

Organizing Your Social Sciences Research Paper: Writing a Case Study
- Purpose of Guide
- Design Flaws to Avoid
- Independent and Dependent Variables
- Glossary of Research Terms
- Narrowing a Topic Idea
- Broadening a Topic Idea
- Extending the Timeliness of a Topic Idea
- Academic Writing Style
- Choosing a Title
- Making an Outline
- Paragraph Development
- Executive Summary
- The C.A.R.S. Model
- Background Information
- The Research Problem/Question
- Theoretical Framework
- Citation Tracking
- Content Alert Services
- Evaluating Sources
- Reading Research Effectively
- Primary Sources
- Secondary Sources
- Tiertiary Sources
- What Is Scholarly vs. Popular?
- Qualitative Methods
- Quantitative Methods
- Using Non-Textual Elements
- Limitations of the Study
- Common Grammar Mistakes
- Writing Concisely
- Avoiding Plagiarism
- Footnotes or Endnotes?
- Further Readings
- Annotated Bibliography
- Dealing with Nervousness
- Using Visual Aids
- Grading Someone Else's Paper
- Types of Structured Group Activities
- Group Project Survival Skills
- Multiple Book Review Essay
- Reviewing Collected Essays
- Writing a Case Study
- About Informed Consent
- Writing Field Notes
- Writing a Policy Memo
- Writing a Research Proposal
- Bibliography
The term case study refers to both a method of analysis and a specific research design for examining a problem, both of which are used in most circumstances to generalize across populations. This tab focuses on the latter--how to design and organize a research paper in the social sciences that analyzes a specific case.
A case study research paper examines a person, place, event, phenomenon, or other type of subject of analysis in order to extrapolate key themes and results that help predict future trends, illuminate previously hidden issues that can be applied to practice, and/or provide a means for understanding an important research problem with greater clarity. A case study paper usually examines a single subject of analysis, but case study papers can also be designed as a comparative investigation that shows relationships between two or among more than two subjects. The methods used to study a case can rest within a quantitative, qualitative, or mixed-method investigative paradigm.
Case Studies . Writing@CSU. Colorado State University; Mills, Albert J. , Gabrielle Durepos, and Eiden Wiebe, editors. Encyclopedia of Case Study Research . Thousand Oaks, CA: SAGE Publications, 2010 ; “What is a Case Study?” In Swanborn, Peter G. Case Study Research: What, Why and How? London: SAGE, 2010.
How to Approach Writing a Case Study Research Paper
General information about how to choose a topic to investigate can be found under the " Choosing a Research Problem " tab in this writing guide. Review this page because it may help you identify a subject of analysis that can be investigated using a single case study design.
However, identifying a case to investigate involves more than choosing the research problem . A case study encompasses a problem contextualized around the application of in-depth analysis, interpretation, and discussion, often resulting in specific recommendations for action or for improving existing conditions. As Seawright and Gerring note, practical considerations such as time and access to information can influence case selection, but these issues should not be the sole factors used in describing the methodological justification for identifying a particular case to study. Given this, selecting a case includes considering the following:
- Does the case represent an unusual or atypical example of a research problem that requires more in-depth analysis? Cases often represent a topic that rests on the fringes of prior investigations because the case may provide new ways of understanding the research problem. For example, if the research problem is to identify strategies to improve policies that support girl's access to secondary education in predominantly Muslim nations, you could consider using Azerbaijan as a case study rather than selecting a more obvious nation in the Middle East. Doing so may reveal important new insights into recommending how governments in other predominantly Muslim nations can formulate policies that support improved access to education for girls.
- Does the case provide important insight or illuminate a previously hidden problem? In-depth analysis of a case can be based on the hypothesis that the case study will reveal trends or issues that have not been exposed in prior research or will reveal new and important implications for practice. For example, anecdotal evidence may suggest drug use among homeless veterans is related to their patterns of travel throughout the day. Assuming prior studies have not looked at individual travel choices as a way to study access to illicit drug use, a case study that observes a homeless veteran could reveal how issues of personal mobility choices facilitate regular access to illicit drugs. Note that it is important to conduct a thorough literature review to ensure that your assumption about the need to reveal new insights or previously hidden problems is valid and evidence-based.
- Does the case challenge and offer a counter-point to prevailing assumptions? Over time, research on any given topic can fall into a trap of developing assumptions based on outdated studies that are still applied to new or changing conditions or the idea that something should simply be accepted as "common sense," even though the issue has not been thoroughly tested in practice. A case may offer you an opportunity to gather evidence that challenges prevailing assumptions about a research problem and provide a new set of recommendations applied to practice that have not been tested previously. For example, perhaps there has been a long practice among scholars to apply a particular theory in explaining the relationship between two subjects of analysis. Your case could challenge this assumption by applying an innovative theoretical framework [perhaps borrowed from another discipline] to the study a case in order to explore whether this approach offers new ways of understanding the research problem. Taking a contrarian stance is one of the most important ways that new knowledge and understanding develops from existing literature.
- Does the case provide an opportunity to pursue action leading to the resolution of a problem? Another way to think about choosing a case to study is to consider how the results from investigating a particular case may result in findings that reveal ways in which to resolve an existing or emerging problem. For example, studying the case of an unforeseen incident, such as a fatal accident at a railroad crossing, can reveal hidden issues that could be applied to preventative measures that contribute to reducing the chance of accidents in the future. In this example, a case study investigating the accident could lead to a better understanding of where to strategically locate additional signals at other railroad crossings in order to better warn drivers of an approaching train, particularly when visibility is hindered by heavy rain, fog, or at night.
- Does the case offer a new direction in future research? A case study can be used as a tool for exploratory research that points to a need for further examination of the research problem. A case can be used when there are few studies that help predict an outcome or that establish a clear understanding about how best to proceed in addressing a problem. For example, after conducting a thorough literature review [very important!], you discover that little research exists showing the ways in which women contribute to promoting water conservation in rural communities of Uganda. A case study of how women contribute to saving water in a particular village can lay the foundation for understanding the need for more thorough research that documents how women in their roles as cooks and family caregivers think about water as a valuable resource within their community throughout rural regions of east Africa. The case could also point to the need for scholars to apply feminist theories of work and family to the issue of water conservation.
Eisenhardt, Kathleen M. “Building Theories from Case Study Research.” Academy of Management Review 14 (October 1989): 532-550; Emmel, Nick. Sampling and Choosing Cases in Qualitative Research: A Realist Approach . Thousand Oaks, CA: SAGE Publications, 2013; Gerring, John. “What Is a Case Study and What Is It Good for?” American Political Science Review 98 (May 2004): 341-354; Mills, Albert J. , Gabrielle Durepos, and Eiden Wiebe, editors. Encyclopedia of Case Study Research . Thousand Oaks, CA: SAGE Publications, 2010; Seawright, Jason and John Gerring. "Case Selection Techniques in Case Study Research." Political Research Quarterly 61 (June 2008): 294-308.
Structure and Writing Style
The purpose of a paper in the social sciences designed around a case study is to thoroughly investigate a subject of analysis in order to reveal a new understanding about the research problem and, in so doing, contributing new knowledge to what is already known from previous studies. In applied social sciences disciplines [e.g., education, social work, public administration, etc.], case studies may also be used to reveal best practices, highlight key programs, or investigate interesting aspects of professional work. In general, the structure of a case study research paper is not all that different from a standard college-level research paper. However, there are subtle differences you should be aware of. Here are the key elements to organizing and writing a case study research paper.
I. Introduction
As with any research paper, your introduction should serve as a roadmap for your readers to ascertain the scope and purpose of your study . The introduction to a case study research paper, however, should not only describe the research problem and its significance, but you should also succinctly describe why the case is being used and how it relates to addressing the problem. The two elements should be linked. With this in mind, a good introduction answers these four questions:
- What was I studying? Describe the research problem and describe the subject of analysis you have chosen to address the problem. Explain how they are linked and what elements of the case will help to expand knowledge and understanding about the problem.
- Why was this topic important to investigate? Describe the significance of the research problem and state why a case study design and the subject of analysis that the paper is designed around is appropriate in addressing the problem.
- What did we know about this topic before I did this study? Provide background that helps lead the reader into the more in-depth literature review to follow. If applicable, summarize prior case study research applied to the research problem and why it fails to adequately address the research problem. Describe why your case will be useful. If no prior case studies have been used to address the research problem, explain why you have selected this subject of analysis.
- How will this study advance new knowledge or new ways of understanding? Explain why your case study will be suitable in helping to expand knowledge and understanding about the research problem.
Each of these questions should be addressed in no more than a few paragraphs. Exceptions to this can be when you are addressing a complex research problem or subject of analysis that requires more in-depth background information.
II. Literature Review
The literature review for a case study research paper is generally structured the same as it is for any college-level research paper. The difference, however, is that the literature review is focused on providing background information and enabling historical interpretation of the subject of analysis in relation to the research problem the case is intended to address . This includes synthesizing studies that help to:
- Place relevant works in the context of their contribution to understanding the case study being investigated . This would include summarizing studies that have used a similar subject of analysis to investigate the research problem. If there is literature using the same or a very similar case to study, you need to explain why duplicating past research is important [e.g., conditions have changed; prior studies were conducted long ago, etc.].
- Describe the relationship each work has to the others under consideration that informs the reader why this case is applicable . Your literature review should include a description of any works that support using the case to study the research problem and the underlying research questions.
- Identify new ways to interpret prior research using the case study . If applicable, review any research that has examined the research problem using a different research design. Explain how your case study design may reveal new knowledge or a new perspective or that can redirect research in an important new direction.
- Resolve conflicts amongst seemingly contradictory previous studies . This refers to synthesizing any literature that points to unresolved issues of concern about the research problem and describing how the subject of analysis that forms the case study can help resolve these existing contradictions.
- Point the way in fulfilling a need for additional research . Your review should examine any literature that lays a foundation for understanding why your case study design and the subject of analysis around which you have designed your study may reveal a new way of approaching the research problem or offer a perspective that points to the need for additional research.
- Expose any gaps that exist in the literature that the case study could help to fill . Summarize any literature that not only shows how your subject of analysis contributes to understanding the research problem, but how your case contributes to a new way of understanding the problem that prior research has failed to do.
- Locate your own research within the context of existing literature [very important!] . Collectively, your literature review should always place your case study within the larger domain of prior research about the problem. The overarching purpose of reviewing pertinent literature in a case study paper is to demonstrate that you have thoroughly identified and synthesized prior studies in the context of explaining the relevance of the case in addressing the research problem.
III. Method
In this section, you explain why you selected a particular subject of analysis to study and the strategy you used to identify and ultimately decide that your case was appropriate in addressing the research problem. The way you describe the methods used varies depending on the type of subject of analysis that frames your case study.
If your subject of analysis is an incident or event . In the social and behavioral sciences, the event or incident that represents the case to be studied is usually bounded by time and place, with a clear beginning and end and with an identifiable location or position relative to its surroundings. The subject of analysis can be a rare or critical event or it can focus on a typical or regular event. The purpose of studying a rare event is to illuminate new ways of thinking about the broader research problem or to test a hypothesis. Critical incident case studies must describe the method by which you identified the event and explain the process by which you determined the validity of this case to inform broader perspectives about the research problem or to reveal new findings. However, the event does not have to be a rare or uniquely significant to support new thinking about the research problem or to challenge an existing hypothesis. For example, Walo, Bull, and Breen conducted a case study to identify and evaluate the direct and indirect economic benefits and costs of a local sports event in the City of Lismore, New South Wales, Australia. The purpose of their study was to provide new insights from measuring the impact of a typical local sports event that prior studies could not measure well because they focused on large "mega-events." Whether the event is rare or not, the methods section should include an explanation of the following characteristics of the event: a) when did it take place; b) what were the underlying circumstances leading to the event; c) what were the consequences of the event.
If your subject of analysis is a person. Explain why you selected this particular individual to be studied and describe what experience he or she has had that provides an opportunity to advance new understandings about the research problem. Mention any background about this person which might help the reader understand the significance of his/her experiences that make them worthy of study. This includes describing the relationships this person has had with other people, institutions, and/or events that support using him or her as the subject for a case study research paper. It is particularly important to differentiate the person as the subject of analysis from others and to succinctly explain how the person relates to examining the research problem.
If your subject of analysis is a place. In general, a case study that investigates a place suggests a subject of analysis that is unique or special in some way and that this uniqueness can be used to build new understanding or knowledge about the research problem. A case study of a place must not only describe its various attributes relevant to the research problem [e.g., physical, social, cultural, economic, political, etc.], but you must state the method by which you determined that this place will illuminate new understandings about the research problem. It is also important to articulate why a particular place as the case for study is being used if similar places also exist [i.e., if you are studying patterns of homeless encampments of veterans in open spaces, why study Echo Park in Los Angeles rather than Griffith Park?]. If applicable, describe what type of human activity involving this place makes it a good choice to study [e.g., prior research reveals Echo Park has more homeless veterans].
If your subject of analysis is a phenomenon. A phenomenon refers to a fact, occurrence, or circumstance that can be studied or observed but with the cause or explanation to be in question. In this sense, a phenomenon that forms your subject of analysis can encompass anything that can be observed or presumed to exist but is not fully understood. In the social and behavioral sciences, the case usually focuses on human interaction within a complex physical, social, economic, cultural, or political system. For example, the phenomenon could be the observation that many vehicles used by ISIS fighters are small trucks with English language advertisements on them. The research problem could be that ISIS fighters are difficult to combat because they are highly mobile. The research questions could be how and by what means are these vehicles used by ISIS being supplied to the militants and how might supply lines to these vehicles be cut? How might knowing the suppliers of these trucks from overseas reveal larger networks of collaborators and financial support? A case study of a phenomenon most often encompasses an in-depth analysis of a cause and effect that is grounded in an interactive relationship between people and their environment in some way.
NOTE: The choice of the case or set of cases to study cannot appear random. Evidence that supports the method by which you identified and chose your subject of analysis should be linked to the findings from the literature review. Be sure to cite any prior studies that helped you determine that the case you chose was appropriate for investigating the research problem.
IV. Discussion
The main elements of your discussion section are generally the same as any research paper, but centered around interpreting and drawing conclusions about the key findings from your case study. Note that a general social sciences research paper may contain a separate section to report findings. However, in a paper designed around a case study, it is more common to combine a description of the findings with the discussion about their implications. The objectives of your discussion section should include the following:
Reiterate the Research Problem/State the Major Findings Briefly reiterate the research problem you are investigating and explain why the subject of analysis around which you designed the case study were used. You should then describe the findings revealed from your study of the case using direct, declarative, and succinct proclamation of the study results. Highlight any findings that were unexpected or especially profound.
Explain the Meaning of the Findings and Why They are Important Systematically explain the meaning of your case study findings and why you believe they are important. Begin this part of the section by repeating what you consider to be your most important or surprising finding first, then systematically review each finding. Be sure to thoroughly extrapolate what your analysis of the case can tell the reader about situations or conditions beyond the actual case that was studied while, at the same time, being careful not to misconstrue or conflate a finding that undermines the external validity of your conclusions.
Relate the Findings to Similar Studies No study in the social sciences is so novel or possesses such a restricted focus that it has absolutely no relation to previously published research. The discussion section should relate your case study results to those found in other studies, particularly if questions raised from prior studies served as the motivation for choosing your subject of analysis. This is important because comparing and contrasting the findings of other studies helps to support the overall importance of your results and it highlights how and in what ways your case study design and the subject of analysis differs from prior research about the topic.
Consider Alternative Explanations of the Findings It is important to remember that the purpose of social science research is to discover and not to prove. When writing the discussion section, you should carefully consider all possible explanations for the case study results, rather than just those that fit your hypothesis or prior assumptions and biases. Be alert to what the in-depth analysis of the case may reveal about the research problem, including offering a contrarian perspective to what scholars have stated in prior research.
Acknowledge the Study's Limitations You can state the study's limitations in the conclusion section of your paper but describing the limitations of your subject of analysis in the discussion section provides an opportunity to identify the limitations and explain why they are not significant. This part of the discussion section should also note any unanswered questions or issues your case study could not address. More detailed information about how to document any limitations to your research can be found here .
Suggest Areas for Further Research Although your case study may offer important insights about the research problem, there are likely additional questions related to the problem that remain unanswered or findings that unexpectedly revealed themselves as a result of your in-depth analysis of the case. Be sure that the recommendations for further research are linked to the research problem and that you explain why your recommendations are valid in other contexts and based on the original assumptions of your study.
V. Conclusion
As with any research paper, you should summarize your conclusion in clear, simple language; emphasize how the findings from your case study differs from or supports prior research and why. Do not simply reiterate the discussion section. Provide a synthesis of key findings presented in the paper to show how these converge to address the research problem. If you haven't already done so in the discussion section, be sure to document the limitations of your case study and needs for further research.
The function of your paper's conclusion is to: 1) restate the main argument supported by the findings from the analysis of your case; 2) clearly state the context, background, and necessity of pursuing the research problem using a case study design in relation to an issue, controversy, or a gap found from reviewing the literature; and, 3) provide a place for you to persuasively and succinctly restate the significance of your research problem, given that the reader has now been presented with in-depth information about the topic.
Consider the following points to help ensure your conclusion is appropriate:
- If the argument or purpose of your paper is complex, you may need to summarize these points for your reader.
- If prior to your conclusion, you have not yet explained the significance of your findings or if you are proceeding inductively, use the conclusion of your paper to describe your main points and explain their significance.
- Move from a detailed to a general level of consideration of the case study's findings that returns the topic to the context provided by the introduction or within a new context that emerges from your case study findings.
Note that, depending on the discipline you are writing in and your professor's preferences, the concluding paragraph may contain your final reflections on the evidence presented applied to practice or on the essay's central research problem. However, the nature of being introspective about the subject of analysis you have investigated will depend on whether you are explicitly asked to express your observations in this way.
Problems to Avoid
Overgeneralization One of the goals of a case study is to lay a foundation for understanding broader trends and issues applied to similar circumstances. However, be careful when drawing conclusions from your case study. They must be evidence-based and grounded in the results of the study; otherwise, it is merely speculation. Looking at a prior example, it would be incorrect to state that a factor in improving girls access to education in Azerbaijan and the policy implications this may have for improving access in other Muslim nations is due to girls access to social media if there is no documentary evidence from your case study to indicate this. There may be anecdotal evidence that retention rates were better for girls who were on social media, but this observation would only point to the need for further research and would not be a definitive finding if this was not a part of your original research agenda.
Failure to Document Limitations No case is going to reveal all that needs to be understood about a research problem. Therefore, just as you have to clearly state the limitations of a general research study , you must describe the specific limitations inherent in the subject of analysis. For example, the case of studying how women conceptualize the need for water conservation in a village in Uganda could have limited application in other cultural contexts or in areas where fresh water from rivers or lakes is plentiful and, therefore, conservation is understood differently than preserving access to a scarce resource.
Failure to Extrapolate All Possible Implications Just as you don't want to over-generalize from your case study findings, you also have to be thorough in the consideration of all possible outcomes or recommendations derived from your findings. If you do not, your reader may question the validity of your analysis, particularly if you failed to document an obvious outcome from your case study research. For example, in the case of studying the accident at the railroad crossing to evaluate where and what types of warning signals should be located, you failed to take into consideration speed limit signage as well as warning signals. When designing your case study, be sure you have thoroughly addressed all aspects of the problem and do not leave gaps in your analysis.
Case Studies . Writing@CSU. Colorado State University; Gerring, John. Case Study Research: Principles and Practices . New York: Cambridge University Press, 2007; Merriam, Sharan B. Qualitative Research and Case Study Applications in Education . Rev. ed. San Francisco, CA: Jossey-Bass, 1998; Miller, Lisa L. “The Use of Case Studies in Law and Social Science Research.” Annual Review of Law and Social Science 14 (2018): TBD; Mills, Albert J., Gabrielle Durepos, and Eiden Wiebe, editors. Encyclopedia of Case Study Research . Thousand Oaks, CA: SAGE Publications, 2010; Putney, LeAnn Grogan. "Case Study." In Encyclopedia of Research Design , Neil J. Salkind, editor. (Thousand Oaks, CA: SAGE Publications, 2010), pp. 116-120; Simons, Helen. Case Study Research in Practice . London: SAGE Publications, 2009; Kratochwill, Thomas R. and Joel R. Levin, editors. Single-Case Research Design and Analysis: New Development for Psychology and Education . Hilldsale, NJ: Lawrence Erlbaum Associates, 1992; Swanborn, Peter G. Case Study Research: What, Why and How? London : SAGE, 2010; Yin, Robert K. Case Study Research: Design and Methods . 6th edition. Los Angeles, CA, SAGE Publications, 2014; Walo, Maree, Adrian Bull, and Helen Breen. “Achieving Economic Benefits at Local Events: A Case Study of a Local Sports Event.” Festival Management and Event Tourism 4 (1996): 95-106.
Writing Tip
At Least Five Misconceptions about Case Study Research
Social science case studies are often perceived as limited in their ability to create new knowledge because they are not randomly selected and findings cannot be generalized to larger populations. Flyvbjerg examines five misunderstandings about case study research and systematically "corrects" each one. To quote, these are:
Misunderstanding 1 : General, theoretical [context-independent knowledge is more valuable than concrete, practical (context-dependent) knowledge. Misunderstanding 2 : One cannot generalize on the basis of an individual case; therefore, the case study cannot contribute to scientific development. Misunderstanding 3 : The case study is most useful for generating hypotheses; that is, in the first stage of a total research process, whereas other methods are more suitable for hypotheses testing and theory building. Misunderstanding 4 : The case study contains a bias toward verification, that is, a tendency to confirm the researcher’s preconceived notions. Misunderstanding 5 : It is often difficult to summarize and develop general propositions and theories on the basis of specific case studies [p. 221].
While writing your paper, think introspectively about how you addressed these misconceptions because to do so can help you strengthen the validity and reliability of your research by clarifying issues of case selection, the testing and challenging of existing assumptions, the interpretation of key findings, and the summation of case outcomes. Think of a case study research paper as a complete, in-depth narrative about the specific properties and key characteristics of your subject of analysis applied to the research problem.
Flyvbjerg, Bent. “Five Misunderstandings About Case-Study Research.” Qualitative Inquiry 12 (April 2006): 219-245.
- << Previous: Reviewing Collected Essays
- Next: Writing a Field Report >>
- Last Updated: Jan 17, 2023 10:50 AM
- URL: https://libguides.pointloma.edu/ResearchPaper

The Ultimate Guide to Qualitative Research - Part 1: The Basics

- Introduction and overview
- What is qualitative research?
- What is qualitative data?
- Examples of qualitative data
- Qualitative vs. quantitative research
- Mixed methods
- Qualitative research preparation
- Theoretical perspective
- Theoretical framework
- Literature reviews
Research question
- Conceptual framework
- Conceptual vs. theoretical framework
Data collection
- Qualitative research methods
- Focus groups
- Observational research
What is a case study?
Applications for case study research, what is a good case study, process of case study design, benefits and limitations of case studies.
- Ethnographical research
- Ethical considerations
- Confidentiality and privacy
- Power dynamics
- Reflexivity
Case studies
Case studies are essential to qualitative research , offering a lens through which researchers can investigate complex phenomena within their real-life contexts. This chapter explores the concept, purpose, applications, examples, and types of case studies and provides guidance on how to conduct case study research effectively.

Whereas quantitative methods look at phenomena at scale, case study research looks at a concept or phenomenon in considerable detail. While analyzing a single case can help understand one perspective regarding the object of research inquiry, analyzing multiple cases can help obtain a more holistic sense of the topic or issue. Let's provide a basic definition of a case study, then explore its characteristics and role in the qualitative research process.
Definition of a case study
A case study in qualitative research is a strategy of inquiry that involves an in-depth investigation of a phenomenon within its real-world context. It provides researchers with the opportunity to acquire an in-depth understanding of intricate details that might not be as apparent or accessible through other methods of research. The specific case or cases being studied can be a single person, group, or organization – demarcating what constitutes a relevant case worth studying depends on the researcher and their research question .
Among qualitative research methods , a case study relies on multiple sources of evidence, such as documents, artifacts, interviews , or observations , to present a complete and nuanced understanding of the phenomenon under investigation. The objective is to illuminate the readers' understanding of the phenomenon beyond its abstract statistical or theoretical explanations.
Characteristics of case studies
Case studies typically possess a number of distinct characteristics that set them apart from other research methods. These characteristics include a focus on holistic description and explanation, flexibility in the design and data collection methods, reliance on multiple sources of evidence, and emphasis on the context in which the phenomenon occurs.
Furthermore, case studies can often involve a longitudinal examination of the case, meaning they study the case over a period of time. These characteristics allow case studies to yield comprehensive, in-depth, and richly contextualized insights about the phenomenon of interest.
The role of case studies in research
Case studies hold a unique position in the broader landscape of research methods aimed at theory development. They are instrumental when the primary research interest is to gain an intensive, detailed understanding of a phenomenon in its real-life context.
In addition, case studies can serve different purposes within research - they can be used for exploratory, descriptive, or explanatory purposes, depending on the research question and objectives. This flexibility and depth make case studies a valuable tool in the toolkit of qualitative researchers.
Remember, a well-conducted case study can offer a rich, insightful contribution to both academic and practical knowledge through theory development or theory verification, thus enhancing our understanding of complex phenomena in their real-world contexts.
What is the purpose of a case study?
Case study research aims for a more comprehensive understanding of phenomena, requiring various research methods to gather information for qualitative analysis . Ultimately, a case study can allow the researcher to gain insight into a particular object of inquiry and develop a theoretical framework relevant to the research inquiry.
Why use case studies in qualitative research?
Using case studies as a research strategy depends mainly on the nature of the research question and the researcher's access to the data.
Conducting case study research provides a level of detail and contextual richness that other research methods might not offer. They are beneficial when there's a need to understand complex social phenomena within their natural contexts.
The explanatory, exploratory, and descriptive roles of case studies
Case studies can take on various roles depending on the research objectives. They can be exploratory when the research aims to discover new phenomena or define new research questions; they are descriptive when the objective is to depict a phenomenon within its context in a detailed manner; and they can be explanatory if the goal is to understand specific relationships within the studied context. Thus, the versatility of case studies allows researchers to approach their topic from different angles, offering multiple ways to uncover and interpret the data .
The impact of case studies on knowledge development
Case studies play a significant role in knowledge development across various disciplines. Analysis of cases provides an avenue for researchers to explore phenomena within their context based on the collected data.

This can result in the production of rich, practical insights that can be instrumental in both theory-building and practice. Case studies allow researchers to delve into the intricacies and complexities of real-life situations, uncovering insights that might otherwise remain hidden.
Types of case studies
In qualitative research , a case study is not a one-size-fits-all approach. Depending on the nature of the research question and the specific objectives of the study, researchers might choose to use different types of case studies. These types differ in their focus, methodology, and the level of detail they provide about the phenomenon under investigation.
Understanding these types is crucial for selecting the most appropriate approach for your research project and effectively achieving your research goals. Let's briefly look at the main types of case studies.
Exploratory case studies
Exploratory case studies are typically conducted to develop a theory or framework around an understudied phenomenon. They can also serve as a precursor to a larger-scale research project. Exploratory case studies are useful when a researcher wants to identify the key issues or questions which can spur more extensive study or be used to develop propositions for further research. These case studies are characterized by flexibility, allowing researchers to explore various aspects of a phenomenon as they emerge, which can also form the foundation for subsequent studies.
Descriptive case studies
Descriptive case studies aim to provide a complete and accurate representation of a phenomenon or event within its context. These case studies are often based on an established theoretical framework, which guides how data is collected and analyzed. The researcher is concerned with describing the phenomenon in detail, as it occurs naturally, without trying to influence or manipulate it.
Explanatory case studies
Explanatory case studies are focused on explanation - they seek to clarify how or why certain phenomena occur. Often used in complex, real-life situations, they can be particularly valuable in clarifying causal relationships among concepts and understanding the interplay between different factors within a specific context.

Intrinsic, instrumental, and collective case studies
These three categories of case studies focus on the nature and purpose of the study. An intrinsic case study is conducted when a researcher has an inherent interest in the case itself. Instrumental case studies are employed when the case is used to provide insight into a particular issue or phenomenon. A collective case study, on the other hand, involves studying multiple cases simultaneously to investigate some general phenomena.
Each type of case study serves a different purpose and has its own strengths and challenges. The selection of the type should be guided by the research question and objectives, as well as the context and constraints of the research.
The flexibility, depth, and contextual richness offered by case studies make this approach an excellent research method for various fields of study. They enable researchers to investigate real-world phenomena within their specific contexts, capturing nuances that other research methods might miss. Across numerous fields, case studies provide valuable insights into complex issues.
Critical information systems research
Case studies provide a detailed understanding of the role and impact of information systems in different contexts. They offer a platform to explore how information systems are designed, implemented, and used and how they interact with various social, economic, and political factors. Case studies in this field often focus on examining the intricate relationship between technology, organizational processes, and user behavior, helping to uncover insights that can inform better system design and implementation.
Health research
Health research is another field where case studies are highly valuable. They offer a way to explore patient experiences, healthcare delivery processes, and the impact of various interventions in a real-world context.

Case studies can provide a deep understanding of a patient's journey, giving insights into the intricacies of disease progression, treatment effects, and the psychosocial aspects of health and illness.
Asthma research studies
Specifically within medical research, studies on asthma often employ case studies to explore the individual and environmental factors that influence asthma development, management, and outcomes. A case study can provide rich, detailed data about individual patients' experiences, from the triggers and symptoms they experience to the effectiveness of various management strategies. This can be crucial for developing patient-centered asthma care approaches.
Other fields
Apart from the fields mentioned, case studies are also extensively used in business and management research, education research, and political sciences, among many others. They provide an opportunity to delve into the intricacies of real-world situations, allowing for a comprehensive understanding of various phenomena.
Case studies, with their depth and contextual focus, offer unique insights across these varied fields. They allow researchers to illuminate the complexities of real-life situations, contributing to both theory and practice.
Whatever field you're in, ATLAS.ti puts your data to work for you
Download a free trial of ATLAS.ti to turn your data into insights.
Understanding the key elements of case study design is crucial for conducting rigorous and impactful case study research. A well-structured design guides the researcher through the process, ensuring that the study is methodologically sound and its findings are reliable and valid. The main elements of case study design include the research question , propositions, units of analysis, and the logic linking the data to the propositions.
The research question is the foundation of any research study. A good research question guides the direction of the study and informs the selection of the case, the methods of collecting data, and the analysis techniques. A well-formulated research question in case study research is typically clear, focused, and complex enough to merit further detailed examination of the relevant case(s).
Propositions
Propositions, though not necessary in every case study, provide a direction by stating what we might expect to find in the data collected. They guide how data is collected and analyzed by helping researchers focus on specific aspects of the case. They are particularly important in explanatory case studies, which seek to understand the relationships among concepts within the studied phenomenon.
Units of analysis
The unit of analysis refers to the case, or the main entity or entities that are being analyzed in the study. In case study research, the unit of analysis can be an individual, a group, an organization, a decision, an event, or even a time period. It's crucial to clearly define the unit of analysis, as it shapes the qualitative data analysis process by allowing the researcher to analyze a particular case and synthesize analysis across multiple case studies to draw conclusions.
Argumentation
This refers to the inferential model that allows researchers to draw conclusions from the data. The researcher needs to ensure that there is a clear link between the data, the propositions (if any), and the conclusions drawn. This argumentation is what enables the researcher to make valid and credible inferences about the phenomenon under study.
Understanding and carefully considering these elements in the design phase of a case study can significantly enhance the quality of the research. It can help ensure that the study is methodologically sound and its findings contribute meaningful insights about the case.
Ready to jumpstart your research with ATLAS.ti?
Conceptualize your research project with our intuitive data analysis interface. Download a free trial today.
Conducting a case study involves several steps, from defining the research question and selecting the case to collecting and analyzing data . This section outlines these key stages, providing a practical guide on how to conduct case study research.
Defining the research question
The first step in case study research is defining a clear, focused research question. This question should guide the entire research process, from case selection to analysis. It's crucial to ensure that the research question is suitable for a case study approach. Typically, such questions are exploratory or descriptive in nature and focus on understanding a phenomenon within its real-life context.
Selecting and defining the case
The selection of the case should be based on the research question and the objectives of the study. It involves choosing a unique example or a set of examples that provide rich, in-depth data about the phenomenon under investigation. After selecting the case, it's crucial to define it clearly, setting the boundaries of the case, including the time period and the specific context.
Previous research can help guide the case study design. When considering a case study, an example of a case could be taken from previous case study research and used to define cases in a new research inquiry. Considering recently published examples can help understand how to select and define cases effectively.
Developing a detailed case study protocol
A case study protocol outlines the procedures and general rules to be followed during the case study. This includes the data collection methods to be used, the sources of data, and the procedures for analysis. Having a detailed case study protocol ensures consistency and reliability in the study.
The protocol should also consider how to work with the people involved in the research context to grant the research team access to collecting data. As mentioned in previous sections of this guide, establishing rapport is an essential component of qualitative research as it shapes the overall potential for collecting and analyzing data.
Collecting data
Gathering data in case study research often involves multiple sources of evidence, including documents, archival records, interviews, observations, and physical artifacts. This allows for a comprehensive understanding of the case. The process for gathering data should be systematic and carefully documented to ensure the reliability and validity of the study.
Analyzing and interpreting data
The next step is analyzing the data. This involves organizing the data , categorizing it into themes or patterns , and interpreting these patterns to answer the research question. The analysis might also involve comparing the findings with prior research or theoretical propositions.
Writing the case study report
The final step is writing the case study report . This should provide a detailed description of the case, the data, the analysis process, and the findings. The report should be clear, organized, and carefully written to ensure that the reader can understand the case and the conclusions drawn from it.
Each of these steps is crucial in ensuring that the case study research is rigorous, reliable, and provides valuable insights about the case.
The type, depth, and quality of data in your study can significantly influence the validity and utility of the study. In case study research, data is usually collected from multiple sources to provide a comprehensive and nuanced understanding of the case. This section will outline the various methods of collecting data used in case study research and discuss considerations for ensuring the quality of the data.
Interviews are a common method of gathering data in case study research. They can provide rich, in-depth data about the perspectives, experiences, and interpretations of the individuals involved in the case. Interviews can be structured , semi-structured , or unstructured , depending on the research question and the degree of flexibility needed.
Observations
Observations involve the researcher observing the case in its natural setting, providing first-hand information about the case and its context. Observations can provide data that might not be revealed in interviews or documents, such as non-verbal cues or contextual information.
Documents and artifacts
Documents and archival records provide a valuable source of data in case study research. They can include reports, letters, memos, meeting minutes, email correspondence, and various public and private documents related to the case.
These records can provide historical context, corroborate evidence from other sources, and offer insights into the case that might not be apparent from interviews or observations.
Physical artifacts refer to any physical evidence related to the case, such as tools, products, or physical environments. These artifacts can provide tangible insights into the case, complementing the data gathered from other sources.
Ensuring the quality of data collection
Determining the quality of data in case study research requires careful planning and execution. It's crucial to ensure that the data is reliable, accurate, and relevant to the research question. This involves selecting appropriate methods of collecting data, properly training interviewers or observers, and systematically recording and storing the data. It also includes considering ethical issues related to collecting and handling data, such as obtaining informed consent and ensuring the privacy and confidentiality of the participants.
Data analysis
Analyzing case study research involves making sense of the rich, detailed data to answer the research question. This process can be challenging due to the volume and complexity of case study data. However, a systematic and rigorous approach to analysis can ensure that the findings are credible and meaningful. This section outlines the main steps and considerations in analyzing data in case study research.
Organizing the data
The first step in the analysis is organizing the data. This involves sorting the data into manageable sections, often according to the data source or the theme. This step can also involve transcribing interviews, digitizing physical artifacts, or organizing observational data.
Categorizing and coding the data
Once the data is organized, the next step is to categorize or code the data. This involves identifying common themes, patterns, or concepts in the data and assigning codes to relevant data segments. Coding can be done manually or with the help of software tools, and in either case, qualitative analysis software can greatly facilitate the entire coding process. Coding helps to reduce the data to a set of themes or categories that can be more easily analyzed.
Identifying patterns and themes
After coding the data, the researcher looks for patterns or themes in the coded data. This involves comparing and contrasting the codes and looking for relationships or patterns among them. The identified patterns and themes should help answer the research question.
Interpreting the data
Once patterns and themes have been identified, the next step is to interpret these findings. This involves explaining what the patterns or themes mean in the context of the research question and the case. This interpretation should be grounded in the data, but it can also involve drawing on theoretical concepts or prior research.
Verification of the data
The last step in the analysis is verification. This involves checking the accuracy and consistency of the analysis process and confirming that the findings are supported by the data. This can involve re-checking the original data, checking the consistency of codes, or seeking feedback from research participants or peers.
Like any research method , case study research has its strengths and limitations. Researchers must be aware of these, as they can influence the design, conduct, and interpretation of the study.
Understanding the strengths and limitations of case study research can also guide researchers in deciding whether this approach is suitable for their research question . This section outlines some of the key strengths and limitations of case study research.
Benefits include the following:
- Rich, detailed data: One of the main strengths of case study research is that it can generate rich, detailed data about the case. This can provide a deep understanding of the case and its context, which can be valuable in exploring complex phenomena.
- Flexibility: Case study research is flexible in terms of design , data collection , and analysis . A sufficient degree of flexibility allows the researcher to adapt the study according to the case and the emerging findings.
- Real-world context: Case study research involves studying the case in its real-world context, which can provide valuable insights into the interplay between the case and its context.
- Multiple sources of evidence: Case study research often involves collecting data from multiple sources , which can enhance the robustness and validity of the findings.
On the other hand, researchers should consider the following limitations:
- Generalizability: A common criticism of case study research is that its findings might not be generalizable to other cases due to the specificity and uniqueness of each case.
- Time and resource intensive: Case study research can be time and resource intensive due to the depth of the investigation and the amount of collected data.
- Complexity of analysis: The rich, detailed data generated in case study research can make analyzing the data challenging.
- Subjectivity: Given the nature of case study research, there may be a higher degree of subjectivity in interpreting the data , so researchers need to reflect on this and transparently convey to audiences how the research was conducted.
Being aware of these strengths and limitations can help researchers design and conduct case study research effectively and interpret and report the findings appropriately.

Ready to analyze your data with ATLAS.ti?
See how our intuitive software can draw key insights from your data with a free trial today.
Have a language expert improve your writing
Run a free plagiarism check in 10 minutes, automatically generate references for free.
- Knowledge Base
- Methodology
- Case Study | Definition, Examples & Methods
Case Study | Definition, Examples & Methods
Published on 5 May 2022 by Shona McCombes . Revised on 30 January 2023.
A case study is a detailed study of a specific subject, such as a person, group, place, event, organisation, or phenomenon. Case studies are commonly used in social, educational, clinical, and business research.
A case study research design usually involves qualitative methods , but quantitative methods are sometimes also used. Case studies are good for describing , comparing, evaluating, and understanding different aspects of a research problem .
Table of contents
When to do a case study, step 1: select a case, step 2: build a theoretical framework, step 3: collect your data, step 4: describe and analyse the case.
A case study is an appropriate research design when you want to gain concrete, contextual, in-depth knowledge about a specific real-world subject. It allows you to explore the key characteristics, meanings, and implications of the case.
Case studies are often a good choice in a thesis or dissertation . They keep your project focused and manageable when you don’t have the time or resources to do large-scale research.
You might use just one complex case study where you explore a single subject in depth, or conduct multiple case studies to compare and illuminate different aspects of your research problem.
Prevent plagiarism, run a free check.
Once you have developed your problem statement and research questions , you should be ready to choose the specific case that you want to focus on. A good case study should have the potential to:
- Provide new or unexpected insights into the subject
- Challenge or complicate existing assumptions and theories
- Propose practical courses of action to resolve a problem
- Open up new directions for future research
Unlike quantitative or experimental research, a strong case study does not require a random or representative sample. In fact, case studies often deliberately focus on unusual, neglected, or outlying cases which may shed new light on the research problem.
If you find yourself aiming to simultaneously investigate and solve an issue, consider conducting action research . As its name suggests, action research conducts research and takes action at the same time, and is highly iterative and flexible.
However, you can also choose a more common or representative case to exemplify a particular category, experience, or phenomenon.
While case studies focus more on concrete details than general theories, they should usually have some connection with theory in the field. This way the case study is not just an isolated description, but is integrated into existing knowledge about the topic. It might aim to:
- Exemplify a theory by showing how it explains the case under investigation
- Expand on a theory by uncovering new concepts and ideas that need to be incorporated
- Challenge a theory by exploring an outlier case that doesn’t fit with established assumptions
To ensure that your analysis of the case has a solid academic grounding, you should conduct a literature review of sources related to the topic and develop a theoretical framework . This means identifying key concepts and theories to guide your analysis and interpretation.
There are many different research methods you can use to collect data on your subject. Case studies tend to focus on qualitative data using methods such as interviews, observations, and analysis of primary and secondary sources (e.g., newspaper articles, photographs, official records). Sometimes a case study will also collect quantitative data .
The aim is to gain as thorough an understanding as possible of the case and its context.
In writing up the case study, you need to bring together all the relevant aspects to give as complete a picture as possible of the subject.
How you report your findings depends on the type of research you are doing. Some case studies are structured like a standard scientific paper or thesis, with separate sections or chapters for the methods , results , and discussion .
Others are written in a more narrative style, aiming to explore the case from various angles and analyse its meanings and implications (for example, by using textual analysis or discourse analysis ).
In all cases, though, make sure to give contextual details about the case, connect it back to the literature and theory, and discuss how it fits into wider patterns or debates.
Cite this Scribbr article
If you want to cite this source, you can copy and paste the citation or click the ‘Cite this Scribbr article’ button to automatically add the citation to our free Reference Generator.
McCombes, S. (2023, January 30). Case Study | Definition, Examples & Methods. Scribbr. Retrieved 27 May 2024, from https://www.scribbr.co.uk/research-methods/case-studies/
Is this article helpful?

Shona McCombes
Other students also liked, correlational research | guide, design & examples, a quick guide to experimental design | 5 steps & examples, descriptive research design | definition, methods & examples.
Research Writing and Analysis
- NVivo Group and Study Sessions
- SPSS This link opens in a new window
- Statistical Analysis Group sessions
- Using Qualtrics
- Dissertation and Data Analysis Group Sessions
- Defense Schedule - Commons Calendar This link opens in a new window
- Research Process Flow Chart
- Research Alignment Chapter 1 This link opens in a new window
- Step 1: Seek Out Evidence
- Step 2: Explain
- Step 3: The Big Picture
- Step 4: Own It
- Step 5: Illustrate
- Annotated Bibliography
- Literature Review This link opens in a new window
- Systematic Reviews & Meta-Analyses
- How to Synthesize and Analyze
- Synthesis and Analysis Practice
- Synthesis and Analysis Group Sessions
- Problem Statement
- Purpose Statement
- Conceptual Framework
- Theoretical Framework
- Quantitative Research Questions
- Qualitative Research Questions
- Trustworthiness of Qualitative Data
- Analysis and Coding Example- Qualitative Data
- Thematic Data Analysis in Qualitative Design
- Dissertation to Journal Article This link opens in a new window
- International Journal of Online Graduate Education (IJOGE) This link opens in a new window
- Journal of Research in Innovative Teaching & Learning (JRIT&L) This link opens in a new window
Writing a Case Study

What is a case study?

A Case study is:
- An in-depth research design that primarily uses a qualitative methodology but sometimes includes quantitative methodology.
- Used to examine an identifiable problem confirmed through research.
- Used to investigate an individual, group of people, organization, or event.
- Used to mostly answer "how" and "why" questions.
What are the different types of case studies?

Note: These are the primary case studies. As you continue to research and learn
about case studies you will begin to find a robust list of different types.
Who are your case study participants?

What is triangulation ?
Validity and credibility are an essential part of the case study. Therefore, the researcher should include triangulation to ensure trustworthiness while accurately reflecting what the researcher seeks to investigate.

How to write a Case Study?
When developing a case study, there are different ways you could present the information, but remember to include the five parts for your case study.

Was this resource helpful?
- << Previous: Thematic Data Analysis in Qualitative Design
- Next: Journal Article Reporting Standards (JARS) >>
- Last Updated: May 16, 2024 8:25 AM
- URL: https://resources.nu.edu/researchtools

- Open access
- Published: 27 June 2011
The case study approach
- Sarah Crowe 1 ,
- Kathrin Cresswell 2 ,
- Ann Robertson 2 ,
- Guro Huby 3 ,
- Anthony Avery 1 &
- Aziz Sheikh 2
BMC Medical Research Methodology volume 11 , Article number: 100 ( 2011 ) Cite this article
782k Accesses
1038 Citations
37 Altmetric
Metrics details
The case study approach allows in-depth, multi-faceted explorations of complex issues in their real-life settings. The value of the case study approach is well recognised in the fields of business, law and policy, but somewhat less so in health services research. Based on our experiences of conducting several health-related case studies, we reflect on the different types of case study design, the specific research questions this approach can help answer, the data sources that tend to be used, and the particular advantages and disadvantages of employing this methodological approach. The paper concludes with key pointers to aid those designing and appraising proposals for conducting case study research, and a checklist to help readers assess the quality of case study reports.
Peer Review reports
Introduction
The case study approach is particularly useful to employ when there is a need to obtain an in-depth appreciation of an issue, event or phenomenon of interest, in its natural real-life context. Our aim in writing this piece is to provide insights into when to consider employing this approach and an overview of key methodological considerations in relation to the design, planning, analysis, interpretation and reporting of case studies.
The illustrative 'grand round', 'case report' and 'case series' have a long tradition in clinical practice and research. Presenting detailed critiques, typically of one or more patients, aims to provide insights into aspects of the clinical case and, in doing so, illustrate broader lessons that may be learnt. In research, the conceptually-related case study approach can be used, for example, to describe in detail a patient's episode of care, explore professional attitudes to and experiences of a new policy initiative or service development or more generally to 'investigate contemporary phenomena within its real-life context' [ 1 ]. Based on our experiences of conducting a range of case studies, we reflect on when to consider using this approach, discuss the key steps involved and illustrate, with examples, some of the practical challenges of attaining an in-depth understanding of a 'case' as an integrated whole. In keeping with previously published work, we acknowledge the importance of theory to underpin the design, selection, conduct and interpretation of case studies[ 2 ]. In so doing, we make passing reference to the different epistemological approaches used in case study research by key theoreticians and methodologists in this field of enquiry.
This paper is structured around the following main questions: What is a case study? What are case studies used for? How are case studies conducted? What are the potential pitfalls and how can these be avoided? We draw in particular on four of our own recently published examples of case studies (see Tables 1 , 2 , 3 and 4 ) and those of others to illustrate our discussion[ 3 – 7 ].
What is a case study?
A case study is a research approach that is used to generate an in-depth, multi-faceted understanding of a complex issue in its real-life context. It is an established research design that is used extensively in a wide variety of disciplines, particularly in the social sciences. A case study can be defined in a variety of ways (Table 5 ), the central tenet being the need to explore an event or phenomenon in depth and in its natural context. It is for this reason sometimes referred to as a "naturalistic" design; this is in contrast to an "experimental" design (such as a randomised controlled trial) in which the investigator seeks to exert control over and manipulate the variable(s) of interest.
Stake's work has been particularly influential in defining the case study approach to scientific enquiry. He has helpfully characterised three main types of case study: intrinsic , instrumental and collective [ 8 ]. An intrinsic case study is typically undertaken to learn about a unique phenomenon. The researcher should define the uniqueness of the phenomenon, which distinguishes it from all others. In contrast, the instrumental case study uses a particular case (some of which may be better than others) to gain a broader appreciation of an issue or phenomenon. The collective case study involves studying multiple cases simultaneously or sequentially in an attempt to generate a still broader appreciation of a particular issue.
These are however not necessarily mutually exclusive categories. In the first of our examples (Table 1 ), we undertook an intrinsic case study to investigate the issue of recruitment of minority ethnic people into the specific context of asthma research studies, but it developed into a instrumental case study through seeking to understand the issue of recruitment of these marginalised populations more generally, generating a number of the findings that are potentially transferable to other disease contexts[ 3 ]. In contrast, the other three examples (see Tables 2 , 3 and 4 ) employed collective case study designs to study the introduction of workforce reconfiguration in primary care, the implementation of electronic health records into hospitals, and to understand the ways in which healthcare students learn about patient safety considerations[ 4 – 6 ]. Although our study focusing on the introduction of General Practitioners with Specialist Interests (Table 2 ) was explicitly collective in design (four contrasting primary care organisations were studied), is was also instrumental in that this particular professional group was studied as an exemplar of the more general phenomenon of workforce redesign[ 4 ].
What are case studies used for?
According to Yin, case studies can be used to explain, describe or explore events or phenomena in the everyday contexts in which they occur[ 1 ]. These can, for example, help to understand and explain causal links and pathways resulting from a new policy initiative or service development (see Tables 2 and 3 , for example)[ 1 ]. In contrast to experimental designs, which seek to test a specific hypothesis through deliberately manipulating the environment (like, for example, in a randomised controlled trial giving a new drug to randomly selected individuals and then comparing outcomes with controls),[ 9 ] the case study approach lends itself well to capturing information on more explanatory ' how ', 'what' and ' why ' questions, such as ' how is the intervention being implemented and received on the ground?'. The case study approach can offer additional insights into what gaps exist in its delivery or why one implementation strategy might be chosen over another. This in turn can help develop or refine theory, as shown in our study of the teaching of patient safety in undergraduate curricula (Table 4 )[ 6 , 10 ]. Key questions to consider when selecting the most appropriate study design are whether it is desirable or indeed possible to undertake a formal experimental investigation in which individuals and/or organisations are allocated to an intervention or control arm? Or whether the wish is to obtain a more naturalistic understanding of an issue? The former is ideally studied using a controlled experimental design, whereas the latter is more appropriately studied using a case study design.
Case studies may be approached in different ways depending on the epistemological standpoint of the researcher, that is, whether they take a critical (questioning one's own and others' assumptions), interpretivist (trying to understand individual and shared social meanings) or positivist approach (orientating towards the criteria of natural sciences, such as focusing on generalisability considerations) (Table 6 ). Whilst such a schema can be conceptually helpful, it may be appropriate to draw on more than one approach in any case study, particularly in the context of conducting health services research. Doolin has, for example, noted that in the context of undertaking interpretative case studies, researchers can usefully draw on a critical, reflective perspective which seeks to take into account the wider social and political environment that has shaped the case[ 11 ].
How are case studies conducted?
Here, we focus on the main stages of research activity when planning and undertaking a case study; the crucial stages are: defining the case; selecting the case(s); collecting and analysing the data; interpreting data; and reporting the findings.
Defining the case
Carefully formulated research question(s), informed by the existing literature and a prior appreciation of the theoretical issues and setting(s), are all important in appropriately and succinctly defining the case[ 8 , 12 ]. Crucially, each case should have a pre-defined boundary which clarifies the nature and time period covered by the case study (i.e. its scope, beginning and end), the relevant social group, organisation or geographical area of interest to the investigator, the types of evidence to be collected, and the priorities for data collection and analysis (see Table 7 )[ 1 ]. A theory driven approach to defining the case may help generate knowledge that is potentially transferable to a range of clinical contexts and behaviours; using theory is also likely to result in a more informed appreciation of, for example, how and why interventions have succeeded or failed[ 13 ].
For example, in our evaluation of the introduction of electronic health records in English hospitals (Table 3 ), we defined our cases as the NHS Trusts that were receiving the new technology[ 5 ]. Our focus was on how the technology was being implemented. However, if the primary research interest had been on the social and organisational dimensions of implementation, we might have defined our case differently as a grouping of healthcare professionals (e.g. doctors and/or nurses). The precise beginning and end of the case may however prove difficult to define. Pursuing this same example, when does the process of implementation and adoption of an electronic health record system really begin or end? Such judgements will inevitably be influenced by a range of factors, including the research question, theory of interest, the scope and richness of the gathered data and the resources available to the research team.
Selecting the case(s)
The decision on how to select the case(s) to study is a very important one that merits some reflection. In an intrinsic case study, the case is selected on its own merits[ 8 ]. The case is selected not because it is representative of other cases, but because of its uniqueness, which is of genuine interest to the researchers. This was, for example, the case in our study of the recruitment of minority ethnic participants into asthma research (Table 1 ) as our earlier work had demonstrated the marginalisation of minority ethnic people with asthma, despite evidence of disproportionate asthma morbidity[ 14 , 15 ]. In another example of an intrinsic case study, Hellstrom et al.[ 16 ] studied an elderly married couple living with dementia to explore how dementia had impacted on their understanding of home, their everyday life and their relationships.
For an instrumental case study, selecting a "typical" case can work well[ 8 ]. In contrast to the intrinsic case study, the particular case which is chosen is of less importance than selecting a case that allows the researcher to investigate an issue or phenomenon. For example, in order to gain an understanding of doctors' responses to health policy initiatives, Som undertook an instrumental case study interviewing clinicians who had a range of responsibilities for clinical governance in one NHS acute hospital trust[ 17 ]. Sampling a "deviant" or "atypical" case may however prove even more informative, potentially enabling the researcher to identify causal processes, generate hypotheses and develop theory.
In collective or multiple case studies, a number of cases are carefully selected. This offers the advantage of allowing comparisons to be made across several cases and/or replication. Choosing a "typical" case may enable the findings to be generalised to theory (i.e. analytical generalisation) or to test theory by replicating the findings in a second or even a third case (i.e. replication logic)[ 1 ]. Yin suggests two or three literal replications (i.e. predicting similar results) if the theory is straightforward and five or more if the theory is more subtle. However, critics might argue that selecting 'cases' in this way is insufficiently reflexive and ill-suited to the complexities of contemporary healthcare organisations.
The selected case study site(s) should allow the research team access to the group of individuals, the organisation, the processes or whatever else constitutes the chosen unit of analysis for the study. Access is therefore a central consideration; the researcher needs to come to know the case study site(s) well and to work cooperatively with them. Selected cases need to be not only interesting but also hospitable to the inquiry [ 8 ] if they are to be informative and answer the research question(s). Case study sites may also be pre-selected for the researcher, with decisions being influenced by key stakeholders. For example, our selection of case study sites in the evaluation of the implementation and adoption of electronic health record systems (see Table 3 ) was heavily influenced by NHS Connecting for Health, the government agency that was responsible for overseeing the National Programme for Information Technology (NPfIT)[ 5 ]. This prominent stakeholder had already selected the NHS sites (through a competitive bidding process) to be early adopters of the electronic health record systems and had negotiated contracts that detailed the deployment timelines.
It is also important to consider in advance the likely burden and risks associated with participation for those who (or the site(s) which) comprise the case study. Of particular importance is the obligation for the researcher to think through the ethical implications of the study (e.g. the risk of inadvertently breaching anonymity or confidentiality) and to ensure that potential participants/participating sites are provided with sufficient information to make an informed choice about joining the study. The outcome of providing this information might be that the emotive burden associated with participation, or the organisational disruption associated with supporting the fieldwork, is considered so high that the individuals or sites decide against participation.
In our example of evaluating implementations of electronic health record systems, given the restricted number of early adopter sites available to us, we sought purposively to select a diverse range of implementation cases among those that were available[ 5 ]. We chose a mixture of teaching, non-teaching and Foundation Trust hospitals, and examples of each of the three electronic health record systems procured centrally by the NPfIT. At one recruited site, it quickly became apparent that access was problematic because of competing demands on that organisation. Recognising the importance of full access and co-operative working for generating rich data, the research team decided not to pursue work at that site and instead to focus on other recruited sites.
Collecting the data
In order to develop a thorough understanding of the case, the case study approach usually involves the collection of multiple sources of evidence, using a range of quantitative (e.g. questionnaires, audits and analysis of routinely collected healthcare data) and more commonly qualitative techniques (e.g. interviews, focus groups and observations). The use of multiple sources of data (data triangulation) has been advocated as a way of increasing the internal validity of a study (i.e. the extent to which the method is appropriate to answer the research question)[ 8 , 18 – 21 ]. An underlying assumption is that data collected in different ways should lead to similar conclusions, and approaching the same issue from different angles can help develop a holistic picture of the phenomenon (Table 2 )[ 4 ].
Brazier and colleagues used a mixed-methods case study approach to investigate the impact of a cancer care programme[ 22 ]. Here, quantitative measures were collected with questionnaires before, and five months after, the start of the intervention which did not yield any statistically significant results. Qualitative interviews with patients however helped provide an insight into potentially beneficial process-related aspects of the programme, such as greater, perceived patient involvement in care. The authors reported how this case study approach provided a number of contextual factors likely to influence the effectiveness of the intervention and which were not likely to have been obtained from quantitative methods alone.
In collective or multiple case studies, data collection needs to be flexible enough to allow a detailed description of each individual case to be developed (e.g. the nature of different cancer care programmes), before considering the emerging similarities and differences in cross-case comparisons (e.g. to explore why one programme is more effective than another). It is important that data sources from different cases are, where possible, broadly comparable for this purpose even though they may vary in nature and depth.
Analysing, interpreting and reporting case studies
Making sense and offering a coherent interpretation of the typically disparate sources of data (whether qualitative alone or together with quantitative) is far from straightforward. Repeated reviewing and sorting of the voluminous and detail-rich data are integral to the process of analysis. In collective case studies, it is helpful to analyse data relating to the individual component cases first, before making comparisons across cases. Attention needs to be paid to variations within each case and, where relevant, the relationship between different causes, effects and outcomes[ 23 ]. Data will need to be organised and coded to allow the key issues, both derived from the literature and emerging from the dataset, to be easily retrieved at a later stage. An initial coding frame can help capture these issues and can be applied systematically to the whole dataset with the aid of a qualitative data analysis software package.
The Framework approach is a practical approach, comprising of five stages (familiarisation; identifying a thematic framework; indexing; charting; mapping and interpretation) , to managing and analysing large datasets particularly if time is limited, as was the case in our study of recruitment of South Asians into asthma research (Table 1 )[ 3 , 24 ]. Theoretical frameworks may also play an important role in integrating different sources of data and examining emerging themes. For example, we drew on a socio-technical framework to help explain the connections between different elements - technology; people; and the organisational settings within which they worked - in our study of the introduction of electronic health record systems (Table 3 )[ 5 ]. Our study of patient safety in undergraduate curricula drew on an evaluation-based approach to design and analysis, which emphasised the importance of the academic, organisational and practice contexts through which students learn (Table 4 )[ 6 ].
Case study findings can have implications both for theory development and theory testing. They may establish, strengthen or weaken historical explanations of a case and, in certain circumstances, allow theoretical (as opposed to statistical) generalisation beyond the particular cases studied[ 12 ]. These theoretical lenses should not, however, constitute a strait-jacket and the cases should not be "forced to fit" the particular theoretical framework that is being employed.
When reporting findings, it is important to provide the reader with enough contextual information to understand the processes that were followed and how the conclusions were reached. In a collective case study, researchers may choose to present the findings from individual cases separately before amalgamating across cases. Care must be taken to ensure the anonymity of both case sites and individual participants (if agreed in advance) by allocating appropriate codes or withholding descriptors. In the example given in Table 3 , we decided against providing detailed information on the NHS sites and individual participants in order to avoid the risk of inadvertent disclosure of identities[ 5 , 25 ].
What are the potential pitfalls and how can these be avoided?
The case study approach is, as with all research, not without its limitations. When investigating the formal and informal ways undergraduate students learn about patient safety (Table 4 ), for example, we rapidly accumulated a large quantity of data. The volume of data, together with the time restrictions in place, impacted on the depth of analysis that was possible within the available resources. This highlights a more general point of the importance of avoiding the temptation to collect as much data as possible; adequate time also needs to be set aside for data analysis and interpretation of what are often highly complex datasets.
Case study research has sometimes been criticised for lacking scientific rigour and providing little basis for generalisation (i.e. producing findings that may be transferable to other settings)[ 1 ]. There are several ways to address these concerns, including: the use of theoretical sampling (i.e. drawing on a particular conceptual framework); respondent validation (i.e. participants checking emerging findings and the researcher's interpretation, and providing an opinion as to whether they feel these are accurate); and transparency throughout the research process (see Table 8 )[ 8 , 18 – 21 , 23 , 26 ]. Transparency can be achieved by describing in detail the steps involved in case selection, data collection, the reasons for the particular methods chosen, and the researcher's background and level of involvement (i.e. being explicit about how the researcher has influenced data collection and interpretation). Seeking potential, alternative explanations, and being explicit about how interpretations and conclusions were reached, help readers to judge the trustworthiness of the case study report. Stake provides a critique checklist for a case study report (Table 9 )[ 8 ].
Conclusions
The case study approach allows, amongst other things, critical events, interventions, policy developments and programme-based service reforms to be studied in detail in a real-life context. It should therefore be considered when an experimental design is either inappropriate to answer the research questions posed or impossible to undertake. Considering the frequency with which implementations of innovations are now taking place in healthcare settings and how well the case study approach lends itself to in-depth, complex health service research, we believe this approach should be more widely considered by researchers. Though inherently challenging, the research case study can, if carefully conceptualised and thoughtfully undertaken and reported, yield powerful insights into many important aspects of health and healthcare delivery.
Yin RK: Case study research, design and method. 2009, London: Sage Publications Ltd., 4
Google Scholar
Keen J, Packwood T: Qualitative research; case study evaluation. BMJ. 1995, 311: 444-446.
Article CAS PubMed PubMed Central Google Scholar
Sheikh A, Halani L, Bhopal R, Netuveli G, Partridge M, Car J, et al: Facilitating the Recruitment of Minority Ethnic People into Research: Qualitative Case Study of South Asians and Asthma. PLoS Med. 2009, 6 (10): 1-11.
Article Google Scholar
Pinnock H, Huby G, Powell A, Kielmann T, Price D, Williams S, et al: The process of planning, development and implementation of a General Practitioner with a Special Interest service in Primary Care Organisations in England and Wales: a comparative prospective case study. Report for the National Co-ordinating Centre for NHS Service Delivery and Organisation R&D (NCCSDO). 2008, [ http://www.sdo.nihr.ac.uk/files/project/99-final-report.pdf ]
Robertson A, Cresswell K, Takian A, Petrakaki D, Crowe S, Cornford T, et al: Prospective evaluation of the implementation and adoption of NHS Connecting for Health's national electronic health record in secondary care in England: interim findings. BMJ. 2010, 41: c4564-
Pearson P, Steven A, Howe A, Sheikh A, Ashcroft D, Smith P, the Patient Safety Education Study Group: Learning about patient safety: organisational context and culture in the education of healthcare professionals. J Health Serv Res Policy. 2010, 15: 4-10. 10.1258/jhsrp.2009.009052.
Article PubMed Google Scholar
van Harten WH, Casparie TF, Fisscher OA: The evaluation of the introduction of a quality management system: a process-oriented case study in a large rehabilitation hospital. Health Policy. 2002, 60 (1): 17-37. 10.1016/S0168-8510(01)00187-7.
Stake RE: The art of case study research. 1995, London: Sage Publications Ltd.
Sheikh A, Smeeth L, Ashcroft R: Randomised controlled trials in primary care: scope and application. Br J Gen Pract. 2002, 52 (482): 746-51.
PubMed PubMed Central Google Scholar
King G, Keohane R, Verba S: Designing Social Inquiry. 1996, Princeton: Princeton University Press
Doolin B: Information technology as disciplinary technology: being critical in interpretative research on information systems. Journal of Information Technology. 1998, 13: 301-311. 10.1057/jit.1998.8.
George AL, Bennett A: Case studies and theory development in the social sciences. 2005, Cambridge, MA: MIT Press
Eccles M, the Improved Clinical Effectiveness through Behavioural Research Group (ICEBeRG): Designing theoretically-informed implementation interventions. Implementation Science. 2006, 1: 1-8. 10.1186/1748-5908-1-1.
Article PubMed Central Google Scholar
Netuveli G, Hurwitz B, Levy M, Fletcher M, Barnes G, Durham SR, Sheikh A: Ethnic variations in UK asthma frequency, morbidity, and health-service use: a systematic review and meta-analysis. Lancet. 2005, 365 (9456): 312-7.
Sheikh A, Panesar SS, Lasserson T, Netuveli G: Recruitment of ethnic minorities to asthma studies. Thorax. 2004, 59 (7): 634-
CAS PubMed PubMed Central Google Scholar
Hellström I, Nolan M, Lundh U: 'We do things together': A case study of 'couplehood' in dementia. Dementia. 2005, 4: 7-22. 10.1177/1471301205049188.
Som CV: Nothing seems to have changed, nothing seems to be changing and perhaps nothing will change in the NHS: doctors' response to clinical governance. International Journal of Public Sector Management. 2005, 18: 463-477. 10.1108/09513550510608903.
Lincoln Y, Guba E: Naturalistic inquiry. 1985, Newbury Park: Sage Publications
Barbour RS: Checklists for improving rigour in qualitative research: a case of the tail wagging the dog?. BMJ. 2001, 322: 1115-1117. 10.1136/bmj.322.7294.1115.
Mays N, Pope C: Qualitative research in health care: Assessing quality in qualitative research. BMJ. 2000, 320: 50-52. 10.1136/bmj.320.7226.50.
Mason J: Qualitative researching. 2002, London: Sage
Brazier A, Cooke K, Moravan V: Using Mixed Methods for Evaluating an Integrative Approach to Cancer Care: A Case Study. Integr Cancer Ther. 2008, 7: 5-17. 10.1177/1534735407313395.
Miles MB, Huberman M: Qualitative data analysis: an expanded sourcebook. 1994, CA: Sage Publications Inc., 2
Pope C, Ziebland S, Mays N: Analysing qualitative data. Qualitative research in health care. BMJ. 2000, 320: 114-116. 10.1136/bmj.320.7227.114.
Cresswell KM, Worth A, Sheikh A: Actor-Network Theory and its role in understanding the implementation of information technology developments in healthcare. BMC Med Inform Decis Mak. 2010, 10 (1): 67-10.1186/1472-6947-10-67.
Article PubMed PubMed Central Google Scholar
Malterud K: Qualitative research: standards, challenges, and guidelines. Lancet. 2001, 358: 483-488. 10.1016/S0140-6736(01)05627-6.
Article CAS PubMed Google Scholar
Yin R: Case study research: design and methods. 1994, Thousand Oaks, CA: Sage Publishing, 2
Yin R: Enhancing the quality of case studies in health services research. Health Serv Res. 1999, 34: 1209-1224.
Green J, Thorogood N: Qualitative methods for health research. 2009, Los Angeles: Sage, 2
Howcroft D, Trauth E: Handbook of Critical Information Systems Research, Theory and Application. 2005, Cheltenham, UK: Northampton, MA, USA: Edward Elgar
Book Google Scholar
Blakie N: Approaches to Social Enquiry. 1993, Cambridge: Polity Press
Doolin B: Power and resistance in the implementation of a medical management information system. Info Systems J. 2004, 14: 343-362. 10.1111/j.1365-2575.2004.00176.x.
Bloomfield BP, Best A: Management consultants: systems development, power and the translation of problems. Sociological Review. 1992, 40: 533-560.
Shanks G, Parr A: Positivist, single case study research in information systems: A critical analysis. Proceedings of the European Conference on Information Systems. 2003, Naples
Pre-publication history
The pre-publication history for this paper can be accessed here: http://www.biomedcentral.com/1471-2288/11/100/prepub
Download references
Acknowledgements
We are grateful to the participants and colleagues who contributed to the individual case studies that we have drawn on. This work received no direct funding, but it has been informed by projects funded by Asthma UK, the NHS Service Delivery Organisation, NHS Connecting for Health Evaluation Programme, and Patient Safety Research Portfolio. We would also like to thank the expert reviewers for their insightful and constructive feedback. Our thanks are also due to Dr. Allison Worth who commented on an earlier draft of this manuscript.
Author information
Authors and affiliations.
Division of Primary Care, The University of Nottingham, Nottingham, UK
Sarah Crowe & Anthony Avery
Centre for Population Health Sciences, The University of Edinburgh, Edinburgh, UK
Kathrin Cresswell, Ann Robertson & Aziz Sheikh
School of Health in Social Science, The University of Edinburgh, Edinburgh, UK
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Sarah Crowe .
Additional information
Competing interests.
The authors declare that they have no competing interests.
Authors' contributions
AS conceived this article. SC, KC and AR wrote this paper with GH, AA and AS all commenting on various drafts. SC and AS are guarantors.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License ( http://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Reprints and permissions
About this article
Cite this article.
Crowe, S., Cresswell, K., Robertson, A. et al. The case study approach. BMC Med Res Methodol 11 , 100 (2011). https://doi.org/10.1186/1471-2288-11-100
Download citation
Received : 29 November 2010
Accepted : 27 June 2011
Published : 27 June 2011
DOI : https://doi.org/10.1186/1471-2288-11-100
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Case Study Approach
- Electronic Health Record System
- Case Study Design
- Case Study Site
- Case Study Report
BMC Medical Research Methodology
ISSN: 1471-2288
- General enquiries: [email protected]
Comparative Literature
“reading art in literature: the marvelous case of ‘the story of the stone’”, a book by dore j. levy.
Reading Art in Literature: The Marvelous Case of “The Story of the Stone” is a literary study of the art objects lavishly deployed by Cao Xueqin (1710–1765?) in his beloved novel (better known as The Dream of the Red Chamber). These objects are intended as expedients to preserving the vanishing culture of his lifetime, while offering their symbolic and allegorical significance as guides to a path of enlightenment.
In March of this year, Comparative Literature professor Dore Levy published her new book, Reading Art in Literature: The Marvelous Case of “The Story of the Stone” . The Story of the Stone (also known as The Dream of the Red Chamber ) is an 18th-century Chinese novel by Cao Xueqin, and is considered to be one of the great classical novels of Chinese literature. Prof. Levy’s book is a literary study of the art objects in Cao Xueqin’s novel.
This study not only illuminates the meaning behind the variety, provenance, placement, and uses of these objects but also how the art objects in the novel function as a guide to the author’s fictional world. These include masterpieces of Chinese painting, treasures from the dowries of the women who married into the Jia family, mystical objects with the power to awaken minds set upon destructive paths, and Prospect Garden, a feat of garden engineering and design meant to honor the emperor’s favor but used to protect the children of the Jia Family from the vicissitudes of adult life beyond its walls.

Dore Levy is Professor of Comparative Literature and Professor of East Asian Studies here at Brown University. She came to Brown in 1981 as the first specialist in a non-western culture in Comparative Literature, and subsequently has taught a broad variety of courses in Asian Studies, with a focus on traditional Chinese culture. Dore’s previous publications include Chinese Narrative Poetry: the Late Han through T'ang Dynasties (Duke University Press) and Ideal and Actual in The Story of the Stone (Columbia University Press).
Join us in congratulating Dore on her publication!
Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals
- My Account Login
- Explore content
- About the journal
- Publish with us
- Sign up for alerts
- Open access
- Published: 24 May 2024
Beyond probability-impact matrices in project risk management: A quantitative methodology for risk prioritisation
- F. Acebes ORCID: orcid.org/0000-0002-4525-2610 1 ,
- J. M. González-Varona 2 ,
- A. López-Paredes 2 &
- J. Pajares 1
Humanities and Social Sciences Communications volume 11 , Article number: 670 ( 2024 ) Cite this article
12 Accesses
Metrics details
- Business and management
The project managers who deal with risk management are often faced with the difficult task of determining the relative importance of the various sources of risk that affect the project. This prioritisation is crucial to direct management efforts to ensure higher project profitability. Risk matrices are widely recognised tools by academics and practitioners in various sectors to assess and rank risks according to their likelihood of occurrence and impact on project objectives. However, the existing literature highlights several limitations to use the risk matrix. In response to the weaknesses of its use, this paper proposes a novel approach for prioritising project risks. Monte Carlo Simulation (MCS) is used to perform a quantitative prioritisation of risks with the simulation software MCSimulRisk. Together with the definition of project activities, the simulation includes the identified risks by modelling their probability and impact on cost and duration. With this novel methodology, a quantitative assessment of the impact of each risk is provided, as measured by the effect that it would have on project duration and its total cost. This allows the differentiation of critical risks according to their impact on project duration, which may differ if cost is taken as a priority objective. This proposal is interesting for project managers because they will, on the one hand, know the absolute impact of each risk on their project duration and cost objectives and, on the other hand, be able to discriminate the impacts of each risk independently on the duration objective and the cost objective.
Similar content being viewed by others

A case study on the relationship between risk assessment of scientific research projects and related factors under the Naive Bayesian algorithm

Compound Matrix-Based Project Database (CMPD)

Risk identification approaches and the number of risks identified: the use of work breakdown structure and business process
Introduction.
The European Commission ( 2023 ) defines a project as a temporary organizational structure designed to produce a unique product or service according to specified constraints, such as time, cost, and quality. As projects are inherently complex, they involve risks that must be effectively managed (Naderpour et al. 2019 ). However, achieving project objectives can be challenging due to unexpected developments, which often disrupt plans and budgets during project execution and lead to significant additional costs. The Standish Group ( 2022 ) notes that managing project uncertainty is of paramount importance, which renders risk management an indispensable discipline. Its primary goal is to identify a project’s risk profile and communicate it by enabling informed decision making to mitigate the impact of risks on project objectives, including budget and schedule adherence (Creemers et al. 2014 ).
Several methodologies and standards include a specific project risk management process (Axelos, 2023 ; European Commission, 2023 ; Project Management Institute, 2017 ; International Project Management Association, 2015 ; Simon et al. 1997 ), and there are even specific standards and guidelines for it (Project Management Institute, 2019 , 2009 ; International Organization for Standardization, 2018 ). Despite the differences in naming each phase or process that forms part of the risk management process, they all integrate risk identification, risk assessment, planning a response to the risk, and implementing this response. Apart from all this, a risk monitoring and control process is included. The “Risk Assessment” process comprises, in turn, risk assessments by qualitative methods and quantitative risk assessments.
A prevalent issue in managing project risks is identifying the significance of different sources of risks to direct future risk management actions and to sustain the project’s cost-effectiveness. For many managers busy with problems all over the place, one of the most challenging tasks is to decide which issues to work on first (Ward, 1999 ) or, in other words, which risks need to be paid more attention to avoid deviations from project objectives.
Given the many sources of risk and the impossibility of comprehensively addressing them, it is natural to prioritise identified risks. This process can be challenging because determining in advance which ones are the most significant factors, and how many risks merit detailed monitoring on an individual basis, can be complicated. Any approach that facilitates this prioritisation task, especially if it is simple, will be welcomed by those willing to use it (Ward, 1999 ).
Risk matrices emerge as established familiar tools for assessing and ranking risks in many fields and industry sectors (Krisper, 2021 ; Qazi et al. 2021 ; Qazi and Simsekler, 2021 ; Monat and Doremus, 2020 ; Li et al. 2018 ). They are now so commonplace that everyone accepts and uses them without questioning them, along with their advantages and disadvantages. Risk matrices use the likelihood and potential impact of risks to inform decision making about prioritising identified risks (Proto et al. 2023 ). The methods that use the risk matrix confer higher priority to those risks in which the product of their likelihood and impact is the highest.
However, the probability-impact matrix has severe limitations (Goerlandt and Reniers, 2016 ; Duijm, 2015 ; Vatanpour et al. 2015 ; Ball and Watt, 2013 ; Levine, 2012 ; Cox, 2008 ; Cox et al. 2005 ). The main criticism levelled at this methodology is its failure to consider the complex interrelations between various risks and use precise estimates for probability and impact levels. Since then, increasingly more academics and practitioners are reluctant to resort to risk matrices (Qazi et al. 2021 ).
Motivated by the drawbacks of using risk matrices or probability-impact matrices, the following research question arises: Is it possible to find a methodology for project risk prioritisation that overcomes the limitations of the current probability-impact matrix?
To answer this question, this paper proposes a methodology based on Monte Carlo Simulation that avoids using the probability-impact matrix and allows us to prioritise project risks by evaluating them quantitatively, and by assessing the impact of risks on project duration and the cost objectives. With the help of the ‘MCSimulRisk’ simulation software (Acebes et al. 2024 ; Acebes et al. 2023 ), this paper determines the impact of each risk on project duration objectives (quantified in time units) and cost objectives (quantified in monetary units). In this way, with the impact of all the risks, it is possible to establish their prioritisation based on their absolute (and not relative) importance for project objectives. The methodology allows quantified results to be obtained for each risk by differentiating between the project duration objective and its cost objective.
With this methodology, it also confers the ‘Risk Assessment’ process cohesion and meaning. This process forms part of the general Risk Management process and is divided into two subprocesses: qualitative and quantitative risk analyses (Project Management Institute, 2017 ). Although Monte Carlo simulation is widely used in project risk assessments (Tong et al. 2018 ; Taroun, 2014 ), as far as we know, the literature still does not contain references that use the data obtained in a qualitative analysis (data related to the probability and impact of each identified risk) to perform a quantitative risk analysis integrated into the project model. Only one research line by A. Qazi (Qazi et al. 2021 ; Qazi and Dikmen, 2021 ; Qazi and Simsekler, 2021 ) appears, where the authors propose a risk indicator with which they determine the level of each identified risk that concerns the established threshold. Similarly, Krisper ( 2021 ) applies the qualitative data of risk factors to construct probability functions, but once again falls in the error of calculating the expected value of the risk for risk prioritisation. In contrast, the novelty proposed in this study incorporates into the project simulation model all the identified risks characterised by their probability and impact values, as well as the set of activities making up the project.
In summary, instead of the traditional risk prioritisation method to qualitatively estimate risk probabilities and impacts, we model probabilities and impacts (duration and cost) at the activity level as distribution functions. When comparing both methods (traditional vs. our proposal), the risk prioritisation results are entirely different and lead to a distinct ranking.
From this point, and to achieve our purpose, the article comes as follows. Literature review summarises the relevant literature related to the research. Methodology describes the suggested methodology. Case study presents the case study used to show how to apply the presented method before discussing the obtained results. Finally, Conclusions draws conclusions about the proposed methodology and identifies the research future lines that can be developed from it.
Literature review
This section presents the literature review on risk management processes and probability-impact matrices to explain where this study fits into existing research. This review allows us to establish the context where our proposal lies in integrated risk management processes. Furthermore, it is necessary to understand the reasons for seeking alternatives to the usual well-known risk matrices.
Risk management methodologies and standards
It is interesting to start with the definition of ‘Risk’ because it is a term that is not universally agreed on, even by different standards and norms. Thus, for example, the International Organization for Standardization ( 2018 ) defines it as “the effect of uncertainty on objectives”, while the Project Management Institute ( 2021 ) defines it as “an uncertain event or condition that, if it occurs, has a positive or negative effect on one or more project objectives”. This paper adopts the definition of risk proposed by Hillson ( 2014 ), who uses a particular concept: “risk is uncertainty that matters”. It matters because it affects project objectives and only the uncertainties that impact the project are considered a ‘risk’.
Other authors (Elms, 2004 ; Frank, 1999 ) identify two uncertainty categories: aleatoric, characterised by variability and the presence of a wide range of possible values; epistemic, which arises due to ambiguity or lack of complete knowledge. Hillson ( 2014 ) classifies uncertainties into four distinct types: aleatoric, due to the reliability of activities; stochastic, recognised as a risk event or a possible future event; epistemic, also due to ambiguity; ontological, that which we do not know (black swan). Except for ontological uncertainty, which cannot be modelled due to absolute ignorance of risk, the other identified uncertainties are incorporated into our project model. For this purpose, the probability and impact of each uncertainty are modelled as distribution functions to be incorporated into Monte Carlo simulation.
A risk management process involves analysing the opportunities and threats that can impact project objectives, followed by planning appropriate actions for each one. This process aims to maximise the likelihood of opportunities occurring and to minimise the likelihood of identified threats materialising.
Although it is true that different authors have proposed their particular way of understanding project risk management (Kerzner, 2022 ; Hillson and Simon, 2020 ; Chapman and Ward, 2003 ; Chapman, 1997 ), we wish to look at the principal methodologies, norms and standards in project management used by academics and practitioners to observe how they deal with risk (Axelos, 2023 ; European Commission, 2023 ; International Organization for Standardization, 2018 ; Project Management Institute, 2017 ; International Project Management Association, 2015 ) (Table 1 ).
Table 1 shows the main subprocesses making up the overall risk management process from the point of view of each different approach. All the aforementioned approaches contain a subprocess related to risk assessment. Some of these approaches develop the subprocess by dividing it into two parts: qualitative assessment and quantitative assessment. Individual project risks are ranked for further analyses or action with a qualitative assessment by evaluating the probability of their occurrence and potential impact. A quantitative assessment involves performing a numerical analysis of the joint effect of the identified individual risks and additional sources of uncertainty on the overall project objectives (Project Management Institute, 2017 ). In turn, all these approaches propose the probability-impact or risk matrix as a technique or tool for prioritising project risks.
Within this framework, a ranking of risks by a quantitative approach applies as opposed to the qualitative assessment provided by the risk matrix. To do so, we use estimates of the probability and impact associated with each identified risk. The project model includes these estimates to determine the absolute value of the impact of each risk on time and cost objectives.
Probability-impact matrix
The risk matrix, or probability-impact matrix, is a tool included in the qualitative analysis for risk management and used to analyse, visualise and prioritise risks to make decisions on the resources to be employed to combat them (Goerlandt and Reniers, 2016 ; Duijm, 2015 ). Its well-established use appears in different sectors, ranging from the construction industry (Qazi et al. 2021 ), oil and gas industries (Thomas et al. 2014 ), to the healthcare sector (Lemmens et al. 2022 ), engineering projects (Koulinas et al. 2021 ) and, of course, project management (International Organization for Standardization, 2019 ; Li et al. 2018 ).
In a table, the risk matrix represents the probability (usually on the vertical axis of the table) and impact (usually on the horizontal axis) categories (Ale et al. 2015 ). These axes are further divided into different levels so that risk matrices of 3×3 levels are found with three levels set for probability and three others to define impact, 5 × 5, or even more levels (Duijm, 2015 ; Levine, 2012 ; Cox, 2008 ). The matrix classifies risks into different risk categories, normally labelled with qualitative indicators of severity (often colours like “Red”, “Yellow” and “Green”). This classification combines each likelihood level with every impact level in the matrix (see an example of a probability-impact matrix in Fig. 1 ).

Probability – impact matrix. An example of use.
There are three different risk matrix typologies based on the categorisation of likelihood and impact: qualitative, semiquantitative, and quantitative. Qualitative risk matrices provide descriptive assessments of probability and consequence by establishing categories as “low,” “medium” or “high” (based on the matrix’s specific number of levels). In contrast, semiquantitative risk matrices represent the input categories by ascending scores, such as 1, 2, or 3 (in a 3×3 risk matrix), where higher scores indicate a stronger impact or more likelihood. Finally, in quantitative risk matrices, each category receives an assignment of numerical intervals corresponding to probability or impact estimates. For example, the “Low” probability level is associated with a probability interval [0.1 0.3] (Li et al. 2018 ).
Qualitative matrices classify risks according to their potential hazard, depending on where they fit into the matrix. The risk level is defined by the “colour” of the corresponding cell (in turn, this depends on the probability and impact level), with risks classified with “red” being the most important and the priority ones to pay attention to, but without distinguishing any risks in the different cells of the same colour. In contrast, quantitative risk matrices allow to classify risks according to their risk level (red, yellow, or green) and to prioritise each risk in the same colour by indicating which is the most important. Each cell is assigned a colour and a numerical value, and the product of the value is usually assigned to the probability level and the value assigned to the impact level (Risk = probability × impact).
Risk matrix use is frequent, partly due to its simple application and easy construction compared to alternative risk assessment methods (Levine, 2012 ). Risk matrices offer a well-defined structure for carrying out a methodical risk assessment, provide a practical justification for ranking and prioritising risks, visually and attractively inform stakeholders, among other reasons (Talbot, 2014 ; Ball and Watt, 2013 ).
However, many authors identify problems in using risk matrices (Monat and Doremus, 2020 ; Peace, 2017 ; Levine, 2012 ; Ni et al. 2010 ; Cox, 2008 ; Cox et al. 2005 ), and even the International Organization for Standardization ( 2019 ) indicates some drawbacks. The most critical problems identified in using risk matrices for strategic decision-making are that risk matrices can be inaccurate when comparing risks and they sometimes assign similar ratings to risks with significant quantitative differences. In addition, there is the risk of giving excessively high qualitative ratings to risks that are less serious from a quantitative perspective. This can lead to suboptimal decisions, especially when threats have negative correlations in frequency and severity terms. Such lack of precision can result in inefficient resource allocation because they cannot be based solely on the categories provided by risk matrices. Furthermore, the categorisation of the severity of consequences is subjective in uncertainty situations, and the assessment of probability, impact and risk ratings very much depends on subjective interpretations, which can lead to discrepancies between different users when assessing the same quantitative risks.
Given this background, several authors propose solutions to the posed problems. Goerlandt and Reniers ( 2016 ) review previous works that have attempted to respond to the problems identified with risk matrices. For example, Markowski and Mannan ( 2008 ) suggest using fuzzy sets to consider imprecision in describing ordinal linguistic scales. Subsequently, Ni et al. ( 2010 ) propose a methodology that employs probability and consequence ranks as independent score measures. Levine ( 2012 ) puts forward the use of logarithmic scales on probability and impact axes. Menge et al. (2018) recommend utilising untransformed values as scale labels due to experts’ misunderstanding of logarithmic scales. Ruan et al. ( 2015 ) suggest an approach that considers decision makers’ risk aversion by applying the utility theory.
Other authors, such as Duijm ( 2015 ), propose a continuous probability consequence diagram as an alternative to the risk matrix, and employing continuous scales instead of categories. They also propose utilising more comprehensive colour ranges in risk matrices whenever necessary to prioritise risks and to not simply accept them. In contrast, Monat and Doremus ( 2020 ) put forward a new risk prioritisation tool. Alternatively, Sutherland et al. ( 2022 ) suggest changing matrix size by accommodating cells’ size to the risk’s importance. Even Proto et al. ( 2023 ) recommend avoiding colour in risk matrices so that the provided information is unbiased due to the bias that arises when using coloured matrices.
By bearing in mind the difficulties presented by the results offered by risk matrices, we propose a quantitative method for risk prioritisation. We use qualitative risk analysis data by maintaining the estimate of the probability of each risk occurring and its potential impact. Nevertheless, instead of entering these data into the risk matrix, our project model contains them for Monte Carlo simulation. As a result, we obtain a quantified prioritisation of each risk that differentiates the importance of each risk according to the impact on cost and duration objectives.
Methodology
Figure 2 depicts the proposed method for prioritising project risks using quantitative techniques. At the end of the process, and with the prioritised risks indicating the absolute value of the impact of each risk on the project, the organisation can efficiently allocate resources to the risks identified as the most critical ones.

Quantitative Risk Assessment Flow Chart.
The top of the diagram indicates the risk phases that belong to the overall risk management process. Below them it reflects the steps of the proposed model that would apply in each phase.
The first step corresponds to the project’s “ risk identification ”. Using the techniques or tools established by the organisation (brainstorming, Delphi techniques, interviews, or others), we obtain a list of the risks ( R ) that could impact the project objectives (Eq. 1 ), where m is the number of risks identified in the project.
Next we move on to the “ risk estimation ” phase, in which a distribution function must be assigned to the probability that each identified risk will appear. We also assign the distribution function associated with the risk’s impact. Traditionally, the qualitative risk analysis defines semantic values (low, medium, high) to assign a level of probability and risk impact. These semantic values are used to evaluate the risk in the probability-impact matrix. Numerical scales apply in some cases, which help to assign a semantic level to a given risk (Fig. 3 ).

Source: Project Management Institute ( 2017 ).
Our proposed model includes the three uncertainty types put forward by Hillson ( 2014 ), namely aleatoric, stochastic and epistemic, to identify and assess different risks. Ontological uncertainty is not considered because it goes beyond the limits of human knowledge and cannot, therefore, be modelled (Alleman et al. 2018a ).
A risk can have aleatoric uncertainty as regards the probability of its occurrence, and mainly for its impact if its value can fluctuate over a set range due to its variability. This aleatoric risk uncertainty can be modelled using a probability distribution function (PDF), exactly as we do when modelling activity uncertainty (Acebes et al. 2015 , 2014 ). As the risk management team’s (or project management team’s) knowledge of the project increases, and as more information about the risk becomes available, the choice of the PDF (normal, triangular, beta, among others) and its parameters become more accurate.
A standard definition of risk is “an uncertain event that, if it occurs, may impact project objectives” (Project Management Institute, 2017 ). A risk, if defined according to the above statement, perfectly matches the stochastic uncertainty definition proposed by Hillson ( 2014 ). Moreover, one PDF that adequately models this type of uncertainty is a Bernoulli distribution function (Vose, 2008 ). Thus for deterministic risk probability estimates (the same as for risk impact), we model this risk (probability and impact) with a Bernoulli-type PDF that allows us to introduce this type of uncertainty into our simulation model.
Finally, epistemic uncertainties remain to be modelled, such as those for which we do not have absolute information about and that arise from a lack of knowledge (Damnjanovic and Reinschmidt, 2020 ; Alleman et al. 2018b ). In this case, risks (in likelihood and impact terms) are classified into different levels, and all these levels are assigned a numerical scale (as opposed to the methodology used in a qualitative risk analysis, where levels are classified with semantic values: “high”, “medium” and “low”).
“ Epistemic uncertainty is characterised by not precisely knowing the probability of occurrence or the magnitude of a potential impact. Traditionally, this type of risk has been identified with a qualitative term: “Very Low”, “Low”, “Medium”, “High” and “Very High” before using the probability-impact matrix. Each semantic category has been previously defined numerically by identifying every numerical range with a specific semantic value (Bae et al. 2004 ). For each established range, project managers usually know the limits (upper and lower) between which the risk (probability or impact) can occur. However, they do not certainly know the value it will take, not even the most probable value within that range. Therefore, we employ a uniform probability function to model epistemic uncertainty (i.e., by assuming that the probability of risk occurrence lies within an equiprobable range of values). Probabilistic representations of uncertainty have been successfully employed with uniform distributions to characterise uncertainty when knowledge is sparse or absent (Curto et al. 2022 ; Vanhoucke, 2018 ; Helton et al. 2006 ).
The choice of the number and range of each level should be subject to a thorough analysis and consideration by the risk management team. As each project is unique, there are ranges within which this type of uncertainty can be categorised. Different ranges apply to assess likelihood and impact. Furthermore for impact, further subdivision helps to distinguish between impact on project duration and impact on project costs. For example, when modelling probability, we can set five probability levels corresponding to intervals: [0 0.05], [0.05 0.2], [0.2 0.5], and so on. With the time impact, for example, on project duration, five levels as follows may apply: [0 1], [1 4], [4 12], …. (measured in weeks, for example).
Modelling this type of uncertainty requires the risk management team’s experience, the data stored on previous projects, and constant consultation with project stakeholders. The more project knowledge available, the more accurate the proposed model is for each uncertainty, regardless of it lying in the number of intervals, their magnitude or the type of probability function (PDF) chosen to model that risk.
Some authors propose using uniform distribution functions to model this type of epistemic uncertainty because it perfectly reflects lack of knowledge about the expected outcome (Eldosouky et al. 2014 ; Vose, 2008 ). On the contrary, others apply triangular functions, which require more risk knowledge (Hulett, 2012 ). Following the work by Curto et al. ( 2022 ), we employ uniform distribution functions.
As a result of this phase, we obtain the model and the parameters that model the distribution functions of the probability ( P ) and impact ( I ) of each identified risk in the previous phase (Eq. 2 ).
Once the risks identified in the project have been defined and their probabilities and impacts modelled, we move on to “ quantitative risk prioritisation ”. We start by performing MCS on the planned project model by considering only the aleatoric uncertainty of activities. In this way, we learn the project’s total duration and cost, which is commonly done in a Monte Carlo analysis. In Monte Carlo Methods (MCS), expert judgement and numerical methods are combined to generate a probabilistic result through simulation routine (Ammar et al. 2023 ). This mathematical approach is noted for its ability to analyse uncertain scenarios from a probabilistic perspective. MCS have been recognised as outperforming other methods due to their accessibility, ease of use and simplicity. MCS also allow the analysis of opportunities, uncertainties, and threats (Al-Duais and Al-Sharpi, 2023 ). This technique can be invaluable to risk managers and helpful for estimating project durations and costs (Ali Elfarra and Kaya, 2021 ).
As inputs to the simulation process, we include defining project activities (duration, cost, precedence relationship). We also consider the risks identified in the project, which are those we wish to prioritise and to obtain a list ordered by importance (according to their impact on not only duration, but also on project cost). The ‘MCSimulRisk’ software application (Acebes, Curto, et al. 2023 ; Acebes, De Antón, et al. 2023 ) allows us to perform MCS and to obtain the main statistics that result from simulation (including percentiles) that correspond to the total project duration ( Tot_Dur ) and to its total cost ( Tot_Cost ) (Eq. 3 ).
Next, we perform a new simulation by including the first of the identified risks ( R 1 ) in the project model, for which we know its probability ( P 1 ) and its Impact ( I 1 ). After MCS, we obtain the statistics corresponding to this simulation ([ Tot_Dur 1 Tot_Cost 1 ]). We repeat the same operation with each identified risk ( R i , i = 1, …, m ) and obtain the main statistics corresponding to each simulation (Eq. 4 ).
Once all simulations (the same number as risks) have been performed, we must choose a confidence percentile to calculate risk prioritisation (Rezaei et al. 2020 ; Sarykalin et al. 2008 ). Given that the total duration and cost results available to us, obtained by MCS, are stochastic and have variability (they are no longer constant or deterministic), we must choose a percentile (α) that conveys the risk appetite that we are willing to assume when calculating. Risk appetite is “ the amount and type of risk that an organisation is prepared to pursue, retain or take ” (International Organization for Standardization, 2018 ).
A frequently employed metric for assessing risk in finance is the Value at Risk (VaR) (Caron, 2013 ; Caron et al. 2007 ). In financial terms, it is traditional to choose a P95 percentile as risk appetite (Chen and Peng, 2018 ; Joukar and Nahmens, 2016 ; Gatti et al. 2007 ; Kuester et al. 2006 ; Giot and Laurent, 2003 ). However in project management, the P80 percentile is sometimes chosen as the most appropriate percentile to measure risk appetite (Kwon and Kang, 2019 ; Traynor and Mahmoodian, 2019 ; Lorance and Wendling, 2001 ).
Finally, after choosing the risk level we are willing to assume, we need to calculate how each risk impacts project duration ( Imp_D Ri ) and costs ( Imp_C Ri ). To do so, we subtract the original value of the total project expected duration and costs (excluding all risks) from the total duration and costs of the simulation in which we include the risk we wish to quantify (Eq. 5 ).
Finally, we present these results on two separate lists, one for the cost impact and one for the duration impact, by ranking them according to their magnitude.
In this section, we use a real-life project to illustrate how to apply the proposed method for quantitative risk prioritisation purposes. For this purpose, we choose an engineering, procurement and construction project undertaken in South America and used in the literature by Votto et al. ( 2020a , 2020b ).
Project description
The project used as an application example consists of the expansion of an industrial facility. It covers a wide spectrum of tasks, such as design and engineering work, procurement of machinery and its components, civil construction, installation of all machinery, as well as commissioning and starting up machines (Votto et al. 2020a , 2020b ).
Table 2 details the parameters that we use to define activities. The project comprises 32 activities, divided into three groups: engineering, procurement and construction (EPC). A fictitious initial activity ( Ai ) and a fictitious final activity ( Af ) are included. We employ triangular distribution functions, whose parameters are the minimum value ( Min ), the most probable value ( Mp ) and the maximum value ( Max ), to model the random duration of activities, expressed as days. We divide the cost of each activity in monetary units into a fixed cost ( FC ), independently of activity duration, and the variable cost ( VC ), which is directly proportional to project duration. As activity duration can vary, and the activity cost increases directly with its duration, the total project cost also exhibits random variations.
Under these conditions, the planned project duration is 300 days and has a planned cost of 30,000 (x1000) monetary units. Figure 4 shows the Planned Value Curve of the project.

Planned value curve of the real-life project.
The next step in the methodology (Fig. 2 ) is to identify the project risks. To do this, the experts’ panel meets, analyses all the project documentation. Based on their personal experience with other similar projects and after consulting all the involved stakeholders, it provides a list of risks (see Table 3 ).
It identifies 11 risks, of which nine have the potential to directly impact the project duration objective (R1 to R9), while six may impact the cost objective (R10 to R15). The risks that might impact project duration and cost have two assigned codes. We identify the project phase and activity on which all the identified risks may have an impact (Table 3 ).
The next step is to estimate the likelihood and impact of the identified risks (qualitative analysis). Having analysed the project and consulted the involved stakeholders, the team determines the project’s different probability and impact levels (duration and cost). The estimation of these ranges depends on the project budget, the estimated project duration, and the team’s experience in assigning the different numerical values to each range. As a result, the project team is able to construct the probability-impact matrix shown in Fig. 5 .

Estimation of the probability and impact ranges.
Each probability range for risk occurrence in this project is defined. Thus for a very low probability (VL), the assigned probability range is between 0 and 3% probability, for a low level (L), the assigned range lies between 3% and 10% probability of risk occurrence, and so on with the other established probability ranges (medium, high, very high).
The different impact ranges are also defined by differentiating between impacts in duration and cost terms. Thus a VL duration impact is between 0 and 5 days, while the same range (VL) in cost is between 0 and 100 (x1000) monetary units. Figure 5 shows the other ranges and their quantification in duration and cost terms.
The combination of each probability level and every impact level coincides in a cell of the risk matrix (Fig. 5 ) to indicate the risk level (“high”, “medium”, and “low”) according to the qualitative analysis. Each cell is assigned a numerical value by prioritising the risks at the same risk level. This work uses the matrix to compare the risk prioritisation results provided by this matrix to those provided by the proposed quantitative method.
A probability and impact value are assigned to each previously identified risk (Table 3 ). Thus, for example, for the risk called “Interruptions in the supply chain”, coded as R3 for impacting activity 13 duration, we estimate an L probability and a strong impact on duration (H). As this same risk might impact the activity 13 cost, it is also coded as R12, and its impact on cost is estimated as L (the probability is the same as in R3; Table 3 ).
Finally, to conclude the proposed methodology and to prioritise the identified risks, we use the “MCSimulRisk” software application by incorporating MCS (in this work, we employ 20,000 iterations in each simulation). Activities are modelled using triangular distribution functions to incorporate project information into the simulation application. Costs are modelled with fixed and variable costs depending on the duration of the corresponding activity. Furthermore, risks (probability and impact) are modelled by uniform distribution functions. Figure 6 depicts the project network and includes the identified risks that impact the corresponding activities.

Network diagram of the project together with the identified risks.
Results and discussion
In order to obtain the results of prioritising the identified risks, we must specify a percentile that determines our risk aversion. This is the measure by which we quantify the risk. Figure 7 graphically justifies the choice of P95 as a risk measure, as opposed to a lower percentile, which corroborates the view in the literature and appears in Methodology . In Fig. 7 , we plot the probability distribution and cumulative distribution functions corresponding to the total project planned cost, together with the cost impact of one of the risks. The impact caused by the risk on the total cost corresponds to the set of iterations whose total cost is higher than that planned (bottom right of the histogram).

Source: MCSimulRisk.
By choosing P95 as VaR, we can consider the impact of a risk on the project in the measure. In this example, for P95 we obtain a total cost value of 3.12 × 10 7 monetary units. Choosing a lower percentile, e.g. P80, means that the value we can obtain with this choice can be considerably lower (3.03 × 10 7 monetary units), and might completely ignore the impact of the risk on the total project cost. However, project managers can choose the percentile that represents their risk aversion.
Once the percentile on which to quantify the risk is chosen, the “MCSimulRisk” application provides us with the desired results for prioritising project risks (Fig. 8 ). For the chosen percentile (P95), which represents our risk appetite for this project, the planned project duration is 323.43 days. In other words, with a 95% probability the planned project will be completed before 323.43 days. Similarly, the P95 corresponding to cost is 30,339 ×1000 monetary units. The application also provides us with the project duration in the first column of Fig. 8 after incorporating all the identified risks (corresponding to a P95 risk appetite) into the planned project. Column 2 of the same figure shows the project cost after incorporating the corresponding risk into the model.

The first column corresponds to the risks identified. Columns Duration_with_Ri and Cost_with_Ri represent the simulation values, including the corresponding risk. Columns Difference_Duration_with_Ri and Difference_Cost_with_Ri represent the difference in duration and cost of each simulation concerning the value obtained for the chosen percentile. Finally, Ranking_Dur and Ranking_Cost represent the prioritisation of risks in duration and cost, respectively.
With the results in the first two columns (total project duration and cost after incorporating the corresponding risks), and by knowing the planned total project duration and cost (without considering risks) for a given percentile (P95), we calculate the values of the following columns in Fig. 8 . Thus column 3 represents the difference between the planned total project duration value (risk-free) and project duration by incorporating the corresponding risk that we wish to quantify. Column 4 prioritises the duration risks by ranking according to the duration that each risk contributes to the project. Column 5 represents the difference between the planned total project cost (risk-free) and the total project cost by incorporating the corresponding risk. Finally, Column 6 represents the ranking or prioritisation of the project risks according to their impact on cost.
To compare the results provided by this methodology in this paper we propose quantitative risk prioritisation, based on MCS. We draw up Table 4 with the results provided by the probability-impact matrix (Fig. 5 ).
The first set of columns in Table 4 corresponds to the implementation of the risk matrix (probability-impact matrix) for the identified risks. The second group of columns represents the prioritisation of risks according to their impact on duration (data obtained from Fig. 8 ). The third group corresponds to the risk prioritisation according to their impact on cost (data obtained from Fig. 8 ).
For the project proposed as an example, we find that risk R3 is the most important one if we wish to control the total duration because it corresponds to the risk that contributes the most duration to the project if it exists. We note that risks R10 to R15 do not impact project duration. If these risks materialise, their contribution to increase (or decrease, as the case may be) project duration is nil.
On the impact on project costs, we note that risk R15 is the most important. It is noteworthy that risk R5 is the fourth most important risk in terms of impact on the total project costs, even though it is initially identified as a risk that impacts project duration. Unlike cost risks (which do not impact the total project duration), the risks that can impact project duration also impact total costs.
We can see that the order of importance of the identified risks differs depending on our chosen method (risk matrix versus quantitative prioritisation). We independently quantify each risk’s impact on the cost and duration objectives. We know not only the order of importance of risks (R3, R5, etc.) but also the magnitude of their impact on the project (which is the absolute delay caused by a risk in duration terms or what is the absolute cost overrun generated by a risk in cost terms). It seems clear that one risk is more important than another, not only because of the estimation of its probability and impact but also because the activity on which it impacts may have a high criticality index or not (probability of belonging to the project’s critical path).
As expected, the contribution to the total duration of the identified risks that impact only cost is zero. The same is not valid for the risks identified to have an impact on duration because the latter also impacts the cost objective. We also see how the risks that initially impact a duration objective are more critical for their impact on cost than others that directly impact the project’s cost (e.g. R5).
Conclusions
The probability-impact matrix is used in project management to identify the risk to which the most attention should be paid during project execution. This paper studies how the risk matrix is adopted by a large majority of standards, norms and methodologies in project management and, at the same time, practitioners and academics recognise it as a fundamental tool in the qualitative risks analysis.
However, we also study how this risk matrix presents particular problems and offers erroneous and contradictory results. Some studies suggest alternatives to its use. Notwithstanding, it continues to be a widely employed tool in the literature by practitioners and academics. Along these lines, with this work we propose an alternative to the probability-impact matrix as a tool to know the most critical risk for a project that can prevent objectives from being fulfilled.
For this purpose, we propose a quantitative method based on MCS, which provides us with numerical results of the importance of risks and their impact on total duration and cost objectives. This proposed methodology offers significant advantages over other risk prioritisation methods and tools, especially the traditional risk matrix. The proposed case study reveals that risk prioritisation yields remarkably different results depending on the selected method, as our findings confirm.
In our case, we obtain numerical values for the impact of risks on total duration and cost objectives, and independently of one another. This result is interesting for project managers because they can focus decision-making on the priority order of risks and the dominant project objective (total duration or total cost) if they do not coincide.
From the obtained results, we find that the risks with an impact on the cost of activities do not influence the total duration result. The risks that impact project duration also impact the total cost target. This impact is more significant than that of a risk that impacts only the activity’s cost. This analysis leads us to believe that this quantitative prioritisation method has incredible potential for academics to extend their research on project risks and for practitioners to use it in the day-to-day implementation of their projects.
The proposed methodology will allow project managers to discover the most relevant project risks so they can focus their control efforts on managing those risks. Usually, implementing risk response strategies might be expensive (control efforts, insurance contracts, preventive actions, or others). Therefore, it is relevant to concentrate only on the most relevant risks. The proposed methodology allows project managers to select the most critical risks by overcoming the problems exhibited by previous methodologies like the probability-impact matrix.
In addition to the above, the risk prioritisation achieved by applying the proposed methodology is based on quantifying the impacts that risks may have on the duration and cost objectives of the project. Finally, we achieve an independent risk prioritisation in duration impact and project cost impact terms. This is important because the project manager can attach more importance to one risk or other risks depending on the priority objective that predominates in the project, the schedule or the total cost.
Undoubtedly, the reliability of the proposed method depends mainly on the accuracy of estimates, which starts by identifying risks and ends with modelling the probability and impact of each risk. The methodology we propose in this paper overcomes many of the problems of previous methodologies, but still has some limitations for future research to deal with. First of all, the results of simulations depend on the estimations of variables (probability distributions and their parameters, risk aversion parameters, etc.). Methodologies for improving estimations are beyond the scope of this research; we assume project teams are sufficient experts to make rational estimationsbased on experience and previous knowledge. Secondly, as risks are assumed to be independent, the contribution or effect of a particular risk can be estimated by including it in simulation and by computing its impact on project cost and duration. This is a reasonable assumption for most projects. In some very complex projects, however, risks can be related to one another. Further research should be done to face this situation.
As an additional research line, we plan to conduct a sensitivity study by simulating many different projects to analyse the robustness of the proposed method.
Finally, it is desirable to implement this methodology in real projects and see how it responds to the reality of a project in, for example, construction, industry, or any other sector that requires a precise and differentiated risk prioritisation.
Data availability
Data will be made available on request.
Acebes F, Curto D, De Antón J, Villafáñez, F (2024) Análisis cuantitativo de riesgos utilizando “MCSimulRisk” como herramienta didáctica. Dirección y Organización , 82(Abril 2024), 87–99. https://doi.org/10.37610/dyo.v0i82.662
Acebes F, De Antón J, Villafáñez F, Poza, D (2023) A Matlab-Based Educational Tool for Quantitative Risk Analysis. In IoT and Data Science in Engineering Management (Vol. 160). Springer International Publishing. https://doi.org/10.1007/978-3-031-27915-7_8
Acebes F, Pajares J, Galán JM, López-Paredes A (2014) A new approach for project control under uncertainty. Going back to the basics. Int J Proj Manag 32(3):423–434. https://doi.org/10.1016/j.ijproman.2013.08.003
Article Google Scholar
Acebes F, Pereda M, Poza D, Pajares J, Galán JM (2015) Stochastic earned value analysis using Monte Carlo simulation and statistical learning techniques. Int J Proj Manag 33(7):1597–1609. https://doi.org/10.1016/j.ijproman.2015.06.012
Al-Duais FS, Al-Sharpi RS (2023) A unique Markov chain Monte Carlo method for forecasting wind power utilizing time series model. Alex Eng J 74:51–63. https://doi.org/10.1016/j.aej.2023.05.019
Ale B, Burnap P, Slater D (2015) On the origin of PCDS - (Probability consequence diagrams). Saf Sci 72:229–239. https://doi.org/10.1016/j.ssci.2014.09.003
Ali Elfarra M, Kaya M (2021) Estimation of electricity cost of wind energy using Monte Carlo simulations based on nonparametric and parametric probability density functions. Alex Eng J 60(4):3631–3640. https://doi.org/10.1016/j.aej.2021.02.027
Alleman GB, Coonce TJ, Price RA (2018a) Increasing the probability of program succes with continuous risk management. Coll Perform Manag, Meas N. 4:27–46
Google Scholar
Alleman GB, Coonce TJ, Price RA (2018b) What is Risk? Meas N. 01(1):25–34
Ammar T, Abdel-Monem M, El-Dash K (2023) Appropriate budget contingency determination for construction projects: State-of-the-art. Alex Eng J 78:88–103. https://doi.org/10.1016/j.aej.2023.07.035
Axelos (2023) Managing Successful Projects with PRINCE2® 7th ed . (AXELOS Limited, Ed.; 7th Ed). TSO (The Stationery Office)
Bae HR, Grandhi RV, Canfield RA (2004) Epistemic uncertainty quantification techniques including evidence theory for large-scale structures. Comput Struct 82(13–14):1101–1112. https://doi.org/10.1016/j.compstruc.2004.03.014
Ball DJ, Watt J (2013) Further thoughts on the utility of risk matrices. Risk Anal 33(11):2068–2078. https://doi.org/10.1111/risa.12057
Article PubMed Google Scholar
Caron F (2013) Quantitative analysis of project risks. In Managing the Continuum: Certainty, Uncertainty, Unpredictability in Large Engineering Projects (Issue 9788847052437, pp. 75–80). Springer, Milano. https://doi.org/10.1007/978-88-470-5244-4_14
Caron F, Fumagalli M, Rigamonti A (2007) Engineering and contracting projects: A value at risk based approach to portfolio balancing. Int J Proj Manag 25(6):569–578. https://doi.org/10.1016/j.ijproman.2007.01.016
Chapman CB (1997) Project risk analysis and management– PRAM the generic process. Int J Proj Manag 15(5):273–281. https://doi.org/10.1016/S0263-7863(96)00079-8
Chapman CB, Ward S (2003) Project Risk Management: Processes, Techniques and Insights (John Wiley and Sons, Ed.; 2nd ed.). Chichester
Chen P-H, Peng T-T (2018) Value-at-risk model analysis of Taiwanese high-tech facility construction. J Manag Eng, 34 (2). https://doi.org/10.1061/(asce)me.1943-5479.0000585
Cox LA (2008) What’s wrong with risk matrices? Risk Anal 28(2):497–512. https://doi.org/10.1111/j.1539-6924.2008.01030.x
Cox LA, Babayev D, Huber W (2005) Some limitations of qualitative risk rating systems. Risk Anal 25(3):651–662. https://doi.org/10.1111/j.1539-6924.2005.00615.x
Creemers S, Demeulemeester E, Van de Vonder S (2014) A new approach for quantitative risk analysis. Ann Oper Res 213(1):27–65. https://doi.org/10.1007/s10479-013-1355-y
Article MathSciNet Google Scholar
Curto D, Acebes F, González-Varona JM, Poza D (2022) Impact of aleatoric, stochastic and epistemic uncertainties on project cost contingency reserves. Int J Prod Econ 253(Nov):108626. https://doi.org/10.1016/j.ijpe.2022.108626
Damnjanovic I, Reinschmidt KF (2020) Data Analytics for Engineering and Construction Project Risk Management . Springer International Publishing
Duijm NJ (2015) Recommendations on the use and design of risk matrices. Saf Sci 76:21–31. https://doi.org/10.1016/j.ssci.2015.02.014
Eldosouky IA, Ibrahim AH, Mohammed HED (2014) Management of construction cost contingency covering upside and downside risks. Alex Eng J 53(4):863–881. https://doi.org/10.1016/j.aej.2014.09.008
Elms DG (2004) Structural safety: Issues and progress. Prog Struct Eng Mater 6:116–126. https://doi.org/10.1002/pse.176
European Commission. (2023) Project Management Methodology. Guide 3.1 (European Union, Ed.). Publications Office of the European Union
Frank M (1999) Treatment of uncertainties in space nuclear risk assessment with examples from Cassini mission implications. Reliab Eng Syst Safe 66:203–221. https://doi.org/10.1016/S0951-8320(99)00002-2
Gatti S, Rigamonti A, Saita F, Senati M (2007) Measuring value-at-risk in project finance transactions. Eur Financ Manag 13(1):135–158. https://doi.org/10.1111/j.1468-036X.2006.00288.x
Giot P, Laurent S (2003) Market risk in commodity markets: a VaR approach. Energy Econ 25:435–457. https://doi.org/10.1016/S0140-9883(03)00052-5
Goerlandt F, Reniers G (2016) On the assessment of uncertainty in risk diagrams. Saf Sci 84:67–77. https://doi.org/10.1016/j.ssci.2015.12.001
Helton JC, Johnson JD, Oberkampf WL, Sallaberry CJ (2006) Sensitivity analysis in conjunction with evidence theory representations of epistemic uncertainty. Reliab Eng Syst Saf 91(10–11):1414–1434. https://doi.org/10.1016/j.ress.2005.11.055
Hillson D (2014) How to manage the risks you didn’t know you were taking. Paper presented at PMI® Global Congress 2014—North America, Phoenix, AZ. Newtown Square, PA: Project Management Institute
Hillson D, Simon P (2020) Practical Project Risk Management. THE ATOM METHODOLOGY (Third Edit, Issue 1). Berrett-Koehler Publishers, Inc
Hulett DT (2012) Acumen Risk For Schedule Risk Analysis - A User’s Perspective . White Paper. https://info.deltek.com/acumen-risk-for-schedule-risk-analysis
International Organization for Standardization. (2018). ISO 31000:2018 Risk management – Guidelines (Vol. 2)
International Organization for Standardization. (2019). ISO/IEC 31010:2019 Risk management - Risk assessment techniques
International Project Management Association. (2015). Individual Competence Baseline for Project, Programme & Portfolio Management. Version 4.0. In International Project Management Association (Vol. 4). https://doi.org/10.1002/ejoc.201200111
Joukar A, Nahmens I (2016) Estimation of the Escalation Factor in Construction Projects Using Value at Risk. Construction Research Congress , 2351–2359. https://doi.org/10.1061/9780784479827.234
Kerzner H (2022) Project Management. A Systems Approach to Planning, Scheduling, and Controlling (Inc. John Wiley & Sons, Ed.; 13th Editi)
Koulinas GK, Demesouka OE, Sidas KA, Koulouriotis DE (2021) A topsis—risk matrix and Monte Carlo expert system for risk assessment in engineering projects. Sustainability 13(20):1–14. https://doi.org/10.3390/su132011277
Krisper M (2021) Problems with Risk Matrices Using Ordinal Scales . https://doi.org/10.48550/arXiv.2103.05440
Kuester K, Mittnik S, Paolella MS (2006) Value-at-risk prediction: A comparison of alternative strategies. J Financ Econ 4(1):53–89. https://doi.org/10.1093/jjfinec/nbj002
Kwon H, Kang CW (2019) Improving project budget estimation accuracy and precision by analyzing reserves for both identified and unidentified risks. Proj Manag J 50(1):86–100. https://doi.org/10.1177/8756972818810963
Lemmens SMP, Lopes van Balen VA, Röselaers YCM, Scheepers HCJ, Spaanderman MEA (2022) The risk matrix approach: a helpful tool weighing probability and impact when deciding on preventive and diagnostic interventions. BMC Health Serv Res 22(1):1–11. https://doi.org/10.1186/s12913-022-07484-7
Levine ES (2012) Improving risk matrices: The advantages of logarithmically scaled axes. J Risk Res 15(2):209–222. https://doi.org/10.1080/13669877.2011.634514
Article ADS Google Scholar
Li J, Bao C, Wu D (2018) How to design rating schemes of risk matrices: a sequential updating approach. Risk Anal 38(1):99–117. https://doi.org/10.1111/risa.12810
Lorance RB, Wendling RV (2001) Basic techniques for analyzing and presentation of cost risk analysis. Cost Eng 43(6):25–31
Markowski AS, Mannan MS (2008) Fuzzy risk matrix. J Hazard Mater 159(1):152–157. https://doi.org/10.1016/j.jhazmat.2008.03.055
Article CAS PubMed Google Scholar
Menge DNL, MacPherson AC, Bytnerowicz TA et al. (2018) Logarithmic scales in ecological data presentation may cause misinterpretation. Nat Ecol Evol 2:1393–1402. https://doi.org/10.1038/s41559-018-0610-7
Monat JP, Doremus S (2020) An improved alternative to heat map risk matrices for project risk prioritization. J Mod Proj Manag 7(4):214–228. https://doi.org/10.19255/JMPM02210
Naderpour H, Kheyroddin A, Mortazavi S (2019) Risk assessment in bridge construction projects in Iran using Monte Carlo simulation technique. Pract Period Struct Des Constr 24(4):1–11. https://doi.org/10.1061/(asce)sc.1943-5576.0000450
Ni H, Chen A, Chen N (2010) Some extensions on risk matrix approach. Saf Sci 48(10):1269–1278. https://doi.org/10.1016/j.ssci.2010.04.005
Peace C (2017) The risk matrix: Uncertain results? Policy Pract Health Saf 15(2):131–144. https://doi.org/10.1080/14773996.2017.1348571
Project Management Institute. (2009) Practice Standard for Project Risk Management . Project Management Institute, Inc
Project Management Institute. (2017) A Guide to the Project Management Body of Knowledge: PMBoK(R) Guide. Sixth Edition (6th ed.). Project Management Institute Inc
Project Management Institute. (2019) The standard for Risk Management in Portfolios, Programs and Projects . Project Management Institute, Inc
Project Management Institute. (2021) A Guide to the Project Management Body of Knowledge: PMBoK(R) Guide. Seventh Edition (7th ed.). Project Management Institute, Inc
Proto R, Recchia G, Dryhurst S, Freeman ALJ (2023) Do colored cells in risk matrices affect decision-making and risk perception? Insights from randomized controlled studies. Risk Analysis , 1–15. https://doi.org/10.1111/risa.14091
Qazi A, Dikmen I (2021) From risk matrices to risk networks in construction projects. IEEE Trans Eng Manag 68(5):1449–1460. https://doi.org/10.1109/TEM.2019.2907787
Qazi A, Shamayleh A, El-Sayegh S, Formaneck S (2021) Prioritizing risks in sustainable construction projects using a risk matrix-based Monte Carlo Simulation approach. Sustain Cities Soc 65(Aug):102576. https://doi.org/10.1016/j.scs.2020.102576
Qazi A, Simsekler MCE (2021) Risk assessment of construction projects using Monte Carlo simulation. Int J Manag Proj Bus 14(5):1202–1218. https://doi.org/10.1108/IJMPB-03-2020-0097
Rehacek P (2017) Risk management standards for project management. Int J Adv Appl Sci 4(6):1–13. https://doi.org/10.21833/ijaas.2017.06.001
Rezaei F, Najafi AA, Ramezanian R (2020) Mean-conditional value at risk model for the stochastic project scheduling problem. Comput Ind Eng 142(Jul):106356. https://doi.org/10.1016/j.cie.2020.106356
Ruan X, Yin Z, Frangopol DM (2015) Risk Matrix integrating risk attitudes based on utility theory. Risk Anal 35(8):1437–1447. https://doi.org/10.1111/risa.12400
Sarykalin S, Serraino G, Uryasev S (2008) Value-at-risk vs. conditional value-at-risk in risk management and optimization. State-of-the-Art Decision-Making Tools in the Information-Intensive Age, October 2023 , 270–294. https://doi.org/10.1287/educ.1080.0052
Simon P, Hillson D, Newland K (1997) PRAM Project Risk Analysis and Management Guide (P. Simon, D. Hillson, & K. Newland, Eds.). Association for Project Management
Sutherland H, Recchia G, Dryhurst S, Freeman ALJ (2022) How people understand risk matrices, and how matrix design can improve their use: findings from randomized controlled studies. Risk Anal 42(5):1023–1041. https://doi.org/10.1111/risa.13822
Talbot, J (2014). What’s right with risk matrices? An great tool for risk managers… 31000risk. https://31000risk.wordpress.com/article/what-s-right-with-risk-matrices-3dksezemjiq54-4/
Taroun A (2014) Towards a better modelling and assessment of construction risk: Insights from a literature review. Int J Proj Manag 32(1):101–115. https://doi.org/10.1016/j.ijproman.2013.03.004
The Standish Group. (2022). Chaos report . https://standishgroup.myshopify.com/collections/all
Thomas P, Bratvold RB, Bickel JE (2014) The risk of using risk matrices. SPE Econ Manag 6(2):56–66. https://doi.org/10.2118/166269-pa
Tong R, Cheng M, Zhang L, Liu M, Yang X, Li X, Yin W (2018) The construction dust-induced occupational health risk using Monte-Carlo simulation. J Clean Prod 184:598–608. https://doi.org/10.1016/j.jclepro.2018.02.286
Traynor BA, Mahmoodian M (2019) Time and cost contingency management using Monte Carlo simulation. Aust J Civ Eng 17(1):11–18. https://doi.org/10.1080/14488353.2019.1606499
Vanhoucke, M (2018). The data-driven project manager: A statistical battle against project obstacles. In The Data-Driven Project Manager: A Statistical Battle Against Project Obstacles . https://doi.org/10.1007/978-1-4842-3498-3
Vatanpour S, Hrudey SE, Dinu I (2015) Can public health risk assessment using risk matrices be misleading? Int J Environ Res Public Health 12(8):9575–9588. https://doi.org/10.3390/ijerph120809575
Article CAS PubMed PubMed Central Google Scholar
Vose, D (2008). Risk Analysis: a Quantitative Guide (3rd ed.) . Wiley
Votto R, Lee Ho L, Berssaneti F (2020a) Applying and assessing performance of earned duration management control charts for EPC project duration monitoring. J Constr Eng Manag 146(3):1–13. https://doi.org/10.1061/(ASCE)CO.1943-7862.0001765
Votto R, Lee Ho L, Berssaneti F (2020b) Multivariate control charts using earned value and earned duration management observations to monitor project performance. Comput Ind Eng 148(Sept):106691. https://doi.org/10.1016/j.cie.2020.106691
Ward S (1999) Assessing and managing important risks. Int J Proj Manag 17(6):331–336. https://doi.org/10.1016/S0263-7863(98)00051-9
Download references
Acknowledgements
This research has been partially funded by the Regional Government of Castile and Leon (Spain) and the European Regional Development Fund (ERDF, FEDER) with grant VA180P20.
Author information
Authors and affiliations.
GIR INSISOC. Dpto. de Organización de Empresas y CIM. Escuela de Ingenierías Industriales, Universidad de Valladolid, Pº Prado de la Magdalena s/n, 47011, Valladolid, Spain
F. Acebes & J. Pajares
GIR INSISOC. Dpto. Economía y Administración de Empresas, Universidad de Málaga, Avda. Cervantes, 2, 29071, Málaga, Spain
J. M. González-Varona & A. López-Paredes
You can also search for this author in PubMed Google Scholar
Contributions
FA developed the conceptualisation and the methodology. JMG contributed to the literature review and interpretations of the results for the manuscript. FA and JP collected the experimental data and developed all the analyses and simulations. AL supervised the project. FA and JP wrote the original draft, while AL and JMG conducted the review and editing. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Correspondence to F. Acebes .
Ethics declarations
Competing interests.
The authors declare no competing interests.
Ethical approval
Ethical approval was not required as the study did not involve human participants.
Informed consent
No human subjects are involved in this study.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ .
Reprints and permissions
About this article
Cite this article.
Acebes, F., González-Varona, J.M., López-Paredes, A. et al. Beyond probability-impact matrices in project risk management: A quantitative methodology for risk prioritisation. Humanit Soc Sci Commun 11 , 670 (2024). https://doi.org/10.1057/s41599-024-03180-5
Download citation
Received : 30 January 2024
Accepted : 13 May 2024
Published : 24 May 2024
DOI : https://doi.org/10.1057/s41599-024-03180-5
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies

Differentiating Lyme arthritis: a case-based review
- Case Based Review
- Published: 25 May 2024
Cite this article

- Ayse Mine Unlu ORCID: orcid.org/0000-0002-5541-0184 1 , 6 ,
- Nanna Skaarup Andersen ORCID: orcid.org/0000-0002-3927-9294 2 , 3 , 4 ,
- Sanne Løkkegaard Larsen ORCID: orcid.org/0000-0003-1923-9890 2 , 3 , 4 ,
- Sigurdur Skarphedinsson ORCID: orcid.org/0000-0001-8440-7040 4 , 5 ,
- Stavros Chrysidis ORCID: orcid.org/0000-0001-8583-6517 1 ,
- Fredrikke Christie Knudtzen ORCID: orcid.org/0000-0001-8348-7819 2 , 5 &
- Philip Rask Lage-Hansen ORCID: orcid.org/0000-0002-1449-254X 1
The incidence or prevalence of Lyme arthritis (LA) in Denmark is unknown and assumed very low. No published cases of polymerase chain reaction (PCR)-confirmed LA from Denmark exist. Clinically, LA does not differ from other rheumatic oligoarthritic disorders posing a differential diagnostic challenge. To review the incidence and prevalence of LA to our knowledge and to present a case series of PCR-confirmed LA cases from Denmark. We conducted a systematic literature review via MEDLINE and EMBASE to explore incidence and prevalence rates of LA. Additionally, we present six cases of patients diagnosed with LA in Denmark. Our literature review identified 23 studies reporting prevalence or incidence, yet only ten studies provided estimates ranging from 1.1 to 280/100.000 in the general population. Our case series identified six patients with LA from a localized region in Southern Denmark; all confirmed by Borrelia -specific real-time PCR from synovial fluid. The diagnostic delay was up to 38 months. All patients except one had a history of previous tick bites; none had erythema migrans lesions. All presented with recurrent arthritis in the knee joint, and two had arthritis in the wrist. The literature review showed an incidence of LA ranging from 1.1 to 15.8 per 100.000 in Europe. Our case series suggests a potentially higher prevalence of LA in Denmark than previously believed. Lack of tick exposure history, antibody assessments and test of Borrelia burgdorferi sensu lato DNA in synovial fluid might lead to misdiagnosed cases potentially explaining the assumed low incidence of LA in Denmark.
This is a preview of subscription content, log in via an institution to check access.
Access this article
Price includes VAT (Russian Federation)
Instant access to the full article PDF.
Rent this article via DeepDyve
Institutional subscriptions
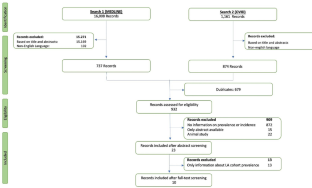
Stanek G, Fingerle V, Hunfeld K-P et al (2011) Lyme borreliosis: clinical case definitions for diagnosis and management in Europe. Clin Microbiol Infect 17:69–79. https://doi.org/10.1111/j.1469-0691.2010.03175.x
Article CAS PubMed Google Scholar
Kullberg BJ, Vrijmoeth HD, van de Schoor F, Hovius JW (2020) Lyme borreliosis: diagnosis and management. BMJ 369:m1041. https://doi.org/10.1136/bmj.m1041
Article PubMed Google Scholar
Rizzoli A, Hauffe H, Carpi G et al (2011) Lyme borreliosis in Europe. Euro Surveill 16:19906
Marques AR, Strle F, Wormser GP (2021) Comparison of Lyme Disease in the United States and Europe. Emerg Infect Dis 27:2017–2024. https://doi.org/10.3201/eid2708.204763
Article PubMed PubMed Central Google Scholar
Ocias LF, Jensen BB, Knudtzen FC et al (2017) [Clinical manifestations, diagnosis and treatment of Lyme borreliosis]. Ugeskr Laeger 179:V01170026
PubMed Google Scholar
Cardenas-de la Garza JA, De la Cruz-Valadez E, Ocampo-Candiani J, Welsh O (2019) Clinical spectrum of Lyme disease. Eur J Clin Microbiol Infect Dis 38:201–208. https://doi.org/10.1007/s10096-018-3417-1
Leth TA, Nymark A, Knudtzen FC et al (2023) Detection of Borrelia burgdorferi sensu lato DNA in cerebrospinal fluid samples following pre-enrichment culture. Ticks Tick Borne Dis 14:102138. https://doi.org/10.1016/j.ttbdis.2023.102138
Steere AC, Malawista SE, Snydman DR et al (1977) Lyme arthritis: an epidemic of oligoarticular arthritis in children and adults in three connecticut communities. Arthritis Rheum 20:7–17. https://doi.org/10.1002/art.1780200102
Steere AC, Broderick TF, Malawista SE (1978) Erythema Chronicum migrans and Lyme arthritis: epidemiologic evidence for a tick vector. Am J Epidemiol 108:312–321. https://doi.org/10.1093/oxfordjournals.aje.a112625
Kwit NA, Nelson CA, Max R, Mead PS (2018) Risk factors for clinician-diagnosed Lyme Arthritis, facial Palsy, Carditis, and Meningitis in patients from High-Incidence States. Open Forum Infect Dis 5:ofx254. https://doi.org/10.1093/ofid/ofx254
Berglund J, Hansen BU, Eitrem R (1995) Lyme arthritis–a common manifestation in a highly endemic area in Sweden. J Rheumatol 22:695–701
CAS PubMed Google Scholar
Söderlin MK, Börjesson O, Kautiainen H et al (2002) Annual incidence of inflammatory joint diseases in a population based study in southern Sweden. Ann Rheum Dis 61:911–915. https://doi.org/10.1136/ard.61.10.911
Haugeberg G, Hansen IJW, Skarpaas T et al (2014) Lyme arthritis in Southern Norway–an endemic area for Lyme borreliosis. BMC Infect Dis 14:185. https://doi.org/10.1186/1471-2334-14-185
Geebelen L, Van Cauteren D, Devleesschauwer B et al (2019) Combining primary care surveillance and a meta-analysis to estimate the incidence of the clinical manifestations of Lyme borreliosis in Belgium, 2015–2017. Ticks Tick Borne Dis 10:598–605. https://doi.org/10.1016/j.ttbdis.2018.12.007
Paradowska-Stankiewicz I, Zbrzeźniak J, Skufca J et al (2023) A retrospective database study of Lyme Borreliosis incidence in Poland from 2015 to 2019: a Public Health concern. Vector Borne Zoonotic Dis 23:247–255. https://doi.org/10.1089/vbz.2022.0049
Huppertz HI, Karch H, Suschke HJ et al (1995) Lyme arthritis in European children and adolescents. The Pediatric Rheumatology Collaborative Group. Arthritis Rheum 38:361–368. https://doi.org/10.1002/art.1780380310
Brestrich G, Hagemann C, Diesing J et al (2024) Incidence of Lyme Borreliosis in Germany: a retrospective observational healthcare claims study. Ticks Tick Borne Dis 15:102326. https://doi.org/10.1016/j.ttbdis.2024.102326
CDC (2021) Lyme arthritis | CDC. In: Centers for Disease Control and Prevention. https://www.cdc.gov/lyme/treatment/LymeArthritis.html . Accessed 18 Apr 2024
Müller T, Locht H, Panum I et al (2021) Lyme arthritis is rare in Eastern Denmark. Dan Med J 68:A05210423
Dessau RB, Bangsborg JM, Ejlertsen T et al (2010) Utilization of serology for the diagnosis of suspected Lyme borreliosis in Denmark: survey of patients seen in general practice. BMC Infect Dis 10:317. https://doi.org/10.1186/1471-2334-10-317
Gynthersen RMM, Tetens MM, Ørbæk M et al (2021) Classification of patients referred under suspicion of tick-borne diseases, Copenhagen, Denmark. Ticks Tick Borne Dis 12:101591. https://doi.org/10.1016/j.ttbdis.2020.101591
Herzer P (1991) Joint manifestations of Lyme borreliosis in Europe. Scand J Infect Dis Suppl 77:55–63
Milewski MD, Cruz AI, Miller CP et al (2011) Lyme arthritis in children presenting with joint effusions. J Bone Joint Surg Am 93:252–260. https://doi.org/10.2106/JBJS.I.01776
Petrulionienė A, Radzišauskienė D, Paulauskas A, Venalis A (2021) Lyme Disease among patients at an ambulatory unit in a highly endemic country: Lithuania. Med (Kaunas) 57:184. https://doi.org/10.3390/medicina57020184
Article Google Scholar
Rauer S, Kastenbauer S, Hofmann H et al (2020) Guidelines for diagnosis and treatment in neurology - Lyme neuroborreliosis. Ger Med Sci 18:Doc03. https://doi.org/10.3205/000279
Skarphédinsson S, Lyholm BF, Ljungberg M et al (2007) Detection and identification of Anaplasma phagocytophilum, Borrelia burgdorferi, and Rickettsia helvetica in Danish Ixodes ricinus ticks. APMIS 115:225–230. https://doi.org/10.1111/j.1600-0463.2007.apm_256.x
Vennestrøm J, Egholm H, Jensen PM (2008) Occurrence of multiple infections with different Borrelia burgdorferi genospecies in Danish Ixodes ricinus nymphs. Parasitol Int 57:32–37. https://doi.org/10.1016/j.parint.2007.07.004
Michelet L, Delannoy S, Devillers E et al (2014) High-throughput screening of tick-borne pathogens in Europe. Front Cell Infect Microbiol 4:103. https://doi.org/10.3389/fcimb.2014.00103
Berglund J, Blomberg I, Hansen BU (1996) Lyme borreliosis in rheumatological practice: identification of Lyme arthritis and diagnostic aspects in a Swedish county with high endemicity. Br J Rheumatol 35:853–860. https://doi.org/10.1093/rheumatology/35.9.853
Huppertz HI, Böhme M, Standaert SM et al (1999) Incidence of Lyme borreliosis in the Würzburg region of Germany. Eur J Clin Microbiol Infect Dis 18:697–703. https://doi.org/10.1007/s100960050381
Christova I, Komitova R (2004) Clinical and epidemiological features of Lyme borreliosis in Bulgaria. Wien Klin Wochenschr 116:42–46. https://doi.org/10.1007/BF03040423
Moniuszko A, Popko J, Guszczyn T et al (2014) Lyme disease with effusion either in hip or knee in children from Podlaskie region treated in clinic in 2004–2010. Przegl Epidemiol 68:425–428
Wilking H, Stark K (2014) Trends in surveillance data of human Lyme borreliosis from six federal states in eastern Germany, 2009–2012. Ticks Tick Borne Dis 5:219–224. https://doi.org/10.1016/j.ttbdis.2013.10.010
Czupryna P, Moniuszko-Malinowska A, Pancewicz S et al (2016) Lyme disease in Poland - A serious problem? Adv Med Sci 61:96–100. https://doi.org/10.1016/j.advms.2015.10.007
Enkelmann J, Böhmer M, Fingerle V et al (2018) Incidence of notified Lyme borreliosis in Germany, 2013–2017. Sci Rep 8:14976. https://doi.org/10.1038/s41598-018-33136-0
Article CAS PubMed PubMed Central Google Scholar
Sundheim KM, Levas MN, Balamuth F et al (2021) Seasonality of Acute Lyme Disease in Children. Trop Med Infect Dis 6:196. https://doi.org/10.3390/tropicalmed6040196
Böhmer MM, Ens K, Böhm S et al (2021) Epidemiological Surveillance of Lyme Borreliosis in Bavaria, Germany, 2013–2020. Microorganisms 9:1872. https://doi.org/10.3390/microorganisms9091872
Download references
Acknowledgements
The authors would like to thank the patients for participating in this case series and the clinicians and technicians at Department of Rheumatology, Microbiology, and Infectious Disease for their involvement in diagnostics and treatment.
The study was conducted without any funding.
Author information
Authors and affiliations.
Department of Rheumatology, University Hospital of Southern Denmark, Esbjerg, DK-6700, Denmark
Ayse Mine Unlu, Stavros Chrysidis & Philip Rask Lage-Hansen
Clinical Center for Emerging and Vectorborne Infections, Odense University Hospital, Odense, DK-5000, Denmark
Nanna Skaarup Andersen, Sanne Løkkegaard Larsen & Fredrikke Christie Knudtzen
Department of Clinical Microbiology, Odense University Hospital, Odense, DK-5000, Denmark
Nanna Skaarup Andersen & Sanne Løkkegaard Larsen
Clinical Microbiology research unit, University of Southern Denmark, Odense, Denmark
Nanna Skaarup Andersen, Sanne Løkkegaard Larsen & Sigurdur Skarphedinsson
Department of Infectious Diseases Q, Odense University Hospital, Odense, DK-5000, Denmark
Sigurdur Skarphedinsson & Fredrikke Christie Knudtzen
Department of Rheumatology, Hospital South West Jutland, Esbjerg, DK-6700, Denmark
Ayse Mine Unlu
You can also search for this author in PubMed Google Scholar
Contributions
Ayse Mine Unlu and Philip Rask Lage-Hansen contributed to the study’s conception and design. Ayse Mine Unlu conducted the systematic literature search, screened the retrieved records, and created the flowchart and table. Ayse Mine Unlu and Philip Rask Lage-Hansen drafted the initial manuscript. Clinicians (Nanna Skaarup Andersen and Sanne Løkkegaard Larsen) from the Department of Clinical Microbiology described and conducted the B.b. s.l. specific PCR analyses. Philip Rask Lage-Hansen and Stavros Chrysidis diagnosed the patients in this case series, with Sigurdur Skarphedinsson consulted regarding antibiotic treatment in all cases. All authors critically reviewed and contributed substantially to the manuscript’s refinement. All authors take full responsibility for the integrity and accuracy of all aspects of the work.
Corresponding author
Correspondence to Ayse Mine Unlu .
Ethics declarations
Ethical approval.
In accordance with Danish national regulations, case reports are not subject to approval by any ethics committee. Written informed consent was obtained from all patients for publication of data pertaining to their medical history and laboratory test results.
Conflict of interest
The authors declare no conflict of interest.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary material 2, rights and permissions.
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Reprints and permissions
About this article
Unlu, A.M., Andersen, N.S., Larsen, S.L. et al. Differentiating Lyme arthritis: a case-based review. Rheumatol Int (2024). https://doi.org/10.1007/s00296-024-05618-0
Download citation
Received : 29 March 2024
Accepted : 10 May 2024
Published : 25 May 2024
DOI : https://doi.org/10.1007/s00296-024-05618-0
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Borrelia burgdorferi sensu lato
- Arthritis, infectious
- Lyme disease
- Case reports
- Find a journal
- Publish with us
- Track your research
- Open access
- Published: 21 May 2024
A modern way to teach and practice manual therapy
- Roger Kerry 1 ,
- Kenneth J. Young ORCID: orcid.org/0000-0001-8837-7977 2 ,
- David W. Evans 3 ,
- Edward Lee 1 , 4 ,
- Vasileios Georgopoulos 1 , 5 ,
- Adam Meakins 6 ,
- Chris McCarthy 7 ,
- Chad Cook 8 ,
- Colette Ridehalgh 9 , 10 ,
- Steven Vogel 11 ,
- Amanda Banton 11 ,
- Cecilia Bergström 12 ,
- Anna Maria Mazzieri 13 ,
- Firas Mourad 14 , 15 &
- Nathan Hutting 16
Chiropractic & Manual Therapies volume 32 , Article number: 17 ( 2024 ) Cite this article
113 Altmetric
Metrics details
Musculoskeletal conditions are the leading contributor to global disability and health burden. Manual therapy (MT) interventions are commonly recommended in clinical guidelines and used in the management of musculoskeletal conditions. Traditional systems of manual therapy (TMT), including physiotherapy, osteopathy, chiropractic, and soft tissue therapy have been built on principles such as clinician-centred assessment , patho-anatomical reasoning, and technique specificity. These historical principles are not supported by current evidence. However, data from clinical trials support the clinical and cost effectiveness of manual therapy as an intervention for musculoskeletal conditions, when used as part of a package of care.
The purpose of this paper is to propose a modern evidence-guided framework for the teaching and practice of MT which avoids reference to and reliance on the outdated principles of TMT. This framework is based on three fundamental humanistic dimensions common in all aspects of healthcare: safety , comfort , and efficiency . These practical elements are contextualised by positive communication , a collaborative context , and person-centred care . The framework facilitates best-practice, reasoning, and communication and is exemplified here with two case studies.
A literature review stimulated by a new method of teaching manual therapy, reflecting contemporary evidence, being trialled at a United Kingdom education institute. A group of experienced, internationally-based academics, clinicians, and researchers from across the spectrum of manual therapy was convened. Perspectives were elicited through reviews of contemporary literature and discussions in an iterative process. Public presentations were made to multidisciplinary groups and feedback was incorporated. Consensus was achieved through repeated discussion of relevant elements.
Conclusions
Manual therapy interventions should include both passive and active, person-empowering interventions such as exercise, education, and lifestyle adaptations. These should be delivered in a contextualised healing environment with a well-developed person-practitioner therapeutic alliance. Teaching manual therapy should follow this model.
Musculoskeletal (MSK) conditions are leading contributors to the burden of global disability and healthcare [ 1 ]. Amongst other interventions, manual therapy (MT) has been recommended for the management of people with MSK conditions in multiple clinical guidelines, for example [ 2 , 3 ].
MT has been described as the deliberate application of externally generated force upon body tissue, typically via the hands, with therapeutic intent [ 4 ]. It includes touch-based interventions such as thrust manipulation, joint mobilisation, soft-tissue mobilisation, and neurodynamic movements [ 5 ]. For people with MSK conditions, this therapeutic intent is usually to reduce pain and improve movement, thus facilitating a return to function and improved quality of life [ 6 ]. Patient perceptions of MT are, however, vague and sit among wider expectations of treatment including education, self-efficacy and the role of exercise, and prognosis [ 7 ].
Although the teaching and practice of MT has invariably changed over time, its foundations arguably remain unaltered and set in biomedical and outdated principles. This paper sets out to review contemporary literature and propose a revised model to inform the teaching and practice of MT.
The aim of this paper is to stimulate debate about the future teaching and practice of manual therapy through the proposal of an evidence-informed re-conceptualised model of manual therapy. The new model dismisses traditional elements of manual therapy which are not supported by research evidence. In place, the model offers a structure based on common humanistic principles of healthcare.
Consenus methodology
We present the literature synthesis and proposed framework as a consensus document to motivate further professional discussion developed through a simple three-stage iterative process over a 5-year period. The consensus methodology was classed as educational development which did not require ethical approval. Stage 1: a change of teaching practice was adopted by some co-authors (VG, RK, EL) on undergraduate and postgraduate Physiotherapy programmes at a UK University in 2018. This was a result of standard institutional teaching practice development which includes consideration of evidence-informed teaching. Stage 2: Input from a broader spectrum of stakeholders was sought, so a group of experienced, internationally-based educators, clinicians, and researchers from across the spectrum of manual therapy was convened. Perspectives were elicited through discussions in an iterative process. Stage 3: Presentations were made by some of the co-authors (VG, RK, SV, KY) to multidisciplinary groups (UK, Europe, North America) and feedback via questions and discussions was incorporated into further co-author discussions on the development of the framework. Consensus was achieved through repeated discussion of relevant elements. Figure 1 summarises the consensus methodology.

Summary and timeline of iterative consensus process for development of framework (MT: Manual Therapy; UG: Undergraduate; PG: Postgraduate)
Clinical & cost effectiveness of manual therapy
Manual therapy has been suggested to be a valuable part of a multimodal approach to managing MSK pain and disability, for example [ 8 ]. The majority of recent systematic reviews of clinical trials report a beneficial effect of MT for a range of MSK conditions, with at least similar effect sizes to other recommended approaches, for example [ 9 ]. Some systematic reviews report inconclusive findings, for example [ 10 ], and a minority report effects that were no better than comparison or sham treatments, for example [ 11 ].
Potential benefits must always be weighed against potential harms, of course. Mild to moderate adverse events from MT (e.g. mild muscle soreness) are common and generally considered acceptable [ 12 ], whilst serious adverse events are very rare and their risk may be mitigated by good practice [ 13 ]. MT has been reported by people with MSK disorders as a preferential and effective treatment with accepted levels of post-treatment soreness [ 14 ].
MT is considered cost-effective [ 15 ] and the addition of MT to exercise packages has been shown to increase clinical and cost-effectiveness compared to exercise alone in several MSK conditions [ 16 , 17 , 18 , 19 , 20 , 21 , 22 , 23 ]. Further, manual therapy has been shown to be less costly and more beneficial than evidence-based advice to stay active [ 24 ].
In summary, MT is considered a useful evidence-based addition to care packages for people experiencing pain and disability associated with MSK conditions. As such, MT continues to be included in national and international clinical guidelines for a range of MSK conditions as part of multimodal care.
Principles of traditional manual therapy (TMT)
Manual therapy has been used within healthcare for centuries [ 4 ] with many branches of MT having appeared (and disappeared) over time [ 25 ]. In developed nations today, MT is most commonly utilised by the formalised professional groups of physiotherapy, osteopathy, chiropractic, as well as groups such as soft tissue therapists. All of these groups have a history that borrows heavily from traditional healers and bone-setters [ 26 ].
Although there are many elements of MT, three principles appear to have become ubiquitous within what we shall now refer to as ‘traditional manual therapy’ (TMT): clinician-centred assessment , patho-anatomical reasoning , and technique specificity [ 27 , 28 , 29 , 30 ]. These principles continue to influence the teaching and practice of manual therapy over recent years, for example [ 31 ].
However, they have become increasingly difficult to defend given a growing volume of empirical evidence to the contrary.
Traditional manual therapy (TMT) principles: origins and problems
Clinician-centred assessment.
TMT has long had an emphasis on what we shall refer to as clinician-centred assessments . Within this, we claim, is an assumption that clinical information is both highly accurate and diagnostically important, for example [ 32 ]. Clinician-centred assessments include, for example, routine imaging, the search for patho-anatomical 'lesions’ and asymmetries, and specialised palpation. Although the focus of this paper is on the ‘hands-on’ examples of client-centred assessment, the notion of imaging is presented below to expose some of the flaws in the underlying belief system for TMT.
The emphasis on clinician-centred assessments has probably been driven, in part, by a desire for objective diagnostic tests which align well with gold-standard imaging. Indeed, since the discovery of x-rays, radiological imaging been used as an assessment for spinal pain – and a justification for using spinal manipulation – particularly in the chiropractic profession [ 33 ]. Contrary to many TMT claims, X-ray imaging is not without risk [ 34 ]. Additionally, until relatively recently (with the advent of magnetic resonance imaging) it was not widely appreciated that patho-anatomical ‘lesions’ believed to explain MSK pain conditions were nearly as common in pain-free individuals as those with pain [ 35 ]. Accordingly, the rates of unnecessary treatments, including surgery, are known to increase when imaging is used routinely [ 36 ]. For patients with non-specific low back pain, for example, imaging does not improve outcomes and risks overdiagnosis and overtreatment [ 37 ]. Hence, despite being objective in nature, the value of imaging for many MSK pain conditions (particularly spinal pain) has reduced drastically with clinical guidelines across the globe recommending against routine imaging for MSK pain of non-traumatic origin [ 38 ]. Even so, the practice of routine imaging continues [ 39 ].
Hands-on interventions are inextricably related to hands-on assessment [ 40 ], and often associated with claims of ‘specialisation’ [ 41 ]. By this we mean where a great level of training and precision are claimed to be necessary for influencing the interpretation of assessment findings, treatment decisions, and/or treatment outcomes. Implicit within this claim is that therapists who are unable to achieve such precision are not able to perform MT to an acceptable level (and thereby are not able to provide benefit to patients).
There are numerous studies that cast doubt over claims of highly specialised palpation skills. Palpation of anatomical landmarks does not reach a clinically acceptable level of validity [ 42 ]. Specialised motion palpation does not appear to be a good method for differentiating people with or without low back pain [ 43 ]. Poor content validity of specialised motion tests have been reported, in line with a lack of acceptable reference standards [ 44 ]. Palpable sensations reported by therapists are unlikely to be due to tissue deformation [ 45 ]. Furthermore, the delivery of interventions based on specialised palpatory findings is no better than non-specialised palpation [ 46 ]. Generally poor reliability of motion palpation skills has been reported, for example [ 47 ] and appear to be independent of clinician experience or training, for example [ 48 ]. Notably, person-centred palpation—for pain and tenderness for example—has slightly higher reliability, but is still fair at best [ 49 ].
This does not mean that palpation is of no use at all though; just that effective manual therapy does not depend upon it. For example, expert therapists can display high levels of interrater reliability during specialised motion palpation [ 50 ]. Focused training can improve the interrater reliability of specialised skills [ 51 ]. However, the validity of the phenomenon remains poor. Given the weight of the evidence and consistency of data over recent decades, we suggest that the role of clinician-centred hands-on assessment is no longer central to contemporary manual therapy.
Patho-anatomical reasoning
The justification for selecting particular MT interventions has historically been based upon the patho-anatomical status of local peripheral tissue [ 52 , 53 , 54 , 55 ]. Patho-anatomical reasoning, we propose, is the framework that links clinician-centred assessments to the desire for highly specific delivery of MT interventionsKey to this is the relationship between a patho-anatomic diagnosis and the assumed mechanisms of action of the intervention employed.
Theories for the mechanisms of action of MT interventions are many. Some of the most prominent include reductions of disc herniations [ 56 ], re-positioning of a bone or joint [ 32 ], removal of intra-articular adhesions [ 57 ], changes in the biomechanical properties of soft tissues [ 58 ], central pain modulation [ 59 ], and biochemical changes [ 60 ]. These theories have been used to justify the choice of certain interventions: a matching of diagnosis (i.e., existence of a lesion) to the effect of treatment takes place. However, most of these mechanistic theories either lack evidence or have been directly contested [ 61 ].
The causal relationship between proposed tissue-based factors such as posture, ergonomic settings, etc. and painful experience has also been disputed [ 62 ]. Although local tissue stiffness has been observed in people with pain, this is typically associated with neuromuscular responses, rather than patho-anatomical changes at local tissue level [ 63 , 64 , 65 , 66 ]. Overall, although some local tissue adaptions have been identified in people with recurrent MSK pain, this is inconsistent and the evidence is currently of low quality [ 67 ] are generally limited to short-term follow-up measures [ 68 ].
Technique specificity
TMT techniques have been taught with an emphasis that a particular direction, ‘grade’ of joint movement, or deformation of tissue at a very specific location in a certain way, is required to achieve a successful treatment outcome.
One problem with a demand for technique specificity in manual therapy is that an intervention does not always result in the intended effect. For example, posteroanterior forces applied during spinal mobilization consistently induce sagittal rotation, as opposed to the assumed posteroanterior translation, for example [ 69 ]. Furthermore, irrespective of the MT intervention chosen, restricting movements to a particular spinal segment is difficult and a regional, non-specific motion is typically induced, for example [ 70 ].
To support technique specificity, comparative data must repeatedly and reproducibly show superiority of outcome from specific MT interventions over non-specific MT, which is consistently not observed [ 71 , 72 , 73 ]. Some studies have demonstrated localised effects of targeted interventions [ 74 ] but there appears to be no difference in outcome related to: the way in which techniques are delivered [ 75 ]; whether technique selection is random or clinician-selected [ 41 ]; or variations in the direction of force or targeted spinal level [ 76 ]. Conversely, there is evidence that non-specific technique application may improve outcomes [ 77 , 78 , 79 ]. Further, sham techniques produce comparable results to specialised approaches [ 11 ].
Passive movement and localised touch have been associated with significant analgesic responses [ 80 ]. These data indicate the presence of an analgesic mechanism. Unfortunately, mechanistic explanation for the therapeutic effects of MT upon pain and disability still remain largely in a ‘black box’ state [ 81 ]. Nevertheless, there are several plausible mechanisms of action to explain the analgesic action of MT interventions, including the activation of modulatory spinal and supraspinal responses [ 82 , 83 , 84 , 85 ]. In support of this, MT interventions have been associated with a variety of neurophysiological responses [ 61 ]. However, it must be acknowledged that these studies provide mechanistic evidence based on association, which is insufficient to make causal claims [ 86 ]. Importantly, none of these neurophysiological responses have been directly related to either the analgesic mechanisms or clinical outcome and may therefore be incidental.
There is evidence that MT does not provide analgesia in injured tissues [ 87 , 88 ]. Conversely, MT has been shown to decrease inflammatory biomarkers [ 89 , 90 , 91 , 92 , 93 ], although these changes have not been evaluated in the longer-term, nor associated with clinical outcomes.
A modern framework for manual therapy
We propose a new direction for the future of MT in which the teaching and practice of this core dimension of MSK care are no longer based on the traditional principles of clinician-centred assessment , patho-anatomical reasoning , and technique specificity .
In doing so, this framework places MT more explicitly as part of person-centred care and appeals to common principles of healthcare, best available evidence, and contemporary theory which avoids unnecessary and over-complicated explanations of observed effects. The framework is simple in terms of implementation and delivery and contextualised by common elements of best practice for healthcare, in line with regulated standard of practice, e.g., [ 94 , 95 , 96 , 97 ]. Our proposal simply illustrates the operationalisation of these common elements through manual therapy.
Too much emphasis has been given to clinician-centred assessments and this should be rebalanced with an increased use of patient-centred assessments, such as a thorough case history, the use of validated patient-reported outcome measures (PROMS), and real-time patient feedback during assessments.
The new framework considers fundamental and humanistic dimensions of touch-based therapies, such as non-specific neuromodulation, communication and sense-making, physical education, and contextual clinical effectiveness. This aligns to contemporary ideas regarding therapeutic alliance and a move towards genuinely holistic healthcare [ 98 , 99 ]. The framework needs to be “open” in order to represent and allow expression of the complexity of the therapeutic encounter. However, to prevent the exploitation of this openness the framework is underpinned by evidence, and any manual therapy approaches without plausible and measurable mechanisms are not supported.
To provide the best care, common healthcare elements such as the safety and comfort of the person seeking help and therapist must be considered, and care should be provided as efficiently as possible. Our framework embraces these dimensions and employs an integration of current evidence. It is transdisciplinary in nature and may be adopted by all MT professions. Figure 1 provides a graphical representation of the framework. It is acknowledged that all components overlap, relate, and influence each. There are two main components: the practical elements on the inside, comprised of safety, comfort, and efficiency, and the conceptual themes on the outer regions, consisting of communication, context, and person-centred care Fig. 2 .

Representation of a modern teaching and practice framework for manual therapy. The image is purposefully designed to be simple, and has been developed primarily to be used as a teaching aid. When displayed in a learning environment, learners and clinicians can quickly refer to the image to check their practice against each element. To keep the image clear, each element of the image is described in detail in the text below”
Practical elements
Safety for people seeking help is a primary concern for all healthcare providers, with the aims to “ prevent and reduce risks, errors and harm that occur to patients [sic] during provision of health care… and to deliver quality essential health services ” [ 100 ]. This, and the notion of safety more generally (including that of the therapist), should be central to way MT is taught and practised.
A fundamentally safe context should be created where there is an absence of any obvious danger or risk of harm to physical or mental health. Consideration should be given to ensuring that communication and consent processes are orientated towards the safety of both the person seeking help and the therapist. The therapist should pay attention to any sense of threat that could be present in the physical, emotional, cognitive and environmental domains of the clinical encounter, and use skilful communication to mitigate anxiety about the assessment or therapeutic process.
Safety should also be considered in the clinical context of the assessment and treatment approach, ensuring that relevant and meaningful safety screenings have been undertaken [ 67 , 101 ]. There remains a need for good, skilful practice and development of manually applied techniques, but this can be achieved without reference to the principles of TMT and without the dogma of a proprietary therapeutic approach.
Comfort suggests that both the person seeking help and the therapist are physically and emotionally content during the assessment and therapeutic process. For example, the person seeking help is agreeable with any necessary state of dress (sociocultural difference should be considered); the person is relaxed and untroubled in whatever position they are in, and is adequately supported whether sitting, standing or recumbent during assessment and treatment; the therapist is comfortable with their positioning and posture; any discomfort produced by the therapeutic process is negotiated and agreed. Any physical mobilisation or touch should be applied with respect to the feedback from the person in relation to their comfort, rather than a pre-determined force based on the notion of resistance. This process requires clinical phronesis, sensitivity, responsivity, dexterity, and embodied communication [ 102 ].
The therapeutic process should be undertaken in a well-organised, competent manner aiming to achieve maximum therapeutic benefit with minimum waste of effort, time, or expense. To enhance the efficiency dimension, the assessment and therapeutic process should be an integral part of a holistic educational and/or activity-based approach to the management of the people which might also address psychological, nutritional, or ergonomic aspects of care, while being aware of social determinants to health. Recommendations exist which serve as a useful guide for enhancing care and promoting self-management in an efficient way [ 103 ].
A principle of this new model of MT is that therapists should not lose sight of the goals they develop with the people they help and ensure that there is coherence between their management aims and their techniques. Therapists should aim to support a person’s self-efficacy and use active approaches to empower them in their recovery. The overall number of therapeutic applications should be made in the context of fostering therapeutic alliance and supporting people to make sense of their situation and symptoms. This should be informed by contemporary views of the effects of manual therapy, emphasising a “physical education process” to promote sense-making and self-efficacy in alliance with the people they aim to help.
Clinical interactions need to be reproducible under a person’s own volition, serving to enhance self-empowerment. For example, someone could be taught how to “self-mobilise” if a positive effect is found with a particular therapeutic application. This should be appropriately scaffolded with behavioural change principles and functional contextualism that promote autonomy and self-management, rather than inappropriate reliance on the therapist [ 103 , 104 ].
An important and emergent notion from the proposed model is to question what constitutes indications for MT given that the model excludes traditional factors which would have informed whether manual therapy is indicated or not for a particular person. The response to this sits within the efficiency and safety dimensions: MT can be beneficial as part of a multi-dimensional approach to management across a broad population of people with musculoskeletal dysfunction, with no evidence to suggest any clinician-centered or patho-anatomical finding influences outcomes. The choice of whether or not to include MT as part of a management strategy should therefore be a product of a lack of contraindications and shared-decision making.
This framework aligns with evidence-based propositions that effectiveness and efficiency in assessment, diagnosis, and outcomes are not reliant on the therapist’s skill set of specialised elements of TMT, but rather other factors—for example variations in pain phenotypes [ 5 ].
Conceptual themes
Communication.
Communication is the overriding critical dimension to the whole therapeutic process and should be aimed at addressing peoples’ fundamental needs to make sense of their symptoms and path to recovery. The delivery and uptake of the therapy should therefore be operationalised in a communication process that meaningfully represents shared-decision making and the best possible attempt to contextualise the therapy in positive and evidence-informed explanations of the process and desired effects [ 105 ].
Within a therapeutic encounter, practitioners must give the time to listen to peoples’ accounts and explanations of their symptoms, including their ideas about their cause [ 106 ]. The assessment and diagnostic process should be a shared endeavour, for example, the negotiation of symptom reproduction. This should be done in a manner that facilitates sense-making, and which simultaneously encourages people to move on from unhelpful beliefs about their symptoms [ 107 , 108 ], encouraging understanding of the uncertain nature of pain and injury. Person-centered communication requires attention to what we communicate and how we communicate across the entire clinical interaction including interview, examination, and management planning [ 109 ]. Therapists need to be open, reflective, aware and responsive to verbal and non-verbal cues, and demonstrate a balance between engaging with people (e.g. eye-gaze) and writing/typing notes during the interview [ 110 , 111 , 112 ].
People should be given the opportunity to discuss their understanding of the diagnosis and options for treatment and rehabilitation. The decision-making process is dialogical, in which alternative options to the offered therapy should also be discussed with the comparative risks and benefits of all available management options, including doing nothing [ 113 , 114 ].
The therapist must fully appreciate the potential consequences of touch without consent. Continual dialogue should ensure that all parties are moving towards mutually agreed goals. The context of the therapy should be explicitly communicated to give appropriate context for any particular intervention as part of a holistic, evidence-based approach [ 115 , 116 , 117 ]. Therapists should be aware that their own beliefs can affect the way they communicate with their people; in the same way, a person’s context affects how they communicate what they expect from their treatment [ 107 , 118 , 119 , 120 ]. The construction of contextual healing scenarios which support positive outcomes, whilst minimising nocebic effects, is critical to effective healthcare [ 121 , 122 , 123 ].
There is a growing academic interest in the nature, role, and purpose of social and affective touch, and any re-framing of MT should consider touch as a means of communication to develop and enhance cooperative communications and strengthen the therapeutic relationship [ 124 , 125 , 126 , 127 , 128 , 129 ]. It can be soothing for a person in pain to experience the caring touch of a professional therapist [ 130 ]; on the other hand, probing, diagnostic, and touch can be experienced as alienating [ 131 , 132 , 133 ]. Touch can alter a person’s sense of body ownership and their ability to recognise and process their emotions by modulating interoceptive precision [ 129 , 134 , 135 ], and intentional touch may be perceived differently from casual, unfocussed touch [ 136 , 137 ]. There is also a thesis that touch generates shared understanding and meaning [ 138 , 139 , 140 ]. This wider appreciation of touch should be embedded in modern MT communication.
The contextual quality of a person’s experience of the therapeutic encounter can affect satisfaction and clinical outcomes [ 141 , 142 , 143 , 144 , 145 ]. The context in which therapeutic care takes place should therefore be developed to enhance this experience. There could be very local, practical aspects of the context, such as the type of passive information available in the clinical space, e.g. replacing biomedical and pathological imagery and objects with positive, active artefacts; judicious and thoughtful organisation and use of treatment tables to discourage a sense of passivity and disempowerment; allocating a comfortable space where communication can take place; colour schemes and light sources which facilitate positivity; ensuring consistency through all clinical and administrative staff promoting encouraging and non-nocebic messages. Importantly, the way the therapist dresses influences peoples’ perception of their healthcare experience [ 146 , 147 ], and that in turn should be contextually and culturally sensitive [ 148 , 149 , 150 ].
Beyond the local clinical space is the broader social environment. The undertaking of MT should serve a role in a person’s engagement with their social environment. For example, someone returning home after engaging with their therapist and disseminating positive health messages within their home and social networks; people acting as advocates for self-empowered healthcare. Furthermore, early data have demonstrated that aligning treatment with the beliefs and values of culturally and linguistically diverse communities enhances peoples’ engagement with their healthcare [ 151 ].
Person-centred care
Here we borrow directly from one of the most established and clinically useful definitions of Person-Centered Medicine [ 152 ]:
“(Person-Centered Medicine is) an affordable biomedical and technological advance to be delivered to patients [sic] within a humanistic framework of care that recognises the importance of applying science in a manner that respects the patients [sic] as a whole person and takes full account of [their] values, preferences, aspirations, stories, cultural context, fears, worries and hopes and thus that recognises and responds to [their] emotional, social and spiritual necessities in addition to [their] physical needs” [ 152 ] , p219.
Person-centred care incorporates a person’s perspective as part of the therapeutic process. In practice, therapists need to communicate in a manner that creates adequate conversational space to elicit a person’s agenda (i.e. understanding, impact of pain, concerns, needs, and goals), which guides clinical interactions. This approach encourages greater partnership in management [ 109 , 153 , 154 ].
A roadmap outlining key actions to implement person-centeredness in clinical practice has been outlined in detail elsewhere [ 155 ]. This includes screening for serious pathology, health co-morbidities and psychosocial factors; adopting effective communication; providing positive health education; coaching and supporting people towards active self-management; and facilitating and managing co-care (when needed) [ 154 ].
It is critical and necessary now to make these features explicit and central to the revised model of MT proposed in this paper. We wish to identify common ground across all MT professions in order to achieve a trans-disciplinary understanding of the evidence supporting the use of MT.
We acknowledge that our arguments here are rooted in empiricism and deliberately based on available research data from within the health science disciplines. We also acknowledge that there is a wider debate about future directions in person-centred care arising from the current evolution of the evidence-based health care movement, which has pointed to the need to learn more about peoples’ lived experiences, to redefine the model of the therapeutic relationship. Although beyond the scope of this paper, a full exploration of modern health care provision involves reconsideration of the ethics and legal requirements of communication and shared decision-making [ 156 , 157 , 158 , 159 ]. The authors envision this paper as a stimulus for self-reflection, stakeholder discussions, and ultimately change that can positively impact outcomes for people who seek manual therapy interventions.
Manual therapy has long been part of MSK healthcare and, given that is likely to continue. Current evidence suggests that effectiveness does not rely on the traditional principles historically developed in any of the major manual therapies. Therefore, the continued teaching and practice based on the principles of clinician-centred palpation , patho-anatomical reasoning , and technique specificity are no longer justified and may well even limit the value of MT.
A revised and reconceptualised framework of MT, based on the humanistic domains of safety, comfort and efficiency and underpinned by the dimensions of communication, context and person-centred care will ensure an empowering, biopsychosocial, evidence-informed approach to MSK care. We propose that the future teaching and practice of MT in physiotherapy, osteopathy, chiropractic, and all associated hands-on professions working within the healthcare field should be based on this new framework.
Availability of data and materials
Young C, Argáez C. CADTH Rapid Response Reports. Manual Therapy for Chronic Non-Cancer Back and Neck Pain: A Review of Clinical Effectiveness. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health. Copyright © 2020 Canadian Agency for Drugs and Technologies in Health.; 2020.
Blanpied PR, Gross AR, Elliott JM, Devaney LL, Clewley D, Walton DM, et al. Neck Pain: Revision 2017. J Orthop Sports Phys Ther. 2017;47(7):A1-a83.
Article PubMed Google Scholar
NICE. Low back pain and sciatica in over 16s: assessment and management. NICE guideline [NG59]. 2016.
Pettman E. A history of manipulative therapy. J Man Manip Ther. 2007;15(3):165–74.
Article PubMed PubMed Central Google Scholar
Damian K, Chad C, Kenneth L, David G. Time to evolve: the applicability of pain phenotyping in manual therapy. J Man Manip Ther. 2022;30(2):61–7.
McCarthy CJ. Combined Movement Theory: Rational Mobilization and Manipulation of the Vertebral Column. London, UK: Churchill Livingstone; 2010.
Google Scholar
Subialka JA, Smith K, Signorino JA, Young JL, Rhon DI, Rentmeester C. What do patients referred to physical therapy for a musculoskeletal condition expect? A qualitative assessment. Musculoskel Sci Pract. 2022;59:102543.
Article Google Scholar
Louw A, Nijs J, Puentedura EJ. A clinical perspective on a pain neuroscience education approach to manual therapy. J Man Manip Ther. 2017;25(3):160–8.
Wilhelm M, Cleland J, Carroll A, Marinch M, Imhoff M, Severini N, et al. The combined effects of manual therapy and exercise on pain and related disability for individuals with nonspecific neck pain: A systematic review with meta-analysis. J Man Manip Ther. 2023;31(6):393–407.
Schenk R, Donaldson M, Parent-Nichols J, Wilhelm M, Wright A, Cleland JA. Effectiveness of cervicothoracic and thoracic manual physical therapy in managing upper quarter disorders - a systematic review. J Man Manipulative Therap. 2021:1–10.
Lavazza C, Galli M, Abenavoli A, Maggiani A. Sham treatment effects in manual therapy trials on back pain patients: a systematic review and pairwise meta-analysis. BMJ Open. 2021;11(5):e045106.
Funabashi M, Pohlman KA, Goldsworthy R, Lee A, Tibbles A, Mior S, et al. Beliefs, perceptions and practices of chiropractors and patients about mitigation strategies for benign adverse events after spinal manipulation therapy. Chiropr Man Therap. 2020;28(1):46.
Rushton A, Carlesso LC, Flynn T, Hing WA, Rubinstein SM, Vogel S, et al. International Framework for Examination of the Cervical Region for Potential of Vascular Pathologies of the Neck Prior to Musculoskeletal Intervention: International IFOMPT Cervical Framework. J Orthop Sports Phys Ther. 2022;53(1):7–22.
Thomas M, Thomson OP, Kolubinski DC, Stewart-Lord A. The attitudes and beliefs about manual therapy held by patients experiencing low back pain: a scoping review. Musculoskelet Sci Pract. 2023;65:102752.
Lilje S, van Tulder M, Wykman A, Aboagye E, Persson U. Cost-effectiveness of specialised manual therapy versus orthopaedic care for musculoskeletal disorders: long-term follow-up and health economic model. Ther Adv Musculoskelet Dis. 2023;15:1759720x221147751.
Article CAS PubMed PubMed Central Google Scholar
Abbott JH, Robertson MC, Chapple C, Pinto D, Wright AA, Leon de la Barra S, et al. Manual therapy, exercise therapy, or both, in addition to usual care, for osteoarthritis of the hip or knee: a randomized controlled trial. 1: clinical effectiveness. Osteoarthritis Cartilage. 2013;21(4):525–34.
Article CAS PubMed Google Scholar
Bove AM, Smith KJ, Bise CG, Fritz JM, Childs JD, Brennan GP, et al. Exercise, Manual Therapy, and Booster Sessions in Knee Osteoarthritis: Cost-Effectiveness Analysis From a Multicenter Randomized Controlled Trial. Phys Ther. 2018;98(1):16–27.
Leininger B, McDonough C, Evans R, Tosteson T, Tosteson AN, Bronfort G. Cost-effectiveness of spinal manipulative therapy, supervised exercise, and home exercise for older adults with chronic neck pain. Spine J. 2016;16(11):1292–304.
Tsertsvadze A, Clar C, Court R, Clarke A, Mistry H, Sutcliffe P. Cost-effectiveness of manual therapy for the management of musculoskeletal conditions: a systematic review and narrative synthesis of evidence from randomized controlled trials. J Manipulative Physiol Ther. 2014;37(6):343–62.
UK Beam Trial Team. United Kingdom back pain exercise and manipulation (UK BEAM) randomised trial: effectiveness of physical treatments for back pain in primary care. BMJ. 2004;329(7479):1377.
Article PubMed Central Google Scholar
UK Beam Trial Team. United Kingdom back pain exercise and manipulation (UK BEAM) randomised trial: cost effectiveness of physical treatments for back pain in primary care. BMJ (Clinical research ed). 2004;329(7479):1381.
van Dongen JM, Groeneweg R, Rubinstein SM, Bosmans JE, Oostendorp RA, Ostelo RW, et al. Cost-effectiveness of manual therapy versus physiotherapy in patients with sub-acute and chronic neck pain: a randomised controlled trial. Eur Spine J. 2016;25(7):2087–96.
Woods B, Manca A, Weatherly H, Saramago P, Sideris E, Giannopoulou C, et al. Cost-effectiveness of adjunct non-pharmacological interventions for osteoarthritis of the knee. PLoS ONE. 2017;12(3):e0172749.
Aboagye E, Lilje S, Bengtsson C, Peterson A, Persson U, Skillgate E. Manual therapy versus advice to stay active for nonspecific back and/or neck pain: a cost-effectiveness analysis. Chiropr Man Therap. 2022;30(1):27.
Paris SV. A History of Manipulative Therapy Through the Ages and Up to the Current Controversy in the United States. J Man Manipulative Ther. 2000;8(2):66–77.
MacDonald CW, Osmotherly PG, Parkes R, Rivett DA. The current manipulation debate: historical context to address a broken narrative. J Man Manipulative Therap. 2019;27(1):1–4.
Fryer G. Intervertebral dysfunction: a discussion of the manipulable spinal lesion. J Am Osteopath Assoc. 2003;6(2):64–73.
McCarthy CJ. Spinal manipulative thrust technique using combined movement theory. Man Ther. 2001;6(4):197–204.
Vickers A, Zollman C. ABC of complementary medicine Massage therapies. BMJ (Clinical research ed). 1999;319(7219):1254–7.
Evans DW. Osteopathic principles: More harm than good? Int J Osteopath Med. 2013;16(1):46–53.
Mourad F, Yousif MS, Maselli F, Pellicciari L, Meroni R, Dunning J, et al. Knowledge, beliefs, and attitudes of spinal manipulation: a cross-sectional survey of Italian physiotherapists. Chiropr Man Therap. 2022;30(1):38.
Cyriax JH, Cyriax PJ. Cyriax's Illustrated Manual of Orthopaedic Medicine. 3rd ed: Butterworth-Heinemann; 1996.
Young KJ. Words matter: the prevalence of chiropractic-specific terminology on Australian chiropractors’ websites. Chiropr Man Therap. 2020;28(1):18.
Jenkins HJ, Downie AS, Moore CS, French SD. Current evidence for spinal X-ray use in the chiropractic profession: a narrative review. Chiropr Man Therap. 2018;26:48.
Brinjikji W, Luetmer PH, Comstock B, Bresnahan BW, Chen LE, Deyo RA, et al. Systematic literature review of imaging features of spinal degeneration in asymptomatic populations. AJNR Am J Neuroradiol. 2015;36(4):811–6.
Mafi JN, McCarthy EP, Davis RB, Landon BE. Worsening trends in the management and treatment of back pain. JAMA Intern Med. 2013;173(17):1573–81.
Hall AM, Aubrey-Bassler K, Thorne B, Maher CG. Do not routinely offer imaging for uncomplicated low back pain. BMJ (Clinical research ed). 2021;372:n291.
PubMed Google Scholar
Lin I, Wiles L, Waller R, Goucke R, Nagree Y, Gibberd M, et al. What does best practice care for musculoskeletal pain look like? Eleven consistent recommendations from high-quality clinical practice guidelines: systematic review. Br J Sports Med. 2020;54(2):79.
Hall AM, Scurrey SR, Pike AE, Albury C, Richmond HL, Matthews J, et al. Physician-reported barriers to using evidence-based recommendations for low back pain in clinical practice: a systematic review and synthesis of qualitative studies using the Theoretical Domains Framework. Implement Sci. 2019;14(1):49.
Eriksson L, Ekenberg L, Melander-Wikman A. The concept of palpation of the shoulder – A basic element of physiotherapy practice: A focus group study with physiotherapists. Adv Physiother. 2012;14(4):183–93.
Nim CG, Downie A, O’Neill S, Kawchuk GN, Perle SM, Leboeuf-Yde C. The importance of selecting the correct site to apply spinal manipulation when treating spinal pain: Myth or reality? A systematic review. Sci Rep. 2021;11(1):23415.
Alexander N, Rastelli A, Webb T, Rajendran D. The validity of lumbo-pelvic landmark palpation by manual practitioners: A systematic review. Int J Osteopath Med. 2021;39:10–20.
Leboeuf-Yde C, van Dijk J, Franz C, Hustad SA, Olsen D, Pihl T, et al. Motion palpation findings and self-reported low back pain in a population-based study sample. J Manipulative Physiol Ther. 2002;25(2):80–7.
Najm WI, Seffinger MA, Mishra SI, Dickerson VM, Adams A, Reinsch S, et al. Content validity of manual spinal palpatory exams - A systematic review. BMC Complement Altern Med. 2003;3:1.
Chaudhry H, Schleip R, Ji Z, Bukiet B, Maney M, Findley T. Three-dimensional mathematical model for deformation of human fasciae in manual therapy. J Am Osteopath Assoc. 2008;108(8):379–90.
Gabriel A, Konrad A, Roidl A, Queisser J, Schleip R, Horstmann T, et al. Myofascial Treatment Techniques on the Plantar Surface Influence Functional Performance in the Dorsal Kinetic Chain. J Sports Sci Med. 2022;21(1):13–22.
PubMed PubMed Central Google Scholar
Nolet PS, Yu H, Côté P, Meyer A-L, Kristman VL, Sutton D, et al. Reliability and validity of manual palpation for the assessment of patients with low back pain: a systematic and critical review. Chiropr Man Therap. 2021;29(1):33.
Seffinger MA, Najm WI, Mishra SI, Adams A, Dickerson VM, Murphy LS, et al. Reliability of spinal palpation for diagnosis of back and neck pain: a systematic review of the literature. Spine. 2004;29(19):E413–25.
Beynon AM, Hebert JJ, Walker BF. The interrater reliability of static palpation of the thoracic spine for eliciting tenderness and stiffness to test for a manipulable lesion. Chiropr Man Therap. 2018;26:49.
Petersen EJ, Thurmond SM, Shaw CA, Miller KN, Lee TW, Koborsi JA. Reliability and accuracy of an expert physical therapist as a reference standard for a manual therapy joint mobilization trial. J Man Manip Ther. 2021;29(3):189–95.
Petersen EJ, Thurmond SM, Buchanan SI, Chun DH, Richey AM, Nealon LP. The effect of real-time feedback on learning lumbar spine joint mobilization by entry-level doctor of physical therapy students: a randomized, controlled, crossover trial. J Man Manip Ther. 2020;28(4):201–11.
Abbott JH, Flynn TW, Fritz JM, Hing WA, Reid D, Whitman JM. Manual physical assessment of spinal segmental motion: intent and validity. Man Ther. 2009;14(1):36–44.
Bialosky JE, Simon CB, Bishop MD, George SZ. Basis for spinal manipulative therapy: a physical therapist perspective. J Electromyogr Kinesiol. 2012;22(5):643–7.
Henderson CN. The basis for spinal manipulation: chiropractic perspective of indications and theory. J Electromyogr Kinesiol. 2012;22(5):632–42.
Sizer PS Jr, Felstehausen V, Sawyer S, Dornier L, Matthews P, Cook C. Eight critical skill sets required for manual therapy competency: a Delphi study and factor analysis of physical therapy educators of manual therapy. J Allied Health. 2007;36(1):30–40.
Ombregt L. A System of Orthopaedic Medicine: Elsevier; 2013.
Cramer GD, Henderson CN, Little JW, Daley C, Grieve TJ. Zygapophyseal joint adhesions after induced hypomobility. J Manipulative Physiol Ther. 2010;33(7):508–18.
George JW, Tunstall AC, Tepe RE, Skaggs CD. The Effects of Active Release Technique on Hamstring Flexibility: A Pilot Study. J Manipulative Physiol Ther. 2006;29(3):224–7.
Bialosky JE, Bishop MD, Price DD, Robinson ME, George SZ. The mechanisms of manual therapy in the treatment of musculoskeletal pain: a comprehensive model. Man Ther. 2009;14(5):531–8.
Plaza-Manzano G, Molina-Ortega F, Lomas-Vega R, Martínez-Amat A, Achalandabaso A, Hita-Contreras F. Changes in biochemical markers of pain perception and stress response after spinal manipulation. J Orthop Sports Phys Ther. 2014;44(4):231–9.
Zusman M. Mechanism of mobilization. Physical Therapy Reviews. 2011;16(4):233–6.
De Carvalho DE, de Luca K, Funabashi M, Breen A, Wong AYL, Johansson MS, et al. Association of Exposures to Seated Postures With Immediate Increases in Back Pain: A Systematic Review of Studies With Objectively Measured Sitting Time. J Manipulative Physiol Ther. 2020;43(1):1–12.
Colloca CJ, Keller TS. Stiffness and neuromuscular reflex response of the human spine to posteroanterior manipulative thrusts in patients with low back pain. J Manipulative Physiol Ther. 2001;24(8):489–500.
Colloca CJ, Keller TS, Gunzburg R. Biomechanical and neurophysiological responses to spinal manipulation in patients with lumbar radiculopathy. J Manipulative Physiol Ther. 2004;27(1):1–15.
Reed WR, Long CR, Kawchuk GN, Sozio RS, Pickar JG. Neural Responses to Physical Characteristics of a High-velocity, Low-amplitude Spinal Manipulation: Effect of Thrust Direction. Spine. 2018;43(1):1–9.
Reed WR, Pickar JG, Sozio RS, Liebschner MAK, Little JW, Gudavalli MR. Characteristics of Paraspinal Muscle Spindle Response to Mechanically Assisted Spinal Manipulation: A Preliminary Report. J Manipulative Physiol Ther. 2017;40(6):371–80.
Devecchi V, Rushton AB, Gallina A, Heneghan NR, Falla D. Are neuromuscular adaptations present in people with recurrent spinal pain during a period of remission? a systematic review. PLoS ONE. 2021;16(4):e0249220.
Pagé I, Nougarou F, Lardon A, Descarreaux M. Changes in spinal stiffness with chronic thoracic pain: Correlation with pain and muscle activity. PLoS ONE. 2018;13(12):e0208790.
Lee RY, McGregor AH, Bull AM, Wragg P. Dynamic response of the cervical spine to posteroanterior mobilisation. Clin Biomech (Bristol, Avon). 2005;20(2):228–31.
Ross JK, Bereznick DE, McGill SM. Determining cavitation location during lumbar and thoracic spinal manipulation: is spinal manipulation accurate and specific? Spine. 2004;29(13):1452–7.
Donaldson M, Petersen S, Cook C, Learman K. A Prescriptively Selected Nonthrust Manipulation Versus a Therapist-Selected Nonthrust Manipulation for Treatment of Individuals With Low Back Pain: A Randomized Clinical Trial. J Orthop Sports Phys Ther. 2016;46(4):243–50.
McCarthy CJ, Potter L, Oldham JA. Comparing targeted thrust manipulation with general thrust manipulation in patients with low back pain. A general approach is as effective as a specific one. A randomised controlled trial. BMJ Open Sport Exerc Med. 2019;5(1):e000514.
Sutlive TG, Mabry LM, Easterling EJ, Durbin JD, Hanson SL, Wainner RS, et al. Comparison of short-term response to two spinal manipulation techniques for patients with low back pain in a military beneficiary population. Mil Med. 2009;174(7):750–6.
Tuttle N, Evans K, Sperotto dos Santos Rocha C. Localised manual therapy treatment has a preferential effect on the kinematics of the targeted motion segment. Musculoskelet Sci Pract. 2021;56:102457.
Ali MN, Sethi K, Noohu MM. Comparison of two mobilization techniques in management of chronic non-specific low back pain. J Bodyw Mov Ther. 2019;23(4):918–23.
de Oliveira RF, Costa LOP, Nascimento LP, Rissato LL. Directed vertebral manipulation is not better than generic vertebral manipulation in patients with chronic low back pain: a randomised trial. J Physiother. 2020;66(3):174–9.
Gevers-Montoro C, Provencher B, Northon S, Stedile-Lovatel JP, Ortega de Mues A, Piché M. Chiropractic Spinal Manipulation Prevents Secondary Hyperalgesia Induced by Topical Capsaicin in Healthy Individuals. Front Pain Res (Lausanne, Switzerland). 2021;2:702429.
Provencher B, Northon S, Piché M. Segmental Chiropractic Spinal Manipulation Does not Reduce Pain Amplification and the Associated Pain-Related Brain Activity in a Capsaicin-Heat Pain Model. Front Pain Res (Lausanne, Switzerland). 2021;2:733727.
Watanabe N, Piché M. Editorial: Mechanisms and Effectiveness of Complementary and Alternative Medicine for Pain Management. Front Pain Res (Lausanne, Switzerland). 2022;3:863751.
Muhsen A, Moss P, Gibson W, Walker B, Jacques A, Schug S, et al. The Association Between Conditioned Pain Modulation and Manipulation-induced Analgesia in People With Lateral Epicondylalgia. Clin J Pain. 2019;35(5):435–42.
Howick J, Glasziou P, Aronson JK. Evidence-based mechanistic reasoning. J Roy Soc Med. 2010;103(11):433–41.
Haavik Taylor H, Murphy B. The effects of spinal manipulation on central integration of dual somatosensory input observed after motor training: a crossover study. J Manipulative Physiol Ther. 2010;33(4):261–72.
Haavik-Taylor H, Murphy B. Cervical spine manipulation alters sensorimotor integration: a somatosensory evoked potential study. ClinNeurophysiol. 2007;118(2):391–402.
Ogura T, Tashiro M, Masud M, Watanuki S, Shibuya K, Yamaguchi K, et al. Cerebral metabolic changes in men after chiropractic spinal manipulation for neck pain. Altern Ther Health Med. 2011;17(6):12–7.
Sparks C, Cleland JA, Elliott JM, Zagardo M, Liu WC. Using functional magnetic resonance imaging to determine if cerebral hemodynamic responses to pain change following thoracic spine thrust manipulation in healthy individuals. J Orthop Sports Phys Ther. 2013;43(5):340–8.
Evans DW. How to gain evidence for causation in disease and therapeutic intervention: from Koch’s postulates to counter-counterfactuals. Med Health Care Philos. 2022;25(3):509–21.
Lascurain-Aguirrebeña I, Newham D, Critchley DJ. Mechanism of Action of Spinal Mobilizations: A Systematic Review. Spine. 2016;41(2):159–72.
Parravicini G, Bergna A. Biological effects of direct and indirect manipulation of the fascial system Narrative review. J Bodyw Mov Ther. 2017;21(2):435–45.
Crane JD, Ogborn DI, Cupido C, Melov S, Hubbard A, Bourgeois JM, et al. Massage therapy attenuates inflammatory signaling after exercise-induced muscle damage. Sci Transl Med. 2012;4(119):119ra13.
Degenhardt BF, Darmani NA, Johnson JC, Towns LC, Rhodes DC, Trinh C, et al. Role of osteopathic manipulative treatment in altering pain biomarkers: a pilot study. J Am Osteopath Assoc. 2007;107(9):387–400.
Kovanur-Sampath K, Mani R, Cotter J, Gisselman AS, Tumilty S. Changes in biochemical markers following spinal manipulation-a systematic review and meta-analysis. Musculoskelet Sci Pract. 2017;29:120–31.
Lohman EB, Pacheco GR, Gharibvand L, Daher N, Devore K, Bains G, et al. The immediate effects of cervical spine manipulation on pain and biochemical markers in females with acute non-specific mechanical neck pain: a randomized clinical trial. J Man Manip Ther. 2019;27(4):186–96.
Teodorczyk-Injeyan JA, McGregor M, Triano JJ, Injeyan SH. Elevated Production of Nociceptive CC Chemokines and sE-Selectin in Patients With Low Back Pain and the Effects of Spinal Manipulation: A Nonrandomized Clinical Trial. Clin J Pain. 2018;34(1):68–75.
Council GC. The Code: Standards of conduct, performance and ethics for chiropractors. GCC; 2019.
Council HaCP. Standards of Proficiency - Physiotherapists. HCPC; 2013.
Council GO. Osteopathic Practice Standards. GOC; 2023.
Therapies TCfST. GCMT Code of Practice, Ethics and Proficiency for Professional Associations. GCMT; 2023.
Daluiso-King G, Hebron C. Is the biopsychosocial model in musculoskeletal physiotherapy adequate? An evolutionary concept analysis. Physiotherapy theory and practice. 2020:1–17.
Søndenå P, Dalusio-King G, Hebron C. Conceptualisation of the therapeutic alliance in physiotherapy: is it adequate? Musculoskelet Sci Pract. 2020;46:102131.
World Health Organisation. Patient Safety 2019 [Available from: https://www.who.int/news-room/fact-sheets/detail/patient-safety#:~:text=Patient%20Safety%20is%20a%20health,during%20provision%20of%20health%20care .
Vogel S, Mars T, Keeping S, Barton T, Marlin N, Froud R, et al. Clinical Risk Osteopathy and Management Scientific Report. 2012.
Ekerholt K, Bergland A. Learning and knowing bodies: Norwegian psychomotor physiotherapists’ reflections on embodied knowledge. Physiother Theory Pract. 2019;35(1):57–69.
Hutting N, Johnston V, Staal JB, Heerkens YF. Promoting the Use of Self-management Strategies for People With Persistent Musculoskeletal Disorders: The Role of Physical Therapists. J Orthop Sports Phys Ther. 2019;49(4):212–5.
Kongsted A, Ris I, Kjaer P, Hartvigsen J. Self-management at the core of back pain care: 10 key points for clinicians. Braz J Phys Therap. 2021.
Elwyn G, Durand MA, Song J, Aarts J, Barr PJ, Berger Z, et al. A three-talk model for shared decision making: multistage consultation process. BMJ (Clinical research ed). 2017;359:j4891.
Broom B. The Practice of Whole Person-Centred Healthcare. In: Anjum RL, Copeland S, Rocca E, editors. Rethinking Causality, Complexity and Evidence for the Unique Patient: A CauseHealth Resource for Healthcare Professionals and the Clinical Encounter. Cham: Springer International Publishing; 2020. p. 215–26.
Chapter Google Scholar
Darlow B, Dowell A, Baxter GD, Mathieson F, Perry M, Dean S. The enduring impact of what clinicians say to people with low back pain. Ann Fam Med. 2013;11(6):527–34.
Stewart M, Loftus S. Sticks and Stones: The Impact of Language in Musculoskeletal Rehabilitation. J Orthop Sports Phys Ther. 2018;48(7):519–22.
Lin I, Wiles L, Waller R, Caneiro JP, Nagree Y, Straker L, et al. Patient-centred care: the cornerstone for high-value musculoskeletal pain management. Br J Sports Med. 2020;54(21):1240–2.
Cowell I, O’Sullivan P, O’Sullivan K, Poyton R, McGregor A, Murtagh G. Perceptions of physiotherapists towards the management of non-specific chronic low back pain from a biopsychosocial perspective: A qualitative study. Musculoskelet Sci Pract. 2018;38:113–9.
Edmond SN, Keefe FJ. Validating pain communication: current state of the science. Pain. 2015;156(2):215–9.
O’Keeffe M, Cullinane P, Hurley J, Leahy I, Bunzli S, O’Sullivan PB, et al. What Influences Patient-Therapist Interactions in Musculoskeletal Physical Therapy? Qualitative Systematic Review and Meta-Synthesis. Phys Ther. 2016;96(5):609–22.
Copnell G. Informed consent in physiotherapy practice: it is not what is said but how it is said. Physiotherapy. 2018;104(1):67–71.
Lee A. Bolam’ to “Montgomery” is result of evolutionary change of medical practice towards ’patient-centred care. Postgrad Med J. 2017;93(1095):46–50.
Lewis J, O’Sullivan P. Is it time to reframe how we care for people with non-traumatic musculoskeletal pain? Br J Sports Med. 2018;52(24):1543–4.
Lewis J, Ridehalgh C, Moore A, Hall K. This is the day your life must surely change: Prioritising behavioural change in musculoskeletal practice. Physiotherapy. 2021.
Lewis JS, Stokes EK, Gojanovic B, Gellatly P, Mbada C, Sharma S, et al. Reframing how we care for people with persistent non-traumatic musculoskeletal pain. Suggestions for the rehabilitation community. Physiotherapy. 2021.
Bishop A, Foster NE, Thomas E, Hay EM. How does the self-reported clinical management of patients with low back pain relate to the attitudes and beliefs of health care practitioners? A survey of UK general practitioners and physiotherapists. Pain. 2008;135(1–2):187–95.
Darlow B, Fullen BM, Dean S, Hurley DA, Baxter GD, Dowell A. The association between health care professional attitudes and beliefs and the attitudes and beliefs, clinical management, and outcomes of patients with low back pain: a systematic review. Eur J Pain (London, England). 2012;16(1):3–17.
Article CAS Google Scholar
Lakke SE, Soer R, Krijnen WP, van der Schans CP, Reneman MF, Geertzen JH. Influence of Physical Therapists’ Kinesiophobic Beliefs on Lifting Capacity in Healthy Adults. Phys Ther. 2015;95(9):1224–33.
Howe LC, Leibowitz KA, Crum AJ. When Your Doctor “Gets It” and “Gets You”: The Critical Role of Competence and Warmth in the Patient-Provider Interaction. Front Psych. 2019;10:475.
Newell D, Lothe LR, Raven TJL. Contextually Aided Recovery (CARe): a scientific theory for innate healing. Chiropr Man Therap. 2017;25:6.
Rossettini G, Camerone EM, Carlino E, Benedetti F, Testa M. Context matters: the psychoneurobiological determinants of placebo, nocebo and context-related effects in physiotherapy. Arch Physiother. 2020;10:11.
Gallace A. Social Touch. In: Olausson H, Wessberg J, Morrison I, McGlone F, editors. Affective Touch and the Neurophysiology of CT Afferents: Springer; 2016.
Gallace A, Spence C. The science of interpersonal touch: an overview. Neurosci Biobehav Rev. 2010;34(2):246–59.
Kelly MA, Nixon L, McClurg C, Scherpbier A, King N, Dornan T. Experience of Touch in Health Care: A Meta-Ethnography Across the Health Care Professions. Qual Health Res. 2018;28(2):200–12.
McGlone F, Cerritelli F, Walker S, Esteves J. The role of gentle touch in perinatal osteopathic manual therapy. Neurosci Biobehav Rev. 2017;72:1–9.
Olausson H, Wessberg J, Morrison I, McGlone F. Affective Touch and the Neurophysiology of CT Afferents: Springer; 2016.
McParlin Z, Cerritelli F, Rossettini G, Friston KJ, Esteves JE. Therapeutic Alliance as Active Inference: The Role of Therapeutic Touch and Biobehavioural Synchrony in Musculoskeletal Care. Front Behav Neurosci. 2022;16:897247.
Meijer LL, Ruis C, van der Smagt MJ, Scherder EJA, Dijkerman HC. Neural basis of affective touch and pain: A novel model suggests possible targets for pain amelioration. J Neuropsychol. 2021.
Allen-Collinson J, Pavey A. Touching moments: phenomenological sociology and the haptic dimension in the lived experience of motor neurone disease. Sociol Health Illn. 2014;36(6):793–806.
Bjorbækmo WS, Mengshoel AM. “A touch of physiotherapy” - the significance and meaning of touch in the practice of physiotherapy. Physiother Theory Pract. 2016;32(1):10–9.
Nummenmaa L, Tuominen L, Dunbar R, Hirvonen J, Manninen S, Arponen E, et al. Social touch modulates endogenous μ-opioid system activity in humans. Neuroimage. 2016;138:242–7.
Calsius J, De Bie J, Hertogen R, Meesen R. Touching the Lived Body in Patients with Medically Unexplained Symptoms. How an Integration of Hands-on Bodywork and Body Awareness in Psychotherapy may Help People with Alexithymia. Front Psychol. 2016;7:253.
Gentsch A, Crucianelli L, Jenkinson P, Fotopoulou A. The touched self: Affective touch and body awareness in health and disease. Affective touch and the neurophysiology of CT afferents Springer; 2016.
Cerritelli F, Chiacchiaretta P, Gambi F, Ferretti A. Effect of Continuous Touch on Brain Functional Connectivity Is Modified by the Operator’s Tactile Attention. Front Hum Neurosci. 2017;11:368.
Tramontano M, Cerritelli F, Piras F, Spanò B, Tamburella F, Piras F, et al. Brain Connectivity Changes after Osteopathic Manipulative Treatment: A Randomized Manual Placebo-Controlled Trial. Brain Sci. 2020;10(12):969.
Øberg GK, Blanchard Y, Obstfelder A. Therapeutic encounters with preterm infants: interaction, posture and movement. Physiother Theory Pract. 2014;30(1):1–5.
Øberg GK, Normann B, Gallagher S. Embodied-enactive clinical reasoning in physical therapy. Physiother Theory Pract. 2015;31(4):244–52.
Consedine S, Standen C, Niven E. Knowing hands converse with an expressive body – An experience of osteopathic touch. Int J Osteopath Med. 2016;19:3–12.
Barbosa CD, Balp MM, Kulich K, Germain N, Rofail D. A literature review to explore the link between treatment satisfaction and adherence, compliance, and persistence. Patient Prefer Adherence. 2012;6:39–48.
Boulding W, Glickman SW, Manary MP, Schulman KA, Staelin R. Relationship between patient satisfaction with inpatient care and hospital readmission within 30 days. Am J Manag Care. 2011;17(1):41–8.
Manary MP, Boulding W, Staelin R, Glickman SW. The patient experience and health outcomes. N Engl J Med. 2013;368(3):201–3.
Sherriff B, Clark C, Killingback C, Newell D. Musculoskeletal practitioners’ perceptions of contextual factors that may influence chronic low back pain outcomes: a modified Delphi study. Chiropr Man Therap. 2023;31(1):12.
Sherriff B, Clark C, Killingback C, Newell D. Impact of contextual factors on patient outcomes following conservative low back pain treatment: systematic review. Chiropr Manual Therap. 2022;30(1):20.
Mercer E, Mackay-Lyons M, Conway N, Flynn J, Mercer C. Perceptions of outpatients regarding the attire of physiotherapists. Physiother Can. 2008;60(4):349–57.
Petrilli CM, Mack M, Petrilli JJ, Hickner A, Saint S, Chopra V. Understanding the role of physician attire on patient perceptions: a systematic review of the literature— targeting attire to improve likelihood of rapport (TAILOR) investigators. BMJ Open. 2015;5(1):e006578.
Beach MC, Fitzgerald A, Saha S. White Coat Hype: Branding Physicians With Professional Attire. JAMA Intern Med. 2013;173(6):467–8.
Bearman G, Bryant K, Leekha S, Mayer J, Munoz-Price LS, Murthy R, et al. Healthcare Personnel Attire in Non-Operating-Room Settings. Infect Control Hosp Epidemiol. 2014;35(2):107–21.
Rehman SU, Nietert PJ, Cope DW, Kilpatrick AO. What to wear today? Effect of doctor’s attire on the trust and confidence of patients. Am J Med. 2005;118(11):1279–86.
Brady B, Veljanova I, Schabrun S, Chipchase L. Integrating culturally informed approaches into physiotherapy assessment and treatment of chronic pain: a pilot randomised controlled trial. BMJ Open. 2018;8(7):e021999.
Miles A, Mezzich JE. The care of the patient and the soul of the clinic: person-centered medicine as an emergent model of clinical practice. Int J Person Centred Med. 2012;1(2):207–22.
Cowell I, McGregor A, O’Sullivan P, O’Sullivan K, Poyton R, Schoeb V, et al. How do physiotherapists solicit and explore patients’ concerns in back pain consultations: a conversation analytic approach. Physiother Theory Pract. 2021;37(6):693–709.
Hutting N, Caneiro JP, Ong'wen MO, Miciak M, Roberts LE. Patient-centered care in musculoskeletal practice: key elements to support clinicians to focus on the person. 2021.
Caneiro JP, Roos EM, Barton CJ, O’Sullivan K, Kent P, Lin I, et al. It is time to move beyond “body region silos” to manage musculoskeletal pain: five actions to change clinical practice. Br J Sports Med. 2020;54(8):438–9.
Greenhalgh T, Howick J, Maskrey N, EBM Renaissance Group. Evidence based medicine: a movement in crisis? Brit Med J. 2014;348:g3725.
Greenhalgh T, Snow R, Ryan S, Rees S, Salisbury H. Six ‘biases’ against patients and carers in evidence-based medicine. Bmc Med. 2015;13(1):200.
Loughlin M, Fuller J, Bluhm R, Buetow S, Borgerson K. Theory, experience and practice. J Eval Clin Pract. 2016;22(4):459–65.
Simpson JK, Innes S. Informed consent, duty of disclosure and chiropractic: where are we? Chiropr Man Therap. 2020;28(1):60.
Download references
Acknowledgements
Use of any animal or human data or tissue.
No funding was received for this paper.
Author information
Authors and affiliations.
School of Health Sciences, Queens Medical Centre, University of Nottingham, Nottingham, NG7 2HA, UK
Roger Kerry, Edward Lee & Vasileios Georgopoulos
Allied Health Research Unit, University of Central Lancashire, Preston, PR1 2HE, UK
Kenneth J. Young
Centre of Precision Rehabilitation for Spinal Pain, School of Sport, Exercise and Rehabilitation Sciences, University of Birmingham, Edgbaston, Birmingham, B15 2TT, UK
David W. Evans
Nottingham CityCare Partnership, Bennerley Rd, Nottingham, NG6 8WR, UK
School of Medicine, University of Nottingham, Queens Medical Centre, Nottingham, NG7 2HA, UK
Vasileios Georgopoulos
Department of Orthopaedics, West Herts Hospitals Trust, Watford, WD18 0HB, UK
Adam Meakins
School of Physiotherapy, Manchester Metropolitan University, Manchester, M15 6GX, UK
Chris McCarthy
Department of Orthopaedics, Duke University, 200 Morris Street, Durham, NC, 27701, USA
School of Sport and Health Sciences, University of Brighton, Darley Rd, Eastbourne, BN20 7UR, UK
Colette Ridehalgh
Clinical Neuroscience, Trafford Building, Brighton and Sussex Medical School, University of Sussex, Brighton, BN1 9PX, UK
University College of Osteopathy, 275 Borough High St, London, SE1 1JE, UK
Steven Vogel & Amanda Banton
Department of Clinical Sciences, Obstetrics and Gynecology, Umeå University, S-90187, Umeå, Sweden
Cecilia Bergström
The School of Soft Tissue Therapy, Exmouth, Devon, EX8 1DQ, UK
Anna Maria Mazzieri
Department of health, LUNEX, Differdange, 4671, Luxembourg
Firas Mourad
Luxembourg Health & Sport Sciences Research Institute A.s.b.l., 50, Avenue du Parc des Sports, Differdange, 4671, Luxembourg
Department of Occupation and Health, School of Organization and Development, HAN University of Applied Sciences, Nijmegen, the Netherlands
Nathan Hutting
You can also search for this author in PubMed Google Scholar
Contributions
Concept and research design: RK, KJY, DWE, EL, AM, VG. Data collection: All authors. Data analysis: All authors. Writing and editing of the manuscript: All authors.
Corresponding author
Correspondence to Kenneth J. Young .
Ethics declarations
Ethics approval and consent to participate.
All participants are co-authors. Ethical approval was not necessary.
Consent for publication
Competing interests.
The authors declare that they have no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Supplementary material 1., rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Kerry, R., Young, K.J., Evans, D.W. et al. A modern way to teach and practice manual therapy. Chiropr Man Therap 32 , 17 (2024). https://doi.org/10.1186/s12998-024-00537-0
Download citation
Received : 18 October 2023
Accepted : 17 April 2024
Published : 21 May 2024
DOI : https://doi.org/10.1186/s12998-024-00537-0
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Manual Therapy
- Evidence-based healthcare
- Person-centred healthcare
- Physiotherapy
- Chiropractic
- Soft-tissue therapy
Chiropractic & Manual Therapies
ISSN: 2045-709X
- Submission enquiries: Access here and click Contact Us
- General enquiries: [email protected]
- Systematic Review
- Open access
- Published: 23 May 2024
Systematic literature review of real-world evidence for treatments in HR+/HER2- second-line LABC/mBC after first-line treatment with CDK4/6i
- Veronique Lambert ORCID: orcid.org/0000-0002-6984-0038 1 ,
- Sarah Kane ORCID: orcid.org/0009-0006-9341-4836 2 na1 ,
- Belal Howidi ORCID: orcid.org/0000-0002-1166-7631 2 na1 ,
- Bao-Ngoc Nguyen ORCID: orcid.org/0000-0001-6026-2270 2 na1 ,
- David Chandiwana ORCID: orcid.org/0009-0002-3499-2565 3 ,
- Yan Wu ORCID: orcid.org/0009-0008-3348-9232 1 ,
- Michelle Edwards ORCID: orcid.org/0009-0001-4292-3140 3 &
- Imtiaz A. Samjoo ORCID: orcid.org/0000-0003-1415-8055 2 na1
BMC Cancer volume 24 , Article number: 631 ( 2024 ) Cite this article
177 Accesses
1 Altmetric
Metrics details
Cyclin-dependent kinase 4 and 6 inhibitors (CDK4/6i) combined with endocrine therapy (ET) are currently recommended by the National Comprehensive Cancer Network (NCCN) guidelines and the European Society for Medical Oncology (ESMO) guidelines as the first-line (1 L) treatment for patients with hormone receptor-positive, human epidermal growth factor receptor 2-negative, locally advanced/metastatic breast cancer (HR+/HER2- LABC/mBC). Although there are many treatment options, there is no clear standard of care for patients following 1 L CDK4/6i. Understanding the real-world effectiveness of subsequent therapies may help to identify an unmet need in this patient population. This systematic literature review qualitatively synthesized effectiveness and safety outcomes for treatments received in the real-world setting after 1 L CDK4/6i therapy in patients with HR+/ HER2- LABC/mBC.
MEDLINE®, Embase, and Cochrane were searched using the Ovid® platform for real-world evidence studies published between 2015 and 2022. Grey literature was searched to identify relevant conference abstracts published from 2019 to 2022. The review was conducted in accordance with PRISMA guidelines (PROSPERO registration: CRD42023383914). Data were qualitatively synthesized and weighted average median real-world progression-free survival (rwPFS) was calculated for NCCN/ESMO-recommended post-1 L CDK4/6i treatment regimens.
Twenty records (9 full-text articles and 11 conference abstracts) encompassing 18 unique studies met the eligibility criteria and reported outcomes for second-line (2 L) treatments after 1 L CDK4/6i; no studies reported disaggregated outcomes in the third-line setting or beyond. Sixteen studies included NCCN/ESMO guideline-recommended treatments with the majority evaluating endocrine-based therapy; five studies on single-agent ET, six studies on mammalian target of rapamycin inhibitors (mTORi) ± ET, and three studies with a mix of ET and/or mTORi. Chemotherapy outcomes were reported in 11 studies. The most assessed outcome was median rwPFS; the weighted average median rwPFS was calculated as 3.9 months (3.3-6.0 months) for single-agent ET, 3.6 months (2.5–4.9 months) for mTORi ± ET, 3.7 months for a mix of ET and/or mTORi (3.0–4.0 months), and 6.1 months (3.7–9.7 months) for chemotherapy. Very few studies reported other effectiveness outcomes and only two studies reported safety outcomes. Most studies had heterogeneity in patient- and disease-related characteristics.
Conclusions
The real-world effectiveness of current 2 L treatments post-1 L CDK4/6i are suboptimal, highlighting an unmet need for this patient population.
Peer Review reports
Introduction
Breast cancer (BC) is the most diagnosed form of cancer in women with an estimated 2.3 million new cases diagnosed worldwide each year [ 1 ]. BC is the second leading cause of cancer death, accounting for 685,000 deaths worldwide per year [ 2 ]. By 2040, the global burden associated with BC is expected to surpass three million new cases and one million deaths annually (due to population growth and aging) [ 3 ]. Numerous factors contribute to global disparities in BC-related mortality rates, including delayed diagnosis, resulting in a high number of BC cases that have progressed to locally advanced BC (LABC) or metastatic BC (mBC) [ 4 , 5 , 6 ]. In the United States (US), the five-year survival rate for patients who progress to mBC is three times lower (31%) than the overall five-year survival rate for all stages (91%) [ 6 , 7 ].
Hormone receptor (HR) positive (i.e., estrogen receptor and/or progesterone receptor positive) coupled with negative human epidermal growth factor 2 (HER2) expression is the most common subtype of BC, accounting for ∼ 60–70% of all BC cases [ 8 , 9 ]. Historically, endocrine therapy (ET) through estrogen receptor modulation and/or estrogen deprivation has been the standard of care for first-line (1 L) treatment of HR-positive/HER2-negative (HR+/HER2-) mBC [ 10 ]. However, with the approval of the cyclin-dependent kinase 4/6 inhibitor (CDK4/6i) palbociclib in combination with the aromatase inhibitor (AI) letrozole in 2015 by the US Food and Drug Administration (FDA), 1 L treatment practice patterns have evolved such that CDK4/6i (either in combination with AIs or with fulvestrant) are currently considered the standard of care [ 11 , 12 , 13 , 14 , 15 , 16 , 17 ]. Other CDK4/6i (ribociclib and abemaciclib) in combination with ET are approved for the treatment of HR+/HER2- LABC/mBC; 1 L use of ribociclib in combination with an AI was granted FDA approval in March 2017 for postmenopausal women (with expanded approval in July 2018 for pre/perimenopausal women and for use in 1 L with fulvestrant for patients with disease progression on ET as well as for postmenopausal women), and abemaciclib in combination with fulvestrant was granted FDA approval in September 2017 for patients with disease progression following ET and as monotherapy in cases where disease progression occurs following ET and prior chemotherapy in mBC (with expanded approval in February 2018 for use in 1 L in combination with an AI for postmenopausal women) [ 18 , 19 , 20 , 21 ].
Clinical trials investigating the addition of CDK4/6i to ET have demonstrated significant improvement in progression-free survival (PFS) and significant (ribociclib) or numerical (palbociclib and abemaciclib) improvement in overall survival (OS) compared to ET alone in patients with HR+/HER2- advanced or mBC, making this combination treatment the recommended option in the 1 L setting [ 22 , 23 , 24 , 25 , 26 , 27 ]. However, disease progression occurs in a significant portion of patients after 1 L CDK4/6i treatment [ 28 ] and the optimal treatment sequence after progression on CDK4/6i remains unclear [ 29 ]. At the time of this review (literature search conducted December 14, 2022), guidelines by the National Comprehensive Cancer Network (NCCN) and the European Society for Medical Oncology (ESMO) recommend various options for the treatment of HR+/HER2- advanced BC in the second-line (2 L) setting, including fulvestrant monotherapy, mammalian target of rapamycin inhibitors (mTORi; e.g., everolimus) ± ET, alpelisib + fulvestrant (if phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit alpha mutation positive [PIK3CA-m+]), poly-ADP ribose polymerase inhibitors (PARPi) including olaparib or talazoparib (if breast cancer gene/partner and localizer of BRCA2 positive [BRCA/PALB2m+]), and chemotherapy (in cases when a visceral crisis is present) [ 15 , 16 ]. CDK4/6i can also be used in 2 L [ 16 , 30 ]; however, limited data are available to support CDK4/6i rechallenge after its use in the 1 L setting [ 15 ]. Depending on treatments used in the 1 L and 2 L settings, treatment in the third-line setting is individualized based on the patient’s response to prior treatments, tumor load, duration of response, and patient preference [ 9 , 15 ]. Understanding subsequent treatments after 1 L CDK4/6i, and their associated effectiveness, is an important focus in BC research.
Treatment options for HR+/HER2- LABC/mBC continue to evolve, with ongoing research in both clinical trials and in the real-world setting. Real-world evidence (RWE) offers important insights into novel therapeutic regimens and the effectiveness of treatments for HR+/HER2- LABC/mBC. The effectiveness of the current treatment options following 1 L CDK4/6i therapy in the real-world setting highlights the unmet need in this patient population and may help to drive further research and drug development. In this study, we conducted a systematic literature review (SLR) to qualitatively summarize the effectiveness and safety of treatment regimens in the real-world setting after 1 L treatment with CDK4/6i in patients with HR+/HER2- LABC/mBC.
Literature search
An SLR was performed in accordance with the Cochrane Handbook for Systematic Reviews of Interventions [ 31 ] and reported in alignment with the Preferred Reporting Items for Systematic Literature Reviews and Meta-Analyses (PRISMA) statement [ 32 ] to identify all RWE studies assessing the effectiveness and safety of treatments used for patients with HR+/HER2- LABC/mBC following 1 L CDK4/6i therapy and received subsequent treatment in 2 L and beyond (2 L+). The Ovid® platform was used to search MEDLINE® (including Epub Ahead of Print and In-Process, In-Data-Review & Other Non-Indexed Citations), Ovid MEDLINE® Daily, Embase, Cochrane Central Register of Controlled Trials, and Cochrane Database of Systematic Reviews by an experienced medical information specialist. The MEDLINE® search strategy was peer-reviewed independently by a senior medical information specialist before execution using the Peer Review of Electronic Search Strategies (PRESS) checklist [ 33 ]. Searches were conducted on December 14, 2022. The review protocol was developed a priori and registered with the International Prospective Register of Systematic Review (PROSPERO; CRD42023383914) which outlined the population, intervention, comparator, outcome, and study design (PICOS) criteria and methodology used to conduct the review (Table 1 ).
Search strategies utilized a combination of controlled vocabulary (e.g., “HER2 Breast Cancer” or “HR Breast Cancer”) and keywords (e.g., “Retrospective studies”). Vocabulary and syntax were adjusted across databases. Published and validated filters were used to select for study design and were supplemented using additional medical subject headings (MeSH) terms and keywords to select for RWE and nonrandomized studies [ 34 ]. No language restrictions were included in the search strategy. Animal-only and opinion pieces were removed from the results. The search was limited to studies published between January 2015 and December 2022 to reflect the time at which FDA approval was granted for the first CDK4/6i agent (palbociclib) in combination with AI for the treatment of LABC/mBC [ 35 ]. Further search details are presented in Supplementary Material 1 .
Grey literature sources were also searched to identify relevant abstracts and posters published from January 2019 to December 2022 for prespecified relevant conferences including ESMO, San Antonio Breast Cancer Symposium (SABCS), American Society of Clinical Oncology (ASCO), the International Society for Pharmacoeconomics and Outcomes Research (ISPOR US), and the American Association for Cancer Research (AACR). A search of ClinicalTrials.gov was conducted to validate the findings from the database and grey literature searches.
Study selection, data extraction & weighted average calculation
Studies were screened for inclusion using DistillerSR Version 2.35 and 2.41 (DistillerSR Inc. 2021, Ottawa, Canada) by two independent reviewers based on the prespecified PICOS criteria (Table 1 ). A third reviewer was consulted to resolve any discrepancies during the screening process. Studies were included if they reported RWE on patients aged ≥ 18 years with HR+/HER2- LABC/mBC who received 1 L CDK4/6i treatment and received subsequent treatment in 2 L+. Studies were excluded if they reported the results of clinical trials (i.e., non-RWE), were published in any language other than English, and/or were published prior to 2015 (or prior to 2019 for conference abstracts and posters). For studies that met the eligibility criteria, data relating to study design and methodology, details of interventions, patient eligibility criteria and baseline characteristics, and outcome measures such as efficacy, safety, tolerability, and patient-reported outcomes (PROs), were extracted (as available) using a Microsoft Excel®-based data extraction form (Microsoft Corporation, WA, USA). Data extraction was performed by a single reviewer and was confirmed by a second reviewer. Multiple publications identified for the same RWE study, patient population, and setting that reported data for the same intervention were linked and extracted as a single publication. Weighted average median real-world progression-free survival (rwPFS) values were calculated by considering the contribution to the median rwPFS of each study proportional to its respective sample size. These weighted values were then used to compute the overall median rwPFS estimate.
Quality assessment
The Newcastle-Ottawa scale (NOS) for nonrandomized (cohort) studies was used to assess the risk of bias for published, full-text studies [ 36 ]. The NOS allocates a maximum of nine points for the least risk of bias across three domains: (1) Formation of study groups (four points), (2) Comparability between study groups (two points), (3) Outcome ascertainment (three points). NOS scores can be categorized in three groups: very high risk of bias (0 to 3 points), high risk of bias (4 to 6), and low risk of bias (7 to 9) [ 37 ]. Risk of bias assessment was performed by one reviewer and validated by a second independent reviewer to verify accuracy. Due to limited methodological data by which to assess study quality, risk of bias assessment was not performed on conference abstracts or posters. An amendment to the PROSPERO record (CRD42023383914) for this study was submitted in relation to the quality assessment method (specifying usage of the NOS).
The database search identified 3,377 records; after removal of duplicates, 2,759 were screened at the title and abstract stage of which 2,553 were excluded. Out of the 206 reports retrieved and assessed for eligibility, an additional 187 records were excluded after full-text review; most of these studies were excluded for having patients with mixed lines of CDK4/6i treatment (i.e., did not receive CDK4/6i exclusively in 1 L) (Fig. 1 and Table S1 ). The grey literature search identified 753 records which were assessed for eligibility; of which 752 were excluded mainly due to the population not meeting the eligibility criteria (Fig. 1 ). In total, the literature searches identified 20 records (9 published full-text articles and 11 conference abstracts/posters) representing 18 unique RWE studies that met the inclusion criteria. The NOS quality scores for the included full-text articles are provided in Table S2 . The scores ranged from four to six points (out of a total score of nine) and the median score was five, indicating that all the studies suffered from a high risk of bias [ 37 ].
Most studies were retrospective analyses of chart reviews or medical registries, and all studies were published between 2017 and 2022 (Table S3 ). Nearly half of the RWE studies (8 out of 18 studies) were conducted in the US [ 38 , 39 , 40 , 41 , 42 , 43 , 44 , 45 ], while the remaining studies included sites in Canada, China, Germany, Italy, Japan, and the United Kingdom [ 46 , 47 , 48 , 49 , 50 , 51 , 52 , 53 , 54 ]. Sample sizes ranged from as few as 4 to as many as 839 patients across included studies, with patient age ranging from 26 to 86 years old.
Although treatment characteristics in the 1 L setting were not the focus of the present review, these details are captured in Table S3 . Briefly, several RWE studies reported 1 L CDK4/6i use in combination with ET (8 out of 18 studies) or as monotherapy (2 out of 18 studies) (Table S3 ). Treatments used in combination with 1 L CDK4/6i included letrozole, fulvestrant, exemestane, and anastrozole. Where reported (4 out of 18 studies), palbociclib was the most common 1 L CDK4/6i treatment. Many studies (8 out of 18 studies) did not report which specific CDK4/6i treatment(s) were used in 1 L or if its administration was in combination or monotherapy.
Characteristics of treatments after 1 L CDK4/6i therapy
Across all studies included in this review, effectiveness and safety data were only available for treatments administered in the 2 L setting after 1 L CDK4/6i treatment. No studies were identified that reported outcomes for patients treated in the third-line setting or beyond after 1 L CDK4/6i treatment. All 18 studies reported effectiveness outcomes in 2 L, with only two of these studies also describing 2 L safety outcomes. The distribution of outcomes reported in these studies is provided in Table S4 . Studies varied in their reporting of outcomes for 2 L treatments; some studies reported outcomes for a group of 2 L treatments while others described independent outcomes for specific 2 L treatments (i.e., everolimus, fulvestrant, or chemotherapy agents such as eribulin mesylate) [ 42 , 45 , 50 , 54 , 55 ]. Due to the heterogeneity in treatment classes reported in these studies, this data was categorized (as described below) to align with the guidelines provided by NCCN and ESMO [ 15 , 16 ]. The treatment class categorizations for the purpose of this review are: single-agent ET (patients who exclusively received a single-agent ET after 1 L CDK4/6i treatment), mTORi ± ET (patients who exclusively received an mTORi with or without ET after 1 L CDK4/6i treatment), mix of ET and/or mTORi (patients who may have received only ET, only mTORi, and/or both treatments but the studies in this group lacked sufficient information to categorize these patients in the “single-agent ET” or “mTOR ± ET” categories), and chemotherapy (patients who exclusively received chemotherapy after 1 L CDK4/6i treatment). Despite ESMO and NCCN guidelines indicating that limited evidence exists to support rechallenge with CDK4/6i after 1 L CDK4/6i treatment [ 15 , 16 ], two studies reported outcomes for this treatment approach. Data for such patients were categorized as “ CDK4/6i ± ET ” as it was unclear how many patients receiving CDK4/6i rechallenge received concurrent ET. All other patient groups that lacked sufficient information or did not report outcome/safety data independently (i.e., grouped patients with mixed treatments) to categorize as one of the treatment classes described above were grouped as “ other ”.
The majority of studies reported effectiveness outcomes for endocrine-based therapy after 1 L CDK4/6i treatment; five studies for single-agent ET, six studies for mTORi ± ET, and three studies for a mix of ET and/or mTORi (Fig. 2 ). Eleven studies reported effectiveness outcomes for chemotherapy after 1 L CDK4/6i treatment, and only two studies reported effectiveness outcomes for CDK4/6i rechallenge ± ET. Eight studies that described effectiveness outcomes were grouped into the “other” category. Safety data was only reported in two studies: one study evaluating the chemotherapy agent eribulin mesylate and one evaluating the mTORi everolimus.
Effectiveness outcomes
Real-world progression-free survival
Median rwPFS was described in 13 studies (Tables 2 and Table S5 ). Across the 13 studies, the median rwPFS ranged from 2.5 months [ 49 ] to 17.3 months [ 39 ]. Out of the 13 studies reporting median rwPFS, 10 studies reported median rwPFS for a 2 L treatment recommended by ESMO and NCCN guidelines, which ranged from 2.5 months [ 49 ] to 9.7 months [ 45 ].
Weighted average median rwPFS was calculated for 2 L treatments recommended by both ESMO and NCCN guidelines (Fig. 3 ). The weighted average median rwPFS for single-agent ET was 3.9 months ( n = 92 total patients) and was derived using data from two studies reporting median rwPFS values of 3.3 months ( n = 70) [ 38 ] and 6.0 months ( n = 22) [ 40 ]. For one study ( n = 7) that reported outcomes for single agent ET, median rwPFS was not reached during the follow-up period; as such, this study was excluded from the weighted average median rwPFS calculation [ 49 ].
The weighted average median rwPFS for mTORi ± ET was 3.6 months ( n = 128 total patients) and was derived based on data from 3 studies with median rwPFS ranging from 2.5 months ( n = 4) [ 49 ] to 4.9 months ( n = 25) [ 54 ] (Fig. 3 ). For patients who received a mix of ET and/or mTORi but could not be classified into the single-agent ET or mTORi ± ET treatment classes, the weighted average median rwPFS was calculated to be 3.7 months ( n = 17 total patients). This was calculated based on data from two studies reporting median rwPFS values of 3.0 months ( n = 5) [ 46 ] and 4.0 months ( n = 12) [ 49 ]. Notably, one study of patients receiving ET and/or everolimus reported a median rwPFS duration of 3.0 months; however, this study was excluded from the weighted average median rwPFS calculation for the ET and/or mTORi class as the sample size was not reported [ 53 ].
The weighted average median rwPFS for chemotherapy was 6.1 months ( n = 499 total patients), calculated using data from 7 studies reporting median rwPFS values ranging from 3.7 months ( n = 249) [ 38 ] to 9.7 months ( n = 121) [ 45 ] (Fig. 3 ). One study with a median rwPFS duration of 5.6 months was not included in the weighted average median rwPFS calculation as the study did not report the sample size [ 53 ]. A second study was excluded from the calculation since the reported median rwPFS was not reached during the study period ( n = 7) [ 41 ].
Although 2 L CDK4/6i ± ET rechallenge lacks sufficient information to support recommendation by ESMO and NCCN guidelines, the limited data currently available for this treatment have shown promising results. Briefly, two studies reported median rwPFS for CDK4/6i ± ET with values of 8.3 months ( n = 302) [ 38 ] and 17.3 months ( n = 165) (Table 2 ) [ 39 ]. The remaining median rwPFS studies reported data for patients classified as “Other” (Table S5 ). The “Other” category included median rwPFS outcomes from seven studies, and included a myriad of treatments (e.g., ET, mTOR + ET, chemotherapy, CDK4/6i + ET, alpelisib + fulvestrant, chidamide + ET) for which disaggregated median rwPFS values were not reported.
Overall survival
Median OS for 2 L treatment was reported in only three studies (Table 2 ) [ 38 , 42 , 43 ]. Across the three studies, the 2 L median OS ranged from 5.2 months ( n = 3) [ 43 ] to 35.7 months ( n = 302) [ 38 ]. Due to the lack of OS data in most of the studies, weighted averages could not be calculated. No median OS data was reported for the single-agent ET treatment class whereas two studies reported median OS for the mTORi ± ET treatment class, ranging from 5.2 months ( n = 3) [ 43 ] to 21.8 months ( n = 54) [ 42 ]. One study reported 2 L median OS of 24.8 months for a single patient treated with chemotherapy [ 43 ]. The median OS data in the CDK4/6i ± ET rechallenge group was 35.7 months ( n = 302) [ 38 ].
Patient mortality was reported in three studies [ 43 , 44 , 45 ]. No studies reported mortality for the single-agent ET treatment class and only one study reported this outcome for the mTORi ± ET treatment class, where 100% of patients died ( n = 3) as a result of rapid disease progression [ 43 ]. For the chemotherapy class, one study reported mortality for one patient receiving 2 L capecitabine [ 43 ]. An additional study reported eight deaths (21.7%) following 1 L CDK4/6i treatment; however, this study did not disclose the 2 L treatments administered to these patients [ 44 ].
Other clinical endpoints
The studies included limited information on additional clinical endpoints; two studies reported on time-to-discontinuation (TTD), two reported on duration of response (DOR), and one each on time-to-next-treatment (TTNT), time-to-progression (TTP), objective response rate (ORR), clinical benefit rate (CBR), and stable disease (Tables 2 and Table S5 ).
Safety, tolerability, and patient-reported outcomes
Safety and tolerability data were reported in two studies [ 40 , 45 ]. One study investigating 2 L administration of the chemotherapy agent eribulin mesylate reported 27 patients (22.3%) with neutropenia, 3 patients (2.5%) with febrile neutropenia, 10 patients (8.3%) with peripheral neuropathy, and 14 patients (11.6%) with diarrhea [ 45 ]. Of these, neutropenia of grade 3–4 severity occurred in 9 patients (33.3%) [ 45 ]. A total of 55 patients (45.5%) discontinued eribulin mesylate treatment; 1 patient (0.83%) discontinued treatment due to adverse events [ 45 ]. Another study reported that 5 out of the 22 patients receiving the mTORi everolimus combined with ET in 2 L (22.7%) discontinued treatment due to toxicity [ 40 ]. PROs were not reported in any of the studies included in the SLR.
The objective of this study was to summarize the existing RWE on the effectiveness and safety of therapies for patients with HR+/HER2- LABC/mBC after 1 L CDK4/6i treatment. We identified 18 unique studies reporting specifically on 2 L treatment regimens after 1 L CDK4/6i treatment. The weighted average median rwPFS for NCCN- and ESMO- guideline recommended 2 L treatments ranged from 3.6 to 3.9 months for ET-based treatments and was 6.1 months when including chemotherapy-based regimens. Treatment selection following 1 L CDK4/6i therapy remains challenging primarily due to the suboptimal effectiveness or significant toxicities (e.g., chemotherapy) associated with currently available options [ 56 ]. These results highlight that currently available 2 L treatments for patients with HR+/HER2- LABC/mBC who have received 1 L CDK4/6i are suboptimal, as evidenced by the brief median rwPFS duration associated with ET-based treatments, or notable side effects and toxicity linked to chemotherapy. This conclusion is aligned with a recent review highlighting the limited effectiveness of treatment options for HR+/HER2- LABC/mBC patients post-CDK4/6i treatment [ 56 , 57 ]. Registrational trials which have also shed light on the short median PFS of 2–3 months achieved by ET (i.e., fulvestrant) after 1 L CDK4/6i therapy emphasize the need to develop improved treatment strategies aimed at prolonging the duration of effective ET-based treatment [ 56 ].
The results of this review reveal a paucity of additional real-world effectiveness and safety evidence after 1 L CDK4/6i treatment in HR+/HER2- LABC/mBC. OS and DOR were only reported in two studies while other clinical endpoints (i.e., TTD, TTNT, TTP, ORR, CBR, and stable disease) were only reported in one study each. Similarly, safety and tolerability data were only reported in two studies each, and PROs were not reported in any study. This hindered our ability to provide a comprehensive assessment of real-world treatment effectiveness and safety following 1 L CDK4/6i treatment. The limited evidence may be due to the relatively short period of time that has elapsed since CDK4/6i first received US FDA approval for 1 L treatment of HR+/HER2- LABC/mBC (2015) [ 35 ]. As such, almost half of our evidence was informed by conference abstracts. Similarly, no real-world studies were identified in our review that reported outcomes for treatments in the third- or later-lines of therapy after 1 L CDK4/6i treatment. The lack of data in this patient population highlights a significant gap which limits our understanding of the effectiveness and safety for patients receiving later lines of therapy. As more patients receive CDK4/6i therapy in the 1 L setting, the number of patients requiring subsequent lines of therapy will continue to grow. Addressing this data gap over time will be critical to improve outcomes for patients with HR+/HER2- LABC/mBC following 1 L CDK4/6i therapy.
There are several strengths of this study, including adherence to the guidelines outlined in the Cochrane Handbook to ensure a standardized and reliable approach to the SLR [ 58 ] and reporting of the SLR following PRISMA guidelines to ensure transparency and reproducibility [ 59 ]. Furthermore, the inclusion of only RWE studies allowed us to assess the effectiveness of current standard of care treatments outside of a controlled environment and enabled us to identify an unmet need in this patient population.
This study had some notable limitations, including the lack of safety and additional effectiveness outcomes reported. In addition, the dearth of studies reporting PROs is a limitation, as PROs provide valuable insight into the patient experience and are an important aspect of assessing the impact of 2 L treatments on patients’ quality of life. The studies included in this review also lacked consistent reporting of clinical characteristics (e.g., menopausal status, sites of metastasis, prior surgery) making it challenging to draw comprehensive conclusions or comparisons based on these factors across the studies. Taken together, there exists an important gap in our understanding of the long-term management of patients with HR+/HER2- LABC/mBC. Additionally, the effectiveness results reported in our evidence base were informed by small sample sizes; many of the included studies reported median rwPFS based on less than 30 patients [ 39 , 40 , 41 , 46 , 49 , 51 , 60 ], with two studies not reporting the sample size at all [ 47 , 53 ]. This may impact the generalizability and robustness of the results. Relatedly, the SLR database search was conducted in December 2022; as such, novel agents (e.g., elacestrant and capivasertib + fulvestrant) that have since received FDA approval for the treatment of HR+/HER2- LABC/mBC may impact current 2 L rwPFS outcomes [ 61 , 62 ]. Finally, relative to the number of peer-reviewed full-text articles, this SLR identified eight abstracts and one poster presentation, comprising half (50%) of the included unique studies. As conference abstracts are inherently limited by how much content that can be described due to word limit constraints, this likely had implications on the present synthesis whereby we identified a dearth of real-world effectiveness outcomes in patients with HR+/HER2- LABC/mBC treated with 1 L CDK4/6i therapy.
Future research in this area should aim to address the limitations of the current literature and provide a more comprehensive understanding of optimal sequencing of effective and safe treatment for patients following 1 L CDK4/6i therapy. Specifically, future studies should strive to report robust data related to effectiveness, safety, and PROs for patients receiving 2 L treatment after 1 L CDK4/6i therapy. Future studies should also aim to understand the mechanism underlying CDK4/6i resistance. Addressing these gaps in knowledge may improve the long-term real-world management of patients with HR+/HER2- LABC/mBC. A future update of this synthesis may serve to capture a wider breadth of full-text, peer-reviewed articles to gain a more robust understanding of the safety, effectiveness, and real-world treatment patterns for patients with HR+/HER2- LABC/mBC. This SLR underscores the necessity for ongoing investigation and the development of innovative therapeutic approaches to address these gaps and improve patient outcomes.
This SLR qualitatively summarized the existing real-world effectiveness data for patients with HR+/HER2- LABC/mBC after 1 L CDK4/6i treatment. Results of this study highlight the limited available data and the suboptimal effectiveness of treatments employed in the 2 L setting and underscore the unmet need in this patient population. Additional studies reporting effectiveness and safety outcomes, in addition to PROs, for this patient population are necessary and should be the focus of future research.

PRISMA flow diagram. *Two included conference abstracts reported the same information as already included full-text reports, hence both conference abstracts were not identified as unique. Abbreviations: 1 L = first-line; AACR = American Association of Cancer Research; ASCO = American Society of Clinical Oncology; CDK4/6i = cyclin-dependent kinase 4/6 inhibitor; ESMO = European Society for Medical Oncology; ISPOR = Professional Society for Health Economics and Outcomes Research; n = number of studies; NMA = network meta-analysis; pts = participants; SABCS = San Antonio Breast Cancer Symposium; SLR = systematic literature review.

Number of studies reporting effectiveness outcomes exclusively for each treatment class. *Studies that lack sufficient information on effectiveness outcomes to classify based on the treatment classes outlined in the legend above. Abbreviations: CDK4/6i = cyclin-dependent kinase 4/6 inhibitor; ET = endocrine therapy; mTORi = mammalian target of rapamycin inhibitor.

Weighted average median rwPFS for 2 L treatments (recommended in ESMO/NCCN guidelines) after 1 L CDK4/6i treatment. Circular dot represents weighted average median across studies. Horizontal bars represent the range of values reported in these studies. Abbreviations: CDK4/6i = cyclin-dependent kinase 4/6 inhibitor; ESMO = European Society for Medical Oncology; ET = endocrine therapy, mTORi = mammalian target of rapamycin inhibitor; n = number of patients; NCCN = National Comprehensive Cancer Network; rwPFS = real-world progression-free survival.
Data availability
All data generated or analyzed during this study are included in this published article [and its supplementary information files]. This study is registered with PROSPERO (CRD42023383914).
Abbreviations
Second-line
Second-line treatment setting and beyond
American Association of Cancer Research
Aromatase inhibitor
American Society of Clinical Oncology
- Breast cancer
breast cancer gene/partner and localizer of BRCA2 positive
Clinical benefit rate
Cyclin-dependent kinase 4/6 inhibitor
Complete response
Duration of response
European Society for Medical Oncology
Food and Drug Administration
Human epidermal growth factor receptor 2
Human epidermal growth factor receptor 2 negative
Hormone receptor
Hormone receptor positive
Professional Society for Health Economics and Outcomes Research
Locally advanced breast cancer
Metastatic breast cancer
Medical Literature Analysis and Retrieval System Online
Medical subject headings
Mammalian target of rapamycin inhibitor
National Comprehensive Cancer Network
Newcastle Ottawa Scale
Objective response rate
Poly-ADP ribose polymerase inhibitor
Progression-free survival
Population, Intervention, Comparator, Outcome, Study Design
Partial response
Preferred Reporting Items for Systematic Literature Reviews and Meta-Analyses
Patient-reported outcomes
- Real-world evidence
San Antonio Breast Cancer Symposium
- Systematic literature review
Time-to-discontinuation
Time-to-next-treatment
Time-to-progression
United States
Łukasiewicz S, Czeczelewski M, Forma A, Baj J, Sitarz R, Stanisławek A, Breast, Cancer—Epidemiology. Risk factors, classification, prognostic markers, and current treatment Strategies—An. Updated Rev Cancers. 2021;13(17):4287.
Google Scholar
World Health Organization (WHO). Breast Cancer Facts Sheet [updated July 12 2023. https://www.who.int/news-room/fact-sheets/detail/breast-cancer .
Arnold M, Morgan E, Rumgay H, Mafra A, Singh D, Laversanne M, et al. Current and future burden of breast cancer: global statistics for 2020 and 2040. Breast. 2022;66:15–23.
Article PubMed PubMed Central Google Scholar
Wilkinson L, Gathani T. Understanding breast cancer as a global health concern. Br J Radiol. 2022;95(1130):20211033.
Article PubMed Google Scholar
Giaquinto AN, Sung H, Miller KD, Kramer JL, Newman LA, Minihan A et al. Breast Cancer Statistics, 2022. CA: A Cancer Journal for Clinicians. 2022;72(6):524– 41.
National Cancer Institute (NIH). Cancer Stat Facts: Female Breast Cancer [updated 2020. https://seer.cancer.gov/statfacts/html/breast.html .
American Cancer Society. Key Statistics for Breast Cancer [ https://www.cancer.org/cancer/types/breast-cancer/about/how-common-is-breast-cancer.html .
Zagami P, Carey LA. Triple negative breast cancer: pitfalls and progress. npj Breast Cancer. 2022;8(1):95.
Article CAS PubMed PubMed Central Google Scholar
Matutino A, Joy AA, Brezden-Masley C, Chia S, Verma S. Hormone receptor-positive, HER2-negative metastatic breast cancer: redrawing the lines. Curr Oncol. 2018;25(Suppl 1):S131–41.
Lloyd MR, Wander SA, Hamilton E, Razavi P, Bardia A. Next-generation selective estrogen receptor degraders and other novel endocrine therapies for management of metastatic hormone receptor-positive breast cancer: current and emerging role. Ther Adv Med Oncol. 2022;14:17588359221113694.
Cardoso F, Senkus E, Costa A, Papadopoulos E, Aapro M, André F, et al. 4th ESO-ESMO International Consensus guidelines for advanced breast Cancer (ABC 4)†. Ann Oncol. 2018;29(8):1634–57.
Article CAS PubMed Google Scholar
US Food Drug Administration. Palbociclib (Ibrance) 2017 [updated March 31, 2017. https://www.fda.gov/drugs/resources-information-approved-drugs/palbociclib-ibrance .
US Food Drug Administration. FDA expands ribociclib indication in HR-positive, HER2-negative advanced or metastatic breast cancer 2018 [updated July 18. 2018. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-expands-ribociclib-indication-hr-positive-her2-negative-advanced-or-metastatic-breast-cancer .
US Food Drug Administration. FDA approves abemaciclib for HR positive, HER2-negative breast cancer 2017 [updated Sept 28. 2017. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-abemaciclib-hr-positive-her2-negative-breast-cancer .
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Breast Cancer 2022 [ https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf .
Gennari A, André F, Barrios CH, Cortés J, de Azambuja E, DeMichele A, et al. ESMO Clinical Practice Guideline for the diagnosis, staging and treatment of patients with metastatic breast cancer. Ann Oncol. 2021;32(12):1475–95.
Beaver JA, Amiri-Kordestani L, Charlab R, Chen W, Palmby T, Tilley A, et al. FDA approval: Palbociclib for the Treatment of Postmenopausal Patients with estrogen Receptor-Positive, HER2-Negative metastatic breast Cancer. Clin Cancer Res. 2015;21(21):4760–6.
US Food Drug Administration. Ribociclib (Kisqali) [ https://www.fda.gov/drugs/resources-information-approved-drugs/ribociclib-kisqali#:~:text=On%20March%2013%2C%202017%2C%20the,hormone%20receptor%20(HR)%2Dpositive%2C .
US Food Drug Administration. FDA approves new treatment for certain advanced or metastatic breast cancers [ https://www.fda.gov/news-events/press-announcements/fda-approves-new-treatment-certain-advanced-or-metastatic-breast-cancers .
US Food Drug Administration. FDA expands ribociclib indication in HR-positive, HER2-negative advanced or metastatic breast cancer. 2018 [ https://www.fda.gov/drugs/resources-information-approved-drugs/fda-expands-ribociclib-indication-hr-positive-her2-negative-advanced-or-metastatic-breast-cancer .
US Food Drug Administration. FDA approves abemaciclib as initial therapy for HR-positive, HER2-negative metastatic breast cancer [ https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-abemaciclib-initial-therapy-hr-positive-her2-negative-metastatic-breast-cancer .
Turner NC, Slamon DJ, Ro J, Bondarenko I, Im S-A, Masuda N, et al. Overall survival with Palbociclib and fulvestrant in advanced breast Cancer. N Engl J Med. 2018;379(20):1926–36.
Slamon DJ, Neven P, Chia S, Fasching PA, De Laurentiis M, Im SA, et al. Phase III randomized study of Ribociclib and Fulvestrant in hormone Receptor-Positive, human epidermal growth factor receptor 2-Negative advanced breast Cancer: MONALEESA-3. J Clin Oncol. 2018;36(24):2465–72.
Goetz MP, Toi M, Campone M, Sohn J, Paluch-Shimon S, Huober J, et al. MONARCH 3: Abemaciclib as initial therapy for advanced breast Cancer. J Clin Oncol. 2017;35(32):3638–46.
Gopalan PK, Villegas AG, Cao C, Pinder-Schenck M, Chiappori A, Hou W, et al. CDK4/6 inhibition stabilizes disease in patients with p16-null non-small cell lung cancer and is synergistic with mTOR inhibition. Oncotarget. 2018;9(100):37352–66.
Watt AC, Goel S. Cellular mechanisms underlying response and resistance to CDK4/6 inhibitors in the treatment of hormone receptor-positive breast cancer. Breast Cancer Res. 2022;24(1):17.
Goetz M. MONARCH 3: final overall survival results of abemaciclib plus a nonsteroidal aromatase inhibitor as first-line therapy for HR+, HER2- advanced breast cancer. SABCS; 2023.
Munzone E, Pagan E, Bagnardi V, Montagna E, Cancello G, Dellapasqua S, et al. Systematic review and meta-analysis of post-progression outcomes in ER+/HER2– metastatic breast cancer after CDK4/6 inhibitors within randomized clinical trials. ESMO Open. 2021;6(6):100332.
Gennari A, André F, Barrios CH, Cortés J, de Azambuja E, DeMichele A, et al. ESMO Clinical Practice Guideline for the diagnosis, staging and treatment of patients with metastatic breast cancer. Annals of Oncology. 2021;32(12):1475-95.
European Society for Medical Oncology (ESMO). ESMO Metastatic Breast Cancer Living Guideline: ER-positive HER2-negative Breast Cancer [updated May 2023. https://www.esmo.org/living-guidelines/esmo-metastatic-breast-cancer-living-guideline/er-positive-her2-negative-breast-cancer .
Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Welch PM VA, editors. Cochrane Handbook for Systematic Reviews of Interventions version 6.2 (updated February 2021). www.training.cochrane.org/handbook : Cochrane; 2021.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. PLoS Med. 2021;18(3):e1003583.
McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS peer review of electronic search strategies: 2015 Guideline Statement. J Clin Epidemiol. 2016;75:40–6.
Fraser C, Murray A, Burr J. Identifying observational studies of surgical interventions in MEDLINE and EMBASE. BMC Med Res Methodol. 2006;6(1):41.
US Food Drug Administration. Palbociclib (Ibrance). Silver Spring, MD: US Food and Drug Administration; 2017.
Book Google Scholar
GA Wells BS, D O’Connell J, Peterson V, Welch M, Losos PT. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses [ https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp .
Lo CK-L, Mertz D, Loeb M. Newcastle-Ottawa Scale: comparing reviewers’ to authors’ assessments. BMC Med Res Methodol. 2014;14(1):45.
Martin JM, Handorf EA, Montero AJ, Goldstein LJ. Systemic therapies following progression on first-line CDK4/6-inhibitor treatment: analysis of real-world data. Oncologist. 2022;27(6):441–6.
Kalinsky KM, Kruse M, Smyth EN, Guimaraes CM, Gautam S, Nisbett AR et al. Abstract P1-18-37: Treatment patterns and outcomes associated with sequential and non-sequential use of CDK4 and 6i for HR+, HER2- MBC in the real world. Cancer Research. 2022;82(4_Supplement):P1-18-37-P1-18-37.
Choong GM, Liddell S, Ferre RAL, O’Sullivan CC, Ruddy KJ, Haddad TC, et al. Clinical management of metastatic hormone receptor-positive, HER2-negative breast cancer (MBC) after CDK 4/6 inhibitors: a retrospective single-institution study. Breast Cancer Res Treat. 2022;196(1):229–37.
Xi J, Oza A, Thomas S, Ademuyiwa F, Weilbaecher K, Suresh R, et al. Retrospective Analysis of Treatment Patterns and effectiveness of Palbociclib and subsequent regimens in metastatic breast Cancer. J Natl Compr Canc Netw. 2019;17(2):141–7.
Rozenblit M, Mun S, Soulos P, Adelson K, Pusztai L, Mougalian S. Patterns of treatment with everolimus exemestane in hormone receptor-positive HER2-negative metastatic breast cancer in the era of targeted therapy. Breast Cancer Res. 2021;23(1):14.
Bashour SI, Doostan I, Keyomarsi K, Valero V, Ueno NT, Brown PH, et al. Rapid breast Cancer Disease Progression following cyclin dependent kinase 4 and 6 inhibitor discontinuation. J Cancer. 2017;8(11):2004–9.
Giridhar KV, Choong GM, Leon-Ferre R, O’Sullivan CC, Ruddy K, Haddad T, et al. Abstract P6-18-09: clinical management of metastatic breast cancer (MBC) after CDK 4/6 inhibitors: a retrospective single-institution study. Cancer Res. 2019;79:P6–18.
Article Google Scholar
Mougalian SS, Feinberg BA, Wang E, Alexis K, Chatterjee D, Knoth RL, et al. Observational study of clinical outcomes of eribulin mesylate in metastatic breast cancer after cyclin-dependent kinase 4/6 inhibitor therapy. Future Oncol. 2019;15(34):3935–44.
Moscetti LML, Riggi L, Sperduti I, Piacentini FOC, Toss A, Barbieri E, Cortesi L, Canino FMA, Zoppoli G, Frassoldati A, Schirone A, Dominici MECF. SEQUENCE OF TREATMENTS AFTER CDK4/6 THERAPY IN ADVANCED BREAST CANCER (ABC), A GOIRC MULTICENTER RETRO/ PROSPECTIVE STUDY. PRELIMINARY RESULTS IN THE RETROSPECTIVE SERIES OF 116 PATIENTS. Tumori. 2022;108(4S):80.
Menichetti AZE, Giorgi CA, Bottosso M, Leporati R, Giarratano T, Barbieri C, Ligorio F, Mioranza E, Miglietta F, Lobefaro R, Faggioni G, Falci C, Vernaci G, Di Liso E, Girardi F, Griguolo G, Vernieri C, Guarneri V, Dieci MV. CDK 4/6 INHIBITORS FOR METASTATIC BREAST CANCER: A MULTICENTER REALWORLD STUDY. Tumori. 2022;108(4S):70.
Marschner NW, Harbeck N, Thill M, Stickeler E, Zaiss M, Nusch A, et al. 232P Second-line therapies of patients with early progression under CDK4/6-inhibitor in first-line– data from the registry platform OPAL. Annals of Oncology. 2022;33:S643-S4
Gousis C, Lowe KMH, Kapiris M. V. Angelis. Beyond First Line CDK4/6 Inhibitors (CDK4/6i) and Aromatase Inhibitors (AI) in Patients with Oestrogen Receptor Positive Metastatic Breast Cancer (ERD MBC): The Guy’s Cancer Centre Experience. Clinical Oncology2022. p. e178.
Endo Y, Yoshimura A, Sawaki M, Hattori M, Kotani H, Kataoka A, et al. Time to chemotherapy for patients with estrogen receptor-positive breast Cancer and cyclin-dependent kinase 4 and 6 inhibitor use. J Breast Cancer. 2022;25(4):296–306.
Li Y, Li W, Gong C, Zheng Y, Ouyang Q, Xie N, et al. A multicenter analysis of treatment patterns and clinical outcomes of subsequent therapies after progression on palbociclib in HR+/HER2- metastatic breast cancer. Ther Adv Med Oncol. 2021;13:17588359211022890.
Amaro CP, Batra A, Lupichuk S. First-line treatment with a cyclin-dependent kinase 4/6 inhibitor plus an aromatase inhibitor for metastatic breast Cancer in Alberta. Curr Oncol. 2021;28(3):2270–80.
Crocetti SPM, Tassone L, Marcantognini G, Bastianelli L, Della Mora A, Merloni F, Cantini L, Scortichini L, Agostinelli V, Ballatore Z, Savini A, Maccaroni E. Berardi R. What is the best therapeutic sequence for ER-Positive/HER2- Negative metastatic breast cancer in the era of CDK4/6 inhibitors? A single center experience. Tumori. 2020;106(2S).
Nichetti F, Marra A, Giorgi CA, Randon G, Scagnoli S, De Angelis C, et al. 337P Efficacy of everolimus plus exemestane in CDK 4/6 inhibitors-pretreated or naïve HR-positive/HER2-negative breast cancer patients: A secondary analysis of the EVERMET study. Annals of Oncology. 2020;31:S382
Luhn P, O’Hear C, Ton T, Sanglier T, Hsieh A, Oliveri D, et al. Abstract P4-13-08: time to treatment discontinuation of second-line fulvestrant monotherapy for HR+/HER2– metastatic breast cancer in the real-world setting. Cancer Res. 2019;79(4Supplement):P4–13.
Mittal A, Molto Valiente C, Tamimi F, Schlam I, Sammons S, Tolaney SM et al. Filling the gap after CDK4/6 inhibitors: Novel Endocrine and Biologic Treatment options for metastatic hormone receptor positive breast Cancer. Cancers (Basel). 2023;15(7).
Ashai N, Swain SM. Post-CDK 4/6 inhibitor therapy: current agents and novel targets. Cancers (Basel). 2023;15(6).
Higgins JPTTJ, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editors. Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (updated February 2022). www.training.cochrane.org/handbook : Cochrane; 2022.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
Serdar CC, Cihan M, Yücel D, Serdar MA. Sample size, power and effect size revisited: simplified and practical approaches in pre-clinical, clinical and laboratory studies. Biochem Med (Zagreb). 2021;31(1):010502.
US Food Drug Administration. FDA approves elacestrant for ER-positive, HER2-negative, ESR1-mutated advanced or metastatic breast cancer [updated January 27 2023. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-elacestrant-er-positive-her2-negative-esr1-mutated-advanced-or-metastatic-breast-cancer .
US Food Drug Administration. FDA approves capivasertib with fulvestrant for breast cancer [updated November 16 2023. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-capivasertib-fulvestrant-breast-cancer .
Download references
Acknowledgements
The authors would like to acknowledge Joanna Bielecki who developed, conducted, and documented the database searches.
This study was funded by Pfizer Inc. (New York, NY, USA) and Arvinas (New Haven, CT, USA).
Author information
Sarah Kane, Belal Howidi, Bao-Ngoc Nguyen and Imtiaz A. Samjoo contributed equally to this work.
Authors and Affiliations
Pfizer, 10017, New York, NY, USA
Veronique Lambert & Yan Wu
EVERSANA, Burlington, ON, Canada
Sarah Kane, Belal Howidi, Bao-Ngoc Nguyen & Imtiaz A. Samjoo
Arvinas, 06511, New Haven, CT, USA
David Chandiwana & Michelle Edwards
You can also search for this author in PubMed Google Scholar
Contributions
VL, IAS, SK, BH, BN, DC, YW, and ME participated in the conception and design of the study. IAS, SK, BH and BN contributed to the literature review, data collection, analysis, and interpretation of the data. VL, IAS, SK, BH, BN, DC, YW, and ME contributed to the interpretation of the data and critically reviewed for the importance of intellectual content for the work. VL, IAS, SK, BH, BN, DC, YW, and ME were responsible for drafting or reviewing the manuscript and for providing final approval. VL, IAS, SK, BH, BN, DC, YW, and ME meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work, and have given their approval for this version to be published.
Corresponding author
Correspondence to Imtiaz A. Samjoo .
Ethics declarations
Ethics approval and consent to participate.
Not applicable.
Consent for publication
Competing interests.
The authors of this manuscript declare that the research presented was funded by Pfizer Inc. and Arvinas. While the support from Pfizer Inc. and Arvinas was instrumental in facilitating this research, the authors affirm that their interpretation of the data and the content of this manuscript were conducted independently and without bias to maintain the transparency and integrity of the research. IAS, SK, BH, and BN are employees of EVERSANA, Canada, which was a paid consultant to Pfizer in connection with the development of this manuscript.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary material 2, rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Lambert, V., Kane, S., Howidi, B. et al. Systematic literature review of real-world evidence for treatments in HR+/HER2- second-line LABC/mBC after first-line treatment with CDK4/6i. BMC Cancer 24 , 631 (2024). https://doi.org/10.1186/s12885-024-12269-8
Download citation
Received : 26 January 2024
Accepted : 16 April 2024
Published : 23 May 2024
DOI : https://doi.org/10.1186/s12885-024-12269-8
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- First-line CDK4/6i
ISSN: 1471-2407
- Submission enquiries: [email protected]
- General enquiries: [email protected]

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- BMC Med Res Methodol
The case study approach
Sarah crowe.
1 Division of Primary Care, The University of Nottingham, Nottingham, UK
Kathrin Cresswell
2 Centre for Population Health Sciences, The University of Edinburgh, Edinburgh, UK
Ann Robertson
3 School of Health in Social Science, The University of Edinburgh, Edinburgh, UK
Anthony Avery
Aziz sheikh.
The case study approach allows in-depth, multi-faceted explorations of complex issues in their real-life settings. The value of the case study approach is well recognised in the fields of business, law and policy, but somewhat less so in health services research. Based on our experiences of conducting several health-related case studies, we reflect on the different types of case study design, the specific research questions this approach can help answer, the data sources that tend to be used, and the particular advantages and disadvantages of employing this methodological approach. The paper concludes with key pointers to aid those designing and appraising proposals for conducting case study research, and a checklist to help readers assess the quality of case study reports.
Introduction
The case study approach is particularly useful to employ when there is a need to obtain an in-depth appreciation of an issue, event or phenomenon of interest, in its natural real-life context. Our aim in writing this piece is to provide insights into when to consider employing this approach and an overview of key methodological considerations in relation to the design, planning, analysis, interpretation and reporting of case studies.
The illustrative 'grand round', 'case report' and 'case series' have a long tradition in clinical practice and research. Presenting detailed critiques, typically of one or more patients, aims to provide insights into aspects of the clinical case and, in doing so, illustrate broader lessons that may be learnt. In research, the conceptually-related case study approach can be used, for example, to describe in detail a patient's episode of care, explore professional attitudes to and experiences of a new policy initiative or service development or more generally to 'investigate contemporary phenomena within its real-life context' [ 1 ]. Based on our experiences of conducting a range of case studies, we reflect on when to consider using this approach, discuss the key steps involved and illustrate, with examples, some of the practical challenges of attaining an in-depth understanding of a 'case' as an integrated whole. In keeping with previously published work, we acknowledge the importance of theory to underpin the design, selection, conduct and interpretation of case studies[ 2 ]. In so doing, we make passing reference to the different epistemological approaches used in case study research by key theoreticians and methodologists in this field of enquiry.
This paper is structured around the following main questions: What is a case study? What are case studies used for? How are case studies conducted? What are the potential pitfalls and how can these be avoided? We draw in particular on four of our own recently published examples of case studies (see Tables Tables1, 1 , ,2, 2 , ,3 3 and and4) 4 ) and those of others to illustrate our discussion[ 3 - 7 ].
Example of a case study investigating the reasons for differences in recruitment rates of minority ethnic people in asthma research[ 3 ]
Example of a case study investigating the process of planning and implementing a service in Primary Care Organisations[ 4 ]
Example of a case study investigating the introduction of the electronic health records[ 5 ]
Example of a case study investigating the formal and informal ways students learn about patient safety[ 6 ]
What is a case study?
A case study is a research approach that is used to generate an in-depth, multi-faceted understanding of a complex issue in its real-life context. It is an established research design that is used extensively in a wide variety of disciplines, particularly in the social sciences. A case study can be defined in a variety of ways (Table (Table5), 5 ), the central tenet being the need to explore an event or phenomenon in depth and in its natural context. It is for this reason sometimes referred to as a "naturalistic" design; this is in contrast to an "experimental" design (such as a randomised controlled trial) in which the investigator seeks to exert control over and manipulate the variable(s) of interest.
Definitions of a case study
Stake's work has been particularly influential in defining the case study approach to scientific enquiry. He has helpfully characterised three main types of case study: intrinsic , instrumental and collective [ 8 ]. An intrinsic case study is typically undertaken to learn about a unique phenomenon. The researcher should define the uniqueness of the phenomenon, which distinguishes it from all others. In contrast, the instrumental case study uses a particular case (some of which may be better than others) to gain a broader appreciation of an issue or phenomenon. The collective case study involves studying multiple cases simultaneously or sequentially in an attempt to generate a still broader appreciation of a particular issue.
These are however not necessarily mutually exclusive categories. In the first of our examples (Table (Table1), 1 ), we undertook an intrinsic case study to investigate the issue of recruitment of minority ethnic people into the specific context of asthma research studies, but it developed into a instrumental case study through seeking to understand the issue of recruitment of these marginalised populations more generally, generating a number of the findings that are potentially transferable to other disease contexts[ 3 ]. In contrast, the other three examples (see Tables Tables2, 2 , ,3 3 and and4) 4 ) employed collective case study designs to study the introduction of workforce reconfiguration in primary care, the implementation of electronic health records into hospitals, and to understand the ways in which healthcare students learn about patient safety considerations[ 4 - 6 ]. Although our study focusing on the introduction of General Practitioners with Specialist Interests (Table (Table2) 2 ) was explicitly collective in design (four contrasting primary care organisations were studied), is was also instrumental in that this particular professional group was studied as an exemplar of the more general phenomenon of workforce redesign[ 4 ].
What are case studies used for?
According to Yin, case studies can be used to explain, describe or explore events or phenomena in the everyday contexts in which they occur[ 1 ]. These can, for example, help to understand and explain causal links and pathways resulting from a new policy initiative or service development (see Tables Tables2 2 and and3, 3 , for example)[ 1 ]. In contrast to experimental designs, which seek to test a specific hypothesis through deliberately manipulating the environment (like, for example, in a randomised controlled trial giving a new drug to randomly selected individuals and then comparing outcomes with controls),[ 9 ] the case study approach lends itself well to capturing information on more explanatory ' how ', 'what' and ' why ' questions, such as ' how is the intervention being implemented and received on the ground?'. The case study approach can offer additional insights into what gaps exist in its delivery or why one implementation strategy might be chosen over another. This in turn can help develop or refine theory, as shown in our study of the teaching of patient safety in undergraduate curricula (Table (Table4 4 )[ 6 , 10 ]. Key questions to consider when selecting the most appropriate study design are whether it is desirable or indeed possible to undertake a formal experimental investigation in which individuals and/or organisations are allocated to an intervention or control arm? Or whether the wish is to obtain a more naturalistic understanding of an issue? The former is ideally studied using a controlled experimental design, whereas the latter is more appropriately studied using a case study design.
Case studies may be approached in different ways depending on the epistemological standpoint of the researcher, that is, whether they take a critical (questioning one's own and others' assumptions), interpretivist (trying to understand individual and shared social meanings) or positivist approach (orientating towards the criteria of natural sciences, such as focusing on generalisability considerations) (Table (Table6). 6 ). Whilst such a schema can be conceptually helpful, it may be appropriate to draw on more than one approach in any case study, particularly in the context of conducting health services research. Doolin has, for example, noted that in the context of undertaking interpretative case studies, researchers can usefully draw on a critical, reflective perspective which seeks to take into account the wider social and political environment that has shaped the case[ 11 ].
Example of epistemological approaches that may be used in case study research
How are case studies conducted?
Here, we focus on the main stages of research activity when planning and undertaking a case study; the crucial stages are: defining the case; selecting the case(s); collecting and analysing the data; interpreting data; and reporting the findings.
Defining the case
Carefully formulated research question(s), informed by the existing literature and a prior appreciation of the theoretical issues and setting(s), are all important in appropriately and succinctly defining the case[ 8 , 12 ]. Crucially, each case should have a pre-defined boundary which clarifies the nature and time period covered by the case study (i.e. its scope, beginning and end), the relevant social group, organisation or geographical area of interest to the investigator, the types of evidence to be collected, and the priorities for data collection and analysis (see Table Table7 7 )[ 1 ]. A theory driven approach to defining the case may help generate knowledge that is potentially transferable to a range of clinical contexts and behaviours; using theory is also likely to result in a more informed appreciation of, for example, how and why interventions have succeeded or failed[ 13 ].
Example of a checklist for rating a case study proposal[ 8 ]
For example, in our evaluation of the introduction of electronic health records in English hospitals (Table (Table3), 3 ), we defined our cases as the NHS Trusts that were receiving the new technology[ 5 ]. Our focus was on how the technology was being implemented. However, if the primary research interest had been on the social and organisational dimensions of implementation, we might have defined our case differently as a grouping of healthcare professionals (e.g. doctors and/or nurses). The precise beginning and end of the case may however prove difficult to define. Pursuing this same example, when does the process of implementation and adoption of an electronic health record system really begin or end? Such judgements will inevitably be influenced by a range of factors, including the research question, theory of interest, the scope and richness of the gathered data and the resources available to the research team.
Selecting the case(s)
The decision on how to select the case(s) to study is a very important one that merits some reflection. In an intrinsic case study, the case is selected on its own merits[ 8 ]. The case is selected not because it is representative of other cases, but because of its uniqueness, which is of genuine interest to the researchers. This was, for example, the case in our study of the recruitment of minority ethnic participants into asthma research (Table (Table1) 1 ) as our earlier work had demonstrated the marginalisation of minority ethnic people with asthma, despite evidence of disproportionate asthma morbidity[ 14 , 15 ]. In another example of an intrinsic case study, Hellstrom et al.[ 16 ] studied an elderly married couple living with dementia to explore how dementia had impacted on their understanding of home, their everyday life and their relationships.
For an instrumental case study, selecting a "typical" case can work well[ 8 ]. In contrast to the intrinsic case study, the particular case which is chosen is of less importance than selecting a case that allows the researcher to investigate an issue or phenomenon. For example, in order to gain an understanding of doctors' responses to health policy initiatives, Som undertook an instrumental case study interviewing clinicians who had a range of responsibilities for clinical governance in one NHS acute hospital trust[ 17 ]. Sampling a "deviant" or "atypical" case may however prove even more informative, potentially enabling the researcher to identify causal processes, generate hypotheses and develop theory.
In collective or multiple case studies, a number of cases are carefully selected. This offers the advantage of allowing comparisons to be made across several cases and/or replication. Choosing a "typical" case may enable the findings to be generalised to theory (i.e. analytical generalisation) or to test theory by replicating the findings in a second or even a third case (i.e. replication logic)[ 1 ]. Yin suggests two or three literal replications (i.e. predicting similar results) if the theory is straightforward and five or more if the theory is more subtle. However, critics might argue that selecting 'cases' in this way is insufficiently reflexive and ill-suited to the complexities of contemporary healthcare organisations.
The selected case study site(s) should allow the research team access to the group of individuals, the organisation, the processes or whatever else constitutes the chosen unit of analysis for the study. Access is therefore a central consideration; the researcher needs to come to know the case study site(s) well and to work cooperatively with them. Selected cases need to be not only interesting but also hospitable to the inquiry [ 8 ] if they are to be informative and answer the research question(s). Case study sites may also be pre-selected for the researcher, with decisions being influenced by key stakeholders. For example, our selection of case study sites in the evaluation of the implementation and adoption of electronic health record systems (see Table Table3) 3 ) was heavily influenced by NHS Connecting for Health, the government agency that was responsible for overseeing the National Programme for Information Technology (NPfIT)[ 5 ]. This prominent stakeholder had already selected the NHS sites (through a competitive bidding process) to be early adopters of the electronic health record systems and had negotiated contracts that detailed the deployment timelines.
It is also important to consider in advance the likely burden and risks associated with participation for those who (or the site(s) which) comprise the case study. Of particular importance is the obligation for the researcher to think through the ethical implications of the study (e.g. the risk of inadvertently breaching anonymity or confidentiality) and to ensure that potential participants/participating sites are provided with sufficient information to make an informed choice about joining the study. The outcome of providing this information might be that the emotive burden associated with participation, or the organisational disruption associated with supporting the fieldwork, is considered so high that the individuals or sites decide against participation.
In our example of evaluating implementations of electronic health record systems, given the restricted number of early adopter sites available to us, we sought purposively to select a diverse range of implementation cases among those that were available[ 5 ]. We chose a mixture of teaching, non-teaching and Foundation Trust hospitals, and examples of each of the three electronic health record systems procured centrally by the NPfIT. At one recruited site, it quickly became apparent that access was problematic because of competing demands on that organisation. Recognising the importance of full access and co-operative working for generating rich data, the research team decided not to pursue work at that site and instead to focus on other recruited sites.
Collecting the data
In order to develop a thorough understanding of the case, the case study approach usually involves the collection of multiple sources of evidence, using a range of quantitative (e.g. questionnaires, audits and analysis of routinely collected healthcare data) and more commonly qualitative techniques (e.g. interviews, focus groups and observations). The use of multiple sources of data (data triangulation) has been advocated as a way of increasing the internal validity of a study (i.e. the extent to which the method is appropriate to answer the research question)[ 8 , 18 - 21 ]. An underlying assumption is that data collected in different ways should lead to similar conclusions, and approaching the same issue from different angles can help develop a holistic picture of the phenomenon (Table (Table2 2 )[ 4 ].
Brazier and colleagues used a mixed-methods case study approach to investigate the impact of a cancer care programme[ 22 ]. Here, quantitative measures were collected with questionnaires before, and five months after, the start of the intervention which did not yield any statistically significant results. Qualitative interviews with patients however helped provide an insight into potentially beneficial process-related aspects of the programme, such as greater, perceived patient involvement in care. The authors reported how this case study approach provided a number of contextual factors likely to influence the effectiveness of the intervention and which were not likely to have been obtained from quantitative methods alone.
In collective or multiple case studies, data collection needs to be flexible enough to allow a detailed description of each individual case to be developed (e.g. the nature of different cancer care programmes), before considering the emerging similarities and differences in cross-case comparisons (e.g. to explore why one programme is more effective than another). It is important that data sources from different cases are, where possible, broadly comparable for this purpose even though they may vary in nature and depth.
Analysing, interpreting and reporting case studies
Making sense and offering a coherent interpretation of the typically disparate sources of data (whether qualitative alone or together with quantitative) is far from straightforward. Repeated reviewing and sorting of the voluminous and detail-rich data are integral to the process of analysis. In collective case studies, it is helpful to analyse data relating to the individual component cases first, before making comparisons across cases. Attention needs to be paid to variations within each case and, where relevant, the relationship between different causes, effects and outcomes[ 23 ]. Data will need to be organised and coded to allow the key issues, both derived from the literature and emerging from the dataset, to be easily retrieved at a later stage. An initial coding frame can help capture these issues and can be applied systematically to the whole dataset with the aid of a qualitative data analysis software package.
The Framework approach is a practical approach, comprising of five stages (familiarisation; identifying a thematic framework; indexing; charting; mapping and interpretation) , to managing and analysing large datasets particularly if time is limited, as was the case in our study of recruitment of South Asians into asthma research (Table (Table1 1 )[ 3 , 24 ]. Theoretical frameworks may also play an important role in integrating different sources of data and examining emerging themes. For example, we drew on a socio-technical framework to help explain the connections between different elements - technology; people; and the organisational settings within which they worked - in our study of the introduction of electronic health record systems (Table (Table3 3 )[ 5 ]. Our study of patient safety in undergraduate curricula drew on an evaluation-based approach to design and analysis, which emphasised the importance of the academic, organisational and practice contexts through which students learn (Table (Table4 4 )[ 6 ].
Case study findings can have implications both for theory development and theory testing. They may establish, strengthen or weaken historical explanations of a case and, in certain circumstances, allow theoretical (as opposed to statistical) generalisation beyond the particular cases studied[ 12 ]. These theoretical lenses should not, however, constitute a strait-jacket and the cases should not be "forced to fit" the particular theoretical framework that is being employed.
When reporting findings, it is important to provide the reader with enough contextual information to understand the processes that were followed and how the conclusions were reached. In a collective case study, researchers may choose to present the findings from individual cases separately before amalgamating across cases. Care must be taken to ensure the anonymity of both case sites and individual participants (if agreed in advance) by allocating appropriate codes or withholding descriptors. In the example given in Table Table3, 3 , we decided against providing detailed information on the NHS sites and individual participants in order to avoid the risk of inadvertent disclosure of identities[ 5 , 25 ].
What are the potential pitfalls and how can these be avoided?
The case study approach is, as with all research, not without its limitations. When investigating the formal and informal ways undergraduate students learn about patient safety (Table (Table4), 4 ), for example, we rapidly accumulated a large quantity of data. The volume of data, together with the time restrictions in place, impacted on the depth of analysis that was possible within the available resources. This highlights a more general point of the importance of avoiding the temptation to collect as much data as possible; adequate time also needs to be set aside for data analysis and interpretation of what are often highly complex datasets.
Case study research has sometimes been criticised for lacking scientific rigour and providing little basis for generalisation (i.e. producing findings that may be transferable to other settings)[ 1 ]. There are several ways to address these concerns, including: the use of theoretical sampling (i.e. drawing on a particular conceptual framework); respondent validation (i.e. participants checking emerging findings and the researcher's interpretation, and providing an opinion as to whether they feel these are accurate); and transparency throughout the research process (see Table Table8 8 )[ 8 , 18 - 21 , 23 , 26 ]. Transparency can be achieved by describing in detail the steps involved in case selection, data collection, the reasons for the particular methods chosen, and the researcher's background and level of involvement (i.e. being explicit about how the researcher has influenced data collection and interpretation). Seeking potential, alternative explanations, and being explicit about how interpretations and conclusions were reached, help readers to judge the trustworthiness of the case study report. Stake provides a critique checklist for a case study report (Table (Table9 9 )[ 8 ].
Potential pitfalls and mitigating actions when undertaking case study research
Stake's checklist for assessing the quality of a case study report[ 8 ]
Conclusions
The case study approach allows, amongst other things, critical events, interventions, policy developments and programme-based service reforms to be studied in detail in a real-life context. It should therefore be considered when an experimental design is either inappropriate to answer the research questions posed or impossible to undertake. Considering the frequency with which implementations of innovations are now taking place in healthcare settings and how well the case study approach lends itself to in-depth, complex health service research, we believe this approach should be more widely considered by researchers. Though inherently challenging, the research case study can, if carefully conceptualised and thoughtfully undertaken and reported, yield powerful insights into many important aspects of health and healthcare delivery.
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
AS conceived this article. SC, KC and AR wrote this paper with GH, AA and AS all commenting on various drafts. SC and AS are guarantors.
Pre-publication history
The pre-publication history for this paper can be accessed here:
http://www.biomedcentral.com/1471-2288/11/100/prepub
Acknowledgements
We are grateful to the participants and colleagues who contributed to the individual case studies that we have drawn on. This work received no direct funding, but it has been informed by projects funded by Asthma UK, the NHS Service Delivery Organisation, NHS Connecting for Health Evaluation Programme, and Patient Safety Research Portfolio. We would also like to thank the expert reviewers for their insightful and constructive feedback. Our thanks are also due to Dr. Allison Worth who commented on an earlier draft of this manuscript.
- Yin RK. Case study research, design and method. 4. London: Sage Publications Ltd.; 2009. [ Google Scholar ]
- Keen J, Packwood T. Qualitative research; case study evaluation. BMJ. 1995; 311 :444–446. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Sheikh A, Halani L, Bhopal R, Netuveli G, Partridge M, Car J. et al. Facilitating the Recruitment of Minority Ethnic People into Research: Qualitative Case Study of South Asians and Asthma. PLoS Med. 2009; 6 (10):1–11. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Pinnock H, Huby G, Powell A, Kielmann T, Price D, Williams S, The process of planning, development and implementation of a General Practitioner with a Special Interest service in Primary Care Organisations in England and Wales: a comparative prospective case study. Report for the National Co-ordinating Centre for NHS Service Delivery and Organisation R&D (NCCSDO) 2008. http://www.sdo.nihr.ac.uk/files/project/99-final-report.pdf
- Robertson A, Cresswell K, Takian A, Petrakaki D, Crowe S, Cornford T. et al. Prospective evaluation of the implementation and adoption of NHS Connecting for Health's national electronic health record in secondary care in England: interim findings. BMJ. 2010; 41 :c4564. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Pearson P, Steven A, Howe A, Sheikh A, Ashcroft D, Smith P. the Patient Safety Education Study Group. Learning about patient safety: organisational context and culture in the education of healthcare professionals. J Health Serv Res Policy. 2010; 15 :4–10. doi: 10.1258/jhsrp.2009.009052. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- van Harten WH, Casparie TF, Fisscher OA. The evaluation of the introduction of a quality management system: a process-oriented case study in a large rehabilitation hospital. Health Policy. 2002; 60 (1):17–37. doi: 10.1016/S0168-8510(01)00187-7. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Stake RE. The art of case study research. London: Sage Publications Ltd.; 1995. [ Google Scholar ]
- Sheikh A, Smeeth L, Ashcroft R. Randomised controlled trials in primary care: scope and application. Br J Gen Pract. 2002; 52 (482):746–51. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- King G, Keohane R, Verba S. Designing Social Inquiry. Princeton: Princeton University Press; 1996. [ Google Scholar ]
- Doolin B. Information technology as disciplinary technology: being critical in interpretative research on information systems. Journal of Information Technology. 1998; 13 :301–311. doi: 10.1057/jit.1998.8. [ CrossRef ] [ Google Scholar ]
- George AL, Bennett A. Case studies and theory development in the social sciences. Cambridge, MA: MIT Press; 2005. [ Google Scholar ]
- Eccles M. the Improved Clinical Effectiveness through Behavioural Research Group (ICEBeRG) Designing theoretically-informed implementation interventions. Implementation Science. 2006; 1 :1–8. doi: 10.1186/1748-5908-1-1. [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Netuveli G, Hurwitz B, Levy M, Fletcher M, Barnes G, Durham SR, Sheikh A. Ethnic variations in UK asthma frequency, morbidity, and health-service use: a systematic review and meta-analysis. Lancet. 2005; 365 (9456):312–7. [ PubMed ] [ Google Scholar ]
- Sheikh A, Panesar SS, Lasserson T, Netuveli G. Recruitment of ethnic minorities to asthma studies. Thorax. 2004; 59 (7):634. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Hellström I, Nolan M, Lundh U. 'We do things together': A case study of 'couplehood' in dementia. Dementia. 2005; 4 :7–22. doi: 10.1177/1471301205049188. [ CrossRef ] [ Google Scholar ]
- Som CV. Nothing seems to have changed, nothing seems to be changing and perhaps nothing will change in the NHS: doctors' response to clinical governance. International Journal of Public Sector Management. 2005; 18 :463–477. doi: 10.1108/09513550510608903. [ CrossRef ] [ Google Scholar ]
- Lincoln Y, Guba E. Naturalistic inquiry. Newbury Park: Sage Publications; 1985. [ Google Scholar ]
- Barbour RS. Checklists for improving rigour in qualitative research: a case of the tail wagging the dog? BMJ. 2001; 322 :1115–1117. doi: 10.1136/bmj.322.7294.1115. [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Mays N, Pope C. Qualitative research in health care: Assessing quality in qualitative research. BMJ. 2000; 320 :50–52. doi: 10.1136/bmj.320.7226.50. [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Mason J. Qualitative researching. London: Sage; 2002. [ Google Scholar ]
- Brazier A, Cooke K, Moravan V. Using Mixed Methods for Evaluating an Integrative Approach to Cancer Care: A Case Study. Integr Cancer Ther. 2008; 7 :5–17. doi: 10.1177/1534735407313395. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Miles MB, Huberman M. Qualitative data analysis: an expanded sourcebook. 2. CA: Sage Publications Inc.; 1994. [ Google Scholar ]
- Pope C, Ziebland S, Mays N. Analysing qualitative data. Qualitative research in health care. BMJ. 2000; 320 :114–116. doi: 10.1136/bmj.320.7227.114. [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Cresswell KM, Worth A, Sheikh A. Actor-Network Theory and its role in understanding the implementation of information technology developments in healthcare. BMC Med Inform Decis Mak. 2010; 10 (1):67. doi: 10.1186/1472-6947-10-67. [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Malterud K. Qualitative research: standards, challenges, and guidelines. Lancet. 2001; 358 :483–488. doi: 10.1016/S0140-6736(01)05627-6. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Yin R. Case study research: design and methods. 2. Thousand Oaks, CA: Sage Publishing; 1994. [ Google Scholar ]
- Yin R. Enhancing the quality of case studies in health services research. Health Serv Res. 1999; 34 :1209–1224. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Green J, Thorogood N. Qualitative methods for health research. 2. Los Angeles: Sage; 2009. [ Google Scholar ]
- Howcroft D, Trauth E. Handbook of Critical Information Systems Research, Theory and Application. Cheltenham, UK: Northampton, MA, USA: Edward Elgar; 2005. [ Google Scholar ]
- Blakie N. Approaches to Social Enquiry. Cambridge: Polity Press; 1993. [ Google Scholar ]
- Doolin B. Power and resistance in the implementation of a medical management information system. Info Systems J. 2004; 14 :343–362. doi: 10.1111/j.1365-2575.2004.00176.x. [ CrossRef ] [ Google Scholar ]
- Bloomfield BP, Best A. Management consultants: systems development, power and the translation of problems. Sociological Review. 1992; 40 :533–560. [ Google Scholar ]
- Shanks G, Parr A. Proceedings of the European Conference on Information Systems. Naples; 2003. Positivist, single case study research in information systems: A critical analysis. [ Google Scholar ]
- Open access
- Published: 24 May 2024
Integration of case-based learning and three-dimensional printing for tetralogy of fallot instruction in clinical medical undergraduates: a randomized controlled trial
- Jian Zhao 1 na1 ,
- Xin Gong 1 na1 ,
- Jian Ding 1 ,
- Kepin Xiong 2 ,
- Kangle Zhuang 3 ,
- Rui Huang 1 ,
- Shu Li 4 &
- Huachun Miao 1
BMC Medical Education volume 24 , Article number: 571 ( 2024 ) Cite this article
65 Accesses
Metrics details
Case-based learning (CBL) methods have gained prominence in medical education, proving especially effective for preclinical training in undergraduate medical education. Tetralogy of Fallot (TOF) is a congenital heart disease characterized by four malformations, presenting a challenge in medical education due to the complexity of its anatomical pathology. Three-dimensional printing (3DP), generating physical replicas from data, offers a valuable tool for illustrating intricate anatomical structures and spatial relationships in the classroom. This study explores the integration of 3DP with CBL teaching for clinical medical undergraduates.
Sixty senior clinical medical undergraduates were randomly assigned to the CBL group and the CBL-3DP group. Computed tomography imaging data from a typical TOF case were exported, processed, and utilized to create four TOF models with a color 3D printer. The CBL group employed CBL teaching methods, while the CBL-3DP group combined CBL with 3D-printed models. Post-class exams and questionnaires assessed the teaching effectiveness of both groups.
The CBL-3DP group exhibited improved performance in post-class examinations, particularly in pathological anatomy and TOF imaging data analysis ( P < 0.05). Questionnaire responses from the CBL-3DP group indicated enhanced satisfaction with teaching mode, promotion of diagnostic skills, bolstering of self-assurance in managing TOF cases, and cultivation of critical thinking and clinical reasoning abilities ( P < 0.05). These findings underscore the potential of 3D printed models to augment the effectiveness of CBL, aiding students in mastering instructional content and bolstering their interest and self-confidence in learning.
The fusion of CBL with 3D printing models is feasible and effective in TOF instruction to clinical medical undergraduates, and worthy of popularization and application in medical education, especially for courses involving intricate anatomical components.
Peer Review reports
Tetralogy of Fallot (TOF) is the most common cyanotic congenital heart disease(CHD) [ 1 ]. Characterized by four structural anomalies: ventricular septal defect (VSD), pulmonary stenosis (PS), right ventricular hypertrophy (RVH), and overriding aorta (OA), TOF is a focal point and challenge in medical education. Understanding anatomical spatial structures is pivotal for learning and mastering TOF [ 2 ]. Given the constraints of course duration, medical school educators aim to provide students with a comprehensive and intuitive understanding of the disease within a limited timeframe [ 3 ].
The case-based learning (CBL) teaching model incorporates a case-based instructional approach that emphasizes typical clinical cases as a guide in student-centered and teacher-facilitated group discussions [ 4 ]. The CBL instructional methods have garnered widespread attention in medical education as they are particularly appropriate for preclinical training in undergraduate medical education [ 5 , 6 ]. The collection of case data, including medical records and examination results, is essential for case construction [ 7 ]. The anatomical and hemodynamic consequences of TOF can be determined using ultrasonography, computed tomography (CT), and magnetic resonance imaging techniques. However, understanding the anatomical structures from imaging data is a slow and challenging psychological reconstruction process for undergraduate medical students [ 8 ]. Three-dimensional (3D) visualization is valuable for depicting anatomical structures [ 9 ]. 3D printing (3DP), which creates physical replicas based on data, facilitates the demonstration of complex anatomical structures and spatial relationships in the classroom [ 10 ].
During the classroom session, 3D-printed models offer a convenient means for hands-on demonstration and communication, similar to facing a patient, enhancing the efficiency and specificity of intra-team communication and discussion [ 11 ]. In this study, we printed TOF models based on case imaging data, integrated them into CBL teaching, and assessed the effectiveness of classroom instruction.
Research participants
The study employed a prospective, randomized controlled design which received approval from the institutional ethics committee. Senior undergraduate students majoring in clinical medicine at Wannan Medical College were recruited for participation based on predefined inclusion criteria. The researchers implemented recruitment according to the recruitment criteria by contacting the class leaders of the target classes they had previously taught. Notably, these students were in their third year of medical education, with anticipation of progressing to clinical courses in the fourth year, encompassing Internal Medicine, Surgery, Obstetrics, Gynecology, and Pediatrics. Inclusion criteria for participants encompassed the following: (1) proficient communication and comprehension abilities, (2) consistent attendance without absenteeism or truancy, (3) absence of failing grades in prior examinations, and (4) capability to conscientiously fulfill assigned learning tasks. Exclusion criteria were (1) absence from lectures, (2) failure to complete pre-and post-tests, and (3) inadequate completion of questionnaires. For their participation in the study, Students were provided access to the e-book “Localized Anatomy,” authored by the investigators, as an incentive for their participation. Voluntary and anonymous participation was emphasized, with participants retaining the right to withdraw from the study at any time without providing a reason.
The study was conducted between May 1st, 2023, and June 30, 2023, from recruitment to completion of data collection. Drawing upon insights gained from a previous analogous investigation which yielded an effect size of 0.95 [ 10 ]. Sample size was computed, guided by a statistical consultant, with the aim of 0.85 power value, predicated on an effect size of 0.8 and a margin of error set at 0.05. A minimum of 30 participants per group was calculated using G*Power software (latest ver. 3.1.9.7; Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany), resulting in the recruitment of a total of 60 undergraduate students. Each participant was assigned an identification number, with codes placed in boxes. Codes drawn from the boxes determined allocation to either the CBL group or the CBL-3DP group. Subsequently, participants were randomly assigned to either the CBL group, receiving instruction utilizing the CBL methodology, or the CBL-3DP group, which received instruction integrating both CBL and 3D Printed models.
Printing of TOF models
Figure 1 A shows the printing flowchart of the TOF models. A typical TOF case was collected from the Yijishan Hospital of Wannan Medical College. The CT angiography imaging data of the case was exported. Mimics Research 20.0 software (Mimics Innovation Suite version 20, Materialize, Belgium) was used for data processing. The cardiovascular module of the CT-Heart tool was employed to adjust the threshold range, independently obtain the cardiac chambers and vessels, post-process the chambers and vessels to generate a hollow blood pool, and merge it with the myocardial volume to construct a complete heart model. The file was imported into Magics 24.0 software (version 24.0; Materialize, Belgium) for correction using the Shell tool page. After repairs, the model entered the smoothing page, where tools such as triangular surface simplification, local smoothing, refinement and smoothing, subdivision of components, and mesh painting were utilized to achieve varying degrees of smoothness. Finally, optimized data were obtained and exported as stereolithography (STL) files. An experienced cardiothoracic surgeon validated the anatomical accuracy of the digital model.
The STL files were imported into a 3D printer (J401Pro; Sailner 3D Technology, China) for model printing. This printer can produce full-color medical models using different materials. The models were fabricated using two distinct materials: rigid and flexible. Both materials are suitable for the observational discussion of the teaching objectives outlined in our study. From the perspective of observing pathological changes in the TOF, there is no significant difference between the two materials.

Experimental flow chart of this study. A TOF model printing flow chart. B The instructional framework
Teaching implementation
Figure 1 B illustrates the instructional framework employed in this study. One week preceding the class session, all the students were tasked with a 30-minute self-study session, focusing on the theoretical content related to TOF as outlined in the Pediatrics and Surgery textbooks, along with a review of pertinent academic literature. Both groups received co-supervision from two basic medicine lecturers boasting over a decade of teaching experience, alongside a senior cardiothoracic surgeon. Teaching conditions remained consistent across groups, encompassing uniform assessment criteria and adherence to predefined teaching time frames, all conducted in a Project-Based Learning (PBL) classroom at Wannan Medical College. Additionally, a pre-course examination was administered to gauge students’ preparedness for self-study.
In adherence to the curriculum guidelines, the teaching objectives aimed to empower students to master TOF’s clinical manifestations, diagnostic modalities, and differential diagnoses, while acquainting them with treatment principles and surgical methodologies. Additionally, the objectives sought to cultivate students’ clinical reasoning abilities and problem-solving skills. the duration of instruction for the TOF theory session was standardized to 25 min. The didactic content was integrated with the TOF case study to construct a coherent pedagogical structure.
During the instructional session, both groups underwent teaching utilizing the CBL methodology. Clinical manifestations and case details of TOF cases were presented to stimulate students’ interest and curiosity. Subsequently, the theory of TOF, including its etiology, pathogenesis, pathologic anatomy, clinical manifestations, diagnostic methods, and therapeutic interventions, was briefly elucidated. Emphasis was then placed on the case, wherein selected typical TOF cases were explained, guiding students in analysis and discussion. Students were organized into four teams under the instructors’ supervision, fostering cooperative learning and communication, thereby deepening their understanding of the disease through continuous inquiry and exploration (Fig. 2 L). In the routinely equipped PBL classroom with standard heart models (Fig. 2 J, K), all students had prior exposure to human anatomy and were familiar with these models. Both groups were provided with four standard heart models for reference, while the CBL-3DP group received additional four 3D-printed models depicting TOF anomalies, enriching their learning experience (Fig. 2 D, G). After the lesson, summarization, and feedback sessions were conducted to consolidate group discussions’ outcomes, evaluate teaching effectiveness, and assess learning outcomes.

Heart models utilized in instructional sessions. A External perspective of 3D digital models. B, C Cross-sectional views following trans-septal sagittal dissection of the 3D digital model (PS: Pulmonary Stenosis; OA: Overriding Aorta; VSD: Ventricular Septal Defect; RVH: Right Ventricular Hypertrophy). D External depiction of rigid 3D printed model. E, F Sagittal sections of the rigid 3D printed model. G External portrayal of flexible 3D printed model. H, I Sagittal sections of the flexible 3D printed model. J, K The normal heart model employed in the instruction of the CBL group. L Ongoing classroom session
Teaching effectiveness assessment
Following the instructional session, participants from the two groups underwent a theoretical examination to assess their comprehension of the taught material. This assessment covered domains such as pathological anatomy, clinical manifestations, imaging data interpretation, diagnosis, and treatment relevant to TOF. Additionally, structured questionnaires were administered to evaluate the efficacy of the pedagogical approach employed. The questionnaire consisted of six questions designed to gauge participants’ understanding of the teaching content, enhancement of diagnostic skills, cultivation of critical thinking and clinical reasoning abilities, bolstering of confidence in managing TOF cases, satisfaction with the teaching mode, and satisfaction with the CBL methodology.
The questionnaire employed a 5-point Likert scale to gauge responses, with 5 indicating “strongly satisfied/agree,” 4 for “satisfied/agree,” 3 denoting “neutral,” 2 reflecting “dissatisfied/disagree,” and 1 indicating “strongly dissatisfied/disagree.” It comprised six questions, with the initial two probing participants’ knowledge acquisition, questions 3 and 4 exploring satisfaction regarding enhanced competence, and the final two assessing satisfaction with teaching methods and modes. Additionally, participants were encouraged to provide suggestions at the end of the questionnaire. To ensure the questionnaire’s validity, five esteemed lecturers in basic medical sciences with more than 10 years of experience verified its content and assessed its Content Validity Ratio and Content Validity Index to ensure alignment with the study’s objectives.
Statistical analysis
Statistical analyses were conducted utilizing GraphPad Prism 9.0 software. Aggregate score data for both groups were presented as mean ± standard deviation (x ± s). The gender comparisons were analyzed with the chi-square (χ2) test, while the other variables were compared using the Mann-Whitney U test. The threshold for determining statistical significance was set at P < 0.05.
Three-dimensional printing models
After configuring the structural colors of each component (Fig. 2 A, B, C), we printed four color TOF models using both rigid and flexible materials, resulting in four life-sized TOF models. Two color TOF models were created using rigid materials (Fig. 2 D, E, F). These models, exhibiting resistance to deformation, and with a firm texture, smooth and glossy surface, and good transparency, allowing visibility of the internal structures, were deemed conducive to teaching and observation. We also fabricated two color TOF models using flexible materials (Fig. 2 G, H, I), characterized by soft texture, opacity, and deformability, allowing for easy manipulation and cutting. It has potential utility beyond observational purposes. It can serve as a valuable tool for simulating surgical interventions and may be employed to create tomographic anatomical specimens. In this study, both material models were suitable for observation in the classroom. The participants were able to discern the four pathological changes characteristic of TOF from surface examination or cross-sectional analysis.
Baseline characteristics of the students
In total, 60 students were included in this study. The CBL group comprised 30 students (14 males and 16 females), with an average age of (21.20 ± 0.76) years. The CBL-3DP group consisted of 30 students (17 males and 13 females) with an average age of 20.96 years. All the students completed the study procedures. There were no significant differences in age, sex ratio, or pre-class exam scores between the two groups ( P > 0.05), indicating that the baseline scores between the two groups were comparable (Table 1 ).
Theoretical examination results
All students completed the research procedures as planned. The post-class theoretical examination encompassed assessment of pathological anatomy, clinical presentations, imaging data interpretation, diagnosis, and treatment pertinent to TOF. Notably, no statistically significant disparities were observed in the scores on clinical manifestations, diagnosis and treatment components between the cohorts, as delineated in Table 2 . Conversely, discernible distinctions were evident whereby the CBL-3DP group outperformed the CBL group notably in pathological anatomy, imaging data interpretation, and overall aggregate scores ( P < 0.05).
Results of the questionnaires
All the 60 participants submitted the questionnaire. Comparing the CBL and CBL-3DP groups, the scores from the CBL-3DP group showed significant improvements in many areas. This included satisfaction with the teaching mode, promotion of diagnostic skills, bolstering of self-assurance in managing TOF cases, and cultivation of critical thinking and clinical reasoning abilities (Fig. 3 B, C, D, E). All of which improved significantly ( P < 0.05 for the first aspects and P < 0.01 for the rest). However, the two groups were not comparable ( P > 0.05) in terms of understanding of the teaching content and Satisfaction with the CBL methodology (Fig. 3 A, F).
Upon completion of the questionnaires, participants were invited to proffer recommendations. Notably, in the CBL group, seven students expressed challenges in comprehending TOF and indicated a need for additional time for consolidation to enhance understanding. Conversely, within the CBL-3DP group, twelve students advocated for the augmentation of model repertoire and the expansion of disease-related data collection to bolster pedagogical efficacy across other didactic domains.

Five-point Likert scores of students’ attitudes in CBL ( n = 30) and CBL-3DP ( n = 30) groups. A Understanding of teaching content. B Promotion of diagnostic skills. C Cultivation of critical thinking and clinical reasoning abilities. D Bolstering of self-assurance in managing TOF cases. E Satisfaction with the teaching mode. F Satisfaction with the CBL methodology. ns No significant difference, * p < 0.05, ** p < 0.01, *** p < 0.001
TOF presents a significant challenge in clinical practice, necessitating a comprehensive understanding for effective diagnosis and treatment [ 12 ]. Traditional teaching methods in medical schools have relied on conventional resources such as textbooks, 2D illustrations, cadaver dissections, and radiographic materials to impart knowledge about complex conditions like TOF [ 13 ]. However, the limitations of these methods in fully engaging students and bridging the gap between theoretical knowledge and practical application have prompted a need for innovative instructional approaches.
CBL has emerged as a valuable tool in medical education, offering students opportunities to engage with authentic clinical cases through group discussions and inquiry-based learning [ 14 ]. By actively involving students in problem-solving and decision-making processes, CBL facilitates the application of theoretical knowledge to real-world scenarios, thus better-preparing students for future clinical practice [ 15 ]. Our investigation revealed that both groups of students exhibited comparable levels of satisfaction with the CBL methodology, devoid of discernible disparities.
CHD presents a formidable challenge due to the intricate nature of anatomical anomalies, the diverse spectrum of conditions, and individual variations [ 16 ]. Utilizing 3D-printed physical models, derived from patient imaging data, can significantly enhance comprehension of complex anatomical structures [ 17 ]. These models have proven invaluable in guiding surgical planning, providing training for junior or inexperienced pediatric residents, and educating healthcare professionals and parents of patients [ 18 ]. Studies indicate that as much as 50% of pediatric surgical decisions can be influenced by the insights gained from 3D printed models [ 19 ]. By providing tangible, anatomically accurate models, 3D printing offers a unique opportunity for people to visualize complex structures and enhance their understanding of anatomical intricacies. Our study utilized full-color, to-scale 3D printed models to illustrate the structural abnormalities associated with TOF, thereby enriching classroom sessions and facilitating a deeper comprehension of the condition.
Comparative analysis between the CBL-3DP group and the CBL group revealed significant improvements in post-test performance, particularly in pathological anatomy and imaging data interpretation. Additionally, questionnaire responses indicated higher levels of satisfaction and confidence among students in the CBL-3DP group, highlighting the positive impact of incorporating 3D printed models into the learning environment, improving the effectiveness of CBL classroom instruction. Despite the merits, our study has limitations. Primarily, participants were exclusively drawn from the same grade level within a single college, possibly engendering bias owing to shared learning backgrounds. Future research could further strengthen these findings by expanding the sample size and including long-term follow-up to assess the retention of knowledge and skills. Additionally, the influence of the 3D models depicting a normal heart on the learning process and its potential to introduce bias into the results warrants consideration, highlighting a need for scrutiny in subsequent studies.
As medical science continues to advance, the need for effective teaching methods becomes increasingly paramount. Our study underscores the potential of combining active learning approaches like CBL with innovative technologies such as 3D printing to enhance teaching effectiveness, improve knowledge acquisition, and foster students’ confidence and enthusiasm in pursuing clinical careers. Moving forward, further research and integration of such methodologies are essential for meeting the evolving demands of medical education, especially in areas involving complex anatomical understanding.
Conclusions
Integrating 3D-printed models with the CBL method is feasible and effective in TOF instruction. The demonstrated success of this method warrants broad implementation in medical education, particularly for complex anatomical topics.
Data availability
All data supporting the conclusions of this research are available upon reasonable request from the corresponding author.
Apitz C, Webb GD, Redington AN. Tetralogy of Fallot. Lancet. 2009;374:1462–71.
Article Google Scholar
Ghosh RM, Jolley MA, Mascio CE, Chen JM, Fuller S, Rome JJ, et al. Clinical 3D modeling to guide pediatric cardiothoracic surgery and intervention using 3D printed anatomic models, computer aided design and virtual reality. 3D Print Med. 2022;8:11.
Chakrabarti R, Wardle K, Wright T, Bennie T, Gishen F. Approaching an undergraduate medical curriculum map: challenges and expectations. BMC Med Educ. 2021;21:341.
Donkin R, Yule H, Fyfe T. Online case-based learning in medical education: a scoping review. BMC Med Educ. 2023;23:564.
Novack JP. Designing cases for case-based immunology teaching in large medical school classes. Front Immunol. 2020;11:995.
Chen HC, Van Den Broek WES, Ten Cate O. The case for use of entrustable professional activities in undergraduate medical education. Acad Med. 2015;90:431–6.
Wang M, Sun Z, Jia M, Wang Y, Wang H, Zhu X, et al. Intelligent virtual case learning system based on real medical records and natural language processing. BMC Med Inf Decis Mak. 2022;22:60.
Yoo S-J, Thabit O, Kim EK, Ide H, Yim D, Dragulescu A, et al. 3D printing in medicine of congenital heart diseases. 3D Print Med. 2015;2:3.
Yammine K, Violato C. A meta-analysis of the educational effectiveness of three-dimensional visualization technologies in teaching anatomy. Anat Sci Educ. 2015;8:525–38.
Miao H, Ding J, Gong X, Zhao J, Li H, Xiong K, et al. Application of 3D-printed pulmonary segment specimens in experimental teaching of sectional anatomy. BMC Surg. 2023;23:109.
Sun Z, Wong YH, Yeong CH. Patient-specific 3D-printed low-cost models in medical education and clinical practice. Micromachines (Basel). 2023;14:464.
Downing TE, Kim YY. Tetralogy of Fallot: general principles of management. Cardiol Clin. 2015;33:531–41. vii–viii.
Jia X, Zeng W, Zhang Q. Combined administration of problem- and lecture-based learning teaching models in medical education in China: a meta-analysis of randomized controlled trials. Med (Baltim). 2018;97:e11366.
McLean SF. Case-based learning and its application in medical and health-care fields: a review of worldwide literature. J Med Educ Curric Dev. 2016;3:JMECD.S20377.
Zeng N, Lu H, Li S, Yang Q, Liu F, Pan H, et al. Application of the combination of CBL teaching method and SEGUE framework to improve the doctor-patient communication skills of resident physicians in otolaryngology department. Bmc Med Educ. 2024;24:201.
Sun Z. Patient-specific 3D-printed models in pediatric congenital heart disease. Children. 2023;10:319.
Meyer-Szary J, Luis MS, Mikulski S, Patel A, Schulz F, Tretiakow D, et al. The role of 3D printing in planning complex medical procedures and training of medical professionals—cross-sectional multispecialty review. IJERPH. 2022;19:3331.
Sun Z, Wee C. 3D printed models in cardiovascular disease: an exciting future to deliver personalized medicine. Micromachines-basel. 2022;13:1575.
Valverde I, Gomez-Ciriza G, Hussain T, Suarez-Mejias C, Velasco-Forte MN, Byrne N, et al. Three-dimensional printed models for surgical planning of complex congenital heart defects: an international multicentre study. Eur J Cardio-thorac. 2017;52:1139–48.
Download references
Acknowledgements
We extend our sincere appreciation to the instructors and students whose invaluable participated in this study.
This paper received support from the Education Department of Anhui Province, China (Grant Numbers 2022jyxm1693, 2022jyxm1694, 2022xskc103, 2018jyxm1280).
Author information
Jian Zhao and Xin Gong are joint first authors.
Authors and Affiliations
Department of Human Anatomy, Wannan Medical College, No.22 West Wenchang Road, Wuhu, 241002, China
Jian Zhao, Xin Gong, Jian Ding, Rui Huang & Huachun Miao
Department of Cardio-Thoracic Surgery, Yijishan Hospital of Wannan Medical College, Wuhu, China
Kepin Xiong
Zhuhai Sailner 3D Technology Co., Ltd., Zhuhai, China
Kangle Zhuang
School of Basic Medical Sciences, Wannan Medical College, Wuhu, China
You can also search for this author in PubMed Google Scholar
Contributions
Jian Zhao and Huachun Miao designed the research. Jian Zhao, Xin Gong, Jian Ding, Kepin Xiong designed the tests and questionnaires. Kangle Zhuang processed the imaging data and printed the models. Xing Gong and Kepin Xiong implemented the teaching. Jian Zhao and Rui Huang collected the data and performed the statistical analysis. Jian Zhao and Huachun Miao prepared the manuscript. Shu Li and Huachun Miao revised the manuscript. Shu Li provided the Funding acquisition. All authors reviewed and approved the final manuscript.
Corresponding authors
Correspondence to Shu Li or Huachun Miao .
Ethics declarations
Ethics approval and consent to participate.
This investigation received ethical approval from the Ethical Committee of School of Basic Medical Sciences, Wannan Medical College (ECBMSWMC2022-1-12). All methodologies adhered strictly to established protocols and guidelines. Written informed consent was obtained from the study participants to take part in the study.
Consent for publication
Written informed consent was obtained from the individuals for the publication of any potentially identifiable images or data included in this article.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary material 2, supplementary material 3, rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Zhao, J., Gong, X., Ding, J. et al. Integration of case-based learning and three-dimensional printing for tetralogy of fallot instruction in clinical medical undergraduates: a randomized controlled trial. BMC Med Educ 24 , 571 (2024). https://doi.org/10.1186/s12909-024-05583-z
Download citation
Received : 03 March 2024
Accepted : 21 May 2024
Published : 24 May 2024
DOI : https://doi.org/10.1186/s12909-024-05583-z
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Medical education
- Case-based learning
- 3D printing
- Tetralogy of fallot
- Medical undergraduates
BMC Medical Education
ISSN: 1472-6920
- Submission enquiries: [email protected]
- General enquiries: [email protected]
Organizing Your Social Sciences Research Assignments
- Annotated Bibliography
- Analyzing a Scholarly Journal Article
- Group Presentations
- Dealing with Nervousness
- Using Visual Aids
- Grading Someone Else's Paper
- Types of Structured Group Activities
- Group Project Survival Skills
- Leading a Class Discussion
- Multiple Book Review Essay
- Reviewing Collected Works
- Writing a Case Analysis Paper
- Writing a Case Study
- About Informed Consent
- Writing Field Notes
- Writing a Policy Memo
- Writing a Reflective Paper
- Writing a Research Proposal
- Generative AI and Writing
- Acknowledgments
A case study research paper examines a person, place, event, condition, phenomenon, or other type of subject of analysis in order to extrapolate key themes and results that help predict future trends, illuminate previously hidden issues that can be applied to practice, and/or provide a means for understanding an important research problem with greater clarity. A case study research paper usually examines a single subject of analysis, but case study papers can also be designed as a comparative investigation that shows relationships between two or more subjects. The methods used to study a case can rest within a quantitative, qualitative, or mixed-method investigative paradigm.
Case Studies. Writing@CSU. Colorado State University; Mills, Albert J. , Gabrielle Durepos, and Eiden Wiebe, editors. Encyclopedia of Case Study Research . Thousand Oaks, CA: SAGE Publications, 2010 ; “What is a Case Study?” In Swanborn, Peter G. Case Study Research: What, Why and How? London: SAGE, 2010.
How to Approach Writing a Case Study Research Paper
General information about how to choose a topic to investigate can be found under the " Choosing a Research Problem " tab in the Organizing Your Social Sciences Research Paper writing guide. Review this page because it may help you identify a subject of analysis that can be investigated using a case study design.
However, identifying a case to investigate involves more than choosing the research problem . A case study encompasses a problem contextualized around the application of in-depth analysis, interpretation, and discussion, often resulting in specific recommendations for action or for improving existing conditions. As Seawright and Gerring note, practical considerations such as time and access to information can influence case selection, but these issues should not be the sole factors used in describing the methodological justification for identifying a particular case to study. Given this, selecting a case includes considering the following:
- The case represents an unusual or atypical example of a research problem that requires more in-depth analysis? Cases often represent a topic that rests on the fringes of prior investigations because the case may provide new ways of understanding the research problem. For example, if the research problem is to identify strategies to improve policies that support girl's access to secondary education in predominantly Muslim nations, you could consider using Azerbaijan as a case study rather than selecting a more obvious nation in the Middle East. Doing so may reveal important new insights into recommending how governments in other predominantly Muslim nations can formulate policies that support improved access to education for girls.
- The case provides important insight or illuminate a previously hidden problem? In-depth analysis of a case can be based on the hypothesis that the case study will reveal trends or issues that have not been exposed in prior research or will reveal new and important implications for practice. For example, anecdotal evidence may suggest drug use among homeless veterans is related to their patterns of travel throughout the day. Assuming prior studies have not looked at individual travel choices as a way to study access to illicit drug use, a case study that observes a homeless veteran could reveal how issues of personal mobility choices facilitate regular access to illicit drugs. Note that it is important to conduct a thorough literature review to ensure that your assumption about the need to reveal new insights or previously hidden problems is valid and evidence-based.
- The case challenges and offers a counter-point to prevailing assumptions? Over time, research on any given topic can fall into a trap of developing assumptions based on outdated studies that are still applied to new or changing conditions or the idea that something should simply be accepted as "common sense," even though the issue has not been thoroughly tested in current practice. A case study analysis may offer an opportunity to gather evidence that challenges prevailing assumptions about a research problem and provide a new set of recommendations applied to practice that have not been tested previously. For example, perhaps there has been a long practice among scholars to apply a particular theory in explaining the relationship between two subjects of analysis. Your case could challenge this assumption by applying an innovative theoretical framework [perhaps borrowed from another discipline] to explore whether this approach offers new ways of understanding the research problem. Taking a contrarian stance is one of the most important ways that new knowledge and understanding develops from existing literature.
- The case provides an opportunity to pursue action leading to the resolution of a problem? Another way to think about choosing a case to study is to consider how the results from investigating a particular case may result in findings that reveal ways in which to resolve an existing or emerging problem. For example, studying the case of an unforeseen incident, such as a fatal accident at a railroad crossing, can reveal hidden issues that could be applied to preventative measures that contribute to reducing the chance of accidents in the future. In this example, a case study investigating the accident could lead to a better understanding of where to strategically locate additional signals at other railroad crossings so as to better warn drivers of an approaching train, particularly when visibility is hindered by heavy rain, fog, or at night.
- The case offers a new direction in future research? A case study can be used as a tool for an exploratory investigation that highlights the need for further research about the problem. A case can be used when there are few studies that help predict an outcome or that establish a clear understanding about how best to proceed in addressing a problem. For example, after conducting a thorough literature review [very important!], you discover that little research exists showing the ways in which women contribute to promoting water conservation in rural communities of east central Africa. A case study of how women contribute to saving water in a rural village of Uganda can lay the foundation for understanding the need for more thorough research that documents how women in their roles as cooks and family caregivers think about water as a valuable resource within their community. This example of a case study could also point to the need for scholars to build new theoretical frameworks around the topic [e.g., applying feminist theories of work and family to the issue of water conservation].
Eisenhardt, Kathleen M. “Building Theories from Case Study Research.” Academy of Management Review 14 (October 1989): 532-550; Emmel, Nick. Sampling and Choosing Cases in Qualitative Research: A Realist Approach . Thousand Oaks, CA: SAGE Publications, 2013; Gerring, John. “What Is a Case Study and What Is It Good for?” American Political Science Review 98 (May 2004): 341-354; Mills, Albert J. , Gabrielle Durepos, and Eiden Wiebe, editors. Encyclopedia of Case Study Research . Thousand Oaks, CA: SAGE Publications, 2010; Seawright, Jason and John Gerring. "Case Selection Techniques in Case Study Research." Political Research Quarterly 61 (June 2008): 294-308.
Structure and Writing Style
The purpose of a paper in the social sciences designed around a case study is to thoroughly investigate a subject of analysis in order to reveal a new understanding about the research problem and, in so doing, contributing new knowledge to what is already known from previous studies. In applied social sciences disciplines [e.g., education, social work, public administration, etc.], case studies may also be used to reveal best practices, highlight key programs, or investigate interesting aspects of professional work.
In general, the structure of a case study research paper is not all that different from a standard college-level research paper. However, there are subtle differences you should be aware of. Here are the key elements to organizing and writing a case study research paper.
I. Introduction
As with any research paper, your introduction should serve as a roadmap for your readers to ascertain the scope and purpose of your study . The introduction to a case study research paper, however, should not only describe the research problem and its significance, but you should also succinctly describe why the case is being used and how it relates to addressing the problem. The two elements should be linked. With this in mind, a good introduction answers these four questions:
- What is being studied? Describe the research problem and describe the subject of analysis [the case] you have chosen to address the problem. Explain how they are linked and what elements of the case will help to expand knowledge and understanding about the problem.
- Why is this topic important to investigate? Describe the significance of the research problem and state why a case study design and the subject of analysis that the paper is designed around is appropriate in addressing the problem.
- What did we know about this topic before I did this study? Provide background that helps lead the reader into the more in-depth literature review to follow. If applicable, summarize prior case study research applied to the research problem and why it fails to adequately address the problem. Describe why your case will be useful. If no prior case studies have been used to address the research problem, explain why you have selected this subject of analysis.
- How will this study advance new knowledge or new ways of understanding? Explain why your case study will be suitable in helping to expand knowledge and understanding about the research problem.
Each of these questions should be addressed in no more than a few paragraphs. Exceptions to this can be when you are addressing a complex research problem or subject of analysis that requires more in-depth background information.
II. Literature Review
The literature review for a case study research paper is generally structured the same as it is for any college-level research paper. The difference, however, is that the literature review is focused on providing background information and enabling historical interpretation of the subject of analysis in relation to the research problem the case is intended to address . This includes synthesizing studies that help to:
- Place relevant works in the context of their contribution to understanding the case study being investigated . This would involve summarizing studies that have used a similar subject of analysis to investigate the research problem. If there is literature using the same or a very similar case to study, you need to explain why duplicating past research is important [e.g., conditions have changed; prior studies were conducted long ago, etc.].
- Describe the relationship each work has to the others under consideration that informs the reader why this case is applicable . Your literature review should include a description of any works that support using the case to investigate the research problem and the underlying research questions.
- Identify new ways to interpret prior research using the case study . If applicable, review any research that has examined the research problem using a different research design. Explain how your use of a case study design may reveal new knowledge or a new perspective or that can redirect research in an important new direction.
- Resolve conflicts amongst seemingly contradictory previous studies . This refers to synthesizing any literature that points to unresolved issues of concern about the research problem and describing how the subject of analysis that forms the case study can help resolve these existing contradictions.
- Point the way in fulfilling a need for additional research . Your review should examine any literature that lays a foundation for understanding why your case study design and the subject of analysis around which you have designed your study may reveal a new way of approaching the research problem or offer a perspective that points to the need for additional research.
- Expose any gaps that exist in the literature that the case study could help to fill . Summarize any literature that not only shows how your subject of analysis contributes to understanding the research problem, but how your case contributes to a new way of understanding the problem that prior research has failed to do.
- Locate your own research within the context of existing literature [very important!] . Collectively, your literature review should always place your case study within the larger domain of prior research about the problem. The overarching purpose of reviewing pertinent literature in a case study paper is to demonstrate that you have thoroughly identified and synthesized prior studies in relation to explaining the relevance of the case in addressing the research problem.
III. Method
In this section, you explain why you selected a particular case [i.e., subject of analysis] and the strategy you used to identify and ultimately decide that your case was appropriate in addressing the research problem. The way you describe the methods used varies depending on the type of subject of analysis that constitutes your case study.
If your subject of analysis is an incident or event . In the social and behavioral sciences, the event or incident that represents the case to be studied is usually bounded by time and place, with a clear beginning and end and with an identifiable location or position relative to its surroundings. The subject of analysis can be a rare or critical event or it can focus on a typical or regular event. The purpose of studying a rare event is to illuminate new ways of thinking about the broader research problem or to test a hypothesis. Critical incident case studies must describe the method by which you identified the event and explain the process by which you determined the validity of this case to inform broader perspectives about the research problem or to reveal new findings. However, the event does not have to be a rare or uniquely significant to support new thinking about the research problem or to challenge an existing hypothesis. For example, Walo, Bull, and Breen conducted a case study to identify and evaluate the direct and indirect economic benefits and costs of a local sports event in the City of Lismore, New South Wales, Australia. The purpose of their study was to provide new insights from measuring the impact of a typical local sports event that prior studies could not measure well because they focused on large "mega-events." Whether the event is rare or not, the methods section should include an explanation of the following characteristics of the event: a) when did it take place; b) what were the underlying circumstances leading to the event; and, c) what were the consequences of the event in relation to the research problem.
If your subject of analysis is a person. Explain why you selected this particular individual to be studied and describe what experiences they have had that provide an opportunity to advance new understandings about the research problem. Mention any background about this person which might help the reader understand the significance of their experiences that make them worthy of study. This includes describing the relationships this person has had with other people, institutions, and/or events that support using them as the subject for a case study research paper. It is particularly important to differentiate the person as the subject of analysis from others and to succinctly explain how the person relates to examining the research problem [e.g., why is one politician in a particular local election used to show an increase in voter turnout from any other candidate running in the election]. Note that these issues apply to a specific group of people used as a case study unit of analysis [e.g., a classroom of students].
If your subject of analysis is a place. In general, a case study that investigates a place suggests a subject of analysis that is unique or special in some way and that this uniqueness can be used to build new understanding or knowledge about the research problem. A case study of a place must not only describe its various attributes relevant to the research problem [e.g., physical, social, historical, cultural, economic, political], but you must state the method by which you determined that this place will illuminate new understandings about the research problem. It is also important to articulate why a particular place as the case for study is being used if similar places also exist [i.e., if you are studying patterns of homeless encampments of veterans in open spaces, explain why you are studying Echo Park in Los Angeles rather than Griffith Park?]. If applicable, describe what type of human activity involving this place makes it a good choice to study [e.g., prior research suggests Echo Park has more homeless veterans].
If your subject of analysis is a phenomenon. A phenomenon refers to a fact, occurrence, or circumstance that can be studied or observed but with the cause or explanation to be in question. In this sense, a phenomenon that forms your subject of analysis can encompass anything that can be observed or presumed to exist but is not fully understood. In the social and behavioral sciences, the case usually focuses on human interaction within a complex physical, social, economic, cultural, or political system. For example, the phenomenon could be the observation that many vehicles used by ISIS fighters are small trucks with English language advertisements on them. The research problem could be that ISIS fighters are difficult to combat because they are highly mobile. The research questions could be how and by what means are these vehicles used by ISIS being supplied to the militants and how might supply lines to these vehicles be cut off? How might knowing the suppliers of these trucks reveal larger networks of collaborators and financial support? A case study of a phenomenon most often encompasses an in-depth analysis of a cause and effect that is grounded in an interactive relationship between people and their environment in some way.
NOTE: The choice of the case or set of cases to study cannot appear random. Evidence that supports the method by which you identified and chose your subject of analysis should clearly support investigation of the research problem and linked to key findings from your literature review. Be sure to cite any studies that helped you determine that the case you chose was appropriate for examining the problem.
IV. Discussion
The main elements of your discussion section are generally the same as any research paper, but centered around interpreting and drawing conclusions about the key findings from your analysis of the case study. Note that a general social sciences research paper may contain a separate section to report findings. However, in a paper designed around a case study, it is common to combine a description of the results with the discussion about their implications. The objectives of your discussion section should include the following:
Reiterate the Research Problem/State the Major Findings Briefly reiterate the research problem you are investigating and explain why the subject of analysis around which you designed the case study were used. You should then describe the findings revealed from your study of the case using direct, declarative, and succinct proclamation of the study results. Highlight any findings that were unexpected or especially profound.
Explain the Meaning of the Findings and Why They are Important Systematically explain the meaning of your case study findings and why you believe they are important. Begin this part of the section by repeating what you consider to be your most important or surprising finding first, then systematically review each finding. Be sure to thoroughly extrapolate what your analysis of the case can tell the reader about situations or conditions beyond the actual case that was studied while, at the same time, being careful not to misconstrue or conflate a finding that undermines the external validity of your conclusions.
Relate the Findings to Similar Studies No study in the social sciences is so novel or possesses such a restricted focus that it has absolutely no relation to previously published research. The discussion section should relate your case study results to those found in other studies, particularly if questions raised from prior studies served as the motivation for choosing your subject of analysis. This is important because comparing and contrasting the findings of other studies helps support the overall importance of your results and it highlights how and in what ways your case study design and the subject of analysis differs from prior research about the topic.
Consider Alternative Explanations of the Findings Remember that the purpose of social science research is to discover and not to prove. When writing the discussion section, you should carefully consider all possible explanations revealed by the case study results, rather than just those that fit your hypothesis or prior assumptions and biases. Be alert to what the in-depth analysis of the case may reveal about the research problem, including offering a contrarian perspective to what scholars have stated in prior research if that is how the findings can be interpreted from your case.
Acknowledge the Study's Limitations You can state the study's limitations in the conclusion section of your paper but describing the limitations of your subject of analysis in the discussion section provides an opportunity to identify the limitations and explain why they are not significant. This part of the discussion section should also note any unanswered questions or issues your case study could not address. More detailed information about how to document any limitations to your research can be found here .
Suggest Areas for Further Research Although your case study may offer important insights about the research problem, there are likely additional questions related to the problem that remain unanswered or findings that unexpectedly revealed themselves as a result of your in-depth analysis of the case. Be sure that the recommendations for further research are linked to the research problem and that you explain why your recommendations are valid in other contexts and based on the original assumptions of your study.
V. Conclusion
As with any research paper, you should summarize your conclusion in clear, simple language; emphasize how the findings from your case study differs from or supports prior research and why. Do not simply reiterate the discussion section. Provide a synthesis of key findings presented in the paper to show how these converge to address the research problem. If you haven't already done so in the discussion section, be sure to document the limitations of your case study and any need for further research.
The function of your paper's conclusion is to: 1) reiterate the main argument supported by the findings from your case study; 2) state clearly the context, background, and necessity of pursuing the research problem using a case study design in relation to an issue, controversy, or a gap found from reviewing the literature; and, 3) provide a place to persuasively and succinctly restate the significance of your research problem, given that the reader has now been presented with in-depth information about the topic.
Consider the following points to help ensure your conclusion is appropriate:
- If the argument or purpose of your paper is complex, you may need to summarize these points for your reader.
- If prior to your conclusion, you have not yet explained the significance of your findings or if you are proceeding inductively, use the conclusion of your paper to describe your main points and explain their significance.
- Move from a detailed to a general level of consideration of the case study's findings that returns the topic to the context provided by the introduction or within a new context that emerges from your case study findings.
Note that, depending on the discipline you are writing in or the preferences of your professor, the concluding paragraph may contain your final reflections on the evidence presented as it applies to practice or on the essay's central research problem. However, the nature of being introspective about the subject of analysis you have investigated will depend on whether you are explicitly asked to express your observations in this way.
Problems to Avoid
Overgeneralization One of the goals of a case study is to lay a foundation for understanding broader trends and issues applied to similar circumstances. However, be careful when drawing conclusions from your case study. They must be evidence-based and grounded in the results of the study; otherwise, it is merely speculation. Looking at a prior example, it would be incorrect to state that a factor in improving girls access to education in Azerbaijan and the policy implications this may have for improving access in other Muslim nations is due to girls access to social media if there is no documentary evidence from your case study to indicate this. There may be anecdotal evidence that retention rates were better for girls who were engaged with social media, but this observation would only point to the need for further research and would not be a definitive finding if this was not a part of your original research agenda.
Failure to Document Limitations No case is going to reveal all that needs to be understood about a research problem. Therefore, just as you have to clearly state the limitations of a general research study , you must describe the specific limitations inherent in the subject of analysis. For example, the case of studying how women conceptualize the need for water conservation in a village in Uganda could have limited application in other cultural contexts or in areas where fresh water from rivers or lakes is plentiful and, therefore, conservation is understood more in terms of managing access rather than preserving access to a scarce resource.
Failure to Extrapolate All Possible Implications Just as you don't want to over-generalize from your case study findings, you also have to be thorough in the consideration of all possible outcomes or recommendations derived from your findings. If you do not, your reader may question the validity of your analysis, particularly if you failed to document an obvious outcome from your case study research. For example, in the case of studying the accident at the railroad crossing to evaluate where and what types of warning signals should be located, you failed to take into consideration speed limit signage as well as warning signals. When designing your case study, be sure you have thoroughly addressed all aspects of the problem and do not leave gaps in your analysis that leave the reader questioning the results.
Case Studies. Writing@CSU. Colorado State University; Gerring, John. Case Study Research: Principles and Practices . New York: Cambridge University Press, 2007; Merriam, Sharan B. Qualitative Research and Case Study Applications in Education . Rev. ed. San Francisco, CA: Jossey-Bass, 1998; Miller, Lisa L. “The Use of Case Studies in Law and Social Science Research.” Annual Review of Law and Social Science 14 (2018): TBD; Mills, Albert J., Gabrielle Durepos, and Eiden Wiebe, editors. Encyclopedia of Case Study Research . Thousand Oaks, CA: SAGE Publications, 2010; Putney, LeAnn Grogan. "Case Study." In Encyclopedia of Research Design , Neil J. Salkind, editor. (Thousand Oaks, CA: SAGE Publications, 2010), pp. 116-120; Simons, Helen. Case Study Research in Practice . London: SAGE Publications, 2009; Kratochwill, Thomas R. and Joel R. Levin, editors. Single-Case Research Design and Analysis: New Development for Psychology and Education . Hilldsale, NJ: Lawrence Erlbaum Associates, 1992; Swanborn, Peter G. Case Study Research: What, Why and How? London : SAGE, 2010; Yin, Robert K. Case Study Research: Design and Methods . 6th edition. Los Angeles, CA, SAGE Publications, 2014; Walo, Maree, Adrian Bull, and Helen Breen. “Achieving Economic Benefits at Local Events: A Case Study of a Local Sports Event.” Festival Management and Event Tourism 4 (1996): 95-106.
Writing Tip
At Least Five Misconceptions about Case Study Research
Social science case studies are often perceived as limited in their ability to create new knowledge because they are not randomly selected and findings cannot be generalized to larger populations. Flyvbjerg examines five misunderstandings about case study research and systematically "corrects" each one. To quote, these are:
Misunderstanding 1 : General, theoretical [context-independent] knowledge is more valuable than concrete, practical [context-dependent] knowledge. Misunderstanding 2 : One cannot generalize on the basis of an individual case; therefore, the case study cannot contribute to scientific development. Misunderstanding 3 : The case study is most useful for generating hypotheses; that is, in the first stage of a total research process, whereas other methods are more suitable for hypotheses testing and theory building. Misunderstanding 4 : The case study contains a bias toward verification, that is, a tendency to confirm the researcher’s preconceived notions. Misunderstanding 5 : It is often difficult to summarize and develop general propositions and theories on the basis of specific case studies [p. 221].
While writing your paper, think introspectively about how you addressed these misconceptions because to do so can help you strengthen the validity and reliability of your research by clarifying issues of case selection, the testing and challenging of existing assumptions, the interpretation of key findings, and the summation of case outcomes. Think of a case study research paper as a complete, in-depth narrative about the specific properties and key characteristics of your subject of analysis applied to the research problem.
Flyvbjerg, Bent. “Five Misunderstandings About Case-Study Research.” Qualitative Inquiry 12 (April 2006): 219-245.
- << Previous: Writing a Case Analysis Paper
- Next: Writing a Field Report >>
- Last Updated: May 7, 2024 9:45 AM
- URL: https://libguides.usc.edu/writingguide/assignments
IMAGES
VIDEO
COMMENTS
A case study is one of the most commonly used methodologies of social research. This article attempts to look into the various dimensions of a case study research strategy, the different epistemological strands which determine the particular case study type and approach adopted in the field, discusses the factors which can enhance the effectiveness of a case study research, and the debate ...
A case study is a detailed study of a specific subject, such as a person, group, place, event, organization, or phenomenon. Case studies are commonly used in social, educational, clinical, and business research. ... To ensure that your analysis of the case has a solid academic grounding, you should conduct a literature review of sources related ...
The function of your paper's conclusion is to: 1) restate the main argument supported by the findings from the analysis of your case; 2) clearly state the context, background, and necessity of pursuing the research problem using a case study design in relation to an issue, controversy, or a gap found from reviewing the literature; and, 3 ...
Case studies play a significant role in knowledge development across various disciplines. Analysis of cases provides an avenue for researchers to explore phenomena within their context based on the collected data. Analysis of qualitative data from case study research can contribute to knowledge development.
Although case studies have been discussed extensively in the literature, little has been written about the specific steps one may use to conduct case study research effectively (Gagnon, 2010; Hancock & Algozzine, 2016).Baskarada (2014) also emphasized the need to have a succinct guideline that can be practically followed as it is actually tough to execute a case study well in practice.
Case studies tend to focus on qualitative data using methods such as interviews, observations, and analysis of primary and secondary sources (e.g., newspaper articles, photographs, official records). Sometimes a case study will also collect quantitative data. Example: Mixed methods case study. For a case study of a wind farm development in a ...
A Case study is: An in-depth research design that primarily uses a qualitative methodology but sometimes includes quantitative methodology. Used to examine an identifiable problem confirmed through research. Used to investigate an individual, group of people, organization, or event. Used to mostly answer "how" and "why" questions.
The purpose of case study research is twofold: (1) to provide descriptive information and (2) to suggest theoretical relevance. Rich description enables an in-depth or sharpened understanding of the case. It is unique given one characteristic: case studies draw from more than one data source. Case studies are inherently multimodal or mixed ...
Case study is a common methodology in the social sciences (management, psychology, science of education, political science, sociology). ... Why is a real case study more puzzling than expected, having read the literature on case study? We assume that the answer lies in a paradox: despite what is suggested by the double singular "case study ...
refers to many exemplary examples from the existing case study literature.1 The examples include some of the best case studies ever done, including a case study that is more than 75 years old but that is still in print. The richness of the examples permits the discussion of the
According to the book Understanding Case Study Research, case studies are "small scale research with meaning" that generally involve the following: The study of a particular case, or a number of cases. That the case will be complex and bounded. That it will be studied in its context. That the analysis undertaken will seek to be holistic.
Case studies are designed to suit the case and research question and published case studies demonstrate wide diversity in study design. There are two popular case study approaches in qualitative research. The first, proposed by Stake ( 1995) and Merriam ( 2009 ), is situated in a social constructivist paradigm, whereas the second, by Yin ( 2012 ...
A case study is a research approach that is used to generate an in-depth, multi-faceted understanding of a complex issue in its real-life context. It is an established research design that is used extensively in a wide variety of disciplines, particularly in the social sciences. A case study can be defined in a variety of ways (Table 5 ), the ...
The case study method is a research strategy that aims to gain an in-depth understanding of a specific phenomenon by collecting and analyzing ... Due to its rising relevance in the literature ...
Examples of literature reviews. Step 1 - Search for relevant literature. Step 2 - Evaluate and select sources. Step 3 - Identify themes, debates, and gaps. Step 4 - Outline your literature review's structure. Step 5 - Write your literature review.
Case studies provide a better understanding of phenomena regarding concrete context-dependent knowledge (Andersen and Kragh 2010; Flyvbjerg 2006: 224), but as literature reviews indicate, there is still confusion regarding the adequate utilization of case study methodology (Welch et al. 2011). This can be interpreted in a way that authors and ...
Most integrative literature reviews are intended to address mature topics or new, emerging topics. In the case of mature topics, the purpose of using an integrative review method is to overview the knowledge base, to critically review and potentially re-conceptualize, and to expand on the theoretical foundation of the specific topic as it develops.
A literature review may consist of simply a summary of key sources, but in the social sciences, a literature review usually has an organizational pattern and combines both summary and synthesis, often within specific conceptual categories.A summary is a recap of the important information of the source, but a synthesis is a re-organization, or a reshuffling, of that information in a way that ...
This paper presents a review of the literature on case study research and comments on the ongoing debate of the value of case study. A research paradigm and its theoretical framework is described. This review focuses extensively on the positions of Merriam (1998), Yin (1981, 1984, 1994, 1999, 2003a, 2003b, 2005), and Stake (1978/2000, 1994, 1995, 2005, 2008) as foundational writers in the area ...
In March of this year, Comparative Literature professor Dore Levy published her new book, Reading Art in Literature: The Marvelous Case of "The Story of the Stone".The Story of the Stone (also known as The Dream of the Red Chamber) is an 18th-century Chinese novel by Cao Xueqin, and is considered to be one of the great classical novels of Chinese literature.
Of 38,353 persons interviewed, 595 were found to have undiagnosed COPD or asthma and 508 underwent randomization: 253 were assigned to the intervention group and 255 to the usual-care group.
The literature reveals varying incidence rates of VA injury during cervical spine surgeries, attributed to different surgical techniques. ... In this case study, we detail an instance wherein a patient underwent C1-C2 instrumentation surgery utilizing a microscope-based AR navigation system. This patient exhibited a notable alleviation of her ...
However, the existing literature highlights several limitations to use the risk matrix. In response to the weaknesses of its use, this paper proposes a novel approach for prioritising project risks.
Our literature review identified 23 studies reporting prevalence or incidence, yet only ten studies provided estimates ranging from 1.1 to 280/100.000 in the general population. Our case series identified six patients with LA from a localized region in Southern Denmark; all confirmed by Borrelia-specific real-time PCR from synovial fluid. The ...
The framework facilitates best-practice, reasoning, and communication and is exemplified here with two case studies. Methods. A literature review stimulated by a new method of teaching manual therapy, reflecting contemporary evidence, being trialled at a United Kingdom education institute. A group of experienced, internationally-based academics ...
To conclude, there are two main objectives of this study. First is to provide a step-by-step guideline to research students for conducting case study. Second, an analysis of authors' multiple case studies is presented in order to provide an application of step-by-step guideline. This article has been divided into two sections.
Literature search. An SLR was performed in accordance with the Cochrane Handbook for Systematic Reviews of Interventions [] and reported in alignment with the Preferred Reporting Items for Systematic Literature Reviews and Meta-Analyses (PRISMA) statement [] to identify all RWE studies assessing the effectiveness and safety of treatments used for patients with HR+/HER2- LABC/mBC following 1 L ...
A case study is a research approach that is used to generate an in-depth, multi-faceted understanding of a complex issue in its real-life context. It is an established research design that is used extensively in a wide variety of disciplines, particularly in the social sciences. A case study can be defined in a variety of ways (Table.
Teaching implementation. Figure 1B illustrates the instructional framework employed in this study. One week preceding the class session, all the students were tasked with a 30-minute self-study session, focusing on the theoretical content related to TOF as outlined in the Pediatrics and Surgery textbooks, along with a review of pertinent academic literature.
A case study is a research method that involves an in-depth analysis of a real-life phenomenon or situation. Learn how to write a case study for your social sciences research assignments with this helpful guide from USC Library. Find out how to define the case, select the data sources, analyze the evidence, and report the results.