Stress Management Interventions for Nurses: Critical Literature Review
Affiliation.
- 1 Mayo Clinic.
- PMID: 31014156
- DOI: 10.1177/0898010119842693
Background: The nursing literature contains numerous studies on stress management interventions for nurses, but their overall levels of evidence remain unclear. Holistic nurses use best-available evidence to guide practice with self-care interventions. Ongoing discovery of knowledge, dissemination of research findings, and evidence-based practice are the foundation of specialized practice in holistic nursing. This literature review aimed to identify the current level of evidence for stress management interventions for nurses. Method: A systematic search and review of the literature was used to summarize existing research related to stress management interventions for nurses and recommend directions for future research and practice. Results: Ninety articles met the inclusion criteria for this study and were categorized and analyzed for scientific rigor. Various stress management interventions for nurses have been investigated, most of which are aimed at treatment of the individual versus the environment. Contemporary studies only moderately meet the identified standards of research design. Issues identified include lack of randomized controlled trials, little use of common measurement instruments across studies, and paucity of investigations regarding organizational strategies to reduce nurses' stress. Conclusion: Future research is indicated to include well-designed randomized controlled trials, standardized measurement tools, and more emphasis on interventions aimed at the environment.
Keywords: burnout; nurse; resilience; stress management; systematic review.

Publication types
- Nurses / psychology*
- Nurses / statistics & numerical data
- Stress, Psychological / psychology
- Stress, Psychological / therapy*
- Open access
- Published: 29 May 2024
The Retrospective Stressor Analysis (RSA): a novel qualitative tool for identifying causes of burnout and mitigation strategies during residency
- Kristin L. Chrouser 1 ,
- Laura Zebib 1 ,
- Blake F. Webb 2 ,
- Tandi Bagian 2 &
- Timothy Arnold 3 , 4
BMC Medical Education volume 24 , Article number: 591 ( 2024 ) Cite this article
65 Accesses
3 Altmetric
Metrics details
Resident physicians are at an increased risk of burnout due to their high-pressure work environments and busy schedules which can lead to poor mental health outcomes and decreased performance quality. Given variability among training programs and institutions across the United States, stressors likely differ, and interventions must be tailored to the local context, but few tools exist to assist in this process.
A tool commonly used in adverse event analysis was adapted into a “retrospective stressor analysis” (RSA) for burnout prevention. The RSA was tested in a group of chief residents studying quality improvement and patient safety in veteran’s hospitals across the United States. The RSA prompted them to identify stressors experienced during their residencies across four domains (clinical practice, career development, personal life, and personal health), perceived causes of the stressors, and potential mitigation strategies.
Fifty-eight chief residents completed the RSA. Within the clinical domain, they describe the stress of striving for efficiency and clinical skills acquisition, all while struggling to provide quality care in high pressure environments. In the career domain, identifying mentors and opportunities for research engagement was stressful. Within their personal lives, a lack of time-constrained their ability to maintain hobbies, relationships, and attend meaningful social events while also reducing their engagement in healthy behaviors such as exercise, optimal nutrition, and attending medical appointments. Within each of these domains, they identified and described stress mitigation strategies at the individual, departmental, and national levels.
The RSA is a novel tool that can identify national trends in burnout drivers while simultaneously providing tailored prevention strategies for residents and their training sites.
Peer Review reports
Resident physicians are vital to the US healthcare system, but burnout rates among residents range from 17–94%, with variation by specialty and program [ 1 , 2 ]. Burnout is characterized by emotional exhaustion, depersonalization, and a reduced sense of personal accomplishment.[ 3 ] External factors like demanding work environments, high patient care standards, long hours, poor work-life balance, lack of mental health support, and mistreatment in the workplace, combined with internal factors such as perfectionist personality, neuroticism, and previous mental health diagnosis, heighten the risk of burnout [ 1 , 4 , 5 , 6 ].
Burnout can be detrimental to resident physicians’ personal and professional well-being, leading to decreased job satisfaction, increasing attrition, depression, substance use, and suicide [ 7 , 8 , 9 ]. Burnout can also have clinical implications, negatively affecting patient access and quality of care. Burned-out physicians are more likely to make medical errors, exhibit increased implicit and explicit biases, and become less productive [ 9 , 10 , 11 , 12 ]. Meta-analyses find that burnout among healthcare providers is associated with reduced patient satisfaction, quality indicators, and perceived patient safety [ 13 , 14 ]. Thus, patient safety, quality of care, and physician wellbeing are inextricably linked. Consequently, the Accreditation Council for Graduate Medical Education (ACGME) has enhanced requirements for residency program accreditation, emphasizing monitoring and maintaining well-being during residency training [ 15 ].
A recent review of interventions to reduce resident burnout notes the current literature is of marginal quality and results are inconclusive [ 16 ]. While self-care initiatives have been shown to alleviate burnout in some small samples, such interventions emphasize modification of internal factors. This shifts the responsibility onto residents and does not address the systemic and environmental factors that promote burnout. Studies suggest that interventions addressing external factors such as work-hour limitations, structured mentorship programs, and access to mental health programs are associated with decreased burnout among residents [ 16 , 17 , 18 , 19 ]. Bakker’s Job Demands-Job Resources Conceptual Model illustrates that burnout is a consequence of chronic work-related stress, when job demands exceed job resources and individuals can no longer cope [ 20 ]. Therefore, effective burnout prevention requires reduction of job demands and/or augmentation of job resources, and should address both internal and external risk factors unique to each specialty and residency program.
Given the ACGME’s interest in burnout prevention, many residency programs use standardized surveys to monitor resident burnout rates. Tailored information can be gleaned from measures such as the Mini ReZ, which assesses the impact of several common residency stressors (e.g., electronic health record, interruptions, sleep impairment) [ 21 , 22 ]. However, causes of burnout will likely change rapidly over time as institutions adopt new technologies, face novel challenges (like COVID-19), or respond to regulatory changes.[ 23 ] For example, the advent of the electronic health record (EHR) rapidly changed documentation processes and created new stressors that increased physician burnout [ 24 ]. In the context of a constantly changing environment, surveys that identify sources of burnout based on the existing literature may fail to promptly capture ever-shifting stressors. Surveys are confined to capturing trends in explicitly asked topics. This limits our ability to capture emerging or unknown stressors. Furthermore, there is a paucity of data on residents’ perceptions of the causes of burnout. Therefore, we need tools that can elucidate burnout drivers and potential prevention strategies in rapidly changing environments from the perspective of impacted individuals. This will aid resource allocation for high-yield improvements.
The adaptation of an adverse event analysis tool can leverage methods that are already familiar to residents in order to generate an understanding of burnout drivers and potential interventions. With growing evidence of the negative impact of burnout on providers, trainees, and patient care, institutions need innovative tools to monitor for new causes of burnout in changing environments. This will allow them to rapidly shift burnout prevention strategies when appropriate. This study aims to 1) characterize recent residency graduates’ perceptions of the drivers of burnout, 2) identify potential interventions for mitigating resident burnout, and 3) assess the utility of the RSA (retrospective stressor analysis) as a novel tool to identify a wider breadth of sources of resident burnout than found in the current literature as well as generate practical strategies to mitigate these causes.
Root-cause analysis (RCA) is a methodology to identify underlying causes of an adverse event and has been used in healthcare to characterize and help prevent future adverse outcomes [ 25 ]. Residents are typically familiar with RCA methodology, including the “five whys” and fishbone diagrams from their patient safety and quality improvement training. The final deliverable of an RCA is a list of “action items” to address or eliminate these underlying causes and prevent similar future problems. Similar to an RCA, this Retrospective Stressor Analysis (RSA) was designed to identify potential underlying causes of stressors and list possible corrective actions/prevention strategies (see Appendix A). The RSA has dual utility to 1) be used by institutions to explore resident perceptions of causes as a cohort and implement resident-derived interventions and 2) be used by residents as an opportunity for self-reflection on their own individual perceived burnout causes and identify actions they can personally take to mitigate burnout and improve resilience.
In March 2022, 87 VA Chief Residents in Quality Improvement and Patient Safety (CRQS) across 67 Veterans Affairs Healthcare Centers were given a homework assignment on Building Resilience/Preventing Burnout. Participants were instructed to recall stressors experienced during their residencies across four domains (clinical practice, career development, personal life, and personal health) that they felt increased their risk of burnout. Then they listed perceived causes of these stressors and potential prevention and mitigation strategies. After aggregating the deidentified data, we coded stressors and mitigation strategies and identified themes within each of the four domains (clinical practice, career development, personal life, and personal health). Evaluating each entry’s content and context, one author (KC) developed codes using thematic analysis. After compiling the initial codebook, a second coder (TA) coded 20% of the entries in each domain. Co-analysis agreement was > 80%, and disagreements were resolved by discussion. Given the large dataset, codes for stressors were then ranked by frequency within each domain and the top 15 illustrated as word clouds. Conceptual themes were identified within each domain.
Preventive strategies for each domain were compiled and categorized by intervention level (personal, departmental, national) and themes were identified. Participants received a deidentified compilation of prevention strategies as a resource to share with their medical education community. The University of Michigan Institutional Review Board reviewed this study and determined it to be exempt and waived ethical approval and consent to participate. The data are available from the corresponding author, Dr. Kristin Chrouser, upon request.
In 2022, 58 chief residents (67%) completed the RSA assignment. All responses were deidentified, so demographic information is not available. Participants identified 1020 stressors (306 clinical, 262 career, 247 personal life, and 205 personal health) and 569 mitigation strategies (165 clinical, 136 career, 133 personal life, and 135 personal health). Qualitative analysis of stressors and mitigation strategies revealed several themes within the four domains.
Themes from clinical practice domain stressors
Participants describe the stresses related to their clinical work (Fig. 1 ), such as high patient volume, patient acuity, challenging patient interactions, poor outcomes, and systems issues, including EHR frustrations, documentation hassles, administrative burden, and lack of backup. They highlighted challenges regarding the management of clinical work, such as striving for efficiency, admitting a lack of knowledge/experience, and asking for help. They were stressed by their adjustments to gaining seniority over the course of training related to role transition, acquiring leadership and teaching skills, and delegation challenges. They describe challenges related to their role as learners, such as time to study, gaining clinical knowledge, and learning procedures. They also describe their emotional experience/response to the stresses of their clinical role, including experiencing imposter syndrome, worry, the weight of responsibilities, emotion management, coping with mistakes, and facing inadequacies.

Clinical Practice Domain: Stressors that increased burnout risk*
*Size of word correlates with frequency of theme
Themes from the career development domain stressors
Participants describe various aspects of career development they considered stressful—such as research, publishing, presentations, teaching, committees, and professional relationships (Fig. 2 ). Many find career planning and career choices difficult, including fellowship decisions. They also recognize challenges in finding and becoming good mentors. Balancing academic and personal priorities and time management were common struggles. They also describe the additional stress of learning to cope with bias, competitiveness, failure, burnout, and performance anxiety.

Career Domain: Stressors that increased burnout risk*
Themes from the personal life domain stressors
Participants describe challenges in maintaining their personal lives as residents (Fig. 3 ). Lack of time is a common complaint, leading to difficulty separating work and home lives while describing concerns with a lack of opportunity to unwind from the stressors of residency. This includes inadequate time to invest in social life and maintain relationships with family and friends, eventually leading to erosion of social support. Social isolation was exacerbated by geographic separation from family support, moving to a new city, and COVID-19 restrictions.

Personal Life Domain: Stressors that increased burnout risk*
Many felt that long work hours led to difficulty coping with home stressors such as caregiving for children, family, and pets. Schedule inflexibility during residency led to missing important social events and being unavailable to manage family emergencies. They also recognized the difficulty of home maintenance, finances, and chores due to a lack of time. Residents described their emotional experience/response to these stresses in their personal lives as leading to guilt and feeling overwhelmed.
Themes from the personal health domain stressors
Participants described various challenges in maintaining their personal health as residents (Fig. 4 ). They described that a lack of time led to an inability to maintain healthy habits such as exercise, nutritious meals, proper hydration, and adequate sleep. Accessing physical and mental healthcare for themselves was difficult due to their schedules and social pressure to prioritize work over healthcare needs. Similarly, due to the demands and expectations of residency, many found it difficult to take a day off when ill.

Personal Health Domain: Stressors that increased burnout risk*
The struggle to cope and manage stress was a common complaint. Many participants noted this was exacerbated by the physical and mental stress of pregnancy and parenthood. They also described various emotional experiences related to their health: fear of COVID-19, feeling out of control, anxiety, and guilt for taking a sick day.
Mitigation strategies at the personal level
Table 1 outlines potential interventions to reduce burnout at various levels. For mitigation strategies on a personal level, many emphasized the importance of maintaining productivity through intentional organization within all domains. For example, within the clinical and career domains, their self-identified need for ongoing clinical learning could be achieved through setting clear goals and creating consistent study schedules, and within the personal domain, by scheduling designated time for relaxation, vacation, hobbies, and quality time with family. Interestingly, this also included creating time to prioritize one’s own health and attend medical appointments. Residents stressed the importance of determining clear personal goals, priorities, and setting expectations both at work and with family members. Many described the need to outsource home tasks, including house cleaning, grocery shopping, and childcare. Also, they described behaviors to automate healthy choices such as meal prepping, not purchasing unhealthy snacks, tracking water intake, and organizing resident meals with healthy options to maintain personal wellness.
Many residents commented on the importance of creating a team-like atmosphere in the work environment, including learning what tasks to delegate and consistently coordinating debrief sessions after adverse patient outcomes. They also discussed the importance of leveraging specific relationships, such as nursing staff, specialists, hospital resources, and asking for help from senior residents or faculty. Many advised the importance of adapting one’s mindset, such as adopting a reflective mindfulness practice, being vulnerable with peers and mentors, and reframing success and failure. A common theme was the importance of peer-to-peer relationships in discussing potential hurdles such as imposter syndrome and creating a culture where open discussion was encouraged.
Mitigation strategies at the departmental level
At the departmental level, participants emphasized the importance of mentorship and coaching. While some encouraged the importance of individually reaching out to potential mentors early and the utility of building peer relationships, others described the role institutions can play in creating mentorship programming. They desired mentors who would discuss imposter syndrome and failure and guide mentees through career and personal decisions. Many felt a need for significant shifts in culture to encourage open communication, sharing failures, and enhancing feedback mechanisms.
Some advised significant changes to patient care responsibilities, such as reduced work hours, capping the number of patients, and reduced note writing. Others described a need for greater standardization of clinical expectations such as templates for best practices, patient handoffs, consults, checklists, and “guides” for workflows in different clinic settings. Many described the need for augmenting the curriculum to include robust mechanisms for research support and increased training during orientation on communication skills, efficiency in the workplace, teaching, navigating difficult cases, managing imposter syndrome, and coping with failure.
Mitigation strategies at the national level
The most cited mitigation strategy across all domains was reducing resident duty hours. While many emphasized the role of institutions in complying with duty hour restrictions, further adjustments to duty hours require top-down implementation by the ACGME. Residents stated that there was a need for greater flexibility to utilize wellness days or sick leave. Given the stressors associated with family planning, many felt the ACGME and/or institutions should provide information and resources for cryopreservation, parental leave, and lactation. Lastly, increasing resident income was suggested as an effective strategy to alleviate resident budgetary stressors, accurately reflect work hours, and compensate some for the added stress of challenging work schedules such as jeopardy call schedules and night-float.
Burnout’s impact on physician well-being and quality of care is well established, and current rates are concerning [ 1 , 5 ]. Therefore, we need tools for ongoing assessment of the underlying causes of resident burnout and identification of potential interventions within local work environments. In this study, we describe the successful use of a novel tool, the retrospective stressor analysis (RSA), informed by the familiar RCA process, to characterize residents’ perceptions of burnout causes and potential mitigation strategies. To our knowledge, the field currently lacks alternatives to survey-based tools that will identify new sources of burnout and provide individuals and institutions with intervention strategies.
Participants in our study highlight how lack of time impacts their well-being in all four domains. This is not surprising as previous studies have shown a significant difference in the burnout rates of residents based on adherence to work-hour restrictions [ 26 ]. Similar to our findings, Mian et al., identified several common stressors among trainees that lead to burnout, such as overwork/sleep deprivation, emotional drain of caring for sick patients, lack of time for personal life outside training, and residency coinciding with major life events such as parenthood [ 27 ]. Related, Linzer et al. found burnout correlated with work-related conditions such as value alignment, teamwork, work control, and time pressures [ 22 ]. The RSA identified similar themes among participants. In addition, the RSA also provided greater context across the four domains to elucidate previously unacknowledged sources of stress, such as career decision-making, acquisition of leadership roles, and coping with adverse patient outcomes. To our knowledge, these have not been previously identified as potential sources of burnout within the resident population. Moreover, participants provided highly specific stressors, such as “variability in clinical preferences among attendings”, and potential mitigation strategies that program directors might find useful when restructuring expectations or generating standardized workflows.
While the RSA may be a novel resource for understanding burnout, there were some challenges with using it in practice. Despite clear instructions to list multiple causes, some participants did not identify more than one potential cause of their stressors, even though this is a common step used in root cause analysis. Failure to identify a variety of causes can reduce the diversity of proposed interventions. Despite this potential limitation, our cohort of residents still generated a large range of interventions for burnout prevention and mitigation. However, if RSA is used in smaller resident samples in the future without encouraging participants to provide a range of causes, this might generate a reduced range of interventions, thus limiting impact. The “personal life” domain was listed prior to “personal health,” so often participants included many factors in the personal life domain that would have been more appropriate under personal health, which made analysis of frequency by domain more challenging.
Moreover, proposed preventive strategies overwhelmingly focused on personal actions, although some participants suggested departmental/institutional/national policy reforms. The Institute for Healthcare Improvement’s Action Hierarchy Tool is used to assist RCA teams in identifying interventions with the strongest effect for sustained and successful system improvement [ 28 ]. Stronger actions are those that do not rely on human memory, such as architectural changes, forced functioning, removing unnecessary steps, and tangible involvement of leadership; while weaker actions, such as trainings and new procedures, rely on humans to remember to perform an action. Many of the recommended interventions identified using the RSA would be classified as weaker actions, as they rely on residents to remember and make time to perform specific tasks such as exercise, mindfulness, studying, and delegating in the clinical space. Future iterations of the tool should encourage the development of stronger intervention actions.
Although these challenges with RSA had minimal effect on data and analysis, our group refined the RSA tool for future data collection. Refinements included adjusting domain order to reduce categorization errors, adding reminders of QI tools useful in collecting a broader range of potential causes (5 whys, fishbone diagram), and providing examples of systemic preventive strategies (e.g., programs, policies). The revised RSA is available in Appendix B. Although our sample size was more than adequate to reach saturation for a qualitative study, the RSA’s usability, generalizability, and utility of our findings may vary among residents. The Chief Residents in Quality Improvement and Patient Safety were already familiar with RCA tools and methods, but this might not be the case for all residents, and future iterations may be informed by piloting the tool in varied resident populations. Participants also provided this data via a homework assignment, and even though they were assured their responses were confidential, fear of being identified by course directors may have influenced their responses. Demographics of participants were not collected, precluding any analysis based on specialty or gender. This is a limitation as burnout causes and mitigation recommendations might differ based on demographic categories.
The RSA provided findings consistent with factors known to contribute to burnout in the literature while generating a broader range of stressors than previously reported. RSA utilization can allow residency programs to identify emerging burnout drivers as medicine changes rapidly and provides a wealth of intervention ideas appropriate to the local context. Engaging residents in developing implementation strategies can serve the dual purpose of reinforcing skills applicable to adverse event analysis techniques and helping prevent resident burnout. Qualitative data assessment from the RSA could also be used by national associations to identify novel stressors and then generate new quantitative survey questions more appropriate for measurement within a larger population.
We adapted a familiar patient safety tool, root cause analysis (RCA), to create the retrospective stressor analysis (RSA) for burnout prevention. This novel tool allowed recent residency graduates to identify stressors they believe increased their risk of burnout and generate practical preventive strategies at personal, institutional, and national levels. Common themes highlighted the difficulty of inflexible schedules and lack of time invested in protective factors such as social support, mentorship, and healthy habits. The RSA is a novel tool that can identify national trends in the drivers of burnout while providing tailored prevention strategies for individuals, training sites, and the ACGME to consider for future implementation.
Disclaimers
The opinions expressed in this presentation are the authors’ own and do not necessarily reflect the view of the Department of Veterans Affairs or the United States government.
Availability of data and materials
The data are available from the corresponding author, Dr. Kristin Chrouser, upon request.
Abbreviations
Retrospective Stressor Analysis
American Council for Graduate Medical Education
Kratzke IM, Woods LC, Adapa K, et al. The Sociotechnical Factors Associated With Burnout in Residents in Surgical Specialties: A Qualitative Systematic Review. J Surg Educ. 2022May 1;79(3):614–23.
Article Google Scholar
Rodrigues H, Cobucci R, Oliveira A, et al. Burnout syndrome among medical residents: A systematic review and meta-analysis. PLoS One. 2018;13(11):e0206840.
Nene Y, Tadi P. Resident Burnout. StatPearls Publishing. 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK553176/ . Cited 2023 Feb 24.
Zhou AY, Panagioti M, Esmail A, et al. Factors associated with burnout and stress in trainee physicians: a systematic review and meta-analysis. JAMA Netw Open. 2020;3(8):e2013761.
Ferguson C, Low G, Shiau G. Resident physician burnout: insights from a Canadian multispecialty survey. Postgrad Med J. 2020Jun 1;96(1136):331–8.
McManus I, Keeling A, Paice E. Stress, burnout and doctors’ attitudes to work are determined by personality and learning style: A twelve year longitudinal study of UK medical graduates. BMC Med. 2004Dec;2(1):29.
Chaukos D, Chad-Friedman E, Mehta DH, et al. Risk and resilience factors associated with resident burnout. Acad Psychiatry. 2017;41(2):189–94.
van der Heijden F, Dillingh G, Bakker A, et al. Suicidal thoughts among medical residents with burnout. Arch Suicide Res. 2008;12(4):344–6.
West CP, Dyrbye LN, Shanafelt TD. Physician burnout: contributors, consequences and solutions. J Intern Med. 2018Jun;283(6):516–29.
Dewa CS, Loong D, Bonato S, Trojanowski L, et al. The relationship between resident burnout and safety-related and acceptability-related quality of healthcare: a systematic literature review. BMC Med Educ. 2017Nov 9;17(1):195.
Scheepers RA, Boerebach BCM, Arah OA, et al. A systematic review of the impact of physicians’ occupational well-being on the quality of patient care. Int J Behav Med. 2015;22(6):683–98.
Dyrbye L, Herrin J, West CP, Wittlin NM, et al. Association of racial bias with burnout among resident physicians. JAMA Netw Open. 2019J 3;2(7):e197457.
Salyers MP, Bonfils KA, Luther L, et al. The Relationship Between Professional Burnout and Quality and Safety in Healthcare: A Meta-Analysis. J Gen Intern Med. 2017Apr 1;32(4):475–82.
Tawfik DS, Scheid A, Profit J, Shanafelt T, et al. Evidence relating health care provider burnout and quality of care. Ann Intern Med. 2019;171(8):555–67.
American Medical Association. ACGME seeks to transform residency to foster wellness. 2015. Available from: https://www.ama-assn.org/medical-residents/medical-resident-wellness/acgme-seeks-transform-residency-foster-wellness . Cited 2023 Feb 24.
Busireddy KR, Miller JA, Ellison K, et al. Efficacy of Interventions to Reduce Resident Physician Burnout: A Systematic Review. J Grad Med Educ. 2017Jun 1;9(3):294–301.
Mullins CH, Gleason F, Wood T, et al. Do internal or external characteristics more reliably predict burnout in resident physicians: a multi-institutional study. J Surg Educ. 2020;77(6):e86-93.
Leung VWY, Konci X, Meterissian S. Is there a role for formal mentorship programs in reducing burnout in surgical residency?: a literature review. Available from: https://www.ijsed.com/article/25104.pdf . Cited 2023 Feb 25.
Clough BA, March S, Chan RJ, et al. Psychosocial interventions for managing occupational stress and burnout among medical doctors: a systematic review. Syst Rev. 2017Jul 17;6(1):144.
Bakker AB, Demerouti E. The job demands-resources model: state of the art. J Manag Psychol. 2007;22(3):309–28.
Maslach C, Jackson SE, Leiter MP. Maslach Burnout Inventory: Third edition. In: Zalaquett CP, editor. Evaluating stress: A book of resources. Lanham, MD, US: Scarecrow Education, xvii; 1997. p. 191–218. Available from: https://psycnet.apa.org/fulltext/1997-09146-011.pdf .
Linzer M, Shah P, Nankivil N, et al. The Mini Z Resident (Mini ReZ): Psychometric Assessment of a Brief Burnout Reduction Measure. J Gen Intern Med. 2023Feb;38(2):545–8.
Cravero AL, Kim NJ, Feld LD, et al. Impact of exposure to patients with COVID-19 on residents and fellows: an international survey of 1420 trainees. Postgrad Med J. 2021;97(1153):706–15.
Yan Q, Jiang Z, Harbin Z, et al. Exploring the relationship between electronic health records and provider burnout: A systematic review. J Am Med Inform Assoc. 2021Apr 23;28(5):1009–21.
Williams PM. Techniques for root cause analysis. Proc. 2001;14(2):154–7.
Google Scholar
Marchalik D, Brems J, Rodriguez A, et al. The Impact of Institutional Factors on Physician Burnout: A National Study of Urology Trainees. Urology. 2019Sep;1(131):27–35.
Mian A, Dahye K, Duane C, et al. Medical student and resident burnout: a review of causes, effects, and prevention. J Fam Med Dis Prev. 2018;31:4.
RCA2: Improving root cause analyses and actions to prevent harm. National Patient Safety Foundation. Available from: https://www.ashp.org/-/media/assets/policy-guidelines/docs/endorsed-documents/endorsed-documents-improving-root-cause-analyses-actions-prevent-harm.ashx . Cited 2023 Jun 19.
Download references
Acknowledgements
Maria Lennox, MS assisted with collating the raw data.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and affiliations.
Department of Urology, University of Michigan, Ann Arbor, MI, USA
Kristin L. Chrouser & Laura Zebib
VHA National Center for Patient Safety, Ann Arbor, MI, USA
Blake F. Webb & Tandi Bagian
Human Factors Engineering Division, Clinical Informatics and Data Management, Office of Health Informatics, Veterans Health Administration, Washington, DC, USA
Timothy Arnold
College of Pharmacy, University of Michigan, Ann Arbor, MI, USA
You can also search for this author in PubMed Google Scholar
Contributions
KC, TB, and TA conceptualized, developed, and designed the research study and tools. KC, TA, LZ, and BW analyzed and organized data. KC and LZ wrote the first draft. All authors edited manuscript drafts, read, and approved the final manuscript.
Corresponding author
Correspondence to Kristin L. Chrouser .
Ethics declarations
Ethical approval and consent to participate.
The University of Michigan Institutional Review Board reviewed this study and determined it to be exempt from ethical approval and consent to participate.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Supplementary material 1., supplementary material 2., rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Chrouser, K.L., Zebib, L., Webb, B.F. et al. The Retrospective Stressor Analysis (RSA): a novel qualitative tool for identifying causes of burnout and mitigation strategies during residency. BMC Med Educ 24 , 591 (2024). https://doi.org/10.1186/s12909-024-05571-3
Download citation
Received : 09 February 2024
Accepted : 17 May 2024
Published : 29 May 2024
DOI : https://doi.org/10.1186/s12909-024-05571-3
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Quality improvement
BMC Medical Education
ISSN: 1472-6920
- Submission enquiries: [email protected]
- General enquiries: [email protected]
Effectiveness of a mobile-based return to work program for decent return to work, fatigue, stress, and quality of working life among cancer survivors
- Published: 21 May 2024
Cite this article

- Kisook Kim 1 &
- Hyohyeon Yoon 1
55 Accesses
Explore all metrics
This study aimed to develop a smartphone mobile application-based supportive return to work (RTW) program for cancer survivors and evaluate its effects on their RTW, fatigue, stress, and quality of working life. This program was developed through a comprehensive process involving literature review, interviews with cancer survivors, and consultations with experts.
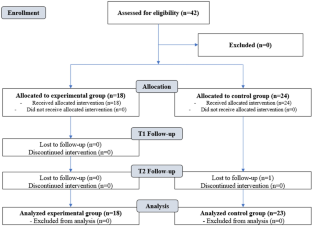
A non-equivalent control group pre- and post-test design was used, with 41 participants assigned to the experimental ( n = 18) and control ( n = 23) groups based on recruitment timing. The experimental group received a 6-week smartphone mobile application-based supportive RTW program comprising “Counseling and Education” and “Self-Management.” Participants completed assessments of decent RTW, fatigue, stress, and quality of working life at baseline and 6 months later. The experimental group completed an additional post-program completion survey.
During the 6-week program, no experimental group participants dropped out. The program’s impact on decent RTW remains unclear. Fatigue ( F = 2.52, p = 0.095) and quality of working life ( F = 0.86, p = 0.434) did not show statistically significant differences. However, there was a significant reduction in stress ( F = 4.59, p = 0.017).
The smartphone application-based RTW program, focusing on self-management and counseling, effectively reduced participants’ stress levels. To further evaluate the effectiveness of the program, a more diverse range of interventions and ongoing programs should be implemented.
Implications for Cancer Survivors
This study underscores the importance of tailored digital interventions to support the RTW of cancer survivors. The use of mobile smartphone applications allows temporal and spatial flexibility in program participation. Interventions involving various activities should be implemented to ensure ongoing participation.
This is a preview of subscription content, log in via an institution to check access.
Access this article
Price includes VAT (Russian Federation)
Instant access to the full article PDF.
Rent this article via DeepDyve
Institutional subscriptions
Similar content being viewed by others

The four-day work week: a chronological, systematic review of the academic literature

The Role of Mental Health on Workplace Productivity: A Critical Review of the Literature

The Effectiveness of Mindfulness-Based Stress Reduction on the Psychological Functioning of Healthcare Professionals: a Systematic Review
Data availability.
The data are not publicly available because they contained information that could compromise the privacy of the research participants.
References
National Cancer Information Center (NCIC). 5-year cancer survivor rate. 2023. https://www.cancer.go.kr/lay1/S1T648C650/contents.do . Accessed 21 Sep 2023.
Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA: Cancer J Clin. 2022;72(1):7–33. https://doi.org/10.3322/caac.21708 .
Article PubMed Google Scholar
Canadian Cancer Society. Canadian Cancer Statistics 2019. Health promotion and chronic disease prevention in Canada. 2019;39(8/9). https://doi.org/10.24095/hpcdp.39.8/9.04 .
Korea Central Cancer Registry. 5-year cancer relative survival rate. NCC. 2024. [cited 2024 Jan 30]. https://www.cancer.go.kr/lay1/S1T648C650/contents.do . Accessed 4 Feb 2024.
Santucci C, Carioli G, Bertuccio P, Malvezzi M, Pastorino U, Boffetta P, Negri E, Bosetti C, La Vecchia C. Progress in cancer mortality, incidence, and survival: a global overview. Eur J Cancer Prev. 2020;29(5):367–81. https://doi.org/10.1097/CEJ.0000000000000594 .
National Cancer Center (NCC). 2019 cancer facts and figures of Korea. 2019. https://www.ncc.re.kr/cancerStatsView.ncc?bbsnum=578&searchKey=total&searchValue=&pageNum=1 . Accessed 21 Sep 2023.
de Jong M, Tamminga SJ, Frings-Dresen MH, de Boer AG. Quality of working life of cancer survivors: associations with health-and work-related variables. Support Care Cancer. 2017;25(5):1475–84. https://doi.org/10.1007/s00520-016-3549-8 .
Han KT, Park EC, Kim SJ, Jang SI, Shin J, Kim CO, et al. Factors affecting the quality of life of Korean cancer survivors who return to the workplace. Asian Pac J Cancer Prev. 2014;15(20):8783–8. https://doi.org/10.7314/apjcp.2014.15.20.8783 .
Kim K, Yoon H. Health-related quality of life among cancer survivors depending on the occupational status. Int J Environ Res Public Health. 2021;18:1–16. https://doi.org/10.3390/ijerph18073803 .
Article Google Scholar
Son MR, Lee JS. Concept analysis on returning to work for cancer survivors. Korean J Mil Nurs. 2014;32(1):119–33.
Google Scholar
Leensen MC, Groeneveld IF, Van Der Heide I, Rejda T, Van Veldhoven PL, Van Berkel S, ... & de Boer AG. Return to work of cancer patients after a multidisciplinary intervention including occupational counselling and physical exercise in cancer patients: a prospective study in the Netherlands. BMJ Open. 2017;7(6): e014746. https://doi.org/10.1136/bmjopen-2016-014746 .
Nakamura K, Masuyama H, Nishida T, Haraga J, Ida N, Saijo M, ... & Hiramatsu Y. Return to work after cancer treatment of gynecologic cancer in Japan. BMC Cancer. 2016;16:1–9. https://doi.org/10.1186/s12885-016-2627-0 .
Shim HY, Mok H, Yang HK, Shin DW, Kim SY, Park JH. A study on cancer survivorship educational programs for health professionals. Korean J Fam Pract. 2017;7(4):483–96. https://doi.org/10.21215/kjfp.2017.7.4.483 .
Kim MH, Kim JS, Kim HN. Return-to-work experiences among nurses after receiving cancer treatment. J Korea Acad-Ind Coop Soc. 2016;17(6):215–25. https://doi.org/10.5762/KAIS.2016.17.6.215 .
Han SJ, Kim HW, Kim MR. Unmet needs for job maintenance of breast cancer survivor. J Korean Acad Fundam Nurs. 2020;27(3):298–309. https://doi.org/10.7739/jkafn.2020.27.3.298 .
Mehnert A. Employment and work-related issues in cancer survivors. Crit Rev Oncol Hematol. 2011;77(2):109–30. https://doi.org/10.1016/j.critrevonc.2010.01.004 .
Bae KR, Cho J. Changes after cancer diagnosis and return to work: experience of Korean cancer patients. BMC Cancer. 2021;21(1):86.
Article PubMed PubMed Central Google Scholar
Jin JH, Lee EJ. Factors influencing quality of working life of cancer survivors after return to the workplace. Korean J Occup Health Nurs. 2018;27(4):203–14. https://doi.org/10.3390/medicina56120721 .
Bae KR, Cho J, Jeon SH. A literature review of return-to-work interventions for cancer survivors. Korean J Occup Health Nurs. 2019;28(2):83–93. https://doi.org/10.5807/kjohn.2019.28.2.83 .
Park H, Kim K. Impact of psycho-social factors on fatigue among breast cancer patients who are currently undergoing radiotherapy. Int J Environ Res Public Health. 2020;17(17):6092.
Lee JH. ‘Decent’ return-to-work (RTW): the relationship among individual, segmented labor market, and RTW program. Health Soc Welfare Rev. 2017;37(2):389–422.
Mehnert A, de Boer A, Feuerstein M. Employment challenges for cancer survivors. Cancer. 2013;119:2151–9. https://doi.org/10.1002/cncr.28067 .
Bae KR. Development of a post-traumatic growth promoting program for working breast cancer patients [dissertation]. Seoul, South Korea: Yonsei University; 2017.
Son MR. Experience of return to work among officers with cancer [dissertation]. Seoul, South Korea: Hanyang University; 2014.
Van Lankveld JJ, Fleer J, Schroevers MJ, Sanderman R, Oudsten BLD, Dekker J. Recruitment problems in psychosocial oncology research. Psychooncology. 2018;27:2296–8. https://doi.org/10.1002/pon.4792 .
Whitaker C, Stevelink S, Fear N. The use of Facebook in recruiting participants for health research purposes: a systematic review. J Med Internet Res. 2019;19(8):e290. https://doi.org/10.2196/jmir.7071 .
Topolovec-Vranic J, Natarajan K. The use of social media in recruitment for medical research studies: a scoping review. J Med Internet Res. 2016;18(11):e286. https://doi.org/10.2196/jmir.5698 .
Kim HK, Yoo YS. Effects of the advanced practice nurse-led psychoeducational program for colorectal cancer survivors. J Korean Acad Nurs. 2022;52(3):245–60. https://doi.org/10.4040/jkan.21207 .
Greidanus MA, de Rijk AE, de Boer AGEM, Bos MEMM, Plaisier PW, Smeenk RM, Frings-Dresen MHW, Tamminga SJ. A randomised feasibility trial of an employer-based intervention for enhancing successful return to work of cancer survivors (MiLES intervention). BMC Public Health. 2021;21(1):1433. https://doi.org/10.1186/s12889-021-11357-9 .
Article CAS PubMed PubMed Central Google Scholar
Ullrich A, Rath HM, Otto U, Kerschgens C, Raida M, HagenAukamp C, et al. Return to work in prostate cancer survivors-findings from a prospective study on occupational reintegration following a cancer rehabilitation program. BMC Cancer. 2018;18(1):751.
Kim KM, Kim HY. The systemic contemplation of sadness mediation program applied to internal senior citizens. J Digit Converg. 2015;13(12):391–400.
Yellen SB, Cella DF, Webster K, Blendowski C, Kaplan E. Measuring fatigue and other anemia-related symptoms with the Functional Assessment of Cancer Therapy (FACT) measurement system. J Pain Symptom Manage. 1997;13(2):63–74. https://doi.org/10.1016/s0885-3924(96)00274-6 .
Article CAS PubMed Google Scholar
Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Social Behav. 1983;24:385–96. https://doi.org/10.2307/2136404 .
Article CAS Google Scholar
Lee J, Shin C, Ko YH, Lim J, Joe SH, Kim S, Han C. The reliability and validity studies of the Korean version of the Perceived Stress Scale. Korean J Psychosom Med. 2012;20(2):127–34.
Lee R, Lee KS, Oh EG, Kim SH. A randomized trial of dyadic peer support intervention for newly diagnosed breast cancer patients in Korea. Cancer Nurs. 2013;36(3):15–22. https://doi.org/10.1097/NCC.0b013e3182642d7c .
Forkan ARM, Khalil I. A probabilistic model for early prediction of abnormal clinical events using vital sign correlations in home-based monitoring. In 2016 IEEE International Conference on Pervasive Computing and Communications (PerCom). 2016;1–9.
Chung BY, Oh EH, Song SJ. Mobile health for breast cancer patients: a systematic review. Asian Oncol Nurs. 2017;17(3):133–42. https://doi.org/10.5388/AON.2017.17.3.133 .
Tamminga SJ, Verbeek JH, Bos MM, Fons G, Kitzen JJ, Plaisier PW, Frings-Dresen MH, de Boer AG. Effectiveness of a hospital-based work support intervention for female cancer patients–a multi-centre randomised controlled trial. PloS One. 2013;8(5):e63271.
Oldervoll L, Thorsen L, Kaasa S, Fossa S, Dahl A, Smastuen M, Nystad R, Hokstad A, Smeland S, Loge J. Inpatient versus outpatient rehabilitation after breast and gynecological cancers-a comparative study. Int J Phys Med Rehabil. 2014;2(187):2–7. https://doi.org/10.1371/journal.pone.0063271 .
Thorsen L, Dahl AA, Nystad R, Kiserud CE, Geirdal AØ, Smeland S. Baseline characteristics in female cancer patients with unimproved work status after an outpatient rehabilitation program and health changes during the intervention. Springerplus. 2016;5:1–7. https://doi.org/10.1186/s40064-016-2663-x .
Schumacher L, Armaou M, Rolf P, Sadhra S, Sutton AJ, Zarkar A, Grunfeld EA. Usefulness and engagement with a guided workbook intervention (WorkPlan) to support work related goals among cancer survivors. BMC Psychol. 2017;5(1):1–10. https://doi.org/10.2196/resprot.5300 .
Van Egmond M, Duijts S, Jonker M, Van Der Beek A, Anema J. Effectiveness of a tailored return to work program for cancer survivors with job loss: results of a randomized controlled trial. Acta Oncol. 2016;55(9–10):1210–9. https://doi.org/10.1080/0284186X.2016.1213417 .
Lamore K, Dubois T, Rothe U, Leonardi M, Girard I, Manuwald U, Nazarov S, Silvaggi F, Guastafierro E, Scaratti C. Return to work interventions for cancer survivors: a systematic review and a methodological critique. Int J Environ Res Public Health. 2019;16(8):1343. https://doi.org/10.3390/ijerph16081343 .
Bandani-Susan B, Montazeri A, Haghighizadeh MH, Araban M. The effect of mobile health educational intervention on body image and fatigue in breast cancer survivors: a randomized controlled trial. Ir J Med Sci. 2022;191(4):1599–605. https://doi.org/10.1007/s11845-021-02738-5 .
Galiano-Castillo N, Cantarero-Villanueva I, Fernández-Lao C, Ariza-García A, Díaz-Rodríguez L, Del-Moral-Ávila R, Arroyo-Morales M. Telehealth system: a randomized controlled trial evaluating the impact of an internet-based exercise intervention on quality of life, pain, muscle strength, and fatigue in breast cancer survivors. Cancer. 2016;122(20):3166–74. https://doi.org/10.1002/cncr.30172 .
Jensen-Johansen MB, Christensen S, Valdimarsdottir H, Zakowski S, Jensen AB, Bovbjerg D, Zachariae R. Effects of an expressive writing intervention on cancer-related distress in Danish breast cancer survivors–results from a nationwide randomized clinical trial. J Psychosoc Oncol. 2013;22(7):1492–500. https://doi.org/10.1002/pon.3193 .
Cheung YT, Tan EHJ, Chan A. An evaluation on the neuropsychological tests used in the assessment of post-chemotherapy cognitive changes in breast cancer survivors. Support Care Cancer. 2012;20:1361–75. https://doi.org/10.1007/s00520-012-1445-4 .
Balak F, Roelen CA, Koopmans PC, Ten Berge EE, Groothoff JW. Return to work after early-stage breast cancer: a cohort study into the effects of treatment and cancer-related symptoms. J Occup Rehabil. 2008;18:267–72. https://doi.org/10.1007/s10926-008-9146-z .
de Jong M, Tamminga SJ, van Es RJJ, Frings-Dresen MHW, de Boer A. The quality of working life questionnaire for cancer survivors (QWLQ-CS): factorial structure, internal consistency, construct validity and reproducibility. BMC Cancer. 2018;18(1):66. https://doi.org/10.1186/s12885-017-3966-1 .
Mewes JC, Steuten LM, Groeneveld IF, de Boer AG, Frings-Dresen MH, Ijzerman MJ, van Harten WH. Return-to-work intervention for cancer survivors: budget impact and allocation of costs and returns in the Netherlands and six major EU-countries. BMC Cancer. 2015;15:1–10. https://doi.org/10.1186/s12885-015-1912-7 .
Seon EA. A legal and institutional study on the treatment improvement in cancer patients. Pub Land L Rev. 2021;95:179–97. https://doi.org/10.1001/archinte.168.6.632 .
Adler NE, Page AEK. Institute of medicine committee on psychosocial services to cancer patients/families in a community setting, eds. Cancer care for the whole patient: meeting psychosocial health needs. Washington, DC: National Academies Press; 2008. https://doi.org/10.17226/11993 .
Lim J, Sohn J, Back J. A study on developing a self-efficacy enhancement program and evaluating its effects for breast cancer survivors. Korean J Soc Welf. 2020;72(2):125–50. https://doi.org/10.1016/j.apjon.2023.100267 .
Download references
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean Government (MSIT) (NRF-2020R1F1A1048591).
Author information
Authors and affiliations.
Department of Nursing, Chung-Ang University, 84, Heukseok-Ro, Dongjak-Gu, Seoul, 06974, Republic of Korea
Kisook Kim & Hyohyeon Yoon
You can also search for this author in PubMed Google Scholar
Contributions
Kisook Kim contributed to the study conception and design. The material preparation was performed by Kisook Kim. Kim and Yoon collected and analyzed the data. The first draft of the manuscript was written by Kisook Kim, and all authors commented on previous versions of the manuscript. All authors have read and approved the final version of the manuscript.
Corresponding author
Correspondence to Hyohyeon Yoon .
Ethics declarations
Ethics approval.
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of University Chung-Ang (Data 2022.01.14/No. 1041078–202201-HR-001–01).
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent for publication
None was obtained because it is inapplicable, given the nature of this study.
Competing interests
The authors have no relevant financial or non-financial interests to disclose.
Additional information
Publisher's note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Reprints and permissions
About this article
Kim, K., Yoon, H. Effectiveness of a mobile-based return to work program for decent return to work, fatigue, stress, and quality of working life among cancer survivors. J Cancer Surviv (2024). https://doi.org/10.1007/s11764-024-01570-x
Download citation
Received : 05 October 2023
Accepted : 13 March 2024
Published : 21 May 2024
DOI : https://doi.org/10.1007/s11764-024-01570-x
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Cancer survivors
- Return to work
- Psychological
- Find a journal
- Publish with us
- Track your research

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- v.8(Spec Iss 4); 2015
A review of the effectiveness of stress management skills training on academic vitality and psychological well-being of college students
P alborzkouh.
* Exceptional Children Psychology, Islamic Azad University, Central Tehran Branch, Iran
** General Psychology, Islamic Azad University, South Tehran Branch, Iran
*** General Psychology, Humanities and Social Sciences Faculty, Paradise University, Gillan Branch, Iran
**** General Psychology, Islamic Azad University, Science and Research Branch, Tehran, Iran
F Shahgholy Ghahfarokhi
***** Clinical Psychology, Islamic Azad University, Science and Research Branch Branch, Isfahan, Iran
Objective: Carrying out the appropriate psychological interventions to improve vitality and mental well-being is critical. The study was carried out to review the effectiveness of stress management training on the academic life and mental well-being of the students of Shahed University.
Methodology: The method used was quasi-experimental with a pretest-posttest plan and control group. Therefore, a total of 40 students of Shahed University of Tehran were selected by a convenience sampling method and were organized into two groups: experimental and control group. Both groups were pretested by using an academic vitality inventory and an 84-question psychological well-being inventory. Then, the experimental group received stress management skills training for ten sessions, and the control group did not receive any intervention. Next, both groups were post-tested, and the data were analyzed with SPSS-21 software by using descriptive and inferential statistical methods.
Findings: The findings showed that the stress management skills training significantly contributed to promoting the academic vitality and psychological well-being of students (p < 0.001).
Conclusions: It was concluded from this research that teaching the methods for dealing with stress was an effective strategy to help students exposed to high stress and pressure, and this was due to its high efficiency, especially when it was held in groups, had a small cost, and it was accepted by the individuals.
Introduction
Challenges during education create sources of stress for students, and put their health at risk, in a way that affects their learning abilities [ 1 ]. Therefore, paying attention to the factors that could have a positive impact on the agreeableness and could increase the positive psychological states, and as a result, the physical and psychological health of the students was of great importance.
Among the important factors that affect people’s ability to adapt to the stresses of studying era is academic vitality [ 2 ]. Academic vitality means an adaptive response to various challenges and barriers experienced during education [ 3 ]. When a person does things spontaneously, does not feel not only frustrated and tired, but also constantly feels the strength and increased energy, and overall has a sense of inner vitality [ 2 ]. Therefore, the academic life has a relationship with the individual’s adaptation to the various situations of the academic period, feelings of self-efficacy and empowerment in the face of challenges, experiencing less anxiety and depression, a sense of responsibility in dealing with the academic tasks and better academic success [ 3 ]. Despite the high importance of academic vitality in the successful confrontation with the challenging academic period, the literature review of the studies managed in Iran showed that few studies were performed on the factors promoting this important variable. Therefore, an attempt to address this research gap increased the need for the current study.
Another important positive psychological state in students is the psychological well-being. The psychological well-being factor is defined as a person’s real talents growth and has six components that are the purpose in life, positive relations with others, personal growth, self-acceptance, autonomy, and environmental mastery [ 4 ]. The purpose in life means having a purpose and direction in life and pursuing them [ 5 ]. Positive relations with the others mean having warm, satisfactory relations along with confidence and empathy [ 6 ]. Personal growth means having a sense of continuous growth and the capacity for it and having an increased sense of efficacy and wisdom [ 4 ]. Self-acceptance means having a positive attitude towards oneself and accepting the various aspects of oneself [ 6 ]. Autonomy means the feeling of self-determination, independence, and self-assessment against personal criteria [ 4 ]. Moreover, environmental mastery means a sense of competence and the ability to manage the complex environment around [ 5 ].
However, one of the most significant parts affecting the psychological health and well-being of individuals is life skills training [ 7 ]. Life skills’ training is critical for students, in a way that on this basis, many universities have started to teach life skills and stress management skills to improve the physical and psychological health of their students in the recent years [ 8 ]. The main objective of the World Health Organization regarding the creation of a life skills plan is in the field of psychological health. Therefore, different societies throughout the world try to promote the implementation and evaluation of the programs training in life skills. It focuses on the growth of mental abilities such as problem-solving, coping with emotions, self-awareness, social harmony, and stress management among children, teenagers, and even adults [ 9 ]. From the life skills, training in stress management skills is critical, because students need to deal effectively with stressful issues and factors. Accordingly, it was thought that teaching stress management skills is very efficient in improving the students’ positive psychological states, in particular, their vitality and mental well-being. Therefore, this study examined the effectiveness of the stress management skills training on the academic life and psychological well-being among Shahed University students.
Methodology
The study was quasi-experimental with a pretest-posttest. The analytical community of the study included all the students of Shahed University of Tehran in the fall of 2015, who were selected with a convenience method. For the calculation of the sample size, the appropriate sample size in experimental studies was of 15 people for each group [ 10 ]. At first, the sample size of 15 individuals was selected for each group. Then, to increase the statistical power and to manage the possible decrease in the number of participants, the sample size of 20 individuals (n = 20) was considered for each group. The sampling was voluntary non-random from among all the students studying at Shahed University. The inclusion criteria included an informed consent and the willingness to participate in the research, the ability to take part in the sessions and to collaborate in carrying out assignments, willingness to cooperate in completing the instruments, and the age range of 18 to 35 years. The exclusion criteria included the lack of desire to participate in the sessions and the absence to more than three courses in the preparation method, the lack of the ability to participate in the sessions, lack of cooperation in carrying out assignments, and receiving any training or psychological therapy that was not part of the program of this research.
The procedure of the study was that from all the students studying at Shahed University, a number was non-randomly and voluntarily selected, and if they met the inclusion criteria, they were randomly assigned to two groups: experimental and control. At the beginning and before starting the study, an informed consent was obtained from all of them to uphold moral considerations, through informing them of the aim of the study and the impact of such studies in improving their psychological status. Then, all the information of the participants were collected, and they were assured that the information would remain confidential by the researcher. Then, the experimental group received group stress management training for ten sessions, and the control group did not receive any intervention. In the end, both groups were post-tested. The protocol of stress management training sessions is presented in Table 1 .
Protocol of stress management skills training sessions
The instruments used in the study included a demographic sample page, an academic vitality questionnaire, and a psychological well-being scale (PWBS-18).
Demographic sample page: The demographic sample page included age, gender, educational level, and marital status. The sample page was prepared and evaluated by the researchers of the study.
Academic vitality questionnaire: This questionnaire was developed by Dehqanizadeh MH, Hosseinchari M (2012) [ 3 ], based on the academic vitality scale of Martin AJ, Marsh HW (2006) [ 15 ], which had four items. After various implementations of the items of the questionnaire, the final version was rewritten, and the result was that the revised version had ten items. Then the items above were again examined in a preliminary study on a sample including 186 high school students, who were chosen by using a cluster random sampling, and their psychometric properties were examined. The results of the examination showed that the obtained Cronbach’s alpha coefficient, by removing [ 3 ] item number 8, was 0.80 and the retest coefficient was 0.73. Also, the range of correlation of the elements with the total score was between 0.51 and 0.68. These results indicated that the items had a satisfactory internal consistency and stability.
Psychological well-being scale (SPWB): Riffe’s mental well-being scale [ 11 ] was made up of 84 questions in Likert’s 7-degree scale (from “strongly disagree” to “agree strongly”). It was a self-report questionnaire, which measured six components of the psychological well-being, including purpose in life, positive relations with others, personal growth, self-acceptance, autonomy, and environmental mastery. The internal consistency coefficients for the components of this questionnaire were obtained from 0.83 to 0.91. In Mohammadpour and Joshanloo research (2014) [ 6 ], the reliability coefficient of this scale with Cronbach’s alpha method for the psychological well-being scale obtained was 0.81. Also, for the subscales of the test including self-compliance, environmental mastery, personal growth and development, link with others, the goal in life, and self-acceptance were obtained at 0.60, 0.64, 0.54, 0.58, 0.65, and 0.61, respectively. A study performed by Kafka and Kozma (2002) was conducted to verify the validity of the items of the Riffe’s psychological well-being scale. The findings showed that there was a high correlation between this scale and the subjective well-being scale (SWB) and the satisfaction with life scale (SWLS). In the present study, the reliability coefficient with Cronbach’s alpha method for the psychological well-being scale obtained was 0.81. Also, for the subscales of the test, including self-compliance, environmental mastery, personal growth and development, relations with others, the goal in life, and self-acceptance were obtained at 0.60, 0.64, 0.54, 0.58, 0.65, and 0.61, respectively.
The SPSS-20 software was used for data analysis. The statistical method used for the data analysis of the research on the level of descriptive statistics was mean, standard deviation, frequency, and frequency percentage indexes, and on the inferential statistics, univariate and multivariate analysis of covariance model were used.
Findings of the research
The demographic properties of the sample present in the study are presented in Table 2 .
Demographic characteristics of the subjects
As presented in Table 1 , the largest frequency of participation belonged to the participants in the age range of 21 to 25 with 14 individuals (35%) and the lowest frequency of individuals in the range of 18 to 20 years, with six individuals (15%). In addition, the mean age of the participants was 24.85, and the standard deviation was 4.41. The other information about the demographic properties of the present sample is provided in Table 2
As shown in Table 3 , the mean scores of purpose in life, positive relations with others, personal growth, self-acceptance, autonomy, environmental mastery, total score of psychological well-being, and academic vitality of posttest were increased in the test group as associated with the control group.
Descriptive stats of academic vitality and psychological well-being scores of the two groups divided by the pretest and posttest
As shown in Table 4 , the null hypothesis of the equality of variances of the two groups in the academic vitality and psychological well-being with all its components was confirmed. It meant that the variances of the two clusters in the population were equal and had no significant difference for the academic vitality and the psychological well-being variable with all its components. Thus, given the compliance with the Levene assumption, the analysis of covariance of the results of the hypothesis of the research were permitted.
Results of Levene test for the examination of the consistency of variances of academic vitality and psychological well-being variables with its components in the posttest stage
As shown in Table 5 , the significance level of all the tests (p < 0.001) indicated that there was a significant difference between the two groups at least in one of the dependent variables (academic vitality and psychological well-being with its components). And, according to the eta square, 0.89 percent of the differences observed among individuals were associated with the effect of the independent variable, which was the intervention method (stress management skills training). On the other hand, given that the statistical power was 0.95, which was higher than 0.80, the sample size was acceptable for the research. The results related to significant differences in any of the dependent variables are listed below.
Results of multivariate analysis of covariance on the scores of posttest with the control of pretest in the academic vitality and psychological well-being variable with its components
According to Table 6 , the significance level was p < 0.001, the hypothesis of the difference between the academic vitality and the psychological well-being with its components in the two groups was confirmed. It stated that 0.54, 0.25, 0.52, 0.64, 0.60, 0.59, 0.45 and 0.81 percent change in the academic vitality, individuals’ purpose in life, positive relations with others, personal growth, self-acceptance, autonomy, environmental mastery, and psychological well-being scores were due to the independent variable (stress management skills training). Therefore, it could be said that stress management skills training increased the academic vitality and the psychological well-being and all of its components.
The results of multivariate analysis of covariance to assess the impact of stress management skills training on the level of psychological well-being and its components in the posttest stage
Discussion and conclusions
Given the aim of this study, which was to examine the effectiveness of stress management skills training on the academic vitality and psychological well-being of the students of Shahed University, the results of the univariate and multivariate analysis of covariance showed that stress management skills training had a significant impact on increasing the academic vitality and psychological well-being. The findings indicated that the stress management skills training had a major impact on increasing the academic life. It was consistent with different studies of Habibi M (2015), Pakdaman A, Ganji K, Ahmadzadeh M (2012), Shirbim Z, Sudani M, Shafi-Abadi A (2008) [ 12 - 14 ].
In explaining their similar finding, Pakdaman A, Ganji K, Ahmadzadeh M (2012) [ 13 ] also stated that life skills training helped in the improvement of the academic conditions of the subjects. In addition, this was because of this training, with growing different skills of the students, helping the students know their strengths and weaknesses, and overall, help the individuals move from weaknesses and skill deficits to capable and strong skills. Therefore, this could provide the students with better educational conditions [ 14 ]. In explaining their similar finding, Shafi-Abadi (2008) stated that teaching life skills, including stress management skills, are one of the ways to improve the mental health of the individuals of the community and to prevent harms. In fact, these teachings protected the health and mental hygiene of the society and protected it against diseases, disabilities, and disturbances in human relations. As a result, the feeling of security and solidarity increased among the members of the society, and then their senses of happiness, vitality, and health increased.
The findings showed that stress management skills’ training has a significant impact on the psychological well-being. It was consistent with the multiple studies of Qadiri-Bahramabadi F, Mikaeli-Manee F (2015), Qanbari N, Habibi M, Shams-Aldini S (2013), Alavi-Arjmand N, Kashaninia Z, Hosseini MA, Reza-Soltani P (2012), Chubforushzadeh A, Kalantari M, Molavi H (2009) [ 16 - 19 ].
In explaining their similar findings, Qadiri-Bahramabadi F, Mikaeli-Manee F (2015) [ 16 ] stated that facing numerous stresses required teaching and learning of appropriate stress management skills. In other words, during stress, individuals must know the necessary coping skills to reduce the effects of stress, and if the pressure was managed and the effective coping skills were applied, the person would be able to get along better with the needs and challenges of his/ her life. Therefore, the intervention of stress management led to the formation of good feelings about oneself, as well as a positive performance in the stable world. It created interest and motivation in people’s lives as well as increasing the self-confidence of the individuals. As a result, it increased the psychological well-being.
In explaining their similar finding, Qanbari N, Habibi M, Shams-Aldini S (2013) [ 17 ] stated that with the help of multiple strategies to manage stress such as relaxation, and muscular relaxation, stress and anxiety could be reduced. The individuals identified the somatic symptoms, and with mastering the ways to acquire relaxation, which was inconsistent with stress, reduced their anxiety and unpleasant feelings, thus increasing the psychological well-being. Also, in explaining their similar finding, Chubforushzadeh A, Kalantari M, Molavi H (2009) [ 19 ], stated that stress management treatments make multiple changes in the individual’s beliefs, feelings, and behaviors. Therefore, improving the individual’s evaluations and coping skills, and the provided practices to integrate the learned separations with real life situations could lead to a decrease in the perceived stress and an increase in the psychological well-being.
Acknowledgement
The authors would like to thank the venerable authorities of Shahed University of Tehran for their assistance. Also, the authors would like to thank all the participants in the study.
Click through the PLOS taxonomy to find articles in your field.
For more information about PLOS Subject Areas, click here .
Loading metrics
Open Access
Peer-reviewed
Research Article
Vitamin C and E antioxidant supplementation may significantly reduce pain symptoms in endometriosis: A systematic review and meta-analysis of randomized controlled trials
Roles Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing
* E-mail: [email protected]
Affiliation Department of Obstetrics and Gynecology, Faculty of Medicine, Pelita Harapan University, Tangerang, Banten, Indonesia
- Patrick Bayu,
- Jacobus Jeno Wibisono
- Published: May 31, 2024
- https://doi.org/10.1371/journal.pone.0301867
- Peer Review
- Reader Comments
The primary challenge encountered by individuals diagnosed with endometriosis is the experience of pain. Emerging research indicates that oxidative stress is implicated in the initiation of pain associated with endometriosis. Vitamins C and E are known for their antioxidative properties. The primary objective of this study is to assess the efficacy of antioxidant supplementation, consisting of these vitamins, in the management of pain associated with endometriosis.
A comprehensive search was conducted on the ClinicalTrials.gov, Scopus, Europe PMC, and Medline databases up until August 23 rd , 2023, utilizing a combination of relevant keywords. This review incorporates literature that examines the relationship between antioxidant supplementation and pain in endometriosis. We employed fixed-effect models to analyze the risk ratio (RR) and present the outcomes together with their corresponding 95% confidence intervals (CI).
A total of five RCTs were incorporated. The results of our meta-analysis indicated that antioxidant supplementation with vitamin C and E combination was associated with higher proportion of endometriosis patients reporting reduced chronic pelvic pain (RR 7.30; 95%CI: 3.27–16.31, p <0.00001, I 2 = 0%), alleviations of dysmenorrhea (RR 1.96; 95%CI: 1.25–3.07, p = 0.003, I 2 = 39%), and dyspareunia (RR 5.08; 95%CI: 2.10–12.26, p = 0.0003, I 2 = 0%) than patients only receiving placebo.
Conclusions
This study suggests the potential ability of vitamin C and E in alleviating pain symptoms experienced by individuals with endometriosis.
Citation: Bayu P, Wibisono JJ (2024) Vitamin C and E antioxidant supplementation may significantly reduce pain symptoms in endometriosis: A systematic review and meta-analysis of randomized controlled trials. PLoS ONE 19(5): e0301867. https://doi.org/10.1371/journal.pone.0301867
Editor: Diego Raimondo, Dipartimento di Scienze Mediche e Chirugiche (DIMEC), Orsola Hospital, ITALY
Received: October 3, 2023; Accepted: March 23, 2024; Published: May 31, 2024
Copyright: © 2024 Bayu, Wibisono. This is an open access article distributed under the terms of the Creative Commons Attribution License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Data Availability: All relevant data are within paper and its Supporting Information files.
Funding: The author(s) received no specific funding for this work.
Competing interests: The authors have declared that no competing interests exist.
1. Introduction
On a global scale, it has been observed that approximately 10 to 15 percent of women within the reproductive age bracket have the medical condition known as endometriosis [ 1 ]. Endometriosis is a pathological condition characterized by the ectopic growth of endometrial tissue beyond the confines of the uterine wall [ 2 ]. In this particular pathological state, the endometrium exhibits the ability to proliferate within several anatomical sites, including the ovaries (ovaries), peritoneal lining of the stomach, intestines, vagina, or urinary system [ 2 ]. The endometrium refers to the specialized tissue that forms the inner lining of the uterus [ 2 , 3 ]. Prior to menstruation, the endometrium undergoes a process of thickening, thereby creating a receptive environment for the implantation of a fertilized ovum [ 2 , 3 ]. In the absence of fertilization, the endometrium undergoes shedding, resulting in the expulsion of menstrual blood from the body [ 2 , 3 ]. In endometriosis, endometrial tissue that grows outside the uterus also thickens but lacks the ability to be shed and expelled from the body [ 2 , 3 ]. This condition induces irritation or inflammation of the tissue surrounding the endometrium, resulting in patient complaints manifested as pain [ 2 , 3 ].
The primary issue experienced by those with endometriosis is frequently pain [ 1 , 4 ]. Pain may be experienced in the context of menstruation (dysmenorrhea), sexual intercourse (dyspareunia), or as a persistent pelvic discomfort occurring outside the menstrual cycle (chronic pelvic pain) [ 1 , 4 ]. When managing the pain associated with endometriosis, healthcare professionals frequently prescribe analgesic medications such as acetaminophen or non-steroidal anti-inflammatory drugs (NSAIDs) [ 4 , 5 ]. The administration of nonsteroidal anti-inflammatory medicines (NSAIDs) frequently leads to adverse effects on the gastrointestinal system, manifesting as abdominal pain, nausea, vomiting [ 6 , 7 ]. In rarer instances, cardiovascular complications such as myocardial infarction (MI) and thromboembolic events may also occur [ 6 , 7 ]. Nonsteroidal anti-inflammatory drugs (NSAIDs) can induce disruptions in renal hemodynamics, hence restricting their administration in individuals with impaired renal function [ 6 , 7 ]. The aforementioned issue frequently represents the primary limitation of nonsteroidal anti-inflammatory drugs (NSAIDs) in the management of pain [ 6 , 7 ].
Emerging research has indicated that the occurrence of oxidative stress is implicated in the development and progression of endometriosis [ 8 ]. Reactive oxygen species (ROS), which exhibit elevated levels in the presence of oxidative stress, are inflammatory agents that have the potential to induce cellular damage [ 8 , 9 ]. Elevated levels of reactive oxygen species (ROS) have been linked to the synthesis of pro-inflammatory cytokines and prostaglandins by macrophages, as well as the stimulation of C-fibers through neurogenic inflammation [ 8 , 9 ]. The involvement of peroxidized lipids and lipoproteins in endometriosis has also been well-documented [ 8 , 9 ]. These mechanisms collectively contribute to the initiation of pain in individuals diagnosed with endometriosis [ 8 , 9 ]. Antioxidants are implicated in the mitigation of reactive oxygen species (ROS) in order to potentially alleviate discomfort associated with endometriosis [ 8 , 9 ]. A number of vitamins and minerals, including as vitamin A, vitamin C, vitamin E, zinc, copper, and selenium, have been identified as possessing antioxidant properties [ 10 ]. Among all of these, vitamin C and vitamin E are two distinct types of vitamins that possess antioxidant properties and exhibit minimal adverse effects, rendering them suitable for daily long-term consumption [ 10 ]. The co-administration of vitamin C and vitamin E is based on the concept of "vitamin E recycling," in which the antioxidant activity of oxidized vitamin E is effectively replenished by other antioxidants, such as vitamin C [ 10 ]. Moreover, the combination of vitamin C and vitamin E may increase the oxidation resistance of total serum lipids more efficiently than supplementation of vitamin E or vitamin C alone [ 10 ]. The objective of this study is to assess the efficacy of antioxidant supplementation with a mix of vitamin C and vitamin E in the treatment of pain associated with endometriosis. We hypothesized that vitamin C and E supplementation can significantly reduce pain symptoms better than placebo in patients with endometriosis.
2. Materials and methods
2.1. eligibility criteria.
The present study has been carried out following the protocols and recommendations specified in the PRISMA statement [ 11 ]. The protocol of this review has been registered in PROSPERO (CRD42023459152). We incorporated all randomized controlled trials (RCTs) that examined the effectiveness of antioxidant supplementation, specifically a combination of vitamin C and vitamin E, in comparison to a placebo, for the purpose of alleviating pain symptoms in women diagnosed with endometriosis. We excluded studies from our current systematic review and meta-analysis if they: (1) did not clearly specify that the participants had been diagnosed with endometriosis; (2) were cell-based or animal studies; (3) did not include a placebo as the comparison group; (4) were not primary investigations; and (5) had not undergone the process of publication.
2.2. Search strategy and study selection
A comprehensive review of the literature was performed, focusing specifically on papers written in the English language. The search encompassed a time frame up until August 23 rd , 2023, and was undertaken across four prominent worldwide databases: Medline, Scopus, Europe PMC, and the ClinicalTrials.gov. The search terms utilized for the literature review were as follows: “(antioxidant OR anti-oxidant OR antioxidative OR vitamin C OR ascorbic acid OR L-ascorbic acid OR vitamin E OR alpha-tocopherol) AND (supplementation OR therapy OR administration) AND (endometriosis OR adenomyosis OR ectopic endometrial tissue OR ectopic endometrium)”. More details regarding the search strategy for each database can be seen in S1 Table of S1 File . The initial search was conducted by two authors. The team also cross-checked the citations exported to the reference manager for consistency and completeness. To identify any additional relevant articles, citation tracking was performed by examining the references of the identified studies, tracking citations, and exploring related articles. Additionally, a follow-up search of gray literature sources was conducted. Titles and abstracts were screened independently by two authors, who excluded articles not relevant to the study. Full-text eligibility was conducted by the same two authors and the discrepancies were addressed in study judgments. S2 Table in S1 File contained the PRISMA 2020 checklist of the manuscript.
2.3. Data extraction
Two reviewers independently retrieved essential data extracted from the eligible articles including characteristics of participants (i.e., age, number of participants in each study arms) in addition to study characteristics (i.e., author last name, year of publication, country, study design, antioxidant content, and study duration). The data was tabulated into Microsoft Excel 2019.
The pain-related outcomes of this investigation were divided into chronic pelvic pain (everyday pain), pain during menstruation (dysmenorrhea), and pain during intercourse (dyspareunia). All of these outcomes were calculated as the proportion of patients who experienced decrease pain sensation during the last follow-up when compared to baseline.
2.4. Risk of bias assessment
The evaluation of potential bias in each study was conducted by two independent reviewers using standardized assessment tools. The Risk of Bias version 2 (RoB v2) was employed to assess the quality of each randomized trials [ 12 ]. This scale incorporates evaluations about the randomization of study participants, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported results of the studies [ 12 ]. The authors’ evaluations were categorized as "low risk," "high risk," or "some concerns" of bias [ 12 ].
2.5. Statistical analysis
The pain-related outcomes were calculated by using the Mantel-Haenszel formula to obtain the risk ratio (RR) along with the 95% confidence interval (95% CI). The I-squared (I 2 ; Inconsistency) statistic was employed to quantify the heterogeneity among research, where values exceeding 50% indicated a substantial or noteworthy level of heterogeneity [ 13 ]. The analysis will commence with the utilization of fixed-effect models. However, in the event that a substantial degree of heterogeneity is detected, a transition to random-effect models will be made. If the number of papers included in the meta-analysis exceeds 10, a funnel plot would be employed to evaluate the presence of publication bias. All analyses in this investigation were conducted using Review Manager 5.4, a software tool developed by the Cochrane Collaboration.
3.1. Study selection and characteristics
In this review we searched 4 databases; Europe PMC (n = 673), Scopus (n = 53), PubMed Medline (n = 32), and ClinicalTrials.gov (n = 6). A total of 764 citations were retrieved for screening. We removed 742 citations as they were found to be duplicates and not eligible based on title/abstracts screening. Of 22 records screened for full-text eligibility, 17 studies were excluded based on the following reasons: seven articles were not using combination of vitamin C and vitamin E as the antioxidant component, six articles lacked data pertaining to the outcomes, and four articles were omitted as they were review articles. Ultimately, the remaining 5 randomized clinical trials (RCTs) [ 14 – 18 ] with a total of 338 endometriosis patients were included in the final analysis ( Fig 1 ). One RCT had triple-blinding method, one RCT had double-blinding method, and the remaining three RCTs did not specify the blinding methods they used. All but one RCT used the combination of vitamin C 1000 mg/day and vitamin E 1200 IU/day as the antioxidant component. These antioxidant or placebo were given to the patients with endometriosis for a total of 8 weeks. A comprehensive overview of the characteristics of each study included in this analysis was provided in Table 1 .
- PPT PowerPoint slide
- PNG larger image
- TIFF original image
https://doi.org/10.1371/journal.pone.0301867.g001
https://doi.org/10.1371/journal.pone.0301867.t001
3.2. Quality of study assessment
Out of the five randomized controlled trials (RCTs) that were included in the analysis, only one demonstrated a "low" risk of bias across all areas of the assessment as determined by the RoB v2 criteria. The four remaining RCTs were classified as having a "some-concern" risk of bias. This classification was based on the absence of clear explanations on the randomization techniques employed and/or inadequate information regarding any deviations from the intended interventions that occurred owing to the specific circumstances of the experiment. Fig 2 provides a comprehensive overview of the risk of bias associated with each RCT.
https://doi.org/10.1371/journal.pone.0301867.g002
3.3. Pain-Related outcomes
3.3.1. chronic pelvic pain (everyday pain)..
The findings of the meta-analysis, which included four randomized controlled trials (RCTs), indicate that antioxidant supplementation with a combination of vitamin C and vitamin E is linked to a higher proportion of endometriosis patients reporting reduced chronic pelvic pain (everyday pain) sensation during follow-up, compared to those who were administered a placebo (RR 7.30; 95%CI: 3.27–16.31, p <0.00001, I 2 = 0%, fixed-effect model) ( Fig 3A ). One RCT by Amini L et al. [ 15 ] reported the chronic pelvic pain (everyday pain) in the numeric scale changes of visual analog score (VAS) from baseline to follow-up. In this RCT, the chronic pelvic pain in the antioxidant group was 66.26 ± 27.84 before treatment then significantly reduced to 12.43 ± 13.28 during the last follow-up at week 8 (p<0.001) [ 15 ]. In contrast, within the placebo group, the baseline chronic pelvic pain score was recorded as 16.96 ± 16.28. However, rather than exhibiting a decrease, this score increased to 18.63 ± 18.35 by the eighth week of follow-up (p = 0.571) [ 15 ]. These results indicate the favorability of antioxidants in reducing chronic pelvic pain caused by endometriosis.
Forest plot that demonstrates antioxidant supplementation containing combination of vitamin C and vitamin E was associated with higher proportion of endometriosis patients who achieved reduction in the chronic pelvic pain (A), dysmenorrhea (B), and dyspareunia (C) symptoms.
https://doi.org/10.1371/journal.pone.0301867.g003
3.3.2. Dysmenorrhea.
The findings of the meta-analysis, which included four randomized controlled trials (RCTs), indicated a notable increase in the proportion of individuals who achieved a substantial alleviation of dysmenorrhea (menstrual discomfort) among those who were administered antioxidants comprising a mix of vitamin C and vitamin E, in comparison to those who got a placebo (RR 1.96; 95%CI: 1.25–3.07, p = 0.003, I 2 = 39%, fixed-effect model) ( Fig 3B ). A RCT by Amini L et al. [ 15 ] reported the dysmenorrhea outcome in the numeric scale changes of visual analog score (VAS) from baseline to follow-up. In this RCT, the menstrual pain (dysmenorrhea) in the antioxidant group was 50.53 ± 32.12 before treatment then significantly reduced to 17.56 ± 16.65 during the last follow-up at week 8 (p<0.001). In contrast, within the placebo group, the baseline dysmenorrhea VAS score was recorded as 51 ± 34.21 and then significantly reduced to 31.56 ± 26.39 by the eighth week of follow-up (p<0.001). However, the reductions in these VAS score of dysmenorrhea were greater in the antioxidant group than the placebo group (-32.37 vs. -19.44, p = 0.002). These results indicate the favorability of antioxidants in reducing menstrual pain (dysmenorrhea) caused by endometriosis.
3.3.3. Dyspareunia.
The findings of the meta-analysis, which included four randomized controlled trials (RCTs), indicated a notable increase in the proportion of individuals who achieved a substantial alleviation of dyspareunia (discomfort during sexual intercourse) among those who were administered antioxidants comprising a mix of vitamin C and vitamin E, in comparison to those who got a placebo (RR 5.08; 95%CI: 2.10–12.26, p = 0.0003, I 2 = 0%, fixed-effect model) ( Fig 3C ). In one included RCT that was conducted by Amini L et al. [ 15 ], the dyspareunia outcome was reported in the numeric scale changes of visual analog score (VAS) from baseline to follow-up. In this RCT, the sexual intercourse pain (dyspareunia) in the antioxidant group was 66.26 ± 28.27 before treatment then significantly reduced to 15.43 ± 18.47 during the last follow-up at week 8 (p<0.001). In contrast, within the placebo group, the baseline dyspareunia VAS score was recorded as 20.73 ± 21.77 and then slightly reduced to 18.1 ± 19.93 by the eighth week of follow-up (p<0.001). However, the reductions in these VAS score of dyspareunia were greater in the antioxidant group than the placebo group (-50.88 vs -2.63, p = 0.006). These results indicate the favorability of antioxidants in reducing menstrual pain (dysmenorrhea) caused by endometriosis.
3.4. Publication bias
Funnel plot analysis was employed to assess publication bias. The present investigation did not perform the assessment of publication bias due to the limited number of research included (less than 10 studies) in each outcomes of interest. Consequently, the evaluation of publication bias lacks the same level of robustness as when there are more than 10 studies available for analysis [ 19 , 20 ].
4. Discussion
The findings of our meta-analysis have confirmed our initial hypothesis where antioxidant supplementation containing vitamin C and vitamin E can reduce the pain symptoms, ranging from chronic pelvic pain, dysmenorrhea, and dyspareunia better than placebo in patients with endometriosis. As aforementioned pathophysiological process of pain development in endometriosis where oxidative stress serves as the culprit, vitamin C and vitamin E can halt this process by scavenging excess reactive oxygen species (ROS) because of their antioxidant properties [ 9 , 10 ].
Both vitamins are able to reduce the inflammatory process by inhibiting the production of several proinflammatory cytokines, such as tumor necrosis factor-alpha (TNF-α), interleukin-1 (IL-1), IL-6, and monocyte-chemotactic protein-1 which may be responsible for responsible for the release of pain-inducing molecules [ 9 , 21 , 22 ]. This inhibition of the inflammatory process is also obtained through the activity of vitamin C and vitamin E which reduce the activity of the cyclooxygenase (COX) enzyme so that it will reduce the process of converting arachidonic acid into prostaglandin E2 (PGE2) which is responsible for modulating pain [ 9 , 23 ]. In addition to inhibiting the inflammatory process, these two vitamins also play a role in reducing oxidative stress due to excess iron or iron deficiency through the regulatory function of iron metabolism [ 9 , 24 , 25 ]. It is this mechanism that underlies the ability of the combination of vitamin C and vitamin E to reduce pain in patients with endometriosis. The background for combining vitamin C with vitamin E is the possibility of a synergistic effect of the two vitamins so that they can strengthen each other’s ability to inhibit lipid peroxidation [ 26 ].
The findings of our study are consistent with previous research conducted by Sukan B et al. [ 27 ] and Zheng S et al. [ 28 ], which also demonstrate the efficacy of antioxidant vitamin supplementation in alleviating pain associated with endometriosis. However, both publications [ 27 , 28 ] discussed antioxidant vitamins in general, while our current work focuses only on the antioxidant capacity of a combination of vitamin C and vitamin E. Moreover, there exist further distinctions between the present investigation and the prior study conducted by Sukan B et al. [ 27 ]. The preceding investigation conducted by Sukan B et al. [ 27 ] is a systematic review without meta-analysis. Systematic review studies would certainly be better if equipped with a meta-analysis because then we can get new data in the form of numbers that can estimate how much influence the intervention has when compared to controls/placebo. Previous study by Sukan B et al. [ 27 ] also does not specifically discuss the ability of vitamin C and vitamin E in reducing pain, but also discusses other substances that have antioxidant capabilities such as caffeic acid, resveratrol, garlic tablets, and a combination of N-acetyl cysteine, alpha lipoic acid and bromelain. Combining these different substances into the meta-analysis will certainly cause significant heterogeneity, so for our current study we only focus on antioxidant supplementation containing a combination of vitamins C and vitamin E. Of the eight studies included in the previous investigation by Sukan B et al. [ 27 ] there are only 3 studies that discuss vitamin C and vitamin E. The remaining five studies discuss other antioxidant substances as previously mentioned [ 27 ]. Meanwhile, our study included a total of 5 RCTs into the analysis, all of which discussed the ability of vitamin C and vitamin E for endometriosis.
There are various limitations inherent in our investigation. Initially, it is noteworthy that all randomized controlled trials (RCTs) incorporated in the study exhibit a comparatively modest sample size, amounting to less than 100 participants. Furthermore, the studies included in the study did not provide sufficient data on changes in pain scores on the Visual Analog Scale (VAS) from baseline to follow-up, hence precluding their inclusion in the meta-analysis. Information regarding the type of endometriosis (e.g. superficial/deep/ovarian) and any co-existing adenomyosis from the included studies is also lacking, therefore cannot be analyzed further. Furthermore, it is important to note that pain is a multifaceted symptom that is influenced by various factors such as the specific location of the disease (e.g., parametrial, sacral plexus), prior surgical procedures, concurrent medical conditions (e.g., interstitial cystitis), as well as peripheral and central sensitization [ 29 ]. Therefore, obtaining this information would greatly enhance the quality of the evidence presented. Regrettably, the included research do not contain this information. In addition, it is worth noting that the randomized controlled trials (RCTs) included in the study had a limited follow-up period of about two months. Consequently, the investigation failed to capture any potential long-term impacts of vitamin C and vitamin E supplementation, specifically in relation to both effectiveness and safety. Ultimately, it is worth noting that a majority of the randomized controlled trials (RCTs) examined in this study, specifically four out of five, exhibit a level of bias that can be categorized as "some-concern." This bias mostly stems from inadequate allocation concealment during the randomization process. Consequently, it is imperative to exercise caution when interpreting the findings of our investigation.
The findings of our systematic review and meta-analysis indicate a potential ability of antioxidant supplementation containing combination of vitamin C and vitamin E in mitigating the pain symptoms that may range from chronic pelvic pain, dysmenorrhea, to dyspareunia in individuals diagnosed with endometriosis. However, further research is required to validate the results of our study by the implementation of meticulously prepared randomized controlled trials (RCTs). These studies should ideally have bigger sample sizes and longer durations to ensure the robustness and reliability of the findings.
Supporting information
https://doi.org/10.1371/journal.pone.0301867.s001
- View Article
- PubMed/NCBI
- Google Scholar
IMAGES
VIDEO
COMMENTS
Stress and Stress Management: A Review. November 2022; ... Stress management is a commonly used phrase with a simple definition. Many studies testing its effectiveness exist in the literature ...
Literature review: Individual: relaxation, CBT, exercise, time management, and employee assistance programme ... Six stress management intervention studies in UK and one in The Netherlands show that training in behavioural techniques improved levels of sickness in psychiatric nurses. Levels of psychological distress reduced following a 15 week ...
Method: A systematic search and review of the literature was used to summarize existing research related to stress management interventions for nurses and recommend directions for future research and practice. Results: Ninety articles met the inclusion criteria for this study and were categorized and analyzed for scientific rigor.
This literature review aimed to evaluate studies examining stress and wellbeing among international students. The review addressed the different types of stressors faced by international students, and some of the individual differences that play an important role in moderating both stress levels and wellbeing.
A literature review was published in 2009 that looked at all the trials till that time which had studied the effects of mindfulness-based stress reduction on stress management in nonclinical populations. 64 The study summarized the results from 10 such trials and found positive effects of mindfulness-based stress reduction though there were ...
The authors critically review the literature within an Allostatic Load framework, with a focus on primary (e.g., stress hormones, anxiety and tension) and secondary (e.g., resting blood pressure, cholesterol, body mass index) mediators, as well as tertiary disease end points (e.g., cardiovascular disease, depression, mortality).
A systematic review was conducted between January and September 2017. The studies considered were research articles dating from 2006 to 2017. To identify the relevant review literature, we chose a period spanning 11-years: January 2006-September 2017, as one of the most frequently cited review papers on stress interventions in the organizational setting is Lamontagne et al. (), which ...
Stress-management studies that were worksite based, assessed a health outcome, and were published in the peer-reviewed literature were included in this review. The main search method was the one described in the lead article to this special issue of the JOURNAL, but supplementary sources included prior reviews of the research literature and ...
A systematic review of stress and stress management interventions for mental health nurses. Journal of Advanced Nursing, 42 (2), 169-200. 10.1046/j.1365-2648.2003.02600.x ... Literature review of role stress/strain on nurses: An international perspective. Nursing & Health Sciences, 3 (3), ...
principally by either addressing the causes of stress or by reducing the impact of stress on an individual. The aim of this chapter is to review the literature on stress management interventions to establish what we know about the effectiveness of different interventions in improving psychological well-being. It is split into three main sections.
Stress among HCWs is pervasive, having been historically studied in advance of the COVID-19 pandemic. ... Stress, a concept that varies widely across the literature, can broadly be described as "what arises when something you care about is at stake" (McGonigal, ... Health Care Management Review, 32 (3), 203-212. 10.1097/01.HMR.0000281626. ...
How can machine learning be used in stress management: A systematic literature review of applications in workplaces and education. Author links open overlay panel Shivani Mittal, Sumedha Mahendra, Viraj Sanap, ... Our systematic review on stress management focuses on the techno-psychological aspect of the human being. In other words, it does ...
This systematic review and meta-analysis aimed to examine the effects of stress management interventions in reducing stress, depression, and anxiety among college students. Two separate meta-analyses of randomized controlled trials were conducted using the random-effects model, for students with high-stress levels ( n = 8) and for the ...
Methods. A single author (MP) searched PubMed and Google Scholar for peer-reviewed articles published at any time in English. Search terms included academic, school, university, stress, mental health, depression, anxiety, youth, young people, resilience, stress management, stress education, substance use, sleep, drop-out, physical health with a combination of any and/or all of the preceding terms.
systematic literature review of stress studies. This review includes the state-of-the-art knowledge of stress in domains such as definition, concepts, history, models, and ... and at least five years of experience in stress research and/or stress management) has been asked to give their written ideas about the theoretical issues of stress ...
Effective techniques for stress management are varied. They typically include behaviors that improve physical health, such as nutrition and exercise, but may also incorporate strategies that improve cognitive and emotional functioning. The stress-reduction approach based on mindfulness practices has recently enjoyed an explosion of interest from a variety of healthcare and epidemiological ...
Resident physicians are vital to the US healthcare system, but burnout rates among residents range from 17-94%, with variation by specialty and program [1, 2].Burnout is characterized by emotional exhaustion, depersonalization, and a reduced sense of personal accomplishment.[] External factors like demanding work environments, high patient care standards, long hours, poor work-life balance ...
Review criteria were met in 31 studies of 1,356 originally retrieved. Three broad categories of interventions emerged from the coding process: mindfulness-type ( n = 12), coping and solutions focused (CSF) ( n = 12) and reflective groups ( n = 7). There is evidence that these interventions can be successful to help doctors deal with stress.
Purpose This study aimed to develop a smartphone mobile application-based supportive return to work (RTW) program for cancer survivors and evaluate its effects on their RTW, fatigue, stress, and quality of working life. This program was developed through a comprehensive process involving literature review, interviews with cancer survivors, and consultations with experts. Methods A non ...
The study was carried out to review the effectiveness of stress management training on the academic life and mental well-being of the students of Shahed University. ... the literature review of the studies managed in Iran showed that few studies were performed on the factors promoting this important variable. Therefore, an attempt to address ...
Background The primary challenge encountered by individuals diagnosed with endometriosis is the experience of pain. Emerging research indicates that oxidative stress is implicated in the initiation of pain associated with endometriosis. Vitamins C and E are known for their antioxidative properties. The primary objective of this study is to assess the efficacy of antioxidant supplementation ...