
- Objective 1: To survey remote workers on their perceptions of work-life balance since setting up home offices.
- Objective 2: To conduct an observational study of daily work routines and family interactions in a home office setting.
- Objective 3: To assess the correlation, if any, between physical boundaries of workspaces and mental boundaries for work in the home setting.
8. Field: Economics
Aim: To evaluate the effects of minimum wage increases on small businesses.
- Objective 1: To analyze cost structures, pricing changes, and profitability of small businesses before and after minimum wage increases.
- Objective 2: To survey small business owners on the strategies they employ to navigate minimum wage increases.
- Objective 3: To examine employment trends in small businesses in response to wage increase legislation.
9. Field: Education
Aim: To explore the role of extracurricular activities in promoting soft skills among high school students.
- Objective 1: To assess the variety of soft skills developed through different types of extracurricular activities.
- Objective 2: To compare self-reported soft skills between students who participate in extracurricular activities and those who do not.
- Objective 3: To investigate the teachers’ perspectives on the contribution of extracurricular activities to students’ skill development.
10. Field: Technology
Aim: To assess the impact of virtual reality (VR) technology on the tourism industry.
- Objective 1: To document the types and popularity of VR experiences available in the tourism market.
- Objective 2: To survey tourists on their interest levels and satisfaction rates with VR tourism experiences.
- Objective 3: To determine whether VR tourism experiences correlate with increased interest in real-life travel to the simulated destinations.
11. Field: Biochemistry
Aim: To examine the role of antioxidants in preventing cellular damage.
- Objective 1: To identify the types and quantities of antioxidants in common fruits and vegetables.
- Objective 2: To determine the effects of various antioxidants on free radical neutralization in controlled lab tests.
- Objective 3: To investigate potential beneficial impacts of antioxidant-rich diets on long-term cellular health.
12. Field: Linguistics
Aim: To determine the influence of early exposure to multiple languages on cognitive development in children.
- Objective 1: To assess cognitive development milestones in monolingual and multilingual children.
- Objective 2: To document the number and intensity of language exposures for each group in the study.
- Objective 3: To investigate the specific cognitive advantages, if any, enjoyed by multilingual children.
13. Field: Art History
Aim: To explore the impact of the Renaissance period on modern-day art trends.
- Objective 1: To identify key characteristics and styles of Renaissance art.
- Objective 2: To analyze modern art pieces for the influence of the Renaissance style.
- Objective 3: To survey modern-day artists for their inspirations and the influence of historical art movements on their work.
14. Field: Cybersecurity
Aim: To assess the effectiveness of two-factor authentication (2FA) in preventing unauthorized system access.
- Objective 1: To measure the frequency of unauthorized access attempts before and after the introduction of 2FA.
- Objective 2: To survey users about their experiences and challenges with 2FA implementation.
- Objective 3: To evaluate the efficacy of different types of 2FA (SMS-based, authenticator apps, biometrics, etc.).
15. Field: Cultural Studies
Aim: To analyze the role of music in cultural identity formation among ethnic minorities.
- Objective 1: To document the types and frequency of traditional music practices within selected ethnic minority communities.
- Objective 2: To survey community members on the role of music in their personal and communal identity.
- Objective 3: To explore the resilience and transmission of traditional music practices in contemporary society.
16. Field: Astronomy
Aim: To explore the impact of solar activity on satellite communication.
- Objective 1: To categorize different types of solar activities and their frequencies of occurrence.
- Objective 2: To ascertain how variations in solar activity may influence satellite communication.
- Objective 3: To investigate preventative and damage-control measures currently in place during periods of high solar activity.
17. Field: Literature
Aim: To examine narrative techniques in contemporary graphic novels.
- Objective 1: To identify a range of narrative techniques employed in this genre.
- Objective 2: To analyze the ways in which these narrative techniques engage readers and affect story interpretation.
- Objective 3: To compare narrative techniques in graphic novels to those found in traditional printed novels.
18. Field: Renewable Energy
Aim: To investigate the feasibility of solar energy as a primary renewable resource within urban areas.
- Objective 1: To quantify the average sunlight hours across urban areas in different climatic zones.
- Objective 2: To calculate the potential solar energy that could be harnessed within these areas.
- Objective 3: To identify barriers or challenges to widespread solar energy implementation in urban settings and potential solutions.
19. Field: Sports Science
Aim: To evaluate the role of pre-game rituals in athlete performance.
- Objective 1: To identify the variety and frequency of pre-game rituals among professional athletes in several sports.
- Objective 2: To measure the impact of pre-game rituals on individual athletes’ performance metrics.
- Objective 3: To examine the psychological mechanisms that might explain the effects (if any) of pre-game ritual on performance.
20. Field: Ecology
Aim: To investigate the effects of urban noise pollution on bird populations.
- Objective 1: To record and quantify urban noise levels in various bird habitats.
- Objective 2: To measure bird population densities in relation to noise levels.
- Objective 3: To determine any changes in bird behavior or vocalization linked to noise levels.
21. Field: Food Science
Aim: To examine the influence of cooking methods on the nutritional value of vegetables.
- Objective 1: To identify the nutrient content of various vegetables both raw and after different cooking processes.
- Objective 2: To compare the effect of various cooking methods on the nutrient retention of these vegetables.
- Objective 3: To propose cooking strategies that optimize nutrient retention.
The Importance of Research Objectives
The importance of research objectives cannot be overstated. In essence, these guideposts articulate what the researcher aims to discover, understand, or examine (Kothari, 2014).
When drafting research objectives, it’s essential to make them simple and comprehensible, specific to the point of being quantifiable where possible, achievable in a practical sense, relevant to the chosen research question, and time-constrained to ensure efficient progress (Kumar, 2019).
Remember that a good research objective is integral to the success of your project, offering a clear path forward for setting out a research design , and serving as the bedrock of your study plan. Each objective must distinctly address a different dimension of your research question or problem (Kothari, 2014). Always bear in mind that the ultimate purpose of your research objectives is to succinctly encapsulate your aims in the clearest way possible, facilitating a coherent, comprehensive and rational approach to your planned study, and furnishing a scientific roadmap for your journey into the depths of knowledge and research (Kumar, 2019).
Kothari, C.R (2014). Research Methodology: Methods and Techniques . New Delhi: New Age International.
Kumar, R. (2019). Research Methodology: A Step-by-Step Guide for Beginners .New York: SAGE Publications.
Doran, G. T. (1981). There’s a S.M.A.R.T. way to write management’s goals and objectives. Management review, 70 (11), 35-36.
Locke, E. A., & Latham, G. P. (2013). New Developments in Goal Setting and Task Performance . New York: Routledge.

Chris Drew (PhD)
Dr. Chris Drew is the founder of the Helpful Professor. He holds a PhD in education and has published over 20 articles in scholarly journals. He is the former editor of the Journal of Learning Development in Higher Education. [Image Descriptor: Photo of Chris]
- Chris Drew (PhD) https://helpfulprofessor.com/author/chris-drew-phd/ 15 Self-Actualization Examples (Maslow's Hierarchy)
- Chris Drew (PhD) https://helpfulprofessor.com/author/chris-drew-phd/ Forest Schools Philosophy & Curriculum, Explained!
- Chris Drew (PhD) https://helpfulprofessor.com/author/chris-drew-phd/ Montessori's 4 Planes of Development, Explained!
- Chris Drew (PhD) https://helpfulprofessor.com/author/chris-drew-phd/ Montessori vs Reggio Emilia vs Steiner-Waldorf vs Froebel
Leave a Comment Cancel Reply
Your email address will not be published. Required fields are marked *
- Privacy Policy
Home » Research Objectives – Types, Examples and Writing Guide
Research Objectives – Types, Examples and Writing Guide
Table of Contents

Research Objectives
Research objectives refer to the specific goals or aims of a research study. They provide a clear and concise description of what the researcher hopes to achieve by conducting the research . The objectives are typically based on the research questions and hypotheses formulated at the beginning of the study and are used to guide the research process.
Types of Research Objectives
Here are the different types of research objectives in research:
- Exploratory Objectives: These objectives are used to explore a topic, issue, or phenomenon that has not been studied in-depth before. The aim of exploratory research is to gain a better understanding of the subject matter and generate new ideas and hypotheses .
- Descriptive Objectives: These objectives aim to describe the characteristics, features, or attributes of a particular population, group, or phenomenon. Descriptive research answers the “what” questions and provides a snapshot of the subject matter.
- Explanatory Objectives : These objectives aim to explain the relationships between variables or factors. Explanatory research seeks to identify the cause-and-effect relationships between different phenomena.
- Predictive Objectives: These objectives aim to predict future events or outcomes based on existing data or trends. Predictive research uses statistical models to forecast future trends or outcomes.
- Evaluative Objectives : These objectives aim to evaluate the effectiveness or impact of a program, intervention, or policy. Evaluative research seeks to assess the outcomes or results of a particular intervention or program.
- Prescriptive Objectives: These objectives aim to provide recommendations or solutions to a particular problem or issue. Prescriptive research identifies the best course of action based on the results of the study.
- Diagnostic Objectives : These objectives aim to identify the causes or factors contributing to a particular problem or issue. Diagnostic research seeks to uncover the underlying reasons for a particular phenomenon.
- Comparative Objectives: These objectives aim to compare two or more groups, populations, or phenomena to identify similarities and differences. Comparative research is used to determine which group or approach is more effective or has better outcomes.
- Historical Objectives: These objectives aim to examine past events, trends, or phenomena to gain a better understanding of their significance and impact. Historical research uses archival data, documents, and records to study past events.
- Ethnographic Objectives : These objectives aim to understand the culture, beliefs, and practices of a particular group or community. Ethnographic research involves immersive fieldwork and observation to gain an insider’s perspective of the group being studied.
- Action-oriented Objectives: These objectives aim to bring about social or organizational change. Action-oriented research seeks to identify practical solutions to social problems and to promote positive change in society.
- Conceptual Objectives: These objectives aim to develop new theories, models, or frameworks to explain a particular phenomenon or set of phenomena. Conceptual research seeks to provide a deeper understanding of the subject matter by developing new theoretical perspectives.
- Methodological Objectives: These objectives aim to develop and improve research methods and techniques. Methodological research seeks to advance the field of research by improving the validity, reliability, and accuracy of research methods and tools.
- Theoretical Objectives : These objectives aim to test and refine existing theories or to develop new theoretical perspectives. Theoretical research seeks to advance the field of knowledge by testing and refining existing theories or by developing new theoretical frameworks.
- Measurement Objectives : These objectives aim to develop and validate measurement instruments, such as surveys, questionnaires, and tests. Measurement research seeks to improve the quality and reliability of data collection and analysis by developing and testing new measurement tools.
- Design Objectives : These objectives aim to develop and refine research designs, such as experimental, quasi-experimental, and observational designs. Design research seeks to improve the quality and validity of research by developing and testing new research designs.
- Sampling Objectives: These objectives aim to develop and refine sampling techniques, such as probability and non-probability sampling methods. Sampling research seeks to improve the representativeness and generalizability of research findings by developing and testing new sampling techniques.
How to Write Research Objectives
Writing clear and concise research objectives is an important part of any research project, as it helps to guide the study and ensure that it is focused and relevant. Here are some steps to follow when writing research objectives:
- Identify the research problem : Before you can write research objectives, you need to identify the research problem you are trying to address. This should be a clear and specific problem that can be addressed through research.
- Define the research questions : Based on the research problem, define the research questions you want to answer. These questions should be specific and should guide the research process.
- Identify the variables : Identify the key variables that you will be studying in your research. These are the factors that you will be measuring, manipulating, or analyzing to answer your research questions.
- Write specific objectives: Write specific, measurable objectives that will help you answer your research questions. These objectives should be clear and concise and should indicate what you hope to achieve through your research.
- Use the SMART criteria: To ensure that your research objectives are well-defined and achievable, use the SMART criteria. This means that your objectives should be Specific, Measurable, Achievable, Relevant, and Time-bound.
- Revise and refine: Once you have written your research objectives, revise and refine them to ensure that they are clear, concise, and achievable. Make sure that they align with your research questions and variables, and that they will help you answer your research problem.
Example of Research Objectives
Examples of research objectives Could be:
Research Objectives for the topic of “The Impact of Artificial Intelligence on Employment”:
- To investigate the effects of the adoption of AI on employment trends across various industries and occupations.
- To explore the potential for AI to create new job opportunities and transform existing roles in the workforce.
- To examine the social and economic implications of the widespread use of AI for employment, including issues such as income inequality and access to education and training.
- To identify the skills and competencies that will be required for individuals to thrive in an AI-driven workplace, and to explore the role of education and training in developing these skills.
- To evaluate the ethical and legal considerations surrounding the use of AI for employment, including issues such as bias, privacy, and the responsibility of employers and policymakers to protect workers’ rights.
When to Write Research Objectives
- At the beginning of a research project : Research objectives should be identified and written down before starting a research project. This helps to ensure that the project is focused and that data collection and analysis efforts are aligned with the intended purpose of the research.
- When refining research questions: Writing research objectives can help to clarify and refine research questions. Objectives provide a more concrete and specific framework for addressing research questions, which can improve the overall quality and direction of a research project.
- After conducting a literature review : Conducting a literature review can help to identify gaps in knowledge and areas that require further research. Writing research objectives can help to define and focus the research effort in these areas.
- When developing a research proposal: Research objectives are an important component of a research proposal. They help to articulate the purpose and scope of the research, and provide a clear and concise summary of the expected outcomes and contributions of the research.
- When seeking funding for research: Funding agencies often require a detailed description of research objectives as part of a funding proposal. Writing clear and specific research objectives can help to demonstrate the significance and potential impact of a research project, and increase the chances of securing funding.
- When designing a research study : Research objectives guide the design and implementation of a research study. They help to identify the appropriate research methods, sampling strategies, data collection and analysis techniques, and other relevant aspects of the study design.
- When communicating research findings: Research objectives provide a clear and concise summary of the main research questions and outcomes. They are often included in research reports and publications, and can help to ensure that the research findings are communicated effectively and accurately to a wide range of audiences.
- When evaluating research outcomes : Research objectives provide a basis for evaluating the success of a research project. They help to measure the degree to which research questions have been answered and the extent to which research outcomes have been achieved.
- When conducting research in a team : Writing research objectives can facilitate communication and collaboration within a research team. Objectives provide a shared understanding of the research purpose and goals, and can help to ensure that team members are working towards a common objective.
Purpose of Research Objectives
Some of the main purposes of research objectives include:
- To clarify the research question or problem : Research objectives help to define the specific aspects of the research question or problem that the study aims to address. This makes it easier to design a study that is focused and relevant.
- To guide the research design: Research objectives help to determine the research design, including the research methods, data collection techniques, and sampling strategy. This ensures that the study is structured and efficient.
- To measure progress : Research objectives provide a way to measure progress throughout the research process. They help the researcher to evaluate whether they are on track and meeting their goals.
- To communicate the research goals : Research objectives provide a clear and concise description of the research goals. This helps to communicate the purpose of the study to other researchers, stakeholders, and the general public.
Advantages of Research Objectives
Here are some advantages of having well-defined research objectives:
- Focus : Research objectives help to focus the research effort on specific areas of inquiry. By identifying clear research questions, the researcher can narrow down the scope of the study and avoid getting sidetracked by irrelevant information.
- Clarity : Clearly stated research objectives provide a roadmap for the research study. They provide a clear direction for the research, making it easier for the researcher to stay on track and achieve their goals.
- Measurability : Well-defined research objectives provide measurable outcomes that can be used to evaluate the success of the research project. This helps to ensure that the research is effective and that the research goals are achieved.
- Feasibility : Research objectives help to ensure that the research project is feasible. By clearly defining the research goals, the researcher can identify the resources required to achieve those goals and determine whether those resources are available.
- Relevance : Research objectives help to ensure that the research study is relevant and meaningful. By identifying specific research questions, the researcher can ensure that the study addresses important issues and contributes to the existing body of knowledge.
About the author

Muhammad Hassan
Researcher, Academic Writer, Web developer
You may also like

Assignment – Types, Examples and Writing Guide

Research Paper Title – Writing Guide and Example

Research Summary – Structure, Examples and...

Research Paper Introduction – Writing Guide and...

Context of the Study – Writing Guide and Examples

Research Gap – Types, Examples and How to...
Research Aims, Objectives & Questions
The “Golden Thread” Explained Simply (+ Examples)
By: David Phair (PhD) and Alexandra Shaeffer (PhD) | June 2022
The research aims , objectives and research questions (collectively called the “golden thread”) are arguably the most important thing you need to get right when you’re crafting a research proposal , dissertation or thesis . We receive questions almost every day about this “holy trinity” of research and there’s certainly a lot of confusion out there, so we’ve crafted this post to help you navigate your way through the fog.
Overview: The Golden Thread
- What is the golden thread
- What are research aims ( examples )
- What are research objectives ( examples )
- What are research questions ( examples )
- The importance of alignment in the golden thread
What is the “golden thread”?
The golden thread simply refers to the collective research aims , research objectives , and research questions for any given project (i.e., a dissertation, thesis, or research paper ). These three elements are bundled together because it’s extremely important that they align with each other, and that the entire research project aligns with them.
Importantly, the golden thread needs to weave its way through the entirety of any research project , from start to end. In other words, it needs to be very clearly defined right at the beginning of the project (the topic ideation and proposal stage) and it needs to inform almost every decision throughout the rest of the project. For example, your research design and methodology will be heavily influenced by the golden thread (we’ll explain this in more detail later), as well as your literature review.
The research aims, objectives and research questions (the golden thread) define the focus and scope ( the delimitations ) of your research project. In other words, they help ringfence your dissertation or thesis to a relatively narrow domain, so that you can “go deep” and really dig into a specific problem or opportunity. They also help keep you on track , as they act as a litmus test for relevance. In other words, if you’re ever unsure whether to include something in your document, simply ask yourself the question, “does this contribute toward my research aims, objectives or questions?”. If it doesn’t, chances are you can drop it.
Alright, enough of the fluffy, conceptual stuff. Let’s get down to business and look at what exactly the research aims, objectives and questions are and outline a few examples to bring these concepts to life.

Research Aims: What are they?
Simply put, the research aim(s) is a statement that reflects the broad overarching goal (s) of the research project. Research aims are fairly high-level (low resolution) as they outline the general direction of the research and what it’s trying to achieve .
Research Aims: Examples
True to the name, research aims usually start with the wording “this research aims to…”, “this research seeks to…”, and so on. For example:
“This research aims to explore employee experiences of digital transformation in retail HR.” “This study sets out to assess the interaction between student support and self-care on well-being in engineering graduate students”
As you can see, these research aims provide a high-level description of what the study is about and what it seeks to achieve. They’re not hyper-specific or action-oriented, but they’re clear about what the study’s focus is and what is being investigated.
Need a helping hand?
Research Objectives: What are they?
The research objectives take the research aims and make them more practical and actionable . In other words, the research objectives showcase the steps that the researcher will take to achieve the research aims.
The research objectives need to be far more specific (higher resolution) and actionable than the research aims. In fact, it’s always a good idea to craft your research objectives using the “SMART” criteria. In other words, they should be specific, measurable, achievable, relevant and time-bound”.
Research Objectives: Examples
Let’s look at two examples of research objectives. We’ll stick with the topic and research aims we mentioned previously.
For the digital transformation topic:
To observe the retail HR employees throughout the digital transformation. To assess employee perceptions of digital transformation in retail HR. To identify the barriers and facilitators of digital transformation in retail HR.
And for the student wellness topic:
To determine whether student self-care predicts the well-being score of engineering graduate students. To determine whether student support predicts the well-being score of engineering students. To assess the interaction between student self-care and student support when predicting well-being in engineering graduate students.
As you can see, these research objectives clearly align with the previously mentioned research aims and effectively translate the low-resolution aims into (comparatively) higher-resolution objectives and action points . They give the research project a clear focus and present something that resembles a research-based “to-do” list.

Research Questions: What are they?
Finally, we arrive at the all-important research questions. The research questions are, as the name suggests, the key questions that your study will seek to answer . Simply put, they are the core purpose of your dissertation, thesis, or research project. You’ll present them at the beginning of your document (either in the introduction chapter or literature review chapter) and you’ll answer them at the end of your document (typically in the discussion and conclusion chapters).
The research questions will be the driving force throughout the research process. For example, in the literature review chapter, you’ll assess the relevance of any given resource based on whether it helps you move towards answering your research questions. Similarly, your methodology and research design will be heavily influenced by the nature of your research questions. For instance, research questions that are exploratory in nature will usually make use of a qualitative approach, whereas questions that relate to measurement or relationship testing will make use of a quantitative approach.
Let’s look at some examples of research questions to make this more tangible.
Research Questions: Examples
Again, we’ll stick with the research aims and research objectives we mentioned previously.
For the digital transformation topic (which would be qualitative in nature):
How do employees perceive digital transformation in retail HR? What are the barriers and facilitators of digital transformation in retail HR?
And for the student wellness topic (which would be quantitative in nature):
Does student self-care predict the well-being scores of engineering graduate students? Does student support predict the well-being scores of engineering students? Do student self-care and student support interact when predicting well-being in engineering graduate students?
You’ll probably notice that there’s quite a formulaic approach to this. In other words, the research questions are basically the research objectives “converted” into question format. While that is true most of the time, it’s not always the case. For example, the first research objective for the digital transformation topic was more or less a step on the path toward the other objectives, and as such, it didn’t warrant its own research question.
So, don’t rush your research questions and sloppily reword your objectives as questions. Carefully think about what exactly you’re trying to achieve (i.e. your research aim) and the objectives you’ve set out, then craft a set of well-aligned research questions . Also, keep in mind that this can be a somewhat iterative process , where you go back and tweak research objectives and aims to ensure tight alignment throughout the golden thread.
The importance of strong alignment
Alignment is the keyword here and we have to stress its importance . Simply put, you need to make sure that there is a very tight alignment between all three pieces of the golden thread. If your research aims and research questions don’t align, for example, your project will be pulling in different directions and will lack focus . This is a common problem students face and can cause many headaches (and tears), so be warned.
Take the time to carefully craft your research aims, objectives and research questions before you run off down the research path. Ideally, get your research supervisor/advisor to review and comment on your golden thread before you invest significant time into your project, and certainly before you start collecting data .
Recap: The golden thread
In this post, we unpacked the golden thread of research, consisting of the research aims , research objectives and research questions . You can jump back to any section using the links below.
As always, feel free to leave a comment below – we always love to hear from you. Also, if you’re interested in 1-on-1 support, take a look at our private coaching service here.

Psst... there’s more!
This post was based on one of our popular Research Bootcamps . If you're working on a research project, you'll definitely want to check this out ...
You Might Also Like:
")
39 Comments

Thank you very much for your great effort put. As an Undergraduate taking Demographic Research & Methodology, I’ve been trying so hard to understand clearly what is a Research Question, Research Aim and the Objectives in a research and the relationship between them etc. But as for now I’m thankful that you’ve solved my problem.

Well appreciated. This has helped me greatly in doing my dissertation.

An so delighted with this wonderful information thank you a lot.
so impressive i have benefited a lot looking forward to learn more on research.

I am very happy to have carefully gone through this well researched article.
Infact,I used to be phobia about anything research, because of my poor understanding of the concepts.
Now,I get to know that my research question is the same as my research objective(s) rephrased in question format.
I please I would need a follow up on the subject,as I intends to join the team of researchers. Thanks once again.

Thanks so much. This was really helpful.

I know you pepole have tried to break things into more understandable and easy format. And God bless you. Keep it up

i found this document so useful towards my study in research methods. thanks so much.

This is my 2nd read topic in your course and I should commend the simplified explanations of each part. I’m beginning to understand and absorb the use of each part of a dissertation/thesis. I’ll keep on reading your free course and might be able to avail the training course! Kudos!

Thank you! Better put that my lecture and helped to easily understand the basics which I feel often get brushed over when beginning dissertation work.

This is quite helpful. I like how the Golden thread has been explained and the needed alignment.

This is quite helpful. I really appreciate!

The article made it simple for researcher students to differentiate between three concepts.

Very innovative and educational in approach to conducting research.

I am very impressed with all these terminology, as I am a fresh student for post graduate, I am highly guided and I promised to continue making consultation when the need arise. Thanks a lot.

A very helpful piece. thanks, I really appreciate it .

Very well explained, and it might be helpful to many people like me.

Wish i had found this (and other) resource(s) at the beginning of my PhD journey… not in my writing up year… 😩 Anyways… just a quick question as i’m having some issues ordering my “golden thread”…. does it matter in what order you mention them? i.e., is it always first aims, then objectives, and finally the questions? or can you first mention the research questions and then the aims and objectives?

Thank you for a very simple explanation that builds upon the concepts in a very logical manner. Just prior to this, I read the research hypothesis article, which was equally very good. This met my primary objective.
My secondary objective was to understand the difference between research questions and research hypothesis, and in which context to use which one. However, I am still not clear on this. Can you kindly please guide?

In research, a research question is a clear and specific inquiry that the researcher wants to answer, while a research hypothesis is a tentative statement or prediction about the relationship between variables or the expected outcome of the study. Research questions are broader and guide the overall study, while hypotheses are specific and testable statements used in quantitative research. Research questions identify the problem, while hypotheses provide a focus for testing in the study.

Exactly what I need in this research journey, I look forward to more of your coaching videos.

This helped a lot. Thanks so much for the effort put into explaining it.

What data source in writing dissertation/Thesis requires?
What is data source covers when writing dessertation/thesis

This is quite useful thanks

I’m excited and thankful. I got so much value which will help me progress in my thesis.

where are the locations of the reserch statement, research objective and research question in a reserach paper? Can you write an ouline that defines their places in the researh paper?

Very helpful and important tips on Aims, Objectives and Questions.

Thank you so much for making research aim, research objectives and research question so clear. This will be helpful to me as i continue with my thesis.

Thanks much for this content. I learned a lot. And I am inspired to learn more. I am still struggling with my preparation for dissertation outline/proposal. But I consistently follow contents and tutorials and the new FB of GRAD Coach. Hope to really become confident in writing my dissertation and successfully defend it.

As a researcher and lecturer, I find splitting research goals into research aims, objectives, and questions is unnecessarily bureaucratic and confusing for students. For most biomedical research projects, including ‘real research’, 1-3 research questions will suffice (numbers may differ by discipline).

Awesome! Very important resources and presented in an informative way to easily understand the golden thread. Indeed, thank you so much.

Well explained

The blog article on research aims, objectives, and questions by Grad Coach is a clear and insightful guide that aligns with my experiences in academic research. The article effectively breaks down the often complex concepts of research aims and objectives, providing a straightforward and accessible explanation. Drawing from my own research endeavors, I appreciate the practical tips offered, such as the need for specificity and clarity when formulating research questions. The article serves as a valuable resource for students and researchers, offering a concise roadmap for crafting well-defined research goals and objectives. Whether you’re a novice or an experienced researcher, this article provides practical insights that contribute to the foundational aspects of a successful research endeavor.

A great thanks for you. it is really amazing explanation. I grasp a lot and one step up to research knowledge.

I really found these tips helpful. Thank you very much Grad Coach.

I found this article helpful. Thanks for sharing this.

thank you so much, the explanation and examples are really helpful
Submit a Comment Cancel reply
Your email address will not be published. Required fields are marked *
Save my name, email, and website in this browser for the next time I comment.
- Print Friendly
- Defining Research Objectives: How To Write Them

Almost all industries use research for growth and development. Research objectives are how researchers ensure that their study has direction and makes a significant contribution to growing an industry or niche.
Research objectives provide a clear and concise statement of what the researcher wants to find out. As a researcher, you need to clearly outline and define research objectives to guide the research process and ensure that the study is relevant and generates the impact you want.
In this article, we will explore research objectives and how to leverage them to achieve successful research studies.
What Are Research Objectives?
Research objectives are what you want to achieve through your research study. They guide your research process and help you focus on the most important aspects of your topic.
You can also define the scope of your study and set realistic and attainable study goals with research objectives. For example, with clear research objectives, your study focuses on the specific goals you want to achieve and prevents you from spending time and resources collecting unnecessary data.
However, sticking to research objectives isn’t always easy, especially in broad or unconventional research. This is why most researchers follow the SMART criteria when defining their research objectives.
Understanding SMART Criteria in Research
Think of research objectives as a roadmap to achieving your research goals, with the SMART criteria as your navigator on the map.
SMART stands for Specific, Measurable, Achievable, Relevant, and Time-bound. These criteria help you ensure that your research objectives are clear, specific, realistic, meaningful, and time-bound.
Here’s a breakdown of the SMART Criteria:
Specific : Your research objectives should be clear: what do you want to achieve, why do you want to achieve it, and how do you plan to achieve it? Avoid vague or broad statements that don’t provide enough direction for your research.
Measurable : Your research objectives should have metrics that help you track your progress and measure your results. Also, ensure the metrics are measurable with data to verify them.
Achievable : Your research objectives should be within your research scope, timeframe, and budget. Also, set goals that are challenging but not impossible.
Relevant: Your research objectives should be in line with the goal and significance of your study. Also, ensure that the objectives address a specific issue or knowledge gap that is interesting and relevant to your industry or niche.
Time-bound : Your research objectives should have a specific deadline or timeframe for completion. This will help you carefully set a schedule for your research activities and milestones and monitor your study progress.
Characteristics of Effective Research Objectives
Clarity : Your objectives should be clear and unambiguous so that anyone who reads them can understand what you intend to do. Avoid vague or general terms that could be taken out of context.
Specificity : Your objectives should be specific and address the research questions that you have formulated. Do not use broad or narrow objectives as they may restrict your field of research or make your research irrelevant.
Measurability : Define your metrics with indicators or metrics that help you determine if you’ve accomplished your goals or not. This will ensure you are tracking the research progress and making interventions when needed.
Also, do use objectives that are subjective or based on personal opinions, as they may be difficult to accurately verify and measure.
Achievability : Your objectives should be realistic and attainable, given the resources and time available for your research project. You should set objectives that match your skills and capabilities, they can be difficult but not so hard that they are realistically unachievable.
For example, setting very difficult make you lose confidence, and abandon your research. Also, setting very simple objectives could demotivate you and prevent you from closing the knowledge gap or making significant contributions to your field with your research.
Relevance : Your objectives should be relevant to your research topic and contribute to the existing knowledge in your field. Avoid objectives that are unrelated or insignificant, as they may waste your time or resources.
Time-bound : Your objectives should be time-bound and specify when you will complete them. Have a realistic and flexible timeframe for achieving your objectives, and track your progress with it.
Steps to Writing Research Objectives
Identify the research questions.
The first step in writing effective research objectives is to identify the research questions that you are trying to answer. Research questions help you narrow down your topic and identify the gaps or problems that you want to address with your research.
For example, if you are interested in the impact of technology on children’s development, your research questions could be:
- What is the relationship between technology use and academic performance among children?
- Are children who use technology more likely to do better in school than those who do not?
- What is the social and psychological impact of technology use on children?
Brainstorm Objectives
Once you have your research questions, you can brainstorm possible objectives that relate to them. Objectives are more specific than research questions, and they tell you what you want to achieve or learn in your research.
You can use verbs such as analyze, compare, evaluate, explore, investigate, etc. to express your objectives. Also, try to generate as many objectives as possible, without worrying about their quality or feasibility at this stage.
Prioritize Objectives
Once you’ve brainstormed your objectives, you’ll need to prioritize them based on their relevance and feasibility. Relevance is how relevant the objective is to your research topic and how well it fits into your overall research objective.
Feasibility is how realistic and feasible the objective is compared to the time, money, and expertise you have. You can create a matrix or ranking system to organize your objectives and pick the ones that matter the most.
Refine Objectives
The next step is to refine and revise your objectives to ensure clarity and specificity. Start by ensuring that your objectives are consistent and coherent with each other and with your research questions.
Make Objectives SMART
A useful way to refine your objectives is to make them SMART, which stands for specific, measurable, achievable, relevant, and time-bound.
- Specific : Objectives should clearly state what you hope to achieve.
- Measurable : They should be able to be quantified or evaluated.
- Achievable : realistic and within the scope of the research study.
- Relevant : They should be directly related to the research questions.
- Time-bound : specific timeframe for research completion.
Review and Finalize Objectives
The final step is to review your objectives for coherence and alignment with your research questions and aim. Ensure your objectives are logically connected and consistent with each other and with the purpose of your study.
You also need to check that your objectives are not too broad or too narrow, too easy or too hard, too many or too few. You can use a checklist or a rubric to evaluate your objectives and make modifications.
Examples of Well-Written Research Objectives
Example 1- Psychology
Research question: What are the effects of social media use on teenagers’ mental health?
Objective : To determine the relationship between the amount of time teenagers in the US spend on social media and their levels of anxiety and depression before and after using social media.
What Makes the Research Objective SMART?
The research objective is specific because it clearly states what the researcher hopes to achieve. It is measurable because it can be quantified by measuring the levels of anxiety and depression in teenagers.
Also, the objective is achievable because the researcher can collect enough data to answer the research question. It is relevant because it is directly related to the research question. It is time-bound because it has a specific deadline for completion.
Example 2- Marketing
Research question : How can a company increase its brand awareness by 10%?
Objective : To develop a marketing strategy that will increase the company’s sales by 10% within the next quarter.
How Is this Research Objective SMART?
The research states what the researcher hopes to achieve ( Specific ). You can also measure the company’s reach before and after the marketing plan is implemented ( Measurable ).
The research objective is also achievable because you can develop a marketing plan that will increase awareness by 10% within the timeframe. The objective is directly related to the research question ( Relevant ). It is also time-bound because it has a specific deadline for completion.
Research objectives are a well-designed roadmap to completing and achieving your overall research goal.
However, research goals are only effective if they are well-defined and backed up with the best practices such as the SMART criteria. Properly defining research objectives will help you plan and conduct your research project effectively and efficiently.
Connect to Formplus, Get Started Now - It's Free!
- research goals
- research objectives
- research roadmap
- smart goals
- SMART research objectives
- Moradeke Owa
You may also like:
Desk Research: Definition, Types, Application, Pros & Cons
If you are looking for a way to conduct a research study while optimizing your resources, desk research is a great option. Desk research...
Subgroup Analysis: What It Is + How to Conduct It
Introduction Clinical trials are an integral part of the drug development process. They aim to assess the safety and efficacy of a new...
Projective Techniques In Surveys: Definition, Types & Pros & Cons
Introduction When you’re conducting a survey, you need to find out what people think about things. But how do you get an accurate and...
Research Summary: What Is It & How To Write One
Introduction A research summary is a requirement during academic research and sometimes you might need to prepare a research summary...
Formplus - For Seamless Data Collection
Collect data the right way with a versatile data collection tool. try formplus and transform your work productivity today..
- Link to facebook
- Link to linkedin
- Link to twitter
- Link to youtube
- Writing Tips
How to Write Research Objectives

3-minute read
- 22nd November 2021
Writing a research paper, thesis, or dissertation ? If so, you’ll want to state your research objectives in the introduction of your paper to make it clear to your readers what you’re trying to accomplish. But how do you write effective research objectives? In this post, we’ll look at two key topics to help you do this:
- How to use your research aims as a basis for developing objectives.
- How to use SMART criteria to refine your research objectives.
For more advice on how to write strong research objectives, see below.
Research Aims and Objectives
There is an important difference between research aims and research objectives:
- A research aim defines the main purpose of your research. As such, you can think of your research aim as answering the question “What are you doing?”
- Research objectives (as most studies will have more than one) are the steps you will take to fulfil your aims. As such, your objectives should answer the question “How are you conducting your research?”
For instance, an example research aim could be:
This study will investigate the link between dehydration and the incidence of urinary tract infections (UTIs) in intensive care patients in Australia.
To develop a set of research objectives, you would then break down the various steps involved in meeting said aim. For example:
This study will investigate the link between dehydration and the incidence of urinary tract infections (UTIs) in intensive care patients in Australia. To achieve this, the study objectives w ill include:
- Replicat ing a small Singaporean study into the role of dehydration in UTIs in hospital patients (Sepe, 2018) in a larger Australian cohort.
- Trialing the use of intravenous fluids for intensive care patients to prevent dehydration.
- Assessing the relationship between the age of patients and quantities of intravenous fluids needed to counter dehydration.
Find this useful?
Subscribe to our newsletter and get writing tips from our editors straight to your inbox.
Note that the objectives don’t go into any great detail here. The key is to briefly summarize each component of your study. You can save details for how you will conduct the research for the methodology section of your paper.
Make Your Research Objectives SMART
A great way to refine your research objectives is to use SMART criteria . Borrowed from the world of project management, there are many versions of this system. However, we’re going to focus on developing specific, measurable, achievable, relevant, and timebound objectives.
In other words, a good research objective should be all of the following:
- S pecific – Is the objective clear and well-defined?
- M easurable – How will you know when the objective has been achieved? Is there a way to measure the thing you’re seeking to do?
- A chievable – Do you have the support and resources necessary to undertake this action? Are you being overly ambitious with this objective?
- R elevant – Is this objective vital for fulfilling your research aim?
- T imebound – Can this action be realistically undertaken in the time you have?
If you follow this system, your research objectives will be much stronger.
Expert Research Proofreading
Whatever your research aims and objectives, make sure to have your academic writing proofread by the experts!
Our academic editors can help you with research papers and proposals , as well as any other scholarly document you need checking. And this will help to ensure that your academic writing is always clear, concise, and precise.
Submit a free sample document today to trial our services and find out more.
Share this article:
Post A New Comment
Got content that needs a quick turnaround? Let us polish your work. Explore our editorial business services.
9-minute read
How to Use Infographics to Boost Your Presentation
Is your content getting noticed? Capturing and maintaining an audience’s attention is a challenge when...
8-minute read
Why Interactive PDFs Are Better for Engagement
Are you looking to enhance engagement and captivate your audience through your professional documents? Interactive...
7-minute read
Seven Key Strategies for Voice Search Optimization
Voice search optimization is rapidly shaping the digital landscape, requiring content professionals to adapt their...
4-minute read
Five Creative Ways to Showcase Your Digital Portfolio
Are you a creative freelancer looking to make a lasting impression on potential clients or...
How to Ace Slack Messaging for Contractors and Freelancers
Effective professional communication is an important skill for contractors and freelancers navigating remote work environments....
How to Insert a Text Box in a Google Doc
Google Docs is a powerful collaborative tool, and mastering its features can significantly enhance your...
Make sure your writing is the best it can be with our expert English proofreading and editing.
- Aims and Objectives – A Guide for Academic Writing
- Doing a PhD
One of the most important aspects of a thesis, dissertation or research paper is the correct formulation of the aims and objectives. This is because your aims and objectives will establish the scope, depth and direction that your research will ultimately take. An effective set of aims and objectives will give your research focus and your reader clarity, with your aims indicating what is to be achieved, and your objectives indicating how it will be achieved.
Introduction
There is no getting away from the importance of the aims and objectives in determining the success of your research project. Unfortunately, however, it is an aspect that many students struggle with, and ultimately end up doing poorly. Given their importance, if you suspect that there is even the smallest possibility that you belong to this group of students, we strongly recommend you read this page in full.
This page describes what research aims and objectives are, how they differ from each other, how to write them correctly, and the common mistakes students make and how to avoid them. An example of a good aim and objectives from a past thesis has also been deconstructed to help your understanding.
What Are Aims and Objectives?
Research aims.
A research aim describes the main goal or the overarching purpose of your research project.
In doing so, it acts as a focal point for your research and provides your readers with clarity as to what your study is all about. Because of this, research aims are almost always located within its own subsection under the introduction section of a research document, regardless of whether it’s a thesis , a dissertation, or a research paper .
A research aim is usually formulated as a broad statement of the main goal of the research and can range in length from a single sentence to a short paragraph. Although the exact format may vary according to preference, they should all describe why your research is needed (i.e. the context), what it sets out to accomplish (the actual aim) and, briefly, how it intends to accomplish it (overview of your objectives).
To give an example, we have extracted the following research aim from a real PhD thesis:
Example of a Research Aim
The role of diametrical cup deformation as a factor to unsatisfactory implant performance has not been widely reported. The aim of this thesis was to gain an understanding of the diametrical deformation behaviour of acetabular cups and shells following impaction into the reamed acetabulum. The influence of a range of factors on deformation was investigated to ascertain if cup and shell deformation may be high enough to potentially contribute to early failure and high wear rates in metal-on-metal implants.
Note: Extracted with permission from thesis titled “T he Impact And Deformation Of Press-Fit Metal Acetabular Components ” produced by Dr H Hothi of previously Queen Mary University of London.
Research Objectives
Where a research aim specifies what your study will answer, research objectives specify how your study will answer it.
They divide your research aim into several smaller parts, each of which represents a key section of your research project. As a result, almost all research objectives take the form of a numbered list, with each item usually receiving its own chapter in a dissertation or thesis.
Following the example of the research aim shared above, here are it’s real research objectives as an example:
Example of a Research Objective
- Develop finite element models using explicit dynamics to mimic mallet blows during cup/shell insertion, initially using simplified experimentally validated foam models to represent the acetabulum.
- Investigate the number, velocity and position of impacts needed to insert a cup.
- Determine the relationship between the size of interference between the cup and cavity and deformation for different cup types.
- Investigate the influence of non-uniform cup support and varying the orientation of the component in the cavity on deformation.
- Examine the influence of errors during reaming of the acetabulum which introduce ovality to the cavity.
- Determine the relationship between changes in the geometry of the component and deformation for different cup designs.
- Develop three dimensional pelvis models with non-uniform bone material properties from a range of patients with varying bone quality.
- Use the key parameters that influence deformation, as identified in the foam models to determine the range of deformations that may occur clinically using the anatomic models and if these deformations are clinically significant.
It’s worth noting that researchers sometimes use research questions instead of research objectives, or in other cases both. From a high-level perspective, research questions and research objectives make the same statements, but just in different formats.
Taking the first three research objectives as an example, they can be restructured into research questions as follows:
Restructuring Research Objectives as Research Questions
- Can finite element models using simplified experimentally validated foam models to represent the acetabulum together with explicit dynamics be used to mimic mallet blows during cup/shell insertion?
- What is the number, velocity and position of impacts needed to insert a cup?
- What is the relationship between the size of interference between the cup and cavity and deformation for different cup types?
Difference Between Aims and Objectives
Hopefully the above explanations make clear the differences between aims and objectives, but to clarify:
- The research aim focus on what the research project is intended to achieve; research objectives focus on how the aim will be achieved.
- Research aims are relatively broad; research objectives are specific.
- Research aims focus on a project’s long-term outcomes; research objectives focus on its immediate, short-term outcomes.
- A research aim can be written in a single sentence or short paragraph; research objectives should be written as a numbered list.
How to Write Aims and Objectives
Before we discuss how to write a clear set of research aims and objectives, we should make it clear that there is no single way they must be written. Each researcher will approach their aims and objectives slightly differently, and often your supervisor will influence the formulation of yours on the basis of their own preferences.
Regardless, there are some basic principles that you should observe for good practice; these principles are described below.
Your aim should be made up of three parts that answer the below questions:
- Why is this research required?
- What is this research about?
- How are you going to do it?
The easiest way to achieve this would be to address each question in its own sentence, although it does not matter whether you combine them or write multiple sentences for each, the key is to address each one.
The first question, why , provides context to your research project, the second question, what , describes the aim of your research, and the last question, how , acts as an introduction to your objectives which will immediately follow.
Scroll through the image set below to see the ‘why, what and how’ associated with our research aim example.

Note: Your research aims need not be limited to one. Some individuals per to define one broad ‘overarching aim’ of a project and then adopt two or three specific research aims for their thesis or dissertation. Remember, however, that in order for your assessors to consider your research project complete, you will need to prove you have fulfilled all of the aims you set out to achieve. Therefore, while having more than one research aim is not necessarily disadvantageous, consider whether a single overarching one will do.
Research Objectives
Each of your research objectives should be SMART :
- Specific – is there any ambiguity in the action you are going to undertake, or is it focused and well-defined?
- Measurable – how will you measure progress and determine when you have achieved the action?
- Achievable – do you have the support, resources and facilities required to carry out the action?
- Relevant – is the action essential to the achievement of your research aim?
- Timebound – can you realistically complete the action in the available time alongside your other research tasks?
In addition to being SMART, your research objectives should start with a verb that helps communicate your intent. Common research verbs include:
Table of Research Verbs to Use in Aims and Objectives
Last, format your objectives into a numbered list. This is because when you write your thesis or dissertation, you will at times need to make reference to a specific research objective; structuring your research objectives in a numbered list will provide a clear way of doing this.
To bring all this together, let’s compare the first research objective in the previous example with the above guidance:
Checking Research Objective Example Against Recommended Approach
Research Objective:
1. Develop finite element models using explicit dynamics to mimic mallet blows during cup/shell insertion, initially using simplified experimentally validated foam models to represent the acetabulum.
Checking Against Recommended Approach:
Q: Is it specific? A: Yes, it is clear what the student intends to do (produce a finite element model), why they intend to do it (mimic cup/shell blows) and their parameters have been well-defined ( using simplified experimentally validated foam models to represent the acetabulum ).
Q: Is it measurable? A: Yes, it is clear that the research objective will be achieved once the finite element model is complete.
Q: Is it achievable? A: Yes, provided the student has access to a computer lab, modelling software and laboratory data.
Q: Is it relevant? A: Yes, mimicking impacts to a cup/shell is fundamental to the overall aim of understanding how they deform when impacted upon.
Q: Is it timebound? A: Yes, it is possible to create a limited-scope finite element model in a relatively short time, especially if you already have experience in modelling.
Q: Does it start with a verb? A: Yes, it starts with ‘develop’, which makes the intent of the objective immediately clear.
Q: Is it a numbered list? A: Yes, it is the first research objective in a list of eight.
Mistakes in Writing Research Aims and Objectives
1. making your research aim too broad.
Having a research aim too broad becomes very difficult to achieve. Normally, this occurs when a student develops their research aim before they have a good understanding of what they want to research. Remember that at the end of your project and during your viva defence , you will have to prove that you have achieved your research aims; if they are too broad, this will be an almost impossible task. In the early stages of your research project, your priority should be to narrow your study to a specific area. A good way to do this is to take the time to study existing literature, question their current approaches, findings and limitations, and consider whether there are any recurring gaps that could be investigated .
Note: Achieving a set of aims does not necessarily mean proving or disproving a theory or hypothesis, even if your research aim was to, but having done enough work to provide a useful and original insight into the principles that underlie your research aim.
2. Making Your Research Objectives Too Ambitious
Be realistic about what you can achieve in the time you have available. It is natural to want to set ambitious research objectives that require sophisticated data collection and analysis, but only completing this with six months before the end of your PhD registration period is not a worthwhile trade-off.
3. Formulating Repetitive Research Objectives
Each research objective should have its own purpose and distinct measurable outcome. To this effect, a common mistake is to form research objectives which have large amounts of overlap. This makes it difficult to determine when an objective is truly complete, and also presents challenges in estimating the duration of objectives when creating your project timeline. It also makes it difficult to structure your thesis into unique chapters, making it more challenging for you to write and for your audience to read.
Fortunately, this oversight can be easily avoided by using SMART objectives.
Hopefully, you now have a good idea of how to create an effective set of aims and objectives for your research project, whether it be a thesis, dissertation or research paper. While it may be tempting to dive directly into your research, spending time on getting your aims and objectives right will give your research clear direction. This won’t only reduce the likelihood of problems arising later down the line, but will also lead to a more thorough and coherent research project.
Finding a PhD has never been this easy – search for a PhD by keyword, location or academic area of interest.
Browse PhDs Now
Join thousands of students.
Join thousands of other students and stay up to date with the latest PhD programmes, funding opportunities and advice.
Research Objectives: The Compass of Your Study
Table of contents
- 1 Definition and Purpose of Setting Clear Research Objectives
- 2 How Research Objectives Fit into the Overall Research Framework
- 3 Types of Research Objectives
- 4 Aligning Objectives with Research Questions and Hypotheses
- 5 Role of Research Objectives in Various Research Phases
- 6.1 Key characteristics of well-defined research objectives
- 6.2 Step-by-Step Guide on How to Formulate Both General and Specific Research Objectives
- 6.3 How to Know When Your Objectives Need Refinement
- 7 Research Objectives Examples in Different Fields
- 8 Conclusion
Embarking on a research journey without clear objectives is like navigating the sea without a compass. This article delves into the essence of establishing precise research objectives, serving as the guiding star for your scholarly exploration.
We will unfold the layers of how the objective of study not only defines the scope of your research but also directs every phase of the research process, from formulating research questions to interpreting research findings. By bridging theory with practical examples, we aim to illuminate the path to crafting effective research objectives that are both ambitious and attainable. Let’s chart the course to a successful research voyage, exploring the significance, types, and formulation of research paper objectives.
Definition and Purpose of Setting Clear Research Objectives
Defining the research objectives includes which two tasks? Research objectives are clear and concise statements that outline what you aim to achieve through your study. They are the foundation for determining your research scope, guiding your data collection methods, and shaping your analysis. The purpose of research proposal and setting clear objectives in it is to ensure that your research efforts are focused and efficient, and to provide a roadmap that keeps your study aligned with its intended outcomes.
To define the research objective at the outset, researchers can avoid the pitfalls of scope creep, where the study’s focus gradually broadens beyond its initial boundaries, leading to wasted resources and time. Clear objectives facilitate communication with stakeholders, such as funding bodies, academic supervisors, and the broader academic community, by succinctly conveying the study’s goals and significance. Furthermore, they help in the formulation of precise research questions and hypotheses, making the research process more systematic and organized. Yet, it is not always easy. For this reason, PapersOwl is always ready to help. Lastly, clear research objectives enable the researcher to critically assess the study’s progress and outcomes against predefined benchmarks, ensuring the research stays on track and delivers meaningful results.
How Research Objectives Fit into the Overall Research Framework
Research objectives are integral to the research framework as the nexus between the research problem, questions, and hypotheses. They translate the broad goals of your study into actionable steps, ensuring every aspect of your research is purposefully aligned towards addressing the research problem. This alignment helps in structuring the research design and methodology, ensuring that each component of the study is geared towards answering the core questions derived from the objectives. Creating such a difficult piece may take a lot of time. If you need it to be accurate yet fast delivered, consider getting professional research paper writing help whenever the time comes. It also aids in the identification and justification of the research methods and tools used for data collection and analysis, aligning them with the objectives to enhance the validity and reliability of the findings.
Furthermore, by setting clear objectives, researchers can more effectively evaluate the impact and significance of their work in contributing to existing knowledge. Additionally, research objectives guide literature review, enabling researchers to focus their examination on relevant studies and theoretical frameworks that directly inform their research goals.
Types of Research Objectives
In the landscape of research, setting objectives is akin to laying down the tracks for a train’s journey, guiding it towards its destination. Constructing these tracks involves defining two main types of objectives: general and specific. Each serves a unique purpose in guiding the research towards its ultimate goals, with general objectives providing the broad vision and specific objectives outlining the concrete steps needed to fulfill that vision. Together, they form a cohesive blueprint that directs the focus of the study, ensuring that every effort contributes meaningfully to the overarching research aims.
- General objectives articulate the overarching goals of your study. They are broad, setting the direction for your research without delving into specifics. These objectives capture what you wish to explore or contribute to existing knowledge.
- Specific objectives break down the general objectives into measurable outcomes. They are precise, detailing the steps needed to achieve the broader goals of your study. They often correspond to different aspects of your research question , ensuring a comprehensive approach to your study.
To illustrate, consider a research project on the impact of digital marketing on consumer behavior. A general objective might be “to explore the influence of digital marketing on consumer purchasing decisions.” Specific objectives could include “to assess the effectiveness of social media advertising in enhancing brand awareness” and “to evaluate the impact of email marketing on customer loyalty.”
Aligning Objectives with Research Questions and Hypotheses
The harmony between what research objectives should be, questions, and hypotheses is critical. Objectives define what you aim to achieve; research questions specify what you seek to understand, and hypotheses predict the expected outcomes.
This alignment ensures a coherent and focused research endeavor. Achieving it necessitates a thoughtful consideration of how each component interrelates, ensuring that the objectives are not only ambitious but also directly answerable through the research questions and testable via the hypotheses. This interconnectedness facilitates a streamlined approach to the research process, enabling researchers to systematically address each aspect of their study in a logical sequence. Moreover, it enhances the clarity and precision of the research, making it easier for peers and stakeholders to grasp the study’s direction and potential contributions.
Role of Research Objectives in Various Research Phases
Throughout the research process, objectives guide your choices and strategies – from selecting the appropriate research design and methods to analyzing data and interpreting results. They are the criteria against which you measure the success of your study. In the initial stages, research objectives inform the selection of a topic, helping to narrow down a broad area of interest into a focused question that can be explored in depth. During the methodology phase, they dictate the type of data needed and the best methods for obtaining that data, ensuring that every step taken is purposeful and aligned with the study’s goals. As the research progresses, objectives provide a framework for analyzing the collected data, guiding the researcher in identifying patterns, drawing conclusions, and making informed decisions.
Crafting Effective Research Objectives

The effective objective of research is pivotal in laying the groundwork for a successful investigation. These objectives clarify the focus of your study and determine its direction and scope. Ensuring that your objectives are well-defined and aligned with the SMART criteria is crucial for setting a strong foundation for your research.
Key characteristics of well-defined research objectives
Well-defined research objectives are characterized by the SMART criteria – Specific, Measurable, Achievable, Relevant, and Time-bound. Specific objectives clearly define what you plan to achieve, eliminating any ambiguity. Measurable objectives allow you to track progress and assess the outcome. Achievable objectives are realistic, considering the research sources and time available. Relevant objectives align with the broader goals of your field or research question. Finally, Time-bound objectives have a clear timeline for completion, adding urgency and a schedule to your work.
Step-by-Step Guide on How to Formulate Both General and Specific Research Objectives
So lets get to the part, how to write research objectives properly?
- Understand the issue or gap in existing knowledge your study aims to address.
- Gain insights into how similar challenges have been approached to refine your objectives.
- Articulate the broad goal of research based on your understanding of the problem.
- Detail the specific aspects of your research, ensuring they are actionable and measurable.
How to Know When Your Objectives Need Refinement
Your objectives of research may require refinement if they lack clarity, feasibility, or alignment with the research problem. If you find yourself struggling to design experiments or methods that directly address your objectives, or if the objectives seem too broad or not directly related to your research question, it’s likely time for refinement. Additionally, objectives in research proposal that do not facilitate a clear measurement of success indicate a need for a more precise definition. Refinement involves ensuring that each objective is specific, measurable, achievable, relevant, and time-bound, enhancing your research’s overall focus and impact.
Research Objectives Examples in Different Fields
The application of research objectives spans various academic disciplines, each with its unique focus and methodologies. To illustrate how the objectives of the study guide a research paper across different fields, here are some research objective examples:
- In Health Sciences , a research aim may be to “determine the efficacy of a new vaccine in reducing the incidence of a specific disease among a target population within one year.” This objective is specific (efficacy of a new vaccine), measurable (reduction in disease incidence), achievable (with the right study design and sample size), relevant (to public health), and time-bound (within one year).
- In Environmental Studies , the study objectives could be “to assess the impact of air pollution on urban biodiversity over a decade.” This reflects a commitment to understanding the long-term effects of human activities on urban ecosystems, emphasizing the need for sustainable urban planning.
- In Economics , an example objective of a study might be “to analyze the relationship between fiscal policies and unemployment rates in developing countries over the past twenty years.” This seeks to explore macroeconomic trends and inform policymaking, highlighting the role of economic research study in societal development.
These examples of research objectives describe the versatility and significance of research objectives in guiding scholarly inquiry across different domains. By setting clear, well-defined objectives, researchers can ensure their studies are focused and impactful and contribute valuable knowledge to their respective fields.
Defining research studies objectives and problem statement is not just a preliminary step, but a continuous guiding force throughout the research journey. These goals of research illuminate the path forward and ensure that every stride taken is meaningful and aligned with the ultimate goals of the inquiry. Whether through the meticulous application of the SMART criteria or the strategic alignment with research questions and hypotheses, the rigor in crafting and refining these objectives underscores the integrity and relevance of the research. As scholars venture into the vast terrains of knowledge, the clarity, and precision of their objectives serve as beacons of light, steering their explorations toward discoveries that advance academic discourse and resonate with the broader societal needs.
Readers also enjoyed

WHY WAIT? PLACE AN ORDER RIGHT NOW!
Just fill out the form, press the button, and have no worries!
We use cookies to give you the best experience possible. By continuing we’ll assume you board with our cookie policy.
Crafting Clear Pathways: Writing Objectives in Research Papers
Struggling to write research objectives? Follow our easy steps to learn how to craft effective and compelling objectives in research papers.

Are you struggling to define the goals and direction of your research? Are you losing yourself while doing research and tend to go astray from the intended research topic? Fear not, as many face the same problem and it is quite understandable to overcome this, a concept called research objective comes into play here.
In this article, we’ll delve into the world of the objectives in research papers and why they are essential for a successful study. We will be studying what they are and how they are used in research.
What is a Research Objective?
A research objective is a clear and specific goal that a researcher aims to achieve through a research study. It serves as a roadmap for the research, providing direction and focus. Research objectives are formulated based on the research questions or hypotheses, and they help in defining the scope of the study and guiding the research design and methodology. They also assist in evaluating the success and outcomes of the research.
Types of Research Objectives
There are typically three main types of objectives in a research paper:
- Exploratory Objectives: These objectives are focused on gaining a deeper understanding of a particular phenomenon, topic, or issue. Exploratory research objectives aim to explore and identify new ideas, insights, or patterns that were previously unknown or poorly understood. This type of objective is commonly used in preliminary or qualitative studies.
- Descriptive Objectives: Descriptive objectives seek to describe and document the characteristics, behaviors, or attributes of a specific population, event, or phenomenon. The purpose is to provide a comprehensive and accurate account of the subject of study. Descriptive research objectives often involve collecting and analyzing data through surveys, observations, or archival research.
- Explanatory or Causal Objectives: Explanatory objectives aim to establish a cause-and-effect relationship between variables or factors. These objectives focus on understanding why certain events or phenomena occur and how they are related to each other.
Also Read: What are the types of research?
Steps for Writing Objectives in Research Paper
1. identify the research topic:.
Clearly define the subject or topic of your research. This will provide a broad context for developing specific research objectives.
2. Conduct a Literature Review
Review existing literature and research related to your topic. This will help you understand the current state of knowledge, identify any research gaps, and refine your research objectives accordingly.
3. Identify the Research Questions or Hypotheses
Formulate specific research questions or hypotheses that you want to address in your study. These questions should be directly related to your research topic and guide the development of your research objectives.
4. Focus on Specific Goals
Break down the broader research questions or hypothesis into specific goals or objectives. Each objective should focus on a particular aspect of your research topic and be achievable within the scope of your study.
5. Use Clear and Measurable Language
Write your research objectives using clear and precise language. Avoid vague terms and use specific and measurable terms that can be observed, analyzed, or measured.
6. Consider Feasibility
Ensure that your research objectives are feasible within the available resources, time constraints, and ethical considerations. They should be realistic and attainable given the limitations of your study.
7. Prioritize Objectives
If you have multiple research objectives, prioritize them based on their importance and relevance to your overall research goals. This will help you allocate resources and focus your efforts accordingly.
8. Review and Refine
Review your research objectives to ensure they align with your research questions or hypotheses, and revise them if necessary. Seek feedback from peers or advisors to ensure clarity and coherence.
Tips for Writing Objectives in Research Paper
1. be clear and specific.
Clearly state what you intend to achieve with your research. Use specific language that leaves no room for ambiguity or confusion. This ensures that your objectives are well-defined and focused.
2. Use Action Verbs
Begin each research objective with an action verb that describes a measurable action or outcome. This helps make your objectives more actionable and measurable.
3. Align with Research Questions or Hypotheses
Your research objectives should directly address the research questions or hypotheses you have formulated. Ensure there is a clear connection between them to maintain coherence in your study.
4. Be Realistic and Feasible
Set research objectives that are attainable within the constraints of your study, including available resources, time, and ethical considerations. Unrealistic objectives may undermine the validity and reliability of your research.
5. Consider Relevance and Significance
Your research objectives should be relevant to your research topic and contribute to the broader field of study. Consider the potential impact and significance of achieving the objectives.
SMART Goals for Writing Research Objectives
To ensure that your research objectives are well-defined and effectively guide your study, you can apply the SMART framework. SMART stands for Specific, Measurable, Achievable, Relevant, and Time-bound. Here’s how you can make your research objectives SMART:
- Specific : Clearly state what you want to achieve in a precise and specific manner. Avoid vague or generalized language. Specify the population, variables, or phenomena of interest.
- Measurable : Ensure that your research objectives can be quantified or observed in a measurable way. This allows for objective evaluation and assessment of progress.
- Achievable : Set research objectives that are realistic and attainable within the available resources, time, and scope of your study. Consider the feasibility of conducting the research and collecting the necessary data.
- Relevant : Ensure that your research objectives are directly relevant to your research topic and contribute to the broader knowledge or understanding of the field. They should align with the purpose and significance of your study.
- Time-bound : Set a specific timeframe or deadline for achieving your research objectives. This helps create a sense of urgency and provides a clear timeline for your study.
Examples of Research Objectives
Here are some examples of research objectives from various fields of study:
- To examine the relationship between social media usage and self-esteem among young adults aged 18-25 in order to understand the potential impact on mental well-being.
- To assess the effectiveness of a mindfulness-based intervention in reducing stress levels and improving coping mechanisms among individuals diagnosed with anxiety disorders.
- To investigate the factors influencing consumer purchasing decisions in the e-commerce industry, with a focus on the role of online reviews and social media influencers.
- To analyze the effects of climate change on the biodiversity of coral reefs in a specific region, using remote sensing techniques and field surveys.
Importance of Research Objectives
Research objectives play a crucial role in the research process and hold significant importance for several reasons:
- Guiding the Research Process: Research objectives provide a clear roadmap for the entire research process. They help researchers stay focused and on track, ensuring that the study remains purposeful and relevant.
- Defining the Scope of the Study: Research objectives help in determining the boundaries and scope of the study. They clarify what aspects of the research topic will be explored and what will be excluded.
- Providing Direction for Data Collection and Analysis: Research objectives assist in identifying the type of data to be collected and the methods of data collection. They also guide the selection of appropriate data analysis techniques.
- Evaluating the Success of the Study: Research objectives serve as benchmarks for evaluating the success and outcomes of the research. They provide measurable criteria against which the researcher can assess whether the objectives have been met or not.
- Enhancing Communication and Collaboration: Clearly defined research objectives facilitate effective communication and collaboration among researchers, advisors, and stakeholders.
Common Mistakes to Avoid While Writing Research Objectives
When writing research objectives, it’s important to be aware of common mistakes and pitfalls that can undermine the effectiveness and clarity of your objectives. Here are some common mistakes to avoid:
- Vague or Ambiguous Language: One of the key mistakes is using vague or ambiguous language that lacks specificity. Ensure that your research objectives are clearly and precisely stated, leaving no room for misinterpretation or confusion.
- Lack of Measurability: Research objectives should be measurable, meaning that they should allow for the collection of data or evidence that can be quantified or observed. Avoid setting objectives that cannot be measured or assessed objectively.
- Lack of Alignment with Research Questions or Hypotheses: Your research objectives should directly align with the research questions or hypotheses you have formulated. Make sure there is a clear connection between them to maintain coherence in your study.
- Overgeneralization : Avoid writing research objectives that are too broad or encompass too many variables or phenomena. Overgeneralized objectives may lead to a lack of focus or feasibility in conducting the research.
- Unrealistic or Unattainable Objectives: Ensure that your research objectives are realistic and attainable within the available resources, time, and scope of your study. Setting unrealistic objectives may compromise the validity and reliability of your research.
In conclusion, research objectives are integral to the success and effectiveness of any research study. They provide a clear direction, focus, and purpose, guiding the entire research process from start to finish. By formulating specific, measurable, achievable, relevant, and time-bound objectives, researchers can define the scope of their study, guide data collection and analysis, and evaluate the outcomes of their research.
Turn your data into easy-to-understand and dynamic stories
When you wish to explain any complex data, it’s always advised to break it down into simpler visuals or stories. This is where Mind the Graph comes in. It is a platform that helps researchers and scientists to turn their data into easy-to-understand and dynamic stories, helping the audience understand the concepts better. Sign Up now to explore the library of scientific infographics.

Subscribe to our newsletter
Exclusive high quality content about effective visual communication in science.
Unlock Your Creativity
Create infographics, presentations and other scientifically-accurate designs without hassle — absolutely free for 7 days!
About Sowjanya Pedada
Sowjanya is a passionate writer and an avid reader. She holds MBA in Agribusiness Management and now is working as a content writer. She loves to play with words and hopes to make a difference in the world through her writings. Apart from writing, she is interested in reading fiction novels and doing craftwork. She also loves to travel and explore different cuisines and spend time with her family and friends.
Content tags
Writing the Research Objectives: 5 Straightforward Examples
The research objective of a research proposal or scientific article defines the direction or content of a research investigation. Without the research objectives, the proposal or research paper is in disarray. It is like a fisherman riding on a boat without any purpose and with no destination in sight. Therefore, at the beginning of any research venture, the researcher must be clear about what he or she intends to do or achieve in conducting a study.
How do you define the objectives of a study? What are the uses of the research objective? How would a researcher write this essential part of the research? This article aims to provide answers to these questions.
Table of Contents
Definition of a research objective.
A research objective describes, in a few words, the result of the research project after its implementation. It answers the question,
“ What does the researcher want or hope to achieve at the end of the research project.”
The research objective provides direction to the performance of the study.
What are the Uses of the Research Objective?
The uses of the research objective are enumerated below:
- serves as the researcher’s guide in identifying the appropriate research design,
- identifies the variables of the study, and
- specifies the data collection procedure and the corresponding analysis for the data generated.
The research design serves as the “blueprint” for the research investigation. The University of Southern California describes the different types of research design extensively. It details the data to be gathered, data collection procedure, data measurement, and statistical tests to use in the analysis.
The variables of the study include those factors that the researcher wants to evaluate in the study. These variables narrow down the research to several manageable components to see differences or correlations between them.
Specifying the data collection procedure ensures data accuracy and integrity . Thus, the probability of error is minimized. Generalizations or conclusions based on valid arguments founded on reliable data strengthens research findings on particular issues and problems.
In data mining activities where large data sets are involved, the research objective plays a crucial role. Without a clear objective to guide the machine learning process, the desired outcomes will not be met.
How is the Research Objective Written?
A research objective must be achievable, i.e., it must be framed keeping in mind the available time, infrastructure required for research, and other resources.
Before forming a research objective, you should read about all the developments in your area of research and find gaps in knowledge that need to be addressed. Readings will help you come up with suitable objectives for your research project.
5 Examples of Research Objectives
The following examples of research objectives based on several published studies on various topics demonstrate how the research objectives are written:
- This study aims to find out if there is a difference in quiz scores between students exposed to direct instruction and flipped classrooms (Webb and Doman, 2016).
- This study seeks to examine the extent, range, and method of coral reef rehabilitation projects in five shallow reef areas adjacent to popular tourist destinations in the Philippines (Yeemin et al ., 2006).
- This study aims to investigate species richness of mammal communities in five protected areas over the past 20 years (Evans et al ., 2006).
- This study aims to clarify the demographic, epidemiological, clinical, and radiological features of 2019-nCoV patients with other causes of pneumonia (Zhao et al ., 2020).
- This research aims to assess species extinction risks for sample regions that cover some 20% of the Earth’s terrestrial surface.
Finally, writing the research objectives requires constant practice, experience, and knowledge about the topic investigated. Clearly written objectives save time, money, and effort.
Once you have a clear idea of your research objectives, you can now develop your conceptual framework which is a crucial element of your research paper as it guides the flow of your research. The conceptual framework will help you develop your methodology and statistical tests.
I wrote a detailed, step-by-step guide on how to develop a conceptual framework with illustration in my post titled “ Conceptual Framework: A Step by Step Guide on How to Make One. “
Evans, K. L., Rodrigues, A. S., Chown, S. L., & Gaston, K. J. (2006). Protected areas and regional avian species richness in South Africa. Biology letters , 2 (2), 184-188.
Thomas, C. D., Cameron, A., Green, R. E., Bakkenes, M., Beaumont, L. J., Collingham, Y. C., … & Hughes, L. (2004). Extinction risk from climate change. Nature, 427(6970), 145-148.
Webb, M., & Doman, E. (2016). Does the Flipped Classroom Lead to Increased Gains on Learning Outcomes in ESL/EFL Contexts?. CATESOL Journal, 28(1), 39-67.
Yeemin, T., Sutthacheep, M., & Pettongma, R. (2006). Coral reef restoration projects in Thailand. Ocean & Coastal Management , 49 (9-10), 562-575.
Zhao, D., Yao, F., Wang, L., Zheng, L., Gao, Y., Ye, J., Guo, F., Zhao, H. & Gao, R. (2020). A comparative study on the clinical features of COVID-19 pneumonia to other pneumonias, Clinical Infectious Diseases , ciaa247, https://doi.org/10.1093/cid/ciaa247
© 2020 March 23 P. A. Regoniel Updated 17 November 2020 | Updated 18 January 2024
Related Posts

Master Content Analysis: An All-in-One Guide

Two Tips on How to Write the Significance of the Study
5 thesis writing tips for greater impact, about the author, patrick regoniel.
Dr. Regoniel, a faculty member of the graduate school, served as consultant to various environmental research and development projects covering issues and concerns on climate change, coral reef resources and management, economic valuation of environmental and natural resources, mining, and waste management and pollution. He has extensive experience on applied statistics, systems modelling and analysis, an avid practitioner of LaTeX, and a multidisciplinary web developer. He leverages pioneering AI-powered content creation tools to produce unique and comprehensive articles in this website.
thank you for clarification
This is excellent
SimplyEducate.Me Privacy Policy

Research Aims and Objectives: The dynamic duo for successful research
Picture yourself on a road trip without a destination in mind — driving aimlessly, not knowing where you’re headed or how to get there. Similarly, your research is navigated by well-defined research aims and objectives. Research aims and objectives are the foundation of any research project. They provide a clear direction and purpose for the study, ensuring that you stay focused and on track throughout the process. They are your trusted navigational tools, leading you to success.
Understanding the relationship between research objectives and aims is crucial to any research project’s success, and we’re here to break it down for you in this article. Here, we’ll explore the importance of research aims and objectives, understand their differences, and delve into the impact they have on the quality of research.
Understanding the Difference between Research Aims and Objectives
In research, aims and objectives are two important components but are often used interchangeably. Though they may sound similar, they are distinct and serve different purposes.
Research Aims:
Research aims are broad statements that describe the overall purpose of your study. They provide a general direction for your study and indicate the intended achievements of your research. Aims are usually written in a general and abstract manner describing the ultimate goal of the research.
Research Objectives:
Research objectives are specific, measurable, and achievable goals that you aim to accomplish within a specified timeframe. They break down the research aims into smaller, more manageable components and provide a clear picture of what you want to achieve and how you plan to achieve it.
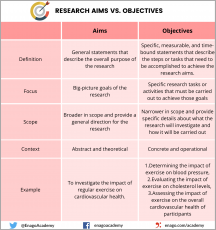
In the example, the objectives provide specific targets that must be achieved to reach the aim. Essentially, aims provide the overall direction for the research while objectives provide specific targets that must be achieved to accomplish the aims. Aims provide a broad context for the research, while the objectives provide smaller steps that the researcher must take to accomplish the overall research goals. To illustrate, when planning a road trip, your research aim is the destination you want to reach, and your research objectives are the specific routes you need to take to get there.
Aims and objectives are interconnected. Objectives play a key role in defining the research methodology, providing a roadmap for how you’ll collect and analyze data, while aim is the final destination, which represents the ultimate goal of your research. By setting specific goals, you’ll be able to design a research plan that helps you achieve your objectives and, ultimately, your research aim.
Importance of Well-defined Aims and Objectives
The impact of clear research aims and objectives on the quality of research cannot be understated. But it’s not enough to simply have aims and objectives. Well-defined research aims and objectives are important for several reasons:
- Provides direction: Clear aims and well-defined objectives provide a specific direction for your research study, ensuring that the research stays focused on a specific topic or problem. This helps to prevent the research from becoming too broad or unfocused, and ensures that the study remains relevant and meaningful.
- Guides research design: The research aim and objectives help guide the research design and methodology, ensuring that your study is designed in a way that will answer the research questions and achieve the research objectives.
- Helps with resource allocation: Clear research aims and objectives helps you to allocate resources effectively , including time, financial resources, human resources, and other required materials. With a well-defined aim and objectives, you can identify the resources required to conduct the research, and allocate them in a way that maximizes efficiency and productivity.
- Assists in evaluation: Clearly specified research aims and objectives allow for effective evaluation of your research project’s success. You can assess whether the research has achieved its objectives, and whether the aim has been met. This evaluation process can help to identify areas of the research project that may require further attention or modification.
- Enhances communication: Well-defined research aims and objectives help to enhance communication among the research team, stakeholders, funding agencies, and other interested parties. Clear aims and objectives ensure that everyone involved in your research project understands the purpose and goals of the study. This can help to foster collaboration and ensure that everyone is working towards the same end goal.
How to Formulate Research Aims and Objectives
Formulating effective research aims and objectives involves a systematic process to ensure that they are clear, specific, achievable, and relevant. Start by asking yourself what you want to achieve through your research. What impact do you want your research to have? Once you have a clear understanding of your aims, you can then break them down into specific, achievable objectives. Here are some steps you can follow when developing research aims and objectives:
- Identify the research question : Clearly identify the questions you want to answer through your research. This will help you define the scope of your research. Understanding the characteristics of a good research question will help you generate clearer aims and objectives.
- Conduct literature review : When defining your research aim and objectives, it’s important to conduct a literature review to identify key concepts, theories, and methods related to your research problem or question. Conducting a thorough literature review can help you understand what research has been done in the area and what gaps exist in the literature.
- Identify the research aim: Develop a research aim that summarizes the overarching goal of your research. The research aim should be broad and concise.
- Develop research objectives: Based on your research questions and research aim, develop specific research objectives that outline what you intend to achieve through your research. These objectives should be specific, measurable, achievable, relevant, and time-bound (SMART).
- Use action verbs: Use action verbs such as “investigate,” “examine,” “analyze,” and “compare” to describe your research aims and objectives. This makes them more specific and measurable.
- Ensure alignment with research question: Ensure that the research aim and objectives are aligned with the research question. This helps to ensure that the research remains focused and that the objectives are specific enough to answer your research question.
- Refine and revise: Once the research aim and objectives have been developed, refine and revise them as needed. Seek feedback from your colleagues, mentors, or supervisors to ensure that they are clear, concise, and achievable within the given resources and timeframe.
- Communicate: After finalizing the research aim and objectives, they should be communicated to the research team, stakeholders, and other interested parties. This helps to ensure that everyone is working towards the same end goal and understands the purpose of the study.
Common Pitfalls to Avoid While Formulating Aims and Objectives
There are several common mistakes that researchers can make when writing research aims and objectives. These include:
- Being too broad or vague: Aims and objectives that are too general or unclear can lead to confusion and lack of focus. It is important to ensure that the aims and objectives are concise and clear.
- Being too narrow or specific: On the other hand, aims and objectives that are too narrow or specific may limit the scope of the research and make it difficult to draw meaningful conclusions or implications.
- Being too ambitious: While it is important to aim high, being too ambitious with the aims and objectives can lead to unrealistic expectations and can be difficult to achieve within the constraints of the research project.
- Lack of alignment: The aims and objectives should be directly linked to the research questions being investigated. Otherwise, this will lead to a lack of coherence in the research project.
- Lack of feasibility: The aims and objectives should be achievable within the constraints of the research project, including time, budget, and resources. Failing to consider feasibility may cause compromise of the research quality.
- Failing to consider ethical considerations: The aims and objectives should take into account any ethical considerations, such as ensuring the safety and well-being of study participants.
- Failing to involve all stakeholders: It’s important to involve all relevant stakeholders, such as participants, supervisors, and funding agencies, in the development of the aims and objectives to ensure they are appropriate and relevant.
To avoid these common pitfalls, it is important to be specific, clear, relevant, and realistic when writing research aims and objectives. Seek feedback from colleagues or supervisors to ensure that the aims and objectives are aligned with the research problem , questions, and methodology, and are achievable within the constraints of the research project. It’s important to continually refine your aims and objectives as you go. As you progress in your research, it’s not uncommon for research aims and objectives to evolve slightly, but it’s important that they remain consistent with the study conducted and the research topic.
In summary, research aims and objectives are the backbone of any successful research project. They give you the ability to cut through the noise and hone in on what really matters. By setting clear goals and aligning them with your research questions and methodology, you can ensure that your research is relevant, impactful, and of the highest quality. So, before you hit the road on your research journey, make sure you have a clear destination and steps to get there. Let us know in the comments section below the challenges you faced and the strategies you followed while fomulating research aims and objectives! Also, feel free to reach out to us at any stage of your research or publication by using #AskEnago and tagging @EnagoAcademy on Twitter , Facebook , and Quora . Happy researching!

This particular material has added important but overlooked concepts regarding my experiences in explaining research aims and objectives. Thank you
Rate this article Cancel Reply
Your email address will not be published.

Enago Academy's Most Popular Articles

- Reporting Research
Academic Essay Writing Made Simple: 4 types and tips
The pen is mightier than the sword, they say, and nowhere is this more evident…

- Old Webinars
- Webinar Mobile App
Improving Research Manuscripts Using AI-Powered Insights: Enago reports for effective research communication
Language Quality Importance in Academia AI in Evaluating Language Quality Enago Language Reports Live Demo…

- AI in Academia
- Trending Now
Simplifying the Literature Review Journey — A comparative analysis of 6 AI summarization tools
Imagine having to skim through and read mountains of research papers and books, only to…

Choosing the Right Analytical Approach: Thematic analysis vs. content analysis for data interpretation
In research, choosing the right approach to understand data is crucial for deriving meaningful insights.…

Comparing Cross Sectional and Longitudinal Studies: 5 steps for choosing the right approach
The process of choosing the right research design can put ourselves at the crossroads of…
Choosing the Right Analytical Approach: Thematic analysis vs. content analysis for…
Comparing Cross Sectional and Longitudinal Studies: 5 steps for choosing the right…
Research Recommendations – Guiding policy-makers for evidence-based decision making

Sign-up to read more
Subscribe for free to get unrestricted access to all our resources on research writing and academic publishing including:
- 2000+ blog articles
- 50+ Webinars
- 10+ Expert podcasts
- 50+ Infographics
- 10+ Checklists
- Research Guides
We hate spam too. We promise to protect your privacy and never spam you.
I am looking for Editing/ Proofreading services for my manuscript Tentative date of next journal submission:

As a researcher, what do you consider most when choosing an image manipulation detector?
This paper is in the following e-collection/theme issue:
Published on 3.6.2024 in Vol 26 (2024)
Electronic Health Literacy Scale-Web3.0 for Older Adults with Noncommunicable Diseases: Validation Study
Authors of this article:
Original Paper
- Wenfei Cai 1 , MEd ;
- Wei Liang 1 , PhD ;
- Huaxuan Liu 2 , PhD ;
- Rundong Zhou 1 , MEd ;
- Jie Zhang 1 , PhD ;
- Lin Zhou 3 , PhD ;
- Ning Su 1 , PhD ;
- Hanxiao Zhu 1 , PhD ;
- Yide Yang 4 , PhD
1 School of Physical Education, Shenzhen University, Shenzhen, China
2 School of Physical Education and Sport Science, Fujian Normal University, Fuzhou, China
3 School of Physical Education, Hebei Normal University, Shijiazhuang, China
4 School of Medicine, Hunan Normal University, Changsha, China
Corresponding Author:
Wei Liang, PhD
School of Physical Education
Shenzhen University
3688 Nanhai Road, Nanshan District
Shenzhen, 518060
Phone: 86 15217940540
Email: [email protected]
Background: In the current digital era, eHealth literacy plays an indispensable role in health care and self-management among older adults with noncommunicable diseases (NCDs). Measuring eHealth literacy appropriately and accurately ensures the successful implementation and evaluation of pertinent research and interventions. However, existing eHealth literacy measures focus mainly on individuals’ abilities of accessing and comprehending eHealth information (Web1.0), whereas the capabilities for web-based interaction (Web2.0) and using eHealth information (Web3.0) have not been adequately evaluated.
Objective: This study aimed to examine the reliability, validity, and measurement invariance of the eHealth Literacy Scale-Web3.0 (eHLS-Web3.0) among older adults with NCDs.
Methods: A total of 642 Chinese older adults with NCDs (mean age 65.78, SD 3.91 years; 55.8% female) were recruited in the baseline assessment, of whom 134 (mean age 65.63, SD 3.99 years; 58.2% female) completed the 1-month follow-up assessment. Baseline measures included the Chinese version of the 24-item 3D eHLS-Web3.0, the Chinese version of the 8-item unidimensional eHealth Literacy Scale (eHEALS), and demographic information. Follow-up measures included the 24-item eHLS-Web3.0 and accelerometer-measured physical activity and sedentary behavior. A series of statistical analyses, for example, Cronbach α, composite reliability coefficient (CR), confirmatory factor analysis (CFA), and multigroup CFA, were performed to examine the internal consistency and test-retest reliabilities, as well as the construct, concurrent, convergent, discriminant, and predictive validities, and the measurement invariance of the eHLS-Web3.0 across gender, education level, and residence.
Results: Cronbach α and CR were within acceptable ranges of 0.89-0.94 and 0.90-0.97, respectively, indicating adequate internal consistency of the eHLS-Web3.0 and its subscales. The eHLS-Web3.0 also demonstrated cross-time stability, with baseline and follow-up measures showing a significant intraclass correlation of 0.81-0.91. The construct validity of the 3D structure model of the eHLS-Web3.0 was supported by confirmatory factor analyses. The eHLS-Web3.0 exhibited convergent validity with an average variance extracted value of 0.58 and a CR value of 0.97. Discriminant validity was supported by CFA results for a proposed 4-factor model integrating the 3 eHLS-Web3.0 subscales and eHEALS. The predictive validity of the eHLS-Web3.0 for health behaviors was supported by significant associations of the eHLS-Web3.0 with light physical activity (β=.36, P =.004), moderate to vigorous physical activity ( β =.49, P <.001), and sedentary behavior ( β =–.26, P =.002). Finally, the measurement invariance of the eHLS-Web3.0 across gender, education level, and residence was supported by the establishment of configural, metric, strong, and strict invariances.
Conclusions: The present study provides timely empirical evidence on the reliability, validity, and measurement invariance of the eHLS-Web3.0, suggesting that the 24-item 3D eHLS-Web3.0 is an appropriate and valid tool for measuring eHealth literacy among older adults with NCDs within the Web3.0 sphere.
Introduction
Noncommunicable diseases (NCDs), known as chronic diseases, result in the mortality of 41 million people annually, equivalent to approximately 74% of all global deaths [ 1 ]. Characterized by high morbidity, high mortality, low control rates, and limited awareness, NCDs impose a considerable financial burden on individuals, their families, and society as a whole, particularly among older patients [ 2 ]. In China, the prevalence rate of NCDs among older adults aged 60 years and older was 50%-75%, as reported in recent epidemiological studies [ 3 - 5 ]. Therefore, NCDs in older adults are a vital public health concern, and their management is a global challenge.
Previous evidence has demonstrated that empowering and educating patients with NCDs to focus on self-management and health promotion is essential [ 2 , 6 ]. Enabling patients to inquire about their medical status, comply with medication instructions, enhance their engagement and compliance in the health care process, adopt healthier lifestyles, and ultimately reduce reliance on constant supervision from health care professionals is a challenging task [ 6 , 7 ]. Nevertheless, facilitating patient self-care is a critical step toward improving the overall health status and alleviating the burden on health care facilities, especially within low- and middle-income countries [ 7 , 8 ].
With the rapid advancement of technology, the internet has become the quickest and most easily accessible resource for obtaining and delivering health information, offering ample opportunities for self-management and health promotion [ 6 , 9 ]. Recent review studies have consistently shown that internet-based health interventions for individuals with NCDs can have a substantial impact on enhancing self-management and patient engagement and compliance with their health care [ 10 , 11 ]. Despite the potential of the internet to improve health care services for NCDs, older adults encounter significant challenges in using digital health technologies [ 12 ]. In particular, the information found on the internet originates from numerous providers and sources that are difficult to regulate, thereby leading to potential problems in terms of accuracy and the potential dissemination of prejudiced content that aligns with the interests and objectives of certain parties involved [ 13 ]. Previous research has highlighted the considerable difficulties faced by older adults in accessing reliable and high-quality health information that addresses their specific health needs [ 14 , 15 ]. Furthermore, studies have revealed that a noteworthy proportion of older internet users lack confidence in their capability to execute basic tasks on the internet [ 15 ]. The challenges mentioned above not only impede older adults from harnessing the internet’s full potential for health care purposes but also exacerbate the digital divide and health disparities [ 12 ]. In such a scenario, eHealth literacy is emphasized in numerous studies as a critical skill that older adults with NCDs must acquire in the digital era of disease management and health care [ 2 , 6 , 16 ].
eHealth literacy, first proposed by Norman and Skinner in 2006 [ 17 ], refers to “individual’s abilities to seek, find, understand, and appraise health information from electronic resources and apply that knowledge to solve a health problem or make a health-related decision.” The concept of eHealth literacy is founded on social cognitive theory, consisting of 6 essential skills or literacies: traditional literacy, health literacy, information literacy, scientific literacy, media literacy, and computer literacy [ 17 , 18 ]. To provide a general assessment of this concept that can assist in clinical decision-making and health promotion planning for individuals or specific samples, Norman and Skinner [ 17 ] developed an 8-item unidimensional eHealth Literacy Scale (eHEALS). The eHEALS is the most well-known and extensively used instrument for assessing eHealth literacy to date [ 19 ]. The reliability and validity of the eHEALS have been extensively examined in diverse cultural contexts, including English [ 17 , 20 ], German [ 21 ], Spanish [ 22 ], Dutch [ 23 ], Italian [ 24 ], Portuguese [ 25 ], Japanese [ 26 ], and Chinese [ 27 ], providing compelling evidence of its efficacy across multiple languages and cultures.
However, as technology continues to advance, there has been an increasing acknowledgment of the necessity to update the content of eHealth literacy to ensure optimal synchronization with the evolving internet landscape [ 23 , 28 , 29 ]. Several studies have raised concerns regarding the unidimensional nature of the eHEALS, as well as its inadequate performance in psychometric evaluations, particularly when using it to measure the usage of novel technologies in seeking and assessing health information [ 23 , 27 - 30 ]. For example, previous research has shown a weak association between eHEALS and eHealth behaviors beyond web-based information-researching skills, indicating the requirement to update the tool [ 23 ]. Furthermore, a recent systematic review indicated that the structure of the eHEALS varied across multiple studies, where a 2-factor or 3-factor structure was also identified in certain studies [ 19 ]. There has also been some questioning of the variability of the items, even though the eHEALS had the same factor construct [ 19 ]. Alongside the influence of cultural contexts, a primary reason for the inconsistencies of the factor structures and corresponding items may be that the eHEALS is outdated for use in evaluating eHealth literacy in the new digital age [ 19 ].
Indeed, the arguments outlined above are reasonable. As per the widely acknowledged generation divisions of internet evolution, the present internet landscape has progressed through 3 distinct phases, starting with Web1.0 (a read-only web) to Web2.0 (ie, a read-write mode that provides a participatory social web with increased collaboration and interaction among consumers, programmers, service providers, and organization) and to current Web3.0 (ie, a read-write-execute mode that provides digital, personalized, and intelligent services; also known as semantic web) [ 23 , 30 , 31 ]. The eHEALS was developed 15 years ago for measuring individuals’ capability related to reading and viewing within a Web1.0 context, and therefore, it is necessary to update it to effectively scale current eHealth usage.
To fill this gap, numerous new measurement tools of eHealth literacy have been developed. One example is the 20-item extended version of the eHEALS (eHEALS-E) created by Petrič et al [ 32 ], which is designed to better encompass the complicated factors contributing to eHealth literacy. However, the eHEALS-E is based on the same definition as the original eHEALS, and therefore, it may also have limitations in measuring only a narrow aspect of eHealth literacy [ 19 ]. Furthermore, second-generation instruments of eHealth literacy have been developed (eg, eHealth Literacy Scale [eHLS], Digital Health Literacy Instrument [DHLI], Transactional eHealth Literacy Instrument, eHealth Literacy Assessment Toolkit, and Chinese version of the electronic eHealth Literacy Scale [C-eHEALS]) to assess a broader spectrum of eHealth literacy concepts, ensuring their relevance in the age of social media and eHealth [ 19 , 28 ]. These measures have provided novel approaches for evaluating eHealth literacy, with some of them specifically designed to measure web communication capabilities. However, their coverage is limited to Web2.0 skills, and evaluation of eHealth literacy content relevant to Web3.0 technologies remains absent [ 33 ]. Recently, Liu et al [ 33 ] developed a 24-item eHealth Literacy Scale-Web3.0 (eHLS-Web3.0) to measure eHealth skills in the context of Web3.0. Compared with previous eHEALS and second-generation eHealth literacy scales, the eHLS-Web3.0 is an improvement consisting of 3 distinct dimensions (ie, acquisition, verification, and application) that evaluates the abilities covering the entire spectrum of Web1.0 (eg, searching, understanding, and identifying), 2.0 (eg, sharing and interactive communication), and 3.0 (eg, recording, self-managing, applying, and adjusting) [ 33 ]. The reliabilities, validities, and measurement invariance of the eHLS-Web3.0 across gender and region have been supported in a previous study with young adults [ 33 ], whereas its psychometric properties remain unexplored in older adults, especially those living with NCDs. Therefore, further research is needed to investigate the applicability and psychometric properties of the eHLS-Web3.0 in older adults with NCDs, which may inform the development of effective interventions to improve eHealth literacy and promote better health care outcomes in this population.
Given the above, the purpose of this study was to examine the reliability, validity, and measure invariance of the eHLS-Web3.0 in a sample of older adults with NCDs. In particular, this study has 3 main objectives. First, the internal consistency and test-retest reliabilities of the eHLS-Web3.0 would be examined. Based on previous studies [ 12 , 17 , 20 , 34 - 36 ], a conventional 1-month time frame for evaluating the test-retest reliability was used in this study. Second, the construct, convergent, concurrent, discriminant, and predictive validities of the 24-item 3D eHLS-Web3.0 would be ascertained. Because the eHEALS has been proven to be a reliable tool for measuring eHealth literacy among older adults with NCDs in previous studies [ 2 , 17 ], this study would use the eHEALS as the criteria scale for the examination of the concurrent validity of the eHLS-Web3.0. Furthermore, considering the content distinction between the eHLS-Web3.0 and the eHEALS, the discriminant validity of the eHLS-Web3.0 would be examined by comparing the eHLS-Web3.0 subscales and the eHEALS. Additionally, previous studies have established a strong association between eHealth literacy and various health behaviors [ 13 , 37 ]. Specifically, eHealth literacy has been shown to positively correlate with health-promoting behaviors (eg, physical activity) and negatively correlate with risk behaviors (eg, sedentary behavior) among young and older adults [ 38 , 39 ]. Therefore, this study would investigate the predictive validity of the eHLS-Web3.0 for 2 specific health behaviors (ie, physical activity and sedentary behavior), given their crucial impact on the physical and mental well-being of older adults with NCDs [ 40 ]. By identifying the predictive validity of the eHLS-Web3.0, this study is expected to make a noteworthy contribution to future research in this field. Finally, considering that gender, education level, and residence are potential correlates of eHealth literacy [ 6 , 33 , 41 ], the measurement invariance of the eHEALS would be examined at the configural, metric, strong, and strict levels across gender, education level, and residence.
Design, Participants, and Procedure
This study applied a 2-wave prospective design. Considering an item-to-response ratio of 1:10 and the recommendation for a minimum sample size of 200 in confirmatory factor analysis (CFA) [ 42 ], 240 participants were required to ensure a robust statistical estimation. With an approximate response rate of 85% and a prior estimated prevalence rate of NCDs of 50% in older adults [ 4 ], a minimum of 564 participants were required to be contacted at the initial recruitment stage. Eligible participants for the study were older adults who met the following inclusion criteria: (1) aged 60 years or older, (2) experiencing at least 1 type of NCD (eg, cardiovascular diseases, cancer, type 2 diabetes, and obesity), (3) no physical mobility restrictions, (4) no cognitive disorders, (5) proficient in reading and understanding Chinese, and (6) having access to a smartphone or laptop.
Participants were recruited from the outpatient departments of 6 hospitals from 3 cities (Shiyan, Wuhan, and Suizhou) of Hubei Province (Central China) using a convenience sampling approach. The survey was implemented using the SOJUMP web-based survey platform (Changsha Ranxing Information Technology Co, Ltd). Two health care professionals undertook an initial review of the scale items to ensure that the wording was appropriate for older adults with NCDs. Subsequently, 6 older adults with NCDs (3 female and 3 male) were invited to complete a pilot assessment aimed at (1) optimizing the design of the electronic questionnaires (eg, using the large font and highlighting the key information) and (2) refining the language and eliminating any errors to ensure that the scale items were easily comprehensible for the target population.
In the main study, participants were provided with a QR code through nurses to gain access to the web-based survey. Before answering the questionnaires, participants were required to sign an informed consent form on the first page of the survey. The web-based survey lasted approximately 20 minutes. To ensure a robust evaluation for the scale test-retest reliability and predictive validity, a minimum of 100 participants were needed [ 43 ]. Accounting for a potential 30% attrition rate (eg, no response and invalid or missing data) [ 4 ], a total of 142 participants were required for the second-wave data collection. Invitations were sent out randomly via SMS text messages to those who had completed the first round of data collection until enough participants agreed to participate in the follow-up survey, scheduled for 1 month later. Participants who agreed to participate in the second round of investigation were requested to revisit the hospital, where 2 qualified assistants guided them to complete the follow-up web-based survey and provided detailed instructions on the use of the accelerometer for data collection.
Ethical Considerations
This study adhered to the principles outlined in the Declaration of Helsinki by the World Medical Association. The Medical Ethics Committee of the Faculty of Medicine at Shenzhen University reviewed and approved this study (PN-202300066). All participants provided signed informed consent for both the primary study and the sensitivity analyses. The data were anonymized to protect participant privacy, and participation in the study was entirely voluntary. As a token of appreciation, participants received a participation fee of 5 RMB (US $0.7) on completing the data collection.
eHealth Literacy Scale-Web3.0
The 24-item eHLS-Web3.0 was originally developed by Liu et al [ 33 ] for the Chinese adult population. This scale comprises 3 dimensions: acquisition (items 1-4 and 11-14), verification (items 5-10), and application (items 15-24). Responses were indicated on a 5-point Likert scale, ranging from 1 (strongly disagree) to 5 (strongly agree). The total score of the scale ranges from 24 to 120, with a higher score indicating a greater level of eHealth literacy. The reliability and validity of the eHLS-Web3.0 have been fully supported by previous research with Chinese young adults (Cronbach α=0.91-0.97).
The 8-item eHEALS was developed by Norman and Skinner [ 17 ] for use among Canadian adolescents. The original scale is unidimensional and has been validated in various countries across diverse populations. The Chinese version of the 8-item eHEALS has been examined in previous studies among older adults with NCDs, where the reliability and validity of the scale have been fully supported (Cronbach α=0.95-0.98).
Health Behaviors
Physical activity and sedentary behavior were measured using the ActiGraph GT3X+ (ActiGraph) on the right side of the waist for 7 consecutive days, with the exception of swimming, bathing, and sleeping time. The accelerometer sampling interval was set at 60-second epochs with a sampling frequency of 30 Hz. Nonwear time was defined by an interval of 60 consecutive minutes of 0 counts per minute, allowing for 2 minutes of nonzero count interruptions. Participants with at least 3 valid days of accelerometer use (2 weekdays and 1 weekend day) and a minimum wear time of 10 hours per day were eligible for inclusion in the data analysis. The Freedson cutoff point was used for categorizing light physical activity (100-1951 counts/minute), moderate to vigorous physical activity (>1951 counts/minute), and sedentary behavior (<100 counts/minute) [ 44 ].
Demographics
The demographic information included age, sex, marital status, education level, residence, monthly income, living situation, and BMI.
Statistical Analyses
The data analyses were performed using IBM SPSS Statistics (version 28.0; IBM Corp) and Mplus 8 (Muthén & Muthén). Data screening and diagnosis tests of data distribution (eg, mean, SD, skewness, and kurtosis) and missing patterns were performed before the descriptive analysis and scale validation. To ensure a reliable estimation for the multidimensional scale, both Cronbach α and composite reliability (CR) coefficients were calculated to evaluate the internal consistency reliability of the eHLS-Web3.0. Additionally, the test-retest reliability was estimated using the intraclass correlation coefficient of pre- and 1-month follow-up data.
The construct validity of the eHLS-Web3.0 was evaluated using CFAs with maximum likelihood estimation. Several goodness-of-fit indices were computed, including robust chi-square ( χ 2 R ), robust chi-square to degrees of freedom ratio ( χ 2 R / df ), comparative-fit index (CFI), Tucker-Lewis index (TLI), root-mean-square error of approximation (RMSEA) and its 90% CI, and standardized root-mean-square residual (SRMR). The following criteria were considered for a satisfactory model goodness of fit: ≤3 for χ 2 R / df , ≥0.9 for CFI and TLI, and ≤0.08 for RMSEA and SRMR [ 45 ].
Convergent validity was assessed by examining the average variance extracted (AVE) and CR for each subscale, with AVE >0.5 and CR >0.7 indicating satisfactory convergent validity for the scale. Concurrent validity was assessed by calculating the zero-order correlations of the eHLS-Web3.0 and its subscales with the eHEALS, adjusted for all demographic confounders. For the discriminant validity, a presumptive 4-factor model incorporating 3 eHLS-Web3.0 subscales and unidimensional eHEALS was estimated in the CFA. The discriminant validity of the subscales was confirmed if the 95% CI of the association between these subscales did encompass the value of 0 and if the Wald chi-square test demonstrated a significant change in model fit after removing a constraint that fixed the factor correlation to zero [ 45 ]. Additionally, structural equation models were performed to assess the predictive validity of the scale by estimating its association with health behaviors, including physical activity and sedentary behavior.
With a sequential model testing approach, multigroup CFA was used to examine the measurement invariance of the eHLS-Web3.0 across gender, education, and residence. Four distinctive levels of measurement invariance were examined by progressively constraining the parameter estimates of the models to be equivalent across the samples: (1) configural invariance, where no parameter estimates were restricted to equality; (2) metric invariance, where factor loadings were constrained to equality; (3) strong invariance, where both factor loadings and item intercepts were constrained to equality; and (4) structural and strict invariance, where all factor loadings, item intercepts, and factor variance and covariance were restricted to equality. The measure invariance was supported if the change in the value of CFI and RMSEA was ≤0.01 and ≤0.015, respectively [ 45 , 46 ].
Descriptive Information of the Study Sample
As outlined in Figure 1 , a total of 642 eligible participants (mean 65.78, SD 3.91 years; 55.8% female) were included in the data analysis, of whom 134 (mean 65.63, SD 3.99 years; 58.2% female) provided valid data at the follow-up assessment. From the diagnostic evaluation, there were no missing data for eHLS-Web3.0 and eHEALS items in the study sample. All the scale items adhered to the normality distribution with absolute values of skewness and kurtosis <1. Descriptive information of the study sample is shown in Table 1 .

a NCD: noncommunicable disease.
b LPA: light physical activity.
c N/A: not applicable.
d MVPA: moderate to vigorous physical activity.
Reliabilities of the eHLS-Web3.0 in the Study Sample
Table 2 shows the mean value, SD, score range, and internal consistency and test-retest reliabilities of the eHLS-Web3.0 in the study sample. Regarding the internal consistency reliability, the eHLS-Web3.0 and its 3 subscales exhibited adequate Cronbach α values (range=0.89-0.94) and CR coefficients (range=0.90-0.97). Regarding the test-retest reliability, 2 time-point measures showed a strong intraclass correlation for the eHLS-Web3.0 and 3 subscales of the eHLS-Web3.0 ( r =0.81-0.91).
Validities of the eHLS-Web3.0 in the Study Sample
For the constructive validity, the results of the CFA showed that the 24-item 3D eHLS-Web3.0 achieved the criteria for good model fit indices in the study sample, with χ 2 R =674.4, df =248, χ 2 R / df =2.72 (<3), CFI=0.952 (>0.9), TLI=0.946 (>0.9), RMSEA=0.052 (90% CI 0.047-0.056; <0.08), and SRMR=0.034 (<0.08). The standardized factor loadings of the eHLS-Web3.0 items ranged from 0.658 to 0.819 (see Table S1 in Multimedia Appendix 1 ).
For concurrent validity, the zero-order correlations between the eHLS-Web3.0 subscales and eHEALS were significant ( r= 0.47-0.76), indicating a satisfactory result, as outlined in Table 3 . The AVE and CR were calculated as 0.58 and 0.97, respectively, using the standardized factor loadings of the items, showing a satisfactory convergent validity of the eHLS-Web3.0.
The latent factor correlations in a proposed 4-factor CFA model (ie, 3 eHLS-Web3.0 subscales and eHEALS) were calculated to evaluate the discriminant validity of the eHLS-Web3.0 subscales and eHEALS in the study sample. The goodness-of-fit indices of the 4-factor model were inferior to those of the original 3-factor eHLS-Web3.0 model, with χ 2 R =2079.8, df =461, χ 2 R / df =4.51, CFI=0.874, TLI=0.865, RMSEA=0.074 (90% CI 0.071-0.077), and SRMR=0.078. Table 4 presents the statistical results of the discriminant validity analysis. Wald chi-square findings were statistically significant in the study sample (all P <.001), and the CIs for each correlation did not contain the value of 0, demonstrating a satisfactory discriminant validity of the eHLS-Web3.0.
In addition, the eHLS-Web3.0 significantly predicted light physical activity ( β =.36, 95% CI 0.19-0.53; P =.004), moderate to vigorous physical activity ( β =.49, 95% CI 0.35-0.62; P <.001), and sedentary behavior ( β =–.26, 95% CI–0.40 to –0.12; P =.002), supporting the predictive validity of the scale for health behaviors. The goodness-of-fit indices indicated a satisfactory result for the 3 models, with χ 2 R =398.3-403.8, df =271, χ 2 R / df =1.47-1.49, CFI=0.949-0.951, TLI=0.944-0.946, RMSEA=0.059-0.060, and SRMR=0.043-0.044.
a P <.001.
a Wald chi-square test: Wald chi-square test constraining the values of the latent interfactor correlations to zero.
b P <.001.
c eHEALS: 8-item eHealth Literacy Scale.
Measurement Invariance of the eHLS-Web3.0 in the Study Sample
Table 5 presents the results of the examination regarding the measurement invariance of the eHLS-Web3.0 across gender, education level, and residence. The configural, metric, strong, and strict models were all shown to have a satisfactory fit to the data for all 3 pairs of subsamples, with ΔCFI <0.01 and ΔRMSEA <0.015. These indices provide support for the invariance of the factorial construct, factor loadings, intercepts, and residual variance of the eHLS-Web3.0 across gender, education level, and residence.
a Chi-square: robust chi-square.
b CFI: comparative fit index.
c ΔCFI: change in the CFI.
d RMSEA: root-mean-square error of approximation.
e ΔRMSEA: change in the RMSEA.
f M0: baseline configural invariance model.
g N/A: not applicable.
h M1: metric invariance model.
i M2: strong invariance model.
j M3: strict invariance model.
Principal Findings
This study aimed to evaluate the reliability, validity, and measurement invariance of the eHLS-Web3.0 for use with older adults who are living with NCDs. In particular, this study examined the internal consistency and test-retest reliabilities, as well as the construct, concurrent, convergent, discriminant, and predictive validities, and the measurement invariance of the eHLS-Web3.0 across gender, education level, and residence. Overall, the results from this study suggest that the eHLS-Web3.0 is a reliable and valid tool for measuring eHealth literacy in Chinese older adults with NCDs.
Regarding the reliabilities, analyses of the Cronbach α and CR coefficients indicated adequate internal consistency reliability for both the eHLS-Web3.0 and its 3 subscales. These findings are consistent with previous research on the use of the eHLS-Web3.0 among Chinese young adults [ 33 ]. It is worth noting that while previous studies have generally supported the reliability of the eHEALS and other eHealth literacy assessments (eg, DHLI and C-eHEALS) among older adults or those with NCDs [ 2 , 27 , 28 ], the novel eHEALS-Web3.0 tool has not yet been evaluated for reliability in older populations. This study is the first to investigate the reliability of the eHEALS-Web3.0 among older adults with NCDs. Additionally, previous psychometric analyses of eHealth literacy measures have primarily focused on internal consistency reliability, with test-retest reliability often overlooked [ 19 , 27 , 28 ]. In contrast, this study further examined the test-retest reliability of the eHLS-Web3.0 and its subscales, and the findings demonstrated a strong cross-time stability for the scale, as evidenced by a significant correlation between baseline and 1-month follow-up measures.
Regarding the construct validity, the CFA results provided support for the 3D model structure of the eHLS-Web3.0 among Chinese older adults with NCDs. The acquisition and verification subscales of the eHEALS-Web3.0 assess individuals’ eHealth abilities in Web1.0 and Web2.0 contexts, similar to the eHEALS and second-general eHealth literacy measures [ 12 , 19 , 27 ]. However, the eHEALS-Web3.0 stands out by also evaluating individuals’ proficiency in applying eHealth information to evolving health needs in the Web3.0 era (ie, the application subscale). As the digital landscape advances, individuals have more opportunities and options to use eHealth information. For instance, they can use eHealth information to make informed health decisions or resolve health-related problems, create their own health data, monitor their health status, interact with others, exchange information, and provide health advice to other health information seekers [ 31 , 33 ]. The 3D eHLS-Web3.0 provides a comprehensive assessment of eHealth literacy, catering to the present digital circumstances.
For other validities of the eHLS-Web3.0, the concurrent validity was confirmed by a significant correlation between the eHLS-Web3.0 and its subscales with the eHEALS, while the AVE and CR supported the convergent validity of the scale. In addition, as the 3 eHLS-Web3.0 subscales and eHEALS differ in conceptual content, a 4-factor model integrating the acquisition, verification, and application subscales and unidimensional eHEALS was established to confirm the discriminant validity of the scale. Although the Wald chi-square test results supported the discriminant validity of the eHLS-Web3.0, a high correlation was observed among the latent factors in the 4-factor model, possibly due to measurement errors [ 47 ]. To validate the earlier findings, zero-order correlations were calculated using composite (averaged) scales. Fortunately, the overall results confirmed the discriminant validity of the scale. Finally, the predictive validity of the eHLS-Web3.0 was supported by a significant positive association between the eHLS-Web3.0 and physical activity, as well as a negative association with sedentary behavior. Previous studies have demonstrated a positive association between eHealth literacy and health-promoting behaviors (eg, physical activity) among diverse populations [ 13 , 37 , 48 ]. However, there is a lack of evidence on the relationship between eHealth literacy and risk behaviors (eg, sedentary behavior). Our findings underline the potential of including eHealth literacy as a modifiable factor in future eHealth interventions to facilitate health behaviors and improve health outcomes among older adults with NCDs.
For measurement invariance, the establishment of configural, metric, strong, and strict invariances demonstrated that the eHLS-Web3.0 is a psychometrically sound instrument for measuring eHealth literacy among Chinese older adults with NCDs, regardless of their gender, education level, and residence. These invariances provide a solid foundation for making appropriate and meaningful transgroup comparisons in future studies.
Limitations and Implications
Some limitations should be noted. First, the nonrandom sampling used in this study may have limited the representativeness of the study findings. Therefore, a stratified random sampling approach is warranted in future studies. Second, given that the study findings are based only on the sample of Chinese older adults with NCDs, one should be cautious when generalizing these results to other samples. Future studies should examine the psychometric properties of the scale across different populations and diverse cultural contexts. Moreover, self-reported measures may result in some response biases (eg, recall bias and social desirability); therefore, the inclusion of objective means for assessing eHealth literacy should be considered in the future. Additionally, it is worth exploring the prediction of eHealth literacy on other health outcomes and examining its underlying mechanisms. Finally, from a pragmatic perspective, it may be beneficial to develop and validate a brief version of the eHLS-Web3.0, particularly with regard to older populations who may struggle with completing lengthy self-reported scales.
Despite the aforementioned limitations, this study addresses a significant gap in the literature by validating and applying the eHLS-Web3.0, a specific measure of eHealth literacy used for Chinese older adults with NCDs in the Web3.0 landscape. Previous reviews have revealed a wide range of influential factors of eHealth literacy as well as a positive correlation between higher eHealth literacy and better health behaviors, knowledge, and attitudes in older adults [ 38 , 49 - 51 ]. These findings indicate the potential for developing eHealth literacy interventions to promote positive health behaviors in the future while considering various socioeconomic and cultural variables. However, previous studies have yielded conflicting results regarding certain physical and psychosocial outcomes [ 38 ], underlining the need for more high-quality research. It is important to note that the success of these efforts largely depends on a reliable and accurate assessment of eHealth literacy [ 52 ].
The findings of this study provide robust support for the reliability, validity, and measurement invariance of the eHLS-Web3.0, indicating that this up-to-date tool can be widely used in future research endeavors to appropriately and accurately assess older adults’ abilities to search for, retrieve, evaluate, and use web-based health resources. This advancement has the potential to significantly contribute to both the field of eHealth literacy research and the development of targeted health promotion programs in the future. As digital technology increasingly infiltrates the health care sector, promoting eHealth literacy among older adults is more critical than ever [ 52 , 53 ]. The development and validation of the eHLS-Web3.0 marks a significant milestone in the field of eHealth literacy research, serving as a necessary foundation for future empirical investigations and targeted interventions aimed at improving eHealth literacy among older adults.
Conclusions
To the best of our knowledge, this is the first study to examine the psychometric properties and measurement invariance of the eHLS-Web3.0 among Chinese older adults with NCDs. This study provides evidence for internal consistency and test-retest reliabilities, construct, concurrent, convergent, discriminant, and predictive validities, and the measurement invariance of the 24-item 3D eHLS-Web3.0 for use with Chinese older adults with NCDs. The eHLS-Web3.0 can serve as a psychometrically sound instrument for assessing eHealth literacy in the Chinese context.
Acknowledgments
This research was funded by the Humanities and Social Science Fund of Ministry of Education of China (23YJCZH121), as well as the Humanities and Social Sciences Revitalization Grant of Shenzhen University (WKZX0312). The funding organizations had no role in the study design, study implementation, manuscript preparation, or publication decision. This work is the responsibility of the authors.
Authors' Contributions
WL, WC, and HL conceived and designed the study. HZ, JZ, RZ, and LZ contributed to the preparation of the study materials. WL, WC, NS, HZ, YY, and LZ collected the data. WL screened and analyzed the data. WL and WC drafted and revised the manuscript. All authors have reviewed and approved the final version of the manuscript.
Conflicts of Interest
None declared.
Standardized factor loadings of the 24-item eHealth Literacy Scale-Web3.0.
- Noncommunicable diseases. World Health Organization. 2022. URL: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases [accessed 2023-08-10]
- Wu Y, Wen J, Wang X, Wang Q, Wang W, Wang X, et al. Associations between e-health literacy and chronic disease self-management in older Chinese patients with chronic non-communicable diseases: a mediation analysis. BMC Public Health. 2022;22(1):2226. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Liu J, Yu W, Zhou J, Yang Y, Chen S, Wu S. Relationship between the number of noncommunicable diseases and health-related quality of life in Chinese older adults: a cross-sectional survey. Int J Environ Res Public Health. 2020;17(14):5150. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Duan Y, Shang B, Liang W, Lin Z, Hu C, Baker JS, et al. Predicting hand washing, mask wearing and social distancing behaviors among older adults during the covid-19 pandemic: an integrated social cognition model. BMC Geriatr. 2022;22(1):91. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Gong JB, Yu XW, Yi XR, Wang CH, Tuo XP. Epidemiology of chronic noncommunicable diseases and evaluation of life quality in elderly. Aging Med (Milton). 2018;1(1):64-66. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Shiferaw KB, Tilahun BC, Endehabtu BF, Gullslett MK, Mengiste SA. E-health literacy and associated factors among chronic patients in a low-income country: a cross-sectional survey. BMC Med Inform Decis Mak. 2020;20(1):181. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Powers MA, Bardsley J, Cypress M, Duker P, Funnell MM, Fischl AH, et al. Diabetes self-management education and support in type 2 diabetes. Diabetes Educ. 2017;43(1):40-53. [ CrossRef ] [ Medline ]
- Dwarswaard J, Bakker EJM, van Staa AL, Boeije HR. Self-management support from the perspective of patients with a chronic condition: a thematic synthesis of qualitative studies. Health Expect. 2016;19(2):194-208. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Bujnowska-Fedak M, Waligóra J, Mastalerz-Migas A. The internet as a source of health information and services. Adv Exp Med Biol. 2019;1211:1-16. [ CrossRef ] [ Medline ]
- Duff OM, Walsh DM, Furlong BA, O'Connor NE, Moran KA, Woods CB. Behavior change techniques in physical activity eHealth interventions for people with cardiovascular disease: systematic review. J Med Internet Res. 2017;19(8):e281. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Duan Y, Shang B, Liang W, Du G, Yang M, Rhodes RE. Effects of eHealth-based multiple health behavior change interventions on physical activity, healthy diet, and weight in people with noncommunicable diseases: systematic review and meta-analysis. J Med Internet Res. 2021;23(2):e23786. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Xie L, Mo PKH. Comparison of eHealth Literacy Scale (eHEALS) and Digital Health Literacy Instrument (DHLI) in assessing electronic health literacy in Chinese older adults: a mixed-methods approach. Int J Environ Res Public Health. 2023;20(4):3293. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Kim K, Shin S, Kim S, Lee E. The relation between eHealth literacy and health-related behaviors: systematic review and meta-analysis. J Med Internet Res. 2023;25:e40778. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Stellefson M, Chaney B, Barry AE, Chavarria E, Tennant B, Walsh-Childers K, et al. Web 2.0 chronic disease self-management for older adults: a systematic review. J Med Internet Res. 2013;15(2):e35. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Stellefson M, Paige SR, Tennant B, Alber JM, Chaney BH, Chaney D, et al. Reliability and validity of the telephone-based eHealth Literacy Scale among older adults: cross-sectional survey. J Med Internet Res. 2017;19(10):e362. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Richtering SS, Hyun K, Neubeck L, Coorey G, Chalmers J, Usherwood T, et al. eHealth literacy: predictors in a population with moderate-to-high cardiovascular risk. JMIR Hum Factors. 2017;4(1):e4. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Norman CD, Skinner HA. eHEALS: the eHealth Literacy Scale. J Med Internet Res. 2006;8(4):e27. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Bandura A. Self-Efficacy: the Exercise of Control. New York. W. H. Freeman; 1997.
- Lee J, Lee EH, Chae D. eHealth literacy instruments: systematic review of measurement properties. J Med Internet Res. 2021;23(11):e30644. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Chung SY, Nahm ES. Testing reliability and validity of the eHealth Literacy Scale (eHEALS) for older adults recruited online. Comput Inform Nurs. 2015;33(4):150-156. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Marsall M, Engelmann G, Skoda EM, Teufel M, Bäuerle A. Measuring electronic health literacy: development, validation, and test of measurement invariance of a revised German version of the eHealth Literacy Scale. J Med Internet Res. 2022;24(2):e28252. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Pérez GP, Almagro BJ, Gómez ÁH, Gómez JIA. Validación de la escala eHealth Literacy (eHEALS) en población universitaria española [Validation of the eHealth Literacy Scale (eHEALS) in Spanish University Students]. Rev Esp Salud Publica. 2015;89(3):329-338. [ FREE Full text ] [ CrossRef ] [ Medline ]
- van der Vaart R, van Deursen AJ, Drossaert CH, Taal E, van Dijk JA, van de Laar MA. Does the eHealth Literacy Scale (eHEALS) measure what it intends to measure? Validation of a Dutch version of the eHEALS in two adult populations. J Med Internet Res. 2011;13(4):e86. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Diviani N, Dima AL, Schulz PJ. A psychometric analysis of the Italian version of the eHealth Literacy Scale using item response and classical test theory methods. J Med Internet Res. 2017;19(4):e114. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Mialhe FL, Moraes KL, de Carvalho Sampaio HA, Brasil VV, da Silva Carvalho Vila V, Soares GH, et al. Evaluating the psychometric properties of the eHealth Literacy Scale in Brazilian adults. Rev Bras Enferm. 2021;75(1):e20201320. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Mitsutake S, Shibata A, Ishii K, Okazaki K, Oka K. [Developing Japanese version of the eHealth Literacy Scale (eHEALS)]. Nihon Koshu Eisei Zasshi. 2011;58(5):361-371. [ Medline ]
- Xu RH, Zhou L, Lu SY, Wong EL, Chang J, Wang D. Psychometric validation and cultural adaptation of the simplified Chinese eHealth Literacy Scale: cross-sectional study. J Med Internet Res. 2020;22(12):e18613. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Chang A, Schulz PJ. The measurements and an elaborated understanding of Chinese eHealth Literacy (C-eHEALS) in chronic patients in China. Int J Environ Res Public Health. 2018;15(7):1553. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Hyde LL, Boyes AW, Evans TJ, Mackenzie LJ, Sanson-Fisher R. Three-factor structure of the eHealth Literacy Scale among magnetic resonance imaging and computed tomography outpatients: a confirmatory factor analysis. JMIR Hum Factors. 2018;5(1):e6. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Tennant B, Stellefson M, Dodd V, Chaney B, Chaney D, Paige S, et al. eHealth literacy and Web 2.0 health information seeking behaviors among baby boomers and older adults. J Med Internet Res. 2015;17(3):e70. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Rudman R, Bruwer R. Defining Web 3.0: opportunities and challenges. Electron Libr. 2016;34(1):132-154. [ CrossRef ]
- Petrič G, Atanasova S, Kamin T. Ill literates or illiterates? Investigating the eHealth literacy of users of online health communities. J Med Internet Res. 2017;19(10):e331. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Liu HX, Chow BC, Liang W, Hassel H, Huang YW. Measuring a broad spectrum of eHealth skills in the Web 3.0 context using an eHealth Literacy Scale: development and validation study. J Med Internet Res. 2021;23(9):e31627. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Zrubka Z, Hajdu O, Rencz F, Baji P, Gulácsi L, Péntek M. Psychometric properties of the Hungarian version of the eHealth Literacy Scale. Eur J Health Econ. 2019;20(Suppl 1):57-69. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Kim H, Yang E, Ryu H, Kim HJ, Jang SJ, Chang SJ. Psychometric comparisons of measures of eHealth literacy using a sample of Korean older adults. Int J Older People Nurs. 2021;16(3):e12369. [ CrossRef ] [ Medline ]
- Collins LM. Research design and methods. In: Birren JE, editor. Encyclopedia of Gerontology (Second Edition). Amsterdam. Elsevier/Academic Press; 2007:433-442.
- Cui GH, Li SJ, Yin YT, Chen LJ, Li JQ, Liang FY, et al. The relationship among social capital, eHealth literacy and health behaviours in Chinese elderly people: a cross-sectional study. BMC Public Health. 2021;21(1):45. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Xie L, Zhang S, Xin M, Zhu M, Lu W, Mo PKH. Electronic health literacy and health-related outcomes among older adults: a systematic review. Prev Med. 2022;157:106997. [ CrossRef ] [ Medline ]
- Hutchesson MJ, Gough C, Müller AM, Short CE, Whatnall MC, Ahmed M, et al. eHealth interventions targeting nutrition, physical activity, sedentary behavior, or obesity in adults: a scoping review of systematic reviews. Obes Rev. 2021;22(10):e13295. [ CrossRef ] [ Medline ]
- Li Y, Fan X, Wei L, Yang K, Jiao M. The impact of high-risk lifestyle factors on all-cause mortality in the US non-communicable disease population. BMC Public Health. 2023;23(1):422. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Lee J, Tak SH. Factors associated with eHealth literacy focusing on digital literacy components: a cross-sectional study of middle-aged adults in South Korea. Digit Health. 2022;8:20552076221102765. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Byrne BM. Structural Equation Modeling with AMOS: Basic Concepts, Applications, and Programming, Second Edition. New York. Routledge, Taylor & Francis Group; 2013.
- Walter SD, Eliasziw M, Donner A. Sample size and optimal designs for reliability studies. Stat Med. 1998;17(1):101-110. [ CrossRef ] [ Medline ]
- Peters TM, Moore SC, Xiang YB, Yang G, Shu XO, Ekelund U, et al. Accelerometer-measured physical activity in Chinese adults. Am J Prev Med. 2010;38(6):583-591. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Liang W, Wang DD, Shang BR, Zhang CQ, Duan YP, Si GY. Further examination of the psychometric properties of the Brief Self-Control Scale: evidence from Chinese athletes and students. Int J Sport Exerc Psychol. 2020;20(1):16-35. [ CrossRef ]
- Cheung GW, Rensvold RB. Evaluating goodness-of-fit indexes for testing measurement invariance. Struct Equ Model Multidiscip J. 2002;9(2):233-255. [ CrossRef ]
- Hagger MS, Hankonen N, Kangro EM, Lintunen T, Pagaduan J, Polet J, et al. Trait self-control, social cognition constructs, and intentions: correlational evidence for mediation and moderation effects in diverse health behaviours. Appl Psychol Health Well Being. 2019;11(3):407-437. [ CrossRef ] [ Medline ]
- Mitsutake S, Shibata A, Ishii K, Oka K. Associations of eHealth literacy with health behavior among adult internet users. J Med Internet Res. 2016;18(7):e192. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Watkins I, Xie B. eHealth literacy interventions for older adults: a systematic review of the literature. J Med Internet Res. 2014;16(11):e225. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Shi Y, Ma D, Zhang J, Chen B. In the digital age: a systematic literature review of the e-health literacy and influencing factors among Chinese older adults. Z Gesundh Wiss. 2023;31(5):679-687. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Chang SJ, Jang SJ, Lee H, Kim H. Building on evidence to improve eHealth literacy in older adults: a systematic review. Comput Inform Nurs. 2021;39(5):241-247. [ CrossRef ] [ Medline ]
- Huang YQ, Liu L, Goodarzi Z, Watt JA. Diagnostic accuracy of eHealth literacy measurement tools in older adults: a systematic review. BMC Geriatr. 2023;23(1):181. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Arcury TA, Sandberg JC, Melius KP, Quandt SA, Leng X, Latulipe C, et al. Older adult internet use and eHealth literacy. J Appl Gerontol. 2020;39(2):141-150. [ FREE Full text ] [ CrossRef ] [ Medline ]
Abbreviations
Edited by T de Azevedo Cardoso; submitted 04.09.23; peer-reviewed by W Yu, S Jiang, B Shang; comments to author 21.11.23; revised version received 11.12.23; accepted 19.04.24; published 03.06.24.
©Wenfei Cai, Wei Liang, Huaxuan Liu, Rundong Zhou, Jie Zhang, Lin Zhou, Ning Su, Hanxiao Zhu, Yide Yang. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 03.06.2024.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work, first published in the Journal of Medical Internet Research, is properly cited. The complete bibliographic information, a link to the original publication on https://www.jmir.org/, as well as this copyright and license information must be included.
- Systematic Review
- Open access
- Published: 24 May 2024
Turnover intention and its associated factors among nurses in Ethiopia: a systematic review and meta-analysis
- Eshetu Elfios 1 ,
- Israel Asale 1 ,
- Merid Merkine 1 ,
- Temesgen Geta 1 ,
- Kidist Ashager 1 ,
- Getachew Nigussie 1 ,
- Ayele Agena 1 ,
- Bizuayehu Atinafu 1 ,
- Eskindir Israel 2 &
- Teketel Tesfaye 3
BMC Health Services Research volume 24 , Article number: 662 ( 2024 ) Cite this article
348 Accesses
Metrics details
Nurses turnover intention, representing the extent to which nurses express a desire to leave their current positions, is a critical global public health challenge. This issue significantly affects the healthcare workforce, contributing to disruptions in healthcare delivery and organizational stability. In Ethiopia, a country facing its own unique set of healthcare challenges, understanding and mitigating nursing turnover are of paramount importance. Hence, the objectives of this systematic review and meta-analysis were to determine the pooled proportion ofturnover intention among nurses and to identify factors associated to it in Ethiopia.
A comprehensive search carried out for studies with full document and written in English language through an electronic web-based search strategy from databases including PubMed, CINAHL, Cochrane Library, Embase, Google Scholar and Ethiopian University Repository online. Checklist from the Joanna Briggs Institute (JBI) was used to assess the studies’ quality. STATA version 17 software was used for statistical analyses. Meta-analysis was done using a random-effects method. Heterogeneity between the primary studies was assessed by Cochran Q and I-square tests. Subgroup and sensitivity analyses were carried out to clarify the source of heterogeneity.
This systematic review and meta-analysis incorporated 8 articles, involving 3033 nurses in the analysis. The pooled proportion of turnover intention among nurses in Ethiopia was 53.35% (95% CI (41.64, 65.05%)), with significant heterogeneity between studies (I 2 = 97.9, P = 0.001). Significant association of turnover intention among nurses was found with autonomous decision-making (OR: 0.28, CI: 0.14, 0.70) and promotion/development (OR: 0.67, C.I: 0.46, 0.89).
Conclusion and recommendation
Our meta-analysis on turnover intention among Ethiopian nurses highlights a significant challenge, with a pooled proportion of 53.35%. Regional variations, such as the highest turnover in Addis Ababa and the lowest in Sidama, underscore the need for tailored interventions. The findings reveal a strong link between turnover intention and factors like autonomous decision-making and promotion/development. Recommendations for stakeholders and concerned bodies involve formulating targeted retention strategies, addressing regional variations, collaborating for nurse welfare advocacy, prioritizing career advancement, reviewing policies for nurse retention improvement.
Peer Review reports
Turnover intention pertaining to employment, often referred to as the intention to leave, is characterized by an employee’s contemplation of voluntarily transitioning to a different job or company [ 1 ]. Nurse turnover intention, representing the extent to which nurses express a desire to leave their current positions, is a critical global public health challenge. This issue significantly affects the healthcare workforce, contributing to disruptions in healthcare delivery and organizational stability [ 2 ].
The global shortage of healthcare professionals, including nurses, is an ongoing challenge that significantly impacts the capacity of healthcare systems to provide quality services [ 3 ]. Nurses, as frontline healthcare providers, play a central role in patient care, making their retention crucial for maintaining the functionality and effectiveness of healthcare delivery. However, the phenomenon of turnover intention, reflecting a nurse’s contemplation of leaving their profession, poses a serious threat to workforce stability [ 4 ].
Studies conducted globally shows that high turnover rates among nurses in several regions, with notable figures reported in Alexandria (68%), China (63.88%), and Jordan (60.9%) [ 5 , 6 , 7 ]. In contrast, Israel has a remarkably low turnover rate of9% [ 8 ], while Brazil reports 21.1% [ 9 ], and Saudi hospitals26% [ 10 ]. These diverse turnover rates highlight the global nature of the nurse turnover phenomenon, indicating varying degrees of workforce mobility in different regions.
The magnitude and severity of turnover intention among nurses worldwide underscore the urgency of addressing this issue. High turnover rates not only disrupt healthcare services but also result in a loss of valuable skills and expertise within the nursing workforce. This, in turn, compromises the continuity and quality of patient care, with potential implications for patient outcomes and overall health service delivery [ 11 ]. Extensive research conducted worldwide has identified a range of factors contributing to turnover intention among nurses [ 11 , 12 , 13 , 14 , 15 , 16 , 17 ]. These factors encompass both individual and organizational aspects, such as high workload, inadequate support, limited career advancement opportunities, job satisfaction, conflict, payment or reward, burnout sense of belongingness to their work environment. The complex interplay of these factors makes addressing turnover intention a multifaceted challenge that requires targeted interventions.
In Ethiopia, a country facing its own unique set of healthcare challenges, understanding and mitigating nursing turnover are of paramount importance. The healthcare system in Ethiopia grapples with issues like resource constraints, infrastructural limitations, and disparities in healthcare access [ 18 ]. Consequently, the factors influencing nursing turnover in Ethiopia may differ from those in other regions. Previous studies conducted in the Ethiopian context have started to unravel some of these factors, emphasizing the need for a more comprehensive examination [ 18 , 19 ].
Although many cross-sectional studies have been conducted on turnover intention among nurses in Ethiopia, the results exhibit variations. The reported turnover intention rates range from a minimum of 30.6% to a maximum of 80.6%. In light of these disparities, this systematic review and meta-analysis was undertaken to ascertain the aggregated prevalence of turnover intention among nurses in Ethiopia. By systematically analyzing findings from various studies, we aimed to provide a nuanced understanding of the factors influencing turnover intention specific to the Ethiopian healthcare context. Therefore, this systematic review and meta-analysis aimed to answer the following research questions.
What is the pooled prevalence of turnover intention among nurses in Ethiopia?
What are the factors associated with turnover intention among nurses in Ethiopia?
The primary objective of this review was to assess the pooled proportion of turnover intention among nurses in Ethiopia. The secondary objective was identifying the factors associated to turnover intention among nurses in Ethiopia.
Study design and search strategy
A comprehensive systematic review and meta-analysis was conducted, examining observational studies on turnover intention among nurses in Ethiopia. The procedure for this systematic review and meta-analysis was developed in accordance with the Preferred Reporting Items for Systematic review and Meta-analysis Protocols (PRISMA-P) statement [ 20 ]. PRISMA-2015 statement was used to report the findings [ 21 , 22 ]. This systematic review and meta-analysis were registered on PROSPERO with the registration number of CRD42024499119.
We conducted systematic and an extensive search across multiple databases, including PubMed, CINAHL, Cochrane Library, Embase, Google Scholar and Ethiopian University Repository online to identify studies reporting turnover intention among nurses in Ethiopia. We reviewed the database available at http://www.library.ucsf.edu and the Cochrane Library to ensure that the intended task had not been previously undertaken, preventing any duplication. Furthermore, we screened the reference lists to retrieve relevant articles. The process involved utilizing EndNote (version X8) software for downloading, organizing, reviewing, and citing articles. Additionally, a manual search for cross-references was performed to discover any relevant studies not captured through the initial database search. The search employed a comprehensive set of the following search terms:“prevalence”, “turnover intention”, “intention to leave”, “attrition”, “employee attrition”, “nursing staff turnover”, “Ethiopian nurses”, “nurses”, and “Ethiopia”. These terms were combined using Boolean operators (AND, OR) to conduct a thorough and systematic search across the specified databases.
Eligibility criteria
Inclusion criteria.
The established inclusion criteria for this meta-analysis and systematic review are as follows to guide the selection of articles for inclusion in this review.
Population: Nurses working in Ethiopia.
Study period: studies conducted or published until 23November 2023.
Study design: All observational study designs, such as cross-sectional, longitudinal, and cohort studies, were considered.
Setting: Only studies conducted in Ethiopia were included.
Outcome; turnover intention.
Study: All studies, whether published or unpublished, in the form of journal articles, master’s theses, and dissertations, were included up to the final date of data analysis.
Language: This study exclusively considered studies in the English language.
Exclusion criteria
Excluded were studies lacking full text or Studies with a Newcastle–Ottawa Quality Assessment Scale (NOS) score of 6 or less. Studies failing to provide information on turnover intention among nurses or studies for which necessary details could not be obtained were excluded. Three authors (E.E., T.G., K.A) independently assessed the eligibility of retrieved studies, other two authors (E.I & M.M) input sought for consensus on potential in- or exclusion.
Quality assessment and data extraction
Two authors (E.E, A.A, G.N) independently conducted a critical appraisal of the included studies. Joanna Briggs Institute (JBI) checklists of prevalence study was used to assess the quality of the studies. Studies with a Newcastle–Ottawa Quality Assessment Scale (NOS) score of seven or more were considered acceptable [ 23 ]. The tool has nine parameters, which have yes, no, unclear, and not applicable options [ 24 ]. Two reviewers (I.A, B.A) were involved when necessary, during the critical appraisal process. Accordingly, all studies were included in our review. ( Table 1 ) Questions to evaluate the methodological quality of studies on turnover intention among nurses and its associated factors in Ethiopia are the followings:
Q1 = was the sample frame appropriate to address the target population?
Q2. Were study participants sampled appropriately.
Q3. Was the sample size adequate?
Q4. Were the study subjects and the setting described in detail?
Q5. Was the data analysis conducted with sufficient coverage of the identified sample?
Q6. Were the valid methods used for the identification of the condition?
Q7. Was the condition measured in a standard, reliable way for all participants?
Q8. Was there appropriate statistical analysis?
Q9. Was the response rate adequate, and if not, was the low response rate.
managed appropriately?
Data was extracted and recorded in a Microsoft Excel as guided by the Joanna Briggs Institute (JBI) data extraction form for observational studies. Three authors (E.E, M.G, T.T) independently conducted data extraction. Recorded data included the first author’s last name, publication year, study setting or country, region, study design, study period, sample size, response rate, population, type of management, proportion of turnover intention, and associated factors. Discrepancies in data extraction were resolved through discussion between extractors.
Data processing and analysis
Data analysis procedures involved importing the extracted data into STATA 14 statistical software for conducting a pooled proportion of turnover intention among nurses. To evaluate potential publication bias and small study effects, both funnel plots and Egger’s test were employed [ 25 , 26 ]. We used statistical tests such as the I statistic to quantify heterogeneity and explore potential sources of variability. Additionally, subgroup analyses were conducted to investigate the impact of specific study characteristics on the overall results. I 2 values of 0%, 25%, 50%, and 75% were interpreted as indicating no, low, medium, and high heterogeneity, respectively [ 27 ].
To assess publication bias, we employed several methods, including funnel plots and Egger’s test. These techniques allowed us to visually inspect asymmetry in the distribution of study results and statistically evaluate the presence of publication bias. Furthermore, we conducted sensitivity analyses to assess the robustness of our findings to potential publication bias and other sources of bias.
Utilizing a random-effects method, a meta-analysis was performed to assess turnover intention among nurses, employing this method to account for observed variability [ 28 ]. Subgroup analyses were conducted to compare the pooled magnitude of turnover intention among nurses and associated factors across different regions. The results of the pooled prevalence were visually presented in a forest plot format with a 95% confidence interval.
Study selection
After conducting the initial comprehensive search concerning turnover intention among nurses through Medline, Cochran Library, Web of Science, Embase, Ajol, Google Scholar, and other sources, a total of 1343 articles were retrieved. Of which 575 were removed due to duplication. Five hundred ninety-three articles were removed from the remaining 768 articles by title and abstract. Following theses, 44 articles which cannot be retrieved were removed. Finally, from the remaining 131 articles, 8 articles with a total 3033 nurses were included in the systematic review and meta-analysis (Fig. 1 ).

PRISMA flow diagram of the selection process of studies on turnover intention among nurses in Ethiopia, 2024
Study characteristics
All included 8 studies had a cross-sectional design and of which, 2 were from Tigray region, 2 were from Addis Ababa(Capital), 1 from south region, 1 from Amhara region, 1 from Sidama region, and 1 was multiregional and Nationwide. The prevalence of turnover intention among nurses ‘ranges from 30.6 to 80.6%. Table 2 .
Pooled prevalence of turnover intention among nurses in Ethiopia
Our comprehensive meta-analysis revealed a notable turnover intention rate of 53.35% (95% CI: 41.64, 65.05%) among Ethiopian nurses, accompanied by substantial heterogeneity between studies (I 2 = 97.9, P = 0.000) as depicted in Fig. 2 . Given the observed variability, we employed a random-effects model to analyze the data, ensuring a robust adjustment for the significant heterogeneity across the included studies.

Forest plot showing the pooled proportion of turnover intention among nurses in Ethiopia, 2024
Subgroup analysis of turnover intention among nurses in Ethiopia
To address the observed heterogeneity, we conducted a subgroup analysis based on regions. The results of the subgroup analysis highlighted considerable variations, with the highest level of turnover intention identified in Addis Ababa at 69.10% (95% CI: 46.47, 91.74%) and substantial heterogeneity (I 2 = 98.1%). Conversely, the Sidama region exhibited the lowest level of turnover intention among nurses at 30.6% (95% CI: 25.18, 36.02%), accompanied by considerable heterogeneity (I 2 = 100.0%) ( Fig. 3 ).

Subgroup analysis of systematic review and meta-analysis by region of turnover intention among nurses in Ethiopia, 2024
Publication bias of turnover intention among nurses in Ethiopia
The Egger’s test result ( p = 0.64) is not statistically significant, indicating no evidence of publication bias in the meta-analysis (Table 3 ). Additionally, the symmetrical distribution of included studies in the funnel plot (Fig. 4 ) confirms the absence of publication bias across studies.

Funnel plot of systematic review and meta-analysis on turnover intention among nurses in Ethiopia, 2024
Sensitivity analysis
The leave-out-one sensitivity analysis served as a meticulous evaluation of the influence of individual studies on the comprehensive pooled prevalence of turnover intention within the context of Ethiopian nurses. In this systematic process, each study was methodically excluded from the analysis one at a time. The outcomes of this meticulous examination indicated that the exclusion of any particular study did not lead to a noteworthy or statistically significant alteration in the overall pooled estimate of turnover intention among nurses in Ethiopia. The findings are visually represented in Fig. 5 , illustrating the stability and robustness of the overall pooled estimate even with the removal of specific studies from the analysis.

Sensitivity analysis of pooled prevalence for each study being removed at a time for systematic review and meta-analysis of turnover intention among nurses in Ethiopia
Factors associated with turnover intention among nurses in Ethiopia
In our meta-analysis, we comprehensively reviewed and conducted a meta-analysis on the determinants of turnover intention among nurses in Ethiopia by examining eight relevant studies [ 6 , 29 , 30 , 31 , 32 , 33 , 34 , 35 ]. We identified a significant association between turnover intention with autonomous decision-making (OR: 0.28, CI: 0.14, 0.70) (Fig. 6 ) and promotion/development (OR: 0.67, CI: 0.46, 0.89) (Fig. 7 ). In both instances, the odds ratios suggest a negative association, signifying that increased levels of autonomous decision-making and promotion/development were linked to reduced odds of turnover intention.

Forest plot of the association between autonomous decision making with turnover intention among nurses in Ethiopia2024

Forest plot of the association between promotion/developpment with turnover intention among nurses in Ethiopia, 2024
In our comprehensive meta-analysis exploring turnover intention among nurses in Ethiopia, our findings revealed a pooled proportion of turnover intention at 53.35%. This significant proportion warrants a comparative analysis with turnover rates reported in other global regions. Distinct variations emerge when compared with turnover rates in Alexandria (68%), China (63.88%), and Jordan (60.9%) [ 5 , 6 , 7 ]. This comparison highlights that the multifaceted nature of turnover intention, influenced by diverse contextual, cultural, and organizational factors. Conversely, Ethiopia’s turnover rate among nurses contrasts with substantially lower figures reported in Israel (9%) [ 8 ], Brazil (21.1%) [ 9 ], and Saudi hospitals (26%) [ 10 ]. Challenges such as work overload, economic constraints, limited promotional opportunities, lack of recognition, and low job rewards are more prevalent among nurses in Ethiopia, contributing to higher turnover intention compared to their counterparts [ 7 , 29 , 36 ].
The highest turnover intention was observed in Addis Ababa, while Sidama region displayed the lowest turnover intention among nurses, These differences highlight the complexity of turnover intention among Ethiopian nurses, showing the importance of specific interventions in each region to address unique factors and improve nurses’ retention.
Our systematic review and meta-analysis in the Ethiopian nursing context revealed a significant inverse association between turnover intention and autonomous decision-making. The odd of turnover intention is approximately reduced by 72% in employees with autonomous decision-making compared to those without autonomous decision-making. This finding was supported by other similar studies conducted in South Africa, Tanzania, Kenya, and Turkey [ 37 , 38 , 39 , 40 ].
The significant association of turnover intention with promotion/development in our study underscores the crucial role of career advancement opportunities in alleviating turnover intention among nurses. Specifically, our analysis revealed that individuals with promotion/development had approximately 33% lower odds of turnover intention compared to those without such opportunities. These results emphasize the pivotal influence of organizational support in shaping the professional environment for nurses, providing substantive insights for the formulation of evidence-based strategies targeted at enhancing workforce retention. This finding is in line with former researches conducted in Taiwan, Philippines and Italy [ 41 , 42 , 43 ].
Our meta-analysis on turnover intention among Ethiopian nurses reveals a considerable challenge, with a pooled proportion of 53.35%. Regional variations highlight the necessity for region-specific strategies, with Addis Ababa displaying the highest turnover intention and Sidama region the lowest. A significant inverse association was found between turnover intention with autonomous decision-making and promotion/development. These insights support the formulation of evidence-based strategies and policies to enhance nurse retention, contributing to the overall stability of the Ethiopian healthcare system.
Recommendations
Federal ministry of health (fmoh).
The FMoH should consider the regional variations in turnover intention and formulate targeted retention strategies. Investment in professional development opportunities and initiatives to enhance autonomy can be integral components of these strategies.
Ethiopian nurses association (ENA)
ENA plays a pivotal role in advocating for the welfare of nurses. The association is encouraged to collaborate with healthcare institutions to promote autonomy, create mentorship programs, and advocate for improved working conditions to mitigate turnover intention.
Healthcare institutions
Hospitals and healthcare facilities should prioritize the provision of career advancement opportunities and recognize the value of professional autonomy in retaining nursing staff. Tailored interventions based on regional variations should be considered.
Policy makers
Policymakers should review existing healthcare policies to identify areas for improvement in nurse retention. Policy changes that address challenges such as work overload, limited promotional opportunities, and economic constraints can positively impact turnover rates.
Future research initiatives
Further research exploring the specific factors contributing to turnover intention in different regions of Ethiopia is recommended. Understanding the nuanced challenges faced by nurses in various settings will inform the development of more targeted interventions.
Strength and limitations
Our systematic review and meta-analysis on nurse turnover intention in Ethiopia present several strengths. The comprehensive inclusion of diverse studies provides a holistic view of the issue, enhancing the generalizability of our findings. The use of a random-effects model accounts for potential heterogeneity, ensuring a more robust and reliable synthesis of data.
However, limitations should be acknowledged. The heterogeneity observed across studies, despite the use of a random-effects model, may impact the precision of the pooled estimate. These considerations should be taken into account when interpreting and applying the results of our analysis.
Data availability
Data set used on this analysis will available from corresponding author upon reasonable request.
Abbreviations
Ethiopian Nurses Association
Federal Ministry of Health
Joanna Briggs Institute
Preferred Reporting Items for Systematic review and Meta-analysis Protocols
Kanchana L, Jayathilaka R. Factors impacting employee turnover intentions among professionals in Sri Lankan startups. PLoS ONE. 2023;18(2):e0281729.
Article CAS PubMed PubMed Central Google Scholar
Boateng AB, et al. Factors influencing turnover intention among nurses and midwives in Ghana. Nurs Res Pract. 2022;2022:4299702.
PubMed PubMed Central Google Scholar
Organization WH. WHO Guideline on Health Workforce Development Attraction, Recruitment and Retention in Rural and Remote Areas, 2021, pp. 1-104.
Hayes LJ, et al. Nurse turnover: a literature review. Int J Nurs Stud. 2006;43(2):237–63.
Article PubMed Google Scholar
Yang H, et al. Validation of work pressure and associated factors influencing hospital nurse turnover: a cross-sectional investigation in Shaanxi Province, China. BMC Health Serv Res. 2017;17:1–11.
Article Google Scholar
Ayalew E et al. Nurses’ intention to leave their job in sub-Saharan Africa: A systematic review and meta-analysis. Heliyon, 2021. 7(6).
Al Momani M. Factors influencing public hospital nurses’ intentions to leave their current employment in Jordan. Int J Community Med Public Health. 2017;4(6):1847–53.
DeKeyser Ganz F, Toren O. Israeli nurse practice environment characteristics, retention, and job satisfaction. Isr J Health Policy Res. 2014;3(1):1–8.
de Oliveira DR, et al. Intention to leave profession, psychosocial environment and self-rated health among registered nurses from large hospitals in Brazil: a cross-sectional study. BMC Health Serv Res. 2017;17(1):21.
Article PubMed PubMed Central Google Scholar
Dall’Ora C, et al. Association of 12 h shifts and nurses’ job satisfaction, burnout and intention to leave: findings from a cross-sectional study of 12 European countries. BMJ Open. 2015;5(9):e008331.
Lu H, Zhao Y, While A. Job satisfaction among hospital nurses: a literature review. Int J Nurs Stud. 2019;94:21–31.
Ramoo V, Abdullah KL, Piaw CY. The relationship between job satisfaction and intention to leave current employment among registered nurses in a teaching hospital. J Clin Nurs. 2013;22(21–22):3141–52.
Al Sabei SD, et al. Nursing work environment, turnover intention, Job Burnout, and Quality of Care: the moderating role of job satisfaction. J Nurs Scholarsh. 2020;52(1):95–104.
Wang H, Chen H, Chen J. Correlation study on payment satisfaction, psychological reward satisfaction and turnover intention of nurses. Chin Hosp Manag. 2018;38(03):64–6.
Google Scholar
Loes CN, Tobin MB. Interpersonal conflict and organizational commitment among licensed practical nurses. Health Care Manag (Frederick). 2018;37(2):175–82.
Wei H, et al. The state of the science of nurse work environments in the United States: a systematic review. Int J Nurs Sci. 2018;5(3):287–300.
Nantsupawat A, et al. Effects of nurse work environment on job dissatisfaction, burnout, intention to leave. Int Nurs Rev. 2017;64(1):91–8.
Article CAS PubMed Google Scholar
Ayalew F, et al. Factors affecting turnover intention among nurses in Ethiopia. World Health Popul. 2015;16(2):62–74.
Debie A, Khatri RB, Assefa Y. Contributions and challenges of healthcare financing towards universal health coverage in Ethiopia: a narrative evidence synthesis. BMC Health Serv Res. 2022;22(1):866.
Moher D, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Reviews. 2015;4(1):1–9.
Moher D, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151(4):264–9.
Moher D et al. Group, P.-P.(2015) Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement.
Institute JB. Checklist for Prevalence Studies. Checkl prevalance Stud [Internet]. 2016;7.
Sakonidou S, et al. Interventions to improve quantitative measures of parent satisfaction in neonatal care: a systematic review. BMJ Paediatr Open. 2020;4(1):e000613.
Egger M, Smith GD. Meta-analysis: potentials and promise. BMJ. 1997;315(7119):1371.
Tura G, Fantahun M, Worku A. The effect of health facility delivery on neonatal mortality: systematic review and meta-analysis. BMC Pregnancy Childbirth. 2013;13:18.
Lin L. Comparison of four heterogeneity measures for meta-analysis. J Eval Clin Pract. 2020;26(1):376–84.
McFarland LV. Meta-analysis of probiotics for the prevention of antibiotic associated diarrhea and the treatment of Clostridium difficile disease. Am J Gastroenterol. 2006;101(4):812–22.
Asegid A, Belachew T, Yimam E. Factors influencing job satisfaction and anticipated turnover among nurses in Sidama zone public health facilities, South Ethiopia Nursing research and practice, 2014. 2014.
Wubetie A, Taye B, Girma B. Magnitude of turnover intention and associated factors among nurses working in emergency departments of governmental hospitals in Addis Ababa, Ethiopia: a cross-sectional institutional based study. BMC Nurs. 2020;19:97.
Getie GA, Betre ET, Hareri HA. Assessment of factors affecting turnover intention among nurses working at governmental health care institutions in east Gojjam, Amhara region, Ethiopia, 2013. Am J Nurs Sci. 2015;4(3):107–12.
Gebregziabher D, et al. The relationship between job satisfaction and turnover intention among nurses in Axum comprehensive and specialized hospital Tigray, Ethiopia. BMC Nurs. 2020;19(1):79.
Negarandeh R et al. Magnitude of nurses’ intention to leave their jobs and its associated factors of nurses working in tigray regional state, north ethiopia: cross sectional study 2020.
Nigussie Bolado G, et al. The magnitude of turnover intention and Associated factors among nurses working at Governmental Hospitals in Southern Ethiopia: a mixed-method study. Nursing: Research and Reviews; 2023. pp. 13–29.
Woldekiros AN, Getye E, Abdo ZA. Magnitude of job satisfaction and intention to leave their present job among nurses in selected federal hospitals in Addis Ababa, Ethiopia. PLoS ONE. 2022;17(6):e0269540.
Rhoades L, Eisenberger R. Perceived organizational support: a review of the literature. J Appl Psychol. 2002;87(4):698.
Lewis M. Causal factors that influence turnover intent in a manufacturing organisation. University of Pretoria (South Africa); 2008.
Kuria S, Alice O, Wanderi PM. Assessment of causes of labour turnover in three and five star-rated hotels in Kenya International journal of business and social science, 2012. 3(15).
Blaauw D, et al. Comparing the job satisfaction and intention to leave of different categories of health workers in Tanzania, Malawi, and South Africa. Global Health Action. 2013;6(1):19287.
Masum AKM, et al. Job satisfaction and intention to quit: an empirical analysis of nurses in Turkey. PeerJ. 2016;4:e1896.
Song L. A study of factors influencing turnover intention of King Power Group at Downtown Area in Bangkok, Thailand. Volume 2. International Review of Research in Emerging Markets & the Global Economy; 2016. 3.
Karanikola MN, et al. Moral distress, autonomy and nurse-physician collaboration among intensive care unit nurses in Italy. J Nurs Manag. 2014;22(4):472–84.
Labrague LJ, McEnroe-Petitte DM, Tsaras K. Predictors and outcomes of nurse professional autonomy: a cross-sectional study. Int J Nurs Pract. 2019;25(1):e12711.
Download references
No funding was received.
Author information
Authors and affiliations.
School of Nursing, College of Health Science and Medicine, Wolaita Sodo University, Wolaita Sodo, Ethiopia
Eshetu Elfios, Israel Asale, Merid Merkine, Temesgen Geta, Kidist Ashager, Getachew Nigussie, Ayele Agena & Bizuayehu Atinafu
Department of Midwifery, College of Health Science and Medicine, Wolaita Sodo University, Wolaita Sodo, Ethiopia
Eskindir Israel
Department of Midwifery, College of Health Science and Medicine, Wachamo University, Hossana, Ethiopia
Teketel Tesfaye
You can also search for this author in PubMed Google Scholar
Contributions
E.E. conceptualized the study, designed the research, performed statistical analysis, and led the manuscript writing. I.A, T.G, M.M contributed to the study design and provided critical revisions. K.A., G.N, B.A., E.I., and T.T. participated in data extraction and quality assessment. M.M. and T.G. K.A. and G.N. contributed to the literature review. I.A, A.A. and B.A. assisted in data interpretation. E.I. and T.T. provided critical revisions to the manuscript. All authors read and approved the final version.
Corresponding author
Correspondence to Eshetu Elfios .
Ethics declarations
Ethical approval.
Ethical approval and informed consent are not required, as this study is a systematic review and meta-analysis that only involved the use of previously published data.
Ethical guidelines
Not applicable.
Consent for publication
Competing interests.
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Elfios, E., Asale, I., Merkine, M. et al. Turnover intention and its associated factors among nurses in Ethiopia: a systematic review and meta-analysis. BMC Health Serv Res 24 , 662 (2024). https://doi.org/10.1186/s12913-024-11122-9
Download citation
Received : 20 January 2024
Accepted : 20 May 2024
Published : 24 May 2024
DOI : https://doi.org/10.1186/s12913-024-11122-9
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Turnover intention
- Systematic review
- Meta-analysis
BMC Health Services Research
ISSN: 1472-6963
- General enquiries: [email protected]
- Open access
- Published: 30 May 2024
Differential attainment in assessment of postgraduate surgical trainees: a scoping review
- Rebecca L. Jones 1 , 2 ,
- Suwimol Prusmetikul 1 , 3 &
- Sarah Whitehorn 1
BMC Medical Education volume 24 , Article number: 597 ( 2024 ) Cite this article
81 Accesses
Metrics details
Introduction
Solving disparities in assessments is crucial to a successful surgical training programme. The first step in levelling these inequalities is recognising in what contexts they occur, and what protected characteristics are potentially implicated.
This scoping review was based on Arksey & O’Malley’s guiding principles. OVID and Embase were used to identify articles, which were then screened by three reviewers.
From an initial 358 articles, 53 reported on the presence of differential attainment in postgraduate surgical assessments. The majority were quantitative studies (77.4%), using retrospective designs. 11.3% were qualitative. Differential attainment affects a varied range of protected characteristics. The characteristics most likely to be investigated were gender (85%), ethnicity (37%) and socioeconomic background (7.5%). Evidence of inequalities are present in many types of assessment, including: academic achievements, assessments of progression in training, workplace-based assessments, logs of surgical experience and tests of technical skills.
Attainment gaps have been demonstrated in many types of assessment, including supposedly “objective” written assessments and at revalidation. Further research is necessary to delineate the most effective methods to eliminate bias in higher surgical training. Surgical curriculum providers should be informed by the available literature on inequalities in surgical training, as well as other neighbouring specialties such as medicine or general practice, when designing assessments and considering how to mitigate for potential causes of differential attainment.
Peer Review reports
Diversity in the surgical workforce has been a hot topic for the last 10 years, increasing in traction following the BlackLivesMatter movement in 2016 [ 1 ]. In the UK this culminated in publication of the Kennedy report in 2021 [ 2 ]. Before this the focus was principally on gender imbalance in surgery, with the 2010 Surgical Workforce report only reporting gender percentages by speciality, with no comment on racial profile, sexuality distribution, disability occurrence, or socioeconomic background [ 3 ].
Gender is not the only protected characteristic deserving of equity in surgery; many groups find themselves at a disadvantage during postgraduate surgical examinations [ 4 ] and at revalidation [ 5 ]. This phenomenon is termed ‘differential attainment’ (DA), in which disparities in educational outcomes, progression rates, or achievements between groups with protected characteristics occur [ 4 ]. This may be due to the assessors’ subconscious bias, or a deficit in training and education before assessment.
One of the four pillars of medical ethics is “justice”, emphasising that healthcare should be provided in a fair, equitable, and ethical manner, benefiting all individuals and promoting the well-being of society as a whole. This applies not only to our patients but also to our colleagues; training should be provided in a fair, equitable, and ethical manner, benefiting all. By applying the principle of justice to surgical trainees, we can create an environment that is supportive, inclusive, and conducive to professional growth and well-being.
A diverse consultant body is crucial for providing high-quality healthcare to a diverse patient population. It has been shown that patients are happier when cared for by a doctor with the same ethnic background [ 6 ]. Takeshita et al. [ 6 ] proposed this is due to a greater likelihood of mutual understanding of cultural values, beliefs, and preferences and is therefore more likely to cultivate a trusting relationship, leading to accurate diagnosis, treatment adherence and improved patient understanding. As such, ensuring that all trainees are justly educated and assessed throughout their training may contribute to improving patient care by diversifying the consultant body.
Surgery is well known to have its own specific culture, language, and social rules which are unique even within the world of medicine [ 7 , 8 ]. Through training, graduates develop into surgeons, distinct from other physicians and practitioners [ 9 ]. As such, research conducted in other medical domains is not automatically applicable to surgery, and behavioural interventions focused on reducing or eliminating bias in training need to be tailored specifically to surgical settings.
Consequently, it’s important that the surgical community asks the questions:
Does DA exist in postgraduate surgical training, and to what extent?
Why does DA occur?
What groups or assessments are under-researched?
How can we apply this knowledge, or acquire new knowledge, to provide equity for trainees?
The following scoping review hopes to provide the surgical community with robust answers for future of surgical training.
Aims and research question
The aim of this scoping review is to understand the breadth of research about the presence of DA in postgraduate surgical education and to determine themes pertaining to causes of inequalities. A scoping review was chosen to provide a means to map the available literature, including published peer-reviewed primary research and grey literature.
Following the methodological framework set out by Arksey and O’Malley [ 10 ], our research was intended to characterise the literature addressing DA in HST, including Ophthalmology, Obstetrics & Gynaecology (O&G). We included literature from English-language speaking countries, including the UK and USA.
Search strategy
We used search terms tailored to our target population characteristics (e.g., gender, ethnicity), concept (i.e., DA) and context (i.e., assessment in postgraduate surgical education). Medline and Embase were searched with the assistance of a research librarian, with addition of synonyms. This was conducted in May 2023, and was exported to Microsoft Excel for further review. The reference lists of included articles were also searched to find any relevant data sources that had yet to be considered. In addition, to identify grey literature, a search was performed for the term “differential attainment” and “disparity” on the relevant stakeholders’ websites (See supplemental Table 1 for full listing). Stakeholders were included on the basis of their involvement in governance or training of surgical trainees.
Study selection
To start we excluded conference abstracts that were subsequently published as full papers to avoid duplications ( n = 337). After an initial screen by title to exclude obviously irrelevant articles, articles were filtered to meet our inclusion and exclusion criteria (Table 1 ). The remaining articles ( n = 47) were then reviewed in their entirety, with the addition of five reports found in grey literature. Following the screening process, 45 studies were recruited for scoping review (Fig. 1 ).
Charting the data
The extracted data included literature title, authors, year of publication, country of study, study design, population characteristic, case number, context, type of assessment, research question and main findings (Appendix 1). Extraction was performed initially by a single author and then subsequently by a second author to ensure thorough review. Group discussion was conducted in case of any disagreements. As charting occurred, papers were discovered within reference lists of included studies which were eligible for inclusion; these were assimilated into the data charting table and included in the data extraction ( n = 8).
Collating, summarizing and reporting the results
The included studies were not formally assessed in their quality or risk of bias, consistent with a scoping review approach [ 10 ]. However, group discussion was conducted during charting to aid argumentation and identify themes and trends.
We conducted a descriptive numerical summary to describe the characteristics of included studies. Then thematic analysis was implemented to examine key details and organise the attainment quality and population characteristics based on their description. The coding of themes was an iterative process and involved discussion between authors, to identify and refine codes to group into themes.
We categorised the main themes as gender, ethnicity, country of graduation, individual and family background in education, socioeconomic background, age, and disability. The number of articles in each theme is demonstrated in Table 2 . Data was reviewed and organised into subtopics based on assessment types included: academic achievement (e.g., MRCS, FRCS), assessments for progression (e.g., ARCP), workplace-based assessment (e.g., EPA, feedback), surgical experience (e.g., case volume), and technical skills (e.g., visuo-spatial tasks).

PRISMA flow diagram
44 articles defined the number of included participants (89,399 participants in total; range of participants across individual studies 16–34,755). Two articles reported the number of included studies for their meta-analysis (18 and 63 included articles respectively). Two reports from grey literature did not define the number of participants they included in their analysis. The characteristics of the included articles are displayed in Table 2 .

Growth in published literature on differential attainment over the past 40 years
Academic achievement
In the American Board of Surgery Certifying Exam (ABSCE), Maker [ 11 ] found there to be no significant differences in terms of gender when comparing those who passed on their first attempt and those who did not in general surgery training, a finding supported by Ong et al. [ 12 ]. Pico et al. [ 13 ] reported that in Orthopaedic training, Orthopaedic In-Training Examination (OITE) and American Board of Orthopaedic Surgery (ABOS) Part 1 scores were similar between genders, but that female trainees took more attempts in order to pass. In the UK, two studies reported significantly lower Membership of the Royal College of Surgeons (MRCS) pass rates for female trainees compared to males [ 4 , 14 ]. However, Robinson et al. [ 15 ] presented no significant gender differences in MRCS success rates. A study assessing Fellowship of the Royal College of Surgeons (FRCS) examination results found no significant gender disparities in pass rates [ 16 ]. In MRCOG examination, no significant gender differences were found in Part 1 scores, but women had higher pass rates and scores in Part 2 [ 17 ].
Assessment for Progression
ARCP is the annual process of revalidation that UK doctors must perform to progress through training. A satisfactory progress outcome (“outcome 1”) allows trainees to advance through to the next training year, whereas non-satisfactory outcomes (“2–5”) suggest inadequate progress and recommends solutions, such as further time in training or being released from the training programme. Two studies reported that women received 60% more non-satisfactory outcomes than men [ 16 , 18 ]. In contrast, in O&G men had higher non-satisfactory ARCP outcomes without explicit reasons for this given [ 19 ].
Regarding Milestone evaluations based from the US Accreditation Council for Graduate Medical Education (ACGME), Anderson et al. [ 20 ] reported men had higher ratings of knowledge of diseases at postgraduate year 5 (PGY-5), while women had lower mean score achievements. This was similar to another study finding that men and women had similar competencies at PGY-1 to 3, and that it was only at PGY-5 that women were evaluated lower than men [ 21 ]. However, Kwasny et al. [ 22 ] found no difference in trainers’ ratings between genders, but women self-rated themselves lower. Salles et al. [ 23 ] demonstrated significant improvement in scoring in women following a value-affirmation intervention, while this intervention did not affect men.
Workplace-based Assessment
Galvin et al. [ 24 ] reported better evaluation scores from nurses for PGY-2 male trainees, while females received fewer positive and more negative comments. Gerull et al. [ 25 ] demonstrated men received compliments with superlatives or standout words, whereas women were more likely to receive compliments with mitigating phrases (e.g., excellent vs. quite competent).
Hayward et al. [ 26 ] investigated assessment of attributes of clinical performance (ethics, judgement, technical skills, knowledge and interpersonal skills) and found similar scoring between genders.
Several authors have studied autonomy given to trainees in theatre [ 27 , 28 , 29 , 30 , 31 ]. Two groups found no difference in level of granted autonomy between genders but that women rated lower perceived autonomy on self-evaluation [ 27 , 28 ]. Other studies found that assessors consistently gave female trainees lower autonomy ratings, but only in one paper was this replicated in lower performance scores [ 29 , 30 , 31 ].
Padilla et al. [ 32 ] reported no difference in entrustable professional activity assessment (EPA) levels between genders, yet women rated themselves much lower, which they regarded as evidence of imposter syndrome amongst female trainees. Cooney et al. [ 33 ] found that male trainers scored EPAs for women significantly lower than men, while female trainers rated both genders similarly. Conversely, Roshan et al. [ 34 ] found that male assessors were more positive in feedback comments to female trainees than male trainees, whereas they also found that comments from female assessors were comparable for each gender.
Surgical Experience
Gong et al. [ 35 ] found significantly fewer cataract operations were performed by women in ophthalmology residency programmes, which they suggested could be due to trainers being more likely to give cases to male trainees. Female trainees also participated in fewer robotic colorectal procedures, with less operative time on the robotic console afforded [ 36 ]. Similarly, a systematic review highlighted female trainees in various specialties performed fewer cases per week and potentially had limited access to training facilities [ 37 ]. Eruchalu et al. [ 38 ] found that female trainees performed fewer cases, that is, until gender parity was reached, after which case logs were equivalent.
Technical skills
Antonoff et al. [ 39 ] found higher scores for men in coronary anastomosis skills, with women receiving more “fail” assessments. Dill-Macky et al. [ 40 ] analysed laparoscopic skill assessment using blinded videos of trainees and unblinded assessments. While there was no difference in blinded scores between genders, when comparing blinded and unblinded scores individually, assessors were less likely to agree on the scores of women compared to men. However, another study about laparoscopic skills by Skjold-Ødegaard et al. [ 41 ] reported higher performance scores in female residents, particularly when rated by women. The lowest score was shown in male trainees rated by men. While some studies showed disparities in assessment, several studies reported no difference in technical skill assessments (arthroscopic, knot tying, and suturing skills) between genders [ 42 , 43 , 44 , 45 , 46 ].
Several studies investigated trainees’ abilities to complete isolated tasks associated with surgical skills. In laparoscopic tasks, men were initially more skilful in peg transfer and intracorporeal knot tying than women. Following training, the performance was not different between genders [ 47 ]. A study on microsurgical skills reported better initial visual-spatial and perceptual ability in men, while women had better fine motor psychomotor ability. However, these differences were not significant, and all trainees improved significantly after training [ 48 ]. A study by Milam et al. [ 49 ] revealed men performed better in mental rotation tasks and women outperformed in working memory. They hypothesised that female trainees would experience stereotype threat, fear of being reduced to a stereotype, which would impair their performance. They found no evidence of stereotype threat influencing female performance, disproving their hypothesis, a finding supported by Myers et al. [ 50 ].
Ethnicity and country of graduation
Most papers reported ethnicity and country of graduation concurrently, for example grouping trainees as White UK graduates (WUKG), Black and minority ethnicity UK graduates (BME UKG), and international medical graduates (IMG). Therefore, these areas will be addressed together in the following section.
When assessing the likelihood of passing American Board of Surgery (ABS) examinations on first attempt, Yeo et al. [ 51 ] found that White trainees were more likely than non-White. They found that the influence of ethnicity was more significant in the end-of-training certifying exam than in the start-of-training qualifying exam. This finding was corroborated in a study of both the OITE and ABOS certifying exam, suggesting widening inequalities during training [ 52 ].
Two UK-based studies reported significantly higher MRCS pass rates in White trainees compared to BMEs [ 4 , 14 ]. BMEs were less likely to pass MRCS Part A and B, though this was not true for Part A when variations in socioeconomic background were corrected for [ 14 ]. However, Robinson et al. [ 53 ] found no difference in MRCS pass rates based on ethnicity. Another study by Robinson et al. [ 15 ] demonstrated similar pass rates between WUKGs and BME UKGs, but IMGs had significantly lower pass rates than all UKGs. The FRCS pass rates of WUKGs, BME UKGs and IMGs were 76.9%, 52.9%, and 53.9%, respectively, though these percentages were not statistically significantly different [ 16 ].
There was no difference in MRCOG results based on ethnicity, but higher success rates were found in UKGs [ 19 ]. In FRCOphth, WUKGs had a pass rate of 70%, higher than other groups of trainees, with a pass rate of only 45% for White IMGs [ 52 ].
By gathering data from training programmes reporting little to no DA due to ethnicity, Roe et al. [ 54 ] were able to provide a list of factors they felt were protective against DA, such as having supportive supervisors and developing peer networks.
Assessment for progression
RCOphth [ 55 ] found higher rates of satisfactory ARCP outcomes for WUKGs compared to BME UKGs, followed by IMGs. RCOG [ 19 ] discovered higher rates of non-satisfactory ARCP outcomes from non-UK graduates, particularly amongst BMEs and those from the European Economic Area (EEA). Tiffin et al. [ 56 ] considered the difference in experience between UK graduates and UK nationals whose primary medical qualification was gained outside of the UK, and found that the latter were more likely to receive a non-satisfactory ARCP outcome, even when compared to non-UK nationals.
Woolf et al. [ 57 ] explored reasons behind DA by conducting interview studies with trainees. They investigated trainees’ perceptions of fairness in evaluation and found that trainees felt relationships developed with colleagues who gave feedback could affect ARCP results, and might be challenging for BME UKGs and IMGs who have less in common with their trainers.
Workplace-based assessment
Brooks et al. [ 58 ] surveyed the prevalence of microaggressions against Black orthopaedic surgeons during assessment and found 87% of participants experienced some level of racial discrimination during workplace-based performance feedback. Black women reported having more racially focused and devaluing statements from their seniors than men.
Surgical experience
Eruchalu et al. [ 38 ] found that white trainees performed more major surgical cases and more cases as a supervisor than did their BME counterparts.
Dill-Macky et al. [ 40 ] reported no significant difference in laparoscopic surgery assessments between ethnicities.
Individual and family background in education
Two studies [ 4 , 16 ] concentrated on educational background, considering factors such as parental occupation and attendance of a fee-paying school. MRCS part A pass rate was significantly higher for trainees for whom Medicine was their first Degree, those with university-educated parents, higher POLAR (Participation In Local Areas classification group) quintile, and those from fee-paying schools. Higher part B pass rate was associated with graduating from non-Graduate Entry Medicine programmes and parents with managerial or professional occupations [ 4 ]. Trainees with higher degrees were associated with an almost fivefold increase in FRCS success and seven times more scientific publications than their counterparts [ 16 ].
Socioeconomic background
Two studies used Index of Multiple Deprivation quintile, the official measure of relative deprivation in England based on geographical areas for grading socioeconomic level. The area was defined at the time of medical school application. Deprivation quintiles (DQ) were calculated, ranging from DQ1 (most deprived) to DQ5 (least deprived) [ 4 , 14 ].
Trainees with history of less deprivation were associated with higher MRCS part A pass rate. More success in part B was associated with history of no requirement for income support and less deprived areas [ 4 ]. Trainees from DQ1 and DQ2 had lower pass rates and higher number of attempts to pass [ 14 ]. A general trend of better outcomes in examination was found from O&G trainees in less deprived quintiles [ 19 ].
Trainees from DQ1 and DQ2 received significantly more non-satisfactory ARCP outcomes (24.4%) than DQ4 and DQ5 (14.2%) [ 14 ].
Trainees who graduated at age less than 29 years old were more likely to pass MRCS than their counterparts [ 4 ].
Authors [ 18 , 56 ] found that older trainees received more non-satisfactory ARCP outcomes. Likewise, there was higher percentage of non-satisfactory ARCP outcomes in O&G trainees aged over 45 compared with those aged 25–29 regardless of gender [ 19 ].
Trainees with disability had significantly lower pass rates in MRCS part A compared to candidates without disability. However, the difference was not significant for part B [ 59 ].
What have we learnt from the literature?
It is heartening to note the recent increase in interest in DA (27 studies in the last 4 years, compared to 26 in the preceding 40) (Fig. 2 ). The vast majority (77%) of studies are quantitative, based in the US or UK (89%), focus on gender (85%) and relate to clinical assessments (51%) rather than examination results. Therefore, the surgical community has invested primarily in researching the experience of women in the USA and UK.
Interestingly, a report by RCOG [ 19 ] showed that men were more likely to receive non-satisfactory ARCP outcomes than women, and a study by Rushd et al. [ 17 ] found that women were more likely to pass part 2 of MRCOG than men. This may be because within O&G men are the “out-group” (a social group or category characterised by marginalisation or exclusion by the dominant cultural group) as 75% of O&G trainees are female [ 60 ].
This contrasts with other specialities in which men are the in-group and women are seen to underperform. Outside of O&G, in comparison to men, women are less likely to pass MRCS [ 4 , 14 ], receive satisfactory ARCP outcome [ 16 , 18 ], or receive positive feedback [ 24 ], whilst not performing the same number of procedures as men [ 34 , 35 ]. This often leads to poor self-confidence in women [ 32 ], which can then worsen performance [ 21 ].
It proves difficult to comment on DA for many groups due to a lack of evidence. The current research suggests that being older, having a disability, graduate entry to medicine, low parental education, and living in a lower socioeconomic area at the time of entering medical school are all associated with lower MRCS pass rates. Being older and having a lower socioeconomic background are also associated with non-satisfactory ARCP outcomes, slowing progression through training.
These characteristics may provide a compounding negative effect – for example having a previous degree will automatically make a trainee older, and living in a lower socioeconomic area makes it more likely their parents will have a non-professional job and not hold a higher degree. When multiple protected characteristics interact to produce a compounded negative effect for a person, it is often referred to as “intersectional discrimination” or “intersectionality” [ 61 ]. This is a concept which remains underrepresented in the current literature.
The literature is not yet in agreement over the presence of DA due to ethnicity. There are many studies that report perceived discrimination, however the data for exam and clinical assessment outcomes is equivocal. This may be due to the fluctuating nature of in-groups and out-groups, and multiple intersecting characteristics. Despite this, the lived experience of BME surgeons should not be ignored and requires further investigation.
What are the gaps in the literature?
The overwhelming majority of literature exploring DA addresses issues of gender, ethnicity or country of medical qualification. Whilst bias related to these characteristics is crucial to recognise, studies into other protected characteristics are few and far between. The only paper on disability reported striking differences in attainment between disabled and non-disabled registrars [ 59 ]. There has also been increased awareness about neurodiversity amongst doctors and yet an exploration into the experience of neurodiverse surgeons and their progress through training has yet to be published [ 62 ].
The implications of being LGBTQ + in surgical training have not been recognised nor formally addressed in the literature. Promisingly, the experiences of LGBTQ + medical students have been recognised at an undergraduate level, so one can hope that this will be translated into postgraduate education [ 63 , 64 ]. While this is deeply entwined with experiences of gender discrimination, it is an important characteristic that the surgical community would benefit from addressing, along with disability. To a lesser extent, the effect of socioeconomic background and age have also been overlooked.
Characterising trainees for the purpose of research
Ethnicity is deeply personal, self-defined, and may change over time as personal identity evolves, and therefore arbitrarily grouping diverse ethnic backgrounds is unlikely to capture an accurate representation of experiences. There are levels of discrimination even within minority groups; colourism in India means dark-skinned Indians will experience more discrimination than light-skinned Indians, even from those within in their own ethnic group [ 65 ]. Therefore, although the studies included in the scoping review accepted self-definitions of ethnicity, this is likely not enough to fully capture the nuances of bias and discrimination present in society. For example, Ellis et al. [ 4 ] grouped participants as “White”, “Mixed”, “Asian”, “Black” and “Other”, however they could have also assigned a skin tone value such as the NIS Skin Colour Scale [ 66 ], thus providing more detail.
Ethnicity is more than genetic heritage; it is also cultural expression. The experience of an IMG in UK postgraduate training will differ from that of a UKG, an Indian UKG who grew up in India, and an Indian UKG who grew up in the UK. These are important distinctions which are noted in the literature (e.g. by Woolf et al., 2016 [ 57 ]) however some do not distinguish between ethnicity and graduate status [ 15 ] and none delve into an individual’s cultural expression (e.g., clothing choice) and how this affects the perception of their assessors.
Reasons for DA
Despite the recognition of inequalities in all specialties of surgery, there is a paucity of data explicitly addressing why DA occurs. Reasons behind the phenomenon must be explored to enable change and eliminate biases. Qualitative research is more attuned to capturing the complexities of DA through observation or interview-based studies. Currently most published data is quantitative, and relies on performance metrics to demonstrate the presence of DA while ignoring the causes. Promisingly, there are a gradually increasing number of qualitative, predominantly interview-based, studies (Fig. 2 ).
To create a map of DA in all its guises, an analysis of the themes reported to be contributory to its development is helpful. In our review of the literature, four themes have been identified:
Training culture
In higher surgical training, for there to be equality in outcomes, there needs to be equity in opportunities. Ellis et al. [ 4 ] recognised that variation in training experiences, such as accessibility of supportive peers and senior role models, can have implications on attainment. Trainees would benefit from targeted support at times of transition, such as induction or at examinations, and it may be that currently the needs of certain groups are being met before others, reinforcing differential attainment [ 4 ].
Experience of assessment
Most literature in DA relates to the presence (or lack of) an attainment gap in assessments, such as ARCP or MRCS. It is assumed that these assessments of trainee development are objective and free of bias, and indeed several authors have described a lack of bias in these high-stakes examinations (e.g., Ong et al., 2019 [ 12 ]; Robinson et al., 2019 [ 53 ]). However, in some populations, such as disabled trainees, there are differences in attainment [ 59 ]. This is demonstrated despite legislation requiring professional bodies to make reasonable adjustments to examinations for disabled candidates, such as additional time, text formatting amendments, or wheelchair-accessible venues [ 67 ]. Therefore it would be beneficial to investigate the implementation of these adjustments across higher surgical examinations and identify any deficits.
Social networks
Relationships between colleagues may influence DA in multiple ways. Several studies identified that a lack of a relatable and inspiring mentor may explain why female or BME doctors fail to excel in surgery [ 4 , 55 ]. Certain groups may receive preferential treatment due to their perceived familiarity to seniors [ 35 ]. Robinson et al. [ 15 ] recognised that peer-to-peer relationships were also implicated in professional development, and the lack thereof could lead to poor learning outcomes. Therefore, a non-discriminatory culture and inclusion of trainees within the social network of training is posited as beneficial.
Personal characteristics
Finally, personal factors directly related to protected characteristics have been suggested as a cause of DA. For example, IMGs may perform worse in examinations due to language barriers, and those from disadvantaged backgrounds may have less opportunity to attend expensive courses [ 14 , 16 ]. Although it is impossible to exclude these innate deficits from training, we may mitigate their influence by recognising their presence and providing solutions.
The causes of DA may also be grouped into three levels, as described by Regan de Bere et al. [ 68 ]: macro (the implications of high-level policy), meso (focusing on institutional or working environments) and micro (the influence of individual factors). This can intersect with the four themes identified above, as training culture can be enshrined at both an institutional and individual level, influencing decisions that relate to opportunities for trainees, or at a macro level, such as in the decisions made on nationwide recruitment processes. These three levels can be used to more deeply explore each of the four themes to enrich the discovery of causes of DA.
Discussions outside of surgery
Authors in General Practice (e.g., Unwin et al., 2019 [ 69 ]; Pattinson et al., 2019 [ 70 ]), postgraduate medical training (e.g., Andrews, Chartash, and Hay, 2021 [ 71 ]), and undergraduate medical education (e.g., Yeates et al., 2017 [ 72 ]; Woolf et al., 2013 [ 73 ]) have published more extensively in the aetiology of DA. A study by Hope et al. [ 74 ] evaluating the bias present in MRCP exams used differential item functioning to identify individual questions which demonstrated an attainment gap between male and female and Caucasian and non-Caucasian medical trainees. Conclusions drawn about MRCP Part 1 examinations may be generalisable to MRCS Part A or FRCOphth Part 1: they are all multiple-choice examinations testing applied basic science and usually taken within the first few years of postgraduate training. Therefore it is advisable that differential item functioning should also be applied to these examinations. However, it is possible that findings in some subspecialities may not be generalisable to others, as training environments can vary profoundly. The RCOphth [ 55 ] reported that in 2021, 53% of ophthalmic trainees identified as male, whereas in Orthopaedics 85% identified as male, suggesting different training environments [ 5 ]. It is useful to identify commonalities of DA between surgical specialties and in the wider scope of medical training.
Limitations of our paper
Firstly, whilst aiming to provide a review focussed on the experience of surgical trainees, four papers contained data about either non-surgical trainees or medical students. It is difficult to draw out the surgeons from this data and therefore it is possible that there are issues with generalisability. Furthermore, we did not consider the background of each paper’s authors, as their own lived experience of attainment gap could form the lens through which they commented on surgical education, colouring their interpretation. Despite intending to include as many protected characteristics as possible, inevitably there will be lived experiences missed. Lastly, the experience of surgical trainees outside of the English-speaking world were omitted. No studies were found that originated outside of Europe or North America and therefore the presence or characteristics of DA outside of this area cannot be assumed.
Experiences of inequality in surgical assessment are prevalent in all surgical subspecialities. In order to further investigate DA, researchers should ensure all protected characteristics are considered - and how these interact - to gain insight into intersectionality. Given the paucity of current evidence, particular focus should be given to the implications of disability, and specifically neurodiversity, in progress through training as they are yet to be explored in depth. In defining protected characteristics, future authors should be explicit and should avoid generalisation of cultural backgrounds to allow authentic appreciation of attainment gap. Few authors have considered the driving forces between bias in assessment and DA, and therefore qualitative studies should be prioritised to uncover causes for and protective factors against DA. Once these influences have been identified, educational designers can develop new assessment methods that ensure equity across surgical trainees.
Data availability
All data provided during this study are included in the supplementary information files.
Abbreviations
Accreditation Council for Graduate Medical Education
American Board of Orthopaedic Surgery
American Board of Surgery
American Board of Surgery Certifying Exam
Annual Review of Competence Progression
Black, Asian, and Minority Ethnicity
Council on Resident Education in Obstetrics and Gynecology
Differential Attainment
Deprivation Quintile
European Economic Area
Entrustable Professional Activities
Fellowship of The Royal College of Ophthalmologists
Fellow of the Royal College of Surgeons
General Medical Council
Higher Surgical Training
International Medical Graduate
In-Training Evaluation Report
Member of the Royal College of Obstetricians and Gynaecologists
Member of the Royal College of Physicians
Member of the Royal College of Surgeons
Obstetrics and Gynaecology
Orthopaedic In-Training Examination
Participation In Local Areas
Postgraduate Year
The Royal College of Ophthalmologists
The Royal College of Obstetricians and Gynaecologists
The Royal College of Surgeons of England
United Kingdom Graduate
White United Kingdom Graduate
Joseph JP, Joseph AO, Jayanthi NVG, et al. BAME Underrepresentation in Surgery Leadership in the UK and Ireland in 2020: An Uncomfortable Truth. The Bulletin of the Royal College of Surgeons of England. 2020; 102 (6): 232–33.
Royal College of Surgeons of England. The Royal College – Our Professional Home. An independent review on diversity and inclusion for the Royal College of Surgeons of England. Review conducted by Baroness Helena Kennedy QC. RCS England. 2021.
Sarafidou K, Greatorex R. Surgical workforce: planning today for the workforce of the future. Bull Royal Coll Surg Engl. 2011;93(2):48–9. https://doi.org/10.1308/147363511X552575 .
Article Google Scholar
Ellis R, Brennan P, Lee AJ, et al. Differential attainment at MRCS according to gender, ethnicity, age and socioeconomic factors: a retrospective cohort study. J R Soc Med. 2022;115(7):257–72. https://doi.org/10.1177/01410768221079018 .
Hope C, Humes D, Griffiths G, et al. Personal Characteristics Associated with Progression in Trauma and Orthopaedic Specialty Training: A Longitudinal Cohort Study.Journal of Surgical Education 2022; 79 (1): 253–59. doi:10.1016/j.jsurg.2021.06.027.
Takeshita J, Wang S, Loren AW, et al. Association of Racial/Ethnic and Gender Concordance Between Patients and Physicians With Patient Experience Ratings. JAMA Network Open. 2022; 3(11). doi:10.1001/jamanetworkopen.2020.24583.
Katz, P. The Scalpel’s Edge: The Culture of Surgeons. Allyn and Bacon, 1999.
Tørring B, Gittell JH, Laursen M, et al. (2019) Communication and relationship dynamics in surgical teams in the operating room: an ethnographic study. BMC Health Services Research. 2019;19, 528. doi:10.1186/s12913-019-4362-0.
Veazey Brooks J & Bosk CL. (2012) Remaking surgical socialization: work hour restrictions, rites of passage, and occupational identity. Social Science & Medicine. 2012;75(9):1625-32. doi: 10.1016/j.socscimed.2012.07.007.
Arksey H & OʼMalley L. Scoping studies: Towards a methodological framework. International Journal of Social Research Methodology. 2005;8(1), 19–32.
Maker VK, Marco MZ, Dana V, et al. Can We Predict Which Residents Are Going to Pass/Fail the Oral Boards? Journal of Surgical Education. 2012;69 (6): 705–13.
Ong TQ, Kopp JP, Jones AT, et al. Is there gender Bias on the American Board of Surgery general surgery certifying examination? J Surg Res. 2019;237:131–5. https://doi.org/10.1016/j.jss.2018.06.014 .
Pico K, Gioe TJ, Vanheest A, et al. Do men outperform women during orthopaedic residency training? Clin Orthop Relat Res. 2010;468(7):1804–8. https://doi.org/10.1007/s11999-010-1318-4 .
Vinnicombe Z, Little M, Super J, et al. Differential attainment, socioeconomic factors and surgical training. Ann R Coll Surg Engl. 2022;104(8):577–82. https://doi.org/10.1308/rcsann.2021.0255 .
Robinson DBT, Hopkins L, James OP, et al. Egalitarianism in surgical training: let equity prevail. Postgraduate Medical Journal. 2020;96 (1141), 650–654. doi:10.1136/postgradmedj-2020-137563.
Luton OW, Mellor K, Robinson DBT, et al. Differential attainment in higher surgical training: scoping pan-specialty spectra. Postgraduate Medical Journal. 2022;99(1174),849–854. doi:10.1136/postgradmedj-2022-141638.
Rushd S, Landau AB, Khan JA, Allgar V & Lindow SW. An analysis of the performance of UK medical graduates in the MRCOG Part 1 and Part 2 written examinations. Postgraduate Medical Journal. 2012;88 (1039), 249–254. doi:10.1136/postgradmedj-2011-130479.
Hope C, Lund J, Griffiths G, et al. Differences in ARCP outcome by surgical specialty: a longitudinal cohort study. Br J Surg. 2021;108. https://doi.org/10.1093/bjs/znab282.051 .
Royal College of Obstetricians and Gynaecologists. Report Differential Attainment 2019. https://www.rcog.org.uk/media/jscgfgwr/differential-attainment-tef-report-2019.pdf [Last accessed 28/12/23].
Anderson JE, Zern NK, Calhoun KE, et al. Assessment of Potential Gender Bias in General Surgery Resident Milestone Evaluations. JAMA Surgery. 2022;157 (12), 1164–1166. doi:10.1001/jamasurg.2022.3929.
Landau SI, Syvyk S, Wirtalla C, et al. Trainee Sex and Accreditation Council for Graduate Medical Education Milestone Assessments during general surgery residency. JAMA Surg. 2021;156(10):925–31. https://doi.org/10.1001/jamasurg.2021.3005 .
Kwasny L, Shebrain S, Munene G, et al. Is there a gender bias in milestones evaluations in general surgery residency training? Am J Surg. 2021;221(3):505–8. https://doi.org/10.1016/j.amjsurg.2020.12.020 .
Salles A, Mueller CM & Cohen GL. A Values Affirmation Intervention to Improve Female Residents’ Surgical Performance. Journal of Graduate Medical Education. 2016;8 (3), 378–383. doi:10.4300/JGME-D-15-00214.1.
Galvin S, Parlier A, Martino E, et al. Gender Bias in nurse evaluations of residents in Obstetrics and Gynecology. Obstet Gynecol. 2015;126(7S–12S). https://doi.org/10.1097/AOG.0000000000001044 .
Gerull KM, Loe M, Seiler K, et al. Assessing gender bias in qualitative evaluations of surgical residents. Am J Surg. 2019;217(2):306–13. https://doi.org/10.1016/j.amjsurg.2018.09.029 .
Hayward CZ, Sachdeva A, Clarke JR. Is there gender bias in the evaluation of surgical residents? Surgery. 1987;102(2):297–9.
Google Scholar
Cookenmaster C, Shebrain S, Vos D, et al. Gender perception bias of operative autonomy evaluations among residents and faculty in general surgery training. Am J Surg. 2021;221(3):515–20. https://doi.org/10.1016/j.amjsurg.2020.11.016 .
Olumolade OO, Rollins PD, Daignault-Newton S, et al. Closing the Gap: Evaluation of Gender Disparities in Urology Resident Operative Autonomy and Performance.Journal of Surgical Education.2022;79 (2), 524–530. doi.org/10.1016/j.jsurg.2021.10.010.
Chen JX, Chang EH, Deng F, et al. Autonomy in the Operating Room: A Multicenter Study of Gender Disparities During Surgical Training. Journal of Graduate Medical Education. 2021;13(5), 666–672. doi: 10.4300/JGME-D-21-00217.1.
Meyerson SL, Sternbach JM, Zwischenberger JB, & Bender EM. The Effect of Gender on Resident Autonomy in the Operating room. Journal of Surgical Education. 2017. 74(6), e111–e118. doi.org/10.1016/j.jsurg.2017.06.014.
Hoops H, Heston A, Dewey E, et al. Resident autonomy in the operating room: Does gender matter? The AmericanJournalofSurgery. 2019; 217(2), 301–305. doi.org/10.1016/j.amjsurg.2018.12.023.
Padilla EP, Stahl CC, Jung SA, et al. Gender Differences in Entrustable Professional Activity Evaluations of General Surgery Residents. Annals of Surgery. 2022;275 (2), 222–229. doi:10.1097/SLA.0000000000004905.
Cooney CM, Aravind P, Hultman CS, et al. An Analysis of Gender Bias in Plastic Surgery Resident Assessment. Journal of Graduate Medical Education. 2021;13 (4), 500–506. doi:10.4300/JGME-D-20-01394.1.
Roshan A, Farooq A, Acai A, et al. The effect of gender dyads on the quality of narrative assessments of general surgery trainees. The American Journal of Surgery. 2022; 224 (1A), 179–184. doi.org/10.1016/j.amjsurg.2021.12.001.
Gong D, Winn BJ, Beal CJ, et al. Gender Differences in Case Volume Among Ophthalmology Residents. Archives of Ophthalmology. 2019;137 (9), 1015–1020. doi:10.1001/jamaophthalmol.2019.2427.
Foley KE, Izquierdo KM, von Muchow MG, et al. Colon and Rectal Surgery Robotic Training Programs: An Evaluation of Gender Disparities. Diseases of the Colon and Rectum. 2020; 63(7), 974–979. doi.org/10.1097/DCR.0000000000001625.
Ali A, Subhi Y, Ringsted C et al. Gender differences in the acquisition of surgical skills: a systematic review. Surgical Endoscopy. 2015;29 (11), 3065–3073. doi:10.1007/s00464-015-4092-2.
Eruchalu CN, He K, Etheridge JC, et al. Gender and Racial/Ethnic Disparities in Operative Volumes of Graduating General Surgery Residents.The Journal of Surgical Research. 2022; 279, 104–112. doi.org/10.1016/j.jss.2022.05.020.
Antonoff MB, Feldman H, Luc JGY, et al. Gender Bias in the Evaluation of Surgical Performance: Results of a Prospective Randomized Trial. Annals of Surgery. 2023;277 (2), 206–213. doi:10.1097/SLA.0000000000005015.
Dill-Macky A, Hsu C, Neumayer LA, et al. The Role of Implicit Bias in Surgical Resident Evaluations. Journal of Surgical Education. 2022;79 (3), 761–768. doi:10.1016/j.jsurg.2021.12.003.
Skjold-Ødegaard B, Ersdal HL, Assmus J et al. Comparison of Performance Score for Female and Male Residents in General Surgery Doing Supervised Real-Life Laparoscopic Appendectomy: Is There a Norse Shield-Maiden Effect? World Journal of Surgery. 2021;45 (4), 997–1005. doi:10.1007/s00268-020-05921-4.
Leape CP, Hawken JB, Geng X, et al. An investigation into gender bias in the evaluation of orthopedic trainee arthroscopic skills. Journal of Shoulder and Elbow Surgery. 2022;31 (11), 2402–2409. doi:10.1016/j.jse.2022.05.024.
Vogt VY, Givens VM, Keathley CA, et al. Is a resident’s score on a videotaped objective structured assessment of technical skills affected by revealing the resident’s identity? American Journal of Obstetrics and Gynecology. 2023;189 (3), 688–691. doi:10.1067/S0002-9378(03)00887-1.
Fjørtoft K, Konge L, Christensen J et al. Overcoming Gender Bias in Assessment of Surgical Skills. Journal of Surgical Education. 2022;79 (3), 753–760. doi:10.1016/j.jsurg.2022.01.006.
Grantcharov TP, Bardram L, Funch-Jensen P, et al. Impact of Hand Dominance, Gender, and Experience with Computer Games on Performance in Virtual Reality Laparoscopy. Surgical Endoscopy 2003;17 (7): 1082–85.
Rosser Jr JC, Rosser LE & Savalgi RS. Objective Evaluation of a Laparoscopic Surgical Skill Program for Residents and Senior Surgeons. Archives of Surgery. 1998; 133 (6): 657–61.
White MT & Welch K. Does gender predict performance of novices undergoing Fundamentals of Laparoscopic Surgery (FLS) training? The American Journal of Surgery. 2012;203 (3), 397–400. doi:10.1016/j.amjsurg.2011.09.020.
Nugent E, Joyce C, Perez-Abadia G, et al. Factors influencing microsurgical skill acquisition during a dedicated training course. Microsurgery. 2012;32 (8), 649–656. doi:10.1002/micr.22047.
Milam LA, Cohen GL, Mueller C et al. Stereotype threat and working memory among surgical residents. The American Journal of Surgery. 2018;216 (4), 824–829. doi:10.1016/j.amjsurg.2018.07.064.
Myers SP, Dasari M, Brown JB, et al. Effects of Gender Bias and Stereotypes in Surgical Training: A Randomized Clinical Trial. JAMA Surgery. 2020; 155(7), 552–560. doi.org/10.1001/jamasurg.2020.1127.
Yeo HL, Patrick TD, Jialin M, et al. Association of Demographic and Program Factors With American Board of Surgery Qualifying and Certifying Examinations Pass Rates. JAMA Surgery 2020; 155 (1): 22–30. doi:0.1001/jamasurg.2019.4081.
Foster N, Meghan P, Bettger JP, et al. Objective Test Scores Throughout Orthopedic Surgery Residency Suggest Disparities in Training Experience. Journal of Surgical Education 2021;78 (5): 1400–1405. doi:10.1016/j.jsurg.2021.01.003.
Robinson DBT, Hopkins L, Brown C, et al. Prognostic Significance of Ethnicity on Differential Attainment in Core Surgical Training (CST). Journal of the American College of Surgeons. 2019;229 (4), e191. doi:10.1016/j.jamcollsurg.2019.08.1254.
Roe V, Patterson F, Kerrin M, et al. What supported your success in training? A qualitative exploration of the factors associated with an absence of an ethnic attainment gap in post-graduate specialty training. General Medical Council. 2019. https://www.gmc-uk.org/-/media/documents/gmc-da-final-report-success-factors-in-training-211119_pdf-80914221.pdf [Last accessed 28/12/23].
Royal College of Ophthalmologists. Data on Differential attainment in ophthalmology and monitoring equality, diversity, and inclusion: Recommendations to the RCOphth. London, Royal College of Ophthalmologists. 2022. https://www.rcophth.ac.uk/wp-content/uploads/2023/01/Differential-Attainment-Report-2022.pdf [Last accessed 28/12/23].
Tiffin PA, Orr J, Paton LW, et al. UK nationals who received their medical degrees abroad: selection into, and subsequent performance in postgraduate training: a national data linkage study. BMJ Open. 2018;8:e023060. doi: 10.1136/bmjopen-2018-023060.
Woolf K, Rich A, Viney R, et al. Perceived causes of differential attainment in UK postgraduate medical training: a national qualitative study. BMJ Open. 2016;6 (11), e013429. doi:10.1136/bmjopen-2016-013429.
Brooks JT, Porter SE, Middleton KK, et al. The Majority of Black Orthopaedic Surgeons Report Experiencing Racial Microaggressions During Their Residency Training. Clinical Orthopaedics and Related Research. 2023;481 (4), 675–686. doi:10.1097/CORR.0000000000002455.
Ellis R, Cleland J, Scrimgeour D, et al. The impact of disability on performance in a high-stakes postgraduate surgical examination: a retrospective cohort study. Journal of the Royal Society of Medicine. 2022;115 (2), 58–68. doi:10.1177/01410768211032573.
Royal College of Obstetricians & Gynaecologists. RCOGWorkforceReport2022. Available at: https://www.rcog.org.uk/media/fdtlufuh/workforce-report-july-2022-update.pdf [Last accessed 28/12/23].
Crenshaw KW. On Intersectionality: Essential Writings. Faculty Books. 2017; 255.
Brennan CM & Harrison W. The Dyslexic Surgeon. The Bulletin of the Royal College of Surgeons of England. 2020;102 (3): 72–75. doi:10.1308/rcsbull.2020.72.
Toman L. Navigating medical culture and LGBTQ identity. Clinical Teacher. 2019;16: 335–338. doi:10.1111/tct.13078.
Torales J, Castaldelli-Maia JM & Ventriglio A. LGBT + medical students and disclosure of their sexual orientation: more than in and out of the closet. International Review of Psychiatry. 2022;34:3–4, 402–406. doi:10.1080/09540261.2022.2101881.
Guda VA & Kundu RV. India’s Fair Skin Phenomena. SKINmed. 2021;19(3), 177–178.
Massey D & Martin JA. The NIS skin color scale. Princeton University Press. 2003.
Intercollegiate Committee for Basic Surgical Examinations.AccessArrangementsandReasonableAdjustmentsPolicyforCandidateswithaDisabilityorSpecificLearningdifficulty. 2020. https://www.intercollegiatemrcsexams.org.uk/-/media/files/imrcs/mrcs/mrcs-regulations/access-arrangements-and-reasonable-adjustments-january-2020.pdf [Last accessed 28/12/23].
Regan de Bere S, Nunn S & Nasser M. Understanding differential attainment across medical training pathways: A rapid review of the literature. General Medical Council. 2015. https://www.gmc-uk.org/-/media/documents/gmc-understanding-differential-attainment_pdf-63533431.pdf [Last accessed 28/12/23].
Unwin E, Woolf K, Dacre J, et al. Sex Differences in Fitness to Practise Test Scores: A Cohort Study of GPs. The British Journal of General Practice: The Journal of the Royal College of General Practitioners. 2019; 69 (681): e287–93. doi:10.3399/bjgp19X701789.
Pattinson J, Blow C, Sinha B et al. Exploring Reasons for Differences in Performance between UK and International Medical Graduates in the Membership of the Royal College of General Practitioners Applied Knowledge Test: A Cognitive Interview Study. BMJ Open. 2019;9 (5): e030341. doi:10.1136/bmjopen-2019-030341.
Andrews J, Chartash D & Hay S. Gender Bias in Resident Evaluations: Natural Language Processing and Competency Evaluation. Medical Education. 2021;55 (12): 1383–87. doi:10.1111/medu.14593.
Yeates P, Woolf K, Benbow E, et al. A Randomised Trial of the Influence of Racial Stereotype Bias on Examiners’ Scores, Feedback and Recollections in Undergraduate Clinical Exams. BMC Medicine 2017;15 (1): 179. doi:10.1186/s12916-017-0943-0.
Woolf K, McManus IC, Potts HWW et al. The Mediators of Minority Ethnic Underperformance in Final Medical School Examinations. British Journal of Educational Psychology. 2013; 83 (1): 135–59. doi:10.1111/j.2044-8279.2011.02060.x.
Hope D, Adamson K, McManus IC, et al. Using Differential Item Functioning to Evaluate Potential Bias in a High Stakes Postgraduate Knowledge Based Assessment. BMC Medical Education. 2018;18 (1): 64. doi:10.1186/s12909-018-1143-0.
Download references
No sources of funding to be declared.
Author information
Authors and affiliations.
Department of Surgery and Cancer, Imperial College London, London, UK
Rebecca L. Jones, Suwimol Prusmetikul & Sarah Whitehorn
Department of Ophthalmology, Cheltenham General Hospital, Gloucestershire Hospitals NHS Foundation Trust, Alexandra House, Sandford Road, Cheltenham, GL53 7AN, UK
Rebecca L. Jones
Department of Orthopaedics, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Suwimol Prusmetikul
You can also search for this author in PubMed Google Scholar
Contributions
RJ, SP and SW conceived the study. RJ carried out the search. RJ, SP and SW reviewed and appraised articles. RJ, SP and SW extracted data and synthesized results from articles. RJ, SP and SW prepared the original draft of the manuscript. RJ and SP prepared Figs. 1 and 2. All authors reviewed and edited the manuscript and agreed to the final version.
Corresponding author
Correspondence to Rebecca L. Jones .
Ethics declarations
Ethics approval and consent to participate.
Not required for this scoping review.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary material 2, rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Jones, R.L., Prusmetikul, S. & Whitehorn, S. Differential attainment in assessment of postgraduate surgical trainees: a scoping review. BMC Med Educ 24 , 597 (2024). https://doi.org/10.1186/s12909-024-05580-2
Download citation
Received : 27 February 2024
Accepted : 20 May 2024
Published : 30 May 2024
DOI : https://doi.org/10.1186/s12909-024-05580-2
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Differential attainment
- Postgraduate
BMC Medical Education
ISSN: 1472-6920
- Submission enquiries: [email protected]
- General enquiries: [email protected]
Log in using your username and password
- Search More Search for this keyword Advanced search
- Latest content
- Current issue
- For authors
- New editors
- BMJ Journals More You are viewing from: Google Indexer
You are here
- Volume 58, Issue 11
- Strength, power and aerobic capacity of transgender athletes: a cross-sectional study
- Article Text
- Article info
- Citation Tools
- Rapid Responses
- Article metrics
- http://orcid.org/0000-0001-7412-1188 Blair Hamilton 1 , 2 ,
- http://orcid.org/0009-0005-9553-3081 Andrew Brown 2 ,
- http://orcid.org/0009-0007-0957-5002 Stephanie Montagner-Moraes 2 ,
- http://orcid.org/0000-0001-9483-3262 Cristina Comeras-Chueca 3 ,
- http://orcid.org/0000-0001-8609-2812 Peter G Bush 2 ,
- http://orcid.org/0000-0002-8526-9169 Fergus M Guppy 4 ,
- http://orcid.org/0000-0001-6210-2449 Yannis P Pitsiladis 5 , 6
- 1 School of Sport and Health Sciences , University of Brighton , Brighton , UK
- 2 School of Applied Sciences University , Brighton , UK
- 3 Health Sciences Faculty , Universidad San Jorge , Zaragoza , Spain
- 4 Heriot-Watt University , Edinburgh , UK
- 5 Department of Movement, Human and Health Sciences , University of Rome ‘Foro Italico’ , Rome , Italy
- 6 Department of Sport, Physical Education and Health , Hong Kong Baptist University , Hong Kong , Hong Kong SAR
- Correspondence to Professor Yannis P Pitsiladis, Department of Sport, Physical Education and Health, Hong Kong Baptist University, Hong Kong, Hong Kong SAR; ypitsiladis{at}hkbu.edu.hk
Objective The primary objective of this cross-sectional study was to compare standard laboratory performance metrics of transgender athletes to cisgender athletes.
Methods 19 cisgender men (CM) (mean±SD, age: 37±9 years), 12 transgender men (TM) (age: 34±7 years), 23 transgender women (TW) (age: 34±10 years) and 21 cisgender women (CW) (age: 30±9 years) underwent a series of standard laboratory performance tests, including body composition, lung function, cardiopulmonary exercise testing, strength and lower body power. Haemoglobin concentration in capillary blood and testosterone and oestradiol in serum were also measured.
Results In this cohort of athletes, TW had similar testosterone concentration (TW 0.7±0.5 nmol/L, CW 0.9±0.4 nmol/), higher oestrogen (TW 742.4±801.9 pmol/L, CW 336.0±266.3 pmol/L, p=0.045), higher absolute handgrip strength (TW 40.7±6.8 kg, CW 34.2±3.7 kg, p=0.01), lower forced expiratory volume in 1 s:forced vital capacity ratio (TW 0.83±0.07, CW 0.88±0.04, p=0.04), lower relative jump height (TW 0.7±0.2 cm/kg; CW 1.0±0.2 cm/kg, p<0.001) and lower relative V̇O 2 max (TW 45.1±13.3 mL/kg/min/, CW 54.1±6.0 mL/kg/min, p<0.001) compared with CW athletes. TM had similar testosterone concentration (TM 20.5±5.8 nmol/L, CM 24.8±12.3 nmol/L), lower absolute hand grip strength (TM 38.8±7.5 kg, CM 45.7±6.9 kg, p = 0.03) and lower absolute V̇O 2 max (TM 3635±644 mL/min, CM 4467±641 mL/min p = 0.002) than CM.
Conclusion While longitudinal transitioning studies of transgender athletes are urgently needed, these results should caution against precautionary bans and sport eligibility exclusions that are not based on sport-specific (or sport-relevant) research.
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/ .
https://doi.org/10.1136/bjsports-2023-108029
Statistics from Altmetric.com
Request permissions.
If you wish to reuse any or all of this article please use the link below which will take you to the Copyright Clearance Center’s RightsLink service. You will be able to get a quick price and instant permission to reuse the content in many different ways.
WHAT IS ALREADY KNOWN ON THIS TOPIC
There is currently a lack of laboratory data on strength, power and V̇O 2 max from transgender athlete populations.
WHAT THIS STUDY ADDS
This research compares laboratory measures of strength, power and V̇O 2 max of transgender male and female athletes to their cisgender counterparts.
Transgender women athletes demonstrated lower performance than cisgender women in the metrics of forced expiratory volume in 1 s:forced vital capacity ratio, jump height and relative V̇O 2 max.
Transgender women athletes demonstrated higher absolute handgrip strength than cisgender women, with no difference found relative to fat-free mass or hand size.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE, OR POLICY
This study provides sport governing bodies with laboratory-based performance-related data from transgender athletes.
Longitudinal studies are needed to confirm if these results are a direct result of gender affirmation hormone therapy.
Sports-specific studies are necessary to inform policy-making.
Introduction
Transgender athletes can experience conflict between the gender that they were assigned and their experienced gender. 1 The question of integrating transgender athletes into their affirmed gender categories is becoming more prominent, with sports’ governing bodies using varied approaches, from bans on transgender women in the female category 2 requiring the reduction of testosterone in the female category for some time 3 to self-identification into the athletes chosen category. 4
As part of gender affirmation hormone therapy (GAHT), some transgender women undergo testosterone suppression (target ≤1.8 nmol/L 5 ) coupled with oestrogen supplementation (target 400–600 pmol/L 5 ), while some transgender men undergo testosterone supplementation (National Health Service (NHS, UK) target 15–20 nmol/L, 6 Endocrine Society Target 11–34.7 nmol/L 7 ). Testosterone is known to impact sporting performances, with differences in circulating testosterone concentration between cisgender men (CM) and women proposed to explain most of the laboratory-measured differences in sports performance. 8 9 GAHT of transgender men and women alters the body composition of transgender athletes via testosterone-mediated effects on fat-free mass 8 and oestrogens on subcutaneous fat distribution 9 and maintenance of muscle mass. 10 An often-held assumption against transgender women athletes competing in the female category of sport is that transgender women have benefited from a high testosterone concentration from assigned male-at-birth puberty until the administration of GAHT that cannot be mitigated 11 and that cisgender women competitors are unable to achieve similar benefits naturally. 12 To date, this assumption has yet to be tested and confirmed in transgender athlete cohorts. The low serum testosterone concentrations from an assigned female-at-birth puberty would hypothetically not give transgender men the competitive advantages of higher testosterone concentrations over CM, and this viewpoint is reflected in the current inclusion sports policies for transgender men. 2
Lab-derived data on a cohort of transgender athletes, as requested in article 6.1b of the International Olympic Committee Framework On Fairness, Inclusion And Non-Discrimination based on Gender Identity and Sex Variations, 4 must be generated to better inform a decision-making process. 13 Therefore, the primary aim of this study was to compare cardiorespiratory fitness, strength and body composition of transgender women and men athletes to that of matched cisgender cohorts.
Study design
This cross-sectional study involved a single visit to the laboratory at the School of Applied Sciences, University of Brighton, UK. Each participant arrived at ~9:00 hours. after an overnight fast and departed from testing at ~15:00 hours. The complete study design can be found in the study protocol, available as a preprint. 14
Recruitment
Following ethical approval (ref: 9496), 75 (19 CM, 12 transgender men, 23 transgender women and 21 cisgender women) participants were recruited through social media advertising on Meta Platforms (Facebook and Instagram, Meta Platforms, California, USA) and X (Twitter, California, USA). Following the initial response, all participants were provided with the participant information sheet by email at least 7 days before being invited to travel to the laboratory, with further oral information about the study procedures and written informed consent provided on their visit to the laboratory.
Participants and eligibility criteria
Participants were required to participate in competitive sports or undergo physical training at least three times per week. Following written consent, participants were asked to record their last four training sessions and self-rate their training intensity for each session on a scale of 1–10 (10=maximum intensity). The mean of the four sessions was recorded to represent the athletes’ training intensity. The transgender athletes must have completed ≥1 year of GAHT, voluntarily disclosed during consent and verified during blood test analysis. The full inclusion/exclusion criteria can be found in the study protocol, available as a preprint. 14 Two cisgender women and one transgender man could not provide blood samples and were consequently excluded from all analyses as their endocrine profiles could not be verified. Furthermore, two transgender women and one cisgender woman were excluded from all analyses due to testosterone concentrations exceeding recommended female testosterone concentrations (2.7 nmol/L 15 ).
Laboratory assessments
Blood sampling and analysis.
Prior to venous blood sampling, haemoglobin concentration ((Hb)) was sampled via the third drop of a Unistik 3 Comfort lancet (Owen Mumford, Woodstock, UK) finger prick capillary blood sample analysed immediately using a HemoCue 201+ (HemoCue AB, Ängelholm, Sweden). Capillary blood was used for (Hb) analysis for practical reasons such as ease of use. It is important to note that the HemoCue 201+used in the present study is expected to yield higher (Hb) values than venous blood. 16 After capillary sampling, one 10 mL whole venous blood sample was collected from an antecubital vein into a BD serum tube (Becton, Dickinson and Company, Wokingham, Berkshire, UK) for serum extraction. Once collected, the tubes were left at room temperature (18°C±5°C) for 1 hour and then stored in a fridge (3°C±2°C) for up to 4 hours before being centrifuged (PK 120 centrifuge, ALC, Winchester, Virginia, USA) using a T515 rotor at 1300G for 10 min at 4°C, before storage at −80°C until analysis. Before analysis, the samples were stored between −25°C and −15°C, thawed at room temp until liquid, vortexing to remix samples, centrifuged at 2876G for 8 min to remove any precipitant and then analysed for participant’s testosterone and oestradiol concentrations on an immunoassay analyser (Roche Cobas 8000 e801, Roche Diagnostics, Burgess Hill, UK).
Body composition and bone mass
Participants’ body mass was measured (OMRON Healthcare, Kyoto, Japan) while participants were lightly dressed, representing clothed body mass. Body composition and bone mass were measured by DXA (Horizon W, Hologic, Massachusetts, USA). Each participant underwent a whole-body, a proximal-femur and a lumbar spine scan. The participant was asked to lie on the scan bed, and the first author (BH) performed all participant placement and scanning for the three scans. Due to inbuilt assumptions of body fat percentage for the head and scanning bed area imitations, whole-body less head data are reported for the whole-body scan. Body mass index (BMI), Fat Mass Index (FMI) and Fat-Free Mass Index (FFMI) were calculated by taking the appropriate mass value and dividing it by height (m 2 ).
Lung function
Lung function was measured using a Vitalograph Alpha spirometer (Vitalograph, Kansas, USA) with an antibacterial filter and a nose clip on the bridge of the participant’s nose. Each participant was asked to perform the flow-volume-loop spirometry to test forced vital capacity (FVC), forced expiratory volume in 1 s (FEV 1 ) and peak expiratory flow. The test was repeated until a trend of declining performance occurred. The highest numeric value for each metric obtained during a test with the correct procedure was then recorded. The FEV1:FVC ratio was used to assess the presence of obstructed lung function.
Strength was measured using a handgrip dynamometer (TAKEI 5401, TAKEI Scientific Instruments, Japan). The participants’ hand sizes were also measured around the metacarpophalangeal joints of both hands prior to testing. Each hand was tested three times in sequential order of left-right to allow each hand to rest; the mean scores were taken from the three attempts for each hand.
Lower body power
Lower body power was measured with the countermovement jump on a JUM001 Jump Mat (Probotics, Alabama, USA). During the test, if the participant went beyond 45° of countermovement or the hands came off the hips, the test would be declared void for that attempt. After recording three legitimate attempts, the mean scores were recorded.
Cardiopulmonary exercise testing
Cardiopulmonary exercise testing was performed using a 95T Engage Treadmill ergometer (Life Fitness, Illinois, USA) and a COSMED QUARK (COSMED, Rome, Italy). All V̇O 2 max tests were conducted and analysed by the first author (BH) to avoid interinvestigator variability. 17 The ramp protocol of Badawy and Muaidi treadmill V̇O 2 max testing 18 was used for each V̇O 2 max test, involving gradual increases in speed every 3 min at a 1% incline. One cisgender man and two cisgender women were excluded from the analysis as they did not meet the required respiratory exchange ratio of ≥1.1 to classify the test as maximal (cisgender men (CM), n=18, transgender men (TM), n=11; cisgender women (CW) n=16; transgender women (TW), n=21).
Statistical analysis
Data meeting the assumptions of normality and homogeneity of variance were analysed using a one-way analysis of variance along with Bonferroni post hoc corrections for pairwise comparisons. Data not meeting the parametric assumptions were compared using a Kruskal-Wallis ANOVA with Dwass-Steel-Critchlow-Fligner post hoc test for multiple comparisons, with an alpha level of 0.05 for both types of analysis. Statistical analysis and presentation are consistent with the checklist for statistical assessment of medical papers statement 19 found in online supplemental files 1–3 at Hamilton et al , The Strength, Power and Aerobic Capacity of Transgender Athletes: A Cross-Sectional Study (Internet). OSF; 2023. Available from: osf.io/a684b.
Supplemental material
Equity, diversity and inclusion statement.
The author group consists of early (n=3) and senior researchers (n=3) from different disciplines and universities (n=3). Two authors are members of a marginalised community; the lead early-career author is a transgender woman, and one of the junior authors is a woman from the global south. Our study population included male and female transgender athletes from within the UK participating in competitive sports in comparison with cisgender male and female athletes participating in competitive sports; thus, findings may not be generalisable to global athlete populations.
Participant characteristics
Our investigation encompassed a diverse cohort of athletes, with endurance sports representing 36% of the athlete cohort, team sports representing 26% and power sports representing 38%. No cisgender or transgender athletes were competing at the national or international level. No significant differences were found in age (F (3–66) =1.9, p=0.14), training intensity score (χ 2 (3) =1.2, p=0.76) or length of GAHT between transgender men and transgender women (F (1–32) =0.5, p=0.48, table 1 ).
- View inline
Significant differences were found in height (F (3–66) =21.3, p<0.001), with CM being taller than transgender men (t (66) =3.8, p=0.002, table 1 ). Transgender women were also taller than transgender men (t (66) =3.3, p=0.01) and cisgender women (t (66) =6.5, p<0.001, table 1 ).
Significant differences were found in clothed mass (F (3–66) =10.6, p<0.001), with transgender women found to be heavier than cisgender women (t (66) =5.6, p<0.001, table 1 ).
BMI was also significantly different between the groups in this Study (F (3–66) =3.6, p=0.02). Transgender women athletes demonstrated higher BMI than cisgender women (t (66) =2.9, p=0.03, table 1 ), with no further differences observed.
Blood measures
There was a significant gender effect on testosterone concentration (F (3–66) =80.6, p<0.001). CM (20.5±5.8 nmol/L) exhibited significantly higher total testosterone concentration than transgender women (0.7±0.5 nmol/L, t (66) = 11.1, p<0.001, figure 1A ). Transgender men (24.8±12.3 nmol/L) had elevated total testosterone concentration compared with transgender women (t (66) =11.3) and cisgender women (0.9±0.4 nmol/L, t (66) =10.9, both p<0.001, figure 1A ). There was also a significant gender effect on oestradiol concentration (F (3−66) =7.6, p<0.001), with transgender women (742.4±801.9 pmol/L) showing higher oestradiol concentration than CM (104.3±24.8 pmol/L, t (66) =4.4 p<0.001), cisgender women (336.0±266.3 pmol/L, t (66) =2.7, p=0.045) and transgender men (150.2±59.4 pmol/L, t (66) =3.4, p=0.01, figure 1B ).
- Download figure
- Open in new tab
- Download powerpoint
Blood measures. (A) testosterone; (B) oestradiol; (C) haemoglobin. *p<0.05, **p<0.01, ***p<0.001, ****p<0.0001. CM, cisgender men; CW, cisgender women; TM, transgender men; TW, transgender women.
Transgender women’s total testosterone concentration (0.7±0.5 nmol/L) falls within the recommendations for GAHT of ≤1.8 nmol/L, 5 and oestradiol concentrations (742.4±801.9 pmol/L) exceed the target of 400–600 pmol/L 5 for GAHT. Transgender men’s testosterone concentration (24.8±12.3 nmol/L) exceeds the NHS target of 15–20 nmol/L 6 for GAHT, although not the Endocrine Society target of 11–34.7 nmol/L. 7
Differences were reported in (Hb) concentration (F (3–66) =3.3, p=0.03), although a post hoc Bonferroni analysis showed no differences between the various groups (CM 142.8±12.5 g/L; transgender men, 143.3±19.5 g/L; transgender women, 131.3±14.2 g/L; cisgender women, 133.3±12.7 g/L; figure 1C ).
DXA assessment
There was a significant gender effect on percentage fat mass (F (3–66) =6.6, p<0.001), with CM having a lower percentage fat mass than transgender women (t (66) =−4.4, p<0.001, table 2 ), with no other differences observed. A significant gender effect was also found on absolute fat mass (F (3–66) =6.6, p<0.001), with transgender women having more absolute fat mass than CM (t (66) =3.8, p=0.002, table 2 ) and cisgender women (t (66) =3.9, p=0.002, table 2 ). FMI measures revealed a gender effect (F (3–66) =5.2, p=0.003), with transgender women found to have a higher FMI than CM (t (66) =3.7, p=0.002, table 2 ) and cisgender women (t (66) =2.8, p=0.04, table 2 ). Android to gynoid ratio analysis (F (3–66) =10.7, p<0.001) revealed cisgender women had a lower ratio than transgender men (t (66) =−2.9, p=0.03, table 2 ), and transgender women (t (66) =−4.0, p=0.001, table 2 ).
Body composition, BMD data, handgrip strength, lower anaerobic power and cardiopulmonary exercise testing
Fat-free mass
There was a significant gender effect on absolute fat-free mass (F (3–66) =24.6, p<0.001), with CM having significantly more absolute fat-free mass than transgender men (t (66) =3.5, p=0.01, table 2 ). Cisgender women had less absolute fat-free mass than transgender men (t (66) =−3.5, p=0.01, table 2 ) and transgender women (t (66) =−6.6, p<0.001, table 2 ). No gender-based effects were found when comparing transgender women athletes to cisgender women athletes, or transgender men athletes to CM athletes in the measures of FFMI (F (3–66) =3.7, p=0.02, table 2 ), percentage of fat-free mass (F (3–66) =2.4, p=0.08, table 2 ) or appendicular FFMI (F (3–66) =5.1, p=0.003, table 2 ).
Bone mineral density
No differences in whole-body bone mineral density (BMD) (F (3–66) =4.6, p=0.01), femoral neck BMD (F (3–66) =1.0, p=0.39, table 2 ), total proximal femur BMD (F (3–66) =1.5, p=0.22, table 2 ) or total lumbar spine BMD (F (3–66) =0.4, p=0.78, table 2 ) were found between transgender athletes and cisgender athletes ( table 2 ).
Lung function data for all groups can be found in table 2 . FEV 1 had an effect of gender (F (3–66) =14.7, p<0.001), with CM having greater FEV 1 than transgender men (t (66) = 4.5, p<0.001, figure 2A ). Transgender women also had greater FEV 1 than cisgender women (t (66) =4.2, p<0.001, figure 2A ) and transgender men (t (66) =2.9, p=0.03, figure 2A ). There was a similar effect of gender on FVC (F (3–66) =21.6, p<0.001, figure 2B ), with CM having greater FVC than transgender men (t (66) =5.2, p<0.001, figure 2B ). Transgender women also had greater FVC than cisgender women (t (66) =5.6, p<0.001, figure 2B ) and transgender men (t (66) =4.0, p=0.001, figure 2B ). A significant effect of gender was also seen on the FEV 1 :FVC ratio (F (3–66) =3.3, p=0.03 figure 2C ), with transgender women showing a reduced FEV 1 :FVC ratio compared with cisgender women (t (66) =−2.8, p=0.04, figure 2C ) with no differences observed in transgender or CM. Peak expiratory flow (F (3–66) =5.5, p=0.002) had a minor gender-based effect, with cisgender women having lower peak expiratory flow than transgender women (t (66) −3.0, p=0.02, figure 2D ).
Lung function measures. (A) Forced rxpiratory volume in 1 s (FEV 1 ); (B) forced vital capacity (FVC) (C) modified Tiffeneau-Pinelli Index (FEV 1 :FVC); (D) peak expiratory flow (PEF). *p<0.05, **p<0.01, ***p<0.001, ****p<0.0001. CM, cisgender men; CW, cisgender women; TM, transgender men; TW, transgender women.
Handgrip strength
Handgrip strength data can be found in table 2 . Absolute right handgrip strength was significantly different between the groups (F (3–66) =10.5, p<0.001), with CM having greater absolute right handgrip strength than transgender men (t (66) =2.9, p=0.03, figure 3B ). Transgender women also had greater absolute right handgrip strength than cisgender women (t (66) =3.2, p=0.01, figure 3B ). Absolute left handgrip was significantly different between the groups (F (3–66) =8.6, p<0.001). However, no differences were found between transgender and cisgender athletes ( figure 3A ). There was no effect on the right (F (3–66) =0.8, p=0.53, figure 3F ) or left-hand grip strength (F (3–66) =1.0, p=0.39, figure 3E ) relative to fat-free mass, nor was there any gender effect on the right (F (3–66) =1.6, p=0.20, figure 3D ) or left-hand grip-strength (F (3–66) =2.1, p=0.11) relative to hand size.
Absolute and relative handgrip strength (GS) measures. (A) Absolute strength (right hand); B) Absolute strength (left hand) (C) relative strength to hand size (right hand); (D) relative strength to hand size (left hand); (E) relative strength to fat-free mass (FFM) (right hand); (F) relative strength to fat-free mass (left hand). *p<0.05, ***p<0.001, ****p<0.0001. CM, cisgender men; CW, cisgender women; TM, transgender men; TW, transgender women.
Lower body anaerobic power
Lower body anaerobic power data are shown in table 2 . Gender had a significant effect on absolute countermovement jump height (F (3–66) =7.2, p<0.001), with CM having greater absolute jump height than transgender women (t (66) =4.5, p<0.001, figure 4A ). A significant effect of gender was found in countermovement jump height relative to fat-free mass (F (3–66) =10.1, p<0.001, figure 4B ), with transgender women found to have lower countermovement jump height relative to fat-free mass than both cisgender women (t (66) =−5.3, p<0.001) and transgender men (t (66) =–3.2, p=0.01, figure 4B ).
Absolute and relative anaerobic power measures. (A) Absolute CMJ height; B) Relative CMJ height to fat-free mass (FFM); (C) absolute peak power; (D) relative peak power to FFM; (E) absolute average power; (F) relative average power to FFM. *p<0.05, **p<0.01, ***p<0.001, ****p<0.0001. CM, cisgender men; CMJ, Counter Movement Jump; CW, cisgender women; TM, transgender men; TW, transgender women.
There was a significant difference in absolute peak power (F (3–66) =8.7, p<0.001), with cisgender women having reduced peak power compared with transgender men (t (66) =−3.3, p=0.01) and transgender women (t (66) =−3.6, p=0.004, figure 4C ). Peak power relative to fat-free mass had a more negligible gender effect (F (3–66) =4.2, p=0.01), with no difference in peak power relative to fat-free mass found between transgender and cisgender athletes ( figure 4D ).
There was a significant gender effect of absolute average power (F (3–66) =5.9, p=0.001), with cisgender women having reduced absolute average power compared with transgender men (t (66) =–3.1, p=0.02, figure 4E ). There was no effect of gender on average power relative to fat-free mass (F (3–66) =2.6, p=0.06, figure 4F ).
Cardiopulmonary exercise testing data are shown in table 2 . A significant effect of gender was found on absolute V̇O 2 max (F (3–62) =14.1, p<0.001) with CM having greater absolute V̇O 2 max than transgender men (t (66) =3.8, p=0.002, figure 5A ) and transgender women (t (66) =4.3, p<0.001, figure 5A ). Relative V̇O 2 max to body mass also showed a significant gender effect (F (3–62) =9.8, p<0.001) with transgender women having lower relative V̇O 2 max than CM (t (66) =–5.3, p<0.001, figure 5B ) and cisgender women (t (66) =−3.3, p=0.01, figure 5B ). No significant gender effect was found on the measure of V̇O 2 max relative to fat-free mass (F (3–62) =2.0, p=0.12).
Absolute and relative cardiopulmonary exercise testing measures. (A) Absolute V̇O 2 max; (B) relative V̇O 2 max to body weight; (C) absolute anaerobic threshold (AT); (D) anaerobic threshold (%V̇O 2 max); (E) relative anaerobic threshold relative to body mass; (F) AT relative to at-free mass (FFM). *p<0.05, **p<0.01, ***p<0.001, ****p<0.0001. CM, cisgender men; CW, cisgender women; TM, transgender men; TW, transgender women.
Gender affected the absolute anaerobic threshold (F (3–62) =14.1, p<0.001), with cisgender (3924±628 mL/min) men having a higher absolute anaerobic threshold than transgender men (3089±546 mL/min, t (66) =4.2, p<0.001, figure 5C ), and transgender women (3122±438 mL/min, t (66) =4.8, p<0.001, figure 5C ). No significant gender effect was found on the measure of anaerobic threshold as a percentage of V̇O 2 max (F (3–62) =0.8, p=0.51, figure 5D ). A gender effect was also seen on the anaerobic threshold relative to body mass (F (3–62) =10.7, p<0.001), with transgender women (38.3±6.6 mL/kg/min) showing a lower relative anaerobic threshold than both cisgender women (47.2±6.1 mL/kg/min, t (66) =–3.3, p=0.01, figure 5E ) and CM (52.2±9.5 mL/kg/min, t (66) =−5.4, p<0.001, figure 5E ). CM also showed a higher relative anaerobic threshold than transgender men (42.1±9.9 mL/kg/min, t (66) =3.3, p=0.01, figure 5E ). Anaerobic threshold relative to fat-free mass also had a small gender effect (F (3–62) =3.2, p=0.03), with transgender women (60.8±12.2 mL/kg FFM /min) having a lower anaerobic threshold relative to fat-free mass than CM (71.2±13.3 mL/kg FFM /min, t (66) =−2.8, p=0.045, figure 5F ).
The results presented in this study provide valuable insights into laboratory-based performance-related metrics of gender-diverse athletes participating in competitive sports. Given the primary aim of GAHT, 20 it is noteworthy that although this study is cross-sectional in design, transgender women’s oestradiol was higher than that of cisgender women ( figure 1B ). The presence of outliers affecting transgender women’s oestrogen concentration ( figure 1B ) is evident. This underscores that transgender women in this cohort of athletes exhibit a distinct endocrine profile from CM and share a similar endocrine profile with cisgender women, whom many transgender women aim to integrate into a sporting category. One of the most noticeable disparities between gender groups was in height and mass ( table 1 ), with CM and transgender women being taller and heavier than their cisgender and transgender counterparts ( table 1 ). Body composition measures (fat mass % and fat-free mass %, table 2 ) between transgender women and cisgender women found no difference. However, transgender women are, on average as a cohort taller and heavier.
In this cohort, the average difference in haemoglobin (Hb) between cisgender women and CM athletes was 7% ( figure 1C ), lower than previously described (12% 8 ). Notably, the (Hb) profiles of all the athlete groups were not significantly different, concurring with earlier research 21 and contradicting research in sedentary populations. 22 (Hb) is crucial in O 2 transport 23 and vital for endurance sports performance, 24 with O 2 delivery to the tissues a limiting factor in V̇O 2 max attainment. 25 The lack of differences in (Hb) is consistent with the lack of observed difference in absolute V̇O 2 max between transgender women, transgender men and cisgender women in this cohort. However, as cardiac output, the most crucial variable influencing V̇O 2 max 25 was not assessed in the present study, a more comprehensive mechanistic explanation for the similar maximal aerobic capacity between groups cannot be provided.
No differences in BMD were observed between transgender and cisgender women athletes in this study ( table 2 ), despite prior research hypothesising that transgender women athletes have a significant BMD advantage over cisgender women. 11 The sample size for each gender was n<30 participants and may be insufficient to characterise BMD differences reliably. Exercise has been shown to have a protective effect on BMD in CM 26 and CW, 27 and our results suggest a protective effect of exercise in transgender women, given that there is evidence of low BMD in transgender women with low weekly sports activity. 28 Nevertheless, the results suggest the complexity of bone health in athlete populations and the need for a more comprehensive assessment to understand the long-term impact of GAHT on transgender athletes’ BMD.
The differences observed in body composition in this population ( table 2 ) indirectly show the potential role of androgens in body composition, owing to the role of oestradiol in fat accumulation 29 and transgender women’s oestradiol concentrations ( figure 1B ) and fat mass ( table 2 ) being greater than all other groups. Body composition differences may have implications for sports that prioritise exercise economy, 30 defined as the average V̇O 2 relative to body mass between submaximal intensities, 31 as athletes with a higher fat mass percentage will present with a lower exercise economy owing to the increased O 2 cost of exercise. 32 The android-to-gynoid ratio analysis ( table 2 ) suggests that hormone therapy ( figure 1A,B ) influences differences in fat distribution patterns. However, fat distribution patterns of the present transgender female athlete cohort ( table 2 ) do not reach ratios previously reported in cisgender female populations (0.8). 33 Understanding these variations is essential for evaluating performance in sports where body composition is a determining factor, for example, weightlifting or boxing.
Cisgender women had lower absolute fat-free mass than transgender men and transgender women ( table 2 ). When analysing absolute fat and fat-free mass data ( table 2 ), these results can be affected by sample size and/or athlete diversity limitations. A purposefully designed future study with height-matched and sport-matched cisgender and transgender female athletes is crucial to understanding differences in these parameters, as they are influenced by height disparities ( table 1 ) and variations in sampled sports.
FVC, FEV 1 and FEV 1 :FVC ratio are higher in athletes than in the normal sedentary control individuals, 34 and there is no difference in all three metrics between aerobic athletes and anaerobic athletes. 35 Therefore, the lung function differences observed in figure 2A,B may be attributed to factors such as skeletal size benefiting lung capacity and function, 36 with transgender women’s FVC results ( figure 2B ) suggesting gender-affirming hormone care did not impact changing lung volumes owing to the GAHTs lack of effect on skeletal stature. 11 Transgender women showed a significantly reduced FEV 1 :FVC ratio compared with cisgender women ( figure 2C ). The FEV 1 :FVC ratio has been used as a screening index for identifying obstructive lung conditions globally, 37 as a lower FEV 1 owing to obstruction of air escaping from the lungs will reduce the FEV 1 :FVC ratio. Transgender women’s results ( figure 2C ) suggest obstructed airflow in the lungs 38 when compared with cisgender women. However, this observation of transgender women is unlikely to be pathological (<0.70), 39 as seen in chronic obstructive pulmonary disease.
Nevertheless, this reduced airflow could potentially lead to exercise-induced dyspnoea, resulting in performance limitations 40 in comparison to cisgender women. When comparing both the CM and transgender women athletes’ groups with identical heights (1.8 m, table 1 ), while both groups exhibit similar FVC, transgender women demonstrate a lower FEV 1 , leading to a reduced FEV 1 :FVC ratio compared with CM, although not significant. If there were a significant difference between CM and transgender women, our preliminary hypothesis would have attributed this divergence to testosterone suppression in transgender women. However, comparing transgender women to cisgender women who do not share similar height and or exhibit a comparable FVC, the observed differences become more complex to interpret. The possibility arises that factors beyond hormonal influences, such as varying levels of aerobic training, may contribute to the significant difference found in the FEV 1 :FVC ratio between transgender women and cisgender women. Further longitudinal investigation is required to elucidate if the causation underlying these pulmonary function disparities is indeed testosterone suppression.
Strength results in figure 3 disagree with previous literature in a non-athlete transgender cohort using the same methodology that showed transgender women and CM had significantly different absolute and relative hand grip strength. 41 Our results showed no differences in absolute strength between transgender women and CM and no difference in relative handgrip between any of the groups in this study ( figure 3 ). These results highlight the differences between athlete and sedentary populations. However, the results relative to hand size also concur with the notion that greater handgrip strength is caused by greater hand size, 42 as there were no differences in results between the four groups when normalised for hand size ( figure 3C,D ). Therefore, investigations with more accurate measures of strength are warranted in transgender athletes.
Transgender women presented lower absolute jump height than CM and lower relative jump height, normalised for fat-free mass, than transgender men and cisgender women ( figure 4 ). These results in this study cohort suggest that transgender women lack lower body anaerobic power compared with the other groups. Transgender women’s higher absolute peak power than cisgender women ( figure 4C ), coupled with higher fat mass potentially driven by higher oestradiol concentrations ( figure 1B ), suggest that transgender women had more inertia to overcome during the explosive phase of the countermovement jump, which may lead to decreased performance. However, when normalised for fat-free mass ( figure 4D ), transgender women’s peak power was lower than that of cisgender women, showing that this cohort also lacks peak power relatively, indicating that the higher fat mass may not be the primary contributing factor. Further investigations are warranted to find the causation of this poor lower anaerobic power performance in transgender women.
The lack of differences in anaerobic threshold (%V̇O 2 max, figure 5D ) suggests that the athletes in this study had a similar fitness status, which is an essential underlying finding given that CM showed greater absolute V̇O 2 max than all groups ( figure 5A ), with no differences between transgender women and cisgender women found, and transgender women exhibited lower relative V̇O 2 max compared with both CM and women ( figure 5B ). In this cohort, the finding of no statistical difference in absolute V̇O 2 max between transgender women and cisgender women contrasts the idea that transgender women’s bigger lung size ( table 2 ) is an inherent respiratory function advantage over cisgender women. 11 Both the absolute and relative V̇O 2 max differences between groups contradict one previous study in non-athlete transgender populations that found transgender women had higher absolute V̇O 2 peak and no difference in relative V̇O 2 peak compared with cisgender women. 41 This contradictory finding further highlights population differences between non-athlete and athlete cohorts while also contradicting literature hypothesising that there would be a baseline gap in aerobic capacity between transgender women and cisgender women. 11 The results in this athlete cohort warrant further research to elucidate the mechanisms behind this deviation, as they may be metabolic, as transgender women also exhibited a lower relative anaerobic threshold ( figure 5E ). The findings in table 2 reveal notable disparities in fat mass, fat-free mass, laboratory sports performance measures and hand-grip strength measures between cisgender male and transgender female athletes. These differences underscore the inadequacy of using cisgender male athletes as proxies for transgender women athletes. Therefore, based on these limited findings, we recommend that transgender women athletes be evaluated as their own demographic group, in accordance with the principles outlined in Article 6.1b of the International Olympic Committee Framework on Fairness, Inclusion and Non-Discrimination based on Gender Identity and Sex Variations. 4
Study limitations
The limitations of this study primarily relate to its cross-sectional design, making it challenging to establish causation or examine if the performance of athletes changes as a result of undergoing GAHT. Longitudinal studies are needed to examine how GAHT, and other factors impact athletes’ physiology and performance over time. Additionally, the composition of the study cohort may not fully represent the diversity of athletes in elite sports from worldwide populations. Athletes from various sporting disciplines and performance levels were included, and the athlete training intensity was self-reported. Therefore, the results may suffer from selection and recall bias. 43 The results may not apply to all levels or ages of athletes, specifically as this research did not include any adolescent athletes competing at the national or international level. The athletes participating in the present study represented a variety of different sports, and this would have undoubtedly impacted the results of the study as different sports stress different training and sports modalities. Exercise type, intensity and duration all have an impact on physiological responses and overall laboratory performance metrics. 44 The subgroups of sports that emerged were also too dissimilar to allow meaningful subgroup analysis. The complexity and difficulty of this area of activity means that while this study provides a starting point for understanding the complex physiology in GAHT and athletic performance, this study does not provide evidence that is sufficient to influence policy for either inclusion or exclusion. However, this is the first study to assess laboratory-based measures of performance in transgender athletes, and this opens up interesting avenues for replication and extension into the longitudinal effects of GAHT on athletic performance.
Future research should include more extensive and diverse samples to enhance the generalisability of findings or smaller, more specific cohorts to hone in on a particular sports discipline. However, such studies may be complex due to the low numbers of transgender athletes. The recruitment method of this study also provided a limitation as social media advertising was used rather than recruitment from a clinical provider. Social media recruitment leaves this study open to sample bias as social media advertising, although great for recruiting hard-to-reach participants for observational studies, 44 45 does not represent a clinical population in 86% of comparisons. 44 As the participants were not recruited from a clinic, this also means that the gender-affirming treatment of the transgender athletes was not controlled. For example, different testosterone suppression methods have different efficacies, 46 and future studies should consider differences in the prescribed GAHT to participants. Lastly, the participants were not screened by a clinician before participation, and any medical conditions were self-reported in the physical activity readiness questionnaire (PAR-Q). This method of medical reporting leaves the data open to self-reporting bias, which can mislead descriptive statistics and causal inferences 47 as participants’ cognitive processes, such as social desirability, can alter participants’ responses. 48 Therefore, it is recommended to use a clinic to screen and recruit participants to avoid such bias in a longitudinal study of transgender athlete sports performance.
Conclusions
This research compares transgender male and transgender female athletes to their cisgender counterparts. Compared with cisgender women, transgender women have decreased lung function, increasing their work in breathing. Regardless of fat-free mass distribution, transgender women performed worse on the countermovement jump than cisgender women and CM. Although transgender women have comparable absolute V̇O 2 max values to cisgender women, when normalised for body weight, transgender women’s cardiovascular fitness is lower than CM and women. Therefore, this research shows the potential complexity of transgender athlete physiology and its effects on the laboratory measures of physical performance. A long-term longitudinal study is needed to confirm whether these findings are directly related to gender-affirming hormone therapy owing to the study’s shortcomings, particularly its cross-sectional design and limited sample size, which make confirming the causal effect of gender-affirmative care on sports performance problematic.
Ethics statements
Patient consent for publication.
Not applicable.
Ethics approval
This study involves human participants and ethical approval for this study has been granted by the School of Applied Sciences Research Ethics Committee of the University of Brighton, Brighton, UK (Ref: 9496). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We thank Associate Professor Ada Cheung of the Department of Medicine (Austin Health) at the University of Melbourne, Australia for her valuable review of this work prior to publication.
- Arcelus J ,
- Bouman WP , et al
- World Aquatics
- USA Gymnastics
- International Olympic Committee
- National Health Service
- Hembree WC ,
- Cohen-Kettenis PT ,
- Gooren L , et al
- Handelsman DJ ,
- Hirschberg AL ,
- Alvero-Cruz JR ,
- Chilibeck P , et al
- Gharahdaghi N ,
- Phillips BE ,
- Szewczyk NJ , et al
- Hilton EN ,
- Lundberg TR
- Hamilton BR ,
- Barrett J , et al
- Hamilton B ,
- Comeras-Chueca C ,
- Bush P , et al
- Leitman SF , et al
- Popović ZB ,
- Badawy MM ,
- Mansournia MA ,
- Collins GS ,
- Nielsen RO , et al
- Malczewska-Lenczowska J ,
- Sitkowski D ,
- Orysiak J , et al
- Roberts TK ,
- French D , et al
- Schmidt W ,
- Bassett DR ,
- Staines KA ,
- Kelley GA , et al
- Hofmeister M
- Rothman MS ,
- Mareschal J ,
- Karsegard VL , et al
- Losnegard T ,
- Schäfer D ,
- V Mendonca G ,
- Imboden MT ,
- Swartz AM , et al
- Rajaure YS ,
- Budhathoki L , et al
- van der Plaat D ,
- Dharmage S , et al
- Min HK , et al
- Schiöler L ,
- Lindberg A , et al
- Anzueto A , et al
- Alvares LAM ,
- Santos MR ,
- Souza FR , et al
- Alahmari KA ,
- Kakaraparthi VN ,
- Reddy RS , et al
- Tripepi G ,
- Dekker FW , et al
- Topolovec-Vranic J ,
- Natarajan K
- Whitaker C ,
- Stevelink S ,
- Leemaqz S ,
- Ooi O , et al
- Mathiowetz N
Supplementary materials
Supplementary data.
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1
- Data supplement 2
- Data supplement 3
X @BlairH_PhD
Contributors BH, FMG and YPP designed the study. Material preparation, reporting and critical revision of the work were performed by BH, PGB, FMG and YPP. Data collection was performed by CC-C, AB, SM-M and BH. BH wrote the first draft of the manuscript, and all authors critically revised subsequent versions until all authors could approve the final manuscript. YPP is the guarantor.
Funding The study has been funded by a research grant awarded by the International Olympic Committee, Lausanne, Switzerland.
Competing interests YPP is a member of the IOC Medical and Scientific Commission, which recently published articles and framework documents on the topic. BH and FMG have recently published articles on the topic on behalf of the International Federation of Sports Medicine (FIMS). All authors declare no further conflict of interest or competing interests.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Read the full text or download the PDF:

An official website of the United States government
The .gov means it's official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you're on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
- Browse Titles
NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
Velentgas P, Dreyer NA, Nourjah P, et al., editors. Developing a Protocol for Observational Comparative Effectiveness Research: A User's Guide. Rockville (MD): Agency for Healthcare Research and Quality (US); 2013 Jan.

Developing a Protocol for Observational Comparative Effectiveness Research: A User's Guide.
- Hardcopy Version at Agency for Healthcare Research and Quality
Chapter 1 Study Objectives and Questions
Scott R Smith , PhD.
The steps involved in the process of developing research questions and study objectives for conducting observational comparative effectiveness research (CER) are described in this chapter. It is important to begin with identifying decisions under consideration, determining who the decisionmakers and stakeholders in the specific area of research under study are, and understanding the context in which decisions are being made. Synthesizing the current knowledge base and identifying evidence gaps is the next important step in the process, followed by conceptualizing the research problem, which includes developing questions that address the gaps in existing evidence. Understanding the stage of knowledge that the study is designed to address will come from developing these initial questions. Identifying which questions are critical to reduce decisional uncertainty and minimize gaps in the current knowledge base is an important part of developing a successful framework. In particular, it is beneficial to look at what study populations, interventions, comparisons, outcomes, timeframe, and settings (PICOTS framework) are most important to decisionmakers in weighing the balance of harms and benefits of action. Some research questions are easier to operationalize than others, and study limitations should be recognized and accepted from an early stage. The level of new scientific evidence that is required by the decisionmaker to make a decision or to take action must be recognized. Lastly, the magnitude of effect must be specified. This can mean defining what is a clinically meaningful difference in the study endpoints from the perspective of the decisionmaker and/or defining what is a meaningful difference from the patient's perspective.
The foundation for designing a new research protocol is the study's objectives and the questions that will be investigated through its implementation. All aspects of study design and analysis are based on the objectives and questions articulated in a study's protocol. Consequently, it is exceedingly important that a study's objectives and questions be formulated meticulously and written precisely in order for the research to be successful in generating new knowledge that can be used to inform health care decisions and actions.
An important aspect of CER 1 and other forms of translational research is the potential for early involvement and inclusion of patients and other stakeholders to collaborate with researchers in identifying study objectives, key questions, major study endpoints, and the evidentiary standards that are needed to inform decisionmaking. The involvement of stakeholders in formulating the research questions increases the applicability of the study to the end-users and facilitates appropriate translation of the results into health care practice and use by patient communities. While stakeholders may be defined in multiple ways, for the purposes of this User's Guide , a broad definition will be used. Hence, stakeholders are defined as individuals or organizations that use scientific evidence for decisionmaking and therefore have an interest in the results of new research. Implicit in this definition of stakeholders is the importance for stakeholders to understand the scientific process, including considerations of bioethics and the limitations of research, particularly with regard to studies involving human subjects. Ideally, stakeholders also should express commitment to using objective scientific evidence to inform their decisionmaking and recognize that disregarding sound scientific methods often will undermine decisionmaking. For stakeholder organizations, it is also advantageous if the organization has well-established processes for transparently reviewing and incorporating research findings into decisions as well as organized channels for disseminating research results.
There are at least seven essential steps in the conceptualization and development of a research question or set of questions for an observational CER protocol. These steps are presented as a general framework in Table 1.1 below and elaborated upon in the subsequent sections of this chapter. The framework is based on the principle that researchers and stakeholders will work together to objectively lay out the research problems, research questions, study objectives, and key parameters for which scientific evidence is needed to inform decisionmaking or health care actions. The intent of this framework is to facilitate communication between researchers and stakeholders in conceptualizing the research problem and the design of a study (or a program of research involving a series of studies) in order to maximize the potential that new knowledge will be created from the research with results that can inform decisionmaking. To do this, research results must be relevant, applicable, unbiased and sufficient to meet the evidentiary threshold for decisionmaking or action by stakeholders. In order for the results to be valid and credible, all persons involved must be committed to protecting the integrity of the research from bias and conflicts of interest. Most importantly, the study must be designed to protect the rights, welfare, and well-being of subjects involved in the research.
Framework for developing and conceptualizing a CER protocol.
- Identifying Decisions, Decisionmakers, Actions, and Context
In order for research findings to be useful for decisionmaking, the study protocol should clearly articulate the decisions or actions for which stakeholders seek new scientific evidence. While only some studies may be sufficiently robust for making decisions or taking action, statements that describe the stakeholders' decisions will help those who read the protocol understand the rationale for the study and its potential for informing decisions or for translating the findings into changes in health care practices. This information also improves the ability of protocol readers to understand the purpose of the study so they can critically review its design and provide recommendations for ways it may be potentially improved. If stakeholders have a need to make decisions within a critical time frame for regulatory, ethical, or other reasons, this interval should be expressed to researchers and described in the protocol. In some cases, the time frame for decisionmaking may influence the choice of outcomes that can be studied and the study designs that can be used. For some stakeholders' questions, research and decisionmaking may need to be divided into stages, since it may take years for outcomes with long lag times to occur, and research findings will be delayed until they do.
In writing this section of the protocol, investigators should ask stakeholders to describe the context in which the decision will be made or actions will be taken. This context includes the background and rationale for the decision, key areas of uncertainty and controversies surrounding the decision, ways scientific evidence will be used to inform the decision, the process stakeholders will use to reach decisions based on scientific evidence, and a description of the key stakeholders who will use or potentially be affected by the decision. By explaining these contextual factors that surround the decision, investigators will be able to work with stakeholders to determine the study objectives and other major parameters of the study. This work also provides the opportunity to discuss how the tools of science can be applied to generate new evidence for informing stakeholder decisions and what limits may exist in those tools. In addition, this initial step begins to clarify the number of analyses necessary to generate the evidence that stakeholders need to make a decision or take other actions with sufficient certainty about the outcomes of interest. Finally, the contextual information facilitates advance planning and discussions by researchers and stakeholders about approaches to translation and implementation of the study findings once the research is completed.
- Synthesizing the Current Knowledge Base
In designing a new study, investigators should conduct a comprehensive review of the literature, critically appraise published studies, and synthesize what is known related to the research objectives. Specifically, investigators should summarize in the protocol what is known about the efficacy, effectiveness, and safety of the interventions and about the outcomes being studied. Furthermore, investigators should discuss measures used in prior research and whether these measures have changed over time. These descriptions will provide background on the knowledge base for the current protocol. It is equally important to identify which elements of the research problem are unknown because evidence is absent, insufficient, or conflicting.
For some research problems, systematic reviews of the literature may be available and can be useful resources to guide the study design. The AHRQ Evidence-based Practice Centers 2 and the Cochrane Collaboration 3 are examples of established programs that conduct thorough systematic reviews, technology assessments, and specialized comparative effectiveness reviews using standardized methods. When available, systematic reviews and technology assessments should be consulted as resources for investigators to assess the current knowledge base when designing new studies and working with stakeholders.
When reviewing the literature, investigators and stakeholders should identify the most relevant studies and guidelines about the interventions that will be studied. This will allow readers to understand how new research will add to the existing knowledge base. If guidelines are a source of information, then investigators should examine whether these guidelines have been updated to incorporate recent literature. In addition, investigators should assess the health sciences literature to determine what is known about expected effects of the interventions based on current understanding of the pathophysiology of the target condition. Furthermore, clinical experts should be consulted to help identify gaps in current knowledge based on their expertise and interactions with patients. Relevant questions to ask to assess the current knowledge base for development of an observational CER study protocol are:
- What are the most relevant studies and guidelines about the interventions, and why are these studies relevant to the protocol (e.g., because of the study findings, time period conducted, populations studied, etc.)?
- Are there differences in recommendations from clinical guidelines that would indicate clinical equipoise?
- What else is known about the expected effects of the interventions based on current understanding of the pathophysiology of the targeted condition?
- What do clinical experts say about gaps in current knowledge?
- Conceptualizing the Research Problem
In designing studies for addressing stakeholder questions, investigators should engage multiple stakeholders in discussions about how the research problem is conceptualized from the stakeholders' perspectives. These discussions will aid in designing a study that can be used to inform decisionmaking. Together, investigators and stakeholders should work collaboratively to determine the major objectives of the study based on the health care decisions facing stakeholders. As pointed out by Heckman, 4 research objectives should be formalized outside considerations of available data and the inferences that can be made from various statistical estimation approaches. Doing so will allow the study objectives to be determined by stakeholder needs rather than the availability of existing data. A thorough discussion of these considerations is beyond the scope of this chapter, but some important considerations are summarized in supplement 1 of this User's Guide.
In order to conceptualize the problem, stakeholders and other experts should be asked to describe the potential relationships between the intervention and important health outcomes. This description will help researchers develop preliminary hypotheses about the stated relationships. Likewise, stakeholders, researchers, and other experts should be asked to enumerate all major assumptions that affect the conceptualization of the research problem, but will not be directly examined in the study. These assumptions should be described in the study protocol and in reporting final study results. By clearly stating the assumptions, protocol reviewers will be better able to assess how the assumptions may influence the study results.
Based on the conceptualization of the research problem, investigators and stakeholders should make use of applicable scientific theory in designing the study protocol and developing the analytic plan. Research that is designed using a validated theory has a higher potential to reach valid conclusions and improve the overall understanding of a phenomenon. In addition, theory will aid in the interpretation of the study findings, since these results can be put in context with the theory and with past research. Depending on the nature of the inquiry, theory from specific disciplines such as health behavior, sociology, or biology could be the basis for designing the study. In addition, the research team should work with stakeholders to develop a conceptual model or framework to guide the implementation of the study. The protocol should also contain one or more figures that summarize the conceptual model or framework as it applies to the study. These figures will allow readers to understand the theoretical or conceptual basis for the study and how the theory is operationalized for the specific study. The figures should diagram relationships between study variables and outcomes to help readers of the protocol visualize relationships that will be examined in the study.
For research questions about causal associations between exposures and outcomes, causal models such as directed acyclic graphs (DAGs) may be useful tools in designing the conceptual framework for the study and developing the analytic plan. The value of DAGs in the context of refining study questions is that they make assumptions explicit in ways that can clarify gaps in knowledge. Free software such as DAGitty is available for creating, editing, and analyzing causal models. A thorough discussion of DAGs is beyond the scope of this chapter, but more information about DAGs is available in supplement 2 of this User's Guide.
The following list of questions may be useful for defining and describing a study's conceptual framework in a CER protocol:
- What are the main objectives of the study, as related to specific decisions to be made?
- What are the major assumptions of decisionmakers, investigators, and other experts about the problem or phenomenon being studied?
- What relationships, if any, do experts hypothesize exist between interventions and outcomes?
What is known about each element of the model?
Can relationships be expressed by causal diagrams?
- Determining the Stage of Knowledge Development for the Study Design
The scientific method is a process of observation and experimentation in order for the evidence base to be expanded as new knowledge is developed. Therefore, stakeholders and investigators should consider whether a program of research comprising a sequential or concurrent series of studies, rather than a single study, is needed to adequately make a decision. Staging the research into multiple studies and making interim decisions may improve the final decision and make judicious use of scarce research resources. In some cases, the results of preliminary studies, descriptive epidemiology, or pilot work may be helpful in making interim decisions and designing further research. Overall, a planned series of related studies or a program of research may be needed to adequately address stakeholders' decisions.
An example of a structured program of research is the four phases of clinical studies used by the Food and Drug Administration (FDA) to reach a decision about whether or not a new drug is safe and efficacious for market approval in the United States. Using this analogy, the final decision about whether a drug is efficacious and safe to be marketed for specific medical indications is based upon the accumulation of scientific evidence from a series of studies (i.e., not from any individual study), which are conducted in multiple sequential phases. The evidence generated in each phase is reviewed to make interim decisions about the safety and efficacy of a new pharmaceutical until ultimately all the evidence is reviewed to make a final decision about drug approval.
Under the FDA model for decisionmaking, initial research involves laboratory and animal tests. If the evidence generated in these studies indicates that the drug is active and not toxic, the sponsor submits an application to the FDA for an “investigational new drug.” If the FDA approves, human testing for safety and efficacy can begin. The first phase of human testing is usually conducted in a limited number of healthy volunteers (phase 1). If these trials show evidence that the product is safe in healthy volunteers, then the drug is further studied in a small number of volunteers who have the targeted condition (phase 2). If phase 2 studies show that the drug has a therapeutic effect and lacks significant adverse effects, trials with large numbers of people are conducted to determine the drug's safety and efficacy (phase 3). Following these trials, all relevant scientific studies are submitted to the FDA for a decision about whether the drug should be approved for marketing. If there are additional considerations like special safety issues, observational studies may be required to assess the safety of the drug in routine clinical care after the drug is approved for marketing (phase 4). Overall, the decisionmaking and research are staged so that the cumulative findings from all studies are used by the FDA to make interim decisions until the final decision is made about whether a medical product will be approved for marketing.
While most decisions about the comparative effectiveness of interventions will not need such extensive testing, it still may be prudent to stage research in a way that allows for interim decisions and sequentially more rigorous studies. On the other hand conditional approval or interim decisions may risk confusing patients and other stakeholders about the extent to which current evidence indicates that a treatment is effective and safe for all individuals with a health condition. For instance, under this staged approach new treatments could rapidly diffuse into a market even when there is limited evidence of long-term effectiveness and safety for all potential users. An illustrative example of this is the case of lung-volume reduction surgery, which was increasingly being used to treat severe emphysema despite limited evidence supporting its safety and efficacy until new research raised questions about the safety of the procedure. 6
Below is one potential categorization for the stages of knowledge development as related to informing decisions about questions of comparative effectiveness:
- Descriptive analysis
- Hypothesis generation
- Feasibility studies/proof of concept
- Hypothesis supporting
- Hypothesis testing
The first stages (i.e., descriptive analysis, hypothesis generation, and feasibility studies) are not mutually exclusive and usually are not intended to provide conclusive results for most decisions. Instead these stages provide preliminary evidence or feasibility testing before larger, more resource-intensive studies are launched. Results from these categories of studies may allow for interim decisionmaking (e.g., conditional approval for reimbursement of a treatment while further research is conducted). While a phased approach to research may postpone the time when a conclusive decision can be reached it does help to conserve resources such as those that may be consumed in launching a large multicenter study when a smaller study may be sufficient. Investigators will need to engage stakeholders to prioritize what stage of research may be most useful for the practical range of decisions that will be made.
Investigators should discuss in the protocol what stage of knowledge the current study will fulfill in light of the actions available to different stakeholders. This will allow reviewers of the protocol to assess the degree to which the evidence generated in the study holds the potential to fill specific knowledge gaps. For studies that are described in the protocol as preliminary, this may also help readers understand other tradeoffs that were made in the design of the study, in terms of methodological limitations that were accepted a priori in order to gather preliminary information about the research questions.
- Defining and Refining Study Questions Using PICOTS Framework
As recommended in other AHRQ methods guides, 7 investigators should engage stakeholders in a dialogue in order to understand the objectives of the research in practical terms, particularly so that investigators know the types of decisions that the research may affect. In working with stakeholders to develop research questions that can be studied with scientific methods, investigators may ask stakeholders to identify six key components of the research questions that will form the basis for designing the study. These components are reflected in the PICOTS typology and are shown below in Table 1.2 . These components represent the critical elements that will help investigators design a study that will be able to address the stakeholders' needs. Additional references that expand upon how to frame research questions can be found in the literature. 8 - 9
PICOTS typology for developing research questions.
The PICOTS typology outlines the key parts of the research questions that the study will be designed to address. 10 As a new research protocol is developed these questions can be presented in preliminary form and refined as other steps in the process are implemented. After the preliminary questions are refined, investigators should examine the questions to make sure that they will meet the needs of the stakeholders. In addition, they should assess whether the questions can be answered within the timeframe allotted and with the resources that are available for the study.
Since stakeholders ultimately determine effectiveness, it is important for investigators to ensure that the study endpoints and outcomes will meet their needs. Stakeholders need to articulate to investigators the health outcomes that are most important for a particular stakeholder to make decisions about treatment or take other health care actions. The endpoints that stakeholders will use to determine effectiveness may vary considerably. Unlike efficacy trials, in which clinical endpoints and surrogate measures are frequently used to determine efficacy, effectiveness may need to be determined based on several measures, many of which are not biological. These endpoints may be categorized as clinical endpoints, patient-reported outcomes and quality of life, health resource utilization, and utility measures. Types of measures that could be used are mortality, morbidity and adverse effects, quality of life, costs, or multiple outcomes. Chapter 6 gives a more extensive discussion of potential outcome measures of effectiveness.
The reliability, validity, and accuracy of study instruments to validly measure the concepts they purport to measure will also need to be acceptable to stakeholders. For instance, if stakeholders are interested in quality of life as an outcome, but do not believe there is an adequate measure of quality of life, then measurement development may need to be done prior to study initiation or other measures will need to be identified by stakeholders.
- Discussing Evidentiary Need and Uncertainty
Investigators and stakeholders should discuss the tradeoffs of different study designs that may be used for addressing the research questions. This dialogue will help researchers design a study that will be relevant and useful to the needs of stakeholders. All study designs have strengths and weaknesses, the latter of which may limit the conclusiveness of the final study results. Likewise, some decisions may require evidence that cannot be obtained from certain designs. In addition to design weaknesses, there are also practical tradeoffs that need to be considered in terms of research resources, like the time needed to complete the study, the availability of data, investigator expertise, subject recruitment, human subjects protection, research budget, difference to be detected, and lost-opportunity costs of doing the research instead of other studies that have priority for stakeholders. An important decision that will need to be made is whether or not randomization is needed for the questions being studied. There are several reasons why randomization might be needed, such as determining whether an FDA-approved drug can be used for a new use or indication that was not studied as part of the original drug approval process. A paper by Concato includes a thorough discussion of issues to consider when deciding whether randomization is necessary. 11
In discussing the tradeoffs of different study designs, researchers and stakeholders may wish to discuss the principal goals of research and ensure that researchers and stakeholders are aligned in their understanding of what is meant by scientific evidence. Fundamentally, research is a systematic investigation that uses scientific methods to measure, collect, and analyze data for the advancement of knowledge. This advancement is through the independent peer review and publication of study results, which are collectively referred to as scientific evidence. One definition of scientific evidence has been proposed by Normand and McNeil 12 as:
… the accumulation of information to support or refute a theory or hypothesis. … The idea is that assembling all the available information may reduce uncertainty about the effectiveness of the new technology compared to existing technologies in a setting where we believe particular relationships exist but are uncertain about their relevance …
While the primary aim of research is to produce new knowledge , the Normand and McNeil concept of evidence emphasizes that research helps create knowledge by reducing uncertainty about outcomes. However, rarely, if at all, does research eliminate all uncertainty around most decisions. In some cases, successful research will answer an important question and reduce uncertainty related to that question, but it may also increase uncertainty by leading to more, better informed questions regarding unknowns. As a result, nearly all decisions face some level of uncertainty even in a field where a body of research has been completed. This distinction is also critical because it helps to separate the research and subsequent actions that decisionmakers may take based on their assessment of the research results. Those subsequent actions may be informed by the research findings but will also be based on stakeholders' values and resources. Hence, as the definition by Normand and McNeil implies, research generates evidence but stakeholders decide whether to act on the evidence. Scientific evidence informs decisions to the extent it can adequately reduce the uncertainty about the problem for the stakeholder. Ultimately, treatment decisions are only guided by an assessment of the certainty that a course of therapy will lead to the outcomes of interest and the likelihood that this conclusion will be affected by the results of future studies.
In conceptualizing a study design, it is important for investigators to understand what constitutes sufficient and valid evidence from the stakeholder's perspective. In other words, what is the type of evidence that will be required to inform the stakeholder's decision to act or make a conscious decision not to take action? Evidence needed for action may vary by type of stakeholder and the scope of decisions that the stakeholder is making. For instance, a stakeholder who is making a population-based decision such as whether to provide insurance coverage for a new medical device with many alternatives may need substantially robust research findings in order to take action and provide that insurance coverage. In this example, the stakeholder may only accept as evidence a study with strong internal validity and generalizability (i.e., one conducted in a nationally representative sample of patients with the disease). On the other hand a patient who has a health condition where there are few treatments may be willing to accept lower-quality evidence in order to make a decision about whether to proceed with treatment despite a higher level of uncertainty about the outcome.
In many cases, there may exist a gradient of actions that can be taken based on available evidence. Quanstrum and Hayward 13 have discussed this gradient and argued that health care decisionmaking is changing, partly because more information is available to patients and other stakeholders about treatment options. As shown in the upper panel (A) in Figure 1.1 , many people may currently believe that health care treatment decisions are basically uniform for most people and under most circumstances. Panel A represents a hypothetical treatment whereby there is an evidentiary threshold or a point at which treatment is always beneficial and should be recommended. On the other hand below this threshold care provides no benefits and treatment should be discouraged. Quanstrum and Hayward argue that increasingly health care decisions are more like the lower panel (B). This panel portrays health care treatments as providing a large zone of discretion where benefits may be low or modest for most people. While above this zone treatment may always be recommended, individuals who fall within the zone may have questionable health benefits from treatment. As a result, different decisionmakers may take different actions based on their individual preferences.
Conceptualization of clinical decisionmaking. See Quanstrum KH, Hayward RA (Reference #). This figure is copyrighted by the Massachusetts Medical Society and reprinted with permission.
In light of this illustration, the following questions are suggested for discussion with stakeholders to help elicit the amount of uncertainty that is acceptable so that the study design can reach an appropriate level of evidence for the decision at hand:
- What level of new scientific evidence does the decisionmaker need to make a decision or take action?
- What quality of evidence is needed for the decisionmaker to act?
- What level of certainty of the outcome is needed by the decisionmaker(s)?
- How specific does the evidence need to be?
- Will decisions require consensus of multiple parties?
Additional Considerations When Considering Evidentiary Needs
As mentioned earlier, different stakeholders may disagree on the usefulness of different research designs, but it should be pointed out that this disagreement may be because stakeholders have different scopes of decisions to make. For example, high-quality research that is conclusive may be needed to make a decision that will affect the entire nation. On the other hand, results with more uncertainty as to the magnitude of the effect estimate(s) may be acceptable in making some decisions such as those affecting fewer people or where the risks to health are low. Often this disagreement occurs when different stakeholders debate whether evidence is needed from a new randomized controlled trial or whether evidence can be obtained from an analysis of an existing database. In this debate, both sides need to clarify whether they are facing the same decision or the decisions are different, particularly in terms of their scope.
Groups committed to evidence-based decisionmaking recognize that scientific evidence is only one component of the process of making decisions. Evidence generation is the goal of research, but evidence alone is not the only facet of evidence-based decisionmaking. In addition to scientific evidence, decisionmaking involves the consideration of (a) values, particularly the values placed on benefits and harms, and (b) resources. 14 Stakeholder differences in values and resources may mean that different decisions are made based on the same scientific evidence. Moreover, differences in values may create conflict in the decisionmaking process. One stakeholder may believe a particular study outcome is most important from their perspective, while another stakeholder may believe a different outcome is the most important for determining effectiveness.
Likewise, there may be inherent conflicts in values between individual decisionmaking and population decisionmaking, even though these decisions are often interrelated. For example, an individual may have a higher tolerance for treatment risk in light of the expected treatment benefits for him or her. On the other hand a regulatory health authority may determine that the population risk is too great without sufficient evidence that treatment provides benefits to the population. An example of this difference in perspective can be seen with how different decisionmakers responded to evidence about the drug Avastin ® (bevacizumab) for the treatment of metastatic breast cancer. In this case, the FDA revoked their approval of the breast cancer indication for Avastin after concluding that the drug had not been shown to be safe and effective for that use. Nonetheless, Medicare, the public insurance program for the elderly and disabled continued to allow coverage when a physician prescribes the drug, even for breast cancer. Likewise, some patient groups were reported to be concerned by the decision since it presumably would deny some women access to Avastin treatment. For a more thorough discussion of these issues around differences in perspective, the reader is referred to an article by Atkins 15 and the examples in Table 1.3 below.
Examples of individual versus population decisions (Adapted from Atkins, 2007).
- Specifying Magnitude of Effect
In order for decisions to be objective, it is important for there to be an a priori discussion with stakeholders about the magnitude of effect that stakeholders believe represents a meaningful difference between treatment options. Researchers will be familiar with the basic tenet that statistically significant differences do not always represent clinically meaningful differences. Hence, researchers and stakeholders will need to have knowledge of the instruments that are used to measure differences and the accuracy, limitations, and properties of those instruments. Three key questions are recommended to use when eliciting from stakeholders the effect sizes that are important to them for making a decision or taking action:
- How do patients and other stakeholders define a meaningful difference between interventions?
- How do previous studies and reviews define a meaningful difference?
- Are patients and other stakeholders interested in superiority or noninferiority as it relates to decisionmaking?
- Challenges to Developing Study Questions and Initial Solutions
In developing CER study objectives and questions, there are some potential challenges that face researchers and stakeholders. The involvement of patients and other stakeholders in determining study objectives and questions is a relatively new paradigm, but one that is consistent with established principles of translational research. A key principle of translational research is that users need to be involved in research at the earliest stages for the research to be adopted. 16 In addition, most research is currently initiated by an investigator, and traditionally there have been few incentives (and some disincentives) to involving others in designing a new research study. Although the research paradigm is rapidly shifting, 17 there is little information about how to structure, process, and evaluate outcomes from initiatives that attempt to engage stakeholders in developing study questions and objectives with researchers. As different approaches are taken to involve stakeholders in the research process, researchers will learn how to optimize the process of stakeholder involvement and improve the applicability of research to the end-users.
The bringing together of stakeholders may create some general challenges to the research team. For instance, it may be difficult to identify, engage, or manage all stakeholders who are interested in developing and using scientific evidence for addressing a problem. A process that allows for public commenting on research protocols through Internet postings may be helpful in reaching the widest network of interested stakeholders. Nevertheless, finding stakeholders who can represent all perspectives may not always be practical or available to the study team. In addition, competing interests among stakeholders may make prioritization of research questions challenging. Different stakeholders have different needs and this may make prioritization of research difficult. Nonetheless, as the science of translational research evolves, the collaboration of researchers with stakeholders will likely become increasingly the standard of practice in designing new research.
To assist researchers and stakeholders with working together, AHRQ has published several online resources to facilitate the involvement of stakeholders in the research process. These include a brief guide for stakeholders that highlights opportunities for taking part in AHRQ's Effective Health Care Program, a facilitation primer with strategies for working with diverse stakeholder groups, a table of suggested tasks for researchers to involve stakeholders in the identification and prioritization of future research, and learning modules with slide presentations on engaging stakeholders in the Effective Health Care Program. 18 - 19 In addition, AHRQ supports the Evidence-based Practice Centers in working with various stakeholders to further develop and prioritize decisionmakers' future research needs, which are published in a series of reports on AHRQ's Web site and on the National Library of Medicine's open-access Bookshelf. 20
Likewise, AHRQ supports the active involvement of patients and other stakeholders in the AHRQ DEcIDE program, in which different models of engagement have been used. These models include hosting in-person meetings with stakeholders to create research agendas; 21 - 22 developing research based on questions posed by public payers such as Centers for Medicare and Medicaid Services; addressing knowledge gaps that have been identified in AHRQ systematic reviews through new research; and supporting five research consortia, each of which involves researchers, patients, and other stakeholders working together to develop, prioritize, and implement research studies.
- Summary and Conclusion
This chapter provides a framework for formulating study objectives and questions, for a research protocol on a CER topic. Implementation of the framework involves collaboration between researchers and stakeholders in conceptualizing the research objectives and questions and the design of the study. In this process, there is a shared commitment to protect the integrity of the research results from bias and conflicts of interest, so that the results are valid for informing decisions and health care actions. Due to the complexity of some health care decisions, the evidence needed for decisionmaking or action may need to be developed from multiple studies, including preliminary research that becomes the underpinning for larger studies. The principles described in this chapter are intended to strengthen the writing of research protocols and enhance the results from the emanating studies, for informing the important decisions facing patients, providers, and other stakeholders about health care treatments and new technologies. Subsequent chapters in this User's Guide provide specific principles for operationalizing the study objectives and research questions in writing a complete study protocol that can be executed as new research.
Checklist: Guidance and key considerations for developing study objectives and questions for observational CER protocols
View in own window
Developing a Protocol for Observational Comparative Effectiveness Research: A User’s Guide is copyrighted by the Agency for Healthcare Research and Quality (AHRQ). The product and its contents may be used and incorporated into other materials on the following three conditions: (1) the contents are not changed in any way (including covers and front matter), (2) no fee is charged by the reproducer of the product or its contents for its use, and (3) the user obtains permission from the copyright holders identified therein for materials noted as copyrighted by others. The product may not be sold for profit or incorporated into any profitmaking venture without the expressed written permission of AHRQ.
- Cite this Page Smith SR. Study Objectives and Questions. In: Velentgas P, Dreyer NA, Nourjah P, et al., editors. Developing a Protocol for Observational Comparative Effectiveness Research: A User's Guide. Rockville (MD): Agency for Healthcare Research and Quality (US); 2013 Jan. Chapter 1.
- PDF version of this title (5.8M)
In this Page
Other titles in these collections.
- AHRQ Methods for Effective Health Care
- Health Services/Technology Assessment Text (HSTAT)
Related information
- PMC PubMed Central citations
- PubMed Links to PubMed
Recent Activity
- Study Objectives and Questions - Developing a Protocol for Observational Compara... Study Objectives and Questions - Developing a Protocol for Observational Comparative Effectiveness Research: A User's Guide
Your browsing activity is empty.
Activity recording is turned off.
Turn recording back on
Connect with NLM
National Library of Medicine 8600 Rockville Pike Bethesda, MD 20894
Web Policies FOIA HHS Vulnerability Disclosure
Help Accessibility Careers
Fats and Cholesterol
When it comes to dietary fat, what matters most is the type of fat you eat. Contrary to past dietary advice promoting low-fat diets , newer research shows that healthy fats are necessary and beneficial for health.
- When food manufacturers reduce fat, they often replace it with carbohydrates from sugar, refined grains, or other starches. Our bodies digest these refined carbohydrates and starches very quickly, affecting blood sugar and insulin levels and possibly resulting in weight gain and disease. ( 1-3 )
- Findings from the Nurses’ Health Study ( 4 ) and the Health Professionals Follow-up Study ( 5 ) show that no link between the overall percentage of calories from fat and any important health outcome, including cancer, heart disease, and weight gain.
Rather than adopting a low-fat diet, it’s more important to focus on eating beneficial “good” fats and avoiding harmful “bad” fats. Fat is an important part of a healthy diet. Choose foods with “good” unsaturated fats, limit foods high in saturated fat, and avoid “bad” trans fat.
- “Good” unsaturated fats — Monounsaturated and polyunsaturated fats — lower disease risk. Foods high in good fats include vegetable oils (such as olive, canola, sunflower, soy, and corn), nuts, seeds, and fish.
- “Bad” fats — trans fats — increase disease risk, even when eaten in small quantities. Foods containing trans fats are primarily in processed foods made with trans fat from partially hydrogenated oil. Fortunately, trans fats have been eliminated from many of these foods.
- Saturated fats , while not as harmful as trans fats, by comparison with unsaturated fats negatively impact health and are best consumed in moderation. Foods containing large amounts of saturated fat include red meat, butter, cheese, and ice cream. Some plant-based fats like coconut oil and palm oil are also rich in saturated fat.
- When you cut back on foods like red meat and butter, replace them with fish, beans, nuts, and healthy oils instead of refined carbohydrates.
Read more about healthy fats in this “Ask the Expert” with HSPH’s Dr. Walter Willett and Amy Myrdal Miller, M.S., R.D., formerly of The Culinary Institute of America
1. Siri-Tarino, P.W., et al., Saturated fatty acids and risk of coronary heart disease: modulation by replacement nutrients. Curr Atheroscler Rep, 2010. 12(6): p. 384-90.
2. Hu, F.B., Are refined carbohydrates worse than saturated fat? Am J Clin Nutr, 2010. 91(6): p. 1541-2.
3. Jakobsen, M.U., et al., Intake of carbohydrates compared with intake of saturated fatty acids and risk of myocardial infarction: importance of the glycemic index. Am J Clin Nutr, 2010. 91(6): p. 1764-8.
4. Hu, F.B., et al., Dietary fat intake and the risk of coronary heart disease in women. N Engl J Med, 1997. 337(21): p. 1491-9.
5. Ascherio, A., et al., Dietary fat and risk of coronary heart disease in men: cohort follow up study in the United States. BMJ, 1996. 313(7049): p. 84-90.
6. Hu, F.B., J.E. Manson, and W.C. Willett, Types of dietary fat and risk of coronary heart disease: a critical review. J Am Coll Nutr, 2001. 20(1): p. 5-19.
Terms of Use
The contents of this website are for educational purposes and are not intended to offer personal medical advice. You should seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website. The Nutrition Source does not recommend or endorse any products.
IMAGES
VIDEO
COMMENTS
Example: Research aim. To examine contributory factors to muscle retention in a group of elderly people. Example: Research objectives. To assess the relationship between sedentary habits and muscle atrophy among the participants. To determine the impact of dietary factors, particularly protein consumption, on the muscular health of the ...
Formulating research objectives has the following five steps, which could help researchers develop a clear objective: 8. Identify the research problem. Review past studies on subjects similar to your problem statement, that is, studies that use similar methods, variables, etc.
The research aim provides the study with direction, while the research objectives set the path to achieving this aim, thereby ensuring the study's efficiency and effectiveness. How to Write Research Objectives. I usually recommend to my students that they use the SMART framework to create their research objectives.
A research objective is defined as a clear and concise statement of the specific goals and aims of a research study. It outlines what the researcher intends to accomplish and what they hope to learn or discover through their research. Research objectives are crucial for guiding the research process and ensuring that the study stays focused and ...
Research Objectives. Research objectives refer to the specific goals or aims of a research study. They provide a clear and concise description of what the researcher hopes to achieve by conducting the research.The objectives are typically based on the research questions and hypotheses formulated at the beginning of the study and are used to guide the research process.
Research Aims: Examples. True to the name, research aims usually start with the wording "this research aims to…", "this research seeks to…", and so on. For example: "This research aims to explore employee experiences of digital transformation in retail HR.". "This study sets out to assess the interaction between student ...
Summary. The importance of research aims and objectives cannot be over-stressed. It is vital to have a very clear understanding of what the research is about and what you are actually trying to achieve. You need to know this. And you need to be able to communicate it to others. Carrying out a research project is rather like going on a journey.
For example, with clear research objectives, your study focuses on the specific goals you want to achieve and prevents you from spending time and resources collecting unnecessary data. However, sticking to research objectives isn't always easy, especially in broad or unconventional research. This is why most researchers follow the SMART ...
Learn how to write clear and concise research aims and objectives with this step-by-step guide from SAGE methods.
To develop a set of research objectives, you would then break down the various steps involved in meeting said aim. For example: This study will investigate the link between dehydration and the incidence of urinary tract infections (UTIs) in intensive care patients in Australia. To achieve this, the study objectives w ill include:
A research aim is a broad statement indicating the general purpose of your research project. It should appear in your introduction at the end of your problem statement, before your research objectives. Research objectives are more specific than your research aim. They indicate the specific ways you'll address the overarching aim.
Summary. One of the most important aspects of a thesis, dissertation or research paper is the correct formulation of the aims and objectives. This is because your aims and objectives will establish the scope, depth and direction that your research will ultimately take. An effective set of aims and objectives will give your research focus and ...
Research objectives are integral to the research framework as the nexus between the research problem, questions, and hypotheses. They translate the broad goals of your study into actionable steps, ensuring every aspect of your research is purposefully aligned towards addressing the research problem.
Steps for Writing Objectives in Research Paper. 1. Identify the Research Topic: Clearly define the subject or topic of your research. This will provide a broad context for developing specific research objectives. 2. Conduct a Literature Review. Review existing literature and research related to your topic.
INTRODUCTION. Scientific research is usually initiated by posing evidenced-based research questions which are then explicitly restated as hypotheses.1,2 The hypotheses provide directions to guide the study, solutions, explanations, and expected results.3,4 Both research questions and hypotheses are essentially formulated based on conventional theories and real-world processes, which allow the ...
The development of the research question, including a supportive hypothesis and objectives, is a necessary key step in producing clinically relevant results to be used in evidence-based practice. A well-defined and specific research question is more likely to help guide us in making decisions about study design and population and subsequently ...
Answer: Research objectives describe concisely what the research is trying to achieve. They summarize the accomplishments a researcher wishes to achieve through the project and provides direction to the study. A research objective must be achievable, i.e., it must be framed keeping in mind the available time, infrastructure required for ...
5 Examples of Research Objectives. The following examples of research objectives based on several published studies on various topics demonstrate how the research objectives are written: This study aims to find out if there is a difference in quiz scores between students exposed to direct instruction and flipped classrooms (Webb and Doman, 2016).
Research aims and objectives are the foundation of any research project. They provide a clear direction and purpose for the study, ensuring that you stay focused and on track throughout the process. They are your trusted navigational tools, leading you to success. Understanding the relationship between research objectives and aims is crucial to ...
Here are three simple steps that you can follow to identify and write your research objectives: 1. Pinpoint the major focus of your research. The first step to writing your research objectives is to pinpoint the major focus of your research project. In this step, make sure to clearly describe what you aim to achieve through your research.
A research design is a strategy for answering your research question using empirical data. Creating a research design means making decisions about: Your overall research objectives and approach. Whether you'll rely on primary research or secondary research. Your sampling methods or criteria for selecting subjects. Your data collection methods.
Moreover, the research objectives should be framed by the researcher before the initiation of the study: a specific, measurable, achievable, realistic, and time-defined (SMART) approach is utilized to devise the objectives based on the research question. It is preferable to have a single primary objective whereas the secondary objectives can be ...
Study objectives: Astrocytes change their intracellular calcium (Ca2+) concentration during sleep/wakefulness states in mice. Furthermore, the Ca2+ dynamics in astrocytes vary depending on the brain region. However, whether alterations in intracellular Ca2+ concentration in astrocytes can affect sleep/wakefulness states and cortical oscillations in a brain region-dependent manner remain unclear.
Objective: This study aimed to examine the reliability, validity, and measurement invariance of the eHealth Literacy Scale-Web3. (eHLS-Web3.0) among older adults with NCDs. Methods: A total of 642 Chinese older adults with NCDs (mean age 65.78, SD 3.91 years; 55.8% female) were recruited in the baseline assessment, of whom 134 (mean age 65.63 ...
Hence, the objectives of this systematic review and meta-analysis were to determine the pooled proportion ofturnover intention among nurses and to identify factors associated to it in Ethiopia. A comprehensive search carried out for studies with full document and written in English language through an electronic web-based search strategy from ...
Introduction Solving disparities in assessments is crucial to a successful surgical training programme. The first step in levelling these inequalities is recognising in what contexts they occur, and what protected characteristics are potentially implicated. Methods This scoping review was based on Arksey & O'Malley's guiding principles. OVID and Embase were used to identify articles, which ...
Objective The primary objective of this cross-sectional study was to compare standard laboratory performance metrics of transgender athletes to cisgender athletes. Methods 19 cisgender men (CM) (mean±SD, age: 37±9 years), 12 transgender men (TM) (age: 34±7 years), 23 transgender women (TW) (age: 34±10 years) and 21 cisgender women (CW) (age: 30±9 years) underwent a series of standard ...
The steps involved in the process of developing research questions and study objectives for conducting observational comparative effectiveness research (CER) are described in this chapter. It is important to begin with identifying decisions under consideration, determining who the decisionmakers and stakeholders in the specific area of research under study are, and understanding the context in ...
New research into B2B content marketing trends for 2024 reveals specifics of AI implementation, social media use, and budget forecasts, plus content success factors. ... (84%, up from 75% last year), and case studies/customer stories (78%, up from 67% last year). Almost three-quarters (71%) use long articles, 60% produce visual content, and 59% ...
Fats and Cholesterol. When it comes to dietary fat, what matters most is the type of fat you eat. Contrary to past dietary advice promoting low-fat diets, newer research shows that healthy fats are necessary and beneficial for health. When food manufacturers reduce fat, they often replace it with carbohydrates from sugar, refined grains, or ...