- SUGGESTED TOPICS
- The Magazine
- Newsletters
- Managing Yourself
- Managing Teams
- Work-life Balance
- The Big Idea
- Data & Visuals
- Reading Lists
- Case Selections
- HBR Learning
- Topic Feeds
- Account Settings
- Email Preferences

It’s a New Era for Mental Health at Work
- Kelly Greenwood

Research on how the past 18 months have affected U.S. employees — and how companies should respond.
In 2019, employers were just starting to grasp the prevalence of mental health challenges at work, the need to address stigma, and the emerging link to diversity, equity, and inclusion (DEI). One silver lining amid all the disruption and trauma over the last two years is the normalization of these challenges. In a follow-up study of their 2019 Mental Health at Work Report, Mind Share Partners’ 2021 Mental Health at Work Report, the authors offer a rare comparison of the state of mental health, stigma, and work culture in U.S. workplaces before and during the pandemic. They also present a summary of what they learned and their recommendations for what employers need to do to support their employees’ mental health.
When we published our research on workplace mental health in October 2019, we never could have predicted how much our lives would soon be upended by the Covid-19 pandemic. Then the murders of George Floyd and other Black Americans by the police; the rise in violence against Asian Americans and Pacific Islanders (AAPIs); wildfires; political unrest; and other major stressors unfolded in quick succession, compounding the damage to our collective mental health.
- Kelly Greenwood is the Founder and CEO of Mind Share Partners , a national nonprofit changing the culture of workplace mental health so both employees and organizations can thrive. Through movement building , custom training, and strategic advising, it normalizes mental health challenges and promotes sustainable ways of working to create a mentally healthy workforce. Follow her on LinkedIn and subscribe to her monthly newsletter.
- Julia Anas is the chief people officer at Qualtrics, the world’s #1 Experience Management (XM) provider and creator of the XM category. At Qualtrics, she is responsible for building a talented and diverse organization and driving employee development as well as organizational design, talent, and succession planning.
Partner Center

Ellice Weaver / Wellcome
Understanding what works for workplace mental health: putting science to work
This report summarises what we’ve learned from our first commission on promising approaches for addressing workplace mental health. It also sets out why businesses and researchers need to work together to take a more scientific approach to supporting mental health at work.
- Share with Facebook
- Share with X
- Share with LinkedIn
- Share with Email
What’s inside
- findings from ten research projects that looked at the evidence behind promising approaches for supporting workplace mental health
- suggested actions businesses can take, based on this evidence
- reflections on gaps in the evidence and why it’s important for businesses and scientists to work together to understand what works.
Who this is for
- policy makers
- researchers.
Key findings
Businesses all over the world are thinking about how they can most effectively support the mental health of their staff. But despite growing interest and investment in workplace mental health initiatives in recent years, there is still so much we don't know about what works and what doesn’t.
In 2020, Wellcome commissioned ten global research teams to look at the existing evidence behind promising approaches for addressing anxiety and depression in the workplace, with a focus on younger workers.
Key findings include:
- Excessive sitting has risks for both physical and mental health. Reducing the time office workers spend sitting by an hour a day may reduce depression symptoms by approximately 10% and anxiety symptoms by around 15%.
- Flexible working can benefit mental health by decreasing the amount of conflict people experience between their work and home lives. This conflict can be a source of stress and may contribute to anxiety and depression.
- More job autonomy is associated with lower rates of anxiety and depression. Employers can increase employees' autonomy by allowing them more freedom to craft how they do their roles.
- There is significant evidence from high-income countries to show that workplace mindfulness interventions have a positive impact on mental health. But far less is known about their effectiveness in low- and middle-income countries.
The research identifies important gaps in our knowledge about what works. Businesses and scientists need to work together to fill these gaps in the evidence to understand how employers can most effectively support the mental health of their staff.
Downloads
Summary report.
- Putting science to work: understanding what works for workplace mental health PDF 7.3 MB
Individual research reports submitted to Wellcome
- Breaking up excessive sitting with light activity PDF 1.1 MB
- Buddying at onboarding PDF 1.2 MB
- Employee autonomy PDF 1.9 MB
- Financial wellbeing interventions PDF 1.1 MB
- Flexible working policies PDF 1.4 MB
- Group psychological first aid for humanitarian workers and volunteers PDF 1.3 MB
- Mental health peer support PDF 1.8 MB
- Mindfulness in hospitality and tourism in low- and middle-income countries PDF 1.8 MB
- Social support interventions for healthcare workers PDF 3.3 MB
- Workforce involvement and peer support networks in low- and middle-income countries PDF 1.4 MB
Contact us
For more information, contact Rhea Newman, Policy and Advocacy Adviser, at [email protected] .
Mental health
Related content .

Mental health at Wellcome: looking forward

Why science needs lived experiences of mental health challenges

Our Nation’s Current Workplace Landscape
Recent surveys suggest...
Written Document on Workplace Well‑Being
We can build workplaces that are engines of well-being, showing workers that they matter, that their work matters, and that they have the workplace resources and support necessary to flourish.
This 30-page Surgeon General’s Framework for Workplace Mental Health and Well-Being offers a foundation that workplaces can build upon. Download the document PDF or continue scrolling to learn more.

The Surgeon General’s Framework for Workplace Mental Health and Well‑Being
Centered on the worker’s voice and equity, these Five Essentials support workplaces as engines of well-being. Each essential is grounded in two human needs, shared across industries and roles. Creating a plan to enact these practices can help strengthen the essentials of workplace well‑being.

Explore the Framework
The first Essential of this Framework is Protection from Harm . Creating the conditions for physical and psychological safety is a critical foundation for ensuring workplace mental health and well-being. This Essential rests on two human needs: safety and security .
Safety is protecting all workers from physical and non-physical harm, including injury, illness, discrimination, bullying, and harassment.
Security is ensuring all workers feel secure financially and in their job future.
*Diversity, equity, inclusion and accessibility
The second Essential of the Framework is Connection and Community . Fostering positive social interactions and relationships in the workplace supports worker well-being. This Essential rests on two human needs: social support and belonging .
Social Support is having the networks and relationships that can offer physical and psychological help, and can mitigate feelings of loneliness and isolation.
Belonging is the feeling of being an accepted member of a group.
The third Essential of this Framework is Work-Life Harmony . Professional and personal roles can together create work and non-work conflicts. The ability to integrate work and non-work demands, for all workers, rests on the human needs of autonomy and flexibility .
Autonomy is how much control a worker has over when, where, and how they do their work.
Flexibility is ability of workers to work when and where is best for them.
The fourth Essential of the Framework is Mattering at Work . People want to know that they matter to those around them and that their work matters. Knowing you matter has been shown to lower stress, while feeling like you do not can raise the risk for depression. This Essential rests on the human needs of dignity and meaning .
Dignity is the sense of being respected and valued.
Meaning in the workplace can refer to the sense of broader purpose and significance of one’s work.
The final Essential of this Framework is Opportunity for Growth . When organizations create more opportunities for workers to accomplish goals based on their skills and growth, workers become more optimistic about their abilities and more enthusiastic about contributing to the organization. This Essential rests on the human needs of learning and a sense of accomplishment .
Learning is the process of acquiring new skills and knowledge in the workplace.
Accomplishment is the outcome of meeting goals and having an impact.
Conclusion & Next Steps
The Surgeon General’s Framework for Workplace Mental Health and Well-Being emphasizes the connection between the well-being of workers and the health of organizations. It offers a foundation and resources that can be used by workplaces of any size, across any industry. Sustainable change must be driven by committed leaders in continuous collaboration with the valued workers who power each workplace. The most important asset in any organization is its people. By choosing to center their voices, we can ensure that everyone has a platform to thrive.
Resources for Supporting Workplace Well‑Being
Visit our resources page to find more information about how to implement the framework in your workplace.
Key Downloads
Essentials for Workplace Mental Health and Well-Being Graphic
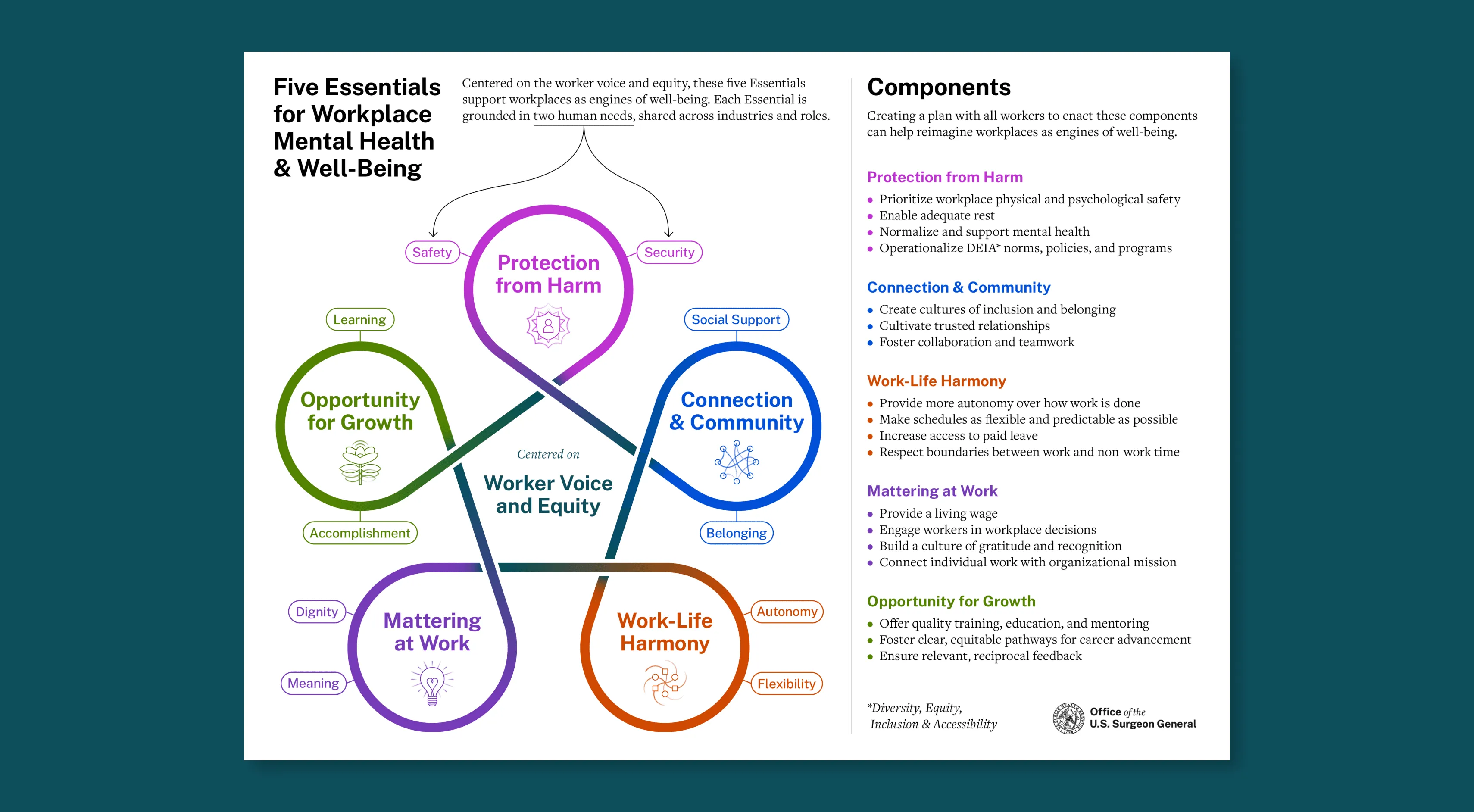
This graphic communicates the Five Essentials for Workplace Mental Health and Well-Being and their respective human needs and components, shared across industries and roles.
Workplace Mental Health and Well-Being Reflection Questions Deck

This is a deck of questions to help leaders reflect on their workplaces and start designing organizational policy and culture around the Five Essentials for Workplace Mental Health & Well-Being.
Official websites use .gov
A .gov website belongs to an official government organization in the United States.
Secure .gov websites use HTTPS
A lock ( ) or https:// means you've safely connected to the .gov website. Share sensitive information only on official, secure websites.
Mental Health in the Workplace
Mental Health Disorders and Stress Affect Working-Age Americans
This issue brief is available for download [PDF – 2 MB]
Mental health disorders are among the most burdensome health concerns in the United States. Nearly 1 in 5 US adults aged 18 or older (18.3% or 44.7 million people) reported any mental illness in 2016.2 In addition, 71% of adults reported at least one symptom of stress, such as a headache or feeling overwhelmed or anxious. 4
Many people with mental health disorders also need care for other physical health conditions, including heart disease, diabetes, respiratory illness, and disorders that affect muscles, bones, and joints. 5–8 The costs for treating people with both mental health disorders and other physical conditions are 2 to 3 times higher than for those without co-occurring illnesses. 9 By combining medical and behavioral health care services, the United States could save $37.6 billion to $67.8 billion a year. 9
About 63% of Americans are part of the US labor force.10 The workplace can be a key location for activities designed to improve well-being among adults. Workplace wellness programs can identify those at risk and connect them to treatment and put in place supports to help people reduce and manage stress. By addressing mental health issues in the workplace, employers can reduce health care costs for their businesses and employees.

Mental Health Issues Affect Businesses and Their Employees
Poor mental health and stress can negatively affect employee:
- Job performance and productivity.
- Engagement with one’s work.
- Communication with coworkers.
- Physical capability and daily functioning.
Mental illnesses such as depression are associated with higher rates of disability and unemployment.
- Depression interferes with a person’s ability to complete physical job tasks about 20% of the time and reduces cognitive performance about 35% of the time. 11
- Only 57% of employees who report moderate depression and 40% of those who report severe depression receive treatment to control depression symptoms. 12
Even after taking other health risks—like smoking and obesity—into account, employees at high risk of depression had the highest health care costs during the 3 years after an initial health risk assessment. 13,14

Employers Can PROMOTE Awareness About the Importance of Mental Health and Stress Management
Workplace health promotion programs have proven to be successful, especially when they combine mental and physical health interventions.
The workplace is an optimal setting to create a culture of health because:
- Communication structures are already in place.
- Programs and policies come from one central team.
- Social support networks are available.
- Employers can offer incentives to reinforce healthy behaviors.
- Employers can use data to track progress and measure the effects.

Action steps employers can take include:
- Make mental health self-assessment tools available to all employees.
- Offer free or subsidized clinical screenings for depression from a qualified mental health professional, followed by directed feedback and clinical referral when appropriate.
- Offer health insurance with no or low out-of-pocket costs for depression medications and mental health counseling.
- Provide free or subsidized lifestyle coaching, counseling, or self-management programs.
- Distribute materials, such as brochures, fliers, and videos, to all employees about the signs and symptoms of poor mental health and opportunities for treatment.
- Host seminars or workshops that address depression and stress management techniques, like mindfulness, breathing exercises, and meditation, to help employees reduce anxiety and stress and improve focus and motivation.
- Create and maintain dedicated, quiet spaces for relaxation activities.
- Provide managers with training to help them recognize the signs and symptoms of stress and depression in team members and encourage them to seek help from qualified mental health professionals.
- Give employees opportunities to participate in decisions about issues that affect job stress.
Success Stories
Many Businesses PROVIDE Employees With Resources to Improve Mental Health and Stress Management
Prudential Financial 15
- Monitors the effect of supervisors on worker well-being, especially when supervisors change.
- Conducts ongoing, anonymous surveys to learn about attitudes toward managers, senior executives, and the company as a whole.
- Normalizes discussion of mental health by having senior leadership share personal stories in video messages.
TiER1 Performance Solutions 16
- Focuses on six key health issues: depression, anxiety, obsessive-compulsive disorder, schizophrenia, bipolar disorder, and addictions as part of its Start the Conversation about Mental Illness awareness campaign.
- Provides resources to assess risk, find information, and get help or support using multiple formats to increase visibility and engagement. For example, information is provided as infographics, e-mails, weekly table tents with reflections and challenges, and videos (educational and storytelling).
Beehive PR 17
- Maintains the “InZone,” a dedicated quiet room that is not connected to a wireless internet signal, which gives employees a place to recharge.
- Combines professional and personal growth opportunities through goal-setting, one-on-one coaching, development sessions, and biannual retreats.
Tripler Army Medical Center 18
- Requires resiliency training to reduce burnout and increase skills in empathy and compassion for staff members who are in caregiver roles. Training sessions mix classroom-style lectures, role-playing, yoga, and improvisational comedy to touch on multiple learning styles.
Certified Angus Beef 19
- Provides free wellness consultations by an on-site clinical psychologist. Employees do not have to take leave to access these services.
- Holds lunchtime learning sessions to reduce stigma about mental health and the services available to employees.
- Offers quarterly guided imagery relaxation sessions to teach stress management strategies.

Houston Texans 20
- Provides comprehensive and integrated physical, mental, and behavioral health insurance coverage, including round-the-clock access to employee assistance program (EAP) services.
- Extends EAP access to anyone living in an employee’s home, with dedicated programming for those who are caring for children or elderly parents.

What Can Be Done?
Strategies for Managing Mental Health and Stress in the Workplace
Health care providers can:
- Ask patients about any depression or anxiety and recommend screenings, treatment, and services as appropriate.
- Include clinical psychologists, social workers, physical and occupational therapists, and other allied health professionals as part of core treatment teams to provide comprehensive, holistic care.
Public health researchers can:
- Develop a “how-to” guide to help in the design, implementation, and evaluation of workplace health programs that address mental health and stress issues.
- Create a mental health scorecard that employers can use to assess their workplace environment and identify areas for intervention.
- Develop a recognition program that rewards employers who demonstrate evidence-based improvements in metrics of mental health and well-being and measurable business results.
- Establish training programs in partnership with business schools to teach leaders how to build and sustain a mentally healthy workforce.
Community leaders and businesses can:
- Promote mental health and stress management educational programs to working adults through public health departments, parks and recreational agencies, and community centers.
- Support community programs that indirectly reduce risks, for example, by increasing access to affordable housing, opportunities for physical activity (like sidewalks and trails), tools to promote financial well-being, and safe and tobacco-free neighborhoods.
- Create a system that employees, employers, and health care providers can use to find community-based programs (for example, at churches and community centers) that address mental health and stress management.
Federal and state governments can:
- Provide tool kits and materials for organizations and employers delivering mental health and stress management education.
- Provide courses, guidance, and decision-making tools to help people manage their mental health and well-being.
- Collect data on workers’ well-being and conduct prevention and biomedical research to guide ongoing public health innovations.
- Promote strategies designed to reach people in underserved communities, such as the use of community health workers to help patients access mental health and substance abuse prevention services from local community groups (for example, churches and community centers).

Employees can:
- Encourage employers to offer mental health and stress management education and programs that meet their needs and interests, if they are not already in place.
- Participate in employer-sponsored programs and activities to learn skills and get the support they need to improve their mental health.
- Serve as dedicated wellness champions and participate in trainings on topics such as financial planning and how to manage unacceptable behaviors and attitudes in the workplace as a way to help others, when appropriate.
- Share personal experiences with others to help reduce stigma, when appropriate.
- Be open-minded about the experiences and feelings of colleagues. Respond with empathy, offer peer support, and encourage others to seek help.
- Adopt behaviors that promote stress management and mental health.
- Eat healthy, well-balanced meals, exercise regularly, and get 7 to 8 hours of sleep a night.
- Take part in activities that promote stress management and relaxation, such as yoga, meditation, mindfulness, or tai chi.
- Build and nurture real-life, face-to-face social connections.
- Take the time to reflect on positive experiences and express happiness and gratitude.
- Set and work toward personal, wellness, and work-related goals and ask for help when it is needed.
Any mental illness is defined as having any mental, behavioral, or emotional disorder in the past year that met Diagnostic and Statistical Manual of Mental Disorders IV (DSM-IV) criteria (excluding developmental disorders and substance use disorders). Mental illness can vary in impact, ranging from no impairment to mild, moderate, and even severe impairment.
Mindfulness is a psychological state of moment-to-moment awareness of your current state without feeling inward judgement about your situation. Mindfulness can be achieved through practices foster control and develop skills such as calmness and concentration.
Self-management is a collaborative, interactive, and ongoing process that involves educators and people with health problems. The educator provides program participants with the information, problem-solving skills, and tools they need to successfully manage their health problems, avoid complications, make informed decisions, and engage in healthy behaviors. These programs can be provided in person, over the phone, or online.
- Substance Abuse and Mental Health Services Administration. Behavioral Health Spending & Use Accounts, 1986-2014. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2016. HHS publication SMA-16-4975.
- National Institute of Mental Health. Mental illness website. https://www.nimh.nih.gov/health/statistics/mental-illness.shtml . Accessed March 29, 2018.
- Centers for Disease Control and Prevention. Data table for Figure 16. Health care visits in the past 12 months among children aged 2-17 and adults aged 18 and over, by age and provider type: United States, 1997, 2006, and 2015. https://www.cdc.gov/nchs/data/hus/2016/fig16.pdf [PDF – 898 KB] . Accessed July 3, 2018.
- American Psychological Association. Stress in America: Coping with Change, Part 1. Washington, DC: American Psychological Association; 2017.
- Merikangas KR, Ames M, Cui L, Ustun TB, Von Korff M, Kessler RC. The impact of comorbidity of mental and physical conditions on role disability in the US adult household population. Arch Gen Psychiatry . 2007;64(10):1180–1188.
- Scott KM, Lim C, Al-Hamzawi A, et al. Association of mental disorders with subsequent chronic physical conditions: work mental health surveys from 17 countries. JAMA Psychiatry . 2016;73(2):150–158.
- Glassman AH. Depression and cardiovascular comorbidity. Dialogues Clin Neurosci . 2007;9(1):9–17.
- Luppino FS, de Wit LM, Bouvy PF, et al. Overweight, obesity, and depression: a systematic review and meta-analysis of longitudinal studies. Arch Gen Psychiatry . 2010;67(3):220–229.
- Melek SP, Norris DT, Paulus J, Matthews K, Weaver A, Davenport S. Potential Economic Impact of Integrated Medical-Behavioral Healthcare: Updated Projections for 2017. Milliman Research Report. Seattle, WA: Milliman, Inc.; 2018.
- US Department of Labor, Bureau of Labor Statistics. Databases, Tables & Calculators by Subject website. Labor force statistics from the Current Population Survey. https://data.bls.gov/timeseries/LNS11300000 . Accessed July 3, 2018.
- Lerner D, Henke RM. What does research tell us about depression, job performance, and work productivity? J Occup Environ Med . 2008;50(4):401–410.
- Dewa CS, Thompson AH, Jacobs P. The association of treatment of depressive episodes and work productivity. Can J Psychiatry . 2011;56(12):743–750.
- Goetzel RZ, Anderson DR, Whitmer RW, et al; Health Enhancement Research Organization (HERO) Research Committee. The relationship between modifiable health risks and health care expenditures: an analysis of the multi-employer HERO health risk and cost database. J Occup Environ Med . 1998;40(10):843–854.
- Goetzel RZ, Pei X, Tabrizi MJ, et al. Ten modifiable health risk factors are linked to more than one-fifth of employer-employee health care spending. Health Aff . 2012;31(11):2474–2484.
- American Psychological Association, Center for Organizational Excellence. The Awards website. Prudential Financial. http://www.apaexcellence.org/awards/organizational-excellence/oea2017 . Accessed July 3, 2018.
- American Psychiatric Association, Center for Workplace Mental Health. The Awards website. TiER1 Performance Solutions. http://workplacementalhealth.org/Case-Studies/Tier1PerformanceSolutions . Accessed July 3, 2018.
- American Psychological Association, Center for Organizational Excellence. The Awards website. Beehive PR. http://www.apaexcellence.org/awards/national/winner/54 . Accessed July 3, 2018.
- American Psychological Association, Center for Organizational Excellence. The Awards website. Resiliency Training. http://www.apaexcellence.org/awards/bphonors/winner/99 . Accessed July 3, 2018.
- American Psychological Association, Center for Organizational Excellence. The Awards website. Setting the Bar for Emotional Wellness. http://www.apaexcellence.org/awards/bphonors/winner/86 . Accessed July 3, 2018.
- American Psychiatric Association, Center for Workplace Mental Health. Case Study website. Houston Texans. http://workplacementalhealth.org/Case-Studies/Houston-Texans . Accessed July 3, 2018.
To receive email updates about Workplace Health Promotion, enter your email address:
Exit Notification / Disclaimer Policy
- The Centers for Disease Control and Prevention (CDC) cannot attest to the accuracy of a non-federal website.
- Linking to a non-federal website does not constitute an endorsement by CDC or any of its employees of the sponsors or the information and products presented on the website.
- You will be subject to the destination website's privacy policy when you follow the link.
- CDC is not responsible for Section 508 compliance (accessibility) on other federal or private website.
The Role of Mental Health on Workplace Productivity: A Critical Review of the Literature
- Review Article
- Published: 15 November 2022
- Volume 21 , pages 167–193, ( 2023 )
Cite this article

- Claire de Oliveira ORCID: orcid.org/0000-0003-3961-6008 1 , 2 , 3 , 4 ,
- Makeila Saka 2 ,
- Lauren Bone 2 &
- Rowena Jacobs ORCID: orcid.org/0000-0001-5225-6321 1
23k Accesses
20 Citations
124 Altmetric
14 Mentions
Explore all metrics
Mental health disorders in the workplace have increasingly been recognised as a problem in most countries given their high economic burden. However, few reviews have examined the relationship between mental health and worker productivity.
To review the relationship between mental health and lost productivity and undertake a critical review of the published literature.
A critical review was undertaken to identify relevant studies published in MEDLINE and EconLit from 1 January 2008 to 31 May 2020, and to examine the type of data and methods employed, study findings and limitations, and existing gaps in the literature. Studies were critically appraised, namely whether they recognised and/or addressed endogeneity and unobserved heterogeneity, and a narrative synthesis of the existing evidence was undertaken.
Thirty-eight (38) relevant studies were found. There was clear evidence that poor mental health (mostly measured as depression and/or anxiety) was associated with lost productivity (i.e., absenteeism and presenteeism). However, only the most common mental disorders were typically examined. Studies employed questionnaires/surveys and administrative data and regression analysis. Few studies used longitudinal data, controlled for unobserved heterogeneity or addressed endogeneity; therefore, few studies were considered high quality.
Despite consistent findings, more high-quality, longitudinal and causal inference studies are needed to provide clear policy recommendations. Moreover, future research should seek to understand how working conditions and work arrangements as well as workplace policies impact presenteeism.
Similar content being viewed by others

Is working in later life good for your health? A systematic review of health outcomes resulting from extended working lives

Workplace Intervention Research: Disability Prevention, Disability Management, and Work Productivity
Researching complex and multi-level workplace factors affecting disability and prolonged sickness absence.
Avoid common mistakes on your manuscript.
1 Introduction
Mental health disorders in the workplace, such as depression and anxiety, have increasingly been recognised as a problem in most countries. Using a human capital approach, the global economic burden of mental illness was estimated to be US$$2.5 trillion in 2010 increasing to US$$6.1 trillion in 2030; most of this burden was due to lost productivity, defined as absenteeism and presenteeism [ 1 ]. Workplaces that promote good mental health and support individuals with mental illnesses are more likely to reduce absenteeism (i.e., decreased number of days away from work) and presenteeism (i.e., diminished productivity while at work), and thus increase worker productivity [ 2 ]. Burton et al. provided a review of the association between mental health and worker productivity [ 3 ]. The authors found that depressive disorders were the most common mental health disorder among most workforces and that most studies examined found a positive association between the presence of mental health disorders and absenteeism (particularly short-term disability absences). They also found that workplace policies that provide employees with access to evidence-based care result in reduced absenteeism, disability and lost productivity [ 3 ].
However, this review is now outdated. Prevalence rates for common mental disorders have increased [ 4 ], while workplaces have also responded with attempts to reduce stigma and the potential economic impact [ 5 ], necessitating the need for an updated assessment of the evidence. Furthermore, given that most of the global economic burden of mental illness is due to lost productivity [ 1 ], it is important to have a good understanding of the existing literature on this outcome. While the previous review focused on the prevalence of certain mental health conditions and the available interventions and workplace policies, this review focused on the measures of lost productivity and the instruments used, as well as the data and methods employed, which the previous review did not examine in depth. Thus, the objectives of this paper were to update the Burton et al. review [ 3 ] on the association between mental health and lost productivity, and undertake a critical review of the literature that has been published since then, specifically how researchers have studied this relationship, the type of data and databases they have employed, the methods they have used, their findings, and the existing gaps in the literature.
We undertook a critical review, i.e., a review that presents, analyses and synthesises evidence from diverse sources by extensively searching the literature and critically evaluating its quality [ 6 ], ultimately identifying the most significant papers in the field. Footnote 1 We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement [ 7 ] to guide our analysis. Our review focused on all studies published since 2008, which examined the relationship between mental health and workplace-related productivity among working-age adults. We used the Population, Intervention, Control, Outcomes, and Study design (known as PICOS) criteria to guide the development of the search strategy.
2.1 Eligibility Criteria
The populations of interest comprised working-age adults (18–65 years old). Studies focusing solely on volunteers and/or caregivers (i.e., unpaid workers) were excluded. The intervention(s), or rather more appropriately the exposure(s), had to be a diagnosis of any mental disorder/illness or self-reported mental health problem(s). Any studies that examined substance use and/or physical health in addition to mental health were included if results were reported separately for mental health-related outcomes. The control or comparator group, where applicable, included working age individuals without a mental disorder/illness or mental health problem(s). The outcome(s) included lost workplace productivity measured by absenteeism, presenteeism, sick leave, short- and/or long-term disability, or job loss. Studies that examined productivity of home-related activities (e.g., housework) were excluded. Studies with an observational study design and/or regression analysis were included; randomised control trials, cost-of-illness studies and economic evaluations were excluded (the first two were only included if they examined the relationship between mental health and lost productivity). Only original studies were considered; however, relevant reviews were retained for reference checking to find relevant studies, which may not have been captured by the search strategy.
2.2 Search Strategy
We searched literature published in English from 1 January 2008 to 31 May 2020. Structured searches were done in MEDLINE and EconLit to capture the most relevant literature published in the medical and economics fields, respectively. We also undertook relevant searches in Google and on specific websites of interest (e.g., UK Parliament Hansard, the National Institute for Health and Care Excellence, the Centre for Mental Health, the Health Foundation, the Institute for Fiscal Studies and the King’s Fund) and a hand search of the references of key papers [ 8 ]. Search terms or strings were developed on the basis of four concepts: population or workplace, intervention/exposure (i.e., presence of mental disorder/illness), work-related outcomes, and study design (see Table 1 ).
2.3 Study Selection
After duplicate records were removed, one reviewer (LB) screened all titles and abstracts while additional reviewers (CdO and RJ) were brought in for discussion, if/where necessary. Articles were excluded either because they did not examine the relationship between mental health and lost productivity (e.g., some cost-of-illness studies) or were mainly focused on physical health. Subsequently, all relevant full-text articles were retrieved and screened by one reviewer (LB) to confirm eligibility; additional reviewers (MS, RJ or CdO) were brought in, if/where necessary.
2.4 Data Extraction
Two reviewers (LB and MS) undertook the data extraction, and an additional reviewer (RJ or CdO) was assigned to resolve any disagreements. The research team developed a data extraction form, based on the Cochrane good practice data extraction form, which included study information (author(s), year of publication), country (where the study was published or conducted), aims of study, study design (cross-sectional, longitudinal), data source(s) (i.e., database(s), surveys/questionnaires), study population (sample size, age range), mental disorder(s) examined, workplace outcome examined (absenteeism, presenteeism, short-term disability, long-term disability, job loss, other), methods employed (statistical analysis, regression model employed), and results/key findings.
2.5 Quality Assessment
We reviewed the methods employed in the studies to assess their quality and robustness, drawing loosely on the Newcastle–Ottawa Scale, a risk-of-bias assessment tool for observational studies [ 9 ]. We paid particular attention to whether studies were able to move beyond simple associations and attempted to address causal inference, where necessary, and whether they took account of endogeneity (i.e., cases where the explained variable and the explanatory variable are determined simultaneously) and/or unobserved heterogeneity (i.e., cases where the presence of unexplained (observed) differences between individuals are associated with the (observed) variables of interest), which are common issues when examining the relationship between mental health and lost productivity. All studies that recognised and/or accounted for these issues were considered high quality. We also examined the type of data/databases employed (i.e., cross-sectional or longitudinal data and representative, population-based samples), findings, and limitations (and the extent to which these impacted the findings), which were also considered when determining the quality of a study.
2.6 Data Synthesis
Given the heterogeneity of studies examined, undertaking a meta-analysis was not possible. Therefore, we undertook a narrative synthesis of the relevant literature, where we synthesised the existing evidence by mental disorder/illness and workplace outcome (absenteeism, presenteeism, sick leave, short- and long-term disability, or job loss), if/where appropriate.
3.1 Study Selection
After all citations were merged and duplicates removed, our search produced 648 unique records, of which 89 full texts were assessed; four studies were obtained from other sources (e.g., Google searches). Ultimately, 38 studies were included in the final review [ 10 , 11 , 12 , 13 , 14 , 15 , 16 , 17 , 18 , 19 , 20 , 21 , 22 , 23 , 24 , 25 , 26 , 27 , 28 , 29 , 30 , 31 , 32 , 33 , 34 , 35 , 36 , 37 , 38 , 39 , 40 , 41 , 42 , 43 , 44 , 45 , 46 , 47 ] (see Fig. 1 ) and relevant data were extracted (see Table 2 and Table A1 in the Appendix for more details).

PRISMA flow diagram
3.2 Overview of Studies
All studies focused on individuals typically between the ages of 18 and 64/65 years. Some studies ( n = 5) examined individuals 20 or 25 years and older [ 11 , 12 , 16 , 28 , 38 ] to account for younger individuals who might still be in school and thus not working, while other studies had different lower and upper age limits (e.g., age 15 [ 25 , 47 ] and age 60 [ 11 , 38 ] years, respectively). Most studies were from the USA ( n = 10; 26%) and the Netherlands ( n = 6; 16%); this result is line with the findings from a review of economic evaluations of workplace mental health interventions [ 48 ]. The remaining studies were from Australia ( n = 4), Japan ( n = 4), South Korea ( n = 3), multiple countries ( n = 4), Brazil ( n = 1), Colombia ( n = 1), Denmark ( n = 1), Finland ( n = 1), Norway ( n = 1), Singapore ( n = 1), and the United Kingdom ( n = 1). Many studies did not specify the setting or industry or state the size of the firm where the study was undertaken (also found elsewhere [ 48 ]); consequently, this information was not included in the data extraction form.
3.3 Measures and Instruments/Tools Used
3.3.1 mental health.
Most studies ( n = 16) examined depression/depressive symptoms, major depressive disorder or other mood disorders (see Fig. 2 ). Two studies examined anxiety and five studied both anxiety and depression. A smaller number of studies examined other disorders—three studies examined attention-deficit hyperactivity disorder (ADHD), two studies focused on bipolar disorder, one examined panic disorder, one studied binge-eating disorder, and one looked at other disorders including mental disorders (depressive symptoms and cognitive function). Three studies looked at mental health broadly speaking (two studies examined poor mental health and another studied common mental disorders). Finally, four studies examined multiple mental disorders (e.g., depression, bipolar disorder, anxiety disorders, emotional disorders, substance use disorders, ADHD). Some studies used a binary indicator for the presence/absence of a mental disorder/poor mental health, while other analyses used different aggregate measures of mental illness or psychological distress, based on the number of recorded symptoms.

Studies by mental disorder. ADHD attention-deficit hyperactivity disorder
A variety of instruments/tools were used to measure mental health, depending on the disorder. Depression was measured using the Kessler Psychological Distress Scale (K6 scale) [ 49 ], Patient Health Questionnaire (PHQ-9) depression scale [ 50 ], Center for Epidemiologic Studies Depression Scale (CES-D) [ 51 ], Short General Health Questionnaire (GHQ-12) [ 52 ], Major Depression Inventory (MDI) [ 53 ], Hamilton Rating Scale for Depression (HAM-D) [ 54 ], and Mental Health Inventory (MHI-5) [ 55 ]. In studies that examined both anxiety and depression ( n = 2), the authors used either the Hospital Anxiety and Depression Scale (HADS) [ 56 ] or the Composite International Diagnostic Interview (CIDI) [ 57 ]. In one study [ 42 ], severity of anxiety and depressive symptoms was assessed using the Beck Anxiety Inventory [ 58 ] and the Inventory for Depressive Symptomatology questionnaire [ 59 ], respectively. In another study [ 33 ], mood disorder was measured using the Mood Disorder Questionnaire (MDQ) [ 60 ]. In one study [ 41 ], ADHD was assessed using the WHO World Mental Health (WMH) survey [ 61 ]; in another [ 35 ], it was assessed using the WHO Adult ADHD Self-Report Scale [ 62 ]. Panic disorders were measured using the Panic Disorder Severity Scale [ 63 ] in one study [ 16 ].
3.3.2 Lost Productivity
Nineteen studies examined both absenteeism and presenteeism, eight studies examined absenteeism only, two studies examined presenteeism only, and nine examined other or several workplace outcomes, such as employment, absenteeism, presenteeism, workplace accidents/injuries, short- and/or long-term disability, activity impairment and/or job loss (see Fig. 3 ).

Studies by workplace outcome
Five studies used the Work Productivity and Activity Impairment (WPAI) questionnaire [ 64 ] (Beck et al. [ 27 ], Jain et al. [ 36 ], Able et al. [ 30 ], Asami et al. [ 31 ], Ling et al. [ 44 ]); three used the WHO’s Health and Work Performance Questionnaire (HWP) [ 65 ] (Hjarsbech et al. [ 18 ], Woo et al. [ 38 ], Park et al. [ 16 ]) to determine absenteeism and presenteeism. A recent systematic review also found that that the WPAI was most frequently applied in economic evaluations and validation studies to measure lost productivity [ 66 ]. Two studies [ 12 , 20 ] used the Work Limitations Questionnaire [ 67 ]. Other studies used a variety of different instruments to measure lost productivity, such as the Trimbos/iMTA questionnaire for Costs Associated with Psychiatric illness (TiC-P) [ 68 ] (Bokma et al. [ 26 ]), the Short-Form Health and Labour Questionnaire [ 69 ] (Bouwmans et al. [ 45 ]), the WHO Disability Assessment Schedule (WHO-DAS) [ 70 ] (de Graaf et al. [ 23 ]) and the Endicott Work Productivity Scale [ 71 ] (McMorris et al. [ 33 ]). One study [ 43 ] made use of four work performance measures to examine lost productivity: WPAI [ 64 ], Work Limitations Questionnaire (WLQ) [ 66 ], Endicott Work Productivity Scale (EWPS) [ 71 ] and Functional Status Questionnaire Work Performance Scale (WPS) [ 72 ].
3.4 Data Sources and Methods
Most studies ( n = 20) employed data collected through surveys/questionnaires, though some used publicly available datasets, such as the Medical Expenditure Panel Survey [ 29 ], the National Comorbidity Survey Replication [ 28 ] and the National Latino and Asian American Study [ 28 ], the US National Health and Wellness Survey [ 44 ], the Household, Income and Labour Dynamics in Australia survey [ 25 , 47 ], and the Singapore Mental Health Study [ 24 ]. One study used administrative claims data [ 32 ]. Three studies made use of linked data, such as Hjarsbech et al. [ 18 ], which linked questionnaires to the Danish National Register of Social Transfer Payments; Erickson et al. [ 43 ], which utilised questionnaires linked to medical records, and Mauramo et al. [ 34 ], which used survey data from the Helsinki Health Study linked to employer's register data on sickness absence. Only one study employed trial data [ 45 ]. Most studies ( n = 29; 76%) employed cross-sectional data; few used longitudinal data ( n = 9; 24%).
3.4.2 Methods
Several studies ( n = 8) used regression analysis to examine the relationship between mental health and lost productivity, namely linear regression [ 11 , 17 ] and logistic regression models [ 25 , 29 , 42 , 45 ]. Two studies employed two-part models, where the first part examined the probability/odds of workers experiencing absenteeism, while the second part modeled the number of hours of absenteeism [ 10 ] or the number of work days missed [ 29 ]. One paper employed Poisson regressions to model the rate of work-lost days (absenteeism) and work-cut days (presenteeism) [ 34 ]. Another study computed Kaplan–Meier survival curves to estimate the mean and median duration of sickness absence due to depressive symptoms [ 40 ], and one estimated a Cox's proportional hazards model to analyse whether and to what extent depressive symptoms at baseline predicted time to onset of first long-term sickness absence during the 1-year follow-up period [ 18 ]. Only one study employed instrumental variables to address the potential endogeneity of the mental illness variable employed [ 28 ] and four employed longitudinal data models [ 13 , 20 , 25 , 47 ].
3.5 Evidence Synthesis
Almost all studies ( n = 36) found a positive (and, many times, a strong) association between the presence of mental illness/disorders or poor mental health and productivity loss measured by absenteeism and/or presenteeism. Nevertheless, there were a few exceptions—one study found that mood disorders were associated with decreased presenteeism (i.e., work performance) but found no significant relationship between mood disorders and absenteeism [ 11 ]. Another study found that individuals with binge-eating disorders reported greater levels of presenteeism and lost productivity than those without but found no effect for absenteeism [ 44 ].
Many studies ( n = 6) on depression examined both absenteeism and presenteeism where the presence of the former was positively associated with the latter (as was the case for studies, which examined only absenteeism and only presenteeism), and the latter was higher among those with higher severity of depression. These findings held in studies examining major depressive disorder and bipolar disorder (though one study found that symptoms of mania or hypomania were not significantly associated with absenteeism) [ 14 ]. Studies examining depression and anxiety (and anxiety alone, including panic disorder) generally examined both absenteeism and presenteeism and found that these disorders were significantly associated with lost productivity. One study found that workers with binge-eating disorder reported greater levels of presenteeism than those without but no differences in absenteeism. All studies on ADHD ( n = 3) examined both absenteeism and presenteeism and found ADHD was associated with more days of missed work and poor work performance. Studies looking at mental health (broadly defined) typically examined absenteeism only, finding a positive relationship between both, though the magnitude of the effect was found to be modest in one study [ 47 ]. Studies examining multiple disorders ( n = 4) also examined both absenteeism and presenteeism. Overall, having a mental disorder was positively associated with lost productivity; however, one study found no significant relationship between mood disorders and alcohol use/dependence and absenteeism [ 11 ].
Many studies ( n = 6) found that higher severity of the disorder or co-occurring mental health conditions was associated with greater productivity loss. For example, Knudsen et al. found that while comorbid anxiety and depression and anxiety alone were significant risk factors for absenteeism, depression alone was not [ 37 ].
Some studies examined outcomes separately for men and women ( n = 5) or examined specific groups ( n = 1). For example, Ammerman et al. examined high-risk, low-income mothers with major depression and found that depression significantly increased the likelihood of absenteeism (i.e., missing workdays) among this group [ 29 ]. However, beyond gender, studies did not report on differences by ethnicity/race and/or age.
Overall, we found that the literature on this topic continues to examine the most common mental disorders (e.g., depression and anxiety) using similar data sources and analysis techniques as the Burton et al. review [ 3 ] (see Table 3 ). However, more recent literature shows that the positive relationship between the presence of mental disorders and lost productivity may not hold in all instances.
4 Discussion
The goal of this review was to provide a comprehensive overview and critical assessment of the most recent literature examining the relationship between mental health and workplace productivity, with a particular focus on data and methods employed. It provides clear evidence that poor mental health is associated with lost productivity, defined as increased absenteeism (i.e., more missed days from work) and increased presenteeism (i.e., decreased productivity at work). However, overall, only three studies were of high quality [ 25 , 28 , 47 ]. Studies with greater rigour and more robust methods, which accounted for unobserved heterogeneity for example, found a similar positive relationship but a smaller effect size [ 25 , 47 ].
Other reviews have also found large significant associations between measures of mental health and lost productivity, such as absenteeism [ 3 , 73 , 74 , 75 ]. For example, Burton et al. [ 3 ] found that depressive disorders were the most common mental health disorder among most workers, with many studies showing a positive association between the presence of mental health conditions and absenteeism, particularly short-term disability absences [ 3 ]. However, we found that studies employing superior methodological study design have shown the strength of the observed association may be smaller than previously thought.
Overall, our findings are in line with those from other reviews [ 73 , 74 , 75 ] and the Burton et al. study [ 3 ]. We too found that the most common disorder examined was depression, followed by depression and anxiety, the most studied workplace outcomes were both absenteeism and presenteeism, and that there was an association between mental disorders and both absenteeism and presenteeism. We found that studies employed a variety of data sources, from data collected from surveys/questionnaires to existing surveys and administrative data. Regression analysis was commonly used to examine the relationship between mental health and lost productivity, though there were some studies where the most appropriate regression model was not used given the outcome examined (e.g., linear regression models were used regardless of the type of outcome examined).
Some studies employed small sample sizes [ 20 , 43 ], which are not representative of the broader population and can thus impact the generalizability of findings, and other studies that did use nationally representative population samples employed cross-sectional designs [ 11 , 42 , 46 ], which can limit causal inference. Therefore, the vast majority did not examine the causal effect of mental health on lost productivity, but rather only the association between the two. A notable exception was Banerjee et al. [ 28 ], who examined the potential endogeneity of the mental illness variable used. Moreover, few studies employed longitudinal data, which can help account for unobserved heterogeneity (that may be correlated with both mental health and lost productivity) and minimise the potential for reverse causality and omitted variable bias; Wooden et al. [ 47 ] and Bubonya et al. [ 25 ] were notable exceptions. Wooden et al. found that the association between poor mental health and the number of annual paid sickness absence days was much smaller once they accounted for unobserved heterogeneity and focused on within-person differences [ 47 ]. For example, the incidence rate ratios for the number of sickness absence days for employed women and men experiencing severe depressive symptoms were 1.31 and 1.38, respectively, in the negative binomial regression models but dropped to 1.10 and 1.13, respectively, once the authors controlled for unobserved heterogeneity through the inclusion of correlated random effects. Thus, it may be that previous research has overstated the magnitude of the association between poor mental health and lost productivity. More studies with rigorous causal inference are required to help strengthen the ability to make informed policy recommendations.
Few studies explored the factors that might explain absenteeism and/or presenteeism due to mental health. Again, the study by Bubonya et al. was a notable exception [ 25 ], providing several important insights on the relationship between mental health and lost productivity. According to the authors, initiatives that limit and help workers manage job stress seem to be the most promising avenue for improving workers’ productivity. Furthermore, the authors found that presenteeism rates among workers with poor mental health were relatively insensitive to work environments, in line with other research from the UK [ 76 ]; consequently, they suggested that developing institutional arrangements that specifically target the productivity of those experiencing mental ill health may prove challenging. These findings are particularly important in the context of the COVID-19 pandemic due to changes in work arrangements and workplaces (e.g., working from home while trying to balance work with home and care responsibilities, hybrid working arrangements, and ensuring workplaces have COVID-19-secure measures in place). This work will be of particular interest to employers and decision makers looking to improve worker productivity.
Most literature examined either depression or anxiety or both, the most common mental disorders. Few studies examined mental disorders such as ADHD, bipolar disorder and eating disorders, and no studies examined schizophrenia and other psychotic disorders, personality disorder or suicidal/self-harm behaviour. More work is needed on these mental disorders, which, although less prevalent and thus less studied, are potentially more work disabling (despite already low employment rates for individuals with these conditions) [ 77 , 78 ]. Other research suggests there are important gender differences [ 25 , 28 ]. For example, Bubonya et al. found that increased job control can help reduce absenteeism for women with good mental health, though not for women in poor mental health [ 25 ]. Banerjee et al. found that the impact of poor mental health on the likelihood of being employed and in the labour force is higher for men [ 28 ]. Future research should ensure that gender differences, as well as other differences (e.g., age, industry, job conditions), are examined to ensure tailored polices are developed and implemented.
There is also a need to better understand the extent to which mental illness decreases productivity at work and the mechanisms through which this occurs, as this could help inform the role of employment policy and practices to minimise presenteeism [ 25 ]. Some research suggests that conducive working conditions, such as part-time employment and having autonomy over work tasks, can help mitigate the negative impact of mental health on presenteeism [ 76 ]. Alongside this, it is important to learn more about the dynamics of the relationship between mental illness and worker productivity to understand the trade-offs between presenteeism and absenteeism [ 25 ]. For example, it would be helpful to understand whether policies that incentivise workers with mental ill health to take time off improve overall productivity by reducing presenteeism. None of the studies in this review explored this trade-off. Finally, more rigorous research on this topic would help achieve a better understanding of the overall economic impact of mental disorders.
This review is not without limitations. It only included studies obtained from a few select databases and did not include grey literature, and only one reviewer screened the titles and abstracts (though the purpose was not to undertake a systematic review); however, it examined papers and reports from select websites of interest. Furthermore, this review only focused on the relationship between mental health and lost productivity. Although lost productivity is an important labour market outcome, there are other outcomes that mental health can impact such as labour force participation, wages/earnings, and part-time versus full time employment. Finally, this review only included studies published in English and therefore may have missed other relevant studies. Nonetheless, this review has several strengths. It provides an updated review on this topic, thus addressing a critical gap in the literature, and examined the type of data and databases employed, the methods used, and the existing gaps in the literature, thus providing a more comprehensive overview of the research done to date.
5 Conclusion
This review found clear evidence that poor mental health, typically measured as depression and/or anxiety, was associated with lost productivity, i.e., increased absenteeism and presenteeism. Most studies used survey and administrative data and regression analysis. Few studies employed longitudinal data, and most studies that used cross-sectional data did not account for endogeneity. Despite consistent findings across studies, more high-quality studies are needed on this topic, namely those that account for endogeneity and unobserved heterogeneity. Furthermore, more work is needed to understand the extent to which mental illness decreases productivity at work and the mechanisms through which this occurs, as well as a better understanding of the dynamics of the relationship between mental illness and worker productivity to understand the trade-offs between presenteeism and absenteeism. For example, future research should seek to understand how working conditions and work arrangements as well as workplace policies (e.g., vacation time and leaves of absence) impact presenteeism.
This type of review differs from a systematic review, which seeks to systematically search for, appraise and synthesise existing evidence, often following existing guidelines on the conduct of a review.
Bloom DE, Cafiero ET, Jané-Llopis E, et al. The global economic burden of noncommunicable diseases. Geneva: World Economic Forum; 2011.
Google Scholar
Hamberg-van Reenen HH, Proper KI, van den Berg M. Worksite mental health interventions: a systematic review of economic evaluations. Occup Environ Med. 2012;69:837–45.
Article PubMed Google Scholar
Burton WN, Schultz AB, Chen C, Edington DW. The association of worker productivity and mental health: a review of the literature. Int J Workplace Health Manag. 2008;1(2):78–94.
Article Google Scholar
McManus S, Bebbington P, Jenkins R, Brugha T, editors. Mental health and wellbeing in England: Adult Psychiatric Morbidity Survey 2014. Leeds: NHS Digital; 2016.
Mental wellbeing at work. Public health guideline [PH22]. London: National Institute for Health and Care Excellence (NICE); 2009. https://www.nice.org.uk/guidance/ph22 (Accessed 28 July 2021).
Grant MJ, Booth A. A typology of reviews: an analysis of 14 review types and associated methodologies. Health Inf Libr J. 2009;26(2):91–108.
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7): e1000097.
Article PubMed PubMed Central Google Scholar
Christensen MK, Lim CCW, Saha S, Plana-Ripoll O, Cannon D, Presley F, Weye N, Momen NC, Whiteford HA, Iburg KM, McGrath JJ. The cost of mental disorders: a systematic review. Epidemiol Psychiatr Sci. 2020;29: e161.
Article CAS PubMed PubMed Central Google Scholar
Wells G, Shea B, O’Connell D, Peterson J, Welch V, Losos M, Tugwell P. The Newcastle–Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses; 2013. http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp .
Uribe JM, Pinto DM, Vecino-Ortiz AI, Gómez-Restrepo C, Rondón M. Presenteeism, absenteeism, and lost work productivity among depressive patients from five cities of Colombia. Value Health Reg Issues. 2017;14:15–9.
Tsuchiya M, Kawakami N, Ono Y, Nakane Y, Nakamura Y, Fukao A, Tachimori H, Iwata N, Uda H, Nakane H, Watanabe M, Oorui M, Naganuma Y, Furukawa TA, Kobayashi M, Ahiko T, Takeshima T, Kikkawa T. Impact of mental disorders on work performance in a community sample of workers in Japan: the World Mental Health Japan Survey 2002–2005. Psychiatry Res. 2012;198(1):140–5.
Toyoshima K, Inoue T, Shimura A, Masuya J, Ichiki M, Fujimura Y, Kusumi I. Associations between the depressive symptoms, subjective cognitive function, and presenteeism of Japanese adult workers: a cross-sectional survey study. Biopsychosoc Med. 2020;14:10.
Suzuki T, Miyaki K, Song Y, Tsutsumi A, Kawakami N, Shimazu A, Takahashi M, Inoue A, Kurioka S. Relationship between sickness presenteeism (WHO-HPQ) with depression and sickness absence due to mental disease in a cohort of Japanese workers. J Affect Disord. 2015;180:14–20.
Simon GE, Ludman EJ, Unützer J, Operskalski BH, Bauer MS. Severity of mood symptoms and work productivity in people treated for bipolar disorder. Bipolar Disord. 2008;10(6):718–25.
Lamichhane DK, Heo YS, Kim HC. Depressive symptoms and risk of absence among workers in a manufacturing company: a 12-month follow-up study. Ind Health. 2018;56(3):187–97.
Park YL, Kim W, Chae JH, Seo OhK, Frick KD, Woo JM. Impairment of work productivity in panic disorder patients. J Affect Disord. 2014;157:60–5.
Johnston DA, Harvey SB, Glozier N, Calvo RA, Christensen H, Deady M. The relationship between depression symptoms, absenteeism and presenteeism. J Affect Disord. 2019;256:536–40.
Article CAS PubMed Google Scholar
Hjarsbech PU, Andersen RV, Christensen KB, Aust B, Borg V, Rugulies R. Clinical and non-clinical depressive symptoms and risk of long-term sickness absence among female employees in the Danish eldercare sector. J Affect Disord. 2011;129(1–3):87–93.
Hilton MF, Scuffham PA, Vecchio N, Whiteford HA. Using the interaction of mental health symptoms and treatment status to estimate lost employee productivity. Aust N Z J Psychiatry. 2010;44(2):151–61.
Hees HL, Koeter MW, Schene AH. Longitudinal relationship between depressive symptoms and work outcomes in clinically treated patients with long-term sickness absence related to major depressive disorder. J Affect Disord. 2013;148(2–3):272–7.
Fernandes MA, Ribeiro HKP, Santos JDM, Monteiro CFS, Costa RDS, Soares RFS. Prevalence of anxiety disorders as a cause of workers’ absence. Rev Bras Enferm. 2018;71(suppl 5):2213–20.
Evans-Lacko S, Knapp M. Global patterns of workplace productivity for people with depression: absenteeism and presenteeism costs across eight diverse countries. Soc Psychiatry Psychiatr Epidemiol. 2016;51(11):1525–37.
de Graaf R, Tuithof M, van Dorsselaer S, ten Have M. Comparing the effects on work performance of mental and physical disorders. Soc Psychiatry Psychiatr Epidemiol. 2012;47(11):1873–83.
Chong SA, Vaingankar JA, Abdin E, Subramaniam M. Mental disorders: employment and work productivity in Singapore. Soc Psychiatry Psychiatr Epidemiol. 2013;48(1):117–23.
Bubonya M, Cobb-Clark DA, Wooden M. Mental health and productivity at work: does what you do matter? Labour Econ. 2017;46:150–65.
Bokma WA, Batelaan NM, van Balkom AJ, Penninx BW. Impact of anxiety and/or depressive disorders and chronic somatic diseases on disability and work impairment. J Psychosom Res. 2017;94:10–6.
Beck A, Crain AL, Solberg LI, Unützer J, Glasgow RE, Maciosek MV, Whitebird R. Severity of depression and magnitude of productivity loss. Ann Fam Med. 2011;9(4):305–11.
Banerjee S, Chatterji P, Lahiri K. Effects of psychiatric disorders on labor market outcomes: a latent variable approach using multiple clinical indicators. Health Econ. 2017;26(2):184–205.
Ammerman RT, Chen J, Mallow PJ, Rizzo JA, Folger AT, Van Ginkel JB. Annual direct health care expenditures and employee absenteeism costs in high-risk, low-income mothers with major depression. J Affect Disord. 2016;190:386–94.
Able SL, Haynes V, Hong J. Diagnosis, treatment, and burden of illness among adults with attention-deficit/hyperactivity disorder in Europe. Pragmat Obs Res. 2014;5:21–33.
Asami Y, Goren A, Okumura Y. Work productivity loss with depression, diagnosed and undiagnosed, among workers in an Internet-based survey conducted in Japan. J Occup Environ Med. 2015;57(1):105–10.
Curkendall S, Ruiz KM, Joish V, Mark TL. Productivity losses among treated depressed patients relative to healthy controls. J Occup Environ Med. 2010;52(2):125–30.
McMorris BJ, Downs KE, Panish JM, Dirani R. Workplace productivity, employment issues, and resource utilization in patients with bipolar I disorder. J Med Econ. 2010;13(1):23–32.
Mauramo E, Lallukka T, Lahelma E, Pietiläinen O, Rahkone O. Common mental disorders and sickness absence. J Occup Environ Med. 2018;60(6):569–75.
Kessler RC, Lane M, Stang PE, Van Brunt DL. The prevalence and workplace costs of adult attention deficit hyperactivity disorder in a large manufacturing firm. Psychol Med. 2009;39(1):137–47.
Jain G, Roy A, Harikrishnan V, Yu S, Dabbous O, Lawrence C. Patient-reported depression severity measured by the PHQ-9 and impact on work productivity: results from a survey of full-time employees in the United States. J Occup Environ Med. 2013;55(3):252–8.
Knudsen AK, Harvey SB, Mykletun A, Øverland S. Common mental disorders and long-term sickness absence in a general working population. The Hordaland Health Study. Acta Psychiatr Scand. 2013;127(4):287–97.
Woo JM, Kim W, Hwang TY, Frick KD, Choi BH, Seo YJ, Kang EH, Kim SJ, Ham BJ, Lee JS, Park YL. Impact of depression on work productivity and its improvement after outpatient treatment with antidepressants. Value Health. 2011;14(4):475–82.
Harvey SB, Glozier N, Henderson M, Allaway S, Litchfield P, Holland-Elliott K, Hotopf M. Depression and work performance: an ecological study using web-based screening. Occup Med (Lond). 2011;61(3):209–11.
Koopmans PC, Roelen CA, Groothoff JW. Sickness absence due to depressive symptoms. Int Arch Occup Environ Health. 2008;81(6):711–9.
de Graaf R, Kessler RC, Fayyad J, ten Have M, Alonso J, Angermeyer M, Borges G, Demyttenaere K, Gasquet I, de Girolamo G, Haro JM, Jin R, Karam EG, Ormel J, Posada-Villa J. The prevalence and effects of adult attention-deficit/hyperactivity disorder (ADHD) on the performance of workers: results from the WHO World Mental Health Survey Initiative. Occup Environ Med. 2008;65(12):835–42.
Plaisier I, Beekman AT, de Graaf R, Smit JH, van Dyck R, Penninx BW. Work functioning in persons with depressive and anxiety disorders: the role of specific psychopathological characteristics. J Affect Disord. 2010;125(1–3):198–206.
Erickson SR, Guthrie S, Vanetten-Lee M, Himle J, Hoffman J, Santos SF, Janeck AS, Zivin K, Abelson JL. Severity of anxiety and work-related outcomes of patients with anxiety disorders. Depress Anxiety. 2009;26(12):1165–71.
Ling YL, Rascati KL, Pawaskar M. Direct and indirect costs among patients with binge-eating disorder in the United States. Int J Eat Disord. 2017;50(5):523–32.
Bouwmans CA, Vemer P, van Straten A, Tan SS, Hakkaart-van RL. Health-related quality of life and productivity losses in patients with depression and anxiety disorders. J Occup Environ Med. 2014;56(4):420–4.
Buist-Bouwman MA, Ormel J, de Graaf R, de Jonge P, van Sonderen E, Alonso J, Bruffaerts R, Vollebergh WA, ESEMeD/MHEDEA 2000 Investigators. Mediators of the association between depression and role functioning. Acta Psychiatr Scand. 2008;118(6):451–8.
Wooden M, Bubonya M, Cobb-Clark D. Sickness absence and mental health: evidence from a nationally representative longitudinal survey. Scand J Work Environ Health. 2016;42(3):201–8.
PubMed Google Scholar
de Oliveira C, Cho E, Kavelaars R, Jamieson M, Bao B, Rehm J. Economic analyses of mental health and substance use interventions in the workplace: a systematic literature review and narrative synthesis. Lancet Psychiatry. 2020;7(10):893–910.
Kessler RC, Andrews G, Colpe LJ, Hiripi E, Mroczek DK, Normand SL, Walters EE, Zaslavsky AM. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol Med. 2002;32:959–76.
Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–13.
Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1(3):385–401.
Goldberg D, Hillier V. A scaled version of the General Health Questionnaire. Psychol Med. 1979;9(1):139–45.
Bech P, Rasmussen N-A, Olsen LR, Noerholm V, Abildgaard W. The sensitivity and specificity of the Major Depression Inventory, using the Present State Examination as the index of diagnostic validity. J Affect Disord. 2001;66:159–64.
Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23:56–62.
Berwick DM, Murphy JM, Goldman PA, Ware JE Jr, Barsky AJ, Weinstein MC. Performance of a five-item mental health screening test. Med Care. 1991;29(2):169–76.
Snaith RP. The Hospital Anxiety And Depression Scale. Health Qual Life Outcomes. 2003;1:29.
Robins LN, Wing J, Wittchen HU, Helzer JE, Babor TF, Burke J, Farmer A, Jablenski A, Pickens R, Regier DA, et al. The Composite International Diagnostic Interview. An epidemiologic Instrument suitable for use in conjunction with different diagnostic systems and in different cultures. Arch Gen Psychiatry. 1988;45(12):1069–77.
Beck AT, Epstein N, Brown G, Steer RA. An inventory for measuring clinical anxiety: psychometric properties. J Consult Clin Psychol. 1988;56(6):893–7.
Rush AJ, Gullion CM, Basco MR, Jarrett RB, Trivedi MH. The Inventory of Depressive Symptomatology (IDS): psychometric properties. Psychol Med. 1996;26(3):477–86.
Hirschfeld RM. The Mood Disorder Questionnaire: a simple, patient-rated screening instrument for bipolar disorder. Prim Care Companion J Clin Psychiatry. 2002;4(1):9–11.
Kessler RC, Haro JM, Heeringa SG, et al. The World Health Organization World Mental Health Survey Initiative. Epidemiol Psychiatr Soc. 2006;15:161–6.
Kessler RC, Adler L, Ames M, Demler O, Faraone S, Hiripi E, Howes MJ, Jin R, Secnik K, Spencer T, Ustun TB, Walters EE. The World Health Organization Adult ADHD Self-Report Scale (ASRS): a short screening scale for use in the general population. Psychol Med. 2005;35(2):245–56.
Shear MK, Brown TA, Barlow DH, Money R, Sholomskas DE, Woods SW, et al. Multicenter collaborative panic disorder severity scale. Am J Psychiatry. 1997;154(11):1571–5.
Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibility of a work productivity and activity impairment instrument. Pharmacoeconomics. 1993;4:353–65.
Kessler RC, Barber C, Beck A, Berglund P, Cleary PD, McKenas D, Pronk N, Simon G, Stang P, Üstün TU, Wang P. The World Health Organization Health and Work Performance Questionnaire (HPQ). J Occup Environ Med. 2003;45(2):156–74.
Hubens K, Krol M, Coast J, Drummond MF, Brouwer WBF, Uyl-de Groot CA, Hakkaart-van RL. Measurement instruments of productivity loss of paid and unpaid work: a systematic review and assessment of suitability for health economic evaluations from a societal perspective. Value Health. 2021;24(11):1686–99.
Lerner D, Amick BC 3rd, Rogers WH, Malspeis S, Bungay K, Cynn D. The Work Limitations Questionnaire. Med Care. 2001;39(1):72–85.
Hakkaart-Van Roijen L. Manual. Trimbos/iMTA questionnaire for Costs associated with Psychiatric Illness (TiC-P adults); 2010. http://www.bmg.eur.nl/english/imta/publications/questionnaires_manuals .
van Roijen L, Essink-Bot M, Koopmanschap MA, et al. Labor and health status in economic evaluation of health care. Int J Technol Assess Health Care. 1996;12(3):405–15.
Janca A, Kastrup M, Katschnig H, López-Ibor JJ Jr, Mezzich JE, Sartorius N. The World Health Organization Short Disability Assessment Schedule (WHO DAS-S): a tool for the assessment of difficulties in selected areas of functioning of patients with mental disorders. Soc Psychiatry Psychiatr Epidemiol. 1996;31(6):349–54.
Endicott J, Nee J. Endicott Work Productivity Scale (EWPS): a new measure to assess treatment effects. Psychopharmacol Bull. 1997;33(1):13–6.
CAS PubMed Google Scholar
Jette AM, Davies AR, Cleary PD, Calkins DR, Rubenstein LV, Fink A, Kosecoff J, Young RT, Brook RH, Delbanco TL. The Functional Status Questionnaire: reliability and validity when used in primary care. J Gen Intern Med. 1986;1(3):143–9.
Duijts SFA, Kant I, Swaen GMH, van den Brandt PA, Zeegers MPA. A meta-analysis of observational studies identifies predictors of sickness absence. J Clin Epidemiol. 2007;60(11):1105–15.
Darr W, Johns G. Work strain, health, and absenteeism: a meta-analysis. J Occup Health Psychol. 2008;13(4):293–318.
Lerner D, Henke RM. What does research tell us about depression, job performance, and work productivity? J Occup Environ Med. 2008;50(4):401–10.
Bryan ML, Bryce AM, Roberts J. Presenteeism in the UK: effects of physical and mental health on worker productivity; 2020; SERPS no. 2020005. ISSN 1749-8368. https://www.sheffield.ac.uk/media/12544/download .
Cook JA. Employment barriers for persons with psychiatric disabilities: update of a report for the President’s Commission. Psychiatr Serv. 2006;57(10):1391–405.
Luciano A, Meara E. Employment status of people with mental illness: national survey data from 2009 and 2010. Psychiatr Serv. 2014;65(10):1201–9.
Download references
Acknowledgements
We thank Kath Wright for her help with the search strategy.
Author information
Authors and affiliations.
Centre for Health Economics, University of York, York, UK
Claire de Oliveira & Rowena Jacobs
Hull York Medical School, Hull and York, UK
Claire de Oliveira, Makeila Saka & Lauren Bone
Institute for Mental Health Policy Research, Centre for Addiction and Mental Health, Toronto, Canada
Claire de Oliveira
Institute of Health Policy, Management and Evaluation, University of Toronto, Toronto, Canada
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Claire de Oliveira .
Ethics declarations
No funding was received for this research.
Conflict of interest
None to declare.
Ethics approval
Not applicable.
Consent to participate
Consent for publication (from patients/participants), availability of data and material, code availability, author contributions.
CdO and RJ conceived and developed the protocol study. LB undertook the search and screened all titles and abstracts. MS extracted the data. CdO and RJ adjudicated any discrepancies in the full-text review. CdO wrote the first draft of the manuscript. CdO and RJ supervised the project. All authors provided critical feedback and helped shape the manuscript. All authors take sole responsibility for the content.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary file1 (DOCX 42 KB)
Rights and permissions.
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Reprints and permissions
About this article
de Oliveira, C., Saka, M., Bone, L. et al. The Role of Mental Health on Workplace Productivity: A Critical Review of the Literature. Appl Health Econ Health Policy 21 , 167–193 (2023). https://doi.org/10.1007/s40258-022-00761-w
Download citation
Accepted : 22 August 2022
Published : 15 November 2022
Issue Date : March 2023
DOI : https://doi.org/10.1007/s40258-022-00761-w
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Find a journal
- Publish with us
- Track your research
More From Forbes
An employer’s guide to mental health awareness in the workplace.
- Share to Facebook
- Share to Twitter
- Share to Linkedin
The stresses and pressure at the office or working remotely can be a cause of the deterioration of ... [+] employees’ mental health and emotional wellbeing.
May is National Mental Health Awareness Month, and creates the opportunity for organizations to bring mental, emotional and physical wellbeing to the forefront. It facilitates in helping to reduce any stigmas surrounding behavioral health issues and highlight how mental illness can impact the workplace, society, families and others.
Stress And Anxiety In The Workplace
The stresses and pressure at the office or working remotely can be a cause of the deterioration of employees’ mental health and emotional wellbeing. The Society of Human Resource Management found that one in three Americans say their mental health is negatively impacted by their jobs. About 30% of the 1,000 workers surveyed in the SHRM study self-reported feeling overwhelmed, and 29% said their jobs make them feel anxious at least once a week.
Some of the reasons for mental health issues and burnout can be due to unreasonable deadlines, a heavy workload, long hours, a toxic environment and a lack of appreciation, recognition, psychological safety and financial security.
Anxiety has surged in recent years, becoming the top mental health issue affecting American workers. Mental health provider ComPsych found that nearly a quarter of people (24%) who reached out for mental health assistance last year did so to help cope with anxiety—topping depression, stress, relationship issues, family issues, addiction and grief.
“It’s clear that as a society, we’ve become more anxious in recent years, and for good reason,” said Dr. Richard A. Chaifetz, founder, CEO and chairman of ComPsych, in a statement. “From the pandemic to ongoing conflicts in Gaza and Ukraine, civil unrest, an unpredictable economy and increasingly polarized political rhetoric surrounding elections, there is a persistent underlying feeling of apprehension and worry.”
The Best Self Cleaning Litter Boxes Tested For Months
Aurora alert: why you now need to pack a bag for sudden solar storms, leak reveals an etf perfect storm could be heading toward bitcoin after 6 trillion fed inflation flip unleashed a crypto price boom.
“For business leaders, there is an imperative to help employees cope with these feelings. Companies who invest in resources for employees ultimately benefit by attracting and retaining a healthier and more productive workforce, allowing both employees and companies to thrive,” he added.
What Managers Should Do Now
Managers should encourage employees to maintain a healthy work-life balance and promote taking advantage of vacation days and paid time off. They can provide flexible schedules or hybrid and remote work options to help employees manage stress and prioritize self-care.
Supervisors should be cognizant of the workloads and deadlines assigned to their employees. Managers should be trained to recognize signs of mental distress and how to respond appropriately. Human resources can disseminate micro-surveys to regularly gauge how workers are feeling. Armed with the anonymous data, they can take appropriate actions to remedy situations.
With a growing need for accessible mental healthcare , employers should emphasize mental health benefits, employee assistance programs, available counseling services offered through the company’s health plans and provide information on how employees can access these resources confidentially.
Organizations can invite mental health professionals and therapists to hold training sessions, and corporate leadership should encourage open discussions about mental health to normalize the conversation.
Moreover, employers can partner with corporate wellness providers to help foster overall health and a more engaged workforce.
Wellhub, formerly known as Gympass, is a comprehensive corporate wellbeing solution connecting millions of employees to a diverse network of partners for not only fitness but also, mindfulness, therapy, nutrition and sleep.
“The rebrand from Gympass to Wellhub is a natural evolution that reflects our commitment to providing a holistic wellbeing solution more than anything else,” said Wellhub founder and CEO Cesar Carvalho in a Zoom interview.
“Today, Wellhub is helping to solve the wellbeing crisis that is plaguing the global workforce,” Carvalho added, by providing a “turnkey solution that unlocks a variety of quality wellness services all in one place.”
It is a business-to-business platform, which means that companies will pay for the app, which enables their workers to gain access to a wide array of worldwide wellness programs, including gyms, studios, Yoga and online videos that workers can attend together. Member companies can help their team explore over 600 activities across the U.S., Europe and Latin America. Employees have over 50,000 studios globally, and more than 70 different wellness apps to choose from that will help improve their overall mental, physical and emotional health.
According to Wellhub’s site, it has helped its corporate clients boost employee physical activity by 178%, reduce annual employee healthcare costs by 25% and improve worker retention by 43%.
The unicorn startup was founded in 2012 in Brazil and has grown to 2.7 million subscribers across 15,000 corporate clients in 11 countries.

- Editorial Standards
- Reprints & Permissions
Join The Conversation
One Community. Many Voices. Create a free account to share your thoughts.
Forbes Community Guidelines
Our community is about connecting people through open and thoughtful conversations. We want our readers to share their views and exchange ideas and facts in a safe space.
In order to do so, please follow the posting rules in our site's Terms of Service. We've summarized some of those key rules below. Simply put, keep it civil.
Your post will be rejected if we notice that it seems to contain:
- False or intentionally out-of-context or misleading information
- Insults, profanity, incoherent, obscene or inflammatory language or threats of any kind
- Attacks on the identity of other commenters or the article's author
- Content that otherwise violates our site's terms.
User accounts will be blocked if we notice or believe that users are engaged in:
- Continuous attempts to re-post comments that have been previously moderated/rejected
- Racist, sexist, homophobic or other discriminatory comments
- Attempts or tactics that put the site security at risk
- Actions that otherwise violate our site's terms.
So, how can you be a power user?
- Stay on topic and share your insights
- Feel free to be clear and thoughtful to get your point across
- ‘Like’ or ‘Dislike’ to show your point of view.
- Protect your community.
- Use the report tool to alert us when someone breaks the rules.
Thanks for reading our community guidelines. Please read the full list of posting rules found in our site's Terms of Service.
Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals
- Explore content
- About the journal
- Publish with us
- Sign up for alerts
- 12 May 2024
Is the Internet bad for you? Huge study reveals surprise effect on well-being
- Carissa Wong
You can also search for this author in PubMed Google Scholar

People who had access to the Internet scored higher on measures of life satisfaction in a global survey. Credit: Ute Grabowsky/Photothek via Getty
A global, 16-year study 1 of 2.4 million people has found that Internet use might boost measures of well-being, such as life satisfaction and sense of purpose — challenging the commonly held idea that Internet use has negative effects on people’s welfare.

US TikTok ban: how the looming restriction is affecting scientists on the app
“It’s an important piece of the puzzle on digital-media use and mental health,” says psychologist Markus Appel at the University of Würzburg in Germany. “If social media and Internet and mobile-phone use is really such a devastating force in our society, we should see it on this bird’s-eye view [study] — but we don’t.” Such concerns are typically related to behaviours linked to social-media use, such as cyberbullying, social-media addiction and body-image issues. But the best studies have so far shown small negative effects, if any 2 , 3 , of Internet use on well-being, says Appel.
The authors of the latest study, published on 13 May in Technology, Mind and Behaviour , sought to capture a more global picture of the Internet’s effects than did previous research. “While the Internet is global, the study of it is not,” said Andrew Przybylski, a researcher at the University of Oxford, UK, who studies how technology affects well-being, in a press briefing on 9 May. “More than 90% of data sets come from a handful of English-speaking countries” that are mostly in the global north, he said. Previous studies have also focused on young people, he added.
To address this research gap, Pryzbylski and his colleagues analysed data on how Internet access was related to eight measures of well-being from the Gallup World Poll , conducted by analytics company Gallup, based in Washington DC. The data were collected annually from 2006 to 2021 from 1,000 people, aged 15 and above, in 168 countries, through phone or in-person interviews. The researchers controlled for factors that might affect Internet use and welfare, including income level, employment status, education level and health problems.
Like a walk in nature
The team found that, on average, people who had access to the Internet scored 8% higher on measures of life satisfaction, positive experiences and contentment with their social life, compared with people who lacked web access. Online activities can help people to learn new things and make friends, and this could contribute to the beneficial effects, suggests Appel.
The positive effect is similar to the well-being benefit associated with taking a walk in nature, says Przybylski.
However, women aged 15–24 who reported having used the Internet in the past week were, on average, less happy with the place they live, compared with people who didn’t use the web. This could be because people who do not feel welcome in their community spend more time online, said Przybylski. Further studies are needed to determine whether links between Internet use and well-being are causal or merely associations, he added.
The study comes at a time of discussion around the regulation of Internet and social-media use , especially among young people. “The study cannot contribute to the recent debate on whether or not social-media use is harmful, or whether or not smartphones should be banned at schools,” because the study was not designed to answer these questions, says Tobias Dienlin, who studies how social media affects well-being at the University of Vienna. “Different channels and uses of the Internet have vastly different effects on well-being outcomes,” he says.
doi: https://doi.org/10.1038/d41586-024-01410-z
Vuorre, M. & Przybylski, A. K. Technol. Mind Behav . https://doi.org/10.1037/tmb0000127 (2024).
Article Google Scholar
Heffer, T. et al. Clin. Psychol. Sci. 7 , 462–470 (2018).
Coyne, S. M., Rogers, A. A., Zurcher, J. D., Stockdale, L. & Booth, M. Comput. Hum. Behav . 104 , 106160 (2020).
Download references
Reprints and permissions
Related Articles

- Public health

How does ChatGPT ‘think’? Psychology and neuroscience crack open AI large language models
News Feature 14 MAY 24

Daniel Kahneman obituary: psychologist who revolutionized the way we think about thinking
Obituary 03 MAY 24

Pandemic lockdowns were less of a shock for people with fewer ties
Research Highlight 01 MAY 24

Could bird flu in cows lead to a human outbreak? Slow response worries scientists
News 17 MAY 24

Neglecting sex and gender in research is a public-health risk
Comment 15 MAY 24
Interpersonal therapy can be an effective tool against the devastating effects of loneliness
Correspondence 14 MAY 24
Inequality is bad — but that doesn’t mean the rich are
Postdoc in CRISPR Meta-Analytics and AI for Therapeutic Target Discovery and Priotisation (OT Grant)
APPLICATION CLOSING DATE: 14/06/2024 Human Technopole (HT) is a new interdisciplinary life science research institute created and supported by the...
Human Technopole
Research Associate - Metabolism
Houston, Texas (US)
Baylor College of Medicine (BCM)
Postdoc Fellowships
Train with world-renowned cancer researchers at NIH? Consider joining the Center for Cancer Research (CCR) at the National Cancer Institute
Bethesda, Maryland
NIH National Cancer Institute (NCI)
Faculty Recruitment, Westlake University School of Medicine
Faculty positions are open at four distinct ranks: Assistant Professor, Associate Professor, Full Professor, and Chair Professor.
Hangzhou, Zhejiang, China
Westlake University
PhD/master's Candidate
PhD/master's Candidate Graduate School of Frontier Science Initiative, Kanazawa University is seeking candidates for PhD and master's students i...
Kanazawa University
Sign up for the Nature Briefing newsletter — what matters in science, free to your inbox daily.
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies
Employee mental health requests have skyrocketed but only a fraction of leaders are making real changes

Good morning!
Workers are having a tough time . Young employees are missing nearly a day of work per week due to stress, the majority of staff members are at risk for burnout, and mental health struggles are the cause of a $47.6 billion productivity loss for the economy every year. Workers are desperate for psychological support, but few bosses are actually attending to their needs .
There was a 74% surge in employees requesting leave or accommodations for mental health-related issues over the past year, according to a new report from Littler, an employment and labor law company. That was followed by a 53% rise in pregnancy -related requests, 50% more hybrid and flexible work inquiries, and a 48% swell in paid sick leave demands.
“People are still dealing with the after effects of the pandemic,” Devjani H. Mishra, a partner at Littler, tells Fortune. “In tandem with that, you have some people newly being diagnosed with mental health conditions that they may have never sought help for before, along with employees becoming more familiar with asking for some kind of accommodation.”
Mishra adds that the data also shows that more staffers are comfortable voicing their concerns to managers.
“Over the last several years there’s been a destigmatizing of people asking for help, and self identifying as needing an accommodation related to mental health,” she says. Venting and sharing feelings on social media while being isolated during the pandemic changed communication styles.
But just because workers are more willing to disclose their mental health struggles with employers doesn’t mean those employers are helping . Only 22% of leaders say their organizations have improved accommodations and leave of absence policies to meet mental health demands over the past year, according to the report. By comparison, 38% of bosses made such concessions for pregnancy conditions and 28% did so for paid sick leave.
Mishra says this care gap largely stems from leaders being untrained on how to identify mental health problems and create adequate solutions. She adds that psychological problems can be complicated, and vary widely person to person. “If someone is having some sort of cognitive difficulty, they can kind of tell you ways that that might manifest, but they can’t tell you all of the ways. It’s not really predictable,” she says. This, combined with employers’ general lack of mental health knowledge, makes it hard for companies to set accommodations.
There is also structural weakness at play when it comes to companies tackling the mental health crisis; company policies tend to lag a couple years behind in adjusting to new workplace dynamics . As organizations are playing catch-up, a gap in care emerges between the time an issue is recognized and when it can be fixed, according to the report.
To best serve workers with psychological conditions, Mishra says that businesses should hire HR managers and business leaders who are educated and equipped to deal with the mental health aspects of the workforce.
“We need to have people that are equipped and better trained to recognize this is a real thing that we’re going to need to deal with.”
Emma Burleigh [email protected]
Around the Table
A round-up of the most important HR headlines.
As the country shifts to meet low-carbon goals, some German industrial companies have banded together to upskill 2.7 million employees that may become redundant. New York Times
The U.S. government and many private companies have made progress filling cyber-related job positions, but have yet to make strides in recruiting women and diverse candidates. Wall Street Journal
McDonald’s and Wendy's shareholders, representing $2.2 trillion in assets, are demanding that the chains enforce a zero-tolerance child labor policy and conduct risk assessments. Washington Post
Watercooler
Everything you need to know from Fortune .
Consequences. Around 700 unionized Virgin Hotel workers went on a two-day strike after the hospitality chain has failed to reach a new contract deal with the union. —AP
Game over. Microsoft employees were stunned after the company shut down several of its Xbox video game studios. — Jason Schreier, Bloomberg
Options. Some company executives are ignoring the RTO trend , saying mandates don’t increase productivity, and are standing behind flexible schedules as a smart business move. — Jane Thier
This is the web version of CHRO Daily, a newsletter focusing on helping HR executives navigate the needs of the workplace. Sign up to get it delivered free to your inbox.
Latest in Newsletters

The Mooch, Andrew Yang, and crypto’s tipping point

AI music may be having a moment, but human songwriters would like a word

To hold team members accountable, trust them, says JLL boss Christian Ulbrich

Bumble sought to win back women, but a ‘celibacy’ ad outraged them instead. How the dating app’s rebrand went wrong

DoorDash’s chief people officer says that HR departments have become research laboratories for new ideas

BlackRock’s COO on how the world’s largest asset manager is harnessing AI
Most popular.

Amazon raised warehouse wages to $15 an hour 5 years ago. Today, half of workers surveyed told researchers they struggle to afford food or rent

Florida HBCU launches investigation after record $238 million ‘gift’ from 30-year-old hemp mogul is deemed likely worthless: ‘I wanted it to be real’

Thousands of North Koreans stole Americans’ identities and took remote-work tech jobs at Fortune 500 companies, DOJ says

Billionaire investor Ray Dalio warns U.S. is ‘on the brink’ and estimates a more than 1 in 3 chance of civil war

Young adults are getting cold feet about their highly anticipated $84 trillion wealth transfer

Jeff Bezos revealed his secret to Amazon’s success 25 years ago: ‘I asked everyone around here to wake up terrified every morning, their sheets drenched in sweat’

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Rand Health Q
- v.7(3); 2018 Apr
Understanding mental health in the research environment
Short abstract.
This study aimed to establish what is known about the mental health of researchers based on the existing literature. The literature identified focuses mainly on stress in the academic workforce and contributory factors in the academic workplace.
This study aimed to establish what is known about the mental health of researchers based on the existing literature. There is limited published evidence on the prevalence of specific mental health conditions among researchers. The majority of the identified literature on prevalence relates to work-related stress among academic staff and postgraduate students in university settings.
Survey data indicate that the majority of university staff find their job stressful. Levels of burnout appear higher among university staff than in general working populations and are comparable to “high-risk” groups such as healthcare workers. The proportions of both university staff and postgraduate students with a risk of having or developing a mental health problem, based on self-reported evidence, were generally higher than for other working populations. Large proportions (>40 per cent) of postgraduate students report symptoms of depression, emotion or stress-related problems, or high levels of stress.
Factors including increased job autonomy, involvement in decision making and supportive management were linked to greater job satisfaction among academics, as was the amount of time spent on research. Opportunities for professional development were also associated with reduced stress. UK higher education (HE) and research staff report worse wellbeing, as compared to staff in other sectors, in most aspects of work that can affect workers' stress levels.
The evidence around the effectiveness of interventions to support the mental health of researchers specifically is thin. Few interventions are described in the literature and even fewer of those have been evaluated.
The Royal Society and Wellcome Trust are interested in better understanding the mental health needs of researchers, and what interventions could be used to support them. This reflects the recent focus on mental health among undergraduate students in the UK, and the concern that others in the academic and wider research environment may have mental health needs that have not been as well explored and considered. This study aims to establish what is currently known about the mental health of researchers based on the existing literature.
Over 6 million working-age people in England have a mental health condition at a given time. The most common diagnosable difficulties among working age adults are anxiety and depression, each of which includes a number of different conditions. Less common but still widespread mental health diagnoses include personality disorders and psychoses such as bipolar disorder and schizophrenia. Many people will have more than one diagnosis at a time, or receive different diagnoses over time.
The causes and triggers of poor mental health are complex and not fully understood. There is evidence that the vast majority of people who experience poor mental health in adulthood first experienced difficulties as children, often from a young age. Risk factors for poor mental health include having a parent with mental health difficulties, growing up in prolonged poverty and housing insecurity, experiences of abuse, neglect and bullying, and traumatic experiences during childhood. Some groups of people have a heightened risk of poor mental health, including some black and ethnic minority communities, people with long-term physical conditions, lesbian, gay, bisexual and transgender people, and people with disabilities.
There is mixed evidence about the extent to which a person's experiences of work contribute to their having a mental health difficulty. Survey evidence suggests that workplace factors such as bullying, insecurity and a lack of control are major causes of mental ill health among staff. On the other hand, there is also evidence that work helps many people to recover from an episode of poor mental health, and there is clear evidence that unemployment is a major risk factor for mental and physical ill health.
Mental ill health and work-related stress are key issues for the labour market as they affect productivity through absenteeism and presenteeism, and are associated with high economic costs for individuals, employers and the economy at large. It has been estimated that poor mental health costs employers in the UK £26 billion nationwide each year, equivalent to £1,035 for every employee in the workforce ( Centre for Mental Health, 2007 ).
Little is known about how mental health needs vary across working environments, or about how to tailor interventions to address different working populations.
The aim of this study was to assess what is known about mental health in research environments through a literature review, and it focused on the UK and comparable research systems. A better understanding of researchers' mental health needs will enable the design of more effective interventions to address them, while a better understanding of evidence gaps can also help guide future research efforts in this area. The following research questions guided the study:
- How are “mental health” and “wellbeing” understood in the context of research environments?
- What is currently known about researchers' mental health and wellbeing, and does it differ from that of other populations?
- What interventions are used to support researchers, and what evidence is there of their effectiveness?
- What are the strengths and limitations of the evidence base in this area?
How Are “Mental Health” and “Wellbeing” Understood in Research Environments?
Overall, the existing literature offers little insight into what sets the research environment apart from other workplaces, or into how mental health, stress, and wellbeing are defined in these contexts. Rather, the majority of the literature identified focuses on describing the levels of stress amongst the academic workforce and, in particular, identifying contributory factors within the workplace. There is little available evidence based on objective clinical assessment about the prevalence of clinically defined mental health conditions and their treatment in this context. The focus on wellbeing raises the issue that although the presence of common mental health conditions does correlate with some of the wellbeing scales used commonly in the literature, more serious (e.g. psychotic) mental illnesses are not necessarily aligned with measurement of wellbeing.
The literature is also almost exclusively focused on universities, with many studies covering all university staff, which will include both researchers and non-research staff. Some studies focused more specifically on researchers, and a more limited group within that looked at particular groups of researchers—most commonly PhD students, reflecting the wider focus on (typically undergraduate) students in the literature around this topic. The majority of the existing research is based on survey data, which is subject to sampling biases, relies on self-reporting, and was not triangulated with other objective indicators, such as absence data.
What Is Currently Known About Researchers' Mental Health and Wellbeing, and How It Differs from Other Populations?
Evidence on the prevalence of work-related stress and mental health problems.
Despite widely reported anecdotal evidence and press coverage of a “mental health crisis” in academia, there is limited published evidence regarding the prevalence of specific mental health conditions among researchers. The majority of the literature on prevalence identified through this review relates to the experience of work-related stress (and arguably the risk of developing a mental health condition as a result of exposure to identified stressors) among academic staff and postgraduate students in university settings.
- Survey data indicate that the majority of university staff find their job stressful. Levels of burnout appear higher among university staff than in general working populations and are comparable to “high-risk” groups such as healthcare workers.
- The proportions of both university staff and postgraduate students with a risk of having or developing a mental health problem, based on self-reported evidence, were generally higher than for other working populations.
- Large proportions (>40 per cent) of postgraduate students report symptoms of depression, emotion or stress-related problems, or high levels of stress.
UK national statistics indicate that only 6.2 per cent of staff disclosed a mental health condition to their university, though academics have been found to be among the occupational groups with the highest levels of common mental disorders with prevalence around 37 per cent. It should be noted, however, that prevalence may generally be over-reported in surveys of occupational groups.
Personal Factors That Contribute to Mental Health Outcomes in the Research Workplace
Gender was the key personal factor that emerged as a determinant for mental health (or its reporting), with women reporting more exposure to stress than men, as well as greater challenges around work-life balance. There was also evidence that personality and perceived competence affect mental health as self-critical personalities are more susceptible to stress, though it is also possible that they are more aware of it or more willing to report it. However, it was unclear whether stress was a result of working conditions in the research environment, or whether research settings attracted particular types of individuals. The results on whether age affects mental health were inconclusive, partly as age is often difficult to disentangle from discussions about rank and seniority. Other factors such as disability, sexuality and minority status were mentioned in a small number of articles in the sample, and these articles indicated that these personal factors generally increase stress.
Environmental Factors Commonly Considered in Surveys of Mental Health and Wellbeing in Workplaces
Based on the Health and Safety Executive's framework, and evidence from the wider literature, we identify six key aspects of work that can affect workers' stress levels: work demands, job control, change management, work relationships, support provided by managers and colleagues, and clarity about one's role.
- These aspects of the work environment can be sources of stress or they can help counteract it.
- Findings from studies of university staff and researchers were consistent with the wider understanding of factors that contribute to stress in workplaces.
- Factors including increased job autonomy, involvement in decision making and supportive management were linked to greater job satisfaction among academics, as was the amount of time spent on research. Opportunities for professional development were also associated with reduced stress.
UK higher education (HE) and research staff report worse wellbeing in most of the six aspects, as compared to staff in other sectors.
- In large-scale surveys, UK higher education staff have reported worse wellbeing than staff in other types of employment (including education, and health and social work) in the areas of work demands, change management, support provided by managers and clarity about one's role.
- The only area where higher education staff have reported higher wellbeing in large-scale surveys is in job control, though even here results are mixed across studies. Wide variability was seen among respondents in relation to the level of support provided by managers and colleagues.
- Job insecurity (real and perceived) appears to be an important issue for those working in the research environment, and particularly for early-career researchers, who are often employed on successive short-term contracts.
PhD students face similar challenges to other researchers and higher education staff.
- The main factors associated with development of depression and other common mental health problems in PhD students are high levels of work demands and work-life conflict, low job control, poor support from the supervisor and exclusion from decision making.
- Believing that PhD work is valuable for one's future career helps reduce stress, as does confidence in one's own research abilities.
Some studies suggested that changes to the UK higher education system had brought increased job stress.
- These studies discussed changes that had occurred in the UK higher education system from the 1990s onwards, and had resulted in increased emphasis on accountability, efficiency and performance management. Study authors suggested that these changes could have brought about increases in job stress for staff working in this system.
- However, data explicitly linking the changes to an increase in stress are limited, partly due to a lack of comparable data from before the 1990s.
Staff who can devote a large proportion of their working time to research have better wellbeing.
- Studies found that spending a larger percentage of one's time on research was associated with reduced stress, and that research-only staff reported lower levels of work-life conflict and had better wellbeing than other higher education institution (HEI) staff. However, this may be to some extent confounded by other characteristics of such researchers (e.g. they may be more senior).
Research on emotionally challenging topics can put staff wellbeing at risk.
- Studies showed that staff involved in research on sensitive topics, such as trauma or abuse, may be emotionally affected by the material they encounter in their work and should receive greater support to mitigate the negative impacts of this work.
Outcomes Related to Poor Mental Health and Wellbeing
In addition to considering the extent to which individuals in research environments suffer from mental health issues, it is important for employers and institutions to recognise that these issues have further implications:
- Job stress and poor workplace wellbeing can contribute to reduced productivity—both through absence and, more importantly, through presenteeism, where researchers attend work and are less productive.
- They can also lead to lower levels of commitment to their research and to institutions—which can be seen in high levels of turnover and through negative attitudes in the workplace.
- Effects on job satisfaction are less clear because of the satisfaction researchers gain from intrinsic factors such as the intellectual stimulation of their work. Several studies note that high levels of job-related stress can coexist with high levels of job satisfaction.
- Effects can also spill over into personal and family life.
The overall effects of these negative outcomes on the sector have not been fully quantified, but estimates drawing on broader experience suggest that the costs could be high. An estimate from Shutler-Jones et al (2008) which has several caveats and assumptions, suggests that the costs to the UK HE sector could be more than £500 million per year (c. 5 per cent of the sector's total annual income). Costs to the economy and the country more widely could also be significant due to the lost potential for scientific advances and due to impacts on the availability of research talent if PhD students fail to complete their studies or choose to leave research subsequently.
What Interventions Are Used to Support Researchers, and What Evidence Is There of Their Effectiveness?
Though poor mental health at work is often related to difficulties that are not caused by work (e.g. childhood adversity, family life and other stressors), support in the workplace can offer benefits. However, the evidence around the effectiveness of interventions to support the mental health of researchers specifically is thin. Few interventions are described in the literature and even fewer of those have been evaluated. Where evaluations have been conducted, they are often of limited utility, either because of the evaluation design or the length of follow-up.
Interventions typically focus on stress and wellbeing rather than clinical mental health conditions, reflecting the wider focus in the literature as described above. In addition, the majority of interventions identified aim to support researchers to deal with workplace stress, but they may not be effective in addressing the root causes of that stress or stresses relating to life outside work. The interventions identified can be broadly classified into four groups: policy changes, communication activities, training, and health-promotion activities.
Focusing specifically on the UK, a range of interventions were piloted and evaluated (to a limited extent) as part of a wellbeing initiative by the Higher Education Funding Council for England (HEFCE) around 2009–2011. These offer scope for further investigation and potentially evaluation now that more time has elapsed. Additionally, the project, though completed in 2011, has spawned a network that is now managed by the Universities and Colleges Employers Association (UCEA), which may offer a route to identify further ongoing initiatives and potentially a space to pursue and evaluate efforts to address these issues in the HE sector.
What Are the Strengths and Limitations of the Evidence Base in This Area?
The existing evidence base is limited, meaning it is not possible to draw robust conclusions about the mental health status and needs of researchers, and how researchers may differ from other populations in this regard. More work is needed to understand both the mental health needs of researchers and how they can be addressed. Particular gaps include the effectiveness of interventions, prevalence of specific mental health needs (rather than stress) among researchers, and any evidence about researchers outside the academic setting. There are also limitations to the quality and design of many of the studies conducted, such as lack of long-term follow-up and absence of control groups.
Based on the evidence gaps identified and the information available, we suggest the following avenues for further research on this topic:
- Study the prevalence of mental health conditions amongst postdoctoral researchers: Further work on prevalence could use a targeted approach building on the recent work by Levecque et al. (2017) , who used a survey to assess the presence of psychological distress and potential psychiatric disorders in a sample of PhD students and compared the results to those of three other sample populations, and Eisenberg et al. (2007) , who surveyed a sample of undergraduate and postgraduate university students to assess prevalence of depressive and anxiety disorders and took steps to address the issue of non-response bias. In particular, we suggest a similar study focusing on postdoctoral researchers, a group that is particularly poorly addressed in the existing literature.
- Map mental health policies and procedures at UK HEIs: The current standard of mental health policies and procedures in UK research institutions is not well understood. We suggest that a mapping of the current policies in place across institutions could be valuable, and could build on standards such as those set out in the Mindful Employer Charter ( Mindful Employer, 2017 ).
- Evaluate the interventions introduced through the HEFCE wellbeing and engagement initiative: The wellbeing initiative established by the HEFCE and subsequently maintained as a network by UCEA offers a range of interventions for evaluation. In the project reporting in 2011, many of the institutions noted that it was too soon to tell whether their interventions had been effective. Though these initiatives generally focus on wellbeing rather than clinical mental health conditions, there is scope to explore with the relevant institutions whether those interventions have developed over the years, and whether data are now available (or could be collected) to provide more useful evaluation of the interventions introduced.
- Investigate and develop the HSE management standards as a framework for workplace mental health management in research environments: As well as providing a framework for workplace stress used in several important surveys, the Health and Safety Executive (HSE) have also set out management standards that describe an approach to identifying sources of workplace stress and addressing them at an organisational level. It could be useful to work through that approach with a university or a research organisation to identify the mechanisms at play in those environments. Doing so could establish the relevance of the approach in this context, and potentially provide a model that could be used more widely in the sector.
- Conduct more and higher-quality evaluations of mental health interventions and publish their results: Broadly, better-quality evaluations are needed to identify what works in this area. There is a need for high-quality studies to test the effectiveness of interventions.
The research described in this article was prepared for the Royal Society and the Wellcome Trust and conducted by RAND Europe.
- Centre for Mental Health. Mental health at work: Developing the business case. 2007. 2017. http://www.centreformentalhealth.org.uk/Handlers/Download.ashx?IDMF=4c278a50-8bd6-4aff-9cf3-7667c0770288 As of May 30.
- Eisenberg D., Gollust S. E., Golbertstein E., Hefner J. L. “Prevalence and correlates of depression, anxiety, and suicidality among university students.” American Journal of Orthopsychiatry. 2007; 77 (4):534–542. [ PubMed ] [ Google Scholar ]
- Levecque K., Anseel F., De Beuckelaer A., Van der Heydan J. and Gisle L. “Work organization and mental health problems in PhD students.” Research Policy. 2017; 46 (4):868–879. [ Google Scholar ]
- Mindful Employer. “Charter for employers”. 2017. http://www.mindfulemployer.net/charter/ As of June 10, 2017.
- Shutler-Jones K. Improving performance through well-being and engagement. 2011. 2017. http://www.qub.ac.uk/safety-reps/sr_webpages/safety_downloads/wellbeing-final-report-2011-web.pdf As of June 10.
School of Social Work
- Academic Programs
- Student Resources
- News & Events
- Faculty & Staff
- Request Info
The Essential Role of Gerontological Social Workers
Thursday, May 16, 2024 • Jaelon Jackson :
By Jaelon Jackson School of Social Work

What do Gerontology Social Workers do?
As we journey through the stages of life, eventually arriving at the challenges and opportunities that come with aging, Gerontological Social Workers emerge as essential guides.
Their role extends far beyond mere service provision; they become compassionate allies, standing by older individuals and their families during times of need. Gerontological or Aging Specialty Social Workers fulfill many responsibilities, including practical assistance, emotional support, and advocacy. Here's a closer look at their vital tasks:
- Practical Assistance : Gerontological Social Workers help older adults access essential services such as healthcare, transportation, and housing. They navigate bureaucratic hurdles with expertise and compassion, ensuring older adults receive the care and support they need to thrive in their later years.
- Emotional Support : Aging can bring about many emotional challenges, from adjusting to life transitions to coping with loss and illness. Gerontological Social Workers offer a listening ear and a supportive presence during emotionally challenging times. They provide counseling, therapy, and support groups to help older adults navigate the complexities of aging with dignity and resilience.
- Advocacy : Gerontological Social Workers are fierce advocates for the rights and well-being of older adults. Social Workers fight against ageism, discrimination, neglect, and abuse, empowering older adults to advocate for themselves and access the resources they need to live fulfilling lives.
What challenges and opportunities do our aging population encounter?
As our society experiences a significant shift in demographics, characterized by a growing number of older adults, a plethora of challenges and opportunities arise for individuals, families, and communities. These challenges include:
- Access to Healthcare : Older adults, especially those residing in rural or underserved areas, may face difficulties in accessing quality healthcare services. Gerontological Social Workers play a pivotal role in connecting them with appropriate healthcare providers and ensuring they receive the care they deserve.
- Preventing Elder Abuse : Elder abuse is a pervasive issue affecting millions of older adults worldwide. Gerontological Social Workers work tirelessly to prevent elder abuse and provide support to victims, helping them navigate legal processes and access resources for recovery.
- Addressing Social Isolation : Social isolation poses a significant concern among older adults, particularly those who live alone or have limited social connections. Gerontological Social Workers devise strategies to foster social connectedness and well-being among older adults, utilizing community resources and support groups to combat loneliness and isolation.
- Ensuring Financial Stability : Financial challenges such as insufficient savings and rising healthcare costs are prevalent among seniors. Gerontological Social Workers provide financial counseling and assistance to promote financial security in later life, ensuring older adults can afford the care and support they need to thrive.
What opportunities are there for our older adult population?
In addition to challenges, aging also presents numerous opportunities for older adults to engage with their communities and lead fulfilling lives. These opportunities include:
- Volunteering/Civic Engagement : Volunteering and engaging in civic activities not only benefit the community but also have health and social benefits for older adults. Gerontological Social Workers encourage older adults to get involved in volunteer work and civic engagement opportunities to stay active and connected.
- Intergenerational Support/Activities : Building strong intergenerational relationships, such as those between grandparents and grandchildren or through mentoring younger generations, fosters a sense of purpose and connection for older adults. Gerontological Social Workers promote intergenerational activities and support networks to enhance well-being across generations.
- Value of Older Workers : Older adults bring valuable skills, wisdom, and institutional knowledge to the workforce. Gerontological Social Workers advocate for the inclusion of older workers in the labor market, highlighting the benefits of mentoring and knowledge transfer between generations.
- Lifelong Learning : Lifelong learning opportunities, such as taking up new hobbies, learning new skills, or traveling to new places, contribute to older adults' cognitive health and overall well-being. Gerontological Social Workers encourage older adults to pursue lifelong learning opportunities to stay mentally and socially engaged.
Why is it crucial to support mental health in older adults?
Ensuring the mental well-being of older adults holds immense importance, often overlooked in discussions about aging and healthcare. The aging process can bring forth various mental health challenges, including:
- Depression : Many older adults experience feelings of sadness or depression as they navigate life transitions, cope with loss, or confront health issues. However, it is important to know that depression is not a "normal” part of aging.
- Anxiety : Anxiety disorders are common among older adults, particularly those facing significant life changes or dealing with chronic health conditions.
- Cognitive Decline : Cognitive decline, including conditions like Alzheimer's disease and other forms of dementia, can have a profound impact on older adults' mental health and overall well-being.
Recognizing the pivotal role of mental health support for older adults, Gerontological Social Workers work diligently to provide access to resources and services essential for maintaining optimal mental well-being. They offer support and coping strategies to assist seniors in adjusting to life transitions and provide crisis intervention when needed.
Moreover, Gerontological Social Workers contribute to suicide prevention efforts by identifying risk factors and facilitating access to mental health services for older adults facing challenges.
As we journey through the intricate tapestry of aging, let us not overlook the invaluable contributions of Gerontological Social Workers. Through their unwavering dedication and tireless efforts, they illuminate the path forward, guiding all of us as we age toward a future filled with dignity, resilience, and well-being.
Learn more about Gerontological Social Work and the aging specialty in our Master of Social Work program.
Stay Connected
- SSW Communications & Marketing Office
- SSW in the Media
- Monthly Newsletters
- Monthly Video News Update
- Courtyard Conversations - Monthly Talk Show
- Marketing Products
- Video Gallery
- Photo Gallery
- SSW Upcoming Events
Address School of Social Work Box 19129 501 W. Mitchell Street Arlington, TX 76019-0129
Phone (Local): 817-272-3181 | (Toll Free): 866-272-3181 Fax : 817-272-5229
The School of Social Work Admissions office is located in Suite 203 in the Social Work and Smart Hospital Building (501 W. Mitchell Street, Arlington, TX 76019).
Follow us on social media
- Faculty/Staff Resources
- Parking Pass Request
- Request Information
- Conference Room/Classroom Reservation
- Special Event Request
- Faculty Academic & Student Affairs Resources
IMAGES
VIDEO
COMMENTS
In a follow-up study of their 2019 Mental Health at Work Report, Mind Share Partners' 2021 Mental Health at Work Report, the authors offer a rare comparison of the state of mental health, stigma ...
The Surgeon General's Framework for Mental Health and Well-Being in the Workplace, which cites research from APA, is designed to encourage organizations to rethink how they protect workers from harm, foster a sense of connection among workers, show workers that they matter, make space for their lives outside work, and support their growth. ...
The relevance of mental health at work goes beyond individual well-being, as it significantly affects coworkers and employers (Harvey et al., 2017). ... Research on employees' mental health and well-being is dominated by quantitative research methods. 90% of the reviewed studies involved quantitative research design, 3.8% qualitative, 5% mixed ...
Work can protect mental health. Almost 60% of the world population is in work (1). All workers have the right to a safe and healthy environment at work. Decent work supports good mental health by providing: a livelihood; a sense of confidence, purpose and achievement; an opportunity for positive relationships and inclusion in a community; and.
Mental health problems and disorders are common among working people and are costly for the affected individuals, employers, and whole of society. This discussion paper provides an overview of the current state of knowledge on the relationship between work and mental health to inform research, policy, and practice. We synthesise available evidence, examining both the role of working conditions ...
This report summarises what we've learned from our first commission on promising approaches for addressing workplace mental health. It also sets out why businesses and researchers need to work together to take a more scientific approach to supporting mental health at work. Published. 10 May 2021. On this page.
An estimated 15% of working-age adults have a mental disorder at any point in time. Depression and anxiety are estimated to cost the global economy US $1 trillion each year driven predominantly by lost productivity. People living with severe mental health conditions are largely excluded from work despite participation in economic activities being important for recovery. The WHO guidelines on ...
The results of APA's 2022 Work and Well-being Survey reveal that seven in 10 workers (71%) believe their employer is more concerned about the mental health of employees now than in the past. This new focus is highly valued by employees. In fact, 81% of individuals said they will be looking for workplaces that support mental health when they ...
In October 2022, U.S. Surgeon General Vivek Murthy, MD, released the office's first-ever Surgeon General's Framework for Workplace Mental Health and Well-Being. The results of APA's 2023 Work in America Survey confirmed that psychological well-being is a very high priority for workers themselves. Specifically:
Work affects both our physical and mental well-being — in good ways and bad. The COVID-19 pandemic brought the relationship between work and well-being into clearer focus. Our Nation's Current Workplace Landscape. Recent surveys suggest... 76%of U.S. workers reported at least one symptom of a mental health condition.
Furthermore, the authors found that presenteeism rates among workers with poor mental health were relatively insensitive to work environments, in line with other research from the UK ; consequently, they suggested that developing institutional arrangements that specifically target the productivity of those experiencing mental ill health may ...
Work can be a protective factor for mental health, but it can also contribute to potential harm. All workers have the right to a safe and healthy environment at work. The Mental health at work: policy brief, developed jointly by WHO and the International Labour Organization, provides a pragmatic framework for implementing the recommendations of the WHO guidelines on mental health at work.
This study examines the mental health imp act of three main factors, namely. work pressure, work duration, and employee gratitude levels. Wor k pressure in this s tudy. is cons idered a challenge ...
Mental illnesses such as depression are associated with higher rates of disability and unemployment. Depression interferes with a person's ability to complete physical job tasks about 20% of the time and reduces cognitive performance about 35% of the time. 11. Only 57% of employees who report moderate depression and 40% of those who report ...
Mental health disorders in the workplace, such as depression and anxiety, have increasingly been recognised as a problem in most countries. Using a human capital approach, the global economic burden of mental illness was estimated to be US$$2.5 trillion in 2010 increasing to US$$6.1 trillion in 2030; most of this burden was due to lost productivity, defined as absenteeism and presenteeism [].
Aims: The Study on Mental Health at Work (S-MGA) generates the first nationwide representative survey enabling the exploration of the relationship between working conditions, mental health and functioning. This paper describes the study design, sampling procedures and data collection, and presents a summary of the sample characteristics. Methods: S-MGA is a representative study of German ...
specifically address the prevention, identification and management of depression and anxiety at the workplace; ♦. supporting individuals with mental health problems; and. ♦. recruitment and retention practices which do not discriminate against people with mental health problems. Objectives of the policy.
The stresses and pressure at the office or working remotely can be a cause of the deterioration of employees' mental health and emotional wellbeing. The Society of Human Resource Management ...
Neglecting sex and gender in research is a public-health risk. Comment 15 MAY 24. Interpersonal therapy can be an effective tool against the devastating effects of loneliness. Correspondence 14 MAY 24
Young employees are missing nearly a day of work per week due to stress, the majority of staff members are at risk for burnout, and mental health struggles are the cause of a $47.6 billion ...
APA's 2021 Work and Well-being Survey found that 87% of employees say that certain actions from their employer would help their mental health. Research supports the connection between mental health disorders and decreased work productivity. Treatment for conditions like depression is significantly associated with improved productivity.
This study aimed to establish what is known about the mental health of researchers based on the existing literature. The literature identified focuses mainly on stress in the academic workforce and contributory factors in the academic workplace. Keywords: Depression, Scientific Professions, Workforce Management, Workplace Wellness Programs.
Competing Interest Statement. The authors have declared no competing interest. Funding Statement. The Centre for Health Economics and Medicines Evaluation, the Bangor Institute for Medical and Health Research, and the Swansea Centre for Health Economics were funded for this work by the Health and Care Research Wales Evidence Centre, itself funded by Health and Care Research Wales on behalf of ...
Cognitive Decline: Cognitive decline, including conditions like Alzheimer's disease and other forms of dementia, can have a profound impact on older adults' mental health and overall well-being. Recognizing the pivotal role of mental health support for older adults, Gerontological Social Workers work diligently to provide access to resources ...
According to Dr Erasito, right now the biggest focus areas in climate change mitigation are food and shelter, with mental health impacts neglected due to a lack of data. "We don't really have good data on the smaller events that have occurred. The big ones like Cyclone Winston, we do, but not the smaller ones," she says. The team plans to ...