- Bipolar Disorder
- Therapy Center
- When To See a Therapist
- Types of Therapy
- Best Online Therapy
- Best Couples Therapy
- Best Family Therapy
- Managing Stress
- Sleep and Dreaming
- Understanding Emotions
- Self-Improvement
- Healthy Relationships
- Student Resources
- Personality Types
- Guided Meditations
- Verywell Mind Insights
- 2024 Verywell Mind 25
- Mental Health in the Classroom
- Editorial Process
- Meet Our Review Board
- Crisis Support

The Process of Conducting Ethical Research in Psychology
Kendra Cherry, MS, is a psychosocial rehabilitation specialist, psychology educator, and author of the "Everything Psychology Book."
:max_bytes(150000):strip_icc():format(webp)/IMG_9791-89504ab694d54b66bbd72cb84ffb860e.jpg "research and ethics in psychology")
Tom Merton / Getty Images
Earlier in psychology history, many experiments were performed with highly questionable and even outrageous violations of ethical considerations. Milgram's infamous obedience experiment , for example, involved deceiving human subjects into believing that they were delivering painful, possibly even life-threatening, electrical shocks to another person.
These controversial psychology experiments played a major role in the development of the ethical guidelines and regulations that psychologists must abide by today. When performing studies or experiments that involve human participants, psychologists must submit their proposal to an institutional review board (IRB) for approval. These committees help ensure that experiments conform to ethical and legal guidelines.
Ethical codes, such as those established by the American Psychological Association, are designed to protect the safety and best interests of those who participate in psychological research. Such guidelines also protect the reputations of psychologists, the field of psychology itself and the institutions that sponsor psychology research.
Ethical Guidelines for Research With Human Subjects
When determining ethical guidelines for research , most experts agree that the cost of conducting the experiment must be weighed against the potential benefit to society the research may provide. While there is still a great deal of debate about ethical guidelines, there are some key components that should be followed when conducting any type of research with human subjects.
Participation Must Be Voluntary
All ethical research must be conducted using willing participants. Study volunteers should not feel coerced, threatened or bribed into participation. This becomes especially important for researchers working at universities or prisons, where students and inmates are often encouraged to participate in experiments.
Researchers Must Obtain Informed Consent
Informed consent is a procedure in which all study participants are told about procedures and informed of any potential risks. Consent should be documented in written form. Informed consent ensures that participants know enough about the experiment to make an informed decision about whether or not they want to participate.
Obviously, this can present problems in cases where telling the participants the necessary details about the experiment might unduly influence their responses or behaviors in the study. The use of deception in psychology research is allowed in certain instances, but only if the study would be impossible to conduct without the use of deception, if the research will provide some sort of valuable insight and if the subjects will be debriefed and informed about the study's true purpose after the data has been collected.
Researchers Must Maintain Participant Confidentiality
Confidentiality is an essential part of any ethical psychology research. Participants need to be guaranteed that identifying information and individual responses will not be shared with anyone who is not involved in the study.
While these guidelines provide some ethical standards for research, each study is different and may present unique challenges. Because of this, most colleges and universities have a Human Subjects Committee or Institutional Review Board that oversees and grants approval for any research conducted by faculty members or students. These committees provide an important safeguard to ensure academic research is ethical and does not pose a risk to study participants.
American Psychological Association. Ethical principles of psychologists and code of conduct .
By Kendra Cherry, MSEd Kendra Cherry, MS, is a psychosocial rehabilitation specialist, psychology educator, and author of the "Everything Psychology Book."

How the Classics Changed Research Ethics
Some of history’s most controversial psychology studies helped drive extensive protections for human research participants. some say those reforms went too far..
- Behavioral Research
- Institutional Review Board (IRB)
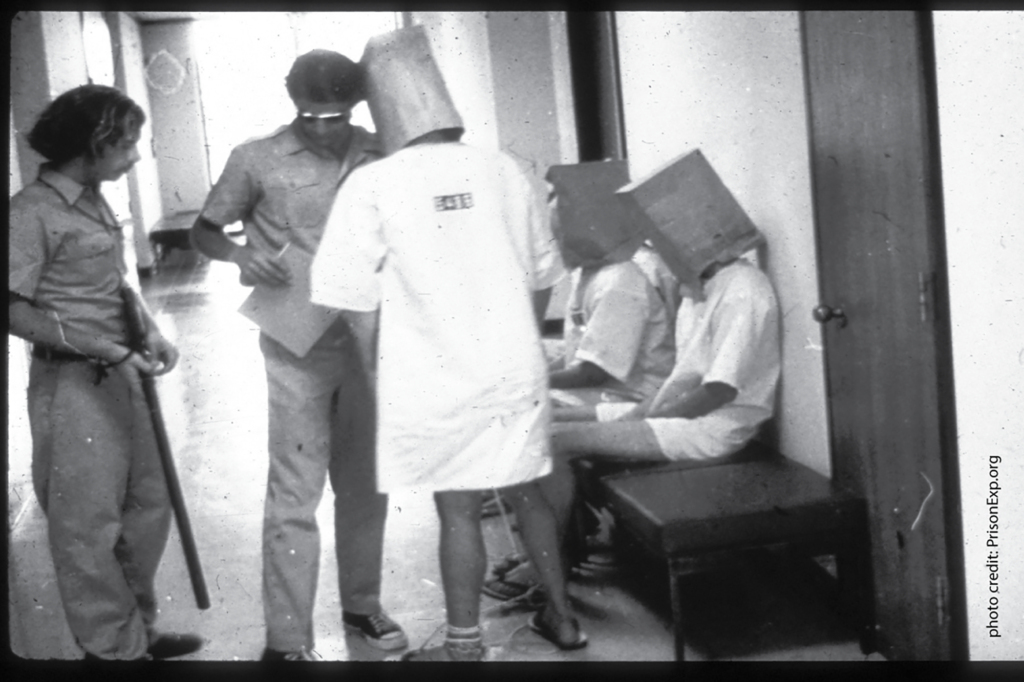
Photo above: In 1971, APS Fellow Philip Zimbardo halted his classic prison simulation at Stanford after volunteer “guards” became abusive to the “prisoners,” famously leading one prisoner into a fit of sobbing. Photo credit: PrisonExp.org
Nearly 60 years have passed since Stanley Milgram’s infamous “shock box” study sparked an international focus on ethics in psychological research. Countless historians and psychology instructors assert that Milgram’s experiments—along with studies like the Robbers Cave and Stanford prison experiments—could never occur today; ethics gatekeepers would swiftly bar such studies from proceeding, recognizing the potential harms to the participants.
But the reforms that followed some of the 20th century’s most alarming biomedical and behavioral studies have overreached, many social and behavioral scientists complain. Studies that pose no peril to participants confront the same standards as experimental drug treatments or surgeries, they contend. The institutional review boards (IRBs) charged with protecting research participants fail to understand minimal risk, they say. Researchers complain they waste time addressing IRB concerns that have nothing to do with participant safety.
Several factors contribute to this conflict, ethicists say. Researchers and IRBs operate in a climate of misunderstanding, confusing regulations, and a systemic lack of ethics training, said APS Fellow Celia Fisher, a Fordham University professor and research ethicist, in an interview with the Observer .
“In my view, IRBs are trying to do their best and investigators are trying to do their best,” Fisher said. “It’s more that we really have to enhance communication and training on both sides.”
‘Sins’ from the past
Modern human-subjects protections date back to the 1947 Nuremberg Code, the response to Nazi medical experiments on concentration-camp internees. Those ethical principles, which no nation or organization has officially accepted as law or official ethics guidelines, emphasized that a study’s benefits should outweigh the risks and that human subjects should be fully informed about the research and participate voluntarily.
See the 2014 Observer cover story by APS Fellow Carol A. Tavris, “ Teaching Contentious Classics ,” for more about these controversial studies and how to discuss them with students.
But the discovery of U.S.-government-sponsored research abuses, including the Tuskegee syphilis experiment on African American men and radiation experiments on humans, accelerated regulatory initiatives. The abuses investigators uncovered in the 1970s, 80s, and 90s—decades after the experiments had occurred—heightened policymakers’ concerns “about what else might still be going on,” George Mason University historian Zachary M. Schrag explained in an interview. These concerns generated restrictions not only on biomedical research but on social and behavioral studies that pose a minute risk of harm.
“The sins of researchers from the 1940s led to new regulations in the 1990s, even though it was not at all clear that those kinds of activities were still going on in any way,” said Schrag, who chronicled the rise of IRBs in his book Ethical Imperialism: Institutional Review Boards and the Social Sciences, 1965–2009.
Accompanying the medical research scandals were controversial psychological studies that provided fodder for textbooks, historical tomes, and movies.
- In the early 1950s, social psychologist Muzafer Sherif and his colleagues used a Boy Scout camp called Robbers Cave to study intergroup hostility. They randomly assigned preadolescent boys to one of two groups and concocted a series of competitive activities that quickly sparked conflict. They later set up a situation that compelled the boys to overcome their differences and work together. The study provided insights into prejudice and conflict resolution but generated criticism because the children weren’t told they were part of an experiment.
- In 1961, Milgram began his studies on obedience to authority by directing participants to administer increasing levels of electric shock to another person (a confederate). To Milgram’s surprise, more than 65% of the participants delivered the full voltage of shock (which unbeknownst to them was fake), even though many were distressed about doing so. Milgram was widely criticized for the manipulation and deception he employed to carry out his experiments.
- In 1971, APS Fellow Philip Zimbardo halted his classic prison simulation at Stanford after volunteer “guards” became abusive to the “prisoners,” famously leading one prisoner into a fit of sobbing.
Western policymakers created a variety of safeguards in the wake of these psychological studies and other medical research. Among them was the Declaration of Helsinki, an ethical guide for human-subjects research developed by the Europe-based World Medical Association. The U.S. Congress passed the National Research Act of 1974, which created a commission to oversee participant protections in biomedical and behavioral research. And in the 90s, federal agencies adopted the Federal Policy for the Protection of Human Subjects (better known as the Common Rule), a code of ethics applied to any government-funded research. IRBs review studies through the lens of the Common Rule. After that, social science research, including studies in social psychology, anthropology, sociology, and political science, began facing widespread institutional review (Schrag, 2010).
Sailing Through Review
Psychological scientists and other researchers who have served on institutional review boards provide these tips to help researchers get their studies reviewed swiftly.
- Determine whether your study qualifies for minimal-risk exemption from review. Online tools are even in development to help researchers self-determine exempt status (Ben-Shahar, 2019; Schneider & McClutcheon, 2018).
- If you’re not clear about your exemption, research the regulations to understand how they apply to your planned study. Show you’ve done your homework and have developed a protocol that is safe for your participants.
- Consult with stakeholders. Look for advocacy groups and representatives from the population you plan to study. Ask them what they regard as fair compensation for participation. Get their feedback about your questionnaires and consent forms to make sure they’re understandable. These steps help you better show your IRB that the population you’re studying will find the protections adequate (Fisher, 2022).
- Speak to IRB members or staff before submitting the protocol. Ask them their specific concerns about your study, and get guidance on writing up the protocol to address those concerns. Also ask them about expected turnaround times so you can plan your submission in time to meet any deadlines associated with your study (e.g., grant application deadlines).
Ben-Shahar, O. (2019, December 2). Reforming the IRB in experimental fashion. The Regulatory Review . University of Pennsylvania. https://www.theregreview.org/2019/12/02/ben-shahar-reforming-irb-experimental-fashion/
Fisher, C. B. (2022). Decoding the ethics code: A practical guide for psychologists (5 th ed.). Sage Publications.
Schneider, S. L. & McCutcheon, J. A. (2018). Proof of concept: Use of a wizard for self-determination of IRB exempt status . Federal Demonstration Partnership. http://thefdp.org/default/assets/File/Documents/wizard_pilot_final_rpt.pdf
Social scientists have long contended that the Common Rule was largely designed to protect participants in biomedical experiments—where scientists face the risk of inducing physical harm on subjects—but fits poorly with the other disciplines that fall within its reach.
“It’s not like the IRBs are trying to hinder research. It’s just that regulations continue to be written in the medical model without any specificity for social science research,” she explained.
The Common Rule was updated in 2018 to ease the level of institutional review for low-risk research techniques (e.g., surveys, educational tests, interviews) that are frequent tools in social and behavioral studies. A special committee of the National Research Council (NRC), chaired by APS Past President Susan Fiske, recommended many of those modifications. Fisher was involved in the NRC committee, along with APS Fellows Richard Nisbett (University of Michigan) and Felice J. Levine (American Educational Research Association), and clinical psychologist Melissa Abraham of Harvard University. But the Common Rule reforms have yet to fully expedite much of the research, partly because the review boards remain confused about exempt categories, Fisher said.
Interference or support?
That regulatory confusion has generated sour sentiments toward IRBs. For decades, many social and behavioral scientists have complained that IRBs effectively impede scientific progress through arbitrary questions and objections.
In a Perspectives on Psychological Science paper they co-authored, APS Fellows Stephen Ceci of Cornell University and Maggie Bruck of Johns Hopkins University discussed an IRB rejection of their plans for a study with 6- to 10-year-old participants. Ceci and Bruck planned to show the children videos depicting a fictional police officer engaging in suggestive questioning of a child.
“The IRB refused to approve the proposal because it was deemed unethical to show children public servants in a negative light,” they wrote, adding that the IRB held firm on its rejection despite government funders already having approved the study protocol (Ceci & Bruck, 2009).
Other scientists have complained the IRBs exceed their Common Rule authority by requiring review of studies that are not government funded. In 2011, psychological scientist Jin Li sued Brown University in federal court for barring her from using data she collected in a privately funded study on educational testing. Brown’s IRB objected to the fact that she paid her participants different amounts of compensation based on need. (A year later, the university settled the case with Li.)
In addition, IRBs often hover over minor aspects of a study that have no genuine relation to participant welfare, Ceci said in an email interview.
“You can have IRB approval and later decide to make a nominal change to the protocol (a frequent one is to add a new assistant to the project or to increase the sample size),” he wrote. “It can take over a month to get approval. In the meantime, nothing can move forward and the students sit around waiting.”
Not all researchers view institutional review as a roadblock. Psychological scientist Nathaniel Herr, who runs American University’s Interpersonal Emotion Lab and has served on the school’s IRB, says the board effectively collaborated with researchers to ensure the study designs were safe and that participant privacy was appropriately protected
“If the IRB that I operated on saw an issue, they shared suggestions we could make to overcome that issue,” Herr said. “It was about making the research go forward. I never saw a project get shut down. It might have required a significant change, but it was often about confidentiality and it’s something that helps everybody feel better about the fact we weren’t abusing our privilege as researchers. I really believe it [the review process] makes the projects better.”
Some universities—including Fordham University, Yale University, and The University of Chicago—even have social and behavioral research IRBs whose members include experts optimally equipped to judge the safety of a psychological study, Fisher noted.
Training gaps
Institutional review is beset by a lack of ethics training in research programs, Fisher believes. While students in professional psychology programs take accreditation-required ethics courses in their doctoral programs, psychologists in other fields have no such requirement. In these programs, ethics training is often limited to an online program that provides, at best, a perfunctory overview of federal regulations.
“It gives you the fundamental information, but it has nothing to do with our real-world deliberations about protecting participants,” she said.
Additionally, harm to a participant is difficult to predict. As sociologist Martin Tolich of University of Otago in New Zealand wrote, the Stanford prison study had been IRB-approved.
“Prediction of harm with any certainty is not necessarily possible, and should not be the aim of ethics review,” he argued. “A more measured goal is the minimization of risk, not its eradication” (Tolich, 2014).
Fisher notes that scientists aren’t trained to recognize and respond to adverse events when they occur during a study.
“To be trained in research ethics requires not just knowing you have to obtain informed consent,” she said. “It’s being able to apply ethical reasoning to each unique situation. If you don’t have the training to do that, then of course you’re just following the IRB rules, which are very impersonal and really out of sync with the true nature of what we’re doing.”
Researchers also raise concerns that, in many cases, the regulatory process harms vulnerable populations rather than safeguards them. Fisher and psychological scientist Brian Mustanski of University of Illinois at Chicago wrote in 2016, for example, that the review panels may be hindering HIV prevention strategies by requiring researchers to get parental consent before including gay and bisexual adolescents in their studies. Under that requirement, youth who are not out to their families get excluded. Boards apply those restrictions even in states permitting minors to get HIV testing and preventive medication without parental permission—and even though federal rules allow IRBs to waive parental consent in research settings (Mustanski & Fisher, 2016)
IRBs also place counterproductive safety limits on suicide and self-harm research, watching for any sign that a participant might need to be removed from a clinical study and hospitalized.
“The problem is we know that hospitalization is not the panacea,” Fisher said. “It stops suicidality for the moment, but actually the highest-risk period is 3 months after the first hospitalization for a suicide attempt. Some of the IRBs fail to consider that a non-hospitalization intervention that’s being tested is just as safe as hospitalization. It’s a difficult problem, and I don’t blame them. But if we have to take people out of a study as soon as they reach a certain level of suicidality, then we’ll never find effective treatment.”
Communication gaps
Supporters of the institutional review process say researchers tend to approach the IRB process too defensively, overlooking the board’s good intentions.
“Obtaining clarification or requesting further materials serve to verify that protections are in place,” a team of institutional reviewers wrote in an editorial for Psi Chi Journal of Psychological Research . “If researchers assume that IRBs are collaborators in the research process, then these requests can be seen as prompts rather than as admonitions” (Domenech Rodriguez et al., 2017).
Fisher agrees that researchers’ attitudes play a considerable role in the conflicts that arise over ethics review. She recommends researchers develop each protocol with review-board questions in mind (see sidebar).
“For many researchers, there’s a disdain for IRBs,” she said. “IRBs are trying their hardest. They don’t want to reject research. It’s just that they’re not informed. And sometimes if behavioral scientists or social scientists are disdainful of their IRBs, they’re not communicating with them.”
Some researchers are building evidence to help IRBs understand the level of risk associated with certain types of psychological studies.
- In a study involving more than 500 undergraduate students, for example, psychological scientists at the University of New Mexico found that the participants were less upset than expected by questionnaires about sex, trauma , and other sensitive topics. This finding, the researchers reported in Psychological Science , challenges the usual IRB assumption about the stress that surveys on sex and trauma might inflict on participants (Yeater et al., 2012).
- A study involving undergraduate women indicated that participants who had experienced child abuse , although more likely than their peers to report distress from recalling the past as part of a study, were also more likely to say that their involvement in the research helped them gain insight into themselves and hoped it would help others (Decker et al., 2011).
- A multidisciplinary team, including APS Fellow R. Michael Furr of Wake Forest University, found that adolescent psychiatric patients showed a drop in suicide ideation after being questioned regularly about their suicidal thoughts over the course of 2 years. This countered concerns that asking about suicidal ideation would trigger an increase in such thinking (Mathias et al., 2012).
- A meta-analysis of more than 70 participant samples—totaling nearly 74,000 individuals—indicated that people may experience only moderate distress when discussing past traumas in research studies. They also generally might find their participation to be a positive experience, according to the findings (Jaffe et al., 2015).
The takeaways
So, are the historians correct? Would any of these classic experiments survive IRB scrutiny today?
Reexaminations of those studies make the question arguably moot. Recent revelations about some of these studies suggest that scientific integrity concerns may taint the legacy of those findings as much as their impact on participants did (Le Texier, 2019, Resnick, 2018; Perry, 2018).
Also, not every aspect of the controversial classics is taboo in today’s regulatory environment. Scientists have won IRB approval to conceptually replicate both the Milgram and Stanford prison experiments (Burger, 2009; Reicher & Haslam, 2006). They simply modified the protocols to avert any potential harm to the participants. (Scholars, including Zimbardo himself, have questioned the robustness of those replication findings [Elms, 2009; Miller, 2009; Zimbardo, 2006].)
Many scholars believe there are clear and valuable lessons from the classic experiments. Milgram’s work, for instance, can inject clarity into pressing societal issues such as political polarization and police brutality . Ethics training and monitoring simply need to include those lessons learned, they say.
“We should absolutely be talking about what Milgram did right, what he did wrong,” Schrag said. “We can talk about what we can learn from that experience and how we might answer important questions while respecting the rights of volunteers who participate in psychological experiments.”
Feedback on this article? Email [email protected] or login to comment.
References
Burger, J. M. (2009). Replicating Milgram: Would people still obey today? American Psychologist , 64 (1), 1–11. https://doi.org/10.1037/a0010932
Ceci, S. J. & Bruck, M. (2009). Do IRBs pass the minimal harm test? Perspectives on Psychological Science , 4 (1), 28–29. https://doi.org/10.1111/j.1745-6924.2009.01084.x
Decker, S. E., Naugle, A. E., Carter-Visscher, R., Bell, K., & Seifer, A. (2011). Ethical issues in research on sensitive topics: Participants’ experiences of stress and benefit . Journal of Empirical Research on Human Research Ethics: An International Journal , 6 (3), 55–64. https://doi.org/10.1525/jer.2011.6.3.55
Domenech Rodriguez, M. M., Corralejo, S. M., Vouvalis, N., & Mirly, A. K. (2017). Institutional review board: Ally not adversary. Psi Chi Journal of Psychological Research , 22 (2), 76–84. https://doi.org/10.24839/2325-7342.JN22.2.76
Elms, A. C. (2009). Obedience lite. American Psychologist , 64 (1), 32–36. https://doi.org/10.1037/a0014473
Fisher, C. B., True, G., Alexander, L., & Fried, A. L. (2009). Measures of mentoring, department climate, and graduate student preparedness in the responsible conduct of psychological research. Ethics & Behavior , 19 (3), 227–252. https://doi.org/10.1080/10508420902886726
Jaffe, A. E., DiLillo, D., Hoffman, L., Haikalis, M., & Dykstra, R. E. (2015). Does it hurt to ask? A meta-analysis of participant reactions to trauma research. Clinical Psychology Review , 40 , 40–56. https://doi.org/10.1016/j.cpr.2015.05.004
Le Texier, T. (2019). Debunking the Stanford Prison experiment. American Psychologist , 74 (7), 823–839. http://dx.doi.org/10.1037/amp0000401
Mathias, C. W., Furr, R. M., Sheftall, A. H., Hill-Kapturczak, N., Crum, P., & Dougherty, D. M. (2012). What’s the harm in asking about suicide ideation? Suicide and Life-Threatening Behavior , 42 (3), 341–351. https://doi.org/10.1111/j.1943-278X.2012.0095.x
Miller, A. G. (2009). Reflections on “Replicating Milgram” (Burger, 2009). American Psychologist , 64 (1), 20–27. https://doi.org/10.1037/a0014407
Mustanski, B., & Fisher, C. B. (2016). HIV rates are increasing in gay/bisexual teens: IRB barriers to research must be resolved to bend the curve. American Journal of Preventive Medicine , 51 (2), 249–252. https://doi.org/10.1016/j.amepre.2016.02.026
Perry, G. (2018). The lost boys: Inside Muzafer Sherif’s Robbers Cave experiment. Scribe Publications.
Reicher, S. & Haslam, S. A. (2006). Rethinking the psychology of tyranny: The BBC prison study. British Journal of Social Psychology , 45 , 1–40. https://doi.org/10.1348/014466605X48998
Resnick, B. (2018, June 13). The Stanford prison experiment was massively influential. We just learned it was a fraud. Vox. https://www.vox.com/2018/6/13/17449118/stanford-prison-experiment-fraud-psychology-replication
Schrag, Z. M. (2010). Ethical imperialism: Institutional review boards and the social sciences, 1965–2009 . Johns Hopkins University Press.
Tolich, M. (2014). What can Milgram and Zimbardo teach ethics committees and qualitative researchers about minimal harm? Research Ethics , 10 (2), 86–96. https://doi.org/10.1177/1747016114523771
Yeater, E., Miller, G., Rinehart, J., & Nason, E. (2012). Trauma and sex surveys meet minimal risk standards: Implications for institutional review boards. Psychological Science , 23 (7), 780–787. https://doi.org/10.1177/0956797611435131
Zimbardo, P. G. (2006). On rethinking the psychology of tyranny: The BBC prison study. British Journal of Social Psychology , 45 , 47–53. https://doi.org/10.1348/014466605X81720
APS regularly opens certain online articles for discussion on our website. Effective February 2021, you must be a logged-in APS member to post comments. By posting a comment, you agree to our Community Guidelines and the display of your profile information, including your name and affiliation. Any opinions, findings, conclusions, or recommendations present in article comments are those of the writers and do not necessarily reflect the views of APS or the article’s author. For more information, please see our Community Guidelines .
Please login with your APS account to comment.
About the Author
Scott Sleek is a freelance writer in Silver Spring, Maryland, and the former director of news and information at APS.

Inside Grants: National Science Foundation Research Data Ecosystems (RDE)
The National Science Foundation’s Research Data Ecosystems (RDE) is a $38 million effort to improve scientific research through modernized data management collection.

Up-and-Coming Voices: Methodology and Research Practices
Talks by students and early-career researchers related to methodology and research practices.

Understanding ‘Scientific Consensus’ May Correct Misperceptions About GMOs, but Not Climate Change
Explaining the meaning of “scientific consensus” may be more effective at countering some types of misinformation than others.
Privacy Overview
https://www.simplypsychology.org/Ethics.html
McLeod, S. \(2015\). Psychology research ethics. Simply Psychology. Retrieved from https://www.simplypsychology.org/Ethics.html.
CITE AS:
McLeod, S. \(2015\). Psychology research ethics. Simply Psychology. https://www.simplypsychology.org/Ethics.html.
- Subject List
- Take a Tour
- For Authors
- Subscriber Services
- Publications
- African American Studies
- African Studies
- American Literature
- Anthropology
- Architecture Planning and Preservation
- Art History
- Atlantic History
- Biblical Studies
- British and Irish Literature
- Childhood Studies
- Chinese Studies
- Cinema and Media Studies
- Communication
- Criminology
- Environmental Science
- Evolutionary Biology
- International Law
- International Relations
- Islamic Studies
- Jewish Studies
- Latin American Studies
- Latino Studies
- Linguistics
- Literary and Critical Theory
- Medieval Studies
- Military History
- Political Science
- Public Health
- Renaissance and Reformation
- Social Work
- Urban Studies
- Victorian Literature
- Browse All Subjects
How to Subscribe
- Free Trials
In This Article Expand or collapse the "in this article" section Ethics in Psychological Practice
Introduction, general overviews.
- Nonrational Factors in Ethical Decision Making
- Scientifically and Professionally Informed Competence
- Emotional Competence
- Risk Management and Boundaries
- Sexual Boundaries
- Boundaries and Technology
- Confidentiality and Record Keeping
- Patients Who Threaten to Harm Others
- Patients Who Threaten to Harm Themselves
- Forensic Psychology
- Informed Consent
- Other Special Topics
- Risk Management (Quality Enhancement)
- Ethics Education and Supervision
Related Articles Expand or collapse the "related articles" section about
About related articles close popup.
Lorem Ipsum Sit Dolor Amet
Vestibulum ante ipsum primis in faucibus orci luctus et ultrices posuere cubilia Curae; Aliquam ligula odio, euismod ut aliquam et, vestibulum nec risus. Nulla viverra, arcu et iaculis consequat, justo diam ornare tellus, semper ultrices tellus nunc eu tellus.
- Abnormal Psychology
- Clinical Psychology
- Counseling Psychology
- Counseling Services in School Psychology
- Diagnostic and Statistical Manual of Mental Disorders (DSM)
Other Subject Areas
Forthcoming articles expand or collapse the "forthcoming articles" section.
- Data Visualization
- Executive Functions in Childhood
- Remote Work
- Find more forthcoming articles...
- Export Citations
- Share This Facebook LinkedIn Twitter
Ethics in Psychological Practice by Samuel Knapp , Leon VandeCreek LAST REVIEWED: 30 September 2013 LAST MODIFIED: 30 September 2013 DOI: 10.1093/obo/9780199828340-0024
Professional ethics refers to the laws, regulations, and standards that govern the profession (including ethics codes), the overarching ethical principles that underlie enforceable standards of conduct, ethical decision-making skills, risk management strategies, and self-regulation (emotional competence). The rules and guidelines for professional conduct are codified in the ethics code of the profession; in psychology this code is titled Ethical Principles of Psychologists and Code of Conduct (American Psychological Association [APA], 2010; hereafter Ethics Code). However, laws and standards cannot address all of the issues that professional psychologists face. Psychologists encounter situations that are too unique or context dependent to be covered in law or in an ethics code. Also, psychologists may encounter situations unanticipated by the ethics code, or they may encounter situations in which overarching ethical principles appear to collide with the law or the policies of an institution that employs them. Consequently, psychologists need to rely on overarching ethical values and engage in decision making. “Risk management” refers to activities that reduce the likelihood that psychologists will be investigated or convicted by a disciplinary body. To recent scholars, risk management strategies should focus on implementing or fulfilling overarching ethical principles. This perspective on allowing overarching ethical principles to guide professional behavior is called “positive ethics.”
These are some of the more referenced textbooks and overviews of ethics for professional psychologists. Each has its own strengths and unique features. Most are developed for graduate students in psychology or related fields. Fisher 2013 focuses primarily on the ethics code itself, whereas Knapp and VandeCreek 2012 , Koocher and Keith-Spiegel 2008 , Pope and Vasquez 2011 , and Kitchener and Anderson 2011 deal with ethics in a broader sense. Bersoff 2008 is an edited text with substantial commentary by the author. Anderson and Handelsman 2010 focuses more on self-reflection and less on factual content.
Anderson, S., and M. M. Handelsman. 2010. Ethics for psychotherapists and counselors: A proactive approach . Malden, MA: Wiley-Blackwell.
Relying heavily on the ethics acculturation model and the use of an ethics autobiography, Anderson and Handelsman provide a series of exercises and discussions designed to socialize young professionals into the profession.
Bersoff, D., ed. 2008. Ethical conflicts in psychology . 4th ed. Washington, DC: American Psychological Association.
This text contains excerpts from some of the more salient articles in professional psychology accompanied by commentary.
Fisher, C. 2013 . Decoding the ethics code: A practical guide for psychologists . 3d ed. Thousand Oaks, CA: SAGE.
Fisher, who was the chair of the committee that recommended changes in the 2002 Ethics Code, clearly explains the principles of the APA Ethics Code, gives useful illustrations, and identifies the rationale behind many of the standards and how they fit into the overall obligations of psychologists. However, the text limits its scope to the Ethics Code and does not consider other areas of ethics such as decision-making models or risk management strategies.
Kitchener, K. S., and S. Anderson. 2011. Foundations of ethical practice, research and teaching in psychology and counseling . New York: Routledge.
The unique strength is its detailed coverage of overarching ethical theories, including the decision-making model proposed.
Knapp, S., and L. VandeCreek. 2012. Practical ethics for psychologists: A positive approach . 2d ed. Washington, DC: American Psychological Association.
Knapp and VandeCreek emphasize positive ethics, or the idea that ethics should focus on more than simply avoiding disciplinary action but should be anchored in an overarching ethical theory that guides a wide range of professional behaviors.
Koocher, G., and P. Keith-Spiegel. 2008. Ethics in psychology and the mental health professions: Standards and cases . 3d ed. New York: Oxford Univ. Press.
This is a classic, with clear coverage of essential issues and entertaining vignettes that illustrate important points.
Pope, K. S., and M. Vasquez. 2011 . Ethics in psychotherapy and counseling: A practical guide . 4th ed. New York: Wiley.
This is a good, practical textbook that emphasizes self-management and self-awareness more than other texts.
back to top
Users without a subscription are not able to see the full content on this page. Please subscribe or login .
Oxford Bibliographies Online is available by subscription and perpetual access to institutions. For more information or to contact an Oxford Sales Representative click here .
- About Psychology »
- Meet the Editorial Board »
- Academic Assessment
- Acculturation and Health
- Action Regulation Theory
- Action Research
- Addictive Behavior
- Adolescence
- Adoption, Social, Psychological, and Evolutionary Perspect...
- Advanced Theory of Mind
- Affective Forecasting
- Affirmative Action
- Ageism at Work
- Allport, Gordon
- Alzheimer’s Disease
- Ambulatory Assessment in Behavioral Science
- Analysis of Covariance (ANCOVA)
- Animal Behavior
- Animal Learning
- Anxiety Disorders
- Art and Aesthetics, Psychology of
- Artificial Intelligence, Machine Learning, and Psychology
- Assessment and Clinical Applications of Individual Differe...
- Attachment in Social and Emotional Development across the ...
- Attention-Deficit/Hyperactivity Disorder (ADHD) in Adults
- Attention-Deficit/Hyperactivity Disorder (ADHD) in Childre...
- Attitudinal Ambivalence
- Attraction in Close Relationships
- Attribution Theory
- Authoritarian Personality
- Bayesian Statistical Methods in Psychology
- Behavior Therapy, Rational Emotive
- Behavioral Economics
- Behavioral Genetics
- Belief Perseverance
- Bereavement and Grief
- Biological Psychology
- Birth Order
- Body Image in Men and Women
- Bystander Effect
- Categorical Data Analysis in Psychology
- Childhood and Adolescence, Peer Victimization and Bullying...
- Clark, Mamie Phipps
- Clinical Neuropsychology
- Cognitive Consistency Theories
- Cognitive Dissonance Theory
- Cognitive Neuroscience
- Communication, Nonverbal Cues and
- Comparative Psychology
- Competence to Stand Trial: Restoration Services
- Competency to Stand Trial
- Computational Psychology
- Conflict Management in the Workplace
- Conformity, Compliance, and Obedience
- Consciousness
- Coping Processes
- Correspondence Analysis in Psychology
- Creativity at Work
- Critical Thinking
- Cross-Cultural Psychology
- Cultural Psychology
- Daily Life, Research Methods for Studying
- Data Science Methods for Psychology
- Data Sharing in Psychology
- Death and Dying
- Deceiving and Detecting Deceit
- Defensive Processes
- Depressive Disorders
- Development, Prenatal
- Developmental Psychology (Cognitive)
- Developmental Psychology (Social)
- Diagnostic and Statistical Manual of Mental Disorders (DSM...
- Discrimination
- Dissociative Disorders
- Drugs and Behavior
- Eating Disorders
- Ecological Psychology
- Educational Settings, Assessment of Thinking in
- Effect Size
- Embodiment and Embodied Cognition
- Emerging Adulthood
- Emotional Intelligence
- Empathy and Altruism
- Employee Stress and Well-Being
- Environmental Neuroscience and Environmental Psychology
- Ethics in Psychological Practice
- Event Perception
- Evolutionary Psychology
- Expansive Posture
- Experimental Existential Psychology
- Exploratory Data Analysis
- Eyewitness Testimony
- Eysenck, Hans
- Factor Analysis
- Festinger, Leon
- Five-Factor Model of Personality
- Flynn Effect, The
- Forgiveness
- Friendships, Children's
- Fundamental Attribution Error/Correspondence Bias
- Gambler's Fallacy
- Game Theory and Psychology
- Geropsychology, Clinical
- Global Mental Health
- Habit Formation and Behavior Change
- Health Psychology
- Health Psychology Research and Practice, Measurement in
- Heider, Fritz
- Heuristics and Biases
- History of Psychology
- Human Factors
- Humanistic Psychology
- Implicit Association Test (IAT)
- Industrial and Organizational Psychology
- Inferential Statistics in Psychology
- Insanity Defense, The
- Intelligence
- Intelligence, Crystallized and Fluid
- Intercultural Psychology
- Intergroup Conflict
- International Classification of Diseases and Related Healt...
- International Psychology
- Interviewing in Forensic Settings
- Intimate Partner Violence, Psychological Perspectives on
- Introversion–Extraversion
- Item Response Theory
- Law, Psychology and
- Lazarus, Richard
- Learned Helplessness
- Learning Theory
- Learning versus Performance
- LGBTQ+ Romantic Relationships
- Lie Detection in a Forensic Context
- Life-Span Development
- Locus of Control
- Loneliness and Health
- Mathematical Psychology
- Meaning in Life
- Mechanisms and Processes of Peer Contagion
- Media Violence, Psychological Perspectives on
- Mediation Analysis
- Memories, Autobiographical
- Memories, Flashbulb
- Memories, Repressed and Recovered
- Memory, False
- Memory, Human
- Memory, Implicit versus Explicit
- Memory in Educational Settings
- Memory, Semantic
- Meta-Analysis
- Metacognition
- Metaphor, Psychological Perspectives on
- Microaggressions
- Military Psychology
- Mindfulness
- Mindfulness and Education
- Minnesota Multiphasic Personality Inventory (MMPI)
- Money, Psychology of
- Moral Conviction
- Moral Development
- Moral Psychology
- Moral Reasoning
- Nature versus Nurture Debate in Psychology
- Neuroscience of Associative Learning
- Nonergodicity in Psychology and Neuroscience
- Nonparametric Statistical Analysis in Psychology
- Observational (Non-Randomized) Studies
- Obsessive-Complusive Disorder (OCD)
- Occupational Health Psychology
- Olfaction, Human
- Operant Conditioning
- Optimism and Pessimism
- Organizational Justice
- Parenting Stress
- Parenting Styles
- Parents' Beliefs about Children
- Path Models
- Peace Psychology
- Perception, Person
- Performance Appraisal
- Personality and Health
- Personality Disorders
- Personality Psychology
- Person-Centered and Experiential Psychotherapies: From Car...
- Phenomenological Psychology
- Placebo Effects in Psychology
- Play Behavior
- Positive Psychological Capital (PsyCap)
- Positive Psychology
- Posttraumatic Stress Disorder (PTSD)
- Prejudice and Stereotyping
- Pretrial Publicity
- Prisoner's Dilemma
- Problem Solving and Decision Making
- Procrastination
- Prosocial Behavior
- Prosocial Spending and Well-Being
- Protocol Analysis
- Psycholinguistics
- Psychological Literacy
- Psychological Perspectives on Food and Eating
- Psychology, Political
- Psychoneuroimmunology
- Psychophysics, Visual
- Psychotherapy
- Psychotic Disorders
- Publication Bias in Psychology
- Reasoning, Counterfactual
- Rehabilitation Psychology
- Relationships
- Reliability–Contemporary Psychometric Conceptions
- Religion, Psychology and
- Replication Initiatives in Psychology
- Research Methods
- Risk Taking
- Role of the Expert Witness in Forensic Psychology, The
- Sample Size Planning for Statistical Power and Accurate Es...
- Schizophrenic Disorders
- School Psychology
- School Psychology, Counseling Services in
- Self, Gender and
- Self, Psychology of the
- Self-Construal
- Self-Control
- Self-Deception
- Self-Determination Theory
- Self-Efficacy
- Self-Esteem
- Self-Monitoring
- Self-Regulation in Educational Settings
- Self-Report Tests, Measures, and Inventories in Clinical P...
- Sensation Seeking
- Sex and Gender
- Sexual Minority Parenting
- Sexual Orientation
- Signal Detection Theory and its Applications
- Simpson's Paradox in Psychology
- Single People
- Single-Case Experimental Designs
- Skinner, B.F.
- Sleep and Dreaming
- Small Groups
- Social Class and Social Status
- Social Cognition
- Social Neuroscience
- Social Support
- Social Touch and Massage Therapy Research
- Somatoform Disorders
- Spatial Attention
- Sports Psychology
- Stanford Prison Experiment (SPE): Icon and Controversy
- Stereotype Threat
- Stereotypes
- Stress and Coping, Psychology of
- Student Success in College
- Subjective Wellbeing Homeostasis
- Taste, Psychological Perspectives on
- Teaching of Psychology
- Terror Management Theory
- Testing and Assessment
- The Concept of Validity in Psychological Assessment
- The Neuroscience of Emotion Regulation
- The Reasoned Action Approach and the Theories of Reasoned ...
- The Weapon Focus Effect in Eyewitness Memory
- Theory of Mind
- Therapy, Cognitive-Behavioral
- Thinking Skills in Educational Settings
- Time Perception
- Trait Perspective
- Trauma Psychology
- Twin Studies
- Type A Behavior Pattern (Coronary Prone Personality)
- Unconscious Processes
- Video Games and Violent Content
- Virtues and Character Strengths
- Women and Science, Technology, Engineering, and Math (STEM...
- Women, Psychology of
- Work Well-Being
- Workforce Training Evaluation
- Wundt, Wilhelm
- Privacy Policy
- Cookie Policy
- Legal Notice
- Accessibility
Powered by:
- [66.249.64.20|81.177.182.174]
- 81.177.182.174
Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
4 The Essence of Ethics for Psychological Researchers and Psychologists
Tanya Machin and Charlotte Brownlow
This chapter uses material from an open access human research ethics e-course developed with the support of an Open Access Teaching Award from the University of Southern Queensland. The original authors were Tanya Machin, Charlotte Brownlow, and Annmaree Jackson. The e-course can be found at https://open.usq.edu.au/course/view.php?id=400 or by directly contacting Tanya at [email protected] or Charlotte at [email protected] .
Introduction
Our aim in this chapter is to provide you with a broad overview of the different ethical codes used in Australia that psychological scientists and psychologists use to guide their work. As a psychology student you’re no doubt used to thinking about ethics as this underpins much of the foundational knowledge you learn in your degree. However, you may be unfamiliar with why ethics are important (although we hope not!) or when or how ethical codes are used. The first ethical code was developed by the National Health and Medical Research Council (NHMRC) and is known as The National Statement on Ethical Conduct in Human Research (NHMRC, 2018b) or the ‘NHMRC code’ or simply ‘the code’. This document consists of a series of guidelines that all researchers – including psychological scientists – need to follow. Australia is unique in that our researchers are governed by this code, but our psychologists are required to adhere to a different ethical code developed by the Australian Psychological Society. Countries such as the United Kingdom or Canada have a combined professional and research code of ethics.
To help you work your way through the chapter, we’ve divided it into several sections, including: ‘Why Do We Have Research Ethics?’, ‘Research Methodology and Risk Management’, ‘Recruitment and Data Collection’, ‘Data and Information Management’, and ‘Merit, Integrity, and Monitoring’. We will then provide a brief overview of the APS code to close the chapter off. Throughout the chapter, we’ll provide some case studies, pose questions for you to reflect on, and perhaps even test your ethical knowledge! Finally, the information contained in this chapter comes from an open access e-course that we wrote. If you have any questions about the e-course or want to use it in your course or program, please contact the authors directly.
Why do we have research ethics?
The history of human experimentation is sometimes considered to be a dark one, with many documented examples of ill-conceived and inhumane medical and psychological experimentation on human beings. While considered ‘unethical’ by today’s standards, these experiments have led to the development and refinement of various national and international laws and guidelines that govern ethical human research.
Case Study: The Tuskegee Syphilis Study
In 1932, the United States of America Public Health Service (PHS) began a twelve-month experiment in Tuskegee, Alabama to study the natural course of untreated syphilis in African American men. The research aimed to determine whether syphilis caused cardiovascular disease more often than neurological damage and to determine if the course of syphilis was different between black and white men. When the study began, there was no known cure for syphilis.
From an ethical perspective, this research provides an excellent case study on how NOT to conduct research responsibly. Researchers initially recruited 600 men: 399 with syphilis and 201 who did not have syphilis. Poor, uneducated African American men were targeted for participation (Centers for Disease Control and Prevention [CDC] (2021)). As an ‘incentive’ to join research, free medical exams, meals, and burial insurance were offered. The PHS never told the participants they were part of a syphilis study – some men thoughts they were being treated for rheumatism or bad stomachs (Brown, 2017). When penicillin became available as the recommended treatment in 1945, the treatment was withheld from participants (Tuskegee University, n.d). The study was initially supposed to be conducted over a six-month period, however, the study ran for 40 years without subsequent ethical review despite the introduction of numerous international ethical guideline documents.
When Dr John Heller, Director of the PHS Venereal Diseases Unit (1943 to 1948), was interviewed about the research project in 1976, he reflected that the men were considered purely as subjects in a study rather than patients who were in need of treatment.
What Did We Learn?
By today’s standards, this research would not be approved by an ethical review body on the basis of:
- lack of voluntary and informed consent processes
- inappropriate use of deception in various stages of research conduct
- use of inappropriate incentives and payments that have likely induced and encouraged the participants to take risks by participating in the research
- withholding known treatments that would benefit the participant once available
- knowingly permitting transmission of the disease to other non-participant individuals (e.g., wives and children of the participant men)
- lack of reporting and monitoring processes.
Video 4.1 provides a 10-minute summary of the Tuskagee Study.
Video 4.1: The Tuskegee Syphilis Study
Governance of Human Research
Today research involving humans is tightly governed. Governance of human research is about establishing both rights for participants in research and the responsibilities of those conducting the research (that’s you as a researcher and your research institution). This can include:
- ethical review and approval
- compliance with legislation, regulations, guidelines and codes of practice
- legal matters – including contracts – and indemnity/insurance frameworks
- financial management, risk management, and site-specific assessment
- institutional policies and procedures for responsible research conduct and managing research misconduct
- management of collaborative research
- research requirements (DIIS, 2005).
Research in Australia is normally conducted under the auspices of the Australian Code for the Responsible Conduct of Research (NHMRC, 2018) and the National Statement on Ethical Conduct in Human Research, (NHMCR, 2018b). Specific national and state legislation may also apply in the protection of participant rights, including relevant privacy laws. Depending on your targeted research population, specific reviews, approvals, and guidelines may also be required – for example, when working with Aboriginal and Torres Strait Islander peoples and communities. You’re responsible for ensuring you’re aware of and comply with the relevant legal and institutional requirements when conducting your research.
The National Statement on Ethical Conduct in Human Research (NHMRC, 2018b) outlines four guiding principles for ethical research. You may want to compare your own research (or research you read about in journal articles) against these checklists to ensure you’re addressing the four guiding principles detailed below.
Research Merit and Integrity
Your research has merit if it is:
- justifiable by its potential benefit – e.g., contribution to knowledge and understanding, improved social welfare and individual wellbeing, within the skills and expertise of researchers
- designed/developed using methods appropriate for achieving the aims of the proposal
- based on a thorough study of the current literature (as well as previous studies)
- designed to ensure respect for the participants is not compromised by the aims of the research by the way it is carried out or by the results
- conducted or supervised by persons or teams with experience, qualifications, and competence that are appropriate for the research.
You are conducting your research with integrity if you and the research team are committed to:
- searching for knowledge and understanding
- following recognised principles of research conduct
- conducting the research honestly
- disseminating and communicating the results (whether favourable or unfavourable) in ways that permit scrutiny and contribute to public knowledge and understanding.
Your research is just if you:
- select, exclude, and include categories of participants fairly, and accurately describe the process in the results of your research
- recruit participants fairly
- ensure there is no unfair burden of participation in research on any particular group(s)
- fairly distribute the benefits of participating in the research
- do not exploit participants in the conduct of your research
- provide fair access to the benefits of the research
- make the research outcomes accessible to research participants in a way that is timely and clear.
Beneficence
Your research demonstrates beneficence if you:
- ensure there is likely benefit of the research to the participants, to the wider community, or both
- assess that the likely benefit of the results justifies any risk of harm or discomfort to the participants
- have designed the research to minimise the risk of harms or discomfort to the participants
- clarify for the participants the potential benefits and the risks of the research
- ensure the welfare of the participants (in the conduct of the research)
- suspend the research where the risks to participants are no longer justified by the potential benefits
- consider whether research should be discontinued or at least modified (in the event it’s suspended)
- notify the review body promptly if you do suspend the research.
Your research demonstrates respect if you:
- abide by the values of research merit and integrity, justice, and beneficence
- have due regard for the welfare, beliefs, perceptions, customs, and cultural heritage of individual (and collective) participants and groups involved in the research
- respect the privacy, confidentiality, and cultural sensitivities of the participants
- fulfil any specific agreements made with participants or their communities
- give due scope throughout the research process to the capacity of individuals to make their own decisions
- empower individuals where possible and protect them as necessary where they may be unable to make their own decisions or have diminished capacity to do so.
Processes of Ethical Review in Australia
Ethical review of human research can be undertaken at various levels, according to the degree of risk involved in the research, and the levels of review established at a research institution. In all cases, the ethical review of human research is undertaken in accordance with the guiding ethical principles and process of research governance and ethical review outlined within the National Statement on Ethical Conduct in Human Research (2018b). With regard to the assessment of risk involved in research this involves:
- identifying any risks
- gauging their probability and severity
- assessing the extent to which they can be minimised
- determining whether they are justified by the potential benefits of the research
- determining how they can be managed.
You’ll be involved in identifying, gauging, minimising, and managing any risks involved in your project – normally as part of preparing and submitting your ethics application. The Human Research Ethics Committee (HREC) – or other ethical review bodies – will review your research proposal to make a judgement on whether the risks are justified by the potential benefits. Individuals you approach to participate in your research will also assess the risks associated with your research as they decide whether or not they consent to participate.
Research methodology and risk management
The research methodology you adopt for your project will be crucial in considering ethical risk and the management of this. There are two broad types of research – quantitative or qualitative methods – and both types of methods have different advantages and disadvantages. The choice of which method you will use is determined by your research question. This topic will explore some of the common approaches to research and some of the associated ethical issues to consider when adopting these.
Research can have an impact on participants both during the conduct of the research and after the research has been completed as they reflect upon their experience of participation (mental) and recovery from any physical demands (e.g., donation of human biospecimens, physical testing, etc.). While this list of potential risks is not exhaustive, some of the common risks are identified below. Risk of participation to a participant (or you and the research team) is generally classified along a continuum, with ‘Inconvenience’ – for activities such as the time required to fill out a survey or take part in an interview – at the low end of the scale, and ‘Harm’ – at the high end of the scale. ‘Discomfort’ is somewhere in the middle, and this can include both physical and psychological aspects. This could include side effects of drugs that participants may need to take in the research or even anxiety when attending a research interview.
All research must have a benefit that either directly or indirectly benefits individuals, groups, or society as a whole. Benefits of research can include gains in specific knowledge, improved individual wellbeing, or increases in the skill or expertise of an individual, group, or organisation. While your research may have no immediate benefit to the participants, it’s worth considering whether participants can benefit from self-reflection on the research topic. For example, you may be interested in parenting styles and discipline, and while your research may not have an immediate benefit to this group of participants, they may benefit from self-reflecting on their own parenting practices.
Managing Risks
Much of the research conducted using human participants will have some degree of remaining risk to a participant or the research, despite any mitigation strategies you’ve applied in the research design phase. Even if the remaining risk is minimal, it’s up to you to develop clear strategies for managing these remaining risks should they eventuate. This is not always an easy task as it can be difficult for you to know if a particular topic will cause distress or harm for an individual participant. Therefore, it’s important for you to think carefully about how you’ll support a participant if they become upset or distressed. You’ll also need to think carefully about government regulations and guidelines.
Ethics Risks – Confidentiality
You may be interviewing children about their television viewing habits when the child reveals information about child abuse. Would you know what to do in this situation? Do you have a legal obligation to report this disclosure? Who can you tell to protect the child while maintaining participant confidentiality?
Finally, when thinking about risks and benefits of the research, you’ll need to consider the following practical elements:
- What is the research theme or question that this project is designed to explore?
- Why is the exploration of this theme or answer to this question worth pursuing?
- How will the planned methodology and methods explore the theme or achieve the aims of the research?
Quantitative Methods
There are many different research methodologies, and the methodology you choose will depend on the research aims, questions, and/or hypotheses.
Research Surveys and Questionnaires
One of the most common methods for conducting research is surveys or questionnaires. In the past, participants would often complete pen-and-paper surveys and either hand them to the researcher or mail the survey to the researcher. Nowadays most researchers would use online survey software such as Qualtrics or Survey Monkey (it’s always best to check with your university to see what survey software they recommend – at USQ we use the USQ Survey Tool , which was developed from LimeSurvey ). Surveys/questionnaires can be quantitative when questions use a closed question format (e.g., Likert scales) or can be qualitative when an open question format is used. Many surveys/questionnaires can contain a combination of the two types of questions (mixed method).
Ethical risks to consider:
- How long will it take participants to complete the survey?
- Could the content of the questions cause/trigger psychological harms, economic harms, or legal harms to participants?
- Could the research cause social harm to participants? Is your survey/questionnaire voluntary and anonymous?
- How secure is the online survey software?
- Where will the data be collected, stored, and transferred? You’ll need to check the terms and conditions of the software licence to ensure you have full access and ownership of the data and are aware of relevant privacy laws.
Additional considerations:
- Make sure you have permission to use any measures or scales that you want to include in your survey or questionnaire – seek permission from the copyright owner as required.
- Ensure you have sufficient qualifications and/or experience to administer and/or analyse the data from the survey or questionnaire if this is a standardised test or test bank.
Ethics Risks – Genetic Testing
Your grandfather provided a human biospecimen 50 years ago for a research project. Advances in medical science mean that it’s now possible to predict with accuracy that you’ll acquire a certain illness. Would you feel comfortable with this information being published? Would you want to know this information?
Qualitative Methodologies
There are many different research methodologies, and the methodology you choose will depend on the research aims, questions, and/or hypotheses. A strength of qualitative research is that it permits a participant to describe their experiences in ways that are meaningful to them, rather than to group their experience using research-derived classifications (Shaughnessy et al. , 2006).
Research Interviews
Interviews involve conducting discussions with a small number of participants to explore a particular phenomenon of interest. Typically, there are three different types of interviews:
- structured interview s where there is a set of predetermined questions that all participants answer in the same order without any variation to the questions
- unstructured interviews where there are no predetermined questions, and the interview is quite informal and unstructured
- semi-structured interviews contain elements from both the structured and unstructured interviews. That is, there are some predetermined questions, but the interviewer can change the order of the questions or ask additional questions for further clarification or to expand on an issue that arises during the interview.
- It’s important to protect your participants’ identities, and this may be done through a process to remove any identifying information, such as replacing a participant’s name with the use of a pseudonym.
- Length of time it takes a participant to complete the interview. This might vary from 10 minutes to a couple of hours. Please try and keep interviews under one hour if you can and offer your participant breaks, water, or snacks if they need them.
- Talking to another person can arouse people’s emotions, and so you may need to consider this risk. That is, you’ll need to consider the content of the questions you’re asking: could they cause/trigger psychological harms, economic harms, or legal harms? Participants may also want to stop the interview if they find the questions distressing or upsetting. If you’re uncertain about whether a participant wants to continue – ask them. If you’re in doubt, you’ll need to stop data collection, contact your supervisors or other members of the research team, and you may need to make a report to your research institution’s ethics office. Remember, if a participant asks to stop an interview you must not under any circumstance try and cajole them into continuing.
- As a researcher, you’ll need to reflect on whether you have the skills to deal with an upset participant. Some topics should be left to interviewers with skills in psychology or counselling.
- Plan ahead and include information about appropriate referral services in the participant information sheet, even if you do not personally think a topic is distressing.
Recruitment and data collection
Recruiting participants in responsible ways is a core part of the research process and something to which careful attention is paid during assessment of the research ethics of a project. This topic will focus on the responsible recruitment of research participants and the collection of data from individuals.
Recruitment of Research Participants
The strategies you use to recruit your participants will be varied, and you’ll need to think carefully about the research methodology you’ve chosen and who your participants are. For example, are you approaching your work from a quantitative perspective? If so, then you’ll need to gather data from lots of participants and therefore your recruitment will need to be broad if you’re trying to take a sample that could be considered representative of a wider population.
If you’re drawing on qualitative methodologies, then your approach might be different in that you’ll likely be focusing on a much smaller number of participants who have a shared experience of a particular phenomenon and are therefore looking for a more homogenous sample. Your recruitment, in this case, would be more targeted.
You also need to carefully consider your inclusion and exclusion criteria for your participants. Do you, for example, want to focus on a particular age group, occupation, or social class? These criteria need to be made explicit in your application form to enable an accurate assessment of the risks associated with your research.
The strategies you choose to recruit your participants’ will also carry different levels of risk, and these need to be considered as part of your research design and ethics reflections.
Recruiting From Your Acquaintance Network
Recruiting people who you know, or friends of friends has the benefit of more straightforward access to your participants. However, one thing to consider if you’re planning to recruit participants through this strategy is social risk. Do the people who you approach feel obliged in some way to take part in the research? Will your relationship with them be compromised in any way if they either refuse to take part in the research or don’t provide the expected responses? Are these participants’ fellow employees within a company, for example, and are there issues of confidentiality and future impacts on working relationships that need to be considered?
These issues will, of course, be influenced again by your research design. If you’re planning a quantitative survey that is anonymous then the social risks will be reduced. However, if you’re planning to interview participants about a sensitive or personal topic then the social risks will be considered higher.
Vulnerable Participants
Some participants are more vulnerable than others in the research process, and as part of your ethics application, you’ll be asked to carefully consider who your target participants are and whether these comprise what are considered a vulnerable population. Such populations include research with a pregnant woman or foetus, children, people with cognitive impairment or mental illness, people considered to be a forensic or involuntary patient, people with impaired capacity for communication, incarcerated individuals or people on parole, those highly dependent on medical care or who are in hospital, military personnel or veterans, Aboriginal and Torres Strait Islander peoples, people in other countries or who would consider English to be a second language, and those who would not usually be considered vulnerable but would be considered vulnerable in the context of the proposed research project.
Children can provide a wealth of important information, but due to their age and cognitive immaturity, special attention needs to be given to safeguarding them in their participation in research. One crucial element is that of consent, which we’ll discuss a bit later in the chapter. Care and attention also need to ensure that the rights of children are protected in terms of confidentiality and potential coercion into participation in projects.
Research that is undertaken within schools may require the additional approval of the education governing body, and therefore careful attention needs to be paid to this in the research planning stages. Also, think carefully about the tasks you’re requiring the children to do. If a child (or their parents) does not consent to taking part in a school-based activity that will comprise the research, what equitable activity will you provide for them to do instead?
Recruitment of Aboriginal and Torres Strait Islander Peoples
There is great diversity across the many Aboriginal and Torres Strait Islander cultures and societies. Application of core values and cultural and local protocols should be determined by the Aboriginal and Torres Strait Islander communities or groups involved in the research. This means you need to engage with the people or communities you want to research to discuss your proposed research and agree to the best way forward prior to seeking your ethical approval.
Unfortunately, that didn’t always occur in the past. Consider, for example, the Cambridge anthropology expedition to the Torres Strait that took place in the late nineteenth century, or later research with indigenous groups that had little contact with white Australian culture but were given tests of cognitive ability without considering how constructs such as intelligence may be expressed in different cultural settings (Dudgeon et al., 2014). In 2016, at the national Australian Psychological Society conference, the APS acknowledged the role psychology played in the mistreatment and erosion of Aboriginal and Torres Strait Islander culture.
It’s therefore important that if you’re undertaking research with Aboriginal and Torres Strait Islanders, you think about the research collaboratively. You may find the Ethical Conduct in Research With Aboriginal and Torres Strait Islander Peoples and Communities: Guidelines for Researchers and Stakeholders (NHRMC, 2018a) informative.
If you’re undertaking health research that is targeting Aboriginal and Torres Strait Islander peoples and communities, you must consult the above guidelines and may find the following useful: Keeping Research on Track II (NHMRC, 2018d) and the Guidelines for Ethical Research in Australian Indigenous Studies (Australian Institute of Aboriginal and Torres Strait Islander Studies [AIATSIS], 2012).
When you think of obtaining consent, what comes to mind? You may indicate that it could involve signing a consent form prior to taking part in the research. While this is a common component of obtaining consent, this may not be suitable – or even practical – if you propose to administer an online survey. Therefore, a well-designed consent strategy will need to be tailored to your potential participants and fit with your research methodology and research methods. Consent should also be viewed as a process, rather than a single point in time event. That is, obtaining consent may be a component of the processes you undertake when consulting, engaging, and negotiating to prepare for your research conduct. This will be especially relevant in the context of research involving Aboriginal and Torres Strait Islander peoples and communities.
The requirement for consent is a relatively new concept, having evolved predominantly through unscrupulous researchers using a participant as a means to an end – for example, the Tuskegee researchers we discussed earlier in the chapter. Subsequently, international and national guidelines, such as the Belmont Report (National Commission for the Protection of Human Subjects of Biomedical and Behavioural Research, 2012) and the National Statement on Ethical Conduct in Human Research, 2007 (updated 2018) (NHMRC, 2018b) have been produced to empower and protect participants to make an informed decision about their participation in research.
Elements of Consent
When obtaining consent from a participant, you need to ensure that it’s provided voluntarily. That is, that the individual has agreed to take part in the research as a result of having being provided sufficient information, understood that information, and not been coerced (or felt pressured), nor overly enticed to partake (through inappropriate incentive or reward).
This raises a number of decision points that you’ll need to work through, for example:
- How much information do I need to provide about the study?
- How will I obtain voluntary participation?
- Who will be involved in recruiting the participants?
- How will I ascertain if the participant understands the information I’ve provided about the project?
- Does the participant have any expectations about the outcomes of the project – for example, in medical research, will they be expecting treatment of a known condition or illness, versus understanding they’re participating in research and may be assigned to a control (i.e., no treatment group)?
- Who needs to be involved in the decision to provide consent? E.g., Will all participants have the capacity for understanding and/or the legal capacity to provide consent? If not, when do others need to be involved in this decision? This would involve situations where the participant lacks the capacity to provide consent, e.g., elderly person with dementia.
Consent Approaches
Normally, ethical review bodies like to see that you can demonstrate that a participant in your research has provided consent. It’s therefore worth considering how you’ve determined the participant has the sufficient capacity to give their consent to take part in the research and how you will document this. Where written consent from a healthy adult participant is provided, this would not normally be a problem. However, for some more sensitive research topics where participants may be reluctant to provide their name or signature, you may need to consider an alternative consent strategy to the traditional written or recorded approach to protect the privacy and confidentiality of your participant. Similarly, if you’re working with children and young people, or with individuals who may be unable to give consent because they’re temporarily or permanently incapable of comprehending their situation or of communicating about it, you’ll need to develop a consent strategy. This strategy will need to empower these individuals to be involved in the decision to participate as much as they are able. You’ll also need to consider who else may need to be involved to provide the required ethical and legal consent. In some cases, such as physical or mental health, participants may not be able to provide consent to participate in the research. For example, if you wanted to observe a person with end-stage dementia they would be unable to give consent, however, an appropriate surrogate – such as someone with a legal power of attorney – may be able to give consent on their behalf. Sometimes people may be temporarily unable to give consent. For instance, if they’re under the influence of drugs or alcohol. Being able to give consent is different when considering research with child participants – children are not assumed to be incompetent due to their age, but there may be additional steps you need to take for children to give their consent. In some cases – for example, research that is conducted in medical care settings such as neonatal intensive care, terminal care, or emergency and intensive care – relevant jurisdictional laws will also need to be considered.
Data and information management
In your ethics application, you’ll need to think critically about the issues of data collection, use, and management of data and information. You will also need to consider ethical issues related to the generation, collection, access, use, analysis, disclosure, storage, retention, disposal, sharing and re-use of data and information. This will be the focus of this section.
Information Versus Research Data Versus Primary Materials
Data generally refers to bits of information. Data can also refer to raw data, cleaned data, transformed data, summary data, and/or metadata (data about data). Data can also refer to research outputs and outcomes. Information, on the other hand, generally refers to data that has been interpreted, analysed, or contextualised, and can take many different forms. You may also see questions in an ethics application about primary materials. This typically refers to physical objects acquired through a process of scholarly investigation from which data may be derived. This may include objects such as ore or biological materials, but also questionnaires, recordings, artworks, and photographs.
Some examples of research data and primary materials can include, but are not limited to:
- what participants say in interviews, focus groups, questionnaires/surveys, personal histories and biographies
- images, audio recordings, and other audiovisual materials
- records generated for administrative purposes (e.g., billing, service provision, etc.) or as required by legislation (e.g., disease notification)
- digital information generated directly by a population through their use of mobile devices and the internet (e.g., Twitter feeds)
- physical specimens or artefacts
- information or reports generated by analysis of existing personal information (from clinical, organisational, social, observational or other sources)
- observations
- results from experimental testing and investigations
- information derived from human biospecimens such as blood, bone, muscle, and urine.
It’s quite common for people to get confused between research methods and primary materials in their ethics application. It’s really important when completing your ethics application that you clearly articulate the context. For example, are you writing about a questionnaire as a research method for obtaining research data, or is the questionnaire the primary material (i.e., the survey instrument)? Remember that reviewers of your application need to be able to understand what you’re trying to say and therefore it’s important to use the correct terminology.
Identification of Information
Information is identifiable if someone is able to identify an individual from information that is included in a thesis or journal article. Types of identifiable information include names, date of birth, address, images or photos, or group affiliation.
Re-identifiable information is information that has had any personal identifiers removed and replaced with a pseudonym and/or a code. Even with these types of precautions, it’s potentially still possible to re-identify that person. For example, you may be interviewing employees at Company X about their workplace health and safety. Company X may only have 20 employees and so it’s possible that some of their individual comments or responses could reveal their identify to people who know the employees at Company X.
No doubt you’ve heard (and most likely read) the term ‘de-identified’. However, ethical review boards prefer the use of either identifiable, re-identifiable, or non-identifiable. This is because the term de-identified can be ambiguous in its meaning. For example, are you proposing that you’ll run a process to remove any personal identifiers from research data/information you collect, to protect an individual’s privacy? Or do you mean that you have collected the information without any personal information in the first place? Many researchers use the term to indicate that they will ‘de-identify’ the participants, which is incorrect, whereas non-identifiable information is data that has never had any individual identifiers or that a process had been applied to to permanently removed any personally identifying information.
It’s also important to remember that the removal of personal identifiers may or may not be ethically required and some research projects may legitimately require the retention of personal identifiers. For example, if you were conducting biographic research into the bullying and subsequent suicide of Charlotte Dawson , you would want to include any personally identifying information such as tweets she made to internet trolls.
Personal Identification and the Law
As an ethical researcher, you’re no doubt thinking about how you can protect the privacy of your participants. In Australia, a participant’s personal information is protected by law under the Privacy Act (1988) . Personal information is not just limited to information about an individual’s private or family life, but also extends to any information or opinion that is about that person or from which they can be reasonably identified (Office of the Australian Information Commissioner [OIAC], 2017). This can include information or opinion about:
- racial or ethnic origin
- political opinions
- religious beliefs
- sexual orientation
- criminal records
- health information
- credit information
- employee record information
- Tax File Number (TFN) information.
Note that this is regardless of whether personal information or opinion is also included within the scope of the Privacy Act (1988), and whether it’s recorded in a material form (or not). So, while the definition of privacy can be quite broad, it’s important that you consider how you collect, use, disseminate, store, and re-use information for research purposes.
To Identify or Not Identify?
You may think it would be simpler to remove any personal information from your research data or information and that would then reduce or eliminate the risk of being able to identify or re-identify any of your participants. In this way, their privacy would be now protected. Right?
Well… the answer is – it depends! There are some research methodologies where it’s entirely appropriate that others know who your research participants were. For example, if you need to match participant responses for questionnaires conducted at two different time points. It’s important to understand that the nature of identifiability can (and often does) change as you collect, use, analyse, disseminate research findings and store your research data and information. For example, data or information might initially be collected in a form that could identify individuals, then coded for analysis and connection to other collected data or information, and then once all the data or information has been collected, the code key might be destroyed, rendering the data or information anonymous.
It’s also worth considering how your participant may want to be represented throughout the research process. Would they be happy to be ‘anonymised’ or would they prefer for their thoughts and opinions to be heard? If you’re researching a sensitive topic that may have repercussions for a participant’s social or work relationships if their identity was known, then you’ll need to discuss this with your participant as well as manage any perceived risk associated with each option. As you can see, there are a lot of decisions you’ll need to make when considering how to manage this aspect of your research project.
The risks related to the identifiability of data and information in research are greatest when the identity of a specific person can reasonably be determined by reference to a specific identifier or a combination of identifiers. This situation may be the case when your recruited participants are part of a small population. This means you should take care in how you report your findings and will need to consider how much detail you provide around things like physical locations, specific recruitment groups, or associated organisations. For example, if you report that school principals from Catholic Education high schools in Central Queensland participated in your study, it may be well known within this community that there are only three schools that would fit this criteria. Therefore, it may not be too hard to link the opinions of the participants reported in your study to the school principals who work in those communities.
Risks may also arise where identifiers have been removed from the data or information and replaced by a code, but where it remains possible to re-identify a specific individual (by cracking the code or linking data to other data sets that contain identifiers). The technology that’s currently available (as well as what may be available in the future) may create new risks for data and/or information that was never labelled with individual identifiers, or from which identifiers have been permanently removed. For example, face recognition software means that people can be automatically identified without providing any specific permission.
Identifiability may also reflect features of the project, such as the nature of the participant sample. Specifically thinking about whether your data includes high-profile individuals or members of small communities versus larger populations. It’s also important to remember that large datasets are not immune to the risk of having participants re-identified.
Privacy, Confidentiality, and Anonymity
Privacy focuses on protecting the personal information of a participant that has taken part in your research project. This is not only an Australian requirement but complies with international laws. Confidentiality is different to privacy and focuses on the obligation of researchers to only use the private information provided to you by a participant for the purpose for which consent was given to you. This is both a moral and legal obligation, and depends on several factors, including the nature of the research and the promises you’ve given to the participants, along with any professional requirements you may need to fulfil. For example, you would typically outline the details of what data and information you plan to collect, use, disseminate, and re-use in an information sheet provided to participants before they take part in your research so they can then give their informed consent to participate. You must then abide by those details to maintain the requirements of confidentiality.
Some professions, however, are legally responsible for reporting certain information if they’re made aware of it. For example, if a teacher, psychologist, or counsellor becomes aware of child abuse, risk of self-harm, or harm to others, this information must be reported. It’s important to know your legal and professional responsibilities to report such information, who you report this information to, the appropriate process that should be followed, and when you can’t keep this information private. You must also inform your participants of these details, and this information is normally found in the information sheet.
When information is collected anonymously from a participant, no personally identifying or re-identifying information is provided. Anonymity, therefore, requires that the identity of a participant is protected because it’s not known to anybody either within or outside the research team. A good example would be when a participant completes an anonymous online questionnaire. Anonymity does not mean that you will not report any identifying information – in many cases you will report some details such as age range of your participants.
In some situations, you may not be able to ensure participants’ confidentiality or anonymity. For example, due to the nature of participating in a focus group, it’s impossible for you to guarantee that a participant’s confidentiality will be protected as there are other people present in the focus group. While you may ask the other participants to keep the discussions or other members in the focus groups confidential, in reality you can’t make someone keep this information confidential. To minimise these risks you could include information within the participant information reminding participants to keep details of the focus group confidential and reiterate this at the commencement of the focus group discussion.
Data Management
As a budding researcher, it’s important that you develop a data management plan that addresses issues related to the generation, collection, access, use, analysis, disclosure, storage, retention, disposal, sharing and re-use of data and information, as well as strategies for minimising risk. Your plan should be developed as early as possible in the research process and should include, but not be limited to, details regarding:
- physical, network, system security and any other technological security measures
- policies and procedures
- contractual and licensing arrangements and confidentiality agreements
- training for members of the project team and others, as appropriate
- the form in which the data or information will be stored during and after the project
- the purposes for which the data or information will be used and/or disclosed
- who owns the copyright and intellectual property
- who will be responsible for managing the data (data custodian)
- the conditions under which access to the data or information may be granted to others
- how the data will be shared for future use
- what information from the data management plan, if any, needs to be communicated to potential participants.
As a researcher, you will need to adopt methods to reduce the risk of identification during the collection, analysis and storage of data and information. Methods you may use include:
- minimising the number of variables collected from each participant
- separation and separate storage of identifiers and content information
- separating the roles of those responsible for the management of identifiers and those responsible for analysing content.
Using the Internet and Other Social Media
Data available on the internet can range from information that’s fully in the public domain to information that’s publicly available but that the creator or poster may consider private.
If you’re using information from social media in your research, you’ll need to consider:
- Is the information in the public or a private domain?
- Is permission required from a webpage, group administrator, or a specific person prior to using the data for research purposes?
- Do the terms and conditions of the webpage allow your research project to be conducted? The onus is on you to check the terms and conditions of each webpage to ensure you’re acting ethically within those guidelines.
- Is the individual who posted the information to a specific site likely to understand that that information could be accessed for research purposes?
How Long Do I Store My Research Data and Information?
Most universities and research institutions will have guidelines outlining their requirements for where data is stored, how long data is stored for, and the security and storage of the data. Typically, there are two stages of data storage: data collection and project completion.
While many people think that once a project is completed, they have to destroy the data, this is actually not the case at all. Instead, there are legally required retention periods for each state and territory across Australia, but a good rule of thumb is to keep the data for as long as it’s practical and responsible to do so. This is particularly helpful if you decide a year or two after the project to publish your research and you need to run additional analyses. If you’re working on a project with others, you’ll also need to consider whether others may want to work with the data in the future and who should retain a copy of the data file.
However, there is a minimum retention period that you’re required to comply with. Generally, research data must be retained for a minimum of five years after the project concludes or is abandoned. However, particular aspects of your research project – such as signed consent forms – may need to be retained for a longer period, e.g., 15 years in Queensland. If your research is significant or results in a patent, the data must be retained for a longer period. Research data from clinical trials has a higher retention requirement again, and some historical-based research may need to be retained indefinitely. It’s your responsibility to review the requirements for the type of research you’re undertaking and to make the appropriate short- and long-term arrangements for the data to be appropriately stored for the minimum required period. For example, if you’re a student working on a project the data should always be given to your supervisor at the completion of your project.
How Do I Store My Research Data and Information?
Research data and information must be kept secure and stored in conditions that are designed to reduce deterioration of the data. Most universities and research institutions will have guidelines for what are considered appropriate conditions, although these will also normally comply with the security and privacy requirements in Australia. While many researchers may use USB drives to store their data, this is NOT considered secure. Unfortunately, we’ve met too many student researchers whose data has been lost because of corrupted or lost USB drives, including when they go through the wash!
It’s therefore considered good research practice to store your research data in at least three separate ways. We recommend you consider using cloud storage to store research data during the active phase of your project as most universities provide free cloud storage for their students. However, you’ll need to think about the following questions when you’re choosing your data storage solutions:
- If you’re using cloud storage to store your date, consider selecting a cloud storage system based in Australia. This ensures the data is protected under Australian laws and regulations.
- Is the storage system appropriate for the data? For example, if you’re collecting sensitive health information or data, you may need additional security protocols.
- Is the storage system appropriate for the life of the research project?
- Can access be shared with other researchers if this is required? This includes other research team members during data collection, and other researchers into the future (but only if you’ve sought consent for the future use of the data in your ethical application).
All information on how you plan to collect, use, and store personal information from your participants needs to be clearly communicated in an information sheet that they can retain and/or ask questions about before they take part in the research.
Merit, integrity and monitoring
Before any research with or about humans, their data, or their tissue is conducted, it’s important for you to critically think about the application of ethical values and principles and incorporate these into your research project. These commonly include research merit and integrity, justice, beneficence, and respect. However, you also need to consider the competence of yourself and your research team to undertake the proposed research methodology and methods. Consideration also needs to be afforded to how you’ll monitor the conduct of your research against what has been approved, and what might occur if an ethics review body receives a complaint about the way you’re conducting the research. Specifically, this topic will focus on values and guiding ethical principles, monitoring approved research, and what occurs when a complaint is made.
Beneficence, Research Merit, Competence, and Integrity
Before you conduct any sort of research, it’s important to think broadly about whether the research has benefit to individuals, groups, or society more generally. A good way to think about beneficence is: Do the benefits of the research outweigh the risks to the participants? When you’re planning your research, your concern should always be that the participants will find the research valuable (and hopefully interesting!), even if there is no immediate benefit to them. Any risks to those who are participating in your research should be minimised (via your research design) and the remaining risks managed, and your participants should be fully informed about both the benefits and risks in taking part in the research.
The conduct of all research will have some level of risk attached, even if this is minimal. For example, social risk may be present when you approach your family or friends to take part in the research or a time imposition risk if you are conducting lengthy interviews, and this will need to be addressed in your ethics application. Of course, the participants will need to be informed in the participant information of any risk that may affect them. Please do not ever try to minimise or downplay the risks of taking part in the research – always be clear and honest with the participants. When thinking about risks, don’t forget to also consider the risks to you as the researcher. For example, if you’re conducting an interview, you should think about the interview time and location and whether this could pose any potential risks. If it does, you also need to think about how you’ll manage that risk.
Research Merit
When thinking about whether research has merit, this means the research is justified, of appropriate quality, and that the project is being conducted by researchers who have experience and competence in that area. More specifically, justification of research means there is a benefit to individuals, groups, or greater society, or that the research will provide new knowledge. Appropriate quality means that the research aims, hypotheses or research questions, methodology, and methods are all appropriate to the research being conducted. Experience and competence means the research investigator or team have suitable training in a range of areas such as cultural and historical understandings for the specific topic, and possess good communication skills.
Research Integrity
Another important principle that relates to both beneficence and research merit is research integrity. Research integrity shows that:
- the researcher has a genuine commitment to gaining a better understanding of specific knowledge
- the research will be disseminated to participants and society more broadly in ways that allow for greater contribution of knowledge on a topic, and for other researchers to critically examine the methods and results
ultimately to preserve and protect the trust that all participants place in research and researchers.
Respect is another important principle in ethical research and embodies a recognition that all human beings are valuable. Regarding research, this means that you, as a researcher, are committed to upholding a participant’s welfare above and beyond completing a specific research project or program. In other words, a participant is not to be treated as a means to justify an end, such as meeting the requirements for your research project, thesis, or survey completion. You also need to assess that you and the research team have appropriate knowledge of cultural groups, values, beliefs, and customs of the people you plan to engage with when conducting the research. It’s vitally important that you understand that culture and cultural difference are complex. While ethical review bodies appreciate that a researcher can’t be expected to ‘know it all’, you should be able to demonstrate that you’re aware of and mindful of any differences in values and culture your proposed participants may have to you, and are able to find appropriate ways to manage these differences.
Three ways to manage difference are:
- If you you’re targeting a specific group and feel that your cultural knowledge of this group could cause harm to the group, you may wish to reconsider the research or the research design.
- If, after careful consideration of the research or research design, you decide to go ahead with the research, you may want to invite someone with knowledge of the targeted participant group into your research team or seek them out as an advisor.
- If your targeted participation group may be vulnerable, also read through the ethical considerations specific to this participant group within the National Statement on Ethical Conduct in Human Research, 2007 (updated 2018).
Another element of being respectful to your participants is making sure they have all the information they need to make an informed choice about taking part in your research. For example, a participant will need to understand what your research is about, why you’re conducting the research, the process of the research (i.e., completing a survey or taking part in an interview) and the exact specifics of what they’ll need to do. This is one reason why it’s important that you write the participant information sheet clearly, concisely, and in plain language. It’s therefore essential that you limit or modify any scientific or discipline-specific words that your participants may have trouble understanding and include any acronyms or initialisms in full in the first instance.
Maintaining and honouring the rights and dignity of the participant is central. This is addressed, in part, through processes of confidentiality and privacy. When conducting research, the researcher will often ask participants detailed information about their life either for demographic purposes or as part of the research. For instance, demographic questions such as annual income or location. Participants need to know that you will respect the information given to you as part of the research process and trust that you will protect and manage that information appropriately. Some research could place the participant at significant risk if other people had access to that information, such as the disclosure of mental health disorders in the participant’s workplace. It’s important that you respect any personal disclosures from the participants and manage this information well. This could include strategies such as anonymising online questionnaires or using pseudonyms for participants who take part in interviews.
Working With People With Autism
Sometimes there are additional things we might need to consider when working with certain communities. One example we can draw on here is the autistic and autism communities. How might we consider the research questions we pose to ensure they’re in alignment with the priorities of these communities? How might we adapt our methods to allow for more inclusive practice? Sometimes we may need to think a little outside the box to ensure meaningful and respectful engagement with our research participants, while still maintaining the highest possible ethical standards. The Australian Autism Research Council (AARC) has recently published commentary on some research priorities and The Cooperative Research Centre for Living with Autism (Autism CRC) has some good guides concerning inclusive research practices .
It’s easy to understand justice when we think about our legal system, but how does justice apply to human research ethics? This principle would typically refer to equity. In other words, we don’t want to exploit the participants who take part in our research. In a similar way, you also need to ensure that any research that involves vulnerable groups:
- has additional safeguards
- includes all people in your research that want to take part
- shares research conclusions in a way that’s appropriate to the individual or the organisation.
Let’s unpack this a little more.
We’ve already discussed the principle of respect. Justice really takes this principle a step further. Think about people who may be considered vulnerable under our ethical guidelines. For example, a person with a disability, children, or those people whose first language is not English. As researchers, you may need to take extra measures to ensure these people are protected. For instance, you may need to have an interpreter present if you interview someone from a linguistically diverse background, or if you’re observing a child you may need to obtain a parent’s permission to approach the child to participate in the research (as well as seeking the child’s assent to participate).
We’ve discussed recruitment already in this chapter, but as students and potential researchers, you need to ensure this process is fair. Most researchers will recruit and select participants either randomly or purposefully. If you’re recruiting a purposive sample, you may need to ensure that no one is left out, particularly those people who may already feel discriminated against or marginalised. In other words, you can’t leave particular participants out of the research simply because it’s more convenient for you, the researcher. For example, you may want to ask school children about their family life, but some children may be excluded because they may be perceived as being difficult due to physical or emotional concerns.
As part of the research process, it’s important that you take the time to disseminate your research to participants, but also to the community more broadly. The way you decide to disseminate your research should be considered in your research planning. Again, make sure you plan how to discuss your research with groups or individuals who may struggle with lengthy research summaries. It’s considered good practice to summarise your research once it’s completed and send your finding through to any interested parties. If you’re a research student, you would make sure this is a one or two page summary rather than sending your participants a copy of your thesis!
As a researcher, you need to periodically assess and verify that the conduct of your research conforms to your approved ethical proposal. This is referred to as ‘monitoring approved research’. Each institution will have their own specific process for monitoring approved research, so we’ll discuss monitoring as a general process. Overall, each research institution will have ultimate responsibility for monitoring its approved research. Typically, you’ll be asked to complete reports at regular periods (depending on the level of risk associated with the research) and at the conclusion of the project. You’ll normally also be required to notify your research institution and the approving ethical review body if anything occurs that was unexpected or occurred in excess of what you expected via an ‘adverse event report’. Many institutions will also provide you with conditions on the ethical approval of your research, so be sure to read your ethics approval carefully! For instance, if there are any complaints from participants about the way you conduct your research, your institution’s approving ethical review body will need to be advised.
Progress reports would normally be required at least on an annual basis by institutions. At this time, you’ll include your research conduct progress to date, your compliance with the approved project, and note any complaints from participants or any changes to your research protocol. It’s important to note that if you decide to make changes to the way you want to conduct the research process, then you must seek approval prior to implementing any of these changes. Normally, this will be undertaken via an amendment application submission and approval process. Examples of when you will need to seek approval via an amendment application include: if one of the research team leaves the project, or if an additional measure or scale is added into a questionnaire.
On very rare occasions, situations may arise where either you, the research institution or the ethical review body may find reasons to discontinue or suspend research conduct. If you need to discontinue your research, be sure to inform both your research institution and the ethical review body as soon as possible. Where the institution or ethical review body suspends or withdraws ethical approval, you need to ensure that all participants are treated fairly and with respect. Where ethical approval is withdrawn, you’re also required to notify your participants about the withdrawal of ethical approval. Additionally, you must cease data collection for the project immediately once advised ethical approval has been suspended or withdrawn.
Complaints About Research
Your research institution may receive complaints about you (as a researcher) or the way in which the research is being conducted. Complaints can be made by research participants, researchers, staff of institutions, and members of the public. In Australia, the majority of research institutions follow the National Health and Medical Research Council (NHMRC)’s Guide to Managing and Investigating Potential Breaches of the Australian Code for the Responsible Conduct of Research, 2018 (commonly referred to as ‘the Code’). This document outlines that breaches of the Code occur on a spectrum, as well as factors to consider when determining the seriousness of a breach. The consideration and management of complaints, together with the principles of procedural fairness and stakeholder responsibilities – both for institutions and researchers – are also provided.
It’s important that you only conduct your research once you’ve been granted full approval by an ethical review body. Any conditions of approval must be maintained or met, and any deviation from the original approval must be approved by the ethical review body prior to you implementing those changes. If you have any questions about what constitutes a deviation or variation, contact your ethics office to discuss the requirements at your institution. Ignorance is not a defence when it comes to complying with the Code requirements, so it’s best to check if you have any questions or doubts.
The APS Code of Ethics
The Australian Psychology Society is the professional body of choice for psychologists in Australia with over 27,000 members (Allied Health Professions Australia, 2021). The organisation has several roles including advocacy and promotion of psychological knowledge, and provides many benefits for its members. The purpose of the APS Code of Ethics is to protect both the welfare of clients and the morals of the profession (APS, n.d.). The Code has three general ethical principles: Respect for the rights and dignity of people and peoples, Propriety, and Integrity. Within each principle are several ethical standards along with explanatory statements. For example, the general principle A (Respect for the rights and dignity of people and people) has an explanatory note that outlines the principle and then provides an explanatory statement before unpacking each specific ethical standard. If you read through the APS Code of Ethics, you’ll see some similarity with the NHMRC Code. However, the APS Code specifically articulates ethical professional conduct and responsibilities required to be adhered to by psychologists in their practice.
While we would love to share with you examples from the APS Code, unfortunately it’s copyrighted. However, if you’re a member of the APS, you have access to the APS Code and we encourage you to download the information and have a look.
No doubt as you read through the chapter, you learnt things you may only have had a small amount of knowledge about. However, we hope you finish the chapter with a better understanding of ethics and some of the decision-making that psychological scientists need to appreciate before they embark on a research project. We also hope that when you’re reading research articles, you can critically reflect on the ethical issues the researchers themselves may have had to consider.
This chapter has been written by Tanya Machin, School of Psychology and Counselling, University of Southern Queensland, and Charlotte Brownlow, Graduate Research School, University of Southern Queensland.
Send us your feedback: We would love to hear from you! Please send us your feedback .
Allied Health Professions Australia. (2021). Australian Psychological Society. https://ahpa.com.au/our-members/australian-psychological-society/
Australian Institute of Aboriginal and Torres Strait Islander Studies. (2012). Guidelines for ethical research in Australian indigenous studies. https://aiatsis.gov.au/research/ethical-research/code-ethics
Australian Psychological Society. (n.d.). Ethics and practice standards. https://psychology.org.au/about-us/what-we-do/ethics-and-practice-standards
National Commission for the Protection of Human Subjects of Biomedical and Behavioural Research. (2012). Belmont report: Ethical principles and guidelines for the protection of human subjects of research. https://videocast.nih.gov/pdf/ohrp_appendix_belmont_report_vol_2.pdf
Brown, D. L. (2017, May 16). You’ve got bad blood: The horror of the Tuskegee syphilis experiment. Washington Post. https://www.washingtonpost.com/news/retropolis/wp/2017/05/16/youve-got-bad-blood-the-horror-of-the-tuskegee-syphilis-experiment/
Centers for Disease Control and Prevention. (2021). The Tuskegee timeline. https://www.cdc.gov/tuskegee/timeline.htm
Dudgeon, P., Rickwood, D., Garvey, D., & Gridley, H. (2014). A history of indigenous psychology. https://www.telethonkids.org.au/globalassets/media/documents/aboriginal-health/working-together-second-edition/wt-part-1-chapt-3-final.pdf
National Health and Medical Research Council. (2018a). Aboriginal and Torres Strait Islander peoples and communities: Guidelines for researchers and stakeholders. https://www.nhmrc.gov.au/about-us/resources/ethical-conduct-research-aboriginal-and-torres-strait-islander-peoples-and-communities
National Health and Medical Research Council. (2018b). National statement on ethical conduct in human research (2007) – Updated 2018. https://www.nhmrc.gov.au/about-us/publications/national-statement-ethical-conduct-human-research-2007-updated-2018
National Health and Medication Research Council. (2018c). Australian code for the responsible conduct of research . https://www.nhmrc.gov.au/about-us/publications/australian-code-responsible-conduct-research-2018
National Health and Medical Research Council. (2018d). Keeping research on track II. https://www.nhmrc.gov.au/about-us/resources/keeping-research-track-ii
Office of the Australian Information Commissioner. (2017) Personal information. https://lawhandbook.sa.gov.au/ch34s02s03.php
Shaughnessy, J. J., Zechmeister, E. B., & Zechmeister, J. S. (2006) Research methods in psychology (7th ed.). McGraw-Hill.
Stark, C. (2019). The essence of ethics for psychologists and aspiring psychologists. In M. E. Norris (Ed.), The Canadian handbook for careers in psychological science . eCampusOntario. https://ecampusontario.pressbooks.pub/psychologycareers/chapter/the-essence-of-ethics-for-psychologists-and-aspiring-psychologists/
Tuskegee University. (2021). About the USPHS syphilis study. https://www.tuskegee.edu/about-us/centers-of-excellence/bioethics-center/about-the-usphs-syphilis-study
Please reference this chapter as:
Machin, T., & Brownlow, C. (2022). The essence of ethics for psychological researchers and psychologists. In T. Machin, T. Machin, C. Jeffries & N. Hoare (Eds.), The Australian handbook for careers in psychological science . University of Southern Queensland. https://usq.pressbooks.pub/psychologycareers/chapter/ethics/
The Australian Handbook for Careers in Psychological Science Copyright © 2022 by Tanya Machin and Charlotte Brownlow is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License , except where otherwise noted.
Share This Book

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Psychiatr Psychol Law
- v.27(3); 2020
Structuring the debate about research ethics in the psychology and law field: an international perspective
Alfred allan.
School of Arts and Humanities, Edith Cowan University, Joondalup, WA, Australia
Forensic psychologists’ role is well established, and they are rightly well regulated because their decisions and behaviour can have a significant impact on people’s rights and interests. Their ethical integrity, however, partly hinges on the psycholegal research products (data, methods and instruments) that they and others use. The ethical regulation of researchers who produce products and their research processes is, however, fragmented, limited and narrow and largely focuses on domestic research. Relatively few scholars have examined the regulation of psycholegal research or commented on the ethical implications of recent court decisions. The purpose of this paper is to start a debate about the ethical regulation of researchers in the psycholegal field and consider methods of improving it to maintain society’s trust in the field.
Psychologists’ role in providing services to law (defined here as the legal, corrective, investigative and justice systems) is well established, and they have a significant impact on the legal rights and interests of many people (see Grisso, 2018 ). The media, courts and professional and regulatory bodies therefore scrutinise forensic psychologists’ behaviour and decisions to determine whether they are ethical (right and good; Allan, 2018 ). Professional bodies (e.g. Australian Psychological Society, APS, 2011, 2013 ) and scholars (see, e.g. Allan, 2015a ; Allan & Grisso, 2014 ) provide ethical advice to forensic psychologists and researchers to explore issues such as the impact of bias, without necessarily identifying them as ethical issues (Kukucka, Kassin, Zapf, & Dror, 2017 ; Zapf & Dror, 2017 ).
Forensic psychologists and others involved in the administration of law (administrators; i.e. lawyers, police officers, policy makers, presiding officers, psychiatrists and social workers), however, rely on psychology and law (psycholegal) researchers’ products (i.e. data, methods and instruments). Researchers’ contributions could therefore have a significant influence on law (e.g. Steinberg, 2013 ), legal precedents (e.g. Miller v Alabama, 2012 ; Roper v Simmons, 2005 ; Zapf, Hubbard, Cooper, Wheeles, & Ronan, 2004 ) and policies (Grisso & Kavanaugh, 2016 ). Their contributions can also have a direct impact on society and individuals. Police using line-ups based on indefensible research might arrest the wrong people or allow offenders to escape (for a debate about this issue see Gronlund, Wixted, & Mickes, 2014 ; Wells, 2014 ). Sentencing courts could detain people who would have desisted if they rely on psychologists’ evidence that was based on risk assessment instruments that lack specificity, whilst courts using evidence obtained with instruments that are not sensitive enough might underestimate offenders’ risk of reoffending. People could suffer harm in both situations because offenders and their families suffer harm if sentences are unnecessarily long, and their victims and their families suffer harm if sentences are too lenient. Society also unnecessarily suffers financially either way, because it carries the cost of detaining and providing expensive treatment programmes to offenders, but also bears much of the financial burden of offending.
Despite the potential impact of their research, courts and scholars have given relatively little attention to the ethics of psycholegal researchers’ activities (Ward & Willis, 2010 ) compared to those of forensic psychologists. This lack of scrutiny is, however, not necessarily an indication that there are no problems, as I demonstrate in the next section. My belief is that psycholegal researchers should avoid even trivial unethical behaviours that could erode society’s and administrators’ trust in their research products and that it is time to start debating research ethics within the psycholegal field. My aim is to start this debate by using five ethical principles to analyse some of the ethical challenges I see and then making tentative proposals regarding how the profession could respond.
Nature of the problem
Psycholegal research has to the best my knowledge escaped major ethical embarrassments, and there has been little public discourse about allegations that have been made. Regehr, Edwardh and Bradford ( 2000 ), for instance, alleged that the researchers collecting the data used to develop the Statistical Risk Appraisal Guide (SRAG; G. T. Harris, Rice, & Quinsey, 1993 ) did not inform participants they were collecting data, or gave them a choice of participating. The importance of this from an ethical perspective is that this instrument forms the basis of the Sex Offender Risk Assessment Guide (SORAG; G. T. Harris, Rice, Quinsey, & Cormier, 2015 ) and the Violence Risk Appraisal Guide (VRAG; Rice & Harris, 1997 ). There has similarly been little debate about Australian (e.g. Director of Public Prosecutions [WA] v Mangolamara, 2007 ), Canadian (e.g. Canada v Ewert, 2016 ; Ewert v Canada, 2015 , 2018 ) and New Zealand (e.g. R v Peta, 2007 ) decisions that raise questions about the field’s ability to produce products that serve all people.
Some of these decisions, however, point to a further underlying ethical question – namely, how the field can prevent the deliberate or inadvertent misuse of its research products. Researchers understand that instruments such as the Static-99 (Hanson & Thornton, 1999 ) are not meant to identify a particular individual as a recidivist or a non-recidivist. The instrument is, however, used for this purpose in Australia, leading to an Australian judge finding that there is no evidence that the Static-99 has any efficacy whatsoever in relation to Australian Indigenous men (see Director of Public Prosecutions [WA] v Samson, 2014 ).
The problem facing the field is that that the public and law administrators’ trust in the field’s products might be eroded by judicial statements about the credibility of psychological research even though the researchers in question might not define themselves as psycholegal researchers. This happened in Brown v Entertainment Merchants Association (EMA, 2011 ) where the United States (US) Supreme Court considered psychological research regarding the impact of video violence ‘unpersuasive’ (p. 17). Justice Scalia was circumspect in explaining this decision but it further erodes the perceived trustworthiness of psychologists who, like other scientists, are steadily losing the trust of the public, particularly conservatives (Gauchat, 2012 ) who see them as social justice advocates who use their research to liberalise public policy (Cofnas, Carl, & Woodley of Menie, 2018 ). Even fair-minded observers could rightly question psychologists’ objectivity given the lack of socio-political diversity (e.g. Redding, 2001 ) within the profession and it allowing situations such as occurred in Brown v EMA (2011) where psychologists made statements that surpass their data or disregard objective disconfirming evidence (e.g. Ferguson, 2013 ). One possible explanation for this phenomenon is that the psychologists used moral disengagement (see Bandura et al., 1996 ) to justify using imperfect products to pursue a liberal moral agenda. Haslam ( 2016 , p. 1), for instance, explains how psychologists through ‘concept creep’ expanded their concepts of harm and vulnerability beyond that of the general public to protect those they define as defenceless. Some psychologists might therefore in the pursuit of goals that they and/or many in society highly value disregard their ethical obligations to be honest, fair and trustworthy. Such a ‘dual commitment to science and advocacy’ (Grisso, 2018 , p. 21) is apparent amongst psycholegal researchers, and this is an issue that the field should consider.
Psycholegal scholars also neglect to write about psycholegal research ethics or the ethics of publishing psycholegal research findings. My search in Law and Human Behavior, Behavioral Science and the Law and Ethics and Behavior using ‘research ethi’ and ‘publi ethi’ as search terms identified no relevant publication. Law and Human Behavior’s revised classification codes similarly do not provide a logical heading for papers on research ethics or directly refer to research ethics (see McAuliff et al., 2019 ). Scholars in particular do not write about the research ethics from an international perspective even though psycholegal research has become a global enterprise. Researchers increasingly work in international teams and/or undertake research outside their own countries, and psychologists and administrators from all over the world use psycholegal researchers’ products. The ethical regulation of research is furthermore still primarily country-centric and fragmented with several bodies directly or indirectly regulating researchers.
Regulatory bodies (e.g. professional licensing or registration boards), for instance, regulate all registered psychologists doing research in their jurisdiction whilst professional bodies (e.g. American Psychological Association, APA) only regulate researchers who are their members. Some people involved in psycholegal research might do so without oversight from any regulatory body. The bodies’ ethical codes and guidelines primarily focus on psychologists ‘conducting research’ (American Psychology and Law Society, APLS, 2011 , p. 1) and ignore psychologists’ other research related roles. These roles include determining psycholegal research agendas and priorities and allocating research funds, and serving as members of institution review boards (IRBs, also known as ethics committees, Schneider, 2006 ), research assistants, reviewers of manuscripts and editors.
IRBs provide the next level of regulation and have become important ethical gatekeepers of psycholegal research in most countries because they approve researchers’ proposals and oversee the execution of their research projects. Schüklenk’s ( 2000 ) conclusions after examining historical cases of breaches of research ethics in medicine were that IRBs are only moderately effective in determining the ethical justification of proposed research projects and ineffective in monitoring the execution and outcomes of research projects. Part of the problem is that IRBs mainly respond to complaints they receive and that their members are often lay people and/or researchers from disciplines who do not necessarily fully understand the subtleties of specific research projects (Schüklenk, 2000 ; Straight, 2009 ).
The peer review process has therefore become the ultimate gatekeeper to ensure that researchers act ethically (Allan, 2015a ). Authors have, however, expressed concern about the effectiveness of the review process in general (e.g. Bohannon, 2013 ; Smith, 2006 ) and the ethical review of researchers’ behaviour in particular (e.g. Kapoor, Young, Coleman, Norko, & Griffith, 2011 ; Koocher & Keith-Spiegel, 2016 ; Levelt, 2012 ). They even question whether some behaviour of editors is ethical (e.g. Lilienfeld, 2002 ; Stone & MacCourt, 2008 ). Editors’ and reviewers’ role as ethical scrutineers of research is further becoming more difficult as the volume of projects grows and researchers increasingly use more sophisticated methods and statistical approaches and tools for analysing data (Kazak, 2018 ; Wright, 2016 ). Editors must therefore increasingly rely on the ethical integrity of researchers whom they know are under pressure to publish and therefore might be careless or dishonest when they submit manuscripts (Schminke, 2009 ; Wright, 2016 ).
Some editors and publishers have formed the Committee on Publication Ethics (COPE) to increase the ethical scrutiny of editors’ and reviewers’ decisions and behaviour (Godlee, 2004 ). COPE published a code of conduct ( 2011 ) and core practices ( n.d. ) to guide editors regarding their specific ethical obligations, but compliance is voluntary, and some recommendations might be difficult to enforce. Angelski, Fernande, Weijer, and Gao ( 2012 ), for instance, found that only 38% ( n = 13) of the editors who participated in their survey (of all 103 English language journals in the Abridged Index Medicus) indicated that they specifically instruct reviewers to reject manuscripts based on ethical grounds alone. The authors do not indicate why editors do not give such instructions but some might believe that there is sufficient ethical scrutiny if IRBs approved the research, feel that they do not have a mandate or resources to make such requests (e.g. Godlee, 2004 ) or doubt that reviewers have the ethical sensitivity, knowledge and skills to undertake a proper ethical analysis of the manuscripts they review (e.g. Pierson, 2015 ). The scope of the COPE guidelines is also narrow, and the editors of the new journals with uncertain reputation that are constantly appearing might not follow them (Roberts, 2016 ).
Contemporary researchers can, however, disseminate their findings online (e.g. blogs) or in grey literature published outside the traditional academic or commercial publication and distribution channels without any review or scam reviews (see Bohannon, 2013 ). Published material falling in these two categories might increase as digital publication has become a lucrative business with authors paying $250 million in 2014 to publish above two million articles in more than 20,000 digital journals (see Bohannon, 2015 ). Researchers might also increase their use of the outlets, as major funding bodies in several regions (Federal Food Drug and Cosmetic Act, 1938 ; Schiltz, 2018 ) require researchers to provide open access to their research findings.
Ethical framework
The profession has traditionally used the principles in codes of ethics (e.g. American Psychological Association, 2002 ; Australian Psychological Society, 2007 ; Canadian Psychological Association, 2017 ) to state its moral ideals. These principles are universally accepted (see Gauthier, Pettifor, & Ferrero, 2010 ; International Association of Applied Psychology [IAAP] and the International Union of Psychological Science [IUPsyS], 2008 ), but the drafters of codes differ regarding how they combine the principles and what they call them (Allan, 2011 ). Given the international approach I am taking, I will use the framework of ethical principles that Allan ( 2018 ) used to examine the ethical challenges that forensic psychologists face internationally – namely, Respect for the dignity of humanity (Respect), Justice, Fidelity or Trust, Care and Responsibility principles.
The Respect principle underlies both human rights law and ethics (Allan, 2013 ) and is of importance to all researchers as it requires them to recognise potential participants’ self-worth, moral and legal rights and interests, autonomy and privacy (including their right to be left alone, Allan, 2015a ). The principle further requires psychologists to be truthful (i.e. honest, open and able to account for their decisions and actions and admit the limitations of their research products and their application).
The Justice principle is of particular importance to the psycholegal field because distributive justice requires psychologists to ensure that the benefits, costs and risks of their research are fairly distributed amongst all people. Distributive justice partly underlies the European Plan S that was launched in 2018 (Schiltz, 2018 ). Procedural justice requires researchers to contribute to fair decision making regarding other people’s rights and interests (Allan, 2015b ).
The Trust principle recognises that psychologists must be trustworthy in order to realise their social purpose (e.g. MacDonald, 1995 ; Parsons, 1968 ). Society, including administrators, cannot determine individual researchers’ competence (i.e. their ability, knowledge and skill) and whether they are acting in society’s best interests, or the reliability of their research products. Society could start mistrusting researchers if courts regularly reject testimony based on psycholegal research products even though the researchers’ own behaviour was ethical.
Psychologists are familiar with the Care principle, which requires them to take reasonable steps to avoid reasonably foreseeable harm and to minimise unavoidable or unintended harm to participants. Researchers’ responsibility, however, extends beyond foreseeable direct and physical harm to participants to include potential indirect and non-physical harm that could occur when others use their research products.
Researchers might be unfamiliar with the Responsibility principle, which reflects psychologists’ collective and individual ethical responsibilities to several entities and people depending on their roles. Society considers psycholegal research important, and governments and public enterprise therefore support researchers by giving them opportunities and funds to do research. Society in return expects psychologists to use their knowledge, skill and experience to the benefit of society as a whole (e.g. MacDonald, 1995 ; Parsons, 1968 ). They must therefore undertake only socially beneficial research and disseminate comprehensible accounts of their research findings as broadly as possible (e.g. Federal Food, Drug and Cosmetic Act, 1938 ; Fuller, Pearson, & Peters, 2016 ). Psycholegal researchers who acquire their professional identity and credibility from their role as psychologists should furthermore refrain from doing anything that could impair the standing of the field and their peers and therefore take steps to protect the reputation of the field when they see peers misbehaving (e.g. Koocher, 2012 ; Koocher & Keith-Spiegel, 2010 ).
These principles apply to all psychologists whether they act collectively or individually as researchers, delegates (e.g. graduate students and research assistants), reviewers or editors. I first consider some of the challenges I believe the psycholegal field as a collective faces and then briefly examine the challenges to individual psychologists in different roles.
Society expects psychology to develop products that benefit it in a manner that all their members equally share the benefits, costs and risks. This includes indigenous, migrant or other minority groups within jurisdictions (e.g. Allan, Dawson, & Allan, 2006 ). Individual researchers cannot meet the needs of all people in the world, but the field’s global 1 reach further implies that researchers should consider the distributive justice implications of their research endeavours in at least those jurisdictions where there are researchers that contribute to the development of their products or practitioners use them. The Ewert case (e.g. Canada v Ewert, 2016 ; Ewert v Canada, 2015 , 2018 ) is, however, a reminder of how far the field still is from achieving these goals even for all groups within the country for which these instruments were developed. The applicant in this case was a Métis (Canadian Aboriginal) man whose legal team argued that a range of well-known psychological tests such as the Psychopathy Checklist–Revised (PCL–R; Hare, 1991 ); VRAG (Quinsey, Harris, Rice, & Cormier, 1998 ); SORAG (Quinsey, Harris, Rice, & Comier, 2006 ); Static-99 (Hanson & Thornton, 1999 ; A. J. R. Harris, Phenix, Hanson, & Thornton, 2003 ; Helmus, Hanson, & Thornton, 2009 ) and the Violence Risk Scale–Sex Offender (VRS–SO; Wong, Olver, Nicholaichuk, & Gordon, 2003 , 2006 ) ‘generate false results and false conclusions when used on Aboriginal persons’ (Canada v Ewert, 2016 , ¶20). The essence of the Supreme Court’s decision is that these instruments, some that were developed in Canada, discriminate against Aboriginal offenders (Ewert v Canada, 2018 ). This discrimination, however, extends beyond offenders because this lack of appropriate instruments places the public, but especially Aboriginal people, at risk because they are more likely to be the victims of Aboriginal offenders (Allan et al., 2018 ). Many practitioners continue to use instruments inappropriately because they are unaware of the ethical implications and/or because they have no appropriate alternatives to use.
Individual researchers have a role to play in minimising the inappropriate use of their research products, as I discuss later, but can do little to influence the behaviour of practitioners. They will in particular find it difficult to independently overcome obstacles that individually or in combination with others make it difficult to satisfy society’s ultimate requirement that the field should meet the realistic needs of all members in an equitable manner. Researchers might, for instance, find it difficult or unattractive to undertake research in certain areas for a variety of reasons, including ideological opinions within society and psychology (e.g. female perpetrated domestic violence, Lee & Lincoln, 2017 ). They might equally anticipate difficulties in ensuring the privacy of research participants when they study small populations (e.g. mass killers) because they could find it difficult to hide participants’ identifying information when they report their findings, especially if they do research in a small jurisdiction.
The field as a collective will have to address these issues and other similar problems that might need a strategic and collaborative approach. The field might, for instance, have to coordinate the development of research methods that will allow researchers to develop risk prediction instruments that satisfy legal and ethical standards for small populations (e.g. indigenous people or migrants) where the base rate of the offending behaviour is low (e.g. sexual and violent offending). A collective attempt might also be necessary to make use of opportunities to obtain research funds for some types of research. Cases such as the Ewert case (Ewert v Canada, 2018 ) might encourage governments to fund the research necessary for them to meet their human rights obligations, and this provides opportunities for the field to fulfil some of its own ethical responsibilities.
The field as a collective is also in a better position to consider emerging ethical issues across the world, encourage research that can inform researchers’ practice and help psychologists understand their ethical responsibilities, including those relevant beyond the jurisdiction that they work in. It could, for instance, promote a more pluralistic discourse by creating opportunities for respectful and informed debate between psycholegal researchers who have diverse values and beliefs. The field could also encourage researchers to undertake research to identify the role of bias in their research in the same way as they are studying the role of partiality in forensic psychologists’ assessment (e.g. Neal & Brodsky, 2016 ; Neal & Grisso, 2014 ; Zapf & Dror, 2017 ). It could aid psychologists by developing ethical guidelines and educating them about their roles as ethical agents, especially within a global context. The field is finally in a stronger position to encourage publishers to endorse these guidelines and monitor that researchers, editors and reviewers implement them.
Researchers
Rosenthal ( 1994 ) pointed out that researchers’ ethical obligations span a wide range of decisions and behaviours that start with their choice of research topics, designs and questions, how they frame these questions and who they invite as participants. Their ethical obligations continue when they execute projects, delegate tasks, choose analytical methods and interpret, report and explain their research findings. Most researchers are intent on behaving ethically, but they are also enthusiastic about their research ideas, getting approval from, and sometimes entering into agreements with, host organisations that can give them access to participants or data. They could therefore commit themselves to projects without fully understanding the challenges and resources they require or fail to identify or ignore or minimise potential ethical problems with their research projects. They might specifically not understand the challenges of projects they undertake in jurisdictions where they are unfamiliar with the law and morals (Benatar & Singer, 2000 ). Researchers might also not understand how their everyday activities and attempts to boost their self-esteem could bias them. Their competition with peers to attract research grants and enhance their careers; commercial interests; and the promotion of ideological or theoretical views might, for instance, bias them (e.g. FeldmanHall et al., 2012 ; Greenwald & Banaji, 1995 ; Greenwald, Pickrell, & Farnham, 2002 ). Those who appreciate the risk of being biased might underestimate how difficult it is even for critical thinkers (Babcock & Loewenstein, 1997 ; Babcock, Loewenstein, & Issacharoff, 1997 ) who are trying their best to do the right thing (for a discussion, see Epley & Caruso, 2004 ) to overcome bias.
Researchers should therefore consider strategies that will simultaneously ensure that their projects are feasible, ethical and unbiased and avoid creating unrealistic expectations from those who support their research. They could do this by planning their projects in detail at the onset and inviting peers whom they trust to be objective or who hold opposing ideological views to critique the research methodology (Grisso & Steinberg, 2005 ). They can further enhance their perceived objectivity by pre-registering their hypotheses, methods and analyses before undertaking their projects (e.g. Van ’t Veer & Giner-Sorolla, 2016 ) and maintaining audit trials of their activities that will allow them to give an account of their research.
Researchers should also consider the broader implications of their studies, such as whether their research is a justifiable use of limited research funds or merely very narrow studies that serve little purpose other than further their careers (Lilienfeld, 2012 ; Nosek & Bar-Anan, 2012 ). Every project cannot benefit every group in society, but researchers should explicitly consider the distributive justice implications of their research. They should ideally undertake projects that will bring benefits to those groups that are currently not well served and strive to distribute the costs of their research fairly by not placing an unnecessary burden on victims (e.g. of human rights abuses, Allan, 2000 ) and offenders (e.g. in drug courts, DeMatteo, Filone, & LaDuke, 2011 ). Researchers could argue that research with victims and offenders is justified because it benefits society as a whole, but this argument is unconvincing when researchers place additional burdens on participants by using their time and adding to the stress they experience (DeMatteo et al., 2011 ).
Professional ethics obliges researchers to go beyond merely complying with the requirements of IRBs when they consider the possible ethical challenges they might encounter. Many researchers find it challenging to avoid placing undue pressure on people to give consent (e.g. Van Loon & Lindegger, 2009 ) or provide inaccurate information (e.g. Bowling & Huang, 2018 ). Psycholegal researchers’ potential participants, however, often have several characteristics that might subtly influence their ability to give free consent and accurate responses. Cultural and literacy issues (e.g. Strickland, Parry, Allan, & Allan, 2017 ) can, for instance, influence detainees’ ability to understand information and make detached decisions. Modest financial incentives and/or contact with friendly attractive research assistants could influence detainees and other participants who are materially, emotionally and socially deprived (e.g. Rosenfeld & Green, 2009 ). Detainees with mental disorders (e.g. Regehr et al., 2000 ) or people under investigation or involved in legal proceedings (e.g. in family or drug courts, DeMatteo et al., 2011 ) typically experience emotional and other stress, and they could agree to participate in research because it is easier to acquiesce or because they fear they might suffer prejudice if they refuse to participate.
Researchers should also consider how they can limit the potential misuse of their research products in a manner that could potentially cause harm. Allan and Dawson ( 2002 ), for instance, had to cease developing a model for predicting Australian Indigenous men’s risk of violence when they found that whilst ‘the recidivism predictive accuracy (95.4%) of the model for the violent offenders was good … the desisting predictive accuracy (55%) was poor’ (p. 10) and that the model was therefore ‘geared toward identifying re-offenders at the expense of non-reoffenders [that] … would only heighten the over representation of Indigenous people within the prison system’ (p. 84).
Delegates and collaborators
Graduate students, research assistants and other research collaborators who are psychologists have a personal and professional responsibility to use their intimate knowledge of projects to identify fabrications and falsifications that might otherwise go undetected (see Koocher, 2012 ). The field might, however, have to find ways to encourage and support whistle-blowers because they report that such disclosure may have a negative effect on their personal lives and their careers (Koocher, 2012 ).
Peer reviewers
The Justice principle obliges those who benefit from the efforts of those who serve as committee members, editors, editorial board members and reviewers to share the burden of reviewing proposals, grant applications and manuscripts (Pierson, 2016 ). The challenge is, however, to find reviewers that understand their own ethical obligations (Gallagher, 2013 ) and are competent to investigate the scientific and ethical appropriateness of researchers’ procedures, including the global ethical implications of their projects and manuscripts. Reviewers might, furthermore, know that they must be procedurally fair and therefore unbiased but, as I pointed out earlier, they might be unable to identify their biases and therefore might not disclose conflicts of interest. Editors and publishers can to a degree regulate reviewers’ behaviour but will find it difficult to, for example, ensure that they respect researchers’ intellectual property rights and refrain from disclosing or using information they obtained during the review process.
The best strategy for the field is arguably to improve reviewers’ ethical knowledge and develop novice reviewers’ skills by identifying and encouraging competent reviewers to present workshops at conferences that specifically focus on reviewers’ ethical obligations. It could also encourage editors to identify and help early career researchers develop their reviewing skills. Editors could do this by giving constructive feedback to inexperienced reviewers, providing them the opportunity to work with experienced reviewers and finding ways of rewarding their contributions.
Editors have all reviewers’ ethical responsibilities plus those that come from their responsibility to monitor the ethical appropriateness of what reviewers do and make the final decisions about the acceptance and publication of manuscripts. Editors should therefore encourage reviewers to be honest and critical in their reports but ensure that the tone and content of their reports are respectful and devoid of intemperate criticism or language that demeans researchers.
Editors should in particular ensure that reviewers are unbiased, and some editors try to do this by allowing authors to disqualify people who they would prefer not to be reviewers. Authors might, however, not be able to identify all the potential conflicted reviewers. An approach that could improve the transparency of reviews would be to remove reviewers’ anonymity. Some reviewers might, however, not give critical reviews because they fear reprisals whilst others might refuse to undertake reviews if they are identified. An alternative approach could be that editors propose a panel of appropriate reviewers and invite authors to make a shortlist that they then use to appoint reviewers.
Editors should monitor reviewers’ reports for any signs of bias such as when they extensively cite themselves and/or their close associates, or instruct authors to read such papers. Reviewers who do this might nevertheless be raising valid points. Editors who accept such manuscripts for publication could consider inviting reviewers to submit their commentaries as short articles that accompany the original manuscripts with the authors’ replies to those commentaries. Open and frank debates of this nature are informative and could combat concerns that the peer review system lacks transparency.
Editors who try to, or expect reviewers to, undertake substantial ethical reviews might find that there is seldom enough information in manuscripts to do that because authors merely report that they had IRB consent to undertake the project. Authors, for instance, routinely report little or no information that allows editors and reviewers to confirm that the participants were fully informed and competent. Editors and reviewers could in many instances be comfortable with blunt statements of compliance, but where the participants might have been vulnerable they have a responsibility to obtain evidence that the participants made voluntary, free and fully informed decisions. Authors will probably resent providing additional information, and there is also a risk of extensive communications between them and editors that could delay publication of papers. Publishers could, however, consider requiring researchers to make their working documents and raw data available in secure online sites where editors and reviewers can access them when required.
An outcome of the wide use of the fields’ research products is that some users might lack a sound understanding of the limitations of these products and therefore use them in an unethical way. Many Australian assessors (see Director of Public Prosecutions [WA] v Mangolamara, 2007 ) and Departments of Corrective Services employees use the Static-99 to identify offenders as recidivists or non-recidivists (Allan, 2015a , 2018 ; Allan et al., 2018 ). This practice is unethical because the Static-99 was not designed for this purpose and has not been validated in Australia, and specifically not for Australian Indigenous men, who are over-represented in the prison system (Allan, 2015a ). Smallbone and Rallings ( 2013 ) therefore considered it necessary to include data about the low true-positive and high false-positive rates of their Static-99 data for Indigenous sexual offenders in the original manuscript they submitted (S. Smallbone, personal communication, September 23, 2013). The editor and reviewers, however, asked them to remove the relevant table and discussion because they considered it inappropriate to report such data for the Static-99. The implication of this deletion is that users of the Static-99, experts instructed by the defendants and lawyers, and therefore courts, are deprived of important data. This appears to be a case where those involved focus on reporting to other scientists and sophisticated users of research (see Fuller et al., 2016 ) without considering the ethical implications of removing the relevant data.
This case demonstrates the need for editors to be sensitive to ethical issues that go beyond merely the normal publication ethics and to take into account the unique circumstances at the location where the data were collected (Salaam & Brown, 2013 ) or might be used. Publishers could consider identifying ethicists whom editors and reviewers can consult if they are uncertain about the ethical appropriateness of manuscripts or the research they are based on.
Editors should specifically consider the ethical aspect of manuscripts and instruct reviewers to do the same. Editors should reject manuscripts when appropriate or require authors to make changes that address their ethical concerns. Editors could also consider adding an editorial caveat regarding the ethical concerns (see Angelski et al., 2012 ) and how they were addressed or inviting the specialist reviewers to write a commentary on the published paper. Such editorial comments and commentaries will serve the additional purpose of providing ethical education to others partaking in the research process and readers and users of the articles.
Psycholegal research is a success story. The field can point to several areas where its research products enhance the administration of justice and protection of the public (e.g. identification of reoffenders). It can also point to the very high number of non-researchers that use its research products, extending from psychologists to other administrators of law. It can even point to the financial rewards it brings to some researchers, which in turn motivates them and others to do psycholegal research. The field has achieved this with minimal external regulation because society and administrators trust researchers and their products.
Society is, however, becoming more critical of researchers, and the field cannot shrug all such criticism off as mere ideological scepticism, because an analysis of the case law points to issues regarding researchers’ objectivity and the distribution of the benefit, harm and risk of their research. Many researchers might not consider the issues raised in these cases as ethical issues, but they are, and if the field fails to address them it could lead to an erosion of society and administrators’ trust in the field. This scrutiny of psycholegal research is likely to increase as the human rights culture develops in more countries, because courts applying human rights law often make findings that indirectly reflect on the field’s research ethics as psychology’s ethics and human rights law share the same foundation (Allan, 2013 ). The field therefore faces the prospect that society directly or through courts could prescribe to it how it should regulate research. Researchers as individuals and a collective can prevent this by aspiring to realise the profession’s ethical principles, even though they most likely will never be able to do so fully because these moral ideas are at the outer limit of what can pragmatically be reached (see Brownlee, 2010 ).
The lack of international professional and/or regulatory bodies with formal legal structures makes it difficult for the field to respond at a global level, but the field could partly overcome this limitation if national bodies that represent psychologists such as the APLS, the APS’s College of Forensic Psychologists and the British Psychological Society’s Division of Forensic Psychology affiliate with a body that has an international structure (e.g. the IAAP), which can then coordinate the field globally. Law’s jurisdictional nature (e.g. Allan, 2011 ) will prevent such a coordinating body from adopting and enforcing a common code, but it could orchestrate the non-regulatory activities of the various national bodies. Editors could encourage authors to submit papers on the ethics of psycholegal research and explicitly instruct reviewers to consider the ethics of the projects that manuscripts are based on. I concede that the article is limited because I mostly draw from areas that I am familiar with, such as the development of instruments to predict the risk of reoffending, and that my ideas are aspirational and many will argue impractical, but the field needs to debate these issues if it wants to maintain the trust of society, and the sooner it starts the better.
Ethical standards
Declaration of conflicts of interest.
Alfred Allan has declared no conflicts of interest
Ethical approval
This article does not contain any studies with human participants or animals performed by the author.
1 The extra-territorial legal responsibilities of psychologists are beyond the ambit of this paper, but psychologists who adhere to the aspirational ethical principles will generally be acting within the ambit of morally acceptable law in most, if not all, jurisdictions as law generally prescribes less aspirational minimum behavioural standards.
- Allan, A. (2000). Truth and reconciliation: A psycholegal perspective . Ethnicity & Health , 5 ( 3–4 ), 191–204. doi: 10.1080/713667457 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Allan, A. (2011). The development of a code for Australian psychologists . Ethics & Behavior , 21 ( 6 ), 435–451. doi: 10.1080/10508422.2011.622176 [ CrossRef ] [ Google Scholar ]
- Allan, A. (2013). Are human rights redundant in the ethical codes of psychologists? Ethics & Behavior , 23 ( 4 ), 251–265. doi: 10.1080/10508422.2013.776480 [ CrossRef ] [ Google Scholar ]
- Allan, A. (2015a). Ethics in psychology and law: An international perspective . Ethics & Behavior , 25 ( 6 ), 443–457. doi: 10.1080/10508422.2014.952006 [ CrossRef ] [ Google Scholar ]
- Allan, A. (2015b). Psychologists and the courts: Ethical issues. In Morrissey S., Reddy P., Davidson G. R. & Allan A. (Eds.), Ethics and professional practice (2nd ed., pp. 103–110). Melbourne, Australia: Cengage. [ Google Scholar ]
- Allan, A. (2018). Moral challenges for psychologists working in psychology and law . Psychiatry, Psychology and Law , 25 ( 3 ), 485–499. doi: 10.1080/13218719.2018.1473173 [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Allan, A., & Dawson, D. (2002). Developing a unique risk of violence tool for Australian Indigenous offenders (Criminology Research Council report: CRC6/00-01). Canberra, Australia: Criminology Research Council. Retrieved from http://crg.aic.gov.au/reports/200001-06.html .
- Allan, A., & Grisso, T. (2014). Ethical principles and the communication of forensic mental health assessments . Ethics & Behavior , 24 ( 6 ), 467–477. doi: 10.1080/10508422.2014.880346 [ CrossRef ] [ Google Scholar ]
- Allan, A., Dawson, D., & Allan, M.M. (2006). Prediction of the risk of male sexual reoffending in Australia . Australian Psychologist , 41 ( 1 ), 60–68. doi: 10.1080/00050060500391886 [ CrossRef ] [ Google Scholar ]
- Allan, A., Parry, C.L., Ferrante, A., Gillies, C., Griffiths, C.S., Morgan, F., … Wong, S.C.P. (2018). Assessing the risk of Australian Indigenous sexual offenders reoffending: A review the research literature and court decisions . Psychiatry, Psychology and Law , 26 ( 2 ), 274–294. doi: 10.1080/13218719.2018.1504242 [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- American Psychological Association. (2002). Ethical principles of psychologists and code of conduct. Retrieved from http://www.apa.org/ethics/code/
- American Psychology and Law Society [APLS]. (2011). Specialty guidelines for forensic psychology. Retrieved from http://www.ap-ls.org/links/professionalsgfp.html
- Angelski, C., Fernande, C.V., Weijer, C., & Gao, J. (2012). The publication of ethically uncertain research: Attitudes and practices of journal editors . BMC Medical Ethics , 13 ( 1 ), 1–6. doi: 10.1186/1472-6939-13-4 [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Australian Psychological Society. (2007). Code of ethics. Retrieved from http://www.psychsociety.org.au/
- Australian Psychological Society. (2013). Guidelines for psychological practice in forensic contexts. Retrieved from https://www.psychology.org.au/Assets/Files/EG-Forensic.pdf
- Babcock, L., & Loewenstein, G. (1997). Explaining bargaining impasse: The role of self-serving biases . The Journal of Economic Perspectives , 11 ( 1 ), 109–126. doi: 10.1257/jep.11.1.109 [ CrossRef ] [ Google Scholar ]
- Babcock, L., Loewenstein, G., & Issacharoff, S. (1997). Creating convergence: Debiasing biased litigants . Law & Social Inquiry , 22 ( 4 ), 913–925. doi: 10.1111/j.1747-4469.1997.tb01092.x [ CrossRef ] [ Google Scholar ]
- Bandura, A., Barbaranelli, C., Caprara, G.V., & Pastorelli, C. (1996). Mechanisms of moral disengagement in the exercise of moral agency . Journal of Personality and Social Psychology , 71 ( 2 ), 364–374. doi: 10.1037/0022-3514.71.2.364 [ CrossRef ] [ Google Scholar ]
- Benatar, S.R., & Singer, P.A. (2000). A new look at international research ethics . BMJ , 321 ( 7264 ), 824–826. doi: 10.1136/bmj.321.7264.824 [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Bohannon, J. (2013). Who’s afraid of peer review? Science , 342 ( 6154 ), 60–65. doi: 10.1126/science.342.6154.60 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Bohannon, J. (2015). How to hijack a journal. Science . Retrieved from https://www.sciencemag.org/news/2015/11/feature-how-hijack-journal [ PubMed ]
- Bowling, N.A., & Huang, J.L. (2018). Your attention please! Towards a better understanding of research participant carelessness . Applied Psychology , 67 ( 2 ), 227–230. doi: 10.1111/apps.12143 [ CrossRef ] [ Google Scholar ]
- Brown v Entertainment Merchants Association [EMA]. (2011). 564 U.S. 08-1448. Retrieved from http://www.supremecourt.gov/opinions/10pdf/08–1448.pdf .
- Brownlee, K. (2010). Moral aspirations and ideals . Utilitas , 22 ( 3 ), 241–257. doi: 10.1093/ojls/gqq006 [ CrossRef ] [ Google Scholar ]
- Canada v Ewert. (2016). FCA 203. Retrieved from http://www.canlii.org/en/ca/fca/doc/2016/2016fca2203/2016fca2203.html .
- Canadian Psychological Association. (2017). Canadian code of ethics for psychologists (4th ed.). Toronto, Canada: Author. Retrieved from https://cpa.ca/docs/File/Ethics/CPA_Code_2017_4thEd.pdf . [ Google Scholar ]
- Cofnas, N., Carl, N., & Woodley Of Menie, M.A. (2018). Does activism in social science explain conservatives’ distrust in scientists ? The American Sociologist , 49 ( 1 ), 135–148. doi: 10.1007/s12108-017-9362-0 [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Committee on Publication Ethics (COPE) (2011). Code of conduct and best practice guidelines for journal editors. Retrieved from https://publicationethics.org/files/Code%20of%20Conduct_2.pdf
- Committee on Publication Ethics (COPE) (n.d.). Core practices. Retrieved from https://publicationethics.org/
- DeMatteo, D., Filone, S., & LaDuke, C. (2011). Methodological, ethical, and legal considerations in drug court research . Behavioral Sciences & the Law , 29 ( 6 ), 806–820. doi: 10.1002/bsl.1011 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Director of Public Prosecutions [WA] v Mangolamara. (2007). WASC 71. Retrieved from http://www.austlii.edu.au/cgi-bin/viewdoc/au/cases/wa/WASC/2007/71.html?context=1;query=mangolamara;mask_path=au/cases/wa/WASC
- Director of Public Prosecutions [WA] v Samson. (2014). WASC 199. Retrieved from http://www.austlii.edu.au/cgi-bin/viewdoc/au/cases/wa/WASC/2014/199.html
- Epley, N., & Caruso, E.M. (2004). Egocentric ethics . Social Justice Research , 17 ( 2 ), 171–187. doi: 10.1023/B:SORE.0000027408.72713.45 [ CrossRef ] [ Google Scholar ]
- Ewert v Canada. (2015). FC 1093. Retrieved from http://www.canlii.org/en/ca/fct/doc/2015/2015fc1093/2015fc1093.html
- Ewert v Canada. (2018). SCC 30. Retrieved from https://scc-csc.lexum.com/scc-csc/scc-csc/en/17133/1/document.do
- Federal Food Drug and Cosmetic Act. (1938). (United States). Retrieved from https://www.fda.gov/RegulatoryInformation/LawsEnforcedbyFDA/FederalFoodDrugandCosmeticActFDCAct/default.htm .
- FeldmanHall, O., Mobbs, D., Evans, D., Hiscox, L., Navrady, L., & Dalgleish, T. (2012). What we say and what we do: The relationship between real and hypothetical moral choices . Cognition , 123 ( 3 ), 434–441. doi: 10.1016/j.cognition.2012.02.001 [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Ferguson, C.J. (2013). Violent video games and the Supreme Court: Lessons for the scientific community in the wake of Brown v Entertainment Merchants Association . American Psychologist , 68 ( 2 ), 57–74. doi: 10.1037/a0030597 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Fuller, T.E., Pearson, M., & Peters, J. (2016). Improving the reporting of health and psychological research . Australian Psychologist , 51 ( 3 ), 182–187. doi: 10.1111/ap.12135 [ CrossRef ] [ Google Scholar ]
- Gallagher, A. (2013). The ethics of reviewing . Nursing Ethics , 20 ( 7 ), 735–736. doi: 10.1177/0969733013506646 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Gauchat, G. (2012). Politicization of science in the public sphere: A study of public trust in the Unites States, 1974 to 2010 . American Sociological Review , 77 ( 2 ), 167–187. doi: 10.1177/0003122412438225 [ CrossRef ] [ Google Scholar ]
- Gauthier, J., Pettifor, J., & Ferrero, A. (2010). The universal declaration of ethical principles for psychologists: A culture-sensitive model for creating and reviewing a code of ethics . Ethics & Behavior , 20 ( 3–4 ), 179–196. doi: 10.1080/10508421003798885 [ CrossRef ] [ Google Scholar ]
- Godlee, F. (2004). Dealing with editorial misconduct: New code of conduct for editors is a first step in self regulation . BMJ , 329 ( 7478 ), 1301–1302. doi: 10.1136/bmj.329.7478.1301 [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Greenwald, A.G., & Banaji, M.R. (1995). Implicit social cognition: Attitudes, self-esteem, and stereotypes . Psychological Review , 102 ( 1 ), 4–27. doi: 10.1037/0033-295X.102.1.4 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Greenwald, A.G., Pickrell, J.E., & Farnham, S.D. (2002). Implicit partisanship: Taking sides for no reason . Journal of Personality and Social Psychology , 83 ( 2 ), 367–379. doi: 10.1037//0022-3514.83.2.367 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Grisso, T. (2018). The evolution of psychology and law. In Grisso T. & Brodsky S.L. (Eds.), The roots of modern psychology and law (pp. 1–28). New York, NY: Oxford. [ Google Scholar ]
- Grisso, T., & Kavanaugh, A. (2016). Prospects for developmental evidence in juvenile sentencing based on Miller v Alabama . Psychology, Public Policy, and Law , 22 ( 3 ), 235–249. doi: 10.1037/law0000090 [ CrossRef ] [ Google Scholar ]
- Grisso, T., & Steinberg, L. (2005). Between a rock and a soft place: Developmental research and the child advocacy process . Journal of Clinical Child & Adolescent Psychology , 34 ( 4 ), 619–627. doi: 10.1207/s15374424jccp3404_4 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Gronlund, S.D., Wixted, J.T., & Mickes, L. (2014). Evaluating eyewitness identification procedures using ROC analyses . Current Directions in Psychological Science , 23 ( 1 ), 3–10. doi: 10.1177/0963721413498891 [ CrossRef ] [ Google Scholar ]
- Hanson, R.K., & Thornton, D. (1999). Static 99: Improving risk assessments for sex offenders. Retrieved from http://www.sgc.gc.ca [ PubMed ]
- Hare, R.D. (1991). The hare psychopathy checklist- revised manual . Toronto, Canada: Multi-Health Systems, Inc. [ Google Scholar ]
- Harris, A.J.R., Phenix, A., Hanson, R.K., & Thornton, D. (2003). Static-99 Coding rules tevised . Ottawa, Canada: Solicitor General, Canada. [ Google Scholar ]
- Harris, G.T., Rice, M.E., & Quinsey, V.L. (1993). Violent recidivism of mentally disordered offenders: The development of a statistical prediction instrument . Criminal Justice and Behavior , 20 ( 4 ), 315–335. doi: 10.1177/0093854893020004001 [ CrossRef ] [ Google Scholar ]
- Harris, G.T., Rice, M.E., Quinsey, V.L., & Cormier, C. (2015). Violent offenders: Appraising and managing risk (3rd ed.). Washington, DC: American Psychological Association. [ Google Scholar ]
- Haslam, N. (2016). Concept creep: Psychology’s expanding concepts of harm and pathology . Psychological Inquiry , 27 ( 1 ), 1–17. doi: 10.1080/1047840X.2016.1082418 [ CrossRef ] [ Google Scholar ]
- Helmus, L., Hanson, R.K., & Thornton, D. (2009). Reporting Static-99 in light of new research on recidivism norms . The Forum , 21 ( 1 ), 38–45. [ Google Scholar ]
- International Association of Applied Psychology [IAAP] and the International Union of Psychological Science [IUPsyS] (2008). Universal declaration of ethical principles for psychologists . Retrieved http://www.am.org/iupsys/resources/ethics/univdecl2008.html
- Kapoor, R., Young, J.L., Coleman, J.T., Norko, M.A., & Griffith, E.E.H. (2011). Ethics in forensic psychiatry publishing . Journal of the American Academy of Psychiatry and the Law , 39 ( 3 ), 332–341. [ PubMed ] [ Google Scholar ]
- Kazak, A.E. (2018). Editorial: Journal article reporting standards . American Psychologist , 73 ( 1 ), 1–2. doi: 10.1037/amp0000263 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Koocher, G.P. (2012). Walter C. Randall lecture on biomedical ethics: Colleagues as a defense against bad science . The Physiologist , 55 ( 2 ), 52–56. [ PubMed ] [ Google Scholar ]
- Koocher, G.P., & Keith-Spiegel, P. (2010). Peers nip misconduct in the bud . Nature , 466 ( 7305 ), 438–440. doi: 10.1038/466438a [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Koocher, G.P., & Keith-Spiegel, P. (2016). Ethics in psychology and the mental health professions: Standards and cases (4th ed.). New York, NY: Oxford University Press. [ Google Scholar ]
- Kukucka, J., Kassin, S.M., Zapf, P.A., & Dror, I.E. (2017). Cognitive bias and blindness: A global survey of forensic science examiners . Journal of Applied Research in Memory and Cognition , 6 ( 4 ), 452–459. doi: 10.1016/j.jarmac.2017.09.001 [ CrossRef ] [ Google Scholar ]
- Lee, A., & Lincoln, R. (2017). Reciprocity and exchange: Perspectives of male victims of family violence. In Petherick W. & Sinnamon G. (Eds.), The psychology of criminal and antisocial behavior: Victim and offender perspectives (pp. 233–256). London, UK: Elsevier. [ Google Scholar ]
- Levelt, W.J.M. (2012). Flawed science: The fraudulent research practices of social psychologist Diederik Stapel. Retrieved from http://www.tilburguniversity.edu/nl/nieuws-en-agenda/finalreportLevelt.pdf
- Lilienfeld, S.O. (2002). A funny thing happened on the way to my American Psychologist publication . American Psychologist , 57 ( 3 ), 225–227. doi: 10.1037/0003-066X.57.3.225 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Lilienfeld, S.O. (2012). Scientific utopia or scientific dystopia? Psychological Inquiry , 23 ( 3 ), 277–280. doi: 10.1080/1047840X.2012.704807 [ CrossRef ] [ Google Scholar ]
- MacDonald, K.M. (1995). The sociology of professions . Thousand Oaks, CA: Sage. [ Google Scholar ]
- McAuliff, B.D., Hunt, J.S., Levett, L.M., Zelechoski, A.D., Scherr, K.C., & DeMatteo, D. (2019). Taking the next steps: Promoting open science and expanding diversity in Law and Human Behavior . Law and Human Behavior , 43 ( 1 ), 1–8. doi: 10.1037/lhb0000322 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Miller v Alabama, U. S. (2012). Retrieved from https://www.supremecourt.gov/opinions/11pdf/10-9646g2i8.pdf .
- Neal, T.M.S., & Brodsky, S.L. (2016). Forensic psychologists’ perceptions of bias and potential correction strategies in forensic mental health evaluations . Psychology, Public Policy, and Law , 22 ( 1 ), 58–76. doi: 10.1037/law0000077 [ CrossRef ] [ Google Scholar ]
- Neal, T.M.S., & Grisso, T. (2014). The cognitive underpinnings of bias in forensic mental health evaluations . Psychology, Public Policy, and Law , 20 ( 2 ), 200–211. doi: 10.1037/a0035824 [ CrossRef ] [ Google Scholar ]
- Nosek, B.A., & Bar-Anan, Y. (2012). Scientific utopia: I. Opening scientific communication . Psychological Inquiry , 23 ( 3 ), 217–243. doi: 10.1080/1047840X.2012.692215 [ CrossRef ] [ Google Scholar ]
- Parsons, T. (1968). Professions. In Sills D. L. (Ed.), International encyclopedia of social sciences (Vol. 12 , pp. 536–546). New York, NY: MacMillan. [ Google Scholar ]
- Pierson, C.A. (2015). Reviewing journal manuscripts: An easy to follow guide for any nurse reviewing journal manuscripts for publication . Oxford, UK: Wiley Blackwell. [ Google Scholar ]
- Pierson, C.A. (2016). Recognizing peer reviewers and why that matters . Journal of the American Association of Nurse Practitioners , 28 ( 1 ), 5–5. doi: 10.1002/2327-6924.12340 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Quinsey, V.L., Harris, G.T., Rice, M.E., & Comier, C.A. (2006). Violent offenders: Appraising and managing risk (2nd ed.). Washington DC: American Psychological Association. [ Google Scholar ]
- Quinsey, V.L., Harris, G.T., Rice, M.E., & Cormier, C.A. (1998). Violent offenders: Appraising and managing risk . Washington, DC: American Psychological Association. [ Google Scholar ]
- R v Peta. (2007). 2 NZLR 627. Retrieved from http://www.lawreports.nz/r-v-peta-2007-2-nzlr-627/
- Redding, R.E. (2001). Sociopolitical diversity in psychology: The case for pluralism . American Psychologist , 56 ( 3 ), 205–215. doi: 10.1037/0003-066X.56.3.205 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Regehr, C., Edwardh, M., & Bradford, J. (2000). Research ethics and forensic patients . The Canadian Journal of Psychiatry , 45 ( 10 ), 892–898. doi: 10.1177/070674370004501003 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Rice, M.E., & Harris, G.T. (1997). Cross-validation and extension of the Violence Risk Appraisal Guide for child molesters and rapists . Law and Human Behavior , 21 ( 2 ), 231–241. doi: 10.1023/A:1024882430242 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Roberts, J. (2016). Predatory journals: Illegitimate publishing and its threat to all readers and authors . The Journal of Sexual Medicine , 13 ( 12 ), 1830–1833. doi: 10.1016/j.jsxm.2016.10.008 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Roper v Simmons, 543 U.S. 551. (2005). Retrieved from https://caselaw.findlaw.com/us-supreme-court/543/551.html .
- Rosenfeld, B., & Green, D. (2009). Ethical and legal issues in conducting treatment research with potentially violent individuals. In Fisher C., Buchanan D. A., & Gable L. (Eds.), Research with high-risk populations: Balancing science, ethics, and law (1st ed., pp. 167–187). Washington DC: American Psychological Association. [ Google Scholar ]
- Rosenthal, R. (1994). Science and ethics in conducting, analyzing, and reporting psychological research . Psychological Science , 5 ( 3 ), 127–134. doi: 10.1111/j.1467-9280.1994.tb00646.x [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Salaam, A.O., & Brown, J. (2013). Ethical dilemmas in psychological research with vulnerable groups in Africa . Ethics & Behavior , 23 ( 3 ), 167–178. doi: 10.1080/10508422.2012.728478 [ CrossRef ] [ Google Scholar ]
- Schiltz, M. (2018). Science without publication paywalls: cOAlition S for the realisation of full and immediate Open Access . PLoS Biology , 16 ( 9 ), e3000031. doi: 10.1371/journal.pbio.3000031 [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Schminke, M. (2009). Editor’s comments: The better angels of our nature-rthics and integrity in the publishing process . Management and Organization Review , 34 ( 4 ), 586–591. doi: 10.5465/amr.2009.44882922 [ CrossRef ] [ Google Scholar ]
- Schneider, J.L. (2006). Professional codes of ethics: Their role and implications for international research . Journal of Contemporary Criminal Justice , 22 ( 2 ), 173–192. doi: 10.1177/1043986206286960 [ CrossRef ] [ Google Scholar ]
- Schüklenk, U. (2000). Protecting the vulnerable: Testing times for clinical research ethics . Social Science & Medicine , 51 ( 6 ), 969–977. doi: 10.1016/S0277-9536(00)00075-7 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Smallbone, S.W., & Rallings, M. (2013). Short-term predictive validity of the Static-99 and Static-99-R for Indigenous and Nonindigenous Australian sexual offenders . Sexual Abuse: A Journal of Research and Treatment , 25 ( 3 ), 302–316. doi: 10.1177/1079063212472937 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Smith, R. (2006). Peer review: A flawed process at the heart of science and journals . Journal of the Royal Society of Medicine , 99 ( 4 ), 178–182. doi: 10.1177/014107680609900414 [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Steinberg, L. (2013). The influence of neuroscience on US Supreme Court decisions about adolescents’ criminal culpability . Nature Reviews Neuroscience , 14 ( 7 ), 513–518. doi: 10.1038/nrn3509 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Stone, A.A., & MacCourt, D.C. (2008). Ethics in forensic psychiatry: Re-imagining the wasteland after 25 years . The Journal of Psychiatry & Law , 36 ( 4 ), 617–643. doi: 10.1177/009318530803600406 [ CrossRef ] [ Google Scholar ]
- Straight, T.M. (2009). Clinical research regulation: Challenges to the institutional review board system . Clinics in Dermatology , 27 ( 4 ), 375–383. doi: 10.1016/j.clindermatol.2009.02.012 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Strickland, J., Parry, C.L., Allan, M.M., & Allan, A. (2017). Alexithymia amongst perpetrators of violent offences in Australia: Implications for rehabilitation . Australian Psychologist , 52 ( 3 ), 230–237. doi: 10.1111/ap.12187 [ CrossRef ] [ Google Scholar ]
- Van ‘T Veer, A.E., & Giner-Sorolla, R. (2016). Pre-registration in social psychology – A discussion and suggested template . Journal of Experimental Social Psychology , 67 , 2–12. doi: 10.1016/j.jesp.2016.03.004 [ CrossRef ] [ Google Scholar ]
- Van Loon, K., & Lindegger, G. (2009). Consent in clinical trials: Perceptions and experiences of a sample of South African researcher . Health SA Gesondheid , 14 ( 1 ), 81–87. doi: 10.4102/hsag.v14i1.463 [ CrossRef ] [ Google Scholar ]
- Ward, T., & Willis, G. (2010). Ethical issues in forensic and correctional research . Aggression and Violent Behavior , 15 ( 6 ), 399–409. doi: 10.1016/j.avb.2010.07.002 [ CrossRef ] [ Google Scholar ]
- Wells, G.L. (2014). Eyewitness identification probative value, criterion shifts, and policy regarding the sequential lineup . Current Directions in Psychological Science , 23 ( 1 ), 11–16. doi: 10.1177/0963721413504781 [ CrossRef ] [ Google Scholar ]
- Wong, S.C.P., Olver, M.E., Nicholaichuk, T., & Gordon, A. (2003). The Violence Risk Scale – Sex Offender version (VRO-SO) . Saskatoon: Regional Psychiatric Centre and University of Saskatchewan. [ Google Scholar ]
- Wong, S.C.P., Olver, M., Nicholaichuk, T., & Gordon, A. (2006). Violence Risk Scale–Sexual version. Retrieved from http://www.psynergy.ca/VRS_VRS-SO.html
- Wright, P.M. (2016). Ensuring research integrity: An editor’s perspective . Journal of Management , 42 ( 5 ), 1037–1043. doi: 10.1177/0149206316643931 [ CrossRef ] [ Google Scholar ]
- Zapf, P.A., & Dror, I.E. (2017). Understanding and mitigating bias in forensic evaluation: lessons from forensic science . International Journal of Forensic Mental Health , 16 ( 3 ), 227–238. doi: 10.1080/14999013.2017.1317302 [ CrossRef ] [ Google Scholar ]
- Zapf, P.A., Hubbard, K.L., Cooper, V.G., Wheeles, M.C., & Ronan, K.A. (2004). Have the courts abdicated their responsibility for determination of competency to stand trial to clinicians? Journal of Forensic Psychology Practice , 4 ( 1 ), 27–44. doi: 10.1300/J158v04n01_02 [ CrossRef ] [ Google Scholar ]
Case Study Research Method in Psychology
Saul Mcleod, PhD
Editor-in-Chief for Simply Psychology
BSc (Hons) Psychology, MRes, PhD, University of Manchester
Saul Mcleod, PhD., is a qualified psychology teacher with over 18 years of experience in further and higher education. He has been published in peer-reviewed journals, including the Journal of Clinical Psychology.
Learn about our Editorial Process
Olivia Guy-Evans, MSc
Associate Editor for Simply Psychology
BSc (Hons) Psychology, MSc Psychology of Education
Olivia Guy-Evans is a writer and associate editor for Simply Psychology. She has previously worked in healthcare and educational sectors.
On This Page:
Case studies are in-depth investigations of a person, group, event, or community. Typically, data is gathered from various sources using several methods (e.g., observations & interviews).
The case study research method originated in clinical medicine (the case history, i.e., the patient’s personal history). In psychology, case studies are often confined to the study of a particular individual.
The information is mainly biographical and relates to events in the individual’s past (i.e., retrospective), as well as to significant events that are currently occurring in his or her everyday life.
The case study is not a research method, but researchers select methods of data collection and analysis that will generate material suitable for case studies.
Freud (1909a, 1909b) conducted very detailed investigations into the private lives of his patients in an attempt to both understand and help them overcome their illnesses.
This makes it clear that the case study is a method that should only be used by a psychologist, therapist, or psychiatrist, i.e., someone with a professional qualification.
There is an ethical issue of competence. Only someone qualified to diagnose and treat a person can conduct a formal case study relating to atypical (i.e., abnormal) behavior or atypical development.

Famous Case Studies
- Anna O – One of the most famous case studies, documenting psychoanalyst Josef Breuer’s treatment of “Anna O” (real name Bertha Pappenheim) for hysteria in the late 1800s using early psychoanalytic theory.
- Little Hans – A child psychoanalysis case study published by Sigmund Freud in 1909 analyzing his five-year-old patient Herbert Graf’s house phobia as related to the Oedipus complex.
- Bruce/Brenda – Gender identity case of the boy (Bruce) whose botched circumcision led psychologist John Money to advise gender reassignment and raise him as a girl (Brenda) in the 1960s.
- Genie Wiley – Linguistics/psychological development case of the victim of extreme isolation abuse who was studied in 1970s California for effects of early language deprivation on acquiring speech later in life.
- Phineas Gage – One of the most famous neuropsychology case studies analyzes personality changes in railroad worker Phineas Gage after an 1848 brain injury involving a tamping iron piercing his skull.
Clinical Case Studies
- Studying the effectiveness of psychotherapy approaches with an individual patient
- Assessing and treating mental illnesses like depression, anxiety disorders, PTSD
- Neuropsychological cases investigating brain injuries or disorders
Child Psychology Case Studies
- Studying psychological development from birth through adolescence
- Cases of learning disabilities, autism spectrum disorders, ADHD
- Effects of trauma, abuse, deprivation on development
Types of Case Studies
- Explanatory case studies : Used to explore causation in order to find underlying principles. Helpful for doing qualitative analysis to explain presumed causal links.
- Exploratory case studies : Used to explore situations where an intervention being evaluated has no clear set of outcomes. It helps define questions and hypotheses for future research.
- Descriptive case studies : Describe an intervention or phenomenon and the real-life context in which it occurred. It is helpful for illustrating certain topics within an evaluation.
- Multiple-case studies : Used to explore differences between cases and replicate findings across cases. Helpful for comparing and contrasting specific cases.
- Intrinsic : Used to gain a better understanding of a particular case. Helpful for capturing the complexity of a single case.
- Collective : Used to explore a general phenomenon using multiple case studies. Helpful for jointly studying a group of cases in order to inquire into the phenomenon.
Where Do You Find Data for a Case Study?
There are several places to find data for a case study. The key is to gather data from multiple sources to get a complete picture of the case and corroborate facts or findings through triangulation of evidence. Most of this information is likely qualitative (i.e., verbal description rather than measurement), but the psychologist might also collect numerical data.
1. Primary sources
- Interviews – Interviewing key people related to the case to get their perspectives and insights. The interview is an extremely effective procedure for obtaining information about an individual, and it may be used to collect comments from the person’s friends, parents, employer, workmates, and others who have a good knowledge of the person, as well as to obtain facts from the person him or herself.
- Observations – Observing behaviors, interactions, processes, etc., related to the case as they unfold in real-time.
- Documents & Records – Reviewing private documents, diaries, public records, correspondence, meeting minutes, etc., relevant to the case.
2. Secondary sources
- News/Media – News coverage of events related to the case study.
- Academic articles – Journal articles, dissertations etc. that discuss the case.
- Government reports – Official data and records related to the case context.
- Books/films – Books, documentaries or films discussing the case.
3. Archival records
Searching historical archives, museum collections and databases to find relevant documents, visual/audio records related to the case history and context.
Public archives like newspapers, organizational records, photographic collections could all include potentially relevant pieces of information to shed light on attitudes, cultural perspectives, common practices and historical contexts related to psychology.
4. Organizational records
Organizational records offer the advantage of often having large datasets collected over time that can reveal or confirm psychological insights.
Of course, privacy and ethical concerns regarding confidential data must be navigated carefully.
However, with proper protocols, organizational records can provide invaluable context and empirical depth to qualitative case studies exploring the intersection of psychology and organizations.
- Organizational/industrial psychology research : Organizational records like employee surveys, turnover/retention data, policies, incident reports etc. may provide insight into topics like job satisfaction, workplace culture and dynamics, leadership issues, employee behaviors etc.
- Clinical psychology : Therapists/hospitals may grant access to anonymized medical records to study aspects like assessments, diagnoses, treatment plans etc. This could shed light on clinical practices.
- School psychology : Studies could utilize anonymized student records like test scores, grades, disciplinary issues, and counseling referrals to study child development, learning barriers, effectiveness of support programs, and more.
How do I Write a Case Study in Psychology?
Follow specified case study guidelines provided by a journal or your psychology tutor. General components of clinical case studies include: background, symptoms, assessments, diagnosis, treatment, and outcomes. Interpreting the information means the researcher decides what to include or leave out. A good case study should always clarify which information is the factual description and which is an inference or the researcher’s opinion.
1. Introduction
- Provide background on the case context and why it is of interest, presenting background information like demographics, relevant history, and presenting problem.
- Compare briefly to similar published cases if applicable. Clearly state the focus/importance of the case.
2. Case Presentation
- Describe the presenting problem in detail, including symptoms, duration,and impact on daily life.
- Include client demographics like age and gender, information about social relationships, and mental health history.
- Describe all physical, emotional, and/or sensory symptoms reported by the client.
- Use patient quotes to describe the initial complaint verbatim. Follow with full-sentence summaries of relevant history details gathered, including key components that led to a working diagnosis.
- Summarize clinical exam results, namely orthopedic/neurological tests, imaging, lab tests, etc. Note actual results rather than subjective conclusions. Provide images if clearly reproducible/anonymized.
- Clearly state the working diagnosis or clinical impression before transitioning to management.
3. Management and Outcome
- Indicate the total duration of care and number of treatments given over what timeframe. Use specific names/descriptions for any therapies/interventions applied.
- Present the results of the intervention,including any quantitative or qualitative data collected.
- For outcomes, utilize visual analog scales for pain, medication usage logs, etc., if possible. Include patient self-reports of improvement/worsening of symptoms. Note the reason for discharge/end of care.
4. Discussion
- Analyze the case, exploring contributing factors, limitations of the study, and connections to existing research.
- Analyze the effectiveness of the intervention,considering factors like participant adherence, limitations of the study, and potential alternative explanations for the results.
- Identify any questions raised in the case analysis and relate insights to established theories and current research if applicable. Avoid definitive claims about physiological explanations.
- Offer clinical implications, and suggest future research directions.
5. Additional Items
- Thank specific assistants for writing support only. No patient acknowledgments.
- References should directly support any key claims or quotes included.
- Use tables/figures/images only if substantially informative. Include permissions and legends/explanatory notes.
- Provides detailed (rich qualitative) information.
- Provides insight for further research.
- Permitting investigation of otherwise impractical (or unethical) situations.
Case studies allow a researcher to investigate a topic in far more detail than might be possible if they were trying to deal with a large number of research participants (nomothetic approach) with the aim of ‘averaging’.
Because of their in-depth, multi-sided approach, case studies often shed light on aspects of human thinking and behavior that would be unethical or impractical to study in other ways.
Research that only looks into the measurable aspects of human behavior is not likely to give us insights into the subjective dimension of experience, which is important to psychoanalytic and humanistic psychologists.
Case studies are often used in exploratory research. They can help us generate new ideas (that might be tested by other methods). They are an important way of illustrating theories and can help show how different aspects of a person’s life are related to each other.
The method is, therefore, important for psychologists who adopt a holistic point of view (i.e., humanistic psychologists ).
Limitations
- Lacking scientific rigor and providing little basis for generalization of results to the wider population.
- Researchers’ own subjective feelings may influence the case study (researcher bias).
- Difficult to replicate.
- Time-consuming and expensive.
- The volume of data, together with the time restrictions in place, impacted the depth of analysis that was possible within the available resources.
Because a case study deals with only one person/event/group, we can never be sure if the case study investigated is representative of the wider body of “similar” instances. This means the conclusions drawn from a particular case may not be transferable to other settings.
Because case studies are based on the analysis of qualitative (i.e., descriptive) data , a lot depends on the psychologist’s interpretation of the information she has acquired.
This means that there is a lot of scope for Anna O , and it could be that the subjective opinions of the psychologist intrude in the assessment of what the data means.
For example, Freud has been criticized for producing case studies in which the information was sometimes distorted to fit particular behavioral theories (e.g., Little Hans ).
This is also true of Money’s interpretation of the Bruce/Brenda case study (Diamond, 1997) when he ignored evidence that went against his theory.
Breuer, J., & Freud, S. (1895). Studies on hysteria . Standard Edition 2: London.
Curtiss, S. (1981). Genie: The case of a modern wild child .
Diamond, M., & Sigmundson, K. (1997). Sex Reassignment at Birth: Long-term Review and Clinical Implications. Archives of Pediatrics & Adolescent Medicine , 151(3), 298-304
Freud, S. (1909a). Analysis of a phobia of a five year old boy. In The Pelican Freud Library (1977), Vol 8, Case Histories 1, pages 169-306
Freud, S. (1909b). Bemerkungen über einen Fall von Zwangsneurose (Der “Rattenmann”). Jb. psychoanal. psychopathol. Forsch ., I, p. 357-421; GW, VII, p. 379-463; Notes upon a case of obsessional neurosis, SE , 10: 151-318.
Harlow J. M. (1848). Passage of an iron rod through the head. Boston Medical and Surgical Journal, 39 , 389–393.
Harlow, J. M. (1868). Recovery from the Passage of an Iron Bar through the Head . Publications of the Massachusetts Medical Society. 2 (3), 327-347.
Money, J., & Ehrhardt, A. A. (1972). Man & Woman, Boy & Girl : The Differentiation and Dimorphism of Gender Identity from Conception to Maturity. Baltimore, Maryland: Johns Hopkins University Press.
Money, J., & Tucker, P. (1975). Sexual signatures: On being a man or a woman.
Further Information
- Case Study Approach
- Case Study Method
- Enhancing the Quality of Case Studies in Health Services Research
- “We do things together” A case study of “couplehood” in dementia
- Using mixed methods for evaluating an integrative approach to cancer care: a case study
Related Articles

Research Methodology
Qualitative Data Coding

What Is a Focus Group?

Cross-Cultural Research Methodology In Psychology

What Is Internal Validity In Research?

Research Methodology , Statistics
What Is Face Validity In Research? Importance & How To Measure

Criterion Validity: Definition & Examples
- Open access
- Published: 27 May 2024
Associations between medical students’ stress, academic burnout and moral courage efficacy
- Galit Neufeld-Kroszynski ORCID: orcid.org/0000-0001-9093-1308 1 na1 ,
- Keren Michael ORCID: orcid.org/0000-0003-2662-6362 2 na1 &
- Orit Karnieli-Miller ORCID: orcid.org/0000-0002-5790-0697 1
BMC Psychology volume 12 , Article number: 296 ( 2024 ) Cite this article
142 Accesses
Metrics details
Medical students, especially during the clinical years, are often exposed to breaches of safety and professionalism. These contradict personal and professional values exposing them to moral distress and to the dilemma of whether and how to act. Acting requires moral courage, i.e., overcoming fear to maintain one’s core values and professional obligations. It includes speaking up and “doing the right thing” despite stressors and risks (e.g., humiliation). Acting morally courageously is difficult, and ways to enhance it are needed. Though moral courage efficacy, i.e., individuals’ belief in their capability to act morally, might play a significant role, there is little empirical research on the factors contributing to students’ moral courage efficacy. Therefore, this study examined the associations between perceived stress, academic burnout, and moral courage efficacy.
A cross-sectional study among 239 medical students who completed self-reported questionnaires measuring perceived stress, academic burnout (‘exhaustion,’ ‘cynicism,’ ‘reduced professional efficacy’), and moral courage efficacy (toward others’ actions and toward self-actions). Data analysis via Pearson’s correlations, regression-based PROCESS macro, and independent t -tests for group differences.
The burnout dimension of ‘reduced professional efficacy’ mediated the association between perceived stress and moral courage efficacy toward others’ actions. The burnout dimensions ‘exhaustion’ and ‘reduced professional efficacy’ mediated the association between perceived stress and moral courage efficacy toward self-actions.
Conclusions
The results emphasize the importance of promoting medical students’ well-being—in terms of stress and burnout—to enhance their moral courage efficacy. Medical education interventions should focus on improving medical students’ professional efficacy since it affects both their moral courage efficacy toward others and their self-actions. This can help create a safer and more appropriate medical culture.
Peer Review reports
Introduction
In medical school, and especially during clinical years, medical students (MS) are often exposed to physicians’ inappropriate behaviors and various breaches of professionalism or safety [ 1 , 2 , 3 ]. These can include lack of respect or sensitivity toward patients and other healthcare staff, deliberate lies and deceptions, breaching confidentiality, inadequate hand hygiene, or breach of a sterile field [ 4 , 5 ]. Furthermore, MS find themselves performing and/or participating in these inappropriate behaviors. For example, a study found that 80% of 3 rd– 4th year MS reported having done something they believed was unethical or having misled a patient [ 6 ]. Another study showed that 47.1–61.3% of females and 48.8–56.6% of male MS reported violating a patient’s dignity, participating in safety breaches, or examining/performing a procedure on a patient without valid consent, following a clinical teacher’s request, as a learning exercise [ 5 ]. These behaviors contradict professional values and MS’ own personal and moral values, exposing them to a dilemma in which they must choose if and how to act.
Taking action requires moral courage, i.e., taking an active stand or acting in the face of wrongdoing or moral injustice jeopardizing mental well-being [ 7 , 8 , 9 , 10 ]. Moral courage includes speaking up and “doing the right thing” despite risks, such as shame, retaliation, threat to reputation, or even loss of employment [ 8 ]. Moral courage is expressed in two main situations: when addressing others’ wrongdoing (e.g., identifying and disclosing a past/present medical error by colleagues/physicians); or when admitting one’s own wrongdoing (e.g., disclosing an error or lack of knowledge) [ 11 ].
Due to its “calling out” nature, acting on moral courage is difficult. A hierarchy and unsafe learning environment inhibits the ability for assertive expression of concern [ 12 , 13 , 14 ]. This leads to concerning findings indicating that only 38% of MS reported that they would approach someone performing an unsafe behavior [ 12 ], and about half claimed that they would report an error they had observed [ 15 ].
Various reasons were suggested to explain why MS, interns, residents, or nurses, hesitate to act in a morally courageous way, including difficulty questioning the decisions or actions of those with more authority [ 12 ], and fear of negative social consequences, such as being disgraced, excluded, attacked, punished, or poorly evaluated [ 13 ]. Other reasons were the wish to fit into the team [ 6 ] and being a young professional experiencing “lack of knowledge” or “unfamiliarity” with clinical subtleties [ 16 ].
Nevertheless, failing to act on moral courage might lead to negative consequences, including moral distress [ 17 ]. Moral distress is a psychological disequilibrium that occurs when knowing the ethically right course of action but not acting upon it [ 18 ]. Moral distress is a known phenomenon among MS [ 19 ], e.g., 90% of MS at a New York City medical school reported moral distress when carrying for older patients [ 20 ]. MS’ moral distress was associated with thoughts of dropping out of medical school, choosing a nonclinical specialty, and increased burnout [ 20 ].
These consequences of moral distress and challenges to acting in a morally courageous way require further exploration of MS’ moral courage in general and their moral courage efficacy specifically. Bandura coined the term self-efficacy, focused on one’s perception of how well s/he can execute the action required to deal successfully with future situations and to achieve desired outcomes [ 21 ]. Self-efficacy plays a significant role in human behavior since individuals are more likely to engage in activities they believe they can handle [ 21 ]. Therefore, self-efficacy regarding a particular skill is a major motivating factor in the acquisition, development, and application of that skill [ 22 ]. For example, individuals’ perception regarding their ability to deal positively with ethical issues [ 23 ], their beliefs that they can handle effectively what is required to achieve moral performance [ 24 ], and to practically act as moral agents [ 25 ], can become a key psychological determinant of moral motivation and action [ 26 ]. Due to self-efficacy’s importance there is a need to learn about moral courage efficacy, i.e., individuals’ belief in their ability to exhibit moral courage through sharing their concerns regarding others and their own wrongdoing. Moral courage efficacy was suggested as important to moral courage in the field of business [ 27 ], but not empirically explored in medicine. Thus, there is no known prevalence of moral courage efficacy toward others and toward one’s own wrongdoing in medicine in general and for MS in particular. Furthermore, the potential contributing factors to moral courage efficacy, such as stress and burnout, require further exploration.
The associations between stress, burnout, and moral courage efficacy
Stress occurs when people view environmental demands as exceeding their ability to cope with them [ 28 ]. MS experience high levels of stress during their studies [ 29 ], due to excessive workload, time management difficulties, work–life balance conflicts, health concerns, and financial worries [ 30 ]. Studies show that high levels of stress were associated with decreased empathy [ 31 ], increased academic burnout, academic dishonesty, poor academic performance [ 32 ], and thoughts about dropping out of medical school [ 33 ]. As stress may impact one’s perceived efficacy [ 34 ], this study examined whether stress can inhibit individuals’ moral courage efficacy to address others’ and their own wrongdoing.
An aspect related to a poor mental state that may mediate the association between stress and MS’ moral courage efficacy is burnout. Burnout includes emotional exhaustion, cynicism toward one’s occupation value, and doubting performance ability [ 35 ]. Burnout is usually work-related and is common in the helping professions [ 60 ]. For students, this concept relates to academic burnout [ 36 ], which includes exhaustion due to study demands, a cynical and detached attitude to studying, and low/reduced professional efficacy, i.e. feeling incompetent as learners [ 37 ].
Burnout has various negative implications for MS’ well-being and professional development. Burnout is associated with psychiatric disorders and thoughts of dropping out of medical school [ 33 ]. Furthermore, MS’ burnout is associated with increased involvement in unprofessional behavior, eroding professional development, diminishing qualities such as honesty, integrity, altruism, and self-regulation [ 38 ], reducing empathy [ 31 , 39 ] and unwillingness to provide care for the medically underserved [ 40 ]. Thus, burnout may also impact MS’ views on their responsibility and perceived ability to promote high-quality care and advocate for patients [ 41 ], possibly leading them to feel reluctant and incapable to act with moral courage [ 42 ]. Earlier studies exploring stress and its various outcomes, found that burnout, and specifically exhaustion, can become a crucial mediator for various harmful outcomes [ 43 ]. Although stress is impactful to creating discomfort, the decision and ability to intervene requires one’s own drive and power. When one is feeling stress, leading to burnout their depleted energy reserves and diminished sense of professional worth likely undermine their perceived power (due to exhaustion) or will (due to cynicism) to uphold professional ethical standards and intervene to advocate for patient care in challenging circumstances, such as the need to speak up in front of authority members. Furthermore, burnout may facilitate a cognitive distancing from professional values and responsibilities, allowing for moral disengagement and reducing the likelihood of morally courageous actions. This mediation role requires further exploration.
This study examined associations between perceived stress, academic burnout, and moral courage efficacy. In addition to the mere associations among the variables, it will be examined whether there is a mediation effect (perceived stress → academic burnout → moral courage efficacy) to gain more insight into possible mechanisms of the development of moral courage efficacy and of protective factors. Understanding these mechanisms has educational benefit for guiding interventions to enhance MS’ moral courage efficacy.
H1: Perceived stress and academic burnout dimensions will be negatively associated with moral courage efficacy dimensions.
H2: Perceived stress will be positively associated with academic burnout dimensions.
H3: Academic burnout dimensions will mediate the association between perceived stress and moral courage efficacy dimensions.
Materials and methods
Sample and procedure.
A quantitative cross-sectional study among 239 MS. Most participants were female (60%), aged 29 or less (90%), and unmarried (75%). About two thirds (64.3%) were at the pre-clinical stage of medical school and about a third (35.7%) at the clinical stage. In December 2019, the research team approached MS through email and social media to participate in the study and complete an online questionnaire. This was a part of a national study focused on MS’ burnout [ 44 ]. The 239 participants were recruited by a convenience sampling. Data were collected online through Qualtrics platform, via anonymous self-reported questionnaires. The University Ethics Committee approved the study, and all participants signed an informed consent form.
Moral courage efficacy —This 8-item instrument, developed for this study, is based on the literature on moral courage, professionalism, and speaking-up, including qualitative and quantitative studies [ 7 , 13 , 45 , 46 , 47 ], and discussions with MS and medical educators. The main developing team included a Ph.D. medical educator expert in communication in healthcare and professionalism; an M.D. psychiatrist expert in decision making, professionalism, and philosophy; a Ph.D. graduate who analyzed MS’ narratives focused on moral dilemmas and moral courage during professionalism breaches; and a Ph.D. candidate focused on assertiveness in medicine [ 14 ]. This allowed the identification of different types of situations MS face that may require moral courage.
As guided by instructions for measuring self-efficacy, which encourage using specific statements that relate to the specific situation and skill required [ 48 ], the instrument measures MS’ perception of their own ability, i.e., self-efficacy, to act based on their moral beliefs when exposed to safety and professionalism breaches or challenges. Due to our qualitative findings indicating that students change their interpretation of the problematic event based on their decision to act in a morally courageous way and that some are exposed to specific professionalism violations while others are not when designing the questionnaire, we decided to make the cases not explicit to specific types of professionalism breaches – e.g., not focused on talking above a patient’s head [ 1 ], but rather general the type of behavior e.g., “behaves immorally”. This decreases the personal interpretation if one behavior is acceptable by this individual; and also decreases the possibility of not answering the question if the individual student has never seen that specific behavior. Furthermore, to avoid “gray areas” in moral issues, we wrote the statements in a manner where there is no doubt whether there is a moral problem (“problematic situation”) [ 47 ], and thus the focus was only on one’s feeling of being capable of speaking up about their concern, i.e., act in a moral courage efficacy (see Table 1 ).
The instrument’s initial development consisted of 14 items addressing various populations, including senior MDs. The 14-item tool included questions regarding the willingness to recommend a second opinion or to convey one’s medical mistake to patients and their families. These actions are less relevant to MS. Thus, we extracted the questionnaire to a parsimonious instrument of 8 items.
The 8 items were divided into two dimensions: others and the self. This division is supported by the literature on moral courage that distinguishes between courage regarding others- vs. self-behavior. Hence, the questionnaire was designed to assess one’s perceived ability to act/speak up in these two dimensions: (a) situations of moral courage efficacy relating to others’ behavior (e.g., “ capable of telling a senior physician if I have detected a mistake s/he might have made ”); (b) situations of moral courage efficacy relating to self (e.g., “ capable of disclosing my mistakes to a senior physician ”). This two-dimension division is important and was absent in former measurements of moral courage. It was also replicated in another study we conducted among MS [ 49 ]. Furthermore, factor analysis with Oblimin rotation supported this two-factor structure (Table 1 ). All items had a high factor loading on the relevant factor (it should be mentioned that item 4 was loaded 0.59 on the relevant factor and 0.32 on the non-relevant factor).
All items are rated on a 5-point Likert scale (0 = to a small extent; 4 = to a very great extent) and are calculated by averaging the answers on the dimension, with higher scores representing higher moral courage efficacy. Internal reliability was α = 0.80 for the “others” dimension and α = 0.84 for the “self” dimension.
Perceived stress —This single-item questionnaire (“How would you rate the level of stress you’ve been experiencing in the last few days?” ) evaluates MS’ perceived stress currently in their life on an 11-point Likert scale (0 = no stress; 10 = extreme stress), with higher scores representing higher perceived stress. It is based on a similar question evaluating MS’ perceived emotional stress [ 29 ]. Even though a multi-item measure might be more stable, previous studies indicated that using a single item is a practical, reliable alternative, with high construct validity in the context of felt/perceived stress, self-esteem, health status, etc [ 43 , 50 , 51 ].
Academic burnout —This 15-item instrument is a translated version [ 44 ] of the MBI-SS (MBI–Student Survey) [ 37 ], a common instrument used to measure burnout in the academic context, e.g. MS [ 52 , 53 ]. It measures students’ feelings of burnout regarding their studies on three dimensions: (a) ‘exhaustion’ (5 items; e.g., “ Studying or attending a class is a real strain for me ”), (b) ‘cynicism’ (4 items; e.g., “ I doubt the significance of my studies ”), (c) lack of personal academic efficacy (‘reduced professional efficacy’) (6 items; “ I feel [un]stimulated when I achieve my study goals ”). Each item is rated on a 7-point Likert scale (0 = never; 6 = always) and is calculated by summing the answers on the dimension (after re-coding all professional efficacy items), with higher scores representing more frequent feelings of burnout. Internal reliability was α = 0.80 for ‘exhaustion’, α = 0.80 for ‘cynicism’, and α = 0.84 for ‘reduced professional efficacy’.
Statistical analyses
IBM-SPSS (version 25) was used to analyze the data. Pearson’s correlations examined all possible bivariate associations between the study variables. PROCESS macro examined the mediation effects (via model#4). The significance of the mediation effects was examined by calculating 5,000 samples to estimate the 95% percentile bootstrap confidence intervals (CIs) of indirect effects of the predictor on the outcome through the mediator [ 54 ]. T -tests for independent samples examined differences between the study variables in the pre-clinic and clinic stages. The defined significance level was set generally to 5% ( p < 0.05).
This study focused on understanding moral courage efficacy, i.e., MS’ perceived ability to speak up and act while exposed to others’ and their own wrongdoing. The sample’s frequencies demonstrate that only 10% of the MS reported that their moral courage efficacy toward the others was “very high to high,” and 54% reported this toward the self. Mean scores demonstrate that regarding the others, MS showed relatively low/moderate levels of moral courage and higher levels regarding the self. As for the variables tested to be associated with moral courage efficacy, MS showed relatively high perceived stress and low-to-moderate academic burnout (see Table 2 for the variables’ psychometric characteristics).
Table 2 also shows the correlations among the study variables. According to Cohen’s (1988) [ 55 ] interpretation of the strength in bivariate associations (Pearson correlation), the effect size is low when r value varies around 0.1, medium when it is around 0.3, and large when it is more than 0.5. Hence, regarding the associations between the two dimensions of moral courage efficacy: we found a moderate positive correlation between the efficacy toward others and the efficacy toward the self. Regarding the associations among the three academic burnout dimensions: we found a strong positive correlation between ‘exhaustion’ and ‘cynicism,’ a weak positive correlation between ‘exhaustion’ and ‘reduced professional efficacy,’ and a moderate positive correlation between ‘cynicism,’ and ‘reduced professional efficacy.’
As for the associations concerning H1, Table 2 indicates that one academic burnout dimension, i.e., ‘reduced professional efficacy,’ had a weak negative correlation with moral courage efficacy toward the others, thus high burnout was associated with lower perceived moral courage efficacy toward others. Additionally, perceived stress and all three burnout dimensions had weak negative correlations with moral courage efficacy toward the self—partially supporting H1.
As for the associations concerning H2, Table 2 indicates that perceived stress had a strong positive correlation with ‘exhaustion,’ a moderate positive correlation with ‘cynicism,’ and a weak positive correlation with ‘reduced professional efficacy’—supporting H2.
Based on these correlations, we conducted regression-based models to examine the unique and complex relationships among the study variable, including their various dimensions, while focusing on the examination of whether academic burnout mediates the association between perceived stress and moral courage efficacy (see Tables 3 and 4 ; and Figs. 1 and 2 ).

A model presenting the association between perceived stress and moral courage efficacy toward others, mediated by academic burnout. Note full arrows contain significant β coefficient values (fractured arrows mean nonsignificance
Focusing on moral courage efficacy toward others
Table 3 and Fig. 1 indicate that perceived stress was positively associated with all three academic burnout dimensions: ‘exhaustion’ (path a 1 ), ‘cynicism’ (path a 2 ), and ‘reduced professional efficacy’ (path a 3 ). These paths support H2. In turn, ‘reduced professional efficacy’ was negatively associated with moral courage efficacy toward the others (path b 3 ), supporting H1. The CIs of the indirect effect (paths a 3 b 3 ) did not contain zero; therefore, perceived stress had a significant indirect effect on moral courage efficacy toward the others, through the burnout dimension ‘reduced professional efficacy.’ This path supports H3.

A model presenting the association between perceived stress and moral courage efficacy towards self, mediated by academic burnout. Note full arrows contain significant β coefficient values (fractured arrows mean non-significance
Focusing on moral courage efficacy toward the self
Table 4 and Fig. 2 also indicate that perceived stress was positively associated with all three academic burnout dimensions: ‘exhaustion’ (path a 4 ), ‘cynicism’ (path a 5 ), and ‘reduced professional efficacy’ (path a 6 ). These paths support H2. In turn, ‘exhaustion’ and ‘reduced professional efficacy’ were negatively associated with moral courage efficacy toward the self (paths b 4 , b 6 respectively). These paths support H1 The CIs of the indirect effects (paths a 4 b 4 , a 6 b 6 ) did not contain zero; therefore, perceived stress had a significant indirect effect on moral courage efficacy toward the self, through the burnout dimensions ‘exhaustion’ and ‘reduced professional efficacy.’ These paths support H3. It should be noted that in this analysis, the initially significant association between perceived stress and moral courage efficacy toward the self (path c 2, representing H1) became insignificant in the existence of academic burnout dimensions (path c’ 2 ). These results demonstrate complete mediation and also support H3.
In addition to examining the complex relationships between stress, academic burnout, and moral courage efficacy among MS, we tested the differences between MS in the pre-clinical and clinical school stages in all study variables. The results indicate non-significant differences in moral courage efficacy. However, medical-school-stage differences were found in stress [t(197.4)=-4.36, p < 0.001] and in one academic burnout dimension [t(233)=-2.40, p < 0.01]. In that way, MS at the clinical stage reported higher levels of perceived stress ( M = 7.32; SD = 2.17) and exhaustion ( M = 19.67; SD = 6.58) than MS in the pre-clinical stage ( M = 5.94; SD = 2.59 and M = 17.48; SD = 6.78, respectively).
This study examined the associations between perceived stress, academic burnout, and moral courage efficacy to understand MS’ perceived ability to speak up and act while exposed to others’ and their own wrongdoing. The findings show that one dimension of burnout, that of ‘reduced professional efficacy,’ mediated the associations between perceived stress and moral courage efficacy toward both others and self. ‘Exhaustion’ mediated the association between perceived stress and moral courage efficacy only toward the self.
Before discussing the meanings of the associations, this study was an opportunity to explore moral courage efficacy occurrence. The findings indicated fairly low/moderate mean scores of perceived ability to speak up and act while confronted with others’ wrongdoing and moderate/high scores of perceived ability while confronted with one’s own wrongdoing. This implies that students do not feel capable enough to share their concerns regarding others’ possible errors and feel more able, but still not enough, to share their own flaws and needs for guidance. These findings require attention, from both patient safety and learning perspectives.
Regarding patient safety, feeling unable to act while confronted with others or self- wrongdoing means that some errors may occur and not be addressed. This is in line with former findings that showed that less than 50% of MS would actually approach someone performing an unsafe behavior [ 12 ], or report an error they had observed [ 15 ]. These numbers are likely to improve in postgraduates as studies showed that between 64 and 79% of interns and residents reported they would likely speak up to an attending when exposed to a safety threat [ 56 , 57 ].
Regarding learning, our MS’ scores must improve for various reasons. First, moderate scores may indicate a psychologically unsafe learning environment, which prevents or discourages sharing uncertainties, especially about others’ behavior, and creates difficulty for students to share their own concerns, limitations, mistakes, and hesitations when feeling incapable or unqualified for a task [ 58 ]. Second, limited sharing of errors may be problematic because by not disclosing their error, students miss the chance to learn from it; [ 59 ] they lose the opportunity for reflective guidance to explore what worked well, what did not, and how to improve [ 59 , 60 ]. Third, if they do not discuss others’ errors or their own, they may deny themselves the necessary support to learn the all-important skills of how to deal with the emotional turmoil and challenges of errors, and how to share the error with a patient or family member [ 61 ]. Furthermore, if MS feel incapable of sharing their concern about a senior’s possible mistake, they miss other learning opportunities—e.g., the senior’s reasoning and clinical judgment may show that a mistake was not made. In this case, the student would miss being shown why they were wrong and what they did do well. Thus, identifying what can enhance moral courage efficacy and practice is needed. The fact that there are no significant differences between pre-clinical and clinical years students in their perceived ability to apply moral courage, may indicate that there is a cultural barrier in perceiving the idea of sharing weakness or of revealing others’ mistakes as unacceptable. Thus, the socialization, in the medical school environment, both in pre-clinical and clinical years, perhaps lacks the encouragement to speak up and provision of safe space.
This study examined the associations between perceived stress, academic burnout, and moral courage efficacy among MS. The findings indicate that, like earlier studies, stress is not directly connected to speaking up [ 62 ] or moral courage. It rather contributes to it indirectly, through the impact of burnout. Beyond the well-established role of stress in explaining burnout [ 63 , 64 ], we identified a negative consequence of burnout—hindering moral courage efficacy. This may help explain the path in which previous studies found burnout to impair MS’ quality of life, how it leads to dropout, and to more medical errors [ 65 ]. When individuals experience the burnout dimension of ‘reduced professional efficacy,’ they may feel less confident and fit, leading them to feel more disempowered to take the risk (required in courage) and share their concerns and hesitations about others’ mistakes and their own challenges. This fits earlier studies indicating that being a young professional experiencing “lack of knowledge” or “unfamiliarity” with clinical subtleties is a barrier to moral courage [ 11 ]. This may have various negative implications, of limited moral courage efficacy, as seen here, as well as paying less attention and not fully addressing their learning needs, leading to a vicious cycle of “feeding” the misfit feeling, potentially increasing their moral distress. Furthermore, those who feel they know less and, therefore, need more support to fill the gap in knowledge and skills, are less inclined to ask for help.
Beside the negative associations between ‘reduced professional efficacy’ and both dimensions of moral courage efficacy (toward others and the self), another dimension of academic burnout—‘exhaustion’—was negatively associated with moral courage efficacy toward the self. This is worrying because when learners are exhausted, their attention is reduced and they are at greater risk of error, as proven in an earlier study [ 65 ]. The current study adds to this information another worry, showing that MS are less willing to share their hesitations about themselves or the mistakes they already made, thus perhaps not preventing the error or fixing it. MS might create an unspoken contract with senior physicians about not exposing each other’s mistakes, with various possible negative implications. Some MS’ tendency to defend physicians’ mistakes was identified elsewhere [ 66 ].
The findings concerning medical-school-stage differences demonstrated that MS in the clinical stage had higher perceived stress and exhaustion levels than MS in the pre-clinical stage. These results support previous studies indicating stress, academic burnout, and more challenging characteristics among more senior students, including a decline in ideals, altruistic attitudes, and empathy during medical school studies; or more exhaustion, cynicism, and higher levels of detached emotions and depression through the years of medical school [ 67 , 68 , 69 ]. These higher levels of stress and exhaustion, can be explained by the senior students’ exposure to the rounds in the hospitals, which requires ongoing learning, more pressure, and a sense of overload in their academic life.
Limitations and future studies
Despite the importance of the findings, the study has several limitations. First, the participants were from one university, and recruited via convenience sampling, including only MS who voluntarily completed the questionnaires, undermining generalizability. To address this limitation, future research should aim to include a more diverse and representative sample of medical students from multiple universities and geographical regions. This would enhance the external validity and applicability of the findings across different educational and cultural contexts. Second, future studies are recommended to follow up on medical students’ stress, academic burnout, and moral courage efficacy over time. Exploring the development of professional efficacy and the barriers to exposing one’s and others’ weaknesses and flaws within the medical environment can help improve the medical culture into a safer space. Third, an intriguing avenue for future research is the exploration of the construct of ‘moral courage efficacy’ within different cohorts of healthcare students throughout their undergraduate and postgraduate years to learn about their moral courage efficacy development as well as and to verify the association between the findings from this newly developed scale and actual moral courage behavior. Additionally, experimental designs, such as interventions to reduce stress and burnout among medical students, could be employed to observe the impact on moral courage efficacy.
Conclusions and implications
This study is a first step in understanding moral courage efficacy and what contributes to it. The study emphasizes the importance of promoting MS’ well-being—in terms of stress and burnout—to enhance their moral courage efficacy. The findings show that the ‘reduced professional efficacy’ mediated the association between perceived stress and moral courage efficacy, toward both the others and self. This has potential implications for safety, learning, and well-being. To encourage MS to develop moral courage efficacy that will potentially increase their morally courageous behavior, we must find ways to reduce their stress and burnout levels. As the learning and work environments are a major cause of burnout [ 38 ], it would be helpful to focus on creating safe spaces where they can share others- and self-related concerns [ 70 ]. The first step is a learning environment promoting students’ overall health and well-being [ 71 ]. Useful additions are processes that support MS while dealing with education- and training-related stresses, improving their academic-professional efficacy, and constructively helping them handle challenging situations through empathic feedback [ 70 ]. This can lead them to a stronger belief in their ability to share safety and professionalism issues, thus enhancing their learning and patient care.
Data availability
No datasets were generated or analysed during the current study.
Karnieli-Miller O, Vu TR, Holtman MC, Clyman SG, Inui TS. Medical students’ professionalism narratives: a window on the informal and hidden curriculum. Acad Med. 2010;85(1):124–33. https://doi.org/10.1097/ACM.0b013e3181c42896 .
Article PubMed Google Scholar
Gaufberg EH, Batalden M, Sands R, Bell SK. The hidden curriculum: what can we learn from third-year medical student narrative reflections? Acad Med. 2010;85(11):1709–16. https://doi.org/10.1097/ACM.0b013e3181f57899 .
Monrouxe LV, Rees CE, Endacott R, Ternan E. Even now it makes me angry: Health care students’ professionalism dilemma narratives. Med Educ. 2014;48(5):502–17. https://doi.org/10.1111/medu.12377 .
Karnieli-Miller O, Taylor AC, Cottingham AH, Inui TS, Vu TR, Frankel RM. Exploring the meaning of respect in medical student education: an analysis of student narratives. J Gen Intern Med. 2010;25(12):1309–14. https://doi.org/10.1007/s11606-010-1471-1 .
Article PubMed PubMed Central Google Scholar
Monrouxe LV, Rees CE, Dennis I, Wells SE. Professionalism dilemmas, moral distress and the healthcare student: insights from two online UK-wide questionnaire studies. BMJ Open. 2015;5(5):e007518. https://doi.org/10.1136/bmjopen-2014-007518 .
Feudtner C, Christakis DA, Christakis NA. Do clinical clerks suffer ethical erosion? Students’ perceptions of their ethical environment and personal development. Acad Med. 1994;69(8):670–9. https://doi.org/10.1097/00001888-199408000-00017 .
Osswald S, Greitemeyer T, Fischer P, Frey D. What is moral courage? Definition, explication, and classification of a complex construct. In: Pury LS, Lopez SJ, editors. The psychology of courage: Modern Research on an ancient Virtue. American Psychological Association; 2010. pp. 149–64. https://doi.org/10.1037/12168-008 .
Murray CJS. Moral courage in healthcare: acting ethically even in the presence of risk. Online J Issues Nurs. 2010;15(3):Manuscript2. https://doi.org/10.3912/OJIN.Vol15No03Man02 .
Article Google Scholar
Kidder RM, Bracy M. Moral Courage A White Paper .; 2001.
Lachman VD. Ethical challenges in Health Care: developing your Moral Compass. Springer Publishing Company; 2009. http://ovidsp.ovid.com/ovidweb.cgi?T=JS . &PAGE=reference&D=psyc6&NEWS=N&AN=2009-11697-000.
Lachman VD. Moral courage: a virtue in need of development? Medsurg Nurs. 2007;16(2):131–3. http://www.embase.com/search/results?subaction=viewrecord&from=export&id=L47004201 .
PubMed Google Scholar
Doyle P, Vandenkerkhof EG, Edge DS, Ginsburg L, Goldstein DH. Self-reported patient safety competence among Canadian medical students and postgraduate trainees: a cross-sectional survey. BMJ Qual Saf. 2015;24:135–41. https://doi.org/10.1136/bmjqs .
Martinez W, Bell SK, Etchegaray JM, Lehmann LS. Measuring moral courage for interns and residents: scale development and initial psychometrics. Acad Med. 2016;91(10):1431–8. https://doi.org/10.1097/ACM.0000000000001288 .
Gutgeld-Dror M, Laor N, Karnieli-Miller O. Assertiveness in physicians’ interpersonal professional encounters: a scoping review. Med Educ Published Online 2023:1–13. https://doi.org/10.1111/medu.15222 .
Madigosky WS, Headrick LA, Nelson K, Cox KR, Anderson T. Changing and sustaining medical students’ knowledge, skills, and attitudes about patient safety and medical fallibility. Acad Med. 2006;81(1):94–101.
Weinzimmer S, Miller SM, Zimmerman JL, Hooker J, Isidro S, Bruce CR. Critical care nurses’ moral distress in end-of-life decision making. J Nurs Educ Pract. 2014;4(6):6–12. https://doi.org/10.5430/jnep.v4n6p6 .
Savel RH, Munro CL. Moral distress, moral courage. Am J Crit Care. 2015;24(4):276–8. https://doi.org/10.1037/a0022283 .
Elpern EH, Covert B, Kleinpell R. Moral distress of staff nurses in a medical intensive care unit. Am J Crit Care. 2005;14(6):523–30. https://doi.org/10.4037/ajcc2005.14.6.523 .
Camp M, Sadler J. Moral distress in medical student reflective writing. AJOB Empir Bioeth. 2019;10(1):70–8. https://doi.org/10.1080/23294515.2019.1570385 .
Perni S, Pollack LR, Gonzalez WC, Dzeng E, Baldwin MR. Moral distress and burnout in caring for older adults during medical school training. BMC Med Educ. 2020;20(1):1–10. https://doi.org/10.1186/s12909-020-1980-5 .
Bandura A. Self-Efficacy: the Exercise of Control. W.H. Freeman; 1997.
Artino AR. Academic self-efficacy: from educational theory to instructional practice. Perspect Med Educ. 2012;1(2):76–85. https://doi.org/10.1007/s40037-012-0012-5 .
May DR, Luth MT, Schwoerer CE. The influence of business ethics education on moral efficacy, moral meaningfulness, and moral courage: a quasi-experimental study. J Bus Ethics. 2014;124(1):67–80. https://doi.org/10.1007/s10551-013-1860-6 .
Hannah ST, Avolio BJ. Moral potency: building the capacity for character-based leadership. Consult Psychol J. 2010;62(4):291–310. https://doi.org/10.1037/a0022283 .
Schaubroeck JM, Hannah ST, Avolio BJ, et al. Embedding ethical leadership within and across organization levels. Acad Manag J. 2012;55(5):1053–78. https://doi.org/10.5465/amj.2011.0064 .
Hannah ST, Avolio BJ, May DR. Moral maturation and moral conation: a capacity approach to explaining moral thought and action. Acad Manag Rev. 2011;36(4):663–85. https://doi.org/10.5465/amr.2010.0128 .
Sekerka LE, Bagozzi RP. Moral courage in the workplace: moving to and from the desire and decision to act. Bus Ethics Eur Rev. 2007;16(2):132–49.
Lazarus RS. Stress and emotion: a New Synthesis. Springer Publishing Company; 1999.
Backović DV, Živojinović JI, Maksimović J, Maksimović M. Gender differences in academic stress and burnout among medical students in final years of education. Psychiatr Danub. 2012;24(2):175–81.
Hill MR, Goicochea S, Merlo LJ. In their own words: stressors facing medical students in the millennial generation. Med Educ Online. 2018;23(1):1530558. https://doi.org/10.1080/10872981.2018.1530558 .
Neumann M, Edelhäuser F, Tauschel D, et al. Empathy decline and its reasons: a systematic review of studies with medical students and residents. Acad Med. 2011;86(8):996–1009. https://doi.org/10.1097/ACM.0b013e318221e615 .
Dyrbye LN, Thomas MR, Shanafelt TD. Medical student distress: causes, consequences, and proposed solutions. Mayo Clin Proc. 2005;80(12):1613–22. https://doi.org/10.4065/80.12.1613 .
Dyrbye LN, Thomas MR, Power DV, et al. Burnout and serious thoughts of dropping out of medical school: a multi-institutional study. Acad Med. 2010;85(1):94–102. https://doi.org/10.1097/ACM.0b013e3181c46aad .
Bresó E, Schaufeli WB, Salanova M. Can a self-efficacy-based intervention decrease burnout, increase engagement, and enhance performance? A quasi-experimental study. Published online 2010. https://doi.org/10.1007/s10734-010-9334-6 .
Maslach C, Leiter MP. Understanding the burnout experience: recent research and its implications for psychiatry. World Psychiatry. 2016;15(2):103–11. https://doi.org/10.1002/wps.20311 .
Galán F, Sanmartín A, Polo J, Giner L. Burnout risk in medical students in Spain using the Maslach Burnout Inventory-Student Survey. Int Arch Occup Environ Health. 2011;84(4):453–9. https://doi.org/10.1007/s00420-011-0623-x .
Schaufeli WB, Martinez IM, Pinto AM, Salanova M, Bakker AB. Burnout and engagement in university students: a cross-national study. J Cross Cult Psychol. 2002;33(5):464–81. https://doi.org/10.1177/0022022102033005003 .
Dyrbye LN, Shanafelt T. A narrative review on burnout experienced by medical students and residents. Med Educ. 2016;50(1):132–49. https://doi.org/10.1111/medu.12927 .
Shin HS, Park H, Lee YM. The relationship between medical students’ empathy and burnout levels by gender and study years. Patient Educ Couns. 2022;105(2):432–9. https://doi.org/10.1016/j.pec.2021.05.036 .
Dyrbye LN, Massie FSJ, Eacker A, et al. Relationship between burnout and professional conduct and attitudes among US medical students. JAMA - J Am Med Assoc. 2010;304(11):1173–80. https://doi.org/10.1001/jama.2010.1318 .
Taormina RJ, Law CM. Approaches to preventing burnout: the effects of personal stress management and organizational socialization. J Nurs Manag. 2000;8(2):89–99. https://doi.org/10.1046/j.1365-2834.2000.00156.x .
Locati F, De Carli P, Tarasconi E, Lang M, Parolin L. Beyond the mask of deference: exploring the relationship between ruptures and transference in a single-case study. Res Psychother Psychopathol Process Outcome. 2016;19(2):89–101. https://doi.org/10.4081/ripppo.2016.212 .
Koeske GF, Daimon R. Student burnout as a mediator of the stress-outcome relationship. Res High Educ. 1991;32:415–431.
Gilbey P, Moffat M, Sharabi-Nov A, et al. Burnout in Israeli medical students: a national survey. BMC Med Educ. 2023;23:55–66. https://doi.org/10.1186/s12909-023-04037-2 .
Konings KJP, Gastmans C, Numminen OH, et al. Measuring nurses’ moral courage: an explorative study. Nurs Ethics. 2022;29(1):114–30. https://doi.org/10.1177/09697330211003211 .
Neufeld-Kroszynski G. Medical students’ professional identity formation: a prospective and retrospective study of students’ perspectives. Published online 2021.
Hauhio N, Leino-Kilpi H, Katajisto J, Numminen O. Nurses’ self-assessed moral courage and related socio-demographic factors. https://doi.org/10.1177/0969733021999763 .
Egbert N, Reed PR. Self-efficacy. In: Kim DK, Dearing JW, editors. Health Communication Research Measures. Peter Lang Publishing; 2016. pp. 203–12.
Farajev N, Michael K, Karnieli-Miller, O. The associations between environmental professionalism, empathy attitudes, communication self-efficacy, and moral courage efficacy among medical students. Unpublished.
Ben-Zur H, Michael K. Positivity and growth following stressful life events: associations with psychosocial, health, and economic resources. Int J Stress Manag. 2020;27(2):126–34. https://doi.org/10.1037/str0000142 .
Keech JJ, Hagger MS, O’Callaghan FV, Hamilton K. The influence of university students’ stress mindsets on health and performance outcomes. Ann Behav Med. 2018;52(12):1046–59. https://doi.org/10.1093/abm/kay008 .
Obregon M, Luo J, Shelton J, Blevins T, MacDowell M. Assessment of burnout in medical students using the Maslach Burnout Inventory-Student Survey: a cross-sectional data analysis. BMC Med Educ. 2020;20(1). https://doi.org/10.1186/s12909-020-02274-3 .
Erschens R, Keifenheim KE, Herrmann-Werner A, et al. Professional burnout among medical students: systematic literature review and meta-analysis. Med Teach. 2019;41(2):172–83. https://doi.org/10.1080/0142159X.2018.1457213 .
Hayes AF. Introduction to Mediation, Moderation, and conditional process analysis: a regression-based Approach. 2nd ed. Guilford; 2018.
Cohen J. Statistical Power Analysis for the behavioral sciences. Routledge; 2013. https://doi.org/10.4324/9780203771587 .
Martinez W, Lehmann LS, Thomas EJ, et al. Speaking up about traditional and professionalism-related patient safety threats: a national survey of interns and residents. BMJ Qual Saf. 2017;26(11):869–80. https://doi.org/10.1136/bmjqs-2016-006284 .
Kesselheim JC, Shelburne JT, Bell SK, et al. Pediatric trainees’ speaking up about unprofessional behavior and traditional patient safety threats. Acad Pediatr. 2021;21(2):352–7.
Edmondson AC. The Fearless Organization: creating Psychological Safety in the Workplace for Learning, Innovation, and growth. Wiley; 2018.
Plews-Ogan M, May N, Owens J, Ardelt M, Shapiro J, Bell SK. Wisdom in medicine: what helps physicians after a medical error? Acad Med. 2016;91(2):233–41. https://doi.org/10.1097/ACM.0000000000000886 .
Karnieli-Miller O. Reflective practice in the teaching of communication skills. Patient Educ Couns. 2020;103(10):2166–72. https://doi.org/10.1016/j.pec.2020.06.021 .
Klasen JM, Driessen E, Teunissen PW, Lingard LA. Whatever you cut, I can fix it: clinical supervisors’ interview accounts of allowing trainee failure while guarding patient safety. BMJ Qual Saf. 2020;29(9):727–34. https://doi.org/10.1136/BMJQS-2019-009808 .
Lyndon A, Sexton JB, Simpson KR, Rosenstein A, Lee KA, Wachter RM. Predictors of likelihood of speaking up about safety concerns in labour and delivery. BMJ Qual Saf. 2012;21(9):791–9. https://doi.org/10.1136/bmjqs-2010-050211 .
Ben-zur H. Burnout, social support, and coping at work among social workers, psychologists, and nurses: the role of challenge/control appraisals. Soc Work Health Care. 2007;45(4):63–82. https://doi.org/10.1300/J010v45n04 .
Haghighi M, Gerber M. Does mental toughness buffer the relationship between perceived stress, depression, burnout, anxiety, and sleep? Int J Stress Manag. 2019;26(3):297–305. https://doi.org/10.1037/str0000106 .
Shanafelt TD, Balch CM, Bechamps G, et al. Burnout and medical errors among American surgeons. Ann Surg. 2010;251(6):995–1000. https://doi.org/10.1097/SLA.0b013e3181bfdab3 .
Fischer MA, Mazor KM, Baril J, Alper E, DeMarco D, Pugnaire M. Learning from mistakes factors that influence how students and residents learn from medical errors. J Gen Intern Med. 2006;21(5):419–23.
Hojat M, Vergare MJ, Maxwell K, et al. The devil is in the third year: a longitudinal study of erosion of empathy in medical school. Acad Med. 2009;84(9):1182–91. https://doi.org/10.1097/ACM.0b013e3181b17e55 .
Chen D, Lew R, Hershman W, Orlander J. A cross-sectional measurement of medical student empathy. J Gen Intern Med. 2007;22(10):1434–8. https://doi.org/10.1007/s11606-007-0298-x .
Spencer J. Decline in empathy in medical education: how can we stop the rot? Med Educ. 2004;38(9):916–8. https://doi.org/10.1111/j.1365-2929.2004.01965.x .
Karnieli-Miller O. Caring for the health and well-being of our learners in medicine as critical actions toward high-quality care. Isr J Health Policy Res. 2022;11(1):10. https://doi.org/10.1186/S13584-022-00517-W .
Dyrbye LN, Thomas MR, Harper W, et al. The learning environment and medical student burnout: a multicentre study. Med Educ. 2009;43(3):274–82. https://doi.org/10.1111/j.1365-2923.2008.03282.x .
Download references
Acknowledgements
The authors wish to thank Dr. Lior Rozental in helping in recruiting students to the study. This study was done as part of Orit Karnieli-Miller’s Endowed chair of the Dr. Sol Amsterdam, Dr. David P. Schumann in Medical Education, Tel Aviv University. This study is written in the blessed memory of Oshrit Bar-El, devoted to enhancing Moral Courage.
The manuscript was partially supported by a grant by the by the Israel Science Foundation (grant no. 1599/21).
Author information
Galit Neufeld-Kroszynski and Keren Michael contributed equally to this work.
Authors and Affiliations
Department of Medical Education, Faculty of Medical & Health Sciences, Tel Aviv University, Tel Aviv, 69778, Israel
Galit Neufeld-Kroszynski & Orit Karnieli-Miller
Department of Human Services, Max Stern Yezreel Valley College, Yezreel Valley, Israel
Keren Michael
You can also search for this author in PubMed Google Scholar
Contributions
GNK: conception and design, interpretation of data, drafting and revision of the manuscript, and final approval of the version to be published; KM: analysis and interpretation of data, drafting and revision of the manuscript, and final approval of the version to be published; OKM: conception and design, interpretation of data, drafting and revision of the manuscript, and final approval of the version to be published.
Corresponding author
Correspondence to Orit Karnieli-Miller .
Ethics declarations
Ethics approval and consent to participate.
This study was conducted in accordance with the principles outlined in the Declaration of Helsinki and received ethical approval by the Ethics Committee of Tel-Aviv University on 31/10/2019. Informed written consent was obtained from all participants before their participation in this study.
Consent for publication
Not applicable.
Previous presentations
Study findings were presented at the Academy for Professionalism in Healthcare Conference, June 2nd, 2022, virtual; and the 7th International Conference on Public Health, August 8th, 2021, virtual.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Neufeld-Kroszynski, G., Michael, K. & Karnieli-Miller, O. Associations between medical students’ stress, academic burnout and moral courage efficacy. BMC Psychol 12 , 296 (2024). https://doi.org/10.1186/s40359-024-01787-6
Download citation
Received : 03 December 2023
Accepted : 13 May 2024
Published : 27 May 2024
DOI : https://doi.org/10.1186/s40359-024-01787-6
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Moral courage
- Self-efficacy
- Medical students
- Professionalism
- Patient safety
BMC Psychology
ISSN: 2050-7283
- General enquiries: [email protected]

Introversion
Introverts aren't who you think they are, research uncovers the realities of introverts in the workplace..
Posted May 29, 2024 | Reviewed by Monica Vilhauer
- What Is Introversion?
- Find a therapist near me

Introverts have long been misunderstood, caricatured, and stereotyped in our extrovert-centric society. From the shy, socially awkward loner to the emotionally fragile genius, these one-dimensional depictions fail to capture the nuanced reality of what it means to be an introvert. Let's start by debunking the most pervasive myth: that introverts are inherently socially anxious and uncomfortable around others.
While it's true that many introverts prefer smaller social settings and tend to be more reserved, this doesn't mean they are inherently socially anxious or uncomfortable. In fact, research has demonstrated that introverts can be just as socially skilled as extroverts. They simply express and recharge their social batteries differently (McCord & Joseph, 2020).
However, it is also important to note that there is a correlation between introversion and social anxiety . Studies have found that introverted individuals are more likely to experience social anxiety compared to their extroverted counterparts (Cain, 2012; Noya & Vernon, 2019). The quiet, reflective nature of introverts can make them more prone to self-consciousness, fear of negative evaluation, and avoidance of social situations (Alexandru, 2021).

While the connection between introversion and social anxiety is well-documented, it's crucial to recognize that this relationship is not absolute or universal. The interplay between introversion, extroversion , and social anxiety is complex and highly individualized. It's important to avoid making broad generalizations and to approach each person with an open and understanding mindset.
While there is some correlation between introversion and social anxiety, many introverts are perfectly comfortable and confident in social settings, while some extroverts may struggle with social anxiety (Cline, 2021). Introversion and social anxiety exist on separate spectrums, and an individual can exhibit characteristics of both. Understanding this more nuanced dynamic is crucial to avoiding overgeneralized assumptions about the relationship between introversion and social discomfort.

Introverts also often face biases and misunderstandings in the workplace, where their quieter, more reflective nature may be perceived negatively compared to extroverted colleagues (McCord & Joseph, 2020). However, workplace diversity, including diversity of personality types, can lead to increased productivity , creativity , and problem-solving. Understanding and accommodating introverts is important for creating inclusive work environments that recognize the value they bring to the table.
Many organizations still tend to favor extroverted traits, such as assertiveness , high energy, and a propensity for public speaking . This can create an environment where introverts feel undervalued or overlooked. Yet there can be immense benefits when organizations actively embrace and accommodate introverted employees. By recognizing the unique strengths of introverts, such as their attention to detail, analytical thinking, and ability to work independently, companies can foster a more inclusive and productive work culture. This, in turn, can lead to increased innovation, problem-solving, and overall organizational success.

Another common misconception is that introverts are passive, submissive, and lacking in confidence . On the contrary, introverts can be highly assertive, ambitious, and self-assured. The key difference is that they tend to be more selective about when and how they express these qualities. Introverts often excel in roles that allow them to work independently and leverage their strengths in analysis, problem-solving, and deep thinking.
The stereotype of the introverted hermit is another common misconception. While some introverts may indeed prefer a more reclusive lifestyle, this is not true of all introverts. Many introverts enjoy social interaction and engagement, but in smaller, more intimate settings. They may simply have a lower need for external stimulation and a preference for directing their energy inward. Assuming all introverts are hermit-like and socially isolated does not reflect the diverse ways introverts contribute to society.

Research also suggests that many introverts may possess a heightened sensory processing sensitivity , which can contribute to their reflective nature and tendency towards deep processing, empathy, and creativity (Aron & Aron, 1997; Jagiellowicz et al., 2011). This, combined with introversion, may lead some introverts to demonstrate exceptional intellectual abilities. Yet we must not overgeneralize. Others may simply prefer to channel their sensitivities into more introspective or niche pursuits (Aron, 2013).
For example, introverted writers' ability to delve deeply into complex topics, to synthesize information in unique ways, and to convey nuanced perspectives can be truly remarkable. I've found that my own introverted tendencies, such as a preference for solitary reflection and a keen eye for detail, have been invaluable assets. It's important to recognize that the introvert's strengths and challenges are not mutually exclusive. By creating work environments and professional development opportunities that cater to the unique needs of introverted individuals, we can unlock their full potential and foster a more diverse, inclusive, and innovative professional landscape.

In reality, introverts are a diverse group, united not by a single set of characteristics but by a preference for introspection, a lower need for external stimulation, and a tendency to direct their energy inward. Recognizing the nuanced interplay between introversion, sensitivity, confidence, social presence, and intellectual giftedness is crucial to avoid conflating distinctly different characteristics, to avoid reductive stereotypes, and to appreciate the full range of introverted personalities and contributions.
Alexandru, R. (2021, September 13). How I've learned to overcome my social anxiety as an introvert. Introvert, Dear. https://introvertdear.com/news/how-ive-learned-to-overcome-my-social-anxiety-as-an-introvert/
Aron, E. N. (2013). Psychotherapy and the highly sensitive person: Improving outcomes for that minority of people who are the majority of clients . Routledge.
Aron, E. N., & Aron, A. (1997). Sensory-processing sensitivity and its relation to introversion and emotionality. Journal of Personality and Social Psychology, 73 (2), 345.
Cain, S. (2012). Quiet: The power of introverts in a world that can't stop talking . Crown.
Cline, R. (2021, June 9). More than introverted: A look at social anxiety disorder. Johnstown Heights Behavioral Health. https://johnstownheights.com/blog/social-anxiety-disorder/
Jagiellowicz, J., Xu, X., Aron, A., Aron, E., Cao, G., Feng, T., & Weng, X. (2011). The trait of sensory processing sensitivity and neural responses to changes in visual scenes. Social Cognitive and Affective Neuroscience, 6 (1), 38-47.
McCord, M. (2020). Expert alert: personality bias . University of Central Florida (Dissertation).
McCord, M. A., & Joseph, D. L. (2020). A framework of negative responses to introversion at work. Personality and Individual Differences, 161 , 109944.
Noya, C., & Vernon, L. (2019). Where are all the introverts hiding? An analysis of introversion in research. Florida Atlantic University Undergraduate Research Journal .

Blake Griffin Edwards is a licensed marriage and family therapist in Washington State.
- Find a Therapist
- Find a Treatment Center
- Find a Psychiatrist
- Find a Support Group
- Find Online Therapy
- United States
- Brooklyn, NY
- Chicago, IL
- Houston, TX
- Los Angeles, CA
- New York, NY
- Portland, OR
- San Diego, CA
- San Francisco, CA
- Seattle, WA
- Washington, DC
- Asperger's
- Bipolar Disorder
- Chronic Pain
- Eating Disorders
- Passive Aggression
- Personality
- Goal Setting
- Positive Psychology
- Stopping Smoking
- Low Sexual Desire
- Relationships
- Child Development
- Self Tests NEW
- Therapy Center
- Diagnosis Dictionary
- Types of Therapy

At any moment, someone’s aggravating behavior or our own bad luck can set us off on an emotional spiral that threatens to derail our entire day. Here’s how we can face our triggers with less reactivity so that we can get on with our lives.
- Emotional Intelligence
- Gaslighting
- Affective Forecasting
- Neuroscience
Women’s emotional roller coasters during pregnancy as a consequence of infertility: a qualitative phenomenological study
- Open access
- Published: 30 May 2024
Cite this article
You have full access to this open access article

- Parisa Hadavibavili ORCID: orcid.org/0000-0002-0135-9651 1 , 2 ,
- Yasemin Hamlaci Başkaya ORCID: orcid.org/0000-0002-1533-8667 1 ,
- Gamze Bayazi̇t ORCID: orcid.org/0009-0004-0816-3960 3 &
- Arif Serhan Cevrioğlu ORCID: orcid.org/0000-0002-3810-6519 4
Women experiencing infertility tend to experience distinct emotions during pregnancy following infertility. Individuals in this population often struggle with psychological and social challenges during pregnancy. This qualitative phenomenological study determines how infertility experiences affect mothers’ mental well-being during pregnancy as well as their experiences and emotions after becoming pregnant. A face-to-face, in-depth interview with 15 women with infertility was conducted between November 2022 and May 2023. The study adhered to ethical guidelines, with informed written consent obtained prior to interviews and voice recordings. The COREQ checklist is applied to follow the EQUATOR guidelines for reporting research and the data were coded using MAXQDA.20 software. A thematic analysis revealed four main themes and 15 codes. Main themes included “Over Emotional Burden,” “Overprotection,” “Overthinking,” and “Social Activity Changes.” Pregnancy after infertility is a unique and emotionally charged experience for women, encompassing a spectrum of feelings that can be difficult to express. The importance of caring for these women and receiving support from their partners, families, and healthcare providers should not be overstated. Healthcare providers should be aware of these emotional challenges so they can provide better support and counselling to improve women’s overall pregnancy experience. It is believed that empathetic communication and tailored support can significantly improve the psychological well-being of this population. Psychologists, psychiatrists, and midwives should also be more attentive to mothers’ emotional challenges and integrate comprehensive emotional support and provide coping mechanisms in perinatal care programs.
Avoid common mistakes on your manuscript.
Introduction
Infertility has been a prevalent health problem in recent generations around the world (Fainberg & Kashanian, 2019 ). Couples with infertility generally struggle with socioeconomic, psychological, physical, and cultural consequences of this condition (Kianfar et al., 2023 ). Based on statistical analysis, 10–15% of the world’s population experience infertility (Bakhtiyar et al., 2019 ). This condition is considered a severe disability and ranks fifth in severity. Considering the causes and duration of infertility, it may significantly affect a couple’s psychological well-being (Borumandnia et al., 2022 ). According to the literature, nearly half of women seeking infertility treatments struggle with disorders aligned with posttraumatic stress disorder. Researchers have also noted that infertility concerns impair coping mechanisms in individuals which result in considerable stress and anxiety among infertile couples (Renzi et al., 2023b ). Nowadays, infertility procedure is often suggested as a double-edged sword that can cause considerable emotional distress, social stigma, and financial concerns in couples (Taebi et al., 2021 ). According to the literature, infertility treatment processes mainly affect women more than men, and infertile women are considered deficient women in some cultures and societies (Olma & Bir, 2018 ; Yao et al., 2018 ). According to a literature, the better quality of life of couples is strongly associated with more success rates in infertility treatments. It also appears that decreased psychological symptoms as well as enhanced emotion regulation abilities may contribute to improved success rates in treatment centers (Renzi et al., 2023a ). Pregnancy after infertility can be a unique and emotionally inspiring experience for infertile couples. However, even after achieving a successful pregnancy, women who have experienced infertility may struggle with psychological and social challenges during pregnancy and after childbirth (Crespo & Bestard, 2016 ). Studies have shown that women who get pregnant after infertility experience some levels of stress and anxiety regarding their fetal and maternal outcomes. Their pregnancy may also result in confusing feelings between excitement and grief (Maehara et al., 2022 ). In the first trimester, the infertile woman often struggles with fears of pregnancy loss, possible fetal abnormalities, and adapting to significant physical changes (Dornelles et al., 2016 ). During the third trimester, anxiety and stress can be caused by the fear of pregnancy complications and preterm labor. Furthermore, infertile women may face challenges in selecting a safe delivery method (Huang et al., 2019 ). According to the literature, there is considerable research on mental health before and after pregnancy in infertile couples (McMahon et al., 2011 ).
In this qualitative study, we aim to investigate how infertility experiences affect mothers’ mental well-being during pregnancy as well as their perspectives and feelings after becoming pregnant.
Study design
This research is a qualitative study with a Heideggerian, hermeneutic phenomenological approach. This study was framed by Heideggerian phenomenology, and its Heideggerian influence extends throughout the entire study. In this approach, personal experience and the interpretation of events is emphasized as significant components of understanding human cognition and behavior (Heidegger, 1996 ). As a method of studying human experience, hermeneutic phenomenology has the unique potential of being able to examine complex phenomena in depth. Methodologies like this are well suited for representing the depth and complexity of individual experiences, providing detailed context to understand the complex interaction of factors influencing individuals’ life experiences (Plager, 1994 ). All in all, this study uses hermeneutic phenomenology because of its suitability to explore human experiences of complex phenomena. This method involves analyzing and reflecting on participants’ life experiences in order to gain a deeper understanding of their subjective perceptions, interpretations, and understandings (Annells, 1996 ).
In this study, the COREQ (Consolidated Criteria for Reporting Qualitative Research) checklist is applied to follow the EQUATOR guidelines for reporting research. This is a 32-item checklist for reporting interviews and focus groups systematically. The checklist provides researchers with a framework for reporting key study design, data collection, and analysis aspects, fostering clarity and reproducibility. The criteria also cover various aspects of qualitative research, including data collection methods, participant recruitment, and analysis processes. Furthermore, following established reporting guidelines facilitates peer review by providing standardized criteria for assessing the validity and quality of qualitative research. In reporting qualitative research, the COREQ checklist emphasizes ethical considerations, such as ensuring participant privacy and providing a clear ethical rationale. Ultimately, adopting EQUATOR guidelines further improves qualitative research reporting standards, as well as improving qualitative research practices more broadly (Hope & King, 2022 ).
Participant selection
This study included participants who got pregnant after being diagnosed with infertility and agreed to participate in interviews. Researchers recruited participants from pregnant women who had experienced infertility and attended the Sakarya Training and Research Hospital’s perinatal clinic between November 2022 and May 2023. The interviewer, who was a registered midwife, obtained patient information from the hospital’s electronic medical records system. In order to recruit participants, A phone call was initially made to inform and gain permission from the participants, and then appointments were scheduled at convenient times and dates using social media and messenger applications such as WhatsApp and Telegram. Interviews took place in a quiet consulting room at the hospital, allowing open and honest communication. Interviews were conducted without the presence of other participants or researchers in order to preserve privacy and confidentiality. In this way, participants were able to share their experiences without concern for their privacy. Participants under 18 years of age and participants who withdraw from the study during the interview are excluded from the study. The registered midwife contacted 20 mothers initially and invited them to participate in the study. One mother declined participation due to her husband’s objection. Another mother cited privacy concerns as the reason for her non-participation. A third mother commented that her pregnancy period was challenging and she wished to forget it. The fourth mother moved to a different hospital and the final mother relocated to a different city in the second trimester. In this study, a comprehensive amount of data was collected and data saturation was deemed sufficient by the authors. A total of 15 mothers participated in the study. The interviews began with open-ended questions such as “How would you describe yourself before and after pregnancy?”, “How has the diagnosis of infertility affected your perspective on pregnancy?”, “How do you evaluate your relationship with your partner after becoming pregnant?”.
Pregnant women who experienced infertility and attended Sakarya Training and Research Hospital’s perinatal clinic between November 2022 and May 2023 were participants in the study. The interviews were conducted without the presence of any other participants or researchers.
Data collection
An in-depth interview was conducted with participants using a sociodemographic form, semi-structured interview form, and a TSCO audio recording device (Model no. TR906, Made in China). A written consent was obtained from participants before the interview and recording. The demographic characteristics of the participants were collected from the patients face-to-face in a quiet consulting room at the hospital. The interview took place during a period when patients were visiting the hospital for routine pregnancy check-ups. We decided on this for patient convenience and time efficiency. Audio recording permission was also obtained before the interviews began from the participants. In order to eliminate hesitation about the study and to encourage the interviewees to answer the questions honestly, the researcher explained to each interviewee that they would be assigned a number based on their order in the interview. After the interview, notes were taken while listening to the recordings. After obtaining written consent, completing sociodemographic forms, and scheduling face-to-face sessions, approximately 25–30-minute interviews were conducted. In qualitative research, the sample size is determined by the concept of data saturation. Data saturation occurs when no new information or themes emerge from the data, indicating that the sample size is adequate (Francis et al., 2010 ). According to our study, themes and insights recurred as the interviews progressed, indicating that the desired themes were thoroughly explored. Data saturation was considered sufficient in the study as all desired themes were adequately explored, and a comprehensive amount of data was collected.
Data analysis
In the study, two researchers contributed as data coders. The data was coded through thematic analysis to form related themes based on the document’s content. In qualitative data, themes can be identified, analyzed, and interpreted through thematic analysis. It emphasizes the active role of the researcher in the process of coding and theme development. Researchers organize and report their analytical observations using themes and psychiatrists are using these versions due to their greater flexibility (Clarke & Braun, 2017 ). Ultimately, 15 codes were determined along with four themes. The corresponding author (Ph.D. candidate) and second researcher (Ph.D.), who were experienced in analyzing qualitative data, classified and identified codes and themes through the study content. The first three authors of this study were female, and the last author was male. All of the authors have considerable experience in infertility and pregnancy and a keen interest in filling a gap in infertile women’s mental health during pregnancy. In the study, the themes were derived from the data rather than being predetermined, and through researchers’ analysis of participants’ responses and experiences, themes emerged initially. A MAXQDA Analytics Pro 2020 program was used to manage the data in this study.
Rigor and trustworthiness
The data’s trustworthiness was assessed based on the suggestions of Guba and Lincoln (Cypress, 2017 ; Guba & Lincoln, 1981 ). A trustworthiness concept can be categorized into credibility and dependability. The concept of credibility corresponds roughly to the concept of internal validity as defined by positive ideologues, while that of dependability corresponds to the concept of reliability. In terms of reliability, transferability, which is external validity, and confirmability, which relies mostly on presentation (Gunawan, 2015 ). The phenomenological approach was used in our study as a qualitative research design to verify the study’s credibility (Rodriguez & Smith, 2018 ). The last researcher, who was an obstetrics and gynecologist and specialized in infertility, reviewed the themes and verified the process’ accuracy. The concept of transferability is traditionally associated with the application or generalization of findings to a wide range of situations. However, qualitative research emphasizes the richness and depth of insights rather than strictly transferring them into other contexts. By examining individuals’ experiences within a specific context, qualitative research illuminates the intricacies and mechanisms underlying a phenomenon (Leung, 2015 ). Through member checking we allow participants to review and verify the findings as part of the research process.
Furthermore, we ensured that the findings were transferable and considered different viewpoints by incorporating multiple perspectives. In order to enhance the dependability of our data and ensure that our findings are accurate and reliable, we use an audit trail. In the audit trail approach, we tried to keep a detailed record of the research process, from decisions to data collection and analysis. A skilled researcher enhances the dependability of data through qualitative research principles, so we provided education courses with certificates for authors with little or no experience in qualitative studies. In order to enhance data confirmability, peer review strategies were used to ensure that the findings accurately reflect the participants’ perspectives and experiences, as well as the researcher’s interpretation, and enabled us to examine the data, analysis, and interpretation critically, ensuring the findings were trustworthy.
Ethical consideration
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Sakarya University on 05.10.2022 by the number E-71522473-050.01.04-171377-258. Informed written consent was obtained from participants before the interview and recording the voice, ensuring that they understood the study’s purpose, procedures, risks, benefits, and confidentiality. All participants were informed that they had the right to withdraw from the research at any time without consequence.
The demographic analysis revealed that the participants were between the ages of 22 and 38, with a mean age of 30.33 ± 4.19. There were 15 women; three graduated from universities, five from high schools, three from secondary schools, and four from primary schools. Eleven women were housewives, three were civil servants, and the remaining one was a family physician. The median duration of infertility was 3.73 years, ranging from 1 to 10 years. All participants except four mentioned female factors as a cause of infertility. One participant had both male and female factors. Two participants mentioned a malefactor, and another mentioned unexplained reasons. Regarding infertility treatment, seven participants got pregnant through IUI, and eight got pregnant through IVF. Some demographic characteristics of the participants are shown in Table 1 .
Mothers’ perspectives on emotional challenges during pregnancy after infertility revealed four themes and 15 codes: (1) Over Emotional Burden, (2) Overprotection, (3) Overthinking, (4) Social Activity Changes. Figure 1 shows the coding tree.

Coding tree of the mothers’ psychological experiences in pregnancy after infertility
Theme 1: Over Emotional Burden
An infertility diagnosis can continue to impact the emotional well-being of the couple after pregnancy, making the perinatal period even more challenging. Pregnancy after experiencing infertility can be a journey filled with a complex combination of emotions, almost like a roller coaster ride of emotions. In the present study, pregnant women with a history of infertility reported intense emotional burdens, including Emotional Roller Coaster, Fear, Anxiety, Hopelessness, and Regret.
Emotional Roller Coaster
The roller coaster represents mothers’ unpredictable emotional ups and downs. Consequently, they feel overwhelmed and incapable of coping with their emotions. The emotional roller coaster women experience post-infertility is complex. An initial feeling of happiness and excitement can quickly turn into anxiety and uncertainty after a successful pregnancy.
“I am moving through some ups and downs emotionally. Actually, I express my emotional state to my husband a little bit, but he manages me well, thanks to him. Sometimes, I cry for no reason; sometimes, I get angry. Things happen momentarily.” (P1, female factor, 1-year infertility)
“Pregnancy was both a dream and a nightmare for me.” (P4, female factor, 4-years infertility)
Fear / Anxiety
It is common and understandable for women to feel fear and anxiety during pregnancy, especially following an infertility diagnosis. There may be a fear of miscarriage, preterm birth, or other complications that women experience during pregnancy, intensified by the memories of previous struggles. The women who participated in the current study stated that they often experience disappointment and uncertainty during pregnancy.
“In the early stages of my pregnancy, I was filled with fears and worries. I was afraid of miscarriage first, then … ” (P13, female factor, 8-years infertility)
“During the early stages of my pregnancy, I was very anxious. It was a fear in my mind to have a fake pregnancy.” (P3, female factor, 1-year infertility)
Hopelessness
Hopelessness after long infertility treatment is a complex and reasonable emotional response in infertile couples. Many couples struggle with infertility for months or even years with repeated medical interventions and emotional challenges.
“I always thought pregnancy was impossible and unachievable for a long time.” (P13, female factor, 8-years infertility)
“There were many difficult experiences for me during infertility treatments, especially waiting in infertility clinics, which were emotionally draining for me. There were pregnant patients waiting in the reception hall. When I saw them, I thought it would never happen to me to be a mother.” (P9, female factor, 6-years infertility)
The experience of pregnancy may cause regret after years of infertility struggle. There are many factors that can contribute to regret, and it is a deeply personal emotion. It may result from a sense of lost control over one’s reproductive journey or from the impact it has had on one’s family and relationships.
“The first few months, I was constantly suffering from illness. I thought I would never recover, and I just wanted to deliver as soon as possible. Even I asked myself, what did we do? I was certain it would not pass. My health isn’t that bad, but it was quite bad.” (P2, female factor, 1-year infertility)
Theme 2: Overprotection
Overprotection is a natural reaction to the possibility of losing something that was so highly desired and hard-earned. When a mother experiences infertility, balancing motherhood and safeguarding pregnancy could be challenging and may lead to overprotection during pregnancy. In this study, this phenomenon is displayed in various aspects, including impacting changes in sexual life, delivery mode preferences, disruptions in social life, and an insistence on maintaining constant check-ups. It is imperative to recognize and address these feelings by healthcare providers to ensure a successful transition to pregnancy and a healthy psychological state.
Changes in Sexual Life
A pregnancy after struggling with infertility can significantly affect a couple’s sexual life. A shift in women’s sexual behaviors is often accompanied by a tendency to overprotection due to fears of potential complications.
“I don’t have a sexual life anymore. As soon as I learned I was pregnant, my husband would not even touch me.” (P4, female factor, 4-years infertility)
“I am afraid of causing harm to the baby, so we don’t want it at all. It is fear, not reluctance, that makes us avoid sexual activity.” (P2, female factor, 1-year infertility)
Delivery Mode Preference
Delivery mode preferences should be based on medical advice and individual circumstances. However, for couples who have experienced infertility, overprotection thoughts can influence their decision-making process. It is imperative to understand the reasons behind preferences and provide comprehensive information during the prenatal period. This will assist couples in making an informed decision.
“I am insistent on a cesarean section because I’m afraid something will happen during labor and harm the baby.” (P15, female factor, 10-years infertility)
Disrupted Social Life
Experiencing a pregnancy after infertility can change one’s social life. Transitioning from infertility to pregnancy can also introduce new dynamics and challenges in social interaction, while the entire experience can be isolating in itself.
“Pregnancy left me socially withdrawn.” (P13, female factor, 8-years infertility)
“Fear of abortion prevented us from having a normal social life during pregnancy. I always had to rest in bed. Consequently, we were socially isolated.” (P8, female factor, 4-years infertility)
Maintaining Constant Check-ups
Couples who experience pregnancy after long-term infertility often maintain continuous perinatal check-ups due to overprotective thoughts and a desire for early detection of potential complications. Anxiety and cautiousness can often increase among women who have struggled with infertility, fearing something unexpected may occur during pregnancy.
“In the first trimester, the doctor told me there might be something wrong with his heartbeat, so I tried to schedule an appointment with another doctor that day or sooner, but I couldn’t find an appointment, so I went to a private hospital right away.” (P2, female factor, 1-year infertility)
“My perinatal care and follow-ups are carried out in two private hospitals, a state hospital, a city hospital, and a university hospital. In other words, I visit for perinatal check-ups in five different hospitals to ease my anxiety and heightened concern. I also remembered that I visited different doctors three days in a row.” (P1, female factor, 1-year infertility)
Theme 3: Overthinking
For many couples struggling with infertility, overthinking during pregnancy is a common phenomenon. The long-term process of infertility treatment and its low success rate often results in considerable uncertainty, disappointment, and anxiety, which can continue to develop during pregnancy and cause mental overload.
In psychology, escapism is the act of removing oneself from issues, stress, or discomforts in the present moment. A number of effective strategies were used by the women in this study.
“I did a lot of knitting, quilting, and embroidery. I was always excited, and I needed to distract my thoughts.” (P15, female factor, 10-years infertility)
Information Hunting
In this study, the process of seeking knowledge, guidance, and reassurance during pregnancy after infertility is known as information hunting.
“During my pregnancy, I downloaded all available pregnancy programs, consulted friends who were pregnant or had delivery experiences, and consulted medical professionals” (P11, female & male factors, 7-years infertility)
“I did a lot of research on the internet about my pregnancy. I even burned my food because of it. My close friends also gave me advice….” (P6, female factor, 1-year infertility)
The Future in Mind
A woman who overcomes infertility and gets pregnant experiences different emotions. Eventually, her fears of losing the pregnancy turn into joy and hope. The mother began to dream about a future with the baby she had been expecting for so long.
“The baby’s coming makes us happy; our happiness depends on our baby. I am very happy and excited. At some point after all these years, I’d like to hear a baby crying at home. The scent of the baby is what I want to smell.” (P5, female factor, 2-years infertility)
“I want to cuddle my baby as soon as possible and put her to sleep with me. Spending time with my baby and going for walks together is what I dream of all the time.” (P4, female factor, 4-years infertility)
Whirlpool of Thought
In this study, the whirlpool of thought does not just refer to the feelings that mothers experience during pregnancy but also the overwhelming thoughts they deal with.
“As time went on, I got more and more worried, and the little things started to affect me very much.” (P7, Male factors, 2-years infertility)
“My priorities changed even while the fetus was still in my abdomen. I became more nervous, and I feared the baby would not move. Everything was planned around the baby.” (P11, female & male factors, 7-years infertility)
Theme 4: Social Activity Changes
For the expecting mother, pregnancy after infertility can cause a variety of social changes. During pregnancy and motherhood, she experiences profoundly personal and emotionally stressful moments.
Care Expectation
An expectant mother has unique expectations when it comes to pregnancy after infertility. During this precious time of infertility, the woman may have heightened emotional and physical needs.
“It would be great to have my mom and husband with me during pregnancy.” (P12, unexplained, 3-years infertility)
“In infertility and during pregnancy, you only need attention and thank God my husband was always by my side.” (P11, female & male factors, 7-years infertility)
Self-Stigma
An unconscious negative belief or feeling of a woman about her infertility process and pregnancy may lead to self-stigma at the time.
“I felt a sense of responsibility towards my husband since I was the one with the infertile factor and responsible for our infertility. I thought I wouldn’t have any chance of getting pregnant.” (P6, female factor, 1-year infertility)
“For a long time prior to becoming pregnant, I felt inadequate and useless in many aspects of my life. Our past difficulties during the infertility treatment process really exhaust me, I think.” (P13, female factor, 8-years infertility)
Spousal Support
Spouse support is imperative to navigating from infertility to a pregnancy process. In this study, most women reported their husbands supported them financially and emotionally during pregnancy.
“My husband liked me much better and started paying more attention to me after getting pregnant. Thank God, he helped me with house chores and didn’t make me tired doing them.” (P4, female factor, 4-years infertility)
“My husband is the most supportive person in my life. I may have talked a lot about him, but he really is my biggest supporter. I feel stronger when he is beside me; he is my source of strength.” (P1, female factor, 1-year infertility)
In this study, participants stated that they experience a variety of mixed emotions, which lead to a feeling of overwhelming following infertility treatment and during pregnancy. Our study identified four dominant themes: Overemotional Burden, Overprotection, Overthinking, and Social Activity Changes. Our results show that, pregnancy after long-term infertility treatments often results in roller-coaster emotions, fear, anxiety, and hopelessness in mothers. According to mothers’ reports, moments during pregnancy they caused mothers anxiety in different trimesters. They also mentioned feeling relieved and emotionally inspired by becoming mothers. The study conducted by Bovin et al. in 2023 showed that approximately 12% of women with infertility mentioned the words anxious and worried, and 8% mentioned disappointment as the most frequent words to describe their feelings even after pregnancy (Boivin et al., 2023 ). Swanson et al. in 2021 also describe the infertility process as full of a roller coaster of emotions and feelings. It is described that the infertility treatment process is characterized by a period of sadness and grief, followed by some renewed sense of hope after getting successful results (Swanson & Braverman, 2021 ).
According to our study, overprotection is reported as a common reaction among pregnant women during interviews. Fear of loss, a desire to safeguard, and long-awaited expectations of a baby can lead to overprotective attitudes, which are reflected in their sexual and social lives adversely and in the perinatal care process. It is also possible for such overprotection to impact the preferred mode of delivery to ensure the baby’s safety. In our study, mothers report decreasing or withdrawing from sexual activity during pregnancy due to fears that they may harm the baby, cause miscarriage, or adversely affect the pregnancy. Mothers also reported social isolation due to their fears of miscarriage or complications during pregnancy. According to our results, mothers need frequent medical check-ups and continuous monitoring to ensure their babies’ health and detect potential complications early to protect their fetuses. According to a study conducted by Fukui in 2021, mother-to-infant bonding scores were positively related to perceived maternal overprotective attitude in late pregnancy (Fukui et al., 2021 ). However, a study conducted by Ohara in 2018 showed that excessive overprotection sense during pregnancy could be determined as a cause of bonding failure during pregnancy. When a mother exhibits overprotective behavior during pregnancy, she generally spends more time in the caring process. As a result, she may not have enough time to establish a motherhood role during pregnancy (Ohara et al., 2018 ). A study conducted by Phan et al. in 2021 reported that approximately 30% of pregnant women had no sexual activity during their pregnancy. Pregnant women in this study were most concerned about infection and damage to the fetus (Phan et al., 2021 ).
In our study, pregnant women described adverse changes in their social life which introduce new dynamics and challenges to their social interaction. A study conducted in 2016 by Velikonja et al. reported that women who get pregnant with assisted reproductive technologies are more likely to be socially marginalized. They also reported greater positive emotions and greater life satisfaction as the pregnancy progressed despite experiencing more medical challenges during the pregnancy (Velikonja et al., 2016 ).
According to our results, mothers experiencing pregnancy following long-term infertility tend to choose delivery modes based on their overprotective attitudes. In 2015, Reichelt et al. reported that the Cesarean rate was significantly higher in pregnancy after infertility than in spontaneous pregnancy compared to 20 years ago (Reichelt et al., 2015 ). A study by Chien et al. in 2015 reported that infertility treatment significantly influences mothers’ decisions about delivery modes. They also found that women who get pregnant with the In vitro fertilization method (IVF) may consider their fetus to be more vulnerable, and a cesarean delivery may be considered a low-risk method for the baby’s safety (Chien et al., 2015 ).
Overthinking in this study highlights how women who experience infertility always struggle with pregnancy-related thoughts. During the infertility treatment period, women may experience uncertainty, disappointment, and anxiety Several times. This condition can even cause psychological overload and mental exhaustion during pregnancy. Mothers in our study mentioned doing handicrafts such as knitting as a way to escape overthinking. Pedro, in 2015, identified escapism as a successful strategy for avoiding overthinking regarding infertility, pregnancy, and delivery in infertile women. Infertile women in this study describe escapism as a way to avoid thinking about anything else except their activities (Pedro, 2015 ). In our study, mothers mentioned they are always in the middle of information hunting online, in person, or consulting resources, even for the most straightforward pregnancy-related questions. A study conducted by Brochu et al. in 2019 reported that approximately 90% of infertile individuals surf the internet for information about infertility treatment processes and attempt to find more mental and medical support (Brochu et al., 2019 ). We believe that overthinking during pregnancy can be calming and exciting, especially when dreaming about the baby. However, when it is exaggerated, it can lead to overwhelming stress and anxiety in mothers. Mothers in our study shared their most precious dreams of holding their new baby after a challenging infertility journey. In our study, it was observed that that most infertile couples think about their future with their expected baby at least once a day.
Pregnancy after infertility results in various social changes for women (Boulet et al., 2017 ). A woman’s emotional experience of infertility and her various concerns and experiences during pregnancy adversely affect her mental health and contribute to the stigma attached to infertility (Zargar et al., 2023 ). In our study, women with female factor infertility often suffer from self-stigma and low self-esteem. According to Lin et al. in 2020, women who experience infertility suffer from low self-confidence and feeling inadequate, which results in self-stigma (Lin et al., 2022 ). In this study, mothers describe spousal support as an essential support system to overcome infertility challenges. In addition, they reported a higher level of mental support following pregnancy, as well as assisting with household chores and other daily activities. According to Choi et al. in 2023, spousal support significantly reduces stress levels in women with infertility. Women with a supportive husband are more likely to develop a more positive attitude towards infertility treatment and can also cope more effectively with infertility challenges (Choi & Moon, 2023 ).
Limitations
The study has limitations, despite providing valuable insight into women’s emotional challenges after infertility. The small sample size limits generalizability of results, since qualitative research inherently cannot be generalized to a broader population. Additionally, a stratified thematic analysis based on factors such as age group, education level, cause of infertility, and number of previous attempts was not feasible due to the high level of variability among the women included in the study. A more nuanced understanding of the diverse experiences would have been possible. A qualitative study involving spouses, family members, and healthcare professionals can provide valuable insight into the emotional challenges pregnant women face after infertility from multiple perspectives. A better understanding of the complexities of this experience could lead to more comprehensive support systems and interventions to help women who are experiencing these emotional challenges.
Pregnancy after infertility is a unique and emotionally charged experience for women, encompassing a spectrum of feelings that can be difficult to express. Our study results show four dominant themes which illustrate women’s complex emotional experiences and coping strategies during pregnancy. In this study, Over Emotional Burden, Overprotection, Overthinking, and Social Activity Changes were mentioned as the most common psychological concerns during pregnancy after infertility. Study results suggest healthcare providers who interact directly with pregnant women should be aware of these emotional burdens to understand mothers better and counsel them more effectively. Midwives, psychologists, and psychiatrists should also be more attentive to mothers’ emotions and provide coping mechanisms. This will enable mothers to experience their pregnancy with fewer possible adverse effects on both mother and fetus. However, research on infertile women’s emotional reactions and mental reactions during pregnancy is still limited. It may result from infertile mothers often concealing their emotions, ideas, and beliefs during pregnancy because they sacrifice themselves for the expected baby. This study can provide a starting point for further qualitative and quantitative studies on the psychological burden of pregnant women who experience infertility for a long time.
Data availability
The data supporting the findings of this study are available upon reasonable request.
Annells, M. (1996). Hermeneutic phenomenology: Philosophical perspectives and current use in nursing research. Journal of Advanced Nursing, 23 (4), 705–713.
Article PubMed Google Scholar
Bakhtiyar, K., Beiranvand, R., Ardalan, A., Changaee, F., Almasian, M., Badrizadeh, A., Bastami, F., & Ebrahimzadeh, F. (2019). An investigation of the effects of infertility on women’s quality of life: A case-control study. BMC Women’s Health, 19 (1), 1–9.
Article Google Scholar
Boivin, J., Oguz, M., Duong, M., Cooper, O., Filipenko, D., Markert, M., Samuelsen, C., & Lenderking, W. R. (2023). Emotional reactions to infertility diagnosis: Thematic and natural language processing analyses of the 1000 dreams survey. Reproductive BioMedicine Online, 46 (2), 399–409.
Borumandnia, N., Majd, H. A., Khadembashi, N., & Alaii, H. (2022). Worldwide trend analysis of primary and secondary infertility rates over past decades: A cross-sectional study. International Journal of Reproductive BioMedicine, 20 (1), 37.
PubMed PubMed Central Google Scholar
Boulet, S. L., Smith, R. A., Crawford, S., Kissin, D. M., & Warner, L. (2017). Health-related quality of life for women ever experiencing infertility or difficulty staying pregnant. Maternal and Child Health Journal, 21 , 1918–1926.
Article PubMed PubMed Central Google Scholar
Brochu, F., Robins, S., Miner, S. A., Grunberg, P. H., Chan, P., Lo, K., Holzer, H. E., Mahutte, N., Ouhilal, S., & Tulandi, T. (2019). Searching the internet for infertility information: A survey of patient needs and preferences. Journal of Medical Internet Research, 21 (12), e15132.
Chien, L. Y., Lee, Y. H., Lin, Y. H., & Tai, C. J. (2015). Women who conceived with infertility treatment were more likely to receive planned cesarean deliveries in Taiwan. Human Fertility, 18 (2), 141–148.
Choi, Y., & Moon, S. H. (2023). Types and characteristics of stress coping in women undergoing infertility treatment in Korea. International Journal of Environmental Research and Public Health, 20 (3), 2648.
Clarke, V., & Braun, V. (2017). Thematic analysis. The Journal of Positive Psychology, 12 (3), 297–298.
Crespo, E., & Bestard, J. (2016). Psychosocial needs of women and their partners after successful assisted reproduction treatment in Barcelona. Reproductive Biomedicine & Society Online, 3 , 90–99.
Cypress, B. S. (2017). Rigor or reliability and validity in qualitative research: Perspectives, strategies, reconceptualization, and recommendations. Dimensions of Critical care Nursing, 36 (4), 253–263.
Dornelles, L., Maccallum, F., Lopes, R., Piccinini, C. A., & Passos, E. (2016). The experience of pregnancy resulting from assisted Reproductive Technology (ART) treatment: A qualitative Brazilian study. Women and Birth, 29 (2), 123–127.
Fainberg, J., & Kashanian, J. A. (2019). Recent advances in understanding and managing male infertility. F1000Research, 8 .
Francis, J. J., Johnston, M., Robertson, C., Glidewell, L., Entwistle, V., Eccles, M. P., & Grimshaw, J. M. (2010). What is an adequate sample size? Operationalising data saturation for theory-based interview studies. Psychology and Health, 25 (10), 1229–1245.
Fukui, N., Motegi, T., Watanabe, Y., Hashijiri, K., Tsuboya, R., Ogawa, M., Sugai, T., Egawa, J., Enomoto, T., & Someya, T. (2021). Perceived parenting before adolescence and parity have direct and indirect effects via depression and anxiety on maternal–infant bonding in the perinatal period. Psychiatry and Clinical Neurosciences, 75 (10), 312–317.
Guba, E. G., & Lincoln, Y. S. (1981). Effective evaluation: Improving the usefulness of evaluation results through responsive and naturalistic approaches . Jossey-Bass.
Google Scholar
Gunawan, J. (2015). Ensuring trustworthiness in qualitative research. Belitung Nursing Journal, 1 (1), 10–11.
Heidegger, M. (1996). Being and time: A translation of Sein Und Zeit . SUNY.
Hope, D. L., & King, M. A. (2022). The ‘so what’of reporting guidelines (Vol. 30, pp. 91–92). Oxford University Press UK.
Huang, M. Z., Sun, Y. C., Gau, M. L., Puthussery, S., & Kao, C. H. (2019). First-time mothers’ experiences of pregnancy and birth following assisted reproductive technology treatment in Taiwan. Journal of Health Population and Nutrition, 38 , 1–11.
Kianfar, F., Mohammadi, K., Zahrakar, K., & Gica, N. (2023). Experience of women with infertility: A qualitative study. Current Psychology , 1–11.
Leung, L. (2015). Validity, reliability, and generalizability in qualitative research. Journal of Family Medicine and Primary care, 4 (3), 324.
Lin, Y. T., Wang, A. W., Wei, S., Hong, J. S., & Hsu, W. Y. (2022). The relationship between infertility family stigma, self-stigma and psychological well-being in female first-visit patients at a reproductive medicine center in Taiwan. Health Psychology Report, 9 (1).
Maehara, K., Iwata, H., Kimura, K., & Mori, E. (2022). Experiences of transition to motherhood among pregnant women following assisted reproductive technology: A qualitative systematic review. JBI Evidence Synthesis, 20 (3), 725–760.
McMahon, C. A., Boivin, J., Gibson, F. L., Fisher, J. R., Hammarberg, K., Wynter, K., & Saunders, D. M. (2011). Older first-time mothers and early postpartum depression: A prospective cohort study of women conceiving spontaneously or with assisted reproductive technologies. Fertility and Sterility, 96 (5), 1218–1224.
Ohara, M., Nakatochi, M., Okada, T., Aleksic, B., Nakamura, Y., Shiino, T., Yamauchi, A., Kubota, C., Morikawa, M., & Murase, S. (2018). Impact of perceived rearing and social support on bonding failure and depression among mothers: A longitudinal study of pregnant women. Journal of Psychiatric Research, 105 , 71–77.
Olma, İ. A., & Bir, K. (2018). Becoming a mother after infertility: a theoretical analysis.
Pedro, A. (2015). Coping with infertility: An explorative study of South African women’s experiences .
Phan, T. C., Hoang, L. B., Tran, T. K., Pham, T. T., Bui, A. V., Dao, H. T., Ngo, T. V., & Tran, C. D. (2021). Fear-related reasons for avoiding sexual intercourse in early pregnancy: A cross-sectional study. Sexual Medicine, 9 (6), 100430–100430.
Plager, K. (1994). Hermeneutic phenomenology. In Interpretive phenomenology: Embodiment, caring, and ethics in health and illness (pp. 65–83).
Reichelt, J., Kyvernitakis, I., Misselwitz, B., Hadji, P., Schmidt, S., & Kalder, M. (2015). A population based evaluation of the mode of delivery in association with infertility treatment from 1990–2012. Zeitschrift für Geburtshilfe und Neonatologie, 219 (01), 37–44.
Renzi, A., Fedele, F., & Di Trani, M. (2023a). Assisted reproductive treatments, quality of life, and alexithymia in couples . Healthcare.
Book Google Scholar
Renzi, A., Mariani, R., Fedele, F., Maniaci, V. G., Petrovska, E., D’Amelio, R., Mazzoni, G., & Di Trani, M. (2023b). Women’s narratives on infertility as a traumatic event: An Exploration of emotional processing through the referential activity linguistic program . Healthcare.
Rodriguez, A., & Smith, J. (2018). Phenomenology as a healthcare research method. Evidence-Based Nursing, 21 (4), 96–98. https://doi.org/10.1136/eb-2018-102990
Swanson, A., & Braverman, A. M. (2021). Psychological components of infertility. Family Court Review, 59 (1), 67–82.
Taebi, M., Kariman, N., Montazeri, A., & Majd, H. A. (2021). Infertility stigma: A qualitative study on feelings and experiences of infertile women. International Journal of Fertility & Sterility, 15 (3), 189.
Velikonja, V. G., Lozej, T., Leban, G., Verdenik, I., & Bokal, E. V. (2016). The quality of life in pregnant women conceiving through in vitro fertilization. Slovenian Journal of Public Health, 55 (1), 1–10.
Yao, H., Chan, C. H. Y., & Chan, C. L. W. (2018). Childbearing importance: A qualitative study of women with infertility in China. Research in Nursing & Health, 41 (1), 69–77.
Zargar, M., Sayyah, M., Nikbakht, R., & Abdipour, Z. (2023). Comparison of psychological disorders during and after pregnancies caused by assisted reproductive treatments and spontaneous pregnancies. Central Nervous System Agents in Medicinal Chemistry (Formerly Current Medicinal Chemistry-Central Nervous System Agents), 23 (3), 204–212.
Download references
Acknowledgements
We sincerely thank the participants for sharing with us all of their experiences, no matter how positive or negative, hoping that no one will suffer as they did.
Open access funding provided by the Scientific and Technological Research Council of Türkiye (TÜBİTAK). This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and affiliations.
Faculty of Health Sciences, Department of Midwifery, Sakarya University, Esentepe Campus, 54100, Serdivan/Sakarya, Türkiye
Parisa Hadavibavili & Yasemin Hamlaci Başkaya
Institute of Health Science, Department of Midwifery, Sakarya University, Sakarya, Türkiye
Parisa Hadavibavili
Training and Research Hospital, Sakarya University, Sakarya, Türkiye
Gamze Bayazi̇t
Department of Obstetrics and Gynaecology, Training and Research Hospital, Sakarya University, Sakarya, Türkiye
Arif Serhan Cevrioğlu
You can also search for this author in PubMed Google Scholar
Contributions
Study design: PHB, YHB.
Data collection: GB.
Data analysis: PHB, YHB.
Study supervision: YHB, ASC.
Manuscript writing: PHB, YHB.
Critical revisions for important intellectual content: PHB, YHB, ASC.
Corresponding author
Correspondence to Parisa Hadavibavili .
Ethics declarations
Conflict of interest.
No conflict of interest has been declared by the authors.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ .
Reprints and permissions
About this article
Hadavibavili, P., Hamlaci Başkaya, Y., Bayazi̇t, G. et al. Women’s emotional roller coasters during pregnancy as a consequence of infertility: a qualitative phenomenological study. Curr Psychol (2024). https://doi.org/10.1007/s12144-024-06158-3
Download citation
Accepted : 15 May 2024
Published : 30 May 2024
DOI : https://doi.org/10.1007/s12144-024-06158-3
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Infertility (MeSH D007246)
- Pregnancy (MeSH D011247)
- Qualitative research (MeSH D036301)
- Mental health (MeSH D008603)
- Fertility (MeSH D005298)
- Find a journal
- Publish with us
- Track your research
IMAGES
VIDEO
COMMENTS
The American Psychological Association's (APA) Ethical Principles of Psychologists and Code of Conduct (hereinafter referred to as the Ethics Code) consists of an Introduction, a Preamble, five General Principles (A-E) and specific Ethical Standards.The Introduction discusses the intent, organization, procedural considerations, and scope of application of the Ethics Code.
The research team. There are examples of researchers being intimidated because of the line of research they are in. The institution in which the research is conducted. salso suggest there are 4 main ethical concerns when conducting SSR: The research question or hypothesis. The treatment of individual participants.
The APA Code of Ethics comprises two key elements: Principles: the underlying ethical foundation on which psychologists should base their practices and decisions, whether they work in mental health, research, or business. Standards: enforceable rules for ethical conduct, the violation of which can have professional and legal ramifications.
A systematic review of empirical research into ethical decision-making in clinical psychology and related fields was therefore indicated, with the aim of summarising the literature available. Although there are some important differences between professions in terms of the training backgrounds and regulatory frameworks, the search was extended ...
For psychology practitioners, the BPS has established Practice Guidelines (BPS 2017 ). In common with the APA code, the BPS Code of Ethics and Conduct sets out four top-level principles: respect, competence, responsibility, and integrity. The Code of Human Research Ethics, which sits under the Code of Ethics and Conduct, similarly sets out four ...
Sangeeta Panicker, PhD, is director of the Research Ethics Office in the Science Directorate of the American Psychological Association. She received her doctorate in cognitive neuroscience from The Catholic University of America, in Washington, DC. She also has Masters' degrees in Psychopharmacology from the University of Cincinnati and in Clinical Psychology from the University of Bombay.
Volume 1: Moral Foundations and Common Themes. Volume 2: Practice, Teaching, and Research. Discussions of ethics in psychology often focus primarily on misconduct, punishment, and legal sanctions, and too often ignore aspirations, values, principles, and virtues. The net effect of this unbalanced approach creates an atmosphere in which ...
Ethics (PSI, 2003).The British Psychological Society is currently revising,The Ethical Principles for Conducting Research with Human Participants (BPS, 1978; q.v.), which share many similarities with the common codes. 2.2 Ethical Considerations in Psychological Research It is important to understand the interdependence of ethics and the research
Ethical decision making in psychological research requires knowledge of the rules and regulations governing its practices as well as the ability to identify and resolve complex ethical conflicts. Researchers use several sources of information when faced with ethical questions, including their knowledge of research and methodology and the advice of colleagues, team members, and institutional ...
The responsible conduct of psychological research is critical to improving our understanding of developmental processes, creating effective treatments and informing public policy. At its most basic level, the study and practice of research ethics entails translating core ethical principles, standards, and ideals into effective and ethical research methods tailored to the characteristics of the ...
BPS Code of Human Research Ethics. This code lays out a set of general principles that are applicable to all research contexts and which are intended to cover all research with human participants. The attached document, written by the BPS Working Party on Ethical Guidelines for Psychological Research and updated in April 2021, is designed to ...
Ethical codes, such as those established by the American Psychological Association, are designed to protect the safety and best interests of those who participate in psychological research. Such guidelines also protect the reputations of psychologists, the field of psychology itself and the institutions that sponsor psychology research.
How the Classics Changed Research Ethics. Some of history's most controversial psychology studies helped drive extensive protections for human research participants. Some say those reforms went too far. Photo above: In 1971, APS Fellow Philip Zimbardo halted his classic prison simulation at Stanford after volunteer "guards" became abusive ...
Psychology Research Ethics. by By Saul McLeod published 2015. Ethics refers to the correct rules of conduct necessary when carrying out research. We have a moral responsibility to protect research participants from harm. However important the issue under investigation psychologists need to remember that they have a duty to respect the rights ...
Ethics in psychology and the mental health professions: Standards and cases. 3d ed. New York: Oxford Univ. Press. This is a classic, with clear coverage of essential issues and entertaining vignettes that illustrate important points. Pope, K. S., and M. Vasquez. 2011. Ethics in psychotherapy and counseling: A practical guide. 4th ed.
Conclusion. . One potentially important aspect of research ethics that garners rare mention in the literature is the professionalism of the researchers. Debate on the ethics of deception may be overlooking the impact of other mundane risks that may impact participants' thoughts and feelings more than deceptive manipulation per se.
Ethics in Psychological Research: Guidelines and Regulations Adam L. Fried and Kate L. Jansen; Chapter 4. Ethics and Regulation of Research With Nonhuman Animals ... Marc N. Coutanche, PhD, is an associate professor of psychology and research scientist in the Learning Research and Development Center at the University of Pittsburgh. Dr.
The Human Research Ethics Committee (HREC) - or other ethical review bodies - will review your research proposal to make a judgement on whether the risks are justified by the potential benefits. ... The APS Code of Ethics. The Australian Psychology Society is the professional body of choice for psychologists in Australia with over 27,000 ...
Revised on May 9, 2024. Ethical considerations in research are a set of principles that guide your research designs and practices. Scientists and researchers must always adhere to a certain code of conduct when collecting data from people. The goals of human research often include understanding real-life phenomena, studying effective treatments ...
This is primarily aimed at first- and second-year undergraduates interested in psychology, ethics in research methods, and quantitative research methods along with high school students and professionals with similar interests. Learn With PsycLearn Essentials.
This scrutiny of psycholegal research is likely to increase as the human rights culture develops in more countries, because courts applying human rights law often make findings that indirectly reflect on the field's research ethics as psychology's ethics and human rights law share the same foundation (Allan, 2013). The field therefore faces ...
A universal approach to data sharing in qualitative research proves impractical, emphasizing the necessity for adaptable, context-specific guidelines that acknowledge the methodology's nuances. Striking a balance between transparency and ethical responsibility requires tailored strategies and thoughtful consideration.
Case studies are in-depth investigations of a person, group, event, or community. Typically, data is gathered from various sources using several methods (e.g., observations & interviews). The case study research method originated in clinical medicine (the case history, i.e., the patient's personal history). In psychology, case studies are ...
Background Medical students, especially during the clinical years, are often exposed to breaches of safety and professionalism. These contradict personal and professional values exposing them to moral distress and to the dilemma of whether and how to act. Acting requires moral courage, i.e., overcoming fear to maintain one's core values and professional obligations. It includes speaking up ...
4. Respect confidentiality and privacy. Upholding individuals' rights to confidentiality and privacy is a central tenet of every psychologist's work. However, many privacy issues are idiosyncratic to the research population, writes Susan Folkman, PhD, in "Ethics in Research with Human Participants" (APA, 2000).
Studies have found that introverted individuals are more likely to experience social anxiety compared to their extroverted counterparts (Cain, 2012; Noya & Vernon, 2019). The quiet, reflective ...
The shared features principle builds on four terms: source objects, target objects, source features, and target features (for more on these terms and the conceptual account from which they derive, see De Houwer et al., 2019).The term 'object' is a general one that refers to many different stimuli: a person, a brand product, a nonsense word, or a social group.
Special issue of the APA journal Translational Issues in Psychological Science, Vol. 6, No. 3, September 2020. This special issue highlights some of the emerging ethical issues in psychological research with human participants and provides guidance for students, trainees, and seasoned professionals who are trying to do good science and to do it well.
Furthermore, following established reporting guidelines facilitates peer review by providing standardized criteria for assessing the validity and quality of qualitative research. In reporting qualitative research, the COREQ checklist emphasizes ethical considerations, such as ensuring participant privacy and providing a clear ethical rationale.