
Chapter 11. Interviewing
Introduction.
Interviewing people is at the heart of qualitative research. It is not merely a way to collect data but an intrinsically rewarding activity—an interaction between two people that holds the potential for greater understanding and interpersonal development. Unlike many of our daily interactions with others that are fairly shallow and mundane, sitting down with a person for an hour or two and really listening to what they have to say is a profound and deep enterprise, one that can provide not only “data” for you, the interviewer, but also self-understanding and a feeling of being heard for the interviewee. I always approach interviewing with a deep appreciation for the opportunity it gives me to understand how other people experience the world. That said, there is not one kind of interview but many, and some of these are shallower than others. This chapter will provide you with an overview of interview techniques but with a special focus on the in-depth semistructured interview guide approach, which is the approach most widely used in social science research.
An interview can be variously defined as “a conversation with a purpose” ( Lune and Berg 2018 ) and an attempt to understand the world from the point of view of the person being interviewed: “to unfold the meaning of peoples’ experiences, to uncover their lived world prior to scientific explanations” ( Kvale 2007 ). It is a form of active listening in which the interviewer steers the conversation to subjects and topics of interest to their research but also manages to leave enough space for those interviewed to say surprising things. Achieving that balance is a tricky thing, which is why most practitioners believe interviewing is both an art and a science. In my experience as a teacher, there are some students who are “natural” interviewers (often they are introverts), but anyone can learn to conduct interviews, and everyone, even those of us who have been doing this for years, can improve their interviewing skills. This might be a good time to highlight the fact that the interview is a product between interviewer and interviewee and that this product is only as good as the rapport established between the two participants. Active listening is the key to establishing this necessary rapport.
Patton ( 2002 ) makes the argument that we use interviews because there are certain things that are not observable. In particular, “we cannot observe feelings, thoughts, and intentions. We cannot observe behaviors that took place at some previous point in time. We cannot observe situations that preclude the presence of an observer. We cannot observe how people have organized the world and the meanings they attach to what goes on in the world. We have to ask people questions about those things” ( 341 ).
Types of Interviews
There are several distinct types of interviews. Imagine a continuum (figure 11.1). On one side are unstructured conversations—the kind you have with your friends. No one is in control of those conversations, and what you talk about is often random—whatever pops into your head. There is no secret, underlying purpose to your talking—if anything, the purpose is to talk to and engage with each other, and the words you use and the things you talk about are a little beside the point. An unstructured interview is a little like this informal conversation, except that one of the parties to the conversation (you, the researcher) does have an underlying purpose, and that is to understand the other person. You are not friends speaking for no purpose, but it might feel just as unstructured to the “interviewee” in this scenario. That is one side of the continuum. On the other side are fully structured and standardized survey-type questions asked face-to-face. Here it is very clear who is asking the questions and who is answering them. This doesn’t feel like a conversation at all! A lot of people new to interviewing have this ( erroneously !) in mind when they think about interviews as data collection. Somewhere in the middle of these two extreme cases is the “ semistructured” interview , in which the researcher uses an “interview guide” to gently move the conversation to certain topics and issues. This is the primary form of interviewing for qualitative social scientists and will be what I refer to as interviewing for the rest of this chapter, unless otherwise specified.

Informal (unstructured conversations). This is the most “open-ended” approach to interviewing. It is particularly useful in conjunction with observational methods (see chapters 13 and 14). There are no predetermined questions. Each interview will be different. Imagine you are researching the Oregon Country Fair, an annual event in Veneta, Oregon, that includes live music, artisan craft booths, face painting, and a lot of people walking through forest paths. It’s unlikely that you will be able to get a person to sit down with you and talk intensely about a set of questions for an hour and a half. But you might be able to sidle up to several people and engage with them about their experiences at the fair. You might have a general interest in what attracts people to these events, so you could start a conversation by asking strangers why they are here or why they come back every year. That’s it. Then you have a conversation that may lead you anywhere. Maybe one person tells a long story about how their parents brought them here when they were a kid. A second person talks about how this is better than Burning Man. A third person shares their favorite traveling band. And yet another enthuses about the public library in the woods. During your conversations, you also talk about a lot of other things—the weather, the utilikilts for sale, the fact that a favorite food booth has disappeared. It’s all good. You may not be able to record these conversations. Instead, you might jot down notes on the spot and then, when you have the time, write down as much as you can remember about the conversations in long fieldnotes. Later, you will have to sit down with these fieldnotes and try to make sense of all the information (see chapters 18 and 19).
Interview guide ( semistructured interview ). This is the primary type employed by social science qualitative researchers. The researcher creates an “interview guide” in advance, which she uses in every interview. In theory, every person interviewed is asked the same questions. In practice, every person interviewed is asked mostly the same topics but not always the same questions, as the whole point of a “guide” is that it guides the direction of the conversation but does not command it. The guide is typically between five and ten questions or question areas, sometimes with suggested follow-ups or prompts . For example, one question might be “What was it like growing up in Eastern Oregon?” with prompts such as “Did you live in a rural area? What kind of high school did you attend?” to help the conversation develop. These interviews generally take place in a quiet place (not a busy walkway during a festival) and are recorded. The recordings are transcribed, and those transcriptions then become the “data” that is analyzed (see chapters 18 and 19). The conventional length of one of these types of interviews is between one hour and two hours, optimally ninety minutes. Less than one hour doesn’t allow for much development of questions and thoughts, and two hours (or more) is a lot of time to ask someone to sit still and answer questions. If you have a lot of ground to cover, and the person is willing, I highly recommend two separate interview sessions, with the second session being slightly shorter than the first (e.g., ninety minutes the first day, sixty minutes the second). There are lots of good reasons for this, but the most compelling one is that this allows you to listen to the first day’s recording and catch anything interesting you might have missed in the moment and so develop follow-up questions that can probe further. This also allows the person being interviewed to have some time to think about the issues raised in the interview and go a little deeper with their answers.
Standardized questionnaire with open responses ( structured interview ). This is the type of interview a lot of people have in mind when they hear “interview”: a researcher comes to your door with a clipboard and proceeds to ask you a series of questions. These questions are all the same whoever answers the door; they are “standardized.” Both the wording and the exact order are important, as people’s responses may vary depending on how and when a question is asked. These are qualitative only in that the questions allow for “open-ended responses”: people can say whatever they want rather than select from a predetermined menu of responses. For example, a survey I collaborated on included this open-ended response question: “How does class affect one’s career success in sociology?” Some of the answers were simply one word long (e.g., “debt”), and others were long statements with stories and personal anecdotes. It is possible to be surprised by the responses. Although it’s a stretch to call this kind of questioning a conversation, it does allow the person answering the question some degree of freedom in how they answer.
Survey questionnaire with closed responses (not an interview!). Standardized survey questions with specific answer options (e.g., closed responses) are not really interviews at all, and they do not generate qualitative data. For example, if we included five options for the question “How does class affect one’s career success in sociology?”—(1) debt, (2) social networks, (3) alienation, (4) family doesn’t understand, (5) type of grad program—we leave no room for surprises at all. Instead, we would most likely look at patterns around these responses, thinking quantitatively rather than qualitatively (e.g., using regression analysis techniques, we might find that working-class sociologists were twice as likely to bring up alienation). It can sometimes be confusing for new students because the very same survey can include both closed-ended and open-ended questions. The key is to think about how these will be analyzed and to what level surprises are possible. If your plan is to turn all responses into a number and make predictions about correlations and relationships, you are no longer conducting qualitative research. This is true even if you are conducting this survey face-to-face with a real live human. Closed-response questions are not conversations of any kind, purposeful or not.
In summary, the semistructured interview guide approach is the predominant form of interviewing for social science qualitative researchers because it allows a high degree of freedom of responses from those interviewed (thus allowing for novel discoveries) while still maintaining some connection to a research question area or topic of interest. The rest of the chapter assumes the employment of this form.
Creating an Interview Guide
Your interview guide is the instrument used to bridge your research question(s) and what the people you are interviewing want to tell you. Unlike a standardized questionnaire, the questions actually asked do not need to be exactly what you have written down in your guide. The guide is meant to create space for those you are interviewing to talk about the phenomenon of interest, but sometimes you are not even sure what that phenomenon is until you start asking questions. A priority in creating an interview guide is to ensure it offers space. One of the worst mistakes is to create questions that are so specific that the person answering them will not stray. Relatedly, questions that sound “academic” will shut down a lot of respondents. A good interview guide invites respondents to talk about what is important to them, not feel like they are performing or being evaluated by you.
Good interview questions should not sound like your “research question” at all. For example, let’s say your research question is “How do patriarchal assumptions influence men’s understanding of climate change and responses to climate change?” It would be worse than unhelpful to ask a respondent, “How do your assumptions about the role of men affect your understanding of climate change?” You need to unpack this into manageable nuggets that pull your respondent into the area of interest without leading him anywhere. You could start by asking him what he thinks about climate change in general. Or, even better, whether he has any concerns about heatwaves or increased tornadoes or polar icecaps melting. Once he starts talking about that, you can ask follow-up questions that bring in issues around gendered roles, perhaps asking if he is married (to a woman) and whether his wife shares his thoughts and, if not, how they negotiate that difference. The fact is, you won’t really know the right questions to ask until he starts talking.
There are several distinct types of questions that can be used in your interview guide, either as main questions or as follow-up probes. If you remember that the point is to leave space for the respondent, you will craft a much more effective interview guide! You will also want to think about the place of time in both the questions themselves (past, present, future orientations) and the sequencing of the questions.
Researcher Note
Suggestion : As you read the next three sections (types of questions, temporality, question sequence), have in mind a particular research question, and try to draft questions and sequence them in a way that opens space for a discussion that helps you answer your research question.
Type of Questions
Experience and behavior questions ask about what a respondent does regularly (their behavior) or has done (their experience). These are relatively easy questions for people to answer because they appear more “factual” and less subjective. This makes them good opening questions. For the study on climate change above, you might ask, “Have you ever experienced an unusual weather event? What happened?” Or “You said you work outside? What is a typical summer workday like for you? How do you protect yourself from the heat?”
Opinion and values questions , in contrast, ask questions that get inside the minds of those you are interviewing. “Do you think climate change is real? Who or what is responsible for it?” are two such questions. Note that you don’t have to literally ask, “What is your opinion of X?” but you can find a way to ask the specific question relevant to the conversation you are having. These questions are a bit trickier to ask because the answers you get may depend in part on how your respondent perceives you and whether they want to please you or not. We’ve talked a fair amount about being reflective. Here is another place where this comes into play. You need to be aware of the effect your presence might have on the answers you are receiving and adjust accordingly. If you are a woman who is perceived as liberal asking a man who identifies as conservative about climate change, there is a lot of subtext that can be going on in the interview. There is no one right way to resolve this, but you must at least be aware of it.
Feeling questions are questions that ask respondents to draw on their emotional responses. It’s pretty common for academic researchers to forget that we have bodies and emotions, but people’s understandings of the world often operate at this affective level, sometimes unconsciously or barely consciously. It is a good idea to include questions that leave space for respondents to remember, imagine, or relive emotional responses to particular phenomena. “What was it like when you heard your cousin’s house burned down in that wildfire?” doesn’t explicitly use any emotion words, but it allows your respondent to remember what was probably a pretty emotional day. And if they respond emotionally neutral, that is pretty interesting data too. Note that asking someone “How do you feel about X” is not always going to evoke an emotional response, as they might simply turn around and respond with “I think that…” It is better to craft a question that actually pushes the respondent into the affective category. This might be a specific follow-up to an experience and behavior question —for example, “You just told me about your daily routine during the summer heat. Do you worry it is going to get worse?” or “Have you ever been afraid it will be too hot to get your work accomplished?”
Knowledge questions ask respondents what they actually know about something factual. We have to be careful when we ask these types of questions so that respondents do not feel like we are evaluating them (which would shut them down), but, for example, it is helpful to know when you are having a conversation about climate change that your respondent does in fact know that unusual weather events have increased and that these have been attributed to climate change! Asking these questions can set the stage for deeper questions and can ensure that the conversation makes the same kind of sense to both participants. For example, a conversation about political polarization can be put back on track once you realize that the respondent doesn’t really have a clear understanding that there are two parties in the US. Instead of asking a series of questions about Republicans and Democrats, you might shift your questions to talk more generally about political disagreements (e.g., “people against abortion”). And sometimes what you do want to know is the level of knowledge about a particular program or event (e.g., “Are you aware you can discharge your student loans through the Public Service Loan Forgiveness program?”).
Sensory questions call on all senses of the respondent to capture deeper responses. These are particularly helpful in sparking memory. “Think back to your childhood in Eastern Oregon. Describe the smells, the sounds…” Or you could use these questions to help a person access the full experience of a setting they customarily inhabit: “When you walk through the doors to your office building, what do you see? Hear? Smell?” As with feeling questions , these questions often supplement experience and behavior questions . They are another way of allowing your respondent to report fully and deeply rather than remain on the surface.
Creative questions employ illustrative examples, suggested scenarios, or simulations to get respondents to think more deeply about an issue, topic, or experience. There are many options here. In The Trouble with Passion , Erin Cech ( 2021 ) provides a scenario in which “Joe” is trying to decide whether to stay at his decent but boring computer job or follow his passion by opening a restaurant. She asks respondents, “What should Joe do?” Their answers illuminate the attraction of “passion” in job selection. In my own work, I have used a news story about an upwardly mobile young man who no longer has time to see his mother and sisters to probe respondents’ feelings about the costs of social mobility. Jessi Streib and Betsy Leondar-Wright have used single-page cartoon “scenes” to elicit evaluations of potential racial discrimination, sexual harassment, and classism. Barbara Sutton ( 2010 ) has employed lists of words (“strong,” “mother,” “victim”) on notecards she fans out and asks her female respondents to select and discuss.
Background/Demographic Questions
You most definitely will want to know more about the person you are interviewing in terms of conventional demographic information, such as age, race, gender identity, occupation, and educational attainment. These are not questions that normally open up inquiry. [1] For this reason, my practice has been to include a separate “demographic questionnaire” sheet that I ask each respondent to fill out at the conclusion of the interview. Only include those aspects that are relevant to your study. For example, if you are not exploring religion or religious affiliation, do not include questions about a person’s religion on the demographic sheet. See the example provided at the end of this chapter.
Temporality
Any type of question can have a past, present, or future orientation. For example, if you are asking a behavior question about workplace routine, you might ask the respondent to talk about past work, present work, and ideal (future) work. Similarly, if you want to understand how people cope with natural disasters, you might ask your respondent how they felt then during the wildfire and now in retrospect and whether and to what extent they have concerns for future wildfire disasters. It’s a relatively simple suggestion—don’t forget to ask about past, present, and future—but it can have a big impact on the quality of the responses you receive.
Question Sequence
Having a list of good questions or good question areas is not enough to make a good interview guide. You will want to pay attention to the order in which you ask your questions. Even though any one respondent can derail this order (perhaps by jumping to answer a question you haven’t yet asked), a good advance plan is always helpful. When thinking about sequence, remember that your goal is to get your respondent to open up to you and to say things that might surprise you. To establish rapport, it is best to start with nonthreatening questions. Asking about the present is often the safest place to begin, followed by the past (they have to know you a little bit to get there), and lastly, the future (talking about hopes and fears requires the most rapport). To allow for surprises, it is best to move from very general questions to more particular questions only later in the interview. This ensures that respondents have the freedom to bring up the topics that are relevant to them rather than feel like they are constrained to answer you narrowly. For example, refrain from asking about particular emotions until these have come up previously—don’t lead with them. Often, your more particular questions will emerge only during the course of the interview, tailored to what is emerging in conversation.
Once you have a set of questions, read through them aloud and imagine you are being asked the same questions. Does the set of questions have a natural flow? Would you be willing to answer the very first question to a total stranger? Does your sequence establish facts and experiences before moving on to opinions and values? Did you include prefatory statements, where necessary; transitions; and other announcements? These can be as simple as “Hey, we talked a lot about your experiences as a barista while in college.… Now I am turning to something completely different: how you managed friendships in college.” That is an abrupt transition, but it has been softened by your acknowledgment of that.
Probes and Flexibility
Once you have the interview guide, you will also want to leave room for probes and follow-up questions. As in the sample probe included here, you can write out the obvious probes and follow-up questions in advance. You might not need them, as your respondent might anticipate them and include full responses to the original question. Or you might need to tailor them to how your respondent answered the question. Some common probes and follow-up questions include asking for more details (When did that happen? Who else was there?), asking for elaboration (Could you say more about that?), asking for clarification (Does that mean what I think it means or something else? I understand what you mean, but someone else reading the transcript might not), and asking for contrast or comparison (How did this experience compare with last year’s event?). “Probing is a skill that comes from knowing what to look for in the interview, listening carefully to what is being said and what is not said, and being sensitive to the feedback needs of the person being interviewed” ( Patton 2002:374 ). It takes work! And energy. I and many other interviewers I know report feeling emotionally and even physically drained after conducting an interview. You are tasked with active listening and rearranging your interview guide as needed on the fly. If you only ask the questions written down in your interview guide with no deviations, you are doing it wrong. [2]
The Final Question
Every interview guide should include a very open-ended final question that allows for the respondent to say whatever it is they have been dying to tell you but you’ve forgotten to ask. About half the time they are tired too and will tell you they have nothing else to say. But incredibly, some of the most honest and complete responses take place here, at the end of a long interview. You have to realize that the person being interviewed is often discovering things about themselves as they talk to you and that this process of discovery can lead to new insights for them. Making space at the end is therefore crucial. Be sure you convey that you actually do want them to tell you more, that the offer of “anything else?” is not read as an empty convention where the polite response is no. Here is where you can pull from that active listening and tailor the final question to the particular person. For example, “I’ve asked you a lot of questions about what it was like to live through that wildfire. I’m wondering if there is anything I’ve forgotten to ask, especially because I haven’t had that experience myself” is a much more inviting final question than “Great. Anything you want to add?” It’s also helpful to convey to the person that you have the time to listen to their full answer, even if the allotted time is at the end. After all, there are no more questions to ask, so the respondent knows exactly how much time is left. Do them the courtesy of listening to them!
Conducting the Interview
Once you have your interview guide, you are on your way to conducting your first interview. I always practice my interview guide with a friend or family member. I do this even when the questions don’t make perfect sense for them, as it still helps me realize which questions make no sense, are poorly worded (too academic), or don’t follow sequentially. I also practice the routine I will use for interviewing, which goes something like this:
- Introduce myself and reintroduce the study
- Provide consent form and ask them to sign and retain/return copy
- Ask if they have any questions about the study before we begin
- Ask if I can begin recording
- Ask questions (from interview guide)
- Turn off the recording device
- Ask if they are willing to fill out my demographic questionnaire
- Collect questionnaire and, without looking at the answers, place in same folder as signed consent form
- Thank them and depart
A note on remote interviewing: Interviews have traditionally been conducted face-to-face in a private or quiet public setting. You don’t want a lot of background noise, as this will make transcriptions difficult. During the recent global pandemic, many interviewers, myself included, learned the benefits of interviewing remotely. Although face-to-face is still preferable for many reasons, Zoom interviewing is not a bad alternative, and it does allow more interviews across great distances. Zoom also includes automatic transcription, which significantly cuts down on the time it normally takes to convert our conversations into “data” to be analyzed. These automatic transcriptions are not perfect, however, and you will still need to listen to the recording and clarify and clean up the transcription. Nor do automatic transcriptions include notations of body language or change of tone, which you may want to include. When interviewing remotely, you will want to collect the consent form before you meet: ask them to read, sign, and return it as an email attachment. I think it is better to ask for the demographic questionnaire after the interview, but because some respondents may never return it then, it is probably best to ask for this at the same time as the consent form, in advance of the interview.
What should you bring to the interview? I would recommend bringing two copies of the consent form (one for you and one for the respondent), a demographic questionnaire, a manila folder in which to place the signed consent form and filled-out demographic questionnaire, a printed copy of your interview guide (I print with three-inch right margins so I can jot down notes on the page next to relevant questions), a pen, a recording device, and water.
After the interview, you will want to secure the signed consent form in a locked filing cabinet (if in print) or a password-protected folder on your computer. Using Excel or a similar program that allows tables/spreadsheets, create an identifying number for your interview that links to the consent form without using the name of your respondent. For example, let’s say that I conduct interviews with US politicians, and the first person I meet with is George W. Bush. I will assign the transcription the number “INT#001” and add it to the signed consent form. [3] The signed consent form goes into a locked filing cabinet, and I never use the name “George W. Bush” again. I take the information from the demographic sheet, open my Excel spreadsheet, and add the relevant information in separate columns for the row INT#001: White, male, Republican. When I interview Bill Clinton as my second interview, I include a second row: INT#002: White, male, Democrat. And so on. The only link to the actual name of the respondent and this information is the fact that the consent form (unavailable to anyone but me) has stamped on it the interview number.
Many students get very nervous before their first interview. Actually, many of us are always nervous before the interview! But do not worry—this is normal, and it does pass. Chances are, you will be pleasantly surprised at how comfortable it begins to feel. These “purposeful conversations” are often a delight for both participants. This is not to say that sometimes things go wrong. I often have my students practice several “bad scenarios” (e.g., a respondent that you cannot get to open up; a respondent who is too talkative and dominates the conversation, steering it away from the topics you are interested in; emotions that completely take over; or shocking disclosures you are ill-prepared to handle), but most of the time, things go quite well. Be prepared for the unexpected, but know that the reason interviews are so popular as a technique of data collection is that they are usually richly rewarding for both participants.
One thing that I stress to my methods students and remind myself about is that interviews are still conversations between people. If there’s something you might feel uncomfortable asking someone about in a “normal” conversation, you will likely also feel a bit of discomfort asking it in an interview. Maybe more importantly, your respondent may feel uncomfortable. Social research—especially about inequality—can be uncomfortable. And it’s easy to slip into an abstract, intellectualized, or removed perspective as an interviewer. This is one reason trying out interview questions is important. Another is that sometimes the question sounds good in your head but doesn’t work as well out loud in practice. I learned this the hard way when a respondent asked me how I would answer the question I had just posed, and I realized that not only did I not really know how I would answer it, but I also wasn’t quite as sure I knew what I was asking as I had thought.
—Elizabeth M. Lee, Associate Professor of Sociology at Saint Joseph’s University, author of Class and Campus Life , and co-author of Geographies of Campus Inequality
How Many Interviews?
Your research design has included a targeted number of interviews and a recruitment plan (see chapter 5). Follow your plan, but remember that “ saturation ” is your goal. You interview as many people as you can until you reach a point at which you are no longer surprised by what they tell you. This means not that no one after your first twenty interviews will have surprising, interesting stories to tell you but rather that the picture you are forming about the phenomenon of interest to you from a research perspective has come into focus, and none of the interviews are substantially refocusing that picture. That is when you should stop collecting interviews. Note that to know when you have reached this, you will need to read your transcripts as you go. More about this in chapters 18 and 19.
Your Final Product: The Ideal Interview Transcript
A good interview transcript will demonstrate a subtly controlled conversation by the skillful interviewer. In general, you want to see replies that are about one paragraph long, not short sentences and not running on for several pages. Although it is sometimes necessary to follow respondents down tangents, it is also often necessary to pull them back to the questions that form the basis of your research study. This is not really a free conversation, although it may feel like that to the person you are interviewing.
Final Tips from an Interview Master
Annette Lareau is arguably one of the masters of the trade. In Listening to People , she provides several guidelines for good interviews and then offers a detailed example of an interview gone wrong and how it could be addressed (please see the “Further Readings” at the end of this chapter). Here is an abbreviated version of her set of guidelines: (1) interview respondents who are experts on the subjects of most interest to you (as a corollary, don’t ask people about things they don’t know); (2) listen carefully and talk as little as possible; (3) keep in mind what you want to know and why you want to know it; (4) be a proactive interviewer (subtly guide the conversation); (5) assure respondents that there aren’t any right or wrong answers; (6) use the respondent’s own words to probe further (this both allows you to accurately identify what you heard and pushes the respondent to explain further); (7) reuse effective probes (don’t reinvent the wheel as you go—if repeating the words back works, do it again and again); (8) focus on learning the subjective meanings that events or experiences have for a respondent; (9) don’t be afraid to ask a question that draws on your own knowledge (unlike trial lawyers who are trained never to ask a question for which they don’t already know the answer, sometimes it’s worth it to ask risky questions based on your hypotheses or just plain hunches); (10) keep thinking while you are listening (so difficult…and important); (11) return to a theme raised by a respondent if you want further information; (12) be mindful of power inequalities (and never ever coerce a respondent to continue the interview if they want out); (13) take control with overly talkative respondents; (14) expect overly succinct responses, and develop strategies for probing further; (15) balance digging deep and moving on; (16) develop a plan to deflect questions (e.g., let them know you are happy to answer any questions at the end of the interview, but you don’t want to take time away from them now); and at the end, (17) check to see whether you have asked all your questions. You don’t always have to ask everyone the same set of questions, but if there is a big area you have forgotten to cover, now is the time to recover ( Lareau 2021:93–103 ).
Sample: Demographic Questionnaire
ASA Taskforce on First-Generation and Working-Class Persons in Sociology – Class Effects on Career Success
Supplementary Demographic Questionnaire
Thank you for your participation in this interview project. We would like to collect a few pieces of key demographic information from you to supplement our analyses. Your answers to these questions will be kept confidential and stored by ID number. All of your responses here are entirely voluntary!
What best captures your race/ethnicity? (please check any/all that apply)
- White (Non Hispanic/Latina/o/x)
- Black or African American
- Hispanic, Latino/a/x of Spanish
- Asian or Asian American
- American Indian or Alaska Native
- Middle Eastern or North African
- Native Hawaiian or Pacific Islander
- Other : (Please write in: ________________)
What is your current position?
- Grad Student
- Full Professor
Please check any and all of the following that apply to you:
- I identify as a working-class academic
- I was the first in my family to graduate from college
- I grew up poor
What best reflects your gender?
- Transgender female/Transgender woman
- Transgender male/Transgender man
- Gender queer/ Gender nonconforming
Anything else you would like us to know about you?
Example: Interview Guide
In this example, follow-up prompts are italicized. Note the sequence of questions. That second question often elicits an entire life history , answering several later questions in advance.
Introduction Script/Question
Thank you for participating in our survey of ASA members who identify as first-generation or working-class. As you may have heard, ASA has sponsored a taskforce on first-generation and working-class persons in sociology and we are interested in hearing from those who so identify. Your participation in this interview will help advance our knowledge in this area.
- The first thing we would like to as you is why you have volunteered to be part of this study? What does it mean to you be first-gen or working class? Why were you willing to be interviewed?
- How did you decide to become a sociologist?
- Can you tell me a little bit about where you grew up? ( prompts: what did your parent(s) do for a living? What kind of high school did you attend?)
- Has this identity been salient to your experience? (how? How much?)
- How welcoming was your grad program? Your first academic employer?
- Why did you decide to pursue sociology at the graduate level?
- Did you experience culture shock in college? In graduate school?
- Has your FGWC status shaped how you’ve thought about where you went to school? debt? etc?
- Were you mentored? How did this work (not work)? How might it?
- What did you consider when deciding where to go to grad school? Where to apply for your first position?
- What, to you, is a mark of career success? Have you achieved that success? What has helped or hindered your pursuit of success?
- Do you think sociology, as a field, cares about prestige?
- Let’s talk a little bit about intersectionality. How does being first-gen/working class work alongside other identities that are important to you?
- What do your friends and family think about your career? Have you had any difficulty relating to family members or past friends since becoming highly educated?
- Do you have any debt from college/grad school? Are you concerned about this? Could you explain more about how you paid for college/grad school? (here, include assistance from family, fellowships, scholarships, etc.)
- (You’ve mentioned issues or obstacles you had because of your background.) What could have helped? Or, who or what did? Can you think of fortuitous moments in your career?
- Do you have any regrets about the path you took?
- Is there anything else you would like to add? Anything that the Taskforce should take note of, that we did not ask you about here?
Further Readings
Britten, Nicky. 1995. “Qualitative Interviews in Medical Research.” BMJ: British Medical Journal 31(6999):251–253. A good basic overview of interviewing particularly useful for students of public health and medical research generally.
Corbin, Juliet, and Janice M. Morse. 2003. “The Unstructured Interactive Interview: Issues of Reciprocity and Risks When Dealing with Sensitive Topics.” Qualitative Inquiry 9(3):335–354. Weighs the potential benefits and harms of conducting interviews on topics that may cause emotional distress. Argues that the researcher’s skills and code of ethics should ensure that the interviewing process provides more of a benefit to both participant and researcher than a harm to the former.
Gerson, Kathleen, and Sarah Damaske. 2020. The Science and Art of Interviewing . New York: Oxford University Press. A useful guidebook/textbook for both undergraduates and graduate students, written by sociologists.
Kvale, Steiner. 2007. Doing Interviews . London: SAGE. An easy-to-follow guide to conducting and analyzing interviews by psychologists.
Lamont, Michèle, and Ann Swidler. 2014. “Methodological Pluralism and the Possibilities and Limits of Interviewing.” Qualitative Sociology 37(2):153–171. Written as a response to various debates surrounding the relative value of interview-based studies and ethnographic studies defending the particular strengths of interviewing. This is a must-read article for anyone seriously engaging in qualitative research!
Pugh, Allison J. 2013. “What Good Are Interviews for Thinking about Culture? Demystifying Interpretive Analysis.” American Journal of Cultural Sociology 1(1):42–68. Another defense of interviewing written against those who champion ethnographic methods as superior, particularly in the area of studying culture. A classic.
Rapley, Timothy John. 2001. “The ‘Artfulness’ of Open-Ended Interviewing: Some considerations in analyzing interviews.” Qualitative Research 1(3):303–323. Argues for the importance of “local context” of data production (the relationship built between interviewer and interviewee, for example) in properly analyzing interview data.
Weiss, Robert S. 1995. Learning from Strangers: The Art and Method of Qualitative Interview Studies . New York: Simon and Schuster. A classic and well-regarded textbook on interviewing. Because Weiss has extensive experience conducting surveys, he contrasts the qualitative interview with the survey questionnaire well; particularly useful for those trained in the latter.
- I say “normally” because how people understand their various identities can itself be an expansive topic of inquiry. Here, I am merely talking about collecting otherwise unexamined demographic data, similar to how we ask people to check boxes on surveys. ↵
- Again, this applies to “semistructured in-depth interviewing.” When conducting standardized questionnaires, you will want to ask each question exactly as written, without deviations! ↵
- I always include “INT” in the number because I sometimes have other kinds of data with their own numbering: FG#001 would mean the first focus group, for example. I also always include three-digit spaces, as this allows for up to 999 interviews (or, more realistically, allows for me to interview up to one hundred persons without having to reset my numbering system). ↵
A method of data collection in which the researcher asks the participant questions; the answers to these questions are often recorded and transcribed verbatim. There are many different kinds of interviews - see also semistructured interview , structured interview , and unstructured interview .
A document listing key questions and question areas for use during an interview. It is used most often for semi-structured interviews. A good interview guide may have no more than ten primary questions for two hours of interviewing, but these ten questions will be supplemented by probes and relevant follow-ups throughout the interview. Most IRBs require the inclusion of the interview guide in applications for review. See also interview and semi-structured interview .
A data-collection method that relies on casual, conversational, and informal interviewing. Despite its apparent conversational nature, the researcher usually has a set of particular questions or question areas in mind but allows the interview to unfold spontaneously. This is a common data-collection technique among ethnographers. Compare to the semi-structured or in-depth interview .
A form of interview that follows a standard guide of questions asked, although the order of the questions may change to match the particular needs of each individual interview subject, and probing “follow-up” questions are often added during the course of the interview. The semi-structured interview is the primary form of interviewing used by qualitative researchers in the social sciences. It is sometimes referred to as an “in-depth” interview. See also interview and interview guide .
The cluster of data-collection tools and techniques that involve observing interactions between people, the behaviors, and practices of individuals (sometimes in contrast to what they say about how they act and behave), and cultures in context. Observational methods are the key tools employed by ethnographers and Grounded Theory .
Follow-up questions used in a semi-structured interview to elicit further elaboration. Suggested prompts can be included in the interview guide to be used/deployed depending on how the initial question was answered or if the topic of the prompt does not emerge spontaneously.
A form of interview that follows a strict set of questions, asked in a particular order, for all interview subjects. The questions are also the kind that elicits short answers, and the data is more “informative” than probing. This is often used in mixed-methods studies, accompanying a survey instrument. Because there is no room for nuance or the exploration of meaning in structured interviews, qualitative researchers tend to employ semi-structured interviews instead. See also interview.
The point at which you can conclude data collection because every person you are interviewing, the interaction you are observing, or content you are analyzing merely confirms what you have already noted. Achieving saturation is often used as the justification for the final sample size.
An interview variant in which a person’s life story is elicited in a narrative form. Turning points and key themes are established by the researcher and used as data points for further analysis.
Introduction to Qualitative Research Methods Copyright © 2023 by Allison Hurst is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License , except where otherwise noted.
Qualitative Interviewing
- Reference work entry
- First Online: 13 January 2019
- Cite this reference work entry

- Sally Nathan 2 ,
- Christy Newman 3 &
- Kari Lancaster 3
4118 Accesses
20 Citations
8 Altmetric
Qualitative interviewing is a foundational method in qualitative research and is widely used in health research and the social sciences. Both qualitative semi-structured and in-depth unstructured interviews use verbal communication, mostly in face-to-face interactions, to collect data about the attitudes, beliefs, and experiences of participants. Interviews are an accessible, often affordable, and effective method to understand the socially situated world of research participants. The approach is typically informed by an interpretive framework where the data collected is not viewed as evidence of the truth or reality of a situation or experience but rather a context-bound subjective insight from the participants. The researcher needs to be open to new insights and to privilege the participant’s experience in data collection. The data from qualitative interviews is not generalizable, but its exploratory nature permits the collection of rich data which can answer questions about which little is already known. This chapter introduces the reader to qualitative interviewing, the range of traditions within which interviewing is utilized as a method, and highlights the advantages and some of the challenges and misconceptions in its application. The chapter also provides practical guidance on planning and conducting interview studies. Three case examples are presented to highlight the benefits and risks in the use of interviewing with different participants, providing situated insights as well as advice about how to go about learning to interview if you are a novice.
This is a preview of subscription content, log in via an institution to check access.
Access this chapter
- Available as PDF
- Read on any device
- Instant download
- Own it forever
- Available as EPUB and PDF
- Durable hardcover edition
- Dispatched in 3 to 5 business days
- Free shipping worldwide - see info
Tax calculation will be finalised at checkout
Purchases are for personal use only
Institutional subscriptions
Baez B. Confidentiality in qualitative research: reflections on secrets, power and agency. Qual Res. 2002;2(1):35–58. https://doi.org/10.1177/1468794102002001638 .
Article Google Scholar
Braun V, Clarke V. Successful qualitative research: a practical guide for beginners. London: Sage Publications; 2013.
Google Scholar
Braun V, Clarke V, Gray D. Collecting qualitative data: a practical guide to textual, media and virtual techniques. Cambridge: Cambridge University Press; 2017.
Book Google Scholar
Bryman A. Social research methods. 5th ed. Oxford: Oxford University Press; 2016.
Crotty M. The foundations of social research: meaning and perspective in the research process. Australia: Allen & Unwin; 1998.
Davies MB. Doing a successful research project: using qualitative or quantitative methods. New York: Palgrave MacMillan; 2007.
Dickson-Swift V, James EL, Liamputtong P. Undertaking sensitive research in the health and social sciences. Cambridge: Cambridge University Press; 2008.
Foster M, Nathan S, Ferry M. The experience of drug-dependent adolescents in a therapeutic community. Drug Alcohol Rev. 2010;29(5):531–9.
Gillham B. The research interview. London: Continuum; 2000.
Glaser B, Strauss A. The discovery of grounded theory: strategies for qualitative research. Chicago: Aldine Publishing Company; 1967.
Hesse-Biber SN, Leavy P. In-depth interview. In: The practice of qualitative research. 2nd ed. Thousand Oaks: Sage Publications; 2011. p. 119–47
Irvine A. Duration, dominance and depth in telephone and face-to-face interviews: a comparative exploration. Int J Qual Methods. 2011;10(3):202–20.
Johnson JM. In-depth interviewing. In: Gubrium JF, Holstein JA, editors. Handbook of interview research: context and method. Thousand Oaks: Sage Publications; 2001.
Kvale S. Interviews: an introduction to qualitative research interviewing. Thousand Oaks: Sage; 1996.
Kvale S. Doing interviews. London: Sage Publications; 2007.
Lancaster K. Confidentiality, anonymity and power relations in elite interviewing: conducting qualitative policy research in a politicised domain. Int J Soc Res Methodol. 2017;20(1):93–103. https://doi.org/10.1080/13645579.2015.1123555 .
Leavy P. Method meets art: arts-based research practice. New York: Guilford Publications; 2015.
Liamputtong P. Researching the vulnerable: a guide to sensitive research methods. Thousand Oaks: Sage Publications; 2007.
Liamputtong P. Qualitative research methods. 4th ed. South Melbourne: Oxford University Press; 2013.
Mays N, Pope C. Quality in qualitative health research. In: Pope C, Mays N, editors. Qualitative research in health care. London: BMJ Books; 2000. p. 89–102.
McLellan E, MacQueen KM, Neidig JL. Beyond the qualitative interview: data preparation and transcription. Field Methods. 2003;15(1):63–84. https://doi.org/10.1177/1525822x02239573 .
Minichiello V, Aroni R, Hays T. In-depth interviewing: principles, techniques, analysis. 3rd ed. Sydney: Pearson Education Australia; 2008.
Morris ZS. The truth about interviewing elites. Politics. 2009;29(3):209–17. https://doi.org/10.1111/j.1467-9256.2009.01357.x .
Nathan S, Foster M, Ferry M. Peer and sexual relationships in the experience of drug-dependent adolescents in a therapeutic community. Drug Alcohol Rev. 2011;30(4):419–27.
National Health and Medical Research Council. National statement on ethical conduct in human research. Canberra: Australian Government; 2007.
Neal S, McLaughlin E. Researching up? Interviews, emotionality and policy-making elites. J Soc Policy. 2009;38(04):689–707. https://doi.org/10.1017/S0047279409990018 .
O’Reilly M, Parker N. ‘Unsatisfactory saturation’: a critical exploration of the notion of saturated sample sizes in qualitative research. Qual Res. 2013;13(2):190–7. https://doi.org/10.1177/1468794112446106 .
Ostrander S. “Surely you're not in this just to be helpful”: access, rapport and interviews in three studies of elites. In: Hertz R, Imber J, editors. Studying elites using qualitative methods. Thousand Oaks: Sage Publications; 1995. p. 133–50.
Chapter Google Scholar
Patton M. Qualitative research & evaluation methods: integrating theory and practice. Thousand Oaks: Sage Publications; 2015.
Punch KF. Introduction to social research: quantitative and qualitative approaches. London: Sage; 2005.
Rhodes T, Bernays S, Houmoller K. Parents who use drugs: accounting for damage and its limitation. Soc Sci Med. 2010;71(8):1489–97. https://doi.org/10.1016/j.socscimed.2010.07.028 .
Riessman CK. Narrative analysis. London: Sage; 1993.
Ritchie J. Not everything can be reduced to numbers. In: Berglund C, editor. Health research. Melbourne: Oxford University Press; 2001. p. 149–73.
Rubin H, Rubin I. Qualitative interviewing: the art of hearing data. 2nd ed. Thousand Oaks: Sage Publications; 2012.
Serry T, Liamputtong P. The in-depth interviewing method in health. In: Liamputtong P, editor. Research methods in health: foundations for evidence-based practice. 3rd ed. South Melbourne: Oxford University Press; 2017. p. 67–83.
Silverman D. Doing qualitative research. 5th ed. London: Sage; 2017.
Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (coreq): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–57. https://doi.org/10.1093/intqhc/mzm042 .
Download references
Author information
Authors and affiliations.
School of Public Health and Community Medicine, Faculty of Medicine, UNSW, Sydney, NSW, Australia
Sally Nathan
Centre for Social Research in Health, Faculty of Arts and Social Sciences, UNSW, Sydney, NSW, Australia
Christy Newman & Kari Lancaster
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Sally Nathan .
Editor information
Editors and affiliations.
School of Science and Health, Western Sydney University, Penrith, NSW, Australia
Pranee Liamputtong
Rights and permissions
Reprints and permissions
Copyright information
© 2019 Springer Nature Singapore Pte Ltd.
About this entry
Cite this entry.
Nathan, S., Newman, C., Lancaster, K. (2019). Qualitative Interviewing. In: Liamputtong, P. (eds) Handbook of Research Methods in Health Social Sciences. Springer, Singapore. https://doi.org/10.1007/978-981-10-5251-4_77
Download citation
DOI : https://doi.org/10.1007/978-981-10-5251-4_77
Published : 13 January 2019
Publisher Name : Springer, Singapore
Print ISBN : 978-981-10-5250-7
Online ISBN : 978-981-10-5251-4
eBook Packages : Social Sciences Reference Module Humanities and Social Sciences Reference Module Business, Economics and Social Sciences
Share this entry
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Publish with us
Policies and ethics
- Find a journal
- Track your research
Have a language expert improve your writing
Run a free plagiarism check in 10 minutes, automatically generate references for free.
- Knowledge Base
- Methodology
- Types of Interviews in Research | Guide & Examples
Types of Interviews in Research | Guide & Examples
Published on 4 May 2022 by Tegan George . Revised on 10 October 2022.
An interview is a qualitative research method that relies on asking questions in order to collect data . Interviews involve two or more people, one of whom is the interviewer asking the questions.
There are several types of interviews, often differentiated by their level of structure. Structured interviews have predetermined questions asked in a predetermined order. Unstructured interviews are more free-flowing, and semi-structured interviews fall in between.
Interviews are commonly used in market research, social science, and ethnographic research.
Table of contents
What is a structured interview, what is a semi-structured interview, what is an unstructured interview, what is a focus group, examples of interview questions, advantages and disadvantages of interviews, frequently asked questions about types of interviews.
Structured interviews have predetermined questions in a set order. They are often closed-ended, featuring dichotomous (yes/no) or multiple-choice questions. While open-ended structured interviews exist, they are much less common. The types of questions asked make structured interviews a predominantly quantitative tool.
Asking set questions in a set order can help you see patterns among responses, and it allows you to easily compare responses between participants while keeping other factors constant. This can mitigate biases and lead to higher reliability and validity. However, structured interviews can be overly formal, as well as limited in scope and flexibility.
- You feel very comfortable with your topic. This will help you formulate your questions most effectively.
- You have limited time or resources. Structured interviews are a bit more straightforward to analyse because of their closed-ended nature, and can be a doable undertaking for an individual.
- Your research question depends on holding environmental conditions between participants constant
Prevent plagiarism, run a free check.
Semi-structured interviews are a blend of structured and unstructured interviews. While the interviewer has a general plan for what they want to ask, the questions do not have to follow a particular phrasing or order.
Semi-structured interviews are often open-ended, allowing for flexibility, but follow a predetermined thematic framework, giving a sense of order. For this reason, they are often considered ‘the best of both worlds’.
However, if the questions differ substantially between participants, it can be challenging to look for patterns, lessening the generalisability and validity of your results.
- You have prior interview experience. It’s easier than you think to accidentally ask a leading question when coming up with questions on the fly. Overall, spontaneous questions are much more difficult than they may seem.
- Your research question is exploratory in nature. The answers you receive can help guide your future research.
An unstructured interview is the most flexible type of interview. The questions and the order in which they are asked are not set. Instead, the interview can proceed more spontaneously, based on the participant’s previous answers.
Unstructured interviews are by definition open-ended. This flexibility can help you gather detailed information on your topic, while still allowing you to observe patterns between participants.
However, so much flexibility means that they can be very challenging to conduct properly. You must be very careful not to ask leading questions, as biased responses can lead to lower reliability or even invalidate your research.
- You have a solid background in your research topic and have conducted interviews before
- Your research question is exploratory in nature, and you are seeking descriptive data that will deepen and contextualise your initial hypotheses
- Your research necessitates forming a deeper connection with your participants, encouraging them to feel comfortable revealing their true opinions and emotions
A focus group brings together a group of participants to answer questions on a topic of interest in a moderated setting. Focus groups are qualitative in nature and often study the group’s dynamic and body language in addition to their answers. Responses can guide future research on consumer products and services, human behaviour, or controversial topics.
Focus groups can provide more nuanced and unfiltered feedback than individual interviews and are easier to organise than experiments or large surveys. However, their small size leads to low external validity and the temptation as a researcher to ‘cherry-pick’ responses that fit your hypotheses.
- Your research focuses on the dynamics of group discussion or real-time responses to your topic
- Your questions are complex and rooted in feelings, opinions, and perceptions that cannot be answered with a ‘yes’ or ‘no’
- Your topic is exploratory in nature, and you are seeking information that will help you uncover new questions or future research ideas
Depending on the type of interview you are conducting, your questions will differ in style, phrasing, and intention. Structured interview questions are set and precise, while the other types of interviews allow for more open-endedness and flexibility.
Here are some examples.
- Semi-structured
- Unstructured
- Focus group
- Do you like dogs? Yes/No
- Do you associate dogs with feeling: happy; somewhat happy; neutral; somewhat unhappy; unhappy
- If yes, name one attribute of dogs that you like.
- If no, name one attribute of dogs that you don’t like.
- What feelings do dogs bring out in you?
- When you think more deeply about this, what experiences would you say your feelings are rooted in?
Interviews are a great research tool. They allow you to gather rich information and draw more detailed conclusions than other research methods, taking into consideration nonverbal cues, off-the-cuff reactions, and emotional responses.
However, they can also be time-consuming and deceptively challenging to conduct properly. Smaller sample sizes can cause their validity and reliability to suffer, and there is an inherent risk of interviewer effect arising from accidentally leading questions.
Here are some advantages and disadvantages of each type of interview that can help you decide if you’d like to utilise this research method.
The four most common types of interviews are:
- Structured interviews : The questions are predetermined in both topic and order.
- Semi-structured interviews : A few questions are predetermined, but other questions aren’t planned.
- Unstructured interviews : None of the questions are predetermined.
- Focus group interviews : The questions are presented to a group instead of one individual.
A structured interview is a data collection method that relies on asking questions in a set order to collect data on a topic. They are often quantitative in nature. Structured interviews are best used when:
- You already have a very clear understanding of your topic. Perhaps significant research has already been conducted, or you have done some prior research yourself, but you already possess a baseline for designing strong structured questions.
- You are constrained in terms of time or resources and need to analyse your data quickly and efficiently
- Your research question depends on strong parity between participants, with environmental conditions held constant
More flexible interview options include semi-structured interviews , unstructured interviews , and focus groups .
A semi-structured interview is a blend of structured and unstructured types of interviews. Semi-structured interviews are best used when:
- You have prior interview experience. Spontaneous questions are deceptively challenging, and it’s easy to accidentally ask a leading question or make a participant uncomfortable.
- Your research question is exploratory in nature. Participant answers can guide future research questions and help you develop a more robust knowledge base for future research.
An unstructured interview is the most flexible type of interview, but it is not always the best fit for your research topic.
Unstructured interviews are best used when:
- You are an experienced interviewer and have a very strong background in your research topic, since it is challenging to ask spontaneous, colloquial questions
- Your research question is exploratory in nature. While you may have developed hypotheses, you are open to discovering new or shifting viewpoints through the interview process.
- You are seeking descriptive data, and are ready to ask questions that will deepen and contextualise your initial thoughts and hypotheses
- Your research depends on forming connections with your participants and making them feel comfortable revealing deeper emotions, lived experiences, or thoughts
The interviewer effect is a type of bias that emerges when a characteristic of an interviewer (race, age, gender identity, etc.) influences the responses given by the interviewee.
There is a risk of an interviewer effect in all types of interviews , but it can be mitigated by writing really high-quality interview questions.
Cite this Scribbr article
If you want to cite this source, you can copy and paste the citation or click the ‘Cite this Scribbr article’ button to automatically add the citation to our free Reference Generator.
George, T. (2022, October 10). Types of Interviews in Research | Guide & Examples. Scribbr. Retrieved 6 May 2024, from https://www.scribbr.co.uk/research-methods/types-of-interviews/
Is this article helpful?

Tegan George
Other students also liked, data collection methods | step-by-step guide & examples, face validity | guide with definition & examples, construct validity | definition, types, & examples.
- Harvard Library
- Research Guides
- Faculty of Arts & Sciences Libraries
Library Support for Qualitative Research
- Interview Research
- Resources for Methodology
- Remote Research & Virtual Fieldwork
Resources for Research Interviewing
Nih-funded qualitative research.
- Oral History
- Data Management & Repositories
- Campus Access
Types of Interviews
- Engaging Participants
Interview Questions
- Conducting Interviews
- Transcription
- Coding and Analysis
- Managing & Finding Interview Data
- UX & Market Research Interviews
Textbooks, Guidebooks, and Handbooks
- The Ethnographic Interview by James P. Spradley “Spradley wrote this book for the professional and student who have never done ethnographic fieldwork (p. 231) and for the professional ethnographer who is interested in adapting the author’s procedures (p. iv). Part 1 outlines in 3 chapters Spradley’s version of ethnographic research, and it provides the background for Part 2 which consists of 12 guided steps (chapters) ranging from locating and interviewing an informant to writing an ethnography. Most of the examples come from the author’s own fieldwork among U.S. subcultures . . . Steps 6 and 8 explain lucidly how to construct a domain and a taxonomic analysis” (excerpted from book review by James D. Sexton, 1980).
- Fundamentals of Qualitative Research by Johnny Saldana (Series edited by Patricia Leavy) Provides a soup-to-nuts overview of the qualitative data collection process, including interviewing, participant observation, and other methods.
- InterViews by Steinar Kvale Interviewing is an essential tool in qualitative research and this introduction to interviewing outlines both the theoretical underpinnings and the practical aspects of the process. After examining the role of the interview in the research process, Steinar Kvale considers some of the key philosophical issues relating to interviewing: the interview as conversation, hermeneutics, phenomenology, concerns about ethics as well as validity, and postmodernism. Having established this framework, the author then analyzes the seven stages of the interview process - from designing a study to writing it up.
- Practical Evaluation by Michael Quinn Patton Surveys different interviewing strategies, from, a) informal/conversational, to b) interview guide approach, to c) standardized and open-ended, to d) closed/quantitative. Also discusses strategies for wording questions that are open-ended, clear, sensitive, and neutral, while supporting the speaker. Provides suggestions for probing and maintaining control of the interview process, as well as suggestions for recording and transcription.
- The SAGE Handbook of Interview Research by Amir B. Marvasti (Editor); James A. Holstein (Editor); Jaber F. Gubrium (Editor); Karyn D. McKinney (Editor) The new edition of this landmark volume emphasizes the dynamic, interactional, and reflexive dimensions of the research interview. Contributors highlight the myriad dimensions of complexity that are emerging as researchers increasingly frame the interview as a communicative opportunity as much as a data-gathering format. The book begins with the history and conceptual transformations of the interview, which is followed by chapters that discuss the main components of interview practice. Taken together, the contributions to The SAGE Handbook of Interview Research: The Complexity of the Craft encourage readers simultaneously to learn the frameworks and technologies of interviewing and to reflect on the epistemological foundations of the interview craft.
- The SAGE Handbook of Online Research Methods by Nigel G. Fielding, Raymond M. Lee and Grant Blank (Editors) Bringing together the leading names in both qualitative and quantitative online research, this new edition is organised into nine sections: 1. Online Research Methods 2. Designing Online Research 3. Online Data Capture and Data Collection 4. The Online Survey 5. Digital Quantitative Analysis 6. Digital Text Analysis 7. Virtual Ethnography 8. Online Secondary Analysis: Resources and Methods 9. The Future of Online Social Research
ONLINE RESOURCES, COMMUNITIES, AND DATABASES
- Interviews as a Method for Qualitative Research (video) This short video summarizes why interviews can serve as useful data in qualitative research.
- Companion website to Bloomberg and Volpe's Completing Your Qualitative Dissertation: A Road Map from Beginning to End, 4th ed Provides helpful templates and appendices featured in the book, as well as links to other useful dissertation resources.
- International Congress of Qualitative Inquiry Annual conference hosted by the International Center for Qualitative Inquiry at the University of Illinois at Urbana-Champaign, which aims to facilitate the development of qualitative research methods across a wide variety of academic disciplines, among other initiatives.
- METHODSPACE An online home of the research methods community, where practicing researchers share how to make research easier.
- SAGE researchmethods Researchers can explore methods concepts to help them design research projects, understand particular methods or identify a new method, conduct their research, and write up their findings. A "methods map" facilitates finding content on methods.
The decision to conduct interviews, and the type of interviewing to use, should flow from, or align with, the methodological paradigm chosen for your study, whether that paradigm is interpretivist, critical, positivist, or participative in nature (or a combination of these).
Structured:
- Structured Interview. Entry in The SAGE Encyclopedia of Social Science Research Methodsby Floyd J. Fowler Jr., Editors: Michael S. Lewis-Beck; Alan E. Bryman; Tim Futing Liao (Editor) A concise article noting standards, procedures, and recommendations for developing and testing structured interviews. For an example of structured interview questions, you may view the Current Population Survey, May 2008: Public Participation in the Arts Supplement (ICPSR 29641), Apr 15, 2011 at https://doi.org/10.3886/ICPSR29641.v1 (To see the survey questions, preview the user guide, which can be found under the "Data and Documentation" tab. Then, look for page 177 (attachment 8).
Semi-Structured:
- Semi-Structured Interview. Entry in The SAGE Encyclopedia of Qualitative Research Methodsby Lioness Ayres; Editor: Lisa M. Given The semi-structured interview is a qualitative data collection strategy in which the researcher asks informants a series of predetermined but open-ended questions. The researcher has more control over the topics of the interview than in unstructured interviews, but in contrast to structured interviews or questionnaires that use closed questions, there is no fixed range of responses to each question.
Unstructured:
- Unstructured Interview. Entry in The SAGE Encyclopedia of Qualitative Research Methodsby Michael W. Firmin; Editor: Lisa M. Given Unstructured interviews in qualitative research involve asking relatively open-ended questions of research participants in order to discover their percepts on the topic of interest. Interviews, in general, are a foundational means of collecting data when using qualitative research methods. They are designed to draw from the interviewee constructs embedded in his or her thinking and rationale for decision making. The researcher uses an inductive method in data gathering, regardless of whether the interview method is open, structured, or semi-structured. That is, the researcher does not wish to superimpose his or her own viewpoints onto the person being interviewed. Rather, inductively, the researcher wishes to understand the participant's perceptions, helping him or her to articulate percepts such that they will be understood clearly by the journal reader.
Genres and Uses
Focus groups:.
- "Focus Groups." Annual Review of Sociology 22 (1996): 129-1524.by David L. Morgan Discusses the use of focus groups and group interviews as methods for gathering qualitative data used by sociologists and other academic and applied researchers. Focus groups are recommended for giving voice to marginalized groups and revealing the group effect on opinion formation.
- Qualitative Research Methods: A Data Collector's Field Guide (See Module 4: "Focus Groups")by Mack, N., et al. This field guide is based on an approach to doing team-based, collaborative qualitative research that has repeatedly proven successful in research projects sponsored by Family Health International (FHI) throughout the developing world. With its straightforward delivery of information on the main qualitative methods being used in public health research today, the guide speaks to the need for simple yet effective instruction on how to do systematic and ethically sound qualitative research. The aim of the guide is thus practical. In bypassing extensive discussion on the theoretical underpinnings of qualitative research, it distinguishes itself as a how-to guide to be used in the field.
In-Depth (typically One-on-One):
- A Practical Introduction to in-Depth Interviewingby Alan Morris Are you new to qualitative research or a bit rusty and in need of some inspiration? Are you doing a research project involving in-depth interviews? Are you nervous about carrying out your interviews? This book will help you complete your qualitative research project by providing a nuts and bolts introduction to interviewing. With coverage of ethics, preparation strategies and advice for handling the unexpected in the field, this handy guide will help you get to grips with the basics of interviewing before embarking on your research. While recognising that your research question and the context of your research will drive your approach to interviewing, this book provides practical advice often skipped in traditional methods textbooks.
- Qualitative Research Methods: A Data Collector's Field Guide (See Module 3: "In-Depth Interviews")by Mack, N., et al. This field guide is based on an approach to doing team-based, collaborative qualitative research that has repeatedly proven successful in research projects sponsored by Family Health International (FHI) throughout the developing world. With its straightforward delivery of information on the main qualitative methods being used in public health research today, the guide speaks to the need for simple yet effective instruction on how to do systematic and ethically sound qualitative research. The aim of the guide is thus practical. In bypassing extensive discussion on the theoretical underpinnings of qualitative research, it distinguishes itself as a how-to guide to be used in the field.
Folklore Research and Oral Histories:
In addition to the following resource, see the Oral History page of this guide for helpful resources on Oral History interviewing.
American Folklife Center at the Library of Congress. Folklife and Fieldwork: A Layman’s Introduction to Field Techniques Interviews gathered for purposes of folklore research are similar to standard social science interviews in some ways, but also have a good deal in common with oral history approaches to interviewing. The focus in a folklore research interview is on documenting and trying to understand the interviewee's way of life relative to a culture or subculture you are studying. This guide includes helpful advice and tips for conducting fieldwork in folklore, such as tips for planning, conducting, recording, and archiving interviews.
An interdisciplinary scientific program within the Institute for Quantitative Social Science which encourages and facilitates research and instruction in the theory and practice of survey research. The primary mission of PSR is to provide survey research resources to enhance the quality of teaching and research at Harvard.
- Internet, Phone, Mail, and Mixed-Mode Surveysby Don A. Dillman; Jolene D. Smyth; Leah Melani Christian The classic survey design reference, updated for the digital age. The new edition is thoroughly updated and revised, and covers all aspects of survey research. It features expanded coverage of mobile phones, tablets, and the use of do-it-yourself surveys, and Dillman's unique Tailored Design Method is also thoroughly explained. This new edition is complemented by copious examples within the text and accompanying website. It includes: Strategies and tactics for determining the needs of a given survey, how to design it, and how to effectively administer it. How and when to use mail, telephone, and Internet surveys to maximum advantage. Proven techniques to increase response rates. Guidance on how to obtain high-quality feedback from mail, electronic, and other self-administered surveys. Direction on how to construct effective questionnaires, including considerations of layout. The effects of sponsorship on the response rates of surveys. Use of capabilities provided by newly mass-used media: interactivity, presentation of aural and visual stimuli. The Fourth Edition reintroduces the telephone--including coordinating land and mobile.
User Experience (UX) and Marketing:
- See the "UX & Market Research Interviews" tab on this guide, above. May include Focus Groups, above.
Screening for Research Site Selection:
- Research interviews are used not only to furnish research data for theoretical analysis in the social sciences, but also to plan other kinds of studies. For example, interviews may allow researchers to screen appropriate research sites to conduct empirical studies (such as randomized controlled trials) in a variety of fields, from medicine to law. In contrast to interviews conducted in the course of social research, such interviews do not typically serve as the data for final analysis and publication.
ENGAGING PARTICIPANTS
Research ethics .
- Human Subjects (IRB) The Committee on the Use of Human Subjects (CUHS) serves as the Institutional Review Board for the University area which includes the Cambridge and Allston campuses at Harvard. Find your IRB contact person , or learn about required ethics training. You may also find the IRB Lifecycle Guide helpful. This is the preferred IRB portal for Harvard graduate students and other researchers. IRB forms can be downloaded via the ESTR Library (click on the "Templates and Forms" tab, then navigate to pages 2 and 3 to find the documents labelled with “HUA” for the Harvard University Area IRB. Nota bene: You may use these forms only if you submit your study to the Harvard University IRB). The IRB office can be reached through email at [email protected] or by telephone at (617) 496-2847.
- Undergraduate Research Training Program (URTP) Portal The URTP at Harvard University is a comprehensive platform to create better prepared undergraduate researchers. The URTP is comprised of research ethics training sessions, a student-focused curriculum, and an online decision form that will assist students in determining whether their project requires IRB review. Students should examine the URTP's guide for student researchers: Introduction to Human Subjects Research Protection.
- Ethics reports From the Association of Internet Researchers (AoIR)
- Respect, Beneficence, and Justice: QDR General Guidance for Human Participants If you are hoping to share your qualitative interview data in a repository after it has been collected, you will need to plan accordingly via informed consent, careful de-identification procedures, and data access controls. Consider consulting with the Qualitative Research Support Group at Harvard Library and consulting with Harvard's Dataverse contacts to help you think through all of the contingencies and processes.
- "Conducting a Qualitative Child Interview: Methodological Considerations." Journal of Advanced Nursing 42/5 (2003): 434-441 by Kortesluoma, R., et al. The purpose of this article is to illustrate the theoretical premises of child interviewing, as well as to describe some practical methodological solutions used during interviews. Factors that influence data gathered from children and strategies for taking these factors into consideration during the interview are also described.
- "Crossing Cultural Barriers in Research Interviewing." Qualitative Social Work 63/3 (2007): 353-372 by Sands, R., et al. This article critically examines a qualitative research interview in which cultural barriers between a white non-Muslim female interviewer and an African American Muslim interviewee, both from the USA, became evident and were overcome within the same interview.
- Decolonizing Methodologies: Research and Indigenous Peoples by Linda Tuhiwai Smith This essential volume explores intersections of imperialism and research - specifically, the ways in which imperialism is embedded in disciplines of knowledge and tradition as 'regimes of truth.' Concepts such as 'discovery' and 'claiming' are discussed and an argument presented that the decolonization of research methods will help to reclaim control over indigenous ways of knowing and being. The text includes case-studies and examples, and sections on new indigenous literature and the role of research in indigenous struggles for social justice.
This resource, sponsored by University of Oregon Libraries, exemplifies the use of interviewing methodologies in research that foregrounds traditional knowledge. The methodology page summarizes the approach.
- Ethics: The Need to Tread Carefully. Chapter in A Practical Introduction to in-Depth Interviewing by Alan Morris Pay special attention to the sections in chapter 2 on "How to prevent and respond to ethical issues arising in the course of the interview," "Ethics in the writing up of your interviews," and "The Ethics of Care."
- Handbook on Ethical Issues in Anthropology by Joan Cassell (Editor); Sue-Ellen Jacobs (Editor) This publication of the American Anthropological Association presents and discusses issues and sources on ethics in anthropology, as well as realistic case studies of ethical dilemmas. It is meant to help social science faculty introduce discussions of ethics in their courses. Some of the topics are relevant to interviews, or at least to studies of which interviews are a part. See chapters 3 and 4 for cases, with solutions and commentary, respectively.
- Research Ethics from the Chanie Wenjack School for Indigenous Studies, Trent University (Open Access) An overview of Indigenous research ethics and protocols from the across the globe.
- Resources for Equity in Research Consult these resources for guidance on creating and incorporating equitable materials into public health research studies that entail community engagement.
The SAGE Handbook of Qualitative Research Ethics by Ron Iphofen (Editor); Martin Tolich (Editor) This handbook is a much-needed and in-depth review of the distinctive set of ethical considerations which accompanies qualitative research. This is particularly crucial given the emergent, dynamic and interactional nature of most qualitative research, which too often allows little time for reflection on the important ethical responsibilities and obligations. Contributions from leading international researchers have been carefully organized into six key thematic sections: Part One: Thick Descriptions Of Qualitative Research Ethics; Part Two: Qualitative Research Ethics By Technique; Part Three: Ethics As Politics; Part Four: Qualitative Research Ethics With Vulnerable Groups; Part Five: Relational Research Ethics; Part Six: Researching Digitally. This Handbook is a one-stop resource on qualitative research ethics across the social sciences that draws on the lessons learned and the successful methods for surmounting problems - the tried and true, and the new.
RESEARCH COMPLIANCE AND PRIVACY LAWS
Research Compliance Program for FAS/SEAS at Harvard : The Faculty of Arts and Sciences (FAS), including the School of Engineering and Applied Sciences (SEAS), and the Office of the Vice Provost for Research (OVPR) have established a shared Research Compliance Program (RCP). An area of common concern for interview studies is international projects and collaboration . RCP is a resource to provide guidance on which international activities may be impacted by US sanctions on countries, individuals, or entities and whether licenses or other disclosure are required to ship or otherwise share items, technology, or data with foreign collaborators.
- Harvard Global Support Services (GSS) is for students, faculty, staff, and researchers who are studying, researching, or working abroad. Their services span safety and security, health, culture, outbound immigration, employment, financial and legal matters, and research center operations. These include travel briefings and registration, emergency response, guidance on international projects, and managing in-country operations.
Generative AI: Harvard-affiliated researchers should not enter data classified as confidential ( Level 2 and above ), including non-public research data, into publicly-available generative AI tools, in accordance with the University’s Information Security Policy. Information shared with generative AI tools using default settings is not private and could expose proprietary or sensitive information to unauthorized parties.
Privacy Laws: Be mindful of any potential privacy laws that may apply wherever you conduct your interviews. The General Data Protection Regulation is a high-profile example (see below):
- General Data Protection Regulation (GDPR) This Regulation lays down rules relating to the protection of natural persons with regard to the processing of personal data and rules relating to the free movement of personal data. It protects fundamental rights and freedoms of natural persons and in particular their right to the protection of personal data. The free movement of personal data within the Union shall be neither restricted nor prohibited for reasons connected with the protection of natural persons with regard to the processing of personal data. For a nice summary of what the GDPR requires, check out the GDPR "crash course" here .
SEEKING CONSENT
If you would like to see examples of consent forms, ask your local IRB, or take a look at these resources:
- Model consent forms for oral history, suggested by the Centre for Oral History and Digital Storytelling at Concordia University
- For NIH-funded research, see this resource for developing informed consent language in research studies where data and/or biospecimens will be stored and shared for future use.
POPULATION SAMPLING
If you wish to assemble resources to aid in sampling, such as the USPS Delivery Sequence File, telephone books, or directories of organizations and listservs, please contact our data librarian or write to [email protected] .
- Research Randomizer A free web-based service that permits instant random sampling and random assignment. It also contains an interactive tutorial perfect for students taking courses in research methods.
- Practical Tools for Designing and Weighting Survey Samples by Richard Valliant; Jill A. Dever; Frauke Kreuter Survey sampling is fundamentally an applied field. The goal in this book is to put an array of tools at the fingertips of practitioners by explaining approaches long used by survey statisticians, illustrating how existing software can be used to solve survey problems, and developing some specialized software where needed. This book serves at least three audiences: (1) Students seeking a more in-depth understanding of applied sampling either through a second semester-long course or by way of a supplementary reference; (2) Survey statisticians searching for practical guidance on how to apply concepts learned in theoretical or applied sampling courses; and (3) Social scientists and other survey practitioners who desire insight into the statistical thinking and steps taken to design, select, and weight random survey samples. Several survey data sets are used to illustrate how to design samples, to make estimates from complex surveys for use in optimizing the sample allocation, and to calculate weights. Realistic survey projects are used to demonstrate the challenges and provide a context for the solutions. The book covers several topics that either are not included or are dealt with in a limited way in other texts. These areas include: sample size computations for multistage designs; power calculations related to surveys; mathematical programming for sample allocation in a multi-criteria optimization setting; nuts and bolts of area probability sampling; multiphase designs; quality control of survey operations; and statistical software for survey sampling and estimation. An associated R package, PracTools, contains a number of specialized functions for sample size and other calculations. The data sets used in the book are also available in PracTools, so that the reader may replicate the examples or perform further analyses.
- Sampling: Design and Analysis by Sharon L. Lohr Provides a modern introduction to the field of sampling. With a multitude of applications from a variety of disciplines, the book concentrates on the statistical aspects of taking and analyzing a sample. Overall, the book gives guidance on how to tell when a sample is valid or not, and how to design and analyze many different forms of sample surveys.
- Sampling Techniques by William G. Cochran Clearly demonstrates a wide range of sampling methods now in use by governments, in business, market and operations research, social science, medicine, public health, agriculture, and accounting. Gives proofs of all the theoretical results used in modern sampling practice. New topics in this edition include the approximate methods developed for the problem of attaching standard errors or confidence limits to nonlinear estimates made from the results of surveys with complex plans.
- "Understanding the Process of Qualitative Data Collection" in Chapter 13 (pp. 103–1162) of 30 Essential Skills for the Qualitative Researcher by John W. Creswell Provides practical "how-to" information for beginning researchers in the social, behavioral, and health sciences with many applied examples from research design, qualitative inquiry, and mixed methods.The skills presented in this book are crucial for a new qualitative researcher starting a qualitative project.
- Survey Methodology by Robert M. Groves; Floyd J. Fowler; Mick P. Couper; James M. Lepkowski; Eleanor Singer; Roger Tourangeau; Floyd J. Fowler coverage includes sampling frame evaluation, sample design, development of questionnaires, evaluation of questions, alternative modes of data collection, interviewing, nonresponse, post-collection processing of survey data, and practices for maintaining scientific integrity.
The way a qualitative researcher constructs and approaches interview questions should flow from, or align with, the methodological paradigm chosen for the study, whether that paradigm is interpretivist, critical, positivist, or participative in nature (or a combination of these).
Constructing Your Questions
Helpful texts:.
- "Developing Questions" in Chapter 4 (pp. 98–108) of Becoming Qualitative Researchers by Corrine Glesne Ideal for introducing the novice researcher to the theory and practice of qualitative research, this text opens students to the diverse possibilities within this inquiry approach, while helping them understand how to design and implement specific research methods.
- "Learning to Interview in the Social Sciences" Qualitative Inquiry, 9(4) 2003, 643–668 by Roulston, K., deMarrais, K., & Lewis, J. B. See especially the section on "Phrasing and Negotiating Questions" on pages 653-655 and common problems with framing questions noted on pages 659 - 660.
- Qualitative Research Interviewing: Biographic Narrative and Semi-Structured Methods (See sections on “Lightly and Heavily Structured Depth Interviewing: Theory-Questions and Interviewer-Questions” and “Preparing for any Interviewing Sequence") by Tom Wengraf Unique in its conceptual coherence and the level of practical detail, this book provides a comprehensive resource for those concerned with the practice of semi-structured interviewing, the most commonly used interview approach in social research, and in particular for in-depth, biographic narrative interviewing. It covers the full range of practices from the identification of topics through to strategies for writing up research findings in diverse ways.
- "Scripting a Qualitative Purpose Statement and Research Questions" in Chapter 12 (pp. 93–102) of 30 Essential Skills for the Qualitative Researcher by John W. Creswell Provides practical "how-to" information for beginning researchers in the social, behavioral, and health sciences with many applied examples from research design, qualitative inquiry, and mixed methods.The skills presented in this book are crucial for a new qualitative researcher starting a qualitative project.
- Some Strategies for Developing Interview Guides for Qualitative Interviews by Sociology Department, Harvard University Includes general advice for conducting qualitative interviews, pros and cons of recording and transcription, guidelines for success, and tips for developing and phrasing effective interview questions.
- Tip Sheet on Question Wording by Harvard University Program on Survey Research
Let Theory Guide You:
The quality of your questions depends on how you situate them within a wider body of knowledge. Consider the following advice:
A good literature review has many obvious virtues. It enables the investigator to define problems and assess data. It provides the concepts on which percepts depend. But the literature review has a special importance for the qualitative researcher. This consists of its ability to sharpen his or her capacity for surprise (Lazarsfeld, 1972b). The investigator who is well versed in the literature now has a set of expectations the data can defy. Counterexpectational data are conspicuous, readable, and highly provocative data. They signal the existence of unfulfilled theoretical assumptions, and these are, as Kuhn (1962) has noted, the very origins of intellectual innovation. A thorough review of the literature is, to this extent, a way to manufacture distance. It is a way to let the data of one's research project take issue with the theory of one's field.
McCracken, G. (1988), The Long Interview, Sage: Newbury Park, CA, p. 31
When drafting your interview questions, remember that everything follows from your central research question. Also, on the way to writing your "operationalized" interview questions, it's helpful to draft broader, intermediate questions, couched in theory. Nota bene: While it is important to know the literature well before conducting your interview(s), be careful not to present yourself to your research participant(s) as "the expert," which would be presumptuous and could be intimidating. Rather, the purpose of your knowledge is to make you a better, keener listener.
If you'd like to supplement what you learned about relevant theories through your coursework and literature review, try these sources:
- Annual Reviews Review articles sum up the latest research in many fields, including social sciences, biomedicine, life sciences, and physical sciences. These are timely collections of critical reviews written by leading scientists.
- HOLLIS - search for resources on theories in your field Modify this example search by entering the name of your field in place of "your discipline," then hit search.
- Oxford Bibliographies Written and reviewed by academic experts, every article in this database is an authoritative guide to the current scholarship in a variety of fields, containing original commentary and annotations.
- ProQuest Dissertations & Theses (PQDT) Indexes dissertations and masters' theses from most North American graduate schools as well as some European universities. Provides full text for most indexed dissertations from 1990-present.
- Very Short Introductions Launched by Oxford University Press in 1995, Very Short Introductions offer concise introductions to a diverse range of subjects from Climate to Consciousness, Game Theory to Ancient Warfare, Privacy to Islamic History, Economics to Literary Theory.
CONDUCTING INTERVIEWS
Equipment and software: .
- Lamont Library loans microphones and podcast starter kits, which will allow you to capture audio (and you may record with software, such as Garage Band).
- Cabot Library loans digital recording devices, as well as USB microphones.
If you prefer to use your own device, you may purchase a small handheld audio recorder, or use your cell phone.
- Audio Capture Basics (PDF) - Helpful instructions, courtesy of the Lamont Library Multimedia Lab.
- Getting Started with Podcasting/Audio: Guidelines from Harvard Library's Virtual Media Lab for preparing your interviewee for a web-based recording (e.g., podcast, interview)
- Camtasia Screen Recorder and Video Editor
- Zoom: Video Conferencing, Web Conferencing
- Visit the Multimedia Production Resources guide! Consult it to find and learn how to use audiovisual production tools, including: cameras, microphones, studio spaces, and other equipment at Cabot Science Library and Lamont Library.
- Try the virtual office hours offered by the Lamont Multimedia Lab!
TIPS FOR CONDUCTING INTERVIEWS
Quick handout: .
- Research Interviewing Tips (Courtesy of Dr. Suzanne Spreadbury)
Remote Interviews:
- For Online or Distant Interviews, See "Remote Research & Virtual Fieldwork" on this guide .
- Deborah Lupton's Bibliography: Doing Fieldwork in a Pandemic
Seeking Consent:
Books and articles: .
- "App-Based Textual Interviews: Interacting With Younger Generations in a Digitalized Social Reallity."International Journal of Social Research Methodology (12 June 2022). Discusses the use of texting platforms as a means to reach young people. Recommends useful question formulations for this medium.
- "Learning to Interview in the Social Sciences." Qualitative Inquiry, 9(4) 2003, 643–668 by Roulston, K., deMarrais, K., & Lewis, J. B. See especially the section on "Phrasing and Negotiating Questions" on pages 653-655 and common problems with framing questions noted on pages 659-660.
- "Slowing Down and Digging Deep: Teaching Students to Examine Interview Interaction in Depth." LEARNing Landscapes, Spring 2021 14(1) 153-169 by Herron, Brigette A. and Kathryn Roulston. Suggests analysis of videorecorded interviews as a precursor to formulating one's own questions. Includes helpful types of probes.
- Using Interviews in a Research Project by Nigel Joseph Mathers; Nicholas J Fox; Amanda Hunn; Trent Focus Group. A work pack to guide researchers in developing interviews in the healthcare field. Describes interview structures, compares face-to-face and telephone interviews. Outlines the ways in which different types of interview data can be analysed.
- “Working through Challenges in Doing Interview Research.” International Journal of Qualitative Methods, (December 2011), 348–66 by Roulston, Kathryn. The article explores (1) how problematic interactions identified in the analysis of focus group data can lead to modifications in research design, (2) an approach to dealing with reported data in representations of findings, and (3) how data analysis can inform question formulation in successive rounds of data generation. Findings from these types of examinations of interview data generation and analysis are valuable for informing both interview practice as well as research design.
Videos:

The way a qualitative researcher transcribes interviews should flow from, or align with, the methodological paradigm chosen for the study, whether that paradigm is interpretivist, critical, positivist, or participative in nature (or a combination of these).
TRANSCRIPTION
Before embarking on a transcription project, it's worthwhile to invest in the time and effort necessary to capture good audio, which will make the transcription process much easier. If you haven't already done so, check out the audio capture guidelines from Harvard Library's Virtual Media Lab , or contact a media staff member for customized recommendations. First and foremost, be mindful of common pitfalls by watching this short video that identifies the most common errors to avoid!
SOFTWARE:
- Adobe Premiere Pro Speech-To-Text automatically generates transcripts and adds captions to your videos. Harvard affiliates can download Adobe Premiere in the Creative Cloud Suite.
- GoTranscript provides cost-effective human-generated transcriptions.
- pyTranscriber is an app for generating automatic transcription and/or subtitles for audio and video files. It uses the Google Cloud Speech-to-Text service, has a friendly graphical user interface, and is purported to work nicely with Chinese.
- Otter provides a new way to capture, store, search and share voice conversations, lectures, presentations, meetings, and interviews. The startup is based in Silicon Valley with a team of experienced Ph.Ds and engineers from Google, Facebook, Yahoo and Nuance (à la Dragon). Free accounts available. This is the software that Zoom uses to generate automated transcripts, so if you have access to a Zoom subscription, you have access to Otter transcriptions with it (applicable in several languages ). As with any automated approach, be prepared to correct any errors after the fact, by hand.
- Panopto is available to Harvard affiliates and generates ASR (automated speech recognition) captions . You may upload compatible audio files into it. As with any automatically generated transcription, you will need to make manual revisions. ASR captioning is available in several languages . Panopto maintains robust security practices, including strong authentication measures and end-to-end encryption, ensuring your content remains private and protected.
- REV.Com allows you to record and transcribe any calls on the iPhone, both outgoing and incoming. It may be useful for recording phone interviews. Rev lets you choose whether you want an AI- or human-generated transcription, with a fast turnaround. Rev has Service Organization Controls Type II (SOC2) certification (a SOC2 cert looks at and verifies an organization’s processing integrity, privacy practices, and security safeguards).
- Scribie Audio/Video Transcription provides automated or manual transcriptions for a small fee. As with any transcription service, some revisions will be necessary after the fact, particularly for its automated transcripts.
- Sonix automatically transcribes, translates, and helps to organize audio and video files in over 40 languages. It's fast and affordable, with good accuracy. The free trial includes 30 minutes of free transcription.
- TranscriptionWing uses a human touch process to clean up machine-generated transcripts so that the content will far more accurately reflect your audio recording.
- Whisper is a tool from OpenAI that facilitates transcription of sensitive audiovisual recordings (e.g., of research interviews) on your own device. Installation and use depends on your operating system and which version you install. Important Note: The Whisper API, where audio is sent to OpenAI to be processed by them and then sent back (usually through a programming language like Python) is NOT appropriate for sensitive data. The model should be downloaded with tools such as those described in this FAQ , so that audio is kept to your local machine. For assistance, contact James Capobianco .
EQUIPMENT:
- Transcription pedals are in circulation and available to borrow from the Circulation desk at Lamont, or use at Lamont Library's Media Lab on level B. For hand-transcribing your interviews, they work in conjunction with software such as Express Scribe , which is loaded on Media Lab computers, or you may download for free on your own machine (Mac or PC versions; scroll down the downloads page for the latter). The pedals are plug-and-play USB, allow a wide range of playback speeds, and have 3 programmable buttons, which are typically set to rewind/play/fast-forward. Instructions are included in the bag that covers installation and set-up of the software, and basic use of the pedals.
NEED HELP?
- Try the virtual office hours offered by the Lamont Multimedia Lab!
- If you're creating podcasts, login to Canvas and check out the Podcasting/Audio guide .
Helpful Texts:
- "Transcription as a Crucial Step of Data Analysis" in Chapter 5 of The SAGE Handbook of Qualitative Data Analysisby Uwe Flick (Editor) Covers basic terminology for transcription, shares caveats for transcribers, and identifies components of vocal behavior. Provides notation systems for transcription, suggestions for transcribing turn-taking, and discusses new technologies and perspectives. Includes a bibliography for further reading.
- "Transcribing the Oral Interview: Part Art, Part Science " on p. 10 of the Centre for Community Knowledge (CCK) newsletter: TIMESTAMPby Mishika Chauhan and Saransh Srivastav
QUALITATIVE DATA ANALYSIS
Software .
- Free download available for Harvard Faculty of Arts and Sciences (FAS) affiliates
- Desktop access at Lamont Library Media Lab, 3rd floor
- Desktop access at Harvard Kennedy School Library (with HKS ID)
- Remote desktop access for Harvard affiliates from IQSS Computer Labs . Email them at [email protected] and ask for a new lab account and remote desktop access to NVivo.
- Virtual Desktop Infrastructure (VDI) access available to Harvard T.H. Chan School of Public Health affiliates
CODING AND THEMEING YOUR DATA
Data analysis methods should flow from, or align with, the methodological paradigm chosen for your study, whether that paradigm is interpretivist, critical, positivist, or participative in nature (or a combination of these). Some established methods include Content Analysis, Critical Analysis, Discourse Analysis, Gestalt Analysis, Grounded Theory Analysis, Interpretive Analysis, Narrative Analysis, Normative Analysis, Phenomenological Analysis, Rhetorical Analysis, and Semiotic Analysis, among others. The following resources should help you navigate your methodological options and put into practice methods for coding, themeing, interpreting, and presenting your data.
- Users can browse content by topic, discipline, or format type (reference works, book chapters, definitions, etc.). SRM offers several research tools as well: a methods map, user-created reading lists, a project planner, and advice on choosing statistical tests.
- Abductive Coding: Theory Building and Qualitative (Re)Analysis by Vila-Henninger, et al. The authors recommend an abductive approach to guide qualitative researchers who are oriented towards theory-building. They outline a set of tactics for abductive analysis, including the generation of an abductive codebook, abductive data reduction through code equations, and in-depth abductive qualitative analysis.
- Analyzing and Interpreting Qualitative Research: After the Interview by Charles F. Vanover, Paul A. Mihas, and Johnny Saldana (Editors) Providing insight into the wide range of approaches available to the qualitative researcher and covering all steps in the research process, the authors utilize a consistent chapter structure that provides novice and seasoned researchers with pragmatic, "how-to" strategies. Each chapter author introduces the method, uses one of their own research projects as a case study of the method described, shows how the specific analytic method can be used in other types of studies, and concludes with three questions/activities to prompt class discussion or personal study.
- "Analyzing Qualitative Data." Theory Into Practice 39, no. 3 (2000): 146-54 by Margaret D. LeCompte This article walks readers though rules for unbiased data analysis and provides guidance for getting organized, finding items, creating stable sets of items, creating patterns, assembling structures, and conducting data validity checks.
- "Coding is Not a Dirty Word" in Chapter 1 (pp. 1–30) of Enhancing Qualitative and Mixed Methods Research with Technology by Shalin Hai-Jew (Editor) Current discourses in qualitative research, especially those situated in postmodernism, represent coding and the technology that assists with coding as reductive, lacking complexity, and detached from theory. In this chapter, the author presents a counter-narrative to this dominant discourse in qualitative research. The author argues that coding is not necessarily devoid of theory, nor does the use of software for data management and analysis automatically render scholarship theoretically lightweight or barren. A lack of deep analytical insight is a consequence not of software but of epistemology. Using examples informed by interpretive and critical approaches, the author demonstrates how NVivo can provide an effective tool for data management and analysis. The author also highlights ideas for critical and deconstructive approaches in qualitative inquiry while using NVivo. By troubling the positivist discourse of coding, the author seeks to create dialogic spaces that integrate theory with technology-driven data management and analysis, while maintaining the depth and rigor of qualitative research.
- The Coding Manual for Qualitative Researchers by Johnny Saldana An in-depth guide to the multiple approaches available for coding qualitative data. Clear, practical and authoritative, the book profiles 32 coding methods that can be applied to a range of research genres from grounded theory to phenomenology to narrative inquiry. For each approach, Saldaña discusses the methods, origins, a description of the method, practical applications, and a clearly illustrated example with analytic follow-up. Essential reading across the social sciences.
- Flexible Coding of In-depth Interviews: A Twenty-first-century Approach by Nicole M. Deterding and Mary C. Waters The authors suggest steps in data organization and analysis to better utilize qualitative data analysis technologies and support rigorous, transparent, and flexible analysis of in-depth interview data.
- From the Editors: What Grounded Theory is Not by Roy Suddaby Walks readers through common misconceptions that hinder grounded theory studies, reinforcing the two key concepts of the grounded theory approach: (1) constant comparison of data gathered throughout the data collection process and (2) the determination of which kinds of data to sample in succession based on emergent themes (i.e., "theoretical sampling").
- “Good enough” methods for life-story analysis, by Wendy Luttrell. In Quinn N. (Ed.), Finding culture in talk (pp. 243–268). Demonstrates for researchers of culture and consciousness who use narrative how to concretely document reflexive processes in terms of where, how and why particular decisions are made at particular stages of the research process.
- The Ethnographic Interview by James P. Spradley “Spradley wrote this book for the professional and student who have never done ethnographic fieldwork (p. 231) and for the professional ethnographer who is interested in adapting the author’s procedures (p. iv) ... Steps 6 and 8 explain lucidly how to construct a domain and a taxonomic analysis” (excerpted from book review by James D. Sexton, 1980). See also: Presentation slides on coding and themeing your data, derived from Saldana, Spradley, and LeCompte Click to request access.
- Qualitative Data Analysis by Matthew B. Miles; A. Michael Huberman A practical sourcebook for researchers who make use of qualitative data, presenting the current state of the craft in the design, testing, and use of qualitative analysis methods. Strong emphasis is placed on data displays matrices and networks that go beyond ordinary narrative text. Each method of data display and analysis is described and illustrated.
- "A Survey of Qualitative Data Analytic Methods" in Chapter 4 (pp. 89–138) of Fundamentals of Qualitative Research by Johnny Saldana Provides an in-depth introduction to coding as a heuristic, particularly focusing on process coding, in vivo coding, descriptive coding, values coding, dramaturgical coding, and versus coding. Includes advice on writing analytic memos, developing categories, and themeing data.
- "Thematic Networks: An Analytic Tool for Qualitative Research." Qualitative Research : QR, 1(3), 385–405 by Jennifer Attride-Stirling Details a technique for conducting thematic analysis of qualitative material, presenting a step-by-step guide of the analytic process, with the aid of an empirical example. The analytic method presented employs established, well-known techniques; the article proposes that thematic analyses can be usefully aided by and presented as thematic networks.
- Using Thematic Analysis in Psychology by Virginia Braun and Victoria Clark Walks readers through the process of reflexive thematic analysis, step by step. The method may be adapted in fields outside of psychology as relevant. Pair this with One Size Fits All? What Counts as Quality Practice in Reflexive Thematic Analysis? by Virginia Braun and Victoria Clark
TESTING OR GENERATING THEORIES
The quality of your data analysis depends on how you situate what you learn within a wider body of knowledge. Consider the following advice:
Once you have coalesced around a theory, realize that a theory should reveal rather than color your discoveries. Allow your data to guide you to what's most suitable. Grounded theory researchers may develop their own theory where current theories fail to provide insight. This guide on Theoretical Models from Alfaisal University Library provides a helpful overview on using theory.
MANAGING & FINDING INTERVIEW DATA
Managing your elicited interview data, general guidance: .
- Research Data Management @ Harvard A reference guide with information and resources to help you manage your research data. See also: Harvard Research Data Security Policy , on the Harvard University Research Data Management website.
- Data Management For Researchers: Organize, Maintain and Share Your Data for Research Success by Kristin Briney. A comprehensive guide for scientific researchers providing everything they need to know about data management and how to organize, document, use and reuse their data.
- Open Science Framework (OSF) An open-source project management tool that makes it easy to collaborate within and beyond Harvard throughout a project's lifecycle. With OSF you can manage, store, and share documents, datasets, and other information with your research team. You can also publish your work to share it with a wider audience. Although data can be stored privately, because this platform is hosted on the Internet and designed with open access in mind, it is not a good choice for highly sensitive data.
- Free cloud storage solutions for Harvard affiliates to consider include: Google Drive , DropBox , or OneDrive ( up to DSL3 )
Data Confidentiality and Secure Handling:
- Data Security Levels at Harvard - Research Data Examples This resource provided by Harvard Data Security helps you determine what level of access is appropriate for your data. Determine whether it should be made available for public use, limited to the Harvard community, or be protected as either "confidential and sensitive," "high risk," or "extremely sensitive." See also: Harvard Data Classification Table
- Harvard's Best Practices for Protecting Privacy and Harvard Information Security Collaboration Tools Matrix Follow the nuts-and-bolts advice for privacy best practices at Harvard. The latter resource reveals the level of security that can be relied upon for a large number of technological tools and platforms used at Harvard to conduct business, such as email, Slack, Accellion Kiteworks, OneDrive/SharePoint, etc.
- “Protecting Participant Privacy While Maintaining Content and Context: Challenges in Qualitative Data De‐identification and Sharing.” Proceedings of the ASIST Annual Meeting 57 (1) (2020): e415-420 by Myers, Long, and Polasek Presents an informed and tested protocol, based on the De-Identification guidelines published by the Qualitative Data Repository (QDR) at Syracuse University. Qualitative researchers may consult it to guide their data de-identification efforts.
- QDS Qualitative Data Sharing Toolkit The Qualitative Data Sharing (QDS) project and its toolkit was funded by the NIH National Human Genome Research Institute (R01HG009351). It provides tools and resources to help researchers, especially those in the health sciences, share qualitative research data while protecting privacy and confidentiality. It offers guidance on preparing data for sharing through de-identification and access control. These health sciences research datasets in ICPSR's Qualitative Data Sharing (QDS) Project Series were de-identified using the QuaDS Software and the project’s QDS guidelines.
- Table of De-Identification Techniques
- Generative AI Harvard-affiliated researchers should not enter data classified as confidential ( Level 2 and above ), including non-public research data, into publicly-available generative AI tools, in accordance with the University’s Information Security Policy. Information shared with generative AI tools using default settings is not private and could expose proprietary or sensitive information to unauthorized parties.
- Harvard Information Security Quick Reference Guide Storage guidelines, based on the data's security classification level (according to its IRB classification) is displayed on page 2, under "handling."
- Email Encryption Harvard Microsoft 365 users can now send encrypted messages and files directly from the Outlook web or desktop apps. Encrypting an email adds an extra layer of security to the message and its attachments (up to 150MB), and means only the intended recipient (and their inbox delegates with full access) can view it. Message encryption in Outlook is approved for sending high risk ( level 4 ) data and below.
Sharing Qualitative Data:
- Repositories for Qualitative Data If you have cleared this intention with your IRB, secured consent from participants, and properly de-identified your data, consider sharing your interviews in one of the data repositories included in the link above. Depending on the nature of your research and the level of risk it may present to participants, sharing your interview data may not be appropriate. If there is any chance that sharing such data will be desirable, you will be much better off if you build this expectation into your plans from the beginning.
- Guide for Sharing Qualitative Data at ICPSR The Inter-university Consortium for Political and Social Research (ICPSR) has created this resource for investigators planning to share qualitative data at ICPSR. This guide provides an overview of elements and considerations for archiving qualitative data, identifies steps for investigators to follow during the research life cycle to ensure that others can share and reuse qualitative data, and provides information about exemplars of qualitative data
International Projects:
- Research Compliance Program for FAS/SEAS at Harvard The Faculty of Arts and Sciences (FAS), including the School of Engineering and Applied Sciences (SEAS), and the Office of the Vice Provost for Research (OVPR) have established a shared Research Compliance Program (RCP). An area of common concern for interview studies is international projects and collaboration . RCP is a resource to provide guidance on which international activities may be impacted by US sanctions on countries, individuals, or entities and whether licenses or other disclosure are required to ship or otherwise share items, technology, or data with foreign collaborators.
Finding Extant Interview Data
Finding journalistic interviews: .
- Academic Search Premier This all-purpose database is great for finding articles from magazines and newspapers. In the Advanced Search, it allows you to specify "Document Type": Interview.
- Guide to Newspapers and Newspaper Indexes Use this guide created to Harvard Librarians to identify newspapers collections you'd like to search. To locate interviews, try adding the term "interview" to your search, or explore a database's search interface for options to limit your search to interviews. Nexis Uni and Factiva are the two main databases for current news.
- Listen Notes Search for podcast episodes at this podcast aggregator, and look for podcasts that include interviews. Make sure to vet the podcaster for accuracy and quality! (Listen Notes does not do much vetting.)
- NPR and ProPublica are two sites that offer high-quality long-form reporting, including journalistic interviews, for free.
Finding Oral History and Social Research Interviews:
- To find oral histories, see the Oral History page of this guide for helpful resources on Oral History interviewing.
- Repositories for Qualitative Data It has not been a customary practice among qualitative researchers in the social sciences to share raw interview data, but some have made this data available in repositories, such as the ones listed on the page linked above. You may find published data from structured interview surveys (e.g., questionnaire-based computer-assisted telephone interview data), as well as some semi-structured and unstructured interviews.
- If you are merely interested in studies interpreting data collected using interviews, rather than finding raw interview data, try databases like PsycInfo , Sociological Abstracts , or Anthropology Plus , among others.
Finding Interviews in Archival Collections at Harvard Library:
In addition to the databases and search strategies mentioned under the "Finding Oral History and Social Research Interviews" category above, you may search for interviews and oral histories (whether in textual or audiovisual formats) held in archival collections at Harvard Library.
- HOLLIS searches all documented collections at Harvard, whereas HOLLIS for Archival Discovery searches only those with finding aids. Although HOLLIS for Archival Discovery covers less material, you may find it easier to parse your search results, especially when you wish to view results at the item level (within collections). Try these approaches:
Search in HOLLIS :
- To retrieve items available online, do an Advanced Search for interview* OR "oral histor*" (in Subject), with Resource Type "Archives/Manuscripts," then refine your search by selecting "Online" under "Show Only" on the right of your initial result list. Revise the search above by adding your topic in the Keywords or Subject field (for example: African Americans ) and resubmitting the search.
- To enlarge your results set, you may also leave out the "Online" refinement; if you'd like to limit your search to a specific repository, try the technique of searching for Code: Library + Collection on the "Advanced Search" page .
Search in HOLLIS for Archival Discovery :
- To retrieve items available online, search for interview* OR "oral histor*" limited to digital materials . Revise the search above by adding your topic (for example: artist* ) in the second search box (if you don't see the box, click +).
- To preview results by collection, search for interview* OR "oral histor*" limited to collections . Revise the search above by adding your topic (for example: artist* ) in the second search box (if you don't see the box, click +). Although this method does not allow you to isolate digitized content, you may find the refinement options on the right side of the screen (refine by repository, subject or names) helpful. Once your select a given collection, you may search within it (e.g., for your topic or the term interview).
UX & MARKET RESEARCH INTERVIEWS
Ux at harvard library .
- User Experience and Market Research interviews can inform the design of tangible products and services through responsive, outcome-driven insights. The User Research Center at Harvard Library specializes in this kind of user-centered design, digital accessibility, and testing. They also offer guidance and resources to members of the Harvard Community who are interested in learning more about UX methods. Contact [email protected] or consult the URC website for more information.
Websites
- User Interviews: The Beginner’s Guide (Chris Mears)
- Interviewing Users (Jakob Nielsen)
Books
- Interviewing Users: How to Uncover Compelling Insights by Steve Portigal; Grant McCracken (Foreword by) Interviewing is a foundational user research tool that people assume they already possess. Everyone can ask questions, right? Unfortunately, that's not the case. Interviewing Users provides invaluable interviewing techniques and tools that enable you to conduct informative interviews with anyone. You'll move from simply gathering data to uncovering powerful insights about people.
- Rapid Contextual Design by Jessamyn Wendell; Karen Holtzblatt; Shelley Wood This handbook introduces Rapid CD, a fast-paced, adaptive form of Contextual Design. Rapid CD is a hands-on guide for anyone who needs practical guidance on how to use the Contextual Design process and adapt it to tactical projects with tight timelines and resources. Rapid Contextual Design provides detailed suggestions on structuring the project and customer interviews, conducting interviews, and running interpretation sessions. The handbook walks you step-by-step through organizing the data so you can see your key issues, along with visioning new solutions, storyboarding to work out the details, and paper prototype interviewing to iterate the design all with as little as a two-person team with only a few weeks to spare *Includes real project examples with actual customer data that illustrate how a CD project actually works.
Videos

Instructional Presentations on Interview Skills
- Interview/Oral History Research for RSRA 298B: Master's Thesis Reading and Research (Spring 2023) Slideshow covers: Why Interviews?, Getting Context, Engaging Participants, Conducting the Interview, The Interview Guide, Note Taking, Transcription, File management, and Data Analysis.
- Interview Skills From an online class on February 13, 2023: Get set up for interview research. You will leave prepared to choose among the three types of interviewing methods, equipped to develop an interview schedule, aware of data management options and their ethical implications, and knowledgeable of technologies you can use to record and transcribe your interviews. This workshop complements Intro to NVivo, a qualitative data analysis tool useful for coding interview data.
NIH Data Management & Sharing Policy (DMSP) This policy, effective January 25, 2023, applies to all research, funded or conducted in whole or in part by NIH, that results in the generation of scientific data , including NIH-funded qualitative research. Click here to see some examples of how the DMSP policy has been applied in qualitative research studies featured in the 2021 Qualitative Data Management Plan (DMP) Competition . As a resource for the community, NIH has developed a resource for developing informed consent language in research studies where data and/or biospecimens will be stored and shared for future use. It is important to note that the DMS Policy does NOT require that informed consent obtained from research participants must allow for broad sharing and the future use of data (either with or without identifiable private information). See the FAQ for more information.
- << Previous: Remote Research & Virtual Fieldwork
- Next: Oral History >>
Except where otherwise noted, this work is subject to a Creative Commons Attribution 4.0 International License , which allows anyone to share and adapt our material as long as proper attribution is given. For details and exceptions, see the Harvard Library Copyright Policy ©2021 Presidents and Fellows of Harvard College.
Introduction to Research Methods
6 qualitative research and interviews.
So we’ve described doing a survey and collecting quantitative data. But not all questions can best be answered by a survey. A survey is great for understanding what people think (for example), but not why they think what they do. If your research is intending to understand the underlying motivations or reasons behind peoples actions, or to build a deeper understanding on the background of a subject, an interview may be the more appropriate data collection method.
Interviews are a method of data collection that consist of two or more people exchanging information through a structured process of questions and answers. Questions are designed by the researcher to thoughtfully collect in-depth information on a topic or set of topics as related to the central research question. Interviews typically occur in-person, although good interviews can also be conducted remotely via the phone or video conferencing. Unlike surveys, interviews give the opportunity to ask follow-up questions and thoughtfully engage with participants on the spot (rather than the anonymous and impartial format of survey research).
And surveys can be used in qualitative or quantitative research – though they’re more typically a qualitative technique. In-depth interviews , containing open-ended questions and structured by an interview guide . One can also do a standardized interview with closed-ended questions (i.e. answer options) that are structured by an interview schedule as part of quantitative research. While these are called interviews they’re far closer to surveys, so we wont cover them again in this chapter. The terms used for in-depth interviews we’ll cover in the next section.
6.1 Interviews
In-depth interviews allow participants to describe experiences in their own words (a primary strength of the interview format). Strong in-depth interviews will include many open-ended questions that allow participants to respond in their own words, share new ideas, and lead the conversation in different directions. The purpose of open-ended questions and in-depth interviews is to hear as much as possible in the person’s own voice, to collect new information and ideas, and to achieve a level of depth not possible in surveys or most other forms of data collection.
Typically, an interview guide is used to create a soft structure for the conversation and is an important preparation tool for the researcher. You can not go into an interview unprepared and just “wing it”; what the interview guide allows you to do is map out a framework, order of topics, and may include specific questions to use during the interview. Generally, the interview guide is thought of as just that — a guide to use in order to keep the interview focused. It is not set in stone and a skilled researcher can change the order of questions or topics in an interviews based on the organic conversation flow.
Depending on the experience and skill level of the researcher, an interview guide can be as simple as a list of topics to cover. However, for consistency and quality of research, the interviewer may want to take the time to at least practice writing out questions in advance to ensure that phrasing and word choices are as clear, objective, and focused as possible. It’s worth remembering that working out the wording of questions in advance allows researchers to ensure more consistency across interview. The interview guide below, taken from the wonderful and free textbook Principles of Sociological Inquiry , shows an interview guide that just has topics.

Alternatively, you can use a more detailed guide that lists out possible questions, as shown below. A more detailed guide is probably better for an interviewer that has less experience, or is just beginning to work on a given topic.

The purpose of an interview guide is to help ask effective questions and to support the process of acquiring the best possible data for your research. Topics and questions should be organized thematically, and in a natural progression that will allow the conversation to flow and deepen throughout the course of the interview. Often, researchers will attempt to memorize or partially memorize the interview guide, in order to be more fully present with the participant during the conversation.
6.2 Asking good Questions
Remember, the purposes of interviews is to go more in-depth with an individual than is possible with a generalized survey. For this reason, it is important to use the guide as a starting point but not to be overly tethered to it during the actual interview process. You may get stuck when respondents give you shorter answers than you expect, or don’t provide the type of depth that you need for your research. Often, you may want to probe for more specifics. Think about using follow up questions like “How does/did that affect you?” or “How does X make you feel?” and “Tell me about a time where X…”
For example, if I was researching the relationship between pets and mental health, some strong open-ended questions might be: * How does your pet typically make you feel when you wake up in the morning? * How does your pet generally affect your mood when you arrive home in the evening? * Tell me about a time when your pet had a significant impact on your emotional state.
Questions framed in this manner leave plenty of room for the respondent to answer in their own words, as opposed to leading and/or truncated questions, such as: * Does being with your pet make you happy? * After a bad day, how much does seeing your pet improve your mood? * Tell me about how important your pet is to your mental health.
These questions assume outcomes and will not result in high quality research. Researchers should always avoid asking leading questions that give away an expected answer or suggest particular responses. For instance, if I ask “we need to spend more on public schools, don’t you think?” the respondent is more likely to agree regardless of their own thoughts. Some wont, but humans generally have a strong natural desire to be agreeable. That’s why leaving your questions neutral and open so that respondents can speak to their experiences and views is critical.
6.3 Analyzing Interview Data
Writing good questions and interviewing respondents are just the first steps of the interview process. After these stages, the researcher still has a lot of work to do to collect usable data from the interview. The researcher must spend time coding and analyzing the interview to retrieve this data. Just doing an interview wont produce data. Think about how many conversations you have everyday, and none of those are leaving you swimming in data.
Hopefully you can record your interviews. Recording your interviews will allow you the opportunity to transcribe them word for word later. If you can’t record the interview you’ll need to take detailed notes so that you can reconstruct what you heard later. Do not trust yourself to “just remember” the conversation. You’re collecting data, precious data that you’re spending time and energy to collect. Treat it as important and valuable. Remember our description of the methodology section from Chapter 2, you need to maintain a chain of custody on your data. If you just remembered the interview, you could be accused of making up the results. Your interview notes and the recording become part of that chain of custody to prove to others that your interviews were real and that your results are accurate.
Assuming you recorded your interview, the first step in the analysis process is transcribing the interview. A transcription is a written record of every word in an interview. Transcriptions can either be completed by the researcher or by a hired worker, though it is good practice for the researcher to transcribe the interview him or herself. Researchers should keep the following points in mind regarding transcriptions: * The interview should take place in a quiet location with minimal background noise to produce a clear recording; * Transcribing interviews is a time-consuming process and may take two to three times longer than the actual interview; * Transcriptions provide a more precise record of the interview than hand written notes and allow the interviewer to focus during the interview.
After transcribing the interview, the next step is to analyze the responses. Coding is the main form of analysis used for interviews and involves studying a transcription to identify important themes. These themes are categorized into codes, which are words or phrases that denote an idea.
You’ll typically being with several codes in mind that are generated by key ideas you week seeking in the questions, but you can also being by using open coding to understand the results. An open coding process involves reading through the transcript multiple times and paying close attention to each line of the text to discover noteworthy concepts. During the open coding process, the researcher keeps an open mind to find any codes that may be relevant to the research topic.
After the open coding process is complete, focused coding can begin. Focused coding takes a closer look at the notes compiled during the open coding stage to merge common codes and define what the codes mean in the context of the research project.
Imagine a researcher is conducting interviews to learn about various people’s experiences of childhood in New Orleans. The following example shows several codes that this researcher extrapolated from an interview with one of their subjects.

6.4 Using interview data
The next chapter will address ways to identify people to interview, but most of the remainder of the book will address how to analyze quantitative data. That shouldn’t be taken as a sign that quantitative data is better, or that it’s easier to use interview data. Because in an interview the researcher must interpret the words of others it is often more challenging to identify your findings and clearly answer your research question. However, quantitative data is more common, and there are more different things you can do with it, so we spend a lot of the textbook focusing on it.
I’ll work through one more example of using interview data though. It takes a lot of practice to be a good and skilled interviewer. What I show below is a brief excerpt of an interview I did, and how that data was used in a resulting paper I wrote. These aren’t the only way you can use interview data, but it’s an example of what the intermediary and final product might look like.
The overall project these are drawn from was concerned with minor league baseball stadiums, but the specific part I’m pulling from here was studying the decline and rejuvenation of downtown around those stadiums in several cities. You’ll see that I’m using the words of the respondent fairly directly, because that’s my data. But I’m not just relying on one respondent and trusting them, I did a few dozen interviews in order to understand the commonalities in people’s perspectives to build a narrative around my research question.

Excerpt from Notes

Excerpt from Resulting Paper
How many interviews are necessary? It actually doesn’t take many. What you want to observe in your interviews is theoretical saturation , where the codes you use in the transcript begin to appear across conversations and groups. If different people disagree that’s fine, but what you want to understand is the commonalities across peoples perspectives. Most research on the subject says that with 8 interviews you’ll typically start to see a decline in new information gathered. That doesn’t mean you won’t get new words , but you’ll stop hearing completely unique perspectives or gain novel insights. At that point, where you’ve ‘heard it all before’ you can stop, because you’ve probably identified the answer to the questions you were trying to research.
6.5 Ensuring Anonymity
One significant ethical concern with interviews, that also applies to surveys, is making sure that respondents maintain anonymity. In either form of data collection you may be asking respondents deeply personal questions, that if exposed may cause legal, personal, or professional harm. Notice that in the excerpt of the paper above the respondents are only identified by an id I assigned (Louisville D) and their career, rather than their name. I can only include the excerpt of the interview notes above because there are no details that might lead to them being identified.
You may want to report details about a person to contextualize the data you gathered, but you should always ensure that no one can be identified from your research. For instance, if you were doing research on racism at large companies, you may want to preface people’s comments by their race, as there is a good chance that white and minority employees would feel differently about the issues. However, if you preface someones comments by saying they’re a minority manager, that may violate their anonymity. Even if you don’t state what company you did interviews with, that may be enough detail for their co-workers to identify them if there are few minority managers at the company. As such, always think long and hard about whether there is any way that the participation of respondents may be exposed.
6.6 Why not both?

We’ve discussed surveys and interviews as different methods the last two chapters, but they can also complement each other.
For instance, let’s say you’re curious to study people who change opinions on abortion, either going from support to opposition or vice versa. You could use a survey to understand the prevalence of changing opinions, i.e. what percentage of people in your city have changed their views. That would help to establish whether this is a prominent issue, or whether it’s a rare phenomenon. But it would be difficult to understand from the survey what makes people change their views. You could add an open ended question for anyone that said they changed their opinion, but many people won’t respond and few will provide the level of detail necessary to understand their motivations. Interviews with people that have changed their opinions would give you an opportunity to explore how their experiences and beliefs have changed in combination with their views towards abortion.
6.7 Summary
In the last two chapters we’ve discussed the two most prominent methods of data collection in the social sciences: surveys and interviews. What we haven’t discussed though is how to identify the people you’ll collect data from; that’s called a sampling strategy. In the next chapter

Interviews can be defined as a qualitative research technique which involves “conducting intensive individual interviews with a small number of respondents to explore their perspectives on a particular idea, program or situation.” [1]
There are three different formats of interviews: structured, semi-structured and unstructured.
Structured interviews consist of a series of pre-determined questions that all interviewees answer in the same order. Data analysis usually tends to be more straightforward because researcher can compare and contrast different answers given to the same questions.
Unstructured interviews are usually the least reliable from research viewpoint, because no questions are prepared prior to the interview and data collection is conducted in an informal manner. Unstructured interviews can be associated with a high level of bias and comparison of answers given by different respondents tends to be difficult due to the differences in formulation of questions.
Semi-structured interviews contain the components of both, structured and unstructured interviews. In semi-structured interviews, interviewer prepares a set of same questions to be answered by all interviewees. At the same time, additional questions might be asked during interviews to clarify and/or further expand certain issues.
Advantages of interviews include possibilities of collecting detailed information about research questions. Moreover, in in this type of primary data collection researcher has direct control over the flow of process and she has a chance to clarify certain issues during the process if needed. Disadvantages, on the other hand, include longer time requirements and difficulties associated with arranging an appropriate time with perspective sample group members to conduct interviews.
When conducting interviews you should have an open mind and refrain from displaying disagreements in any forms when viewpoints expressed by interviewees contradict your own ideas. Moreover, timing and environment for interviews need to be scheduled effectively. Specifically, interviews need to be conducted in a relaxed environment, free of any forms of pressure for interviewees whatsoever.
Respected scholars warn that “in conducting an interview the interviewer should attempt to create a friendly, non-threatening atmosphere. Much as one does with a cover letter, the interviewer should give a brief, casual introduction to the study; stress the importance of the person’s participation; and assure anonymity, or at least confidentiality, when possible.” [2]
There is a risk of interviewee bias during the primary data collection process and this would seriously compromise the validity of the project findings. Some interviewer bias can be avoided by ensuring that the interviewer does not overreact to responses of the interviewee. Other steps that can be taken to help avoid or reduce interviewer bias include having the interviewer dress inconspicuously and appropriately for the environment and holding the interview in a private setting. [3]
My e-book, The Ultimate Guide to Writing a Dissertation in Business Studies: a step by step assistance offers practical assistance to complete a dissertation with minimum or no stress. The e-book covers all stages of writing a dissertation starting from the selection to the research area to submitting the completed version of the work within the deadline.John Dudovskiy

[1] Boyce, C. & Neale, P. (2006) “Conducting in-depth Interviews: A Guide for Designing and Conducting In-Depth Interviews”, Pathfinder International Tool Series
[2] Connaway, L.S.& Powell, R.P.(2010) “Basic Research Methods for Librarians” ABC-CLIO
[3] Connaway, L.S.& Powell, R.P.(2010) “Basic Research Methods for Librarians” ABC-CLIO
- University Libraries
- Research Guides
- Topic Guides
- Research Methods Guide
- Interview Research
Research Methods Guide: Interview Research
- Introduction
- Research Design & Method
- Survey Research
- Data Analysis
- Resources & Consultation
Tutorial Videos: Interview Method
Interview as a Method for Qualitative Research

Goals of Interview Research
- Preferences
- They help you explain, better understand, and explore research subjects' opinions, behavior, experiences, phenomenon, etc.
- Interview questions are usually open-ended questions so that in-depth information will be collected.
Mode of Data Collection
There are several types of interviews, including:
- Face-to-Face
- Online (e.g. Skype, Googlehangout, etc)
FAQ: Conducting Interview Research
What are the important steps involved in interviews?
- Think about who you will interview
- Think about what kind of information you want to obtain from interviews
- Think about why you want to pursue in-depth information around your research topic
- Introduce yourself and explain the aim of the interview
- Devise your questions so interviewees can help answer your research question
- Have a sequence to your questions / topics by grouping them in themes
- Make sure you can easily move back and forth between questions / topics
- Make sure your questions are clear and easy to understand
- Do not ask leading questions
- Do you want to bring a second interviewer with you?
- Do you want to bring a notetaker?
- Do you want to record interviews? If so, do you have time to transcribe interview recordings?
- Where will you interview people? Where is the setting with the least distraction?
- How long will each interview take?
- Do you need to address terms of confidentiality?
Do I have to choose either a survey or interviewing method?
No. In fact, many researchers use a mixed method - interviews can be useful as follow-up to certain respondents to surveys, e.g., to further investigate their responses.
Is training an interviewer important?
Yes, since the interviewer can control the quality of the result, training the interviewer becomes crucial. If more than one interviewers are involved in your study, it is important to have every interviewer understand the interviewing procedure and rehearse the interviewing process before beginning the formal study.
- << Previous: Survey Research
- Next: Data Analysis >>
- Last Updated: Aug 21, 2023 10:42 AM
The qualitative research interview
Affiliation.
- 1 Department of Family Medicine, University of Medicine and Dentistry at Robert Wood Johnson Medical School, Somerset, New Jersey 08873, USA. [email protected]
- PMID: 16573666
- DOI: 10.1111/j.1365-2929.2006.02418.x
Background: Interviews are among the most familiar strategies for collecting qualitative data. The different qualitative interviewing strategies in common use emerged from diverse disciplinary perspectives resulting in a wide variation among interviewing approaches. Unlike the highly structured survey interviews and questionnaires used in epidemiology and most health services research, we examine less structured interview strategies in which the person interviewed is more a participant in meaning making than a conduit from which information is retrieved.
Purpose: In this article we briefly review the more common qualitative interview methods and then focus on the widely used individual face-to-face in-depth interview, which seeks to foster learning about individual experiences and perspectives on a given set of issues. We discuss methods for conducting in-depth interviews and consider relevant ethical issues with particular regard to the rights and protection of the participants.
Publication types
- Research Support, N.I.H., Extramural
- Research Support, Non-U.S. Gov't
- Data Collection / methods
- Ethics, Research
- Interpersonal Relations
- Interviews as Topic / methods*
- Qualitative Research*
Grants and funding
- 1D12HP00167/PHS HHS/United States
- Privacy Policy
Home » Qualitative Research – Methods, Analysis Types and Guide
Qualitative Research – Methods, Analysis Types and Guide
Table of Contents

Qualitative Research
Qualitative research is a type of research methodology that focuses on exploring and understanding people’s beliefs, attitudes, behaviors, and experiences through the collection and analysis of non-numerical data. It seeks to answer research questions through the examination of subjective data, such as interviews, focus groups, observations, and textual analysis.
Qualitative research aims to uncover the meaning and significance of social phenomena, and it typically involves a more flexible and iterative approach to data collection and analysis compared to quantitative research. Qualitative research is often used in fields such as sociology, anthropology, psychology, and education.
Qualitative Research Methods

Qualitative Research Methods are as follows:
One-to-One Interview
This method involves conducting an interview with a single participant to gain a detailed understanding of their experiences, attitudes, and beliefs. One-to-one interviews can be conducted in-person, over the phone, or through video conferencing. The interviewer typically uses open-ended questions to encourage the participant to share their thoughts and feelings. One-to-one interviews are useful for gaining detailed insights into individual experiences.
Focus Groups
This method involves bringing together a group of people to discuss a specific topic in a structured setting. The focus group is led by a moderator who guides the discussion and encourages participants to share their thoughts and opinions. Focus groups are useful for generating ideas and insights, exploring social norms and attitudes, and understanding group dynamics.
Ethnographic Studies
This method involves immersing oneself in a culture or community to gain a deep understanding of its norms, beliefs, and practices. Ethnographic studies typically involve long-term fieldwork and observation, as well as interviews and document analysis. Ethnographic studies are useful for understanding the cultural context of social phenomena and for gaining a holistic understanding of complex social processes.
Text Analysis
This method involves analyzing written or spoken language to identify patterns and themes. Text analysis can be quantitative or qualitative. Qualitative text analysis involves close reading and interpretation of texts to identify recurring themes, concepts, and patterns. Text analysis is useful for understanding media messages, public discourse, and cultural trends.
This method involves an in-depth examination of a single person, group, or event to gain an understanding of complex phenomena. Case studies typically involve a combination of data collection methods, such as interviews, observations, and document analysis, to provide a comprehensive understanding of the case. Case studies are useful for exploring unique or rare cases, and for generating hypotheses for further research.
Process of Observation
This method involves systematically observing and recording behaviors and interactions in natural settings. The observer may take notes, use audio or video recordings, or use other methods to document what they see. Process of observation is useful for understanding social interactions, cultural practices, and the context in which behaviors occur.
Record Keeping
This method involves keeping detailed records of observations, interviews, and other data collected during the research process. Record keeping is essential for ensuring the accuracy and reliability of the data, and for providing a basis for analysis and interpretation.
This method involves collecting data from a large sample of participants through a structured questionnaire. Surveys can be conducted in person, over the phone, through mail, or online. Surveys are useful for collecting data on attitudes, beliefs, and behaviors, and for identifying patterns and trends in a population.
Qualitative data analysis is a process of turning unstructured data into meaningful insights. It involves extracting and organizing information from sources like interviews, focus groups, and surveys. The goal is to understand people’s attitudes, behaviors, and motivations
Qualitative Research Analysis Methods
Qualitative Research analysis methods involve a systematic approach to interpreting and making sense of the data collected in qualitative research. Here are some common qualitative data analysis methods:
Thematic Analysis
This method involves identifying patterns or themes in the data that are relevant to the research question. The researcher reviews the data, identifies keywords or phrases, and groups them into categories or themes. Thematic analysis is useful for identifying patterns across multiple data sources and for generating new insights into the research topic.
Content Analysis
This method involves analyzing the content of written or spoken language to identify key themes or concepts. Content analysis can be quantitative or qualitative. Qualitative content analysis involves close reading and interpretation of texts to identify recurring themes, concepts, and patterns. Content analysis is useful for identifying patterns in media messages, public discourse, and cultural trends.
Discourse Analysis
This method involves analyzing language to understand how it constructs meaning and shapes social interactions. Discourse analysis can involve a variety of methods, such as conversation analysis, critical discourse analysis, and narrative analysis. Discourse analysis is useful for understanding how language shapes social interactions, cultural norms, and power relationships.
Grounded Theory Analysis
This method involves developing a theory or explanation based on the data collected. Grounded theory analysis starts with the data and uses an iterative process of coding and analysis to identify patterns and themes in the data. The theory or explanation that emerges is grounded in the data, rather than preconceived hypotheses. Grounded theory analysis is useful for understanding complex social phenomena and for generating new theoretical insights.
Narrative Analysis
This method involves analyzing the stories or narratives that participants share to gain insights into their experiences, attitudes, and beliefs. Narrative analysis can involve a variety of methods, such as structural analysis, thematic analysis, and discourse analysis. Narrative analysis is useful for understanding how individuals construct their identities, make sense of their experiences, and communicate their values and beliefs.
Phenomenological Analysis
This method involves analyzing how individuals make sense of their experiences and the meanings they attach to them. Phenomenological analysis typically involves in-depth interviews with participants to explore their experiences in detail. Phenomenological analysis is useful for understanding subjective experiences and for developing a rich understanding of human consciousness.
Comparative Analysis
This method involves comparing and contrasting data across different cases or groups to identify similarities and differences. Comparative analysis can be used to identify patterns or themes that are common across multiple cases, as well as to identify unique or distinctive features of individual cases. Comparative analysis is useful for understanding how social phenomena vary across different contexts and groups.
Applications of Qualitative Research
Qualitative research has many applications across different fields and industries. Here are some examples of how qualitative research is used:
- Market Research: Qualitative research is often used in market research to understand consumer attitudes, behaviors, and preferences. Researchers conduct focus groups and one-on-one interviews with consumers to gather insights into their experiences and perceptions of products and services.
- Health Care: Qualitative research is used in health care to explore patient experiences and perspectives on health and illness. Researchers conduct in-depth interviews with patients and their families to gather information on their experiences with different health care providers and treatments.
- Education: Qualitative research is used in education to understand student experiences and to develop effective teaching strategies. Researchers conduct classroom observations and interviews with students and teachers to gather insights into classroom dynamics and instructional practices.
- Social Work : Qualitative research is used in social work to explore social problems and to develop interventions to address them. Researchers conduct in-depth interviews with individuals and families to understand their experiences with poverty, discrimination, and other social problems.
- Anthropology : Qualitative research is used in anthropology to understand different cultures and societies. Researchers conduct ethnographic studies and observe and interview members of different cultural groups to gain insights into their beliefs, practices, and social structures.
- Psychology : Qualitative research is used in psychology to understand human behavior and mental processes. Researchers conduct in-depth interviews with individuals to explore their thoughts, feelings, and experiences.
- Public Policy : Qualitative research is used in public policy to explore public attitudes and to inform policy decisions. Researchers conduct focus groups and one-on-one interviews with members of the public to gather insights into their perspectives on different policy issues.
How to Conduct Qualitative Research
Here are some general steps for conducting qualitative research:
- Identify your research question: Qualitative research starts with a research question or set of questions that you want to explore. This question should be focused and specific, but also broad enough to allow for exploration and discovery.
- Select your research design: There are different types of qualitative research designs, including ethnography, case study, grounded theory, and phenomenology. You should select a design that aligns with your research question and that will allow you to gather the data you need to answer your research question.
- Recruit participants: Once you have your research question and design, you need to recruit participants. The number of participants you need will depend on your research design and the scope of your research. You can recruit participants through advertisements, social media, or through personal networks.
- Collect data: There are different methods for collecting qualitative data, including interviews, focus groups, observation, and document analysis. You should select the method or methods that align with your research design and that will allow you to gather the data you need to answer your research question.
- Analyze data: Once you have collected your data, you need to analyze it. This involves reviewing your data, identifying patterns and themes, and developing codes to organize your data. You can use different software programs to help you analyze your data, or you can do it manually.
- Interpret data: Once you have analyzed your data, you need to interpret it. This involves making sense of the patterns and themes you have identified, and developing insights and conclusions that answer your research question. You should be guided by your research question and use your data to support your conclusions.
- Communicate results: Once you have interpreted your data, you need to communicate your results. This can be done through academic papers, presentations, or reports. You should be clear and concise in your communication, and use examples and quotes from your data to support your findings.
Examples of Qualitative Research
Here are some real-time examples of qualitative research:
- Customer Feedback: A company may conduct qualitative research to understand the feedback and experiences of its customers. This may involve conducting focus groups or one-on-one interviews with customers to gather insights into their attitudes, behaviors, and preferences.
- Healthcare : A healthcare provider may conduct qualitative research to explore patient experiences and perspectives on health and illness. This may involve conducting in-depth interviews with patients and their families to gather information on their experiences with different health care providers and treatments.
- Education : An educational institution may conduct qualitative research to understand student experiences and to develop effective teaching strategies. This may involve conducting classroom observations and interviews with students and teachers to gather insights into classroom dynamics and instructional practices.
- Social Work: A social worker may conduct qualitative research to explore social problems and to develop interventions to address them. This may involve conducting in-depth interviews with individuals and families to understand their experiences with poverty, discrimination, and other social problems.
- Anthropology : An anthropologist may conduct qualitative research to understand different cultures and societies. This may involve conducting ethnographic studies and observing and interviewing members of different cultural groups to gain insights into their beliefs, practices, and social structures.
- Psychology : A psychologist may conduct qualitative research to understand human behavior and mental processes. This may involve conducting in-depth interviews with individuals to explore their thoughts, feelings, and experiences.
- Public Policy: A government agency or non-profit organization may conduct qualitative research to explore public attitudes and to inform policy decisions. This may involve conducting focus groups and one-on-one interviews with members of the public to gather insights into their perspectives on different policy issues.
Purpose of Qualitative Research
The purpose of qualitative research is to explore and understand the subjective experiences, behaviors, and perspectives of individuals or groups in a particular context. Unlike quantitative research, which focuses on numerical data and statistical analysis, qualitative research aims to provide in-depth, descriptive information that can help researchers develop insights and theories about complex social phenomena.
Qualitative research can serve multiple purposes, including:
- Exploring new or emerging phenomena : Qualitative research can be useful for exploring new or emerging phenomena, such as new technologies or social trends. This type of research can help researchers develop a deeper understanding of these phenomena and identify potential areas for further study.
- Understanding complex social phenomena : Qualitative research can be useful for exploring complex social phenomena, such as cultural beliefs, social norms, or political processes. This type of research can help researchers develop a more nuanced understanding of these phenomena and identify factors that may influence them.
- Generating new theories or hypotheses: Qualitative research can be useful for generating new theories or hypotheses about social phenomena. By gathering rich, detailed data about individuals’ experiences and perspectives, researchers can develop insights that may challenge existing theories or lead to new lines of inquiry.
- Providing context for quantitative data: Qualitative research can be useful for providing context for quantitative data. By gathering qualitative data alongside quantitative data, researchers can develop a more complete understanding of complex social phenomena and identify potential explanations for quantitative findings.
When to use Qualitative Research
Here are some situations where qualitative research may be appropriate:
- Exploring a new area: If little is known about a particular topic, qualitative research can help to identify key issues, generate hypotheses, and develop new theories.
- Understanding complex phenomena: Qualitative research can be used to investigate complex social, cultural, or organizational phenomena that are difficult to measure quantitatively.
- Investigating subjective experiences: Qualitative research is particularly useful for investigating the subjective experiences of individuals or groups, such as their attitudes, beliefs, values, or emotions.
- Conducting formative research: Qualitative research can be used in the early stages of a research project to develop research questions, identify potential research participants, and refine research methods.
- Evaluating interventions or programs: Qualitative research can be used to evaluate the effectiveness of interventions or programs by collecting data on participants’ experiences, attitudes, and behaviors.
Characteristics of Qualitative Research
Qualitative research is characterized by several key features, including:
- Focus on subjective experience: Qualitative research is concerned with understanding the subjective experiences, beliefs, and perspectives of individuals or groups in a particular context. Researchers aim to explore the meanings that people attach to their experiences and to understand the social and cultural factors that shape these meanings.
- Use of open-ended questions: Qualitative research relies on open-ended questions that allow participants to provide detailed, in-depth responses. Researchers seek to elicit rich, descriptive data that can provide insights into participants’ experiences and perspectives.
- Sampling-based on purpose and diversity: Qualitative research often involves purposive sampling, in which participants are selected based on specific criteria related to the research question. Researchers may also seek to include participants with diverse experiences and perspectives to capture a range of viewpoints.
- Data collection through multiple methods: Qualitative research typically involves the use of multiple data collection methods, such as in-depth interviews, focus groups, and observation. This allows researchers to gather rich, detailed data from multiple sources, which can provide a more complete picture of participants’ experiences and perspectives.
- Inductive data analysis: Qualitative research relies on inductive data analysis, in which researchers develop theories and insights based on the data rather than testing pre-existing hypotheses. Researchers use coding and thematic analysis to identify patterns and themes in the data and to develop theories and explanations based on these patterns.
- Emphasis on researcher reflexivity: Qualitative research recognizes the importance of the researcher’s role in shaping the research process and outcomes. Researchers are encouraged to reflect on their own biases and assumptions and to be transparent about their role in the research process.
Advantages of Qualitative Research
Qualitative research offers several advantages over other research methods, including:
- Depth and detail: Qualitative research allows researchers to gather rich, detailed data that provides a deeper understanding of complex social phenomena. Through in-depth interviews, focus groups, and observation, researchers can gather detailed information about participants’ experiences and perspectives that may be missed by other research methods.
- Flexibility : Qualitative research is a flexible approach that allows researchers to adapt their methods to the research question and context. Researchers can adjust their research methods in real-time to gather more information or explore unexpected findings.
- Contextual understanding: Qualitative research is well-suited to exploring the social and cultural context in which individuals or groups are situated. Researchers can gather information about cultural norms, social structures, and historical events that may influence participants’ experiences and perspectives.
- Participant perspective : Qualitative research prioritizes the perspective of participants, allowing researchers to explore subjective experiences and understand the meanings that participants attach to their experiences.
- Theory development: Qualitative research can contribute to the development of new theories and insights about complex social phenomena. By gathering rich, detailed data and using inductive data analysis, researchers can develop new theories and explanations that may challenge existing understandings.
- Validity : Qualitative research can offer high validity by using multiple data collection methods, purposive and diverse sampling, and researcher reflexivity. This can help ensure that findings are credible and trustworthy.
Limitations of Qualitative Research
Qualitative research also has some limitations, including:
- Subjectivity : Qualitative research relies on the subjective interpretation of researchers, which can introduce bias into the research process. The researcher’s perspective, beliefs, and experiences can influence the way data is collected, analyzed, and interpreted.
- Limited generalizability: Qualitative research typically involves small, purposive samples that may not be representative of larger populations. This limits the generalizability of findings to other contexts or populations.
- Time-consuming: Qualitative research can be a time-consuming process, requiring significant resources for data collection, analysis, and interpretation.
- Resource-intensive: Qualitative research may require more resources than other research methods, including specialized training for researchers, specialized software for data analysis, and transcription services.
- Limited reliability: Qualitative research may be less reliable than quantitative research, as it relies on the subjective interpretation of researchers. This can make it difficult to replicate findings or compare results across different studies.
- Ethics and confidentiality: Qualitative research involves collecting sensitive information from participants, which raises ethical concerns about confidentiality and informed consent. Researchers must take care to protect the privacy and confidentiality of participants and obtain informed consent.
Also see Research Methods
About the author

Muhammad Hassan
Researcher, Academic Writer, Web developer
You may also like

Questionnaire – Definition, Types, and Examples

Case Study – Methods, Examples and Guide

Observational Research – Methods and Guide

Quantitative Research – Methods, Types and...

Qualitative Research Methods

Explanatory Research – Types, Methods, Guide
Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals
- Explore content
- About the journal
- Publish with us
- Sign up for alerts
- Published: 22 March 2008
Methods of data collection in qualitative research: interviews and focus groups
- P. Gill 1 ,
- K. Stewart 2 ,
- E. Treasure 3 &
- B. Chadwick 4
British Dental Journal volume 204 , pages 291–295 ( 2008 ) Cite this article
1.69m Accesses
1041 Citations
40 Altmetric
Metrics details
Interviews and focus groups are the most common methods of data collection used in qualitative healthcare research
Interviews can be used to explore the views, experiences, beliefs and motivations of individual participants
Focus group use group dynamics to generate qualitative data
Qualitative research in dentistry
Conducting qualitative interviews with school children in dental research
Analysing and presenting qualitative data
This paper explores the most common methods of data collection used in qualitative research: interviews and focus groups. The paper examines each method in detail, focusing on how they work in practice, when their use is appropriate and what they can offer dentistry. Examples of empirical studies that have used interviews or focus groups are also provided.
You have full access to this article via your institution.
Similar content being viewed by others

Interviews in the social sciences

A review of technical and quality assessment considerations of audio-visual and web-conferencing focus groups in qualitative health research
Professionalism in dentistry: deconstructing common terminology, introduction.
Having explored the nature and purpose of qualitative research in the previous paper, this paper explores methods of data collection used in qualitative research. There are a variety of methods of data collection in qualitative research, including observations, textual or visual analysis (eg from books or videos) and interviews (individual or group). 1 However, the most common methods used, particularly in healthcare research, are interviews and focus groups. 2 , 3
The purpose of this paper is to explore these two methods in more detail, in particular how they work in practice, the purpose of each, when their use is appropriate and what they can offer dental research.
Qualitative research interviews
There are three fundamental types of research interviews: structured, semi-structured and unstructured. Structured interviews are, essentially, verbally administered questionnaires, in which a list of predetermined questions are asked, with little or no variation and with no scope for follow-up questions to responses that warrant further elaboration. Consequently, they are relatively quick and easy to administer and may be of particular use if clarification of certain questions are required or if there are likely to be literacy or numeracy problems with the respondents. However, by their very nature, they only allow for limited participant responses and are, therefore, of little use if 'depth' is required.
Conversely, unstructured interviews do not reflect any preconceived theories or ideas and are performed with little or no organisation. 4 Such an interview may simply start with an opening question such as 'Can you tell me about your experience of visiting the dentist?' and will then progress based, primarily, upon the initial response. Unstructured interviews are usually very time-consuming (often lasting several hours) and can be difficult to manage, and to participate in, as the lack of predetermined interview questions provides little guidance on what to talk about (which many participants find confusing and unhelpful). Their use is, therefore, generally only considered where significant 'depth' is required, or where virtually nothing is known about the subject area (or a different perspective of a known subject area is required).
Semi-structured interviews consist of several key questions that help to define the areas to be explored, but also allows the interviewer or interviewee to diverge in order to pursue an idea or response in more detail. 2 This interview format is used most frequently in healthcare, as it provides participants with some guidance on what to talk about, which many find helpful. The flexibility of this approach, particularly compared to structured interviews, also allows for the discovery or elaboration of information that is important to participants but may not have previously been thought of as pertinent by the research team.
For example, in a recent dental public heath study, 5 school children in Cardiff, UK were interviewed about their food choices and preferences. A key finding that emerged from semi-structured interviews, which was not previously thought to be as highly influential as the data subsequently confirmed, was the significance of peer-pressure in influencing children's food choices and preferences. This finding was also established primarily through follow-up questioning (eg probing interesting responses with follow-up questions, such as 'Can you tell me a bit more about that?') and, therefore, may not have emerged in the same way, if at all, if asked as a predetermined question.
The purpose of research interviews
The purpose of the research interview is to explore the views, experiences, beliefs and/or motivations of individuals on specific matters (eg factors that influence their attendance at the dentist). Qualitative methods, such as interviews, are believed to provide a 'deeper' understanding of social phenomena than would be obtained from purely quantitative methods, such as questionnaires. 1 Interviews are, therefore, most appropriate where little is already known about the study phenomenon or where detailed insights are required from individual participants. They are also particularly appropriate for exploring sensitive topics, where participants may not want to talk about such issues in a group environment.
Examples of dental studies that have collected data using interviews are 'Examining the psychosocial process involved in regular dental attendance' 6 and 'Exploring factors governing dentists' treatment philosophies'. 7 Gibson et al . 6 provided an improved understanding of factors that influenced people's regular attendance with their dentist. The study by Kay and Blinkhorn 7 provided a detailed insight into factors that influenced GDPs' decision making in relation to treatment choices. The study found that dentists' clinical decisions about treatments were not necessarily related to pathology or treatment options, as was perhaps initially thought, but also involved discussions with patients, patients' values and dentists' feelings of self esteem and conscience.
There are many similarities between clinical encounters and research interviews, in that both employ similar interpersonal skills, such as questioning, conversing and listening. However, there are also some fundamental differences between the two, such as the purpose of the encounter, reasons for participating, roles of the people involved and how the interview is conducted and recorded. 8
The primary purpose of clinical encounters is for the dentist to ask the patient questions in order to acquire sufficient information to inform decision making and treatment options. However, the constraints of most consultations are such that any open-ended questioning needs to be brought to a conclusion within a fairly short time. 2 In contrast, the fundamental purpose of the research interview is to listen attentively to what respondents have to say, in order to acquire more knowledge about the study topic. 9 Unlike the clinical encounter, it is not to intentionally offer any form of help or advice, which many researchers have neither the training nor the time for. Research interviewing therefore requires a different approach and a different range of skills.
The interview
When designing an interview schedule it is imperative to ask questions that are likely to yield as much information about the study phenomenon as possible and also be able to address the aims and objectives of the research. In a qualitative interview, good questions should be open-ended (ie, require more than a yes/no answer), neutral, sensitive and understandable. 2 It is usually best to start with questions that participants can answer easily and then proceed to more difficult or sensitive topics. 2 This can help put respondents at ease, build up confidence and rapport and often generates rich data that subsequently develops the interview further.
As in any research, it is often wise to first pilot the interview schedule on several respondents prior to data collection proper. 8 This allows the research team to establish if the schedule is clear, understandable and capable of answering the research questions, and if, therefore, any changes to the interview schedule are required.
The length of interviews varies depending on the topic, researcher and participant. However, on average, healthcare interviews last 20-60 minutes. Interviews can be performed on a one-off or, if change over time is of interest, repeated basis, 4 for example exploring the psychosocial impact of oral trauma on participants and their subsequent experiences of cosmetic dental surgery.
Developing the interview
Before an interview takes place, respondents should be informed about the study details and given assurance about ethical principles, such as anonymity and confidentiality. 2 This gives respondents some idea of what to expect from the interview, increases the likelihood of honesty and is also a fundamental aspect of the informed consent process.
Wherever possible, interviews should be conducted in areas free from distractions and at times and locations that are most suitable for participants. For many this may be at their own home in the evenings. Whilst researchers may have less control over the home environment, familiarity may help the respondent to relax and result in a more productive interview. 9 Establishing rapport with participants prior to the interview is also important as this can also have a positive effect on the subsequent development of the interview.
When conducting the actual interview it is prudent for the interviewer to familiarise themselves with the interview schedule, so that the process appears more natural and less rehearsed. However, to ensure that the interview is as productive as possible, researchers must possess a repertoire of skills and techniques to ensure that comprehensive and representative data are collected during the interview. 10 One of the most important skills is the ability to listen attentively to what is being said, so that participants are able to recount their experiences as fully as possible, without unnecessary interruptions.
Other important skills include adopting open and emotionally neutral body language, nodding, smiling, looking interested and making encouraging noises (eg, 'Mmmm') during the interview. 2 The strategic use of silence, if used appropriately, can also be highly effective at getting respondents to contemplate their responses, talk more, elaborate or clarify particular issues. Other techniques that can be used to develop the interview further include reflecting on remarks made by participants (eg, 'Pain?') and probing remarks ('When you said you were afraid of going to the dentist what did you mean?'). 9 Where appropriate, it is also wise to seek clarification from respondents if it is unclear what they mean. The use of 'leading' or 'loaded' questions that may unduly influence responses should always be avoided (eg, 'So you think dental surgery waiting rooms are frightening?' rather than 'How do you find the waiting room at the dentists?').
At the end of the interview it is important to thank participants for their time and ask them if there is anything they would like to add. This gives respondents an opportunity to deal with issues that they have thought about, or think are important but have not been dealt with by the interviewer. 9 This can often lead to the discovery of new, unanticipated information. Respondents should also be debriefed about the study after the interview has finished.
All interviews should be tape recorded and transcribed verbatim afterwards, as this protects against bias and provides a permanent record of what was and was not said. 8 It is often also helpful to make 'field notes' during and immediately after each interview about observations, thoughts and ideas about the interview, as this can help in data analysis process. 4 , 8
Focus groups
Focus groups share many common features with less structured interviews, but there is more to them than merely collecting similar data from many participants at once. A focus group is a group discussion on a particular topic organised for research purposes. This discussion is guided, monitored and recorded by a researcher (sometimes called a moderator or facilitator). 11 , 12
Focus groups were first used as a research method in market research, originating in the 1940s in the work of the Bureau of Applied Social Research at Columbia University. Eventually the success of focus groups as a marketing tool in the private sector resulted in its use in public sector marketing, such as the assessment of the impact of health education campaigns. 13 However, focus group techniques, as used in public and private sectors, have diverged over time. Therefore, in this paper, we seek to describe focus groups as they are used in academic research.
When focus groups are used
Focus groups are used for generating information on collective views, and the meanings that lie behind those views. They are also useful in generating a rich understanding of participants' experiences and beliefs. 12 Suggested criteria for using focus groups include: 13
As a standalone method, for research relating to group norms, meanings and processes
In a multi-method design, to explore a topic or collect group language or narratives to be used in later stages
To clarify, extend, qualify or challenge data collected through other methods
To feedback results to research participants.
Morgan 12 suggests that focus groups should be avoided according to the following criteria:
If listening to participants' views generates expectations for the outcome of the research that can not be fulfilled
If participants are uneasy with each other, and will therefore not discuss their feelings and opinions openly
If the topic of interest to the researcher is not a topic the participants can or wish to discuss
If statistical data is required. Focus groups give depth and insight, but cannot produce useful numerical results.
Conducting focus groups: group composition and size
The composition of a focus group needs great care to get the best quality of discussion. There is no 'best' solution to group composition, and group mix will always impact on the data, according to things such as the mix of ages, sexes and social professional statuses of the participants. What is important is that the researcher gives due consideration to the impact of group mix (eg, how the group may interact with each other) before the focus group proceeds. 14
Interaction is key to a successful focus group. Sometimes this means a pre-existing group interacts best for research purposes, and sometimes stranger groups. Pre-existing groups may be easier to recruit, have shared experiences and enjoy a comfort and familiarity which facilitates discussion or the ability to challenge each other comfortably. In health settings, pre-existing groups can overcome issues relating to disclosure of potentially stigmatising status which people may find uncomfortable in stranger groups (conversely there may be situations where disclosure is more comfortable in stranger groups). In other research projects it may be decided that stranger groups will be able to speak more freely without fear of repercussion, and challenges to other participants may be more challenging and probing, leading to richer data. 13
Group size is an important consideration in focus group research. Stewart and Shamdasani 14 suggest that it is better to slightly over-recruit for a focus group and potentially manage a slightly larger group, than under-recruit and risk having to cancel the session or having an unsatisfactory discussion. They advise that each group will probably have two non-attenders. The optimum size for a focus group is six to eight participants (excluding researchers), but focus groups can work successfully with as few as three and as many as 14 participants. Small groups risk limited discussion occurring, while large groups can be chaotic, hard to manage for the moderator and frustrating for participants who feel they get insufficient opportunities to speak. 13
Preparing an interview schedule
Like research interviews, the interview schedule for focus groups is often no more structured than a loose schedule of topics to be discussed. However, in preparing an interview schedule for focus groups, Stewart and Shamdasani 14 suggest two general principles:
Questions should move from general to more specific questions
Question order should be relative to importance of issues in the research agenda.
There can, however, be some conflict between these two principles, and trade offs are often needed, although often discussions will take on a life of their own, which will influence or determine the order in which issues are covered. Usually, less than a dozen predetermined questions are needed and, as with research interviews, the researcher will also probe and expand on issues according to the discussion.
Moderating a focus group looks easy when done well, but requires a complex set of skills, which are related to the following principles: 15
Participants have valuable views and the ability to respond actively, positively and respectfully. Such an approach is not simply a courtesy, but will encourage fruitful discussions
Moderating without participating: a moderator must guide a discussion rather than join in with it. Expressing one's own views tends to give participants cues as to what to say (introducing bias), rather than the confidence to be open and honest about their own views
Be prepared for views that may be unpalatably critical of a topic which may be important to you
It is important to recognise that researchers' individual characteristics mean that no one person will always be suitable to moderate any kind of group. Sometimes the characteristics that suit a moderator for one group will inhibit discussion in another
Be yourself. If the moderator is comfortable and natural, participants will feel relaxed.
The moderator should facilitate group discussion, keeping it focussed without leading it. They should also be able to prevent the discussion being dominated by one member (for example, by emphasising at the outset the importance of hearing a range of views), ensure that all participants have ample opportunity to contribute, allow differences of opinions to be discussed fairly and, if required, encourage reticent participants. 13
Other relevant factors
The venue for a focus group is important and should, ideally, be accessible, comfortable, private, quiet and free from distractions. 13 However, while a central location, such as the participants' workplace or school, may encourage attendance, the venue may affect participants' behaviour. For example, in a school setting, pupils may behave like pupils, and in clinical settings, participants may be affected by any anxieties that affect them when they attend in a patient role.
Focus groups are usually recorded, often observed (by a researcher other than the moderator, whose role is to observe the interaction of the group to enhance analysis) and sometimes videotaped. At the start of a focus group, a moderator should acknowledge the presence of the audio recording equipment, assure participants of confidentiality and give people the opportunity to withdraw if they are uncomfortable with being taped. 14
A good quality multi-directional external microphone is recommended for the recording of focus groups, as internal microphones are rarely good enough to cope with the variation in volume of different speakers. 13 If observers are present, they should be introduced to participants as someone who is just there to observe, and sit away from the discussion. 14 Videotaping will require more than one camera to capture the whole group, as well as additional operational personnel in the room. This is, therefore, very obtrusive, which can affect the spontaneity of the group and in a focus group does not usually yield enough additional information that could not be captured by an observer to make videotaping worthwhile. 15
The systematic analysis of focus group transcripts is crucial. However, the transcription of focus groups is more complex and time consuming than in one-to-one interviews, and each hour of audio can take up to eight hours to transcribe and generate approximately 100 pages of text. Recordings should be transcribed verbatim and also speakers should be identified in a way that makes it possible to follow the contributions of each individual. Sometimes observational notes also need to be described in the transcripts in order for them to make sense.
The analysis of qualitative data is explored in the final paper of this series. However, it is important to note that the analysis of focus group data is different from other qualitative data because of their interactive nature, and this needs to be taken into consideration during analysis. The importance of the context of other speakers is essential to the understanding of individual contributions. 13 For example, in a group situation, participants will often challenge each other and justify their remarks because of the group setting, in a way that perhaps they would not in a one-to-one interview. The analysis of focus group data must therefore take account of the group dynamics that have generated remarks.
Focus groups in dental research
Focus groups are used increasingly in dental research, on a diverse range of topics, 16 illuminating a number of areas relating to patients, dental services and the dental profession. Addressing a special needs population difficult to access and sample through quantitative measures, Robinson et al . 17 used focus groups to investigate the oral health-related attitudes of drug users, exploring the priorities, understandings and barriers to care they encounter. Newton et al . 18 used focus groups to explore barriers to services among minority ethnic groups, highlighting for the first time differences between minority ethnic groups. Demonstrating the use of the method with professional groups as subjects in dental research, Gussy et al . 19 explored the barriers to and possible strategies for developing a shared approach in prevention of caries among pre-schoolers. This mixed method study was very important as the qualitative element was able to explain why the clinical trial failed, and this understanding may help researchers improve on the quantitative aspect of future studies, as well as making a valuable academic contribution in its own right.
Interviews and focus groups remain the most common methods of data collection in qualitative research, and are now being used with increasing frequency in dental research, particularly to access areas not amendable to quantitative methods and/or where depth, insight and understanding of particular phenomena are required. The examples of dental studies that have employed these methods also help to demonstrate the range of research contexts to which interview and focus group research can make a useful contribution. The continued employment of these methods can further strengthen many areas of dentally related work.
Silverman D . Doing qualitative research . London: Sage Publications, 2000.
Google Scholar
Britten N . Qualitative interviews in healthcare. In Pope C, Mays N (eds) Qualitative research in health care . 2nd ed. pp 11–19. London: BMJ Books, 1999.
Legard R, Keegan J, Ward K . In-depth interviews. In Ritchie J, Lewis J (eds) Qualitative research practice: a guide for social science students and researchers . pp 139–169. London: Sage Publications, 2003.
May K M . Interview techniques in qualitative research: concerns and challenges. In Morse J M (ed) Qualitative nursing research . pp 187–201. Newbury Park: Sage Publications, 1991.
Stewart K, Gill P, Treasure E, Chadwick B . Understanding about food among 6-11 year olds in South Wales. Food Culture Society 2006; 9 : 317–333.
Article Google Scholar
Gibson B, Drenna J, Hanna S, Freeman R . An exploratory qualitative study examining the social and psychological processes involved in regular dental attendance. J Public Health Dent 2000; 60 : 5–11.
Kay E J, Blinkhorn A S . A qualitative investigation of factors governing dentists' treatment philosophies. Br Dent J 1996; 180 : 171–176.
Pontin D . Interviews. In Cormack D F S (ed) The research process in nursing . 4th ed. pp 289–298. Oxford: Blackwell Science, 2000.
Kvale S . Interviews . Thousand Oaks: Sage Publications, 1996.
Hammersley M, Atkinson P . Ethnography: principles in practice . 2nd ed. London: Routledge, 1995.
Kitzinger J . The methodology of focus groups: the importance of interaction between research participants. Sociol Health Illn 1994; 16 : 103–121.
Morgan D L . The focus group guide book . London: Sage Publications, 1998.
Book Google Scholar
Bloor M, Frankland J, Thomas M, Robson K . Focus groups in social research . London: Sage Publications, 2001.
Stewart D W, Shamdasani P M . Focus groups. Theory and practice . London: Sage Publications, 1990.
Krueger R A . Moderating focus groups . London: Sage Publications, 1998.
Chestnutt I G, Robson K F. Focus groups – what are they? Dent Update 2002; 28 : 189–192.
Robinson P G, Acquah S, Gibson B . Drug users: oral health related attitudes and behaviours. Br Dent J 2005; 198 : 219–224.
Newton J T, Thorogood N, Bhavnani V, Pitt J, Gibbons D E, Gelbier S . Barriers to the use of dental services by individuals from minority ethnic communities living in the United Kingdom: findings from focus groups. Primary Dent Care 2001; 8 : 157–161.
Gussy M G, Waters E, Kilpatrick M . A qualitative study exploring barriers to a model of shared care for pre-school children's oral health. Br Dent J 2006; 201 : 165–170.
Download references
Author information
Authors and affiliations.
Senior Research Fellow, Faculty of Health, Sport and Science, University of Glamorgan, Pontypridd, CF37 1DL,
Research Fellow, Academic Unit of Primary Care, University of Bristol, Bristol, BS8 2AA,
Dean and Professor of Dental Public Health, School of Dentistry, Dental Health and Biological Sciences, School of Dentistry, Cardiff University, Heath Park, Cardiff, CF14 4XY,
E. Treasure
Professor of Paediatric Dentistry, School of Dentistry, Dental Health and Biological Sciences, School of Dentistry, Cardiff University, Heath Park, Cardiff, CF14 4XY,
B. Chadwick
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to P. Gill .
Additional information
Refereed paper
Rights and permissions
Reprints and permissions
About this article
Cite this article.
Gill, P., Stewart, K., Treasure, E. et al. Methods of data collection in qualitative research: interviews and focus groups. Br Dent J 204 , 291–295 (2008). https://doi.org/10.1038/bdj.2008.192
Download citation
Published : 22 March 2008
Issue Date : 22 March 2008
DOI : https://doi.org/10.1038/bdj.2008.192
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
This article is cited by
Imprisonment for south ethiopian people living with hiv presents a double health burden: lived experiences of prisoners.
- Terefe Gone Fuge
- George Tsourtos
- Emma R Miller
BMC Health Services Research (2024)
Employees’ experiences of a large-scale implementation in a public care setting: a novel mixed-method approach to content analysis
- My Säfström
- Ulrika Löfkvist
Translating brand reputation into equity from the stakeholder’s theory: an approach to value creation based on consumer’s perception & interactions
- Olukorede Adewole
International Journal of Corporate Social Responsibility (2024)
Heteronormative biases and distinctive experiences with prostate cancer among men who have sex with men: a qualitative focus group study
- Evan Panken
- Noah Frydenlund
- Channa Amarasekera
BMC Urology (2024)
The experience of the irreligious conversion: analysis of the spiritual transition toward skepticism from traditional religions in young adults residing in Santiago, Chile
- Consuelo Calderón Villarreal
SN Social Sciences (2024)
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies


Comparing Focus Groups and In-depth Interviews for Market Research
by MOS Legal | Last updated on May 4, 2024 | Published on Apr 29, 2024 | Interview Transcription

Focus groups and in-depth interviews are feasible methods for doing qualitative market research and understanding the “how” and “why” of decision-making processes. Focus groups bring people together for collaborative conversation, whereas in-depth interviews provide perspectives from people who may have no collective impact. While both approaches are valuable tools for research studies and provide large volumes of data, they are not necessarily interchangeable. An interview transcription service can transcribe both types of interviews into text format to extract valuable information from them.
Focus Groups in Market Research
Focus group interviews involve gathering a group of individuals to provide input on a product. A moderator leads the session and engages with the focus group participants, questioning them about the product. The idea is to start an open and truthful group discussion. Questions are predetermined and used to elicit comprehensive responses from group members. Market research involves not just gathering replies, but also observing reactions. Focus groups provide us a deeper understanding of real-world responses. The similarities and variances among individuals will also be shown. Market analysts use focus groups to acquire vital data. Focus group sessions normally have about ten participants and run about 90 minutes.
Conducting Interviews for Market Research
These are in-depth interviews mainly for collecting qualitative data. Researchers ask the recruited respondents questions and encourage them to provide insightful answers. In-depth interviews typically include open-ended questions, making them perfect for gathering relevant information about a product or service. These interviews are generally the best option for gaining a deeper understanding of a subject. Participants in in-depth interviews have the interviewer’s entire attention, allowing them to delve further into the topic matter. Such interviews are particularly useful for understanding the decision-making process. The talk revolves around a unique experience that can provide deep insights. Face-to-face interviews can run anywhere from 45 to 60 minutes.
Always Remember Pragmatics
While the study’s intent should always be used to drive selection, so should more pragmatic objectives. Obtaining information is the primary purpose. Apart from event rates, there are other factors to consider.
- Variety – Studies that span a large demography will require the same variety in their study. While interviews can be useful in certain situations, focus groups often allow researchers to acquire information without sacrificing accuracy.
- Representation – Access is one of the most important aspects of qualitative research. Based on the rate of responses and availability, an interview may be the study’s only option.
- Detail – While interviewers have more room for detail, focus groups provide a completely different type of detail. Depending on the topic, researchers may want to observe how a decision is reached or obtain feedback from a group.
Which Method to Choose?
The decision between focus groups and interviews is influenced by a variety of criteria, including research objectives, money, timeframe, and target audience.
Here are some factors for selecting the right approach:
- Depth versus breadth : In-depth interviews are helpful for gaining thorough insights into individual perspectives. Focus groups are an effective way to investigate multiple perspectives and group dynamics. Focus groups are more beneficial in the early stages of research whereas in-depth interviews are better suited to the latter stages of research.
- Resource allocation : Take into account the available resources, such as budget, time, and manpower. In-depth interviews may demand more resources per participant, whereas focus groups can accommodate numerous participants in a single session.
- Research goals : Align the chosen method with the unique study goals. Focus groups are useful for testing concepts, generating ideas, and investigating group norms. Individual interviews, on the other hand, are ideal for delving into personal experiences, preferences, or sensitive themes.
- Consider participants’ preferences and comfort levels : Some people prefer the secrecy and seclusion of individual interviews, but others like group contact in focus groups.
Do you want help with recruitment?
Read our blog post How Do Interview Transcription Services Help HR in Recruiting
Both focus groups and in-depth interviews have distinct advantages for acquiring qualitative data for market research. Understanding their differences and strengths enables researchers to make more educated judgments based on research objectives, participant profiles, and resource availability. Choosing the proper approach allows researchers to unearth useful insights that enable informed decision-making and successful outcomes in market research projects. Interview transcription services can efficiently transcribe both focus group and in-depth interviews for market research by utilizing skilled transcribers, innovative technology, and customizable methodologies.
Transform your interviews into actionable insights with our services.
Call us at (800) 670-2809!
Recent Posts
How to use media transcription services for a better workflow.
Media transcription is converting spoken language from audio or video files into text. The process involves transcribing every word, ensuring accuracy and reliability. Media transcription services play a crucial role in various industries, offering numerous benefits...
How Telephone Transcription Enhances Accessibility
In the fast-paced business world, countless crucial conversations unfold over the telephone. From pivotal meetings and insightful interviews to collaborative conference calls and customer interactions, recalling the specifics of these interactions can be challenging....
Podcasting with Impact: Steps to Successfully Publish Your Podcast Transcripts
Over the past decade, there has been a significant rise in the number of Americans tuning in to podcasts. According to the "The Infinite Dial" report by Edison Research, as of 2023, 42% of Americans age 12 and above had listened to a podcast in the previous month....
Transforming Legal Workflow: How AI Enhances Deposition Transcription
Assessing the credibility of a key witness before a trial through the deposition process is crucial and often pivotal to the outcome. Deposition transcripts serve as valuable evidence, allowing lawyers to evaluate the credibility of a witness, uncover information that...
What Is Business Transcription? Let’s Dig Deeper
Capturing and preserving information is crucial, especially in today's fast-paced business world. That's where business transcription services come in. But what exactly is it, and how can it benefit your organization? Let's delve deeper. Simply put, business...
Related Posts

Interview Transcription Tactics: Best Practices for Efficiency and Accuracy
by Julie Clements | Feb 16, 2024 | Interview Transcription
As a journalist, researcher, content creator, or other professional, conducting interviews to gather firsthand accounts of experiences or opinions is an essential aspect of your work. When it comes to transcribing these interviews, accuracy and efficiency are crucial...

6 Tips to Transcribe Remote Interviews
by MOS Legal | Aug 1, 2023 | Interview Transcription , Digital Transcription
The prevalence of remote work has increased significantly in recent times. Remote interviews have become a crucial part of the hiring process. Interview transcription services are available to document remote interviews. Transcripts enable hiring managers to review interview highlights or occurrences that are ..

Interviewing Techniques for Assessing Soft Skills: Evaluating Communication, Teamwork, and Adaptability
by Julie Clements | Jul 4, 2023 | Digital Transcription , Interview Transcription
When hiring candidates for a particular role, employers look beyond technical skills. They look for soft skills — those interpersonal and personal attributes that define how we interact with others and navigate the complexities …
- Open access
- Published: 02 May 2024
General practice nurse perceptions of barriers and facilitators to implementation of best-practice dementia care recommendations—a qualitative interview study
- Caroline Gibson 1 , 4 ,
- Dianne Goeman 1 , 5 ,
- Dimity Pond 6 ,
- Mark Yates 2 , 4 &
- Alison Hutchinson 3 , 5
BMC Primary Care volume 25 , Article number: 147 ( 2024 ) Cite this article
57 Accesses
Metrics details
Introduction
With an aging population and a growing prevalence of people living with dementia, the demand for best-practice dementia care in general practice increases. There is an opportunity to better utilise the nurse role within the primary care team to meet this increasing demand in the provision of care for people living with dementia. However, general practice nurses have limited knowledge in the provision of best-practice care for people living with dementia and their carer(s). A number of best-practice dementia care recommendations contained in the Australian Clinical Practice Guidelines and Principles of Care for People with Dementia have been identified as highly relevant to the role of the general practice nurse.
To explore general practice nurses’ perspectives on published best-practice dementia care recommendations relevant to their role and identify barriers and facilitators to their implementation into clinical practice.
Thirteen Australian general practice nurses took part in this qualitative interview study. The research questions for this study were addressed within a paradigmatic framework of social constructionism. Data were transcribed verbatim and thematically analysed.
There was a high level of agreement between general practice nurses that the recommendations were important, reflected best-practice dementia care and were relevant to their role. However the recommendations were perceived as limited in their usefulness to nurses’ clinical practice due to being too vague and lacking direction. Four main themes were identified describing barriers and facilitators to operationalising best-practice dementia care.: creating a comfortable environment; changing approach to care; optimising the general practice nurse role and working collaboratively. Nine sub-themes were described: physical environment; social environment; complexity of care; care planning for the family; professional role and identity, funding better dementia care, education, networking and resources; different roles, one team; and interagency communication.
This study identified several factors that need addressing to support general practice nurses to integrate best-practice dementia care recommendations into daily clinical practice. The development of interventions needs to include strategies to mitigate potential barriers and enhance facilitators that they perceive impact on their delivery of best-practice care for people living with dementia and their carer(s). The knowledge gained in this study could be used to develop multi-faceted interventions informed by theoretical implementation change models to enable the general practice nurse to operationalise best-practice dementia care recommendations.
Peer Review reports
Dementia is a complex chronic disease and a leading cause of disability among older people [ 1 ]. Worldwide, dementia is expected to affect almost 50 million people, and this number is predicted to double by 2050, placing significant pressure on healthcare systems [ 2 ]. To better meet the chronic and cumulative dementia healthcare needs [ 3 ], there is a growing global health policy commitment to a more proactive approach to the diagnosis and management of people living with dementia (PLWD) in the primary care setting [ 1 ].
Nurses working in general practice, henceforth referred to as general practice nurse (GPN), are significant contributors in the delivery of primary care [ 4 ]. It is well established that GPN interventions in the management of chronic disease lead to cost effective positive health outcomes [ 5 ]. The proactive, planned and person-centred principles of chronic disease management [ 6 ] align with best practice principles of dementia care [ 7 ]. This suggests that chronic disease management models of care can provide a framework for the provision of nursing care to PLWD and their carer(s) [ 8 , 9 ]. However, as GPNs have limited knowledge in the recognition of cognitive impairment and care planning for PLWD [ 10 ], practical guidance could assist them to increase their capability to better meet the diverse and complex needs of PLWD and their carer(s) [ 11 ]. The most effective models of care are informed by evidence-based clinical practice guidelines customised for the intended end-user [ 12 ]. A Delphi study of GPNs’ perceptions of the Australian Clinical Practice Guidelines and Principles of Care for People with Dementia [ 13 ] was recently undertaken to identify the recommendations that were of high relevance to their role. [ 14 ].
While establishing the most relevant guidelines to the GPN role is important, more than guidelines are needed to improve GPNs’ provision of dementia care [ 15 , 16 ]. For GPNs to successfully operationalise best-practice dementia care recommendations in their daily practice, effective implementation strategies guided by theoretical frameworks [ 17 ], need to first consider potential barriers and facilitators [ 16 ]. Whilst barriers to optimal dementia care by the primary care team, with a focus on general practitioners, have been well identified [ 1 , 3 , 18 , 19 , 20 ], few studies have investigated barriers and facilitators specific to the GPN provision of dementia care [ 11 ]. To our knowledge this paper is the first to report on a qualitative study that explores the barriers and facilitators perceived by GPNs to impact on their delivery of published best-practice care recommendations for PLWD and their carer(s).
Research aim
In order to better understand the factors influencing GPNs’ implementation of best-practice dementia care recommendations, the aims of the study were to:
Gain greater insight into GPNs’ perspectives on the recommendations in relation to their delivery of dementia care.
Identify barriers and facilitators to GPNs’ implementation of the recommendations in the General Practice setting.
Study design
The research questions for this study were addressed within a paradigmatic framework of social constructionism. Social constructionism theory is concerned with the processes by which people describe, explain, or account for the world in which they live [ 21 ]. The theory of social constructionism posits that much of what individuals perceive as 'reality' is actually the outcome of a dynamic process of construction influenced by social conventions and structures [ 22 ]. This theory offers a broad lens to explore the ‘reality’ of the nurse provision of dementia care by understanding GPN experience and perceptions of their role and perceived barriers and enablers in provision of best practice dementia care.
A qualitative design with semi-structured interviews was used to explore the views of GPNs in relation to the research questions. Semi-structured interviews have the potential to provide a deeper understanding of participant experience than would be obtained from quantitative methods [ 23 ]. This approach also allowed for the study participants to raise topics important to them that may not have previously been thought of as pertinent by the research team [ 24 ]. The consolidated criteria for reporting qualitative research (COREQ) checklist [ 25 ] was used for reporting the research.
Participants
A purposive sample of Australian GPNs were recruited. The method described by Francis et al. [ 26 ] was used to determine an adequate sample size. Initially, 10 interviews were conducted. Sampling ceased when there were three consecutive interviews without additional themes identified. At the point when no new themes or codes were generated, data saturation was deemed to have been reached [ 27 ].
Recruitment
Participants were recruited through promotion of the study on Australian primary care nursing organisations’ websites and social media. These organisations included the Australian Primary Health Care Nurse Association and Practice Nurse networks. Interested GPNs contacted the primary researcher using the email included in the study promotion. The primary researcher forwarded the participant information and consent form (PICF) to each potential participant. On return of the signed consent form an interview time was arranged. As described in the study promotion, each study participant received a $100 gift card in appreciation of their time and contribution to the study.
Data collection
The interviews were conducted by the primary researcher, a PhD candidate and registered nurse in primary care. The participants were informed the study was part of the primary researchers’ PhD research. No relationship between the interviewer and the participant was established prior to the study commencement. The interviews took place in February and March 2023 using the ZOOM on-line platform [ 28 ]. The demographics survey and interview guide were sent to each study participant with the completed demographics survey returned prior to the interview taking place. The interviews ranged between 21 and 61 min, with an average length of 38 min (total minutes = 498 min). The interview discussion was audio-recorded with consent and transcribed verbatim by a professional medical transcription service. The transcripts were not checked by participants as clarification of meaning was sought at the time of discussion.
Interview guide
The interview guide (Fig. 1 ) was provided to participants prior to the interview so they had time to consider the five recommendations (Fig. 2 ) and the guiding questions. The questions were designed by the authors to probe participant perspectives on topics related to the research question.

Recommendations highly relevant to the GPN role contained in the Australian Clinical Practice Guidelines and Principles of Care for People with Dementia
Data analysis
The data were coded and analysed using Braun and Clarke’s six steps of thematic analysis; familiarisation, generating codes, constructing themes, revising and defining themes and reporting [ 27 ]. All study authors read the transcripts and met to discuss initial impressions of the data in the context of the research aims. Following this, two authors (CG and DG) developed the initial coding framework according to deductive codes identified from study aims and interview guide. CG and DG then independently conducted deductive and inductive coding of three interviews and met again to note any new codes and establish agreement in the final analytic coding framework. The transcribed interviews and codes were entered into the NVivo11 qualitative software [ 29 ]. CG and DG then independently coded all data by systematically going through each transcript, highlighting meaningful salient text and attaching an appropriate code from the final analytic coding framework. When new concepts emerged, the coders met to discuss and propose additional inductive codes. Any discrepancies were resolved via consensus The transcripts were reviewed to apply new codes. Each code was noted as either ‘barrier’ or ‘facilitator’, depending on the context in which the code occurred. An example of the coding framework is described in Table 1 .
The data analysis phase was designed to maximise trustworthiness and authenticity. Using a systematic approach to develop the coding framework provided rigour with inter-rater reliability testing [ 30 ] and an auditable trail of evidence for data transparency enhanced the credibility of findings [ 31 ]. The primary researcher (CG) maintained a diary of subjective involvement in the study for reflexive analysis with the aim of reducing researcher bias in the data analysis, acknowledging her own subjectivity as a nurse with GPN experience and the influence that this may have had on the study.
Patient and public involvement
There was no patient or public involvement in this study. However, consumers were involved in the development of the Australian Clinical Practice Guidelines and Principles of Care for People with Dementia [ 13 ] from which the five recommendations discussed by the study participants were drawn.
Ethics approval
This project was approved by the University of Newcastle’s Human Research Ethics Committee, Approval No. H – 2022 0363.
Thirteen GPNs participated in the study (Table 2 ). The participants were all female, aged between 30 and 69 years. Ten (77%) participants had 6 years or more experience as a general practice nurse. All participants had experience in chronic disease management. Ten (77%) participants self-reported participating in dementia training, although the type of training was not specified. All Australian states were represented except Tasmania. The two territories were not represented.
GPNs’ perceptions of recommendations overall
Overall, GPNs thought there was a great deal of overlap between the five recommendations and that all were important in delivering care to people living with dementia. Some GPNs chose more than one of the five recommendations as important; some said all were. All the GPNs also described limitations in the usefulness of the recommendations to their clinical practice. For example, they were described as “ long and wordy " (GPN 1), “ waffly ” (GPN 8), “ fluffy ” (GPN 5) and “ repetitive and overlapping’ ”(GPN 10). The GPNs wanted guidelines and recommendations that were easily “a ccessible [and] just make it smart and encompass the majority of what we need to be doing” (GPN 8).
In the interviews, the study participants did not discuss each recommendation separately and specifically. They considered the recommendations in the context of the provision of dementia care overall and the barriers and facilitators often portrayed the same phenomenon from different angles. The four themes and nine sub-themes were identified that described the GPNs perspectives on the factors that impacted on good dementia care provision are presented in Fig. 3 .

GPN perceptions of the five recommendations—themes and sub-themes
Theme Creating a comfortable environment
Sub-theme physical environment.
The majority of GPNs highlighted the physical environment of the general practice clinic as a significant barrier to the provision of good dementia care as “the environment is not set up for people with dementia. It's not a good place to have them in. When we’re even bringing them down into the consulting rooms, even though it's a quiet space, it's very distracting. Even the carers are distracted when they come and see us, so you don't get as much information even out of the carer. I think in primary care, if we could give them more care in the home where they're comfortable and supported, that would be much more ideal than what we're doing at my practice anyway”. (GPN4).
Sub-theme Social environment
In addition to providing a better environment for the provision of care, conducting a home visit was also seen as facilitating better care as it provided contextual understanding of the impact of dementia on the person and carer(s). One nurse described how a home visit provided information that potentially delayed entry into permanent care.
“you can see for yourself about how they're actually managing, and they're happy, because she is at home, … and they’re both managing, and they’ve got services in place … their house is clean, there's no clutter, there's ramps, there's grab rails. …. You can let the GP know. You can stop pushing and pressing for them to go into care because at the moment they're actually managing okay. Why ruin that?” (GPN 13).
The therapeutic nurse-patient relationship was viewed as an important element of creating a supportive environment. The building of rapport and trust enabled the nurse to “ have those difficult conversations that people don’t like to have. But they're important to have, and then if a patient feels that they can open up to you, and trust you, they tell the nurses very different things than they tell the doctors” (GPN 13) . The GPNs felt that a positive nurse-patient relationship also created a safe environment, which could help mitigate the social stigma of dementia and fear and denial of the condition that were described as barriers to the provision of appropriate care. Dementia was described as “ one of those illnesses where it's still hidden. Families don't want to admit that they've got a patient or a relative with dementia. It's hard” (GPN 8). The GPNs felt that they had the potential to “make it not a scary subject, because a lot of people link it with dying. It's like blowing the lid off, letting the cat out of the box that it's not a dirty secret, there’s nothing to be ashamed of.” (GPN 10) It was also felt that it was important to reassure people that the nurse’s role was to provide support to live at home. “ They do have that really preconceived idea, the first thing they say is what—when I say what’s your plan for the next phase of your life? I am not going into a nursing home, that’s the first thing they say to me and I’m going okay, well, that’s not my job to tell you to go to a nursing home. It’s to provide support” (GPN 9).
Theme Changing approach to care
Sub-theme complexity of care.
All the GPNs described that providing care for PLWD was different to routine care and required a change in approach. However, many of the study participants felt there was a lack of knowledge and skills to provide care to meet the complex needs of PLWD. “You're just expecting—when you see a name and an age and a medical history on a file, you're expecting a certain flow to go to that consult. When they arrive, it all goes out the window, and then you're floundering wondering how on earth you can help this person in the same way that you would help others. It's really, it's such a difficult presentation to deal with. If you don't have nurses in general practice that understand how to care for someone with dementia, trying to treat them like somebody without it, you're going to miss things. So, I think we do need to alter the way that we care for people with dementia, and I don't think that nurses in general practice are really trained in how to do that” (GPN 4).
A few GPNs stated that it was essential to consider the impact of dementia when providing chronic disease management for other conditions. “If you’ve got someone who comes in with diabetes and they have a cognitive impairment, and you wanted to address the diabetes… It changes the way you approach [the care]. The nurses who aren’t so confident don’t want to talk about problems with dementia, but they’re talking about diabetes with someone, and ignore the other parts…you can’t, it’s all rolled into the one patient that you’re dealing with, not the one disease. If they’re doing a care plan and the patient has diabetes and dementia, they need to be on equal status… …so that you don’t miss one and highlight the other one” (GPN 12).
There was agreement amongst all GPNs that dementia could not be ignored. Early recognition and provision of care was perceived as essential to preventing future problems. “Prevention is better than cure… prevent the complications of cognitive decline in patients by implementing services and strategies before it gets too bad. When you start to notice that it's mild and patients’ relatives are starting to notice changes too, that is when you intervene, not when it's six months later and they can’t tell you what their name is. Early intervention is key” (GPN 12).
Identifying health and social care needs and linking people with community support services was perceived as a key element in the provision of dementia care to both the PLWD and their carer(s). “ Being able to navigate where services could be implemented to assist, community-based services, respite, extra nursing support “ ( GPN 13) and “get those support services in earlier, I say to them, you'll be able to be more independent, more safe, [stay] longer in your house” ( GPN 3). One GPN went so far as to state that “a good practice or a good practice nurse knows what's available in her community ” (GPN 2). However, all the GPNs acknowledged that it was difficult to know what services were available and this lack of knowledge was a barrier to care. “ If we’ve got the knowledge of how to help and point people in the right direction, it makes such a big difference. But it’s tricky if we’re lacking the knowledge of where to send people to or providing that service ” (GPN 11). GPNs stated that locating services was “ a minefield in itself… each area seems very different about what support is out there” (GPN 9) and there is a constant need to “keep up with what services are around your local area, because that's constantly changing” (GPN 3).
All GPNs talked about the complexity of the health and social care needs associated with dementia as a barrier to care. “ [providing care] covers everything from their ability to drive, their ability to stay at home, their planning for the future, advanced care plans, power of attorney, it’s pretty overwhelming… It can sometimes be a really slow, slow process” (GPN 3). Taking it slowly, however, was seen as a facilitator as it allowed time to build trust and be respectful of changing needs “[the GPN] shouldn’t address everything all at once, it should be a step-by-step process, help, when and how they want the help, I can suggest things one year, and the next year I go back, and it's like, have you done anything about that? No, no. It's like, okay. It can sometimes be a really slow, slow process. That's fine, because that's building the trust, it should be a step-by-step process” (GPN 9).
Continuity of care was perceived as important to regular reviews and providing care to address the changing needs of PLWD. However, the study participants described how a largely part-time and stressed workforce were significant barriers to continuity of care. “I think the fact that most of us don’t work full-time its difficult following up. Just having different nurses in their care, is often a big barrier. If they’re coming back to see the same nurse, then you can follow-up on their care. Okay, that didn’t work. Let’s try this. What about we put this into place? Let’s tweak that. It’s a huge workload and you’re just trying to get through everyone, get through people, get people sorted. Then if referrals get lost, how do we know? People fall through the cracks” (GPN 11).
Sub-theme Care planning for the family
GPNs described how the provision of care usually focuses on one patient’s needs, the goals they identify and the actions they agree to undertake. However, when providing care for a PLWD it is necessary to involve the carer(s) in care planning and decision-making. One nurse said “ being able to tailor an individualised plan for a family, would be my ideal world situation” (GPN 6). Part of the care provision for the PLWD was to provide support to the carer to maintain their own health and well-being particularly given the carer role in enabling the PLWD to remain living in the community as their cognitive decline progresses.
“There needs to be a more detailed assessment ongoing evaluation of both them and how their carers are coping, because it gets missed until there’s a big crash and burn, … because if you don’t care for the carer the house is going to fall apart. It will collapse” (GPN 12).
Theme Optimising the role general practice nurse
Sub-theme professional role and identity.
All GPNs in the study perceived the nurse to be the best primary care health professional to provide dementia care. “We are perfectly suited. We already know [the patient and family], we’ve got a rapport … they appreciate my effort, and they sense the caring. They will come and see me where they may not see your experts, because it's all too hard or intimidating. You do have a knowledge base, everyone is so lost and frightened and scared, just even if you don't do jack except be there and say, oh this must be really unsettling for all of you, or wow, you're doing a fantastic job. You have done something for that person already, or by people carer and the person. The general practice nurse is totally underutilised, they're in the perfect place. They have the knowledge, they have the rapport, they have the skills. You need to use them pretty much” (GPN 5).
The GPNs felt that part of their value in dementia care was that, unlike the doctor, they could provide more holistic psychosocial care “with a GP, it's time pressured…that whole psychosocial aspect doesn’t ever get met, or it's pushed to the back and it's like, okay, we’ll deal with that later. That later, never comes. So, I know, as a nurse, I do a lot of that listening to the family members. The doctor is just there to write my scripts and send me for referrals, and fix me, but the nurse will take care of me. So, I think it's the value of having a nurse within a general practice is huge. I would say for any patient that has dementia, is just to have regular reviews with the nurse, we can prevent hospitalisations” (GPN 13).
The majority of nurses discussed a lack of empowerment as a health professional, which was perceived as demoralising and a barrier to provision of dementia care. “If it was more nurse led, I believe the nurses would actually be more inclined to follow up and do something on it. But we make these recommendations to the doctor and expect that they follow up on it. The nurse does all of this work, makes recommendations to the doctor, and then the doctor goes, okay, well, all right, we’ll order you a blood test, okay, see you next week. Yeah. It's so frustrating. Then the nurses just go, well, what's the point in doing all of this work?” (GPN 6). One nurse described how being respected professionally facilitated care. “ I'm very lucky where I am. I've got great GPs and they do take what I say not just, oh, she's just the nurse, and she’s trying to just make me busy or do something, find something that’s not there. They actually respect my position, and my knowledge, and experience and say, oh, okay, if that’s what you think let’s bring him back next week, and let’s do a memory test and let’s take it from there” (GPN 13 ).
Sub-theme Funding better dementia care
Australian general practice funding is paid on a fee-for-service basis, with GPs paid for each service they provide. Study participants stated the primary care funding model does not allow for the time required to provide care for PLWD and carer(s) “ because you’re dealing in general practice with an adult in a time slot that is [not]altered for people with dementia or Alzheimer's. We're just expected to care for them in the same timeframe with the same amount of funding as what we get for everybody else. It doesn't work” (GPN 4).
The GPNs all agreed that the primary care funding model also restricted their ability to involve the carer. “there should be a Medicare rebate allowing the family member or the caregiver to come for an appointment and sit down, speak to us without having to bring the actual person who the appointment's about with them because it's ridiculous that they have to have that family member in the building for us to see them. We'll quite often have our people cancel appointments because it's not a good day to bring them out. Then what that does to their caregiver mentally, they're needing to come for support and someone to talk to about what's happened, and they've now had to cancel the appointment because they don't want to take their loved one out that particular day. It's just not very supportive” (GPN 4).
All GPNs believed that funding nurse-led dementia care would facilitate the delivery of best-practice dementia care and that the PLWD and or their carer(s) should be able to “ make an appointment with the nurse. You don’t need to have the doctor involved. The nurse can actually just say these are the steps that we would need to do, where do you think your parent is at, what sort of support work would you like. That’s all pretty easy to do. Then you bring the doctor in as needed rather than the other way around. You can say all right, well, it sounds like we need to make an appointment with mum, I’ll do a 75-year-old assessment, then they’ll see the doctor. I’ll make sure that the doctor’s on board with what you’d like to happen and it might take three or four visits to get this all happening” (GPN 9).
Sub-theme Education, networking and resources
A lack of organisational investment in primary care nurse formal dementia education was perceived as a significant barrier to increasing knowledge and skills. “I know in the hospitals, often they get paid education days—tell me the last nurse who got paid a paid education day. Why does the practice not just go, okay, our needs are dementia, okay, we're going to send you guys to these courses on these days. But it's because practices, usually they're privately run, they don't get funding from the government to send nurses to those kinds of things so they don't. We don't have time to take time off work to go and seek out education” (GPN 6). They expressed frustration that there would not be an expectation for other health professionals to work in areas they were not trained for. “during the appointments you just feel like just out of your depth really, you've got an adult coming in for an issue that you see all the time, but they don't act the same as your adult population. So, I feel like it should almost be categorised like the way that they provide us with specialist training. If you're going into paediatrics, you know that you're going into an environment where things are very different, and you're given that information and that help and support on how to manage. But you're not really given that information, help or support on how to change your behaviour to get what you need and to give what you need to people with dementia” (GPN 4).
All the GPNs in the study discussed the value of mentoring and networking as effective ways of learning new knowledge and skills and receiving support if they were unsure of what to do. “I really like the idea of networking and getting people from other practices to share how they change their practice or how they can manage, having support that way. Maybe creating a community of care amongst nurses designed around people caring for dementia. I'm part of a wound care group. So, we meet once a month at a place and discuss different issues in wound care. Having something like that for dementia where you meet up with the other nurses and just have those conversations about what they've struggled within their practice, how they've overcome and that support, I think that would be amazing” (GPN 3).
All the GPNs wanted easily accessible resources that provided direction on what to do “ it needs to be a bit of a one-stop shop. So, if they do this, if their memory’s 19, okay, this is what you might consider next; what’s the next step? Have you considered their driver’s license? Have you considered support in the home? Even before that, it’s like ticking off advanced care plans, guardianship, power of attorney…obviously it’s going to be like a basic guideline, you’re not going to get everything into it. But just to give you a bit of an idea. Okay, does the GP know? Have you done an MMSE? Then work out a referral pathway from there” (GPN 11).
Theme Working collaboratively
Sub-theme different roles, one team.
Collaboration both within the general practice clinic and with external agencies was perceived by all GPNs as a facilitator for dementia care. A hierarchical structure with a separation of the GP, GPN and receptionist role, and a perceived lack of trust that the GP will inetegrate the nurse’s findings into their management, compromised the ability of the nurse to provide dementia care. “we need to be able to work as a team more efficiently … there's the doctor and then there's the nurse and then there's a receptionist after that—and they actually do play a big part in a lot of ways as well. The nurses and doctors [need to] see that we're actually on the same team doing two different parts, and it's not as much of a hierarchy as it is a team. Like, we make our recommendations to the doctor and then we have to trust that the doctor will pass them on and implement them. But often that doesn't happen… if you look at a hospital, if they have a patient who has a difficult, complex case in a hospital, they call a multidisciplinary team together with the family and they sit down and they create a care plan for them. Yes, it is usually a short-term plan to achieve a common goal, but that's what they do. But I guess it would be cool to see us in general practice doing that with the doctor. We might not be able to get the other disciplines in clinic and that's fair, but between the nurses and the GPs to go clinically, GPs, you can order this range of tests and this is necessary and, nurses, we can do this, this and this. That would be cool to see and we would be able to create a more individualised plan for the patients then” (GPN 6).
Subtheme Interagency communication
The lack of shared information between health and community service agencies was seen as a significant barrier to the provision of care to PLWD and their carer(s). “ there needs to be increased interagency communication. The left hand needs to know what the right hand is doing. A little less bureaucracy and a bit more sharing of information, if it’s health professional sharing information, it should be allowable. You’re not gossiping" (GPN 1).
The GPNs reported that the lack of communication with other agencies involved in a patient’s care led to poor care continuity and difficulty in ensuring the PLWD and carer(s’) needs were being met. “if I can [find] out [from the community care provider] what’s happening. Then if there [are] holes and cracks, when I see that patient next time, I can go, oh okay. I see that this, this and this has been done. Okay, what’s happening now? Something else has happened. Okay, we need to sort that and you might need this. Then get them back in and add another referral in. Whereas now they’re coming back and you don’t know what’s happened or what has been done” (GPN 11). One GPN reported how good collaborative relationships with other care providers facilitated provision of care “There’s two homecare providers in town that I’ve actually got very good rapport with. They let me know if there’s issues. If there’s issues, something like, you know, they’re not taking [their medications] the message gets back to the homecare support supervisor who gets in touch with me and we work out what happens next” (GPN 12).
The emphasis on care for PLWD and their carer(s) is increasingly focussed on supporting people and families to live as well as possible with dementia across the disease trajectory [ 32 ]. Optimising the role of GPNs has the potential to deliver best-practice dementia care in the primary care setting where dementia is reluctantly disclosed, poorly recognised, under diagnosed, and less than optimally managed [ 1 ]. In this study, the GPNs thought that the five published best-practice dementia care recommendations contained in the Australian Clinical Practice Guidelines and Principles of Care for People with Dementia [ 13 ] as best-practice dementia care and highly relevant to the role of the GPN [ 14 ] were too vague to easily put into practice. The study participants reported that they considered all five of the recommendations were important in delivering care to people living with dementia. The study participants reported multiple barriers and facilitators to their implementation.
As reported in previous studies, the GPNs in this study strongly believed that they were better suited than the general practitioner to provide care for PLWD and their carer(s) and should be included in a team-based approach to care [ 11 ]. All study participants perceived their approach to care as holistic [ 11 , 33 ] based on building therapeutic relationships, which is well established as essential to the delivery of person-centred dementia care [ 34 , 35 ]. This approach to care underpins all five best-practice recommendations under investigation in this study [ 14 ]. The strong belief they could support PLWD and their carer(s) was perceived as a significant facilitator to the implementation of best practice dementia care recommenndations into daily practice by the GPN.
Further facilitators to the implementation of the best-practice dementia care recommendations identified by the GPNs in this study included being proactive in having a conversation about dementia, integrating dementia into other chronic disease management care delivery, and taking a dyadic approach to care. These elements of care are supported in the literature as essential in meeting the health and social care needs of both the PLWD and the carer(s). Stigma, fear and denial are significant barriers to people concerned about their cognition and or families seeking out information and support [ 36 ]. The use of effective and thoughtful communication by GPNs can potentially mitigate stigmatizing beliefs and stereotypes associated with dementia and encourage open conversations [ 37 ]. Findings of studies in primary care suggest that supporting the PLWD without due consideration of the carer(s) can result in poorer health outcomes for both [ 3 , 38 ]. GPNs already have a well-established and accepted role in chronic disease management [ 39 ]. Given that it is common for PLWD to have at least one other long-term health condition [ 32 , 40 ] and higher rates of hospitalisation compared with people living without dementia [ 41 ], high-quality care needs to address the impact of dementia in all chronic disease management interventions.
All GPNs in this study described a lack of knowledge and skills as a barrier to provision of best-practice dementia care, particularly in recognising potential dementia, initiating a conversation about cognition and knowing what services were available to support PLWD and their carer(s). Poor knowledge and skills is well recognised as a barrier to dementia care provision; however, few formal education programs target GPNs [ 42 ] and it is known that translation of education, particularly as a single activity, to clinical practice is poor [ 3 , 41 , 43 ]. In this study GPNs highly valued access to peer support through informal networking, mentorship, and formal and informal access to specialist support as opportunities to improve knowledge, skills and confidence. This was, in part, due to the reported barriers to accessing formal education, including lack of funding, time and organisational support. It is known that networking and mentoring can facilitate communication and knowledge sharing between nurses and offer opportunities for peer support [ 41 ] and, with the increasing acceptability and use of technology-based meetings, may be a more flexible and accessible alternative to formal training programs, particularly for sole practitioners and those working in rural and remote healthcare settings [ 44 ]. However, the design and implementation of networking strategies, such as communities of practice, that effectively support information sharing and knowledge transfer is not well understood [ 44 ].
All the GPNs in this study reported a need for easily accessible resources, including guidelines, checklists and care pathways, to inform best-practice dementia care. To our knowledge there are limited resources available targeting GPNs. It is also well-established that guidelines do not always impact clinical practice change [ 16 ]. Care pathways have been described in the literature as a process to develop and implement well-organised care and improve quality and efficiency [ 45 ]. Effective care pathways depend on enhanced team work [ 45 ] and a lack of team work was identified by all GPNs as a significant barrier to best practice dementia care. This suggests that general practice team culture change would be needed as part of the developmemt and implementation of dementia care pathways.
Environmental contexts, including primary care funding models, the internal general practice team culture, limited open communication with external agencies and a largely part-time nurse workforce presented significant barriers to GPNs providing best-practice dementia care. Nurses employed in general practice in the main work for either small businesses or corporate chains and do not generate income unless working under the direction of the general practitioner. Research has shown that GPNs do not routinely collaborate in patient care and decision-making with the dotor but are delegated tasks that generate income for the practice [ 46 ]. The GPN usually has to rely on the doctor to follow through on the GPN’s recommendations for care which, as reported in this study, often does not happen. This lack of professional autonomy and status and a medical practitioner activity-based funding model further entrench the hierarchy, and as described by nurses in this study, result in the nurses feeling demoralised and disincentivised, presenting a significant barrier to provision of best-practice dementia care. GPNs described the development of trusting practitioner-patient relationships and continuity of care as important in the delivery of person-centred dementia care. However the study participants described themselves as a largely part-time workforce which impeded contiunty of care. Authors of the Australian Primary Care Nurse workforce survey (2019) [ 47 ] reported that 49.6% of survey respondents worked part-time.
Strengths and limitations
A strength of this study was the use of semi-structured interviews to facilitate primary care nurses to contribute, explore and clarify their views on a research topic that little is known. Another strength was the structured analysis process. The high level of agreement between the themes generated independently by the authors increase our confidence in the results.
The use of a convenience sample can decrease trustworthiness. However, including an experienced group of primary care nurses, the majority of which had some degree of dementia training, meant they could actively reflect on and provide insightful responses to the research questions, enriching the findings about their role in the care of people living with dementia.
A limitation was the small sample size as it is likely not representative of all GPNs, however there was considerable consistency in responses. Not all states and territories of Australia were represented in the study population, with no GPNs from the Australian Capital Territory and Northern Territory and Tasmania included. However, as shown in the Australian Primary Care Nurse workforce survey (2019) [ 47 ] these three regions of Australia comprise only 9.4% of the primary location of place of work for Australian GPNs. Similarly, no males participated in the study. In the Australian Primary Care Nurse workforce survey (2019) data [ 47 ] 96.1% of the workforce was female and only 3.8% were male.
Implications of study findings
As the number of PLWD and their carer(s) increases, the GPN role in dementia care provision within the primary care team needs to be optimised. Theoretical frameworks for the development and operationalisation of complex interventions describe. understanding barriers and enablers as an essential initial step. The knowledge gained in this study can potentially inform the development of multi-faceted interventions to support the GPN provision of best practice dementia care.
This study identifies a number of practitioner and organisational level factors that impact on GPNs ability to integrate best-practice dementia care recommendations into daily clinical practice. Strategies to mitigate these barriers and enhance the facilitators that GPNs perceive prevent the delivery of best-practice care for PLWD and their carer(s) need to be implemented.
Availability of data and materials
The transcripts analysed in this study are available from the corresponding author on reasonable request.
Abbreviations
General Practitioner
General Practice Nurse
Person/ People living with Dementia
Aminzadeh F, Molnar FJ, Dalziel WB, Ayotte D. A review of barriers and enablers to diagnosis and management of persons with dementia in primary care. Can Geriatr J. 2012;15(3):85–94.
Article PubMed PubMed Central Google Scholar
Prince M, Comas-Herrera A, Knapp M, Guerchet M, Karagiannidou M. Improving healthcare for people living with dementia. London: Alzheimer’s Disease International (ADI); 2016.
Fox C, Maidment I, Moniz-Cook E, White J, Thyrian JR, Young J, et al. Optimising primary care for people with dementia. Ment Health Fam Med. 2013;10(3):143–51.
PubMed PubMed Central Google Scholar
Norful A, Martsolf G, de Jacq K, Poghosyan L. Utilization of registered nurses in primary care teams: a systematic review. Int J Nurs Stud. 2017;74:15–23.
Stephen C, McInnes S, Halcomb E. The feasibility and acceptability of nurse-led chronic disease management interventions in primary care: an integrative review. J Adv Nurs. 2018;74(2):279–88.
Article PubMed Google Scholar
Noel MA, Kaluzynski TS, Templeton VH. Quality dementia care: integrating caregivers into a chronic disease management model. J Appl Gerontol. 2017;36(2):195–212.
Reuben DB, Epstein-Lubow G, Evertson LC, Jennings LA. Chronic disease management: why dementia care is different. Am J Manag Care. 2022;28(12):e452–4.
Frost R, Rait G, Aw S, Brunskill G, Wilcock J, Robinson L, Knapp M, Hogan N, Harrison Dening K, Allan L, Manthorpe J, Walters K, PriDem team. Implementing post diagnostic dementia care in primary care: a mixed-methods systematic review. Aging Ment Health. 2021;25(8):1381–94.
Australia D. Submission to the primary health care advisory group. Discussion paper: better outcomes for people with chronic and complex health conditions through primary health care. Melbourne; 2015.
Evripidou M, Charalambous A, Middleton N, Papastavrou E. Nurses’ knowledge and attitudes about dementia care: systematic literature review. Perspect Psychiatr Care. 2019;55(1):48–60.
Gibson C, Goeman D, Hutchinson A, Yates M, Pond D. The provision of dementia care in general practice: practice nurse perceptions of their role. BMC Fam Pract. 2021;22(1):110.
Graham ID, Logan J, Harrison MB, Straus SE, Tetroe J, Caswell W, et al. Lost in knowledge translation: time for a map? J Contin Educ Health Prof. 2006;26(1):13–24.
Guidelines Adaptation Committee. Clinical Practice Guidelines and Principles of Care for People with Dementia. Sydney Australia: NHMRC Partnership Centre for Dealing with Cognitive and Related Functional Decline in Older People; 2016.
Google Scholar
Gibson C, Goeman D, Yates M, Pond D. Identifying the Clinical Practice Guidelines and Principles of Care for People with Dementia relevant to primary care nurse role: a Delphi study Under review. 2022.
Surr CA, Parveen S, Smith SJ, Drury M, Sass C, Burden S, et al. The barriers and facilitators to implementing dementia education and training in health and social care services: a mixed-methods study. BMC Health Serv Res. 2020;20(1):512.
Fischer F, Lange K, Klose K, Greiner W, Kraemer A. Barriers and strategies in guideline implementation—a scoping review. Healthcare. 2016;4(3):36.
Grol R, Grimshaw J. From best evidence to best practice: effective implementation of change in patients’ care. Lancet. 2003;362(9391):1225–30.
Mansfield E, Noble N, Sanson-Fisher R, Mazza D, Bryant J. Primary care physicians’ perceived barriers to optimal dementia care: a systematic review. Gerontologist. 2018;59(6):e697–708.
Article Google Scholar
Phillips J, Pond D, Goode S. Timely diagnosis of dementia: can we do better? A report for Alzheimer's Australia. Paper 24. Canberra; 2011.
Arsenault-Lapierre G, Le Berre M, Rojas-Rozo L, McAiney C, Ingram J, Lee L, et al. Improving dementia care: insights from audit and feedback in interdisciplinary primary care sites. BMC Health Serv Res. 2022;22(1):353.
Crotty Ma. The foundations of social research : meaning and perspective in the research process. London; Thousand Oaks: Sage Publications, 2003. ©1998; 2003.
Berger PL, Luckmann T. The social construction of reality : a treatise in the sociology of knowledge. Harmondsworth: Penguin; 1971.
Britten N. Qualitative interviews in health research. In: Pope C, Mays N, editors. Qualitative research in healthcare. 3rd ed. London: BMJ Books; 2006.
Gill P, Stewart K, Treasure E, Chadwick B. Methods of data collection in qualitative research: interviews and focus groups. Br Dent J. 2008;204(6):291–5.
Article CAS PubMed Google Scholar
Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–57.
Francis JJ, Johnston M, Robertson C, Glidewell L, Entwistle V, Eccles MP, et al. What is an adequate sample size? Operationalising data saturation for theory-based interview studies. Psychol Health. 2010;25(10):1229–45.
Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101.
Banyai I. Zoom. New York: Viking; 1995.
Lumivero (2020) NVivo (Version 13, 2020 R1), www.lumivero.com .
Roberts K, Dowell A, Nie J-B. Attempting rigour and replicability in thematic analysis of qualitative research data; a case study of codebook development. BMC Med Res Methodol. 2019;19(1):66.
Ritchie J, Spencer L. The qualitative researcher's companion. 2002. 2023/09/25. Thousand Oaks. Thousand Oaks, California: SAGE Publications, Inc. Available from: https://methods.sagepub.com/book/the-qualitative-researchers-companion . Accessed 25 Sept 2023.
Bamford C, Wilcock J, Brunskill G, Wheatley A, Harrison Dening K, Manthorpe J, et al. Improving primary care based post-diagnostic support for people living with dementia and carers: developing a complex intervention using the Theory of Change. PLoS One. 2023;18(5):e0283818-e.
Karrer M, Hirt J, Zeller A, Saxer S. What hinders and facilitates the implementation of nurse-led interventions in dementia care? A scoping review. BMC Geriatr. 2020;20(1):1–13.
Manthorpe J, Samsi K. Person-centered dementia care: current perspectives. Clin Interv Aging. 2016;11:1733–40.
Van Mierlo LD, Meiland FJM, Van Hout HPJ, Dröes RM. Toward an evidence-based implementation model and checklist for personalized dementia care in the community. Int Psychogeriatr. 2016;28(5):801–13.
Kim S, Richardson A, Werner P, Anstey KJ. Dementia stigma reduction (DESeRvE) through education and virtual contact in the general public: a multi-arm factorial randomised controlled trial. Dementia (London). 2021;20(6):2152–69.
Harper L, Dobbs BM, Stites SD, Sajatovic M, Buckwalter K, Burgener SC. Stigma in dementia: it’s time to talk about it. Curr Psychiatr. 2019;18(7):16–23.
Parker D, Mills S, Abbey J. Effectiveness of interventions that assist caregivers to support people with dementia living in the community: a systematic review. Int J Evid Based Healthc. 2008;6(2):137–72.
PubMed Google Scholar
Halcomb EJ, Davidson PM, Salamonson Y, Ollerton R, Griffiths R. Nurses in Australian general practice: implications for chronic disease management. J Clin Nurs. 2008;17(5a):6–15.
Bunn F, Burn A-M, Goodman C, Rait G, Norton S, Robinson L, et al. Comorbidity and dementia: a scoping review of the literature. BMC Med. 2014;12(1):1–15.
Sadak T, Borson S. Six domains of health: a practical approach to identifying priorities in dementia care. Front Dement. 2023;2.
Islam MM, Parkinson A, Burns K, Woods M, Yen L. A training program for primary health care nurses on timely diagnosis and management of dementia in general practice: an evaluation study. Int J Nurs Stud. 2020;105:103550.
Perry M, Drašković I, Lucassen P, Vernooij-Dassen M, van Achterberg T, Rikkert MO. Effects of educational interventions on primary dementia care: a systematic review. Int J Geriatr Psychiatry. 2011;26(1):1–11.
James-McAlpine J, Larkins S, Nagle C. Exploring the evidence base for communities of practice in health research and translation: a scoping review. Health Res Policy Syst. 2023;21(1):55.
Vanhaecht K, Panella M, van Zelm R, Sermeus W. An overview on the history and concept of care pathways as complex interventions. Int J Care Pathw. 2010;14(3):117–23.
McInnes S, Peters K, Bonney A, Halcomb E. An integrative review of facilitators and barriers influencing collaboration and teamwork between general practitioners and nurses working in general practice. J Adv Nurs. 2015;71(9):1973–85.
Nguyen VNB, Brand G, Gardiner S, Moses S, Collison L, Griffin K, et al. A snapshot of Australian primary health care nursing workforce characteristics and reasons they work in these settings: a longitudinal retrospective study. Nurs Open. 2023;10(8):5462–75.
Download references
Acknowledgements
Not applicable.
This research contributes to a larger program of work being conducted by the Australian Community of Practice in Research in Dementia (ACcORD), which is funded by a Dementia Research Team Grant (APP1095078) from the National Health and Medical Research Council. Caroline Gibson is supported by a University of Newcastle Postgraduate Research Scholarship from the Faculty of Health and Medicine.
Author information
Authors and affiliations.
University of Newcastle, School of Medicine and Public Health, Callaghan, NSW, 2308, Australia
Caroline Gibson & Dianne Goeman
Deakin University, School of Medicine, Geelong, Australia
Deakin University, School of Nursing and Midwifery, Burwood, Australia
Alison Hutchinson
Grampians Health, Ballarat, Australia
Caroline Gibson & Mark Yates
Faculty of Medicine, Nursing and Health Sciences, The Alfred Centre, Melbourne, Monash University, Clayton, Australia
Dianne Goeman & Alison Hutchinson
University of Tasmania, Wicking Dementia and Teaching Centre, Hobart, Australia
Dimity Pond
You can also search for this author in PubMed Google Scholar
Contributions
CG conceived the study. CG, DG, DP AH and MY contributed to the study design. CG and DG drafted the manuscript. CG and DG independently coded all the data and MY assisted with resolving any discrepancies in the coding. AH, MY and DP provided critical commentary on subsequent versions of the manuscript. All authors have read and approved the final version.
Corresponding author
Correspondence to Caroline Gibson .
Ethics declarations
Ethics approval and consent to participate.
All methods were carried out in accordance with relevant guidelines and regulations.
Informed consent to participate in the study was obtained from all subjects.
Consent for publication
Competing interests.
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Gibson, C., Goeman, D., Pond, D. et al. General practice nurse perceptions of barriers and facilitators to implementation of best-practice dementia care recommendations—a qualitative interview study. BMC Prim. Care 25 , 147 (2024). https://doi.org/10.1186/s12875-024-02401-9
Download citation
Received : 27 November 2023
Accepted : 23 April 2024
Published : 02 May 2024
DOI : https://doi.org/10.1186/s12875-024-02401-9
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- General practice nurses
- Care planning
- Primary care
- Best-practice recommendations
BMC Primary Care
ISSN: 2731-4553
- General enquiries: [email protected]
- Open access
- Published: 05 May 2024
A qualitative interview study to determine barriers and facilitators of implementing automated decision support tools for genomic data access
- Vasiliki Rahimzadeh 1 ,
- Jinyoung Baek 2 ,
- Jonathan Lawson 2 &
- Edward S. Dove 3
BMC Medical Ethics volume 25 , Article number: 51 ( 2024 ) Cite this article
Metrics details
Data access committees (DAC) gatekeep access to secured genomic and related health datasets yet are challenged to keep pace with the rising volume and complexity of data generation. Automated decision support (ADS) systems have been shown to support consistency, compliance, and coordination of data access review decisions. However, we lack understanding of how DAC members perceive the value add of ADS, if any, on the quality and effectiveness of their reviews. In this qualitative study, we report findings from 13 semi-structured interviews with DAC members from around the world to identify relevant barriers and facilitators to implementing ADS for genomic data access management. Participants generally supported pilot studies that test ADS performance, for example in cataloging data types, verifying user credentials and tagging datasets for use terms. Concerns related to over-automation, lack of human oversight, low prioritization, and misalignment with institutional missions tempered enthusiasm for ADS among the DAC members we engaged. Tensions for change in institutional settings within which DACs operated was a powerful motivator for why DAC members considered the implementation of ADS into their access workflows, as well as perceptions of the relative advantage of ADS over the status quo. Future research is needed to build the evidence base around the comparative effectiveness and decisional outcomes of institutions that do/not use ADS into their workflows.
Peer Review reports
Introduction
Genomics is among the most data-prolific scientific fields and is expected to surpass the storage needs and analytic capacities of Twitter, YouTube, and astronomy combined by as soon as 2025 [ 1 ]. To meet rising demands for genomic data and their efficient collection and use, national genomics initiatives [ 2 ] rely on largescale repositories to pool data resources and incentivize data sharing [ 3 , 4 , 5 ]. The “data commons” model has since become the flagship approach for many of these initiatives [ 6 ], and prioritizes research collaboration and data access over proprietary exclusion in the data [ 3 ]. Data access committees (DACs) are principally charged with ensuring only bona fide researchers conducting research permitted by participants’ informed consent are approved to access the data [ 7 ]. DACs are typically staffed by research compliance officers, researchers, and sometimes data security professionals. DAC members can be paid or serve as volunteers and, at a basic level, arbitrate access to data given requests meet minimum requirements for data protection and compliance. Critiques of compliance-only responsibilities and the growing appreciation of data privacy risks among the general public has raised questions about whether DACs ought to weigh in on issues of social and scientific value of the data projects [ 8 ]. Our prior empirical work [ 9 ] suggests there is debate around this scope of DAC oversight, particularly as it relates to considerations of data ethics that are traditionally the domain of institutional ethics committees.
Cheah and Piasecki, for example, propose that DACs have responsibilities to both promote data sharing and protect the interests of individuals and communities about whom the shared data relate: “data access should be granted as long as the data reuse fulfils the criterion of having even a minimal social value, and minimal risk to data subjects and their communities” [ 7 ]. In this way, DACs anchor responsible data sharing ecosystems since they govern access to and compliant use of genomic and, increasingly, other health data [ 10 , 11 , 12 ].
However, DACs may not contribute to efficient data access provisions as effectively as other review models may allow [ 13 ]. In the standard model of data access review, DACs manually review a data requester’s application and assess it against pre-defined criteria. Criteria may include appropriateness of the data requested, data use terms set by data providers, and data privacy and security requirements set by the institution and by law [ 7 ]. As with most, if not all, human-mediated activities, manual review of these criteria can be a laborious and error-prone process. For example, DACs may interpret language describing permitted data uses differently, and the terms themselves can sometimes be ambiguous [ 14 ]. Faced with this ambiguity, DACs are forced to make subjective judgments about whether requests for data access truly align with permitted data uses, if these permissions have been preserved at all. Inconsistencies in how data use terms are articulated in consent forms and subsequently interpreted and executed by DACs across the biomedical ecosystem [ 14 ] can lead to delayed and inconsistent data access decisions, and risk violating the terms by which patients or participants contributed their data in the first place.
Other steps in the data access pipeline can also contribute to research delays. Emerging research suggests there is growing inefficiency, inconsistency, and error in the manual, entirely human-mediated review of data access agreements [ 13 , 15 ] which are executed in finalizing approved data access requests. Many researchers furthermore still rely on the traditional method of copying-and-downloading data once approved. The copy-download approach multiplies security risks [ 11 ], and is quickly becoming unreasonable given the expanding size and complexities of genomic datasets [ 16 , 17 ].
Standards’ developers and software engineers have therefore sought to semi-automate three axes of data access control within cloud environments – user authentication, review of access requests, and concordance of the proposed research with the data use terms of the data requested [ 14 ]. Automated decision support (ADS) systems are a coordinated system of algorithms, software, and ontologies [ 18 ] that aid in categorizing, archiving, and/or acting on decision tasks for data access review. The Data Use Oversight System (DUOS) typifies one such automated decision support [ 19 ]. In recent beta tests, DUOS was successfully shown to concur 100% of the time with human-decided access requests [ 15 ], and also codifies 93% of genomic datasets in NIH’s dbGaP [ 20 ].
While ADS can supplement human DACs with semi-automated technical solutions, no systematic investigation has sought to characterize relevant barriers and facilitators to ADS in practice [ 21 ]. Moreover, we lack understanding of how DAC members perceive the value added by ADS, if any, on the quality and effectiveness of data access review decisions, as well as what challenges they anticipate in adopting ADS considering the myriad organizational structures within which DACs operate.
Now is an opportune time to study the implementation barriers and facilitators to using ADS solutions for data access as their development converges with large-scale data migration to the cloud that can result in near-instant data access decisions. The genomics community can learn important lessons from previous attempts at (premature) ADS implementation without purposeful stakeholder engagement in public health [ 22 ], law enforcement [ 23 ] and in clinical care [ 24 ]. In this article, we report empirical findings on the “constellation of processes” relevant for implementing ADS for genomic data access management and provide practical recommendations for institutional data stewards that are considering or have already implemented ADS in this context.
We conducted a qualitative description study that engaged prospective end users of ADS for genomic data governance to explore: What are the barriers and opportunities of implementing automated workflows to manage access requests to genomic data collections, and what effect do ADS have on DAC review quality and effectiveness? We adopted Damshroder and colleagues’ definition of implementation as the “critical gateway between an organizational decision to adopt an intervention and the routine use of that intervention” [ 25 ] in order to “study the constellation of processes intended to get an intervention into use within an organization” [ 25 ]. We applied the Consolidated Framework for Implementation Research (CFIR) to compare genomic data access processes and procedures to better understand implementation processes for automated workflows to manage genomic data access across international, publicly funded genomic data repositories. The CFIR provides a “menu of constructs” associated with five domains of effective implementation which have been rigorously meta-theorized—that is, synthesized from many implementation theories (Fig. 1 ). In addition, the CFIR provides a practical guide to systematically assess potential barriers and facilitators ahead of an innovation’s implementation (L. Damschroder et al. 2015). The CFIR is also easily customizable to unveiling bioethical issues during implementation in genomics and has been applied in prior work (Burke and Korngiebel, 2015; Smit et al., 2020).

Adapted Consolidated Framework for Implementation Research (CFIR) and associated domains (Intervention Characteristics, Individuals, Process, Inner Setting, Outer Setting) used to structure 13 qualitative interviews on the relevant factors mediating implementation of automated decision support tools for genomic data access management and sharing among publicly funded genomic data repositories worldwide
The interview guide was developed specifically for this study and is available in Supplementary Materials 2 .
Data collection
We conducted a total of 13 semi-structured interviews with 17 DAC members between 27 April and 24 August 2022. Prospective interviewees indicated their interest in being invited to a follow up interview following their participation in a previous survey published elsewhere [ 9 ]. All interviews were conducted virtually and audio/video recorded on Zoom. We used validated interview guides from the official CFIR instrument repository ( https://cfirguide.org/evaluation-design/qualitative-data/ ) to probe the barriers and opportunities of implementing ADS solutions for DAC review of data access requests. Interviews lasted between 45 and 60 min and included 29 questions adapted from the CFIR instrument to fit the ADS context (e.g. Inner Setting, Outer Setting, Intervention Characteristics etc.). The specific interview guide used is available in Supplementary Materials 2 . Interviewees were also recruited from the Data Access Committee Review Standards Working Group (DACReS WG) chaired by authors VR, JL, and ESD, as well as from an internet search of publicly funded genomic data repositories worldwide.
Data analysis
We first applied a deductive coding frame to the interview transcripts based on a framework analysis approach (Pope, Ziebland, and Mays 2000) and the publicly accessible CFIR codebook available in the Supplemental Materials 1 . To ensure the reliability of conclusions drawn, two independent reviewers (VR and JB) tested the coding schema on three transcripts until reaching a recommended interrater reliability score of 0.83 before analyzing the remaining qualitative dataset. All coding discrepancies during the coding pilot were resolved by consensus discussion.
Geographical, Institutional, and Demographic Background of Participants
41% of interviewees worked within U.S.-based DACs, while the remaining 59% of interviewees represented DACs at institutions in Canada, the U.K., Spain, Tunisia, Australia, and Japan (Table 1 ). Nearly 60% of interviewees worked at a non-profit research institute, 24% represented an academic-affiliated research institution, 12% represented a government research agency, and 6% were affiliated with a research consortium. 76% of interview participants identified as female, and 24% as male.
Opportunities for ADS
We categorized the frequency of CFIR implementation factors referenced in our interviews in Table 2 . Our findings suggest that there are three major facilitators to implementing ADS for genomic data governance: (1) external policy and need for efficient workflows, (2) institutional ability to scale the ADS, and (3) interoperability.
External policy and need for efficient workflows
Participants considered adopting ADS to comply with new data sharing mandates from research funders (e.g. National Institutes of Health) and those imposed by peer reviewed journals. The demand for and scope of compliant data access review has had a ripple effect on ethics oversight bodies [ 26 ], including DACs, as a result of these new requirements [ 9 ]. Most DAC members we engaged with currently perform their reviews manually. Members review all data access requests individually or as a committee and make decisions on each request received in the order they were received. Given the anticipated increase in the number of data access requests [ 27 ], our participants noted the reduced workload and costs associated with ADS could contribute to better review efficiencies, without a concomitant loss in review quality and risk of noncompliance with data use conditions.
We found that participants perceived that ADS could reduce DAC member workload by streamlining the intake process for data access requests and verifying that the request matched the terms of use in the original consent obtained at data collection. Indeed, participants noted the initial screening of Data Access Requests (DARs) was a common rate-limiting step in the submission to decision process. DACs often begin the review process by verifying that all necessary information is documented in the request (e.g. study purpose, datasets requested, ethics review). This step can be time-consuming because the requirements can vary depending on the researcher’s institution and the datasets they request. We requested that participants share a copy of their DAR form before, during, or after the interview to compare what information DACs typically required to process a DAR. We found the form fields as well as length of the DAR (from 3 to 18 pages) differed considerably. Our participants believed that this is where ADS could be useful by automatically flagging missing information and documents, verifying the authenticity of a requester’s identity and the submitted documents, and then sending notifications to requesters if more information is needed. As one interviewee put it:
Because one of the biggest concerns in our DAC is that sometimes it takes too much time to be read by all the nine members. … They’re institutional directors or university professors. So I think it will help. Maybe if you have 50% of the work done by an automated system, so you just have to do the 50%. I think … this will be a good motivation for them saying ‘OK’ [to implement ADS]. ‑ Participant M.
Scalability and cost effectiveness
Participants also believed ADS-enabled workflows could be scalable, cost-effective solutions to management of not just newly generated data, but also for legacy data when grant funding ends because ADS can easily store and quickly present data use conditions and audit past DAC reviews. Two interviewees discussed the challenges of finding cost effective solutions to managing legacy datasets:
Actually there are lots of costs related to data sharing, particularly if I’m sharing data from the 1990s, for example. I don’t have any money or budget anymore to prepare the data [for secondary uses]. … And similarly, when it comes to these reports [on data sharing activities], there’s no extra money for doing the work to create those reports. But we’re having to report back over assets from years, decades in fact. And there was always just a little bit of a hint ‘oh well, maybe we’ll find some money’. No, no, you have to find it out on your own. ‑ Participant F. I mean potentially as we grow over the years, you know what’s going to happen. … we’ve also discussed some scenarios, where, for example, we find ourselves with a larger amount of requests coming in, [and] we only accept applications up to certain days and then, we open this next quarter, close it again. But there potentially could be room for automation depending on the increase in request in the coming years. ‑ Participant A.
Retention and sustainability of human resources
Participants also discussed retention of repository staff and DAC membership as an evolving human resource factor that would motivate ADS adoption. For example, some participants shared that ADS could be helpful when DAC members or data generators leave the institution, disrupting review continuity and consistency. Unlike for large, well-funded government repositories, many DACs at smaller institutions lack human resources to ensure long-term data preservation and access management for data of increasing complexity and volume:
As the program scales, the participant diversity scales, the data diversity scales. I think it is almost impossible to see a scenario where we do not rely on some level of automation to support human decision making about what is responsible use. ‑ Participant J.
Interoperability
According to the DAC members we interviewed, ADS tools could provide centralized, interoperable solutions to facilitate inter-organizational and international data sharing. Participants perceived that ADS could motivate use of standardized request forms, access agreements, dataset identifiers, and methods for verifying researcher identities. For example, one participant commented:
But this [ADS] will free up a lot of time in the process is it also potentially means that it will become easier for, if you’re working in a team to hand off tasks as well because you will have a single system. … Also, consistency between organizations. If we have multiple organizations take this up, it’s going to mean less lead time. [Let’s] say people take a new job in a new place. We’ll actually have some software that people will recognize and be able to use and uptake, which we’ve been trying to go towards without ethics approval processes within the hospital and health services… [standardized] systems makes it easier for actual communication between organizations on processes, because everyone kind of begins to know what’s happening. ‑ Participant E.
(b) Barriers to implementing ADS .
Despite clear advantages of ADS for genomic data access management, our interviewees identified significant barriers to implementation within DAC workflows, including: (1) lower priority compared to more immediate governance challenges, (2) ill equipped personnel and structures within the institution, (3) costs, and (4) degree of human oversight.
Prioritization
Many participants reported that institutional leadership prioritized other competing research data needs over investing in new data governance structures (e.g. generating quality data, increasing diversity in datasets, collaborating with underrepresented groups of researchers and participants, and releasing datasets). Participants believed researchers in general understand why quality and effective review of data access is important for responsible genomic data sharing but are firstly concerned with data quality. Another suspected reason that ADS implementation ranked lower on institutional priorities was that there had not yet been a significant data incident. As one participant put it:
I don’t think that the program thinks it is a very high priority to streamline any of the [data access oversight] process. I think that it will either take something bad happening and then realizing that we need additional capacities on [DAC], or some other hiccup to really promote that need. ‑ Participant O.
Because budgets for data governance are not always included in grants, researchers may be less motivated to invest in the additional, largely unpaid work related to data governance. Insufficient resourcing for data sharing and governance mechanisms prospectively in research study design inevitably challenge the downstream execution of data governance upon deposit of the research data once generated, according to at least one DAC member we interviewed:
We found that some people don’t prioritize [data governance] because it’s not helpful to them, because it’s not our primary function as a department. You know, we’re producing new data. That’s usually what people, researchers are doing. They’re not thinking about what happens to their old data. So, it’s not much of a priority. Having said that, research funders are getting very keen for us to use their data. So, there is that sort of tug [of war]. … If I go into a senior team meeting, you know, something else will be the priority. ‑ Participant F.
Structural characteristics of an organization
We also found a close correlation between several structural characteristics of the institution (e.g. years in operation, number of personnel, and database size) and participants’ perceived barriers to ADS implementation. For instance, many participants served on DACs that were established within the last 1–3 years coinciding with the creation of the institution’s database. As the datasets grow, and more researchers are attracted to the resource, there is greater potential to overwhelm existing management processes. It is precisely at this early juncture that DACs would benefit from weighing their ADS options, and proactively address relevant barriers ahead of any plans for implementation. Some DAC members preferred to gain more experience with existing data access management in these early years of data release before integrating ADS “because we’re not sure how [name of participant’s country] citizens feel or consider about the automatic decision on data sharing.” Participant K.
While cost was not a primary concern for ADS implementation at well-funded big data repositories, it was a significant barrier for DAC members working at smaller repositories, individual research departments, or research programs associated with a genomics consortium who were more often supported by research grants or contracts rather than an independent funding source.
“We [data governance office] are supported through project-specific funding. … Governance ends up being a little bit of this indirectly supported component of our work and services. That has limited the ways in which we can innovate around governance. … We don’t have a huge budget.” ‑ Participant N.
Without dedicated budget for human and material resources, some DAC members were concerned that the initial investment in ADS and significant changes to current workflows would be key issues, to say nothing of new education and training materials and updates to internal policies, among other ancillary revisions to internal workflows.
Lack of human oversight
While some DAC members were enthusiastic about improvements in efficiency and consistency of ADS, participants unanimously rejected the idea of fully automating access management: “no matter what we do with automation that I feel there always needs to be that human element who’s coming in and checking. So, there will always be that barrier to upscaling” Participant E. Other participants emphasized that prior to implementation, they would need to gauge how research participants at their own institution as well as the general public would react to ADS for data access review.
Participants were also skeptical that ADS could adequately assess complex, sensitive data reuse issues which they felt required a deep understanding of ethical, legal, and sociocultural contexts within which data were collected, used, and shared. Some DAC members reported asking data requesters to clarify their study purpose and justify their need for specific datasets in recognition of these sociocultural dimensions.
I’m also someone who thinks that it’s important to be very critical about what’s the nature of the work being done. Maybe it’s solid from a scientific point of view. But are there other concerns from other perspectives that need to be taken into account? That is partly why we have community members on the [committee], and that’s something I’m not sure can be simplified or automated.”
However, when it comes to automating anything that requires reviewing information where there might be a lot of nuances, where there might be a lot of interpretation that’s required, I’m a little bit more hesitant simply because I think to some extent you do need some room for a little bit of mulling over the information, … and I think there are some information that come through with requests, that don’t neatly fit into check boxes. ‑ Participant B.
Overall, participants perceived that ADS tools could be well positioned to help DACs streamline data access compliance. While believed to beneficial, ADS solutions were unlikely to immediately or directly advance the research organization’s core mission (e.g. collecting quality data and driving scientific discoveries and innovations). One of the most challenging barriers to implementation is the relative low priority of, and lack of institutional investment in, data infrastructures that could adapt as the dynamics of genomic data generation and storage change over time. Participants tended to regard ADS implementation, as well as data governance workflow solutions, as a lower priority compared to regulatory compliance, investigator support, and database curation, among other competing demands on DAC member time.
Most research grants allow investigators to apply for support for data collection and analysis, but rarely establish actual governance structures needed to stand up access management services. We found that executive buy-in was a major driver for ADS support in the cases of some repositories and the lack or administrative or leadership buy in a major detractor for others, namely repositories at smaller research institutions or laboratories. Therefore, part of the challenge of making ADS adoption a higher institutional priority is convincing institutional leadership of their added value and the net benefit of investing in data governance solutions and infrastructures generally.
Delaying infrastructure upgrades has consequences for the future utility of the repository in the longer term. Some of our study participants, for example, believed researchers were drawn to their databases not because of their data access policies and practices, but because of the quality and diversity of their datasets. However, this quality-driven perspective contrasts with findings from a study of genetic researchers suggesting that ease of access is at least marginally important when choosing a database for their research [ 28 ]. We reason that repositories which invest in efficient, scalable, and compliant access decision processes are likely to attract more users to their resources than repositories which do not evolve such processes to meet the pace of data generation and higher data demand. It is also worth noting that funders have a direct role to play in accelerating the pace of data science as researchers are expected to do more with fewer resources and in less time.
Developing more streamlined workflows emerged as a primary benefit that many participants anticipated from adopting ADS. Participants were most enthusiastic about applying ADS for time consuming and tedious tasks, such as preliminary review and quality control checks for data access request forms that are needed to initiate the data access decision process. Applying ADS to facilitate these workflows could free DAC members to dedicate more time to deliberate on more substantive ethics issues raised by data access requests.
While data governance has often been considered auxiliary work, new research findings and new U.S. federal government policies, such as the National Institutes of Health Data Management and Sharing (DMS) Policy, have elevated its importance by placing additional requirements for data sharing [ 29 ]. The new DMS Policy was but one example of distinct legislative reforms that have influenced cultures of data sharing shaping DAC work, as well as the institutional practices and governance tools developed to complement this culture. To be sure, such legislative and institutional context influenced participant responses and particular implementation preparedness factors for ADS such as “structural characteristics of the organization.”
The DMS Policy will accelerate the accumulation of an enormous number of datasets. In the absence of interventions, including but not limited to ADS, the DMS Policy will significantly raise costs associated with data storage and management. We concluded from our participants that databases/repositories are frequently developed specifically to share research data generated from federal funds without attention to existing databases and other resources in mind within which to deposit their data. “Blind” database creation is often done with good intentions; however, it can inadvertently introduce myriad access pathways that make the data effectively “shared” but undiscoverable and is another issue where ADS tools could intervene. One participant’s narrative about their need to transfer legacy data from a repository facing permanent closure puts the problem of unsustainable databases in sharp relief. The participant’s example suggested that there is need for more efficient and sustainable solutions for data access management and sharing that can endure even when repositories themselves do not. Moreover, there is reasonable cause to have a contingency plan for publicly funded data shared via non-publicly supported repositories in the event the repository closes or changes in policy or personnel. Standardized ADS solutions could easily interoperate between the two types of repositories and facilitate legacy data transfer, if and when required.
Limitations
Our results should be considered in light of several methodological limitations. While geographically diverse, many of our interview participants were affiliated with DACs based at large, well-resourced research institutions. It is likely that responses and perceptions of implementation factors related to ADS would differ substantially if more DACs from low- or under-resourced institutions were represented in our sample. Our data collection design relies on self-reports of institutional data access policy and procedures. Many interview participants were aware of the Global Alliance for Genomics and Health, and the data access committee review standards we were principally involved in developing [ 30 ]. Thus, while we endeavored to create a safe, open environment for participants to share their honest views, social desirability bias related to our prior work may have influenced how participants responded. Lastly, CFIR predefines sociological constructs relevant to implementation. Our analysis was therefore limited only to those constructs covered in the framework, whereas others might have emerged inductively if we adopted an alternative analytic frame.
In this article, we reported findings from semi-structured qualitative interviews with DAC members from around the world on the relevant barriers and facilitators of implementing ADS for genomic data access management. Our findings suggest there is general support for pilot studies that test ADS performance for certain tasks in data access management workflows, such as cataloging data types, verifying user credentials, and tagging datasets for use terms. Participants indicated that ADS should supplement, but not replace, DAC member work. This sentiment was especially strong with respect to tasks that were perceived to require sensitivity and human value-judgments such as privacy protections, group harms, and study purpose. Nonetheless, our findings offer cautious optimism regarding the ways in which algorithms, software, and other machine-readable ontologies could streamline aspects of DAC decision-making while also enabling new opportunities for improving consistency and fairness in DAC decisions.
To that end, we conclude with practical recommendations for institutional data stewards that are considering or have already implemented ADS for data access management. First, repositories and institutions that support databases and other resources should prioritize infrastructural upgrades and factor them into associated budgets. Ensuring proper investment in, and human/material resource support for, these upgrades ensures the repository can help ensure its utility even as the complexity and volume of genomic and associated health datasets grow. Second, DACs should prepare to put in place today what data access management and sharing processes they foresee the repository needing tomorrow. For DAC members looking to integrate ADS or other semi-automated tools into their workflows, buy-in from executive leadership should be obtained at the earliest stages of this transition. DAC members should consider substantiating the need for semi/automated solutions with concrete trend data about the frequency of data access requests relative to the time from request to decision and extrapolate these numbers to judge what the anticipated demand for repository will be in 1, 5, and 10 years. Tracking and transparently reporting data access request volume, access decisions, and other committee operations is likewise important not just for internal purposes, but also to demonstrate responsible data stewardship in action to prospective data contributors.
Third, DACs should refrain from implementing ADS wholesale without complementary human oversight of data access request intake and decisions. Pilot testing where ADS tools can be applied to the most time-consuming tasks will require taking inventory of the inputs required for each task along the data access decision workflow. Fourth, DACs should consider what human and material resources will be needed to integrate ADS effectively. These resources include DAC member expertise, computer equipment, and software development, not to mention member education and training resources. Finally, DACs should collaborate on setting standards for how data access requests should be adjudicated and tailor ADS tools in line with these consensus criteria. There is ongoing work to this effect as part of the Ethical Provenance Subgroup of the Global Alliance for Genomics and Health (including the development of an "Ethical Provenance Toolkit"); additional representation from repositories that steward other diverse health datasets would be ideal to coordinate access management strategies across the field.
The explosion in the volume and complexity of genomic and associated health data is converging with the need to manage access more efficiently to these data. Such trends point intuitively to solutions that can help to alleviate, or at least prevent bottlenecks in the access process to preserve the scientific and social value of data generated from public investments in research. To put ADS solutions to the test, future research should compare access decisions and their outcomes between institutions who do/not use such tools for data access management; and examine whether ADS delivers on its efficiency promises and whether it liberates DAC member time previously spent addressing procedural matters – allowing more opportunities for committee deliberation on substantive ethics issues.
Data availability
Materials described in the manuscript and data supporting our findings can be made available upon request. All requests should be directed to Vasiliki Rahimzadeh, PhD at [email protected].
Stephens ZD, Lee SY, Faghri F, Campbell RH, Zhai C, Efron MJ, Iyer R, Schatz MC, Sinha S, Robinson GE. Big Data: Astronomical or Genomical? PLoS Biol. 2015;13:e1002195. https://doi.org/10.1371/journal.pbio.1002195 .
Article Google Scholar
IQVIA Institute for Human Data. Science understanding the Global Landscape of genomic initiatives: Progress and Promise.
Cook-Deegan R, McGuire AL. Moving beyond Bermuda: sharing data to build a medical information commons. Genome Res. 2017;27:897–901. https://doi.org/10.1101/gr.216911.116 .
Evans B. (2019). Genomic data commons. Governing Privacy in Knowledge Commons, 75–105.
Contreras JL, Knoppers BM. The genomic commons. Annu Rev Genom Hum Genet. 2018;19:429–53. https://doi.org/10.1146/annurev-genom-083117-021552 .
Grossman RL. Ten lessons for data sharing with a data commons. Sci Data. 2023;10:120. https://doi.org/10.1038/s41597-023-02029-x .
Cheah PY, Piasecki J. Data Access committees. BMC Med Ethics. 2020;21:1–8. https://doi.org/10.1186/s12910-020-0453-z .
Murtagh MJ, Blell MT, Butters OW, Cowley L, Dove ES, Goodman A, Griggs RL, Hall A, Hallowell N, Kumari M, et al. Better governance, better access: practising responsible data sharing in the METADAC governance infrastructure. Hum Genomics. 2018;12. https://doi.org/10.1186/s40246-018-0154-6 .
Lawson J, Rahimzadeh V, Baek J, Dove ES. Achieving Procedural Parity in Managing Access to genomic and related Health data: A Global Survey of Data Access Committee members. Biopreserv Biobank. 2023;bio20220205. https://doi.org/10.1089/bio.2022.0205 .
Shabani M, Thorogood A, Borry P. Who should have access to genomic data and how should they be held accountable? Perspectives of Data Access Committee members and experts. Eur J Hum Genet. 2016;24:1671–5. https://doi.org/10.1038/ejhg.2016.111 .
Ramos EM, Din-Lovinescu C, Bookman EB, McNeil LJ, Baker CC, Godynskiy G, Harris EL, Lehner T, McKeon C, Moss J, A Mechanism for Controlled Access to GWAS Data: Experience of the GAIN Data Access Committee. Am J Hum Genet. 2013;92:479–88. https://doi.org/10.1016/j.ajhg.2012.08.034 .
Shabani M, Knoppers BM, Borry P. From the principles of genomic data sharing to the practices of data access committees. EMBO Mol Med. 2015;7:507–9. https://doi.org/10.15252/emmm.201405002 .
Mello MM, Triantis G, Stanton R, Blumenkranz E, Studdert DM. Waiting for data: barriers to executing data use agreements. Science. 2020;367:150–2. https://doi.org/10.1126/science.aaz7028 .
Lawson J, Cabili MN, Kerry G, Boughtwood T, Thorogood A, Alper P, Bowers SR, Boyles RR, Brookes AJ, Brush M, et al. The Data Use Ontology to streamline responsible access to human biomedical datasets. Cell Genomics. 2021;1:100028. https://doi.org/10.1016/j.xgen.2021.100028 .
Lawson J. Empirical validation of an Automated Approach to Data Use Oversight. Cell Genomics Forthcoming; 2021.
Van der Auwera G, O’Connor B. Genomics in the Cloud: using Docker, GATK, and WDL in Terra. 1st ed. O’Reilly Media; 2020.
Birger C, Hanna M, Salinas E, Neff J, Saksena G, Livitz D, Rosebrock D, Stewart C, Leshchiner I, Baumann A, et al. FireCloud, a scalable cloud-based platform for collaborative genome analysis: strategies for reducing and controlling costs. (Bioinformatics). 2017. https://doi.org/10.1101/209494 .
Rahimzadeh V, Lawson J, Rushton G, Dove ES. Leveraging algorithms to improve decision-making workflows for genomic data Access and Management. Biopreserv Biobank. 2022. https://doi.org/10.1089/bio.2022.0042 .
Data Use Ontology. (2022).
Lawson J, Ghanaim EM, Baek J, Lee H, Rehm HL. Aligning NIH’s existing data use restrictions to the GA4GH DUO standard. Cell Genomics. 2023;3:100381. https://doi.org/10.1016/j.xgen.2023.100381 .
Rahimzadeh V, Lawson J, Baek J, Dove ES. Automating justice: an ethical responsibility of computational Bioethics. Am J Bioeth. 2022;22:30–3. https://doi.org/10.1080/15265161.2022.2075051 .
Obermeyer Z, Powers B, Vogeli C, Mullainathan S. Dissecting racial bias in an algorithm used to manage the health of populations. Science. 2019;366:447–53. https://doi.org/10.1126/science.aax2342 .
Hartzog W, Conti G, Nelson J, Shay LA. Inefficiently Automated Law Enforcement. Mich State Law Rev. 2016;1763:1763–96.
Google Scholar
Ledford H. Millions affected by racial bias in healthcare algorithm. Nature. 2019;574:608–10.
Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009;4. https://doi.org/10.1186/1748-5908-4-50 .
Rahimzadeh V, Serpico K, Gelinas L. Institutional review boards need new skills to review data sharing and management plans. Nat Med. 2023;1–3. https://doi.org/10.1038/s41591-023-02292-w .
Cabili MN, Lawson J, Saltzman A, Rushton G, O’Rourke P, Wilbanks J, Rodriguez LL, Nyronen T, Courtot M, Donnelly S, et al. Empirical validation of an automated approach to data use oversight. Cell Genomics. 2021;1:100031. https://doi.org/10.1016/j.xgen.2021.100031 .
Trinidad MG, Ryan KA, Krenz CD, Roberts JS, McGuire AL, De Vries R, Zikmund-Fisher BJ, Kardia S, Marsh E, Forman J, et al. Extremely slow and capricious: a qualitative exploration of genetic researcher priorities in selecting shared data resources. Genet Sci. 2023;25:115–24. https://doi.org/10.1016/j.gim.2022.09.003 .
Final NIH. Policy for Data Management and Sharing https://grants.nih.gov/grants/guide/notice-files/NOT-OD-21-013.html .
Global Alliance for Genomics and Health. (2021). Data Access Committee Guiding Principles and Procedural Standards Policy.
Download references
Acknowledgements
The authors wish to thank members of the Data Access Committee Review Standards Working Group, and the Regulatory and Ethics Work Stream of the Global Alliance for Genomics and Health for their contributions to the intellectual community that inspired this work.
This study was funded by the National Human Genome Research Institute as an Administrative Supplement grant to the AnVIL program for the Study of Bioethical Issues [U24HGO10262].
Author information
Authors and affiliations.
Center for Medical Ethics and Health Policy, Baylor College of Medicine, 1 Baylor Plaza, Suite 310DF, Houston, TX, 77098, USA
Vasiliki Rahimzadeh
Broad Institute of MIT and Harvard, Cambridge, MA, USA
Jinyoung Baek & Jonathan Lawson
School of Law, University of Edinburgh, Edinburgh, UK
Edward S. Dove
You can also search for this author in PubMed Google Scholar
Contributions
Authors VR, JL and ED conceptualized, designed, and carried out the study. Author JB led in the data collection and analysis and drafting of early manuscript drafts. All authors, VR, JB, JL and ED took part in writing and editing the manuscript, responding to peer reviewer comments and approved the final version.
Corresponding author
Correspondence to Vasiliki Rahimzadeh .
Ethics declarations
Ethical approval.
This study was reviewed and approved the Stanford University Institutional Review Board. All participants were informed of the purpose of the study, funding, risks and benefits at the time of invitation. Informed consent was obtained from all participants prior to the interview and participants were provided opportunities to ask any questions about the study procedures.
Consent for publication
Not applicable.
Competing interests
All authors are members of the Regulatory and Ethics Work Stream of the Global Alliance for Genomics and Health. JL is co-lead of the Data Use Ontology, leads the Data Use Oversight System and is a member of the Broad Institute Data Access Committee.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary material 2, rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Rahimzadeh, V., Baek, J., Lawson, J. et al. A qualitative interview study to determine barriers and facilitators of implementing automated decision support tools for genomic data access. BMC Med Ethics 25 , 51 (2024). https://doi.org/10.1186/s12910-024-01050-y
Download citation
Received : 09 January 2024
Accepted : 26 April 2024
Published : 05 May 2024
DOI : https://doi.org/10.1186/s12910-024-01050-y
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Data access committee
- Implementation science
- Decision support
- Genomic data
BMC Medical Ethics
ISSN: 1472-6939
- General enquiries: [email protected]
Root out friction in every digital experience, super-charge conversion rates, and optimise digital self-service
Uncover insights from any interaction, deliver AI-powered agent coaching, and reduce cost to serve
Increase revenue and loyalty with real-time insights and recommendations delivered straight to teams on the ground
Know exactly how your people feel and empower managers to improve employee engagement, productivity, and retention
Take action in the moments that matter most along the employee journey and drive bottom line growth
Whatever they’re are saying, wherever they’re saying it, know exactly what’s going on with your people
Get faster, richer insights with qual and quant tools that make powerful market research available to everyone
Run concept tests, pricing studies, prototyping + more with fast, powerful studies designed by UX research experts
Track your brand performance 24/7 and act quickly to respond to opportunities and challenges in your market
Meet the operating system for experience management
- Free Account
- For Digital
- For Customer Care
- For Human Resources
- For Researchers
- Financial Services
- All Industries
Popular Use Cases
- Customer Experience
- Employee Experience
- Employee Exit Interviews
- Net Promoter Score
- Voice of Customer
- Customer Success Hub
- Product Documentation
- Training & Certification
- XM Institute
- Popular Resources
- Customer Stories
Market Research
- Artificial Intelligence
- Partnerships
- Marketplace
The annual gathering of the experience leaders at the world’s iconic brands building breakthrough business results.
- English/AU & NZ
- Español/Europa
- Español/América Latina
- Português Brasileiro
- REQUEST DEMO
- Experience Management
- Ultimate Guide to Market Research
- Qualitative Research Interviews
Try Qualtrics for free
How to carry out great interviews in qualitative research.
11 min read An interview is one of the most versatile methods used in qualitative research. Here’s what you need to know about conducting great qualitative interviews.
What is a qualitative research interview?
Qualitative research interviews are a mainstay among q ualitative research techniques, and have been in use for decades either as a primary data collection method or as an adjunct to a wider research process. A qualitative research interview is a one-to-one data collection session between a researcher and a participant. Interviews may be carried out face-to-face, over the phone or via video call using a service like Skype or Zoom.
There are three main types of qualitative research interview – structured, unstructured or semi-structured.
- Structured interviews Structured interviews are based around a schedule of predetermined questions and talking points that the researcher has developed. At their most rigid, structured interviews may have a precise wording and question order, meaning that they can be replicated across many different interviewers and participants with relatively consistent results.
- Unstructured interviews Unstructured interviews have no predetermined format, although that doesn’t mean they’re ad hoc or unplanned. An unstructured interview may outwardly resemble a normal conversation, but the interviewer will in fact be working carefully to make sure the right topics are addressed during the interaction while putting the participant at ease with a natural manner.
- Semi-structured interviews Semi-structured interviews are the most common type of qualitative research interview, combining the informality and rapport of an unstructured interview with the consistency and replicability of a structured interview. The researcher will come prepared with questions and topics, but will not need to stick to precise wording. This blended approach can work well for in-depth interviews.
Free eBook: The qualitative research design handbook
What are the pros and cons of interviews in qualitative research?
As a qualitative research method interviewing is hard to beat, with applications in social research, market research, and even basic and clinical pharmacy. But like any aspect of the research process, it’s not without its limitations. Before choosing qualitative interviewing as your research method, it’s worth weighing up the pros and cons.
Pros of qualitative interviews:
- provide in-depth information and context
- can be used effectively when their are low numbers of participants
- provide an opportunity to discuss and explain questions
- useful for complex topics
- rich in data – in the case of in-person or video interviews , the researcher can observe body language and facial expression as well as the answers to questions
Cons of qualitative interviews:
- can be time-consuming to carry out
- costly when compared to some other research methods
- because of time and cost constraints, they often limit you to a small number of participants
- difficult to standardise your data across different researchers and participants unless the interviews are very tightly structured
- As the Open University of Hong Kong notes, qualitative interviews may take an emotional toll on interviewers
Qualitative interview guides
Semi-structured interviews are based on a qualitative interview guide, which acts as a road map for the researcher. While conducting interviews, the researcher can use the interview guide to help them stay focused on their research questions and make sure they cover all the topics they intend to.
An interview guide may include a list of questions written out in full, or it may be a set of bullet points grouped around particular topics. It can prompt the interviewer to dig deeper and ask probing questions during the interview if appropriate.
Consider writing out the project’s research question at the top of your interview guide, ahead of the interview questions. This may help you steer the interview in the right direction if it threatens to head off on a tangent.
Avoid bias in qualitative research interviews
According to Duke University , bias can create significant problems in your qualitative interview.
- Acquiescence bias is common to many qualitative methods, including focus groups. It occurs when the participant feels obliged to say what they think the researcher wants to hear. This can be especially problematic when there is a perceived power imbalance between participant and interviewer. To counteract this, Duke University’s experts recommend emphasising the participant’s expertise in the subject being discussed, and the value of their contributions.
- Interviewer bias is when the interviewer’s own feelings about the topic come to light through hand gestures, facial expressions or turns of phrase. Duke’s recommendation is to stick to scripted phrases where this is an issue, and to make sure researchers become very familiar with the interview guide or script before conducting interviews, so that they can hone their delivery.
What kinds of questions should you ask in a qualitative interview?
The interview questions you ask need to be carefully considered both before and during the data collection process. As well as considering the topics you’ll cover, you will need to think carefully about the way you ask questions.
Open-ended interview questions – which cannot be answered with a ‘yes’ ‘no’ or ‘maybe’ – are recommended by many researchers as a way to pursue in depth information.
An example of an open-ended question is “What made you want to move to the East Coast?” This will prompt the participant to consider different factors and select at least one. Having thought about it carefully, they may give you more detailed information about their reasoning.
A closed-ended question , such as “Would you recommend your neighbourhood to a friend?” can be answered without too much deliberation, and without giving much information about personal thoughts, opinions and feelings.
Follow-up questions can be used to delve deeper into the research topic and to get more detail from open-ended questions. Examples of follow-up questions include:
- What makes you say that?
- What do you mean by that?
- Can you tell me more about X?
- What did/does that mean to you?
As well as avoiding closed-ended questions, be wary of leading questions. As with other qualitative research techniques such as surveys or focus groups, these can introduce bias in your data. Leading questions presume a certain point of view shared by the interviewer and participant, and may even suggest a foregone conclusion.
An example of a leading question might be: “You moved to New York in 1990, didn’t you?” In answering the question, the participant is much more likely to agree than disagree. This may be down to acquiescence bias or a belief that the interviewer has checked the information and already knows the correct answer.
Other leading questions involve adjectival phrases or other wording that introduces negative or positive connotations about a particular topic. An example of this kind of leading question is: “Many employees dislike wearing masks to work. How do you feel about this?” It presumes a positive opinion and the participant may be swayed by it, or not want to contradict the interviewer.
Harvard University’s guidelines for qualitative interview research add that you shouldn’t be afraid to ask embarrassing questions – “if you don’t ask, they won’t tell.” Bear in mind though that too much probing around sensitive topics may cause the interview participant to withdraw. The Harvard guidelines recommend leaving sensitive questions til the later stages of the interview when a rapport has been established.
More tips for conducting qualitative interviews
Observing a participant’s body language can give you important data about their thoughts and feelings. It can also help you decide when to broach a topic, and whether to use a follow-up question or return to the subject later in the interview.
Be conscious that the participant may regard you as the expert, not themselves. In order to make sure they express their opinions openly, use active listening skills like verbal encouragement and paraphrasing and clarifying their meaning to show how much you value what they are saying.
Remember that part of the goal is to leave the interview participant feeling good about volunteering their time and their thought process to your research. Aim to make them feel empowered , respected and heard.
Unstructured interviews can demand a lot of a researcher, both cognitively and emotionally. Be sure to leave time in between in-depth interviews when scheduling your data collection to make sure you maintain the quality of your data, as well as your own well-being .
Recording and transcribing interviews
Historically, recording qualitative research interviews and then transcribing the conversation manually would have represented a significant part of the cost and time involved in research projects that collect qualitative data.
Fortunately, researchers now have access to digital recording tools, and even speech-to-text technology that can automatically transcribe interview data using AI and machine learning. This type of tool can also be used to capture qualitative data from qualitative research (focus groups,ect.) making this kind of social research or market research much less time consuming.
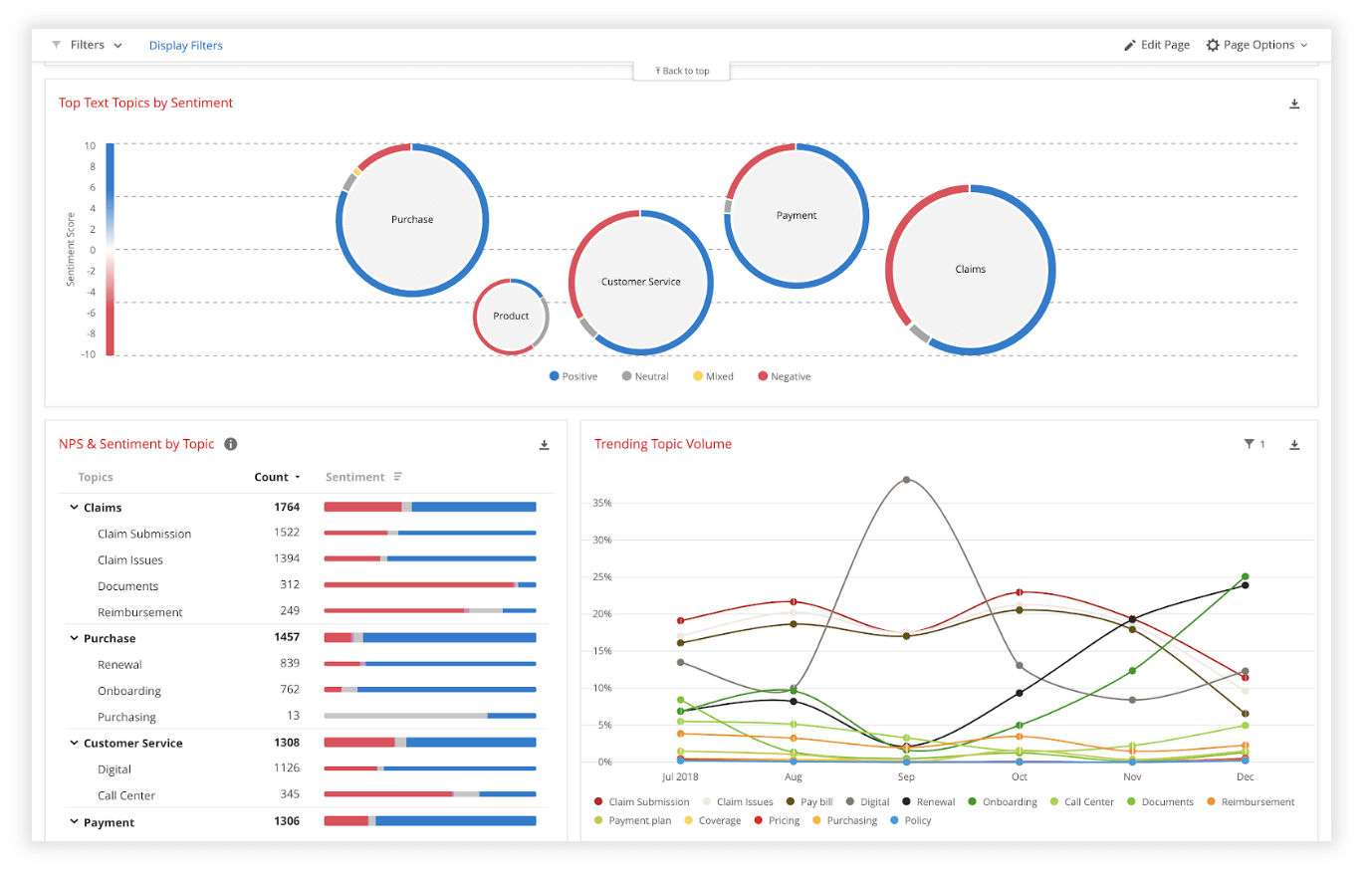
Data analysis
Qualitative interview data is unstructured, rich in content and difficult to analyse without the appropriate tools. Fortunately, machine learning and AI can once again make things faster and easier when you use qualitative methods like the research interview.
Text analysis tools and natural language processing software can ‘read’ your transcripts and voice data and identify patterns and trends across large volumes of text or speech. They can also perform khttps://www.qualtrics.com/experience-management/research/sentiment-analysis/
which assesses overall trends in opinion and provides an unbiased overall summary of how participants are feeling.
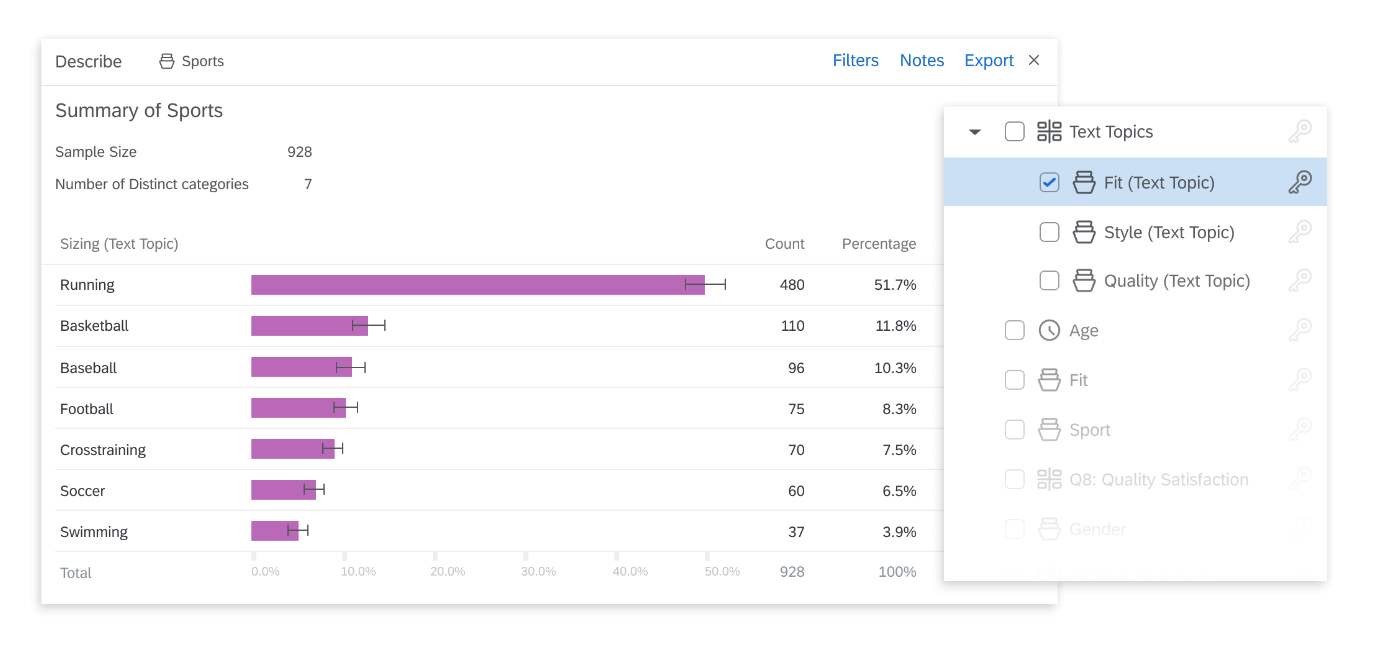
Another feature of text analysis tools is their ability to categorise information by topic, sorting it into groupings that help you organise your data according to the topic discussed.
All in all, interviews are a valuable technique for qualitative research in business, yielding rich and detailed unstructured data. Historically, they have only been limited by the human capacity to interpret and communicate results and conclusions, which demands considerable time and skill.
When you combine this data with AI tools that can interpret it quickly and automatically, it becomes easy to analyse and structure, dovetailing perfectly with your other business data. An additional benefit of natural language analysis tools is that they are free of subjective biases, and can replicate the same approach across as much data as you choose. By combining human research skills with machine analysis, qualitative research methods such as interviews are more valuable than ever to your business.
Related resources
Video in qualitative research 10 min read, descriptive research 8 min read, market intelligence 9 min read, qualitative research questions 11 min read, ethnographic research 11 min read, business research methods 12 min read, qualitative research design 12 min read, request demo.
Ready to learn more about Qualtrics?
- Reference Manager
- Simple TEXT file
People also looked at
Original research article, older adults' experiences of wellbeing during the covid-19 pandemic: a comparative qualitative study in italy and switzerland.

- 1 Faculty of Social Sciences, University of Geneva, Geneva, Switzerland
- 2 Swiss Center of Expertise in Life Course Research (LIVES), Geneva, Switzerland
- 3 Faculty of Social Work, University of Applied Sciences and Arts Western Switzerland (HETSL/HES-SO), Lausanne, Switzerland
Background: Particularly at the beginning of the pandemic, adults aged 65 and older were portrayed as a homogeneously vulnerable population due to the elevated health risks associated with contracting the COVID-19 disease. This portrayal, combined with travel restrictions, closures of economic sectors, country-wide lockdowns, and suggestions by governmental authorities to limit social contact, had important implications for the wellbeing of older individuals. However, older adults are a heterogeneous population who relies on different resources to cope with stressful periods, like the COVID-19 pandemic. Simultaneously, countries also employed different measures to contain the virus. Research thus far has focused on the short-term consequences of the pandemic, but studies have yet to address its long-term consequences.
Objectives: We explore older adults' lived experiences nearly 2 years after the pandemic onset. Moreover, we focus on the bordering countries of Switzerland and Italy, who employed contrasting containment measures. This paper analyzes (1) How the COVID-19 pandemic impacted the experiences of wellbeing of older adults in these regions and (2) How older adults coped with the stressors brought about by the pandemic, in particular social distancing.
Methods: The paper draws on 31 semi-structured interviews with 11 Swiss natives residing in Switzerland, 10 Italian migrants residing in Switzerland, and 10 Italian natives residing in Italy. Interviews were conducted from December 2021 to March 2022.
Results: Coping mechanisms of the three groups related to acceptance, hobbies, cognitive reframing, telephone use, vaccine use and social distancing. However, results show heterogeneous experiences of wellbeing, with Swiss natives sharing more positive narratives than the other two groups. Moreover, Italian migrants and Italian natives expressed the long-term negative consequences of the pandemic on their experienced wellbeing.
1 Introduction
In March of 2020, the WHO declared COVID-19 a pandemic, making it an international public health problem ( WHO, 2020 ). Beyond physical illness, the pandemic disrupted millions of lives around the globe through closures of schools, shops, and borders; it separated individuals from friends and family, and it caused job losses and financial strain ( Hiscott et al., 2020 ). However, in the public discourse it was especially older adults who were portrayed as a homogeneously vulnerable and frail group ( Jordan et al., 2020 ; Ayalon et al., 2021 ; Maggiori et al., 2022 ). Indeed, older people had higher mortality rates than younger ones ( Dadras et al., 2022 ). They also suffered from decreased physical activity due to social distancing measures, impacting their physical health ( Oliveira et al., 2022 ). Moreover, in comparison to pre-pandemic levels, older adults reported higher rates of anxiety and depression ( Webb and Chen, 2022 ; Segerstrom et al., 2023 ) and lower subjective wellbeing ( Maggiori et al., 2022 ).
However, compared to their younger counterparts, older adults also reported less pandemic-related stress, less social isolation, less life changes ( Birditt et al., 2021 ), and lower rates of anxiety and depression ( Webb and Chen, 2022 ). Furthermore, older adults' resilience was shown through their ability to develop coping strategies to maintain a certain level of subjective and psychological wellbeing ( Finlay et al., 2021 ; Fuller and Huseth-Zosel, 2021 ; Bustamante et al., 2022 ; Facal et al., 2022 ; Mau et al., 2022 ).
Nonetheless, the ability to cope with the stressors brought about by the pandemic was influenced by factors on the micro-, meso-, and macro- levels. On the micro-level, studies have revealed that characteristics like being in good health, previous experiences of adversity, stable financial status, and social networks positively affected individuals' ability to cope with the pandemic ( Guzman et al., 2023 ), while having a migration background was associated with increased pandemic-related worry ( Ludwig-Dehm et al., 2023 ) and loneliness ( Pan et al., 2021 ). At the meso-level, neighborhood parks and nature were positively related to mental and physical health ( Bustamante et al., 2022 ; Guzman et al., 2023 ). At the macro-level, stricter physical distancing measures mandated by governments were associated with worse mental health ( Mendez-Lopez et al., 2022 ). The heterogeneity of older adults' characteristics, resources, and lived experiences, as well as the differences in countries' containment measures thus call for research further exploring how older adults coped with the pandemic in different contexts.
Most studies to date focus on older individuals' wellbeing during the first lockdown in the spring of 2020 ( Seifert and Hassler, 2020 ; Cipolletta and Gris, 2021 ; Falvo et al., 2021 ; Finlay et al., 2021 ; Fuller and Huseth-Zosel, 2021 ; McKinlay et al., 2021 ; Whitehead and Torossian, 2021 ; Bustamante et al., 2022 ; Facal et al., 2022 ; Gonçalves et al., 2022 ; Kremers et al., 2022 ) or during the first year following the pandemic onset ( Fiocco et al., 2021 ; Atzendorf and Gruber, 2022 ; Brooks et al., 2022 ; Cohn-Schwartz et al., 2022 ; Derrer-Merk et al., 2022a ; Garner et al., 2022 ; Maggiori et al., 2022 ; Mau et al., 2022 ; Donizzetti and Capone, 2023 ). However, few studies have been published thus far addressing the second year of the pandemic and its long-term impact on older adults' wellbeing ( Gallè et al., 2021 ; König and Isengard, 2023 ). Moreover, studies have analyzed the pandemic's impact on the physical health of migrants of all ages in comparison to native-born populations in Western Europe ( Canevelli et al., 2020 ; Aldea, 2022 ; Khlat et al., 2022 ), but to the best of our knowledge, none have addressed the differences in the lived experiences of wellbeing among older migrant and native populations with a focus on coping strategies. Furthermore, there is a paucity of literature comparing the experiences of wellbeing and coping strategies between countries that implemented contrasting COVID-19 containment measures.
We aim to bridge this gap by comparing the experiences of older adults in Italy and Switzerland – countries that implemented different COVID-19 containment measures – nearly 2 years after the pandemic onset. Specifically, we study older Swiss natives residing in Switzerland, older Italian natives residing in Italy, and older Italian migrants residing in Switzerland. This allows us to explore the experiences of wellbeing of older adults who lived under strict restriction measures, namely Italian residents, to those of adults who lived under more relaxed measures, namely Swiss natives and Italian migrants living in Switzerland. Furthermore, comparing Swiss natives and Italian migrants allows us to analyze the experiences of two groups who lived the pandemic in the same context, yet who have had different life courses. More particularly, because older Italian migrants in Switzerland often have attachments to Italy and take part in transnational practices ( Ludwig-Dehm et al., 2023 ), their inclusion in the study allows us to explore how the situation in their country of origin impacted their COVID-19 experiences from abroad.
This paper aims to analyze (1) How the COVID-19 pandemic impacted the experiences of wellbeing of older adults in Switzerland and Italy and (2) How older adults coped with the stressors brought about by the pandemic, in particular social distancing.
2 Contextual background: the Swiss and Italian contexts
Despite the geographical proximity between Switzerland and Italy, the two countries implemented quite different containment measures as a response to the virus.
Compared to other European countries, on average Switzerland implemented less stringent containment measures throughout the pandemic, despite being just as impacted ( Pleninger et al., 2022 ). The first phase of the pandemic, classified by the Federal Council as an “extraordinary situation,” lasted from March 16 to June 19, 2020 ( Sager and Mavrot, 2020 ; Maggiori et al., 2022 ; Pleninger et al., 2022 ). From March 16 until April 26, the Swiss government gradually imposed measures closing borders, canceling cultural and sports events, banning all public and private manifestations, closing schools, restaurants, bars, as well as shops and services deemed to be unessential, and banning gatherings of more than five people. Older adults in particular were advised to stay at home and to avoid in-person social interactions with members outside their household. From April 26, 2020 containment measures were slowly eased, and on June 19, 2020, the classification of the pandemic changed from “extraordinary” to “special” ( Sager and Mavrot, 2020 ; Pleninger et al., 2022 ).
During the next 2 years, Switzerland saw a series of tightening and easing of containment measures, which included regulations on mandatory vaccines or COVID-19 tests to access bars and restaurants, and mandatory masks to be worn in shops and public transport. All restrictions were then lifted on April 1, 2022 ( FOPH, 2022 ).
Throughout the pandemic up until the data collection for this article – between December 2021 and March 2022 – the Swiss government largely relied on cooperation from the public. Although in certain periods shops, restaurants, and schools were closed, Swiss residents still enjoyed a certain amount of freedom to move and have social gatherings, albeit limited. Overall, it was left up to the individuals to regulate their behaviors within certain limits.
The Italian government, on the other hand, imposed more stringent measures throughout the pandemic. Late January 2020, the government declared a national emergency, and in February 2020, Italy was the epicenter of the health crisis in Europe ( Ferrante, 2022 ). The Italian government quickly established lockdown “red” zones in certain areas of Northern Italy, which led to the closure of schools and restrictions of movement: residents could leave their areas of residence only for necessities like work, health reasons or family emergencies, or grocery shopping. These restrictions were applied in waves to the entire country, and on March 11 the government imposed a national lockdown, also named the “stay at home” decree ( Bull, 2021 ). This entailed closure of borders, schools, restaurants and bars, and all nonessential shops and services. Travel between regions was prohibited and residents' movement was only allowed for essential reasons. The first Italian lockdown ended on May 3, 2020, after which most shops, restaurants, bars, and services gradually reopened while maintaining COVID-19 safety protocols ( Bosa et al., 2021 ).
During the next 2 years, Italy also experienced a series of loosening and tightening of restrictions, but these were often more stringent than the ones imposed in Switzerland. For instance, during the second wave of the pandemic, which took place in autumn of 2020 and winter of 2021, curfews from 11 pm to 5 am were mandated and restaurants and bars had to close at 6 pm. During this time, Italian residents were strongly recommended to leave their homes only for work or health reasons, and these restrictions were gradually eased by mid-2021 ( SkyTG24, 2020 ; Bosa et al., 2021 ). In April 2022, Italy declared an end to the state of emergency, and thereafter lifted all restrictions ( Amanto, 2022 ).
Both Italy and Switzerland were successful in containing the spread of the virus ( Ferrante, 2022 ; Pleninger et al., 2022 ), but at what cost to people's wellbeing?
3 A theoretical framework to understand wellbeing and coping strategies among older adults
3.1 wellbeing.
Research on wellbeing largely encompasses two forms: objective wellbeing and subjective wellbeing. The first refers to objective indicators like income, health, and living conditions. The second refers to individuals' experiences of wellbeing and to their evaluations of their lives. It is often measured with indicators like positive and negative affect, happiness, life satisfaction, and satisfaction with various life domains like social relationships, financial situation, and neighborhood conditions ( Bartram, 2012 ; Diener, 2012 ; Veenhoven, 2012 , 2017 ). In this paper, we use the term wellbeing to refer to the latter concept – to individuals' subjective experiences of wellbeing.
Some objective indicators are indeed correlated to subjective indicators – being in good health, for instance is positively associated with life satisfaction ( Helliwell, 2003 ; Deaton, 2008 ; Clark et al., 2018 ) and, to a certain extent, so is income ( Clark et al., 2008 ; Clark, 2011 ; De Jong, 2015 ). Studies have also debated to what extent wellbeing is dependent on genes and individual personality traits ( Bartels, 2015 ; Røysamb et al., 2018 ), and to what extent it is dependent on external factors like social contexts and life events ( Helliwell and Putnam, 2004 ). But overall, the consensus is that wellbeing is influenced by both genetic and environmental characteristics ( Røysamb et al., 2014 ; Luhmann et al., 2021 ).
Most studies employ a quantitative approach and explore a wide array of determinants of wellbeing, ranging from age, to health, to income and education, to relationships and divorce, to social norms and institutions, and so on ( Clark et al., 2018 ). Qualitative studies on wellbeing are less common ( Bartram, 2012 ), but they valuably provide information on participants' perceptions, views and beliefs that are unaffected by researchers' pre-determined ideologies ( Delle Fave et al., 2011 ). Especially in a context like that of the COVID-19 pandemic – a disruptive process that homogeneously categorized an entire group as vulnerable and forced individuals world-wide to reorganize their lives – a qualitative approach allows for nuanced, in-depth analyses of people's experiences of wellbeing (and vulnerability).
3.2 Older adults' vulnerability
Independently of the pandemic context, older adults are often characterized as particularly frail and vulnerable ( Fried et al., 2001 ; Clegg et al., 2013 ). This is often due the age-related decline in physiological and psychological systems, which renders this population vulnerable to falls, hospitalization, or sudden health changes triggered by minor events, and makes them more reliant on others for care ( Fried et al., 2001 ; Clegg et al., 2013 ). But vulnerability in old age is not a dichotomous state of vulnerable vs. not vulnerable, as was suggested in the public discourse during the COVID-19 pandemic. According to the life-course approach employed by Spini et al. (2017) , vulnerability is defined as:
“a weakening process and a lack of resources in one or more life domains that, in specific contexts, exposes individuals or groups to (1) negative consequences related to sources of stress, (2) an inability to cope effectively with stressors, and (3) an inability to recover from stressors or to take advantage of opportunities by a given deadline.” ( Spini et al., 2017 , p. 8)
It is a dynamic process between stress and resources that occurs at the intersection of different areas of life (like health, work, family, etc.), and on several levels (macro-, meso-, or micro-levels) throughout the life course ( Spini et al., 2017 ). When faced with a stressful situation like the COVID-19 pandemic, individuals must rely on the resources they accumulated throughout the life course – referred to as reserves ( Cullati et al., 2018 ) – in order to cope with life adversities. These reserves include, but are not limited to, physical and mental health, economic savings, cultural capital resulting from education, social networks, and emotional and cognitive reserves ( Cullati et al., 2018 ). It is in times of shocks that these reserves become the most important and mediate the impact of stressors on individuals' wellbeing; it is also during these adverse periods that inequalities between individuals' reserves become the most apparent ( Widmer, 2022 ), leading to situations of vulnerability.
In old age, physical reserves diminish, and older adults' ability to fight infectious diseases decreases, putting them in a vulnerable situation ( Bajaj et al., 2021 ). However, physical reserves are related to events and conditions throughout the lifespan. For example, the combination of disadvantageous childhood socioeconomic conditions, coupled with adverse adult socioeconomic conditions, increase the probability of chronic health diseases ( Galobardes et al., 2007 ). Aging adults are thus not all equally vulnerable to the risks associated with COVID-19; their vulnerability is associated to a wide variety of life-course experiences and factors, only some of which directly related to age ( Oris et al., 2020 ; Sneed and Krendl, 2022 ).
3.3 Pandemic impact on older adults' wellbeing
In the context of the COVID-19 pandemic, researchers have studied different measures related to wellbeing, like loneliness, social isolation, worry, anxiety, and others. This section draws on the literature focusing on various experiences of wellbeing during the pandemic among older adults.
Following the implementation of virus containment and social distancing measures, many countries reported an increase in loneliness among older adults in comparison to pre-pandemic levels ( Luchetti et al., 2020 ; Seifert and Hassler, 2020 ; Holaday et al., 2021 ; Macdonald and Hülür, 2021 ; Rodney et al., 2021 ; Van Tilburg et al., 2021 ; Zaninotto et al., 2022 ; see also literature review by Su et al., 2023 ). Feelings of loneliness were particularly prevalent among older adults with no children, lower-income individuals, those living alone, and those reporting depressive symptoms ( Seifert and Hassler, 2020 ; O'Shea et al., 2021 ), which highlights the role of resources and reserves in mediating the pandemic's impact on wellbeing.
Furthermore, older adults in countries all around the world experienced higher levels of stress, worry, anxiety, and depression in comparison to pre-pandemic levels. These negative mental health outcomes were more common among older single adults, among older adults of lower socioeconomic groups ( Kola et al., 2021 ; Webb and Chen, 2022 ; Wettstein et al., 2022a ; Zaninotto et al., 2022 ), among those with poor self-rated health ( Wettstein et al., 2022a ), and among those who were already socially isolated prior to the pandemic ( Macleod et al., 2021 ). Social isolation is correlated to declining physical and mental health, increased mortality, and lower quality of life, and the social distancing measures introduced by the pandemic exacerbated these risks ( Macleod et al., 2021 ).
Most studies published to date, in May 2023, concentrate on the initial weeks of the pandemic and largely focus on singular countries. Atzendorf and Gruber (2022) 's research, however, focused on the weeks following the first wave, between June and August 2020 and used SHARE data to analyze the medium-term consequences of the first pandemic wave across 25 European countries and Israel. They found that older adults in countries with high death rates and stringent measures were at increased risk of feeling depressed or lonely. Similarly, Mendez-Lopez et al. (2022) used the same data and revealed that countries' greater stringency in physical distancing measures was associated with worse mental health. This is particularly pertinent for this paper, as both Italy and Switzerland were badly hit by the pandemic ( Ferrante, 2022 ; Pleninger et al., 2022 ), but they differed in containment strategies: while Italian residents were severely limited in their mobility, Swiss residents benefitted from a certain amount of freedom. Atzendorf and Gruber (2022) revealed that Italian older adults reported increased feelings of loneliness and depression after the pandemic onset to a greater extent than Swiss older adults.
The only study to date analyzing older adults' wellbeing during the two years following the pandemic onset showed that most older Europeans did not feel lonely before or during the pandemic. However, for some, feelings of loneliness increased, particularly among the less educated, those living alone, and those isolated at home ( König and Isengard, 2023 ).
Moreover, the characterization of older adults as a homogeneous, exceptionally vulnerable population ( Petretto and Pili, 2020 ; Seifert, 2021 ) engendered negative self-perceptions of aging ( Losada-Baltar et al., 2021 ; Seifert, 2021 ), which have been associated with loneliness and psychological distress among older adults ( Losada-Baltar et al., 2021 ). Their homogenous representation and the resulting ageist narrative also led to feelings of anger, increased anxiety, and perceptions of loss of autonomy and individualism by this older population ( Derrer-Merk et al., 2022a , b ).
Although research has documented the negative impact of the pandemic on older adults, studies have also suggested that in some ways, older adults did not suffer as much as their younger counterparts, as documented in the literature review by Seckman (2023) . Older adults in the United States reported less pandemic-related stress, less social isolation ( Birditt et al., 2021 ), and greater emotional wellbeing ( Carstensen et al., 2020 ) than younger adults. The same result was found among Chinese adults ( Jiang, 2020 ). Similarly, in Italy older adults reported less loneliness compared to younger age groups ( Luchetti et al., 2020 ).
Independently of the pandemic context, older migrants are more vulnerable to loneliness and social isolation due to language and cultural barriers, low social capital, and dependence on children for support ( Neville et al., 2018 ; Sidani et al., 2022 ). Moreover, older migrants often occupy disadvantaged socioeconomic positions and are in worse health than natives in the host country ( Bolzman and Vagni, 2018 ; WHO, 2018 ). The pandemic and the related reduced social contacts may have thus rendered older migrants particularly vulnerable to social isolation, loneliness and negative mental health outcomes ( Pan et al., 2021 ; Sidani et al., 2022 ). In fact, a study on older Chinese migrants in Belgium and the Netherlands revealed that reduced social participation and financial insecurity increased migrants' loneliness levels ( Pan et al., 2021 ).
Furthermore, migrants often engage in transnational practices, linking them in various ways to their country of origin ( Ciobanu and Ludwig-Dehm, 2020 ). The pandemic restrictions changed some of these transnational practices through travel bans and border closures ( Nehring and Hu, 2022 ), which may influence older migrants' wellbeing. A survey conducted within the same research project as this paper, found that Italian migrants in Switzerland reported higher levels of worry about the COVID-19 pandemic than Swiss natives, and this difference is largely explained by engagement in transnational practices ( Ludwig-Dehm et al., 2023 ).
Despite the increasing proportion of older migrants in Europe ( UNDESA, 2020 ), research on the impact of the pandemic on older migrants' wellbeing is scarce.
3.4 Coping strategies of older adults
Research has shown that aging adults are capable of adapting and coping to various events and circumstances ( Klausen, 2020 ; Settersten et al., 2020 ). Coping refers to the cognitive and behavioral efforts one carries out to prevent, tolerate, or diminish certain situations ( Lazarus and Folkman, 1984 ; Carver, 2013 ; Biggs et al., 2017 ), and studies have found that older adults are particularly able to engage in such behaviors to diminish stressors ( Yancura and Aldwin, 2008 ; Carstensen et al., 2020 ). Coping strategies are often grouped into emotion-focused and problem-focused strategies ( Lazarus and Folkman, 1984 ; Aldwin and Revenson, 1987 ; Biggs et al., 2017 ). The first refers to strategies intended to regulate one's emotional reactions to the problem, while the latter refers to behaviors and cognitions aimed at directly managing or solving a problem ( Yancura and Aldwin, 2008 ; Biggs et al., 2017 ). This includes strategies aimed at avoiding thinking about the problem – like keeping oneself busy – as well as strategies aimed at finding the positive aspects of a stressful situation ( Aldwin and Yancura, 2004 ).
Older adults' ability to engage in these strategies can be partly explained by Carstensen's (2021) Socioemotional Selectivity Theory, which posits that social and emotional goals change depending on the perception of how much time one has left to live. As one grows older or approaches the end of their life due to illnesses or frailty, goals shift and people tend to value smaller and more meaningful social networks, they tend to spend more time with close partners, and they use cognitive resources to process more positive information ( Carstensen, 2021 ).
Another aspect related to older adults' coping abilities concerns the aforementioned reserves accumulated throughout the life-course. Accumulation of social resources, cultural and economic capital, health reserves, and the acquisition of coping skills allow older adults to endure stressful situations or, on the contrary, the lack of such reserves can penalize them ( Grundy, 2006 ; Cullati et al., 2018 ; Settersten et al., 2020 ).
In addition to the wellbeing consequences for older adults, studies have addressed the coping mechanisms developed by this population throughout the first wave of the pandemic. In a qualitative study, Gonçalves et al. (2022) interviewed older adults in Brazil, the United States, Italy, and Portugal, and revealed that social isolation engendered feelings of restriction in terms of interaction with friends and family and ability to participate in leisure activities. At the same time, older adults were also able to cope with the situation by dedicating their time to hobbies, using technological resources to stay close to friends and family, or involving themselves in religious and spiritual activities. Despite the different cultures and contexts of this study's participants, researchers found homogeneity in their coping mechanisms. Several studies confirmed these findings with different samples of older U.S. American adults ( Finlay et al., 2021 ; Fuller and Huseth-Zosel, 2021 ; Whitehead and Torossian, 2021 ), and Bustamante et al. (2022) revealed that time spent in parks and outdoor spaces boosted physical, mental, and social wellbeing.
Similarly, Mau et al. (2022) found that for older Danish adults, adapting to the situation by reframing their mindset, finding ways to maintain social contacts and a sense of community, and staying active were important coping behaviors that helped them maintain a good level of wellbeing. In Italy, older adults experienced the first pandemic wave in heterogeneous ways: those who felt alone pre-pandemic expressed that isolation had a negative impact on their wellbeing. Others were able to cope with the situation by exploring hobbies and maintaining contacts with friends and family through telephone use ( Cipolletta and Gris, 2021 ).
However, the only study on older migrants' wellbeing and coping strategies by Pan et al. (2021) found that neither problem-focused coping strategies, nor emotion-focused coping protected against increased loneliness during the pandemic.
These studies reveal that, at least for the first half of 2020, older adults employed coping mechanisms to endure the pandemic, but we still know little of their experiences after the first COVID-19 wave. A longitudinal qualitative study on Canadian older persons explored their experiences over a 10-month period from May 2020 to February 2021 ( Brooks et al., 2022 ). It found that the longevity of pandemic restrictions was partially responsible for older adults' declines in wellbeing. Simultaneously, participants used similar coping mechanism employed during the first pandemic wave to maintain their wellbeing: they stayed active, found ways to stay in contact with friends and family, and adopted positive mindsets.
Nonetheless, cross-country research on the experiences of wellbeing among older adults, and more particularly in the years following the pandemic onset, is still scarce. We therefore aim to bridge this gap by exploring the lived experiences and coping mechanisms of older individuals in two countries that had contrasting COVID-19 containment measures like Italy and Switzerland. Furthermore, we analyze how having connections to both countries, as is the case of Italian migrants in Switzerland, influences the lived experiences of these individuals.
4 Data and methods
Our study focuses on three groups of older adults (65+): (1) Swiss natives, defined as individuals who were born in Switzerland and whose parents were also born in Switzerland, (2) Italian international migrants from the south of Italy, defined as individuals who were born in southern Italy, whose parents were also born in Italy, and who migrated to Switzerland, and (3) Italian natives, defined as those who were born in the south of Italy, resided in the south of Italy at the time of the research, and whose parents were also born in Italy. There are several reasons for the inclusion of these specific groups in our study. First, Italians constitute one of the largest cohorts of foreign nationals aged 65 and above residing in Switzerland ( FSO, 2020 ). Second, a significant part of older Italians migrated to Switzerland between the 1950s and 1970s, with the majority originating from economically disadvantaged regions of Southern Italy ( Wessendorf, 2007 ). They primarily migrated for financial reasons or to reunite with family who had relocated as labor migrants ( Bolzman et al., 2004 ; Riaño and Wastl-Walter, 2006 ), and we therefore analyze older adults with a very specific migration background. Third, by comparing migrants from Southern Italy to natives from the same regions, we can explore the lived experiences of individuals who were raised in similar social contexts.
The sample for this paper is derived from an original quantitative survey conducted between June and November 2020 in the project TransAge: “Transnational aging among older migrants and natives: A strategy to overcome vulnerability.” Respondents to the qualitative interviews had already participated to the TransAge survey and had agreed to be further contacted for a follow-up interview. In total, 31 individuals participated to the study, of which 11 were Swiss natives, 10 were Italian migrants residing in Switzerland, and 10 were Italian natives residing in Italy.
To ensure diversity of wellbeing experiences among each of the three groups, we attempted to recruit individuals with low and high levels of life satisfaction. To do so, we based ourselves on Diener's Satisfaction with Life Scale ( Diener et al., 1985 ), included in the TransAge questionnaire. More specifically, we focused on the scale item “I am satisfied with my life.” In the survey, participants were asked to indicate the strength of their agreement with this statement on a scale ranging from 1 (strongly agree) to 7 (strongly disagree). We thus contacted a roughly equal number of participants who stated being satisfied with their lives (scores 6 or 7) and participants who were less satisfied (scores 5 or less). Simultaneously, we checked the general life satisfaction scores drawing on the 5-item scale to assure coherence between the single-item and the total score ( Diener et al., 1985 ).
The first author conducted semi-structured one-to-one interviews with the 31 community-dwelling older adults between December 2021 and March 2022, during the fifth wave of COVID-19, when social distancing was still strongly advised. Consequently, all interviews were done by telephone, 1 except for one participant who preferred to meet in person. Participation in the study was voluntary, and all participants gave oral consent to be interviewed and recorded. Interviews lasted an average of 45 min, and they were conducted in French or Italian. They were audio-recorded and subsequently transcribed verbatim and anonymized. Participant quotes in this paper were translated into English by the first author, and every participant was given a pseudonym.
Participants were asked open-ended questions that prompted them to reflect on their experiences throughout the pandemic. First, they were asked to describe their feelings at the beginning of the pandemic, any impact that the confinement period had on their wellbeing, on their social habits, oron their daily lives. They were also encouraged to share how they coped with this period. They were then asked to reflect on the years after the onset of the sanitary crisis and describe any difficulties they faced and any strategies used to surmount these difficulties. Participants were also invited to share what their daily and social lives looked like at the time of interview, and how they felt about any long-lasting changes they may have experienced.
Interviews were analyzed using an inductive thematic analysis using qualitative coding software NVivo. The study was approved by the Ethics Committee of the Faculty of Social Sciences of the University of Geneva.
5.1 Sample description
The 11 Swiss natives and 10 Italian migrants resided in the Swiss cantons of Geneva, Vaud, or Ticino, while the 10 Italian natives resided in the Italian regions of Sicily, Apulia, Sardinia, Abruzzo, Basilicata, or Campania. Participant characteristics by group are shown in Table 1 . In comparison to the larger TransAge quantitative study, there is an over-representation of participants with medium and higher level of education among Italian migrants and natives, which will be taken into consideration in the discussion of the results.

Table 1 . Sample charactertistics.
5.2 Comparative accounts of wellbeing in times of pandemic
When recounting their experiences throughout the first 2 years of the pandemic in Switzerland and Italy, participants across the three groups coupled their narratives, whether positive or negative, with coping strategies they employed to manage the impact of the pandemic on their wellbeing. The themes that we identified correspond to emotion-focused coping and problem-focused coping strategies documented in the coping literature ( Lazarus and Folkman, 1984 ; Aldwin and Revenson, 1987 ; Biggs et al., 2017 ). Emotion-focused coping refers to strategies aimed at regulating the emotions that arise because of a stressful situation, which also includes engagement in activities as a way to distract oneself. Problem-focused coping, on the other hand, refers to behaviors and cognitions targeted toward solving or managing a problem ( Yancura and Aldwin, 2008 ). Strategies like social contact through telephone use involves elements of both emotion-focused and problem-focused coping. It refers to emotional support received by friends and family, it can entail concrete help in understanding how to confront an adverse situation, and it is a strategy directed at compensating for decreased in-person contact ( Aldwin and Yancura, 2004 ).
Table 2 shows the behaviors adopted by participants that correspond to these two overarching coping mechanisms. We found that certain strategies adopted during the first lockdown were no longer used at the time of interview. Thus, in Table 2 , we list the themes found in the data by pandemic period.

Table 2 . Coping strategies used at pandemic onset and at time of interview.
During the first months of the pandemic, the primary emotion-focused strategies adopted by older adults in our sample related to acceptance of the health crisis, keeping busy through hobbies and exercise, appreciation of the natural environment, and attitudes aimed at “finding the silver lining,” which involves strategies aimed at trying to find the positive aspects of the problem at hand, and which the literature often refers to as cognitive reframing ( Aldwin and Yancura, 2004 ; Robson and Troutman-Jordan, 2014 ). In terms of problem-focused coping, participants evoked the importance of social distancing measures both during the initial lockdown and at the time of interview, and many later relied on vaccines as a mean to decrease the probability of severe illness.
The subsequent sections are organized as follows: First, we detail, by group, participants' experiences of wellbeing during the first lockdown and the coping strategies they adopted to face this period. Then, we analyze how social distancing measures and decreased social contacts impacted participants in each of the three groups, and we outline participants' social habits and coping strategies at the time of interview.
5.2.1 Wellbeing during the first lockdown
Although participants in all three groups used similar coping strategies throughout the pandemic, their narratives of wellbeing differed.
5.2.1.1 Experiences of Swiss natives
All Swiss native older adults, except for one, described the first confinement period in positive terms and expressed not having been particularly bothered by it. They often associated their wellbeing to being able to keep busy through various hobbies and interests, and by enjoying the natural landscapes around them, as indicated in the following excerpts:
“I think I was very relaxed…I have so many books at home...I have the watercolors, I have so many things to do here, creatively, with my hands or with my head, it doesn't bother me, so...the confinement didn't bother me at all.” (Irène, 77, F, Swiss native) “So, at home, my wife plays the piano. She has a gentleman who comes to the house. Oh yeah, she hasn't had a lesson in a year at home, but she took lessons with Zoom. You know how it is. So, she has a lot of work, piano homework. I did a little bit of crafting. I did a little bit of Spanish with French-Spanish classes.” (Nicolas, 71, M, Swiss native) “We remained a little locked up. But we had…it was a beautiful weather. There was the spring and everything, everything was beautiful. We enjoyed our patio. We got back to reading. We did a lot of stuff like that.” (Lydia, 79, F, Swiss native)
Some Swiss participants mentioned increased telephone use to share moments with friends and family. Others described their wellbeing by comparing themselves to others, thus engaging in cognitive strategies to frame their attitude and outlook on the situation. François, for instance, often spends part of the year in Barcelona, and when talking about his wellbeing, he compares the Swiss restrictions to those of Barcelona. He elaborates:
“We were very lucky because we weren't confined like…in Barcelona. In Switzerland, that wasn't the case. Of course, there were things we couldn't do any more, but there was still a lot for us to do. We could take the car, we could go for a walk. Well, the borders were closed. Well, we didn't suffer, my wife and I…our sons either.” (François, 81, M, Swiss native)
When reflecting on the virus-containment measures, others simply stated that they just had to accept the situation and adapt their behaviors accordingly. Pierre, for example, states:
“You have to adapt. We adapt by respecting the rules, not like people who cheat [by not following the rules]. We respect the rules, but we adapt.” (Pierre, 71, M, Swiss native)
Overall, the first months of the pandemic were described in positive terms by most of Swiss older adults. Most of them portrayed themselves as being in good health and they did not evoke fears related to the virus. However, one Swiss participant expressed the negative impact of this period on his wellbeing. He recounts:
“[We lived this period] quite badly because we were old, very old. The Ticino police chief was more or less telling everybody to put us in the freezer. I mean, not quite like that…he made a statement that caused quite a stir…[The situation] was not very conducive to being cheerful, let's say.” (Gianni, 88, M, Swiss Native)
For Gianni, the government lockdown meant being “stuck at home,” as he says, and relying on institutional support. His quote shows the way he experienced the confinement measures and the public discourse as an older-old person.
5.2.1.2 Experiences of Italian migrants in Switzerland
Similarly to Swiss natives, Italian migrants residing in Switzerland used cognitive strategies to frame the lockdown's impact on their wellbeing. They, too, evoked Switzerland's lenient containment measures as an important aspect that helped them surmount this period, particularly in terms of the freedom it gave them to spend time in nature. Giulia, for example, explains:
“Here in Switzerland, here in Geneva, I didn't feel this need for freedom like in other countries. For me, we were free here. I live near a park, I could take my walk every day. I have a small but very nice little apartment that has visibility on both sides, left and right, so I didn't feel like I was in prison.” (Giulia, 70, F, Italian migrant)
Italian migrants also turned to activities like reading, taking walks, and exercising to keep themselves busy during this period. However, although they lived the pandemic in the same context as the Swiss natives, there was more heterogeneity in Italian migrants' narratives of this containment period. While most stated that they simply accepted the situation and the lockdown did not negatively impact their wellbeing, some expressed feelings of loneliness and isolation. Gabriele (69, M), for example, says he felt isolated from the outside world at the beginning of the pandemic, he described his life during this period as monotonous. However, he kept himself busy by going on walks and exercising.
Others tried to overcome their feelings of loneliness by staying in communication with family, but it was not always helpful. When asked about any difficulties he faced during the lockdown, Alberto explains:
“A little bit of loneliness and missing family, that's it. It weighed on me a little bit. We used to phone my children, but no luck. My children also suffered; my youngest daughter suffered a lot and now we slowly recover.” (Alberto, 77, M, Italian migrant)
Italian migrants in Switzerland still hold transnational ties to their country of origin; a quantitative analysis of the TransAge survey found a higher level of worry about the pandemic among Italian migrants in Switzerland in comparison to Swiss natives ( Ludwig-Dehm et al., 2023 ). We were therefore interested in investigating whether Italian migrants evoked the COVID-19 situation in Italy when describing their own experiences of wellbeing, but none of our participants organically elicited Italy's situation in their narratives. We subsequently asked participants whether they were impacted in any way by the pandemic in Italy, and responses were heterogeneous. A large part expressed not having been impacted at all, others stated that they were sorry for the high numbers of deaths in Italy and they kept in contact with family, but were not particularly affected. Few of our participants, however, disclosed the emotional suffering they experienced due to Italy's high death rates, as demonstrated by the following quotes:
“I felt tremendous suffering […] I followed a lot, every day I was watching the Italian news. And it was, for me it was just – I don't want to say worse than the war, it was a virtual war, people dying without weapons, people dying without the bombs, without being machine-gunned, but they were dying like flies.” (Giulia, 70, F, Italian migrant) “Terrible, I felt really bad, I mean I don't know why we got to that point.” (Sara, 78, F, Italian migrant)
Although Italian migrants and Swiss natives lived the pandemic in the same context and both used similar coping strategies during the first confinement period, interviews show that Italian migrants' experiences were slightly more heterogeneous than Swiss natives', with a few migrants expressing feelings of loneliness and emotional anguish, emotions that were absent in Swiss natives' accounts.
5.2.1.3 Experiences of Italian natives
In comparison to Swiss natives and Italian migrants in Switzerland, most Italian natives residing in Italy expressed feelings of worry, sadness, and fear when recounting their lockdown experiences, but most of them coupled their hardships with feelings of acceptance. Tommaso, for example, recounts:
“To hear on television, from the media, that there are deaths and deaths and deaths, obviously the concern is there. The fear, the terror even, of suffering these negative effects.” (Tommaso 84, M, Italian native)
But later, when discussing the lockdown, he continues:
“I stayed peacefully at home with a nice long beard, growing it out. I accepted it, though, because those were the rules. You had to accept them.” (Tommaso, 84, M, Italian native)
Similarly, Paolino couples the dismay brought on by the pandemic lockdown with feelings of acceptance, as well as behaviors aimed at avoiding contagion. He explains:
“The beginning of the pandemic I accepted it begrudgingly, at home, and I stayed at home despite my habits, because having lived a life always on the move – until now I was always around. That thing, the pandemic, I accepted it, and for 3 months I stayed at home, I would only go get some groceries, the bare minimum.” (Paolino, 86, M, Italian native)
In contrast to Swiss natives and Italian migrants, few Italian natives mentioned having turned to hobbies to fill up their time during the first lockdown. Some mentioned the importance of spending time outside, of having a balcony or a garden. Most of them cited phoning friends and family for emotional support, to pass time, and to update each other on their health, and most declared having used the phone for communication more than pre-COVID times. To respect social distancing rules, one participant even used intercom to communicate with family in the same building; she says:
“We used to talk to each other by intercom and by phone, we all live in the same building, so by intercom, by phone we used to talk to each other, and then if somebody went out, they would walk by the kitchen door, which was made of glass, and then we would see each other.” (Rosa, 71, F, Italian native)
Despite the coping strategies employed by Italian natives, their narratives of the lockdown presented an overarching theme of dejection, which was less present in Italian migrants' experiences and nearly absent in those of the Swiss natives in our sample.
5.2.2 Wellbeing after 2 years of the COVID-19 pandemic: the role of social contacts
Notwithstanding the different narratives of wellbeing among the three groups, the previous sections indicate that everyone inevitably experienced a decrease in physical social contacts resulting from the COVID-19 containment policies. Given the importance of social networks for individuals' wellbeing ( Helliwell and Putnam, 2004 ; Elgar et al., 2011 ; Amati et al., 2018 ), we aimed to inquire how social distancing regulations impacted participants' perceived wellbeing in the 2 years after the onset of the pandemic.
Our interviews reveal heterogeneous responses to social distancing; nonetheless, regardless of the perceived impact on their wellbeing, most participants employed behavior-focused coping strategies aimed at reducing probability of contagion and illness. These strategies consisted of either vaccination for the participant, social distancing habits, or a combination of the two. In some cases, these strategies were successful in supporting participants' experienced wellbeing. In other cases, they preserved one's physical wellbeing at the cost of their subjective wellbeing.
In the next sections, we explore how each of the three groups was impacted by decreased social contacts, how these sentiments developed throughout the pandemic, and how participants employed the above-mentioned coping strategies at the time of interview.
5.2.2.1 Experiences of Swiss natives
Just like the lockdown did not seem to negatively impact most Swiss older adults in our study, neither did the imposed social distancing measures and related decrease in social contacts. Most of them experienced a slight change of social habits, which entailed seeing friends and family less frequently during the previous 2 years in comparison to pre-COVID times. However, these changes did not have a consequential negative impact for most of our Swiss participants. Social distancing was often described as bothersome or strange, but easily managed. Martin, for example, states:
“Yeah, [the pandemic] restricts our freedom to see – as I'm a pretty tactile person, it's true that it changes me a little bit. Friends, I kiss them less. That's what affects me a little bit more – I have to be less, much less tactile than I was with everyone, to give kisses to the left and to the right. Well, it's a bit weird.” (Martin, 75, Swiss Native)
This quote represents the sentiments expressed by most Swiss natives: they were not completely unaffected, but they were able to adapt to the changes in social habits without important repercussions for their wellbeing. At the time of interview, nearly 2 years after the pandemic onset, most Swiss older adults explained their social habits were similar to their pre-pandemic habits, but they also adopted strategies to be able to fulfill their social desires while avoiding contagion or severe illness. Most Swiss participants mentioned being vaccinated and expressed the importance of listening to scientists' advice on the preventative measures to take. These strategies helped them adjust their behaviors accordingly and feel more protected. Martin, for instance, has resumed seeing friends, but only under certain self-imposed rules. He explains,
“If we see each other, we are all vaccinated. We are not safe from catching it but at least we are less likely to get sick. And then, we avoid those who don't want to be vaccinated or those who are not vaccinated.” (Martin, 75, Swiss native)
However, one Swiss participant shared the negative experiences that followed him and his wife throughout the course of the pandemic. During the lockdown, Gianni expressed being “stuck at home,” and this lack of freedom and decreased social contacts persisted until the time of the interview, 2 years later. He says,
“Now with these problems of…the danger of contagion, and so it makes us less, less mobile, less free to live, right? Basically now, even though the lockdown has not been declared, we try to go out as little as possible, not to mingle with people so we don't get infected.” (Gianni, M, 88, Swiss native)
While most Swiss older adults were able to resume their social lives by adopting behaviors to avoid illness, the social distancing measured employed by Gianni – the oldest among our Swiss participants – allow him to preserve his physical wellbeing at the cost of his subjective wellbeing.
5.2.2.2 Experiences of Italian migrants in Switzerland
In comparison to older Swiss natives, the perceived impact of social distancing measures was more heterogeneous among Italian migrants. At the time of interview, only a minority of participants said they had resumed their pre-pandemic social habits, although most slowly started seeing small groups of friends again. Like in Gianni's case, for many Italian migrants, the social distancing strategies adopted to preserve their physical wellbeing had negative repercussions on their experienced wellbeing. One participant, for example, shared that the fear of contagion remained even after containment restrictions were eased, and his personal relationships suffered. He explains,
“I lost touch with friends, you couldn't get together, you couldn't go shopping, the only thing I could do was go [walk] in the forest. Then, even when the restrictions were eased, it had affected me so much that it was hard to get together. When we got together […] we had a drink and then left. There was always that fear between us.” (Giacomo, 68, M, Italian migrant)
Giacomo looks back at his life before the pandemic with melancholy, but he also elicits the importance of acceptance and reframing one's mindset to surmount the situation. He shares:
“[Before COVID-19] we used to get together on Friday nights, play cards, drink, smoke, and for 2 years we haven't done it and I don't think we're going to start again. It's difficult because people have become distrustful, we've been wounded and we're licking our wounds. Let's put it this way. You have to get over it, direct your life differently and move on. I don't want to stay at home waiting for death.” (Giacomo, 68, M).
Although some participants were wary of resuming social activities at the time of interview, most slowly started seeing friends again while continuing to employ social distancing measures. Giulia, for instance, explains:
“[Before the pandemic] maybe we went to the restaurant once a month, or once every 2 months. But that was a lot. But we haven't done this anymore, and I didn't – and we don't even feel like doing it anymore. Now if we go to a restaurant, we go at noon…and we stand outside on the terrace because we keep being careful.” (Giulia, 70, F, Italian migrant)
Despite the slow return to a social life and the continued safety measures employed, the pandemic had a long-lasting impact on the wellbeing of most Italian older migrants, as evidenced by the following excerpts:
“I feel insecure, maybe because of the pandemic, because of the war that's going on 2 […] I feel insecure and I tell myself I don't need this […] Insecure in the sense that I say, enough of the pandemic; insecure not physically, but in the sense that it destabilizes me [mentally] […] In the sense that I used to be able to imagine the following years and now I can't.” (Sara, 78, F, Italian migrant) “It's 2 years that I lost and that I cannot get back. […] I lost 2 years that I won't get back. I don't even know if I'll be able to – to feel better.” (Giulia, 70, F, Italian migrant).
5.2.2.3 Experiences of Italian natives in Italy
The perceived impact of the social distancing measures was notably detrimental for the experienced wellbeing of Italian natives in Italy. Most cited the lack of social contacts as the primary difficulty faced throughout the pandemic. For many, the fear instilled by the pandemic prevented them from resuming their social activities at the time of interview, despite most participants being vaccinated. This engendered feelings of sadness, anxiety, and loneliness among many Italian participants, as evidence by the following quotes:
“What I dislike is not being able to have company, because I'm all about friendships, company, laughter, and I don't like loneliness. […Before the pandemic] we used to organize trips with an association, so we would spend 15 days together, and every 2 months we would meet in an institution and spend the day together, we would eat together. With girlfriends, we would go out and take a walk in the countryside when we had nice days, and so I miss all of that now.” (Martina, 84, F, Italian native) “Now the fact of going out and putting the mask on […], continually having to disinfect your hands when you go out, when you go get groceries, having to be careful not to get too close to people, [hoping] that in stores there aren't too many people. These – this anxiety that it gives you, that as long as you are at home, it's different. But when you go out for necessities, or go to the hospital for a visit – in short, it's anxiety, that's it. You try to – every person you meet seems to be an enemy.” (Rosa, 72, F, Italian Native) “I have a lot of fear, really a lot, and this has prevented me from going out and also from having a social life. My social life has almost disappeared, because partly the fear, partly my age, and so the result is that while before I used to go to concerts, I used to go to the movies, now we have – my husband and I – we have canceled everything, we don't go anymore, and so there is a lot of sadness.” (Alice, 75, F, Italian native)
Although some expressed feeling safer due to the vaccine, the fear induced by the virus was still present 2 years following the pandemic onset. Many Italian natives described the continued use of their phones to communicate with friends and family – more so than during pre-pandemic times – and this kept them company. Nonetheless, most expressed that while at the beginning they tried to accept the circumstances, the pandemic had started to weigh on them and negatively influence their wellbeing. Only one Italian native shared that the changes in social habits did not have a substantial impact on his wellbeing:
“[The pandemic] did not substantially change my life, nor my family's. Of course, there were occasions when we would have liked – during the holidays, for example – to spend more time with friends. We gave this up, and we think and hope that it was accepted by our friends. In any case, this withdrawal was nothing out the ordinary, so it was nothing irrational. Let's say that it did not affect our life, our wellbeing.” (Lorenzo, 74, M, Italian native)
Yet, even for a person like Lorenzo who estimates that his wellbeing was not lowered by the pandemic, his social habits have changed, which was observed for most of the Italian natives in Italy.
6 Discussion
The objective of this study was to provide insight into older adults' experiences of wellbeing as well as the coping strategies employed to overcome difficulties brought about by the pandemic, in particular social distancing. Our contribution to the existing literature is 4-fold: (1) we explored older adults' lived experiences not only through their recollection of the first months of the pandemic, but also through their narratives of wellbeing and coping 2 years after the pandemic onset, (2) we analyzed the experiences of older migrants, an underrepresented population in wellbeing and COVID-19-related research, (3) we compared the experiences of two groups – Swiss natives and Italian migrants – who lived the pandemic in the same context, and (4) we compared the experiences of older adults who were subject to strict containment measures – as was the case of Italian natives – to those of adults who benefitted from more lax restrictions.
The following section discusses the results of the qualitative interviews, as well as the study limitations and implications for future policy.
While many of our interviews highlight the negative consequences of the pandemic for older adults' wellbeing in Switzerland and Italy, they also emphasize the heterogeneity of older individuals' experiences, as well as their ability to adapt and cope with stressful situations. Swiss natives and Italian migrants lived the pandemic in the same context, one that did not impose strong stay-at-home order and allowed for a certain freedom of movement. Yet, we found pronounced differences in their descriptions of wellbeing, both in the narratives concerning the first lockdown in 2020, and in the narratives addressing the following years, until time of interview.
Most Swiss natives presented positive accounts of the lockdown period; their descriptions were often coupled with coping strategies they employed to address the COVID-19 containment measures. Consistently with previous studies on coping during the pandemic, in the first months of the pandemic Swiss older adults relied on hobbies to keep busy, closeness to nature, acceptance of the sanitary situation, and cognitive strategies to find the silver lining of living through a world-wide crisis ( Finlay et al., 2021 ; Fuller and Huseth-Zosel, 2021 ; Whitehead and Torossian, 2021 ; Brooks et al., 2022 ; Bustamante et al., 2022 ; Mau et al., 2022 ). Most participants described their wellbeing as unaffected even at the time of interview, 2 years after the pandemic onset. Although they described the inevitable decrease in physical contacts as bothersome, most were able to adopt behavioral strategies that involved vaccination and continued social distancing measures that kept them safe while fulfilling their social needs.
Even though Italian migrants experienced the pandemic in the same context as Swiss natives, their accounts of the lockdown and the following years were more heterogeneous. During the first months of the pandemic, they used coping strategies like those of the Swiss natives: they spent their time in nature, kept busy through hobbies, and they, too, positively referred to the freedom they felt due to Switzerland's relaxed containment measures. At this time, only some participants expressed feelings of sadness and loneliness. However, when reflecting on the entirety of the previous 2 years, most participants shared the negative impact of the pandemic on their wellbeing. Although many slowly resumed social activities at the time of interview, they evoked a continued sense of fear, distrust, and dejection. Many of their interviews demonstrated that the social distancing behaviors that allowed them to keep themselves physically safe diminished their wellbeing.
Due to the qualitative nature of this article, it is not possible to firmly assert that the different experiences of wellbeing among Swiss natives and Italian migrants are due to inequalities in reserves. However, we can posit that, at least for some Italian migrants in Switzerland, their ability to cope with the pandemic may have been partly influenced by their lower level of reserves in comparison to those of Swiss natives.
Most Italian migrants in our study migrated to Switzerland in the 1960s and 1970s, as part of the wave of labor migrants who moved from regions of Italy that lacked economic opportunities ( Bolzman and Vagni, 2018 ; Dones and Ciobanu, 2022 ). Quantitative studies have revealed that, compared to older Swiss natives, older Italian migrants in Switzerland have lower education levels, report themselves in worse health, and generally occupied lower-skilled jobs ( Bolzman and Vagni, 2018 ). For many, the migration to Switzerland as labor workers was followed by a lack of opportunities to improve their socio-economic circumstances, leaving them in worse situations in comparison to their Swiss counterparts. These disadvantaged conditions may have engendered psychological stresses that may have accumulated over the life course ( Dannefer, 2003 ; Settersten et al., 2020 ), thereby impacting migrants' ability to build the adequate reserves to successfully cope with life shocks.
In our qualitative sample of Italian migrants there is an overrepresentation of highly educated participants and of participants in a comfortable financial situation, as represented by the measure “making ends meet” in Table 1 ( Dones, 2023 ). However, on average they still have lower education levels than Swiss natives. Moreover, independently of current socioeconomic status, most participants spoke of the poverty and lack of jobs they experienced during their youth in Italy, which ultimately led them to migrate. In addition, when reflecting on other hardships encountered during their lifetimes, most cited the difficulties encountered when they migrated: discrimination, having to learn another language, detachment from family in Italy, and getting accustomed to a foreign country. Along with the disadvantaged socioeconomic conditions some participants experienced throughout the lifespan, most experienced migration-related stressors that, accumulated over the life course, may have impacted their capacity to cope with life shocks and with the pandemic in the same way that Swiss natives did. Moreover, the capacity to act in old age is dependent on the life course and the accumulation of reserves ( Settersten et al., 2020 ), making in this case a difference between the older Swiss and older migrants.
Although Italian migrants did employ similar coping mechanisms, for most, these coping strategies were not successful in combatting the negative impact of the pandemic on their experienced wellbeing. This finding is in line with research by Pan et al. (2021) , which revealed that coping strategies like increased telephone contact and increased participation in individual activities did not protect older Chinese migrants against loneliness.
Another possible explanation for the lower wellbeing expressed by Italian migrants compared to Swiss natives relates to transnational practices and attachment to the home country. Although participants did not mention their attachment to Italy when recounting their pandemic experiences, some did share the negative impact the Italian situation had on their wellbeing. Previous research stemming from the TransAge project has revealed that greater attachment to Italy correlates to greater worry about the COVID-19 pandemic ( Ludwig-Dehm et al., 2023 ), which may have thereby impacted Italian migrants' lived experiences. Similarly, we found one case of transnational attachment among Swiss natives. The ties to Barcelona led François to value the confinement situation in Switzerland.
In comparison to older adults residing in Switzerland, older Italian natives expressed more negative emotions and difficulties when describing both the first COVID-19 lockdown and the subsequent years. Most adopted coping strategies like acceptance and increased telephone use for social contact, but the fear brought about by the virus followed them until the time of interview. This prevented most from resuming social activities, despite being vaccinated, and many expressed continued feelings of sadness, loneliness, and anxiety.
When considering the particularly negative experiences of Italian natives in Italy, we cannot propose that these were related to the various types of reserves accumulated through life, as our participants led heterogeneous life-courses. Indeed, there may be a variety of influencing factors that have the potential to affect the wellbeing of older Italian adults. One of these factors could hypothetically relate to the strict confinement measures employed by the Italian government throughout the first 2 years of the pandemic. Research thus far has revealed that countries' stringency of physical distancing regulations was associated with higher incidence of loneliness and depression among older adults ( Atzendorf and Gruber, 2022 ; Mendez-Lopez et al., 2022 ). Additionally, a study on older adults in Italy showed that restrictive measures significantly impacted the quality of life, psychological wellbeing, and mobility of older adults ( Tosato et al., 2022 ). Although no studies have yet been published on the long-term consequences of strict containment measures, our exploratory results could point to the negative impact of such regulations on older adults' experiences of wellbeing. However, this is simply a theoretical proposition and further studies on the subject are needed to firmly establish a correlation between stringency of confinement regulations and wellbeing.
Moreover, Italian natives relied on telephone communication as a coping mechanism more than the other two groups. While staying in touch with family and friends through phone and other media use has been correlated with life satisfaction during the first semi-lockdown in Switzerland ( Dones et al., 2022 ), studies found that non-personal communication does not substitute face-to-face interactions and it is not a protective strategy against loneliness among older adults ( Pan et al., 2021 ; König and Isengard, 2023 ). Further research should thus address the effectiveness of different coping strategies in times of crisis.
6.1 Limitations, strengths, and suggestions for future research
This study does not come without limitations. Due to the qualitative nature of the research and the relatively small sample size, results cannot be generalized even though saturation of responses was reached. In addition, our study did not explore the experiences of many people who lived alone during the pandemic, a population that might have been particularly at risk of social isolation. Similarly, there is a possibility that older adults with lower levels of wellbeing may not have been willing to participate to the research, although some research participants shared their difficulties and negative experiences of the pandemic. Lastly, to be able to better understand the role of reserves in older adults' experiences of the pandemic, longitudinal, quantitative data would be necessary.
Nonetheless, this article sheds light on several aspects. First, despite the homogeneous representation of older adults as frail and vulnerable ( Petretto and Pili, 2020 ; Ayalon et al., 2021 ; Maggiori et al., 2022 ), the pandemic impact on wellbeing is not the same for all older adults, as demonstrated by emerging studies ( Wettstein et al., 2022a , b ) and by the different experiences of this article's older populations. Second, despite the employment of coping strategies used by all participants, their effectiveness in mediating the long-term impact of the pandemic on experiences of wellbeing differed among groups. Third, the long-term impact of the pandemic and the various containment strategies needs further examination. As the case of Italian migrants in Switzerland shows, some older migrants experienced the beginning of the pandemic in quite positive ways, but their narratives of their situation 2 years after the pandemic onset showed an overall negative effect on their wellbeing.
The share of older adults in Europe continues to increase ( Eurostat, 2023 ), as does the share of older migrants ( UNDESA, 2020 ). The advancements of the last few decades have reduced the dependence of older adults and have increased life expectancy. At the same time, social inequalities and inter-individual diversity make of today's older adults an increasingly heterogeneous group ( Oris et al., 2020 ). The consideration of this heterogeneity should be at the core of not only scientific research, but also of policy interventions, as grouping all older adults under the “vulnerable and frail” umbrella propagates against narratives that can lead to increased psychological distress and negative self-perceptions of aging ( Losada-Baltar et al., 2021 ; Derrer-Merk et al., 2022a , b ).
To account for the diversity in older adults' lives, research on the long-term impact of the pandemic should adopt a life-course approach to further analyze how differing trajectories engender situations of resilience or vulnerability. Given the increase of share of older migrants, their underrepresentation in COVID-19 and wellbeing research, and the possible long-term effects of having a migration background, special consideration should be allotted to them. Moreover, studies should further address the effectiveness of coping strategies among different populations. Lastly, in cases of future health crises, governments should have an increased regard for the negative consequences of stringent confinement measures, as social isolation and physical inactivity among older adults are correlated with increased hospitalization, depression, cognitive impairment, and reduced quality of life ( Cacioppo et al., 2010 ; Cacioppo and Cacioppo, 2014 ; Ozemek et al., 2019 ).
Data availability statement
The datasets presented in this article are not readily available because the qualitative interviews analyzed in this study are not publicly available. For now, they are available from RC on reasonable request. Requests to access the datasets should be directed to RC, oana.ciobanu@hetsl.ch .
Ethics statement
The studies involving humans were approved by the Ethics Committee of the Faculty of Social Sciences of the University of Geneva. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants' legal guardians/next of kin because participation in the study was voluntary, and all participants gave oral consent to be interviewed and recorded.
Author contributions
ID drafted the interview guidelines, carried out the data collection and analysis, and was the major contributor in writing the manuscript. RC supervised the project, reviewed and approved the interview guidelines, provided article references, read parts of the interviews, and contributed to the discussion and conclusion. All authors read and approved the final manuscript.
This work was funded by the Swiss National Science Foundation through the Professorship Grant “Transnational Aging among Older Migrants and Natives: A Strategy to Overcome Vulnerability” (Grant Number PP00P1_179077/1).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. ^ Of these phone interviews, one was done through WhatsApp audio, the rest through the regular phone line.
2. ^ The participant is referring to the war between Russia and Ukraine, which had just begun at the time of interview.
Aldea, N. (2022). Mortality impact of the COVID-19 epidemic on immigrant populations in Spain. SSM Pop. Health 20:101291. doi: 10.1016/j.ssmph.2022.101291
PubMed Abstract | Crossref Full Text | Google Scholar
Aldwin, C. M., and Revenson, T. A. (1987). Does coping help? A reexamination of the relation between coping and mental health. J. Pers. Soc. Psychol. 53, 337–348. doi: 10.1037/0022-3514.53.2.337
Aldwin, C. M., and Yancura, L. A. (2004). “Coping and health: a comparison of the stress and trauma literatures,” in Trauma and Health: Physical Health Consequences of Exposure to Extreme Stress , eds P. P. Schnurr and B. L. Green (London: American Psychological Association), 99–125.
Google Scholar
Amanto, A. (2022). Italy Ends COVID-19 State of Emergency, Curbs to be Lifted Gradually. Reuters . Available online at: https://www.reuters.com/world/europe/italy-ends-covid-19-state-emergency-curbs-be-lifted-gradually-2022-04-01/ (accessed April 1, 2022).
Amati, V., Meggiolaro, S., Rivellini, G., and Zaccarin, S. (2018). Social relations and life satisfaction: the role of friends. Genus 74, 1–18. doi: 10.1186/s41118-018-0032-z
Atzendorf, J., and Gruber, S. (2022). Depression and loneliness of older adults in Europe and Israel after the first wave of COVID-19. Eur. J. Ageing 19, 849–861. doi: 10.1007/s10433-021-00640-8
Ayalon, L., Chasteen, A., Diehl, M., Levy, B. R., Neupert, S. D., Rothermund, K., et al. (2021). Aging in times of the COVID-19 pandemic: avoiding ageism and fostering intergenerational solidarity. The J. Gerontol. Series B 76, e49–e52. doi: 10.1093/geronb/gbaa051
Bajaj, V., Gadi, N., Spihlman, A. P., Wu, S. C., Choi, C. H., Moulton, V. R., et al. (2021). Aging, immunity, and COVID-19: How age influences the host immune response to coronavirus infections? Front. Physiol. 11:571416. doi: 10.3389/fphys.2020.571416
Bartels, M. (2015). Genetics of wellbeing and its components satisfaction with life, happiness, and quality of life: a review and meta-analysis of heritability studies. Behav. Genetics 45, 137–156. doi: 10.1007/s10519-015-9713-y
Bartram, D. (2012). Elements of a sociological contribution to happiness studies. Sociol. Compass 6, 644–656. doi: 10.1111/j.1751-9020.2012.00483.x
Crossref Full Text | Google Scholar
Biggs, A., Brough, P., and Drummond, S. (2017). “Lazarus and Folkman's psychological stress and coping theory,” in The Handbook of Stress and Health , eds C. L. Cooper and J. Campbell Quick (London: John Wiley and Sons, Ltd),349–364.
Birditt, K. S., Turkelson, A., Fingerman, K. L., Polenick, C. A., and Oya, A. (2021). Age differences in stress, life changes, and social ties during the COVID-19 pandemic: implications for psychological well-being. The Gerontol. Cite 61, 205–216. doi: 10.1093/geront/gnaa204
Bolzman, C., Poncioni-Derigo, R., Vial, M., and Fibbi, R. (2004). Older labour migrants' well being in Europe: the case of Switzerland. Ageing Soc. 24, 411–429. doi: 10.1017/S0144686X03001557
Bolzman, C., and Vagni, G. (2018). “‘And we are still here': Life courses and life conditions of Italian, Spanish and Portuguese retirees in Switzerland,” in Gender, Family, and Adaptation of Migrants in Europe , eds I. Vlase and B. Voicu (New York, NY: Palgrave Macmillan), 67–89.
Bosa, I., Castelli, A., Castelli, M., Ciani, O., Compagni, A., Galizzi, M. M., et al. (2021). Response to COVID-19: was Italy (un)prepared? Health Econ. Policy Law 17, 1–13. doi: 10.1017/S1744133121000141
Brooks, E., Mohammadi, S., Mortenson, W., Ben, B. C. L., Tsukura, C., Rash, I., et al. (2022). ‘Make the most of the situation'. Older adults' experiences during COVID-19: a longitudinal, qualitative study. J. Appl. Gerontol. 41, 2205–2213. doi: 10.1177/07334648221105062
Bull, M. (2021). The Italian government response to COVID-19 and the making of a prime minister. Contempo. Italian Polit. 13, 149–165. doi: 10.1080/23248823.2021.1914453
Bustamante, G., Guzman, V., Kobayashi, L. C., and Finlay, J. (2022). Mental health and well-being in times of COVID-19: a mixed-methods study of the role of neighborhood parks, outdoor spaces, and nature among US older adults. Health Place 76:102813. doi: 10.1016/j.healthplace.2022.102813
Cacioppo, J. T., and Cacioppo, S. (2014). Older adults reporting social isolation or loneliness show poorer cognitive function 4 years later. Evid. Based Nurs. 17, 59–60. doi: 10.1136/eb-2013-101379
Cacioppo, J. T., Hawkley, L. C., and Thisted, R. A. (2010). Perceived social isolation makes me sad: 5-year cross-lagged analyses of loneliness and depressive symptomatology in the chicago health, aging, and social relations study. Psychol. Aging 25, 453–463. doi: 10.1037/a0017216
Canevelli, M., Palmieri, L., Raparelli, V., Punzo, O., Donfrancesco, C., Noce, C., et al. (2020). COVID-19 mortality among migrants living in Italy. Ann. Ist. Super Sanità 56, 373–377. doi: 10.4415/ANN_20_03_16
Carstensen, L. L. (2021). Socioemotional selectivity theory: the role of perceived endings in human motivation. The Gerontol. Cite 61, 1188–1196. doi: 10.1093/geront/gnab116
Carstensen, L. L., Shavit, Y. Z., and Barnes, J. T. (2020). Age advantages in emotional experience persist even under threat from the COVID-19 pandemic. Psychol. Sci. 31, 1374–1385. doi: 10.1177/0956797620967261
Carver, C. (2013). “Coping,” in Encyclopedia of Behavioral Medicine , eds M. D. Gellman and J. R. Turner (New York, NY: Springer New York), 496–500.
Ciobanu, R. O., and Ludwig-Dehm, S. M. (2020). Life in limbo: old-age transnationalism. The Gerontol. 60, 322–330. doi: 10.1093/geront/gnz166
Cipolletta, S., and Gris, F. (2021). Older people's lived perspectives of social isolation during the first wave of the COVID-19 pandemic in Italy. Public Health 18:832. doi: 10.3390/ijerph182211832
Clark, A. E. (2011). Income and happiness: Getting the debate straight. Appl. Res. Q. Life 6, 253–263. doi: 10.1007/s11482-011-9150-x
Clark, A. E., Flèche, S., Layard, R., Powdthavee, N., and Ward, G. (2018). The Origins of Happiness (NED-New) . Princeton, NJ: Princeton University Pres.
Clark, A. E., Frijters, P., and Shields, M. A. (2008). Relative income, happiness, and utility: An explanation for the Easterlin paradox and other puzzles. J. Econ. Lit. 46, 95–144. doi: 10.1257/jel.46.1.95
Clegg, A., Young, J., Iliffe, S., Rikkert, M. O., and Rockwood, K. (2013). Frailty in elderly people. The Lancet 381, 752–762. doi: 10.1016/S0140-6736(12)62167-9
Cohn-Schwartz, E., Vitman-Schorr, A., and Khalaila, R. (2022). Physical distancing is related to fewer electronic and in-person contacts and to increased loneliness during the COVID-19 pandemic among older Europeans. Q. Life Res. 31, 1033–1042. doi: 10.1007/s11136-021-02949-4
Cullati, S., Kliegel, M., and Widmer, E. (2018). Development of reserves over the life course and onset of vulnerability in later life. Nat. Hum. Behav. 2, 551–558. doi: 10.1038/s41562-018-0395-3
Dadras, O., SeyedAlinaghi, S., Karimi, A., Shamsabadi, A., Qaderi, K., Ramezani, M., et al. (2022). COVID-19 mortality and its predictors in the elderly: A systematic review. Health Sci. Rep. 5:657. doi: 10.1002/hsr2.657
Dannefer, D. (2003). Cumulative advantage/disadvantage and the life course: cross-fertilizing age and social science theory. The J. Gerontol. Series B Psychol. Sci. Soc. Sci. 58, S327–S337. doi: 10.1093/geronb/58.6.S327
De Jong, H. (2015). “Living standards in a modernizing world - A long-run perspective on material wellbeing and human development,” in Global Handbook of Quality of Life , eds W. Glatzer, L. Camfield, V. Møller, and M. Rojas (Cham: Springer), 45–74.
Deaton, A. (2008). Income, health, and well-being around the world: evidence from the Gallup World Poll. J. Econ. Persp. 22, 53–72. doi: 10.1257/jep.22.2.53
Delle Fave, A., Brdar, I., Freire, T., Vella-Brodrick, D., and Wissing, M. (2011). The eudaimonic and hedonic components of happiness: qualitative and quantitative findings. Soc. Indic. Res. 100, 185–207. doi: 10.1007/s11205-010-9632-5
Derrer-Merk, E., Ferson, S., Mannis, A., Bentall, R. P., and Bennett, K. M. (2022a). Belongingness challenged: exploring the impact on older adults during the COVID-19 pandemic. PLoS ONE 17, 1–19. doi: 10.1371/journal.pone.0276561
Derrer-Merk, E., Reyes-Rodriguez, M., Salazar, A. M., Guevara, M., Rodríguez, G., Fonseca, A. M., et al. (2022b). Is protecting older adults from COVID-19 ageism? A comparative cross-cultural constructive grounded theory from the United Kingdom and Colombia. J. Soc. Issues 78, 900–923. doi: 10.1111/josi.12538
Diener, E. (2012). New findings and future directions for subjective well-being research. Am. Psychol. 67, 590–597. doi: 10.1037/a0029541
Diener, E., Emmons, R. A., Larsen, R. J., and Griffin, S. (1985). The satisfaction with life scale. J. Pers. Assess. 49, 71–75. doi: 10.1207/s15327752jpa4901_13
Dones, I. (2023). Life satisfaction among Italian migrants, Italian stayers, and Swiss natives: who fares better? Comp. Pop. Stu. 48, 457–492. doi: 10.12765/CPoS-2023-18
Dones, I., and Ciobanu, R. O. (2022). Older migrants' life satisfaction. GeroPsych 35, 55–66. doi: 10.1024/1662-9647/a000288
Dones, I., Ciobanu, R. O., and Baeriswyl, M. (2022). (Im)mobilities and life satisfaction in times of COVID-19: THE case of older persons in Switzerland. Int. Health Trends Persp. 2, 35–50. doi: 10.32920/ihtp.v2i1.1590
Donizzetti, A. R., and Capone, V. (2023). Ageism and the pandemic: risk and protective factors of well-being in older people. Geriatrics 8:14. doi: 10.3390/geriatrics8010014
Elgar, F. J., Davis, C. G., Wohl, M. J., Trites, S. J., Zelenski, J. M., Martin, M. S., et al. (2011). Social capital, health and life satisfaction in 50 countries. Health Place 17, 1044–1053. doi: 10.1016/j.healthplace.2011.06.010
E. M Janssen, J. H. M., Nieuwboer, M. S., Olde Rikkert, M. G. M., and Peeters, G. M. E. E. (2022). The psychosocial adaptability of independently living older adults to COVID-19 related social isolation in the Netherlands: a qualitative study. Health Soc. Care Commun. 30, e67–e74. doi: 10.1111/hsc.13436
Eurostat (2023). Population Structure and Ageing . Available online at: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Population_structure_and_ageing (accessed May 03, 2023).
Facal, D., Rodríguez-González, R., Martínez-Santos, A. E., and Gandoy-Crego, M. (2022). Positive and negative feelings among spanish young–old and old–old during the lockdown of the COVID-19 first wave. Clin. Gerontol. 45, 31–35. doi: 10.1080/07317115.2021.1929633
Falvo, I., Zufferey, M. C., Albanese, E., and Fadda, M. (2021). Lived experiences of older adults during the first COVID-19 lockdown: a qualitative study. PLoS ONE 16, 1–18. doi: 10.1371/journal.pone.0252101
Ferrante, P. (2022). The first 2 years of COVID-19 in Italy: incidence, lethality, and health policies. Front. Pub. Health 10:743. doi: 10.3389/fpubh.2022.986743
Finlay, J. M., Kler, J. S., O'Shea, B. Q., Eastman, M. R., Vinson, Y. R., Kobayashi, L. C., et al. (2021). Coping during the COVID-19 pandemic: a qualitative study of older adults across the United States. Front. Pub. Health 9, 1–12. doi: 10.3389/fpubh.2021.643807
Fiocco, A. J., Gryspeerdt, C., and Franco, G. (2021). Stress and adjustment during the COVID-19 pandemic: a qualitative study on the lived experience of canadian older adults. Int. J. Environ. Res. Pub. Health 18:24. doi: 10.3390/ijerph182412922
FOPH (2022). Coronavirus: Federal Council to Lift Measures – Mask Requirement on Public Transport and in Healthcare Institutions and Isolation in the Event of Illness to Remain Until End of March. Available online at: https://www.bag.admin.ch/bag/en/home/das-bag/aktuell/medienmitteilungen.msg-id-87216.html (accessed April 27, 2023).
Fried, L. P., Tangen, C. M., Walston, J., Newman, A. B., Hirsch, C., Gottdiener, J., et al. (2001). Frailty in older adults: evidence for a phenotype. J. Geront. Med. Sci. 56:545770. doi: 10.1093/gerona/56.3.M146
FSO (2020). “ Foreign Population.” Federal Statistical Office . Available online at: https://www.bfs.admin.ch/bfs/en/home/statistics/population/migration-integration/foreign.html (accessed January 13, 2023).
Fuller, H. R., and Huseth-Zosel, A. (2021). Lessons in resilience: initial coping among older adults during the COVID-19 pandemic. The Gerontol. Cite Gerontol. 61, 114–125. doi: 10.1093/geront/gnaa170
Gallè, F., Sabella, E. A., Roma, P., Ferracuti, S., Molin, D., Diella, G., et al. (2021). Knowledge and lifestyle behaviors related to COVID-19 pandemic in people over 65 years old from southern Italy. Int. J. Environ. Res. Pub. Health 18:10872. doi: 10.3390/ijerph182010872
Galobardes, B., Lynch, J., and Smith, G. D. (2007). Measuring socioeconomic position in health research. Br. Med. Bullet . 82, 21–37. doi: 10.1093/bmb/ldm001
Garner, I. W., Varey, S., Navarro-Pardo, E., Marr, C., and Holland, C. A. (2022). An observational cohort study of longitudinal impacts on frailty and well-being of COVID-19 lockdowns in older adults in England and Spain. Health Soc. Care Commun. 30, e2905–e2916. doi: 10.1111/hsc.13735
Gonçalves, A. R., Barcelos, J. L. M., Duarte, A. P., Lucchetti, G., Gonçalves, D. R., Silva e Dutra, F. C. M., et al. (2022). Perceptions, feelings, and the routine of older adults during the isolation period caused by the COVID-19 pandemic: a qualitative study in four countries. Aging Mental Health 26, 911–918. doi: 10.1080/13607863.2021.1891198
Grundy, E. (2006). Ageing and vulnerable elderly people: european perspectives. Ageing Soc. 26, 105–134. doi: 10.1017/S0144686X05004484
Guzman, V., Doyle, D., Foley, R., Craven, P., Crowe, N., Wilson, P., et al. (2023). Socio-ecological determinants of older people's mental health and wellbeing during the COVID-19 pandemic: a qualitative analysis within the Irish context. Front. Pub. Health 12:1148758. doi: 10.3389/fpubh.2023.1148758
Helliwell, J. F. (2003). How's life? Combining individual and national variables to explain subjective well-being. Econ. Modell. 20, 331–360. doi: 10.1016/S0264-9993(02)00057-3
Helliwell, J. F., and Putnam, R. D. (2004). The social context of well-being. Philos. Trans. Royal Soc. London Series Biol. Sci. 359, 1435–1446. doi: 10.1098/rstb.2004.1522
Hiscott, J., Alexandridi, M., Muscolini, M., Tassone, E., Palermo, E., Soultsioti, M., et al. (2020). The global impact of the coronavirus pandemic. Cytokine Growth Factor Rev. 53, 1–9. doi: 10.1016/j.cytogfr.2020.05.010
Holaday, L. W., Oladele, C. R., Miller, S. M., Dueñas, M. I., Roy, B., Ross, J. S., et al. (2021). Loneliness, sadness, and feelings of social disconnection in older adults during the COVID-19 pandemic. J. Am. Geriatr. Soc. 70, 329–340. doi: 10.1111/jgs.17599
Jiang, D. (2020). Perceived stress and daily well-being during the COVID-19 outbreak: the moderating role of age. Front. Psychol. 11:571873. doi: 10.3389/fpsyg.2020.571873
Jordan, R. E., Adab, P., and Cheng, K. K. (2020). COVID-19: risk factors for severe disease and death. BMJ 12:m1198. doi: 10.1136/bmj.m1198
Khlat, M., Ghosn, W., Guillot, M., Vandentorren, S., Delpierre, C., Desgrées du Loû, A., et al. (2022). Impact of the COVID-19 crisis on the mortality profiles of the foreign-born in France during the first pandemic wave. Soc. Sci. Med. 313:115160. doi: 10.1016/j.socscimed.2022.115160
Klausen, S. H. (2020). Understanding older adults' wellbeing from a philosophical perspective. J. Happiness Stu. 21, 2629–2648. doi: 10.1007/s10902-019-00197-5
Kola, L., Kohrt, B. A., Hanlon, C., Naslund, J. A., Sikander, S., Balaji, M., et al. (2021). COVID-19 mental health impact and responses in low-income and middle-income countries: reimagining global mental health. The Lancet Psychiatr. 8, 535–550. doi: 10.1016/S2215-0366(21)00025-0
König, R., and Isengard, B. (2023). Coping with COVID-19: older europeans and the challenges of connectedness and loneliness. Soc. Inclusion 11, 310–323. doi: 10.17645/si.v11i1.6072
Lazarus, R., and Folkman, S. (1984). Stress, Appraisal, and Coping . Cham: Springer.
Losada-Baltar, A., Jiménez-Gonzalo, L., Gallego-Alberto, L., Pedroso-Chaparro, M., Fernandes-Pires, J., and Márquez-González, M. (2021). “We are staying at home.” association of self-perceptions of aging, personal and family resources, and loneliness with psychological distress during the lock-down period of COVID-19. The J. Gerontol. Series B 76, e10–e16. doi: 10.1093/geronb/gbaa048
Luchetti, M., Lee, J. H., Aschwanden, D., Sesker, A., Strickhouser, J. E., Terracciano, A., et al. (2020). The trajectory of loneliness in response to COVID-19. Am. Psychol. 75, 897–908. doi: 10.1037/amp0000690
Ludwig-Dehm, S. M., Dones, I., and Ciobanu, R. O. (2023). Between here and there: comparing the worry about the pandemic between older Italian international migrants and natives in Switzerland. Comp. Migr. Stu. 11, 1–24. doi: 10.1186/s40878-023-00331-6
Luhmann, M., Krasko, J., and Terwiel, S. (2021). “Subjective well-being as a dynamic construct,” in The Handbook of Personality Dynamics and Processes (Amsterdam: Elsevier), 1231–1249.
Macdonald, B., and Hülür, G. (2021). Well-being and loneliness in swiss older adults during the COVID-19 pandemic: the role of social relationships. Gerontologist 61, 240–250. doi: 10.1093/geront/gnaa194
Macleod, S., Tkatch, R., Kraemer, S., Fellows, A., McGinn, M., Schaeffer, J., et al. (2021). COVID-19 era social isolation among older adults. Geriatrics 6, 1–15. doi: 10.3390/geriatrics6020052
Maggiori, C., Dif-Pradalier, M., and Villani, M. (2022). ““Vous êtes à risque, restez à la maison”. Les 65+ face à la COVID-19,” in COVID-19 Les Politiques Sociales à l'épreuve de la Pandémie , eds E. Rosenstein and S. Mimouni (Verlag: Seismo Verlag AG), 273–286.
Mau, M., Fabricius, A. M., and Klausen, S. H. (2022). Keys to well-being in older adults during the COVID-19 pandemic: personality, coping and meaning. Int. J. Q. Stu. Health Well-Being 17:669. doi: 10.1080/17482631.2022.2110669
McKinlay, A. R., Fancourt, D., and Burton, A. (2021). A qualitative study about the mental health and wellbeing of older adults in the UK during the COVID-19 pandemic. BMC Geriatr. 21:439. doi: 10.1186/s12877-021-02367-8
Mendez-Lopez, A., Stuckler, D., McKee, M., Semenza, J. C., and Lazarus, J. V. (2022). The mental health crisis during the COVID-19 pandemic in older adults and the role of physical distancing interventions and social protection measures in 26 European countries. SSM – Pop. Health 17:101017. doi: 10.1016/j.ssmph.2021.101017
Nehring, D., and Hu, Y. (2022). COVID-19, nation-sates and fragile transnationalism. Sociology 56, 183–190. doi: 10.1177/00380385211033729
Neville, S., Wright-St Clair, V., Montayre, J., Adams, J., and Larmer, P. (2018). Promoting Age-Friendly Communities: an Integrative Review of Inclusion for Older Immigrants. Journal of Cross-Cultural Gerontology 33, 427–440. doi: 10.1007/s10823-018-9359-3
Oliveira, M. R., Sudati, I. P., Konzen, V. D. M., de Campos, D., Wibelinger, A. C., Correa, L. M., et al. (2022). COVID-19 and the impact on the physical activity level of elderly people: A systematic review. Exp. Gerontol. 159:111675. doi: 10.1016/j.exger.2021.111675
Oris, M., Ramiro Farinas, D., Pujol Rodríguez, R., and Abellán, A. (2020). “La crise comme révélateur de la position sociale des personnes âgées,” in Le regard des Sciences Sociales , eds F. Gamba, M. Nardone, T. Ricciardi, and S. Cattacin (Geneva: Seismo), 179–191.
O'Shea, B. Q., Finlay, J. M., Kler, J., Joseph, C. A., and Kobayashi, L. C. (2021). Loneliness among US adults aged ≥55 early in the COVID-19 pandemic. Pub. Health Rep. 136, 754–764. doi: 10.1177/00333549211029965
Ozemek, C., Lavie, C. J., and Rognmo, Ø. (2019). Global physical activity levels - Need for intervention. Prog. Cardiovascular Dis. 62, 102–107. doi: 10.1016/j.pcad.2019.02.004
Pan, H., Fokkema, T., Switsers, L., Dury, S., Hoens, S., De Donder, L., et al. (2021). Older Chinese migrants in coronavirus pandemic: exploring risk and protective factors to increased loneliness. Eur. J. Ageing 18, 207–215. doi: 10.1007/s10433-021-00625-7
Petretto, D. R., and Pili, R. (2020). Ageing and COVID-19: What is the role for elderly people? Geriatrics 5:25. doi: 10.3390/geriatrics5020025
Pleninger, R., Streicher, S., and Sturm, J. E. (2022). Do COVID-19 containment measures work? Evidence from Switzerland. Swiss J. Econ. Stat. 158:5. doi: 10.1186/s41937-022-00083-7
Riaño, Y., and Wastl-Walter, D. (2006). Immigration policies, state discourses on foreigners, and the politics of identity in Switzerland. Environ. Plann. A 38, 1693–1713. doi: 10.1068/a37411
Robson, J. P. Jr., and Troutman-Jordan, M. (2014). A concept analysis of cognitive reframing. J. Theor. Constr. Testing 18, 55–59.
Rodney, T., Josiah, N., and Baptiste, D. (2021). Loneliness in the time of COVID-19: Impact on older adults. J. Adv. Nurs. 77:14856. doi: 10.1111/jan.14856
Røysamb, E., Nes, R. B., Czajkowski, N. O., and Vassend, O. (2018). Genetics, personality and wellbeing. A twin study of traits, facets and life satisfaction. Sci. Rep. 8, 1–13. doi: 10.1038/s41598-018-29881-x
Røysamb, E., Nes, R. B., and Vittersø, J. (2014). Well-Being: Heritable and Changeable. Stability of Happiness. Amsterdam: Elsevier, 9–36.
Sager, F., and Mavrot, C. (2020). Switzerland's COVID-19 policy response: consociational crisis management and neo-corporatist reopening. Eur. Policy Anal. 6:293. doi: 10.1002/epa2.1094
Seckman, C. (2023). The impact of COVID-19 on the psychosocial well-being of older adults: a literature review. J. Nurs. Scholarship 55, 97–111. doi: 10.1111/jnu.12824
Segerstrom, S. C., Crosby, P., Witzel, D. D., Kurth, M. L., Choun, S., Aldwin, C. M., et al. (2023). Adaptation to changes in COVID-19 pandemic severity: across older adulthood and time scales. Psychol. Aging . 22:7390 doi: 10.1037/pag0000739
Seifert, A. (2021). Older adults during the COVID-19 pandemic – Forgotten and stigmatized? Int. Soc. Work 64, 275–278. doi: 10.1177/0020872820969779
Seifert, A., and Hassler, B. (2020). Impact of the COVID-19 pandemic on loneliness among older adults. Front. Sociol. 5, 1–6. doi: 10.3389/fsoc.2020.590935
Settersten, R. A., Bernardi, L., Härkönen, J., Antonucci, T. C., Dykstra, P. A., Heckhausen, J., et al. (2020). Understanding the effects of Covid-19 through a life course lens. Adv. Life Course Res. 45:100360. doi: 10.1016/j.alcr.2020.100360
Sidani, S., Northwood, M., Sethi, B., Zhuang, Z. C., and Edhi, K. (2022). Social isolation and loneliness in older immigrants during COVID-19: a scoping review. Int. J. Migr. Health Soc. Care 18, 164–178. doi: 10.1108/IJMHSC-08-2021-0071
SkyTG24 (2020). Coronavirus, dai locali alle Palestre: Tutte le Misure nel Nuovo Dpcm di ottobre . Available online at: https://tg24.sky.it/cronaca/2020/10/25/nuovo-dpcm-conte-ottobre#00 (accessed October 25, 2020).
Sneed, R. S., and Krendl, A. C. (2022). What factors are associated with psychological vulnerability and resiliency among older adults during the COVID-19 pandemic? J. Gerontol. B. Psychol. Sci. Soc. 77, 1–4. doi: 10.1093/geronb/gbac027
Spini, D., Bernardi, L., and Oris, M. (2017). Toward a life course framework for studying vulnerability. Res. Hum. Dev. 14, 5–25. doi: 10.1080/15427609.2016.1268892
Su, Y., Rao, W., Li, M., Caron, G., D'Arcy, C., Meng, X., et al. (2023). Prevalence of loneliness and social isolation among older adults during the COVID-19 pandemic: a systematic review and meta-analysis. Int. Psychogeriatr. 35, 229–241. doi: 10.1017/S1041610222000199
Tosato, M., Ciciarello, F., Zazzara, M. B., Janiri, D., Pais, C., Cacciatore, S., et al. (2022). Lifestyle changes and psychological well-being in older adults during COVID-19 pandemic. Clin. Geriatr. Med. 38, 449–459. doi: 10.1016/j.cger.2022.05.002
UNDESA (2020). International Migrant Stock 2020. United Nations Department of Economic and Social Affairs. Available online at: https://www.un.org/development/desa/pd/content/international-migrant-stock (accessed January 13, 2023).
Van Tilburg, T. G., Steinmetz, S., Stolte, E., Van Der Roest, H., and Vries, D. H. (2021). Loneliness and mental health during the COVID-19 pandemic: a study among dutch older adults. J. Gerontol. B Psychol. Sci. Soc. Sci. 76, 249–255. doi: 10.1093/geronb/gbaa111
Veenhoven, R. (2012). “Happiness: Also known as “life satisfaction” and “subjective well-being,” in Handbook of Social Indicators and Quality of Life Research , eds K. Land, A. Michalos, and M. Sirgy (Cham: Springer Netherlands), 63–77.
PubMed Abstract | Google Scholar
Veenhoven, R. (2017). “Measures of happiness: Which to choose?,” in Metrics of Subjective Well-Being: Limits and Improvements , eds G. Brulé and F. Maggino (Cham: Springer International Publishing), 65–84.
Webb, L. M., and Chen, C. Y. (2022). The COVID-19 pandemic's impact on older adults' mental health: contributing factors, coping strategies, and opportunities for improvement. Int. J. Geriatr. Psychiatr. 37:5647. doi: 10.1002/gps.5647
Wessendorf, S. (2007). ‘Roots migrants': transnationalism and ‘return' among second-generation italians in Switzerland. J. Ethnic Migr. Stu. 33, 1083–1102. doi: 10.1080/13691830701541614
Wettstein, M., Nowossadeck, S., and Vogel, C. (2022a). Well-being trajectories of middle-aged and older adults and the corona pandemic: No “COVID-19 effect” on life satisfaction, but increase in depressive symptoms. Psychol. Aging 37, 175–189. doi: 10.1037/pag0000664
Wettstein, M., Wahl, H.-W., and Schlomann, A. (2022b). The impact of the COVID-19 pandemic on trajectories of well-being of middle-aged and older adults: a multidimensional and multidirectional perspective. J. Happiness Stu. 23, 3577–3604. doi: 10.1007/s10902-022-00552-z
Whitehead, B. R., and Torossian, E. (2021). Older adults' experience of the COVID-19 pandemic: a mixed-methods analysis of stresses and joys. The Gerontol. 61, 36–47. doi: 10.1093/geront/gnaa126
WHO (2018). Health of Older Refugees and Migrants. Geneva: WHO.
WHO (2020). WHO Director-General's Opening Remarks at the Media Briefing on COVID-19 - 11 March 2020 . Available online at: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19 (accessed March 11, 2020).
Widmer, E. (2022). “COVID-19 et développement des vulnérabilités: Entre normes déroutantes et manque de réserves,” in COVID-19 Tome II: Les politiques sociales à l'épreuve de la pandémie , eds E. Rosenstein and S. Mimouni (Geneva: Seismo), 225–240.
Yancura, L. A., and Aldwin, C. M. (2008). Coping and health in older adults. Curr. Psychiatr. Rep. 10, 10–15. doi: 10.1007/s11920-008-0004-7
Zaninotto, P., Iob, E., Demakakos, P., and Steptoe, A. (2022). Immediate and Longer-term changes in the mental health and well-being of older adults in England during the COVID-19 pandemic. JAMA Psychiatr. 79:151. doi: 10.1001/jamapsychiatry.2021.3749
Keywords: migration, coping, subjective wellbeing, health crisis, vulnerability
Citation: Dones I and Ciobanu RO (2024) Older adults' experiences of wellbeing during the COVID-19 pandemic: a comparative qualitative study in Italy and Switzerland. Front. Sociol. 9:1243760. doi: 10.3389/fsoc.2024.1243760
Received: 21 June 2023; Accepted: 15 April 2024; Published: 01 May 2024.
Reviewed by:
Copyright © 2024 Dones and Ciobanu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY) . The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Iuna Dones, iuna.dones@hesge.ch
This article is part of the Research Topic
Community Series in Mental Illness, Culture, and Society: Dealing with the COVID-19 Pandemic, volume VIII
- Open access
- Published: 04 May 2024
Delivering clinical tutorials to medical students using the Microsoft HoloLens 2: A mixed-methods evaluation
- Murray Connolly 1 ,
- Gabriella Iohom 1 ,
- Niall O’Brien 2 ,
- James Volz 2 ,
- Aogán O’Muircheartaigh 3 ,
- Paschalitsa Serchan 3 ,
- Agatha Biculescu 3 ,
- Kedar Govind Gadre 3 ,
- Corina Soare 1 ,
- Laura Griseto 3 &
- George Shorten 1
BMC Medical Education volume 24 , Article number: 498 ( 2024 ) Cite this article
12 Altmetric
Metrics details
Mixed reality offers potential educational advantages in the delivery of clinical teaching. Holographic artefacts can be rendered within a shared learning environment using devices such as the Microsoft HoloLens 2. In addition to facilitating remote access to clinical events, mixed reality may provide a means of sharing mental models, including the vertical and horizontal integration of curricular elements at the bedside. This study aimed to evaluate the feasibility of delivering clinical tutorials using the Microsoft HoloLens 2 and the learning efficacy achieved.
Following receipt of institutional ethical approval, tutorials on preoperative anaesthetic history taking and upper airway examination were facilitated by a tutor who wore the HoloLens device. The tutor interacted face to face with a patient and two-way audio-visual interaction was facilitated using the HoloLens 2 and Microsoft Teams with groups of students who were located in a separate tutorial room. Holographic functions were employed by the tutor. The tutor completed the System Usability Scale, the tutor, technical facilitator, patients, and students provided quantitative and qualitative feedback, and three students participated in semi-structured feedback interviews. Students completed pre- and post-tutorial, and end-of-year examinations on the tutorial topics.
Twelve patients and 78 students participated across 12 separate tutorials. Five students did not complete the examinations and were excluded from efficacy calculations. Student feedback contained 90 positive comments, including the technology’s ability to broadcast the tutor’s point-of-vision, and 62 negative comments, where students noted issues with the audio-visual quality, and concerns that the tutorial was not as beneficial as traditional in-person clinical tutorials. The technology and tutorial structure were viewed favourably by the tutor, facilitator and patients. Significant improvement was observed between students’ pre- and post-tutorial MCQ scores (mean 59.2% Vs 84.7%, p < 0.001).
Conclusions
This study demonstrates the feasibility of using the HoloLens 2 to facilitate remote bedside tutorials which incorporate holographic learning artefacts. Students’ examination performance supports substantial learning of the tutorial topics. The tutorial structure was agreeable to students, patients and tutor. Our results support the feasibility of offering effective clinical teaching and learning opportunities using the HoloLens 2. However, the technical limitations and costs of the device are significant, and further research is required to assess the effectiveness of this tutorial format against in-person tutorials before wider roll out of this technology can be recommended as a result of this study
Peer Review reports
Introduction
Clinical tutorials which include encounters with real patients are recognised as integral elements in medical education [ 1 , 2 , 3 ]. Sir William Osler famously stated that “medicine is learned by the bedside and not in the classroom.” [ 4 ] However, many medical schools are facing challenges in delivering clinical education to students in an environment where there are increasing numbers of students, a limited number of patients and tutors, and increased scrutiny regarding the costs and environmental impacts of travel [ 5 , 6 , 7 , 8 ]. The COVID-19 pandemic also had a significant impact on in-person medical education in many countries, where students’ access to patients was severely curtailed [ 9 , 10 ]..
The argument that medical education requires interactive tutorials on actual patients is supported by various educational theories. Bandura’s Social Learning Theory and Social Cognitive Theory propose that students learn via attention, retention, reproduction and motivation [ 11 , 12 ]. This supports the need for direct observation and modelling of relevant clinical role-models participating in doctor-patient interactions [ 13 , 14 ]..
The Constructivist theory is based on the premise that the act of learning is based on a process which connects new knowledge to pre-existing knowledge [ 15 , 16 ]. Vertical Integration in medical education involves the integration of aspects of the curriculum across time, namely the integration of basic sciences and clinical sciences [ 17 , 18 , 19 ]..
Providing medical education within these frameworks, prioritising student exposure to direct interactions with clinicians and patients, and vertical integration of curriculum material, in situations where physical access to patients may be limited by numbers, logistics or infection control concerns poses a significant challenge to medical schools around the world. Utilising technology to facilitate the delivery of clinical education remotely may present a solution to these issues.
The broadcast of bedside tutorials to a remote location can be delivered using a “third-person” perspective, via a fixed or mobile broadcasting device, or using a first-person perspective, via a device mounted on the tutor. Devices which provide a first-person perspective are typically head-mounted-display devices (HMDs). The capabilities of these devices range widely, from basic two-way communication with a remote location, to devices with Augmented Reality (AR) and Mixed Reality (MR) functions which allow the integration of holographic artefacts into tutorials.
Augmented reality (AR) is a virtual environment that allows the user to view both their physical environment and virtual elements in real-time. Mixed Reality (MR) is an extension of AR which allows the real and holographic elements to interact [ 20 , 21 ]..
The use of AR and MR are expanding in many industries including healthcare, education, engineering, and manufacturing [ 22 , 23 , 24 ]. MR investigated in a variety of settings pertaining to medical education. Many early studies focused on teaching relevant anatomy, and more recently studies have evaluated the use of MR in procedural training, and its use in streaming of clinical ward-rounds to medical students [ 25 , 26 , 27 , 28 , 29 , 30 , 31 , 32 , 33 ]..
Head-mounted-display devices which offer MR experiences are growing in number and capability [ 34 ].The Microsoft HoloLens2 is one such device which enables the creation of an immersive Mixed Reality environment and can superimpose holographic images onto the user’s surroundings.
The HoloLens 2 has a number of specific capabilities which can be utilised in the virtual delivery of in-person clinical tutorials.The device can facilitate educationally effective, three-way communication between students, tutors and patients, as well as facilitating the incorporation of mixed reality elements into tutorials. The MR capabilities may provide a means of sharing holographic artefacts such as images and diagrams, which can allow the vertical and horizontal integration of curricular elements at the bedside.Utilisation of the MR capabilities of the device may improve student experiences and learning, in particular through instructional scaffolding (e.g rendering cell, organ or system pathways proximate to a patient) [ 35 ] Given the device’s connectivity capabilities, students can be in a separate geographical location to the patient and tutor. This has the potential to decrease student travel requirements and enables the delivery of tutorials to students in multiple different locations simultaneously [ 36 ]. The tutorial can also be delivered to a greater number of students than would be practical in a traditional bedside clinical tutorial environment. This can decrease the burden on both tutors and patients in comparison to multiple smaller group sessions. Finally, infection control risks are reduced as only the tutor enters patients’ environments.
Study goals
There is little published research to date which robustly evaluates the use of the HoloLens in replicating bedside tutorials while also incorporating mixed reality elements into the tutorials. The aims of this study are to evaluate the use of the Microsoft HoloLens 2 device to deliver a tutorial on preoperative anaesthetic history and upper airway examination to medical students in a remote location, while incorporating MR holograms in the tutorial delivery. Specific objectives include evaluating the feasibility of delivering tutorials with the HoloLens device, assessing the learning efficacy of these tutorials, and assessing student, tutor, facilitator, and patient perspectives of the tutorials.
This study was approved by the Clinical Research Ethic Committee of the Cork Teaching Hospitals, and the University College Cork Research and Postgraduate Affairs Committee. All participants including students, patients, tutor and technical facilitator provided written informed consent prior to inclusion in the study.
Study population
University College Cork medical students from two cohorts, third year Graduate-Entry and fourth year Direct-Entry medical students attending a tertiary referral teaching hospital for a clinical attachment with the Department of Anaesthesia and Intensive Care Medicine were invited to participate in the study. Both groups are in their second-last year of medical training, and thus have completed modules and examinations in basic medical sciences and clinical practice in the preceding years, with a maximum of 1 week experience in the field of anaesthesia [ 37 , 38 , 39 ]. Patients attending Cork University Hospital for scheduled surgery were selected and approached for consent by tutors according to clinical relevance. All participants were 18 years or over and were deemed capable of providing consent. Each student provided information on their age, gender and previous third-level qualifications.
Tutorial Sturcture
A one-hour tutorial focusing on completing a preoperative history and focused assessment of the upper airway was developed by MC (adjunct clinical lecturer), GI (Senior Clinical Lecturer) and GS (Professor) in line with the University curriculum’s learning objectives. (Fig. 1 ) Tutorials were delivered on a weekly basis to groups of third year Graduate Entry and fourth year Direct Entry medical students across the 2021–2022 academic year.

Preoperative Anaesthetic History and Focused Preoperative Assessment of the upper airway tutorial structure
All tutorials were delivered by one tutor (MC) and assisted by a technical facilitator (NOB), both males aged in their thirties, who enabled the connection between the site of the clinical encounter and nearby tutorial room. The tutor had no prior experience with the HoloLens 2 device or other AR HMDs prior to participation in this study; the facilitator had significant experience in its use. The tutor was given a period of familiarisation with the device which included using the Microsoft “HoloLens Tips” app, which provides a structured tutorial on the various hand gestures used to control the device, as well as a number of practice calls in order to test the network and audiovisual equipment in the tutorial room [ 40 ]. This familiarisation period totalled approximately 3 hours.
During the tutorial, the tutor (MC) interacted with a patient (face to face) in the pre-or postoperative units and remotely with a small group of [ 6 , 7 , 8 , 9 , 10 ] students in a nearby tutorial room. The remote interaction occurred via Hololens 2 worn by the tutor, institutional Wi-Fi (Eduroam), and Microsoft Teams.He demonstrated and explained the techniques of preoperative history taking and preoperative upper airway assessment.
Throughout the patient assessment the tutor interacted both with the patient and with the students as if conducting an in-person tutorial, providing additional information, asking the students pertinent questions, and expanding on the findings of the patient’s history and physical examination. Students communicated with the patient by asking questions via the tutor.
Resources employed
Resources necessary to provide the tutorials via the HoloLens included capital costs of the HoloLens device (€3500) and microphone (€88) as well as annual licence costs of €275 per user ( n = 4). Human resources employed in developing the tutorials and trialling equipment included approximately 20 hours of training, remote assistance (Microsoft) and collaboration between the tutor (MC), Professor (GS) and facilitator (NOB), as well as 5 hours input from the Senior Clinical Lecturer (GI).
Internet connectivity
An internet connection of at least 1.5mpbs of bandwidth is recommended by Microsoft for best audio, visual and content sharing experience [ 41 ]. Secure, password protected wireless internet access via the University institutional network (Eduroam) was utilised by both tutor and students.
In most tutorials, broadcasts were hosted by an MSI running the Windows 10 operating system, audio was amplified using a Bose SoundLink Mini portable speaker and video was screened via a HDMI cable to a 36″ monitor. In one tutorial students accessed the tutorial via their personal smartphones or laptops. In order to bypass the noise cancellation technology within the HoloLens an external microphone (Saramonic SmartMic+UC L/weight Smartphone Mic USB-C) and 3.5 mm earphone were used.
Dynamics 365 Remote Assist application was used, in-tandem with Microsoft Teams, to host each video call. This connection allowed the students to see the tutors field of vision and hear both the tutor and patient. Hand gestures including the “hand-ray”, “air-tap”, “air-tap and hold” and “start-gesture” were used to control the HMD and manipulate the holographic artefacts. Relevant holographic artefacts were superimposed during the tutorial. This included the insertion of diagramatic representaions of the Mallampati scoring system and Thyromental Distance during the airway assessment portion of the tutorial [Fig. 2 (a) and (b)]. The holographic pointer and “drawing” functions were used by the tutor to highlight relevant upper airway structures and emphasise information on the holographic diagrams [Fig. 2 (c) and (d)].

a Assessment of Mallampati Score. b Assessment of Thyromental Distance. c Identification of thyroid cartilage using holographic pointer. d Illustration of holographic “drawing” function
Assessment of tutor perceptions
Immediately after completion of the first tutorial, the tutor completed a System Usability Scale assessment and on completion of the last tutorial, the tutor and facilitator summarised their perceptions of using the HMD.
Assessment of student perceptions
Immediately after completion of the tutorial, students completed a modified Evaluation of Technology-Enhanced Learning Materials: Learner Perceptions (ETELM-LP) questionnaire in order to assess their perceptions of the tutorial, which incorporated a seven-point Likert Scale and open questions [ 42 ]. Cronbach’s Alpha was calculated after exclusion of question 1 and reverse scoring of questions 13 and 15.
Three students also took part in semi-stuctured interviews via Microsoft Teams. Researchers undertook this study from an interpretive approach [ 43 ]. The interviews were conducted by JV, and followed a template of questions and corresponding probes from which the interviewer expanded as appropriate [Additional file 1 ]. The template served as a foundation from which the interviewer expanded as appropriate. The interviews were recorded and transcribed. Analysis of the interview transcripts and questionnare responses was performed using Dedoose Qualitative Research Software Version 4.3.Qualitative data from interviews and feedback questionnaires were coded thematically in alignment with Clarke and Braun’s suggestions for qualitative analysis [ 44 ]. Following the initial thematic coding, researchers conducted a content analysis to strengthen the interpretation of results. Illustrative quotes were chosen based on the representativeness of the theme or subtheme and the clarity of their intrinsic interpretation. In alignment with current literature, the quotes selected were determined to be illustrative of the point, reflective of patterns observed, and relatively succinct [ 45 ]..
Assessment of patient perceptions
On completion of the tutorials, patients were also asked to complete a mixed quantitative and qualitative questionnaire in order to assess their perceptions of the tutorial.
Assessment of learning efficacy
We carried out a prospective non-comparative study of tutorial efficacy. Students completed a pre-tutorial Multiple Choice Question (MCQ) examination to assess baseline knowledge [Additional file 2 ], and a post-tutorial MCQ two to 3 days later [Additional file 3 ]. Students then completed an end-of-year assessment two to 5 months later consisting of a data interpretation exam and an Objective Structured Clinical Examination (OSCE) which focused on preoperative history taking and preoperative assessment of the upper airway respectively [Additional files 4 and 5 ]. These examinations were written by an investigator and the University Senior Clinical Lecturer in line with University standards. Examination results were converted to percentages and the data interpretation and OSCE results were combined to give a total End-of-Year result.
The Chi-Squared test was used to compare direct-entry and graduate-entry student demographics. Welch’s two-sample t-Test assuming unequal variances was used to compare student group ages. The Shapiro Wilk and Kolmogorov-Smirnov Tests were used to assess to normality of distribution of student assessment scores for data sets less than 50 and greater than 50 respectively. The Mann-Whitney U Test was performed to compare group performance in assessments and overall student performance between the pre- and post-tutorial examinations, and between the post-tutorial and End-of-Year scores. Cohen’s d was calculated for the pre and post-tutorial MCQ scores to assess effect size.
Twelve tutorials were completed involving 12 separate patients and 78 students. Four students did not complete the post-tutorial MCQ and one did not complete the End-of-Year assessments due to illness related absences. These students were excluded from efficacy calculations. Baseline characteristics of the student participants are summarised in Table 1 . As expected the graduate-entry students was a significantly older cohort (graduate-entry median age 26 vs direct-entry mean of 22). Mean age of patient participants was 43.25, with an SD of 16.48, and a range of 18–64.
Feasibility
We found that it was feasible to use the HoloLens2 to facilitate weekly bedside tutorials on live patients in a busy, tertiary referral teaching hospital. No tutorials were cancelled or postponed due to technology-related issues. Of note, in order to improve the audio quality of the patient’s voice, it was neccessary to add the USB microphone, which is not routinely supplied with the HoloLens 2. The tutorials were also dependent on secure Wi-Fi access for both tutor and students, the presence of a tutorial facilitator to control the equipment at the student end, and access to a quiet space to examine the patient.
Tutor feedback
The sole tutor (MC) completed the System Usability Scale score, which was 72.5 (a score > 68 is deemed above average). The tutor (MC) stated that the HoloLens 2 was found to be comfortable to wear, the visor was unobtrusive and did not interfere with interaction with the patient or impede visualisation of clinical signs. The interaction with the device via hand gestures was relatively smooth and intuitive after the intial familiarisation period and the MR functions including the insertion of holographic diagrams, pointing, drawing and highlighting were useful. The holographic artefacts were visible throughout the tutorials at a “brightness” setting of seven out of 10.
Occasionally when talking to the students via the HMD, it was not clear to the patient if the tutor was talking to the patient or to the students. Utilising a structured pattern of speech such as “I am now talking to the students” was found to be useful to overcome this issue.
Facilitator feedback
The technical facilitator (NOB) found that the set-up of the live broadcast to the students was akin to that of a video presentation and that the learning curve for hosting the tutorials was short as the Dynamic 365 Remote Assist application was quite similar to general videoconferencing software. He noted that patient proximity to the tutor was essential to ensure adequate audio quality and referenced an example where a supine patient was farther from the device than normal and that patient responses had to be repeated by the tutor. Backgound noise was noted as a “minor issue and transient in nature”, and the technical facilitator accepted that a certain amount of background noise was unavoidable in an active hospital ward.
Student feedback
Quantitative student feedback via the modified ETELM-LP questionnaire is summarised in Fig. 3 . Results are presented as (mean, SD) and refer to a seven-point Likert scale. Students had little experience in MR prior to the tutorial (1.7, 1.29). They found the audio and visual quality was clear and that the MR elements of the tutorial were useful. Most agreed the tutorial approximated a live patient encounter (5.69, 1.26), was more beneficial than a PowerPoint-based tutorial, and were neutral when asked if it was as beneficial as a live clinical encounter (5, 1.69). They did not agree that the tutorial structure required inappropriately high technology skill levels on the part of the students, nor that the MR elements served as a distraction. Most agreed that they would like MR to be incorporated into further tutorials (6.05, 1). Cronbach’s Alpha, excluding question 1 was calculated as 0.86, displaying good internal consistency.

Student Modified ETELM-LP Scores. 7 point Likert scale with 7 as strongly agree and 1 as strongly disagree. Presented as Mean +/− 1 Standard Deviation
Student qualitative feedback results
Analysis of written and verbal feedback from 78 students identified 90 specific positive excerpts and 62 negatives (Table 2 ). Positive feedback included the technology’s ability to broadcast the tutor’s point-of-vision, the inclusion of holographic artefacts, and the remote nature of the tutorial. Negative feedback included issues with the audio-visual stream quality, the fact that students were not able to individually carry out the practical examination, and 11 students expressed concerns that the tutorial was not as useful as traditional in-person bedside clinical tutorials.
Three students participated in semi-structured interviews. The limited sense of “presence” and interaction with the patient were identified as limitations to the format by all three interviewees. With respect to the physical examination one student explained he would have preferred to “experience it yourself, and have a look and feel and touch”. Specific mention was made of the value of combining broadcast (patient) and rendered (schematics) images, “The adding of the images … right next to the patient was really, really helpful”. This may indicate the potential to employ this format to support vertical and horizontal integration of curricular elements. All three interviewed students reported either a six or seven (on a verbal scale of 1–7) when asked to recommend this technology for inclusion in the medical curriculum.
Patient feedback
Quantitative feedback data from patient questionnaires is summarised in Fig. 4 . Most patients had little experience with MR in the past (mean, SD: 1.75, 1.48) apart from one patient who scored 6. All agreed that the communication with the tutor was clear, that they felt safe, that the experience was enjoyable and that they would participate in a similar session in the future. Six of seven expressed that it was preferable to both small (5 or less) and large group in-person tutorials. Most patients did not agree that the HoloLens served as a distraction or made them uncomfortable.

Patient Feedback Questionnaire Results. 7 point Likert scale with 7 as strongly agree and 1 as strongly disagree. Presented as Mean +/− 1 Standard Deviation
Five patients gave qualitative feedback. Positive comments included that “it is good to see that you are moving on with new technology”, “it was well explained beforehand so I was very comfortable” and “it was fantastic to teach students when they can’t be at the bedside. Very unobtrusive”. One patient commented that “sometimes not sure if he [the tutor] was talking to me or the students” and another commented that “it would be lovely to see who I was talking to [the student group]”.
Learning efficacy
Student examination scores are sumarised in Table 3 and Fig. 5 . Student assessment scores were not normally distrubuted. A statistically significant improvement was observed between overall students’ pre and post tutorial MCQ scores (mean 59.2% Vs 84.7%, p < 0.001). Cohen’s d was 0.612, indicating a medium effect size. There was a statistically significant difference in student performance between the post tutorial MCQ and the composite End-of-Year scores (84.7% Vs 82.2%, p < 0.05). There were no statistically significant differences found between the graduate-entry and direct-entry students for any individual examination.

Boxplot of overall student assessment scores
Mixed Reality headsets offer several novel capabilities which can facilitate remote education and vertical and horizontal integration of curriculum elements, particularly when aligned with appropriate educational theories such as Constructivism and Social Cognitive Theory. A large number of studies have focused on applying the technology in surgical and anatomical subject fields [ 46 ]. However, there are significant gaps in the evidence base, particularly studies specific to anaesthesiology, clinical exam, and addressing the provision of interactive tutorials to remote locations. Our study has demonstrated that it is feasible and effective to use the Microsoft HoloLens 2, incorporating its Mixed Reality functions to provide a live bedside tutorial on anaesthetic preoperative assessment to students situated in a remote location. Feedback from students, patients and the tutor were generally positive. Quantitative feedback from students regarding the audio-visual quality was mainly positive, however technical issues were noted, and preference for in-person tutorials was expressed by a minority of students.
Mill et al. previously examined the feasibility of the HoloLens 2 in broadcasting medical ward rounds [ 26 ]. While papers such as that by Mill et al. demonstrated the feasibility of utilizing the HoloLens 2 HMD to stream educational ward-rounds, they did not utilize the MR functions of the HMD, nor assess the learning efficacy of the device [ 26 ]. This study incorporates both quantitative and qualitative feedback from multiple sources, namely students, patients, the tutor, and tutorial facilitator. We believe this demonstrates a robust examination of the perceptions of the relevant stakeholders involved in the provision of clinical tutorials to medical students. Our findings that the tutorials were feasible, agreeable to both patients and students, and that students had occasional audio-visual difficulties are consistent with those of Mill et al. Our study additionally demonstrates that incorporation of holographic artefacts is both feasible and regarded by the tutor and students as useful, and that the tutorials provide effective knowledge acquisition.
Our tutorial format aimed to reproduce some of the educationally relevant components of an in-person tutorial. Other suggested structures advocate streaming video of the physician as opposed to the physician’s point-of-view [ 47 ]. The HoloLens 2 device allows the students to view the tutor’s field of vision which we argue is superior, and student feedback reflected this. This viewpoint allows students to appreciate in real time the clinical signs demonstrated during the clinical examination and correlate these with the holographic diagrammatic examples used. The MR environment provides an ideal setting to facilitate vertical integration in real time by displaying holographic artefacts of anatomical, physiological and pathological information, as well as patient specific data such as radiological imaging or lab results while interacting with a patient. Furthermore, delivering tutorials remotely reduces infection-control concerns and allows delivery to greater numbers of students in multiple locations.
Preserving patient confidentiality is essential in medical practice and education. In our study, both the HMD and devices at the student end were connected to secure institutional Wi-Fi and accessed via University accounts. Also, access to the audio-visual stream was controlled by the technical facilitator, and the students were located in a supervised tutorial room. It would be essential to control both access to the tutorial and the environment to which it is broadcast to maintain confidentiality.
Limitations
Our study design has a number of limitations. It is non-comparative, and thus we are unable to draw conclusions regarding the relative learning experience or efficacy associated with tutorials delivered via the HoloLens device and the more traditional in-person bedside tutorials. Additionally, the different assessment methods between the MCQs and end of year examinations make direct measurement of knowledge retention difficult. The number of patients involved in the study was relatively small, and thus interpretation of both quantitative and qualitative data must be viewed in this context, and the generalisability of the data is low. The feedback from the tutor and tutorial facilitator must be viewed in the context that they were study investigators.
There are a number of limitations specific to research involving the HoloLens. Common limitations in studying the learning effects of the HoloLens in tested roles include the absence of validated measures and comprehensive evaluation instruments. Unlike other technologies, there are no benchmarks, datasets, or standard standardized protocols to specifically evaluate augmented reality systems, experiences, and methodologies [ 48 , 49 , 50 ]. Although the viewpoint offered to the students by the HoloLens allows the students to appreciate what the tutor is demonstrating, one drawback to this is that the focus of attention is primarily controlled by the tutor, and thus it is difficult for the tutorial to challenge the students to select the relevant areas to attend to. Depending on the tutorial topic and structure, an ideal virtual format may provide three perspectives: the tutors view, a third person view of the clinical encounter, and where applicable, an instrument’s view.
Regarding the generalisability of our study to other tutorial topics, the appreciation of clinical signs which would require palpation or auscultation would be beyond the current capabilities of the HoloLens 2 and therefore, careful tutorial design and topic selection is necessary.
Our results demonstrate the feasibility of facilitating remote bedside tutorials on preoperative anaesthetic assessment using the HoloLens 2. The tutorial structure was found to be agreeable to students, patients, and tutors. Provision of tutorials in the format described in this study may be an option for situations where students’ access to live bedside tutorials are limited. However, further research is required to characterise the role, potential and limitations of incorporating Mixed Reality into clinical medical education in a broader context. Poor audio-visual quality and lack of hands-on practice were found to be the most frequent issues identified in our study and may be significant limitations to the use of this technology in wider medical education. There are significant costs involved in developing the infrastructure and expertise necessary to provide tutorials in this format. Prior to this technology being adopted by educational institutions, we recommend the completion studies to compare the learning efficacy of MR facilitated remote tutorials and traditional in-person bedside tutorials.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- Augmented Reality
Evaluation of Technology-Enhanced Learning Materials: Learner Perceptions
Head-Mounted Display
Interquartile Range
Multiple Choice Question
- Mixed Reality
Objective Structured Clinical Examination
Standard Deviation
Keifenheim KE, Teufel M, Ip J, Speiser N, Leehr EJ, Zipfel S, et al. Teaching history taking to medical students: a systematic review. BMC Med Educ. 2015;15(1):159.
Article Google Scholar
Wessely S. Making doctors: an institutional apprenticeship. BMJ. 1998;316(7132):713.
Dornan T, Tan N, Boshuizen H, Gick R, Isba R, Mann K, et al. How and what do medical students learn in clerkships? Experience based learning (ExBL). Adv Health Sci Educ Theory Pract. 2014;19(5):721–49.
Stone MJ. The wisdom of sir William Osler. Am J Cardiol. 1995;75(4):269–76.
Walsh K. E-learning in medical education: the potential environmental impact. Educ Prim Care. 2018;29(2):104–6.
Sherpa JR, Donahue L, Tsai J, Nguemeni Tiako MJ. The planetary benefit of suspending USMLE step 2 CS: estimating carbon emissions associated with US medical Students' travel to testing centers. Yale J Biol Med. 2023;96(2):185–8.
Sharma D, Rizzo J, Nong Y, et al. Virtual Learning Decreases the Carbon Footprint of Medical Education. Dermatol Ther (Heidelb). 2024;14(4):853–9. https://doi.org/10.1007/s13555-024-01120-4 .
Medical Schools Council. The expansion of medical student numbers in the United Kingdom. London: MSC; 2021. Available at https://www.medschools.ac.uk/media/2899/the-expansion-of-medical-student-numbers-in-the-unitedkingdom-msc-position-paper-october-2021.pdf . Accessed April 2024.
Harries AJ, Lee C, Jones L, Rodriguez RM, Davis JA, Boysen-Osborn M, et al. Effects of the COVID-19 pandemic on medical students: a multicenter quantitative study. BMC Med Educ. 2021;21(1):14.
Choi B, Jegatheeswaran L, Minocha A, Alhilani M, Nakhoul M, Mutengesa E. The impact of the COVID-19 pandemic on final year medical students in the United Kingdom: a national survey. BMC Med Educ. 2020;20(1):206.
Bandura A. Social learning theory. Oxford: Prentice-Hall; 1977.
Irby DM. Clinical teaching and the clinical teacher. J Med Educ. 1986;61(9 Pt 2):35–45.
Google Scholar
Horsburgh J, Ippolito K. A skill to be worked at: using social learning theory to explore the process of learning from role models in clinical settings. BMC Med Educ. 2018;18(1):156.
Park J, Woodrow SI, Reznick RK, Beales J, MacRae HM. Observation, reflection, and reinforcement: surgery faculty members' and residents' perceptions of how they learned professionalism. Acad Med. 2010;85(1):134–9.
Dennick R. Constructivism: reflections on twenty five years teaching the constructivist approach in medical education. Int J Med Educ. 2016;7:200–5.
Steffe LP, Gale J, editors. Constructivism in education. 1st ed. New York: Routledge; 1995.
Kulasegaram KM, Martimianakis MA, Mylopoulos M, Whitehead CR, Woods NN. Cognition before curriculum: rethinking the integration of basic science and clinical learning. Acad Med. 2013;88(10):1578–85.
Wijnen-Meijer M, van den Broek S, Koens F, ten Cate O. Vertical integration in medical education: the broader perspective. BMC Med Educ. 2020;20(1):509.
Brauer DG, Ferguson KJ. The integrated curriculum in medical education: AMEE guide no. 96. Medical Teacher. 2015;37(4):312–22.
Azuma RT. A survey of augmented reality. Presence: teleoperat virt environ. 1997;6(4):355–85.
Hu HZ, Feng XB, Shao ZW, Xie M, Xu S, Wu XH, et al. Application and Prospect of mixed reality Technology in Medical Field. Curr Med Sci. 2019;39(1):1–6.
Garzón J, Pavón J, Baldiris S. Systematic review and meta-analysis of augmented reality in educational settings. Virt Real. 2019;23(4):447–59.
Hantono BS, Nugroho LE, Santosa PI, editors. Meta-Review of Augmented Reality in Education. 2018 10th International Conference on Information Technology and Electrical Engineering (ICITEE); 2018 24–26 July 2018.
Hanna MG, Ahmed I, Nine J, Prajapati S, Pantanowitz L. Augmented Reality Technology Using Microsoft HoloLens in Anatomic Pathology. Arch Pathol Lab Med. 2018;142(5):638-644. https://doi.org/10.5858/arpa.2017-0189-OA .
Eckert M, Volmerg JS, Friedrich CM. Augmented reality in medicine: systematic and bibliographic review. JMIR Mhealth Uhealth. 2019;7(4):e10967.
Mill T, Parikh S, Allen A, Dart G, Lee D, Richardson C, et al. Live streaming ward rounds using wearable technology to teach medical students: a pilot study. BMJ Simul Technol Enhanc Learn. 2021;7(6):494–500.
Lia H, Paulin G, Yi N, Haq H, Emmanuel S, Ludig K, Keri Z, Lasso A, Yeo C, Andrews J, Fichtinger G. HoloLens in suturing training. Proc. SPIE 10576, Medical Imaging 2018: Image-Guided Procedures, Robotic Interventions, and Modeling, 2018;1057628. https://doi.org/10.1117/12.2293934 .
Carmigniani J, Furht B, Anisetti M, Ceravolo P, Damiani E, Ivkovic M. Augmented reality technologies, systems and applications. Multimed Tools Appl. 2011;51(1):341–77.
Silvero Isidre A, Friederichs H, Müther M, Gallus M, Stummer W, Holling M. Mixed reality as a teaching tool for medical students in neurosurgery. Med Int. 2023;59(10)
Kolecki R, Pręgowska A, Dąbrowa J, Skuciński J, Pulanecki T, Walecki P, et al. Assessment of the utility of mixed reality in medical education. Translat Res Anatom. 2022;28:100214.
Robinson BL, Mitchell TR, Brenseke BM. Evaluating the use of mixed reality to teach gross and microscopic respiratory anatomy. Med Sci Educ. 2020;30(4):1745–8.
Maniam P, Schnell P, Dan L, Portelli R, Erolin C, Mountain R, et al. Exploration of temporal bone anatomy using mixed reality (HoloLens): development of a mixed reality anatomy teaching resource prototype. J Vis Commun Med. 2020;43(1):17–26.
Kumar N, Pandey S, Rahman E. A novel three-dimensional interactive virtual face to facilitate facial anatomy teaching using Microsoft HoloLens. Aesth Plast Surg. 2021;45(3):1005–11.
Cipresso P, Giglioli IAC, Raya MA, Riva G. The Past, Present, and Future of Virtual and Augmented Reality Research: A Network and Cluster Analysis of the Literature. Front Psychol. 2018;9:2086. https://doi.org/10.3389/fpsyg.2018.02086 .
Quarles J, Lampotang S, Fischler I, Fishwick P, Lok B. Scaffolded learning with mixed reality. Comput Graph. 2009;33(1):34–46.
Palumbo A. Microsoft HoloLens 2 in medical and healthcare context: state of the art and future prospects. Sensors (Basel). 2022;22(20)
University College Cork. Book of Modules 2023. [Internet]. Cork. Cited March 2024. Available from: https://ucc-ie-public.courseleaf.com/modules /.
University College Cork School of Medicine. Medicine (Graduate Entry) (MB, BCh, BAO Degrees) - CK791 Programme Requirements 2023. [Internet]. Cork. Cited March 2024. Available from: https://ucc-iepublic.courseleaf.com/programmes/bmbbg/#programmerequirementstext .
University College Cork School of Medicine. Medicine (MB, BCh, BAO Degrees) - CK701 Programme Requirements 2023. Internet. CorkCited March 2024. Available from: https://ucc-ie-public.courseleaf.com/programmes/bmbb/#programmerequirementstext .
Microsoft Corporation. HoloLens Tips 2023. Internet. [Internet]. Cited March 2024. Available from: https://www.microsoft.com/en-us/p/hololens-tips/9pd4cxkklc47?activetab=pivot:overviewtab .
Microsoft Corporation. Infrastructure Guidelines for HoloLens. Microsoft Learn. [Internet]. Cited October 2022. Available from: https://learn.microsoft.com/en-us/hololens/hololens-commercial-infrastructure .
Cook DA, Ellaway RH. Evaluating technology-enhanced learning: A comprehensive framework. Med Teach. 2015;37(10):961–70.
Thompson Burdine J, Thorne S, Sandhu G. Interpretive description: A flexible qualitative methodology for medical education research. Med Educ. 2021;55(3):336–43.
Clarke V, Braun V. Teaching thematic analysis: overcoming challenges and developing strategies for effective learning. Psychol. 2013;26:120–3.
Lingard L. Beyond the default colon: effective use of quotes in qualitative research. Perspect Med Educ. 2019;8(6):360–4.
Tang YM, Chau KY, Kwok APK, Zhu T, Ma X. A systematic review of immersive technology applications for medical practice and education - trends, application areas, recipients, teaching contents, evaluation methods, and performance. Educ Res Rev. 2022;35:100429.
Pennell CE, Kluckow H, Chen SQ, Wisely KM, Walker BL. Live-streamed ward rounds: a tool for clinical teaching during the COVID-19 pandemic. Med J Aust. 2020;213(7):306–8.e1.
Herron J. Augmented reality in medical education and training. J Electron Resour Med Libr. 2016;13:1–5.
Gerup J, Soerensen CB, Dieckmann P. Augmented reality and mixed reality for healthcare education beyond surgery: an integrative review. Int J Med Educ. 2020;11:1–18.
Barsom EZ, Graafland M, Schijven MP. Systematic review on the effectiveness of augmented reality applications in medical training. Surg Endosc. 2016;30(10):4174–83.
Download references
Acknowledgements
The authors would like to acknowledge the assistance from members of the UCC College of Medicine and Health, including Dr. Colm O’Tuathaigh, Dr. Gabriella Rizzo, Dr. Pat Henn and Professor Paula O’Leary, as well as Ms. Michelle Donovan in the UCC Centre for Digital Education.
This study received funding and research support through the UCC Learning Analytics LITE programme, which is funded through the Strategic Alignment of Teaching and Learning Enhancement fund. The UCC Learning Analytics LITE programme provided logistical and research support in study design and funds were used to hire assistance in data interpretation.
This study also received funding from the UCC College of Medicine and Health which was utilised to purchase the HoloLens 2 Device and associated licences.
Author information
Authors and affiliations.
Cork University Hospital and University College Cork, Cork, Ireland
Murray Connolly, Gabriella Iohom, Corina Soare & George Shorten
University College Cork, Cork, Ireland
Niall O’Brien & James Volz
Cork University Hospital, Cork, Ireland
Aogán O’Muircheartaigh, Paschalitsa Serchan, Agatha Biculescu, Kedar Govind Gadre & Laura Griseto
You can also search for this author in PubMed Google Scholar
Contributions
MC lead the design of the study, carried out the tutorials, analysed both quantitative and qualitative data and was the primary author of the manuscript. GI contributed to the design of the study, the student examinations contributed to writing the manuscript. NOB contributed to the technical and logistical design of the study and acted as technical facilitator for the tutorials and contributed to manuscript composition. JV designed, completed and analysed the semi-structured student interviews and contributed to manuscript composition. AOM, PS, AB, LG and supervised and analysed student examination data. KGG analysed student demographic data and student examination data. CS contributed to initial evaluation of the HoloLens device and tutorial design. GS played a central role in study design and completion and was a major contributor in manuscript composition.
Corresponding author
Correspondence to Murray Connolly .
Ethics declarations
Ethics approval and consent to participate.
This study was approved by the Clinical Research Ethic Committee of the Cork Teaching Hospitals, and the University College Cork Research and Postgraduate Affairs Committee. All methods were carried out in accordance with guidelines and regulations as set out by the ethics and research committees. All participants provided informed consent to participate in the study.
Consent for publication
All participants including students, patients, tutor and technical facilitator provided written informed consent prior to inclusion in the study. Participants who’s identifiable images are included provided informed consent for publication of identifiable information/ images in an open access journal.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1., additional file 2., additional file 3., additional file 4., additional file 5., rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Connolly, M., Iohom, G., O’Brien, N. et al. Delivering clinical tutorials to medical students using the Microsoft HoloLens 2: A mixed-methods evaluation. BMC Med Educ 24 , 498 (2024). https://doi.org/10.1186/s12909-024-05475-2
Download citation
Received : 09 March 2023
Accepted : 26 April 2024
Published : 04 May 2024
DOI : https://doi.org/10.1186/s12909-024-05475-2
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Medical Education
BMC Medical Education
ISSN: 1472-6920
- Submission enquiries: [email protected]
- General enquiries: [email protected]
- Open access
- Published: 01 May 2024
Health system lessons from the global fund-supported procurement and supply chain investments in Zimbabwe: a mixed methods study
- Abaleng Lesego 1 ,
- Lawrence P. O. Were 1 , 2 ,
- Tsion Tsegaye 1 ,
- Rafiu Idris 3 ,
- Linden Morrison 3 ,
- Tatjana Peterson 3 ,
- Sheza Elhussein 3 ,
- Esther Antonio 4 ,
- Godfrey Magwindiri 4 ,
- Ivan Dumba 5 ,
- Cleyland Mtambirwa 5 ,
- Newman Madzikwa 5 ,
- Raiva Simbi 5 ,
- Misheck Ndlovu 6 &
- Tom Achoki 1
BMC Health Services Research volume 24 , Article number: 557 ( 2024 ) Cite this article
146 Accesses
Metrics details
The Global Fund partnered with the Zimbabwean government to provide end-to-end support to strengthen the procurement and supply chain within the health system. This was accomplished through a series of strategic investments that included infrastructure and fleet improvement, training of personnel, modern equipment acquisition and warehouse optimisation. This assessment sought to determine the effects of the project on the health system.
This study employed a mixed methods design combining quantitative and qualitative research methods. The quantitative part entailed a descriptive analysis of procurement and supply chain data from the Zimbabwe healthcare system covering 2018 – 2021. The qualitative part comprised key informant interviews using a structured interview guide. Informants included health system stakeholders privy to the Global Fund-supported initiatives in Zimbabwe. The data collected through the interviews were transcribed in full and subjected to thematic content analysis.
Approximately 90% of public health facilities were covered by the procurement and distribution system. Timeliness of order fulfillment (within 90 days) at the facility level improved from an average of 42% to over 90% within the 4-year implementation period. Stockout rates for HIV drugs and test kits declined by 14% and 49% respectively. Population coverage for HIV treatment for both adults and children remained consistently high despite the increasing prevalence of people living with HIV. The value of expired commodities was reduced by 93% over the 4-year period.
Majority of the system stakeholders interviewed agreed that support from Global Fund was instrumental in improving the country's procurement and supply chain capacity. Key areas include improved infrastructure and equipment, data and information systems, health workforce and financing. Many of the participants also cited the Global Fund-supported warehouse optimization as critical to improving inventory management practices.
It is imperative for governments and donors keen to strengthen health systems to pay close attention to the procurement and distribution of medicines and health commodities. There is need to collaborate through joint planning and implementation to optimize the available resources. Organizational autonomy and sharing of best practices in management while strengthening accountability systems are fundamentally important in the efforts to build institutional capacity.
Peer Review reports
The Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund), together with its Zimbabwean national and international stakeholders have continued to invest in health system strengthening to improve public health in the country. These investments have been guided by systemwide strategic assessments to understand the fundamental challenges facing the Zimbabwean health system [ 1 , 2 , 3 , 4 ].
Given the strategic importance of access to essential medicines, vaccines, and other health technologies as a strategic pillar of any health system [ 4 , 5 ], the Global Fund supported the Ministry of Health and Child Care (MOHCC) through the United Nations Development Program (UNDP) to undertake a comprehensive assessment of the national procurement and supply chain management (PSCM) system in 2013 [ 6 ]. This assessment aimed to develop a strategic vision and costed action plan for improvement. This covered both upstream and downstream aspects of PSCM. The strategic purpose was to help the MOHCC launch a coordinated approach to invest in PSCM improvements and enhance coordination and cooperation in managing all health commodities across the health system [ 3 , 6 , 7 ].
Subsequently, the Global Fund supported several initiatives aimed at the realization of the improvements proposed by the comprehensive assessment undertaken by UNDP [ 6 ]. These initiatives primarily encompassed end-to-end supply chain assistance in critical areas, including demand quantification and forecasting, warehousing capacity development, fleet improvement, distribution systems, and waste management systems. Other support aspects focused on warehouse optimization, data and information management systems, and personnel training [ 7 , 8 ]. In general, warehouse optimization is the process of improving the efficiency and effectiveness of warehouse operations. It involved refining workflows, leveraging technology, enhancing spatial utilization, and ensuring precise inventory management [ 6 , 7 ].
More specifically, the Global Fund provided funds for the construction of warehouses for the National Pharmaceutical Company of Zimbabwe (NATPHARM) to facilitate the smooth handling of health commodities. Additionally, this support extended to water supplies (in terms of sinking boreholes) for various warehouses, water tanks, and booster pumps for the other branches. Global Fund also supported NATPHARM in constructing two incinerators in the two main cities, Harare, and Bulawayo to handle pharmaceutical waste effectively [ 9 , 10 ].
Through Global Fund support, NATPHARM also received modern warehouse equipment such as forklifts, pallet jacks and rolling ladders, and data and information management system support for better visibility and effective handling of health commodities. The support further extended to optimising the Harare branch warehouse with modern receiving and transit capabilities to serve other feeder locations and the procurement of modern delivery trucks to facilitate the distribution of commodities. Global Fund support also extended to personnel training and retention for the effective functioning of NATPHARM and the broader procurement and supply system [ 3 , 6 , 9 ].
Focusing on quality assurance and safety of medicines and other health commodities, Global Fund supported the Medicines Control Authority of Zimbabwe (MCAZ) to develop capacity in quality testing of all commodities procured through grants. MCAZ was also supported with the installation of solar panels that allowed for an uninterrupted power supply to facilitate smooth operations at the organization. The Global Fund support was also critical in the upgrading of the biology and chemistry laboratories to attain WHO prequalification standards [ 8 , 9 , 11 ]. Similarly, there was direct support from the Global Fund to facilitate pharmacovigilance activities, such as adverse drug reactions reporting using electronic systems. All these measures were meant to ensure that the medicines and health commodities consumed in the Zimbabwean health system were safe and quality-assured [ 4 , 5 , 9 , 11 ].
The overarching project by the Global Fund to support the Zimbabwean government was designed and implemented in response to the nationally identified gaps and opportunities that were established through various research and consultative efforts [ 3 , 4 , 6 , 8 ]. The project was kickstarted in the first quarter of 2019 and continued through 2021, with various project components being implemented in a phased approach to achieve the national targets [ 3 , 4 , 7 , 10 , 11 ]. To ensure effective coordination, accountability, and avoidance of duplicative efforts, the project was designed and implemented in close coordination with other partners represented in the National Health Development Partners Coordination Forum (HDPCF), Health Sector Technical Working Group (HSTWG), and the Global Fund Country Coordination Mechanism (CCM), among others [ 3 , 4 , 6 , 8 , 10 ]. There was regular reporting to the respective coordination mechanisms to track progress as well as troubleshoot any implementation issues as they arose [ 6 , 9 ].
Overall, the gaps identified through the various assessments commissioned by the Global Fund included a lack of effective coordination, poor inventory and order management, human resource constraints, and warehousing and storage inefficiencies [ 12 , 13 ]. Therefore, the focus of the Global Fund support was to retool the Zimbabwean PSCM system to be efficient, cost-effective and responsive to the population's health needs, particularly in the face of global epidemics and pandemics such as HIV/AIDS and COVID-19 [ 14 , 15 , 16 , 17 , 18 ].
In an attempt to resolve these issues, healthcare systems around the world are working on streamlining their supply chains through various health system strengthening measures [ 19 , 20 , 21 , 22 ]. Therefore, the objective of this analysis was to assess the overall effects of the Global Fund-supported investments in the Zimbabwean PSCM system and document the lessons learned to inform future programming efforts to strengthen healthcare systems.
The assessment covered a period of 2018 -2021 and employed both qualitative and quantitative research methods. Figure 1 . illustrates the convergent mixed methods study design that was applied. In this study design, both the qualitative and quantitative data collection and analyses are implemented simultaneously, and the insights merged to provide a fuller picture [ 23 ].

Convergent mixed methods design
The quantitative part of the study entailed collecting and analysing administrative data covering priority indicators that are routinely reported on the Zimbabwe PSCM. Meanwhile, the qualitative part comprised of key informant interviews (KII) focusing on stakeholders within the healthcare system to give perspective to the observed data trends. Insight from the two parts of the analysis were merged and subjected to comparative assessment and interpretation to ensure that a consistent picture emerged [ 23 , 24 ]. More details on the methods are provided in later sections.
Analytical framework
The overall analytical approach espoused in this assessment was anchored on the logical relationships of the building blocks of the health system as described by the World Health Organization (WHO) health system framework [ 5 ]. Figure 2 shows the analytical framework, which illustrates the results chain cascading from the Global Fund-supported initiatives to the expected improvements in intermediate and long-term outcomes related to PSCM, including the availability of medicines, reduced wastage, and overall improvements in population-level coverage [ 4 , 5 ].

Analytic framework
Overall, the framework graphically displays the results Global Fund intended to achieve through its support to the Zimbabwean PSCM. The "theory of change" that underlies the Global Fund’s strategy is revealed through the arrows in the diagram that identify “causal” linkages through which various intermediate results interact to make progress toward the overall goal of improving health system performance [ 3 , 5 ].
Quantitative research
The quantitative research entailed a detailed descriptive analysis of the operational data that was routinely reported across the Zimbabwe PSCM system. Table 1 . shows some of the key performance indicators (KPI) that were considered in our analysis.
Data collection, management and analysis
The data used in this analysis were obtained from the routinely reported operational data that included the NATPHARM-operated warehouses and healthcare facilities in the country. The data were extracted from the various data management systems operated by the different institutions, cleaned, and collated into a comprehensive dataset in the form of a spreadsheet covering the period of the assessment. The database was examined for completeness and accuracy by cross-referencing the corresponding progress reports for specific periods. Trends of priority indicators were compared over time, as they related to Global Fund support to the PSCM space.
Qualitative research
The qualitative assessment entailed KIIs with health system stakeholders who were knowledgeable and intimately involved in the Global Fund-supported initiatives and its intended beneficiaries. This included provincial and district management teams, hospital and clinic personnel, and other stakeholders in the Zimbabwe health system. Informed consent was obtained from each study participant involved in the study. The data collection protocol ensured that all study participants fully understood the objectives of the study and consented verbally to provide the required information.
As previously stated, the literature review helped map and identify critical organisations involved in the PSCM space, and more specifically, those involved in the procurement and health system strengthening activities supported by the Global Fund. A full list of those organisations is provided on Table 2 .
Sampling techniques
Convenience purposive sampling was used to select key informants and in-depth interviews [ 23 ]. Our sample was supplemented using snowball sampling methods (also called chain sampling). The initial respondents referred other potential respondents until no new information was forthcoming or achieved saturation. Efforts were made to be all-inclusive, involving various stakeholder groups and organisations intimately linked to the operations of the Zimbabwe PSCM landscape.
This comprised of KIIs using a structured interview guide that covered various thematic areas relevant to the assessment to obtain a comprehensive perspective of the impact of the Global Fund-supported initiatives in the country. In its development, testing and validation, the key informant guide was pretested and adapted to ensure suitability for the task. In view of the restrictions imposed to prevent the spread of COVID-19 infections at the time of the study, some KIIs were conducted online using multimedia channels such as Zoom, Skype, and telephonically.
Three research assistants supported the two project leaders in conducting the KIIs. After each interview, all notes taken by the research assistant were checked by the two project leaders to ensure completeness and readability to minimise recording errors. In addition, a tape recorder was used for interviews to assist with reference post data collection. All the recordings were stored in a pin-protected cloud storage which was only accessible by the two project evaluation leaders. Qualitative data obtained from the KIIs were transcribed in full and then manually analysed applying thematic content analysis. Where there was a divergence of opinion, an agreement was established through discussion with three members of the project evaluation team. In thematic analysis, data from interview transcripts were grouped into similar concepts. This approach was appropriate for semi-structured expert interviews as it is used to code text with a predefined coding system that can then be refined and completed with new themes emerging [ 23 , 24 ]. Our initial coding system was defined during the desk review stage and continuously updated in the successive phases of data collection employing a deductive approach of qualitative research. The emerging themes were not preconceived (desk review) but emerged from the data during the coding process, while the global themes were the highest-order themes that emerged from the data and were broad enough to capture the essence of the entire dataset [ 23 ]. The codes are presented in a tabular format in the results section below.
This section presents both the quantitative and qualitative research results from the study. The quantitative results comprise of trends of the priority operational PSCM indicators for the relevant period. The qualitative results present the perspectives of the key health stakeholders involved in the Zimbabwe healthcare system.
Quantitative results
Table 3 shows that the total warehouse capacity across the Zimbabwean health system increased by 37.8% between 2018 and 2021.
Of the 1500 public health facilities in Zimbabwe coverage by the PSCM system was consistently high between the years 2018 and 2021, averaging 94%, and increasing by 13.6% over the same period. However, order fulfillment rate within 90 days, for 1410 reporting health facilities was consistently below 50% from 2018 to 2020, despite the reported high coverage for the health facilities by the PSCM in the country. Notably, this indicator showed remarkable improvement to 91% in 2021, from an average of 42% from the previous three years. More specifically, the order fill rate for Tenofovir 300mg/ lamivudine 300mg/efavirenz 600mg (TLE 600mg) improved despite the significant drop observed in 2020. However, when comparing 2018 and 2021, the order fill rate for this specific HIV drug increased by around 36.5%, while the stockout rates for the same drug at the central stores declined by about 14.5% over the same period.
Table 3 further shows a 44% drop of order fill rates for the Determine HIV Test Kit between 2018 and 2020 for the 1410 reporting health facilities, only to recover in the year 2021, where order fill rates improved to 83%. At the same time, the stockout rates for the Determine HIV Test Kit at the central stores declined by 49% between 2018 and 2021.
Figure 3 shows the estimated average population coverage for HIV treatment for adults and children, from 2018 to 2020, at 92% and 71%, respectively. The figure shows that there was limited variation in the population level coverage over the years, despite the estimated increase in the number of people living with HIV over the same period. The national target for this indicator is 95%.

Adult and paediatric HIV treatment population coverage
Figure 4 shows the proportion of the value of the expired stock in the 7 warehouses, over three years, between 2019 and 2021, which demonstrates a declining trend over time. The highest expiry was in quarter 4 2019 at 1.9%, compared with the lowest in quarter 3 2021 at 0.1%. This represents a 93% reduction in value of expired stock.

Percentage value of expired stock
Figure 5 shows the combined stock-taking variance valued in United States Dollar terms across 7 warehouses over a three-year period. The stock variance shows a declining trend over the three-year period to negligible values at the end of 2021.

Stock-taking variance
Figure 6 shows the temporal trend of the number of days that it took NATPHARM to resolve the stock variances across the different warehouses in the country. Overall, there is a decline from the average of 8 days from the December 2018 stocktake (with Harare warehouse as an outliner at 25 days), to an average of 1 day in the December 2021 stocktake, where all warehouses converge.

Duration to resolve stock variance
Table 4 shows the funding levels in USD$ to support the diagnostic capacity for Covid-19, comprising of the polymerase chain reaction test (PCR) and rapid diagnostic tests (RDT). The table further shows the PSCM related costs, the total test done, and positive cases identified over the two-year period. The total funding between 2020 and 2021 increased by 290%, with testing levels increasing by 490% over the same period. The average Covid-19 positivity rate in 2020 was 6.4% while the positivity rate for 2021, was 3.1%, indicating a greater than 50% drop.
Qualitative results
Most of the participants interviewed acknowledged that the Global Fund support to NATPHARM and the broader Zimbabwean health system had been central in improving the overall performance of the health system through improved availability of essential medicines and other health commodities. This was largely achieved by ramping up the various components of the PSCM value chain and related operations, leading to efficiency, effectiveness and reliability.
Table 5 shows the codes, emerging and global themes from the thematic content analysis. The emerging themes revolved around the lack of infrastructure and equipment curtailing warehouse operations before the Global Fund support. Data gaps and poor product visibility were also emerging themes, as were the effects of the old fleet on the overall supply and distribution system. Similarly, issues of infrastructure, capacity, and personnel training gaps emerged as crucial themes hindering quality assurance within the PSCM. Global themes also largely focused on infrastructural inadequacy leading to underperformance. Improvements leading to better handling of commodities; data and information systems, enhancing visibility and supporting accuracy in forecasts; improvements in the distribution systems enabled by newer fleets also featured as global themes. Similarly, better trained and motivated personnel, able to perform critical functions; capacity to ensure the quality and safety of medicines and other health commodities; and the need for effective multistakeholder partnerships to improve effectiveness and sustainability of health systems, were key themes.
NATPHARM operations
According to the NATPHARM management, warehouse improvement and optimisation exercise resulted in better visibility and improved efficiency in the operations related to the commodity handling across the entire value chain. More specifically, the processes related to stock taking improved markedly over time according to the reports presented by various organizations that had been commissioned to undertake the stock audits.
“ …. warehouse optimisation supported implementing an inventory management system which conformed with bin location and variant codes, according to different donors. The result was improved, faster and more accurate stock takes, a sharp reduction of variances and more streamlined order processing ” Participant, NATPHARM.
Further, it was reported by various participants that order processing and deliveries had improved to be timely and on schedule as a result of the improved visibility and efficiency harnessed across the PSCM. Similarly, there was consensus that receiving processes and documentation had significantly improved through the support offered by Global Fund particularly towards warehouse optimization. The improvements in the data management systems and related trainings were also cited as contributory to the overall trend that was observed.
“ Reporting quality has greatly improved and is now timely, accurate and complete. This helps in accurate forecasting of demand, which in turn avoids unnecessary wastage and expiries” Participant MOHCC.
There was consensus from the majority of participants interviewed that the fleet improvements had improved the availability of essential commodities vital for the effective management of high burden diseases; HIV/AIDS, Malaria and Tuberculosis in Zimbabwe. According to participants from a local health facility, this was evidenced by low stockout rates for the key commodities needed to manage these three conditions effectively. The new fleet was reported to facilitate deliveries from various warehouses to the recipient health facilities on a regular basis. This level of distributional access coupled with better demand forecasting as a result of improved data use, was noted as critical in the improved availability of medicines and health commodities at the health facility levels.
Further, respondents in the leadership of NATPHARM revealed that the Global Fund support had benefited the overall financial position of the organisation by tapping into efficiencies harnessed through the various measures that have been implemented. Some of the support measures that resulted in efficiency improvements include, the warehouse optimization, pharmaceutical waste management and fleet improvements, which ultimately reduced operational costs.
For example, it was noted that running a newer fleet of vehicles led to lower maintenance and fuelling costs than previously was the case, when deliveries were done using older vehicles. Similarly, it was noted that pharmaceutical waste resulting from expired medicines and other health commodities was expensive to store and dispose, particularly when engaging third party organizations. However, this additional cost was reportedly in the decline, as a result of the investment in the incinerators for waste management.
“ The provision of incinerators for waste management has resulted in huge savings in terms of the cost of waste destruction. It has also resulted in significant compliance with environmental health regulations.”, Participant, NATPHARM.
MCAZ operations
Majority of the participants agreed that the Global Fund support to MCAZ strengthened its overall capacity to handle the requisite safety and quality assurance needs to effectively support the procurement functions for medicines and other health commodities within the country and regionally. The installation of solar panels to provide uninterrupted electricity power supply for the operations of the organization was cited as a huge advantage allowing for improved performance, in a country where power supply is unreliable. Similarly, other participants cited, the support for MCAZ laboratories to obtain the WHO prequalification status, as a major step towards effectiveness and sustainability for the organization; citing the fact that MCAZ is offering quality assurance services regionally at a fee.
“ We [MCAZ] now have the capacity to conduct the safety and quality assurance tests needed to support the procurement of commodities in the country and the region. We [MCAZ] even recently won the tender to support the regional procurement activities ”, Participant, MCAZ.
Based on the results framework provided in Fig. 3 , there is clear evidence that the Global Fund-supported initiatives resulted in positive improvements in the overall performance of the Zimbabwean PSCM system. However, it is important to recognise some of the assessment’s limitations in interpreting these findings. First, the results reported are for a limited observation period and a limited set of indicators, which are largely confined to the national level analysis, missing out on granular subnational and commodity-specific analysis that could be more informative. Secondly, this study was not conceptualised before the onset of the intervention reported here (i.e., Global Fund-supported initiatives), and therefore, no specific steps were taken to develop an appropriate prospective research design and data collection strategy to support a more rigorous assessment. Therefore, the study relied on secondary PSCM data that were sparse and covered a limited period. Third, the study could be subject to confounding relationships with other concurrent interventions being implemented by other health system stakeholders that have direct or indirect effects on the PSCM system, complicating impact attribution to specific interventions. Forth, the analysis focused only on a narrow subset of medicines and commodities related to HIV/AIDS and COVID-19. However, despite these limitations, every effort has been made to use the most up-to-date and complete information available, including validation using official reports and collaborative reported data with key informant interviews.
The estimated population coverage for HIV treatment for both adults and children remained consistently high despite the increasing prevalence in the country. It was estimated that adults living with HIV increased by 10% from a baseline of 2018, to reach 1.3M in 2020, while children living with HIV increased by 24%, from a baseline of 2018, to reach 75 000 in 2020 [ 3 , 4 , 9 ]. As a key last mile population outcome, it can be rightly assumed that high HIV treatment coverage in the Zimbabwean system emanated from strengthened inventory management functionality and improved delivery of orders supported by a modern fleet of vehicles, which allowed for meeting the supply target of four quarterly rounds [ 3 , 8 ]. Population coverage is an important performance measure for a health system. It unites two important concepts; need and utilisation of an intervention to improve health [ 25 ]. In our case, the intervention is HIV treatment and the population in need is those living with HIV needing treatment; and the proportion with access and able to use the treatment they need, represents population coverage. This is a fundamentally important consideration as various health systems, including low- and middle-income countries, are making universal health coverage (UHC) efforts. There is no question, that improved access to essential medicines and other health technologies is a fundamental cornerstone towards UHC [ 1 , 5 , 26 ].
Other intermediate indicators that are critical for progress towards improved availability of medicines and other health commodities and hence UHC, also showed significant improvements that could be attributed to Global Fund-supported initiatives. For example, reduced wastage and decreasing value of expired health commodities reported, point towards improving efficiency across the value chain. As noted earlier, efficiency is one of the fundamental expectations of an effective health system outlined in the WHO health system framework [ 3 , 5 ]. The diminishing value of expiries could be ascribed to various factors, including the improved workflow processes and data accuracy at NATPHARM. This improvement which is associated with better visibility of commodities across the value chain could be attributed to investments made by Global Fund such as the enterprise resource planning platform, coupled with concomitant training and supervision.
Through Global Fund’s assistance to NATPHARM, automation of tasks such as stock management, ordering, and other operational activities was central and contributory to driving the observed improvements in the handling of commodities; reduction of wastage and expiries and improving availability. Similarly, better inventory management and warehouse optimization activities such as decongestion resulted in quicker, timely, more accurate, and well-documented stock takes, improving overall commodity management.
Variances between stock on hand and physical counts were used to determine whether facilities are conducting period checks on their stocks and therefore calculating monthly consumption of commodities accurately. As such the variance across commodities should be zero. Low variance indicates that the stocks at hand are generally similar and do not vary widely from the physical stock counts, while high variance indicates that the respective values have greater variability and are more widely dispersed from one another. There is clear evidence pointing towards the reduction in stock variances when comparing stock on hand and physical counts across the different warehouses in the country over time. This trend can be attributed to better visibility of commodities at the warehouses and training of personnel which was supported by the Global Fund [ 2 , 9 ]. Similarly, the number of days it took the NATPHARM personnel to resolve stock variances showed a dramatic reduction, from an average of 8 days to 1 day in a span of 3 years. This observed trend could also further support the claim that overall, the Global Fund supported initiatives produced the desired results.
With the advent of Covid-19, the effects of the Global Fund support on the PSCM became evident considering the robust response the country was able to mount particularly in terms of diagnostics [ 9 ]. The country was able to rapidly roll out COVID-19 testing, reaching many people between 2020 and 2021. Similarly, the Covid-19 positivity rates declined from 6.4% to about 3.1% over the same period. High positivity rates may indicate that the health system is only testing the sickest patients who seek medical attention and is not casting a wide enough net to know how much of the virus is spreading within its communities. A low rate of positivity on the other hand, can be seen as a sign that a health system has sufficient testing capacity for the size of the Covid-19 outbreak and is testing enough of its population to make informed decisions about reopening the economy. The WHO guidance is that countries which have conducted extensive testing for COVID-19, should remain at 5% or lower positivity rate for at least 14 days.
Safe pharmaceutical waste management and disposal is a primary consideration of any effective health system in completing the PSCM loop [ 27 ]. The Global Fund supported the investment in MOHCC operated incinerators. These investments could largely be associated with reduction in the cost of storage, handling and disposal of the expired stock, particularly when considering that certain space was rented from third parties which often charged a premium. Safe pharmaceutical waste disposal also became more priority with the increased supplies that resulted from the efforts to tackle the Covid-19 pandemic.
Despite signs of progress, there was temporary faltering of indicators- namely, order fill and stockout rates; associated with key commodities for effective management of HIV in the year 2020, warranting an explanation. The drop in Tenofovir/Lamivudine/Efavirenz (TLE 600mg) in 2020 could be linked to several factors. In the year 2019, the Zimbabwe MOHCC adopted new treatment regimens containing Dolutegravir. This means, newly HIV positive clients were started on Dolutegravir regimen as standard of care rather than the previous first line treatment which then surged Tenofovir/Lamivudine/Dolutegravir 50mg order fill rate, while having the opposite effect on the old regimen. Lastly, the effects of COVID-19 pandemic cannot be underestimated as the global supply chain systems were logged with delays which caused disruptions and inefficiencies in health systems in many countries [ 28 ]. In the same period, Determine HIV Test Kit rebounded from stocking out in central stores because of strengthened warehouse optimization activities, including better inventory management, purposeful stock taking, and approval processes contributed to the lowering of stockout rates.
The Global Fund-supported initiatives were also instrumental in building capacity by training key personnel for the effective implementation of activities related to the procurement and supply chain management function [ 8 , 29 , 30 ]. Better quantification and forecasting capabilities (due to data availability through e-LMIS and personnel training), improved warehousing capacity to hold a wide portfolio of products, and direct delivery to facilities through a modern fleet could have contributed to the high population coverage reported [ 26 , 30 , 31 ]. According to the WHO health system framework, effective leadership is required to coordinate all the functions of the health system in order to achieve the desired outcomes [ 5 ]. Therefore, it is sensible to conclude that, the reported health system improvements could not have happened without effective leadership and well-trained staff tasked with coordination and management across the PSCM value chain. It can be further inferred that the training and capacity development measures offered to the NATPHARM personnel were consequential in supporting the broader health system to meet its overall objectives, including improving PSCM performance [ 2 , 7 , 29 ].
Similarly, adequate infrastructure, equipment, data, and information management systems are crucial ingredients for a well-functioning health system, according to the WHO health system framework [ 4 , 5 , 9 ]. The Global Fund-supported initiatives were central in supporting these aspects of the health system through improved warehousing capacity, of modern equipment, installation of solar panels, fleet improvement and deployment of an electronic-logistic management information system (e-LMIS). The cumulative benefits of these investments include optimised procurement and distribution of commodities leading to a reduction in stockout rates and timely order refills to meet the population health needs [ 9 ].
Based on these findings, it would be reasonable to conclude that the Global Fund-supported initiatives in Zimbabwe contributed positively to strengthening the health system, particularly through the improved performance of the various indicators linked to the PSCM system at national and regional warehouses, as well as health facilities. Considering the prevailing health needs in the country, the implementation of this project and the manner of investments provide a basis and playbook for further support to make progress. This is particularly true considering the various competing priorities in the Zimbabwean healthcare system amidst resource constraints [ 3 , 6 , 8 ]. This was largely underpinned on the overarching focus on UHC and the critical role that an effective PSCM plays towards that very objective [ 3 , 12 , 13 , 14 ].
The Global Fund-supported project in Zimbabwe worked through the existing national coordination mechanisms where various key stakeholders, including MOHCC and NATPHARM, were involved in all key strategic planning and implementation decisions, ensuring country leadership and ownership. It was clear from the outset that this approach required sound partnership, transparency, and accountability among all the involved stakeholders, to deliberate and find common ground, guided by the overarching objective to make progress towards UHC.
The question of securing the gains and ensuring sustainability is fundamental for donor supported health programs in low- and middle- income countries. To make progress, it is imperative for health system stakeholders, including governments and donor organizations that are keen to sustainably strengthen health systems to pay close attention to critical areas like the procurement and distribution of health commodities. It is critical to collaborate with key stakeholders through joint planning and implementation to optimize the available resources. Organizational autonomy coupled with strong data driven accountability systems and the sharing of best management practices are fundamentally important in this discourse.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request and once written permission is obtained from NATPHARM.
Abbreviations
Country Coordination Mechanism
Health Development Partners Coordination Forum
Health Sector Technical Working Group
Key Informant Interview
Medicines Control Authority of Zimbabwe
Ministry of Health and Child Care
National Pharmaceutical Company of Zimbabwe
Polymerase Chain Reaction
Procurement and Supply Chain Management
Rapid Diagnostic Tests
Tenofovir Lamivudine Efavirenz
Universal Health Coverage
United Nations Development Program
World Health Organization
UNDP. Healthy systems for healthy people: UNDP and Global Fund support to strengthen financial and risk management for the delivery of health services in Zimbabwe. New York: United Nations Development Programme; 2020.
UNDP. Healthy systems for healthy people: UNDP and Global Fund support to strengthen the national health management information system. New York: United Nations Development Programme; 2020.
MOHCC. Investment case for the national health strategy 2021-2025. Harare: Accelerating investments towards Universal Health Coverage; 2020.
Google Scholar
MOHCC. National health strategy 2021–2025. Harare: Ministry of Health and Child Care; 2020.
WHO. Everybody business: strengthening health systems to improve health outcomes: WHO’s framework. Geneva: WHO; 2007.
Group EH. Comprehensive assessment of the supply chain for health commodities in the public sector in Zimbabwe. Harare: United Nations Development Programme; 2013.
MOHCC. Analysis and findings from the Zimbabwe supply chain human resource assessment. Harare: Ministry of Health and Child Care; 2012.
UNDP. Healthy systems for healthy people: the impact of UNDP-managed Global Fund investments in procurement and supply chain systems in Zimbabwe. Harare: United Nations Development Programme ; 2020.
Global Fund. Audit report: Global Fund Grants in Zimbabwe. Geneva: The Global Fund; 2020
MOHCC. Zimbabwe electronic logistics management information system baseline assessment report December 2018 to January 2019. Harare: Ministry of Health and Child Care ; 2019.
MOHCC. Zimbabwe comprehensive laboratory assessment. Harare: Ministry of Health and Child Care; 2016.
Privett N, Gonsalvez D. The top ten global health supply chain issues: perspectives from the field. ORHC. 2014;3(4):226–30. https://doi.org/10.1016/j.orhc.2014.09.002 .
Article Google Scholar
Yadav P. Health product supply chains in developing countries: diagnosis of the root causes of underperformance and an agenda for reform. Health Syst Reform. 2015;1(2):142–54. https://doi.org/10.4161/23288604.2014.968005 .
Article PubMed Google Scholar
Seidman G, Atun R. Do changes to supply chains and procurement processes yield cost savings and improve availability of pharmaceuticals, vaccines or health products? A systematic review of evidence from low-income and middle-income countries. BMJ Global Health. 2017;2:e000243.
Article PubMed PubMed Central Google Scholar
Windisch R, Waiswa P, Neuhann F, Scheibe F, Savigny DD. Scaling up antiretroviral therapy in Uganda: using supply chain management to appraise health systems strengthening. Global Health. 2011;7:25. https://doi.org/10.1186/1744-8603-7-25 .
Cyn-Young P, Kijin K, Susann R, Steven B, Woo KJ, Tayag MC, et al. This brief examines the global shortage of the personal protective equipment (PPE) needed to tackle COVID-19 and suggests policy implications. Manila: Asian Development Bank; 2020.
Dai T, Zaman MH, Padula WV, Davidson PM. Supply chain failures amid Covid-19 signal a new pillar for global health preparedness. J Clin Nurs. 2021;30(1–2):e1–3. https://doi.org/10.1111/jocn.15400 .
Ghaffar A, Rashidian A, Khan W, Tariq M. Verbalising importance of supply chain management in access to health services. J Pharm Policy Pract. 2021;14(Suppl 1):91. https://doi.org/10.1186/s40545-021-00352-5 . ( 1–3 ).
Jahre M, Dumoulin L, Greenhalgh LB, Hudspeth C, Limlim P, Spindler A. Improving health in developing countries: reducing complexity of drug supply chains. JHLSCM. 2012;2(1):54–84. https://doi.org/10.1108/20426741211226000 .
Vledder M, Friedman J, Sjoblom M, Brown T, Yadav P. Improving supply chain for essential drugs in low-income countries: results from a large scale randomized experiment in Zambia. Health Syst Reform. 2019;5(2):158–77. https://doi.org/10.1080/23288604.2019.1596050 .
Agrawal P, Barton I, Bianco RD, Hovig D, Sarley D, Yadav P. Moving medicine, moving minds: helping developing countries overcome barriers to outsourcing health commodity distribution to boost supply chain performance and strengthen health systems. Glob Health Sci Pract. 2016;4(3):359–65. https://doi.org/10.9745/GHSP-D-16-00130 .
Arora M, Gigras Y. Importance of supply chain management in healthcare of third world countries. IJSOM. 2018;5(1):101–6. https://doi.org/10.22034/2018.1.7 .
Creswell J, Creswell JD. Research design: qualitative, quantitative, and mixed methods approaches. London: Sage; 2018.
Achoki T, Lesego A. The imperative for systems thinking to promote access to medicines, efficient delivery, and cost-effectiveness when implementing health financing reforms: a qualitative study. Int J Equity Health. 2017;16:53. https://doi.org/10.1186/s12939-017-0550-x . (1-13).
Colson KE, Dwyer-Lindgren L, Achoki T, Fullman N, Schneider M, Mulenga P, et al. Benchmarking health system performance across districts in Zambia: a systematic analysis of levels and trends in key maternal and child health interventions from 1990 to 2010. BMC Med. 2015;13:69. https://doi.org/10.1186/s12916-015-0308-5 . 1-14.
Githendu P, Morrison L, Silaa R, Pothapregada S, Asiimwe S, Idris R, et al. Transformation of the Tanzania medical stores department through global fund support: an impact assessment study. BMJ Open. 2020;10(e040276):1–12. https://doi.org/10.1136/bmjopen-2020-040276 .
MOHCC. Infection Control and Waste Management Plan (ICWMP). Harare: Ministry of Health and Child Care; 2022.
Moosavi J, Fathollahi-Fard AM, Dulebenets MA. Supply chain disruption during the COVID-19 pandemic: recognizing potential disruption management strategies. Int J Disaster Risk Reduct. 2022;75:102983. https://doi.org/10.1016/j.ijdrr.2022.102983 .
Albano GL, Ballarin A, Sparro M. Framework agreements and repeated purchases: the basic economics and a case study on the acquisition of it services. In: International Public Procurement Conference. Milan: The International Public Procurement Conference; 2010.
OECD. Manual for framework agreements. Paris: Organization for Economic Co-operation and Development; 2014.
Arney L, Yadav P, Miller R, Wilkerson T. Strategic contracting practices to improve procurement of health commodities. Glob Health Sci Pract. 2014;2(3):295–306. https://doi.org/10.9745/GHSP-D-14-00068 .
Download references
Acknowledgements
The authors would like to thank the participants from the different organizations in Zimbabwe that provided feedback during the study. They are also grateful to the management of the various organizations that allowed their staff to participate and provided premises and other resources that were used during the interviews. Gratitude to Sarah Gurrib who proofread the manuscript and offered useful comments.
The study was funded by the Global Fund to Fight AIDs, Tuberculosis and Malaria. The funder had no role in the study design, data collection, data analysis, data interpretation, or writing of the article. All authors had full access to study data and had final responsibility for the decision to submit for publication.
Author information
Authors and affiliations.
Africa Institute for Health Policy, P.O. Box 57266-00200, Nairobi, Kenya
Abaleng Lesego, Lawrence P. O. Were, Tsion Tsegaye & Tom Achoki
Department of Health Sciences & Department of Global Health, Boston University, Boston, U.S.A.
Lawrence P. O. Were
Global Fund to Fight AIDs, Tuberculosis and Malaria, Geneva, Switzerland
Rafiu Idris, Linden Morrison, Tatjana Peterson & Sheza Elhussein
PricewaterhouseCoopers, Harare, Zimbabwe
Esther Antonio & Godfrey Magwindiri
National Pharmaceutical Company of Zimbabwe, Harare, Zimbabwe
Ivan Dumba, Cleyland Mtambirwa, Newman Madzikwa & Raiva Simbi
Medicines Control Authority of Zimbabwe, Harare, Zimbabwe
Misheck Ndlovu
You can also search for this author in PubMed Google Scholar
Contributions
Tom Achoki (TA), Rafiu Idris (RI), Lawrence Were (LW) and Abaleng Lesego (AL) conceptualized and designed the study. AL, TA, and Godfrey Magwindiri (GM) collected and analyzed data. TA and AL drafted the manuscript. Tsion Tsegaye (TT), Linden Morrison (LM), Tatjana Peterson (TP), Sheza Elhussein (SE), Esther Antonio(EA), Ivan Dumba (ID), Cleyland Mtambirwa (CM), Newman Madzikwa(NM), Raiva Simbi (RS), Misheck Ndlovu (MN) and LW did the critical revisions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Correspondence to Tom Achoki .
Ethics declarations
Ethics approval and consent to participate.
Ethical approval including the consent procedure for participants was obtained from the Ethics Committee of the MOHCC Department of Research and NATPHARM, Harare Zimbabwe. The conduct and methods of this study adhered to the tenets outlined in the Declaration of Helsinki. Informed consent was obtained from each study participant involved in the study. The data collection protocol ensured that all study participants fully understood the objectives of the study and consented in writing to provide the required information. Before the interview commenced, the participants also consented verbally and confirmed that they had understood the objectives of the study and that they could opt out of the interview at any time without prejudice. No sensitive or personally identifying information was collected regarding the study participants.
Consent for publication
Not applicable.
Competing Interests
RI, LM, TP and SE declare that they are fulltime employees at the Global Fund to Fight AIDs, Tuberculosis and Malaria. EA and GM declare that they are fulltime employees at PricewaterhouseCoopers. ID, CM, NM and RS are fulltime employees at National Pharmaceutical Company of Zimbabwe. The rest of the authors declare that they have no competing interests.
Additional information
Publisher's note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Lesego, A., Were, L.P.O., Tsegaye, T. et al. Health system lessons from the global fund-supported procurement and supply chain investments in Zimbabwe: a mixed methods study. BMC Health Serv Res 24 , 557 (2024). https://doi.org/10.1186/s12913-024-11028-6
Download citation
Received : 06 March 2023
Accepted : 22 April 2024
Published : 01 May 2024
DOI : https://doi.org/10.1186/s12913-024-11028-6
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Health systems
- Procurement and supply chain management
- Global fund
- Donor funded programs
- Development assistance for health
- Health systems strengthening
BMC Health Services Research
ISSN: 1472-6963
- General enquiries: [email protected]
IMAGES
VIDEO
COMMENTS
There are several types of interviews, often differentiated by their level of structure. Structured interviews have predetermined questions asked in a predetermined order. Unstructured interviews are more free-flowing. Semi-structured interviews fall in between. Interviews are commonly used in market research, social science, and ethnographic ...
Introduction. Interviewing people is at the heart of qualitative research. It is not merely a way to collect data but an intrinsically rewarding activity—an interaction between two people that holds the potential for greater understanding and interpersonal development. Unlike many of our daily interactions with others that are fairly shallow ...
Interviewing. This is the most common format of data collection in qualitative research. According to Oakley, qualitative interview is a type of framework in which the practices and standards be not only recorded, but also achieved, challenged and as well as reinforced.[] As no research interview lacks structure[] most of the qualitative research interviews are either semi-structured, lightly ...
Qualitative interviewing provides a method for collecting rich and detailed information about ... structure should reflect the goals and stage of your research. Less structured interviews are most appropriate for early stages of research because they ... Qualitative Research & Evaluation Methods. Sage Publications. Rubin, Herbert J., and Irene ...
Abstract. Qualitative interviewing is a foundational method in qualitative research and is widely used in health research and the social sciences. Both qualitative semi-structured and in-depth unstructured interviews use verbal communication, mostly in face-to-face interactions, to collect data about the attitudes, beliefs, and experiences of ...
Types of Interviews in Research | Guide & Examples. Published on 4 May 2022 by Tegan George. Revised on 10 October 2022. An interview is a qualitative research method that relies on asking questions in order to collect data. Interviews involve two or more people, one of whom is the interviewer asking the questions.
InterViews by Steinar Kvale Interviewing is an essential tool in qualitative research and this introduction to interviewing outlines both the theoretical underpinnings and the practical aspects of the process. After examining the role of the interview in the research process, Steinar Kvale considers some of the key philosophical issues relating ...
Abstract. In-depth interviews are a versatile form of qualitative data collection used by researchers across the social sciences. They allow individuals to explain, in their own words, how they ...
A qualitative research interview is a one-to-one data collection session between a researcher and a participant. Interviews may be carried out face-to-face, over the phone or via video call using a service like Skype or Zoom. There are three main types of qualitative research interview - structured, unstructured or semi-structured.
6. Qualitative Research and Interviews. So we've described doing a survey and collecting quantitative data. But not all questions can best be answered by a survey. A survey is great for understanding what people think (for example), but not why they think what they do. If your research is intending to understand the underlying motivations or ...
The methods of qualitative data collection most commonly used in health research are document study, observations, semi-structured interviews and focus groups [1, 14, 16, 17]. Document study These can include personal and non-personal documents such as archives, annual reports, guidelines, policy documents, diaries or letters.
It is the most widely used method in qualitative research. It is flexible, inexpensive, and does not inter-fere with the researcher's life the way that ethnography does. This chapter looks at qualitative interviewing and how it compares to other types of collect-ing evidence in research, particularly structured interviewing and ethnography.
Abstract. Qualitative interviews are widely used in qualitative and mixed methods research designs in applied linguistics, including case studies, ethnographies, interview studies, and narrative research. This entry discusses commonly used forms of interviews and provides examples to show how researchers use interview accounts to generate ...
Interviews can be defined as a qualitative research technique which involves "conducting intensive individual interviews with a small number of respondents to explore their perspectives on a particular idea, program or situation." There are three different formats of interviews: structured, semi-structured and unstructured.
Introduce yourself and explain the aim of the interview. Devise your questions so interviewees can help answer your research question. Have a sequence to your questions / topics by grouping them in themes. Make sure you can easily move back and forth between questions / topics. Make sure your questions are clear and easy to understand.
In this article we briefly review the more common qualitative interview methods and then focus on the widely used individual face-to-face in-depth interview, which seeks to foster learning about individual experiences and perspectives on a given set of issues. ... The qualitative research interview Med Educ. 2006 Apr;40(4):314-21. doi: 10.1111 ...
The most common methods of data collection used in qualitative research are interviews and focus groups. While these are primarily conducted face-to-face, the ongoing evolution of digital ...
Three types of interviews are common in social health: (1) Structured; (2) semi‑structured; and (3) narrative interview. These range in a format including speci ed sets of questions to the ...
is directed. This is the most commonly used type of interview used in qualitative research and many studies illustrate its use in the context of diabetes and diabetes self‑management.[8‑17] The semi‑structured interview guide provides a clear set of instructions for interviewers and can provide reliable, comparable qualitative data.
Qualitative Research. Qualitative research is a type of research methodology that focuses on exploring and understanding people's beliefs, attitudes, behaviors, and experiences through the collection and analysis of non-numerical data. It seeks to answer research questions through the examination of subjective data, such as interviews, focus ...
There are a variety of methods of data collection in qualitative research, including observations, textual or visual analysis (eg from books or videos) and interviews (individual or group). 1 ...
Focus groups and in-depth interviews are feasible methods for doing qualitative market research and understanding the "how" and "why" of decision-making processes. Focus groups bring people together for collaborative conversation, whereas in-depth interviews provide perspectives from people who may have no collective impact.
A qualitative design with semi-structured interviews was used to explore the views of GPNs in relation to the research questions. Semi-structured interviews have the potential to provide a deeper understanding of participant experience than would be obtained from quantitative methods [ 23 ].
Data access committees (DAC) gatekeep access to secured genomic and related health datasets yet are challenged to keep pace with the rising volume and complexity of data generation. Automated decision support (ADS) systems have been shown to support consistency, compliance, and coordination of data access review decisions. However, we lack understanding of how DAC members perceive the value ...
A qualitative research interview is a one-to-one data collection session between a researcher and a participant. Interviews may be carried out face-to-face, over the phone or via video call using a service like Skype or Zoom. There are three main types of qualitative research interview - structured, unstructured or semi-structured.
Contexts A radio interview. Interviews can happen in a wide variety of contexts: Employment.A job interview is a formal consultation for evaluating the qualifications of the interviewee for a specific position. One type of job interview is a case interview in which the applicant is presented with a question or task or challenge, and asked to resolve the situation.
Methods: The paper draws on 31 semi-structured interviews with 11 Swiss natives residing in Switzerland, 10 Italian migrants residing in Switzerland, and 10 Italian natives residing in Italy. Interviews were conducted from December 2021 to March 2022. ... Respondents to the qualitative interviews had already participated to the TransAge survey ...
The interviews were recorded and transcribed. Analysis of the interview transcripts and questionnare responses was performed using Dedoose Qualitative Research Software Version 4.3.Qualitative data from interviews and feedback questionnaires were coded thematically in alignment with Clarke and Braun's suggestions for qualitative analysis ...
This study employed a mixed methods design combining quantitative and qualitative research methods. The quantitative part entailed a descriptive analysis of procurement and supply chain data from the Zimbabwe healthcare system covering 2018 - 2021. The qualitative part comprised key informant interviews using a structured interview guide.